

Abstract
Studies have shown that individuals’ choice of a life partner predicts their life outcomes, from their relationship satisfaction to their career success. The present study examined whether the reach of one’s spouse extends even further, to the ultimate life outcome: mortality. A dyadic survival analysis using a representative sample of elderly couples (N = 4,374) followed for up to 8 years showed that a 1-standard-deviation-higher level of spousal life satisfaction was associated with a 13% lower mortality risk. This effect was robust to controlling for couples’ socioeconomic situation (e.g., household income), both partners’ sociodemographic characteristics, and baseline health. Exploratory mediation analyses pointed toward partner and actor physical activity as sequential mediators. These findings suggest that life satisfaction has not only intrapersonal but also interpersonal associations with longevity and contribute to the fields of epidemiology, positive psychology, and relationship research.
Keywords: life satisfaction, mortality, dyadic analyses, couples, open materials
Research has consistently shown that life satisfaction is associated with longevity (for a review, see Diener & Chan, 2011). For example, meta-analyses of long-term prospective studies have shown that higher life satisfaction predicts lower risk of mortality over decades (Chida & Steptoe, 2008). Although this literature has demonstrated an intrapersonal effect of life satisfaction (i.e., an effect of an individual’s life satisfaction on that individual’s mortality), it is less clear whether life satisfaction has interpersonal effects as well. In particular, does an individual’s life satisfaction affect the mortality risk of his or her spouse?
Epidemiological studies have demonstrated the importance of contextual characteristics (e.g., neighborhood characteristics; Bosma, Dike van de Mheen, Borsboom, & Mackenbach, 2001) for individuals’ longevity. Adopting the interpersonal perspective (Zayas, Shoda, & Ayduk, 2002), I propose that the characteristics (e.g., life satisfaction) of the people who are close to an individual can also make up that person’s context and, potentially, affect his or her life outcomes. For example, life satisfaction has been associated with healthy behaviors such as physical exercise (Kim, Kubzansky, Soo, & Boehm, 2017). Given that spouses tend to affect each other’s lifestyle (Jackson, Steptoe, & Wardle, 2015), having a happy spouse might increase one’s likelihood of engaging in healthy behaviors. In addition, happiness has been associated with helping behavior (O’Malley & Andrews, 1983). Hence, having a happy partner might be related to experiencing support from that partner and, consequently, might improve one’s health and longevity.
Indeed, a recent study found that spousal life satisfaction was associated with individuals’ self-rated health (Chopik & O’Brien, 2017), although such interpersonal effects were not detected for doctor-diagnosed chronic conditions (Chopik & O’Brien, 2017) or for inflammation markers (Uchino et al., 2018). None of the existing studies have explored whether spousal life satisfaction predicts individuals’ mortality. The present research examined this question using panel data of approximately 4,400 elderly couples in the United States. In addition, a set of exploratory mediation analyses tested the role of partner support as well as partner and actor physical activity as potential mechanisms for such an association.
Finally, it is possible that the level of spousal life satisfaction per se matters much less than the extent to which it is similar to individuals’ own life satisfaction. A growing body of research has underscored the level of congruence between partners’ dispositional characteristics as an important factor for their relationship and life outcomes (Dyrenforth, Kashy, Donnellan, & Lucas, 2010). Therefore, in an additional set of analyses, I explored whether the level of actor-partner similarity in life satisfaction was associated with actor mortality.
Method
Participants
The data for this study came from the Health and Retirement Study (HRS; http://hrsonline.isr.umich.edu/), a nationally representative panel study of American adults ages 50 and older and their spouses. It is sponsored by the National Institute on Aging (Grant No. NIA U01AG009740) and is conducted by the University of Michigan. HRS is particularly well suited for the present investigation because it collects data from both spouses. Starting in 2006, the study has included a measure of life satisfaction, as part of a self-report questionnaire that participants are asked to complete on their own and return by mail. For one half of the sample, life satisfaction was first measured in 2006, and for the other half, it was first measured in 2008. These data were combined into a baseline assessment. I selected participants who had a spouse or a live-in partner at baseline (95.7% of the participants who had a live-in partner were officially married).1 After I removed cases with missing values on key variables (actor life satisfaction, partner life satisfaction, survival time), the final sample consisted of 8,748 individuals (mean age at baseline = 67.17, SD = 9.75; 50.0% male). This sample size was large enough for even small effects to be detected with 80% power (at α = .05). Of the 4,374 couples, 99.5% were heterosexual. Data from participants who remained alive throughout the observation period (n = 6,643) or were lost to follow-up (n = 656) were censored.2
The data and materials for HRS can be accessed at its Website (http://hrsonline.isr.umich.edu/). The computer code for the analyses reported here can be accessed at the Open Science Framework (https://osf.io/geq9x/).
Measures
Life satisfaction
Life satisfaction was measured with the Satisfaction With Life Scale (Diener, Emmons, Larsen, & Griffin, 1985). This scale includes five items (e.g., “I am satisfied with my life”). Because a 6-point response scale was used in 2006 and a 7-point response scale was used in 2008 (both scales ranged from strongly disagree to strongly agree), I rescaled the responses to range from 1 to 10.3 The scale had good reliability (2006 subsample: α = .89; 2008 subsample: α = .88). The analyses included both partner and actor life satisfaction.
Mortality
The HRS data set included information on participants’ vital status (1 = deceased, 0 = alive) through December 2014. This information came from the National Death Index (Centers for Disease Control and Prevention, 2017), the spouse’s report, or both. Survival time was computed in months, starting from the month of the baseline interview and ending with death or censoring (in December 2014).
Additional variables
Perceived partner support was measured by participants’ ratings of the extent to which their partners provided them with social support (seven items; e.g., “How much can you rely on [your partner] if you have a serious problem?” “How much can you open up to [your partner] if you need to talk about your worries?” “How much does [your partner] let you down when you are counting on him/her?”; all items are provided in the Supplemental Material available online). Responses were given on a 4-point scale (1 = a lot, 4 = not at all) and were recoded such that higher values reflected stronger support. Each person’s recoded responses were then averaged (2006 subsample: α = .82; 2008 subsample: α = .84).
Actor and partner physical activity were assessed with two questions. Both partners indicated how often they engaged in vigorous activities (e.g., jogging, cycling, digging with a spade or shovel) and moderately energetic activities (e.g., gardening, cleaning the car, walking at a moderate pace, dancing). Responses to both questions were given on a 4-point scale (1 = more than once a week, 2 = once a week, 3 = one to three times a month, 4 = hardly ever or never) and were recoded such that higher values reflected higher frequency. The frequencies of vigorous and moderately energetic activity were related to each other (r = .36, p < .001), so I combined the responses to these two questions to form an indicator of physical activity.
To make sure that any observed association between partner life satisfaction and actor mortality was not driven by an overlap with sociodemographic characteristics or baseline health (e.g., one spouse’s health problems might negatively affect both spouses’ life satisfaction and mortality), I included a range of control variables in the analyses. Specifically, I controlled for actor and partner self-rated health (1 = poor, 5 = excellent), as well as morbidity, measured with the number of doctor-diagnosed chronic conditions (hypertension, diabetes, cancer, lung disease, coronary heart disease, stroke, arthritis, incontinence, psychiatric problems; although this list is not comprehensive, it covers major causes of death). Further control variables included actor gender (1 = male, 0 = female), actor and partner age at baseline, actor and partner ethnicity (1 = Caucasian, 0 = other), actor and partner education (1 = less than high school, 2 = general education diploma, 3 = high school diploma, 4 = some college, 5 = college and above), and baseline year (1 = 2008, 0 = 2006). Given that the household financial situation is likely to affect both partners’ life satisfaction and longevity, the analyses also included baseline household income (total annual household income in dollars, log transformed). To account for partner mortality, the analyses included a variable indicating whether the partner died during the observation period (1 = deceased, 0 = alive).
Results
Means and standard deviations of the variables, as well as their zero-order correlations, are provided in Table S1 in the Supplemental Material. During the observation period, 16.6% (n = 1,449) of the sample died. The survival time ranged from 2 to 104 months (8.67 years) and averaged 50.5 months (4.21 years). An examination of differences between survivors and decedents revealed that the latter were older, t(8746) = 33.57, p < .001; were more likely to be male, χ2(1, N = 8,748) = 191.90, p < .001; were less educated, t(8745) = 11.33, p < .001; and were less wealthy, t(2703) = 14.43, p < .001. They also were more likely to have chronic diseases, t(1955) = 20.66, p < .001; were less likely to engage in physical activity, t(8591) = 17.84, p < .001; and reported poorer self-rated health, t(1959) = 23.51, p < .001, and lower life satisfaction, t(1976) = 6.55, p < .001. Similarly, decedents’ spouses, compared with survivors’ spouses, were older, t(8746) = 24.53, p < .001; were less educated, t(2031) = 9.70, p < .001; reported more chronic conditions, t(8745) = 11.00, p < .001; reported a lower level of physical activity, t(8591) = 10.91, p < .001; and had poorer self-rated health, t(8741) = 8.13, p < .001. They also reported lower relationship satisfaction, t(1922) = 7.97, p < .001, and lower life satisfaction, t(1986) = 5.09, p < .001. Finally, decedents’ spouses were more likely than survivors’ spouses to die within the observation period, χ2(1, N = 8,748) = 202.61, p < .001.
To determine whether partner life satisfaction predicted actor mortality, I used multilevel (dyadic) survival analysis. Specifically, because time was measured on a continuous scale (in months), I used the Cox proportional hazards model. Given the clustered time-to-event data (individuals were clustered within dyads), I used an extension of the Cox model that accounts for correlated observations by implementing robust sandwich variance estimators. The analyses were conducted with the survival package (Therneau, 2015) in R. Note that using a frailty model with penalized likelihood estimation produced the same results (see Table S4 in the Supplemental Material).
Time to event was measured in months, from the baseline measurement of life satisfaction until death or censoring. I additionally checked for robustness of the results by conducting analyses using participants’ age as a time scale. These analyses provided the same results and are reported in the Supplemental Material (Table S4). All continuous variables were standardized before analysis, so the coefficients can be interpreted in terms of standard deviations.
The full estimation results are presented in Table S2 in the Supplemental Material. Model 1 showed that greater partner life satisfaction at baseline was associated with lower actor mortality risk. Specifically, a 1-standard-deviation-higher level of spousal life satisfaction was associated with a 13% lower risk of dying within the following 8 years (hazard ratio, or HR = 0.87, 95% confidence interval, or CI = [0.83, 0.91], p < .001). Figure 1 plots the cumulative hazard of death during the observation period, separately for individuals with a happy spouse (life satisfaction above the median) and individuals with an unhappy spouse (life satisfaction below the median). The figure shows that as time went by, the mortality risk of individuals with a happy spouse rose more slowly than the mortality risk of individuals with an unhappy spouse.
Fig. 1.
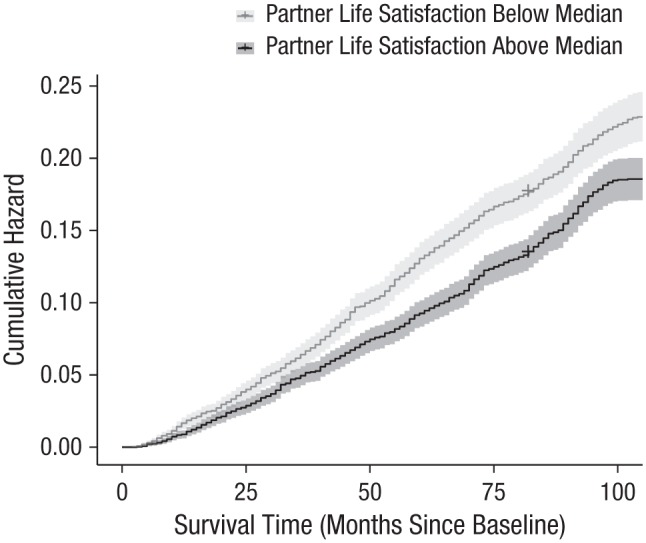
Cumulative hazard of death (including 95% confidence bands) during the observation period. Results are shown separately for individuals whose spouses reported life satisfaction below the median at baseline and those whose spouses reported life satisfaction above the median at baseline.
To make sure that this effect was not just a result of confounding with participants’ own life satisfaction, I added actor life satisfaction at baseline in Model 2 (see Table S2 in the Supplemental Material). The results showed that both greater actor life satisfaction at baseline (HR = 0.86, 95% CI = [0.82, 0.91], p < .001) and greater partner life satisfaction at baseline(HR = 0.92, 95% CI = [0.87, 0.97], p = .001) were associated with lower mortality risk.
Model 3 (see Table S2 in the Supplemental Material) showed that these effects were robust to controlling for major sociodemographic variables: actor gender, actor and partner age, actor and partner ethnicity, actor and partner education level, household income, baseline year, and couple type (same-sex vs. heterosexual4). A 1-standard deviation-higher level of actor life satisfaction was associated with an 18% lower mortality risk (HR = 0.82, 95% CI = [0.78, 0.86], p < .001), and a 1-standard deviation-higher level of partner life satisfaction was associated with a 10% lower mortality risk (HR = 0.90, 95% CI = [0.85, 0.95], p < .001).
In Model 4, I added actor and partner health indicators (self-rated health and morbidity) and partner mortality (whether the partner died during the observation period). The effect of actor life satisfaction on actor mortality was rendered nonsignificant (HR = 0.96, 95% CI = [0.90, 1.02], p = .155). In contrast, the effect of partner life satisfaction remained (HR = 0.92, 95% CI = [0.87, 0.97], p = .005).
Similarity effect
To explore whether the level of actor-partner similarity in life satisfaction was associated with actor mortality, I used a dyadic polynomial regression analysis, the state-of-the-art approach to testing similarity effects (Weidmann, Schönbrodt, Ledermann, & Grob, 2017). Actor mortality was regressed on actor and partner life satisfaction (xa and xp), their interaction term (xaxp), and the quadratic terms (xa2 and xp2). The quadratic and interaction terms were not significant (ps > .57). The only terms with significant effects were the linear terms of actor life satisfaction (HR = 0.85, 95% CI = [0.79, 0.92], p < .001) and partner life satisfaction (HR = 0.93, 95% CI = [0.86, 0.996], p = .039). Hence, I concluded that the data do not provide evidence for a similarity effect. Overall, these results suggest that having a partner who is more satisfied with life is associated with lower mortality regardless of one’s own level of life satisfaction.
Exploratory mediation analyses
The variables available in the data set allowed me to explore two potential mediation processes. First, I hypothesized that individuals with a happier partner experience more partner support, and that greater perceived partner support is associated with lower mortality. However, an examination of the zero-order associations among partner life satisfaction, perceived partner support, and actor mortality revealed that this mediation path is unlikely: Although having a happier partner was indeed associated with greater perceived partner support (r = .27, 95% CI = [.25, .29], p < .001), perceived partner support was not related to actor mortality (HR = 0.99, 95% CI = [0.94, 1.04], p = .69).
Second, I explored the role of partner and actor physical activity as sequential mediators. Specifically, on the basis of previous research (Kim et al., 2017), I hypothesized that greater partner life satisfaction is associated with increased partner physical activity, which in turn is associated with greater actor physical activity (Jackson et al., 2015) and, consequently, lower actor mortality. A look at the zero-order associations showed that, indeed, partner life satisfaction was positively associated with partner physical activity (r = .17, 95% CI = [.15, .19], p < .001), partner and actor physical activity were positively related to each other (r = .24, 95% CI = [.22, .26], p < .001), and actor physical activity negatively predicted actor mortality (HR = 0.75, 95% CI = [0.71, 0.79], p < .001).
Therefore, I proceeded to test for sequential mediation using multilevel structural equation modeling. The model (see Fig. S1 in the Supplemental Material included a set of multilevel (participants nested within couples) regression equations, in which partner life satisfaction predicted partner physical activity (path a, multilevel linear regression), partner physical activity predicted actor physical activity (path d, multilevel linear regression), and actor physical activity predicted actor mortality (path b, multilevel Cox regression). The indirect effect was computed by multiplying the a, d, and b paths, and its significance was tested using the delta method. The model included random intercepts for actor and partner physical activity and actor mortality and used clustered robust standard errors. The analyses were conducted with Stata/MP Version 14.2.
The results showed that partner life satisfaction was positively associated with partner physical activity (b = 0.08, 95% CI = [0.07, 0.09], p < .001), which in turn was positively associated with actor physical activity (b = 0.23, 95% CI = [0.20, 0.26], p < .001), which was negatively associated with actor mortality (HR = 0.64, 95% CI = [0.61, 0.68], p < .001). The coefficient for the indirect effect was significant, b = −0.008, 95% CI = [−0.01, −0.006], p < .001, which provided support to the sequential mediation. The indirect effect was robust to adding the control variables as predictors of both the mediators and the dependent variable (see Table S5 in the Supplemental Material).
Exploratory moderation analyses
I explored whether the effect of partner life satisfaction on actor mortality depended on various actor and partner characteristics: gender, age, ethnicity, education, income, health indicators, physical activity, perceived partner support, and partner mortality. I ran 16 models testing the interactions between partner life satisfaction and these variables (by adding the respective interaction terms, one at a time, to Model 4; see Table S2 in the Supplemental Material). The only significant interaction was between partner life satisfaction and partner mortality (HR = 1.15, 95% CI = [1.02, 1.31], p = .027). Partner life satisfaction was negatively associated with actor mortality only when the partner remained alive through the end of the observation period (partner alive: HR = 0.90, 95% CI = [0.83. 0.96], p = .003; partner deceased: HR = 1.03, 95% CI = [0.93, 1.15], p = .553). Yet the exploratory nature of these analyses and the multiple testing do not allow strong conclusions to be drawn.
Discussion
Previous research has shown that individuals’ career success and relationship and life satisfaction are predicted by their spouses’ dispositional characteristics (Dyrenforth et al., 2010; Solomon & Jackson, 2014). The present research suggests that spouses’ reach might extend even further. A dyadic survival analysis using the data from 4,374 couples showed that having a spouse who was more satisfied with life was associated with reduced mortality.
What explains this interpersonal effect of life satisfaction? Exploratory mediation analyses established partner and actor physical activity as sequential mediators. One partner’s life satisfaction was associated with his or her increased physical activity, which in turn was related to increased physical activity in the other partner, which predicted that partner’s mortality. Yet, given the correlational nature of these data, these results should be interpreted with caution.
It is noteworthy that the effect of spousal life satisfaction was comparable in size to the effects of other well-established predictors of mortality, such as education and income (in the present study, HRs = 0.90 for partner life satisfaction, 0.93 for household income, and 0.91 for actor education). In fact, spousal life satisfaction predicted mortality as strongly as (and even more robustly than) an individual’s own life satisfaction and as strongly as basic personality traits, such as neuroticism and extraversion, predicted mortality in previous work (Jokela et al., 2013).
Although most existing research on predictors of mortality has focused nearly exclusively on individuals’ own characteristics, the present analyses revealed that the characteristics of a person who is close to an individual, such as a spouse, might be an equally important determinant of that individual’s mortality. Continuing this line of research, future studies might explore whether the interpersonal effect of life satisfaction on mortality is restricted to (marital) dyads or whether it extends to larger social networks.
To conclude, happiness is a desirable trait in a romantic partner, and marriage to a happy person is more likely to last than is marriage to an unhappy person (Lucas, 2005). The present study showed that having a happier spouse is associated not only with a longer marriage but also with a longer life.
Supplementary Material
Acknowledgments
I would like to thank Anthony M. Evans for his statistical advice and general support.
Additional analyses using only married couples produced identical results (see Table S4 in the Supplemental Material).
These two groups of censored observations did not differ from each other on any variable included in the analyses, except for the number of chronic conditions: Participants who dropped out reported fewer chronic conditions (M = 1.87, SD = 1.40) than did participants who stayed in the panel (M = 2.07, SD = 1.46), t(7296) = 3.46, p = .001.
As a robustness check, I used standardization to normalize the data instead (i.e., I standardized the values within the two subsamples). The analyses using the standardized scale produced the same results as the analyses presented in the main text (see Table S3 in the Supplemental Material).
Being part of a same-sex couple positively predicted mortality (HR = 2.72, p = .018; there were 9 gay and 11 lesbian couples in the sample). The interaction between couple type (gay vs. lesbian) and actor gender was not significant (HR = 0.38, p = .260).
Footnotes
Action Editor: James K. McNulty served as action editor for this article.
Author Contributions: O. Stavrova is the sole author of this article and is responsible for its content.
ORCID iD: Olga Stavrova  https://orcid.org/0000-0002-6079-4151
https://orcid.org/0000-0002-6079-4151
Declaration of Conflicting Interests: The author(s) declared that there were no conflicts of interest with respect to the authorship or the publication of this article.
Supplemental Material: Additional supporting information can be found at http://journals.sagepub.com/doi/suppl/10.1177/0956797619835147
Open Practices:

All analysis code for this study has been made publicly available via the Open Science Framework and can be accessed at https://osf.io/geq9x/. The data are available through the Health and Retirement Study’s Web site (http://hrsonline.isr.umich.edu/). The design and analysis plans for this study were not preregistered. The complete Open Practices Disclosure for this article can be found at http://journals.sagepub.com/doi/suppl/10.1177/0956797619835147. This article has received the badge for Open Materials. More information about the Open Practices badges can be found at http://www.psychologicalscience.org/publications/badges.
References
- Bosma H., Dike van de Mheen H., Borsboom G. J. J. M., Mackenbach J. P. (2001). Neighborhood socioeconomic status and all-cause mortality. American Journal of Epidemiology, 153, 363–371. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. (2017). National Death Index [Data file]. Retrieved from http://www.cdc.gov/nchs/ndi.htm
- Chida Y., Steptoe A. (2008). Positive psychological well-being and mortality: A quantitative review of prospective observational studies. Psychosomatic Medicine, 70, 741–756. [DOI] [PubMed] [Google Scholar]
- Chopik W. J., O’Brien E. (2017). Happy you, healthy me? Having a happy partner is independently associated with better health in oneself. Health Psychology, 36, 21–30. [DOI] [PubMed] [Google Scholar]
- Diener E., Chan M. Y. (2011). Happy people live longer: Subjective well-being contributes to health and longevity. Applied Psychology: Health and Well-Being, 3, 1–43. [Google Scholar]
- Diener E., Emmons R. A., Larsen R. J., Griffin S. (1985). The Satisfaction With Life Scale. Journal of Personality Assessment, 49, 71–75. [DOI] [PubMed] [Google Scholar]
- Dyrenforth P. S., Kashy D. A., Donnellan M. B., Lucas R. E. (2010). Predicting relationship and life satisfaction from personality in nationally representative samples from three countries: The relative importance of actor, partner, and similarity effects. Journal of Personality and Social Psychology, 99, 690–702. [DOI] [PubMed] [Google Scholar]
- Jackson S. E., Steptoe A., Wardle J. (2015). The influence of partner’s behavior on health behavior change: The English Longitudinal Study of Ageing. JAMA Internal Medicine, 175, 385–392. [DOI] [PubMed] [Google Scholar]
- Jokela M., Batty G. D., Nyberg S. T., Virtanen M., Nabi H., Singh-Manoux A., Kivimäki M. (2013). Personality and all-cause mortality: Individual-participant meta-analysis of 3,947 deaths in 76,150 adults. American Journal of Epidemiology, 178, 667–675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim E. S., Kubzansky L. D., Soo J., Boehm J. K. (2017). Maintaining healthy behavior: A prospective study of psychological well-being and physical activity. Annals of Behavioral Medicine, 51, 337–347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lucas R. (2005). Time does not heal all wounds: A longitudinal study of reaction and adaptation to divorce. Psychological Science, 16, 945–950. [DOI] [PubMed] [Google Scholar]
- O’Malley M. N., Andrews L. (1983). The effect of mood and incentives on helping: Are there some things money can’t buy? Motivation and Emotion, 7, 179–189. [Google Scholar]
- Solomon B. C., Jackson J. J. (2014). The long reach of one’s spouse: Spouses’ personality influences occupational success. Psychological Science, 25, 2189–2198. [DOI] [PubMed] [Google Scholar]
- Therneau T. M. (2015). A package for survival analysis in S (Version 2.38) [Computer software]. Retrieved from https://CRAN.R-project.org/package=survival
- Uchino B. N., Kent R. G., Cronan S., Smith T. W., Diener E., Joel S., Bosch J. (2018). Life satisfaction and inflammation in couples: An actor–partner analysis. Journal of Behavioral Medicine, 41, 22–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weidmann R., Schönbrodt F. D., Ledermann T., Grob A. (2017). Concurrent and longitudinal dyadic polynomial regression analyses of Big Five traits and relationship satisfaction: Does similarity matter? Journal of Research in Personality, 70, 6–15. [Google Scholar]
- Zayas V., Shoda Y., Ayduk O. N. (2002). Personality in context: An interpersonal systems perspective. Journal of Personality, 70, 851–900. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.