

Abstract
Background:
Carpal tunnel syndrome is a common compressive neuropathy of the median nerve. Compared with standard release, the efficacy, safety, and postoperative complications of limited carpal tunnel release remain controversial. The purpose of this study was to compare the effects of the 2 treatments.
Methods:
The English-language literature was searched using MEDLINE, Web of Science, and Embase. Randomized controlled trials that compared standard and limited incision for carpal tunnel release were included in the meta-analysis. Strength, interval to return to activities, the rate of adverse events, effectiveness, and operative time were compared.
Results:
Thirteen randomized controlled trials (RCTs) containing 1020 patients were included. Limited incision treated patients showed better early recovery of grip strength (mean difference [MD], 4.25 [0.86–7.65]; P = .01) and pinch strength (MD, 1.37 [0.24–2.51]; P = .02) but no advantage after more than 6 months. Patients treated with limited incision showed an earlier return to activities (MD,−8.80 [−9.21 to −8.39]; P < .01) and reduced operative time (standardized mean difference [SMD], −1.68 [−3.24 to−0.12]; P = .04). The rate of adverse event was significantly higher in standard group compared with that in limited group (risk ratio [RR] 0.61, 95% CI 0.38–0.96, P = .03).
Conclusions:
Limited incision release allows us to return to activities early, reduces operative time, decreases rate of adverse events, and improves strength during the early postoperative period. Results at 6 months or longer are similar according to current data. However, the results of this meta-analysis should be interpreted with caution due to heterogeneity amongst the included studies.
Keywords: carpal tunnel syndrome, limited-incision, meta-analysis, review, standard-incision
1. Introduction
Carpal tunnel syndrome (CTS), affects more than 60 million people worldwide,[1] is a compressive neuropathy of the median nerve that can cause hand pain, numbness, and tingling.[2–4] Initial treatment of carpal tunnel syndrome involves nonoperative measures such as splinting, rest, nonsteroidal anti-inflammatory drugs (NSAIDs), physiotherapy, and corticosteroid injection.[5–9] The first open release was completed by Herbert Galloway in 1924,[10] is indicated in recalcitrant cases. In the United States, more than 350,000 surgical operations are performed for carpal tunnel syndrome each year.[11]
For many surgeons, standard open carpal tunnel release with a long palmer curvilinear incision is still the preferred surgical procedure.[4] Although the standard carpal tunnel release has proven effective and safe, the limited method offer better appearance and minor wound complications compared with the standard open method.[12] Also, the limited technology provides an early return to activities, an early recovery of grip strength and pinch strength.[9] A meta-analysis with a large sample size may be necessary to detect such complications and differences in other outcome measures.[13] Although limited carpal tunnel release has been applied for more than 2 decades, its availability and overall patient outcome remain controversial relative to standard release. Previous meta-analyses have been conducted to compare these procedures but there are important methodological flaws in their inclusion criteria, outcome parameters and validity assessment.[14]
The objective of our meta-analysis was to compare the clinical outcomes of patients with carpal tunnel syndrome treated with a limited versus standard approach based on high-level evidence from RCTs. The clinical outcomes included postoperative complications, symptom relief, short-term and long-term intensity recovery, interval return to activities, and operative time.
2. Materials and methods
2.1. Literature search
We searched the MEDLINE, Web of Science, and Embase for all relevant literature through to June 2017 that were controlled or comparative studies exploring whether limited incision compared with standard incision for carpal tunnel release is better. The following search terms and Boolean operators were used: (“carpal tunnel syndrome” or “CTS”) and (“small” or “limited” or “double”) and (“open” or “traditional” or “standard”). This search was limited to human subjects. This study only includes full-text articles published in English. We also manually searched the references in the relevant articles to identify other studies that may be eligible and repeat the process until further research cannot be determined. Ethical approval and patient consent were not required for this study, given that this was a meta-analysis, which utilized published data.
2.2. Eligibility criteria
The meta-analysis was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.[15] The inclusion criteria were limited to RCTs that compared limited and standard carpal tunnel releases. Laboratory or anatomic studies, abstracts, descriptive or nontherapeutic, and review or technique articles studies also were excluded. Studies that analyzed the same group of patients were consolidated to prevent duplication of data, and data from the longer follow-up were preferentially used.
2.3. Data extraction and outcome measures
Two researchers independently extracted each relevant data included in the study into a data table. The items included in the data sheet were the first author, publication year, follow-up times, sample size of the limited and standard groups, total number of study participants, type of surgery, primary outcome, and complications. The data format of each of the 2 researchers was compared and the differences were resolved through discussion until consensus was reached.
The following outcomes and complications were investigated in this meta-analysis: strength, interval to return to activities, complications, symptom relief, and operative time were analyzed.
2.4. Data synthesis and statistical analysis
Perform a pooled analysis to compare several clinical outcome measures between groups, depending on the availability of the data. A random-effects model was selected to calculate the statistical heterogeneity of the included trials using Review Manager Version 5.2.11 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). Differences were expressed as RRs with 95% confidence intervals (CIs) for dichotomous outcomes and weighted mean differences (WMDs) with 95% CIs for continuous outcomes. Heterogeneity was analyzed with both the Chi-square test and the I2 test. The P value of <.05 for the Chi-square test was interpreted as evidence of statistical heterogeneity, and I2 was used to estimate total variation across the studies. A fixed-effect model was adopted if there was no statistical evidence of heterogeneity, and a random-effect model was adopted if statistically significant heterogeneity was present. Studies with an I2 statistic of 25% to 50% were considered to have low heterogeneity, those with an I2 statistic of 50% to 75% had moderate heterogeneity, and those with an I2 statistic of >75% had high heterogeneity. If the standard deviation (SD) for a given outcome was not reported in a study, it was computed from other provided statistics, including the 95% CI, standard error (SE), interquartile range, or P value. When the SD could not be determined, it was imputed using the mean of the values reported by the other studies.[16] Continuous data were analyzed through the inverse-variance statistical method and computation of the SMD or MD and 95% CI. Forest plots were generated and presented for the following chief outcomes: grip and pinch strength at 6 months or greater, operative time, effectiveness, complications, and interval to return to activities.
2.5. Assessment of methodological quality
To assess the quality of the study, the authors independently evaluated the study without masking the trial name. The evaluators followed the instructions provided in the Cochrane Handbook for Systematic Reviews of Interventions.[17] The following domains were assessed: random sequence generation, allocation concealment, blinding, incomplete data outcomes, revealing of selective outcomes, and any remaining biases. When the information in the study was not sufficient, try to contact the author to ensure the research is properly assessed.
3. Result
3.1. Literature search results
Around 150 articles without duplications were identified from a total of 282 records, and 131 articles were excluded after reviewing titles and abstracts. After evaluating the full text of the remaining 19 studies, a further 6 full-text articles were excluded. As a result, 13 unique studies were included in this meta-analysis.[18–30] A flowchart demonstrating the search process for locating related research is presented in Figure 1.
Figure 1.
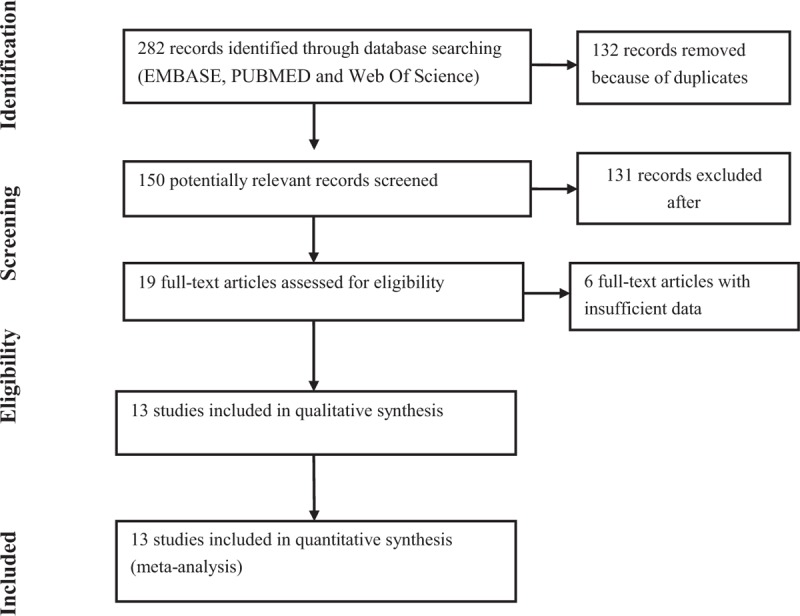
Flow diagram of the literature search of studies.
3.2. Characteristics of included studies
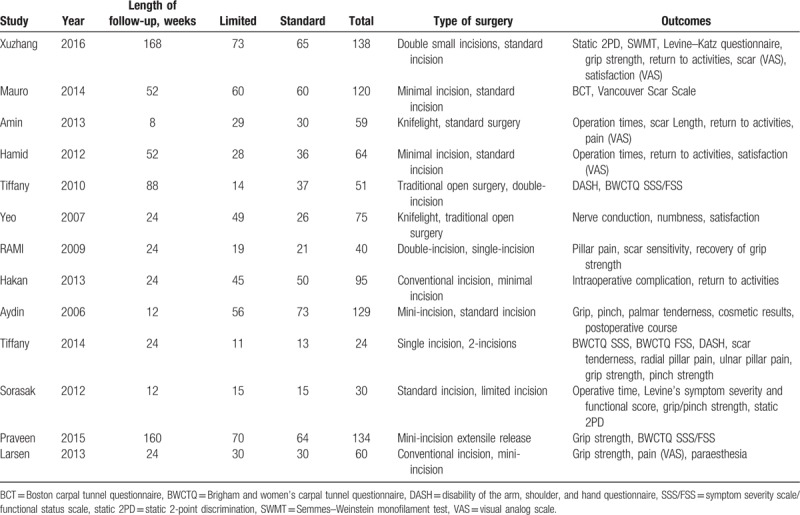
The main characteristics of the 13 RCTs included in the meta-analysis are presented in Table 1. These studies were published between 2006 and 2016. The sizes of the RCTs ranged from 24 to 138 patients. There were 1019 patients at the time of final follow-up. A total of 499 patients underwent limited incision, and the remaining 520 patients received standard surgery. Limited incision operations include: single-small incision surgery, double-small incision surgery, and Knifelight. The traditional surgical approach is a standard incision (incision >5 cm in length. Follow-up for all patients ranged from 8 to 168 weeks.
Table 1.
Basic characteristics of the 13 included studies and patients in studies.
4. Main results of this analysis
4.1. Grip strength
A total of 232 patients in 4 studies were compared the grip strength of the limited incision and the standard incision. Due to the heterogeneity between groups of grip strength is small (I2 < 50%), a fixed effect model is adopted. Patients treated with limited carpal tunnel release showed greater grip strength (MD, 4.25 [0.86–7.65]; P = .01)[19,25,28,29] (Fig. 2). However, when long-term follow-up at 6 months or more, no differences remained between techniques in the recovery of grip strength (MD, 0.7 [−1.38–2.79]; P = .5).[19,28,29]
Figure 2.

The forest plots show the mean difference in grip strength.
4.2. Pinch strength
We compared the pinch strength of the limited incision and the standard incision in a total of 192 patients in 3 studies. Because the heterogeneity between groups of the recovery of pinch strength is small (I2 = 25%), a fixed effect model is used. Patients treated with limited carpal tunnel release showed greater pinch strength (MD, 1.37 [0.24–2.51]; P = .02)[19,25,29] (Fig. 3). But, when long-term follow-up at 6 months or more, it did not remain statistical significance between techniques in pinch strength (MD, 8.09 [−2.00– 18.19]; P = .12).[19,25,29]
Figure 3.

The forest plots show the mean difference in pinch strength.
4.3. Return to activities
A total of 536 patients in 6 studies were compared the interval to return to activities of the limited incision and the standard incision. On account of the heterogeneity between the groups of interval to return to activities is small (I2 = 49%), a fixed effect model is used. Patients who treated with limited carpal tunnel release returned to activities earlier than patients who treated with standard release (MD,−8.80 [−9.21 to −8.39]; P < .01)[18,21,22,24,26,29] (Fig. 4).
Figure 4.

The forest plot shows the mean difference in the interval to return to activities (days).
4.4. Operative time
We collected 159 patients from 3 studies to compare the operative time with limited incision and standard incision. Because the heterogeneity between the groups of operative time is high (I2 > 50%), a random effect model is put into used. And the operative time was shorter for limited compared with standard release (MD, −1.68 [−3.24 to−0.12]; P = .04).[18,21,25]
4.5. Effectiveness and adverse events
In addition, we collected data from 13 studies, such as BCT, 2PD, scar issues, pillar pain, etc., which are listed in the table. It did not compare the operative time, grip/pinch strength and time of returned to activities because the above has been analyzed. The study records of these events were relatively inconsistent among studies, so we without performing further subgroup analysis. We divided it into 2 parts, one for adverse events (Table 2) and the other for effectiveness (Table 3). Using the fixed effect model, the rate of adverse event was significantly lower in limited group compared with that in standard group (RR 0.61, 95% CI 0.38–0.96, P = .03) (Fig. 5).
Table 2.
Adverse events in limited-incision and standard-incision groups.

Table 3.
Effectiveness in limited-incision and standard-incision groups.
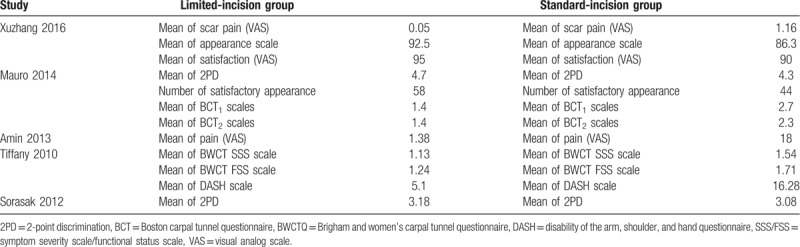
Figure 5.
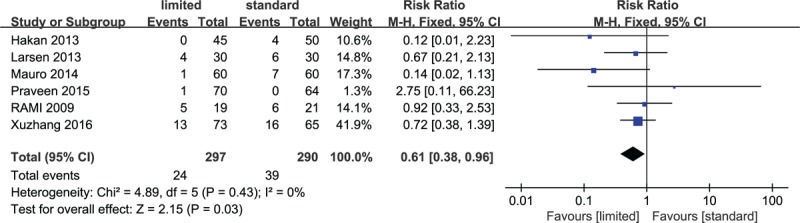
Forest plot showing the rate of adverse events between the limited group and the standard group.
4.6. Publication bias and sensitivity analysis
A funnel plot (Fig. 6) of the analysis of the interval to return to activities appeared essentially symmetric in relation to the pooled estimate from the meta-analysis, indicating minimal publication bias. The risk of bias is demonstrated graphically in Figure 7 and summarized in Figure 8.
Figure 6.
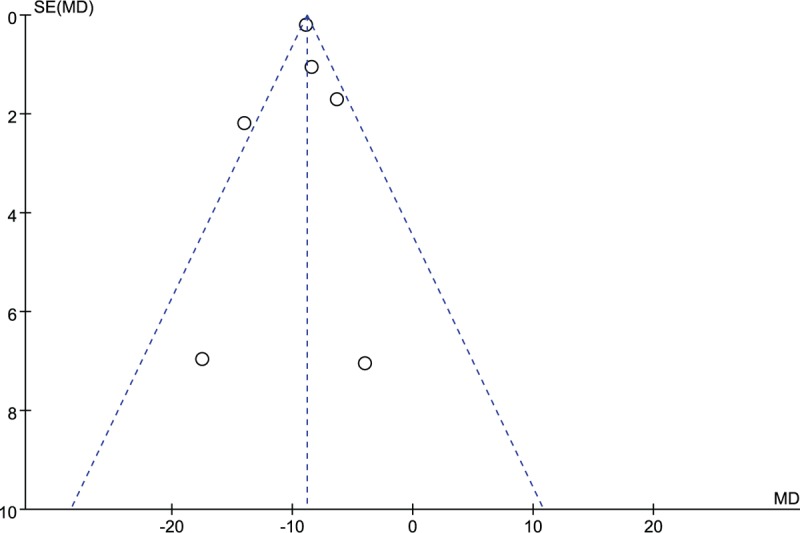
The funnel plot shows the relative symmetry of the pooled estimate relative to the meta-analysis, indicating minimal publication bias.
Figure 7.

Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies.
Figure 8.
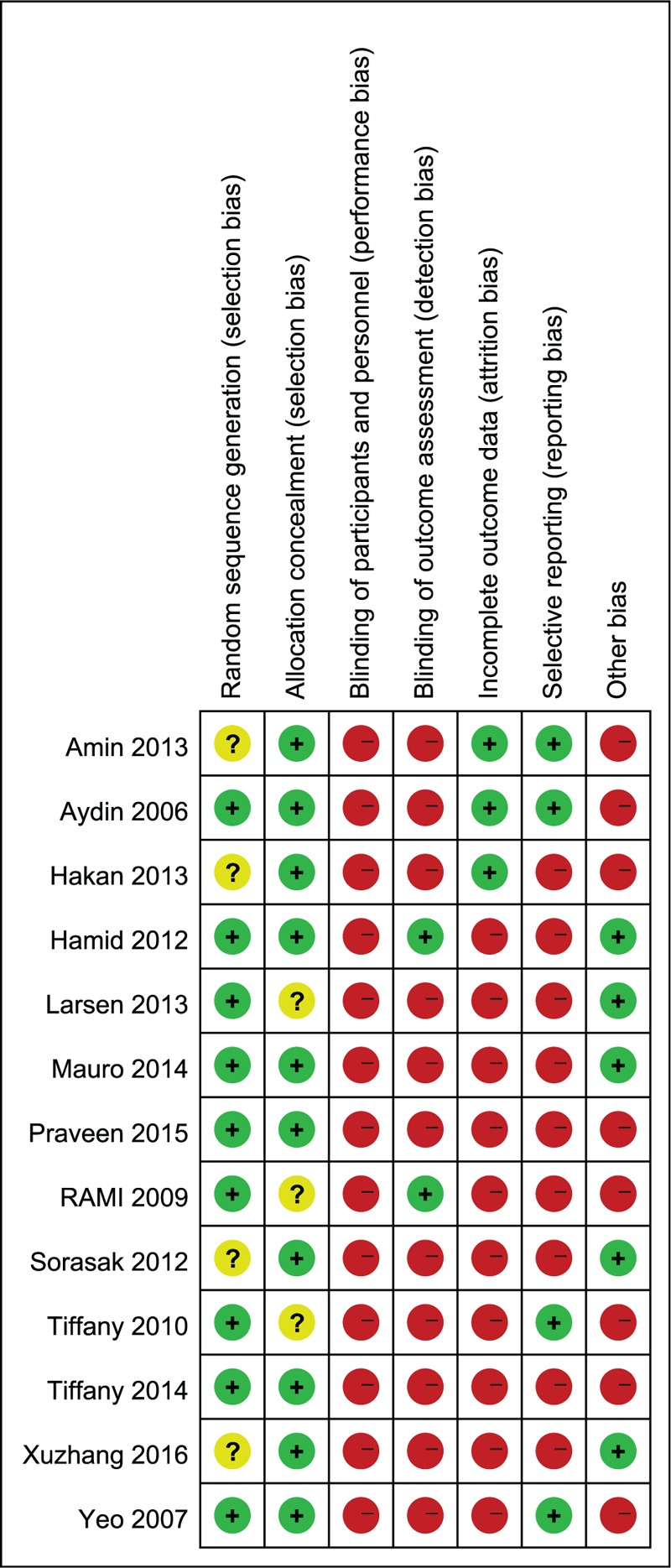
Risk of bias summary: review authors’ judgments about each risk of bias item for each included study.
Because of patient characteristics, type of surgery, operator and other confounding factors were inconsistent between studies, we further performed a sensitivity analysis to identify potential sources of heterogeneity. We tried to remove any one of the literature in the study, and the results which did not change much were still statistically significant. The P value < .05 was judged to be statistically significant unless otherwise specified.
5. Discussion
Carpal tunnel release with division of the transverse carpal ligament, a fundamental solution to the treatment of median nerve compression, has been a highly successful procedure for the treatment of CTS. Carpal tunnel release surgery has evolved several years to decrease the complications and side effects associated with the operation procedures. Traditional surgical incisions, endoscopy, and small incisions that were newly emerged in recent years, people are striving to explore ways to achieve maximum therapeutic effect at minimal cost. All procedures have been proven to successfully relieve the symptoms of CTS, but each method is associated with various complications and side effects.[26] Studies have shown that carpal tunnels are released through small incisions, combining the advantages of standard open carpal tunnel release and endoscopic carpal tunnel release. Its advantages include minimally invasive surgery, good visualization of the operating area, less technically challenging surgery, low wound complication rate, and good appearance. Compared to standard open methods, limited methods provide better appearance and mild wound complications. Compared to endoscopic methods, our technology does not require expensive equipment.[29,31,32] Furthermore, a number of RCTs have been conducted to date without showing clear advantages of any procedure, and neither of these techniques is clearly favored at present. Thus, the purpose of our meta-analysis was to determine whether limited compared with standard relief provides better symptom relief, short- and long-term strength; different risks of complications such as nerve injury, pain, and reoperation; allows an earlier return to activities; and takes less operative time.
Meta-analysis is usually regarded as an efficient method to integrate effective study results and provide a basis for rational decision making.[33] This meta-analysis pooled 13 studies. This study demonstrated that limited incisions performed better than conventional incisions in terms of reduced operative time, early strength recovery, reduced postoperative scarring, and reduced postoperative recovery time. It is particularly good at recovering early strength, cutting down the incidence of adverse events and reducing the interval to return to activities after surgery. In general, small incision surgery has a shorter surgical incision than traditional incision surgery, which means that it can reduce the operation time to a greater extent, reduce the surgical scar, and reduce the risk of damage to the small blood vessels and small nerves in the skin. Therefore, small incision surgery has smaller surgical scars, shorter operative time, shorter recovery time, less risk of pain and numbness around the incision, and less risk of re-clamping of the median nerve due to bleeding. When special tools, such as light knife, are used to protect the median nerve, the operation time will be shorter and the risk of damaging the median nerve will be less. However, in the long-term (more than 6 months) strength recovery, there was no significant difference between the 2 surgical methods.
There are limitations to this meta-analysis, our analysis was based on a limited number of studies, several of which have modest sample sizes. Compared to a review with a larger overall sample size, our study is more likely to overestimate or underestimate the true results. As there are virtually no validated instruments to assess patient satisfaction, this endpoint was omitted from the meta-analysis even though it was reported in some of the studies. To minimize heterogeneity, we excluded endoscopic surgeries and investigated only standard and open limited surgery. The patients, duration of follow-up, and types of surgical procedures used were varied among the included studies. Including double-incision or single-incision might result in an increased heterogeneity and impact upon the conclusions found in this study. Most of the included studies were from the United States and only one study was from China. It is unclear whether the results of our meta-analysis can be applied to other countries. We hope that future studies will be conducted in other countries to evaluate whether the results of this study are generalizable.
The study conducted by Gulsen et al[22] is of low quality and may have introduced bias into our meta-analysis. As a result, we conducted an additional analysis in which this study was omitted from the calculation of results. Removing this study did not alter any of the meta-analysis outcomes, which revealed that the results of the present review were robust to a certain degree.
According to our study, surgical treatment of carpal tunnel syndrome with a limited incision has shorter operative time, significantly improved short-term strength recovery, and less scarring and rapid return to activities. Although limited incision surgery has so many advantages, surgeons still need to be aware that small incision surgery also has limitation. Patients, who have carpal tunnel bone occupying, abnormal muscle abdomen, mass, carpal bone deformity healing and nerve position variation, treated by limited carpal tunnel release will increase the difficulty of surgery or even failure. Therefore, B-ultrasound, x-ray and/or MRI should be performed to exclude these patients before surgery.[34] For recurrent cases, the structure is more complicated than the initial one, and it is not suitable for limited carpal tunnel release.
In conclusion, in this meta-analysis of randomized clinical trials, we compared the effect of limited incision release versus standard incision release for carpal tunnel syndrome, certain benefits of limited incision are noted, which include a good restoration of grip and pinch strength, a low rate of complications, reduce operative time, and rapid return to activities. Despite these encouraging findings, surgeons still need to know that small incision surgery also has limitation. Patients, not suitable for limited carpal tunnel release, should be excluded before surgery. Anyhow, we should interpret the results with caution and further large-scale, well-designed RCTs on this theme are still needed.
Author contributions
Conceptualization: Gaocen Li, Kunlun Yu, Dehu Tian.
Data curation: Gaocen Li, Lingde Kong, Ningzhao Kou, Dehu Tian.
Formal analysis: Gaocen Li, Lingde Kong, Ningzhao Kou, Jiangbo Bai, Dehu Tian.
Investigation: Gaocen Li, Lingde Kong, Ningzhao Kou, Kunlun Yu, Dehu Tian.
Methodology: Gaocen Li, Lingde Kong, Ningzhao Kou, Yanxue Wang, Kunlun Yu, Jiangbo Bai, Dehu Tian.
Project administration: Dehu Tian.
Software: Gaocen Li, Lingde Kong, Yanxue Wang, Dehu Tian.
Supervision: Gaocen Li, Yanxue Wang.
Validation: Gaocen Li, Ningzhao Kou, Yanxue Wang, Kunlun Yu, Jiangbo Bai.
Visualization: Gaocen Li, Ningzhao Kou, Yanxue Wang, Kunlun Yu, Jiangbo Bai.
Writing – original draft: Gaocen Li, Lingde Kong, Dehu Tian.
Writing – review & editing: Dehu Tian.
Footnotes
Abbreviations: BCT = Boston Carpal Tunnel questionnaire, BWCTQ = Brigham and Women's Carpal Tunnel Questionnaire, CI = confidence interval, CTS = carpal tunnel syndrome, DASH = Disability of the Arm, Shoulder, and Hand questionnaire, MD = mean difference, NSAIDs = nonsteroidal anti-inflammatory drugs, PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses, RCTs = randomized controlled trials, RR = risk ratio, SD = standard deviation, SE = standard error, SMD = standardized mean difference, SSS/FSS = Symptom Severity Scale/Functional Status Scale, static 2PD = static 2-point discrimination, SWMT = Semmes–Weinstein monofilament test, WMD = weighted mean difference.
GL and LK contributed equally to this work.
The authors have no conflicts of interest to disclose.
References
- [1].Chammas M. Carpal tunnel syndrome. Chir Main 2014;33:75–94. [DOI] [PubMed] [Google Scholar]
- [2].Leinberry CF, Rivlin M, Maltenfort M, et al. Treatment of carpal tunnel syndrome by members of the American Society for Surgery of the Hand: a 25-year perspective. J Hand Surg Am 2012;37:1997–2003. [DOI] [PubMed] [Google Scholar]
- [3].Newington L, Harris EC, Walker-Bone K. Carpal tunnel syndrome and work. Best Pract Res Clin Rheumatol 2015;29:440–53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Aroori S, Spence RA. Carpal tunnel syndrome. Ulster Med J 2008;77:6–17. [PMC free article] [PubMed] [Google Scholar]
- [5].Tanriverdi M, Hosbay Z, Candan AZ. The relationship of the pain on the upper extremity functions and quality of life in patients with carpal tunnel syndrome. J Back Musculoskelet Rehabil 2018. [DOI] [PubMed] [Google Scholar]
- [6].Evers S, Bryan AJ, Sanders TL, et al. Corticosteroid injections for carpal tunnel syndrome: long-term follow-up in a population-based cohort. Plast Reconstr Surg 2017;140:338–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Meems M, Spek V, Kop WJ, et al. Mechanical wrist traction as a non-invasive treatment for carpal tunnel syndrome: a randomized controlled trial. Trials 2017;18:464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Nanno M, Kodera N, Tomori Y, et al. Electrophysiological assessment for splinting in the treatment of carpal tunnel syndrome. Neurol Med Chir (Tokyo) 2017;57:472–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Chammas M, Boretto J, Burmann LM, et al. Carpal tunnel syndrome—part II (treatment). Rev Bras Ortop 2014;49:437–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Amadio PC. The first carpal tunnel release? J Hand Surg Br 1995;20:40–1. [DOI] [PubMed] [Google Scholar]
- [11].Owings MF, Kozak LJ. Ambulatory and inpatient procedures in the United States, 1996. Vital Health Stat 13 1998;139:1–19. [PubMed] [Google Scholar]
- [12].Oh WT, Kang HJ, Koh IH, et al. Morphologic change of nerve and symptom relief are similar after mini-incision and endoscopic carpal tunnel release: a randomized trial. BMC Musculoskelet Disord 2017;18:65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Atroshi I, Larsson GU, Ornstein E, et al. Outcomes of endoscopic surgery compared with open surgery for carpal tunnel syndrome among employed patients: randomised controlled trial. BMJ 2006;332:1473. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Vasiliadis HS, Georgoulas P, Shrier I, et al. Endoscopic release for carpal tunnel syndrome. Cochrane Database Syst Rev 2014;D8265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med 2009;151:264–9. W64. [DOI] [PubMed] [Google Scholar]
- [16].Sayegh ET, Strauch RJ. Open versus endoscopic carpal tunnel release: a meta-analysis of randomized controlled trials. Clin Orthop Relat Res 2015;473:1120–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Kong L, Zhang Y, Shen Y. Operative versus nonoperative treatment for displaced midshaft clavicular fractures: a meta-analysis of randomized clinical trials. Arch Orthop Trauma Surg 2014;134:1493–500. [DOI] [PubMed] [Google Scholar]
- [18].Aslani HR, Alizadeh K, Eajazi A, et al. Comparison of carpal tunnel release with three different techniques. Clin Neurol Neurosurg 2012;114:965–8. [DOI] [PubMed] [Google Scholar]
- [19].Castillo TN, Yao J. Prospective randomized comparison of single-incision and two-incision carpal tunnel release outcomes. Hand (N Y) 2014;9:36–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Murthy PG, Goljan P, Mendez G, et al. Mini-open versus extended open release for severe carpal tunnel syndrome. Hand (N Y) 2015;10:34–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Heidarian A, Abbasi H, Hasanzadeh HM, et al. Comparison of knifelight surgery versus conventional open surgery in the treatment of carpal tunnel syndrome. Iran Red Crescent Med J 2013;15:385–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Gulsen I, Ak H, Evcili G, et al. A retrospective comparison of conventional versus transverse mini-incision technique for carpal tunnel release. ISRN Neurol 2013;2013:721830. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [23].Castillo TN, Yao J. Comparison of longitudinal open incision and two-incision techniques for carpal tunnel release. J Hand Surg Am 2010;35:1813–9. [DOI] [PubMed] [Google Scholar]
- [24].Larsen MB, Sorensen AI, Crone KL, et al. Carpal tunnel release: a randomized comparison of three surgical methods. J Hand Surg Eur Vol 2013;38:646–50. [DOI] [PubMed] [Google Scholar]
- [25].Suppaphol S, Worathanarat P, Kawinwongkovit V, et al. The comparison between limited open carpal tunnel release using direct vision and tunneling technique and standard open carpal tunnel release: a randomized controlled trial study. J Med Assoc Thai 2012;95:532–6. [PubMed] [Google Scholar]
- [26].Tarallo M, Fino P, Sorvillo V, et al. Comparative analysis between minimal access versus traditional accesses in carpal tunnel syndrome: a perspective randomised study. J Plast Reconstr Aesthet Surg 2014;67:237–43. [DOI] [PubMed] [Google Scholar]
- [27].Keramettin A, Cengiz C, Nilgun C, et al. Microsurgical open mini uniskin incision technique in the surgical treatment of carpal tunnel syndrome. Neurol India 2006;54:64–7. [DOI] [PubMed] [Google Scholar]
- [28].Hamed AR, Makki D, Chari R, et al. Double- versus single-incision technique for open carpal tunnel release. Orthopedics 2009;32:733–7. [DOI] [PubMed] [Google Scholar]
- [29].Zhang X, Huang X, Wang X, et al. A randomized comparison of double small, standard, and endoscopic approaches for carpal tunnel release. Plast Reconstr Surg 2016;138:641–7. [DOI] [PubMed] [Google Scholar]
- [30].Yeo KQ, Yeo EM. Comparison of the results of open carpal tunnel release and KnifeLight carpal tunnel release. Singapore Med J 2007;48:1131–5. [PubMed] [Google Scholar]
- [31].Beck JD, Deegan JH, Rhoades D, et al. Results of endoscopic carpal tunnel release relative to surgeon experience with the Agee technique. J Hand Surg Am 2011;36:61–4. [DOI] [PubMed] [Google Scholar]
- [32].Papageorgiou CD, Georgoulis AD, Makris CA, et al. Difficulties and early results of the endoscopic carpal tunnel release using the modified Chow technique. Knee Surg Sports Traumatol Arthrosc 1998;6:189–93. [DOI] [PubMed] [Google Scholar]
- [33].Zhang YZ, Kong LD, Cao JM, et al. Incidence of subsequent vertebral body fractures after vertebroplasty. J Clin Neurosci 2014;21:1292–7. [DOI] [PubMed] [Google Scholar]
- [34].Kang HJ, Jung SH, Yoon HK, et al. Carpal tunnel syndrome caused by space occupying lesions. Yonsei Med J 2009;50:257–61. [DOI] [PMC free article] [PubMed] [Google Scholar]