

To the Editor: A 51-year-old woman presented with a palpable mass in the lower outer region of the left breast. There was no history of skin redness or nipple discharge. Craniocaudal mammography [Figure 1A] showed a circular homogenous mass with well-defined margins and without calcification located in the posterior region of the left breast. Ultrasonography (US) [Figure 1B] of the left breast demonstrated a heterogeneous, hypoechoic lesion with an accompanying peripheral blood flow signal. The resistance index (RI) and elastic score were 0.6 and 4.0, respectively. Magnetic resonance imaging again displayed an approximately 2.6 cm × 2.5 cm mass with characteristic decreased signal intensity on T1-weighted images, and an area of very high-signal intensity was observed in fat-suppressed T2-weighted images in the lower outer region of her left breast [Figure 1C]. Additionally, the lesion presented a high signal on diffusion weighted imaging [Figure 1D], and the apparent diffusion coefficient (ADC) value of this tumor was 0.893 × 10−3 mm2/s. On contrast-enhanced T1-weighted fat-saturated images [Figure 1E], the lesion revealed heterogeneous rim enhancement, and its time-intensity curve showed a plateau pattern.
Figure 1.
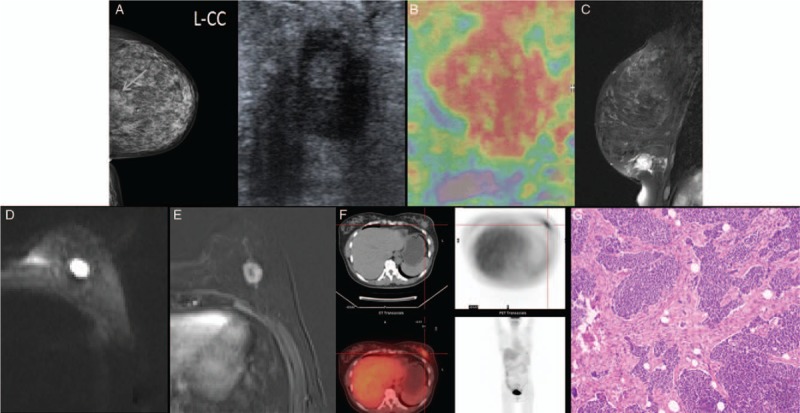
Small-cell carcinoma of the left breast in a 51-year-old woman. (A) Craniocaudal mammography showed a circular homogenous mass with well-defined margins and without calcification located on the posterior region of the left breast. (B) Ultrasonography demonstrated a heterogeneous, hypoechoic lesion in the left breast with a RI and elastic score of 0.6 and 4, respectively. (C) Sagittal fat-suppressed T2-weighted images displayed a mass with a smooth border with an area of very high-signal intensity. (D) Diffusion weighted imaging presented the lesion with a high signal. (E) Axial T1-weighted fat-saturated contrast-enhanced magnetic resonance image of the left breast revealed a heterogeneous rim enhancement mass. (F) Fluorine 18 fluorodeoxyglucose integrated positron emission tomography and computed tomography showed accumulation in the breast lesion and no evidence of extramammary accumulation. (G) Pathology specimen of the mass reveled infiltrating nests of small cells in the fibrotic stroma, which were suggestive of small-cell carcinoma (hematoxylin-eosin staining, original magnification ×200).
The patient underwent US-guided core-needle biopsy of the left breast mass, and pathologic evaluation presented the diagnosis of small-cell carcinoma (SCC). Fluorine 18 fluorodeoxyglucose integrated positron emission tomography and computed tomography (18FDG PET-CT) scan showed accumulation in the left breast with no evidence of extramammary accumulation [Figure 1F]. Combined with the imaging findings on all modalities and the patient's consent, a surgery that included “local expansion of the left breast cancer resection, and left axillary sentinel lymph node biopsy” was performed. Reports of post-operative pathology [Figure 1G] revealed infiltrating nests of small cells in the fibrotic stroma, showing that the tumor is composed of small round cells with hyperchromatic nuclei, a scant cytoplasm, and small sheet necrosis on the edge. Immunohistochemically, evaluations of the estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), and thyroid transcription factor 1 were all negative, whereas the Ki-67 proliferation index was >90%. Furthermore, carcinoma cells were all positive for neuroendocrine differentiation markers, including synaptophysin, chromogranin A, neuron-specific enolase, and CD56. These results indicated the diagnosis of primary SCC of the breast (PSCCB). Subsequent to surgery, the patient was treated with a total of four cycles of post-surgical chemotherapy containing etoposide and cisplatin.
PSCCB is an uncommon type of invasive breast cancer accompanying neuroendocrine features with unknown pathogenesis, but some researchers reported that PSCCB was considered to originate from multipotent stem cells that have developed neuroendocrine features.[1] PSCCB accounts for <1% of primary breast cancers[1,2] and has a mean age of onset of 53 years (range, 28–81) in the population of patients with breast cancer. Clinical manifestations of PSCCB are untypical, and patients often present to a doctor with a palpable breast mass discovered after an accidental physical examination.[2]
There are few reports concerning its imaging features. On the basis of previous studies and the present case report, PSCCB is composed of SCC and carcinoma in situ (DCIS) components pathologically, we assume that the imaging features of PSCCB may be different owing to the difference in the ratio of the pathologic components of PSCCB. When DCIS is larger and SCC is fewer in proportion components of PSCCB, the imaging findings were analogous to that of DCIS.[3] When SCC accounts for the majority and DCIS is less, the tumor shows a high degree of malignancy and rapid growth, which often leads to the formation or necrosis of central “scar-like fibers.” Therefore, the multimodality imaging depicted the breast lesion as a mass with a clear margins, a high intra-tumoral signal intensity on T2-weighted images, low ADC value, heterogeneous rim enhancement, and plateau or wash-out pattern,[4] these imaging findings were analogous to that of the triple negative breast cancer (TNBC). In our case, the multimodal imaging findings were similar to that of TNBC, suggesting that the pathologic components of PSCCB are predominated by SCC and DCIS ranks the secondary position, which are consistent with the pathologic report of this case. PSCCB should be differentiated from the following mammary epithelial tumors on imaging based on their listed characteristics: Mucinous carcinoma: histologic findings of mucinous carcinoma were mucin devoid of neoplastic epithelium and clusters of tumor cells in the colloid stroma, which represented benign morphologic features, difficulty in the differentiation with PSCCB, the characteristic performance of mucinous carcinoma was persistent enhancement pattern and a very higher ADC value, the ADC value of mucinous carcinoma were even greater than most benign lesions. Medullary carcinoma: the tumor was defined as a well-circumscribed carcinoma composed of poorly differentiated cells with scant stroma and prominent lymphoid infiltration, and central necrosis secondary to hemorrhage was a common feature, corresponding to the imaging features difficulty in the differentiation with PSCCB. Pathologic biopsy is the gold standard for diagnosis of SCC of the breast. PSCCB is much less common than metastases from other small cell cancers; however, the diagnosis of PSCCB should be made when the absence of other primary lesions is confirmed by PET-CT or other general imaging examinations. For the present case, PET-CT findings suggested that there were no extra breast lesions, and the final diagnosis was PSCCB combined with the pathologic findings. In particular, the presence of the DCIS component can favor the diagnosis of SCC as a primary breast tumor.
As a rare malignant tumor, most information about the outcome and treatments of PSCCB derive from a limited number of cases reported in the literature. At present, there are no treatment guidelines or consensus for PSCCB. In accordance with the guidelines for the diagnosis and treatment of invasive breast cancer and small-cell lung cancer, surgery, radiotherapy, chemotherapy, endocrine therapy, and molecular targeted therapy can be selected in clinical practice. Kanat et al[2] carried out a retrospective analysis on the expression of hormone receptors in 53 cases of PSCCB, and approximately 75% of PSCCB was negative for either ER or PR. However, HER2 overexpression had seldom been reported in these tumors, which classified them as belonging to the TNBC, our case met it, in this regard, endocrine therapy and molecular targeted therapy may be less effective in PSCCB, surgical resection combined with adjuvant radiotherapy and chemotherapy is the most essential therapeutic approach, and there are individual differences in the clinical treatment effect. In the retrospective series conducted by Kanat et al,[2] the result showed a mortality rate of 18.9% with a mean follow-up 20.75 months (range, 3–60). To summarize, the early recognition of PSCCB from multimodality imaging may be vital in pretreatment planning and prognosis prediction, as well as in improving the understanding of the biologic behavior of this disease. Early active and effective surgery combined with adjuvant radiotherapy and chemotherapy is helpful to improve the prognosis of patients with PSCCB.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initial will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Funding
This study was supported by a grant of Lanzhou Talent Innovation and Entrepreneurship Project Foundation of China (No. 2017-RC-76).
Conflicts of interest
None.
Footnotes
How to cite this article: Guo ZZ, Feng W, Liu HF, Lu XR, Lei JQ. Value of multimodality imaging in diagnosing primary small cell carcinoma of breast. Chin Med J 2019;00:00–00. doi: 10.1097/CM9.0000000000000226
References
- 1.Mirza IA, Shahab N. Small cell carcinoma of the breast. Semin Oncol 2007; 34:64–66. doi: 10.1053/j.seminoncol.2006.10.029. [DOI] [PubMed] [Google Scholar]
- 2.Kanat O, Kilickap S, Korkmaz T, Ustaalioglu Oven BB, Canhoroz M, Cubukcu E, et al. Primary small cell carcinoma of the breast: report of seven cases and review of the literature. Tumori 2011; 97:473–478. doi: 10.1700/950.10400. [DOI] [PubMed] [Google Scholar]
- 3.Amano M, Ogura K, Ozaki Y, Tamai M, Kitabatake T, Fujisawa M, et al. Two cases of primary small cell carcinoma of the breast showing non-mass-like pattern on diagnostic imaging and histopathology. Breast Cancer 2015; 22:437–441. doi: 10.1007/s12282-012-0397-3. [DOI] [PubMed] [Google Scholar]
- 4.Mariscal A, Balliu E, Díaz R, Casas JD, Gallart AM. Primary oat cell carcinoma of the breast: imaging features. AIR Am J Roentgenol 2004; 183:1169–1171. doi: 10.2214/ajr.183.4.1831169. [DOI] [PubMed] [Google Scholar]