

Abstract
Background
The quick sequential organ failure assessment (qSOFA) score has recently been introduced to the emergency department (ED) and wards, and it predicted a higher number of deaths among patients with sepsis compared with baseline risk. However, studies about the application of the qSOFA score are limited in prehospital settings. Thus, this study aimed to assess the performance of prehospital qSOFA score in predicting the risk of mortality among patients with infection.
Methods
This single center, retrospective cohort study was conducted in a Japanese tertiary care teaching hospital between April 2016 and March 2017. We enrolled all consecutive adult patients transported to the hospital by ambulance and admitted to the ED due to a suspected infection. We calculated the prehospital qSOFA score using the first vital sign obtained at the scene by emergency medical service (EMS) providers. The primary outcome was in-hospital mortality. The Cox proportional hazards model was used to assess the association between prehospital qSOFA positivity and in-hospital mortality.
Results
Among the 925 patients admitted to the ED due to a suspected infection, 51.1% (473/925) were prehospital qSOFA-positive and 48.9% (452/925) were prehospital qSOFA-negative. The in-hospital mortality rates were 14.0% (66/473) in prehospital qSOFA-positive patients and 6.0% (27/452) in prehospital qSOFA-negative patients. The Cox proportional hazard regression model revealed a strong association between prehospital qSOFA score and in-hospital mortality (adjusted hazard ratio: 2.41, 95% confidence interval: 1.51–3.98; p <0.01).
Conclusions
Among the patients with suspected infection who were admitted at the ED, a strong association was observed between the prehospital qSOFA score and in-hospital mortality. In order to use this score in clinical practice, future study is necessary to evaluate how infection is suspected in the prehospital arena.
Introduction
Sepsis is a global health burden with high prevalence and mortality rates. The time intervals from the first medical contact to the diagnosis of sepsis and the initiation of treatments, particularly the rapid administration of antibiotic, were associated with lower mortality rates [1–4]. For an accurate and early identification of patients suspected with sepsis and for the improvement of patient outcomes, an international task force of experts redefined sepsis syndrome and introduced the quick sequential (sepsis-related) organ failure assessment (qSOFA) score for non-intensive care unit (ICU) setting in 2016 [5]. Seymour et al. and Sepsis-3 Task Force have reported that qSOFA in the emergency department (ED) and wards predicted a higher number of deaths compared with baseline risk [2], and they recommended that the “qSOFA criteria should be used outside of the ICU to prompt clinicians to further investigate for organ dysfunction and to initiate or escalate therapy as appropriate.”
Prehospital care of sepsis has attracted broad attention. Like prehospital interventions for other time-sensitive conditions, including cardiac arrest, acute myocardial infarction, and stroke, prehospital care of sepsis is a promising intervention that improves outcomes [6–9]. Several prehospital screening tools used for the identification of sepsis have been developed before the introduction of the qSOFA score. However, they lack accuracy [10–14]. As in the EDs and wards, the qSOFA score may be used in prehospital setting because of its simple scoring system that uses only vital signs. However, studies that have investigated the relationship between qSOFA in the prehospital setting and patient outcomes are limited [15–17].
To address the knowledge gap in the literature, we calculated the prehospital qSOFA score using the first vital sign obtained at the scene by emergency medical service (EMS) providers and investigated the association between prehospital qSOFA score and in-hospital mortality in our community. This study aimed to assess the performance of prehospital qSOFA score in predicting the risk of mortality among patients with infection.
Materials and methods
Ethics approval and consent to participate
The institutional review board of Okinawa Chubu Hospital approved the study protocol (H30-90). Because of the retrospective nature of this study and the de-identification of personal data, the board waived the need for informed consent.
Study design, setting, and patients
This was an observational study conducted at Okinawa Chubu Hospital, a tertiary care teaching hospital with 550 hospital beds and 14 ICU beds in Japan, between April 2016 and March 2017. We accepted patients who were transported from six EMS agencies in our district, with a population of approximately 460,000.
We examined the data of all adult (≥ 18 years) patients who were admitted to the ED by EMS agencies and were registered with the diagnosis name of an International Classification of Diseases, Tenth Revision (ICD-10) code indicative of infection (A00-B99, certain infectious and parasitic diseases; G00-05, neurologic infection; I30-32 and J38-40, endo/myocarditis; J00-06, J09-18, J20-22, J36, J40, and J85-86, respiratory infection; K35-37, appendicitis; K57, diverticulitis; K61, K63, K65, and K67, peritonitis and intestinal abscess; K75.0, liver abscess; K81 and K83, cholecystitis and cholangitis; L00-08, skin and soft tissue infections; M00-03 and M86, infective arthritis and osteomyelitis; N10 and N30, urinary tract infection; and N70-76, inflammatory disease of the female pelvic organ) on the electronic medical record between April 2016 and March 2017. In addition, because infection and sepsis are often undercoded, we also assessed for patients who received antibiotic treatments during their hospital stay.
We excluded patients whose EMS records were missing. Patients who did not receive antibiotics within 48 hours after ED arrival were also excluded because they were less likely to have severe bacterial infection. The other exclusion criterion was patients who had do-not-resuscitate (DNR) code prior to ED admission.
Data collection
The demographic information of the patients and related characteristics were obtained from in-hospital electronic medical records and paper-based EMS records. We collected data for analyses, which included age, sex, comorbidities, use of immunosuppressants, location prior to ED admission, prehospital and ED triage vital signs, laboratory data, primary site of infection, type of organisms, ICU admission, length of ICU stay, length of hospital stay, and prevalence of bacteremia and in-hospital mortality. We checked the presence of comorbidities that were categorized in the Charlson comorbidity index (CCI) [18]. Laboratory data included leucocyte count, hematocrit levels, platelet count, PT-INR, and serum sodium, potassium, CRP, glucose, and lactate levels. The primary site of infection was diagnosed by means of confirmation via clinical, radiological, and microbiological examinations. The type of organisms was determined based on various culture results. Bacteremia was diagnosed if we detected the same microorganisms from two sets of blood culture bottles.
Measurement of the primary exposure factors
The qSOFA score had three criteria: assigning one point for alteration in mental status (Glasgow coma scale [GCS] score <15), systolic blood pressure ≤ 100 mmHg, and respiratory rate ≥ 22/min, respectively. We calculated the prehospital qSOFA score using the first vital sign obtained at the scene by EMS providers. If the vital sign was not recorded at the scene, we adopted the first vital sign en route instead. For the prehospital evaluation of mental status, the Japanese EMS providers have adopted the Japan coma scale (JCS) instead of the GCS since its introduction in 1974 [19]. JCS has four main grades (grade 0: alert; grade 1: possible verbal response without any stimulation, not lucid; grade 2: possible eye-opening, verbal and motor response upon stimulation; and grade 3: no eye-opening and coma upon stimulation). Therefore, we count JCS grades 1, 2, and 3 as one point of the qSOFA for alteration in mental status. According to previous studies, we defined prehospital qSOFA positivity or negativity as the prehospital qSOFA score ≥ 2 or < 2, respectively [2, 5].
Outcome measures
The primary outcome measure was in-hospital all-cause mortality. The secondary outcomes were 28- and 90-day mortality as confirmed by follow-up visits after discharge.
Statistical analysis
Continuous data were presented as medians with interquartile range (IQR) and were compared using the Mann-Whitney U test. Categorical data were presented as proportions and were compared using Fisher’s exact test when appropriate. We used the Kaplan-Meier plots to describe the survival of prehospital qSOFA-positive and qSOFA-negative patients and to compare the survival curves with the log-rank test. Moreover, the Cox proportional hazards model was used in assessing the association between the prehospital qSOFA positivity and in-hospital mortality censored during the discharge day and 28 and 90 days after ED admission after adjusting for other risk factors of mortality. Based on a priori knowledge, the following variables were incorporated into the primary multivariable models: age, sex, presence of chronic health condition, and location prior to ED admission. We defined chronic health condition as congestive heart failure, dementia, chronic pulmonary disease, rheumatologic disease, mild liver disease, diabetes with complications, hemiplegia, renal disease, hematologic malignancy, moderate or severe liver disease, metastatic solid tumor, and AIDS/HIV, which were comorbidities of the CCI associated with prognosis [20, 21]. We considered the use of immunosuppressants as chronic health condition because it increases the risk of infection.
A subgroup analysis of in-hospital mortality was conducted to validate the interaction between subgroup factors and the prehospital qSOFA score. Subgroups were defined by age, sex, presence of chronic health condition, location prior to ED admission, and site of infection. We set the age threshold to 75 years or over according to the definition of elderly individuals in Japan. The site of infection was categorized as respiratory or other sites in accordance to prior study [22]. We used the Cox proportional hazard model for analyses after adjusting the same covariates used in the main group analysis except for the variable for stratification. All statistical analyses were performed using R (The R Foundation for Statistical Computing, ver. 3.2.4) and JMP Pro software (ver. 1.31, SAS Institute Inc., Cary, NC, the USA). All tests were two-tailed; p values < 0.05 were considered statistically significant.
Results
The flow diagram of patient recruitment is shown in Fig 1. From April 2016 to March 2017, a total of 1385 patients were admitted to the ED due to a suspected infection. Of these patients, 460 were excluded due to the following reasons: missing EMS record, lack of antibiotic treatment within 48 hours of ED arrival, and assignment of DNR code prior to ED admission. Finally, 925 patients were enrolled for our analyses. Among the 925 patients, 51.1% (473/925) and 48.9% (452/925) were positive and negative for prehospital qSOFA, respectively.
Fig 1. Flow diagram of patient recruitment.
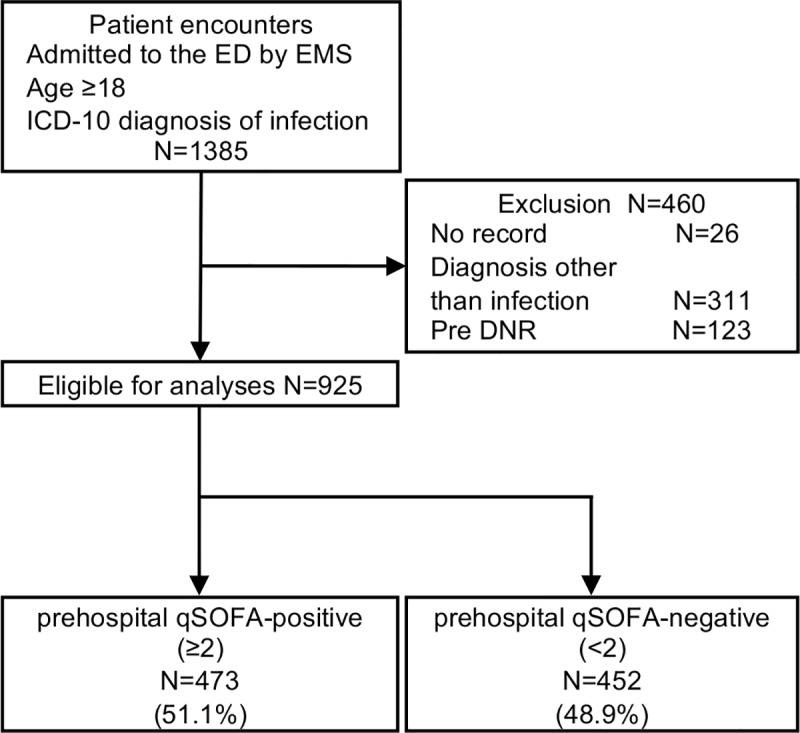
Pre DNR suggests patients who had do-not-resuscitate (DNR) code prior to ED admission. Abbreviations: ED, emergency department; EMS, emergency medical service; ICD-10, International Classification of Diseases, Tenth Revision; DNR, do-not-resuscitate; qSOFA, quick sequential organ failure assessment.
The demographic information of patients, characteristics at presentation, and hospital course after ED admission are summarized in Table 1 and S1 Table. Prehospital qSOFA-positive patients were slightly older than prehospital qSOFA-negative patients (prehospital qSOFA-positive: 82 [IQR 71–88] vs prehospital qSOFA-negative: 79 [IQR 67–86], p<0.01) and a higher number of patients were from a nursing home (prehospital qSOFA-positive: 40.6% [192/473] vs prehospital qSOFA-negative: 18.6% [84/452], p<0.01). No difference was observed between the two groups in terms of sex. Hemiplegia (prehospital qSOFA-positive: 27.9% [132/473] vs prehospital qSOFA-negative: 13.3% [60/452], p<0.01) and dementia (prehospital qSOFA-positive: 21.4% [101/473] vs prehospital qSOFA-negative: 10.8% [49/452], p<0.01) were observed more frequently in prehospital qSOFA-positive patients than in prehospital qSOFA-negative patients. Body temperature was similar between the two groups. Laboratory results were similar except for PT-INR (prehospital qSOFA-positive: 1.13 [IQR: 1.04–1.25] vs prehospital qSOFA-negative: 1.08 [IQR: 1.02–1.18], p<0.01), serum sodium levels (prehospital qSOFA-positive: 135 [IQR: 131–139] vs prehospital qSOFA-negative: 136 [IQR: 132–138], p<0.05), serum potassium levels (prehospital qSOFA-positive: 4.1 [IQR: 3.7–4.5] vs prehospital qSOFA-negative: 3.9 [IQR: 3.5–4.3], p<0.01), and lactic acid levels (prehospital qSOFA-positive: 1.8 [IQR: 1.1–3.3] vs prehospital qSOFA-negative: 1.5 [IQR: 1.1–2.2], p<0.01) between the two groups. Site of infection, type of organisms, and bacteremia did not significantly differ between the two groups. The number of prehospital qSOFA-positive patients who were admitted in the ICU was slightly higher than that of prehospital qSOFA-negative patients. However, no significant difference was observed between the two groups (prehospital qSOFA-positive: 11.0% [52/473] vs prehospital qSOFA-negative: 8.6% [39/452], p = 0.269).
Table 1. Demographic data and characteristics of patients.
| prehospital qSOFA | prehospital qSOFA | ||
|---|---|---|---|
| negative (<2) | positive (≥2) | ||
| (N = 452) | (N = 473) | p value | |
| Age (median [IQR]) | 79 [67, 86] | 82 [71, 88] | <0.01 |
| Male (%) | 227 (50.2) | 242 (51.2) | 0.79 |
| Comorbidities (%) | |||
| Diabetes with complication | 35 (7.7) | 24 (5.1) | 0.11 |
| Congestive heart failure | 14 (3.1) | 17 (3.6) | 0.72 |
| Chronic pulmonary disease | 46 (10.2) | 46 (9.7) | 0.83 |
| Mild liver disease | 11 (2.4) | 9 (1.9) | 0.65 |
| Moderate-severe liver disease | 13 (2.9) | 12 (2.5) | 0.84 |
| Renal disease | 20 (4.4) | 20 (4.2) | 1.00 |
| Rheumatologic disease | 20 (4.4) | 24 (5.1) | 0.76 |
| Hemiplegia or paraplegia | 60 (13.3) | 132 (27.9) | <0.01 |
| Dementia | 49 (10.8) | 101 (21.4) | <0.01 |
| Hematologic malignancy | 8 (1.8) | 14 (3.0) | 0.28 |
| Metastatic solid tumor | 17 (3.8) | 18 (3.8) | 1.00 |
| AIDS/HIV | 1 (0.22) | 0 (0) | 0.49 |
| Immunosuppressant | 39 (8.6) | 27 (5.7) | 0.10 |
| Location (%) | <0.01 | ||
| Home | 314 (69.5) | 232 (49.1) | |
| Nursing home | 84 (18.6) | 192 (40.6) | |
| Medical faculty | 54 (12.0) | 49 (10.4) | |
| Prehospital vital (median [IQR]) | |||
| Systolic blood pressure, mmHg | 130 [120, 150] | 120 [100, 140] | <0.01 |
| Heart rate, /min | 98 [84, 112] | 102 [88, 120] | <0.01 |
| Respiratory rate, /min | 24 [20, 30] | 30 [24, 32] | <0.01 |
| Japan Coma Scale | 0 [0, 0] | 1 [1, 2] | <0.01 |
| Glasgow Coma Scale | 15 [15, 15] | 10 [8, 13] | <0.01 |
| Body temperature, Celsius | 37.7 [36.9, 38.6] | 37.9 [37.0, 38.9] | <0.01 |
| ED triage vital (median [IQR]) | |||
| Systolic blood pressure, mmHg | 134 [120, 150] | 120 [100, 140] | <0.01 |
| Heart rate, /min | 98 [85, 110] | 103 [88, 120] | <0.01 |
| Respiratory rate, /min | 22 [20, 27.75] | 24 [20, 30] | <0.01 |
| Glasgow Coma Scale | 15 [13, 15] | 11 [9, 14] | <0.01 |
| Body temperature, Celsius | 37.7 [37.0, 38.6] | 37.9 [37.0, 38.9] | 0.29 |
| Bacteremia (%) | 75 (16.6) | 81 (17.1) | 0.86 |
| ICU Admission (%) | 39 (8.6) | 52 (11.0) | 0.27 |
| ICU LOS (median [IQR]) | 0 [0, 0] | 0 [0, 0] | 0.24 |
| Hospital LOS (median [IQR]) | 11 [7, 19] | 12 [8, 18.5] | 0.56 |
The prehospital qSOFA score was assessed using the first vital sign obtained at the scene and was taken by EMS providers.
Abbreviation: qSOFA, quick sequential organ failure assessment; IQR, interquartile range; ED, emergency department; ICU, intensive care unit; LOS, length of stay; EMS, emergency medical service.
The primary and secondary outcomes are shown in Fig 2 and Table 2. Overall, the in-hospital mortality rate was 10.1% (93/925), and 14.0% (66/473) of prehospital qSOFA-positive patients died compared to 6.0% (27/452) of prehospital qSOFA-negative patients on discharge day. With regard to the secondary outcomes, 15.9% (61/384) of prehospital qSOFA-positive patients died compared to 6.3% (23/363) of prehospital qSOFA-negative patients 28 days after ED admission, and 24.4% (83/340) of prehospital qSOFA-positive patients died compared to 10.3% (34/329) of prehospital qSOFA-negative patients 90 days after ED admission. The Kaplan-Meier plots of survival showed a significant difference between the two groups (p <0.001). The Cox proportional hazard regression model revealed that prehospital qSOFA positivity has a strong association with in-hospital mortality (unadjusted hazards ratio [HR]: 2.45, 95% confidence interval [CI]: 1.58–3.92; p <0.01). After adjusting for confounders (age, gender, chronic health condition, and location prior to ED admission), prehospital qSOFA positivity still has a strong association with in-hospital mortality (adjusted HR: of 2.41, 95% CI: 1.51–3.98; p <0.01).
Fig 2. Kaplan-Meier curves stratified as prehospital qSOFA-positive or prehospital qSOFA-negative.

A, In-hospital mortality censored at the discharge day. B, 28-day mortality censored 28 days after ED admission. C, 90-day mortality censored 90 days after ED admission. The vertical tick marks on the curves represent censoring due to survival discharge. p value < 0.01 (log-rank test). Abbreviation: qSOFA, quick sequential organ failure assessment; ED, emergency department.
Table 2. Unadjusted & adjusted hazard ratios for mortality in patients who were positive for prehospital qSOFA.
| HR (95% CI) | p value | |
|---|---|---|
| In-hospital mortality | ||
| Unadjusted | 2.45 (1.58–3.92) | <0.01 |
| Adjustment 1 | 2.39 (1.53–3.84) | <0.01 |
| Adjustment 2 | 2.51 (1.58–4.13) | <0.01 |
| Adjustment 3 | 2.41 (1.51–3.98) | <0.01 |
| 28-day mortality | ||
| Unadjusted | 2.55 (1.60–4.22) | <0.01 |
| Adjustment 1 | 2.48 (1.55–4.10) | <0.01 |
| Adjustment 2 | 2.58 (1.59–4.32) | <0.01 |
| Adjustment 3 | 2.39 (1.46–4.03) | <0.01 |
| 90-day mortality | ||
| Unadjusted | 2.36 (1.58–3.59) | <0.01 |
| Adjustment 1 | 2.30 (1.54–3.51) | <0.01 |
| Adjustment 2 | 2.50 (1.65–3.86) | <0.01 |
| Adjustment 3 | 2.35 (1.54–3.65) | <0.01 |
The primary analysis was performed with the Cox proportional hazard regression model and in-hospital mortality censored at the discharge day and 28 and 90 days after ED admission.
Adjustment 1 was for the demographic characteristics of patients (age and sex).
Adjustment 2 was for the demographic characteristics of patients, as previously mentioned, and presence of any chronic health condition (congestive heart failure, dementia, chronic pulmonary disease, rheumatologic disease, mild liver disease, diabetes with complications, hemiplegia, renal disease, hematologic malignancy, moderate or severe liver disease, metastatic solid tumor, AIDS/HIV, and use of immunosuppressants).
Adjustment 3 was for the demographic characteristics of patients and chronic health condition, as previously mentioned, and location prior to ED admission (home, nursing home, and medical facility).
Abbreviation: qSOFA, quick sequential organ failure assessment; HR, hazard ratio; CI, confidence interval; ED, emergency department.
The association between prehospital qSOFA positivity and in-hospital mortality remained significant among the pre-specified subgroups of patients except for the subgroup of patients with respiratory infection. In 478 patients with respiratory infection, the association was not significant (adjusted HR: 1.67, 95% CI: 0.85–3.44; p = 0.14). The details of the subgroup analyses are shown in Table 3.
Table 3. Hazard ratios for in-hospital mortality in patients who are positive for prehospital qSOFA stratified as pre-specified subgroups.
| Number of case | HR (95% CI) | p value | |
|---|---|---|---|
| Age | |||
| < 75 years | 308 | 3.98 (1.49–12.57) | <0.01 |
| ≥ 75 years | 617 | 1.85 (1.06–3.38) | <0.05 |
| Sex | |||
| Male | 469 | 1.94 (1.03–3.80) | <0.05 |
| Female | 456 | 3.49 (1.59–8.51) | <0.01 |
| Chronic health condition | |||
| Yes | 546 | 2.09 (1.22–3.73) | <0.01 |
| No | 379 | 2.36 (1.04–5.84) | <0.05 |
| Location prior to ED admission | |||
| Home | 546 | 2.06 (1.11–3.94) | <0.05 |
| Nursing home or medical facility | 379 | 3.42 (1.55–8.74) | <0.01 |
| Site of infection | |||
| Respiratory | 478 | 1.67 (0.85–3.44) | 0.14 |
| Others | 447 | 3.30 (1.66–7.09) | <0.01 |
Subgroup analyses were performed with the Cox proportional hazard regression model and in-hospital mortality censored at the discharge day. The demographic characteristics of patients, chronic health condition, and location prior to ED admission were incorporated into the multivariable models except for each stratification variable.
Abbreviation: qSOFA, quick sequential organ failure assessment; HR, hazard ratio; CI, confidence interval; ED, emergency department.
Discussion
In this single center retrospective cohort study of 925 ED patients with suspected infection, a strong association was observed between prehospital qSOFA score and in-hospital mortality (adjusted HR: 2.41, 95% CI: 1.51–3.98; p <0.01). The association remained consistent between prehospital qSOFA and other outcomes (28- and 90-day mortality) and among various subgroups.
Currently, several studies have investigated the performance of the prehospital qSOFA score [15–17, 23–26]. Vaittinada Ayar P et al. have reported that in-hospital mortality rate was significantly higher in patients with prehospital qSOFA positivity among 332 patients suspected with infection (prehospital qSOFA-positive: 41% [55/133] vs prehospital qSOFA-negative: 18% [36/199], p<0.001) [24]. Shu E et al. have evaluated the prehospital qSOFA score of patients who were brought by EMS personnel and analyzed the prognostic value of the prehospital qSOFA score among 428 patients diagnosed with infection. They showed that an increase in prehospital qSOFA score was associated with in-hospital mortality (positive likelihood ratio 3.99, 95% CI: 2.21–7.21) [25]. In both of these studies, no covariate adjustments were made.
Our study results were in accordance with those of prior studies and have validated the association between the prehospital qSOFA score and mortality rate using the Cox proportional hazard regression model with covariate adjustments. We assessed the proportional hazard assumption in the primary analysis. Our study had a larger sample size (925 patients) than prior studies. In addition, subgroup analyses confirmed that the association between the prehospital qSOFA score and in-hospital mortality was consistent across different subgroups. In patients with respiratory infection, qSOFA might overly assess the risk of mortality. Most patients with respiratory infection had elevated respiratory rate and thus had increased qSOFA scores due to respiratory infection regardless of severity (adjusted HR: 1.67, 95% CI: 0.85–3.44; p = 0.14). Importantly, 6.0% (27/452) of prehospital qSOFA-negative patients died in our study. Although the prehospital qSOFA score had a significant association with mortality among patients with suspected infection, it had low sensitivity for mortality [5, 27–30].
The need to recognize infected patients in the prehospital setting was more and more emphasized. In April 2018, the Surviving Sepsis Campaign Task Force published the new revision of the sepsis bundle (hour-1 bundle), which recommends the complete initiation of resuscitation and treatments of patients with sepsis within 1 hour from the time of triage in the ED [31, 32]. Once EMS providers identified patients with infection before their arrival at the hospital, prehospital qSOFA score was an effective tool in estimating the mortality rate.
Our study had several limitations. First, it was a single-center, retrospective study. Therefore, the results cannot be generalized. Second, due to the difference between JCS and GCS, a GCS score < 15 may be misclassified as JCS 0, such as that in a patient who had good verbal and motor response without any stimulation but who was unable to open his/her eyes. However, this misclassification was a bias that acts on reducing the mortality difference between the prehospital qSOFA-positive and qSOFA-negative groups. However, the association between the prehospital qSOFA score and in-hospital mortality was still observed. Finally, we did not compare the prehospital qSOFA score with other severity or prehospital screening tools.
Conclusions
Among the various subgroups of patients with suspected infection who were admitted in the ED, a strong association was found between the prehospital qSOFA score and in-hospital mortality. In order to use this score in clinical practice, future study is necessary to evaluate how infection is suspected in the prehospital arena.
Supporting information
The prehospital qSOFA score was assessed using the first vital sign obtained at the scene and taken by EMS providers.
Abbreviation: qSOFA, quick sequential organ failure assessment; IQR, interquartile range; PT-INR, prothrombin time-international normalized ratio; Na, serum sodium; K, serum potassium; CRP, C-reactive protein; GNR, gram-negative rods; GNC, gram-negative cocci; GPC, gram-positive cocci; GPR, gram-positive rods; EMS, emergency medical service.
(PDF)
Acknowledgments
We thank all the staff of Okinawa Chubu Hospital. We would like to thank Editage (http://www.editage.jp) for their English language editing service. This work was performed at Okinawa Chubu Hospital.
Data Availability
Data cannot be shared publicly because of the regulation of IRB at Okinawa Kenritsu Chubu Hospital. Data are available from the Institutional Data Access / Ethics Committee (contact via SK or xx031112@pref.okinawa.lg.jp) for researchers who meet the criteria for access to confidential data.
Funding Statement
The authors received no specific funding for this work.
References
- 1.Gu WJ, Wang F, Bakker J, Tang L, Liu JC. The effect of goal-directed therapy on mortality in patients with sepsis—earlier is better: a meta-analysis of randomized controlled trials. Crit Care. 2014;18(5):570 Epub 2014/10/21. 10.1186/s13054-014-0570-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Seymour CW, Liu VX, Iwashyna TJ, Brunkhorst FM, Rea TD, Scherag A, et al. Assessment of Clinical Criteria for Sepsis. Jama. 2016;315(8). 10.1001/jama.2016.0288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Leisman DE, Doerfler ME, Ward MF, Masick KD, Wie BJ, Gribben JL, et al. Survival Benefit and Cost Savings From Compliance With a Simplified 3-Hour Sepsis Bundle in a Series of Prospective, Multisite, Observational Cohorts. Crit Care Med. 2017;45(3):395–406. Epub 2016/12/13. 10.1097/CCM.0000000000002184 . [DOI] [PubMed] [Google Scholar]
- 4.Pruinelli L, Westra BL, Yadav P, Hoff A, Steinbach M, Kumar V, et al. Delay Within the 3-Hour Surviving Sepsis Campaign Guideline on Mortality for Patients With Severe Sepsis and Septic Shock. Crit Care Med. 2018;46(4):500–5. Epub 2018/01/04. 10.1097/CCM.0000000000002949 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315(8):801–10. Epub 2016/02/24. 10.1001/jama.2016.0287 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ong MEH, Perkins GD, Cariou A. Out-of-hospital cardiac arrest: prehospital management. The Lancet. 2018;391(10124):980–8. 10.1016/s0140-6736(18)30316-7 [DOI] [PubMed] [Google Scholar]
- 7.Okubo M, Gibo K, Wallace DJ, Komukai S, Izawa J, Kiyohara K, et al. Regional variation in functional outcome after out-of-hospital cardiac arrest across 47 prefectures in Japan. Resuscitation. 2018;124:21–8. 10.1016/j.resuscitation.2017.12.030 [DOI] [PubMed] [Google Scholar]
- 8.Moyer P, Ornato JP, Brady WJ Jr., Davis LL, Ghaemmaghami CA, Gibler WB, et al. Development of systems of care for ST-elevation myocardial infarction patients: the emergency medical services and emergency department perspective. Circulation. 2007;116(2):e43–8. Epub 2007/06/01. 10.1161/CIRCULATIONAHA.107.184047 . [DOI] [PubMed] [Google Scholar]
- 9.Abdullah AR, Smith EE, Biddinger PD, Kalenderian D, Schwamm LH. Advance hospital notification by EMS in acute stroke is associated with shorter door-to-computed tomography time and increased likelihood of administration of tissue-plasminogen activator. Prehosp Emerg Care. 2008;12(4):426–31. Epub 2008/10/17. 10.1080/10903120802290828 . [DOI] [PubMed] [Google Scholar]
- 10.Seymour CW, Kahn JM, Cooke CR, Watkins TR, Heckbert SR, Rea TD. Prediction of critical illness during out-of-hospital emergency care. JAMA. 2010;304(7):747–54. Epub 2010/08/19. 10.1001/jama.2010.1140 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wallgren UM, Castren M, Svensson AE, Kurland L. Identification of adult septic patients in the prehospital setting: a comparison of two screening tools and clinical judgment. Eur J Emerg Med. 2014;21(4):260–5. Epub 2013/10/02. 10.1097/MEJ.0000000000000084 . [DOI] [PubMed] [Google Scholar]
- 12.Bayer O, Schwarzkopf D, Stumme C, Stacke A, Hartog CS, Hohenstein C, et al. An Early Warning Scoring System to Identify Septic Patients in the Prehospital Setting: The PRESEP Score. Acad Emerg Med. 2015;22(7):868–71. Epub 2015/06/27. 10.1111/acem.12707 . [DOI] [PubMed] [Google Scholar]
- 13.Polito CC, Isakov A, Yancey AH 2nd, Wilson DK, Anderson BA, Bloom I, et al. Prehospital recognition of severe sepsis: development and validation of a novel EMS screening tool. Am J Emerg Med. 2015;33(9):1119–25. Epub 2015/06/14. 10.1016/j.ajem.2015.04.024 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Smyth MA, Brace-McDonnell SJ, Perkins GD. Identification of adults with sepsis in the prehospital environment: a systematic review. BMJ Open. 2016;6(8):e011218 Epub 2016/08/09. 10.1136/bmjopen-2016-011218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dorsett M, Kroll M, Smith CS, Asaro P, Liang SY, Moy HP. qSOFA Has Poor Sensitivity for Prehospital Identification of Severe Sepsis and Septic Shock. Prehospital Emergency Care. 2017;21(4):489–97. 10.1080/10903127.2016.1274348 [DOI] [PubMed] [Google Scholar]
- 16.Jouffroy R, Saade A, Carpentier A, Ellouze S, Philippe P, Idialisoa R, et al. Triage of Septic Patients Using qSOFA Criteria at the SAMU Regulation: A Retrospective Analysis. Prehospital Emergency Care. 2017;22(1):84–90. 10.1080/10903127.2017.1347733 . [DOI] [PubMed] [Google Scholar]
- 17.Tusgul S, Carron PN, Yersin B, Calandra T, Dami F. Low sensitivity of qSOFA, SIRS criteria and sepsis definition to identify infected patients at risk of complication in the prehospital setting and at the emergency department triage. Scand J Trauma Resusc Emerg Med. 2017;25(1):108 Epub 2017/11/05. 10.1186/s13049-017-0449-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–83. Epub 1987/01/01. . [DOI] [PubMed] [Google Scholar]
- 19.Ohta T, Waga S, Handa W, Saito I, Takeuchi K. [New grading of level of disordered consiousness (author's transl)]. No Shinkei Geka. 1974;2(9):623–7. Epub 1974/09/01. . [PubMed] [Google Scholar]
- 20.Frenkel WJ, Jongerius EJ, Mandjes-van Uitert MJ, van Munster BC, de Rooij SE. Validation of the Charlson Comorbidity Index in acutely hospitalized elderly adults: a prospective cohort study. J Am Geriatr Soc. 2014;62(2):342–6. Epub 2014/02/14. 10.1111/jgs.12635 . [DOI] [PubMed] [Google Scholar]
- 21.Quan H, Li B, Couris CM, Fushimi K, Graham P, Hider P, et al. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–82. Epub 2011/02/19. 10.1093/aje/kwq433 . [DOI] [PubMed] [Google Scholar]
- 22.Freund Y, Lemachatti N, Krastinova E, Van Laer M, Claessens Y-E, Avondo A, et al. Prognostic Accuracy of Sepsis-3 Criteria for In-Hospital Mortality Among Patients With Suspected Infection Presenting to the Emergency Department. Jama. 2017;317(3). 10.1001/jama.2016.20329 [DOI] [PubMed] [Google Scholar]
- 23.Jouffroy R, Saade A, Ellouze S, Carpentier A, Michaloux M, Carli P, et al. Prehospital triage of septic patients at the SAMU regulation: Comparison of qSOFA, MRST, MEWS and PRESEP scores. The American Journal of Emergency Medicine. 2018;36(5):820–4. 10.1016/j.ajem.2017.10.030 [DOI] [PubMed] [Google Scholar]
- 24.Vaittinada Ayar P, Delay M, Avondo A, Duchateau F-X, Nadiras P, Lapostolle F, et al. Prognostic value of prehospital quick sequential organ failure assessment score among patients with suspected infection. European Journal of Emergency Medicine. 2018. 10.1097/mej.0000000000000570 . [DOI] [PubMed] [Google Scholar]
- 25.Shu E, Ives Tallman C, Frye W, Boyajian JG, Farshidpour L, Young M, et al. Pre-hospital qSOFA as a predictor of sepsis and mortality. Am J Emerg Med. 2018. Epub 2018/10/17. 10.1016/j.ajem.2018.09.025 . [DOI] [PubMed] [Google Scholar]
- 26.Kitahara O, Nishiyama K, Yamamoto B, Inoue S, Inokuchi S. The prehospital quick SOFA score is associated with in-hospital mortality in noninfected patients: A retrospective, cross-sectional study. PLoS One. 2018;13(8):e0202111 Epub 2018/08/17. 10.1371/journal.pone.0202111 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Askim A, Moser F, Gustad LT, Stene H, Gundersen M, Asvold BO, et al. Poor performance of quick-SOFA (qSOFA) score in predicting severe sepsis and mortality—a prospective study of patients admitted with infection to the emergency department. Scand J Trauma Resusc Emerg Med. 2017;25(1):56 Epub 2017/06/11. 10.1186/s13049-017-0399-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hwang SY, Jo IJ, Lee SU, Lee TR, Yoon H, Cha WC, et al. Low Accuracy of Positive qSOFA Criteria for Predicting 28-Day Mortality in Critically Ill Septic Patients During the Early Period After Emergency Department Presentation. Annals of Emergency Medicine. 2018;71(1):1–9.e2. 10.1016/j.annemergmed.2017.05.022 [DOI] [PubMed] [Google Scholar]
- 29.Williams JM, Greenslade JH, McKenzie JV, Chu K, Brown AFT, Lipman J. Systemic Inflammatory Response Syndrome, Quick Sequential Organ Function Assessment, and Organ Dysfunction: Insights From a Prospective Database of ED Patients With Infection. Chest. 2017;151(3):586–96. Epub 2016/11/24. 10.1016/j.chest.2016.10.057 . [DOI] [PubMed] [Google Scholar]
- 30.Canet E, Taylor DM, Khor R, Krishnan V, Bellomo R. qSOFA as predictor of mortality and prolonged ICU admission in Emergency Department patients with suspected infection. J Crit Care. 2018;48:118–23. Epub 2018/09/04. 10.1016/j.jcrc.2018.08.022 . [DOI] [PubMed] [Google Scholar]
- 31.Levy MM, Evans LE, Rhodes A. The Surviving Sepsis Campaign Bundle: 2018 Update. Crit Care Med. 2018;46(6):997–1000. Epub 2018/05/17. 10.1097/CCM.0000000000003119 . [DOI] [PubMed] [Google Scholar]
- 32.Spiegel R, Farkas JD, Rola P, Kenny J-E, Olusanya S, Marik PE, et al. The 2018 Surviving Sepsis Campaign’s Treatment Bundle: When Guidelines Outpace the Evidence Supporting Their Use. Annals of Emergency Medicine. 2018. 10.1016/j.annemergmed.2018.06.046 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
The prehospital qSOFA score was assessed using the first vital sign obtained at the scene and taken by EMS providers.
Abbreviation: qSOFA, quick sequential organ failure assessment; IQR, interquartile range; PT-INR, prothrombin time-international normalized ratio; Na, serum sodium; K, serum potassium; CRP, C-reactive protein; GNR, gram-negative rods; GNC, gram-negative cocci; GPC, gram-positive cocci; GPR, gram-positive rods; EMS, emergency medical service.
(PDF)
Data Availability Statement
Data cannot be shared publicly because of the regulation of IRB at Okinawa Kenritsu Chubu Hospital. Data are available from the Institutional Data Access / Ethics Committee (contact via SK or xx031112@pref.okinawa.lg.jp) for researchers who meet the criteria for access to confidential data.