

Abstract
Background
Allergic rhinitis is a common condition affecting both adults and children. Patients experience symptoms of nasal obstruction, rhinorrhoea, sneezing and nasal itching, which may affect their quality of life.
Nasal irrigation with saline (salty water), also known as nasal douching, washing or lavage, is a procedure that rinses the nasal cavity with isotonic or hypertonic saline solutions. It can be performed with low positive pressure from a spray, pump or squirt bottle, with a nebuliser or with gravity‐based pressure in which the person instils saline into one nostril and allows it to drain out of the other. Saline solutions are available over the counter and can be used alone or as an adjunct to other therapies.
Objectives
To evaluate the effects of nasal saline irrigation in people with allergic rhinitis.
Search methods
The Cochrane ENT Information Specialist searched the ENT Trials Register; CENTRAL; Ovid MEDLINE; Ovid Embase; CINAHL; Web of Science; ClinicalTrials.gov; ICTRP and additional sources for published and unpublished trials. The date of the search was 23 November 2017.
Selection criteria
Randomised controlled trials (RCTs) comparing nasal saline irrigation, delivered by any means and with any volume, tonicity and alkalinity, with (a) no nasal saline irrigation or (b) other pharmacological treatments in adults and children with allergic rhinitis. We included studies comparing nasal saline versus no saline, where all participants also received pharmacological treatment (intranasal corticosteroids or oral antihistamines).
Data collection and analysis
We used the standard methodological procedures expected by Cochrane. Primary outcomes were patient‐reported disease severity and a common adverse effect ‐ epistaxis. Secondary outcomes were disease‐specific health‐related quality of life (HRQL), individual symptom scores, general HRQL, the adverse effects of local irritation or discomfort, ear symptoms (pain or pressure) and nasal endoscopy scores. We used GRADE to assess the quality of the evidence for each outcome; this is indicated in italics.
Main results
We included 14 studies (747 participants). The studies included children (seven studies, 499 participants) and adults (seven studies, 248 participants). No studies reported outcomes beyond three months follow‐up. Saline volumes ranged from 'very low' to 'high' volume. Where stated, studies used either hypertonic or isotonic saline solution.
Nasal saline versus no saline treatment
All seven studies (112 adults; 332 children) evaluating this comparison used different scoring systems for patient‐reported disease severity, so we pooled the data using the standardised mean difference (SMD). Saline irrigation may improve patient‐reported disease severity compared with no saline at up to four weeks (SMD ‐1.32, 95% confidence interval (CI) ‐1.84 to ‐0.81; 407 participants; 6 studies; low quality) and between four weeks and three months (SMD ‐1.44, 95% CI ‐2.39 to ‐0.48; 167 participants; 5 studies; low quality). Although the evidence was low quality the SMD values at both time points are considered large effect sizes. Subgroup analysis showed the improvement in both adults and children. Subgroup analyses for volume and tonicity were inconclusive due to heterogeneity.
Two studies reported methods for recording adverse effects and five studies mentioned them. Two studies (240 children) reported no adverse effects (epistaxis or local discomfort) in either group and three only reported no adverse effects in the saline group.
One study (48 children) reported disease‐specific HRQL using a modified RCQ‐36 scale. It was uncertain whether there was a difference between the groups at any of the specified time points (very low quality). No other secondary outcomes were reported.
Nasal saline versus no saline with adjuvant use of intranasal steroids or oral antihistamines
Three studies (40 adults; 79 children) compared saline with intranasal steroids versus intranasal steroids alone; one study (14 adults) compared saline with oral antihistamines versus oral antihistamines alone. It is uncertain if there is a difference in patient‐reported disease severity at up to four weeks (SMD ‐0.60, 95% CI ‐1.34 to 0.15; 32 participants; 2 studies; very low quality) or from four weeks to three months (SMD ‐0.32, 95% CI ‐0.85 to 0.21; 58 participants; 2 studies; very low quality). Although none of the studies reported methods for recording adverse effects, three mentioned them: one study (40 adults; adjuvant intranasal steroids) reported no adverse effects (epistaxis or local discomfort) in either group; the other two only reported no adverse effects in the saline group.
It is uncertain if saline irrigation in addition to pharmacological treatment improved disease‐specific HRQL at four weeks to three months, compared with pharmacological treatment alone (SMD ‐1.26, 95% CI ‐2.47 to ‐0.05; 54 participants; 2 studies; very low quality). No other secondary outcomes were reported.
Nasal saline versus intranasal steroids
It is uncertain if there was a difference in patient‐reported disease severity between nasal saline and intranasal steroids at up to four weeks (MD 1.06, 95% CI ‐1.65 to 3.77; 14 participants; 1 study), or between four weeks and three months (SMD 1.26, 95% CI ‐0.92 to 3.43; 97 participants; 3 studies), or indisease‐specific HRQL between four weeks and three months (SMD 0.01, 95% CI ‐0.73 to 0.75; 83 participants; 2 studies). Only one study reported methods for recording adverse effects although three studies mentioned them. One (21 participants) reported two withdrawals due to adverse effects but did not describe these or state which group. Three studies reported no adverse effects (epistaxis or local discomfort) with saline, although one study reported that 27% of participants experienced local discomfort with steroid use. No other secondary outcomes were reported.
Authors' conclusions
Saline irrigation may reduce patient‐reported disease severity compared with no saline irrigation at up to three months in both adults and children with allergic rhinitis, with no reported adverse effects. No data were available for any outcomes beyond three months. The overall quality of evidence was low or very low. The included studies were generally small and used a range of different outcome measures to report disease severity scores, with unclear validation. This review did not include direct comparisons of saline types (e.g. different volume, tonicity).
Since saline irrigation could provide a cheap, safe and acceptable alternative to intranasal steroids and antihistamines further high‐quality, adequately powered research in this area is warranted.
Plain language summary
Nasal saline for allergic rhinitis
Background
Allergic rhinitis is inflammation (swelling and/or irritation) of the inside of the nose caused by allergies. It is common in both children and adults. Allergic rhinitis can be intermittent (fewer than four days per week, or four weeks per year) or persistent (more than four days per week, or four weeks per year). The allergy can be caused by many different things but common allergens (things causing allergy) are: grass or tree pollen, mould, dust mites or animal dander (tiny flakes of skin). People with allergic rhinitis experience symptoms (nasal obstruction, runny nose, nasal itching and sneezing) that may affect their quality of life.
Nasal saline irrigation (also known as nasal douche, wash or lavage) is a procedure that rinses the nasal cavity with saline (salt water) solutions. How saline works is not fully understood but it is probably through making the mucus (snot) thinner, making it easier to remove and also removing some of the allergens from the nose that cause irritation. Nasal saline irrigation can be performed with sprays, pumps or squirt bottles. Saline solutions can be isotonic (the same concentration of salt that is found in the body ‐ 0.9% NaCl) or hypertonic (more salty than found in the body ‐ more than 0.9% NaCl). Although saline irrigation is thought to be safe there have been reports of epistaxis (nosebleeds) and irritation or discomfort in the nose and ears. This therapy is available without prescription and can be used alone or as an add‐on to other pharmacological treatment for allergic rhinitis, such as intranasal (in the nose) steroids and oral antihistamines).
Search date
The evidence is up to date to November 2017.
Study characteristics
We found 14 studies with a total of 747 participants (260 adults; 487 children). The volume of saline used in the studies varied: five studies used 'very low' volumes (nasal sprays providing less than 5 mL saline per nostril per application), two studies used low‐volume (between 5 and 59 mL saline per nostril per application introduced with a syringe) and four studies used high‐volume solutions (more than 60 mL per nostril per application). Eight studies used hypertonic saline, five used isotonic saline and three studies did not provide this information. Two studies used two different types of saline solutions.
Study funding sources
Seven studies did not say how they were funded. The other seven were funded either by the investigators' department or research grants from regional or national government. No studies were funded by pharmaceutical companies.
Key results
Nasal saline irrigation compared with no saline irrigation
Nasal saline irrigation may have benefits in both adults and children in relieving the symptoms of allergic rhinitis compared to no saline irrigation and it is unlikely to be associated with adverse effects. It is not possible to tell from this review whether there is a difference between the different volumes and concentrations of saline solution.
Adding nasal saline irrigation onto 'pharmacological' allergic rhinitis treatment
It is uncertain whether adding nasal saline irrigation to pharmacological treatment (intranasal steroids or oral antihistamines) helps to improve the symptoms of allergic rhinitis compared to using pharmacological treatments alone. The use of nasal saline irrigation is unlikely to be associated with adverse effects.
Nasal saline irrigation compared to 'pharmacological' allergic rhinitis treatment
There is not enough evidence to know whether nasal saline irrigation is better, worse or the same as using intranasal steroids. No studies reporting the outcomes we were interested in compared nasal saline irrigation with oral antihistamines.
Quality of evidence
The overall quality of evidence for nasal saline irrigation compared with no saline treatment was eitherlow quality (our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect) or very low quality (we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect). This was because the studies were mostly very small and used different methods to measure the same outcome. Since saline irrigation could provide a cheap, safe and acceptable alternative to intranasal steroids and antihistamines further high‐quality studies are needed.
Summary of findings
Summary of findings for the main comparison. Saline versus no saline treatment for allergic rhinitis.
| Saline versus no saline treatment for allergic rhinitis | ||||||
|
Patient or population: allergic rhinitis Setting: secondary care Intervention: saline Comparison: no saline treatment | ||||||
| Outcomes | Relative effect (95% CI) | Anticipated absolute effects* (95% CI) | Certainty of the evidence (GRADE) | What happens | ||
| Without saline | With saline | Difference | ||||
| Disease severity score (up to 4 weeks) Assessed with: various instruments Follow‐up: range 1 week to 4 weeks № of participants: 407 (322 children; 85 adults) (6 RCTs) 2 |
— | — | — | SMD 1.32 lower (1.84 lower to 0.81 lower) | ⊕⊕⊝⊝ LOW 1 | Saline irrigation may improve the patient‐reported disease severity compared with no saline treatment in both children and adults. The mean difference in disease severity score was 1.32 standard deviations lower (1.84 to 0.81 lower) with saline compared to no saline. This translates into a decrease of approximately 1.97 points (1.21 to 2.74) on a 0‐ to 10‐point VAS for nasal symptoms (lower = better). |
| Disease severity score (4 weeks to 6 months) Assessed with: various instruments Follow‐up: range 6 weeks to 8 weeks № of participants: 167 (102 children; 65 adults) (5 RCTs) 2 |
— | — | — | SMD 1.44 lower (2.39 lower to 0.48 lower) | ⊕⊕⊝⊝ LOW 1 | Saline irrigation may improve the patient‐reported disease severity compared with no saline treatment in both children and adults. The mean difference in disease severity score was 1.44 standard deviations lower (2.39 to 0.489 lower) with saline compared to no saline. This translates into a decrease of approximately 2.98 points (0.99 to 5.98) on a 0‐ to 10‐point VAS for nasal symptoms (lower = better). |
| Individual symptom scores ‐ not measured | — | — | No studies measured this outcome. | |||
| Epistaxis Follow‐up: range 4 weeks to 6 weeks № of participants: 240 (all children) (2 RCTs) | Not pooled | Study population | ⊕⊕⊝⊝ LOW 3 | 2 studies (240 children) reported no adverse effects in either arm. Both studies included only children. | ||
| 0% | Not pooled | Not pooled | ||||
| Disease‐specific HRQL Assessed with: RCQ‐36 quality of life questionnaire Scale from: 0 to 140, lower = better Follow‐up: 4 weeks № of participants: 42 (all children) (1 RCT) |
— | The mean disease specific HRQL ‐ Up to 4 weeks without saline was 19.26 | — | MD 3.32 lower (11.35 lower to 4.71 higher) | ⊕⊝⊝⊝ VERY LOW 4 | It is uncertain whether saline improves the disease‐specific quality of life at 4 weeks, compared with no saline, because the quality of the evidence is very low. The study included only children. |
| Disease‐specific HRQL ‐ 4 weeks to 6 months Assessed with: RCQ‐36 Scale from: 0 to 140 follow‐up: 6 weeks № of participants: 42 (all children) (1 RCT) | — | The mean disease specific HRQL ‐ 4 weeks to 6 months without saline was 15.94 | — | MD 2.06 lower (8.38 lower to 4.26 higher) | ⊕⊝⊝⊝ VERY LOW 4 | It is uncertain whether saline improves the disease‐specific quality of life at 6 weeks, compared with no saline, because the quality of the evidence is very low. The study included only children. |
| Other adverse effects: local irritation Follow‐up: range 4 weeks to 6 weeks № of participants: 240 (all children) (2 RCTs) | Not pooled | Study population | ⊕⊕⊝⊝ LOW 3 | 2 studies (240 children) reported no adverse effects in either arm. 3 further studies (68 children; 44 adults) reported no adverse effects in the saline arm. There is no information for the control arm. | ||
| 0% | Not pooled | Not pooled | ||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; HRQL: health‐related quality of life; MD: mean difference; RCQ‐36: Thai rhinoconjunctivitis quality of life scale; RCT: randomised controlled trial; SMD: standardised mean difference; VAS: visual analogue scale | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1Low‐quality evidence. Downgraded by one level due to risk of bias (all of the studies used different scales for which the validation is unknown). Downgraded by one level due to inconsistency (there is statistical heterogeneity within the results possibly due to the variations in tonicity, volume and method of application of saline used).
2Different instruments were used to assess the disease severity score. A summary of these can be found in Table 4.
3Low‐quality evidence. Downgraded by two levels due to risk of bias (the reporting of the adverse outcomes was very poor and it was unclear whether the adverse effects were systematically sought).
4Very low‐quality evidence. Downgraded by two levels for risk of bias (results came from one study using an instrument for which the validation status is unknown with a high risk of performance and detection bias). Downgraded by one level for imprecision (the results are imprecise due to the small sample size and the confidence intervals are very wide).
Summary of findings 2. Saline irrigation plus pharmacological treatment versus pharmacological treatment alone for allergic rhinitis.
| Nasal saline plus pharmacological treatment versus pharmacological treatment alone for allergic rhinitis | ||||||
|
Patient or population: allergic rhinitis Setting: secondary care Intervention: saline plus pharmacological treatment (intranasal steroids or oral antihistamines) Comparison: pharmacological treatment alone | ||||||
| Outcomes | Relative effect (95% CI) | Anticipated absolute effects* (95% CI) | Certainty of the evidence (GRADE) | What happens | ||
| Without saline | With saline | Difference | ||||
| Disease severity score (up to 4 weeks) Assessed with: various instruments used Follow‐up: 4 weeks № of participants: 32 (18 children; 14 adults) (2 RCTs)1 |
— | — | — | SMD 0.6 lower (1.34 lower to 0.15 higher) |
⊕⊝⊝⊝ VERY LOW 2 | It is uncertain whether saline in addition to pharmacological treatment (antihistamines or steroids) improves patient‐reported severity scores at 4 weeks, compared with pharmacological treatment alone. |
| Disease severity score (4 weeks to 6 months) Assessed with: various instruments used Follow‐up: 3 months № of participants: 58 (18 children; 40 adults) (2 RCTs) 1 | — | — | — | SMD 0.32 lower (0.85 lower to 0.21 higher) |
⊕⊝⊝⊝ VERY LOW 2 | It is uncertain whether saline in addition to pharmacological treatment (antihistamines or steroids) improves patient‐reported severity scores at 3 months, compared with pharmacological treatment alone. |
| Individual symptom scores ‐ not measured | — | — | No studies measured this outcome. | |||
| Adverse effects ‐ epistaxis № of participants: 58 (2 RCTs) (18 children; 40 adults) |
Three studies made statements about adverse effects. One study (40 adults) indicated that "all [treatments were] tolerated well, none [of the participants] had adverse events" (Wu 2014) and the other two studies (62 children) reported that nasal irrigation with saline was well accepted in all patients and no adverse effect was reported with the use of saline (Li 2009). | ⊕⊝⊝⊝ VERY LOW 3 | It is uncertain whether there is a difference in adverse effects between the groups. None of the studies specifically mentioned epistaxis as an adverse effect. | |||
| Health‐related quality of life (4 weeks to 6 months) Assessed with: various instruments № of participants: 54 (all adults) (2 RCTs)4 |
— | — | — | SMD 1.26 lower (2.47 lower to 0.05 lower) |
⊕⊝⊝⊝ VERY LOW 5 | It is uncertain whether saline in addition to pharmacological treatment (antihistamines or steroids) improves health‐related quality of life at 4 weeks to 6 months, compared with pharmacological treatment alone. |
| Other adverse effects: local irritation Follow‐up: range 4 weeks to 6 weeks № of participants: 58 (18 children;40 adults) (2 RCTs) | None of the studies specifically mentioned local irritation as an adverse effect. Two studies made statements about adverse effects. One study (40 adults) indicated that "all [treatments were] tolerated well, none [of the participants] had adverse events" (Wu 2014) and the other (18 children) that "Nasal irrigation with saline was well accepted in all patients and no adverse effect was reported” (Li 2009). | ⊕⊝⊝⊝ VERY LOW 3 | It is uncertain whether there is a difference in adverse effects between the groups as no adverse effects were reported. | |||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; RCT: randomised controlled trial; SMD: standardised mean difference | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1Different instruments were used to assess the disease severity score. A summary of these can be found in Table 4.
2 Very low‐quality evidence. Downgraded by two levels due to risk of bias (studies were generally poorly conducted with a high risk of bias; the validation status of the symptom severity scores used is unknown). Downgraded by one level due to imprecision (the results are imprecise with small sample sizes and wide confidence intervals).
3Very low‐quality evidence. Downgraded by two levels due to risk of bias (studies were generally poorly conducted with a high risk of bias and it is unclear whether adverse effects were systemically reported). Downgraded by one level due to imprecision (very small sample size).
4Rogkakou 2005 used the 'Global Impact' score for the Rhinasthma quality of life instrument. Wu 2014 used the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) but the range of possible scores is not reported.
5Very low‐quality evidence. Downgraded by two levels due to risk of bias (studies were generally poorly conducted with a high risk of bias; it is unclear whether the instruments used were validated and the scale in one remains unknown). Downgraded by one level due to inconsistency (there is significant statistical heterogeneity between the results). Downgraded by one level due to imprecision (sample size is very small and so the confidence intervals are very wide).
Background
Description of the condition
According to the Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines (ARIA 2008), allergic rhinitis is defined clinically by nasal hypersensitivity symptoms induced by an immunologically mediated (most often IgE‐dependent) inflammation of the nasal mucous membranes after exposure to an offending allergen. Common allergic triggers include house dust mites, pollens (from trees, grasses, shrubs and weeds), animal dander or fungi, which occur naturally in the environment. In addition, allergic rhinitis can be caused by triggers to which a person is exposed in the course of their work (occupational exposure). These may include vegetable proteins, enzymes and chemicals (BSACI 2017).
Symptoms of allergic rhinitis may include nasal obstruction (blockage or congestion), rhinorrhoea (which can be anterior leading to nasal discharge, or posterior leading to post‐nasal drip), nasal itching and sneezing (ARIA 2008). In addition to nasal symptoms, some people with allergic rhinitis also report eye symptoms (watering, redness, itching) and ear symptoms such as pain, pressure or feeling of fullness; however, aural (ear) symptoms have also been reported as an adverse effect of nasal saline irrigation (Chusakul 2013). There is evidence that people with allergic rhinitis may experience decreased quality of life due to issues such as loss of sleep, secondary daytime fatigue, impaired school and work performance, decreased cognitive functioning and decreased long‐term productivity (Schoenwetter 2004).
Allergic rhinitis is commonly classified into 'intermittent' and 'persistent' disease. Intermittent allergic rhinitis is diagnosed when symptoms are present for less than four days per week or for less than four weeks. Persistent allergic rhinitis is diagnosed when symptoms are present more frequently than four days per week and for at least four consecutive weeks (ARIA 2008). The presence of intermittent or persistent disease may be related to the type of allergic triggers for allergic rhinitis, for example intermittent allergic rhinitis may be linked to the release of a certain type of tree pollen (such as elm tree pollen) occurring once a year for a period of a few weeks.
Prior to 2001, allergic rhinitis was classified into 'seasonal', 'perennial' and 'occupational', based on the time of exposure. Seasonal allergic rhinitis was used to define mainly 'outdoor' allergens such as tree pollens, which were not present consistently throughout the year, whereas the term 'perennial' allergic rhinitis was used for 'indoor' allergens where exposure was thought to be consistent throughout the year. The ARIA 2001 guidelines attempted to make the classification more useful in the real world by introducing the terms 'intermittent' and 'persistent' to classify the disease. The previous classification had been felt to be inadequate as it was noted that in certain situations a seasonal allergen may occur year round (e.g. grass pollen allergy in Southern California) or symptoms of perennial allergy may not always be present all year round (e.g. in the Mediterranean area where levels of house dust mite allergen are low in the summer). Thus the change to intermittent and persistent was made (ARIA 2001).
The ARIA guidelines further classify allergic rhinitis into 'mild' and 'moderate/severe' depending on the person's severity of symptoms and the impact of the condition on their quality of life. Moderate/severe allergic rhinitis is diagnosed when one or more of the following items are present: sleep disturbance; impairment of daily activities, leisure or sport; impairment of school or work; or troublesome symptoms (ARIA 2008).
The diagnosis of allergic rhinitis is based upon clinical symptoms combined with laboratory studies demonstrating the presence of allergen‐specific IgE in the skin (skin prick test) or blood (serum IgE). A review of epidemiological studies estimated that 10% to 15% of adults have allergic rhinitis based on both the presence of symptoms and a positive skin prick test (Mims 2014). However, the number is higher when people reporting either just symptoms (up to 34%) or a positive skin prick test (up to 53.9%, testing 10 allergens) are considered (Mims 2014). There are a wide range of estimates for the prevalence of allergic rhinitis in children (10% to 40%). These differences in estimates may be attributable to both the geographical location of the study, the method of diagnosis used (whether a skin prick test was completed or whether the diagnosis was based on symptoms), or both (Mims 2014).
Traditionally there has appeared to be a higher prevalence of allergic rhinitis in countries with a 'western lifestyle' (USA and Europe), where reported prevalence rates vary between 10% and 30% (ARIA 2008). For areas outside these regions, Katelaris et al completed a review of global prevalence studies, which identified a great diversity in the prevalence estimates of allergic rhinitis both between and within countries (Katelaris 2012). The review concluded that "the prevalence of allergic rhinitis is increasing and its adverse impact on the quality of life of affected individuals is increasingly recognised" (Katelaris 2012). The increase in prevalence has been hypothesised as being due to increasing urbanisation and modification of lifestyles, which has led to reduced exposure to environmental allergens during early childhood resulting in a weaker immune system and consequent development of allergies, commonly known as the 'hygiene hypothesis' (ARIA 2008).
There is a well‐established link between allergic rhinitis and asthma. A literature review identified that 40% of patients with allergic rhinitis had asthma (Kim 2008). The proportion of patients with asthma reporting symptoms of allergic rhinitis ranged from 30% to 80%. This connection is perhaps unsurprising as both allergic rhinitis and asthma are based on shared physiological immune responses to an identified foreign substance (allergen) (Kim 2008).
Treatment options for allergic rhinitis include allergen avoidance, pharmacological therapy and immunotherapy. Pharmacological therapies include various classes of medications, including antihistamines, intranasal corticosteroids and anti‐leukotrienes (ARIA 2008). Nasal saline has been used as a 'natural' remedy for centuries and recent Cochrane Reviews have evaluated its efficacy as a potential treatment or adjunct to pharmacological treatment for chronic rhinosinusitis and upper respiratory tract infections (Chong 2016; King 2015).
Description of the intervention
Saline can be deposited in the nasal cavity in various forms, including sprays, drops, nebulisers and irrigations. The volume of nasal saline from sprays and nebulisers can vary greatly. These can be very low‐volume devices (< 5 mL per nostril) through to squeeze bottles and Neti pots, which are usually high‐volume devices (> 60 mL). While nasal saline sprays reach the nasal cavity adequately, there is some evidence to suggest that high pressure and volume saline is more effective in penetrating the adjacent sinus cavities (Wormald 2004).
The saline solutions available are hypotonic (with a concentration of less than 0.9% NaCl), physiologic (with a concentration of 0.9% NaCl) and hypertonic (with a concentration of greater than 0.9% NaCl). There is some evidence in other conditions that the tonicity of the saline solution alters its efficacy (Berjis 2011; Rabago 2005). In addition, the pH of saline solutions has been investigated and there is some evidence that solutions buffered with sodium bicarbonate (increased alkalinity) may have an impact on the nasal symptoms of people with allergic rhinitis (Chusakul 2013).
How the intervention might work
The physiological mechanisms underlying any benefit of the use of nasal saline are not fully understood but it is commonly proposed that the primary mechanism of action is mechanical (Barham 2015). This may include clearance of mucus (saline thins mucus and helps to clear it out) (Elkins 2011), and removal of airborne allergens and inflammation mediators such as histamine (Georgitis 1994). There is some evidence to suggest that at some concentrations nasal saline may improve ciliary beat function (Bonnomet 2016) and mucociliary function (Hermelingmeier 2012). Adverse effects of nasal saline irrigation are thought to be rare and generally mild but may include ear fullness, stinging of the nasal mucosa and epistaxis (nosebleed) (Khianey 2012).
Why it is important to do this review
Allergic rhinitis is a highly prevalent condition in adults and children, with a large impact on patients and high healthcare costs: both direct, from the cost of repeat healthcare visits and of chronic medical therapy, and indirect, via absenteeism and lost productivity (Schoenwetter 2004).
Previous Cochrane Reviews have demonstrated some possible benefit of saline in adults with chronic rhinosinusitis (Chong 2016) and in people with upper respiratory tract infections (King 2015). The two most recent systematic reviews identified on the use of nasal saline in allergic rhinitis had latest search dates of 2010 (Hermelingmeier 2012) and December 2011 (Khianey 2012). Khianey 2012 limited their inclusion criteria to studies published in English and also included studies in populations with a range of different sinonasal conditions including upper respiratory tract infection and chronic rhinosinusitis. Hermelingmeier 2012 specified the population as people with seasonal or perennial allergic rhinitis. This review looked at prospective trials (including before and after studies) and only included studies published in English or German. Both reviews identified potential benefits for people in terms of symptom improvement and found that saline irrigation was well tolerated, but both reviews highlighted the need for further research in this area in order for definitive conclusions to be drawn. This review will include recently published studies and we will apply no restriction with regard to language of publication.
Objectives
To evaluate the effects of nasal saline irrigation in people with allergic rhinitis.
Methods
Criteria for considering studies for this review
Types of studies
We included studies with the following design characteristics:
randomised controlled trials, including cluster‐randomised trials and quasi‐randomised trials, and cross‐over trials if the data from the first phase were available;
participants were followed up for at least two weeks.
We excluded studies with the following design characteristics:
randomised participants by side of nose (within‐patient controlled) because it is difficult to ensure that the effects of any of the interventions considered can be localised; or
perioperative studies, where the sole purpose of the study was to investigate the effect of nasal saline irrigation on surgical outcomes.
Types of participants
Patients (adults and children) with clinical symptoms characteristic of allergic rhinitis with a positive radioallergosorbent test (RAST) or skin prick test (SPT).
We excluded studies that included a majority (more than 50%) of participants with:
non‐allergic rhinitis;
chronic rhinosinusitis;
acute sinusitis;
cystic fibrosis;
immunotherapy started within the prior year;
any alteration of allergic rhinitis‐specific pharmacotherapy (antihistamines, intranasal corticosteroids, anti‐leukotrienes) during the trial;
aspirin‐exacerbated respiratory disease;
surgery for turbinate reduction within three months prior to study.
Had we found a study that included a mixed group of participants, we would have excluded it if more than 50% of the participants met the 'excluded' population criteria above, unless the study reported the results for the different populations separately. Similarly, if there had been a study where more than 50% of the people had allergic rhinitis we would have included the study but, where possible, we would only have used the results for the population with allergic rhinitis providing the randomisation had been stratified.
Types of interventions
The use of saline, as an active treatment, delivered to the nose by any means (douche, irrigation, pulsed, spray or nebuliser).
Tonicity: we included all concentrations of saline. 'Hypotonic' was defined as a concentration of less than 0.9% NaCl, 'physiologic' as 0.9% NaCl and 'hypertonic' as greater than 0.9% NaCl.
Volume: we included all volumes of saline treatments. 'Very low‐volume' related to misting sprays or other delivery methods where the volume of application is likely to be less than 5 mL per nostril per application. 'Low‐volume' was defined as between 5 mL and 59 mL per nostril per application. 'High‐volume' was defined as a volume of 60 mL or greater per nostril per application.
We included studies investigating 'buffered' saline solutions where the aim was to adjust the pH of the solution. We excluded studies that used formulations of saline solution that contained other additives, such as xylitol, antibacterials and surfactants. We also excluded studies using other formulations, such as lactated Ringer's solution.
There was no minimum duration of treatment.
Comparisons
The main comparison pairs were:
nasal saline versus no saline irrigation;
nasal saline plus pharmacological treatment versus pharmacological treatment alone.
Other possible comparison pairs included:
nasal saline versus pharmacological treatment.
The term 'pharmacological treatment' refers to commonly accepted treatments for allergic rhinitis such as oral antihistamines and intranasal corticosteroids, as recommended by internationally accepted treatment guidelines, such as the ARIA guidelines (ARIA 2008).
Types of outcome measures
We analysed the following outcomes in the review, but we did not use them as a basis for including or excluding studies.
Primary outcomes
Disease severity, as measured by patient‐reported symptom score (such as the Total Nasal Symptom Score (TNSS) questionnaire and visual analogue scales (VAS)).
Significant local adverse effects: epistaxis.
Secondary outcomes
Disease‐specific health‐related quality of life, using validated disease‐specific health‐related quality of life scores, such as the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ), Mini Rhinoconjunctivitis Quality of Life Questionnaire (MiniRQLQ) and Rhinitis Symptom Utility Index (RSUI).
-
Individual symptom scores for the following symptoms:
anterior rhinorrhoea (runny nose): where a study reports 'rhinorrhoea' as the outcome, in the absence of a definition within the paper we assumed that this measured anterior rhinorrhoea. Where the authors reported a combined outcome for anterior and posterior rhinorrhoea and we were not able to obtain individual results, we recorded this as a combined 'anterior and posterior rhinorrhoea' category;
posterior rhinorrhoea (post‐nasal drip);
nasal blockage or congestion or obstruction;
nasal itching;
sneezing.
Generic health‐related quality of life, using validated generic quality of life scores, such as the SF‐36, EQ‐5D and other well‐validated instruments.
Any other local adverse effects: local irritation, discomfort.
Aural symptoms: ear pain, pressure or feeling of fullness.
Endoscopic score (e.g. Lund‐Mackay/Lund‐Kennedy).
As both short‐term and long‐term effects are important we evaluated efficacy outcomes at the following time points:
up to four weeks from the start of treatment (particularly relevant for intermittent allergic rhinitis);
from four weeks to six months;
from six months to 12 months; and
at more than 12 months (particularly relevant for persistent allergic rhinitis).
Where a study reported data for an outcome at more than one time point, we included the data for the longest of each of the four time points above. For example, if a study reported outcomes at one week, three weeks and 12 weeks from the start of treatment, we used the three‐week results (for the up to four weeks time point) and the 12‐week results (for the four weeks to six months time point). We paid attention during the analysis to the prevention of 'double counting' of studies when presenting summary results.
For adverse effects, we analysed data from the longest time periods available.
Search methods for identification of studies
The Cochrane ENT Information Specialist conducted systematic searches for randomised controlled trials and controlled clinical trials. There were no language, publication year or publication status restrictions. The date of the search was 23 November 2017.
Electronic searches
The Information Specialist searched:
the Cochrane ENT Trials Register (searched via CRS Web 23 November 2017);
the Cochrane Register of Controlled Trials (CENTRAL) (searched via CRS Web 23 November 2017);
Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Ovid MEDLINE(R) Daily and Ovid MEDLINE(R) (1946 to 23 November 2017);
Ovid EMBASE (1974 to 23 November 2017);
Ovid CAB Abstracts (1910 to 23 November 2017);
EBSCO CINAHL (1982 to 23 November 2017);
Ovid AMED (1985 to 23 November 2017);
LILACS, lilacs.bvsalud.org (searched 23 November 2017);
KoreaMed (searched via Google Scholar 23 November 2017);
IndMed, www.indmed.nic.in (searched 23 November 2017);
PakMediNet, www.pakmedinet.com (searched 23 November 2017);
Web of Knowledge, Web of Science (1945 to 23 November 2017);
ClinicalTrials.gov (searched via the Cochrane Register of Studies 23 November 2017);
World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP), www.who.int/ictrp (searched 23 November 2017).
The Information Specialist modelled subject strategies for databases on the search strategy designed for CENTRAL. Where appropriate, they were combined with subject strategy adaptations of the highly sensitive search strategy designed by Cochrane for identifying randomised controlled trials and controlled clinical trials (as described in the Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0, Box 6.4.b. (Handbook 2011). Search strategies for major databases including CENTRAL are provided in Appendix 1.
Searching other resources
We scanned the reference lists of identified publications for additional trials and contacted trial authors where necessary. In addition, the Information Specialist searched Ovid MEDLINE and theCochrane Library to retrieve existing systematic reviews relevant to this systematic review, so that we could scan their reference lists for additional trials. The Information Specialist also ran non‐systematic searches of Google Scholar to retrieve grey literature and other sources of potential trials.
Data collection and analysis
Selection of studies
At least two review authors (KH, SG, KS, GS) independently screened all titles and abstracts of the studies obtained from the database searches to identify potentially relevant studies. Two review authors (KH, CP) evaluated the full text of each potentially relevant study to determine whether it met the inclusion and exclusion criteria for this review.
We resolved any differences by discussion and consensus, with the involvement of a third author for clinical and/methodological input had it been necessary.
Data extraction and management
Two review authors (KH and KS) independently extracted data from each study using a standardised data collection form (see Appendix 2). Whenever a study had more than one publication, we retrieved all publications to ensure complete extraction of data. Where there were discrepancies in the data extracted by different review authors, we checked these against the original reports and we resolved differences by discussion and consensus, with the involvement of a third author or a methodologist where necessary. We contacted the original study authors for clarification or for missing data whenever required. If we found differences between publications of a study, we contacted the original authors for clarification. We used data from the main paper(s) where no further information was found.
We included key characteristics of the studies, such as study design, setting, sample size, population and how outcomes were defined or collected in the studies. In addition, we also collected baseline information on prognostic factors or effect modifiers. For this review, this included:
age of participants;
intermittent or persistent allergic rhinitis;
type of allergic trigger (e.g. mites, pollens, animals, etc.);
severity of allergic rhinitis ('mild' or 'moderate/severe' as defined in ARIA 2008).
For the outcomes of interest to the review, we extracted the findings of the studies on an available case analysis basis; i.e. we included data from all participants available at the time points based on the treatment randomised whenever possible, irrespective of compliance or whether participants had received the treatment as planned.
In addition to extracting prespecified information about study characteristics and aspects of methodology relevant to risk of bias, we extracted the following summary statistics for each trial and each outcome:
For continuous data: the mean values, standard deviations and number of participants for each treatment group. Where endpoint data were not available, we extracted the values for change from baseline. We analysed data from measurement scales such as RQLQ as continuous data.
For binary data: the numbers of participants experiencing an effect and the number of participants assessed at the time point.
For ordinal scale data: if the data appeared to be approximately normally distributed or if the analysis that the investigators performed suggested parametric tests were appropriate, then we treated the outcome measures as continuous data. If data had been available, we would have converted into binary data.
We prespecified the time points of interest for the outcomes in this review (Types of outcome measures). While studies had reported data at multiple time points, we only extracted the longest available data within the time points of interest. For example, if a study reported data at one, two and four weeks, we only extracted and analysed the data for the four‐week follow‐up.
Extracting data from figures
Where values for primary or secondary outcomes were shown as figures within the paper we contacted the study authors to try to obtain the raw values. When the raw values were not provided, we extracted information from the graphs using an online data extraction tool (http://arohatgi.info/WebPlotDigitizer/app/), using the best quality version of the relevant figures available.
Assessment of risk of bias in included studies
KH and KS undertook assessment of the risk of bias of the included studies independently, with the following taken into consideration, as guided by theCochrane Handbook for Systematic Reviews of Interventions (Handbook 2011):
sequence generation;
allocation concealment;
blinding;
incomplete outcome data;
selective outcome reporting; and
other sources of bias.
We used the Cochrane 'Risk of bias' tool in RevMan 5.3 (RevMan 2014), which involves describing each of these domains as reported in the trial and then assigning a judgement about the adequacy of each entry: 'low', 'high' or 'unclear' risk of bias.
Measures of treatment effect
We summarised the effects of dichotomous outcomes (e.g. proportion of participants with symptom resolution) as risk ratios (RR) with 95% confidence intervals (CIs). For the key outcomes that were presented in the 'Summary of findings' tables, we also expressed the results as absolute numbers based on the pooled results and compared to the assumed risk. We would have calculated the number needed to treat to benefit (NNTB) using the pooled results had it made sense to do so. The assumed baseline risk would typically be either (a) the median of the risks of the control groups in the included studies, this being used to represent a 'medium‐risk population' or, alternatively, (b) the average risk of the control groups in the included studies used to represent the 'study population' (Handbook 2011). Had a large number of studies been available, and where appropriate, we would have also presented additional data based on the assumed baseline risk in (c) a low‐risk population and (d) a high‐risk population.
For continuous outcomes, we expressed treatment effects as a mean difference (MD) with standard deviation (SD). When different scales were used to measure the same outcome we used the standardised mean difference (SMD), and we provided a clinical interpretation of the SMD values.
Unit of analysis issues
This review did not use data from phase II of cross‐over studies or from studies where the participant was not the unit of randomisation, i.e. studies where the side of the nose (right versus left) was randomised.
If we had found cluster‐randomised trials, we would have analysed these according to the methods in section 16.3.3 of the Cochrane Handbook for Systematic Reviews of Interventions (Handbook 2011).
Dealing with missing data
We contacted study authors via email whenever the outcome of interest was not reported if the methods of the study suggest that the outcome had been measured. We did the same if not all data required for meta‐analysis were reported, unless the missing data were standard deviations. When standard deviation data were not available we approximated these using the standard estimation methods from P values, standard errors or 95% CIs if these were reported, as detailed in the Cochrane Handbook for Systematic Reviews of Interventions (Handbook 2011). Had it been impossible to estimate these, we would have contacted the study authors.
Apart from imputations for missing standard deviations, we did not conduct any other imputations. We extracted and analysed data for all outcomes using the available case analysis method.
Assessment of heterogeneity
We assessed clinical heterogeneity (which may be present even in the absence of statistical heterogeneity) by examining the included trials for potential differences between studies in the types of participants recruited (including age of participants), interventions or controls used and the outcomes measured.
We assessed statistical heterogeneity by visually inspecting the forest plots and by considering the Chi² test (with a significance level set at P < 0.10) and the I² statistic, which calculates the percentage of variability that is due to heterogeneity rather than chance, with I² values over 50% suggesting substantial heterogeneity (Handbook 2011).
Assessment of reporting biases
We assessed reporting bias as between‐study publication bias and within‐study outcome reporting bias.
Outcome reporting bias (within‐study reporting bias)
We assessed within‐study reporting bias by comparing the outcomes reported in the published report against the study protocol, whenever this could be obtained. If the protocol was not available, we compared the outcomes reported to those listed in the methods section. If results are mentioned but not reported adequately in a way that allows analysis (e.g. the report only mentions whether the results were statistically significant or not), bias in a meta‐analysis is likely to occur. We tried to find further information from the study authors. If no further information was obtained, we noted this as being a 'high' risk of bias. Where there was insufficient information to judge the risk of bias we noted this as an 'unclear' risk of bias (Handbook 2011).
Publication bias (between‐study reporting bias)
We had planned to create funnel plots if sufficient studies (more than 10) were available for an outcome. If we had observed asymmetry of the funnel plot, we had planned to conduct more formal investigation using the methods proposed by Egger 1997.
Data synthesis
We conducted all meta‐analyses using Review Manager 5.3 (RevMan 2014). For dichotomous data, we analysed treatment differences as a risk ratio (RR) calculated using the Mantel‐Haenszel methods. We would have analysed time‐to‐event data using the generic inverse variance method.
For continuous outcomes, if all the data were from the same scale, we pooled mean values obtained at follow‐up with the change in outcomes (i.e. difference between pre‐ versus post‐treatment values) and reported this as a MD. However, if the SMD had to be used as an effect measure, we would not have pooled change and endpoint data.
When statistical heterogeneity is low, random‐effects versus fixed‐effect methods yield trivial differences in treatment effects. However, when statistical heterogeneity is high, the random‐effects method provides a more conservative estimate of the difference.
Subgroup analysis and investigation of heterogeneity
Where data were available, we conducted some subgroup analyses regardless of whether statistical heterogeneity was observed, as these were widely suspected to be potential effect modifiers. For this review, this included the following.
Volume of saline delivery (e.g. 'very low', 'low' and 'high' volume). There is evidence of a difference in effectiveness between high‐ and low‐volume saline irrigation in people with chronic sinonasal symptoms (Pynnonen 2007).
Tonicity of saline solution (hypertonic, isotonic and hypotonic solutions). There is some evidence in other conditions that tonicity may have an effect on the efficacy of nasal saline (Berjis 2011; Rabago 2005).
Alkalinity of saline solution. There is evidence that increased alkalinity of the saline solution improves some nasal symptoms (Chusakul 2013).
Participant age (children, adults or mixed population). There may be differences in physiology that are unknown and compliance and volumes may well be quite different in the paediatric population compared to adults.
We initially planned to present the main analyses of this review according to the volume of saline delivery, however we changed this to present the initial analyses subgrouped by age during the process of the review (Differences between protocol and review). We presented all other subgroup analysis results in tables and as forest plots.
In addition to the subgroups above, we had planned to conduct the following subgroup analyses in the presence of statistical heterogeneity:
method of delivery (e.g. nebuliser, spray, irrigation);
duration of treatment;
frequency of allergic rhinitis symptoms (e.g. intermittent or persistent as defined by ARIA 2008), where an older study using the 'seasonal' and 'perennial' classification was used, we would have interpreted 'seasonal' as 'intermittent' and 'perennial' as 'persistent' allergic rhinitis unless there was specific information in the paper that would make this inappropriate;
severity of symptoms (mild, moderate/severe as defined by ARIA 2008).
When studies had a mixed group of participants, we had planned to analyse the study as one of the subgroups (rather than as a mixed group) if more than 80% of the participants belong to one category. For example, if 81% of participants were over 18, we would have analysed the study as though the participants were adults.
Sensitivity analysis
We had planned to carry out sensitivity analyses to determine whether the findings were robust to the decisions made in the course of identifying, screening and analysing the trials. We had planned to conduct sensitivity analysis for the following factors, whenever possible:
impact of model chosen: fixed‐effect versus random‐effects model;
risk of bias of included studies: evaluating the impact of missing data on the results of the studies due to participant attrition, to determine whether the missing outcome data for the participants in the trial could have influenced the results of the review;
how outcomes were measured: we planned to investigate the impact of including data where the validity of the measurement instrument used was unclear.
If any of these investigations had found a difference in the size of the effect or heterogeneity, we would have mentioned this in the Effects of interventions section.
GRADE and 'Summary of findings' table
Using the GRADE approach, at least two review authors (KH, KS) independently rated the overall quality of evidence using the GDT tool (http://www.guidelinedevelopment.org/) for the main comparison pairs listed in the Types of interventions section. The quality of evidence reflects the extent to which we are confident that an estimate of effect is correct and we applied this in the interpretation of results. There are four possible ratings: high, moderate, low and very low. A rating of high quality of evidence implies that we are confident in our estimate of effect and that further research is very unlikely to change our confidence in the estimate of effect. A rating of very low quality implies that any estimate of effect obtained is very uncertain.
The GRADE approach rates evidence from RCTs that do not have serious limitations as high quality. However, several factors can lead to the downgrading of the evidence to moderate, low or very low. The degree of downgrading is determined by the seriousness of these factors:
study limitations (risk of bias);
inconsistency;
indirectness of evidence;
imprecision; and
publication bias.
We included a 'Summary of findings' table, constructed according to the recommendations described in Chapter 10 of the Cochrane Handbook for Systematic Reviews of Interventions (Handbook 2011). We included the following outcomes in the 'Summary of findings' table: patient‐reported disease severity score, individual symptom scores, significant adverse effects (epistaxis), disease‐specific health‐related quality of life and other adverse effects (local irritation/discomfort).
Results
Description of studies
Results of the search
The searches retrieved a total of 1402 references after removal of duplicates. We identified three additional references from other sources. We screened the titles and abstracts and subsequently removed 1319 references. We assessed 86 full texts for eligibility of which we excluded 66 references; we excluded 31 of these references (29 studies) with reasons recorded in the review (Excluded studies).
We included 16 references (14 studies). We did not identify any ongoing studies. There are four references awaiting assessment (see below).
A flow chart of study retrieval and selection is provided in Figure 1.
1.
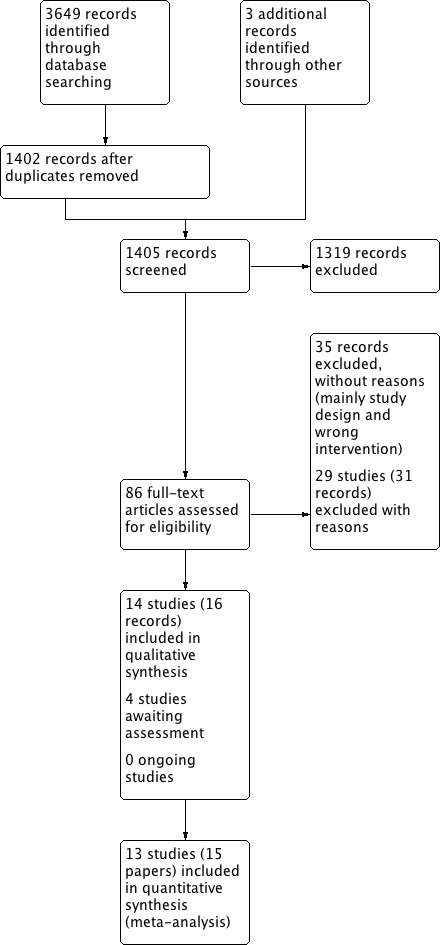
Study flow diagram.
Included studies
All of the 14 studies (16 references) included were parallel‐group randomised controlled trials (RCTs). Two studies were described as 'single‐blinded' whereas the remaining 12 were non‐blinded studies. All except one were single‐centre studies. Seven studies included two treatment arms and seven included three treatment arms. The range of follow‐up varied from 7 days to 12 weeks. Full details can be found in the Characteristics of included studies table.
Setting
The studies came from five countries: six were conducted in Italy (Di Berardino 2017; Garavello 2003; Garavello 2005; Garavello 2010; Marchisio 2012; Rogkakou 2005), five in China (Chen 2014; Li 2009; Lin 2017; Ning 2011; Wu 2014), and one in each in Thailand (Chairattananon 2013), Turkey (Yasar 2013) and the USA (Cordray 2005).
The setting of the studies is not clearly described within the papers. We assumed that most studies recruited their participants from secondary care but one study was conducted in family practices (primary care) (Cordray 2005), and four other studies were very unclear about the setting (Di Berardino 2017; Garavello 2005; Li 2009; Wu 2014).
Population
A total of 747 participants were involved in the studies. The sample size of the studies ranged from 14 to 160 participants. Only one study included more than 100 participants and the median study size was 46 participants.
Age
Seven studies included only children (Chairattananon 2013; Chen 2014; Garavello 2003; Garavello 2005; Li 2009; Marchisio 2012; Yasar 2013). Six of these reported the mean age, which ranged from 6 to 11 years. The median of the mean ages was 9.4 years. Only one study included children of less than five years (Chen 2014).
Seven studies only included adults (Cordray 2005; Di Berardino 2017; Garavello 2010; Lin 2017; Ning 2011; Rogkakou 2005; Wu 2014). Five studies reported the mean ages of the participants and these ranged from 24 to 47 years. The median of the mean ages was 33.9 years.
Sex
Thirteen of the 14 included studies included both males and females. The proportion of males in the studies ranged from 39% to 62%. One study included only pregnant women (Garavello 2010).
Diagnosis
Eleven studies diagnosed participants with allergic rhinitis and two specified that included participants had allergic rhinoconjunctivitis (Di Berardino 2017; Garavello 2005). Lin 2017 only included participants with allergic rhinitis and chronic cough (lasting for eight weeks or more).
Five studies stated (or it could be interpreted) that they included participants with persistent allergic rhinitis, and six included participants with seasonal allergic rhinitis. Further details of the type and severity of allergic rhinitis, and the allergen type, for participants included in the studies are shown in Table 3.
1. Summary of study characteristics.
| Population | Intervention | Comparison | ||||||||
| Study ID | N | Severity | Intermittent/ persistent | Allergen | Tonicity | Volume1 | Administration methods | Adjuvant | Treatment duration | |
| Chairattananon 2013 (Thailand) | 48 Children |
Mild/moderate | Not stated (persistent) | House dust mite, cockroach, cat, dog, grass, moulds | 'Normal'/isotonic saline | 90 mL (high) |
2 times per day using Hashi® Nasal Rinser | If needed: cetirizine and pseudoephedrine | 8 weeks | No saline treatment |
| Chen 2014 (China) | 61 Children |
Moderate/severe | Persistent | House dust mites and mould | Hypertonic (sea water) | Not given | 4 to 6 sprays, 2 times per day | 200 μg fluticasone propionate nasal spray daily | 4 weeks | Steroids alone |
| Cordray 2005 (USA) | 21 Adults |
Not stated | Seasonal (intermittent) |
Pollen and Alternaria | 1. Hypertonic Dead Sea saline spray | Not given | 2 sprays, 3 times per day | None | 7 days | Aqueous triamcinolone spray (110 μg into each nostril once daily) |
| 2. Normal saline spray | Not given | 2 sprays, 3 times per day | None | 7 days | Aqueous triamcinolone spray (110 μg into each nostril once daily) | |||||
| Di Berardino 2017 (Italy) | 40 Adults (allergic rhinoconjunctivitis) |
Not stated | Seasonal (intermittent) | Grass pollen | Hypertonic (% not given) | 0.15 mL (very low) |
2 times per day, using a nasal aerosol spray | Rescue antihistamines | 6 days | No saline treatment |
| Garavello 2003 (Italy) | 20 Children |
Not stated | Seasonal (intermittent) | Parietaria pollen | Hypertonic (3%) | 2.5 mL (very low) |
3 times per day, using disposable syringe | Rescue antihistamines | 6 weeks | No saline treatment |
| Garavello 2005 (Italy) | 52 Children (allergic rhinoconjunctivitis) |
Not stated | Seasonal (intermittent) | Grass pollen | Hypertonic (3%) | 0.15 mL (very low) |
3 times per day, spray from bottle fitted with an atomiser | Not reported | 7 weeks | No saline treatment |
| Garavello 2010 (Italy) | 44 Adults (pregnant women) |
Not stated | Seasonal (intermittent) | Parietaria pollen | Hypertonic (3%) | 10 mL (low) |
3 times per day, using disposable syringe | Rescue antihistamines | 6 weeks | No saline treatment |
| Li 2009 (China) | 26 Children |
Moderate/severe | Persistent | House dust mites and mould | 'Normal' (0.9%) | 500 mL (high) |
2 times per day using positive‐pressure nasal irrigation applicator | 256 μg budesonide nasal spray daily | 4 weeks | Steroids alone |
| 2 times per day using positive‐pressure nasal irrigation applicator | None | 4 weeks | Steroids alone | |||||||
| Lin 2017 (China) | 50 Adults (allergic rhinitis with chronic cough) |
Not stated | Persistent | House dust mites | 'Normal' (0.9%) | 100 mL (high) |
Nasal pharyngeal irrigation (pumping saline solution from a solution bag hung on a drip stand overhead into each nostril and allowing it to run out of the mouth) | Not stated | 4 weeks | Steroids alone |
| Marchisio 2012 (Italy) | 220 Children |
Not stated | Seasonal (intermittent) | Grass pollen including orchard and rye grass | 1. Hypertonic (2.7%) | 20 mL (low) |
2 times per day, irrigation using bulb syringe | Rescue antihistamines | 4 weeks | No saline treatment |
| 2. 'Normal' (0.9%) | 20 mL (low) |
2 times per day, irrigation using bulb syringe | Rescue antihistamines | 4 weeks | No saline treatment | |||||
| Ning 2011 (China) | 30 Adults |
Moderate/severe | Persistent | Mugwort pollen | Not stated | Not stated: 1 'puff' (very low) | 2 times per day, using a nasal aerosol spray | Not reported | 2 weeks | No saline treatment |
| Not reported | 2 weeks | Budesonide, 128 µg per nostril per day | ||||||||
| Rogkakou 2005 (Italy) | 14 Adults |
Not stated | Persistent | House dust mites and/or Parietaria | Hypertonic (% not given) | Not given | Not given | Cetirizine, orally, 10 mg/day | 4 weeks | Antihistamines alone |
| Wu 2014 (China) | 61 Adults |
Not stated | Not stated | Not stated | 'Normal' (% not given) | 75 mL (high) |
2 times per day, no method given | Budesonide, intranasal steroid spray, 64 µg/spray, 1 spray twice day (in morning and at night) | 3 months | Steroids alone |
| 2 times per day, no method given | None | 3 months | Steroids alone | |||||||
| Yasar 2013 (Turkey) | 60 Children |
Mild, moderate and severe | Persistent and seasonal | Not stated | Not stated | Not stated "2 puffs" (very low) |
2 'puffs' per nostril per day, using a nasal aerosol spray | Mometasone furoate (2 puffs in each nostril per day) | 8 weeks | Steroids alone |
1Volume reported as per nostril per application. The volume categories were defined as: VERY LOW: less than 5 ml per nostril per application; LOW: between 5 ml to 59 ml per nostril per application; HIGH: ≥ 60 ml per nostril per application.
Interventions
Saline solution
Details of the tonicity, volume and method of administration of the saline solution are provided in Table 3.
In summary:
Eight studies used hypertonic saline and five studies used isotonic ('normal') saline. Three studies did not provide any information about tonicity.
Five studies used very low‐volume saline, two used low‐volume saline and four used high‐volume saline. Three studies did not provide information on the volume.
Five studies allowed oral antihistamines to be used as rescue medication when needed (Chairattananon 2013; Di Berardino 2017; Garavello 2005; Garavello 2010; Marchisio 2012). Chairattananon 2013 stated that pseudoephedrine was also prescribed as rescue medication.
The duration of treatment ranged from seven days to three months.
Comparisons
Saline versus no saline treatment
Seven studies compared nasal saline irrigation with no saline treatment (Chairattananon 2013; Di Berardino 2017; Garavello 2003; Garavello 2005; Garavello 2010; Marchisio 2012; Ning 2011). Marchisio 2012 was a three‐arm study that compared two different types of nasal saline (hypertonic and isotonic saline) with no saline treatment.
Saline plus pharmacological treatment versus pharmacological treatment alone
Three studies included arms where both nasal saline irrigation and intranasal corticosteroids were given. The intranasal steroids given were budesonide nasal spray in Li 2009 (256 μg/day for four weeks, 128 μg/day for four weeks and 64 μg/day for four weeks) and Wu 2014 (128 µg/day for three months); and fluticasone proportionate nasal spray in Chen 2014 (200 μg/day for four weeks, 100 μg/day for four weeks and 50 μg/day for four weeks). It was not explicitly stated in any of the studies in which order the saline and steroid treatments were given.
One study used an oral antihistamine (10 mg/day cetirizine) in addition to saline irrigation for four weeks (Rogkakou 2005).
Saline versus intranasal corticosteroids
Seven studies compared nasal saline irrigation with intranasal steroid treatment. Intranasal steroids were:
mometasone furoate (one study; Yasar 2013);
aqueous triamcinolone (one study; Cordray 2005).
We considered the doses for these treatments to be within the normal clinical range and details can be found in the Characteristics of included studies table.
Saline versus intranasal antihistamines
One study compared saline irrigation with intranasal antihistamines (two puffs of azelastine in each nostril per day (1 puff = 0.14 mg)) for eight weeks. This study did not report any of the primary or secondary outcomes defined in the review (Yasar 2013).
Outcomes
One study did not report any relevant outcomes as the aim of the study was to measure nasal cavity volumes using acoustic rhinometry (Yasar 2013).
Primary outcomes
Disease severity, as measured by patient‐reported symptom score
Twelve studies reported a patient‐reported disease severity score. These scores differed greatly in the method of reporting from combined visual analogue scales for all symptoms, to individual scales for up to 10 symptoms. The summary scores were also all constructed differently. Only one paper reported validation of the scales that they used (Lin 2017). A summary of the scales used is in Table 4.
2. Summary of patient‐reported disease severity scores.
| Study ID | Symptoms measured | Score for each symptom | Summation (total range) | Notes |
| Chairattananon 2013 | 'Nasal symptoms' | Visual analogue scale | Completed once at end of study (0 to 10) | Lower score = worse symptoms |
| Chen 2014 | 1. Nasal itching 2. Rhinorrhoea 3. Nasal obstruction 4. Sneezing |
0 to 3 scale (0 = no symptoms, 3 = severe symptoms) |
Total scores represented the sums of scores for the 4 symptoms (range: 0 to 12) | No measures of variance presented and insufficient details to impute them. Authors were contacted but no response was received. |
| Cordray 2005 | Not measured | |||
| Di Berardino 2017 | 1. Nasal itching 2. Nasal discharge 3. Nasal obstruction 4. Sneezing |
0 to 2 scale (0 = no symptoms, 2 = intolerable symptoms) | Daily scores for each symptom were added together then summed for each day of the 7‐day trial period (range: 0 to 56) | — |
| Garavello 2003 | 1. Nasal itching 2. Rhinorrhoea 3. Nasal obstruction 4. Sneezing |
0 to 4 scale (0 = no symptoms, 4 = worst symptoms) | Daily scores for each symptom were summed. The daily scores were averaged to calculate 'mean daily rhinitis score' per participant for each week (range: 0 to 16). | — |
| Garavello 2005 | 1. Nasal discharge 2. Nasal blockage 3. Eye redness 4. Eye itching |
0 to 3 scale (0 = none, 3 = severe) | Daily scores for each symptom were summed. The daily scores were averaged to calculate a 'mean daily rhinitis score' per participant for each week of the pollen season (probable range: 0 to 12, see notes section). | Paper reports that the total range was 0 to 16. Authors were contacted for clarification but there was no response. |
| Garavello 2010 | 1. Nasal itching 2. Rhinorrhoea 3. Nasal obstruction 4. Sneezing |
0 to 4 scale (0 = none; 1 = slight; 2 = mild; 3 = moderate; 4 = severe) | Daily scores for each symptom were summed. The daily scores were averaged to calculate a 'mean daily rhinitis score' per participant for each week of the pollen season (range: 0 to 16). | — |
| Li 2009 | 1. Sneezing/itching 2. Rhinorrhoea 3. Nasal congestion 4. Postnasal drip/snorting |
0 to 3 scale (0 = no symptom) | Individual symptom scores were summed to give a total score (range: 0 to 12) | — |
| Lin 2017 | 1. Nasal obstruction 2. Rhinorrhoea 3. Sneezing 4. Nasal pruritis |
Visual analogue scale | Completed once at end of study (0 to 10) | Lower score = less severe symptoms |
| Marchisio 2012 | 1. Nasal itching 2. Rhinorrhoea 3. Nasal obstruction 4. Sneezing |
1 to 4 (1 = no symptoms, 4 = severe) | Nasal score was calculated as the mean of the sum of scores of each nasal symptom (range: 1 to 4) | Rhinorrhoea was assessed by physician |
| Ning 2011 | 1. Sneezing 2. Rhinorrhoea 3. Blocked nose/congestion 4. Itchy nose |
1 to 3 (higher = worse symptoms) | Symptom score was calculated as the sum of the individual symptoms (range: 4 to 12) | — |
| Rogkakou 2005 | 1. Rhinorrhoea 2. Itching 3. Sneezing 4. Stuffy nose 5. Watery eyes 6. Itching 7. Conjunctival hyperaemia 8. Palpebral oedema |
4‐point scale (0 = none, 3 = severe) | The sum of the symptom scores for each week of the study was calculated (range: 0 to 24) | Night‐time symptom scores were also reported by participants but not presented in this review |
| Wu 2014 | 1. Nasal obstruction 2. Itching 3. Sneezing 4. Nasal discharge 5. Eye itching 6. Eye swelling 7. Tearing 8. Eye pain 9. Coughing 10. Difficulty breathing |
0 to 10 (0 = least symptoms, 10 = most symptoms) | The method for combining is not clear. The results are likely to be an average of the individual symptoms (range: 0 to 10). | — |
Significant local adverse effects: epistaxis
Adverse effects were not well reported in the studies. Only four studies specifically mentioned in their methods section that adverse effects would be routinely reported (Chairattananon 2013; Garavello 2005; Garavello 2010; Lin 2017). Of the 10 studies that mentioned adverse effects in their results section, six only reported on the nasal saline irrigation group (Chairattananon 2013; Chen 2014; Garavello 2005; Garavello 2010; Li 2009; Marchisio 2012), and three reported on adverse effects in both study arms (Garavello 2003; Lin 2017; Wu 2014). The remaining study indicated that there were withdrawals due to adverse effects but it was not clear to which groups the participants were allocated (Cordray 2005).
Secondary outcomes
Disease‐specific health‐related quality of life
Five studies measured disease‐specific health‐related quality of life. Two studies used the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) (Cordray 2005; Wu 2014), although the studies constructed the overall score in a different way. Lin 2017 used the mini‐RQLQ, a shortened version of the full RQLQ, Rogkakou 2005 used the Rhinasthma® questionnaire and Chairattananon 2013 used a questionnaire specific to Thai allergic rhinoconjunctivitis patients (RCQ‐36). Further details of each scale can be found in the study‐specific section of the Characteristics of included studies table.
Individual symptom scores
No studies reported individual symptom scores.
Generic health‐related quality of life
No studies measured generic health‐related quality of life.
Any other local adverse effects: local irritation, discomfort
See the section above on significant local adverse effects.
Aural symptoms: ear pain, pressure or feeling of fullness
No studies specifically mentioned aural symptoms as either a symptom of allergic rhinitis or as an adverse effect of treatment.
Endoscopic score
Only Marchisio 2012 reported the use of an endoscopy score as an outcome. This study graded the turbinate swelling on a range of 0 to 3 and reported the change at four weeks from baseline in the proportion of children with moderate to severe swelling of the turbinate.
Excluded studies
We formally excluded 29 studies (31 papers) that most closely matched the inclusion criteria (Characteristics of excluded studies).
Population
We excluded four studies as they investigated the use of saline irrigation in people with chronic rhinosinusitis, not allergic rhinitis (Bachmann 2000; Heatley 2001; Rabago 2002; Shoseyov 1998). In addition, we excluded one study as despite including people with allergic rhinitis, the condition was diagnosed by symptoms and not using one of the diagnostic tests specified in our inclusion criteria (Chowdary 2017).
Intervention
We excluded four studies due to the wrong intervention. Two studies used thermal water rather than saline (Barbieri 2002; Mora 2002), one compared saline against a non‐standard treatment for allergic rhinitis (Luffa Operculate) (NCT01248325 2010) and one used tap water, rather than saline (Xiong 2014).
Study design
We excluded five studies because the study design was a single arm with no comparison group (Barberi 2016a; Barberi 2016b; Jan 2013; Nguyen 2014; Tomooka 2000).
Comparisons of saline studies
We excluded 15 studies (17 references) due to the comparison being between different saline solutions, rather than a comparison of saline with no saline treatment or pharmacological treatment for allergic rhinitis (ChiCTR‐INR‐16009778 2016; Chusakul 2012; Del Giudice 2011; Lin 2014; Malizia 2017; NCT01326247 2011; NCT02729012 2016; Polasek 1987; Satdhabudha 2012; Singh 2016; TCTR20150923001 2015; TCTR20160120001 2016; TCTR20160913003 2016; Ural 2009; Valencia Chavez 2015).
Awaiting assessment studies
There are four studies awaiting assessment. One study is awaiting translation (Krcmova 2011). Three studies were published as abstracts only and the full‐text papers, or further information, could not be obtained despite attempts to contact the study authors (Hausfeld 2007; Lee 2017; Manole 2013). See Characteristics of studies awaiting classification.
Risk of bias in included studies
See Figure 2 for a 'Risk of bias' graph (our judgements about each risk of bias item presented as percentages across all included studies) and Figure 3 for a 'Risk of bias' summary (our judgements about each risk of bias item for each included study).
2.
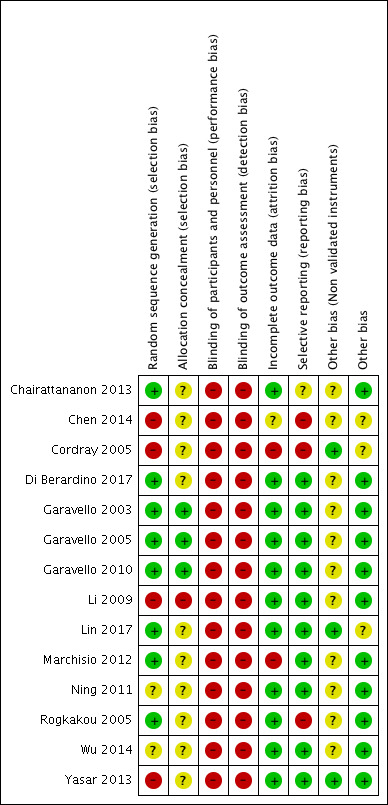
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
3.
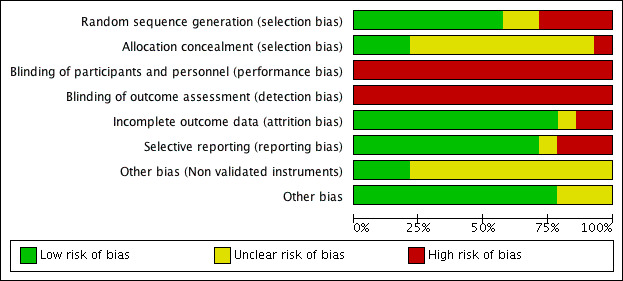
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
Random sequence generation
We assessed four studies as high risk of bias for random sequence generation.
Chen 2014 did not mention the methods of randomisation in the paper and we noted that there was unequal distribution between the groups and very limited information about the baseline characteristics of the population included by allocated group.
Li 2009 describes the participants as "randomised" in the abstract but uses the word "divided" in the methods section with no further details. In addition, there was a lack of information about baseline characteristics.
In Yasar 2013 it is unclear whether the participants were randomised to study groups as the paper states that the participants were "classified" into three groups. Although baseline characteristics for age and gender were given and did not differ between groups, other baseline characteristics were not provided.
Cordray 2005 states that the study was "randomised" but no methods are described and it is not even clear how many were randomised to each group. The paper also lacked baseline characteristics for the groups.
We assessed two studies as having unclear risk of bias as the papers indicated that the participants were "randomised" but no details of the methods are presented (Ning 2011; Wu 2014).
We assessed the remaining eight studies as at low risk of bias for random sequence generation.
Allocation concealment
One study had a high risk of allocation concealment bias, as there were an unequal number of participants in each arm and no baseline characteristics are provided so there is a concern that the investigators may have known the group to which they were allocating participants (Li 2009).
There were 10 studies that did not provide any information about the methods used to ensure that the investigators allocating participants to the groups could not influence the allocation and we assessed these as having unclear risk of bias (Chairattananon 2013; Chen 2014; Cordray 2005; Di Berardino 2017; Marchisio 2012; Ning 2011; Rogkakou 2005; Wu 2014; Yasar 2013).
The remaining three studies were at low risk of allocation concealment bias.
Blinding
Blinding of participants and personnel
We judged all of the studies to be at high risk of bias. Thirteen studies were non‐blinded and many of these compared saline with no saline treatment so there were practical issues that meant blinding of participants would not have been possible. Cordray 2005 describes their study in the abstract as "single‐blinded" but does not provide details of which aspect of the trial this relates to as the three different trial arms had different regimens: the saline was given three times daily whereas the steroid was given once daily and no placebo is mentioned. We assessed this as insufficient protection from participants and personnel from knowing the treatment group to which they were allocated.
Blinding of outcome assessors
We assessed all of the included studies to be at high risk of bias. None of the studies mentioned that the outcome assessors were blinded to treatment group. As most of the outcomes were participant‐reported, and the participants were not blinded, blinding of outcome assessors was not possible.
Incomplete outcome data
We assessed two studies to be at high risk of attrition bias due to a rate of withdrawal above 25%. In Cordray 2005, 29% of participants withdrew but the authors did not provide any reasons for withdrawals or state whether there were differences between groups. Marchisio 2012 noted that 25% of the participants in the no saline treatment group did not complete the study. The dropout rate was imbalanced between the groups although reasons were provided. More people dropped out of the no saline treatment group because of the use of rescue medications.
One study was at unclear risk of bias as although no withdrawals were mentioned the paper did not provide enough information to determine whether all the participants included in the study completed (Chen 2014).
We assessed the remaining 11 studies as at low risk of bias.
Selective reporting
We assessed three studies as at high risk of reporting bias. Chen 2014 had incomplete reporting of outcomes in the paper. Cordray 2005 was the only study that reported withdrawals due to adverse effects, yet failed to provide information about the nature of the effects or in which treatment groups they occurred. Rogkakou 2005 failed to report any measures of variation for their results.
One study was at unclear risk of selective reporting bias (Chairattananon 2013). One outcome was mentioned in the results section (use of antibiotics) but was not identified in the methods section. In addition, there was some confusion between the published abstract and the draft full paper (provided by personal communication with the authors) regarding which quality of life instrument was used.
We assessed the remaining 10 studies as at low risk of selective reporting as, despite not having a protocol available, all of the outcomes mentioned in their methods sections were reported in the results.
Other potential sources of bias
Use of non‐validated instruments
We assessed three studies as at low risk of bias. In Lin 2017, references were provided for the papers reporting validation of the different outcomes. Yasar 2013 did not report any relevant outcomes. In Cordray 2005, the only outcome of relevance that was reported had been measured using a validated scale.
We assessed the remaining 11 studies as at unclear risk of bias because they did not mention the validation of the instruments used to measure the patient‐reported disease severity score. In addition, Wu 2014 and Chairattananon 2013 appeared to use variations of validated health‐related quality of life scales but did not discuss the impact that this may have had on the results.
Other bias
A general lack of information provided in two papers led to them being assessed as having unclear risk of other bias (Chen 2014; Cordray 2005).
We identified no other sources of bias in the remaining 12 studies.
Funding sources
Funding was mentioned in seven studies. Two studies reported that no external financial support was received (Di Berardino 2017; Yasar 2013). Five studies received funding from national or regional governmental funds (Chen 2014; Li 2009; Lin 2017; Ning 2011; Wu 2014).
No information was provided about funding in the remaining seven studies.
Declarations of interest
Four studies made a declaration in the paper that none of the authors had conflicts of interest (Di Berardino 2017; Lin 2017; Marchisio 2012; Yasar 2013). None of the 10 remaining studies provide any declarations of interest.
Effects of interventions
Comparison 1. Saline versus no saline treatment
Seven studies (444 participants) compared saline treatment with no saline treatment. Four used hypertonic saline (Di Berardino 2017; Garavello 2003; Garavello 2005; Garavello 2010) and one used isotonic solution (Chairattananon 2013). One study did not provide details of tonicity (Ning 2011). One study included two saline groups, one using isotonic saline and one using hypertonic saline (Marchisio 2012); for the initial analyses we combined these saline groups.
1.1. Disease severity, as measured by patient‐reported symptom score
All seven studies presented data for disease severity using a number of different scales; a summary can be found in Table 4.
One study asked participants to rate their "overall nasal symptoms" on a 0 to 10 visual analogue scale (lower score = WORSE symptoms) (Chairattananon 2013).
Five of the remaining six studies asked participants to measure the same symptoms: rhinorrhoea, nasal blockage, nasal itching and sneezing (Di Berardino 2017; Garavello 2003; Garavello 2010; Marchisio 2012; Ning 2011). One study recorded different symptoms (nasal discharge, nasal blockage, eye redness, eye itching) (Garavello 2005).
Due to the differences in the scales used, we used a standardised mean difference (SMD) in the analysis.
Up to four weeks
Six studies reported results at up to four weeks. The results showed that people using saline irrigation had lower symptom scores than people in the no saline treatment group (SMD ‐1.32, 95% confidence interval (CI) ‐1.84 to ‐0.81; 407 participants; 6 studies; I2 = 75%) (Analysis 1.1). Due to the statistical heterogeneity identified, we used a random‐effects model. The heterogeneity was driven mainly by the large apparent effect in Garavello 2010. Removing this study reduced the heterogeneity to a low level and the result still significantly favoured the use of saline irrigation. This SMD represents a large effect size and translates into a decrease of approximately 1.97 points (1.21 to 2.74) on a 0‐ to 10‐point visual analogue scale for nasal symptoms (lower = better) (low‐quality evidence).
1.1. Analysis.
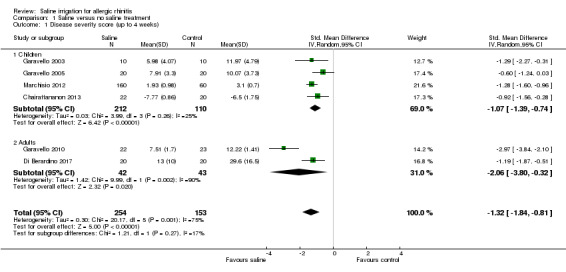
Comparison 1 Saline versus no saline treatment, Outcome 1 Disease severity score (up to 4 weeks).
Subgroup analysis results show that both children (SMD ‐1.07, 95% CI ‐1.39 to ‐0.74; 322 participants; 4 studies; I2 = 25%) and adults (SMD ‐2.06, 95% CI ‐3.80 to ‐0.32; 85 participants; 2 studies; I2 = 90%) reported improved symptoms with saline compared to no saline. There was no evidence of a difference between the age subgroups.
Four weeks to six months
Five studies reported results at between six and eight weeks. The results showed that people using saline irrigation had lower symptom scores than people in the no saline group (SMD ‐1.44, 95% CI ‐2.39 to ‐0.48; 167 participants; 5 studies; I2 = 86%) (Analysis 1.2). We used a random‐effects model due to the presence of statistical heterogeneity. The heterogeneity did not reduce after removing Garavello 2010 and the result still significantly favoured the use of saline irrigation. This SMD represents a large effect size and translates into a decrease of approximately 2.98 points (0.99 to 5.98) on a 0‐ to 10‐point visual analogue scale for nasal symptoms (lower = better) (low‐quality evidence).
1.2. Analysis.
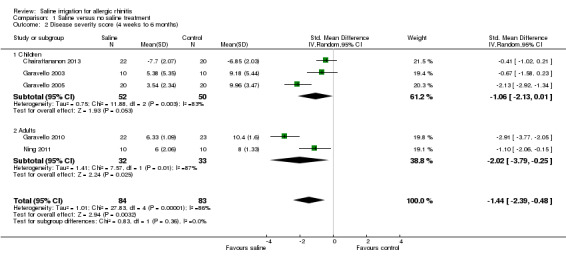
Comparison 1 Saline versus no saline treatment, Outcome 2 Disease severity score (4 weeks to 6 months).
Subgroup analysis show that both children (SMD ‐1.06, 95% CI ‐2.13 to 0.01; 102 participants; 3 studies; I2 = 83%) and adults (SMD ‐2.02, 95% CI ‐3.79 to ‐0.25; 65 participants; 2 studies; I2 = 87%) reported improved symptoms with saline compared to no saline, but there was no evidence of a difference between the subgroups for the different ages.
1.2. Significant local adverse effects: epistaxis
Three studies reported methods for collecting information about adverse effects in their methods section (Chairattananon 2013; Garavello 2005; Garavello 2010). Five studies made a statement about adverse effects in their results section. Of these, two studies (240 children) reported that there were no adverse effects in either of the treatment groups although epistaxis was not specifically mentioned as being sought (low‐quality evidence) (Garavello 2003; Marchisio 2012). The remaining three studies only provided information that no adverse effects were reported in the saline treatment arm (Chairattananon 2013; Garavello 2003; Marchisio 2012).
1.3. Disease‐specific health‐related quality of life
One study (Chairattananon 2013; 42 children) reported disease‐specific health‐related quality of life using the Thai Rhinoconjunctivitis Quality of Life scale (RCQ‐36). This questionnaire has 36 items each measured on a 0 to 4 scale, however only 35 items were used in this study (range 0 to 140), higher score = worse quality of life.
Up to four weeks
It is uncertain whether there is an improvement in disease‐specific quality of life with saline irrigation compared with no saline treatment at four weeks in children (mean difference (MD) ‐3.32, 95% CI ‐11.35 to 4.71; 42 participants; 1 study) (Analysis 1.3) (very low‐quality evidence).
1.3. Analysis.
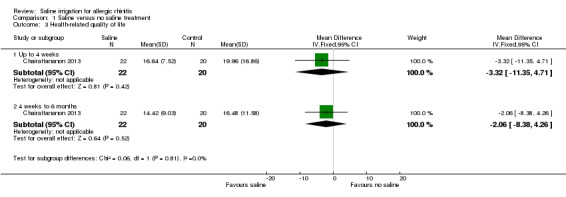
Comparison 1 Saline versus no saline treatment, Outcome 3 Health‐related quality of life.
Four weeks to six months
It is uncertain whether there is an improvement in disease‐specific quality of life with saline irrigation compared with no saline treatment at eight weeks in children (MD ‐2.06, 95% CI ‐8.38 to 4.26; 42 participants; 1 study) (Analysis 1.3) (very low‐quality evidence).
1.4. Individual symptom scores
No studies reported symptom scores for the individual symptoms of anterior rhinorrhoea (runny nose), posterior rhinorrhoea (post‐nasal drip), nasal blockage/congestion/obstruction, nasal itching or sneezing.
1.5. Generic health‐related quality of life
No studies reported generic health‐related quality of life.
1.6. Any other local adverse effects: local irritation, discomfort
Five studies made a statement about adverse effects. Two studies (240 children) reported that no adverse effects were experienced in either of the treatment groups (Garavello 2003; Marchisio 2012), although it is unclear whether the specific adverse effects of local irritation and discomfort were sought (low‐quality evidence).
The remaining three studies (68 children, 44 adults) reported that there were no adverse effects in the 'active' treatment group (i.e. saline irrigation) although again it is unclear whether the specific adverse effects of local irritation and discomfort were sought (Chairattananon 2013; Garavello 2005; Garavello 2010).
1.7. Aural symptoms: ear pain, pressure or feeling of fullness
No studies reported aural symptoms.
1.8. Endoscopic score (e.g. Lund‐Mackay/Lund‐Kennedy)
No studies reported endoscopy scores (for example, Lund‐Mackay or Lund‐Kennedy).
One study (220 children) reported the change from baseline at four weeks in the proportion of children with moderate to severe swelling of the turbinates. The group using hypertonic saline irrigation showed a significant reduction in the percentage of children with moderate to severe turbinate swelling (‐31.2%, 95% CI ‐16.5% to ‐46.0%), whereas the groups using isotonic saline and no saline irrigation both showed a non‐significant reduction in the proportion of children with moderate to severe turbinate swelling (‐5.1%, 95% CI ‐9.9% to 19.9% and ‐5.0%, 95% CI ‐11.9% to 21.9%, respectively) (Marchisio 2012).
Subgroup analysis
We stated in the protocol that analyses would be completed with regards to the volume, tonicity and alkalinity of the solution, irrespective of statistical heterogeneity. The only outcome that had enough data to be included in the subgroup analysis was that of patient‐reported disease severity. It should be noted that there is statistical heterogeneity within these results, which is probably due to the different scoring systems used and so all of the results must be treated with caution.
Volume
When we classified the results into volume subgroups, all of the saline volume categories showed improvement in patient‐reported disease severity compared with no saline treatment at up to four weeks:
Very low‐volume saline (less than 5 mL/nostril per application): SMD ‐0.96, 95% CI ‐1.39 to ‐0.52; 100 participants; 3 studies; I2 = 5%.
Low‐volume saline (between 5 mL and 60 mL/nostril per application): SMD ‐2.07, 95% CI ‐3.73 to ‐0.42; 265 participants; 2 studies; I2 = 92%.
High‐volume saline (more than 60 mL/nostril per application): SMD ‐0.92, 95% CI ‐1.56 to ‐0.28; 42 participants; 1 study.
See Analysis 4.1.
4.1. Analysis.
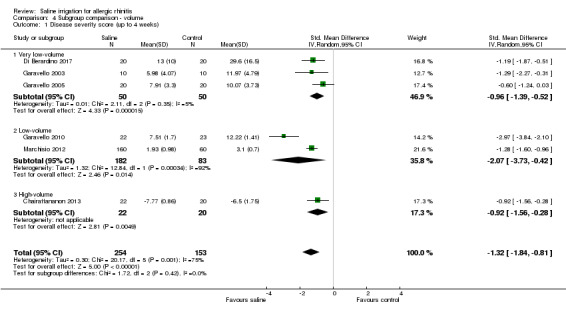
Comparison 4 Subgroup comparison ‐ volume, Outcome 1 Disease severity score (up to 4 weeks).
The results for four weeks to six months (range of follow‐up six to eight weeks) were as follows:
Very low‐volume saline (less than 5 mL/nostril per application): SMD ‐1.33, 95% CI ‐2.22 to ‐0.44; 80 participants; 3 studies; I2 = 67%.
Low‐volume saline (between 5 mL and 60 mL/nostril per application): SMD ‐2.91, 95% CI ‐3.77 to ‐2.05; 45 participants; 1 study.
High‐volume saline (more than 60 mL/nostril per application): SMD ‐0.41, 95% CI ‐1.02 to 0.21; 42 participants; 1 study.
See Analysis 4.2.
4.2. Analysis.
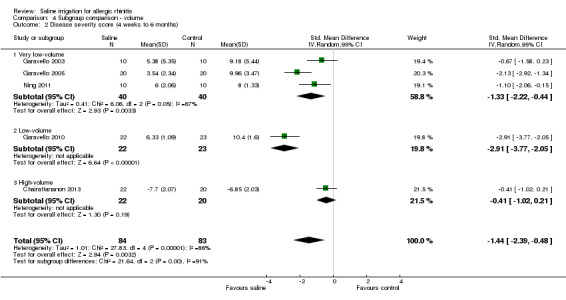
Comparison 4 Subgroup comparison ‐ volume, Outcome 2 Disease severity score (4 weeks to 6 months).
The tests for subgroup differences did not indicate statistical differences between the subgroups at either time point.
Tonicity
For this subgroup analysis we separated out the results for the three‐arm trial comparing two different saline solutions (hypertonic and isotonic saline) with no saline treatment (Marchisio 2012), but we split the denominator in the no saline treatment group between the comparisons in the two separate groups to ensure that people in the no saline treatment group were not counted twice.
When we classified the results into tonicity subgroups, all of the saline tonicity categories showed improvement in patient‐reported disease severity compared with no saline treatment at up to four weeks:
Isotonic or 'normal' saline (0.9%): SMD ‐0.82, 95% CI ‐1.18 to ‐0.47; 152 participants; 2 studies; I2 = 0%.
Hypertonic saline (> 0.9%): SMD ‐1.72, 95% CI ‐2.62 to ‐0.82; 255 participants; 5 studies; I2 = 87%.
See Analysis 5.1.
5.1. Analysis.
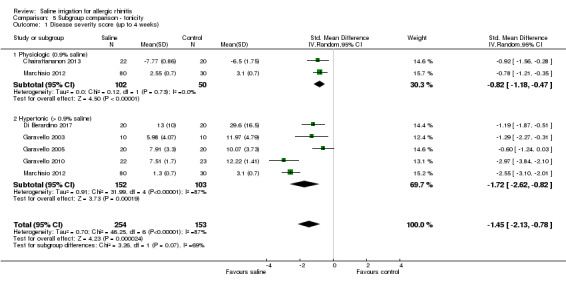
Comparison 5 Subgroup comparison ‐ tonicity, Outcome 1 Disease severity score (up to 4 weeks).
The results for between four weeks and six months (range of follow‐up six to eight weeks) were as follows:
Isotonic or 'normal' saline (0.9%): SMD ‐0.41, 95% CI ‐1.02 to 0.21; 42 participants; 1 study.
Hypertonic saline (> 0.9%): SMD ‐1.91, 95% CI ‐3.14 to ‐0.68; 105 participants; 3 studies; I2 = 84%.
See Analysis 5.2.
5.2. Analysis.
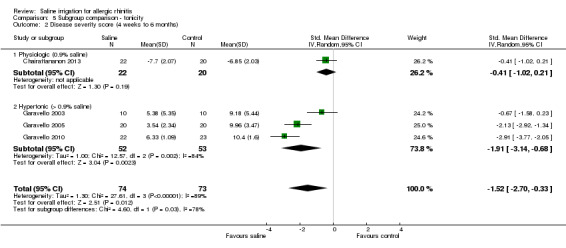
Comparison 5 Subgroup comparison ‐ tonicity, Outcome 2 Disease severity score (4 weeks to 6 months).
In both instances the effect size for treatment with hypertonic solution was greater than with normal saline. The tests for subgroup differences did not indicate statistical differences at up to four weeks, but did suggest that there may have been a difference at between four weeks and six months (P = 0.03, I2 = 78.3%). However, it can seen that there is considerable heterogeneity in the results of the group using hypertonic saline.
Alkalinity
The alkalinity of solutions was not well reported in the studies and so it was not possible to undertake this subgroup analysis.
No further subgroup analyses were undertaken.
Comparison 2. Adding saline irrigation to pharmacological treatment
Three studies (119 participants) compared saline irrigation with intranasal steroids against intranasal steroids alone. One study (14 adults) compared saline irrigation with oral antihistamine against oral antihistamines alone.
2.1. Disease severity, as measured by patient‐reported symptom score
Four studies reported this outcome (Chen 2014; Li 2009; Rogkakou 2005; Wu 2014). Chen 2014 did not present sufficient data in the paper to use in the meta‐analysis and no response was received after we attempted to contact the author, so only narrative results are presented. Each of the studies included in the meta‐analysis used different scoring mechanisms and included different symptoms (Table 4):
Li 2009 and Chen 2014: reported four symptoms each measured on a four‐point scale (0 to 3 scale, 0 = no symptoms). The sum of the scores gave a total score (total range 0 to 12).
Rogkakou 2005: reported eight symptoms each measured on a four‐point scale (0 to 3, 0 = no symptoms). The sum of the symptom scores was calculated (total range 0 to 24).
Wu 2014: reported 10 symptoms each measured on a 0 to 10 visual analogue scale (VAS) (0 = least symptoms). These scores were averaged to give a final range of 0 to 10.
Up to four weeks
Two studies (18 children, 14 adults) reported patient‐reported disease severity at up to four weeks. In one study all participants also used oral antihistamines (Rogkakou 2005), and in the other study all participants also used intranasal steroids (Li 2009). It is uncertain whether saline irrigation in addition to pharmacological treatment (oral antihistamines or intranasal steroids) improved symptom scores at four weeks compared with pharmacological treatment alone (SMD ‐0.60, 95% CI ‐1.34 to 0.15; 32 participants; 2 studies; I2 = 0%) (Analysis 2.1)(very low‐quality evidence).
2.1. Analysis.
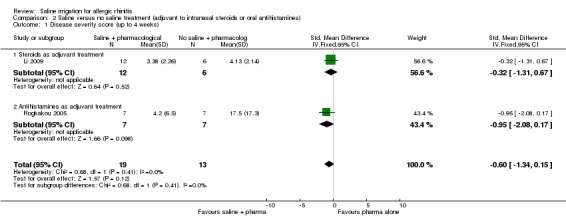
Comparison 2 Saline versus no saline treatment (adjuvant to intranasal steroids or oral antihistamines), Outcome 1 Disease severity score (up to 4 weeks).
Chen 2014 reported higher mean values for disease severity (more severe symptoms) in the intranasal steroid group (4.16, 17 children), compared with the group receiving saline and intranasal steroids (3.26, 26 children) at four weeks using an instrument with a total range of 0 to 12. The authors reported that there was a significant difference between groups (P < 0.05) but they did not provide information on the variance of the results and no response was received from the author after a request for further information.
Four weeks to six months
Two studies (18 children; 40 adults) in which all participants also used intranasal steroids reported patient‐reported diease severity at three months (Li 2009; Wu 2014). It is uncertain whether saline irrigation in addition to intranasal steroids improved symptom scores at three months compared with pharmacological treatment alone (SMD ‐0.32, 95% CI ‐0.85 to 0.21; 58 participants; 2 studies; I2 = 0%) (Analysis 2.2) (very low‐quality evidence).
2.2. Analysis.
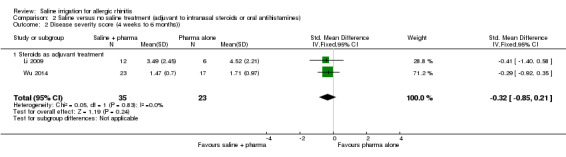
Comparison 2 Saline versus no saline treatment (adjuvant to intranasal steroids or oral antihistamines), Outcome 2 Disease severity score (4 weeks to 6 months)).
Chen 2014 reported higher mean values for disease severity (more severe symptoms) in the intranasal steroid group (4.27, 17 children) compared with the group receiving saline and intranasal steroids (3.37, 26 children) at three months using an instrument with a total range of 0 to 12.
2.2. Significant local adverse effects: epistaxis
None of the studies specifically mentioned how adverse effects would be sought in their study methods; nor did they mention epistaxis as an adverse effect. Three studies made statements about adverse effects. One study (40 adults) indicated that "all [treatments were]tolerated well, none [of the participants] had adverse events" (Wu 2014) and the other two studies (62 children) reported that nasal irrigation with saline was well accepted in all patients and no adverse effects were reported in the saline group (Chen 2014; Li 2009) (very low‐quality evidence).
2.3. Disease‐specific health‐related quality of life
Two studies including only adults measured disease‐specific health‐related quality of life at between four weeks and three months.
Rogkakou 2005, where all participants also used oral antihistamines, used the Rhinasthma quality of life instrument (range 0 to 100, lower = better quality of life) at four weeks. We present the results for the 'global impact', which is a synthetic score covering the entire questionnaire. Standard deviations for the results were not presented and so we imputed these from the P values.
Wu 2014, where all participants also used intranasal steroids, used the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) (unclear range, lower = better quality of life) at three months.
Due to these differences, we used the SMD in the analysis.
Four weeks to six months
It is uncertain whether saline irrigation in addition to pharmacological treatment (oral antihistamines or intranasal steroids) improved health‐related quality of life at four weeks to three months compared with pharmacological treatment alone (SMD ‐1.26, 95% CI ‐2.47 to ‐0.05; 54 adult participants; 2 studies; I2 = 63%). We used a random‐effects model due to statistical heterogeneity (Analysis 2.3) (very low‐quality evidence).
2.3. Analysis.
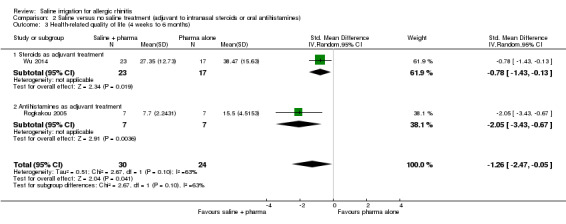
Comparison 2 Saline versus no saline treatment (adjuvant to intranasal steroids or oral antihistamines), Outcome 3 Health‐related quality of life (4 weeks to 6 months).
2.4. Individual symptom scores
No studies reported symptom scores for the individual symptoms of anterior rhinorrhoea (runny nose), posterior rhinorrhoea (post‐nasal drip), nasal blockage/congestion/obstruction, nasal itching or sneezing.
2.5. Generic health‐related quality of life
No studies reported generic health‐related quality of life.
2.6. Any other local adverse effects: local irritation, discomfort
None of the studies specifically mentioned local irritation or discomfort as an adverse effect. Two studies made statements about adverse effects. One (40 adults) indicated that "all [treatments were]tolerated well, none [of the participants] had adverse events" (Wu 2014) and the other (18 children) stated that "Nasal irrigation with saline was well accepted in all patients and no adverse effect was reported” (Li 2009) (very low‐quality evidence).
2.7. Aural symptoms: ear pain, pressure or feeling of fullness
No studies reported aural symptoms of ear pain, pressure or feeling of fullness.
2.8. Endoscopic score (e.g. Lund‐Mackay/Lund‐Kennedy)
No studies reported endoscopic scores.
Comparison 3. Saline versus intranasal steroids
Seven studies (89 children, 129 adults) compared saline nasal irrigation with intranasal steroids (Chen 2014; Cordray 2005; Li 2009; Lin 2017; Ning 2011; Wu 2014; Yasar 2013), although Yasar 2013 (40 children) did not report any of the primary or secondary outcomes for this review.
One study included two saline arms (hypertonic and normal saline) (Cordray 2005), for which we combined the results for these analyses.
3.1. Disease severity, as measured by patient‐reported symptom score
Five studies measured disease severity using a patient‐reported symptom score (Chen 2014; Li 2009; Lin 2017Ning 2011; Wu 2014).
Two of these studies could not be included in the quantitative results: Chen 2014 did not present sufficient data in the paper to be used in the meta‐analysis and no response was received after we attempted to contact the author, therefore only narrative results are presented. Ning 2011 used median values and interquartile ranges to describe the results in the intranasal steroid arm, and means with standard deviations in the arm receiving saline.
Each of the three studies included in the quantitative results used different scales, which are summarised in Table 4.
Li 2009: Four symptoms: sneezing/itching, rhinorrhoea, nasal congestion and postnasal drip/snorting, each measured on a four‐point scale (0 to 3 scale, 0 = no symptom). The sum of the scores gave a total score (total range 0 to 12).
Lin 2017: Four symptoms: nasal obstruction, rhinorrhoea, sneezing and nasal pruritis, measured as a "total nasal score" on a visual analogue scale (0 to 10).
Wu 2014: Ten symptoms: nasal obstruction, itching, sneezing, nasal discharge, eye itching, eye swelling, tearing, eye pain, coughing and difficulty breathing, each measured on a 0 to 10 visual analogue scale (VAS) (0 = least symptoms). These scores were averaged to give a final range of 0 to 10.
Due to these differences, when we performed meta‐analyses that included more than one study we used the SMD.
Up to four weeks
One study (14 children) presented results for symptom severity. It is uncertain whether there is a difference in symptom severity score between the intranasal steroid and the saline irrigation groups at four weeks (MD 1.06, 95% CI ‐1.65 to 3.77) (Analysis 3.1).
3.1. Analysis.
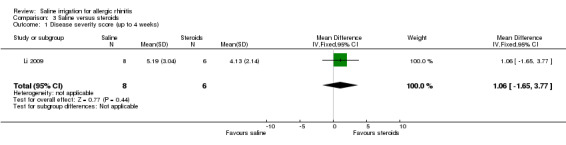
Comparison 3 Saline versus steroids, Outcome 1 Disease severity score (up to 4 weeks).
Chen 2014 reported higher mean values for disease severity (more severe symptoms) in the saline group (5.44, 18 children) compared with the intranasal steroid group (4.11, 17 children) at four weeks using an instrument with a total range of 0 to 12.
Four weeks to six months
Three studies (83 adults, 14 children) showed that intranasal steroids may improve patient‐reported symptom scores compared with saline irrigation at four weeks to three months (SMD 1.26, 95% CI ‐0.92 to 3.43; 97 participants; three studies; I2 = 95%). We used a random‐effects model due to unexplained heterogeneity (Analysis 3.2).
3.2. Analysis.
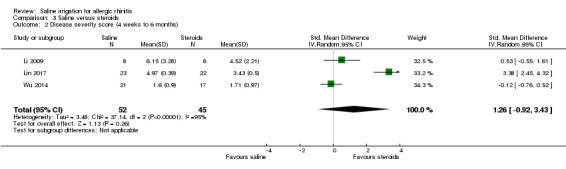
Comparison 3 Saline versus steroids, Outcome 2 Disease severity score (4 weeks to 6 months).
Chen 2014 reported higher mean values for disease severity (more severe symptoms) in the saline group (6.58, 18 children) compared with the intranasal steroid group (4.27, 17 children) at 12 weeks using an instrument with a total range of 0 to 12.
3.2. Significant local adverse effects: epistaxis
One study reported the recording of adverse effects in their methods section although epistaxis was not specifically mentioned as being sought or identified in any of the studies. Of the five studies that mentioned adverse effects in their results, Cordray 2005 (21 adults) reported that two participants withdrew from the study due to adverse effects but they did not provide further information as to the nature of the effects or to which groups the participants were allocated. Wu 2014 (38 adults) mentioned that all treatments were "well tolerated" and Lin 2017 (45 adults) reported that none of the saline irrigation group experienced adverse effects but that 27.3% of the intranasal steroid group reported adverse effects (although none were reported as epistaxis). The remaining two studies only noted that there were no adverse effects in the saline irrigation group; there was no information for the groups allocated to intranasal steroids (Chen 2014; Li 2009).
3.3. Disease‐specific health‐related quality of life
Two studies reported disease‐specific health‐related quality of life:
Wu 2014: used the Rhinoconjunctivitis Quality of Life Questionnaire (RQLQ) (unclear range, lower = better quality of life).
Lin 2017: used the mini‐RQLQ, a shortened version of the RQLQ tool (0 to 84, lower = better quality of life).
Due to these differences, when we performed meta‐analyses that included more than one study we used the SMD.
Four weeks to six months
Two studies (83 adults) indicated that it is uncertain whether there is a difference in disease‐specific quality of life between the saline irrigation and intranasal steroid groups at three months (SMD 0.01, 95% CI ‐0.73 to 0.75; 83 participants; 2 studies; I2 = 65%). We used a random‐effects model due to heterogeneity (Analysis 3.3).
3.3. Analysis.
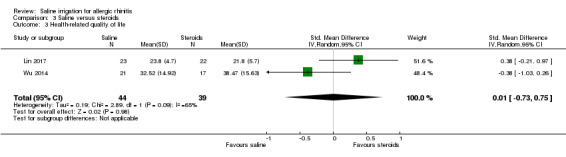
Comparison 3 Saline versus steroids, Outcome 3 Health‐related quality of life.
3.4. Individual symptom scores
No studies reported symptom scores for the individual symptoms of anterior rhinorrhoea (runny nose), posterior rhinorrhoea (post‐nasal drip), nasal blockage/congestion/obstruction, nasal itching or sneezing.
3.5. Generic health‐related quality of life
No studies reported generic health‐related quality of life.
3.6. Any other local adverse effects: local irritation, discomfort
See section 3.2 above. Only Lin 2017 (45 adults) specifically mentioned local irritation or discomfort, where 6/22 (27.3%) of participants using intranasal steroids reported pharyngitis (sore throat) compared to no reports in the group using saline treatment (risk ratio (RR) 0.07, 95% CI 0.00 to 1.24) (Analysis 3.4).
3.4. Analysis.
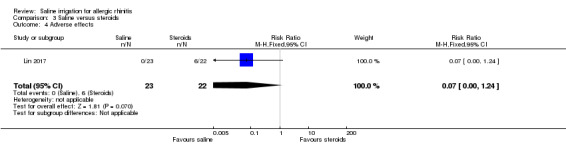
Comparison 3 Saline versus steroids, Outcome 4 Adverse effects.
3.7. Aural symptoms: ear pain, pressure or feeling of fullness
No studies reported aural symptoms of ear pain, pressure or feeling of fullness.
3.8. Endoscopic score (e.g. Lund‐Mackay/Lund‐Kennedy)
No studies reported endoscopic scores.
Comparison 4. Saline versus intranasal antihistamines
One study (40 children) compared saline irrigation with intranasal antihistamines but did not report any of the primary or secondary outcomes of this review (Yasar 2013).
Discussion
Summary of main results
This review includes seven studies comparing nasal saline irrigation with no saline treatment where no background pharmacological treatment was used (Table 1), and four studies comparing saline irrigation with no saline treatment where all participants used pharmacological treatment for allergic rhinitis (intranasal steroids: three studies; oral antihistamines: one study) (Table 2).
Seven studies compared nasal saline irrigation against intranasal steroid treatment. One study compared saline irrigation against intranasal antihistamines but no relevant outcomes were presented.
Saline versus no saline treatment (no background treatment)
There may be an improvement in patient‐reported disease severity with saline irrigation compared to no saline treatment at up to four weeks and at up to eight weeks (low‐quality evidence). It is uncertain whether there are differences between the saline and no saline groups with respect to disease‐specific health‐related quality of life at up to four weeks and at eight weeks (very low‐quality evidence). Of the five studies that made statements about adverse effects, no adverse effects were reported in either the saline arms (five studies) or no saline arms (two studies) (low‐quality evidence). No other prespecified outcomes were reported.
Subgroup analysis for volume indicated that all of the volumes of saline irrigation may have reduced patient symptom severity but there was significant heterogeneity within the results. With respect to tonicity, the effect size for treatment with hypertonic solution was greater than with normal saline, although there was considerable heterogeneity in the results.
Saline plus pharmacological treatment versus pharmacological treatment alone (intranasal steroids or oral antihistamines)
It is uncertain whether there are differences between saline irrigation and no saline treatment, when used alongside pharmacological treatment, in patient‐reported disease severity or disease‐specific health‐related quality of life (very low‐quality evidence). No adverse effects were reported. No other outcomes were reported.
Saline versus intranasal steroids
It is uncertain whether there are differences between saline and intranasal steroid treatment for any of the outcomes reported. The quality of the evidence is very low.
Overall completeness and applicability of evidence
The evidence included studies in both children and adults, including a study in pregnant women. The included saline solutions varied greatly with respect to the volume and tonicity of saline and are likely to be representative of the solutions available in practice.
Adverse effects were not well reported in the included studies. In many studies the methods section did not detail how adverse effects would be defined or recorded, and in many the results just included one statement indicating that 'no adverse effects were reported'. There have been adverse effects reported in other populations using nasal saline irrigation. Cochrane Reviews investigating the use of nasal saline irrigation in people with other conditions have noted the adverse effects of epistaxis and local irritation/discomfort (Chong 2016; King 2015). The author team have identified that in addition to nasal symptoms, people with allergic rhinitis using saline irrigation may also complain of aural symptoms, which could influence their adherence.
The maximum duration of treatment in the studies was three months and so it is not known whether the efficacy in reducing symptoms is maintained over a longer period, or if there are longer‐term adverse effects that were not reported in the studies.
Quality of the evidence
The quality of the evidence for the outcomes as assessed with GRADE is low or very low. The studies were generally small with poor description of methodology. The lack of information about the validation of instruments used to assess patient‐reported disease severity limited our confidence in the results. It is likely that the variety of different saline interventions used within the studies (volumes, tonicity, duration of treatment), and differences in the disease severity scores, resulted in the heterogeneity observed in the results.
Potential biases in the review process
Four of the studies were conducted in China, two of which required translation from Chinese. There may have been other studies published in the Chinese literature that were not identified through our searches.
For the comparison of saline irrigation with no saline treatment, this review did not look at the number of people who required the use of rescue medication during the study, although a number of studies did state that rescue medication (usually oral antihistamines) was allowed. If there was a variation between the two treatment groups with regards to the number requiring rescue medication this may have had an impact on the effect sizes reported, although this is likely to increase the effect size for saline irrigation compared to no saline treatment. Future updates could consider taking this into account; for example, the Chairattananon study used a combined 'nasal symptom and medication' score, which helped to account for this (Chairattananon 2013).
We did not include studies using saline as a 'placebo' treatment in comparison to 'active' allergic rhinitis treatments (such as intranasal steroids). In these studies, which are looking primarily at the efficacy and safety of the 'active' treatment, the characteristics of the saline placebo are often poorly reported. In addition, the saline placebo is often mixed with other excipients to more closely mimic the active intervention.
Agreements and disagreements with other studies or reviews
Comparison with systematic reviews looking at nasal saline irrigation for allergic rhinitis
We found two systematic reviews. Each included both randomised and non‐randomised clinical trials (e.g. before‐after studies). The conclusions of the reviews did not contradict the findings of our review:
Hermelingmeier 2012: "Saline nasal irrigation (SNI) using isotonic solution can be recommended as complementary therapy in AR. It is well tolerated, inexpensive, easy to use, and there is no evidence showing that regular, daily SNI adversely affects the patient’s health or causes unexpected side effects."
Khianey 2012: "Overall, the data appear to demonstrate some small clinical benefit to nasal saline irrigation. Nasal saline irrigation is well tolerated, with minimal side effects. Further definitive studies are needed to optimize efficacy."
Comparison with Cochrane Reviews looking at nasal saline irrigation for other populations
We found two Cochrane Reviews investigating the use of nasal saline irrigation in other populations. Both highlighted the low quality of the evidence as a limiting factor in drawing conclusions.
Chong 2016 investigated nasal saline irrigation in people with chronic rhinosinusitis. The authors only found two studies with very different populations, methods of nasal irrigation and comparisons. They found that the quality of evidence was very low and that it was difficult to draw conclusions.
King 2015 examined the use of nasal saline irrigation in people with upper respiratory tract infections (URTIs). They concluded: "Nasal saline irrigation possibly has benefits for relieving the symptoms of acute URTIs. However, the included trials were generally too small and had a high risk of bias, reducing confidence in the evidence supporting this."
Authors' conclusions
Implications for practice.
For people with allergic rhinitis
There is low‐quality evidence that nasal saline irrigation may have benefits in both adults and children in relieving symptoms of allergic rhinitis compared to no saline treatment. The use of nasal saline irrigation is unlikely to be associated with adverse effects. It is unclear which is the best type of saline irrigation to use with respect to volume, strength and how often to use it.
For clinicians
There is low‐quality evidence that using saline irrigation may reduce patient‐reported disease severity compared with no saline treatment at up to four weeks and between four weeks and three months in both adults and children. The reporting of adverse effects in the studies was very poor but no studies reported adverse effects with the use of saline. This review did not look at direct comparisons of saline type (e.g. volume, tonicity and frequency of administration). No longer‐term outcomes (after three months) were identified. There is a lack of evidence to compare saline irrigation to pharmacological treatments.
For funders
Although saline may be an effective treatment for reducing symptoms of allergic rhinitis (low‐quality evidence), there is generally a lack of information about its use. Further research is needed: this may include both systematic reviews comparing types of saline (volume, tonicity, frequency of administration), as we excluded 15 studies from this review that made these comparisons, and well‐conducted primary trials (see Implications for research).
Implications for research.
Evidence
As of November 2017, we have identified 14 studies that investigated the use of nasal saline irrigation in allergic rhinitis. The studies were generally small (median sample size = 46 participants) and poorly reported. The evidence identified indicates that there may be benefits in terms of patient‐reported disease severity when compared with no saline treatment but the range of unvalidated instruments used, along with heterogeneity in the study characteristics, made it difficult to draw definite conclusions. The reporting of adverse effects was very poor in the studies.
We consider that more research on the use of nasal saline in allergic rhinitis is very important. We propose that the following aspects should be considered when designing trials:
Population
-
Separate trials should be completed in children and in adults as the setting for recruitment and the outcomes are likely to be different.
Children should be recruited from secondary care clinics where better diagnostic testing is available and recruitment is likely to be easier.
Adults could be recruited into large, multicentre, primary care trials, although appropriate diagnosis testing should be a prerequisite.
Trials should be adequately powered and imbalances in prognostic factors (for example, allergen type) must be accounted for in the statistical analysis.
Study participants should bediagnosed with allergic rhinitis using appropriate diagnostic methods including clinical symptoms characteristic of allergic rhinitis with a positive radioallergosorbent test (RAST) or skin prick test (SPT).
Intervention and comparison
Any trial should be pragmatic and consider the use of saline irrigation as an adjunct to pharmacological treatments (such as intranasal steroids and antihistamines).
In adults in primary care, a trial of saline irrigation compared with intranasal corticosteroids could be considered.
Investigators should consider the volume, tonicity, alkalinity, temperature and frequency of administration of the saline irrigation used.
If people with seasonal allergic rhinitis are included within the trial, it should be conducted at a time of the year when symptoms are expected to occur. All trials should be completed for a sufficient duration to determine whether continued use of saline nasal irrigation has additional benefits or harms. Studies should consider investigating the effect of longer‐term use of nasal saline (e.g. more than six months).
Outcomes
Studies should focus on outcomes that are important to people with allergic rhinitis and use validated instruments to measure these, in particular using standard, validated, patient‐reported disease severity scores and disease‐specific health‐related quality of life scores. People may find dichotomised outcomes easiest to interpret; for example, the percentage of participants achieving a minimal clinically important difference (MCID) or improvement for that outcome. Such MCIDs or cut‐off points should be included in the study protocol and clearly outlined in the methods section.
Adverse effects should be defined at the start of the trial and methods for reporting these should be clearly stated in the protocol.
Symptom scores should include both nasal and ocular symptoms (such as eye redness and eye itching) as many people will experience these with allergic rhinitis.
The duration of the trial needs to be carefully considered. The current evidence only includes trials that had up to a three‐month treatment duration. There are still unanswered questions about the benefits and harms of long‐term use of nasal saline for persistent allergic rhinitis.
Trials and other high‐quality studies should use consistent outcomes and adhere to reporting guidelines, such as CONSORT, so that results can be compared across future trials. The development of a standardised set of outcomes, or core outcome set, for allergic rhinitis, agreed by researchers, clinicians and patients, will facilitate this process.
Acknowledgements
We would like to acknowledge Samantha Cox for her input into the Search methods for identification of studies section and Jenny Bellorini for her help with copy editing the review.
We are grateful to Professor Wytske Fokkens for peer reviewing the manuscript and to consumer referee Theresa Wrangham for her helpful comments.
We would also like to thank:
Minsi Cai for translation of Ning 2011;
Yu‐Tian Xiao for translation of Wu 2014;
Jan Strojil for translation of Krcmova 2011.
This project was supported by the National Institute for Health Research, via Cochrane Infrastructure, Cochrane Programme Grant or Cochrane Incentive funding to Cochrane ENT. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
Appendices
Appendix 1. Search strategies
| CENTRAL (CRS Web) | MEDLINE (Ovid) | Embase (Ovid) | Web of Science (Web of Knowledge) |
| 1 MESH DESCRIPTOR Rhinitis AND CENTRAL:TARGET 2 MESH DESCRIPTOR Conjunctivitis AND CENTRAL:TARGET 3 (rhinit* or Rhinoconjunctivitis or conjunctivitis):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 4 #1 OR #2 OR #3 AND CENTRAL:TARGET 5 MESH DESCRIPTOR Allergens EXPLODE ALL AND CENTRAL:TARGET 6 MESH DESCRIPTOR pollen EXPLODE ALL AND CENTRAL:TARGET 7 MESH DESCRIPTOR Hypersensitivity EXPLODE ALL AND CENTRAL:TARGET 8 (allerg* or hypersensitivit* or perennial or nonseason* or season* or pollen* or dust or hair* or dander or mite*):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 9 #5 OR #6 OR #7 OR #8 AND CENTRAL:TARGET 10 #4 AND #9 AND CENTRAL:TARGET 11 MESH DESCRIPTOR Rhinitis, Allergic EXPLODE ALL AND CENTRAL:TARGET 12 MESH DESCRIPTOR Conjunctivitis, Allergic EXPLODE ALL AND CENTRAL:TARGET 13 (hayfever or "hay fever" or pollenosis or pollinosis or SAR or PAR):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 14 #10 OR #11 OR #12 OR #13 AND CENTRAL:TARGET 15 MESH DESCRIPTOR Solutions AND CENTRAL:TARGET 16 MESH DESCRIPTOR Hypertonic Solutions AND CENTRAL:TARGET 17 MESH DESCRIPTOR Saline Solution, Hypertonic EXPLODE ALL AND CENTRAL:TARGET 18 MESH DESCRIPTOR Isotonic Solutions EXPLODE ALL AND CENTRAL:TARGET 19 MESH DESCRIPTOR Sodium Chloride EXPLODE ALL AND CENTRAL:TARGET 20 MESH DESCRIPTOR Mineral Waters EXPLODE ALL AND CENTRAL:TARGET 21 MESH DESCRIPTOR Seawater EXPLODE ALL AND CENTRAL:TARGET 22 MESH DESCRIPTOR Hypotonic Solutions EXPLODE ALL AND CENTRAL:TARGET 23 (saline or "sodium chloride" or saltwater or hypertonic* or hypotonic* or isotonic* or hypersaline or "sea water" or seawater or ((salt* or thermal or mineral or sulfur* or bromic or iodic* or bromide or iodine or bromine) and (water* or solution*))):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 24 #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 AND CENTRAL:TARGET 25 MESH DESCRIPTOR Therapeutic Irrigation AND CENTRAL:TARGET 26 MESH DESCRIPTOR Nasal Lavage EXPLODE ALL AND CENTRAL:TARGET 27 MESH DESCRIPTOR Administration, Inhalation EXPLODE ALL AND CENTRAL:TARGET 28 MESH DESCRIPTOR Administration, Intranasal EXPLODE ALL AND CENTRAL:TARGET 29 MESH DESCRIPTOR Nasal Sprays EXPLODE ALL AND CENTRAL:TARGET 30 MESH DESCRIPTOR Buffers EXPLODE ALL AND CENTRAL:TARGET 31 ((douch* or spray* or lavag* or wash* or rinse* or rinsing or irrigat* or pulsed or nebulise* or aerosol* or buffer* or atomis* or atomiz* or (squeeze and bottle))):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 32 ((intranasal or inhalation* or irrigator)):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 33 #25 or #26 or #27 or #28 or #29 or #30 or #31 or #32 AND CENTRAL:TARGET 34 #24 and #33 AND CENTRAL:TARGET 35 ((sterimar or NeilMed or nasaline or navage or marimer or physiomer or Emcur or "simply saline" or "nasal mist" or ayr or salex or "otrovin saline" or ISCS or Prorhinel or SSBI)):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 36 ((nasal or intranasal or sinus or nose or sinonasal) ADJ3 (irrigation* or rinsing or rinse* or wash* or lavage or douch* or hygiene)):AB,EH,KW,KY,MC,MH,TI,TO AND CENTRAL:TARGET 37 MESH DESCRIPTOR Mineral Waters EXPLODE ALL WITH QUALIFIER TU AND CENTRAL:TARGET 38 #34 or #35 or #36 or #37 AND CENTRAL:TARGET 39 #14 and #38 AND CENTRAL:TARGET |
1 Rhinitis/ 2 Conjunctivitis/ 3 (rhinit* or Rhinoconjunctivitis or conjunctivitis).ab,kf,ti. 4 1 or 2 or 3 5 exp Allergens/ 6 exp Pollen/ 7 exp Hypersensitivity/ 8 (allerg* or hypersensitivit* or perennial or nonseason* or season* or pollen* or dust or hair* or dander or mite*).ab,kf,ti. 9 5 or 6 or 7 10 4 and 9 11 exp Rhinitis, Allergic/ 12 exp Conjunctivitis, Allergic/ 13 (hayfever or "hay fever" or pollenosis or pollinosis or SAR or PAR).ab,kf,ti. 14 10 or 11 or 12 or 13 15 Solutions/ 16 Hypertonic Solutions/ 17 exp Saline Solution, Hypertonic/ 18 exp isotonic solutions/ 19 exp Sodium Chloride/ 20 exp Mineral Waters/ 21 exp seawater/ 22 exp Hypotonic Solutions/ 23 (saline or "sodium chloride" or saltwater or hypertonic* or hypotonic* or isotonic* or hypersaline or "sea water" or seawater or ((salt* or thermal or mineral or sulfur* or bromic or iodic* or bromide or iodine or bromine) and (water* or solution*))).ab,kf,ti. 24 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 25 Therapeutic Irrigation/ 26 exp Nasal Lavage/ 27 exp Administration, Inhalation/ 28 exp Administration, Intranasal/ 29 exp Nasal Sprays/ 30 exp Buffers/ 31 (douch* or spray* or lavag* or wash* or rinse* or rinsing or irrigat* or pulsed or nebulise* or aerosol* or buffer* or atomis* or atomiz* or (squeeze and bottle)).ab,kf,ti. 32 (intranasal or inhalation* or irrigator).ab,kf,ti. 33 25 or 26 or 27 or 28 or 29 or 30 or 31 or 32 34 24 and 33 35 (sterimar or NeilMed or nasaline or navage or marimer or physiomer or Emcur or "simply saline" or "nasal mist" or ayr or salex or "otrovin saline" or ISCS or Prorhinel or SSBI).ab,kf,ti. 36 ((nasal or intranasal or sinus or nose or sinonasal) adj3 (irrigation* or rinsing or rinse* or wash* or lavage or douch* or hygiene)).ab,kf,ti. 37 exp Mineral Waters/tu [Therapeutic Use] 38 34 or 35 or 36 or 37 39 14 and 38 |
1 rhinitis/ 2 conjunctivitis/ 3 (rhinit* or Rhinoconjunctivitis or conjunctivitis).ab,kw,ti. 4 1 or 2 or 3 5 exp allergen/ 6 exp pollen/ 7 exp hypersensitivity/ 8 (allerg* or hypersensitivit* or perennial or nonseason* or season* or pollen* or dust or hair* or dander or mite*).ab,kw,ti. 9 5 or 6 or 7 or 8 10 4 and 9 11 exp allergic rhinitis/ 12 exp allergic conjunctivitis/ 13 (hayfever or "hay fever" or pollenosis or pollinosis or SAR or PAR).ab,kw,ti. 14 10 or 11 or 12 or 13 15 "solution and solubility"/ 16 exp hypertonic solution/ 17 exp sodium chloride/ 18 exp isotonic solution/ 19 exp mineral water/ 20 exp sea water/ 21 exp hypotonic solution/ 22 (saline or "sodium chloride" or saltwater or hypertonic* or hypotonic* or isotonic* or hypersaline or "sea water" or seawater or ((salt* or thermal or mineral or sulfur* or bromic or iodic* or bromide or iodine or bromine) and (water* or solution*))).ab,kw,ti. 23 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 24 lavage/ 25 exp nasal lavage/ 26 exp inhalational drug administration/ 27 exp intranasal drug administration/ 28 exp nose spray/ 29 exp buffer/ 30 (douch* or spray* or lavag* or wash* or rinse* or rinsing or irrigat* or pulsed or nebulise* or aerosol* or buffer* or atomis* or atomiz* or (squeeze and bottle)).ab,kw,ti. 31 (intranasal or inhalation* or irrigator).ab,kw,ti. 32 24 or 25 or 26 or 27 or 28 or 29 or 30 or 31 33 23 and 32 34 (sterimar or NeilMed or nasaline or navage or marimer or physiomer or Emcur or "simply saline" or "nasal mist" or ayr or salex or "otrovin saline" or ISCS or Prorhinel or SSBI).ab,kw,ti. 35 ((nasal or intranasal or sinus or nose or sinonasal) adj3 (irrigation* or rinsing or rinse* or wash* or lavage or douch* or hygiene)).ab,kw,ti. 36 33 or 34 or 35 37 14 and 36 |
#1 TOPIC: (rhinit* or Rhinoconjunctivitis or conjunctivitis) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #2 TOPIC: (allerg* or hypersensitivit* or perennial or nonseason* or season* or pollen* or dust or hair* or dander or mite*) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #3 #2 AND #1 Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #4 TOPIC: (hayfever or "hay fever" or pollenosis or pollinosis) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #5 #4 OR #3 Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #6 TOPIC: ((saline or "sodium chloride" or saltwater or hypertonic* or hypotonic* or isotonic* or hypersaline or "sea water" or seawater or ((salt* or thermal or mineral or sulfur* or bromic or iodic* or bromide or iodine or bromine) and (water* or solution*)))) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #7 TOPIC: ((douch* or spray* or lavag* or wash* or rinse* or rinsing or irrigat* or pulsed or nebulise* or aerosol* or buffer* or atomis* or atomiz* or (squeeze and bottle))) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #8 TOPIC: ((intranasal or inhalation* or irrigator)) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #9 #8 OR #7 Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #10 #9 AND #6 Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #11 TOPIC: ((sterimar or NeilMed or nasaline or navage or marimer or physiomer or Emcur or "simply saline" or "nasal mist" or ayr or salex or "otrovin saline" or ISCS or Prorhinel or SSBI)) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #12 TOPIC: ((nasal or intranasal or sinus or nose or sinonasal) NEAR/3 (irrigation* or rinsing or rinse* or wash* or lavage or douch* or hygiene)) Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #13 #12 OR #11 OR #10 Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years #14 #13 AND #5 Indexes=SCI‐EXPANDED, CPCI‐S Timespan=All years |
| CINAHL (EBSCO) | ICTRP | ClinicalTrials.gov | LILACS |
| S37 S14 AND S36 S36 S32 OR S33 OR S34 OR S35 S35 (MH "Mineral Water/TU") S34 TX (nasal or intranasal or sinus or nose or sinonasal) N3 (irrigation* or rinsing or rinse* or wash* or lavage or douch* or hygiene) S33 TX (sterimar or NeilMed or nasaline or navage or marimer or physiomer or Emcur or "simply saline" or "nasal mist" or ayr or salex or "otrovin saline" or ISCS or Prorhinel or SSBI) S32 S23 AND S31 S31 S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 S30 TX (intranasal or inhalation* or irrigator) S29 TX (douch* or spray* or lavag* or wash* or rinse* or rinsing or irrigat* or pulsed or nebulise* or aerosol* or buffer* or atomis* or atomiz* or (squeeze and bottle)) S28 (MH “Buffers+”) S27 (MH “Administration, Intranasal+”) S26 (MH “Administration, Inhalation+”) S25 (MH “Nasal Lavage+”) S24 (MH “Therapeutic Irrigation”) S23 S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 S22 TX saline or "sodium chloride" or saltwater or hypertonic* or hypotonic* or isotonic* or hypersaline or "sea water" or seawater or ((salt* or thermal or mineral or sulfur* or bromic or iodic* or bromide or iodine or bromine) and (water* or solution*)) S21 (MH “Hypotonic Solutions+”) S20 (MH "Mineral Water") S19 (MH “Sodium Chloride+”) S18 (MH “isotonic solutions+”) S17 (MH “Saline Solution, Hypertonic+”) S16 (MH “Hypertonic Solutions”) S15 (MH “Solutions”) S14 S10 OR S11 OR S12 OR S13 S13 TX hayfever or "hay fever" or pollenosis or pollinosis or SAR or PAR S12 (MH “Conjunctivitis, Allergic+”) S11 (MH "Rhinitis, Allergic, Perennial") OR (MH "Rhinitis, Allergic, Seasonal") S10 S8 AND S9 S9 S4 OR S5 OR S6 OR S7 S8 S1 OR S2 OR S3 S7 TX allerg* or hypersensitivit* or perennial or nonseason* or season* or pollen* or dust or hair* or dander or mite*) S6 (MH “Hypersensitivity+”) S5 (MH “Pollen+”) S4 (MH "Allergens+") S3 TX rhinit* or Rhinoconjunctivitis or conjunctivitis S2 (MH “Conjunctivitis”) S1 (MH "Rhinitis") |
rhinit* AND saline OR rhinit* AND salt AND water OR hayfever AND saline OR hayfever AND salt AND water |
via CRS Web 1 (rhinit* or Rhinoconjunctivitis or conjunctivitis or hayfever or "hay fever" or pollenosis or pollinosis or SAR or PAR):AB,EH,KW,KY,MC,MH,TI,TO AND INSEGMENT 2 (saline or "sodium chloride" or saltwater or hypertonic* or hypotonic* or isotonic* or hypersaline or "sea water" or seawater or ((salt* or thermal or mineral or sulfur* or bromic or iodic* or bromide or iodine or bromine) and (water* or solution*))):AB,EH,KW,KY,MC,MH,TI,TO AND INSEGMENT 3 (sterimar or NeilMed or nasaline or navage or marimer or physiomer or Emcur or "simply saline" or "nasal mist" or ayr or salex or "otrovin saline" or ISCS or Prorhinel or SSBI):AB,EH,KW,KY,MC,MH,TI,TO AND INSEGMENT 4 (nasal or intranasal or sinus or nose or sinonasal) AND (irrigation* or rinsing or rinse* or wash* or lavage or douch* or hygiene):AB,EH,KW,KY,MC,MH,TI,T AND INSEGMENT 5 #2 OR #3 OR #4 6 #1 AND #5 7 (nct*):AU AND INSEGMENT 8 #6 AND #7 via Clincialtrials.gov ( rhinitis OR hayfever OR Rhinoconjunctivitis OR pollenosis OR pollinosis OR "hay fever" ) AND ( saline OR salt AND water OR “sodium chloride” OR saltwater OR hypertonic OR hypotonic OR isotonic OR hypersaline OR "sea water" OR seawater OR sterimar OR NeilMed OR nasaline OR navage OR marimer OR physiomer OR Emcur OR "nasal mist" OR ayr OR salex OR "otrovin saline" OR ISCS OR Prorhinel OR SSBI OR irrigation OR rinsing OR rinse OR wash OR lavage OR douch OR douching OR hygiene OR salt AND solution ) | Interventional Studies |
(TW:rhinit* OR TW:rinit OR TW:hayfever OR TW:”hay fever” OR TW:pollinosis OR TW:pollenosis) AND (TW:salin* OR TW: water* OR TW: Agua*) |
Appendix 2. Data extraction form
| REF ID: | Study title: |
| Date of extraction: | Extracted by: |
| General comments/notes (internal for discussion): |
| Flow chart of trial | ||
| Group A (Intervention) | Group B (Comparison) | |
| No. of people screened | ||
| No. of participants randomised ‐ all | ||
| No. randomised to each group | ||
| No. receiving treatment as allocated | ||
| No. not receiving treatment as allocated ‐ Reason 1 ‐ Reason 2 |
||
| No. dropped out (no follow‐up data for any outcome available) |
||
| No. excluded from analysis1 (for all outcomes) ‐ Reason 1 ‐ Reason 2 |
||
| 1This should be the people who received the treatment and were therefore not considered 'dropouts' but were excluded from all analyses (e.g. because the data could not be interpreted or the outcome was not recorded for some reason). | ||
| Information to go into 'Characteristics of included studies' table | |
| Methods | X arm, double/single/non‐blinded, [multicentre] parallel‐group/cross‐over/cluster‐RCT, with x duration of treatment and x duration of follow‐up |
| Participants |
Location: country, no. of sites etc. Setting of recruitment and treatment: Sample size:
Participant (baseline) characteristics:
Inclusion criteria:[state diagnostic criteria used for allergic rhinitis, polyps score if available] Exclusion criteria: |
| Interventions |
Intervention (n = x): intervention name including tonicity, method of administration [including volume], frequency of administration, duration of treatment Comparator group (n = y): Use of additional interventions (common to both treatment arms): |
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Secondary outcomes:
Other outcomes reported by the study:
|
| Funding sources | 'No information provided'/'None declared'/State source of funding |
| Declarations of interest | 'No information provided'/'None declared'/State conflict |
| Notes | |
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Quote: "…" Comment: |
|
| Allocation concealment (selection bias) | Quote: "…" Comment: |
|
| Blinding of participants and personnel (performance bias) | Quote: "…" Comment: |
|
| Blinding of outcome assessment (detection bias) | Quote: "…" Comment: |
|
| Incomplete outcome data (attrition bias) | Quote: "…" Comment: |
|
| Selective reporting (reporting bias) | Quote: "…" Comment: |
|
| Other bias (see section 8.15) Insensitive/non‐validated instrument? |
Quote: "…" Comment: |
|
| Other bias (see section 8.15) | Quote: "…" Comment: |
| Findings of study: continuous outcomes | |||||||
| Results (continuous data table) | |||||||
| Outcome | Group A | Group B | Other summary stats/Notes | ||||
| Mean | SD | N | Mean | SD | N | Mean difference (95% CI), P values etc. | |
| Disease‐specific HRQL (instrument name/range) Time point: |
|||||||
| Generic HRQL (instrument name/range) Time point: |
|||||||
| Symptom score (overall) (instrument name/range) Time point: |
|||||||
|
Added total ‐ if scores reported separately for each symptom (range) Time point: |
|||||||
| Nasal blockage/obstruction/congestion (instrument name/range) |
|||||||
| Nasal discharge (anterior or posterior rhinorrhoea ‐ specify which one if it is known) (instrument name/range) |
|||||||
| Sneezing (instrument name/range) |
|||||||
| Nasal itching (instrument name/range) |
|||||||
| Endoscopic score (instrument name/range) |
|||||||
| Comments: | |||||||
| Results (dichotomous data table) | ||||||
| Outcome | Intervention | Group A | Group B | Other summary stats/notes | ||
| No. of people with events | No. of people analysed | No. of people with events | No. of people analysed | P values, RR (95% CI), OR (95% CI) | ||
| Epistaxis/nosebleed | Nasal saline | |||||
| Local irritation (sore throat, oral thrush, discomfort) | Nasal saline | |||||
| Local adverse effects: Eustachian tube dysfunction | Nasal saline | |||||
| The following adverse effects will only be extracted if the comparison arm is one of the interventions indicated | ||||||
| Osteoporosis (minimum 6 months) | INCS | |||||
| Stunted growth (children, minimum 6 months) | INCS | Can also be measured as average height | ||||
| Mood disturbances | Oral steroids | |||||
| Gastrointestinal disturbances (diarrhoea, nausea, vomiting, stomach irritation) | Oral steroids Antibiotics |
|||||
| Insomnia | Oral steroids | |||||
| Osteoporosis (minimum 6 months) | INCS Oral steroids |
|||||
| Skin irritation | Antibiotics | |||||
| Anaphylaxis or other serious allergic reactions such as Stevens‐Johnson syndrome | Antibiotics | |||||
| Antihistamine and decongestant adverse effects: somnolence, irritability, insomnia, rhinitis medicamentosa, prolonged middle ear effusion | Antihistamines/decongestants | |||||
| Comments: | ||||||
Data and analyses
Comparison 1. Saline versus no saline treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Disease severity score (up to 4 weeks) | 6 | 407 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.32 [‐1.84, ‐0.81] |
| 1.1 Children | 4 | 322 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.07 [‐1.39, ‐0.74] |
| 1.2 Adults | 2 | 85 | Std. Mean Difference (IV, Random, 95% CI) | ‐2.06 [‐3.80, ‐0.32] |
| 2 Disease severity score (4 weeks to 6 months) | 5 | 167 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.44 [‐2.39, ‐0.48] |
| 2.1 Children | 3 | 102 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.06 [‐2.13, 0.01] |
| 2.2 Adults | 2 | 65 | Std. Mean Difference (IV, Random, 95% CI) | ‐2.02 [‐3.79, ‐0.25] |
| 3 Health‐related quality of life | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 3.1 Up to 4 weeks | 1 | 42 | Mean Difference (IV, Fixed, 95% CI) | ‐3.32 [‐11.35, 4.71] |
| 3.2 4 weeks to 6 months | 1 | 42 | Mean Difference (IV, Fixed, 95% CI) | ‐2.06 [‐8.38, 4.26] |
Comparison 2. Saline versus no saline treatment (adjuvant to intranasal steroids or oral antihistamines).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Disease severity score (up to 4 weeks) | 2 | 32 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.60 [‐1.34, 0.15] |
| 1.1 Steroids as adjuvant treatment | 1 | 18 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.32 [‐1.31, 0.67] |
| 1.2 Antihistamines as adjuvant treatment | 1 | 14 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.95 [‐2.08, 0.17] |
| 2 Disease severity score (4 weeks to 6 months)) | 2 | 58 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.32 [‐0.85, 0.21] |
| 2.1 Steroids as adjuvant treatment | 2 | 58 | Std. Mean Difference (IV, Fixed, 95% CI) | ‐0.32 [‐0.85, 0.21] |
| 3 Health‐related quality of life (4 weeks to 6 months) | 2 | 54 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.26 [‐2.47, ‐0.05] |
| 3.1 Steroids as adjuvant treatment | 1 | 40 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.78 [‐1.43, ‐0.13] |
| 3.2 Antihistamines as adjuvant treatment | 1 | 14 | Std. Mean Difference (IV, Random, 95% CI) | ‐2.05 [‐3.43, ‐0.67] |
Comparison 3. Saline versus steroids.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Disease severity score (up to 4 weeks) | 1 | 14 | Mean Difference (IV, Fixed, 95% CI) | 1.06 [‐1.65, 3.77] |
| 2 Disease severity score (4 weeks to 6 months) | 3 | 97 | Std. Mean Difference (IV, Random, 95% CI) | 1.26 [‐0.92, 3.43] |
| 3 Health‐related quality of life | 2 | 83 | Std. Mean Difference (IV, Random, 95% CI) | 0.01 [‐0.73, 0.75] |
| 4 Adverse effects | 1 | 45 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.07 [0.00, 1.24] |
Comparison 4. Subgroup comparison ‐ volume.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Disease severity score (up to 4 weeks) | 6 | 407 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.32 [‐1.84, ‐0.81] |
| 1.1 Very low‐volume | 3 | 100 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.96 [‐1.39, ‐0.52] |
| 1.2 Low‐volume | 2 | 265 | Std. Mean Difference (IV, Random, 95% CI) | ‐2.07 [‐3.73, ‐0.42] |
| 1.3 High‐volume | 1 | 42 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.92 [‐1.56, ‐0.28] |
| 2 Disease severity score (4 weeks to 6 months) | 5 | 167 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.44 [‐2.39, ‐0.48] |
| 2.1 Very low‐volume | 3 | 80 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.33 [‐2.22, ‐0.44] |
| 2.2 Low‐volume | 1 | 45 | Std. Mean Difference (IV, Random, 95% CI) | ‐2.91 [‐3.77, ‐2.05] |
| 2.3 High‐volume | 1 | 42 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.41 [‐1.02, 0.21] |
Comparison 5. Subgroup comparison ‐ tonicity.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Disease severity score (up to 4 weeks) | 6 | 407 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.45 [‐2.13, ‐0.78] |
| 1.1 Physiologic (0.9% saline) | 2 | 152 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.82 [‐1.18, ‐0.47] |
| 1.2 Hypertonic (> 0.9% saline) | 5 | 255 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.72 [‐2.62, ‐0.82] |
| 2 Disease severity score (4 weeks to 6 months) | 4 | 147 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.52 [‐2.70, ‐0.33] |
| 2.1 Physiologic (0.9% saline) | 1 | 42 | Std. Mean Difference (IV, Random, 95% CI) | ‐0.41 [‐1.02, 0.21] |
| 2.2 Hypertonic (> 0.9% saline) | 3 | 105 | Std. Mean Difference (IV, Random, 95% CI) | ‐1.91 [‐3.14, ‐0.68] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Chairattananon 2013.
| Methods | 2‐arm, non‐blinded, parallel‐group RCT, with 8 weeks duration of treatment and follow‐up | |
| Participants |
Location: Bangkok, Thailand Setting of recruitment and treatment: secondary care: Department of Allergy and Immunology, Paediatric Department Sample size: 48
Participant (baseline) characteristics:
Inclusion criteria: aged between 5 and 15 years with: (1) clinical diagnosis of allergic rhinitis (ARIA guideline) (2) positive skin prick test to one or more of common aeroallergens, house dust mite, cockroach, cat, dog, grass, moulds) and/or specific IgE to aeroallergens (3) combined daily total nasal symptom score and medication score (CSM) at randomisation between 3 to 9 (mild to moderate symptoms) Exclusion criteria: (1) Use of intranasal steroids more than 3 times per week for 2 weeks prior to enrolment (2) Use of nasal irrigation for at least 1 month or more than 3 times per week for 1 month prior to entry (3) Uncontrolled asthma, sinusitis, severe nasal septum deviation, intolerance to nasal saline irrigation, severe symptoms need to be treat with intranasal corticosteroid |
|
| Interventions |
Intervention (n = 25): isotonic saline nasal irrigation, 90 mL per nostril twice per day for 8 weeks. Irrigation was done via a Hashi® Nasal Rinser. Comparator group (n = 23): no saline solution Use of additional interventions (common to both treatment arms): participants were prescribed cetirizine and pseudoephedrine as needed |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Secondary outcomes: none reported Other outcomes reported by the study:
|
|
| Funding sources | No information provided | |
| Declarations of interest | No information provided | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The computer generated random numbers with block randomization in two groups were used." Comment: adequate information about randomisation schedule |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information about allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: the study was not blinded |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: it does not appear that the outcome assessors were blinded to treatment group |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: 6 participants (14.3%) did not finish the trial. These were evenly split between the groups (3 participants in each group) and reasons were provided. |
| Selective reporting (reporting bias) | Unclear risk | Comment: no protocol was identified on ClinicalTrials.gov or the Thai registry of clinical trials, although a trial protocol is mentioned in the results. One outcome was presented in the results section, but was not mentioned in the methods (e.g. use of antibiotics). There is a difference between the previously published abstract and the full paper with regards to the quality of life instrument used. There is no overall range given for the quality of life instrument used. |
| Other bias (Non validated instruments) | Unclear risk | Comment: there is a link to a paper for the quality of life instrument (RCQ‐36) but the scoring system appears to be different and no explanation is given as to why a 0 to 4 scale (rather than a 1 to 5 scale) is used |
| Other bias | Low risk | Comment: no other sources of bias were identified |
Chen 2014.
| Methods | 3‐arm, non‐blinded, parallel‐group RCT, with 12‐week duration of treatment and follow‐up | |
| Participants |
Location: Shanghai, China Setting of recruitment and treatment: secondary care: Department of Otolaryngology at Shanghai Children Hospital Sample size: 61
Participant (baseline) characteristics:
Inclusion criteria: the diagnosis of allergic rhinitis was confirmed by history, physical examination and skin prick tests for a battery of common allergens Exclusion criteria: marked septum deviation, prior nasal surgery, nasal polyposis and symptoms of infection |
|
| Interventions |
Intranasal steroid group (n = 17): 200 μg fluticasone propionate nasal spray (Flonase, GlaxoSmithKline UK) daily for 4 weeks, followed by administration of 100 mg daily for 4 weeks and 50 mg daily for another 4 weeks Seawater saline group (n = 18): 4 to 6 sprays of seawater, twice a day for nasal irrigation from a commercial positive‐pressure nasal irrigation applicator (Nasal Cleaner; physiological seawater, Nantong Apon Medical Appliance Co., China). Treatment for 12 weeks. Intranasal steroid PLUS seawater saline group (n = 26): both interventions as above for 12 weeks Use of additional interventions (common to both treatment arms): no information provided |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Other outcomes reported by the study:
|
|
| Funding sources | “This study was supported by a Project of the Shanghai Committee of Science and Technology, China (Grant No. 12411952407).” | |
| Declarations of interest | No information provided | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: "…randomly assigned…" Comment: unclear methods of randomisation. Some concern that there were more participants in the combination group compared with the other treatment groups but because of the small sample size it is difficult to know if this is by chance. There is no information about the baseline characteristics of the participants in the text. |
| Allocation concealment (selection bias) | Unclear risk | Comment: there is no information regarding allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: this was an open study and no blinding was completed |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: there was no blinding and the main outcome was a patient‐reported symptom score and so some bias in the results may have occurred. People who were in the combined group will have known they were receiving 'double' treatment. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: no withdrawals were reported. However, there is not enough information to determine if all of the participants included in the trial completed, or if there were some lost to follow‐up. |
| Selective reporting (reporting bias) | High risk | Comment: no protocol could be identified on ClinicalTrials.gov or the Chinese clinical trials registry (chictr.org.cn). The outcomes reported in the methods section are presented although only in graphical form. No standard deviations for the symptom scores are provided. Precise P values are not provided. |
| Other bias (Non validated instruments) | Unclear risk | Comment: it is unclear whether the symptom scoring system used is validated. The paper provides a table with a reference to an external paper but there is no related reference in the bibliography, so it is not possible to check. |
| Other bias | Unclear risk | Comment: no other sources of bias were identified |
Cordray 2005.
| Methods | 3‐arm, single‐blinded, parallel‐group RCT, with 7‐day duration of treatment and follow‐up | |
| Participants |
Location: Oklahoma, USA Setting of recruitment and treatment: primary care: family practice Sample size: 21
Participant (baseline) characteristics:
Inclusion criteria: 18 years of age and experienced at least 2 of the 6 symptoms (nasal stuffiness, watery/itchy eyes, rhinorrhoea, sneezing, postnasal drainage and itchy throat/cough) at presentation and had to have a positive skin puncture test for seasonal allergies Exclusion criteria: chronic sinusitis, nasal polyposis, a deviated nasal septum or history of nasal septal perforation and recent nasal or sinus surgery; the use of an antihistamine, cromolyn, decongestant, or a topical or systemic corticosteroid within the preceding 2 weeks or an immunotherapeutic agent within the preceding 2 years |
|
| Interventions |
Dead Sea saline (n = 5): intranasal hypertonic Dead Sea saline spray, 2 sprays into each nostril 3 times daily for 7 days. No volume given. Intranasal corticosteroid group (n = 5): aqueous triamcinolone spray (110 μg into each nostril once daily) for 7 days ‘Control’ normal saline group (n = 5): nasal saline spray, 2 sprays into each nostril 3 times daily for 7 days Use of additional interventions (common to both treatment arms): none stated. The use of antihistamines was not allowed during treatment. |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Other outcomes reported by the study: None reported |
|
| Funding sources | No information provided | |
| Declarations of interest | No information provided | |
| Notes | The RQLQ is a validated instrument containing 28 questions regarding 7 domains: activities, sleep, practical problems, nasal symptoms, eye symptoms and other symptoms. For each domain, participants rate themselves as to how much their symptoms have affected them during the previous week on a scale of 0 to 6 (0 = no effect on quality of life). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: "Patients were randomised…" Comment: no information regarding the process for randomisation. 21 people were enrolled in the study and 15 people were randomised. No information given about the baseline characteristics per group. |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information regarding the processes used for allocating the participants to groups and whether the investigating clinicians could have influenced this |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "…single‐blind, placebo controlled study…." Comment: although the paper states that the trial was single‐blind, it provides no information regarding who was blinded and how this was maintained given the intranasal steroid intervention had different a different frequency of administration to the saline groups |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: there is a lack of information regarding who was blinded and how the blinding was maintained given the different intervention regimens |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "During the study, 6 of the 21 participants withdrew" Comment: 6/21 (28.6%) of participants withdrew. The overall reasons for dropping out were listed but as the paper did not give the number randomised to each group or the numbers withdrawing from each group there may be bias. |
| Selective reporting (reporting bias) | High risk | Comment: no protocol for the trial was identified on ClinicalTrials.gov. Although the results present the values for the results before and after treatment, no standard deviations are provided and no information regarding the difference between groups was included. Reporting of adverse effects was not completed well. The paper reports that 2 participants withdrew due to adverse reactions but no information was provided regarding what the events were, nor which groups the participants were allocated to. |
| Other bias (Non validated instruments) | Low risk | Quote: "The RQLQ is a reliable, validated instrument with strong discriminative properties" |
| Other bias | Unclear risk | Comment: there is a general lack of information provided in the paper regarding how the interventions were applied (tonicity, volume of saline sprays), the process of randomisation, numbers randomised to each group, the numbers dropping out from each group and how that would have affected the results, the baseline characteristics for each group. |
Di Berardino 2017.
| Methods | 2‐arm, non‐blinded, single‐centre, parallel‐group RCT, with 2 periods of 6 days each, one during low pollen season (1 to 7 April) and one during peak pollen season (27 April to 3 May), duration of treatment and follow‐up (duration of pollen season) | |
| Participants |
Location: Italy Setting of recruitment and treatment: unclear setting: University of Milan Sample size: 40
Participant (baseline) characteristics:
Inclusion criteria: (a) a typical clinical history of seasonal allergic rhinoconjunctivitis, and (b) marked positivity of the skin‐prick test results (wheal > 5 mm) to grass pollen extracts in a hydroglyceric solution titrated at 30,000 biologic units/mL according to the established guidelines Exclusion criteria: (a) the coexistence of nasal polyposis and/or bronchial asthma, (b) sensitisation to other allergens, (c) previous specific immunotherapy, (d) chronic use of nasal decongestants or corticosteroids and (e) smoking |
|
| Interventions |
Intervention (n = 20): atomised hypertonic phosphate‐buffered solution, at pH 6.1 (Atomix; Tred, Milan, Italy), one puff (0.13 mL) in both nostrils 3 times per day, duration = 6 days in low pollen season (1 to 7 April) and 6 days in the peak pollen season (27 April to 3 May) Comparator group (n = 20): no saline Use of additional interventions (common to both treatment arms): antihistamines when needed (cetirizine 10 mg once a day). Participants were asked to record the frequency of administration and dosage as well. |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Secondary outcomes: none listed Other outcomes reported by the study: Mucociliary clearance, ocular symptoms, consumption of antihistamines |
|
| Funding sources | "No external funding sources reported.” | |
| Declarations of interest | "The authors have no conflicts of interest to declare pertaining to this article.” | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The patients were randomly divided into two groups according to the randomization tables." Comment: adequate sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Comment: there is no information regarding the allocation concealment in this study |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: it does not appear that the participants or healthcare professionals in this study were blinded to treatment group |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: it does not appear that outcome assessors in this study were blinded to treatment group |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: it does not appear that any participant who was randomised failed to compete the study |
| Selective reporting (reporting bias) | Low risk | Comment: no protocol was mentioned in the paper or found on ClinicalTrials.gov or the European Clinical Trials Registry How the nasal symptom score was measured and summarised is not well described in the paper and no overall range of scores is given in the paper. However, these data were provided by personal communication with the authors. |
| Other bias (Non validated instruments) | Unclear risk | Comment: it is not clear if the instrument used to measure the nasal symptoms was validated. It is a different scale to those used in other papers. |
| Other bias | Low risk | Comment: no other risk of bias identified |
Garavello 2003.
| Methods | 2‐arm, non‐blinded, parallel‐group RCT, with 6 weeks duration of treatment and follow‐up | |
| Participants |
Location: Italy Setting of recruitment and treatment: secondary care: Department of Otolaryngology, San Gerardo Hospital Sample size: 20
Participant (baseline) characteristics:
Inclusion criteria: (1) typical anamnesis for seasonal allergic rhinitis for at least 2 years; (2) positive prick tests to Parietaria pollen extracts in a hydroglyceric solution titrated at 20.00 biological units (BU)/ml; (3) positive RAST to Parietaria pollens of at least class 2 Exclusion criteria: presence of symptoms of asthma, urticaria or eczema, a clinically relevant sensitisation to other allergens and the use of specific immunotherapy within the past 2 years |
|
| Interventions |
Intervention (n = 10): hypertonic saline solution (3%), room temperature, 2.5 mL in each nostril administered by disposable syringe, 3 times daily for 6 weeks Comparator group (n = 10): no saline solution Use of additional interventions (common to both treatment arms): participants were allowed to use oral antihistamines as rescue medications. The use was recorded and presented as an outcome. |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Secondary outcomes: none reported Other outcomes reported by the study:
|
|
| Funding sources | No information provided | |
| Declarations of interest | No information provided | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "…randomization was performed according to a computer‐generated list unknown to the physicians." Comment: adequate generation of randomised schedule |
| Allocation concealment (selection bias) | Low risk | Quote: "…randomization was performed according to a computer‐generated list unknown to the physicians." Comment: clinicians were unaware of the randomisation schedule during randomisation |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: participants were not blinded to treatment |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: participants were not blinded to treatment. Given the main outcome was participant‐reported this may have influenced the results. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: all randomised participants completed the trial |
| Selective reporting (reporting bias) | Low risk | Comment: no protocol available on ClinicalTrials.gov or European Clinical Trial Registry All outcomes listed in the methods section are reported in the results section |
| Other bias (Non validated instruments) | Unclear risk | Comment: it is unclear whether the symptom scoring system is a validated scale |
| Other bias | Low risk | Comment: no other sources of bias were identified |
Garavello 2005.
| Methods | 2‐arm, non‐blinded, parallel‐group RCT, with 7‐week duration of treatment and follow‐up | |
| Participants |
Location: Italy Setting of recruitment and treatment: not stated Sample size: 44
Participant (baseline) characteristics:
Inclusion criteria: 1) typical anamnesis for seasonal allergic rhinoconjunctivitis; 2) marked positivity of the skin prick tests (≥ 2 plus) to grass pollen extracts in a hydroglyceric solution titrated at 20,000 biological units Exclusion criteria: 1) presence of nasal polyposis and/or bronchial asthma; b) sensitisation to other allergens and c) previous specific immunotherapy |
|
| Interventions |
Intervention (n = 22): nasal rinsing 3 times daily. Each rinsing consisted of 3 sprays per nostril (1 spray = x50 μL) nebulised at a mass median aerodynamic diameter of about 18 μm. Solution was hypertonic saline solution (NaCl 3%, 925 ± 30 mosm/kg, pH 7.45 ± 0.2) in a bottle fitted with an atomiser for paediatric use. Treatment time 7 weeks Comparator group (n = 22): no saline treatment Use of additional interventions (common to both treatment arms): oral antihistamines were allowed when needed; the intake of antihistamines was reported |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Secondary outcomes:
Other outcomes reported by the study: Mean number of daily antihistamine treatments per participant per week |
|
| Funding sources | No information provided | |
| Declarations of interest | No information provided | |
| Notes | The study authors reported in the paper that the range for the disease severity scale was from 0 to 16. However, it is unclear whether this is a reporting error as the total range for 4 symptoms each measured on a 0 to 3 scale should be 0 to 12. We contacted the authors to clarify this but no response was received. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were…randomly assigned to the active or control group according to randomisation tables." Comment: references Garavello 2003 for methods |
| Allocation concealment (selection bias) | Low risk | Quote: "This randomization was performed according to a computer‐generated list unknown to the physicians.…" (Garavello 2003) Comment: references Garavello 2003 for methods |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: blinding was not possible in this trial |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: outcomes were assessed by participants/carers who were not blinded to treatment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: 4/44 (9.1%) participants did not complete the trial and the dropouts were balanced between groups (2 in each group) with reasons provided Plausible effect size among missing outcomes is not enough to have a clinically relevant impact on observed effect size |
| Selective reporting (reporting bias) | Low risk | Comment: no protocol available for the trial through ClinicalTrials.gov or European Clinical Trials Registry. The outcomes as described in the methods section are recorded in the results section. They are recorded in the same way as other similar papers (Garavello 2003), which reduces the chance of selective outcome reporting. |
| Other bias (Non validated instruments) | Unclear risk | Comment: a summary symptom score of 4 elements is included (nasal discharge, nasal blockage, ocular itching and ocular reddening), each measured on a scale of 0 to 3. It is not clear if this is a validated score. |
| Other bias | Low risk | Comment: no other biases identified |
Garavello 2010.
| Methods | 2‐arm, non‐blinded, parallel‐group RCT, with 6 weeks duration of treatment and follow‐up | |
| Participants |
Location: Italy Setting of recruitment and treatment: secondary care: ENT clinic, outpatient Sample size: 52
Participant (baseline) characteristics:
Inclusion criteria: (1) typical anamnesis for seasonal allergic rhinitis; (2) marked positivity of the prick tests (≥ 2 plus) to Parietaria pollen extracts and assessed according to the already known guidelines, and (3) uncomplicated pregnancy with expected delivery date after the pollen season Exclusion criteria: (1) coexistence of nasal polyposis and/or bronchial asthma; (2) sensitisation to other allergens, and (3) previous specific immunotherapy |
|
| Interventions |
Intervention (n = 26): 20 mL (10 mL in each nostril) sterile, room temperature, hypertonic saline solution (NaCl 3%, 925 ± 30 mosm/kg, pH 7.45 ± 0.2) administered using a disposable syringe, 3 times a day
Instructed to energetically breathe in during administration. Treatment continued for 6 weeks. Comparator group (n = 26): no local therapy Use of additional interventions (common to both treatment arms): oral antihistamines when needed. Participants were asked to record the relative intake. Choice of preparation and dose was left to participants. |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Secondary outcomes:
Other outcomes reported by the study: The mean number of antihistamines assumption per participant per week for each week of the pollen season; nasal resistance |
|
| Funding sources | No information provided | |
| Declarations of interest | No information provided | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomly assigned to the active or control group according to randomization tables." Comment: adequate randomisation |
| Allocation concealment (selection bias) | Low risk | Quote: "Sealed opaque envelopes containing the treatment allocation were opened after randomization just before the initiation of the study period. The allocation sequence was prepared by one of the authors (E.S.). Another author (W.G.) enrolled and assigned patients to the treatment groups." Comment: adequate allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Women and physicians were not blinded to treatment allocation." Comment: blinding was not possible due to the nature of the interventions used in the trial |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: blinding of participants was not possible and the main outcome measures were patient reported, which may lead to bias in the outcomes |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: 7/52 participants (13%) did not complete the trial. This was balanced between the treatment groups. The reasons for non‐completion were given and were balanced. Plausible effect size among missing outcomes is not enough to have a clinically relevant impact on observed effect size. |
| Selective reporting (reporting bias) | Low risk | Comment: no protocol was identified on ClinicalTrials.gov or the European Clinical Trials Registry. The outcomes as reported in the methods section are reported in the results. Adverse effects are not well reported in the paper. |
| Other bias (Non validated instruments) | Unclear risk | Comment: it is unclear if the rating scale to measure symptoms was validated |
| Other bias | Low risk | Comment: no sources of 'other' bias were identified |
Li 2009.
| Methods | 3‐arm, non‐blinded, parallel‐group RCT, with 12‐week duration of treatment and follow‐up | |
| Participants |
Location: China Setting of recruitment and treatment: not stated Sample size: 26
Participant (baseline) characteristics:
Inclusion criteria: the diagnosis of allergic rhinitis was confirmed by history, physical examination and skin prick test with a battery of common allergens. All participants presented with nasal oedema and vicious secretion. Exclusion criteria: marked septum deviation, prior nasal surgery, nasal polyposis and symptoms of infection |
|
| Interventions |
Steroid only group (n = 6): 256 μg budesonide nasal spray daily for 4 weeks, followed by 128 μg and 64 μg daily for 4 weeks. Total treatment time = 12 weeks Saline only group (n = 8): 500 mL of normal saline (0.9% sodium chloride solution) was used twice a day for nasal irrigation with a commercial positive‐pressure nasal irrigation applicator Steroid PLUS saline (n = 12): both the 'saline' and 'steroid' treatments Use of additional interventions (common to both treatment arms): all participants had a 10 mg loratadine tablet daily for 2 weeks in combination with other managements |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Secondary outcomes:
Other outcomes reported by the study: Nasal signs (combined score of colour of nasal turbinates, nasal secretions, swelling of turbinates and retropharyngeal inflammation), mucociliary clearance and concentration of soluble intercellular adhesion molecule |
|
| Funding sources | "National Natural Science Fund (No. 30572025, No. 30700935) and the Natural Science Fund of Jiangsu Province (No. BK2007610).” | |
| Declarations of interest | No information provided | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Quote: "randomised" Comment: although the methods section uses the word "randomised" the abstract uses "divided" and there is no information about the methods to be able to determine how randomisation was completed. The groups have unequal numbers of participants (6, 8 and 12) and there is a lack of baseline demographics to be able to determine whether they were similar. |
| Allocation concealment (selection bias) | High risk | Comment: there is no information regarding allocation concealment. As the abstract uses the word "divided" and there are unequal numbers of participants in each arm there is a concern that selection bias may have occurred. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: the study was not blinded, although it is unlikely that the study could have been blinded given the nature of the intervention |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: it would not have been possible to blind the patient‐reported outcome (symptom score). However, the other outcomes (signs, mucociliary clearance etc.) could have been blinded as they were not participant‐assessed. The paper does not indicate that this occurred. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: it appears that everyone that entered the study completed it |
| Selective reporting (reporting bias) | Low risk | Comment: no protocol for the trial was identified on ClinicalTrials.gov or on the Chinese Registry of Clinical Trials. All outcomes reported in the methods section of the protocol are presented in the results. |
| Other bias (Non validated instruments) | Unclear risk | Comment: it is unclear if the rating scale used to measure symptoms was validated. The paper mentioned relating to the scale is not a validation paper. |
| Other bias | Low risk | Comment: no further causes of bias were identified |
Lin 2017.
| Methods | 2‐arm, non‐blinded, single‐centre, parallel‐group RCT, with 30‐day duration of treatment and follow‐up | |
| Participants |
Location: China Setting of recruitment and treatment: university hospital ENT clinic Sample size: 50
Participant (baseline) characteristics:
Inclusion criteria: cough for ≥ 8 weeks, reporting nasal secretions at the back of the throat, having elevated specific immunoglobulin E levels to house dust mite and having persistent allergic rhinitis according to the ARIA guidelines Exclusion criteria: asthma and gastroesophageal reflux disease (GERD) |
|
| Interventions |
Intervention (n = 23): saline, topical nasal‐pharyngeal irrigation 200 mL, "normal" (isotonic) saline with a temperature of 40°C, twice daily (in the morning and evening), pumping a 100 mL solution from a saline solution bag hung on a drip stand overhead into each nostril and allowing it to run out of the mouth. Treatment duration = 30 days. Comparator group (n = 22): topical nasal spray of fluticasone propionate 100 µg twice daily (one spray of 50 µg in each nostril in the morning and evening). Treatment duration = 30 days. Use of additional interventions (common to both treatment arms): during the whole study period, the participants were instructed not to use any other drugs |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Secondary outcomes:
Other outcomes reported by the study: Cough symptom score, Leicester cough questionnaire, capsaicin cough challenge, lung function test, assessment of inflammatory mediators (histamine, leukotriene C4, prostaglandin D2 and the major basic protein from nasal lavage fluid) |
|
| Funding sources | "This work was supported by the National Natural Science Foundation (grant 81371076), and the Shanghai Suburb Tertiary Hospital Clinical Capacity Building Project (grant SHDC12015905)” | |
| Declarations of interest | "The authors have no conflicts of interest to declare pertaining to this article” | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "A 30‐day treatment regimen was assigned in accordance with an independently generated random code to one of the following groups…" Comment: independently generated random code |
| Allocation concealment (selection bias) | Unclear risk | Comment: there is no information about allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: participants and healthcare professionals were not blinded to the treatment group. There may have been a difference in treatment between the 2 groups with the saline group required to attend clinic as an outpatient for their treatment. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: it does not appear that the people assessing the outcomes (participants and/or healthcare professionals) were blinded to the treatment group |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: 45/50 participants (90%) completed the trial. The loss to follow‐up was similar between the groups (88% and 92%) but it is not clear what the reasons for loss to follow‐up in each group were. |
| Selective reporting (reporting bias) | Low risk | Comment: no protocol was identified on ClinicalTrials.gov or on Chinese Clinical Trials Registry. A protocol number was provided in the paper (2014‐179), but it was not possible to find the protocol. The outcomes as listed in the methods are presented in full in the results section. |
| Other bias (Non validated instruments) | Low risk | Comment: the outcomes relevant to this review (mini‐RQLQ) and VAS for total nasal symptoms were both validated in this population and references are given to the relevant validation papers |
| Other bias | Unclear risk | Comment: no other sources of bias found |
Marchisio 2012.
| Methods | 3‐arm, single‐blinded, multicentre, parallel‐group RCT, with 4 weeks duration of treatment and follow‐up | |
| Participants |
Location: Italy, 2 sites (Milan and Naples) Setting of recruitment and treatment: secondary care: 2 paediatric hospitals Sample size: 240
Participant (baseline) characteristics:
Inclusion criteria: children aged 5 to 9 years with seasonal grass pollen‐related allergic rhinitis diagnosed on the basis of their history (seasonal allergic rhinitis in the period of grass pollen antigen circulation for at least 1 year with documented rhinorrhoea, obstruction, nasal itching and sneezing), positive skin test reactions to pollen extracts, including orchard and rye grass (Lofarma Allergens, Milano, Italy), and a physical examination at the time of enrolment Exclusion criteria: congenital or acquired immunodeficiency, cancer, autoimmune disease, congenital or early onset chronic diseases capable of modifying respiratory function (such as cystic fibrosis or bronchodysplasia), nasal septum deviation or craniofacial malformations, asthma, the use of systemic or local steroids or antihistamines in the previous month, the use of immunotherapy in the previous 2 years |
|
| Interventions |
Intervention 1 (n = 80): hypertonic saline (2.7% sodium chloride solution) at room temperature, irrigation using bulb syringe, 20 mL per nostril at a low positive pressure, 2 times per day (morning and evening). Duration of treatment was approximately 10 seconds. Total treatment time = 4 weeks. Intervention 2 (n = 80): 'normal' saline (0.9% sodium chloride solution) at room temperature, irrigation using bulb syringe, 20 mL per nostril at a low positive pressure, 2 times per day (morning and evening). Duration of treatment was approximately 10 seconds. Total treatment time = 4 weeks. Comparator group (n = 80): no saline treatment Use of additional interventions (common to both treatment arms): children were allowed to use an oral antihistamine (loratadine 5 mg once a day if they weighed < 30 kg, 10 mg once a day if they weighed > 30 kg) as a rescue treatment to control rhinitis symptoms when required, but not intranasal steroids |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Secondary outcomes:
Other outcomes reported by the study: Turbinate swelling, degree of adenoidal hypertrophy, diagnosis of OME, use of rescue medication, compliance and satisfaction |
|
| Funding sources | No information provided | |
| Declarations of interest | "All authors report no conflicts of interest relevant to this article.” | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The enrolled children were randomly assigned I: I :I to receive… on the basis of a computer‐generated randomization list in blocks of six." Comment: adequate randomisation methods |
| Allocation concealment (selection bias) | Unclear risk | Quote: "…the treatment assignments were made by a single investigator in each center (SB and MC)." Comment: unclear how allocation concealment was maintained, although it was completed by one investigator |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "The bottles were unlabelled and similar in appearance." Comment: although efforts were made to ensure blinding of the 2 saline solutions, this is not the comparison of interest for this review. It was not possible to blind all of the treatment groups as one was a 'no saline treatment'. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "The parents were instructed not to discuss the assignment with the only investigators responsible for the clinical and instrumental follow‐up (PM and AV), who remained blinded to the group assignment until the end of the study." Comment: this would be low risk for the outcomes that were assessed by physician, but not for those outcomes that were assessed by participants (e.g. nasal symptoms), which are of interest in this review |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: there do not seem to be any participants lost to follow‐up in either of the saline groups. In the 'no saline treatment' group 20/80 of the participants (25%) did not complete the study. Reasons for this are provided. The main reason was because of the use of intranasal steroids. Including these participants is likely to have made the 'no saline treatment' group appear more effective than it was. |
| Selective reporting (reporting bias) | Low risk | Comment: no protocol for the study was identified on ClinicalTrials.gov or European Clinical Trials Registry. All outcomes as stated in the methods section were reported in the results. |
| Other bias (Non validated instruments) | Unclear risk | Comment: it is not clear if the methods used to evaluate the nasal scores were validated The investigators allowed participants to score 3 nasal symptoms (nasal itching, nasal obstruction and sneezing) and let doctors score rhinorrhoea, which is different to other Total Nasal Symptom Scores measured in other papers |
| Other bias | Low risk | Comment: no other sources of bias were identified |
Ning 2011.
| Methods | 3‐arm, (no blinding described), single‐centre, parallel‐group RCT, with 2 weeks PLUS the length of pollen season duration of treatment and follow‐up | |
| Participants |
Location: China Setting of recruitment and treatment: secondary care: outpatient clinic, Department of Otorhinolaryngology, Peking University People's Hospital, Beijing Sample size: 30
Participant (baseline) characteristics:
Inclusion criteria: diagnosis of mugwort main trigger allergic rhinitis with confirmation in the clinic, according to 2004 Chinese Medical Association ENT conference diagnostic criteria Exclusion criteria: glucocorticoid contraindication |
|
| Interventions |
Intranasal steroid (n = 10): budesonide, 64 µg given morning and evening via nasal puff per side. (Daily dose of 256 µg). Treatment started 2 weeks prior to the pollen season (dates estimated from the dates of the pollen season the previous year) and continued for the duration of the pollen season. Saline group (n = 10): same administration method and frequency of administration as budesonide. No information about tonicity or dose of saline administered. Treatment duration = 2 weeks PLUS duration of pollen season. No saline treatment (n = 10): no intervention given Use of additional interventions (common to both treatment arms): no information |
|
| Outcomes |
Study outcomes: Primary outcomes:
Secondary outcomes: none reported Other outcomes reported by the study: Time of onset of symptoms (early in the pollen season, middle, late) Number of attacks Ratio of participants who relapsed in each group |
|
| Funding sources | Ministry of Science and Technology of the People's Republic China, National 15 Priority Areas Funding "Allergic Rhinitis Diagnosis and Prevention Research" No: 2007BA118B115 | |
| Declarations of interest | No information provided | |
| Notes | Translated from Chinese by Aidan Tan and Minsai Cai | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Participants were randomised into three groups" Comment: no further details given |
| Allocation concealment (selection bias) | Unclear risk | Comment: there is no description about the allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: placebo with saline was given when compared to the intranasal steroid group, but the paper does not state whether the participants and healthcare professionals were blinded to treatment group |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: no description of blinding of assessment |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: all 30 participants were followed up during the treatment. Nasal symptom scores, attack time of each participant and the ratio of participants who underwent relapse were all reported in the results. |
| Selective reporting (reporting bias) | Low risk | Comment: no protocol was identified on ClinicalTrials.gov or the Chinese Clinical Trials Registry All of the outcomes listed in the methods section were reported in the results section |
| Other bias (Non validated instruments) | Unclear risk | Comment: the study used the 2004 Chinese Medical Association ENT conference allergic rhinitis diagnostic criteria/guidelines. It is not clear if this is a validated scale. |
| Other bias | Low risk | No other sources of bias were identified |
Rogkakou 2005.
| Methods | 2‐arm, non‐blinded, parallel‐group RCT, with 4‐week duration of treatment and follow‐up | |
| Participants |
Location: Italy Setting of recruitment and treatment: secondary care: Allergy and Respiratory Diseases Department, University of Genoa Sample size: 14
Participant (baseline) characteristics:
Inclusion criteria: age between 18 and 65 years with clinical history of persistent allergic rhinitis (symptoms present 4 days or more a week) for at least 1 year and a positive skin prick test (mean wheal diameter > 3 mm) or RAST (at least class II) for house dust mites or/and Parietaria. They also had to be symptomatic during the run‐in period (total symptom score > 6). Exclusion criteria: anatomical abnormalities of the nasal cavity or relevant associated diseases (i.e. vasomotor rhinitis, glaucoma, uveitis, infections, malignancies) People with asthma requiring continuous inhaled steroids and pregnant women |
|
| Interventions |
Intervention (n = 7): hypertonic saline (Iperclean® UCB Pharma) 4 times a day. No volume given. Treatment duration = 4 weeks. Comparator group (n = 7): no saline Use of additional interventions (common to both treatment arms): cetirizine, orally, 10 mg/day. Treatment duration = 4 weeks. |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Secondary outcomes: none reported Other outcomes reported by the study: Night‐time symptoms, acoustic rhinometry |
|
| Funding sources | No information provided | |
| Declarations of interest | No information provided | |
| Notes | Rhinasthma® questionnaire results presented the domains of 'lower airways (LA)', 'upper airways (UA)' and 'respiratory allergy impact' (RAI) separately, but only the results for 'global impact', which is a synthetic score covering the entire questionnaire, were used for this review | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "…patients were randomized through a computer‐generated list..." Comment: adequate sequence generation |
| Allocation concealment (selection bias) | Unclear risk | Comment: no information is provided about allocation concealment |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: this was an open study. Participants and personnel were aware of the treatment group to which they had been allocated. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: the primary outcomes are participant‐reported and the participants were not blinded to the treatment group |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: it does not appear that any of the randomised participants dropped out of the study or were lost to follow‐up |
| Selective reporting (reporting bias) | High risk | Comment: there was no protocol for the study found on ClinicalTrials.gov or the European Clinical Trials Registry. The outcomes set out in the methods section were well reported in the results section, although measures of variation were not provided for the quality of life outcome. |
| Other bias (Non validated instruments) | Unclear risk | Comment: the paper provides a reference for the Rhinasthma® quality of life score, which indicates that this scoring system has good overall psychometric properties No information is provided, however, for the validation of the symptom scoring |
| Other bias | Low risk | Comment: no other risks of bias were identified |
Wu 2014.
| Methods | 3‐arm, non‐blinded, single‐centre, parallel‐group RCT with 3‐month duration of treatment and follow‐up | |
| Participants |
Location: China Setting of recruitment and treatment: not stated; treatment carried out in outpatients, Guangzhou Sample size: 61
Participant (baseline) characteristics:
Inclusion criteria: allergic rhinitis diagnosed with a skin prick test Exclusion criteria: (1) use of antihistamines or steroid medications (orally or nasally) in past 4 weeks, (2) chronic progressive respiratory problems, (3) severe systemic illness, (4) nasal growths/previous trauma/obvious nasal septum deformity, (5) previous sinusitis, (6) upper or lower respiratory illness, (7) alcoholic/drug abuse/poor habit history |
|
| Interventions |
Steroids group (n = 17): budesonide, intranasal steroid spray, 64 µg/spray, 1 spray twice day (in morning and at night). Treatment duration = 3 months. Saline group (n = 21): normal saline (no concentration information), 75 mL, twice a day (in morning and at night). Treatment duration = 3 months. Steroids PLUS saline group (n = 23): both of the above interventions, using the steroid spray after the nasal irrigation. Treatment duration = 3 months. Additional treatments: no information provided |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes:
Other outcomes reported by the study:
|
|
| Funding sources | "National Priority Research Theme Respiratory Disease funded (No: 2007DA780154F090)” | |
| Declarations of interest | No information provided | |
| Notes | The RQLQ is a validated instrument containing 28 questions regarding 7 domains: activities, sleep, practical problems, nasal symptoms, eye symptoms and other symptoms. For each domain, participants rate themselves as to how much their symptoms have affected them during the previous week on a scale of 0 to 6 (0 = no effect on quality of life). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "participants were randomly allocated to groups…" Comment: no further description given; cannot tell how randomisation sequence was done |
| Allocation concealment (selection bias) | Unclear risk | Comment: no description of allocation concealment was given |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: no statement on blinding was given |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "...standardised collection form was used for demographics and outcomes" Comment: no statement on blinding was given. Single statement as above, regarding how data were collected. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "All participants tolerated the treatment well, with no adverse events and completed the period of treatment" Comment: none of the participants withdrew from the trial or were lost to follow‐up |
| Selective reporting (reporting bias) | Low risk | Comment: no protocol available from ClinicalTrials.gov or the Chinese Clinical Trials Registry All of the outcomes listed in the methods section were reported in the results section. |
| Other bias (Non validated instruments) | Unclear risk | Comment: RQLQ is validated for this group of people. It appears that there is a Mandarin Chinese version of this questionnaire but it is not known whether this has been validated. No reference to the validation was provided in the paper. Visual analogue scales were used for patient‐reported symptoms. |
| Other bias | Low risk | Comment: no other sources of bias identified |
Yasar 2013.
| Methods | 3‐arm, non‐blinded, parallel‐group RCT, with 8‐week duration of treatment and follow‐up | |
| Participants |
Location: Cumhuriyet University, Turkey Setting of recruitment and treatment: secondary care: paediatric allergy and ENT department Sample size: 60
Participant (baseline) characteristics:
Inclusion criteria: participants with histories of allergic rhinitis with skin prick test, nasal smear, Phadiatop, total IgE and complete blood count tests used to confirm diagnosis Exclusion criteria: septal deviation, nasal polyp and adenoid pads, and people with rhinosinusitis who had received treatment in the past |
|
| Interventions |
Antihistamine (n = 20): 2 puffs of azelastine in each nostril per day (1 puff = 0.14 mg). Duration of treatment = 8 weeks. Intranasal steroid (n = 20): 2 puffs of mometasone furoate in each nostril per day (1 puff = 200 µg). Duration of treatment = 8 weeks. Nasal saline (n = 20): 2 puffs of isotonic sea water nasal saline spray (STERIMAR) in each nostril per day. Duration of treatment = 8 weeks. Use of additional interventions (common to both treatment arms): not listed |
|
| Outcomes |
Outcomes of interest in the review: Primary outcomes: no primary outcomes of interest were reported Secondary outcomes: no secondary outcomes of interest were reported Other outcomes reported by the study: Nasal cavity volumes measured using acoustic rhinometry |
|
| Funding sources | "The authors received no financial support for the research and/or authorship of this article.” | |
| Declarations of interest | "The authors declared no conflicts of interest with respect to the authorship and/or publication of this article” | |
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Comment: it is unclear if the participants were randomised to study group in this trial. The paper states that the participants were "classified" into 3 groups. Randomisation was not mentioned. Although baseline characteristics for the age and gender were given and did not differ between groups, other baseline characteristics were not provided. |
| Allocation concealment (selection bias) | Unclear risk | Comment: there is no information in the paper to detail how the participants were allocated to the treatment groups |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comment: participants and healthcare professionals were not blinded to treatment group, despite the treatments being administered in the same way and on the same regimen |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Comment: there is no information regarding the blinding of outcome assessors to the treatment group. This would have been feasible to complete. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: there do not appear to be any participants who were not analysed in the results of the trial |
| Selective reporting (reporting bias) | Low risk | Comment: there was only one outcome that was measured, which was nasal volume estimated using acoustic rhinometry. This was reported in full in the results section. |
| Other bias (Non validated instruments) | Low risk | Comment: the only outcome reported was not an outcome of interest in this review |
| Other bias | Low risk | Comment: no other source of potential bias in the study was identified |
ARIA: Allergic Rhinitis and its Impact on Asthma guidelines ENT: ear, nose and throat F: female M: male OME: otitis media with effusion RAST: radioallergosorbent test RCT: randomised controlled trial RQLQ: Rhinoconjunctivitis Quality of Life Questionnaire VAS: visual analogue scale
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Bachmann 2000 | POPULATION: chronic rhinosinusitis not allergic rhinitis |
| Barberi 2016a | STUDY DESIGN: single‐arm study; no comparison group |
| Barberi 2016b | STUDY DESIGN: single‐arm study; no comparison group |
| Barbieri 2002 | INTERVENTION: thermal water, not saline solution |
| ChiCTR‐INR‐16009778 2016 | COMPARISON: both treatment groups received saline solution; the study compared hydrogen‐rich saline with 'normal' saline nasal irrigation |
| Chowdary 2017 | POPULATION: the included population was 'allergic rhinitis' but this was not confirmed with skin prick testing or radioallergosorbent test (RAST) |
| Chusakul 2012 | COMPARISON: both treatment groups received saline solution; the study compared buffered and un‐buffered saline solutions |
| Del Giudice 2011 | COMPARISON: both treatment groups received saline solution; the study compared irrigation with ischia thermal water with irrigation with isotonic saline |
| Heatley 2001 | POPULATION: chronic rhinosinusitis not allergic rhinitis |
| Jan 2013 | STUDY DESIGN: single‐arm study; no comparison group |
| Lin 2014 | COMPARISON: both treatment groups received saline solution; the study compared the use of saline solutions at 3 different temperatures (15°C, 25°C and 40°C) |
| Malizia 2017 | COMPARISON: both treatment groups received saline solution; the study compared buffered hypertonic saline versus normal saline solution |
| Mora 2002 | INTERVENTION: thermal water, not saline solution |
| NCT01248325 2010 | COMPARISON: treatment in comparison arm was Luffa Operculate, which is not a standard treatment for allergic rhinitis The status of this study on the ClinicalTrials.gov website was last updated in November 2010 |
| NCT01326247 2011 | COMPARISON: both treatment groups received saline solution; the study compared "hyper‐mineral chloride sodium water" with 0.9% nasal saline solution The ClinicalTrials.gov website indicates that this study has been completed and a reference for the full paper is provided |
| NCT02729012 2016 | COMPARISON: both treatment groups received saline solution; the study compared hypertonic (3%) saline solution with 0.9% saline solution The ClinicalTrials.gov website indicates that this study has been completed; no study results are posted and there is no reference to the full paper |
| Nguyen 2014 | STUDY DESIGN: single‐arm study; no comparison group |
| Polasek 1987 | POPULATION: the majority of participants had chronic rhinosinusitis not allergic rhinitis COMPARISON: both treatment groups received saline solution; the study compared Prorhinel® with isotonic saline solution |
| Rabago 2002 | POPULATION: chronic rhinosinusitis not allergic rhinitis |
| Satdhabudha 2012 | COMPARISON: both treatment groups received saline solution; the study compared buffered and un‐buffered saline solutions |
| Shoseyov 1998 | POPULATION: chronic rhinosinusitis not allergic rhinitis |
| Singh 2016 | Hypertonic seawater saline versus intranasal normal saline; the study compared hypertonic seawater saline versus intranasal normal saline |
| TCTR20150923001 2015 | COMPARISON: both treatment groups received saline solution; the study compared 1.8% and 0.9% nasal saline solutions The trial record was last updated in September 2015; the status of the study was 'active, not recruiting' at this time point |
| TCTR20160120001 2016 | COMPARISON: both treatment groups received saline solution; the study compared 3 different treatment arms; 2 different solutions of 0.9% nasal saline and one 1.8% saline solution The trial record was last updated in May 2016; the status of the study was 'recruiting' at this time point |
| TCTR20160913003 2016 | COMPARISON: both treatment groups received saline solution; the study compared hypotonic nasal saline irrigation with 'normal' isotonic saline irrigation |
| Tomooka 2000 | STUDY DESIGN: single‐arm study; no comparison group |
| Ural 2009 | COMPARISON: both treatment groups received saline solution; the study compared isotonic with hypertonic saline |
| Valencia Chavez 2015 | COMPARISON: both treatment groups received saline solution; the study compared seawater diluted to 0.9% with 0.9% isotonic nasal saline solution |
| Xiong 2014 | INTERVENTION: no saline solution was used: the 'active' treatment group received tap water; the control group received no nasal irrigation |
Characteristics of studies awaiting assessment [ordered by study ID]
Hausfeld 2007.
| Methods | Randomised controlled trial |
| Participants | 103 participants (aged 19 to 82) with allergic and/or vasomotor rhinitis |
| Interventions | All participants received triamcinolone acetonide nasal spray (intranasal steroid spray) Group 1: ENTSOL® spray ‐ buffered hypertonic saline nasal spray Group 2: no saline nasal spray Treatment duration = 3 to 6 weeks |
| Outcomes | Septal irrigation |
| Notes | Tried to contact the authors for more information but no response was received ENTSOL® gel (buffered hypertonic saline nasal gel) was given to participants in either group who were experiencing nasal irritation |
Krcmova 2011.
| Methods | Randomised controlled trial |
| Participants | 30 adult (14 to 79 years) allergic patients with diagnosis of persistent allergic rhinitis |
| Interventions | All participants received oral antihistamine Group 1: saline solution (PantheNose spray) Group 2: no saline solution Intranasal steroids were allowed if symptoms worsened Treatment duration = 4 to 6 weeks |
| Outcomes | Use of steroid treatment, quality of life for activities, sleep, other, practical problems, nasal problems, eye problems, feelings, 10‐point VAS (symptoms?) |
| Notes | 1 further translation from Czech required |
Lee 2017.
| Methods | Randomised controlled trial |
| Participants | 20 children with allergic rhinitis and asthma |
| Interventions | Group 1: daily isotonic saline nasal irrigation for 12 weeks Group 2: control group All participants received montelukast or inhaled ciclesonide, and levocetirizine as adjuvant treatment |
| Outcomes | Rhinitis Control Assessment Test (RCAT), Asthma Control Test (ACT), forced expiratory volume in 1 second (FEV1), provocative concentration of methacholine causing a 20% fall in FEV1 (PC20) and oral fractional exhaled nitric oxide (FeNO) |
| Notes | Attempted to contact the author but no response was received |
Manole 2013.
| Methods | Unclear ‐ no mention of randomisation in the abstract |
| Participants | 92 participants between 8 and 18 years with allergic rhinitis |
| Interventions | All participants received oral desloratadine (antihistamine) Group 1: hypertonic saline irrigation Group 2: no saline irrigation Treatment duration = 7 days |
| Outcomes | Daily symptom diary card Acoustic rhinometry, radiography (Water's projection), patient‐reported scales of general discomfort, nasal airway obstruction, agreeableness of the irrigation |
| Notes | Attempted to contact the author but no response received |
Differences between protocol and review
We had initially stated that we would present the initial results by volume of saline solution. This was changed to show the primary results by age of the participants within the study. This was because we felt it was more important to know whether the intervention worked for the different population groups.
The published protocol contained conflicting statements on the inclusion of studies according to the duration of treatment and follow‐up. We modified the methods section to ensure consistency. There was no minimum duration of treatment and follow‐up. Had results been available after the completion of treatment we would have reported these as they may provide useful information regarding the duration of effects of saline.
Contributions of authors
Karen Head drafted and revised the protocol. For the full review she screened abstracts, completed full‐text screening, completed data extraction, completed data analysis and GRADE analysis, and drafted and revised the review.
Kornkiat Snidvongs reviewed and edited the protocol. For the full review he screened abstracts, completed data extraction, reviewed and edited the full review, and provided clinical guidance at all stages.
Simon Glew reviewed and edited the protocol. For the full review he screened abstracts, reviewed and edited the full review, and provided clinical guidance at all stages.
Glenis Scadding reviewed and edited the protocol. For the full review she screened abstracts, reviewed and edited the full review, and provided clinical guidance at all stages.
Anne Schilder reviewed and edited the protocol. For the full review she reviewed and edited the full review, and provided clinical guidance at all stages.
Carl Philpott reviewed and edited the protocol. For the full review he completed full‐text screening, reviewed and edited the full review, and provided clinical guidance at all stages.
Claire Hopkins reviewed and edited the protocol. For the full review she reviewed and edited the full review, and provided clinical guidance at all stages.
Sources of support
Internal sources
No sources of support supplied
External sources
-
National Institute for Health Research, UK.
Infrastructure funding for Cochrane ENT
Cochrane Review Support Programme, UK.
Declarations of interest
Karen Head: none known.
Kornkiat Snidvongs: none known. Kornkiat Snidvongs is an Associate Editor for Cochrane ENT, but had no role in the editorial process for this review.
Simon Glew: none known.
Glenis Scadding: none known.
Anne GM Schilder: Anne Schilder is joint Co‐ordinating Editor of Cochrane ENT, but had no role in the editorial process for this review. Her evidENT team at UCL is supported in part by the National Institute of Health Research University College London Hospitals Biomedical Research Centre. Their research is funded by the NIHR and EU Horizon2020. She is the national chair of the NIHR Clinical Research Network ENT Specialty. She is the Surgical Specialty Lead for ENT for the Royal College of Surgeons of England's Clinical Trials Initiative. She is co‐investigator on the NIHR PGfAR grant 'Defining best Management for Adults with Chronic RhinOsinusitis: the MACRO Programme'. In her role as director of the NIHR UCLH BRC Deafness and Hearing Problems Theme, she acts as an advisor on clinical trial design and delivery to a range of biotech companies.
Carl Philpott: Carl Philpott has previously received consultancy fees from the companies Acclarent, Navigant, Aerin Medical and Entellus. He is joint chief investigator on the NIHR PGfAR grant 'Defining best Management for Adults with Chronic RhinOsinusitis: the MACRO Programme.
Claire Hopkins: Claire Hopkins has received financial support from several companies involved in producing instruments for sinus surgery. She is joint chief investigator on the NIHR PGfAR grant 'Defining best Management for Adults with Chronic RhinOsinusitis: the MACRO Programme.
New
References
References to studies included in this review
Chairattananon 2013 {published and unpublished data}
- Chairattananon C, Pensrichon R, Veskitkul J, Pacharn P, Piboonpocanun O, Visitsunthorn N, et al. Efficacy of saline nasal irrigation in children with allergic rhinitis. Allergy: European Journal of Allergy and Clinical Immunology 2013;68:359. [Google Scholar]
Chen 2014 {published data only (unpublished sought but not used)}
- Chen JR, Jin L, Li XY. The effectiveness of nasal saline irrigation (seawater) in treatment of allergic rhinitis in children. International Journal of Pediatric Otorhinolaryngology 2014;78(7):1115‐8. [DOI] [PubMed] [Google Scholar]
Cordray 2005 {published data only}
- Cordray S, Harjo JB, Miner L. Comparison of intranasal hypertonic dead sea saline spray and intranasal aqueous triamcinolone spray in seasonal allergic rhinitis. Ear, Nose, & Throat Journal 2005;84(7):426‐30. [PubMed] [Google Scholar]
Di Berardino 2017 {published and unpublished data}
- Berardino F, Zanetti D, D'Amato G. Nasal rinsing with an atomized spray improves mucociliary clearance and clinical symptoms during peak grass pollen season. American Journal of Rhinology & Allergy 2017;31(1):40‐3. [DOI] [PubMed] [Google Scholar]
Garavello 2003 {published data only (unpublished sought but not used)}
- Angrisano A. Hypertonic saline nasal wash: effect on grass pollen rhinitis in children. Allergy and Clinical Immunology International 2003;1(Suppl 1):P‐16‐4. [Google Scholar]
- Garavello W, Romagnoli M, Sordo L, Gaini RM, Berardino C, Angrisano A. Hypersaline nasal irrigation in children with symptomatic seasonal allergic rhinitis: a randomized study. Pediatric Allergy and Immunology 2003;14(2):140‐3. [DOI] [PubMed] [Google Scholar]
Garavello 2005 {published data only (unpublished sought but not used)}
- Garavello W, Berardino F, Romagnoli M, Sambataro G, Gaini RM. Nasal rinsing with hypertonic solution: an adjunctive treatment for pediatric seasonal allergic rhinoconjunctivitis. International Archives of Allergy and Immunology 2005;137(4):310‐4. [DOI] [PubMed] [Google Scholar]
- Garavello W, Berardino F, Romagnoli M, Sambataro G, Gaini RM, et al. Nasal rinsing with hypertonic solution: an adjunctive treatment for pediatric seasonal allergic rhinoconjunctivitis. Proceedings of the 9th International Conference on Pediatric Otorhinolaryngology (ESPO), Paris, France, 18‐21 June 2006. 2006:Abstract No. 369.
Garavello 2010 {published data only}
- Garavello W, Somigliana E, Acaia B, Gaini L, Pignataro L, Gaini RM. Nasal lavage in pregnant women with seasonal allergic rhinitis: a randomized study. International Archives of Allergy and Immunology 2010;151(2):137‐41. [DOI] [PubMed] [Google Scholar]
Li 2009 {published data only}
- Li H, Sha Q, Zuo K, Jiang H, Cheng L, Shi J, et al. Nasal saline irrigation facilitates control of allergic rhinitis by topical steroid in children. ORL; Journal for Oto‐rhino‐laryngology and Its Related Specialties 2009;71(1):50‐5. [DOI] [PubMed] [Google Scholar]
Lin 2017 {published data only (unpublished sought but not used)}
- Lin L, Chen Z, Cao Y, Sun G. Normal saline solution nasal‐pharyngeal irrigation improves chronic cough associated with allergic rhinitis. American Journal of Rhinology & Allergy 2017;31(2):96‐104. [DOI] [PubMed] [Google Scholar]
Marchisio 2012 {published data only}
- Marchisio P, Varricchio A, Baggi E, Bianchini S, Capasso ME, Torretta S, et al. Hypertonic saline is more effective than normal saline in seasonal allergic rhinitis in children. International Journal of Immunopathology and Pharmacology 2012;25(3):721‐30. [DOI] [PubMed] [Google Scholar]
Ning 2011 {published data only}
- Ning X, Xing Z, Wang M, Gao Z. To investigate the effect of pretreatment with budesonide spray in patients with allergic rhinitis. Lin Chuang Er Bi Yan Hou Ke za Zhi [Journal of Clinical Otorhinolaryngology] 2011;25(14):633‐5. [PubMed] [Google Scholar]
Rogkakou 2005 {published data only (unpublished sought but not used)}
- Rogkakou A, Guerra L, Massacane P, Baiardini I, Baena‐Cagnani R, Zanella CH, et al. Effects on symptoms and quality of life of hypertonic saline nasal spray added to antihistamine in persistent allergic rhinitis‐‐a randomized controlled study. European Annals of Allergy and Clinical Immunology 2005;37(9):353‐6. [PubMed] [Google Scholar]
Wu 2014 {published data only}
- Wu M, Wang Q, Zhang K, Wu K, Zhang Y, Wang Z, et al. The effect of nasal irrigation in the treatment of allergic rhinitis. Lin Chuang Er Bi Yan Hou Ke za Zhi [Journal of Clinical Otorhinolaryngology] 2014;28(5):287‐9. [PubMed] [Google Scholar]
Yasar 2013 {published data only}
- Yasar M, Uysal IO, Altuntas EE, Cevit O, Muderris S. Effects of topical sprays on allergy‐induced nasal obstruction in children. Kulak Burun Bogaz Ihtisas Dergisi: KBB [Journal of Ear, Nose, and Throat] 2013;23(4):217‐24. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Bachmann 2000 {published data only}
- Bachmann G, Hommel G, Michel O. Effect of irrigation of the nose with isotonic salt solution on adult patients with chronic paranasal sinus disease. European Archives of Oto‐ Rhino‐Laryngology 2000;257(10):537‐41. [DOI] [PubMed] [Google Scholar]
Barberi 2016a {published data only}
- Barberi S, D'Auria E, Bernardo L, Ferrara F, Pietra B, Pinto F, et al. Hypertonic saline monotherapy in children with perennial allergic rhinitis: a pilot study. Journal of Biological Regulators & Homeostatic Agents 2016;30(1):271‐5. [PubMed] [Google Scholar]
Barberi 2016b {published data only}
- Barberi S, D Auria E, Bernardo L, Pinto F, Pietra B, Ciprandi G. Isotonic saline in children with perennial allergic rhinitis. Journal of Biological Regulators & Homeostatic Agents 2016;30(2):605‐8. [PubMed] [Google Scholar]
Barbieri 2002 {published data only}
- Barbieri M, Salami A, Mora F, Casazza A, Sovatzis A, Teglia R, et al. Behavior of serum IgE and IgA in patients with allergic rhinitis treated with iodine bromide thermal water. Acta Otorhinolaryngologica Italica 2002;22(4):215‐9. [PubMed] [Google Scholar]
ChiCTR‐INR‐16009778 2016 {published data only}
- ChiCTR‐INR‐16009778 2016. A randomized, double‐blind, controlled study of the efficacy and safety of hydrogen rich saline irrigation in patients with rhinitis to improve the physiological function of nasal mucosa. http://www.chictr.org.cn/showproj.aspx?proj=16557.
Chowdary 2017 {published data only}
- Chowdary Gaddipatti R, Rao SP, Rajiv K, Jain M. Isotonic nasal spray versus fluticasone nasal spray in treatment of allergic rhinitis. International Journal of Otolaryngology 2017;3(3):581‐4. [Google Scholar]
Chusakul 2012 {published data only}
- Chusakul S, Warathanasin S, Suksangpanya N, Phannaso C, Ruxrungtham S, Snidvongs K, et al. Comparison of buffered and nonbuffered nasal saline irrigations in treating allergic rhinitis. Laryngoscope 2013;123(1):53‐6. [DOI] [PubMed] [Google Scholar]
Del Giudice 2011 {published data only}
- Giudice MM, Decimo F, Maiello N, Leonardi S, Parisi G, Golluccio M, et al. Effectiveness of ischia thermal water nasal aerosol in children with seasonal allergic rhinitis: a randomized and controlled study. International Journal of Immunopathology and Pharmacology 2011;24(4):1103‐9. [DOI] [PubMed] [Google Scholar]
Heatley 2001 {published data only}
- Heatley DG, McConnell KE, Kille TL, Leverson GE. Nasal irrigation for the alleviation of sinonasal symptoms. Otolaryngology ‐ Head and Neck Surgery 2001;125(1):44‐8. [DOI] [PubMed] [Google Scholar]
Jan 2013 {published data only}
- Jan RL. The efficacy of nasal saline aerosol purging on allergic rhinitis and rhinosinusitis patients. Allergy: European Journal of Allergy and Clinical Immunology 2013;68:34. [Google Scholar]
Lin 2014 {published data only}
- Lin L, Yan W, Zhao X. Treatment of allergic rhinitis with normal saline nasal irrigation at different temperature. Chinese Journal of Otorhinolaryngology Head and Neck Surgery 2014;49:109‐14. [PubMed] [Google Scholar]
Malizia 2017 {published data only}
- Malizia V, Fasola S, Ferrante G, Cilluffo G, Montalbano L, Landi M, et al. Efficacy of buffered hypertonic saline nasal irrigation for nasal symptoms in children with seasonal allergic rhinitis: a randomized controlled trial. International Archives of Allergy and Immunology 2017;174(2):97‐103. [DOI] [PubMed] [Google Scholar]
Mora 2002 {published data only}
- Mora R, Chiarlone M, Crippa B, Mora F, Barbieri M. Nasal irrigations with sulphurea water in the treatment of the oral allergy syndrome. Medicina Clinica e Termale 2002;14(48):287‐90. [Google Scholar]
NCT01248325 2010 {published data only}
- NCT01248325. A study of Luffa Operculate nasal solution 5mg/mL compared with saline (NaCl 09%) for the relief of nasal obstruction. https://clinicaltrials.gov/ct2/show/NCT01248325?term=NCT01248325&rank=1.
NCT01326247 2011 {published data only}
- NCT01326247. Effectiveness of therapy with a thermal water nasal aerosol in children with seasonal allergic rhinitis. https://clinicaltrials.gov/ct2/show/NCT01326247?term=NCT01326247&rank=1. [DOI] [PubMed]
NCT02729012 2016 {published data only}
- NCT02729012. Effects of hypertonic saline solution (NACL 3%+NAHCO3) on nasal inflammation in children with AR. RinASol ‐ Pilot Study. https://clinicaltrials.gov/ct2/show/NCT02729012?term=NCT02729012&rank=1.
Nguyen 2014 {published data only}
- Nguyen SA, Psaltis AJ, Schlosser RJ. Isotonic saline nasal irrigation is an effective adjunctive therapy to intranasal corticosteroid spray in allergic rhinitis. American Journal of Rhinology & Allergy 2014;28(4):308‐11. [DOI] [PubMed] [Google Scholar]
Polasek 1987 {published data only}
- Polasek O, Haudenschild P. A double blind cross‐over study of the effects of a nasal wash with Prorhinel by perennial rhinitis. Therapeutische Umschau 1987;44(12):978‐81. [PubMed] [Google Scholar]
Rabago 2002 {published data only}
- Rabago D, Zgierska A, Mundt M, Barrett B, Bobula J, Maberry R. Efficacy of daily hypertonic saline nasal irrigation among patients with sinusitis: a randomized controlled trial. Journal of Family Practice 2002;51(12):1049‐55. [PubMed] [Google Scholar]
Satdhabudha 2012 {published data only}
- NCT01441778. Efficacy of buffered hypertonic saline (BHS) nasal irrigation in allergic rhinitis (AR) children. https://clinicaltrials.gov/ct2/show/NCT01441778?term=NCT01441778&rank=1.
- Satdhabudha A, Poachanukoon O. Efficacy of buffered hypertonic saline nasal irrigation in children with symptomatic allergic rhinitis: a randomized double‐blind study. International Journal of Pediatric Otorhinolaryngology 2012;76(4):583‐8. [DOI] [PubMed] [Google Scholar]
Shoseyov 1998 {published data only}
- Shoseyov D, Bibi H, Shai P, Shoseyov N, Shazberg G, Hurvitz H. Treatment with hypertonic saline versus normal saline nasal wash of pediatric chronic sinusitis. Journal of Allergy and Clinical Immunology 1998;101(5):602‐5. [DOI] [PubMed] [Google Scholar]
Singh 2016 {published data only}
- Singh R, Galagali JR, Kumar S, Bahurupi Y, Chandrachood M. Comparative study of intranasal hypertonic seawater saline versus intranasal normal saline in allergic rhinitis. International Journal of Otorhinolaryngology and Head and Neck Surgery 2016;3(1):104‐7. [Google Scholar]
TCTR20150923001 2015 {published data only}
- TCTR20150923001. Properties of self‐prepared nasal saline irrigation and clinical outcome in patient with chronic allergic rhinitis. http://www.clinicaltrials.in.th/index.php?tp=regtrials&menu=trialsearch&smenu=fulltext&task=search&task2=view1&id=1464 (first received 23 September 2015).
TCTR20160120001 2016 {published data only}
- TCTR20160120001. Efficacy and safety in self‐prepared nasal saline irrigation and clinical outcome in patient with allergic rhinitis. http://www.clinicaltrials.in.th/index.php?tp=regtrials&menu=trialsearch&smenu=fulltext&task=search&task2=view1&id=1701 (first received 20 January 2016).
TCTR20160913003 2016 {published data only}
- TCTR20160913003. The efficacy of hypotonic saline and isotonic saline irrigation on nasal symptoms and mucociliary clearance in allergic rhinitis. http://www.clinicaltrials.in.th/index.php?tp=regtrials&menu=trialsearch&smenu=fulltext&task=search&task2=view1&id=2066 (first received 13 September 2016).
Tomooka 2000 {published data only}
- Tomooka LT, Murphy C, Davidson TM. Clinical study and literature review of nasal irrigation. Laryngoscope 2000;110(7):1189‐93. [DOI] [PubMed] [Google Scholar]
Ural 2009 {published data only}
- Ural A, Oktemer TK, Kizil Y, Ileri F, Uslu S. Impact of isotonic and hypertonic saline solutions on mucociliary activity in various nasal pathologies: clinical study. Journal of Laryngology and Otology 2009;123(5):517‐21. [DOI] [PubMed] [Google Scholar]
Valencia Chavez 2015 {published data only}
- Efficiency of treatment of allergic rhinitis with seawater by a randomized clinical trial. http://registroclinico.sld.cu/en/trials/RPCEC00000200‐En (first received 25 September 2015).
- Valencia Chavez ML, Soler Terranova W, Rosique Gracia J, Morales Munera O. Efficacy of seawater for the treatment of allergic rhinitis: a randomized clinical trial. Social Medicine (Social Medicine Publication Group) 2015;9(2):63‐72. [Google Scholar]
Xiong 2014 {published data only}
- Xiong M, Fu XY, Deng WT, Lai HW, Yang CH. Tap water nasal irrigation in adults with seasonal allergic rhinitis: a randomized double‐blind study. European Archives of Oto‐Rhino‐Laryngology 2014;271(6):1549‐52. [DOI] [PubMed] [Google Scholar]
References to studies awaiting assessment
Hausfeld 2007 {published data only (unpublished sought but not used)}
- Hausfeld JN. Buffered hypertonic saline nasal spray and gel as treatment modifiers in allergic and vasomotor rhinitis. Journal of Allergy and Clinical Immunology; American Academy of Allergy, Asthma and Immunology (AAAI) 63rd Annual Meeting San Diego, Ca, USA, February 23‐27. 2007; Vol. 119:S230 (Abstract 905).
Krcmova 2011 {published data only}
- Krcmova I, Mala E. Saline solutions as a supportive therapy in the concurrent treatment of allergic rhinitis. Alergie 2011;13(1):66‐71. [Google Scholar]
Lee 2017 {published data only (unpublished sought but not used)}
- Lee J, Ryu G, Kim M, Yang H, Kim S, et al. The effects of saline nasal irrigation on allergic rhinitis and asthma in children. Allergy 2017;72(S103):561. [Google Scholar]
Manole 2013 {published data only (unpublished sought but not used)}
- Manole F. Effect of nasal irrigation in the treatment of rhinitis in children. European Academy of Allergy and Clinical Immunology and World Allergy Organization World Allergy and Asthma Congress. 2013.
Additional references
ARIA 2001
- Bousquet J, Cauwenberge P, Khaltaev N. Allergic Rhinitis and Its Impact on Asthma. Journal of Allergy and Clinical Immunology 2001;108(5):S147‐334. [DOI] [PubMed] [Google Scholar]
ARIA 2008
- Bousquet J, Khaltaev N, Cruz AA, Denburg J, Fokkens WJ, Togias A, et al. Allergic Rhinitis and its Impact on Asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen). Allergy 2008;63:8‐160. [DOI] [PubMed] [Google Scholar]
Barham 2015
- Barham H, Harvey R. Nasal saline irrigation: therapeutic or homeopathic. Brazilian Journal of Otorhinolaryngology 2015;81(5):457‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Berjis 2011
- Berjis N, Sonbolastan SM, Okhovat SH, Narimani AA, Razmjui J. Normal saline versus hypertonic 3% saline: its efficacy in non‐acute rhinosinusitis. Iranian Journal of Otorhinolaryngology 2011;23:23‐8. [Google Scholar]
Bonnomet 2016
- Bonnomet A, Luczka E, Coraux C, Gabory L. Non‐diluted seawater enhances nasal ciliary beat frequency and wound repair speed compared to diluted seawater and normal saline. International Forum of Allergy & Rhinology 2016;6(10):1062‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
BSACI 2017
- Scadding GK, Kariyawasam HH, Scadding G, Mirakian R, Buckley RJ, et al. BSACI guidelines for the management of allergic and non‐allergic rhinitis (Revised Edition 2017). Clinical and Experimental Allergy 2017;47(7):856‐89. [DOI: 10.1111/cea.12953] [DOI] [PubMed] [Google Scholar]
Chong 2016
- Chong LY, Head K, Hopkins C, Philpott C, Glew S, Scadding G, et al. Saline irrigation for chronic rhinosinusitis. Cochrane Database of Systematic Reviews 2016, Issue 4. [DOI: 10.1002/14651858.CD011995.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Chusakul 2013
- Chusakul S, Warathanasin S, Suksangpanya N, Phannaso C, Ruxrungtham S, Snidvongs K, et al. Comparison of buffered and nonbuffered nasal saline irrigations in treating allergic rhinitis. Laryngoscope 2013;123:53‐6. [DOI] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ (Clinical research ed.) 1997;315(7109):629‐34. [PUBMED: 9310563] [DOI] [PMC free article] [PubMed] [Google Scholar]
Elkins 2011
- Elkins MR, Bye PTP. Mechanisms and applications of hypertonic saline. Journal of the Royal Society of Medicine 2011;104:S2‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Georgitis 1994
- Georgitis JW. Nasal hyperthermia and simple irrigation for perennial rhinitis. Changes in inflammatory mediators. Chest 1994;106(5):1487‐92. [DOI] [PubMed] [Google Scholar]
Handbook 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Hermelingmeier 2012
- Hermelingmeier KE, Weber RK, Hellmich M, Heubach CP, Mosges R. Nasal irrigation as an adjunctive treatment in allergic rhinitis: a systematic review and meta‐analysis. American Journal of Rhinology & Allergy 2012;26(5):e119‐25. [DOI: 10.2500/ajra.2012.26.3787] [DOI] [PMC free article] [PubMed] [Google Scholar]
Katelaris 2012
- Katelaris CH, Lee BW, Potter PC, Maspero JF, Cingi C, Lopatin A, et al. Prevalence and diversity of allergic rhinitis in regions of the world beyond Europe and North America. Clinical & Experimental Allergy 2012;42(2):186–207. [DOI] [PubMed] [Google Scholar]
Khianey 2012
- Khianey R, Oppenheimer J. Is nasal saline irrigation all it is cracked up to be?. Annals of Allergy, Asthma & Immunology 2012;109:20‐8. [DOI] [PubMed] [Google Scholar]
Kim 2008
- Kim H, Bouchard J, Renzi PM. The link between allergic rhinitis and asthma: a role for antileukotrienes?. Canadian Respiratory Journal 2008;15(2):91‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
King 2015
- King D, Mitchell B, Williams CP, Spurling GKP. Saline nasal irrigation for acute upper respiratory tract infections. Cochrane Database of Systematic Reviews 2015, Issue 4. [DOI: 10.1002/14651858.CD006821.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mims 2014
- Mims JW. Epidemiology of allergic rhinitis. International Forum of Allergy & Rhinology 2014;4:S18‐20. [DOI] [PubMed] [Google Scholar]
Pynnonen 2007
- Pynnonen MA, Mukerji SS, Kim HM, Adams ME, Terrell JE. Nasal saline for chronic sinonasal symptoms: a randomized controlled trial. Archives of Otolaryngology‐‐Head & Neck Surgery 2007;133(11):1115‐20. [DOI] [PubMed] [Google Scholar]
Rabago 2005
- Rabago D, Pasic T, Zgierska A, Mundt M, Barrett B, Maberry R. The efficacy of hypertonic saline nasal irrigation for chronic sinonasal symptoms. Otolaryngology ‐ Head and Neck Surgery 2005;133:3‐8. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Schoenwetter 2004
- Schoenwetter WF, Dupclay L Jr, Appajosyula S, Botteman MF, Pashos CL. Economic impact and quality‐of‐life burden of allergic rhinitis. Current Medical Research and Opinion 2004;20(3):305‐17. [DOI] [PubMed] [Google Scholar]
Wormald 2004
- Wormald PJ, Cain T, Oates L, Hawke L, Wong I. A comparative study of three methods of nasal irrigation. Laryngoscope 2004;14:2224–7. [DOI] [PubMed] [Google Scholar]