

Abstract
Aims
This paper presents updated prevalence estimates of awareness, ever‐use, and current use of nicotine vaping products (NVPs) from 14 International Tobacco Control Policy Evaluation Project (ITC Project) countries that have varying regulations governing NVP sales and marketing.
Design, Setting, Participants and Measurements
A cross‐sectional analysis of adult (≥ 18 years) current smokers and ex‐smokers from 14 countries participating in the ITC Project. Data from the most recent survey questionnaire for each country were included, which spanned the period 2013–17. Countries were categorized into four groups based on regulations governing NVP sales and marketing (allowable or not), and level of enforcement (strict or weak where NVPs are not permitted to be sold): (1) most restrictive policies (MRPs), not legal to be sold or marketed with strict enforcement: Australia, Brazil, Uruguay; (2) restrictive policies (RPs), not approved for sale or marketing with weak enforcement: Canada, Malaysia, Mexico, New Zealand; (3) less restrictive policies (LRPs), legal to be sold and marketed with regulations: England, the Netherlands, Republic of Korea, United States; and (4) no regulatory policies (NRPs), Bangladesh, China, Zambia. Countries were also grouped by World Bank Income Classifications. Country‐specific weighted logistic regression models estimated adjusted NVP prevalence estimates for: awareness, ever/current use, and frequency of use (daily versus non‐daily).
Findings
NVP awareness and use were lowest in NRP countries. Generally, ever‐ and current use of NVPs were lower in MRP countries (ever‐use = 7.1–48.9%; current use = 0.3–3.5%) relative to LRP countries (ever‐use = 38.9–66.6%; current use = 5.5–17.2%) and RP countries (ever‐use = 10.0–62.4%; current use = 1.4–15.5%). NVP use was highest among high‐income countries, followed by upper–middle‐income countries, and then by lower–middle‐income countries.
Conclusions
With a few exceptions, awareness and use of nicotine vaping products varied by the strength of national regulations governing nicotine vaping product sales/marketing, and by country income. In countries with no regulatory policies, use rates were very low, suggesting that there was little availability, marketing and/or interest in nicotine vaping products in these countries where smoking populations are predominantly poorer. The higher awareness and use of nicotine vaping products in high income countries with moderately (e.g. Canada, New Zealand) and less (e.g. England, United States) restrictive policies, is likely due to the greater availability and affordability of nicotine vaping products.
Keywords: E‐cigarettes, global, income classification, nicotine vaping products (NVPs); smoking; international; regulations, policies, survey
Introduction
The world‐wide popularity of nicotine vaping products (NVPs)—otherwise known as electronic cigarettes— has increased dramatically in recent years, with the majority of users being current and former smokers 1, 2, 3, 4. NVPs are widely available in many countries throughout the world in various retail outlets and online. Euromonitor data have shown that the retail sales value of vaping products accounted for 1.5% of the global nicotine market in 2017 5. While cigarettes still accounted for 90% of nicotine market sales in 2017, the growth of the retail sales value of the NVP market during 2017 was estimated to be 50.7%, compared to growth in the cigarette market of 2.8% 5. Moreover, NVPs are now the most popular quit smoking aid in several countries, including the United States, England and Canada, surpassing the use of licensed nicotine replacement therapy (NRT) and prescription‐only medications 2, 6, 7.
Scientists, clinicians, advocates and public health organizations have engaged in extensive debate about a broad range of issues, including the impact of NVPs on the health of users and non‐users, whether they are effective for smoking cessation, whether they might increase smoking among youth, whether they might re‐normalize smoking and, ultimately, whether the net impact on smoking prevalence and population health is positive or negative 8, 9. Two recent comprehensive reviews by the National Academy of Sciences, Engineering and Medicine (NASEM) 10 and Public Health England (PHE) 11 summarized the scientific evidence to date on NVPs, and have stated similar conclusions, that using an NVP is far less risky than smoking combustible cigarettes. However, in reflecting the evidence, both reports also stated that NVPs contain constituents that are not inert and probably carry some health risks. Both NASEM and PHE support the position that NVPs may be helpful to smokers who are trying to stop smoking cigarettes; however, both have also stated that the use of NVPs by non‐smokers should be discouraged. Other organizations, such as the World Health Organization (WHO) 12 and the International Union Against Tuberculosis and Lung Diseases 13, have taken a more precautionary approach towards NVPs, suggesting that given the uncertainty about long‐term health risks and benefits, NVPs should not be promoted for smoking cessation until a clear health advantage can be demonstrated 14. The WHO has urged countries to implement policies that would restrict the sale, promotion and use of electronic cigarettes 15.
The global divide about the uncertainty of the possible risks and benefits of NVPs has led governments to adopt diverse approaches towards regulating the sale, marketing and use of NVPs in public places 16. As of 2018, the sale of vaping products (with or without nicotine) has been banned in 27 countries, nine countries have banned the sale of NVPs, and 36 countries permit the sale of NVPs with diverse regulations (e.g. minimum age of purchase, advertising and promotion, packaging, product regulation, taxes, etc.) 17. For example, in May 2016, the European Union (EU) implemented regulatory policies governing the sale and marketing of consumer NVPs (e.g. not medicinal NVPs) under the EU Tobacco Products Directive (EU TPD) 18, 19, which was transposed into United Kingdom (UK) law through the UK Tobacco and Related Products Regulations 2016 (UK regulations implementing the EU TPD) 20, and into the Dutch Tobacco and Smoking Products Law 21. The EU TPD rules prohibit marketing elements on NVP packaging, specify a minimum age for purchase (18+ years), prohibit cross‐border advertising and promotion of NVPs, and include a number of requirements to guarantee product safety, such as maximum nicotine content. In addition, the UK has an advertising code of practice 22, 23 which restricts marketing content, such that NVP marketing must be socially responsible, and not appeal to youth. In the United States, NVP regulations were introduced in August 2016 under the Food and Drug Administration (FDA) Deeming Rule 24. Some new requirements and restrictions were applied to NVPs at that time (e.g. age requirements for purchase); however, there were no changes to pre‐existing NVP marketing (advertising is still permitted in all channels).
Evidence concerning the patterns of NVP use indicates that the uptake and continued use is likely to be influenced by the NVP regulatory policy environment 25, 26. Previous research showed some evidence (with a few exceptions) of lower awareness and use of NVPs in countries that had banned them compared to countries that had fewer sales and marketing restrictions 26. Since these findings, NVP use has increased dramatically in many countries, especially where laws have not restricted the sale and marketing of vaping products, for example in the United States 27, 28, 29. In England, where the sale of NVPs is legal and the concept of harm reduction has largely been embraced by public health organizations 11, 30, 31, it has been shown that the use of NVPs by current smokers and recent ex‐smokers is higher than most other countries world‐wide, particularly in countries that have more restrictive NVP regulations 4, 32, 33, 34, 35, 36, and also compared to other EU countries with similar NVP regulations under the EU TPD 2, 3, 37.
However, although there is information about NVP use patterns across a range of countries or regions (mainly from high‐income nations), there are significant limitations in the comparability of findings from studies in different countries due to differing methodologies (e.g. sampling, definitions of NVP use and measurement methods), thus making valid cross‐country comparisons difficult.
This study includes a broad and comprehensive evaluation of NVP use, as it incorporates comparable data from a wide range of countries from the ITC Project, which largely share common methodologies (particularly the same measurements of the NVP outcomes). Furthermore, this study is an extension of the previously published paper that examined NVP (e‐cigarette) awareness and use among 10 ITC countries 26. However, these data are now outdated, as the findings suggested that both the regulatory environment and survey timing were probably associated with considerable variability in NVP use estimates. Also, given the rapid growth of the NVP market, the increase in number of products available, major public health endorsements of NVPs, changing public perceptions about NVPs 38, 39, 40, and/or the implementation of (stricter) regulations in various countries, estimates of NVP use have been shown to be variable over time 41. Therefore, these data from 14 ITC countries, with differing levels of economic development and tremendous variability in regulations governing NVP sales and marketing, provide a fertile landscape for exploring the possible impact of regulatory policies on NVP use. The aims of this paper are to provide: (1) prevalence estimates of NVP awareness, ever‐use, current use, and daily use among smokers and recent ex‐smokers; and (2) qualitative observations of plausible patterns for differing (or similar) estimates between countries.
Methods
Design, setting and participants
This study is a cross‐sectional analysis of adult (≥ 18 years) current smokers (daily or non‐daily) and recent ex‐smokers (quit smoking ≤ last 2 years) from 14 countries participating in the ITC Project: Australia, Bangladesh, Brazil, Canada, China, England, Malaysia, Mexico, the Netherlands, New Zealand, Republic of Korea, the United States, Uruguay and Zambia. According to World Bank criteria, eight of the countries are high‐income countries (HICs: Australia, Canada, England, New Zealand, Republic of Korea, Uruguay, the Netherlands and the United States); four are upper–middle‐income countries (UMICs: Brazil, China, Malaysia and Mexico), and two are lower–middle‐income countries (LMICs: Bangladesh and Zambia). Data from the most recent survey year for each country were included, which spanned the period from 2013 to 2017 (see Table 1).
Table 1.
Sample characteristics and survey details (unweighted).
| Country | N | Year(s) of survey data collection | Survey mode | Male n (%) | Mean age | Daily smoker n (%) |
|---|---|---|---|---|---|---|
| Australiaa | 1490 | Wave 1 July 2016–November 2016 | Web | 762 (51.1) | 49.7 | 1215 (81.5) |
| Smokers | 1339 | |||||
| Recent ex‐smokers | 151 | |||||
| Bangladesh | 2033 | Wave 4 October 2014–April 2015 | Face‐to‐face | 1977 (97.2) | 39.2 | 1841 (90.6) |
| Smokers | 1878 | |||||
| Recent ex‐smokers | 155 | |||||
| Brazil | 1340 | Wave 3 September 2016–November 2016 | Phone | 648 (48.4) | 51.6 | 1135 (84.7) |
| Smokers | 1216 | |||||
| Recent ex‐smokers | 124 | |||||
| Canadaa | 3576 | Wave 1 July 2016–November 2016 | Web | 1671 (46.7) | 41.2 | 2220 (62.1) |
| Smokers | 3215 | |||||
| Recent ex‐smokers | 361 | |||||
| China | 3604 | Wave 5 November 2013–July 2015 | Face‐to‐face | 3394 (94.2) | 51.2 | 3239 (89.9) |
| Smokers | 3432 | |||||
| Recent ex‐smokers | 172 | |||||
| Englanda | 4220 | Wave 1 July 2016–November 2016 | Web | 2281 (54.1) | 41.5 | 2880 (68.3) |
| Smokers | 3886 | |||||
| Recent ex‐smokers | 334 | |||||
| Malaysia | 1824 | Wave 6 February 2013–January 2014 | Phone | 1806 (99.0) | 30.5 | 1608 (88.2) |
| Smokers | 1703 | |||||
| Recent ex‐smokers | 121 | |||||
| Mexico | 839 | Wave 7 November 2014–March 2015 | Face‐to‐face | 466 (55.5) | 42.3 | 541 (64.5) |
| Smokers | 776 | |||||
| Recent ex‐smokers | 63 | |||||
| Netherlands | 1645 | Wave 10 November 2016–December 2016 | Web | 791 (48.1) | 38.8 | 1109 (67.4) |
| Smokers | 1213 | |||||
| Recent ex‐smokers | 432 | |||||
| New Zealanda | 1068 | Wave 1 October 2016–Aprrl 2017 | Phone | 446 (41.8) | 44.7 | 722 (67.6) |
| Smokers | 853 | |||||
| Recent ex‐smokers | 215 | |||||
| Republic of Koreaa | 2000 | Wave 1 June 2016–July 2016 | Phone | 1800 (90.0) | 43.5 | 1896 (94.8) |
| Smokers | 2000 | |||||
| Recent ex‐smokers | 0 | |||||
| United Statesa | 2552 | Wave 1 July 2016–November 2016 | Web | 1323 (51.8) | 44.0 | 1850 (72.5) |
| Smokers | 2327 | |||||
| Recent ex‐smokers | 225 | |||||
| Uruguay | 1310 | Wave 5 July 2014–November 2014 | Face‐to‐face | 600 (45.8) | 40.9 | 1070 (81.7) |
| Smokers | 1181 | |||||
| Recent ex‐smokers | 129 | |||||
| Zambia | 1145 | Wave 2 August 2014–October 2014 | Face‐to‐face | 1095 (95.6) | 40.1 | 914 (79.8) |
| Smokers | 1045 | |||||
| Recent ex‐smokers | 106 |
Between‐country comparisons cannot be made due to differences in survey timing and sequence of the questions in the survey.
New country cohort sample (wave 1). Note, for the ITC 4CV1 Project (Australia, Canada, England and the United States), the new cohort sampling web panel frame also included 2501 re‐contact participants from the previous 4C waves 1–9 cohort.
Smokers are classified as daily or non‐daily users of cigarettes; recent ex‐smokers quit smoking cigarettes ≤ 2 years ago.
Methodological details on data collection for each country are available via the ITC Project website. In brief, the sample in each country was designed to be representative of smokers, and used either probability‐based sampling frames or non‐probability samples (or a combination of those) for initial recruitment. Respondents were recruited via address‐based sampling frames, random‐digit‐dialling (RDD) sampling frames, web‐based or address‐based panels, or a combination of these frames. Weights were constructed for each country (to adjust for the sampling design) and were calibrated using data from national health surveys or household enumeration data for countries with face‐to‐face surveys.
Respondents at the survey wave analysed in this study were re‐contact/cohort respondents (recruited in previous survey waves) and/or new (replenishment) respondents to compensate for attrition from the last cohort survey, or if it was the initial survey (wave 1) of a new cohort. Supporting information, Table S1 shows the percentages of the country samples that were derived from re‐contact (cohort) versus replenishment respondents.
The newly recruited replenishment participants for each country were selected using the same sampling design as the previous survey wave, with some exceptions. For Australia, Canada, England and the United States, the latest wave of data came from wave 1 of the ITC Four Country Smoking and Vaping Survey (ITC 4CV1) 42, which is an is an expansion of the 2002–15 ITC Four Country (ITC 4C) Survey 43. Four parallel surveys conducted in Canada, United States, England and Australia included adults (aged 18+) who reported to be currently smoking cigarettes and/or using an NVP, or a former smoker. The sample in each country was designed to be as representative as possible of cigarette smokers and NVP users (e.g. by age and sex), and consisted of re‐contacted respondents from the ITC 4C cohort and new respondents from online panels (using either probability‐based sampling frames or non‐probability opt‐in panels, or a combination of these). Detailed descriptions of the methods used in each country are presented in the ITC 4C and 4CV1 technical reports 42, 43 and in the Thompson et al. 4CV1 methods paper 44. New Zealand respondents (wave 1) were drawn from the New Zealand Health Survey 45, and respondents from the Republic of Korea (wave 1) were recruited using a dual telephone RDD sampling frame (fixed‐line/landline or mobile phone) 46.
All surveys were in the country's native language(s) and were administered either via phone, face‐to‐face interviews or online (Table 1). Research ethics approval for all surveys was obtained from the University of Waterloo (Canada), and for each individual country from the country‐specific institution. All participants provided consent prior to survey completion.
Measures
All country‐specific surveys can be found at the ITC Project website. The variables included in this study are briefly described herein.
Demographics
Demographic characteristics were assessed with standard questions on sex, age, highest educational attainment (categorized into low, moderate, and high to broadly equate them for comparison across countries), and monthly household income (categorized into low, moderate and high). Each country's technical report provides details on education and income categorization 47.
Tobacco‐related data
Frequency of smoking: daily smoker versus non‐daily smoker (≤ weekly) versus not at all (quit smoking ≤ 2 years ago).
NVP (e‐cigarette) outcome variables
Respondents from all countries were asked: ‘Have you ever heard of electronic cigarettes or e‐cigarettes?’ (response options: yes, no, don't know or refused). If the respondent answered ‘no/don't know’, then they did not receive the subsequent NVP questions and were coded as ‘no’ for the other NVP outcome variables.
The subsequent NVP questions were: (1) ‘Have you ever tried an e‐cigarette?’ (yes versus no); and if ‘yes’, (2) ‘Do you currently use an electronic cigarette?’ (yes versus no); and if ‘yes’, (3) ‘How often do you use an e‐cigarette?’. Supporting information, Table S2 describes the exact questions for each outcome variable by country.
Respondents who had missing data (e.g. refused to answer a question about NVPs) were excluded from the analyses. Only respondents who selected ‘yes’ or ‘no’/‘I don't know’ (coded as ‘no’) were considered valid responses. Across the 14 countries, 15 respondents were excluded because they had missing data for at least one of the outcome measures (four in Bangladesh, one in Brazil, three in China, five in Mexico and two in Zambia).
Use of a vaping product that contained nicotine versus no nicotine was reported among current daily and weekly vapers from eight countries where the survey question was available (Australia, Canada, China, England, the Netherlands, New Zealand, Republic of Korea and the United States). Vapers were asked: ‘What is the strength of the e‐liquid you currently use most?’. This was coded into ‘no nicotine’ (0 mg) versus ‘yes, nicotine’ (≥ 1 mg).
Country NVP regulatory policies
Countries were categorized into four groups based on regulations governing NVP sales and marketing (prohibited versus not prohibited) and the strength of enforcement (strict or weak where NVPs were not permitted to be sold) at the time of the country's survey (see Fig. 1).
Most restrictive policies (MRPs): NVPs are not legal to be sold with strict enforcement of NVP regulations: the sale, advertising, promotion and sponsorship of NVPs is prohibited in Australia (non‐nicotine vaping products are classified as legal consumer products). Nicotine and non‐nicotine vaping product sale, importation and promotion is explicitly banned by an amendment/decree in Uruguay. A resolution prohibits the sale, advertisement, distribution and importation of vaping products, and as tobacco products, their use in public places and public transportation is prohibited by a decree in Brazil.
Restrictive policies (RPs): NVPs are not approved to be sold with weak enforcement of NVP regulations: in Canada and New Zealand, NVPs were not approved for sale, and marketing of NVPs was prohibited; however, due to weak enforcement of the regulations, NVPs were widely available for purchase in speciality shops or online; vaping products without nicotine were widely available in many retails locations (including pharmacies, grocery stores, etc.). In Malaysia, nicotine was classified as a class C poison under the Poisons Act and Control of Drugs and Cosmetics Regulations, and therefore NVPs were prohibited from sale. At the time of the survey this law was not strongly enforced, and generally NVPs were still widely available on the market. Finally, in Mexico, a national tobacco control law prohibited the sale, distribution, exhibition and promotion of NVPs; however, enforcement was generally weak and NVPs were widely available for purchase.
Less restrictive policies (LRPs): NVPs are legal for sale, and (some) marketing is allowable: These LRP countries (England, the United States, Republic of Korea and the Netherlands) allow NVPs to be sold and marketed through various channels (but only at point of sale in the Netherlands). In the EU, the EU TPD prohibits any cross‐border marketing and restrictions apply, such as age limit for purchasing NVPs and safety and packaging requirements. Additional restrictions may apply based on country‐specific codes (e.g. in the United Kingdom, as described above) 22, 23.
No regulatory policies (NRPs): there were no NVP regulatory policies in Bangladesh, China or Zambia. However, NVPs were not generally available for sale.
Figure 1.

Country classification based on the strength of regulatory policies for the sale and marketing of nicotine vaping products (NVPs) during country survey data collection. 1Uruguay and Brazil also prohibit the sale and marketing of non‐nicotine vaping products. 2Malaysia: There is no existing law related directly to the legality of NVP products (the government applied an existing law to the sale of e‐liquids particularly those with nicotine). Nicotine is classified as a class C poison under the Poisons Act 1952 and Control of Drugs and Cosmetics Regulations 1984. Therefore, the sale, distribution or importation of unlicensed nicotine‐containing e‐cigarettes is prohibited
Analyses
Descriptive statistics were used on unweighted data to describe the characteristics of the study respondents. For all subsequent analyses, data were weighted in order to obtain a population estimate of the four NVP outcomes.
Each of the country samples (once weighted) were designed to be representative of cigarette smokers. However, this was not the case for ex‐smokers for the majority of the countries. In nine of the ITC countries, ex‐smokers were initially recruited as smokers, then quit smoking, and were subsequently retained at follow‐up waves. Consequently, conclusions about ex‐smokers should be interpreted more carefully. In contrast, the new ITC 4CV1 samples in Canada, Australia, United States and England, and New Zealand included the recruitment of ex‐smokers who had quit smoking at the time of the ITC survey. The ITC 4CV1 study was not specifically designed to measure NVP prevalence (mainly owing to the oversampling of NVP users to reach target sample sizes); consequently, the prevalence estimates reported in the current paper were obtained from national benchmark surveys (as opposed to the ITC 4CV1 data itself) in Canada (2015), the United States (2016), England (2016) and Australia (2016). This is particularly true for Australia, where NVP users in the (unweighted) ITC 4CV1 Australia sample were greatly over‐represented.
In each country, an adjusted logistic regression model estimating predicted probabilities using marginal standardization 48 was conducted for each of the four outcomes: (i) awareness (ever heard of) NVPs, (ii) ever‐tried/used NVPs, (iii) current NVP use (daily/weekly/monthly) and (iv) daily NVP use. Each model adjusted for smoking status (daily smoker versus non‐daily smoker versus ex‐smoker), sex and age. This was performed first for the overall sample, and then separately by smoking status.
Statistical comparisons between countries were not carried out due to the nature of the data, mainly owing to differences in survey timing, sampling designs and/or how the sampling weights were calculated. In other words, because of those differences, it would be difficult to tell if statistically significant differences between countries are the result of differences in attitudes to smoking and use of NVPs, or from differing methodologies. Therefore, differences between countries are discussed qualitatively. All analyses were conducted with SUDAAN version 11.0.1.
Results
Figures 2, 3, 4, 5, 6, 7 present the prevalence of self‐reported NVP awareness, ever‐use, current use and daily use, as well as current use by smoking status (smokers versus ex‐smokers), and the percentage of daily and weekly vapers who self‐reported the use of nicotine in their vaping product. The graphs also depict the type of regulatory environment (NRP, LRP, RP and MRP countries), country income classification (HIC, UMIC or LMIC) and survey date. Supporting information, Table S3 presents the prevalence estimates with 95% confidence intervals for the four outcomes by country and smoking status.
Figure 2.

Awareness (ever heard) of nicotine vaping products (NVPs) among smokers and recent ex‐smokers (weighted %)
Figure 3.

Ever‐used nicotine vaping products (NVPs) among smokers and recent ex‐smokers (weighted %)
Figure 4.

Current use (daily, weekly or monthly) of nicotine vaping products (NVPs) among smokers and recent ex‐smokers (weighted %)
Figure 5.

Daily use of nicotine vaping products (NVPs) among smokers and recent ex‐smokers (weighted %)
Figure 6.
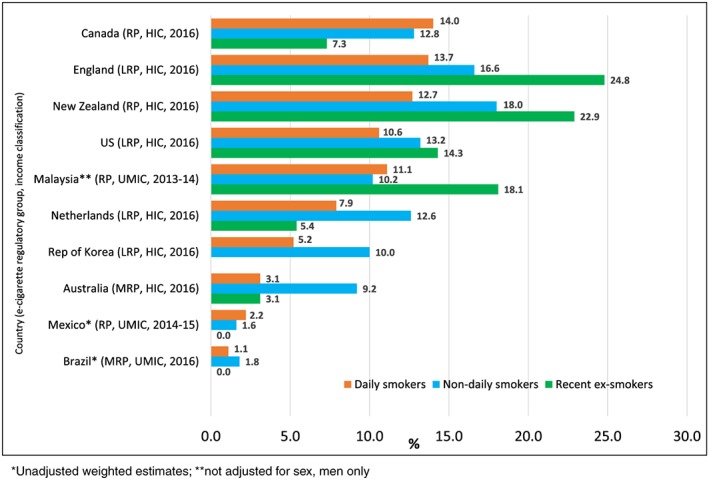
Prevalence of current nicotine vaping products (NVPs) use by smoking status (weighted %). [Colour figure can be viewed at wileyonlinelibrary.com]
Figure 7.

Daily and weekly users using vaping products with nicotine (% yes, weighted). [Colour figure can be viewed at wileyonlinelibrary.com]
Prevalence of awareness of NVPs among the overall sample (smokers and ex‐smokers) ranged from 3.1% in Zambia to 99.4% in England (Fig. 2 ); ever‐use ranged from 0.4% in Zambia to 66.6% in England (Fig. 3); current use ranged from 0% in Zambia to 17.2% in England (Fig. 4); and daily use ranged from 0% in Zambia and Bangladesh to 9.4% in England (Fig. 5).
The outcomes patterns varied by both regulatory policy group and country income. First, awareness and use were lowest in NRP countries (range: awareness = 3.1–59.3%; ever‐use = 0.4–10.4%; current use = 0–0.6%). Ever‐use and current use of NVPs were lower in MRP countries (ever‐use: 7.1–48.9%; current use = 0.3–3.5%), relative to LRP (ever‐use = 38.9–66.6%; current use = 5.5–17.2%) and RP (ever‐use = 10.0–62.4%; current use = 1.4–15.5%) countries.
Daily use was highest for two LRP countries: England (9.4%) and the United States (6.6%) and two RP countries: New Zealand (7.8%) and Canada (4.4%). All other countries had daily use rates < 4%. With the exception of Mexico (0.5%), relative to LRP and RP countries, daily use was lower in all MRP countries: Uruguay (0.1%), Brazil (0.4%) and Australia (1.7%), and NRP countries: China (0.2%), Bangladesh (0.0%) and Zambia (0.0%) (Fig. 5).
Secondly, regardless of regulatory policies, and with the exception of Uruguay, NVP awareness, ever‐use, current use, and daily use were highest among HICs (awareness = 51.8–99.4%; ever‐use = 7.1–66.6%; current use = 0.1–17.2%; and daily use = 0.1–9.4%), followed by UMICs (awareness = 61.0–86.9%; ever‐use = 10.0–39.0%; current use = 1.0–11.5%; and daily use = 0.4–3.7%), and then LMICs (awareness = 23.1–59.3%; ever‐use = 0.4–10.4%; current use = 0.0–0.6%; and daily use = 0.0–0.2%).
The prevalence of current NVP use by smoking frequency varied by country, with higher rates of non‐daily smokers currently using NVPs than daily smokers in seven countries (England, New Zealand, United States, the Netherlands, RP, Brazil and Australia). A greater percentage of recent ex‐smokers reported using NVPs than current smokers (daily or non‐daily) in three of the countries (England, New Zealand and Malaysia; see Fig. 6). The majority of daily and weekly vapers reported that their vaping device had nicotine (> 50% in seven of the eight countries where data were available), with the exception of China. Daily vapers had higher rates of using vaping devices with nicotine than non‐daily users in all eight countries (see Fig. 7).
Discussion
These findings update those of a previous study of 10 ITC countries 26, providing the largest multi‐country investigation of NVP awareness and use among smokers and ex‐smokers in countries with differing NVP sale and marketing regulations and economic levels. Similar to the previous study by Gravely et al. 26, the present findings show that, with a few exceptions, there were considerable differences between countries in awareness, ever‐use and current/daily use of NVPs; therefore, these findings continue to suggest that awareness and use patterns vary according to the level and strength of the regulatory environment. Rates of use were much higher in LRP and RP countries, particularly in England, United States, Canada and New Zealand, where NVPs are widely available for sale in retail and/or speciality shops, and where smokers have commonly reported using them for smoking cessation 2, 4, 6, 7.
In contrast to many of the LRP and RP countries, rates of use were quite low in the MRP countries (Australia, Uruguay and Brazil), indicating that strict regulation and enforcement of NVP laws in these countries may have limited smokers’ access to these products and/or discouraged smokers from using them. In the three countries with no regulations governing NVP sales, awareness and use rates were very low, which suggests that there was little marketing and/or interest in NVPs in these countries. In Bangladesh and Zambia, other tobacco alternatives are prevalent due to low cost and/or socio‐cultural reasons (for example, bidis 49 and smokeless tobacco in Bangladesh 50, and roll‐your‐own/loose‐leaf tobacco in Zambia 51). In these nations, where the highest prevalence of tobacco use is among those in the poorer low‐ and middle‐income segments, NVPs would probably not do well on the market due to smoker's preferences for cheap and other widely available forms of tobacco. Therefore, it is not surprising that these governments have not been politically or economically motivated to address NVP policies. Notably, in China half the respondents were aware of NVPs, but there was a low rate of current (10%) and daily use (0.6%). This low prevalence of NVP use probably reflects the fact that the China National Tobacco Company, a state‐owned enterprise, has a monopoly of the cigarette market (accounting for 98% of domestic sales) 52, and has largely prevented NVPs from entering the domestic market‐place.
NVP prevalence estimates varied by country income. NVP awareness and use were greatest in HICs and lowest in LMICs. Two HICs were exceptions to this pattern: Uruguay (low awareness and use) and Australia (low use). Similarly, a study by Palipudi et al. found the same income gradient pattern, where awareness of NVPs was lower in LMICs and higher in HICs 34. The pattern was not the same for NVP use however, as there were little differences between estimates based on country income. This may reflect the strict NVP regulatory policies in both of the HICs (Qatar and Greece ), which was also found in this study (e.g. Uruguay and Australia). It should be noted, however, that research on NVP use has primarily been conducted in HICs, whereas data from LMICs are limited. Given this gap in the literature, the positive relationship between NVP use and country income gradient, moderated by regulatory environment (e.g. MRP HIC countries had much lower rates of EC use than the other HIC countries), more research using longitudinal cohort data are needed to further examine the impact of strict regulation on both NVP use and smoking rates.
The findings suggest that there may be other plausible explanations for the level of NVP awareness and use, particularly the harm reduction environment (e.g. government acceptability and support for using NVPs as a quit‐smoking aid, particularly for smokers who are struggling to quit smoking, or who do not plan to quit smoking) and regionalization. The concept of using NVPs to replace cigarette smoking as a harm reduction strategy has been a hotly debated topic. Less than a decade ago, many countries implemented policies to restrict access to vaping products. However, this was not the case for England, a country where NVPs have been embraced by PHE and the Royal College of Physicians as a harm reduction strategy 11, 30, whereas most public health agencies in the other countries have not followed similarly, including the Netherlands, which has similar NVP regulations. This may explain why all prevalence estimates were highest in England. In contrast, governments in Australia, Brazil and Uruguay have taken the opposite position. These countries have banned the sale of nicotine NVPs (including non‐nicotine NVPs in Brazil and Uruguay, and in some states in Australia) 17, 53 on the grounds that NVPs should be subject to evidentiary review and should be restricted or banned until more evidence about their safety and efficacy are available.
With regard to regionalization, countries with similar characteristics and geography (e.g. regional location) seemed to have similar NVP prevalence estimates. For example, prevalence of ever‐use and current use in Mexico were similar to the other MRP Latin American countries (Uruguay and Brazil), and although there is a law banning the sale of nicotine NVPs in Mexico, it was categorized as an RP country because of weak enforcement, resulting in high accessibility 35 and high prevalence among Mexican adolescents 54, 55. The Netherlands was more closely aligned to other European countries as opposed to the other LRP and HIC countries in this study, including England. For example, daily use of NVPs in the Netherlands was 1.8% for smokers (data not shown), comparable to other ITC EU countries—2% in Greece, 1% in Germany, Romania, Hungary, Spain and Poland (2016 ITC data) 56 and 2.3% for the EU 57. This EU regionalization effect may be partly because these countries are all regulated under the EU TPD. In contrast, Canada and the United States differed in the legality of the sale and marketing of NVPs, but estimates for all outcomes were very similar, therefore suggesting that countries that are close in proximity share similar use patterns.
Interestingly, previous Eurobarometer data (2014) have also shown this ‘regionalization pattern’ 32, where overall population prevalence of NVP use was generally similar among many of the countries, ranging from 0 to 2% in the majority of EU countries to 4% in France and the United Kingdom. However, the prevalence of NVP use among smokers and ex‐smokers was highest in the United Kingdom (11 and 8%, respectively) compared to all the other EU countries, therefore indicating that when governments and large public health organizations support using e‐cigarettes for smoking cessation, there is an additive effect on usage rates.
Another pattern among the majority of countries in this study, regardless of the NVP regulatory environment and country income, was the much higher rate of having ‘ever‐tried’ an NVP relative to those who continued to use an NVP on a more regular basis. This has been consistently shown in other studies, indicating that there is high curiosity to try NVPs in many countries, but a low percentage who continue to regular use 11, 29, 58. Some of the reasons reported in the literature for discontinued use have included: trying them only out of curiosity, beliefs that they are harmful, and reporting that they are not as satisfying as regular cigarettes 11.
Although this study has provided national estimates of NVP awareness and use among current smokers and ex‐smokers from multiple countries, there are some limitations to consider. First, between‐country differences in prevalence estimates were not compared statistically. Although statistical comparisons are feasible, these would be inappropriate because of differences in survey timing and sampling designs between countries. Furthermore, qualitative comparisons made herein should be interpreted cautiously due to differences between countries in sampling design coverage, recruitment methods (e.g. online panels, RDD or household enumeration), interviewing methods and linguistic differences. Secondly, this study did not compare within‐country trends in NVP awareness and use over time, because two countries were new cohorts (New Zealand, Republic of Korea), four countries differed in survey modes and sampling techniques used at previous survey waves (Canada, United States, England, Australia) and two countries did not have a question about NVP use in the previous survey (Brazil, Mexico). Thirdly, results for the ex‐smoker samples should be interpreted with caution, because most of the country samples were not designed to be representative of the entire population of ex‐smokers (i.e. most ex‐smokers were recruited as smokers and retained in the longitudinal cohort). Fourthly, current and daily NVP estimates should be interpreted cautiously, as sample sizes were small in some countries resulting in wide variability in those estimates (e.g. as seen in Figs 4 and 5). Finally, this study is cross‐sectional in nature (and therefore cannot determine the direction of the relationship between NVP policies and use). This study does, however, offer important observations, especially with regard to how the strength and implementation of regulatory policies may shape behaviour of NVP use by current and former smokers. As many governments around the world have implemented a broad range of regulatory policies on the sale and marketing of NVPs, and in other domains that would affect NVP use (e.g. taxation and vape‐free laws), further international studies with longitudinal data—that can both inform governments about policy approaches and/or policy changes— are urgently needed.
Declaration of interests
K.M.C. has received payment as a consultant to Pfizer, Inc., for service on an external advisory panel to assess ways to improve smoking cessation delivery in health care settings. K.M.C. has also served as paid expert witness in litigation filed against the tobacco industry. D.H., J.F.T. and G.T.F. have served as expert witnesses on behalf of governments in litigation involving the cigarette industry. All other authors have no conflicts of interest to declare.
Supporting information
Table S1 Proportion of Country Sample that is Re‐contact (Cohort) or Newly Recruited Respondents.
Table S2 Survey Questions: Ever‐tried and Current Use/Frequency of E‐cigarettes.
Table S3 Adjusted* Prevalence Estimates With 95% Confidence Intervals for Vaping Product (E‐cigarette) Awareness, Ever‐use, Current Use and Daily Use By Country and Smoking Status.
Acknowledgements
The ITC country data in this paper were supported by grants from the US National Cancer Institute (P01CA138389, P01CA200512, R01 TW010652), the Canadian Institutes of Health Research (MOP 115016, FDN 148477), the National Health and Medical Research Council of Australia (APP1106451), the Korean Ministry of Health and Welfare, the Dutch Cancer Foundation (KWF) (UM 2014‐7210), the National Cancer Institute of Brazil (INCA), Pan‐American Health Organization (PAHO), Brazil Fundação do Câncer (BR/LOA/1500048.001), the Chinese Centre for Disease Control and Prevention, the Health Research Council of New Zealand (GA215F 15/072), the New Zealand Ministry of Health and the Mexican Consejo Nacional de Ciencia y Tecnología (Salud‐2007‐C01‐70032 and Salud‐2013‐01‐202671). S.G. was supported by a Canadian Cancer Society (CCS) Career Development Award in Cancer Prevention (no. 703858). G.T.F. was supported by a Senior Investigator Award from the Ontario Institute for Cancer Research and a Prevention Scientist Award from the Canadian Cancer Society Research Institute. The authors would also like to gratefully acknowledge the reviewers for their insightful comments and suggestions which served to strengthen this paper.
Gravely, S. , Driezen, P. , Ouimet, J. , Quah, A. C. K. , Cummings, K. M. , Thompson, M. E. , Boudreau, C. , Hammond, D. , McNeill, A. , Borland, R. , Thrasher, J. F. , Edwards, R. , Omar, M. , Hitchman, S. C. , Yong, H.‐H. , Barrientos‐Gutierrez, T. , Willemsen, M. C. , Bianco, E. , Boado, M. , Goma, F. M. , Seo, H. G. , Nargis, N. , Jiang, Y. , Perez, C. D. A. , and Fong, G. T. (2019) Prevalence of awareness, ever‐use and current use of nicotine vaping products (NVPs) among adult current smokers and ex‐smokers in 14 countries with differing regulations on sales and marketing of NVPs: cross‐sectional findings from the ITC Project. Addiction, 114: 1060–1073. 10.1111/add.14558.
Footnotes
World Bank Countries and Economies: https://data.worldbank.org/country
ITC Project: http://www.itcproject.org/methods
The categorization of ‘like‐countries’ into four NVP regulatory policy groups was based on communication with in‐country experts (including the ITC Country Principal Investigators) and/or Ministry of Health representatives. Information from the Institute for Global Tobacco Control ‘Country Laws Regulating E‐cigarettes’ was also used to verify laws: https://globaltobaccocontrol.org/e‐cigarette_policyscan
References
- 1. Glasser A. M., Collins L., Pearson J. L., Abudayyeh H., Niaura R. S., Abrams D. B. et al Overview of electronic nicotine delivery systems: a systematic review. Am J Prev Med 2017; 52: e33–e66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. West R., Beard E., Brown, J . Trends in electronic cigarette use in England: the smoking toolkit study. 2017. Available at: http://www.smokinginengland.info/latest‐statistics/ (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qJ9hzgb on 31 January 2019).
- 3. Farsalinos K. E., Poulas K., Voudris V., Le Houezec J. Electronic cigarette use in the European Union: analysis of a representative sample of 27 460 Europeans from 28 countries. Addiction 2016; 111: 2032–2040. [DOI] [PubMed] [Google Scholar]
- 4. Li J., Newcombe R., Walton D. The prevalence, correlates and reasons for using electronic cigarettes among New Zealand adults. Addict Behav 2015; 45: 245–251. [DOI] [PubMed] [Google Scholar]
- 5. Foundation for a Smoke‐Free World . Global trends in nicotine. 2018. Available at: https://www.smokefreeworld.org/sites/default/files/fsfw‐report‐trends‐in‐nicotine‐1005201811.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qJLe7rQ on 31 January 2019).
- 6. Caraballo R. S., Shafer P. R., Patel D., Davis K. C., McAfee T. A. Quit methods used by US adult cigarette smokers, 2014–2016. Prev Chronic Dis 2017; 14: 160600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Reid J. L., Hammond D., Rynard V. L., Madfhill C. L., Burkhalter R. Tobacco Use in Canada: Patterns and Trends, 2017th edn. Waterloo, ON: Propel Centre for Population Health Impact, University of Waterloo; Available at: https://uwaterloo.ca/propel/tobacco‐use‐canada‐patterns‐and‐trends (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qJbPlZI on 31 January 2019). [Google Scholar]
- 8. Green L. W., Fielding J. E., Brownson R. C. The debate about electronic cigarettes: harm minimization or the precautionary principle. Annu Rev Public Health 2018; 39: 189–191. [DOI] [PubMed] [Google Scholar]
- 9. Editorial (no authors listed) E‐cigarettes—aid to smoking cessation or smokescreen? Lancet 2014; 384: 829. [DOI] [PubMed] [Google Scholar]
- 10. National Academies of Sciences, Engineering, and Medicine . Public Health Consequences of E‐cigarettes. Washington, DC: The National Academies Press; 2018. Available at: https://www.nap.edu/read/24952/chapter/1 (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qK4gQWi on 31 January 2019). [Google Scholar]
- 11. McNeill A., Brose L. S., Calder R., Bauld L., Robson D. Evidence review of ecigarettes and heated tobacco products 2018 A report commissioned by Public Health England. London: Public Health England; 2018. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/684963/Evidence_review_of_e-cigarettes_and_heated_tobacco_products_2018.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qKIVZk4 on 31 January 2019). [Google Scholar]
- 12. World Health Organization (WHO) . Electronic nicotine delivery systems and electronic non‐nicotine delivery systems (ENDS/ENNDS). Report by WHO. Conference of the Parties to the WHO Framework Convention on Tobacco Control. FCTC/COP/7/11. August 2016. Seventh session. Delhi, India, 7–12 November 2016. Available at: http://www.who.int/fctc/cop/cop7/FCTC_COP_7_11_EN.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qKOVBoq on 31 January 2019).
- 13. International Union Against Tuberculosis and Lung Disease . Position statement on electronic cigarettes (ECs) or electronic nicotine delivery systems (ENDS). October 2013. Available at: https://www.theunion.org/what‐we‐do/publications/official/body/E‐cigarette_statement_FULL.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qKe0Bym on 31 January 2019).
- 14. O'Leary R., Borland R., Stockwell T., MacDonald M. Claims in vapour device (e‐cigarette) regulation: a narrative policy framework analysis. Int J Drug Policy 2017; 44: 31–40. [DOI] [PubMed] [Google Scholar]
- 15. Gulland A. WHO urges restrictions on e‐cigarettes. BMJ 2016; 355: i5991. [Google Scholar]
- 16. Kennedy R. D., Awopegba A., De Leon E., Cohen J. E. Global approaches to regulating electronic cigarettes. Tob Control 2017; 26: 440–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Institute for Global Tobacco Control . Johns Hopkins Bloomberg School of Public Health. Country Laws Regulating E‐cigarettes: A Policy Scan. Baltimore, MD: Johns Hopkins Bloomberg School of Public Health; March 2018. Available at: https://www.globaltobaccocontrol.org/e-cigarette_policyscan (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qKl0aoP on 31 January 2019). [Google Scholar]
- 18. European Commission . Revision of the tobacco products directive. 2016; Available at: https://ec.europa.eu/health/tobacco/products/revision_en (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qL4gbPz on 31 January 2019).
- 19. European Parliament and the Council of European Union . Directive 2014/40/EU of the European Parliament and of the council of 3 April 2014 on the approximation of the laws, regulations and administrative provisions of the member states concerning the manufacture, presentation and sale of tobacco and related products and repealing directive 2001/37/EC. Luxembourg: Publications Office of the European Union; 2014. [Google Scholar]
- 20. UK Parliament . The tobacco and related products regulations 2016, no. 507. Consumer Protection. Available at: http://www.legislation.gov.uk/uksi/2016/507/pdfs/uksi_20160507_en.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qLGpJ8m on 31 January 2019).
- 21. Institute for Global Tobacco Control . Country Laws regulating E‐cigarettes. The Netherlands. Available at: https://www.globaltobaccocontrol.org/e‐cigarette/netherlands (accessed 14 February 2019) (Archived at http://www.webcitation.org/76BS054Sj on 14 February 2019).
- 22. The Advertising Standards Authority Ltd (trading as ASA) and The Committee of Advertising Practice Ltd (CAP) . Electronic cigarettes. July 2017; Available at: https://www.asa.org.uk/advice‐online/electronic‐cigarettes.html (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qLOQvA7 on 31 January 2019).
- 23. The Advertising Standards Authority Ltd (trading as ASA) and The Committee of Advertising Practice Ltd (CAP) . 22 electronic cigarettes CAP code. The Tobacco and Related Products Regulations 2016. Available at: https://www.asa.org.uk/type/non_broadcast/code_section/22.html (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qLVygcn on 31 January 2019).
- 24. Food and Drug Administration (FDA) . FDA's deeming regulations for E‐cigarettes, cigars, and all other tobacco products. Available at: https://www.fda.gov/tobaccoproducts/labeling/rulesregulationsguidance/ucm394909.htm (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qLc8nej on 31 January 2019).
- 25. Yong H. H., Hitchman S. C., Cummings K. M., Borland R., Gravely S. M., McNeill A. et al Does the regulatory environment for e‐cigarettes influence the effectiveness of e‐cigarettes for smoking cessation? Longitudinal findings from the ITC four country survey. Nicotine Tob Res 2017; 19: 1268–1276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Gravely S., Fong G. T., Cummings K. M., Yan M., Quah A. C. K., Borland R. et al Awareness, trial, and current use of electronic cigarettes in 10 countries: findings from the ITC project. Int J Environ Res Public Health 2014; 11: 11691–11704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. McMillen R. C., Gottlieb M. A., Shaefer R. M., Winickoff J. P., Klein J. D. Trends in electronic cigarette use among U.S. adults: use is increasing in both smokers and nonsmokers. Nicotine Tob Res 2015; 17: 1195–1202. [DOI] [PubMed] [Google Scholar]
- 28. Choi K., Bestrashniy J., Forster J. Trends in awareness, use of, and beliefs about electronic cigarette and snus among a longitudinal cohort of US Midwest young adults. Nicotine Tob Res 2018; 20: 239–245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Bao W., Xu G., Lu J., Snetselaar L. G., Wallace R. B. Changes in electronic cigarette use among adults in the United States, 2014–2016. JAMA 2018; 319: 2039–2041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Royal College of Physicians (RCP) Nicotine without smoke: tobacco harm reduction. London: RCP; 2016. Available at: https://shop.rcplondon.ac.uk/products/nicotine-without-smoke?variant=17451373061 (accesed 31 January 2019) (Archived at http://www.webcitation.org/75qN3np1h on 31 January 2019). [Google Scholar]
- 31. Public Health England . E‐cigarettes: a developing public health consensus. Joint statement on e‐cigarettes by Public Health England and other UK public health organisations. July 2016; Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/534708/E‐cigarettes_joint_consensus_statement_2016.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qLnMhzF on 31 January 2019).
- 32. Cavalcante T. M., Szklo A. S., Perez C. A., Thrasher J. F., Szklo M., Ouimet J. et al Electronic cigarette awareness, use, and perception of harmfulness in Brazil: findings from a country that has strict regulatory requirements. Cad Saude Publica 2017; 33: e00074416. [DOI] [PubMed] [Google Scholar]
- 33. Tabuchi T., Shinozaki T., Kunugita N., Nakamura M., Tsuji I. The Japan ‘society and new tobacco’ internet survey (JASTIS): a longitudinal internet cohort study of heat‐not‐burn tobacco products, electronic cigarettes and conventional tobacco products in Japan. J Epidemiol 2018; 10.2188/jea.JE20180116 (Epub ahead of print). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Palipudi K. M., Mbulo L., Morton J., Mbulo L., Bunnell R., Blutcher‐Nelson G. et al Awareness and current use of electronic cigarettes in Indonesia, Malaysia, Qatar, and Greece: findings from 2011–2013 global adult tobacco surveys. Nicotine Tob Res 2016; 18: 501–507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Zavala‐Arciniega L., Reynales‐Shigematsu L. M., Lozano P., Rodriguez‐Andrade M. A., Arillo‐Santillan E., Thrasher J. F. Patterns of awareness and use of electronic cigarettes in Mexico, a middle‐income country that bans them: results from a 2016 national survey. Prev Med 2018; 116: 211–218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Australian Institute of Health and Welfare . National Drug Strategy Household Survey [NDSHS] 2016—key findings. Available at: https://www.aihw.gov.au/reports/illicit‐use‐of‐drugs/ndshs‐2016‐key‐findings/contents/tobacco‐smoking (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qLuJqm6 on 31 January 2019).
- 37. Filippidis F. T., Laverty A. A., Gerovasili V., Vardavas C. I. Two‐year trends and predictors of e‐cigarette use in 27 European Union member states. Tob Control 2017; 26: 98–104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. European Commission . Attitudes of Europeans towards tobacco and electronic cigarettes. Special Eurobarometer 429. May 2015. Available at: http://ec.europa.eu/commfrontoffice/publicopinion/archives/ebs/ebs_429_en.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qMASXsO on 31 January 2019).
- 39. Majeed B. A., Weaver S. R., Gregory K. R., Whitney C. F., Slovic P., Pechacek T. F. et al Changing perceptions of harm of E‐cigarettes among U.S. adults, 2012‐2015. Am J Prev Med 2017; 52: 331–338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Brose L. S., Brown J., Hitchman S. C., McNeill A. Perceived relative harm of electronic cigarettes over time and impact on subsequent use. A survey with 1‐year and 2‐year follow‐ups. Drug Alcohol Depend 2015; 157: 106–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Coleman B., Rostron B., Johnson S. E., Persoskie A., Pearson J., Stanton C. et al Transitions in electronic cigarette use among adults in the population assessment of tobacco and health (PATH) study, waves 1 and 2 (2013–2015). Tob Control 2018; 10.1136/tobaccocontrol-2017-054174. (Epub ahead of print). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. ITC Project . ITC Four Country Smoking and Vaping Survey, Wave 1 (4CV1) Technical Report. University of Waterloo, Waterloo, Ontario, Canada; Medical University of South Carolina, Charleston, South Carolina, USA; Cancer Council Victoria, Melbourne, Australia; King's College London, London, UK; 2018. Available at: https://www.itcproject.org/files/4CE1_Technical_Report-28Nov2017.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qMJ0UTW on 31 January 2019)
- 43. International Tobacco Control (ITC) Project . ITC Four Country Waves 2 to 8 (2003–2011)Technical Report. University of Waterloo, Waterloo, Ontario, Canada; Medical University of South Carolina, Charleston, SC, United States; VicHealth Centre for Tobacco Control, Carlton, Australia; Cancer Control Victoria, Melbourne, Australia; King's College London, London, UK; University of Stirling, Stirling, UK; and the Open University, Milton Keynes, UK. 2011. Available at: https://www.itcproject.org/files/4c-w28-tech-report-sept2011.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qMOL26a on 31 January 2019).
- 44. Thompson M. E., Fong G. T., Boudreau C., Driezen P., Li G., Gravely S. et al Methods of the ITC Four Country Smoking and Vaping Survey, wave 1 (2016). Addiction; 2018. 10.1111/add.14528. [Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. International Tobacco Control (ITC) Project . ITC New Zealand wave 1 survey (2016–2017) technical report. University of Waterloo. (December 2017)]. Waterloo, Ontario, Canada and University of Otago, New Zealand. Available at: http://www.itcproject.org/files/ITC_NZL_W1_Tech_Report‐18Dec17‐final.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qMXFSd1 on 31 January 2019).
- 46. International Tobacco Control (ITC) Project . ITC Korea Survey wave 1 (new cohort) technical report. University of Waterloo, Waterloo, Ontario, Canada, and National Cancer Center, Republic of Korea (March 2017). Available at: https://www.itcproject.org/files/KOR1‐TechReport‐Mar23,2017‐Final.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qMf7Hnn on 31 January 2019).
- 47. International Tobacco Control (ITC) Policy Evaluation Project . Technical reports. Available at: https://www.itcproject.org/technical‐report/ (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qMlk1Nq on 31 January 2019).
- 48. Muller C. J., MacLehose R. F. Estimating predicted probabilities from logistic regression: different methods correspond to different target populations. Int J Epidemiol 2014; 43: 962–970. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Roy A. Tobacco consumption and the poor: an ethnographic analysis of hand‐rolled cigarette [bidi] use in Bangladesh. Ethnography 2011; 13: 162–188. [Google Scholar]
- 50. Nargis N., Thompson M. E., Fong G. T., Driezen P., Hussain A. K., Ruthbah U. H. et al Prevalence and patterns of tobacco use in Bangladesh from 2009 to 2012: evidence from international tobacco control [ITC] study. PLOS ONE 2015; 10: e0141135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Kaai S., Goma, F. , Phiri M., Zulu R., Chirwa K., Meng G. et al Prevalence, beliefs, and predictors of roll‐your‐own (RYO) cigarette use among African smokers: findings from the ITC Zambia survey. Presented at SRNT 2018. Baltimore, USA. POS1–50. Available at: https://cdn.ymaws.com/www.srnt.org/resource/resmgr/conferences/2018_Annual_Meeting/65388_SRNT_2018_Abstract_fin.pdf (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qMqrDZe on 31 January 2019).
- 52. Martin ABB. The Chinese government is getting rich selling cigarettes. Available at: https://www.bloomberg.com/tosv2.html?vid=&uuid=a961c9e0-258f-11e9-b5b5-8799b77d77bd&url=L25ld3MvYXJ0aWNsZXMvMjAxNC0xMi0xMi90aGUtY2hpbmVzZS1nb3Zlcm5tZW50LWlzLWdldHRpbmctcmljaC1zZWxsaW5nLWNpZ2FyZXR0ZXM= (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qMx77cB on 31 January 2019).
- 53. Agência Nacional de Vigilância Sanitária . Resolução RDC n° 46, de 28 de agosto de 2009. Proíbe a comercialização, importação e propaganda de quaiquer dispositivo eletrônico para fumar, conhecidos como cigarro eletrônico. Diário Oficial da União 2009.
- 54. Lozano P., Barrientos‐Gutierrez I., Arillo‐Santillan E., Morello P., Mejia R., Sargent J. D. et al A longitudinal study of electronic cigarette use and onset of conventional cigarette smoking and marijuana use among Mexican adolescents. Drug Alcohol Depend 2017; 180: 427–430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Thrasher J. F., Abad‐Vivero E. N., Barrientos‐Gutierrez I., Perez‐Hernandez R., Reynales‐Shigematsu L. M., Mejia R. et al Prevalence and correlates of E‐cigarette perceptions and trial among early adolescents in Mexico. J Adolesc Health 2016; 58: 358–365. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Fong, G.T. , Vardavas, C. , Fernández, E. , Mons, U. , Zatoński, W. , Przewoźniak, K. et al EUREST‐PLUS: ITC 6E wave 1: key findings. In, Fong, G.T., & Vardavas, C. (Chairs), EUREST‐PLUS: monitoring the implementation of the Tobacco Products Directive. Round table symposium presentation. May 2017. Available at: https://eurestplus.eu/news‐and‐events (accessed 31 January 2019) (Archived at http://www.webcitation.org/75qNCBJuu on 31 January 2019).
- 57. Farsalinos K. E., Poulas K., Voudris V., Le Houezec J. Prevalence and correlates of current daily use of electronic cigarettes in the European Union: analysis of the 2014 Eurobarometer survey. Intern Emerg Med 2017; 12: 757–763. [DOI] [PubMed] [Google Scholar]
- 58. Harrell P. T., Simmons V. N., Pineiro B., Correa J. B., Menzie N. S., Meltzer L. R. et al E‐cigarettes and expectancies: why do some users keep smoking? Addiction 2015; 110: 1833–1843. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1 Proportion of Country Sample that is Re‐contact (Cohort) or Newly Recruited Respondents.
Table S2 Survey Questions: Ever‐tried and Current Use/Frequency of E‐cigarettes.
Table S3 Adjusted* Prevalence Estimates With 95% Confidence Intervals for Vaping Product (E‐cigarette) Awareness, Ever‐use, Current Use and Daily Use By Country and Smoking Status.