

Abstract
The use of sterile surgical gloves in wound dressing is not new. It has been used previously in dressing of fresh wounds and in adjunct to the negative pressure wound management. Herein we describe an interesting case of burn wound dressing of hand in a child. Low cost, easy availability, better patient compliance and lesser chances of wound infection are special attributes of glove dressing.
Keywords: Burn, latex gloves, scalds, silver sulfadiazine, wound
Introduction
Sterile Surgical gloves (SSgl) are generally used in the operating room during surgical procedures.[1] Sterilized single use medical gloves are used in the wards for dressing change.[2] SSgl has been mentioned previously for skin graft fixation after fresh burn on the hand.[3] They have also been utilized to fix skin graft in adjunct to negative pressure therapy to resurface burn wounds after correction of severe post burn contractures.[4] In the following case description, we illustrate a simple, compliant method of hand burn wound dressing in a paediatric patient.
Case Description
A 1-year-old male toddler arrived in emergency services with burns on the right hand. A detailed history by his mother revealed the cause of burn to be scalds due to accidental hand immersion in a bucket of hot water at home. Immediately after the burn, some antibiotic ointment was applied over the affected hand and he was rushed to a nearby primary health care facility. In the dispensary after a formal survey, some antibiotic ointment was applied over the burnt area and dressed with sterile cotton gauze.
On presentation at our emergency, the child was restless and febrile with a temperature of 100.8 Fahrenheit (F). A quick general survey was done, and tetanus immunization was administered. A through local examination revealed second degree deep dermal burn on the right hand involving both the dorsal [Figure 1a] and palmar aspects [Figure 1b]. Under Ketamine anesthesia, the affected hand was washed thoroughly with normal saline and all blisters debrided. No fasciotomy was deemed necessary. Silver sulfadiazine cream (SSD) 1% was applied evenly over the burnt hand and dressing done with sterile cotton gauze pads and bandaged. Oral antibiotic and paracetamol were given after the child was fully conscious.
Figure 1.
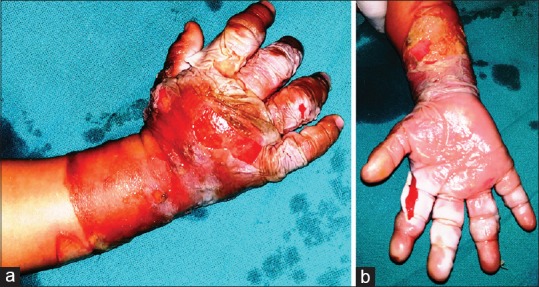
(a): Dorsal view of the burnt right hand on presentation, (b): Palmar view of the burnt right hand on presentation
The next day the child was again restless. He had two spikes of fever, highest being 102.4 F. Intravenous fluids and precautionary antibiotics were started. The dressing was soaked, and we observed dirt over the soaked area probably due to surface contact with surroundings by the anxious child. The child was again taken to the operating room for dressing change. After removing the soaked dressing, the SSD cream was washed off with normal saline. The entire area was again covered with SSD cream [Figure 2a]. This time the wound with the antibiotic on it was covered a No. 6 latex sterile surgical glove. [Figure 2b] The subsequent pictures of wound healing are shown from Figures 3 and 4.
Figure 2.

(a): A thick layer of 1% SSD cream applied on the burnt right hand before applying glove dressing. (b): “Hand in glove dressing” applied to the entire burnt right hand. (c): Malleable splint applied on the burnt right hand over the “hand in glove dressing”
Figure 3.

(a): Palmar view of the partially healed wound on day 11. (b): Dorsal view of the partially healed wound on day 11
Figure 4.
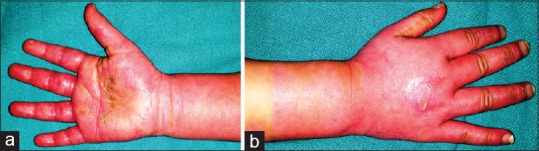
(a): Palmar view of completely healed wound on day 18. (b): Dorsal view of completely healed wound on day 18
Subsequent dressing changes were done on alternate days. We recorded normal temperatures of the child after second dressing change. The child allowed dressing change without any anesthesia after fourth dressing. The child was discharged from the hospital on the 12th day. Regular hand physiotherapy was advised to the parents during the day and malleable splint [Figure 2c] was given for the night to avoid any post burn contracture formation. The child has been on regular follow up for two months now. The progress of wound healing has been shown at day 11 on both palmar [Figure 3a] and dorsal aspect [Figure 3b]. All his wounds have healed satisfactorily on palmar aspect [Figure 4a] and dorsal aspect [Figure 4b] at day 18. Parents are continuing massage therapy and splintage as suggested to them.
Discussion
Scalds are the most common cause of burn injuries in children[5] Children are more susceptible to hand burns due to their inquisitive behavior.[6] Pediatric skin is thinner and their inherent slower withdrawal response from burn source often causes deeper burns at lower temperatures.[7] Fortunately they have a thicker subcutaneous adipose tissue which prevents tendon injuries even in deeper injuries.[7]
Most of the second degree burns on the hand in children do not require surgical intervention.[7] They can be efficiently managed by thorough wound cleansing followed by dressing with a broad-spectrum antibiotic cream like SSD.[8] This is followed by upper limb elevation which reduces edema on the hands and eventually assists in faster healing. This gives satisfactory results in adults mostly as they are compliant this therapy.
In children, however, the scenario is slightly different. Many a times we have noticed that after a burn injury, they are restless. They are not stable at one place and wish to move around. In the process, they place their dressed hand to various objects around. This leads to contamination of the dressing with dirt and if the dressing is soaked then it will cause local wound sepsis. This eventually leads to systemic symptoms and abnormal wound healing with unfavorable sequelae like septicemia and hand contractures in the long run. The wound management can be ameliorated with glove dressing.
The gloves that we used in the dressing are made up of natural rubber latex [Figure 5a]. It is sterilized with ethylene oxide or gamma irradiated and is powder free [Figure 5b]. These gloves are available free of cost in our hospital through government funding. The smallest size available (no. 6) was used in our case [Figure 5b]. The wound, SSD cream, and then the gloves complex is then covered with a sterile gauze cotton and bandage.
Figure 5.
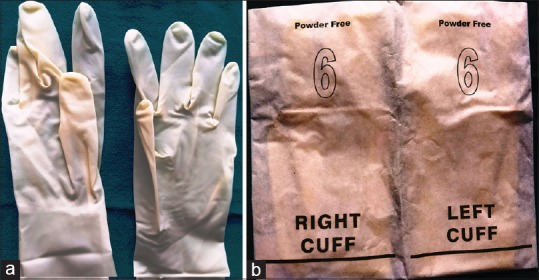
(a): Latex surgical gloves no. 6 is used for wound dressing. (b): Commonly used sterile powder free latex surgical glove pack that is commonly available in the hospital
We noticed from the first dressing onwards that the child was more relaxed as he could move his hand more freely now. Parents were also less concerned with controlling the hands of their child. We could also find less antibiotic cream seepage onto the outer dressing which also means diminished chances of wound contamination from outside sources. This intrinsic compliance from the child boosted the confidence of the parents which led to their better participation during dressing changes and ultimately prompted excellent results. However, these gloves have essential disadvantage of latex allergy.[9] Caution is warranted in its indiscriminate use. Proper clinical profile of the child regarding any kind of allergy is required to avoid any undesirable situation. A prospective study with large number of patients will outline its safe usage guidelines to optimize results.
Conclusion
Sterile surgical glove can be a useful method of dressing of hand burn specifically in pediatric patients. Low cost, ubiquitous availability, patient compliance, and lesser chances of wound infection can lead to its wider usage.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Tanner J. Choosing the right surgical glove: An overview and update. Br J Nurs. 2008;17:740–4. doi: 10.12968/bjon.2008.17.12.30292. [DOI] [PubMed] [Google Scholar]
- 2.Kramer A, Assadian O. Indications and requirements for single-use medical gloves. GMS Hyg Infect Control. 2016;11:Doc01. doi: 10.3205/dgkh000261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mashiko T, Ohnishi F, Oka A, Kawauchi T, Shiokawa I, Yamakawa T, et al. Usefulness of surgical glove dressing: A novel technique for skin graft fixation after hand burns. J Plast Reconstr Aesthet Surg. 2013;66:1304–6. doi: 10.1016/j.bjps.2013.04.031. [DOI] [PubMed] [Google Scholar]
- 4.Kamolz LP, Lumenta DB. Topical negative pressure therapy for skin graft fixation in hand and feet defects: A method for quick and easy dressing application—the “sterile glove technique”. Burns. 2013;39:814–5. doi: 10.1016/j.burns.2012.09.019. [DOI] [PubMed] [Google Scholar]
- 5.Krishnamoorthy V, Ramaiah R, Bhananker SM. Pediatric burn injuries. Int J Crit Illn Sci. 2012;2:128–34. doi: 10.4103/2229-5151.100889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Abu-Sittah GS, El Khatib AM, Dibo SA. Thermal injury to the hand: Review of the literature. Ann Burns Fire Disasters. 2011;24:175–85. [PMC free article] [PubMed] [Google Scholar]
- 7.Feldmann ME, Evans J, O SJ. Early management of the burned pediatric hand. J Craniofac Surg. 2008;19:942–50. doi: 10.1097/SCS.0b013e318175f38d. [DOI] [PubMed] [Google Scholar]
- 8.Fox CL, Jr, Modak SM. Mechanism of silver sulfadiazine action on the burn wound infections. Antimicrob Agents Chemother. 1974;5:582–8. doi: 10.1128/aac.5.6.582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kumar RP. Latex allergy in clinical practice. Indian J Dermatol. 2012;57:66–70. doi: 10.4103/0019-5154.92686. [DOI] [PMC free article] [PubMed] [Google Scholar]