

Abstract
Entero-urinary fistulas are uncommon in urological practice and may have widely varying aetiologies ranging from benign to malignant or iatrogenic in nature. All permutations of entero-urinary fistulas have been reported in the literature except an appendico-renal fistula. Here, we present one such case, presenting with urinary tract infections and perineal urethrocutaneous fistulae. He was ultimately diagnosed to have a spontaneous appendico-renal fistula as underlying pathology behind the symptoms.
Keywords: urinary tract infections, urethritis, urological surgery, urology
Background
Appendico-urinary fistulas are rare clinical entities often diagnosed only during surgical exploration. While appendix-vesical and ureteric fistulas are known, an appendico-renal fistula has never earlier been reported. Herein, we describe a rare case of spontaneous reno-appendicular fistula in association with chronic granulomatous pyelonephritis presenting as non-healing urethrocutaneous fistulae in the perineum. Such appendico-renal fistula has not been described previously in the literature.
Case presentation
A 20-year-old man presented with conditions of bilateral flank pain for 12 years. He had earlier undergone open cystolithotomy and left pyelolithotomy, 16 and 12 years back, respectively. This time, he presented at an outside centre with perineal abscess for which incision and drainage was done precipitating urethracutaneous fistulae at the base of penis and perineum. In view of these findings, suprapubic cystostomy (SPC) was done. Ultrasonography suggested bilateral renal stones. Six months later, a urethrocystoscopy was performed at the same centre reporting mild bulbar urethral narrowing and suprapubic cystostomy (SPC) was removed. However, in view of non-resolution of fistulae, he was referred to our tertiary care centre.
Investigations
The suprapubic catheter was replaced. Retrograde urethrogram (figure 1) showed multiple urethrocutaneous fistulae with mild bulbar urethral narrowing. Ultrasonography and Non-contrast CT abdomen showed right staghorn renal calculus with marked perinephric and periureteric fat stranding and left inferior calyceal calculus. On renal dynamic scan, the right kidney was not visualised and the left kidney was normal.
Figure 1.

(A) Retrograde urethrogram showing proximal bulbar urethracutaneous fistula with distal narrowing. (B) Non-contrast CT showing right xanthogranulomatus changes (dashed circle). A thickened inflamed luminal structure (double arrow) with tiny concretions and lying in the vicinity was later identified as appendix on surgical exploration.
Treatment
Considering stones as a cause of recurrent infections and non-healing of fistulae, it ws decided to clear the patient of all stones before any reconstructive surgery for urethra and fistulae. A diagnostic urethrocystoscopy and left retrograde intrarenal surgery was performed. Scopy revealed a normal penile urethra, multiple false tracts and synechiae in bulbar urethra. The bladder was normal. Left inferior calyceal calculus was fragmented and extracted. Double J stent was removed subsequently.
Right nephrectomy was then planned. A repeat non contrast computed tomography (NCCT) was done to ensure clearance on the left side. It also showed irregular and small right kidney with perinephric inflammatory changes with renal calculus and extrarenal calcifications with an inflamed appendix with appendicolith. Amid dense intraoperative adhesions to duodenum, colon and liver, the appendix was also found pulled up and adherent to renal parenchyma on the anterior aspect. A definite appendico-renal fistula was demonstrated between the appendix and the pelvicalyceal system of the kidney spanning through the parenchyma (figure 2).
Figure 2.
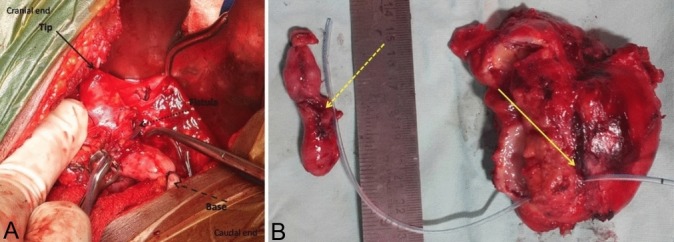
(A) Intraoperative image during right nephrectomy through combined extraperitoneal and intraperitoneal flank approach, showing the appendix adherent to renal parenchyma and forming appendico-renal fistula (dotted arrow). A feeding tube could be passed easily into the pelvicalyceal system. The tip of the appendix is cranial (bold arrow) while its base (dashed arrow) has been ligated and separated from the cecum. (B) Specimen demonstrating appendico-renal fistula with a feeding tube going into the pelvicalyceal system through the fistula opening (bold Arrow) and coming out through the laterally opened kidney specimen. Dashed arrow represents the corresponding opening in the mid of appendix.
Outcome and follow-up
Histopathology of the specimen revealed chronic pyelonephritic changes with large necrotising granulomas and focal bone formation. No xanthogranulomatous change or acid-fast bacilli were noted and tubercular culture was negative. There were mixed inflammatory infiltrates and transmural ulceration in the appendix and numerous triple phosphates crystals identified in its luminal aspect. The patient had an uneventful recovery. By 3 months, the urethrocutaneous fistulae had also healed spontaneously. On clamping the suprapubic catheter, the patient was able to void with good flow without any difficulty. The SPC was removed after 1 week. Urethra was re-evaluated to be normal during percutaneous nephrolithotomy for the left renal calculus after 4 months. He was asymptomatic at 1-year follow-up.
Discussion
Appendico-urinary fistulae have been described as complications of appendicitis. However, they are rare presentations of an otherwise frequent diagnosis. While appendico-vesical fistulisation is the most common scenario in a spontaneous onset appendico-urinary fistula, appendico-ureteric fistula following appendicitis has also been documented. Renal involvement in the form of renal cellulitis, acute pyelonephritis or calyceal rupture following acute obstruction of ureter has been described as a complication of an appendicitis.1 2 However, by virtue of the relative far location of kidney from the appendix, and thick parenchyma a reno-appendicular fistula has never earlier been reported to the best of our knowledge.
The exact cause of appendico-renal fistula in our case remains unconfirmed. Xanthogranulomatous inflammation does have the tendency to involve adjacent organs and may lead to fistula formation. Reno-colic and reno-cutaneous fistula have been described in its presence. Rare presentations, such as reno-pleural fistula, are also described as a complication of chronic pyelonephritis.3–5 However, neither renal pathologies nor appendicitis complications are known to incite appendico-renal fistula as such.
Xanthogranulomatous pyelonephritis is classified into three stages: stage I—the lesion is confined to the kidney (nephric), stage II—when it extends to Gerota’s space (perinephric) and stage III—the extension to the perinephric space or retroperitoneal structures (paranephric) by Malek et al.6
A preoperative contrast CT scan may add valuable clinical information, especially in such complicated cases. However, because we did not suspect a reno-enteric fistula, based on history, examination and other available investigations, we did not ask for contrast CT. Whether a fistula would have been picked up even with CECT remains unknown given the fact that kidney was absolutely non-functional and the fistula was with appendix. Complications following inflammation of the appendix, including abscess formation, perforation and appendicular lump formation are not uncommon. In this particular case, the patient did not have any symptoms that could have suggested gastrointestinal tract involvement. However, retrograde reassessment of the NCCT does suggest the presence of an appendicolith, and appendix lying in close relation to the anterior aspect of the right kidney. Oral and intravenous contrasts were not given during the CT study as fistula was not suspected based on clinical evaluation. Another peculiarity, in this case, is the intraperitoneal location of the appendix. A retrocolic fixed location of the appendix brings the appendix in relative proximity to the urinary tract. Despite the intraperitoneal location, only appendix being involved in the inflammatory process of the kidney is intriguing, raising suspicion that it might be an appendicular pathology to start with and involving kidney and urinary tract secondarily. However, a prior history of stone disease and renal stones on imaging point it to be a renal pathology. The clinical presentation of this case as non-resolving urethrocutaneous fistulae is also uncommon, with most common presentations being flank pain, fever, weight loss, anorexia or a renal mass.7 Presence of an entero-urinary fistula renders a patient prone to urinary infections and one such lower urinary tract infection would have likely led to development of perineal abscess in this case. Regardless, appendiculo-renal fistula is a very rare entity and extensive literature search did not yield any report mentioning such findings.
Learning points.
This case re-emphasises the possibility of entero-urinary fistula as a cause of recurrent urinary infection and non-healing urethritis/urethral fistulae.
Appendico-renal fistula is very rare, owing to anatomical remoteness between the two organs.
Treating the seat of recurrent infections is must and prerequisite before any reconstructive procedure is contemplated.
Footnotes
Contributors: We (RN and PK), the authors of the manuscript titled ’Spontaneous appendico-renal fistula: clinical presentation and management of a previously unreported entity' hereby state that we have made an individual contribution to the writing of the article and not just been involved with the patient’s care. Substantial contribution has been made by both of us in the conception and design, acquisition of data or analysis and interpretation of data, drafting the article or revising it critically for important intellectual content and final approval of the version published. We agree to be accountable for the article and to ensure that all questions regarding the accuracy or integrity of the article are investigated and resolved.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
Patient consent for publication: Obtained.
References
- 1. Jones WG, Barie PS. Urological manifestations of acute appendicitis. J Urol 1988;139:1325–8. 10.1016/S0022-5347(17)42911-9 [DOI] [PubMed] [Google Scholar]
- 2. Mammen A, Ponnambathayil S, Varma KK, et al. A rare complication of appendicitis: appendiculorenal sinus with renal cellulitis. Pediatr Surg Int 2005;21:582–4. 10.1007/s00383-005-1450-5 [DOI] [PubMed] [Google Scholar]
- 3. Arriagada S D, Donoso F A, Cruces R P, et al. [Nephrobronchial fístula in pediatric patient: case report]. Arch Argent Pediatr 2014;112:e156–9. 10.5546/aap.2014.e156 [DOI] [PubMed] [Google Scholar]
- 4. Soeprijanto B, Djatisoesanto W, Sandhika W. Communicating fistula between colocutan and nephrocutan with renal stones and renal replacement lipomatosis. A case report. Urol Case Rep 2017;10:16–18. 10.1016/j.eucr.2016.10.012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Park BK, Kim GH. [Pyeloduodenal fistula caused by renal calculi]. Korean J Gastroenterol 2018;71:229–33. 10.4166/kjg.2018.71.4.229 [DOI] [PubMed] [Google Scholar]
- 6. Malek RS, Elder JS. Xanthogranulomatous pyelonephritis: a critical analysis of 26 cases and of the literature. J Urol 1978;119:589–93. 10.1016/S0022-5347(17)57559-X [DOI] [PubMed] [Google Scholar]
- 7. Bingöl-Koloğlu M, Ciftçi AO, Senocak ME, et al. Xanthogranulomatous pyelonephritis in children: diagnostic and therapeutic aspects. Eur J Pediatr Surg 2002;12:42–8. 10.1055/s-2002-25085 [DOI] [PubMed] [Google Scholar]