

Abstract
Background:
CrossFit is a popular weightlifting sport, with participants who report significant improvements in physical health; however, others argue that CrossFit exposes participants to an increased risk and severity of injury. We address this through a retrospective cohort study.
Purpose/Hypothesis:
The purpose of this study was to compare the likelihood of self-reported injury and severity in CrossFit and traditional weightlifting in the previous 2 years. We hypothesized that CrossFit participants would have a higher 2-year likelihood of injury and medical care compared with a traditional weightlifting cohort.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Anonymous volunteers who participated regularly in CrossFit or traditional weightlifting routines completed a 15-question survey that queried workout routine, injury history, and medical care due to a weightlifting injury. Inclusion criteria included those older than 18 years who were active participants in CrossFit and weightlifting. Unpaired t-test analyses were conducted to compare means of continuous data between participants in CrossFit and traditional weightlifting. A multivariant logistic regression model was used to assess the association of training routine, sex, and age with those sustaining at least 1 injury within the past 2 years.
Results:
A total of 411 participants (122 CrossFit; 289 traditional weightlifting) completed the questionnaire. Those following a CrossFit routine were 1.30 times more likely to be injured (95% CI, 1.075-1.57; P = .0067) and 1.86 times more likely to seek medical attention (95% CI, 1.40-2.48; P < .0001). In a multivariant logistic regression analysis adjusting for sex and age, injury was 2.26 times more likely in the CrossFit group (95% CI, 1.42-3.62; P = .0010). In both groups, shoulder injuries were most common (46.41%), followed by lower back (38.28%) and hip injuries (9.09%).
Conclusion:
Athletes participating in CrossFit are more likely to be injured and to seek medical treatment compared with participants in traditional weightlifting. Despite these findings, the increased likelihood of injury may have less to do with the exercises involved with CrossFit and more related to the intensity with which the exercises are performed, and thus increased awareness is needed to prevent further injuries.
Keywords: weightlifting, injury prevention, CrossFit, muscle injuries
CrossFit has emerged as a highly popular workout routine that consists of high-intensity plyometric, gymnastic, and Olympic weightlifting exercises performed in rapid succession. Founded in 2000, CrossFit has become a multi–billion dollar industry, with 11,000 CrossFit gyms worldwide as of 2015 and more than 200,000 participants signed up to compete at the 2014 CrossFit games.1,14 Studies have demonstrated that this group-based training program promotes multiple health benefits, including improvements in anaerobic capacity, cardiovascular fitness, and body composition.13,17
Some concern has been raised in the popular media regarding whether CrossFit routines expose participants to increased risk of injury.6 Despite these concerns, current studies have failed to consistently demonstrate an increased risk of injury among CrossFit participants. To date, available studies have reported the incidence of injury during CrossFit training varying from 2.71 to 3.1 per 1000 hours.2,9 These injury rates are similar to published rates for recreational tennis players (1.6-3.0 injuries per 1000 hours),10,12,19 triathletes (2.5-5.4 injuries per 1000 hours),4,11 and traditional weightlifters (2.7-5.5 injuries per 1000 hours).5,15,16,21 However, no study has directly compared the incidence of injury among CrossFit participants versus those using a traditional weightlifting routine in a comparable geographic location and at the same time point, and none has investigated the severity of injuries incurred. This direct comparison is relevant to our patients, as most weightlifters identify as either primarily following a CrossFit routine or primarily following a traditional weightlifting routine, as well as to clinicians in general whose patients may present for counseling on popular weightlifting routines.
The purpose of this study was to compare the 2-year incidence rates and severity of self-reported injury among CrossFit participants and those using a traditional weightlifting routine. Secondary aims included determining the characteristics of injury for each fitness program (ie, location of injury and specific activity performed during injury) and determining whether age, sex, and/or any supplement types were independently associated with increased rate of injury. We hypothesized that CrossFit participants would have a higher 2-year incidence and severity of self-reported injury compared with the traditional weightlifting cohort.
Methods
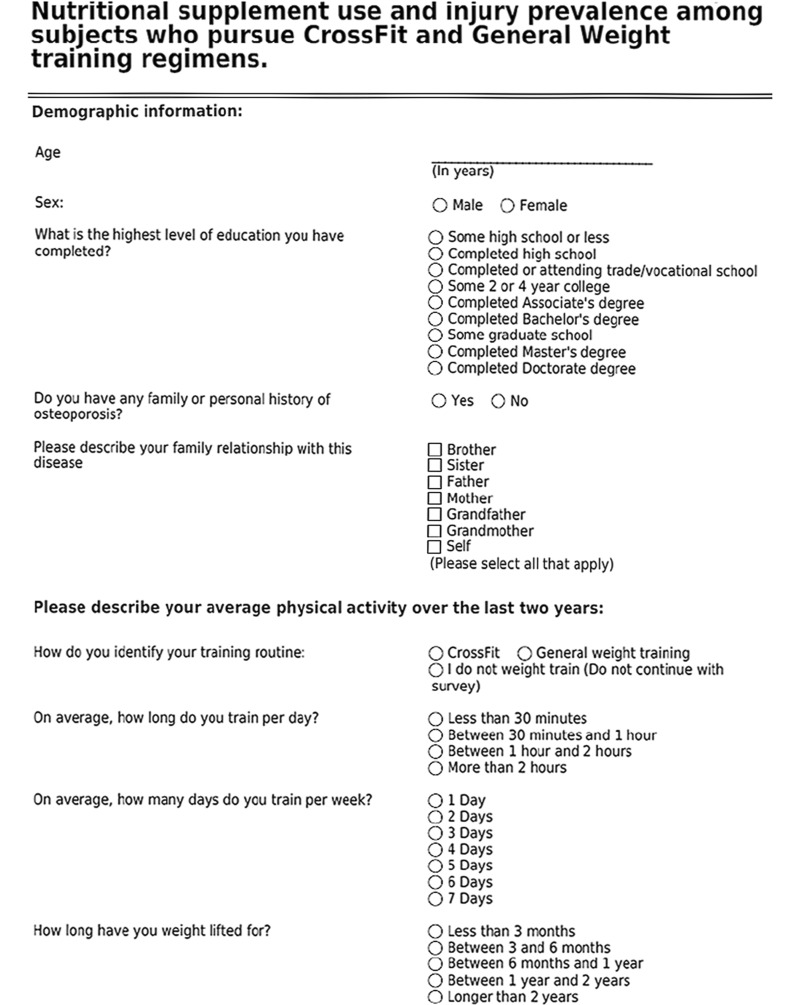
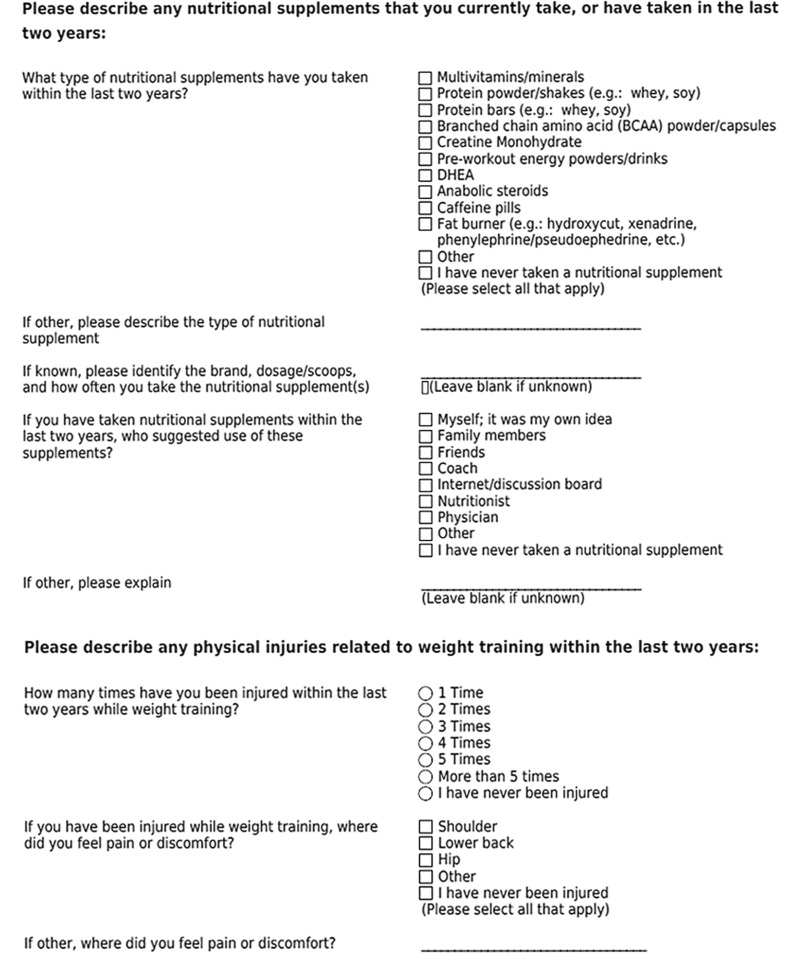
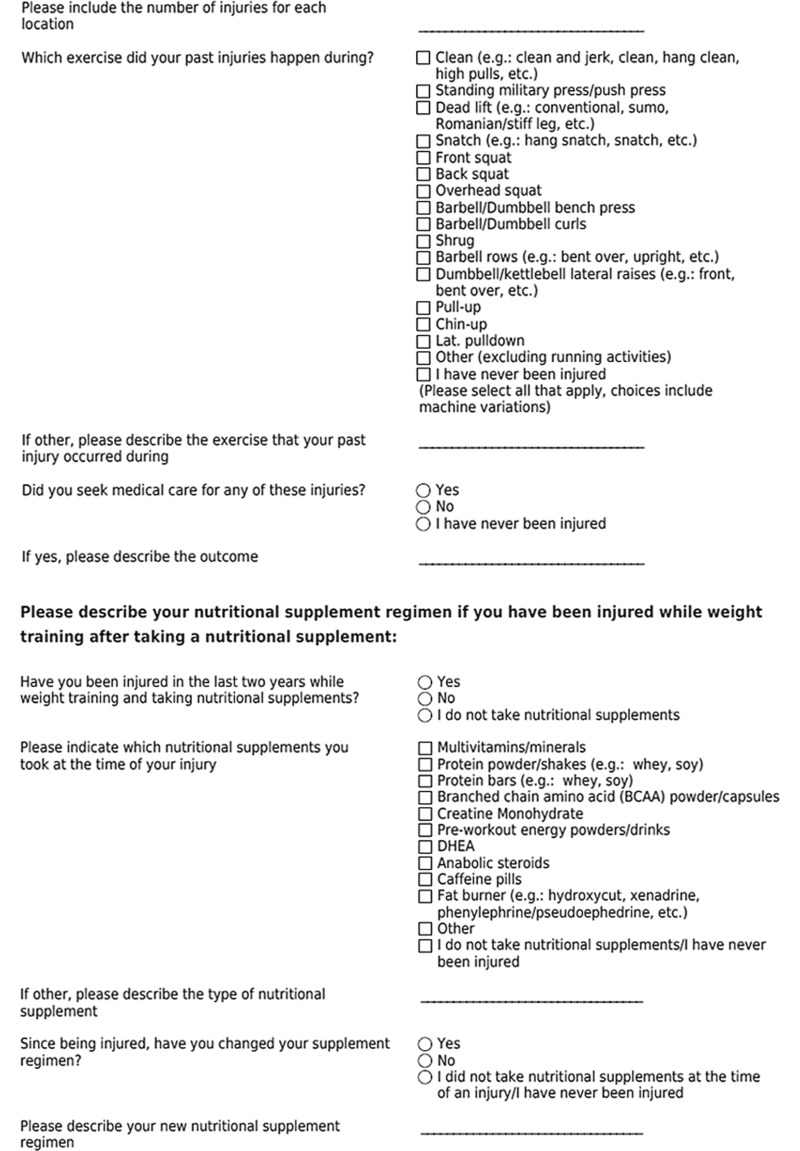
A survey consisting of 15 questions was developed to query physically active individuals regarding injury history and supplement use during the past 2 years (see the Appendix). In addition to providing demographic data, individuals were asked to define themselves as participants in either traditional weightlifting or CrossFit. Participants were instructed to self-determine whether an event should be considered an injury; no defined qualifiers were provided to participants. Individuals were also asked to list the body region injured, activity being performed at time of injury, and whether medical treatment was sought. The total composition of each workout during which an injury occurred was not requested. Participants listed the use of any supplements, including vitamins, anabolic steroids and their precursors, creatine, protein and amino acid powders and bars, and energy drinks. This study met the criteria for exempt research according to the policies of our institution and the provisions of applicable federal regulations.
From August 2015 through January 2016, the 15-question survey was distributed to 7 consenting fitness centers in the state of Pennsylvania (4 traditional fitness clubs and 3 CrossFit clubs) and 5 hospital and medical school email mailing lists hosted within our institution. These data were aggregated and subsequently maintained in a blinded manner. Volunteers at each facility anonymously completed the questionnaire. Study data were collected and managed through use of REDCap (research electronic data capture) tools hosted at our institution. This specific program was chosen for its secure, web-based application designed to support data capture for research studies and assist with analysis.
Data were collected through questionnaires in both paper and electronic form. The electronic forms were stored in REDCap. All responses were collected anonymously. The paper questionnaires were distributed at 7 gymnasiums within a 100-mile radius of the study area, and the electronic REDCap questionnaires were emailed to 5 mailing lists of our institution, which included the hospital and the college of medicine. We obtained written permission from the gymnasiums and email mailing list operators to distribute the questionnaires.
Study participants had to be 18 years or older and to identify as active weightlifters. Respondents were excluded if they were unable to consent or if they completed the questionnaire incorrectly or incompletely. The study population included those who self-identified as either CrossFit participants or traditional weightlifters. In our questionnaire, we defined traditional weightlifting as any action that involves the participant using free weights consistently. Although many CrossFit participants may fall into our definition of traditional weightlifting, participants of the survey were instructed to select only 1 group: CrossFit or traditional weightlifting.
Surveys distributed at gymnasiums were placed on a table near the entrance of the gym. A Summary Explanation of Research Document was provided with both electronic and paper surveys. Individuals who chose to participate in the study completed the paper questionnaire and placed it through the slit of a closed container adjacent to the recruitment flyer. Surveys that were completed electronically were automatically stored in REDCap after submission. Completion of the questionnaire implied voluntary consent to participate in the study.
If the questionnaire was completed incorrectly or incompletely, the survey was discarded and excluded from analysis. All data that were collected from the paper questionnaires were manually entered into the REDCap online questionnaire by a single investigator (J.L.E.) throughout the length of the study.
Data analyses were performed with SAS 9.4 software. The chi-square test, univariable relative risk, multivariant logistic regression, and 95% CIs were used to calculate the statistical significance between differences in injury likelihood between 2 groups. Statistical analyses involving comparison of means of continuous data were performed through use of unpaired t-test analyses. A multivariant logistic regression analysis was fit to assess the association of training routine, sex, and age with those sustaining at least 1 injury within the past 2 years and was used to estimate the relative risk of a dichotomous outcome. Statistical significance was set with a P value of less than .05.
Results
A total of 454 questionnaires were submitted. Of these, 43 (9.91%) were excluded based on inclusion and exclusion criteria. Of the 411 participants included, 122 (29.68%) self-identified as practicing a CrossFit routine whereas 289 (70.32%) followed a traditional weightlifting routine. The total included participants exceeded our desired sample size (400) to be representative of active weightlifters in the United States. The CrossFit respondents were significantly older on average (37.45 years) than those respondents participating in traditional weightlifting (31.62 years) (P < .0001). A significantly higher percentage of women comprised the CrossFit group (56.60%) compared with the traditional weightlifting group (30.10%) (P < .0001). Those participating in CrossFit reported exercising 4.40 days per week, whereas traditional weightlifters participated in a workout routine 4.50 days per week. Both groups reported training 1 to 2 hours per day.
In the 2 years prior to completing the questionnaire, 50.85% of respondents sustained a workout-related injury: 60.67% of those participating in CrossFit reported being injured during training compared with 46.71% of traditional weightlifters (P = .0098). Among the injured, 64.86% of CrossFit participants reported seeking medical care for the injury, whereas 34.81% of traditional weightlifters sought medical treatment (P < .0001). Those following a CrossFit routine were 1.30 times more likely to be injured and were 1.86 times more likely to seek medical attention following the injury compared with those using a traditional weightlifting routine. In a multivariant logistic regression analysis adjusting for sex and age, injury was 2.26 times more likely in the CrossFit group compared with the traditional weightlifting group (95% CI, 1.42-3.62; P = .0010).
The mean ± SD age of those injured within the past 2 years (32.82 ± 11.55 years) was not statistically different from the age of those who were not injured (33.90 ± 12.83 years) (P = .37). In a multivariant logistic regression analysis adjusting for training routine and sex, the injury risk was decreased by 13% for every 10-year increase in age.
Although a higher proportion of males reported being injured (54.51% of males vs 44.87% of females), no significant difference existed between sex and reported injury (P = .058). In a multivariant logistic regression analysis adjusting for training routine and age, the injury in the past 2 years was 1.80 times higher among males than females (95% CI, 1.17-2.75; P = .0070).
In both groups, the shoulder was the most common site of injury (46.41%), followed by lower back (38.28%) and hip (9.09%). CrossFit participants most commonly reported being injured while performing clean and jerk movements (18.90%), deadlift movements (18.90%), and snatch movements (16.20%), whereas traditional weightlifters were most commonly injured while performing barbell and dumbbell bench press movements (23.70%), deadlift movements (21.50%), and back squat movements (17.0%).
Most participants in each group (91.8% CrossFit, 88.2% traditional weightlifting; P = .29) reported supplement use. No significantly increased incidence of injury was found for respondents who reported supplement use compared with those who denied supplement use (39.78% vs 38.64%, P = .88). A breakdown of injury rate comparison of various supplements is presented in Table 1.
TABLE 1.
All-Subject Overall Injury Rates of Supplement Users Versus Nonusers
| Injury Rate, % (n/N) | |||
|---|---|---|---|
| Users | Nonusers | χ2 (P Value) | |
| Multivitamin | 53.03 (140/264) | 46.94 (69/147) | 1.40 (.24) |
| Protein powder | 54.30 (164/302) | 41.28 (45/109) | 5.43 (.020) |
| Protein bars | 56.67 (119/210) | 44.78 (90/201) | 5.81 (.016) |
| Branched chain amino acids | 61.22 (60/98) | 47.60 (149/313) | 5.54 (.019) |
| Creatine | 71.58 (68/95) | 44.62 (141/316) | 21.24 (<.001) |
| Preworkout energy | 59.85 (76/127) | 46.83 (133/284) | 5.95 (.015) |
| Dehydroepiandrosterone (DHEA) | 61.54 (8/13) | 50.50 (201/398) | 0.61 (.043) |
| Anabolic steroids | 83.33 (5/6) | 50.37 (204/405) | 2.57 (.11) |
| Caffeine | 51.52 (17/33) | 50.79 (192/378) | 0.0063 (.94) |
| Fat burner | 53.49 (23/43) | 50.54 (186/368) | 0.13 (.71) |
| Other | 61.76 (21/34) | 49.87 (188/377) | 1.77 (.18) |
Discussion
In the early 2000s, CrossFit emerged as a trendy and highly publicized exercise program. The workout uses a mixture of aerobics, calisthenics, and free weights in order to accomplish the “workout of the day.” CrossFit describes its program as highly intense and claims that it can be tailored to any fitness level.8 CrossFit engenders a camaraderie and competition that energize its participants and can push individuals to their personal limits. There is no doubt that adherence to the program leads to decreased body fat percentage, increased aerobic endurance, and increased lean body mass.13,17 CrossFit’s culture of strenuous exercise, however, leads to a more rapid rate of muscle fatigue than other weightlifting routines. Some experts claim that combining this muscle fatigue with the complex movements associated with Olympic weightlifting leads to an increased rate of injury among CrossFit participants compared with their general weightlifting counterparts.9 However, scientific data supporting this claim are limited.
Our study cohort of 411 individuals demonstrated that CrossFit participants carry 1.30 times higher risk of injury (95% CI, 1.075-1.57; P = .0067) and were 1.86 times more likely to seek medical attention following the injury than those using a traditional weightlifting routine (95% CI, 1.40-2.48; P < .0001). When the comparison of injury was adjusted for sex and age, the likelihood of sustaining an injury in the past 2 years was 2.26 times higher in the CrossFit group. Both groups appeared to exercise the same number of hours per week. According to our results, CrossFit participants were more likely to be women and were older than our cohort of traditional weightlifters. However, those who reported injury were significantly more likely to be male and younger than those who were not injured. The body region most likely to be injured was the shoulder.
These results parallel those reported by Weisenthal et al,20 who studied injury rates and patterns among 386 CrossFit athletes. Those authors similarly found that males were more likely to sustain injuries than females (P = .03) and that shoulder and lower back were the most common locations of injury. However, the injury rate in that study was 19.4% compared with the injury rate of 60.67% found in our CrossFit cohort. In the Weisenthal et al20 study, injury was more rigorously defined to occur within the past 6 months (as opposed to 2 years in our study) and to include at least 1 of the following criteria: (1) total removal from CrossFit training or other outside routine physical activities for more than 1 week; (2) modification of normal training activities in duration, intensity, or mode for more than 2 weeks; or (3) any physical complaint severe enough to warrant a visit to a health professional.20 In our study, injury was not defined in a comparable manner due to the subjective nature of injury and subsequent pain; if a participant recalled an injury within the past 2 years, we deemed this significant enough to be included. Furthermore, in the study by Weisenthal et al,20 injury rate was significantly decreased when a trainer was involved (P = .028). The use of a trainer was not investigated in our study. Furthermore, previous injury to the same area of reported injury was not queried in our study even though 1 study of CrossFit athletes indicated that 33.3% of reported injuries sustained were exacerbations of a previous injury.18
Overall, supplement use did not predispose individuals to an increased risk of injury. However, almost all supplements engineered for muscle building (protein powder and protein bars, branched chain amino acids, and creatine) and those marketed as preworkout energy drinks were associated with a significantly increased risk of injury. This finding may be a result of more consistent attendance or more strenuous activities attempted by those who used supplements for muscular gains as opposed to the general public. In addition, participants who used anabolic steroids and dehydroepiandrosterone (DHEA) had much higher rates of injuries, but comparisons with nonusers did not reach significance. This result is likely a result of the small sample size of those who reported anabolic steroid and DHEA use.
No data may be extracted from this study directly, but considering the combination of these findings, we surmise that even though CrossFit was associated with increased likelihood and severity of injury, the increased likelihood and severity of injury may had less to do with the exercises involved in CrossFit (many of the same exercises and body regions accounted for a similar percentage of injury in both CrossFit and traditional weightlifting groups) and more related to the intensity with which the exercises were performed. We defend this conclusion because, at its core, CrossFit provides an environment of “natural camaraderie, competition, and fun of sport or game”8 that combats the boredom that contributes to nonadherence to exercise routines. Specifically, an individual’s motivation to achieve his or her personal goals may increase when that person is exposed to a perceived obligation to either outperform others or to live up to the expectations of others cheering for the participant. This situation may lead CrossFit participants to push themselves beyond their own physical fatigue limit and may ultimately lead to technical form breakdown, loss of control, and injury. Perhaps a CrossFit trainer would be able to identify any alteration in form and, thus, protect the athlete from injury. These are certainly areas for further research.
We would expect that younger male bodybuilders participating in traditional weightlifting would carry similar increased injury risks. Therefore, we caution those who participate in CrossFit and traditional weightlifting and attempt to add muscle mass with muscle-building or preworkout energy supplements. This cohort should be especially careful when performing clean and jerk, deadlift, and snatch movements during CrossFit training and barbell and dumbbell bench press, deadlift, and back squat movements during traditional weightlifting. Undoubtedly, many of those who reported an injury concluded that the gains obtained from their workout routine outweighed the injury risk.
This study has several weaknesses. First, this study, like other survey studies, is subject to sampling and selection bias. Furthermore, the study may have underreported the total number of injuries because some individuals may have stopped exercising because of the injury. Second, all of the survey respondents were located within a 100-mile radius of the study site and may not be representative of other geographical areas. For example, our CrossFit group contained significantly more women and was significantly older than the traditional weightlifting group. This relationship may not represent the CrossFit population in other regions and may have skewed our data. Additionally, questionnaires sent to the earlier mentioned email lists did not contain unique links; the survey relied on integrity of its respondents to not complete multiple surveys. Third, we did not gauge the experience of the participant or the use of a trainer. Both a preparticipation training session and use of a trainer have been associated with decreased injury rates among CrossFit participants.20 Fourth, we did not determine whether the injury was a new injury or a reinjury of a preexisting condition. Fifth, the study used a broad definition of injury and, as such, injury numbers may have been over- or underreported attributable to participants not classifying an injury correctly due to lack of a proper definition. Additionally, although “seeking medical attention” may be viewed as a proxy for injury severity, we made no validated measure to quantify the extent of injury. Even though many participants reported sustaining an injury within the past 2 years, the injuries sustained were not severe enough to prevent these athletes from returning to physical activity or they would not have completed the survey, which was distributed only to those who were still exercising. Sixth, our definition of traditional weightlifting may encompass those within the CrossFit cohort; however, survey participants were asked to classify themselves into only 1 group. A combination group was intentionally excluded as an option, so as to discretely characterize outcomes based on what routine type participants identified with the most. Seventh, the recall accuracy may have introduced further bias into the study. Our inclusion criteria of injury held a longer time interval for recall than most other studies. Although the longer time interval allowed us to capture more injury data, it likely subjected the study to increased recall bias. One study7 of Australian football players who were asked to recall injury within the past year demonstrated that only 80% accurately recalled the number of injuries and body regions injured; however, all were able to recall the presence of an injury during that time period.
Conclusion
The study findings are summarized as follows:
Participants following a CrossFit routine were 1.30 times more likely to self-report an injury and were 1.86 times more likely to seek medical attention than those using a traditional weightlifting routine.
Among both CrossFit and traditional weightlifting participants, self-reported shoulder injuries were most common, followed by lower back injuries and hip injuries.
After adjustment for training routine and age, males were more likely to sustain a self-reported injury during CrossFit or traditional weightlifting.
After adjustment for training routine and sex, the likelihood of sustaining at least 1 self-reported injury during CrossFit or traditional weightlifting decreased by 13% for every 10-year increase in age.
CrossFit, the most well-known and frequently used high-intensity training program in weightlifting, is associated with an increased risk of injury compared with traditional weightlifting. As with participants in traditional weightlifting, CrossFit participants, especially those taking bodybuilding supplements and energy drinks, should “recognize their own limitations and challenges”3 to limit potential risk of injury.
Appendix
Study Questionnaire
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Penn State Clinical & Translational Research Institute, Clinical and Translational Science Awards (CTSA) program (NIH/NCATS grant numbers UL1 TR000127 and UL1 TR002014). The contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH or NCATS. R.A.G. has received research support from Aesculap. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Penn State College of Medicine Institutional Review Board (study ID No. 00003001).
References
- 1. Achauer H. Rise of the open. CrossFit Games https://games.crossfit.com/article/209585-rise-open. Published March 27, 2014. Accessed September 13, 2018.
- 2. Aune KT, Powers JM. Injuries in an extreme conditioning program. Sports Health. 2017;9(1):52–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Bergeron MF, Nindl BC, Deuster PA, et al. Consortium for Health and Military Performance and American College of Sports Medicine consensus paper on extreme conditioning programs in military personnel. Curr Sports Med Rep. 2011;10(6):383–389. [DOI] [PubMed] [Google Scholar]
- 4. Buist I, Bredeweg SW, Lemmink KAPM, van Mechelen W, Diercks RL. Predictors of running-related injuries in novice runners enrolled in a systematic training program: a prospective cohort study. Am J Sports Med. 2010;38(2):273–280. [DOI] [PubMed] [Google Scholar]
- 5. Calhoon G, Fry AC. Injury rates and profiles of elite competitive weightlifters. J Athl Train. 1999;34(3):232–238. [PMC free article] [PubMed] [Google Scholar]
- 6. Cooperman S. Getting fit, even if it kills you. New York Times. https://www.nytimes.com/2005/12/22/fashion/thursdaystyles/getting-fit-even-if-it-kills-you.html. Published December 22, 2005. Accessed September 13, 2018.
- 7. Gabbe BJ, Finch CF, Bennell KL, Wajswelner H. How valid is a self reported 12 month sports injury history? Br J Sports Med. 2003;37(6):545–547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Glassman G. Understanding CrossFit. CrossFit Journal. http://journal.crossfit.com/2007/04/understanding-crossfit-by-greg.tpl. Published April 1, 2007. Accessed September 13, 2018.
- 9. Hak PT, Hodzovic E, Hickey B. The nature and prevalence of injury during CrossFit training [published online November 22, 2013]. J Strength Cond Res. doi:10.1519/JSC.0000000000000318 [DOI] [PubMed] [Google Scholar]
- 10. Jayanthi N, Sallay HP, Przbylski M. Skill-level related injuries in recreational competitive tennis players. Med Sci Tennis. 2005;(10):12–15. [Google Scholar]
- 11. Korkia PK, Tunstall-Pedoe DS, Maffulli N. An epidemiological investigation of training and injury patterns in British triathletes. Br J Sports Med. 1994;28(3):191–196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Kühne CA, Zettl RP, Nast-Kolb D. Injuries—and frequency of complaints in competitive tennis- and leisure sports [in German]. Sportverletz Sportschaden. 2004;18(2):85–89. [DOI] [PubMed] [Google Scholar]
- 13. Murawska-Cialowicz E, Wojna J, Zuwala-Jagiello J. CrossFit training changes brain-derived neurotrophic factor and irisin levels at rest, after Wingate and progressive tests, and improves aerobic capacity and body composition of young physically active men and women. J Physiol Pharmacol. 2015;66(6):811–821. [PubMed] [Google Scholar]
- 14. Ozanian M. How CrossFit became a $4 billion brand. https://www.forbes.com/sites/mikeozanian/2015/02/25/how-crossfit-became-a-4-billion-brand/#35805b51f960. Published February 25, 2015. Accessed September 13, 2018.
- 15. Raske A, Norlin R. Injury incidence and prevalence among elite weight and power lifters. Am J Sports Med. 2002;30(2):248–256. [DOI] [PubMed] [Google Scholar]
- 16. Requa RK, DeAvilla LN, Garrick JG. Injuries in recreational adult fitness activities. Am J Sports Med. 1993;21(3):461–467. [DOI] [PubMed] [Google Scholar]
- 17. Smith MM, Sommer AJ, Starkoff BE, Devor ST. CrossFit-based high-intensity power training improves maximal aerobic fitness and body composition. J Strength Cond Res. 2013;27(11):3159–3172. [DOI] [PubMed] [Google Scholar]
- 18. Summitt RJ, Cotton RA, Kays AC, Slaven EJ. Shoulder injuries in individuals who participate in CrossFit training. Sports Health. 2016;8(6):541–546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Vriend I, Van Kampen B, Schmikli S, Eckhardt J, Schoots W, Den Hertog P. Ongevalsletsels en Sport kaart gehracht Amsterdam Consum en Veiligh. Ongevallen En Beweg Ned. 2005. [Google Scholar]
- 20. Weisenthal BM, Beck CA, Maloney MD, DeHaven KE, Giordano BD. Injury rate and patterns among CrossFit athletes. Orthop J Sports Med. 2014;2(4):2325967114531177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Winwood PW, Hume PA, Cronin JB, Keogh JWL. Retrospective injury epidemiology of strongman athletes. J Strength Cond Res. 2014;28(1):28–42. [DOI] [PubMed] [Google Scholar]