

Abstract
Few studies have explored relations among sexual assault and prospective development of high-risk behaviors among adolescent girls. The present study examined longitudinal associations among child sexual assault (CSA) and high-risk behaviors (nonexperimental alcohol and drug use; delinquent behavior) in a nationally representative sample of adolescent girls aged 12 ‒ 17. Using path modeling, findings provided support for the link between CSA and nonexperimental alcohol use, drug use, and delinquent behavior after controlling for demographic characteristics and Time 1 functioning. Additionally, past 6-month post-traumatic stress disorder assessed at Time 1 was significantly associated with CSA and delinquency measured at Time 2, although the indirect effects did not reach traditional levels of significance. These findings suggest that CSA may potentiate risk for a number of public health problems.
Keywords: sexual assault, substance use, delinquency
Approximately 1.8 million adolescents report exposure to at least one incident of child sexual assault (CSA) [1]. CSA lifetime prevalence ranges from 14% to 26%, with a disproportionate number of girls impacted [2–5]; making this a significant public health concern in the United States. CSA increases risk for dysfunction into adulthood [6,7], including heightened rates of post-traumatic stress disorder (PTSD) and anxiety [8], depression [8], suicide attempts [6], attention and impulsivity problems[9],substance use[4,10],and delinquency[11].CSA increases persistent negative affect [12], and victims may self-medicate with drugs or alcohol, consistent with the self-medication hypothesis [13]. Thus, adolescents may engage in high-risk behaviors (i.e., substance abuse and delinquency), as a means of “acting out” the depression or anger that arises from a stressor, such as CSA. Indeed, anger has been found to mediate CSA and delinquency among adolescents [14], in support of general strain theory. Associations between CSA and substance use are especially profound among adolescents girls [10], highlighting need to examine relationships among this population.
CSA and Substance Use
Fifty percent of U.S. adolescents reported using substances at some point in their lifetime [15]. Further, results from a nationally representative sample demonstrated that 25.2% of adolescents met criteria for alcohol abuse, 11.2% for drug use, and 7.4% for both [16]. Female CSA victims were three times as likely to report substance use problems compared to nonabused girls (40.5% vs. 14%) [17], which was consistent across multiple substances [18]. Further, PTSD symptoms were not significantly related to the relationship between CSA and substance use [16], suggesting that the link is not accounted for by PTSD symptoms.
CSA and Delinquent Behavior
Adolescent CSA victims were twice as likely to be arrested for a violent offense (13.6% vs. 6.3%) and 1.35 times more likely to be arrested for a property offense (9.2% vs. 6.3%) [19]. Risk for delinquency is even higher when PTSD symptoms are involved, as adolescents who reported CSA and PTSD engaged in delinquency behaviors more frequently than CSA adolescents without history of PTSD (odds ratio [OR] = 2.4) [16]. Of particular relevance, research has indicated a significant link between CSA and delinquent behavior among girls, but not among boys [19].
CSA and Multiple High-Risk Behaviors
Substance use and delinquency are more likely to occur simultaneously in adolescence than during other developmental periods [20], as 25% of adolescents detained for delinquent acts reported alcohol use, 70% drug use, and 75% either alcohol or drug use [21]. Developmentally, adolescence is associated with heightened risk taking behavior, as adolescents are less likely to perceive situations, such as substance use and delinquency, as harmful [22,23]. Youth who simultaneously engage in these behaviors are at increased risk for detrimental outcomes including physical health problems, lower life expectancy, psychosocial adjustment problems, and difficulty transitioning to adulthood [24]. Females, specifically, who engage in substance use or delinquency are unlikely to abstain from these behaviors later in development [20].
Aims of the Current Study
While the link between CSA and high-risk behaviors has been established [10,11,19], less information is available regarding the simultaneous effects of CSA, substance use, and delinquent behaviors. Analysis from the National Survey of Adolescents (NSA) [25] indicated that CSA predicted high-risk behaviors among adolescent girls; however, reverse relationships were not significant (i.e., high-risk behaviors did not predict subsequent CSA). Associations between CSA and individual high-risk behaviors were not examined. As PTSD mediated the link between CSA and delinquency, but not CSA and substance use [16], it is also important to examine PTSD. To our knowledge, no study has utilized a nationally representative sample of adolescent girls and longitudinal design to investigate relationships between CSA, subsequent onset of alcohol use, drug use, and delinquent behavior, and postonset PTSD.
This study longitudinally examines the relations among CSA, substance use (i.e., nonexperimental alcohol use and nonexperimental drug use), and delinquent behavior among girls, utilizing a nationally representative sample of adolescents. We hypothesized that CSA would predict each type of subsequent high-risk behavior (nonexperimental alcohol use, nonexperimental drug use, and delinquent behavior) after controlling for earlier levels of that behavior. Given high association between CSA, PTSD, and high-risk behaviors, as well as the impact of PTSD on CSA and delinquency but not CSA and substance use [16], it is important to examine mediation of PTSD.
Methods
The NSA-replication was a longitudinal telephone survey of 3,614 youths, aged 12 17 years, living in U.S. households. The NSA-R identified the prevalence of physical assault, sexual assault, and witnessed violence in the home, school, and community, and mental health problems commonly associated with victimization, such as PTSD, depression, substance use, and delinquency.
Participants
The NSA-R included a national household probability sample and oversample of urban-dwelling adolescents. Recruitment began following Institutional Review Board approval. Sample selection and interviewing were conducted by Schulman, Ronca, and Bucuvalas, Inc. The initial probability sample used a multistage, stratified, area probability, random-digit-dialing six-stage sampling procedure. The urban dwelling sample used similar selection procedures limited to telephone banks within urban areas defined by the Census Bureau. Detailed information on sampling procedures are contained in Kilpatrick et al. [26].
Parents in 6,694 households with an eligible adolescent completed a brief structured interview; 5,426 (81%) consented for adolescents to be interviewed. A total of 188 adolescents (2.8%) refused to be interviewed; 119 (2.2%) interviews were initiated but not completed; and 1,505 (28.5%) adolescents were unreachable or not available for interview. Thus, 3,614 cases (67%) resulted in complete interviews at Time 1 (T1), including 2,459 from the national cross-section and 1,155 from the urban-dwelling adolescents sampling.
Of these adolescents, 2,511 (69%) completed the follow-up assessment at Time 2 (T2; mean between T1 and 2 = 15.29 months, standard deviation = 4.58 months). The 1,103 uncompleted T2 assessments were due to technical problems or nonworking number (29%); inability to reach the participant (24%); adolescent refusal during T2 recontact (17%); wrong telephone number (12%); ineligibility (9%); or only partial completion of the interview (9%). To examine attrition, effect sizes compared participants who completed versus did not complete the T2 assessment. Effect sizes were small for all CSA and high-risk behavior variables (range of d = 0.04−0.13); indicating minimal differences between completers and noncompleters on all variables.
Because adolescents were oversampled in urban areas, cases were weighted to maximize representativeness to the 2005 U.S. adolescent population. Cell weights restored urban cases to their true proportion of the urban/suburban/rural variable, based on 2005 U.S. Census estimates. Next, cell weights adjusted the weights based on age and sex. Generated sample frequencies were computed by age cohort and sex and compared this distribution to the U.S. Census estimates, and weightings were assigned to each sex × age group cell within the sample. This procedure resulted in weighted sample distributions that closely approximated 2005 U.S. Census estimates.
Of the weighted sample of 3,614 participants, the sample of 1,763 girls between aged 12 and 17 (M = 14.50, standard deviation = 1.72) was used in the current analysis, with 9% of girls aged 15‒17. The study included only girls, given that only 3.8% of boys reported any sexual assault incident at T1 and 0.5% at T2. Sixty-eight percent of girls (N = 1,205) self-identified their race as Caucasian, 14% (N = 237) as African-American, 10% (N = 185) as Hispanic, 2% (N = 36) as Asian/Pacific Islander, 3% (N = 47) as Native American and 3% (N = 52) did not report race information.
Measures
A highly structured telephone interview with trained interviewers obtained information regarding demographics, sexual assault, and high-risk behaviors (i.e., alcohol use, nonexperimental alcohol use, drug use, nonexperimental drug use, and delinquency). T1 responses for CSA and high-risk behaviors were based upon lifetime prevalence, while T2 responses included information since the last interview.
Demographics:
Adolescents reported on current age, gender, and race coded into five dummy-coded variables (Caucasian, African-American, Hispanic, Asian/Pacific Islander, or Native American).
CSA was assessed using a module from the original NSA, which can be obtained by contacting the authors [26]. CSA was defined as (a) unwanted vaginal or anal penetration by an object, finger, or penis; (b) unwanted oral sex; (c) another person touching the adolescent’s genitalia against their will; or (d) adolescent unwillingly touching another’s genitalia. To be deemed as CSA, the participant had to answer affirmatively to at least one question. This scale demonstrated high internal consistency in this study (a = 0.99). Approximately 11.5% of adolescents had experienced one of the four CSA incidences in their lifetimes and 3.7% experienced one or more CSA incidences between T1 and T2.
High-risk behaviors:
Alcohol use was assessed using a modified version of the substance use and delinquency assessment modules from the original NSA, which can be obtained by contacting the authors [26]. Nonexperimental alcohol use (termed “alcohol use”) included one question assessing whether adolescents had ever gotten drunk or very high from alcohol (yes/no). Approximately 7.2% of adolescents reported that they had gotten drunk or very high from alcohol in their lifetimes at T1 and 8.3% between the T1 and T2 interviews.
Nonexperimental drug use (termed “drug use”) included one question assessing whether adolescents had used drugs on four or more occasions (yes/no). Drug use was characterized by marijuana, inhalants, or hard drugs, including cocaine, heroin, lysergic acid diethylamide, or nonmedical use of prescription drugs. Nonmedical use of prescription drugs was included due to its growing prevalence among adolescent populations [27], subjective effects, addictive potential, and lethality similar to that of other hard drugs. Approximately 9.7% of adolescents had used drugs on four or more occasions in their lifetimes, while 8.3% between the T1 and T2 interviews.
Delinquent behavior was assessed with a modified version of the National Youth Survey, which included whether the adolescent had (a) purposely damaged or destroyed property; (b) stolen something, including a vehicle; (c) beaten up or physically attacked someone; (d) broken into a vehicle, office building, store, or house to steal something; (e) sold drugs; (f) been involved in a gang fight; (g) used force to get money or things from others; (h) attacked someone with or without a weapon; (i) forced someone to do something sexual; or (j) been arrested or in jail. The responses were summed for a total delinquent behavior score, which demonstrated moderate internal consistency (a = 0.48). A dichotomous variable reflecting whether the adolescent had engaged in one or more behaviors was used; 13.8% of adolescents reported at least one lifetime delinquent behavior at T1, and 7.5% between the T1 and T2 interviews.
PTSD was assessed using the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition criteria. Past 6-month PTSD was determined using questions about presence or absence of individual symptoms.
Procedure
Interviews were conducted in English using computer-assisted telephone interviewing [26]. Interviewers provided parents with a study description and interview topics, informed them the adolescent could refuse to answer any questions or terminate the interview at any time, and obtained parental permission to contact the adolescent. Adolescent assent was obtained.
Steps were taken to ensure adolescents could answer questions freely and privately: (1) interviewers asked whether privacy could be assured and he/she could answer in an open and honest manner. If the adolescent could not, the interview was rescheduled; (2) the interview was primarily designed with closed-ended questions to reduce likelihood of negative consequences if others were listening. Following completion, adolescents received an NSA certificate of participation and monetary compensation of $5.
Several steps were taken to recontact participants for T2 assessment, including (1) contacting participants at the telephone number on file, (2) obtaining three additional telephone numbers from past residences using ChoicePoint Credit Information Bureau, (3) sending letters to the last known address, and (4) recontacting ChoicePoint after 3 months to obtain updated telephone numbers.
Participant Protection
Participants were offered the toll-free number for Child Help, a counseling program for at-risk youth. Participants were debriefed to assess for distress and immediate intervention or referral. Federal guidelines for studies funded by the U.S. Department of Justice preclude investigators from disclosing information without participant consent. A “person in danger” response protocol was used to assess and progressively intervene in potentially dangerous situations such as suicidality or violence. Participants indicating that they (a) had been sexually assaulted in the past year, (b) had been hit or physically assaulted by a family member living in the household in the past year, (c) had not disclosed the sexual or physical assault to anyone, or (d) who expressed current suicidal ideation, were contacted by a trained clinician who assessed the situation and intervened if necessary. Adolescents in current danger were encouraged to tell a trusted adult and ask for help or seek help from a school counselor or other available professional. Clinicians followed up with participants and were prepared to intervene with local professionals if the adolescent was unwilling. However, no reports of confidentiality breach were made.
Data Analysis
Analyses were conducted in Mplus version 8.0. Approximately 71.2% (n = 1,255) of T1 participants provided data at T2. There were no significant differences between those who did and did not return for follow-up in terms of Wave 1 reports of CSA and alcohol use; however, those who reported lifetime drug use, χ2(1, n = 1,763) = 4.7, p < .05, and delinquency, χ2(1, n = 1,763) = 23.2, p < .001, at Wave 1 were less likely to return for the Wave 2 follow-up. To address missing data, primary analyses were conducted using maximum likelihood estimation with robust standard errors (SEs), which uses all available data to test various combinations of population parameter estimates until it identifies the parameter estimates that yield the best fit to the data as indicated by the highest log-likelihood value [28]. This approach, referred to as full information maximum likelihood, is asymptotically equivalent to multiple imputation [28].
To address whether CSA at T1 was associated with CSA, alcohol use, drug use, and delinquency at T2, we used a path modeling framework. Because outcome variables were dichotomous, the categorical option was utilized along with Monte Carlo integration. To address our secondary aim of examining the possible mediational role of PTSD in the association between T1 CSA and T2 risk behaviors and CSA, Cole and Maxwell’s [29] approach to testing mediation (indirect effects) with two waves of data was used. Indirect effects were calculated as the product of coefficients. In addition to examining path coefficients, effect size measures (e.g., ORs, R2) were examined to understand the magnitude of associations and the ratio of variance explained in the model to the total variance in the model.
Results
Preliminary data analysis
Descriptive statistics on the prevalence and incidence of CSA, each of the high-risk behaviors, and past 6-month PTSD are presented in Table 1. Correlations between study variables and CSA were small (range=.07 ‒.22; see Table 1).
Table 1.
Preliminary statistics and bivariate correlations
| Prevalence | Bivariate correlations | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| (% Yes, n) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
| 1. T1 CSA | 11.5%, n = 200 | - | .19** | .17** | .22** | .19** | .14** | .21** | .16** | .17** |
| 2. T2 CSA | 3.7%, n = 46 | – | .10** | .07* | .14** | .15** | .14** | .11** | .16** | |
| High-risk behaviors T1 | – | – | – | – | – | – | – | |||
| 3. Alcohol use | 7.2%, n = 127 | – | .40** | .26** | .21** | .32** | .24** | .12** | ||
| 4. Drug use | 9.7%, n = 170 | .33** | .20** | .36** | .20** | .14** | ||||
| 5. Delinquency | 13.8%, n = 243 | - | .17** | .15** | .35** | .17** | ||||
| High-risk behaviors T2 | – | – | – | |||||||
| 6. Alcohol use since T1 | 8.3%, n = 104 | – | .40** | .27** | .13** | |||||
| 7. Drug use since T1 | 8.3%, n = 104 | – | – | .32** | .11** | |||||
| 8. Delinquency since T1 | 7.5%, n = 95 | – | .14** | |||||||
| 9. T1 past 6-month PTSD | 5.8%, n = 105 | – | ||||||||
Note: Time 1 includes lifetime prevalence of sexual assault or high-risk behaviors, while Time 2 includes incidence of child sexual assault or high-risk behavior since last interview (M = 15.29 months, standard deviation = 4.58 months).
p < .05.
p < .001.
Covariate analyses
To examine whether age and ethnicity (dichotomized into white and non-white) should be covariates in the models, we examined potential bivariate differences in outcomes of interest. Older age was positively associated with CSA, B =.27, SE = .05, p < .001, alcohol use, B = .54, SE = .07, p < .001, druguse, B = .62, SE = .06, p < .001, and delinquency, B = .27, SE =.04, p <.001, at T1, and alcohol use, B = .45, SE = .07, p < .001, drug use, B = .46, SE = .07, p < .001, and delinquency, B = .16, SE = .07, p < .001, at T2. Age did not predict CSA at T2, χ2(1, n = 1,255) = 2.5, p = .12.
Although there were no ethnic differences in CSA at T1, χ2(1, n = 1,763) = 3.4, p = .07 or T2, χ2(1, n = 1,255) = 1.7, p = .20, or in alcohol use, x2(1, n = 1,763) = 2.8, p = .10, or drug use, χ2(1, n = 1,763) = 1.5, p = .22, at T1, white adolescents were more likely to report alcohol use, χ2(1, n = 1,255) = 7.8, p < .001, and drug use, χ2(1, n = 1,255) = 6.1, p < .001 at T2. Non-white adolescents were more likely to report delinquency at T1, χ2(1, n = 1,763) = 53.5, p < .001, and T2, χ2(1, n = 1,255) = 4.8, p < .05.
Direct Effects Modeling
We hypothesized that T1 CSA would predict subsequent alcohol use, drug use, and delinquent behavior between T1 and T2 above and beyond contributions at T1. To replicate past findings that early sexual victimization is associated with revictimization, the association between lifetime CSA history assessed at T1 and CSA occurring between T1 and T2 also was modeled. Age and white race/ethnicity were included as covariates by regressing T1 variables on both. Unstandardized estimates, SEs, and ORs are presented in Table 2 and standardized path coefficients are presented in Figure 1. CSA at T1 was positively associated with CSA, alcohol use, drug use, and delinquency at T2 after controlling for alcohol use, drug use, and delinquency as well as age and ethnicity. Standardized path coefficients ranged from .13 to .32. Girls who reported T1 CSA were 7.3 times more likely to report CSA, 2.3 times more likely to report alcohol use and delinquency at T2, and 2.98 times more likely to report drug use at T3 compared to girls who did not report T1 CSA.
Table 2.
Direct and indirect effects
| Direct effects | Estimate | Standard error | T | Odds ratio |
|---|---|---|---|---|
| T2 CSA on T1 CSA | 1.99 | .40 | 4.96*** | 7.32 |
| T2 CSA on T1 PTSD | 1.24 | .57 | 2.19* | 3.47 |
| T2 CSA on race | −.62 | .37 | −1.66+ | .54 |
| T2 CSA on age | −.05 | .11 | −.45 | .95 |
| T2 alcohol use on T1 CSA | .84 | .34 | 2.49* | 2.32 |
| T2 alcohol use on T1 alcohol use | 1.13 | .37 | 3.09** | 3.09 |
| T2 alcohol use on T1 PTSD | .80 | .44 | 1.83+ | 2.23 |
| T2 alcohol use on race | 1.19 | .39 | 3.09** | 3.30 |
| T2 alcohol use on age | .45 | .08 | 5.37*** | 1.57 |
| T2 drug use on T1 CSA | 1.09 | .35 | 3.12** | 2.98 |
| T2 drug use on T1 drug use | 1.88 | .34 | 5.53** | 6.53 |
| T2 drug use on T1 PTSD | .41 | .55 | .76 | 1.51 |
| T2 drug use on race | .84 | .36 | 2.31 | 2.31 |
| T2 drug use on age | .34 | .10 | 3.43*** | 1.41 |
| T2 delinquency on T1 CSA | .81 | .36 | 2.24* | 2.26 |
| T2 delinquency on T1 drug use | 2.28 | .30 | 7.50*** | 9.76 |
| T2 delinquency on T1 PTSD | .90 | .44 | 2.04* | 2.46 |
| T2 delinquency on race | −.37 | .30 | −1.23 | .69 |
| T2 delinquency on age | −.03 | .09 | −.29 | .97 |
| T1 PTSD on T1 CSA^ | .10 | .03 | 3.24*** | – |
| Indirect effects | – | |||
| T1 CSA –T1 PTSD – T2 CSA | .13 | .07 | 1.88+ | |
| T1 CSA – T1 PTSD – T2 alcohol | .08 | .05 | 1.53 | – |
| T1 CSA – T1 PTSD – T2 drug use | .04 | .06 | .74 | – |
| T1 CSA – T1 PTSD – T2 delinquency | .09 | .05 | 1.69+ | – |
Used to calculate subsequent indirect effects, – not estimated
p < .10
p < .05
p < .01
p < .001
Figure 1.
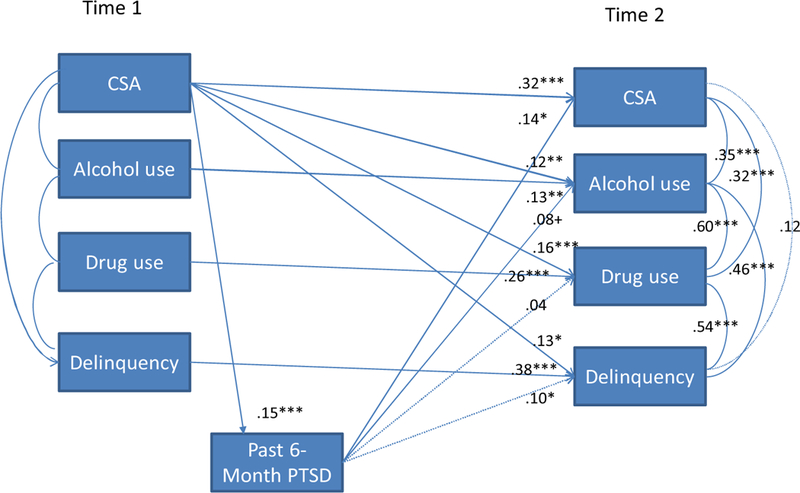
Standardized path coefficients for direct effects.
Indirect Effects Modeling
As shown in Table 2, there was a significant direct effect between T1 CSA and T1 PTSD, but T1 PTSD was only significantly positively associated with CSA and delinquency at T2. None of the indirect effects reached traditional levels of significance; however, there was a trend for PTSD to have an indirect effect between CSA at T1 and both CSA at T2 and delinquency at T2.
The variance accounted for in each outcome ranged from 15% for CSA at T2 to 21% for delinquency, 27% for drug use, and 28% for alcohol use at T1. Older age was significantly positively associated with alcohol and drug use, and white ethnicity was significantly positively associated with alcohol use. Within assessment waves, variable residuals were significantly correlated, which is to be expected given vast literature on linkages between variables of interest.
Discussion
Results build upon literature using a nationally representative sample of adolescent girls and a longitudinal design to examine specific relations among CSA, substance use (i.e., nonexperimental alcohol use, nonexperimental drug use), and delinquent behavior. Consistent with past research [30], girls who experienced CSA at T1 had elevated odds of CSA at T2, and PTSD partially mediated this association, although results did not meet traditional levels of significance. Consistent with hypotheses, findings supported the link between CSA and alcohol use, drug use, and delinquent behavior, which is consistent with past literature [4,10,11,18,25]. The finding that CSA among adolescent girls was related to subsequent high-risk behaviors is consistent with general strain and coping theories, which posit that exposure to stressors can increase general negative affect, including emotional responses such as depression and anger. In turn, adolescents may regulate the internal experience of negative affect (by using alcohol or drugs) or avoid feeling negative affect (by acting out angrily and engaging in delinquency). Additional studies should examine coping and general strain theories in relation to other high-risk behaviors that frequently occur following exposure to CSA among adolescents, such as risky and/or impulsive sexual behavior and bullying that may be associated with aggression.
Past 6-month PTSD at T1 partially mediated associations between T1 CSA and subsequent CSA and delinquency, but it did not mediate associations between CSA and alcohol and drug use after controlling for age and ethnicity. Findings are consistent with earlier findings that PTSD mediates links between CSA and delinquency but not substance use [16]. Findings add to a growing literature suggesting that PTSD symptoms mediate associations between early abuse and later revictimization among college women [30], by showing that associations extend to adolescent girls.
Limitations
While this study provides insight regarding the detrimental link between sexual assault and high-risk behaviors among adolescent girls, several limitations should be noted. First, the study utilized self-report, retrospective assessment data, which increased the likelihood of common method variance and limited comprehensive assessment of CSA and high-risk behaviors. Second, some of the measures were modified from previous nationally representative studies, but lacked extensive validation. Future studies should validate these scales. Third, as the assessment of PTSD symptoms included an overall symptom inventory, rather than directly linking symptoms to a specific CSA incident, it is unknown whether PTSD symptoms are directly related to the CSA incident or to another incident of trauma exposure. Additionally, substance use was assessed as a single item, which may not have fully addressed the level of substance use engaged in adolescents.
Adolescents without household telephones were not sampled in this study. However, data indicate that most households are equipped with telephone coverage, indicating that this sample is representative of the majority of U.S. adolescents [31]. Fourth, only a limited number of high-risk variables were included, although adolescents may engage in additional high-risk behaviors such as sexual behavior and bullying. Similarly, additional contextual (e.g., family or neighborhood) or intraindividual (e.g., mental health) factors were not included; additional studies should investigate whether these factors influence CSA or high-risk behaviors. Additionally, attrition could have influenced our findings, as only 69% of T1 participants completed T2. However, data indicated few differences between completers and noncompleters. Finally, results were based on a 2-year time span, which limits investigation of long-term trends.
Implications for Future Research, Policy, and Practice
Findings have significant implications in prevention and intervention for adolescent girls exposed to CSA. Specifically, results provide support for the relationship between CSA and subsequent substance use and delinquency, which highlights the importance of addressing high-risk behaviors within treatment interventions following CSA. The field has begun to utilize integrated interventions to address these concerns, although empirical data supporting the efficacy and effectiveness of these approaches are limited. Thus, further development and empirical investigations of these Promising interventions are imperative to preventing high-risk behaviors following CSA exposure among adolescents.
Overall, findings build upon literature demonstrating that CSA among adolescents is associated with subsequent high-risk behaviors. Further research utilizing multimeasure, multi-informant approaches would increase generalization and knowledge regarding these relationships. Increased evidence for this link further support the importance of prevention and intervention services that target girls, specifically, and that address CSA prevention as well as engagement in high-risk behaviors.
IMPLICATIONS AND CONTRIBUTION.
These findings have significant implications in prevention and intervention services for adolescent girls exposed to sexual assault. Specifically, results provide support for the relationship between child sexual assault and subsequent substance use and delinquency, which highlights the importance of addressing high-risk behaviors within current treatment interventions following sexual assault.
Acknowledgments
This research was supported by grant 5K12DA031794–03 from NIDA to support the first author, and grant 1R01 HD046830–01 from NICHD to the last author. The views in this article do not necessarily represent those of the agency supporting this research.
References
- [1].Kilpatrick DG, Saunders BE, Smith DW. Youth victimization: Prevalence and implications. Research in brief Washington, DC: US Department of Justice, Office of Justice Programs; 2003. [Google Scholar]
- [2].Finkelhor D, Shattuck A, Turner HA, Hamby SL. The lifetime prevalence of child sexual abuse and sexual assault assessed in late adolescence. J Adolesc Health 2014;55:329–33. [DOI] [PubMed] [Google Scholar]
- [3].Finkelhor D, Turner H, Ormrod R, et al. National survey of children’s exposure to violence. Juv Justice Bull 2009. Office of Juvenile Justice and Delinquency Prevention. Retrieved from www.ncjrs.gov/pdffiles1/ojjdp/grants/248444.pdf. [Google Scholar]
- [4].Hamburger ME, Leeb RT, Swahn MH. Childhood maltreatment and early alcohol use among high-risk adolescents. J Studies Alcohol Drugs 2008;69:291–5. [DOI] [PubMed] [Google Scholar]
- [5].Molnar BE, Buka SL, Kessler RC. Child sexual abuse and subsequent psychopathology: Results from the National Comorbidity Survey. Am J Public Health 2001;91:753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Tomasula JL, Anderson LM, Littleton HL, Riley-Tillman TC. The association between sexual assault and suicidal activity in a national sample. School Psychol Q 2012;27:109. [DOI] [PubMed] [Google Scholar]
- [7].Young MS, Harford K-L, Kinder B, Savell JK. The relationship between childhood sexual abuse and adult mental health among undergraduates: Victim gender doesn’t matter. J Interpers Violence 2007;22:1315–31. [DOI] [PubMed] [Google Scholar]
- [8].Chang C, Kaczkurkin AN, Mclean CP, Foa EB. Emotion regulation is associated with PTSD and depression among female adolescent survivors of childhood sexual abuse. Psychol Trauma 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [9].Briscoe-Smith AM, Hinshaw SP. Linkages between child abuse and attention-deficit/hyperactivity disorder in girls: Behavioral and social correlates. Child Abuse Neglect 2006;30:1239–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Marotta PL. Childhood adversities and substance misuse among the incarcerated: Implications for treatment and practice in correctional settings. Subst Use Misuse 2017;52:717–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Watts SJ. The link between child abuse and neglect and delinquency: Examining the mediating role of social bonds. Victims Offenders 2017;12:700–17. [Google Scholar]
- [12].Marx BP, Heidt JM, Gold SD. Perceived uncontrollability and unpredictability, self-regulation, and sexual revictimization. Rev Gen Psychol 2005;9:67. [Google Scholar]
- [13].Khantzian EJ. The self-medication hypothesis of substance use disorders: A reconsideration and recent applications. Harvard Rev Psychiatry 1997;4:231–44. [DOI] [PubMed] [Google Scholar]
- [14].Sigfusdottir ID, Asgeirsdottir BB, Gudjonsson GH, Sigurdsson JF. A model of sexual abuse’s effects on suicidal behavior and delinquency: The role of emotions as mediating factors. J Youth Adolesc 2008;37:699–712. [Google Scholar]
- [15].Substance Abuse and Mental Health Services Administration (SAMHSA). National Survey on Drug Use and Health (NSDUH) www.samhsa.gov/data/sites; 2014. [Google Scholar]
- [16].Kmett Danielson C, Macdonald A, Amstadter AB, et al. Risky behaviors and depression in conjunction with—or in the absence of—lifetime history of PTSD among sexually abused adolescents. Child Maltreatment 2010;15:101–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Simpson TL, Miller WR. Concomitance between childhood sexual and physical abuse and substance use problems: A review. Clin Psychol Rev 2002;22:27–77. [DOI] [PubMed] [Google Scholar]
- [18].Bailey JA, McCloskey LA. Pathways to adolescent substance use among sexually abused girls. J Abnormal Child Psychol 2005;33:39–53. [DOI] [PubMed] [Google Scholar]
- [19].Siegel JA, Williams LM. The relationship between child sexual abuse and female delinquency and crime: A prospective study. J Res Crime Delinq 2003;40:71–94. [Google Scholar]
- [20].Monahan KC, Rhew IC, Hawkins JD, Brown EC. Adolescent pathways to co-occurring problem behavior: The effects of peer delinquency and peer substance use. J Res Adolesc 2014;24:630–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].National Center on Addiction and Substance Abuse. Trends in substance use and treatment needs among inmates Final Report to the National Institute of Justice; New York, NY, 2002. [Google Scholar]
- [22].Eaton DK, Kann L, Kinchen S, et al. Youth risk behavior surveillance—United States, 2011. Morbid Mortal Week Rep: Surveill Summ 2012;61:1–162. [PubMed] [Google Scholar]
- [23].Spurrier M, Blaszczynski A. Risk perception in gambling: A systematic review. J Gambl Stud 2014;30:253–76. [DOI] [PubMed] [Google Scholar]
- [24].Lindberg LD, Boggess S, Williams S. Multiple threats: The co-occurrence of teen health risk behaviors 2000. [Google Scholar]
- [25].Begle AM, Hanson RF, Danielson CK, et al. Longitudinal pathways of victimization, substance use, and delinquency: Findings from the National Survey of Adolescents. Addict Behav 2011;36:682–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Kilpatrick DG, Ruggiero KJ, Acierno R, et al. Violence and risk of PTSD, major depression, substance abuse/dependence, and comorbidity: Results from the National Survey of Adolescents. J Consult Clin Psychol 2003;71:692. [DOI] [PubMed] [Google Scholar]
- [27].McCauley JL, Danielson CK, Amstadter AB, et al. The role of traumatic event history in non-medical use of prescription drugs among a nationally representative sample of US adolescents. J Child Psychol Psychiatry 2010;51:84–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Graham JW, Olchowski AE, Gilreath TD. How many imputations are really needed? Some practical clarifications of multiple imputation theory. Prev Sci 2007;8:206–13. [DOI] [PubMed] [Google Scholar]
- [29].Cole DA, Maxwell SE. Testing mediational models with longitudinal data: Questions and tips in the use of structural equation modeling. J Abnorm Psychol 2003;112:558. [DOI] [PubMed] [Google Scholar]
- [30].Risser HJ, Hetzel-Riggin MD, Thomsen CJ, McCanne TR. PTSD as a mediator of sexual revictimization: The role of reexperiencing, avoidance, and arousal symptoms. J Trauma Stress 2006;19:687–98. [DOI] [PubMed] [Google Scholar]
- [31].Keeter S, Miller C, Kohut A, et al. Consequences of reducing nonresponse in a national telephone survey. Public Opin Q 2000;64:125–48. [DOI] [PubMed] [Google Scholar]