

Abstract
Fever may be the only sign of an underlying infection in neutropenic cancer patients. Unrecognized fever and untreated infections can lead to progressive sepsis and possibly death. The importance of early recognition, timely antibiotics, and treatment is crucial to favorable outcomes. The primary objective of this study was to evaluate the treatment of adult cancer patients with febrile neutropenia for compliance with National Comprehensive Cancer Network (NCCN) febrile neutropenia guidelines at our institution, UCHealth Memorial Hospital. Secondary objectives were to examine antibiotic selection, culture results, time to antibiotics, all-cause mortality, and length of hospital stay. This was a single-center, retrospective chart review of hospitalized neutropenic patients undergoing active chemotherapy. Neutropenia and fever were defined based on NCCN Guidelines. A total of 223 neutropenic patients were hospitalized between October 15, 2015, and December 31, 2016. Overall, 16 patients met the inclusion criteria for chemotherapy-induced neutropenia with fever. Compliance with the NCCN guideline standards was seen in seven (43.8%) patients. Antibiotics administered within 60 minutes of presentation was the lowest standard with adherence in eight (50%) patients. Empiric monotherapy antibiotic regimens were initiated in 11 (68.8%) patients; eight (50%) received cefepime and three (18.8%) received meropenem. At our institution, full compliance with the NCCN febrile neutropenia guidelines is not optimal. This study demonstrates the need for process improvement initiatives, including the addition of an electronic health record alert to flag patients undergoing active chemotherapy. It also warrants promoting the use of our institution’s emergency department febrile neutropenia treatment pathway to providers to improve overall compliance.
Febrile neutropenia is an oncologic emergency requiring immediate evaluation and treatment. It is associated with high rates of morbidity and mortality (Keng et al., 2015; Ko et al., 2015; Rosa & Goldani, 2014; Zuckermann et al., 2008). Fever may be the first or only sign that there is an underlying infection in neutropenic cancer patients (Rosa & Goldani, 2014). An inflammatory response can be suppressed in patients when the neutrophil-mediated component of the immune system is affected by myelosuppressive chemotherapy (Rosa & Goldani, 2014). Unrecognized fever and untreated infection can lead to progressive sepsis and possibly death. The importance of early recognition and timely antibiotics and treatment is crucial to favorable outcomes in these patients.
Several guidelines have been created by professional organizations for the evaluation and management of neutropenic fever in cancer patients. Recommendations from the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology for the Prevention and Treatment of Cancer-Related Infections are used to assist in the decision-making process about care for patients with febrile neutropenia (NCCN, 2017). These guidelines have been used to develop and implement an emergency department (ED) treatment pathway for patients who present with febrile neutropenia at our institution, UCHealth Memorial Hospital. However, availability of treatment pathways does not ensure adoption in clinical practice and may not always lead to changes in professional behavior (Zuckermann et al., 2008).
The NCCN Guidelines recommend empiric broad-spectrum antibiotics be initiated immediately after blood cultures have been drawn within 60 minutes of presentation of neutropenic fever. Intravenous (IV) antibiotic monotherapy with one of the following is listed as a Category 1 recommendation in the NCCN Guidelines: cefepime, imipenem, meropenem, or piperacillin-tazobactam (National Comprehensive Cancer Network, 2017). The NCCN Guidelines also address the use of empiric vancomycin, citing specific clinical scenarios where empiric vancomycin is recommended. These include clinically apparent IV catheter-related infections, blood cultures positive for gram-positive bacteria, known colonization of methicillin-resistant Staphylococcus aureus, clinical instability, and soft-tissue infection (National Comprehensive Cancer Network, 2017). The guidelines also recommend at least two sets of blood cultures with a set collected simultaneously from each lumen of an existing central line and from a peripheral vein site (National Comprehensive Cancer Network, 2017). Two blood culture sets from separate venipunctures should be sent if there is no central line. The initial laboratory tests should include a complete blood cell count (CBC) with differential analysis and blood chemistry tests to assess liver function (total bilirubin, albumin, alanine aminotransferase [ALT], aspartate aminotransferase [AST]) and renal function (blood urea nitrogen [BUN], creatinine, electrolytes; National Comprehensive Cancer Network, 2017).
Few studies have looked at general adherence to febrile neutropenia guidelines. The evidence suggests that there are wide variations in practice patterns regarding adherence to the NCCN Guidelines among providers (Wright et al., 2013). Underuse of ED pathways and historically inconsistent febrile neutropenia management may lead to adverse outcomes in this vulnerable population (Wright et al., 2013). The objective of this study was to examine compliance with NCCN febrile neutropenia guideline recommendations, including time to antibiotics, appropriate antibiotic treatment, blood cultures, and laboratory draws.
METHODS
This was a single-center, retrospective chart review of neutropenic patients aged 18 years or older, hospitalized between October 15, 2015, and December 31, 2016. Patients were identified in the electronic health record as neutropenic if they met the NCCN Guideline definition of less than or equal to 500 neutrophils/µL or less than or equal to 1,000 neutrophils/µL and predicted to decline to less than or equal to 500 neutrophils/µL within 48 hours of presentation (Figure 1). Patients were included in the analysis if they were (1) actively undergoing chemotherapy as noted in the chart and if they (2) presented with a fever within 12 hours of admission or prior to admission if clearly documented in the chart. Fever was defined by NCCN Guidelines to be a single oral temperature greater than or equal to 38.3°C or greater than or equal to 38.0°C sustained over 1 hour. Patients who were hospitalized for nonchemotherapy-induced neutropenia were excluded from the study.
Figure 1.

Selection of study patients
The primary endpoint was overall guideline compliance rates. Secondary endpoints included individual guideline compliance rates, antibiotic selection, culture results, time to antibiotics, all-cause mortality, and length of hospital stay. These endpoints were selected to determine if prolonged time to empiric therapy or choice of antibiotic was associated with morbidity and mortality. Data collected included patient demographics, cancer history, Eastern Cooperative Oncology Group (ECOG) performance status, documented patient allergies to antibiotics, use of granulocyte colony-stimulating factor (GCSF) for primary prophylaxis, empiric antibiotics administered within 60 and 120 minutes of presentation, antibiotic therapy, laboratory data on CBC with differential, comprehensive metabolic panel (CMP), and site of blood culture draw. Time to antibiotic administration was determined from the patient’s initial triage vital readings to the barcode scanning of the drug label. This was a conservative time frame that may have led to overreporting of guideline compliance since not all patients have vitals read immediately post check-in. All-cause mortality was collected solely from the electronic health record for a period of 3 months after hospitalization for febrile neutropenia. For data analysis, descriptive statistics were performed using Microsoft Excel.
RESULTS
A total of 223 neutropenic patients were hospitalized at our institution between October 15, 2015, and December 31, 2016. Overall, 16 patients met the defined inclusion criteria. Baseline characteristics are defined in Table 1. Nine (56.2%) patients were admitted to the oncology service and seven (43.8%) were admitted to the medical service. Patients’ primary cancer was classified into the following groups: breast (6 patients; 37.5%), colorectal (5 patients; 31.3%), leukemia (3 patients; 18.8%) or other (2 patients; 12.5%; esophageal cancer, myelodysplastic syndrome). Baseline ECOG performance status ranged from 0 to 2 upon admission, with nine (56.3%) patients having an ECOG performance status of 1. Primary prophylaxis with GCSF was noted in four (25%) patients. All four patients had a diagnosis of breast cancer and received a single dose of pegfilgrastim (Neulasta) after a dose-dense, high febrile neutropenia risk chemotherapy regimen.
Table 1.
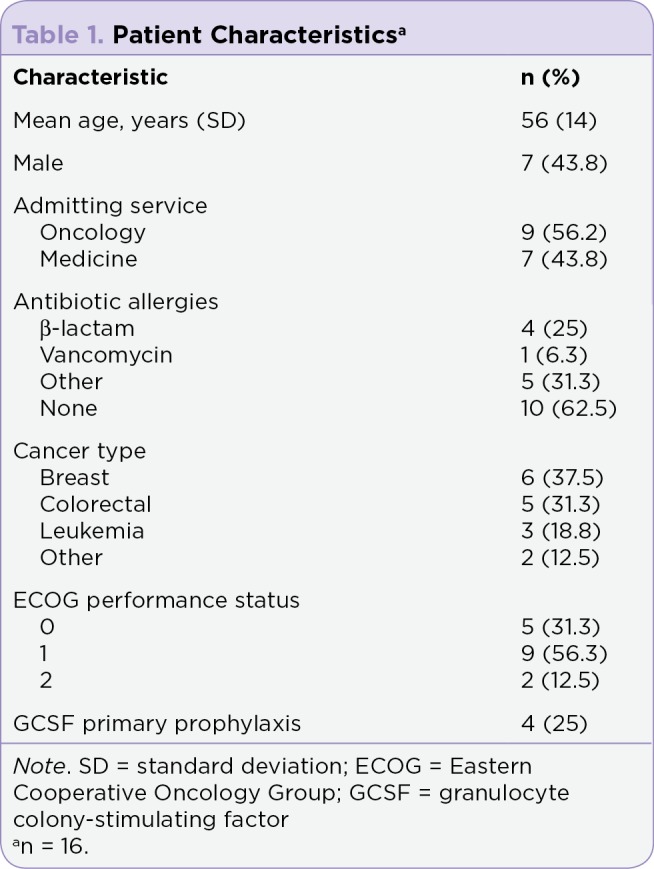
Patient Characteristicsa
Full compliance with the NCCN Guidelines was seen in seven (43.8%) hospitalized patients (Table 2). Empiric antibiotic therapy was started in all study patients; however, time to antibiotics differed among the population. An antibiotic initiated within the guideline standard recommendation of 60 minutes from presentation was recorded in eight (50%) patients, and a total of 12 (75%) patients had received antibiotics by 120 minutes. Two sets of blood cultures were drawn in 15 (94%) patients and 13 (81.3%) had at least two separate blood culture sites. Two patients who had two sets of cultures drawn fell out of compliance with the separate site guideline standard because it was not documented in the patient chart. Initial laboratory draws were completed in all study patients in compliance with guidelines.
Table 2.
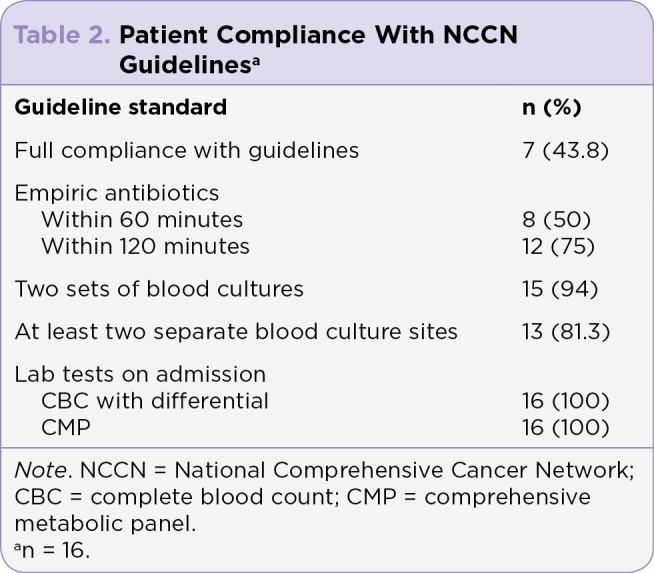
Patient Compliance With NCCN Guidelinesa
Secondary outcomes are reported in Table 3. Empiric antibiotic monotherapy was initiated with cefepime in eight (50%) patients and meropenem in three (18.8%) patients. A deciding factor for antibiotic selection was antibiotic allergy history. Of the four (25%) patients with β-lactam allergies, only one (6.3%) had an anaphylactic reaction and subsequently received meropenem empirically. Cefoxitin was ordered erroneously in one (6.3%) patient as initial empiric therapy and was immediately changed to cefepime after only one dose was given. The addition of vancomycin to empiric antibiotic therapy with cefepime was initiated in four (25%) patients. Two (50%) of the four patients were initiated on vancomycin based on documented clinical instability and/or sepsis per NCCN Guidelines. Other secondary outcomes included positive blood cultures, which were found in only two (12.5%) patients. These cultures reported either Escherichia coli or Streptococcus viridans. The all-cause mortality rate of 6.3% was due to a single patient who died of progression of their cancer diagnosis within 10 months from admission. The overall median hospital length of stay was found to be 4 days.
Table 3.
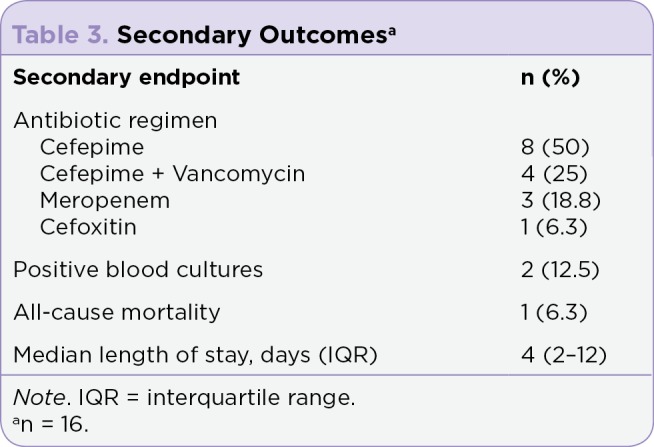
Secondary Outcomesa
DISCUSSION
This study included patients with a wide range of baseline characteristics with varying chemotherapy regimens and cancer diagnoses. Although this study was originally designed to include all types of patient admissions, all study patients were admitted through the ED during the study time frame. Despite the fact that all patients presented to the ED with febrile neutropenia, there were four patients who also presented to an outpatient clinic prior to coming to the ED for evaluation. This key piece of information may help to identify areas of improvement in the treatment of our febrile neutropenic patients. Special consideration should be made to patients who present with a fever and low neutrophil count at their outpatient oncology clinic visit. These patients would be candidates for a direct admission to the hospital if the provider categorized them as high risk or requiring IV antibiotic therapy. A direct admission to the hospital has the possibility of decreasing time to empiric antibiotics and improving patient outcomes. Additionally, our organization is working on a process to identify low-risk patients who may qualify for oral antibiotic therapy at home.
Appropriate monotherapy empiric antibiotics were initiated in 11 (68.8%) patients. These included regimens with cefepime or meropenem. Both of these antibiotics are Category 1 recommendations from the NCCN Guidelines for the treatment of febrile neutropenia. Our rates were lower in comparison to a previous study that found guideline-based antibiotics were administered to 79% of febrile neutropenic patients over a 10-year timeframe (Wright et al., 2013). Out of the four patients (25%) initiated on empiric vancomycin, two (50%) were initiated appropriately per guideline standards. These two patients presented with clinical instability and/or sepsis, which was documented by the provider on admission in the patient chart. Wright and colleagues (2013) also found widespread use of empiric vancomycin in 37% of their study cohort, which was higher in comparison to our study population. The appropriate initiation of empiric vancomycin was identified as an opportunity for improvement at our institution. Vancomycin was started on two patients without a clear indication or documented reasoning. In these cases, vancomycin was initiated before an oncologist was consulted to care for the patients. An opportunity for improvement includes education to ED providers and hospitalists regarding the use and indication for empiric vancomycin therapy.
Full compliance with NCCN Guideline standards was seen in seven (43.8%) patients. A strength of this study was that all guideline standards were included in this analysis. Antibiotic therapy initiated within 60 minutes of presentation was reported as the lowest standard in eight (50%) patients. Prolonged time to antibiotic administration has been associated with increased hospital length of stay with community-acquired pneumonia. The Surviving Sepsis Campaign has shown that antibiotics within the first hour after recognition has improved survival rates (Keng et al., 2015; Rhodes et al., 2017). In the febrile neutropenic population, a previous cohort study found that early antibiotic administration was associated with higher survival rates, and with each hour delay in the time to antibiotics, the risk for mortality increased by 18% (Rosa & Goldani, 2014). Due to the low inclusion rate of our study, we failed to show any association between prolonged time to antibiotics and mortality.
A focus area in our institution’s ED febrile neutropenic treatment process was to decrease time to antibiotics. In order to shorten the time to treatment, early recognition of febrile neutropenic patients is crucial. We are currently investigating the implementation of an electronic health record alert to flag patients who have active chemotherapy orders. This may help identify febrile patients who present with no other symptoms and who do not yet have a CBC resulted. This can also encourage the early treatment of patients who present with reported fevers from home and who may have taken an antipyretic prior to admission to ED.
One of the major challenges of this study design was the difficulty in correctly identifying patients with febrile neutropenia. Many patients presented with subjective fever prior to admission that was not subsequently documented. This significantly limited the number of patients eligible for inclusion. At our institution we have a high-volume ED, approximately 135,000 visits annually, with high-acuity patients and a significant number of patients with nonchemotherapy-induced neutropenia. These neutropenic patients had diagnoses that included viral leukopenia, chronic thrombocytopenia, and sepsis. Additionally, the retrospective study design may have limited the clinical picture and presentation of study patients. Time from onset of fever to antibiotic administration was not included in this study. This factor could affect the relationship between time from ED presentation to antibiotics and patient outcomes. Lastly, this study was performed at a single center and caution should be taken when generalizing the results. A future study should expand the eligibility time frame by at least 10 years to include more patients in the final analysis and increase study power.
To improve the treatment of febrile neutropenia at our institution, it is important to promote the use of our institution’s ED febrile neutropenia pathway to providers. Since the end of the study period, our hospital has implemented the use of IV push antibiotics in the ED, including cefepime. This may also play a role in reducing time to treatment. Education to staff at our institution will focus on time sensitivity in the recognition of febrile neutropenic patients and the appropriate initiation of empiric vancomycin. Finally, the consideration of direct admission for patients presenting to outpatient clinics or reporting fever at home also presents an opportunity for decreasing the time to treatment.
Current literature demonstrates the importance of the relationship between time to antibiotics and outcomes in septic patients (Rhodes et al., 2017). Although our study findings lack power, they still support the need for early recognition and treatment in not only septic patients, but also in those presenting with febrile neutropenia. Our results highlight the need for education to providers to ensure guideline standards are being met. This study adds to the literature by assessing all guideline standards for the initial management of febrile neutropenia in addition to time to antibiotic administration. We have identified factors to target for process improvement based on these standards.
CONCLUSION
The results of this study suggest that overall NCCN Guideline adherence at our institution is low, especially with respect to time to initiate antibiotics within 60 minutes of presentation. In addition, there is inappropriate initiation of empiric vancomycin in this patient population as defined by the NCCN Guidelines.
Based on the results of this study, our institution is working on implementing provider training, including early recognition of febrile neutropenic patients, use of our institution’s ED febrile neutropenia treatment pathway, and appropriate indications for empiric vancomycin. Future studies are necessary to further assess the effectiveness of the implementation of these process improvement plans.
Footnotes
Dr. Jeffers has served on the advisory board for Takeda Oncology and Tesaro. Dr. Goldsmith and Dr. Kalis have no conflicts of interest to disclose.
References
- 1.Keng Michael K, Thallner Elaine A, Elson Paul, Ajon Christine, Sekeres Jennifer, Wenzell Candice M, Seastone David J, Gallagher Erika M, Weber Catherine M, Earl Marc A, Mukherjee Sudipto, Pohlman Brad, Cober Eric, Foster Virginia B, Yuhas Joy, Kalaycio Matt E, Bolwell Brian J, Sekeres Mikkael A. Reducing Time to Antibiotic Administration for Febrile Neutropenia in the Emergency Department. Journal of oncology practice. 2015;11:450–455. doi: 10.1200/JOP.2014.002733. [DOI] [PubMed] [Google Scholar]
- 2.Ko Byuk Sung, Ahn Shin, Lee Yoon-Seon, Kim Won Young, Lim Kyung Soo, Lee Jae-Lyun. Impact of time to antibiotics on outcomes of chemotherapy-induced febrile neutropenia. Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer. 2015;23:2799–2804. doi: 10.1007/s00520-015-2645-5. [DOI] [PubMed] [Google Scholar]
- 3.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Prevention and Treatment of Cancer-Related Infections. v2.2017. 2017 Retrieved from https://www.nccn.org/professionals/physician_gls/pdf/infections.pdf.
- 4.Rhodes Andrew, Evans Laura E, Alhazzani Waleed, Levy Mitchell M, Antonelli Massimo, Ferrer Ricard, Kumar Anand, Sevransky Jonathan E, Sprung Charles L, Nunnally Mark E, Rochwerg Bram, Rubenfeld Gordon D, Angus Derek C, Annane Djillali, Beale Richard J, Bellinghan Geoffrey J, Bernard Gordon R, Chiche Jean-Daniel, Coopersmith Craig, De Backer Daniel P, French Craig J, Fujishima Seitaro, Gerlach Herwig, Hidalgo Jorge Luis, Hollenberg Steven M, Jones Alan E, Karnad Dilip R, Kleinpell Ruth M, Koh Younsuk, Lisboa Thiago Costa, Machado Flavia R, Marini John J, Marshall John C, Mazuski John E, McIntyre Lauralyn A, McLean Anthony S, Mehta Sangeeta, Moreno Rui P, Myburgh John, Navalesi Paolo, Nishida Osamu, Osborn Tiffany M, Perner Anders, Plunkett Colleen M, Ranieri Marco, Schorr Christa A, Seckel Maureen A, Seymour Christopher W, Shieh Lisa, Shukri Khalid A, Simpson Steven Q, Singer Mervyn, Thompson B Taylor, Townsend Sean R, Van der Poll Thomas, Vincent Jean-Louis, Wiersinga W Joost, Zimmerman Janice L, Dellinger R Phillip. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive care medicine. 2017;43:304–377. doi: 10.1007/s00134-017-4683-6. [DOI] [PubMed] [Google Scholar]
- 5.Rosa Regis G, Goldani Luciano Z. Cohort study of the impact of time to antibiotic administration on mortality in patients with febrile neutropenia. Antimicrobial agents and chemotherapy. 2014;58:3799–3803. doi: 10.1128/AAC.02561-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Wright Jason D, Neugut Alfred I, Ananth Cande V, Lewin Sharyn N, Wilde Elizabeth T, Lu Yu-Shiang, Herzog Thomas J, Hershman Dawn L. Deviations from guideline-based therapy for febrile neutropenia in cancer patients and their effect on outcomes. JAMA internal medicine. 2013;173:559–568. doi: 10.1001/jamainternmed.2013.2921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Zuckermann J, Moreira L B, Stoll P, Moreira L M, Kuchenbecker R S, Polanczyk C A. Compliance with a critical pathway for the management of febrile neutropenia and impact on clinical outcomes. Annals of hematology. 2008;87:139–145. doi: 10.1007/s00277-007-0390-7. [DOI] [PubMed] [Google Scholar]