

Abstract
Background
Initial arch wires are the first arch wires to be inserted into the fixed appliance at the beginning of orthodontic treatment and are used mainly for the alignment of teeth by correcting crowding and rotations. With a number of different types of orthodontic arch wires available for initial tooth alignment, it is important to understand which wire is most efficient, as well as which wires cause least amount of root resorption and pain during the initial aligning stage of treatment. This is an update of the review entitledInitial arch wires for alignment of crooked teeth with fixed orthodontic braces, which was first published in 2010.
Objectives
To assess the effects of initial arch wires for the alignment of teeth with fixed orthodontic braces, in terms of the rate of tooth alignment, amount of root resorption accompanying tooth movement, and intensity of pain experienced by patients during the initial alignment stage of treatment.
Search methods
Cochrane Oral Health's Information Specialist searched the following databases: Cochrane Oral Health's Trials Register (to 5 October 2017), the Cochrane Central Register of Controlled Trials (CENTRAL) (the Cochrane Library, 2017, Issue 9), MEDLINE Ovid (1946 to 5 October 2017), and Embase Ovid (1980 to 5 October 2017. The US National Institutes of Health Trials Registry (ClinicalTrials.gov) and the World Health Organization International Clinical Trials Registry Platform were searched for ongoing trials. No restrictions were placed on the language or date of publication when searching the electronic databases.
Selection criteria
We included randomised controlled trials (RCTs) of initial arch wires to align teeth with fixed orthodontic braces. We included only studies involving participants with upper or lower, or both, full arch fixed orthodontic appliances.
Data collection and analysis
Two review authors were responsible for study selection, 'Risk of bias' assessment and data extraction. We resolved disagreements by discussion between the review authors. We contacted corresponding authors of included studies to obtain missing information. We assessed the quality of the evidence for each comparison and outcome as high, moderate, low or very low, according to GRADE criteria.
Main results
For this update, we found three new RCTs (228 participants), bringing the total to 12 RCTs with 799 participants. We judged three studies to be at high risk of bias, and three to be at low risk of bias; six were unclear. None of the studies reported the adverse outcome of root resorption. The review assessed six comparisons.
1. Multistrand stainless steel versus superelastic nickel‐titanium (NiTi) arch wires. There were five studies in this group and it was appropriate to undertake a meta‐analysis of two of them. There is insufficient evidence from these studies to determine whether there is a difference in rate of alignment between multistrand stainless steel and superelastic NiTi arch wires (mean difference (MD) ‐7.5 mm per month, 95% confidence interval (CI) ‐26.27 to 11.27; 1 study, 48 participants; low‐quality evidence). The findings for pain at day 1 as measured on a 100 mm visual analogue scale suggested that there was no meaningful difference between the interventions (MD ‐2.68 mm, 95% CI ‐6.75 to 1.38; 2 studies, 127 participants; moderate‐quality evidence).
2. Multistrand stainless steel versus thermoelastic NiTi arch wires. There were two studies in this group, but it was not appropriate to undertake a meta‐analysis of the data. There is insufficient evidence from the studies to determine whether there is a difference in rate of alignment between multistrand stainless steel and thermoelastic NiTi arch wires (low‐quality evidence). Pain was not measured.
3. Conventional NiTi versus superelastic NiTi arch wires. There were three studies in this group, but it was not appropriate to undertake a meta‐analysis of the data. There is insufficient evidence from these studies to determine whether there is any difference between conventional and superelastic NiTi arch wires with regard to either alignment or pain (low‐ to very low‐quality evidence).
4. Conventional NiTi versus thermoelastic NiTi arch wires. There were two studies in this group, but it was not appropriate to undertake a meta‐analysis of the data. There is insufficient evidence from these studies to determine whether there is a difference in alignment between conventional and thermoelastic NiTi arch wires (low‐quality evidence). Pain was not measured.
5. Single‐strand superelastic NiTi versus coaxial superelastic NiTi arch wires. There was only one study (24 participants) in this group. There is moderate‐quality evidence that coaxial superelastic NiTi can produce greater tooth movement over 12 weeks (MD ‐6.76 mm, 95% CI ‐7.98 to ‐5.55). Pain was not measured.
6. Superelastic NiTi versus thermoelastic NiTi arch wires. There were three studies in this group, but it was not appropriate to undertake a meta‐analysis of the data. There is insufficient evidence from these studies to determine whether there is a difference in alignment or pain between superelastic and thermoelastic NiTi arch wires (low‐quality evidence).
Authors' conclusions
Moderate‐quality evidence shows that arch wires of coaxial superelastic nickel‐titanium (NiTi) can produce greater tooth movement over 12 weeks than arch wires made of single‐strand superelastic NiTi. Moderate‐quality evidence also suggests there may be no difference in pain at day 1 between multistrand stainless steel arch wires and superelastic NiTi arch wires. Other than these findings, there is insufficient evidence to determine whether any particular arch wire material is superior to any other in terms of alignment rate, time to alignment, pain and root resorption.
Plain language summary
What are the best materials to use for the first arch wire in a fixed brace?
Review question
We wanted to find out the best kind of wire arches for orthodontists to use when putting braces on people’s teeth to make them straighter. Our review evaluated whether different types of initial arch wires result in important differences, such as faster straightening of teeth, reduced pain or reduced side effects, such as the shortening of the tooth root during treatment with braces?
Background
Orthodontic treatment is undertaken worldwide to correct crowded, twisted, buried or prominent front teeth. This treatment is normally given in adolescence or adulthood. Fixed orthodontic appliances (braces) consist of brackets bonded to the teeth that are connected by arch wires, which exert forces on the teeth. The first (initial) type of arch wire, inserted at the beginning of treatment, is for correcting crowded and twisted teeth.
Over recent years, a number of new materials (various mixtures ('alloys') of nickel and titanium (NiTi)) have been developed, which show a range of different properties in the laboratory and which manufacturers claim offer benefits in terms of tooth alignment. This is an update of the review entitledInitial arch wires for alignment of crooked teeth with fixed orthodontic braces, which was first published in 2010.
Study characteristics
We searched for studies on 5 October 2017. We were interested in 'randomised controlled trials' (RCTs), which are studies in which participants are assigned randomly to the interventions being compared. We found 12 RCTs with 799 participants, all of whom had upper or lower full arch fixed braces, or both. The studies evaluated different initial arch wires, but they were poorly conducted or reported, or both, and their results are likely to be biased. The studies varied in a number of other aspects of orthodontic treatment, compared different types of initial arch wires and reported different outcomes at different times. None of the studies reported both potential benefits (straightening) and harms (pain or side effects such as tooth root shortening).
Main results
We found moderate‐quality evidence that coaxial superelastic nickel‐titanium (NiTi) can produce greater tooth movement over 12 weeks than single‐strand superelastic NiTi. We found moderate‐quality evidence that there is no difference in pain at day 1 between multistrand stainless steel versus superelastic NiTi arch wires. There is insufficient evidence from our included studies to know if any other particular initial arch wire material is better or worse than another, or if they function equally well, with regard to speed of straightening, pain or tooth shortening in people undergoing orthodontic treatment.
Quality of the evidence
There was moderate‐quality evidence that coaxial superelastic NiTi can produce greater tooth movement than single‐strand superelastic NiTi, and that there is no real difference in pain whether whether arch wires are made with multistrand stainless steel or superelastic NiTi. The quality of the evidence for all other comparisons and outcomes was low or very low. Overall, the evidence about initial arch wires in orthodontic treatment is very limited, with comparisons often assessed by one small study with problems in its design. The findings are imprecise and unreliable so more research is needed.
Summary of findings
Background
Description of the condition
Contemporary orthodontic treatment involves the use of both fixed and removable appliances. In recent years, it has been shown that the quality of the results obtained with fixed orthodontic appliances is superior to that obtained with removable orthodontic appliances (O'Brien 1993; Richmond 1993). Treatment with fixed orthodontic appliances has therefore become dominant in orthodontic practice throughout the world.
Orthodontic treatment is mainly carried out for adolescents and adults, and is concerned primarily with correcting crowded, rotated, buried or prominent front teeth. Epidemiological investigation reveals that there is a considerable range in estimates of proportion of 13‐ to 15‐year‐olds requiring orthodontic treatment, from 29% in Nairobi (Ng'ang'a 1997) to 77% in northeast Brazil (Marques 2007). It is also reported that over 52.3% of 12‐year‐old children in South Africa have an identifiable malocclusion (Van Wyk 2005), and 23.5% of the 12‐year‐olds and 18.5% of 15‐ to 16‐year‐olds in Spain have a definite treatment need (Manzanera 2009). The percentage of 12‐ and 15‐year‐olds in the UK with unmet orthodontic treatment need are 37% and 20%, respectively (HSCIC 2015). Adults also request orthodontic treatment, and comprised about 24% of cases in US orthodontic practices in 2014 (Keim 2014).
Description of the intervention
Fixed orthodontic appliance treatment uses arch wires to exert force upon teeth.
Treatment is carried out in stages and selection of appropriate arch wires contribute to treatment success. There is no one arch wire ideal for all stages of fixed appliance treatment. The initial arch wire is the first arch wire to be inserted into the fixed appliance at the beginning of the treatment and is used mainly for correcting crowding and minor tooth rotations. Light, continuous forces (also known as optimal forces) are thought to be the most desirable to achieve controlled and predictable tooth movement with minimum harm to the teeth and supporting tissues (Ballard 2009; Burstone 1981; Burstone 1985; Linge 1991). Clinically, this means that optimal forces result in the maximum speed of tooth movement with the minimum of root resorption and pain for the patient.
The forces delivered by the arch wires depend largely on the physical properties of the wire material and dimensions of the wire. The initial arch wires must be biocompatible and ideally have:
low stiffness to deliver light forces on activation;
high strength and resistance to permanent deformation;
good range to be able to maximise activations so there is elastic behaviour over weeks to months;
ease of engagement within fixed appliance attachments;
low cost (Kapila 1989; Kusy 1997; Proffit 2000).
The performance of arch wires is determined not only by the material properties, but also by geometric factors, such as the cross‐sectional shape (whether the arch wire is circular, rectangular, or square), length (i.e. interbracket span) and diameter. It is a general rule that for a certain material, as the diameter of a wire decreases, its strength decreases, while conversely as diameter increases, its stiffness increases. There has been an evolution of the materials available to apply forces to teeth (Evans 1996; Kusy 1997; Kusy 2007; Quintão 2009). The earliest wires were judged by their structural properties, that is, strength and flexibility. Wire size and shape then became more important as the stiffness of materials available at that time were virtually identical. Now it is possible to have wires that are the same size and shape, but of variable stiffness because of the mechanical properties of their constituent materials.
Precious metal alloys (e.g. gold) were historically used for the fabrication of initial arch wires, but high material costs limited their use and they are now virtually obsolete in orthodontics. Stainless steel replaced gold, offering comparatively good strength and springiness, corrosion resistance and low cost. Stainless steel arch wires can be bent to almost any desired shape without breaking. Increasing the length of wire using loops increases the flexibility of the arch wire to enable use as an initial aligning arch wire. This can be time consuming as each wire must be customised by the orthodontist for the individual patient. Another method of increasing the flexibility of stainless steel arch wires was the development of a multistrand wire. Multistrand wires are generated by twisting two or more strands of a small diameter wire (≤ 0.01 inch), therefore turning a springy wire into a cable. Among stainless steel wires, multistrand wires offer an impressive combination of strength and spring qualities. The properties of multistrand wires depend both on the characteristics of the individual wire strands and on how tightly they have been woven together during their manufacture (Kusy 1997; Proffit 2000).
The developments in nickel‐titanium (NiTi) wire technology have resulted in a decline in the popularity of stainless steel wires for initial alignment. However, stainless steel arch wires are still used by a small proportion of orthodontists. NiTi is a metal alloy that can exist in two different crystalline or lattice forms namely the martensitic (M) form and the austenitic (A) form. Each has its own physical and mechanical properties. Transition between the two forms or phases can be induced by applied stress or a change in temperature and this changes the properties of the wire without affecting its integrity. Alternatively, a NiTi alloy can be manufactured in a stable form, so that there is no possibility of phase transition. Wires manufactured as the active form have both phases existing simultaneously in variable proportions. It is the ability of the two phases to coexist that gives rise to the superelastic properties of active NiTi alloys. Superelasticity (also known as plateau behaviour) means that wires exert about the same force irrespective of whether they are deflected either a relatively small or large distance, which is a unique and extremely desirable characteristic, especially in initial aligning arch wires. The temperature at which the alloy converts from one phase to another is known as the transition temperature (TTR) and this can be preset during manufacturing.
It is important to have an understanding of the transitions that NiTi materials undergo to make full use of the benefits of these properties (Santoro 2001a; Santoro 2001b). Austenite is the high‐temperature form of the alloy and is able to memorise a preformed shape. When a wire is predominantly austenite, it behaves more elastically than stainless steel but is not superelastic. To activate superelasticity requires the formation of the martensite form. This is the low‐temperature form of the alloy and is easily pliable. It is generated by cooling below the TTR, but can be helped by deflecting the wire at least 2 mm. This is called stress‐induced martensitic transformation (SIMT). However, this SIMT raises the preset TTR. For maximum clinical effectiveness, the TTR should be set near to or just below mouth temperature, but the TTR should be calculated under proper conditions of deflection to take into account the conditions experienced during clinical use.
NiTi wires can be classified according to the crystal structure and phase transformation as follows (Evans 1996).
Stabilised, e.g. Nitinol, Titanal and Orthonol
Superelastic active austenitic, e.g. Sentalloy
Thermodynamic‐active martensitic, e.g. copper‐NiTi and Neosentalloy
Graded thermodynamic, e.g. Bioforce
At the clinical level, the elastic properties of NiTi are independent of whether it is operating clinically in the austenitic or superelastic plateau. It is likely that, in clinical use, many superelastic wires do not exhibit superelastic or plateau behaviour or require excessive deflection to do so. They may also be delivering excessive force even in the presence of plateau behaviour (Santoro 2001b). Despite commercial claims, low values of force delivery remain theoretical and are based on in vitro testing for most NiTi alloys (Santoro 2001a). These need to be verified through properly designed clinical trials, taking into account the temperature range of testing, method of ligation, interbracket distance, bracket type and length of wire.
The selection of an appropriate NiTi wire can be difficult. There is often a lack of accurate information about expected TTRs. This is compounded by variation in properties between batches from the same manufacturer and between different manufacturers for supposedly similar wires (Bellini 2016). There also needs to be better clarity about product terminology with reference to standard or approved definitions in order to make meaningful comparisons and substantiate manufacturers' claims of improved clinical performance of the bewildering array of new products offered to the orthodontist.
How the intervention might work
Manufacturers of arch wires claim that arch wire materials have specific properties, determined by laboratory testing, that make them ideal for use in clinical orthodontics. However, as described above, there are a number of factors that may be expected to influence the performance of any given arch wire in clinical use. Type of wire and properties produced during manufacture (Bellini 2016), type and size of brackets used, distance between brackets, degree of initial 'misalignment' of teeth and duration of treatment may all influence the success of orthodontic treatment.
Manufacturers' claims of increased efficiency of the newer arch wire alloys are used to justify their increased cost. Stainless steel archwires deliver springiness by bending loops (increasing the length of the wire) or winding several wires of small diameter around each other (coax or multi‐strand). NiTi arch wires have many theoretical advantages over other wire types for the initial alignment of teeth. Perhaps the most important is that superelastic NiTi arch wires are said to exert the same force irrespective of whether they are deflected a little or a lot, which is particularly valuable in the initial alignment stage.
Why it is important to do this review
Cochrane Oral Health undertook an extensive prioritisation exercise in 2014 to identify a core portfolio of titles that were the most clinically important ones to maintain in the Cochrane Library (Worthington 2015). This review was identified as a priority title by the orthodontic expert panel (Cochrane Oral Health priority review portfolio).
Many studies support manufacturers' claims concerning the performance of various arch wire types in a controlled laboratory environment. However, for orthodontists and their patients, the performance of these materials in vivo is much more important. Early clinical trials failed to demonstrate improved alignment associated with the new arch wire materials. There is a need for a systematic review to critically appraise and summarise the results of clinical trials comparing the effects of different materials used for initial arch wires. With a number of orthodontic arch wires available for initial tooth alignment, it is important to understand which wire is most efficient in terms of rate of alignment, as well as which wire causes the least amount of root resorption and pain during the initial aligning stage of orthodontic treatment. We must emphasise that this review analyses the initial archwires only and does not assess other orthodontic stages.
Objectives
To assess the effects of initial arch wires for the alignment of teeth with fixed orthodontic braces, in terms of the rate of tooth alignment, amount of root resorption accompanying tooth movement, and intensity of pain experienced by patients during the initial alignment stage of treatment.
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) in this review.
Types of participants
We included participants with upper or lower, or both, full arch fixed orthodontic appliances. We excluded participants with palatal expansion devices or extraoral appliances that were being used concurrently. We also excluded participants who had had previous active orthodontic treatment or relevant medical history.
Types of interventions
Initial arch wires are the first arch wires inserted into fixed orthodontic appliances at the beginning of treatment. This excludes arch wires used at subsequent orthodontic appointments. The comparisons between arch wires were undertaken in terms of their:
material;
cross‐sectional shape; and
cross‐sectional size.
Types of outcome measures
Primary outcomes
Alignment rate: tooth movement measured over a period of time (e.g. measured over 4, 8 or 12 weeks)
Incidence/prevalence and amount of root resorption
Secondary outcomes
Time to next/working arch wire
Time to alignment
Pain: intensity of pain experienced by participants measured on a visual analogue scale (VAS) or categorical scale, and duration of pain. We assessed pain scores at specific time points after the initial arch wires had been inserted. In addition, we considered analgesic consumption to be an indirect measurement of pain.
Search methods for identification of studies
Electronic searches
Cochrane Oral Health's Information Specialist conducted systematic searches in the following databases for RCTs and controlled clinical trials. There were no language, publication year or publication status restrictions:
Cochrane Oral Health’s Trials Register (searched 5 October 2017) (Appendix 1);
Cochrane Central Register of Controlled Trials (CENTRAL; 2017, Issue 9) in the Cochrane Library (searched 5 October 2017) (Appendix 2);
MEDLINE Ovid (1946 to 5 October 2017) (Appendix 3);
Embase Ovid (1980 to 5 October 2017) (Appendix 4).
Subject strategies were modelled on the search strategy designed for MEDLINE Ovid. Where appropriate, they were combined with subject strategy adaptations of the highly sensitive search strategy designed by Cochrane for identifying RCTs and controlled clinical trials as described in the Cochrane Handbook for Systematic Reviews of Interventions, Chapter 6 (Lefebvre 2011).
Searching other resources
The following trial registries were searched for ongoing studies:
US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (clinicaltrials.gov; searched 5 October 2017) (Appendix 5);
World Health Organization International Clinical Trials Registry Platform (apps.who.int/trialsearch; searched 5 October 2017) (Appendix 6).
Grey literature
We searched conference proceedings and abstracts via IADR Abstract Search Form (https://iadr.abstractarchives.com/search, from 2012 to 2017) (Appendix 7).
Handsearching
We carried out handsearching of the following journals:
American Journal of Orthodontics and Dentofacial Orthopedics (1986 to November 2017);
The Angle Orthodontist (1994 to September 2017);
European Journal of Orthodontics (1979 to October 2017);
Journal of Orthodontics (formerly the British Journal of Orthodontics) (2000 to September 2017);
Seminars in Orthodontics (1995 to September 2017);
Clinical Orthodontics and Research (1998 to December 2016);
Australian Orthodontic Journal (1956 to December 2016).
Reference lists
We checked the reference lists of potential clinical trials to identify any additional studies.
Correspondence
We contacted the corresponding authors of all included studies in an attempt to identify unpublished or ongoing studies and to clarify trial details, if required. We contacted manufacturers to confirm the type of arch wires and also asked about their knowledge of any unpublished or ongoing clinical trials.
Data collection and analysis
Selection of studies
Two review authors independently assessed the titles and abstracts (when available) of all reports identified by the search strategies as being potentially relevant to the review. The search was designed to be sensitive and include controlled clinical trials, these were filtered out early in the selection process if they were not randomised. We then obtained the full reports for all studies that appeared to meet the inclusion criteria, or if there was insufficient information to make a clear decision, or where there was disagreement between the review authors about eligibility. We assessed the full reports to verify whether the studies met the inclusion criteria. Any disagreements between the two review authors were resolved by discussion or the involvement of another review author as an arbiter. We kept a record of all decisions made about the identified studies. The review authors were not blinded to author(s), institution or site of publication of all studies.
We used the following screening exclusion criteria.
Studies other than RCTs
Studies not investigating fixed appliance orthodontic treatment
Studies not investigating initial arch wire interventions, including those with multiple wires as part of a sequence
Data extraction and management
Two review authors carried out data extraction independently and in duplicate. We resolved all disagreements by discussion with one of the other review authors in the team.
We collected the following data on a customised data collection form.
Date that the study was conducted
Year of publication
Treatments including details of material, size and brand of arch wire and type of fixed orthodontic appliances that were used
Duration of follow‐up
Sample size and the number of male participants and female participants per study group
Age of participants
Outcome measures
We recorded data on the cost of arch wires and amount of time for arch wire placement.
Assessment of risk of bias in included studies
Two review authors independently undertook the 'Risk of bias' assessment in each of the included studies. We resolved disagreements by discussion or the involvement of another review author. We carried out 'Risk of bias' assessments using the Cochrane tool for assessing risk of bias and we completed a 'Risk of bias' table for each study as outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011a). We assessed seven domains, namely sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective outcome reporting and other sources of bias according to the tool. Each domain included one or more specific entries in a 'Risk of bias' table. Within each entry, we described what was reported in the study and assigned a judgement relating to the risk of bias for that entry. Where the study clearly reported methodology, we gave a judgment of 'low risk' of bias or 'high risk' of bias. Where trial methodology was unclear, we judged a domain at 'unclear risk' of bias, unless and until further information was available.
After taking into account the additional information provided by the authors of the studies, we assessed the overall risk of bias in included studies over all seven domains. We graded studies into the following categories.
Low risk of bias (plausible bias unlikely to seriously alter the results)
Moderate risk of bias (plausible bias that raises some doubt about the results)
High risk of bias (plausible bias that seriously weakens confidence in the results)
We reassessed all nine studies included in the previous version of the review (Jian 2013), as we were uncertain that the judgements made in 2013 were fully justified, especially in terms of blinding and selective outcome reporting.
Measures of treatment effect
We planned to follow the statistical procedures outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Deeks 2011) and to analyse the data using Review Manager 5 (RevMan 5) software (RevMan 2014), and report it according to Cochrane criteria. We calculated the risk ratio (RR) and corresponding 95% confidence intervals (CIs) for dichotomous data, and mean difference (MD) and 95% CIs for the continuous data.
Unit of analysis issues
Most of the included studies randomised participants to different types of initial arch wires. However, when the unit of randomisation was a dental arch, and a participant contributed more than one dental arch to the study, there was potential for unit of analysis errors to occur. If this was unclear, we planned to ask study authors to clarify how this dependence had been accounted for in the analysis. If no adjustment had been made, we would have taken this into account in interpreting the confidence interval of the effect size (Whiting‐O'Keefe 1984).
Where repeated measures were made (e.g. pain measurements over several days), we chose to report only pain outcomes on days 1 and 7 as these time points are likely to provide clinically meaningful data.
Dealing with missing data
We contacted the original investigators of the studies to request any missing data or identify the reason for missing data. However, due to the absence of individual participant data, it was impossible to undertake an intention‐to‐treat analysis.
Assessment of heterogeneity
For each meta‐analysis, we assessed clinical heterogeneity by examining characteristics of studies and similarities between types of participants, interventions and outcomes. We used Cochrane's Chi2 test to determine the presence of statistical heterogeneity at a significance level of 0.1 (Deeks 2011). We used the I2 statistic (Higgins 2003) (plus 95% CI) to quantify the degree of statistical heterogeneity as follows:
0% to 40% may indicate slight heterogeneity;
30% to 60% may indicate moderate heterogeneity;
50% to 90% may indicate substantial heterogeneity;
75% to 100% may indicate very substantial heterogeneity.
Where there was substantial or very substantial heterogeneity, we provided a narrative description of the results instead of pooling data.
Assessment of reporting biases
Although we had planned to assess reporting biases, it was not appropriate to use funnel plots to assess publication bias along with the statistical methods described by Egger 1997, because we did not undertake any meta‐analyses.
Data synthesis
We planned to conduct meta‐analyses, but these were not possible because the included studies involved a variety of interventions. We would have calculated MDs with 95% CIs for continuous outcomes, and RRs with 95% confidence intervals for dichotomous outcomes, using the fixed‐effect model for fewer than four studies, and the random‐effects model for four or more studies.
Subgroup analysis and investigation of heterogeneity
We proposed subgroup analysis for different age groups, however, we were unable to undertake a meta‐analysis, so subgroup analysis was not possible.
Sensitivity analysis
Although we had planned to carry out sensitivity analysis to examine the effect of risk of bias on the assessment of the overall estimates of effect, we could not do this because we did not undertake any meta‐analyses.
'Summary of findings' table
We created a 'Summary of findings' table for each comparison and presented summary information for alignment rate, time to alignment, pain and root resorption. Two review authors independently assessed the quality of the evidence using GRADE criteria (GRADE 2004; Schünemann 2011).
Results
Description of studies
See Characteristics of included studies and Characteristics of excluded studies.
Results of the search
The search on 5 October 2017 identified 957 articles, with 609 records after duplicate removal. After scanning the titles and abstracts, we considered nine articles to be potentially eligible. We obtained the full‐texts of these reports, and three studies (four reports) were eligible for inclusion in this update. Therefore, we added three studies to the previous review (Abdelrahman 2015a; Sandhu 2013; Quintão 2005), giving a total of 12 studies that fulfilled the criteria for inclusion (Abdelrahman 2015a; Cioffi 2012; Cobb 1998; Evans 1998; Fernandes 1998; Jones 1992; O'Brien 1990; Pandis 2009; Quintão 2005; Sandhu 2013; Sebastian 2012; West 1995). Figure 1 shows the flow of records and studies in this review.
1.
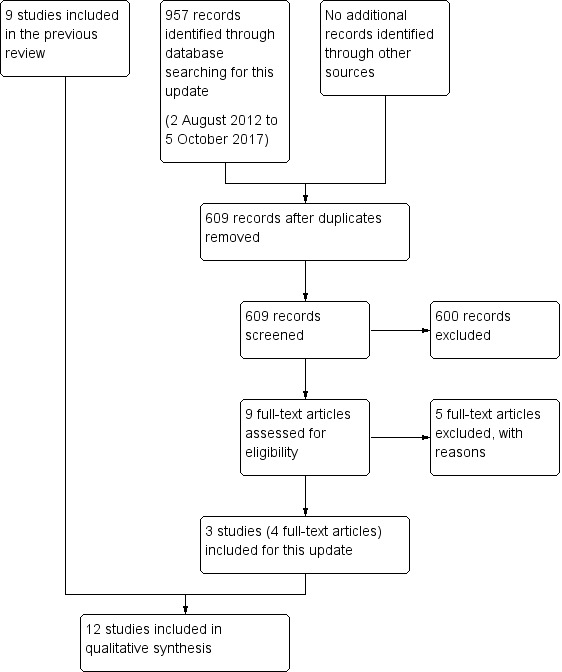
Study flow diagram
Included studies
Design
Of the 12 included studies, eight studies were two‐arm, parallel‐group design (Cioffi 2012; Fernandes 1998; Jones 1992; O'Brien 1990; Pandis 2009; Sandhu 2013; Sebastian 2012; West 1995); three studies were three‐arm, parallel‐group design (Abdelrahman 2015a; Cobb 1998; Evans 1998); and one study was four‐arm, parallel‐group design (Quintão 2005). In addition, Evans 1998 was factorial design, and Cobb 1998 was a stratified RCT with the bracket slot size as a stratification factor. Moreover, five studies were double‐blind RCTs (Abdelrahman 2015a; Cioffi 2012; Pandis 2009; Sandhu 2013; Sebastian 2012).
Two studies reported external funding sources (Cobb 1998; Evans 1998); one reported internal funding sources (Cioffi 2012), and O'Brien 1990 reported the supplement of arch wires; the other eight did not report any information concerning funding.
Settings
Of the 12 included studies, four were conducted in the UK (Evans 1998; Jones 1992; O'Brien 1990; West 1995), two in India (Sandhu 2013; Sebastian 2012), and one each in Brazil (Quintão 2005), Greece (Pandis 2009), Italy (Cioffi 2012), Jordan (Abdelrahman 2015a), Norway (Fernandes 1998), and the USA (Cobb 1998).
The settings for the included studies were university clinics, faculty practices and private practices: five in university clinics (Cioffi 2012; Evans 1998; Jones 1992; Quintão 2005; West 1995); Pandis 2009 in private practices; Cobb 1998 in both university practices and faculty practices; Abdelrahman 2015a and Fernandes 1998 in both university practices and private practices; and the other three studies' settings were unknown. Eight studies were set in a single centre (Cioffi 2012; Jones 1992; O'Brien 1990; Pandis 2009; Quintão 2005; Sandhu 2013; Sebastian 2012; West 1995), Evans 1998 in two centres, Fernandes 1998 in three centres, Cobb 1998 in 13 centres, and it was not clear if Abdelrahman 2015a was a single‐ or multi‐centre study.
Participants
The 12 included studies randomised a total of 799 participants with 952 arches to different arch wires. All the studies reported participant age. Nine studies reported the sex of the participants (Abdelrahman 2015a; Cioffi 2012; Fernandes 1998; Jones 1992; Pandis 2009; Quintão 2005; Sandhu 2013; Sebastian 2012; West 1995), with Sebastian 2012 including only female participants.
Lower arch wires only were placed and assessed in three studies (Pandis 2009; Sandhu 2013; Sebastian 2012). Upper arch wires only were placed and assessed in one study (O'Brien 1990). Upper or lower arch wires, or both, were placed and assessed in seven studies (Cioffi 2012; Cobb 1998; Evans 1998; Fernandes 1998; Jones 1992; Quintão 2005; West 1995). Upper or lower arch wires, or both, were placed but only lower arch wires assessed in one study (Abdelrahman 2015a).
Sample sizes
The sample sizes ranged from 24 to 128 participants. Eight studies reported the sample size calculation (Abdelrahman 2015a; Cioffi 2012; Evans 1998; Jones 1992; Pandis 2009; Sandhu 2013; Sebastian 2012; West 1995).
Interventions
The 12 included studies evaluated different arch wire materials and diameters, placed with different types and sizes of brackets, and reported different outcomes, measured in different ways, at different time points. It was difficult to place the arch wires used in the included studies into groups because there was little information reported about the specific characteristics of each arch wire material, possibly due to the commercial sensitivity of such detailed information. For this reason, we have noted all the available information, including trade names, in the Characteristics of included studies tables.
The studies made the following comparisons.
Multistrand stainless steel versus
Superelastic NiTi (Cobb 1998; Jones 1992; Quintão 2005; Sandhu 2013; West 1995), including superelastic ion‐implanted NiTi (Cobb 1998)
Thermoelastic NiTi (Evans 1998; Quintão 2005).
Conventional NiTi versus
Superelastic NiTi (Abdelrahman 2015a; Fernandes 1998; O'Brien 1990)
Thermoelastic NiTi (Abdelrahman 2015a), including copper thermoelastic NiTi (Pandis 2009)
-
Superelastic single‐stranded NiTi versus
Superelastic coaxial NiTi (Sebastian 2012)
Thermoelastic NiTi (Abdelrahman 2015a; Cioffi 2012; Quintão 2005).
All of the studies compared two or more types of round wires apart from Evans 1998, where both types of wires were 0.016 x 0.022‐inch and rectangular in cross‐section.
Outcomes
Primary outcomes
Alignment rate
Seven studies measured this outcome (Abdelrahman 2015a; Cobb 1998; Evans 1998; O'Brien 1990; Quintão 2005; Sebastian 2012; West 1995).
Abdelrahman 2015a reported mean Little's Irregularity Index (LII) (Little 1975) of three different NiTi arch wire groups at 0 weeks (initial treatment), 8 weeks and 16 weeks.
Cobb 1998 measured anterior irregularity each month following arch wire placement but presented results in graphs only and did not report data for rate of alignment.
Evans 1998 used a factorial design in which arches were randomly allocated to different arch wire types. This trial reported tooth movement after four and eight weeks of treatment as contact point movement (mm) for each archwire. However, due to the design used, we would have expected data to be analysed taking into account the pair of arch wires in each participant and in which arch the wire was placed. The report states the mean movement for each wire as if this were independent of other confounding factors.
O'Brien 1990 reported the rate of alignment in terms of the three‐dimensional contact point movements of the upper anterior arches over a period of 35 days.
Quintão 2005 measured the three‐dimensional contact point movements of two different steels and two different NiTi arch wires based on LII after eight weeks of treatment.
Sebastian 2012 reported alignment associated with two different NiTi arch wires after 4, 8 and 12 weeks.
West 1995 reported mean duration of the trial for each wire, with 95% CIs, but in the absence of a clearly defined endpoint for the trial we were unable to interpret this as time to alignment. Alignment was reported as an index of tooth alignment (NiTi/stainless steel).
Incidence/prevalence and amount of root resorption
No included study in this systematic review reported root resorption.
Secondary outcomes
Time to next/working arch wire
Only one included study measured this outcome, and reported time to next arch wire for each wire type but did not appear to adjust for the paired nature of the data and did not present any estimates of variance (Evans 1998).
Time to alignment
Cobb 1998 measured time to alignment, and defined alignment as an Irregularity Index of 2 mm or less. However, no numerical data were reported (graphs only).
Pandis 2009 reported mean time to alignment for the comparison between conventional NiTi and thermoelastic copper NiTi arch wires.
Abdelrahman 2015a reported mean time (weeks) to alignment of three different NiTi arch wire groups.
Pain
Four studies reported intensity of pain measured on a 100 mm VAS as an outcome, daily over the seven days following arch wire placement (Cioffi 2012; Fernandes 1998; Jones 1992; Sandhu 2013). One reported analgesic consumption as an outcome (Fernandes 1998).
Excluded studies
We excluded 10 studies because our examination of the full papers indicated that they were not RCTs (Abdelrahman 2015b; Dalstra 2004; Huffman 1983; Jones 1984; Jones 1990; Kuftinec 1980; Lew 1988; Marković 2015; Sandhu 2012; Weiland 2003). We excluded two studies because the intervention was an arch wire sequence rather than an initial arch wire (Mandall 2006; Ong 2011), and six studies because the interventions were not initial arch wires for alignment (AlQabandi 1999; Campos 2013; Farzanegan 2012; Fleming 2009a; Fleming 2009b; Pandis 2007). Two studies were published only as abstracts and our attempts to obtain either a full report or additional information from the study authors were unsuccessful (Bloom 1998; Chekay 1999).
We excluded one ongoing study from the previous version of this review from this update (Bernhold 2001). This study was published as an abstract and attempts to contact the study author were unsuccessful, but the abstract contained insufficient information to include in this review.
Risk of bias in included studies
The summary of our 'Risk of bias' assessments for included studies is shown in Figure 2; a 'Risk of bias' graph is shown in Figure 3 and details of our assessments are shown in the 'Risk of bias' tables of the Characteristics of included studies.
2.
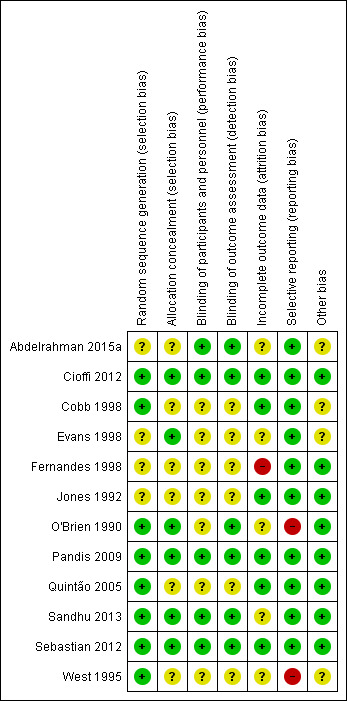
Risk of bias summary: review authors' judgements about each risk of bias item for each included study
3.
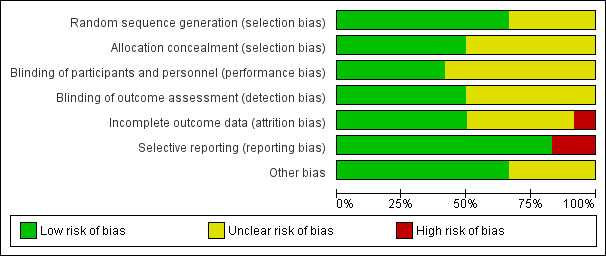
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies
Allocation
Sequence generation
Seven studies described the method of sequence generation clearly (Cioffi 2012; Cobb 1998; Pandis 2009; Quintão 2005; Sandhu 2013; Sebastian 2012; West 1995), and the lead author of O'Brien 1990 provided this information on request. We assessed these eight studies as being at low risk of bias for this domain. In the remaining four studies, there was no information provided on the method of sequence generation and therefore we assessed this domain at unclear risk of selection bias.
Allocation concealment
Four studies reported allocation concealment clearly (Cioffi 2012; Pandis 2009; Sandhu 2013; Sebastian 2012), and information was provided in two studies (Evans 1998; O'Brien 1990), so we assessed these six studies as low risk of bias for this domain. The remaining six studies did not mention allocation concealment in their methods and therefore we assessed them to be at unclear risk of bias.
Blinding
Blinding of participants
Blinding of participants is likely to be important in terms of reducing performance bias in studies where the outcome is subjective, for example, participant‐reported pain. We assessed the five double‐blind RCTs to be at low risk of bias for this domain (Abdelrahman 2015a; Cioffi 2012; Pandis 2009; Sandhu 2013; Sebastian 2012). We assessed the remaining seven studies as being at unclear risk of performance bias.
Blinding of outcome assessors
Blinding of outcome assessment was clearly reported in five double‐blind RCTs (Abdelrahman 2015a; Cioffi 2012; Pandis 2009; Sandhu 2013; Sebastian 2012), and the study author supplied this information for O'Brien 1990, so we assessed these six studies as being at low risk of performance and detection bias. In the remaining six studies, there was no information provided on the method of sequence generation and we therefore assessed this domain as being at unclear risk of bias.
Incomplete outcome data
In four studies (Cioffi 2012; Pandis 2009; Quintão 2005; Sebastian 2012), all randomised participants were included in the outcome evaluations. In another two studies, the participants lost to follow‐up occupied less than 10% (Cobb 1998; Jones 1992). We evaluated these six studies as being at low risk of attrition bias.
In three studies (Abdelrahman 2015a; Evans 1998; Sandhu 2013), the ratio of participants excluded from analysis was between 10% and 20%. O'Brien 1990 and West 1995 did not report the numbers of evaluated participants. Thus we considered the risk of attrition bias to be unclear in these five studies.
Fernandes 1998 had some data (up to 38%) missing from some time points in both groups and we assessed it to be at high risk of attrition bias.
Selective reporting
Ten studies reported all their planned outcomes (Abdelrahman 2015a; Cioffi 2012; Cobb 1998; Evans 1998; Fernandes 1998; Jones 1992; Pandis 2009; Quintão 2005; Sandhu 2013; Sebastian 2012), so we assessed these studies as being at low risk of reporting bias. We assessed two studies as being at high risk of bias: in O'Brien 1990, the pain data that were recorded during the investigation were not reported since the researchers found these "not to be sufficiently reliable for analysis"; and West 1995 reported Index of Tooth Allignment (ITA) graphically only, without mean or median for each type of wire.
Other potential sources of bias
We considered four studies to be at risk of other sources of bias. In Abdelrahman 2015a, some participants had upper arches treated, the effect of which could not be estimated. The stratified randomisation on two slot sizes might have biased the results in Cobb 1998. The use of two different types of brackets might have affected the outcomes in Evans 1998. West 1995 did not report the ligation systems and slot sizes, so it was unclear whether the results were biased. We considered the remaining studies to be at low risk of other potential sources of bias.
Overall risk of bias
Three studies were at low risk (Cioffi 2012; Pandis 2009; Sebastian 2012), three studies were at high risk (Fernandes 1998; O'Brien 1990; West 1995), and the remaining six studies were at unclear risk.
Effects of interventions
See: Table 1; Table 2; Table 3; Table 4; Table 5; Table 6
Summary of findings for the main comparison. Multistrand stainless steel versus superelastic nickel‐titanium (NiTi) arch wires.
| Multistrand stainless steel versus superelastic NiTi arch wires | ||||||
|
Population: people receiving orthodontic treatment with fixed appliances
Settings: university clinics, faculty practices and private practices
Intervention: superelastic NiTi Control: multistrand stainless steel | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Superelastic NiTi | |||||
| Alignment rate between first molars Little's Irregularity Index Follow‐up: 8 weeks | Mean alignment rate in the control groups was 22.90 mm/8 weeks (11.45 mm per month) |
Mean alignment rate between first molars in the intervention groups was 7.5 mm/8 weeks faster (11.27 slower to 26.27 faster) | 48 (1 study) | ⊕⊕⊝⊝ low1 |
Cobb 1998 reported no statistically significant difference without numerical data. In West 1995, the superelastic NiTi wire was found to produce a statistically significant improved alignment of lower teeth, but there was no difference in upper teeth. |
|
| Time to alignment | Not measured | |||||
| Pain day 1 VAS (0‐100 mm) Follow‐up: 14‐15 days | Mean pain day 1 in the control groups ranged from 23.7 to 26.4 mm |
Mean pain day 1 in the intervention groups was 2.68 mm higher (1.38 lower to 6.75 higher) | 127 (2 studies) | ⊕⊕⊕⊝ moderate2 | MD of pain day 7 (multistrand stainless steel vs superelastic NiTi) was ‐0.37, 95% CI ‐0.91 to 0.17. | |
| Root resorption | Not measured | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; NiTi: nickel‐titanium | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded two levels due to very serious imprecision. 2Downgraded one level due to serious imprecision.
Summary of findings 2. Multistrand stainless steel versus thermoelastic nickel‐titanium (NiTi) arch wires.
| Multistrand stainless steel versus thermoelastic NiTi arch wires | ||||||
|
Population: people receiving orthodontic treatment with fixed appliances
Settings: university clinics, faculty practices and private practices
Intervention: thermoelastic NiTi Control: multistrand stainless steel | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Thermoelastic NiTi | |||||
| Alignment rate between first molars Little's Irregularity Index Follow‐up: 8 weeks | Mean alignment rate in the control groups was 22.90 mm/8 weeks (11.45 mm per month) |
Mean alignment rate between first molars in the intervention groups was 8.78 slower (27.79 slower to 10.23 faster) | 42 (1 study) | ⊕⊕⊝⊝ low1 | Evans 1998 also showed no statistically significant difference of alignment rate over 8 weeks. | |
| Time to alignment | Not measured | |||||
| Pain | Not measured | |||||
| Root resorption | Not measured | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; NiTi: nickel‐titanium | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded two levels due to very serious imprecision.
Summary of findings 3. Conventional nickel‐titanium (NiTi) versus superelastic NiTi arch wires.
| Conventional NiTi versus superelastic NiTi arch wires | ||||||
|
Population: people receiving orthodontic treatment with fixed appliances
Settings: university clinics, faculty practices and private practices
Intervention: superelastic NiTi Control: conventional NiTi | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Superelastic NiTi | |||||
| Alignment rate between canines Little's Irregularity Index Follow‐up: about 5 weeks | Mean alignment rate in the control groups was
1.42 mm/about 5 weeks (1.34 mm per month) |
Mean alignment rate between canines in the intervention groups was 0.28 faster (0.33 slower to 0.89 faster) | 40 (1 study) | ⊕⊝⊝⊝ very low1,2 | Abdelrahman 2015a also reported no statistically significant difference of alignment rate over 8 or 16 weeks. | |
| Time to alignment Follow‐up: 16 weeks | Mean time to alignment in the control groups was 9.8 weeks | Mean time to alignment in the intervention groups was 0.3 longer (1.14 shorter to 1.74 longer) | 49 (1 study) | ⊕⊕⊝⊝ low2 | ||
| Pain day 1 VAS (0‐100 mm) Follow‐up: 7 days | Mean pain in the control groups was 37.8 | Mean pain day 1 in the intervention groups was 1.1 mm lower (15.1 lower to 12.9 higher) | 79 (1 study) | ⊕⊝⊝⊝ very low1,2 | MD of pain day 7 (multistrand stainless steel versus superelastic NiTi) was ‐0.40, 95% CI ‐4.61 to 3.81 RR of analgesic consumption within 7 days (multistrand stainless steel versus superelastic NiTi) was 2.58, 95% CI 0.52 to 12.81 |
|
| Root resorption | Not measured | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; NiTi: nickel‐titanium; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded one level due to serious risk of bias: one study at high risk. 2Downgraded two levels due to very serious imprecision.
Summary of findings 4. Conventional nickel‐titanium (NiTi) versus thermoelastic NiTi arch wires.
| Conventional NiTi versus thermoelastic NiTi arch wires | ||||||
|
Population: people receiving orthodontic treatment with fixed appliances
Settings: university clinics, faculty practices and private practices
Intervention: thermoelastic NiTi Control: conventional NiTi | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Thermoelastic NiTi | |||||
| Alignment rate ratio (hazard ratio of Kaplan‐Meier survival estimates) Follow‐up: 6 months | Alignment rate ratio (thermoelastic: conventional) was 1.3 (0.68 to 2.50) |
HR 1.3 (0.68 to 2.50) |
60 (1 study) |
⊕⊕⊝⊝ low1 | Abdelrahman 2015a also reported no statistically significant difference of alignment rate over 8 or 16 weeks. | |
| Time to alignment Follow‐up: 16 weeks | Mean time to alignment in the control groups was 9.8 weeks | Mean time to alignment in the intervention groups was 0.2 shorter (1.64 shorter to 1.24 longer) | 49 (1 study) | ⊕⊕⊝⊝ low1 | ||
| Pain | Not measured | |||||
| Root resorption | Not measured | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; HR: hazard ratio; NiTi: nickel‐titanium | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded two levels due to very serious imprecision.
Summary of findings 5. Single‐strand superelastic nickel‐titanium (NiTi) versus coaxial superelastic NiTi arch wires.
| Single‐strand superelastic NiTi versus coaxial superelastic NiTi arch wires | ||||||
|
Population: people receiving orthodontic treatment with fixed appliances
Settings: university clinics, faculty practices and private practices
Intervention: coaxial superelastic NiTi Control: single‐strand superelastic NiTi | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Coaxial superelastic NiTi | |||||
| Alignment rate between canines Little's Irregularity Index Follow‐up: 12 weeks | Mean alignment rate in the control groups was
2.327 mm/8 weeks (1.164 mm per month) |
Mean alignment rate between canines in the intervention groups was 5.07 faster (4.16 faster to 5.99 faster) | 24 (1 study) | ⊕⊕⊕⊝ moderate1 | Sandhu 2013 reported that MD of alignment rate between canines over 12 weeks (single‐strand superelastic NiTi versus coaxial superelastic NiTi) was ‐6.76, 95% CI ‐7.98 to ‐5.55. | |
| Time to alignment | Not measured | |||||
| Pain | Not measured | |||||
| Root resorption | Not measured | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; NiTi: nickel‐titanium | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded from high to moderate as this finding needs to be confirmed as it is based on a single study of only 24 participants.
Summary of findings 6. Superelastic nickel‐titanium (NiTi) versus thermoelastic NiTi arch wires.
| Superelastic NiTi versus thermoelastic NiTi arch wires | ||||||
|
Population: people receiving orthodontic treatment with fixed appliances
Settings: university clinics, faculty practices and private practices
Intervention: thermoelastic NiTi Control: superelastic NiTi | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | Number of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
| Control | Thermoelastic NiTi | |||||
| Alignment rate between first molars Little's Irregularity Index Follow‐up: 8 weeks | Mean alignment rate in the control groups was 30.40 mm/8 weeks (15.20 mm per month) | Mean alignment rate between first molars in the intervention groups was 16.28 slower (36.61 slower to 4.05 faster) | 46 (1 study) | ⊕⊕⊝⊝ low1 | Abdelrahman 2015a also reported no statistically significant difference of alignment rate over 8 or 16 weeks | |
| Time to alignment Follow‐up: 16 weeks | Mean time to alignment in the control groups was 10.1 weeks | Mean time to alignment in the intervention groups was 0.5 shorter (1.78 shorter to 0.78 longer) | 50 (1 study) | ⊕⊕⊝⊝ low1 | ||
| Pain day 1 VAS (0‐100 mm) Follow‐up: 7 days | Mean pain in the control groups was 36.0 | Mean pain day 1 in the intervention groups was 7.0 mm lower (26.56 lower to 12.56 higher) | 30 (1 study) | ⊕⊕⊝⊝ low1 | MD of pain day 7 (superelastic NiTi versus thermoelastic NiTi) was 2.30, 95% CI ‐12.09 to 16.69 | |
| Root resorption | Not measured | |||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; MD: mean difference; NiTi: nickel‐titanium | ||||||
| GRADE Working Group grades of evidence High quality: we are very confident that the true effect lies close to that of the estimate of the effect. Moderate quality: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low quality: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect. Very low quality: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect. | ||||||
1Downgraded two levels due to very serious imprecision.
We have placed the arch wires evaluated in the included studies into six groups according to the materials used in the arch wires being compared.
1. Multistrand stainless steel versus superelastic nickel‐titanium (NiTi) arch wires
There are five studies in this group, all of which made different comparisons and reported different outcomes (Table 1).
Alignment rate
0.0175‐inch multistrand stainless steel wire versus 0.016‐inch austenitic‐NiTi wire or 0.016‐inch austenitic‐NiTi wire versus surface ion implantation
One three‐arm study compared 0.0175‐inch multistrand stainless steel wire (Wildcat) to 0.016‐inch austenitic‐NiTi wire (Sentalloy) or the same 0.016‐inch austenitic‐NiTi wire with surface ion implantation (Cobb 1998). Cobb 1998 measured both alignment rate per month and time to next working arch wire but reported outcomes only as graphical figures, with no numerical data reported. They did not report outcomes for root resorption, time to alignment or pain. There was a unit of analysis error in this study in that randomisation was at the participant level and outcome was reported at the arch level. There were also differences in the type of appliances used, but this was stratified in the randomisation. The paper reported that there was no statistically significant difference between the three arch wires in rate of alignment, but given the unit of analysis error, this result must be interpreted with caution.
Multistrand stainless steel versus superelastic NiTi
Three, two‐arm studies in this group compared multistrand stainless steel with superelastic NiTi.
Jones 1992 compared 0.015‐inch multistrand stainless steel wire (Twistflex) with 0.014‐inch superelastic NiTi wire (heavy Japanese NiTi).
West 1995 compared 0.0155‐inch multistrand stainless steel wire (Dentaflex) with 0.014‐inch superelastic NiTi wire (NiTi).
Sandhu 2013 compared 0.0175‐inch multistranded stainless steel (six‐stranded, Unitek) with 0.016‐inch superelastic nickel‐titanium (austenitic active, Unitek).
West 1995 assessed tooth alignment by means of three‐dimensional contact point movements of the anterior segment and the whole dental arches using the ITA. The main difference between ITA and LII is that the positions of the anatomic contact points are digitised in three dimensions and the process may be extended to the whole dental arch. The effects of the two arch wires were compared by an analysis of covariance using the means of triplicate log ITA scores, reported as an adjusted mean ratio of ITA scores (NiTi/StSt). In the mandibular anterior segment, the superelastic NiTi wire was found to produce a statistically significant improvement in alignment in comparison to the multistrand steel wire, but there was no difference in the labial segment of the maxilla (see Table 7).
1. Multistrand stainless steel versus superelastic NiTi.
| Table 1: West 1995 | |||
| 6 weeks' follow‐up |
3‐dimensional alignment‐adjusted geometric mean ratio of ITA scores NiTi/StSt |
95% CI | P value |
| Upper arch (between first molars) | 1.03 | 0.92 to 1.15 | 0.56 |
| Lower arch (between first molars) | 1.13 | 1.03 to 1.24 | 0.01 |
CI = confidence interval; ITA = Index of Tooth Alignment; NiTi = nickel‐titanium; P = probability; StSt = stainless steel
Conventional stainless steel, multistrand stainless steel, superelastic NiTi versus thermoelastic NiTi
One, four‐arm study compared conventional stainless steel, multistrand stainless steel, superelastic NiTi with thermoelastic NiTi.
Quintão 2005 compared 0.014‐inch conventional stainless steel (SS Gold Accuform, reference 03‐014‐63, Dentsply‐GAC International, NY, USA), 0.0155‐inch multistranded stainless steel (SS Pentacat Accuform, reference 03‐016‐23, Dentsply‐GAC International, NY, USA), 0.016‐inch superelastic NiTi (Sentalloy 0.016", Accuform, reference 511‐02, Dentsply‐GAC International, NY, USA) with 0.016‐inch thermoactivated NiTi (Thermal nickel‐titanium, G & H). The three‐dimensional movement of the contact points, after eight weeks' treatment with four different wires, was measured based on LII, shown in Analysis 1.1: There was no difference in rate of alignment between multistrand stainless steel group and superelastic NiTi group (MD ‐7.5, 95% CI ‐26.27 to 11.27).
1.1. Analysis.
Comparison 1 Multistrand stainless steel versus superelastic NiTi arch wires, Outcome 1 Alignment rate (mm/8 weeks, Between first molars).
Pain
As mentioned, three, two‐arm studies in this group compared multistrand stainless steel with superelastic NiTi. West 1995 did not measure pain.
Jones 1992 and Sandhu 2013 reported the intensity of pain over a 15‐day period after placement of an initial arch wire. Pain was self‐reported by participants using a 100 mm VAS. Though only part of the outcome data (VAS within 7 days) were reported in detail, other studies have shown that pain levels generally return to baseline levels at six or seven days after the initial wires have been placed (Erdinç 2004; Firestone 1999; Ngan 1989; Scheurer 1996), which suggests that any differences in pain or discomfort between intervention groups are likely to be minimal after seven days. There did not appear to be any meaningful difference in pain between the groups, as measured on a VAS scale, at either day 1 (MD ‐2.68, 95% CI ‐6.75 to 1.38) or day 7 (MD ‐0.37, 95% CI ‐0.91 to 0.17; Analysis 1.2; Analysis 1.3).
1.2. Analysis.
Comparison 1 Multistrand stainless steel versus superelastic NiTi arch wires, Outcome 2 Pain (VAS, day 1).
1.3. Analysis.
Comparison 1 Multistrand stainless steel versus superelastic NiTi arch wires, Outcome 3 Pain (VAS, day 7).
2. Multistrand stainless steel versus thermoelastic NiTi arch wires
There are two studies in this group. They made different comparisons and reported different outcomes (Evans 1998; Quintão 2005) (Table 2).
Alignment rate
Evans 1998 in a three‐arm trial, compared 0.0155‐inch multistrand stainless steel wire (Dentaflex) with 0.016 x 0.022‐inch medium force active M‐NiTi wire (Titanium Heat Memory Wire) or 0.016 x 0.022‐inch graded force active M‐NiTi wire (Bioforce Sentalloy). Participants were seen at four‐week intervals and alginate impressions of the dental arches included in the trial were taken at baseline, four weeks and eight weeks. They assessed the alignment rate by the changes of contact point distances of the anterior and posterior segments and the whole arch in two‐ and three‐dimensional measurements. The numerical data comparing the different arch wires presented in the paper is for both two‐dimensional changes and three‐dimensional changes between time points (model variables are subject, order and upper or lower arch), and the trial found no difference in rate of alignment between the arch wire groups (see Table 8).
2. Multistrand stainless steel versus thermoelastic NiTi arch wires.
| Table 2: Evans 1998 | |||||
| 8 weeks' follow‐up |
Multistrand StSt |
Thermoelastic NiTi | ANOVA F statistic* | P value | |
| Heat memory NiTi | M‐NiTi | ||||
| Both arches (between first molars) Arch movement in mm 2‐dimensional |
5.30 | 6.32 | 6.05 | 0.05 | 0.95 |
| Both arches (between first molars) Arch movement in mm 3‐dimensional |
5.73 | 6.12 | 6.62 | 0.30 | 0.74 |
P = probability; NiTi = nickel‐titanium; StSt = stainless steel
*ANOVA F ratio test adjusted for subject, order and upper or lower arch
Quintão 2005, in a four‐arm trial, showed no statistically significant difference in alignment rate between multistrand stainless steel and thermoelastic NiTi (Analysis 2.1).
2.1. Analysis.
Comparison 2 Multistrand stainless steel versus thermoelastic NiTi arch wires, Outcome 1 Alignment rate (mm/8 weeks, between first molars).
3. Conventional NiTi compared with superelastic NiTi arch wires
Three studies made this comparison and reported different outcomes (Abdelrahman 2015a; Fernandes 1998; O'Brien 1990) (Table 3).
Alignment rate
One study evaluated 0.016‐inch NiTi wire (Nitinol) compared to 0.016‐inch superelastic NiTi wire (Titanol) (O'Brien 1990). The rate of initial tooth alignment was assessed by three‐dimensional contact point movements of the upper labial segments. There was no statistically significant difference between these two intervention groups in terms of tooth movement (MD ‐0.28, 95% CI ‐0.89 to 0.33) (Analysis 3.1).
3.1. Analysis.
Comparison 3 Conventional NiTi versus superelastic NiTi arch wires, Outcome 1 Alignment rate (mm/till next arch wires, between canines).
Abdelrahman 2015a, a three‐arm study, evaluated 0.014‐inch conventional Nitinol wire (Unitek) compared to 0.014‐inch superelastic NiTi wire (Unitek) and 0.014‐inch thermoelastic NiTi wire (Unitek). The rate of initial tooth alignment was assessed by LII of the lower labial segments over 8 weeks. There was no statistically significant difference between these two intervention groups in terms of tooth movement (MD ‐0.01, 95% CI ‐1.39 to 1.36) (Analysis 3.2).
3.2. Analysis.
Comparison 3 Conventional NiTi versus superelastic NiTi arch wires, Outcome 2 Alignment rate (mm/8 weeks, between canines).
Time to alignment
Time to alignment (weeks) showed no statistically significant difference between the two groups (MD ‐0.30, 95% CI ‐1.74 to 1.14) (Analysis 3.3) (Abdelrahman 2015a).
3.3. Analysis.
Comparison 3 Conventional NiTi versus superelastic NiTi arch wires, Outcome 3 Time to alignment (weeks).
Pain
One study evaluated 0.014‐inch NiTi wire (Nitinol) compared to 0.014‐inch superelastic NiTi wire (Sentalloy) (Fernandes 1998). This trial reported the intensity of pain during the initial alignment stage of treatment for seven days evaluated by a 100 mm VAS, and the consumption of analgesics. There was no difference between the two arch wire groups in pain intensity on day 1 (11 hours after wire placement) (Analysis 3.4), or day 7 (Analysis 3.5), and no difference in analgesic consumption (Analysis 3.6).
3.4. Analysis.
Comparison 3 Conventional NiTi versus superelastic NiTi arch wires, Outcome 4 Pain (VAS, day 1).
3.5. Analysis.
Comparison 3 Conventional NiTi versus superelastic NiTi arch wires, Outcome 5 Pain (VAS, day 7).
3.6. Analysis.
Comparison 3 Conventional NiTi versus superelastic NiTi arch wires, Outcome 6 Pain (analgesic consumption within 7 days).
4. Conventional NiTi versus thermoelastic NiTi arch wires
Two studies made this comparison but reported different outcomes (Abdelrahman 2015a; Pandis 2009) (Table 4).
Alignment rate
Pandis 2009 evaluated 0.016‐inch NiTi wire (ModernArch) compared to 0.016‐inch thermal copper NiTi wire (Ormco). In this trial, with 60 participants, time to alignment of the six lower labial segment teeth only, was assessed from intraoral measurements of LII by a fine‐tip digital calliper. There was no difference between wire types in alignment rate ratio (Analysis 4.1), but predictably, severely crowded cases (LII > 5 mm) took significantly longer to align than moderately crowded (LII < 5 mm) cases. This trial did not report outcomes for time to next arch wire, root resorption with each wire type or pain.
4.1. Analysis.
Comparison 4 Conventional NiTi versus thermoelastic NiTi arch wires, Outcome 1 Alignment rate ratio.
In Abdelrahman 2015a, there was no statistically significant difference in the alignment rate over 8 weeks between conventional and thermoelastic NiTi (Analysis 4.2).
4.2. Analysis.
Comparison 4 Conventional NiTi versus thermoelastic NiTi arch wires, Outcome 2 Alignment rate (mm/8 weeks, between canines).
Time to alignment
Time to alignment (weeks) showed no statistically significant difference between the two groups (MD 0.20, 95% CI ‐1.24 to 1.64) (Analysis 4.3) (Abdelrahman 2015a).
4.3. Analysis.
Comparison 4 Conventional NiTi versus thermoelastic NiTi arch wires, Outcome 3 Time to alignment (weeks).
5. Single‐strand superelastic NiTi versus coaxial superelastic NiTi arch wires
Only one study made this comparison (Sebastian 2012) (Table 5).
Alignment rate
Sebastian 2012 compared 0.016‐inch single‐stranded superelastic NiTi wire (Rematitan Lite Wire) to 0.016‐inch coaxial (multistranded) superelastic NiTi wire (Regular 7 Stranded Supercable Wire) and reported alignment rate per month for the lower labial segment only. Measurements were made on dental casts taken at 4, 8 and 12 weeks after initial arch wire placement, using a co‐ordinate‐measuring machine that calculated mean tooth movement at each time point. Over the 8 and 12 weeks of the study, the coaxial superelastic NiTi arch wire induced greater tooth movement (Analysis 5.1; Analysis 5.2).
5.1. Analysis.
Comparison 5 Single‐strand superelastic NiTi versus coaxial superelastic NiTi arch wires, Outcome 1 Alignment rate (mm/8 weeks, between canines).
5.2. Analysis.
Comparison 5 Single‐strand superelastic NiTi versus coaxial superelastic NiTi arch wires, Outcome 2 Alignment rate (mm/12 weeks, between canines).
6. Superelastic NiTi versus thermoelastic NiTi arch wires
Three studies compared superelastic NiTi wire with thermoelastic NiTi wire (Abdelrahman 2015a; Cioffi 2012; Quintão 2005) (Table 6).
Alignment rate
Quintão 2005 showed no statistically significant difference in the alignment rate within first molars over 8 weeks between superelastic and thermoelastic NiTi (MD 16.28, 95% CI ‐4.05 to 36.61) (Analysis 6.1).
6.1. Analysis.
Comparison 6 Superelastic NiTi versus thermoelastic NiTi arch wires, Outcome 1 Alignment rate (mm/8 weeks, between first molars).
Abdelrahman 2015a showed no statistically significant difference in the alignment rate within canines over 8 weeks between superelastic and thermoelastic NiTi (MD ‐0.10, 95% CI ‐1.44 to 1.25) (Analysis 6.2).
6.2. Analysis.
Comparison 6 Superelastic NiTi versus thermoelastic NiTi arch wires, Outcome 2 Alignment rate (mm/8 weeks, between canines).
Time to alignment
In Abdelrahman 2015a, there was no statistically significant difference in the time to alignment between superelastic and thermoelastic NiTi (Analysis 6.3).
6.3. Analysis.
Comparison 6 Superelastic NiTi versus thermoelastic NiTi arch wires, Outcome 3 Time to alignment (weeks).
Pain
In Cioffi 2012, 0.016‐inch single‐stranded, superelastic NiTi arch wire was compared to a thermoelastic heat‐activated NiTi wire of the same diameter. Participants self‐assessed pain on a 100 mm VAS at five time points each day for seven days. There was no difference in mean reported pain between the two groups on day 1 or day 7 (Analysis 6.4; Analysis 6.5).
6.4. Analysis.
Comparison 6 Superelastic NiTi versus thermoelastic NiTi arch wires, Outcome 4 Pain (VAS, day 1).
6.5. Analysis.
Comparison 6 Superelastic NiTi versus thermoelastic NiTi arch wires, Outcome 5 Pain (VAS, day 7).
Discussion
Summary of main results
Twelve randomised controlled clinical trials (RCTs) including a total of 799 participants (952 arches) satisfied the inclusion criteria for this review. Studies were generally small (sample size: mean 67, range 24 to 128 participants). Duration of follow‐up varied between one week and six months. We assessed three studies at high risk of bias, three at low risk and six at unclear risk.
We grouped the studies into six main comparisons.
Multistrand stainless steel versus superelastic nickel‐titanium arch wires (Table 1). There were five studies in this group and it was only appropriate to undertake a meta‐analysis of two of them. There is insufficient evidence from these studies to determine whether there is a difference in rate of alignment in either of these two studies (low‐quality evidence). The evidence for pain at day 1 suggests that there is no meaningful difference between multistrand stainless steel and superelastic NiTi arch wires (pain day 1 MD ‐2.68 mm, 95% CI ‐6.75 to 1.38; moderate‐quality evidence).
Multistrand stainless steel versus thermoelastic nickel‐titanium arch wires (Table 2). There were two studies in this group, but it was not appropriate to undertake a meta‐analysis of the data. There is insufficient evidence from the studies to determine whether there is a difference in rate of alignment between multistrand stainless steel and thermoelastic NiTi arch wires (low‐quality evidence).
Conventional nickel‐titanium versus superelastic nickel‐titanium arch wires (Table 3). There were three studies in this group, but it was not appropriate to undertake a meta‐analysis of the data. There is insufficient evidence from these studies to determine whether there is any difference between conventional and superelastic NiTi arch wires with regard to either alignment or pain (low‐ to very‐low quality evidence).
Conventional nickel‐titanium versus thermoelastic nickel‐titanium arch wires (Table 4). There were two studies in this group, but it was not appropriate to undertake a meta‐analysis of the data. There is insufficient evidence from these studies to determine whether there is a difference in rate of alignment between conventional and thermoelastic NiTi arch wires (low‐quality evidence).
Single‐strand superelastic nickel‐titanium versus coaxial superelastic nickel‐titanium arch wires (Table 5). There was only one study in this group. There is moderate‐quality evidence that coaxial superelastic NiTi can produce greater tooth movement over 12 weeks (MD ‐6.76, 95% CI ‐7.98 to ‐5.55).
Superelastic nickel‐titanium versus thermoelastic nickel‐titanium arch wires (Table 6). There were three studies in this group, but it was not appropriate to undertake a meta‐analysis of the data. There is insufficient evidence from these studies to determine whether there is a difference in alignment or pain between superelastic and thermoelastic NiTi arch wires (low‐quality evidence).
All in all, there is insufficient evidence in this review to determine whether any specific arch wire type is better than another in terms of rate of tooth alignment or pain experienced during alignment other than the moderate‐quality evidence that suggests that initial arch wires made of coaxial superelastic NiTi can produce greater tooth movement over 12 weeks than those made of single‐strand superelastic nickel‐titanium, and there is no difference in pain at day 1 between multistrand stainless steel and superelastic NiTi arch wires. No studies assessed root resorption.
Overall completeness and applicability of evidence
There has been a great deal of research into developing orthodontic arch wire materials with properties that could enhance the initial alignment phase of orthodontic treatment, either by increasing the speed of alignment or reducing pain or both. However, there is a big gap between the abundant materials research and manufacturers' claims of superior products, and the absence of clinical evidence that these newer materials make a difference in people undergoing orthodontic treatment.
Studies included in the review were conducted in several places around the world, and both upper and lower arches were involved, hence the evidence is widely applicable. However, four studies included both juvenile (age < 18 years) and adult (age < 30 years) participants (Abdelrahman 2015a; Cioffi 2012; Cobb 1998; West 1995), others included only participants under 18 years old and Sebastian 2012 included only female participants. We considered that the difference in demographic characteristics might play a role in alignment and intensity of pain during the initial alignment stage of treatment. Each study evaluated a different comparison and there was variation in the way outcomes were measured and reported. One study that reported alignment did not include data in a form that could be used in this review (Cobb 1998). We could rarely pool the data. For these reasons, we should be careful how we apply the evidence.
Other than the initial arch wires, we also paid attention to other aspects of orthodontic treatment that might influence the results of this review. They are discussed below.
Brackets
Seven studies specified the bracket type, which was used for all participants: 0.022 × 0.028‐inch slot Gemini 3M (Unitek) Roth Rx brackets (Abdelrahman 2015a); 0.022 x 0.028‐inch slot metal brackets (Cioffi 2012); preadjusted bioprogressive edgewise 0.018 x 0.030‐inch slot (Jones 1992); self ligating brackets with 0.022‐inch slot (In Ovation‐R) (Pandis 2009), but different molar tubes (Speed System Orthodontics, Ontario, Canada) accompanied their use in this trial; 0.022 x 0.028‐inch brackets and slot ring tubes (GAC International, NY, USA) (Quintão 2005); 0.022x0.028‐inch slot twin brackets (Roth prescription, Gemini Metal Brackets; 3M Unitek Corporation, Monrovia, CA, USA) (Sandhu 2013); and 0.022 x 0.028‐inch slot MBT prescription brackets (Sebastian 2012).
Both 0.018 inch and 0.022‐inch slot edgewise appliances were used by Cobb 1998: twin brackets on all teeth for the 0.022‐inch system, and for the 0.018‐inch system twin brackets were used on the maxillary central and lateral incisors with a mix of single and twin brackets for the remaining teeth.
Edgewise brackets were used by O'Brien 1990, but dimensions and bracket type were not stated. In Fernandes 1998, "as far as possible, the brackets used were standardised". Type of brackets used were not stated in two studies (Evans 1998; West 1995), other than in the authors' dissertations.
In addition, bracket debonding may have also influenced the results if rebonding was not performed soon after the bracket became debonded. Unfortunately, only one study considered this variable (Evans 1998).
Details regarding bracket type (material/dimensions) should be specified and standardised in future studies.
Method of ligation
The studies varied in the description of the method of ligation used. In four studies, the method of ligation was specified for trial participants: elastomeric modules (Cobb 1998); elastomeric modules or steel ties (Sebastian 2012); elastic ligatures using a standard Mathieu pliers (Cioffi 2012); and self ligating (Pandis 2009). In five studies, ligation was not mentioned (Abdelrahman 2015a; Fernandes 1998; Jones 1992; Quintão 2005; Sandhu 2013).
Three studies described ligation as follows.
O'Brien 1990: The "arch wire was tied with ligatures into the brackets, with the operator attempting to achieve complete engagement where clinically possible".
Cobb 1998: clinicians were asked to follow their usual practice but to "ligate the wire as fully into each bracket as possible with no teeth omitted from the attachment to the wire".
Evans 1998: "...ligated as fully as possible into the bracket with the clinicians preferred method usually elastomeric rings".
However, none of these studies reported the number of participants in each of the randomised groups who did not have complete engagement, 'full ligation' or each type of ligature.
The method of ligation should be specified, standardised and reported fully in future studies.
Operators
The number of operators participating in the studies varied between one and 13: one (Pandis 2009; Quintão 2005); two (Cioffi 2012; O'Brien 1990; Sandhu 2013); five (West 1995); six (Evans 1998); eight (of which six were postgraduate students) (Sebastian 2012); and 13 (Cobb 1998). Two studies did not report the number of operators in the published papers (Abdelrahman 2015a; Jones 1992). Where important aspects of orthodontic treatment (such as bracket type, dimension and ligation) that may influence the outcomes of the studies varied by operator, the number of operators in these studies was another uncontrolled variable.
Extractions
Some of the participants in these studies underwent extraction of teeth as part of their orthodontic treatment. Three studies reported the extraction of at least one premolar (Abdelrahman 2015a; Jones 1992; Sandhu 2013), and three studies reported that there were no extractions (Cioffi 2012; Pandis 2009; Sebastian 2012). However, six studies did not specify whether or not participants had undergone tooth extraction as part of their orthodontic treatment (Cobb 1998; Evans 1998; Fernandes 1998; O'Brien 1990; Quintão 2005; West 1995).
Duration of trials, time of outcome assessment
This also varied between the studies included in this review. Two studies evaluated the first seven days following arch wire placement (Cioffi 2012; Fernandes 1998). One evaluated up until day 15 (Jones 1992) and one until day 14 (Sandhu 2013). O'Brien 1990 reported a mean duration of 37 days. West 1995 reported a duration of six weeks, Evans 1998 and Quintão 2005 reported a duration of eight weeks, Sebastian 2012 reported a duration of 12 weeks, Abdelrahman 2015a reported a duration of 16 weeks, Pandis 2009 reported a duration of six months, and Cobb 1998 reported a duration of 12 months.
O'Brien 1990 and West 1995 were of short duration, but this was appropriate as these studies only observed the amount of tooth movement in the first month of treatment and not the mean rate of initial alignment. Ideally, the duration of studies should be standardised with a longer observation period for full alignment.
Assessment of crowding and alignment
Alignment can be measured in several ways. Four studies used the irregularity index first described by Little 1975 (Abdelrahman 2015a; Cobb 1998; O'Brien 1990; Pandis 2009). This index (as originally described) addresses the sum of the five contact point displacements for the mandibular anterior teeth, regardless of any irregularities in the buccal segments. Three studies used the index of tooth alignment (ITA), which includes an assessment of the whole dental arch (Evans 1998; Quintão 2005; West 1995). An assessment of the contact point discrepancies for the whole arch is a useful outcome measure, especially when crowding/irregularities occur in the canine, premolar and molar regions.
There are two main methods of recording the amount of crowding: direct measurement in the mouth with a digital vernier calliper (Abdelrahman 2015a; Cobb 1998; Pandis 2009), and indirect measurement on stone casts with electronic callipers or in three dimensions with instruments such as the reflex metrograph. Both methods have drawbacks. When using direct measurement, the examiner(s) will require calibration at the start and regular recalibration throughout the trial period, to ensure consistency of the measurements. A second problem with direct measurements is blinding. To reduce bias, the examiner should be blinded to group allocation at the time of recording, which may complicate the operation of the trial. Indirect measurement on casts can resolve this problem when the casts are measured in a random order and the assessors are blinded to allocation. However, indirect measurement in three dimensions requires specialised instruments, such as the Reflex Metrograph (O'Brien 1990) and the Reflex Microscope (Evans 1998; Quintão 2005; West 1995), which adds to the cost of a clinical study. Another problem with three‐dimensional indirect measurements is that of identifying the fiducial points on each cast, which are important for ascertaining adequate reproducibility of the measurements.
Planning future studies
When future studies are planned, greater consideration should be given to study design in order to reduce bias. Future studies should consider standardisation of study design to make results comparable. This would involve clear inclusion criteria (such as whether people requiring extractions can be included), together with factors such as orthodontic appliance system, bracket type, slot size and the ligation method being prespecified, as these may have been important confounders among the studies that were included in this review. It is desirable that a standardised measure of alignment and pain be used as an outcome measure. Both the LII and ITA may be ideal measures for alignment and we recommend researchers concurrently use multiple measures to measure the outcome. Intra‐oral scanning might be an alternative method to directly measure the amount of crowding, and time‐to‐event data of alignment rate is also recommended, if feasible. For pain, consecutive records of pain VAS at more time points for the first week are desired.
We did not include economic considerations in this review, however, we acknowledge that the cost of arch wires, amount of time required for ligation, overall number of appointments (including any additional appointments required for breakages, e.g. wire fracture) and type of orthodontic care provider (overheads may be more expensive in hospital settings compared to practice‐based care), will unavoidably influence the selection of initial arch wires. Evaluation of these outcomes is desirable in future studies.
Quality of the evidence
This review included 12 RCTs and 799 participants randomised to treatment. We assessed three studies at high risk of bias, three at low risk and six at unclear risk. We assessed the quality of evidence as low or very low for most outcomes in the six comparisons (see Table 1; Table 2; Table 3; Table 4; Table 5; Table 6). We assessed three studies as being at high risk of bias overall, two because of reporting bias (O'Brien 1990; West 1995), and the other because of incomplete outcome data (Fernandes 1998). We downgraded the quality of the evidence when studies we had assessed as being at overall high risk of bias contributed to the comparison.
Most analyses considered only one study in the outcome or the subgroup. Only two subgroups consisted of two studies, and neither had any heterogeneity (Analysis 1.2; Analysis 1.3). Hence we did not downgrade the quality of the evidence for inconsistency.
The number of events and sample sizes of most studies were insufficient and we downgraded the evidence for imprecision. The result was accurate enough in only one comparison (Analysis 5.1; Analysis 5.2), which included only one study (Sebastian 2012); however, we thought it appropriate to downgrade this evidence from high to moderate as it was based on a single study of 24 participants and the findings should be confirmed in a larger trial.
We did not downgrade any of the evidence for indirectness.
Due to the limited number of included studies (fewer than six in one outcome), we did not generate funnel plots to examine the publication bias across studies thus we did not downgrade any evidence for this.
Therefore, we assessed the quality of evidence as moderate for two outcomes: alignment rate between canines for the comparison of single‐strand superelastic NiTi versus coaxial superelastic NiTi arch wires (Table 5), and pain at day 1 for the comparison of multistrand stainless steel versus superelastic NiTi arch wires (Table 1). We downgraded the quality of the evidence to very low for alignment rate between canines and pain at day 1 for the comparison of conventional NiTi versus superelastic NiTi arch wires (Table 3). The quality of the evidence was low for the other comparisons and outcomes.
Potential biases in the review process
We used a sensitive search strategy for this review and made every effort to identify all relevant studies. We did not exclude studies due to language restrictions. We tried to contact authors of studies investigating initial arch wires for the alignment of teeth with fixed orthodontic appliances by email and postal mail to identify unpublished studies or additional information about their studies; however, only a few study authors replied (Jones 1992; O'Brien 1990; Weiland 2003).
Two review authors independently collected and analysed data, and we resolved any disagreement between review authors by discussion or the assistance of Cochrane Oral Health to minimise bias during the review process.
Agreements and disagreements with other studies or reviews
We identified only one published systematic review (Riley 2009). This included both randomised clinical trials and controlled clinical trials, while only randomised clinical trials were included in our Cochrane Review. Riley 2009 only focused on one outcome "objective measurement of alignment/irregularity" to assess the effectiveness of arch wires for alignment, while our review also evaluated the amount of root resorption along with tooth movement and the intensity of pain experienced by participants during the initial alignment stage of treatment. Riley 2009 included seven studies, five of which we included in our Cochrane Review (Cobb 1998; Evans 1998; Jones 1992; O'Brien 1990; West 1995), and two of which we excluded from our review (Dalstra 2004; Pandis 2007). We included four studies in our review that Riley 2009 did not (Cioffi 2012; Fernandes 1998; Pandis 2009; Sebastian 2012). Data extraction, assessment of the evidence quality and author conclusions were mainly in agreement in the two reviews.
Authors' conclusions
Implications for practice.
Moderate‐quality evidence shows that coaxial superelastic nickel‐titanium (NiTi) can produce greater tooth movement over 12 weeks than single‐strand superelastic NiTi. Moderate‐quality evidence also suggests that there may be no difference in pain at day 1 between multistrand stainless steel versus superelastic NiTi arch wires. Other than these findings, there is insufficient evidence to determine whether any particular arch wire material is superior to any other in terms of alignment rate, time to alignment, pain and root resorption.
Implications for research.
This review suggests a need for more well‐designed randomised controlled trials (RCTs) in order to determine which initial arch wire is most effective. However, in designing future studies, the following need to be considered.
Treatment, except for the intervention, should be as specified, so as to be as similar as possible among the trial participants (in terms of brackets, appliances, ligation systems, need for extractions) and details of these aspects of treatment should be reported for each group.
Studies should report both benefits (speed of alignment) and possible harms (such as pain and root resorption), and be of sufficient duration to enable these outcomes to be measured.
Consideration needs to be given to using standardised measurements for evaluating tooth movement or alignment and pain.
Clear inclusion and exclusion criteria should be set. Care should be taken to avoid unit of analysis errors where dental arches are the unit of randomisation. Adults should be included in studies to increase the generalisability of the results.
An a priori sample size calculation should be carried out.
Attempts should be made to minimise missing data.
Data on comparative costs associated with each wire (e.g. cost of wires, additional visits required to deal with breakages, bracket debonding) would be useful.
Clinical studies should follow the guidelines produced by the CONSORT Group to ensure that all relevant information is provided (Moher 2005).
What's new
| Date | Event | Description |
|---|---|---|
| 23 May 2018 | New citation required and conclusions have changed | Three new studies identified and included Moderate‐quality evidence now available for two comparisons (different outcomes) |
| 8 November 2017 | New search has been performed | Searches updated to 5 October 2017 Methods updated, including risk of bias assessment and addition of 'Summary of findings' tables Some 'Risk of bias' judgements revised for studies included in the previous version of the review Changes to authorship and title |
History
Protocol first published: Issue 3, 2009 Review first published: Issue 4, 2010
| Date | Event | Description |
|---|---|---|
| 25 March 2013 | New search has been performed | Searches updated to 2 August 2012 |
| 25 March 2013 | New citation required but conclusions have not changed | Three new studies identified and included with no changes to the conclusions. Methods updated. Changes to authorship and title |
Acknowledgements
We would like to acknowledge the assistance of Anne Littlewood (Information Specialist, Cochrane Oral Health) in developing the search strategy, and Laura MacDonald, Jayne Harrison and Helen Worthington (Cochrane Oral Health) in editing this update. We thank Denise Mitchell for copy editing.
We would like to thank Philip Riley, Samer Mheissen, Aman Ulhaq and Philip Benson for their comments and suggestions on this update.
We would like to thank Luisa Fernandez Mauleffinch, Zongdao Shi, Zhihe Zhao, Taixiang Wu and Susan Furness for their contribution to the previous published versions of the review.
Appendices
Appendix 1. Cochrane Oral Health Trials Register search strategy
From October 2016, searches of the Cochrane Oral Health Trials Register for this review were undertaken using the Cochrane Register of Studies and the search strategy below:
("orthodontic wire*" or archwire* or "arch wire*" or arch‐wire* or "superelastic wire*" or "super‐elastic wire*" or "stainless steel wire*" or "stainless‐steel wire*" or NiTi or Ni‐Ti or "nickel titanium wire*" or "nickel‐titanium wire*"):ti,ab
Previous searches were undertaken using the Procite software, and the search strategy below:
("orthodontic wire*" or archwire* or "arch wire*" or arch‐wire* or "superelastic wire*" or "super‐elastic wire*" or "stainless steel wire*" or "stainless‐steel wire*" or NiTi or Ni‐Ti or "nickel titanium wire*" or "nickel‐titanium wire*")
Appendix 2. Cochrane Central Register of Controlled Clinical Trials (CENTRAL) search strategy
#1 MeSH descriptor ORTHODONTIC WIRES explode all trees #2 (archwire* in All Text or "arch wire*" in All Text or arch‐wire* in All Text or "orthodontic wire*" in All Text) #3 ("superelastic wire*" in All Text or "super‐elastic wire*" in All Text) #4 ("stainless steel wire*" in All Text or "stainless‐steel wire*" in All Text) #5 ((NiTi in All Text near/6 wire in All Text) or (Ni‐Ti in All Text near/6 wire in All Text) or ("nickel titanium" in All Text near/6 wire in All Text) or (nickel‐titanium in All Text near/6 wire in All Text)) #6 (#1 or #2 or #3 or #4 or #5)
Appendix 3. MEDLINE Ovid search strategy
1. exp Orthodontic Wires/ 2. "orthodontic wire$".mp. 3. archwire$ or "arch wire" or arch‐wire$.mp. 4. "superelastic wire" or "super‐elastic wire".mp. 5. "stainless steel wire"or "stainless‐steel wire".mp. 6. (NiTi adj3 wire$) or (Ni‐Ti adj3 wire$) or ("nickel titanium" adj3 wire) or (nickel‐titanium adj3 wire).mp. 7. (CuNiTi adj3 wire$) or (Cu‐NiTi adj3 wire$) or (Cu‐Ni‐Ti adj3 wire$) or (copper‐nickel‐titanium adj3 wire) or ("copper nickel titanium" adj3 wire).mp. 8. or/1‐7
This subject search was linked to the Cochrane Highly Sensitive Search Strategy (CHSSS) for identifying randomised trials in MEDLINE: sensitivity‐maximising version (2008 revision) as referenced in Chapter 6.4.11.1 and detailed in box 6.4.c of theCochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 [updated March 2011] (Lefebvre 2011).
1. randomized controlled trial.pt. 2. controlled clinical trial.pt. 3. randomized.ab. 4. placebo.ab. 5. drug therapy.fs. 6. randomly.ab. 7. trial.ab. 8. groups.ab. 9. or/1‐8 10. exp animals/ not humans.sh. 11. 9 not 10
Appendix 4. Embase Ovid search strategy
1. exp Orthodontic Wires/ 2. "orthodontic wire$".mp. 3. archwire$ or "arch wire" or arch‐wire$.mp. 4. "superelastic wire" or "super‐elastic wire".mp. 5. "stainless steel wire" or "stainless‐steel wire".mp. 6. (NiTi adj3 wire$) or (Ni‐Ti adj3 wire$) or ("nickel titanium" adj3 wire$) or (nickel‐titanium adj3 wire$).mp. 7. or/1‐6
This subject search was linked to Cochrane Oral Health’s filter for identifying RCTs in Embase Ovid:
1. random$.ti,ab. 2. factorial$.ti,ab. 3. (crossover$ or cross over$ or cross‐over$).ti,ab. 4. placebo$.ti,ab. 5. (doubl$ adj blind$).ti,ab. 6. (singl$ adj blind$).ti,ab. 7. assign$.ti,ab. 8. allocat$.ti,ab. 9. volunteer$.ti,ab. 10. CROSSOVER PROCEDURE.sh. 11. DOUBLE‐BLIND PROCEDURE.sh. 12. RANDOMIZED CONTROLLED TRIAL.sh. 13. SINGLE BLIND PROCEDURE.sh. 14. or/1‐13 15. (exp animal/ or animal.hw. or nonhuman/) not (exp human/ or human cell/ or (human or humans).ti.) 16. 14 NOT 15
Appendix 5. US National Institutes of Health Ongoing Trials Register (ClinicalTrials.gov) search strategy
(orthodontic* and wire*)
(orthodontic* and archwire*)
Appendix 6. World Health Organization International Clinical Trials Registry Platform search strategy
orthodontic* and wire* or orthodontic* and archwire*
Appendix 7. IADR Abstract search strategy
Abstract Title, Body & Authors = "arch wire"
Limit search by Year = 2012 & 2013 & 2014 & 2015 & 2016 & 2017
Data and analyses
Comparison 1. Multistrand stainless steel versus superelastic NiTi arch wires.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Alignment rate (mm/8 weeks, Between first molars) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Pain (VAS, day 1) | 2 | 127 | Mean Difference (IV, Fixed, 95% CI) | ‐2.68 [‐6.75, 1.38] |
| 3 Pain (VAS, day 7) | 2 | 127 | Mean Difference (IV, Fixed, 95% CI) | ‐0.37 [‐0.91, 0.17] |
Comparison 2. Multistrand stainless steel versus thermoelastic NiTi arch wires.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Alignment rate (mm/8 weeks, between first molars) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
Comparison 3. Conventional NiTi versus superelastic NiTi arch wires.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Alignment rate (mm/till next arch wires, between canines) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Alignment rate (mm/8 weeks, between canines) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Time to alignment (weeks) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4 Pain (VAS, day 1) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5 Pain (VAS, day 7) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6 Pain (analgesic consumption within 7 days) | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected |
Comparison 4. Conventional NiTi versus thermoelastic NiTi arch wires.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Alignment rate ratio | 1 | Hazard Ratio (Fixed, 95% CI) | Totals not selected | |
| 2 Alignment rate (mm/8 weeks, between canines) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3 Time to alignment (weeks) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
Comparison 5. Single‐strand superelastic NiTi versus coaxial superelastic NiTi arch wires.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Alignment rate (mm/8 weeks, between canines) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Alignment rate (mm/12 weeks, between canines) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
Comparison 6. Superelastic NiTi versus thermoelastic NiTi arch wires.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Alignment rate (mm/8 weeks, between first molars) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2 Alignment rate (mm/8 weeks, between canines) | 1 | 50 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐1.44, 1.25] |
| 3 Time to alignment (weeks) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4 Pain (VAS, day 1) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5 Pain (VAS, day 7) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Abdelrahman 2015a.
| Methods |
Study design: double‐blind RCT, 3 parallel groups Location: Jordan Setting: private orthodontic practice clinics and graduate dental clinics in Jordan University of Science and Technology Number of centres: not stated Study period: January 2012‐June 2013 Funding source: not stated |
|
| Participants | Inclusion criteria: people requiring lower arch only or upper and lower fixed orthodontic appliance therapy Exclusion criteria: previous active orthodontic treatment; spacing in the lower anterior region; treatment plans that included extraction of a lower incisor; a blocked‐out tooth that did not allow for placement of the bracket at the initial bonding appointment; a relevant medical history; poor oral hygiene or periodontally compromised teeth Number randomised: 87 participants (87 lower arches) Number evaluated: 74 participants (74 lower arches) (male/female 28/46; mean age 18.6 ± 4.6 years) | |
| Interventions |
Comparison: superelastic NiTi vs thermoelastic NiTi vs conventional NiTi Group A (n = 25): 0.014‐inch superelastic NiTi aligning archwire (3M Unitek) Group B (n = 25): 0.014‐inch thermoelastic NiTi aligning archwire (3M Unitek) Group C (n = 24): 0.014‐inch conventional Nitinol aligning archwire (3M Unitek) All participants received lower arch only or both upper and lower fixed orthodontic appliance therapy, but only the lower arches were analysed. All participants received 0.022 × 0.028‐inch slot Gemini 3M (Unitek) Roth Rx brackets, and a supply of relief wax was provided. Operators: not stated |
|
| Outcomes | Alignment rate: tooth movement measured on LII at 2, 4, 6, 8, 10, 12, 14 and 16 weeks (indirectly) Time to alignment |
|
| Notes |
Sample size calculation: "Sample size calculation on the basis of previous studies revealed that using at least 75 subjects would provide adequate statistical power (80%) to detect a significant difference between the three types of archwires (P<.05). To compensate for nonresponsive and incomplete data, 12 additional patients were recruited." Baseline comparability: no variable was identified to discriminate the 3 groups. ANOVA and Chi2 tests confirmed no significant differences between the groups in relation to age (P = 0.26), gender (P = 0.86), treatment modality (P = 0.96), pretreatment degree of crowding (P = 0.96), class of malocclusion (P = 0.883), or maximum point of displacement (P = 0.11). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk |
Quote: "A consecutive sample of 74 patients requiring lower only or upper and lower fixed orthodontic appliances were randomly allocated into three different archwires" Comment: method of sequence generation not described |
| Allocation concealment (selection bias) | Unclear risk | Comment: method of allocation concealment not described |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Low risk | Quote: "Participants and outcome assessor were blinded to the allocated groups" |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Low risk | Quote: "Participants and outcome assessor were blinded to the allocated groups" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: 13 participants (14.9%) excluded from analysis |
| Selective reporting (reporting bias) | Low risk | Comment: planned outcomes reported |
| Other bias | Unclear risk |
Quote: "the overall study sample size consisted of 87 patients requiring lower arch only or upper and lower fixed orthodontic appliance therapy." Comment: some participants had upper arches but the number was not stated. The maxillary tooth movement might have an effect to the lower, which was not eliminated in randomisation. |
Cioffi 2012.
| Methods |
Study design: double‐blind RCT, 2 parallel groups Location: Naples, Italy Setting: Section of Orthodontics, Department of Oral Sciences, University of Naples Federico II Number of centres: 1 Study period: 9 months, starting from January 2009 Funding source: Polo delle Scienze e Tecnologie per la Vita, University of Naples Federico II |
|
| Participants |
Inclusion criteria: full permanent dentition, excluding permanent second and third molars Exclusion criteria: active periodontal disease, planned extractive orthodontic treatment, reports of previous orthodontic treatment, skeletal asymmetries, or systemic diseases that might affect pain perception, or therapy for painful conditions Number randomised: 30 participants (male/female 11/19; age 11‐26 years) Number evaluated: 30 participants (30 arches, upper/lower 23/7) (group A: male/female 6/9, mean age 14.7 ± 3.4 years; group B: male/female 5/10, mean age 14.7 ± 4.2 years) |
|
| Interventions |
Comparison: superelastic NiTi vs thermoelastic NiTi Group A (n = 15, upper/lower 11/4): 0.016‐inch superelastic NiTi (Unitek) Group B (n = 15, upper/lower 12/3): 0.016‐inch heat‐activated NiTi (HANT) (Unitek) Metal orthodontic brackets (slots 0.22 x 0.28 inch) bonded to either maxillary or mandibular arch. Assigned arch wires were placed and tied into the brackets with elastomeric ligatures. Appliance was positioned between 1400 and 1700 hours in all participants Operators: 2 clinical instructors |
|
| Outcomes | Pain: intensity of pain measured on a 100 mm VAS at 08:00, 12:00, 16:00, 20:00 and 24:00 hours daily for 7 days | |
| Notes |
Sample size calculation: 14 participants per group necessary to detect difference of 20 mm on VAS with 80% power and α=0.05 Baseline comparability: "The male‐to‐female ratio was similar between groups." "The Student t test showed that both SE and HANT groups were similar at baseline for age and arch‐length discrepancy and that arch‐length discrepancy did not differ between maxillary and mandibular dental arches." |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "After bracket positioning, patients were randomly selected for insertion of round 0.016‐inch superelastic (SE) (Unitek) or heat‐activated (HANT) (Unitek) archwires using a custom‐made Java applet." |
| Allocation concealment (selection bias) | Low risk | Quote: "The allocation procedure was performed by one of the authors (R.M.) who was blinded to patient names and identifications." |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Low risk | Quote: "Patients were blinded to the allocation group." |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Low risk | Quote: "A single examiner (A.P.), who was blinded to patient allocation (her data set did not include allocation groups)" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: no withdrawals |
| Selective reporting (reporting bias) | Low risk | Comment: planned outcomes reported |
| Other bias | Low risk | Comment: no other sources of bias identified |
Cobb 1998.
| Methods |
Study design: RCT, 3 parallel groups, stratified randomised design Location: Chapel Hill, USA Setting: graduate clinic or faculty practice, University of North Carolina School of Dentistry Number of centres: 13 Study period: 12 months (start date not stated) Funding source: in part by a contract from Spire Corporation (who supplied one of arch wires), under the terms of an SBIR (small business initiative) grant from the National Institute of Dental Research |
|
| Participants |
Inclusion criteria: Pretreatment Irregularity Index > 5.0 mm; presence of all permanent anterior teeth; aged 10‐30 years; no anterior tooth extraction or reapproximation during alignment; no anterior tooth vertically malpositioned > 3.0 mm from arch form; no anterior tooth completely blocked from arch form; no periodontal pocketing > 4 mm; no craniofacial syndrome Exclusion criteria: not stated Number randomised: 126 participants (158 arches, upper/lower 73/85) (age 10‐30 years) (group A: mean age 16.3 ± 5.1 years; group B: mean age 17.3 ± 6.7 years; group C: mean age 15.2 ± 3.8 years) Number evaluated: 123 participants (155 arches, upper/lower 72/83) |
|
| Interventions |
Comparison: multistrand stainless steel vs NiTi vs ion‐implanted NiTi Group A (n = 47 arches, upper/lower 18/29): 0.0175‐inch 3‐strand stainless steel (Wildcat, GAC) Group B (n = 48 arches, upper/lower 24/24): 0.016‐inch austenitic NiTi (Sentalloy, GAC) Group C (n = 60 arches, upper/lower 30/30): 0.016‐inch austenitic ion‐implanted NiTi (Sentalloy implanted, Spire Corp) 14 blocks of 9 participants (total 126 participants) allocated: 7 blocks to 18‐mm slot edgewise appliance and 7 to blocks to 22‐mm slot edgewise appliances. Assigned arch wires were placed and tied into the brackets with elastomeric ligatures. Operators: orthodontists in 13 faculties (number of orthodontists not stated) |
|
| Outcomes | Alignment rate: tooth movement measured on LII at 4 weeks and until the Irregularity Index dropped to ≤ 2 mm (at approximately 6 months) | |
| Notes |
Sample size calculation: not stated Baseline comparability: "To verify that the three archwire groups were equivalent before treatment, χ2 tests were used for dichotomous variables (gender, slot size, premolar extraction, etc.) and analysis of variance for continuous variables (age, initial severity). There were no statistically significant differences initially between the groups for any characteristics." Other information: further information requested from the study authors but we received no reply |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "For each attending faculty member, a block of 9 patients was created and a balanced randomization to archwire occurred within each block." "Using bracket slot size as a stratification factor, a stratified blocked randomization was performed to assign patients to a specific archwire type." |
| Allocation concealment (selection bias) | Unclear risk | Comment: allocation concealment not stated |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Unclear risk | Comment: blinding of participants and personnel not stated |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Unclear risk | Comment: blinding of outcome assessment not stated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: 3 participants (2.4%) excluded from analysis |
| Selective reporting (reporting bias) | Low risk | Comment: planned outcomes reported |
| Other bias | Unclear risk | Comment: it was unclear whether the stratified randomised design had biased the results |
Evans 1998.
| Methods |
Study design: RCT, 3 parallel groups, factorial design Location: Cardiff, Wales, UK Setting: not stated Number of centres: 2 Study period: in 1996 Funding source: Welsh Scheme for the Development of Health and Social Research |
|
| Participants |
Inclusion criteria: ≤ 18 years; upper and lower fixed appliances required; no previous orthodontic treatment; any initial phase of expansion with a quadhelix had been stabilised for 2 months; any initial phase of active distal molar movement had been stable for 2 months Exclusion criteria: people who may have experienced periodontal disease and hence loss of attachment Number randomised: 56 participants (112 arches, upper/lower 56/56) (age < 18 years) Number evaluated: 51 participants (98 arches, upper/lower 49/49) (47 participants had data for both arches, 2 had data for upper arches and 2 for lower arches) |
|
| Interventions |
Comparison: multistrand stainless steel vs martensitic NiTi vs different martensitic NiTi Group A (n = 31 arches, upper/lower 14/17): 0155‐inch multistrand stainless steel (Dentaflex, Dentarium) Group B (n = 32 arches, upper/lower 19/13): 016/022‐inch medium force active martensitic NiTi (Titanium Heat Memory Wire, American Orthodontics) Group C (n = 35 arches, upper/lower 16/19): 016/022‐inch graded force, active martensitic NiTi (Bioforce Sentalloy, GAC) Bracket types: A Company Siamese brackets 0.022 Roth prescription in Centre 1 and Orthocare Spectrum I Siamese brackets 0.022 Roth prescription in Centre 2 Operators: 6 operators |
|
| Outcomes | Alignment rate: tooth movement measured on LII at 4 and 8 weeks (indirectly) Time to next arch wire (no variance estimates) |
|
| Notes |
Sample size calculation: "100 dental arches in this trial, in other words 50 subjects (50 upper and 50 lower arches), would provide adequate statistical power (80%) to detect a significant difference in the performance of any two separate arch wires (p < 0.05)." Baseline comparability: not stated Other information: MScD dissertation reported: 1. Centre 1 ‐ A Company Siamese brackets Roth prescription 0.022, Centre 2 ‐ Orthocare Spectrum I Siamese brackets 0.022 Roth prescription; 2. Arch wire allocation was predetermined via a randomised sealed nested envelope technique. Type of ligation based on operator preference, variable and not reported. No further information was obtained from the study authors. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Allocation was predetermined and randomized." |
| Allocation concealment (selection bias) | Low risk | Quote: "randomised sealed nested envelope technique" from MScD dissertation |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Unclear risk | Comment: blinding of participants and personnel not stated |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Unclear risk | Comment: blinding of outcome assessment not stated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: 14 arches (12.5%) excluded from analysis |
| Selective reporting (reporting bias) | Low risk | Comment: planned outcomes reported |
| Other bias | Unclear risk |
Quote: "The allocated arch wire was then ligated by one of six clinicians as fully as possible into the bracket with the clinicians preferred method (usually elastomeric rings)." Comment: unclear risk. MScD dissertation also reported: 1. Centre 1 ‐ A Company Siamese brackets Roth prescription 0.022, Centre 2 ‐ Orthocare Spectrum I Siamese brackets 0.022 Roth prescription. The use of brackets of different types was not randomised. Two centres used different brackets and the sample size of each centre was not stated. The effect of brackets could not be estimated. |
Fernandes 1998.
| Methods |
Study design: RCT, 2 parallel groups Location: Oslo, Norway Setting: an orthodontic clinic and 2 private practices Number of centres: 3 Study period: not stated Funding source: not stated |
|
| Participants |
Inclusion criteria: white participants starting active orthodontic treatment, no quadhelix or other palatal expansion device present, no extraoral appliance to be used, full arch edgewise fixed appliance, no analgesics taken prior to procedure Exclusion criteria: none stated Number randomised: 128 participants (male/female 72/56; median age 12.5 years, age 9‐16 years) Number evaluated: 128 participants (136 arch wires, upper/lower 73/63) (Group A: male/female 28/35, mean age 12.5 years; Group B: male/female 28/37, mean age 12.6 years) (8 participants had data for both arches, 65 for upper arches and 55 for lower arches) |
|
| Interventions |
Comparison: conventional NiTi vs superelastic NiTi Group A (n = 63 participants, 66 arches, upper/lower 35/31): 0.014‐inch Nitonol (Nitonol, Unitek) Group B (n = 65 participants, 70 arches, upper/lower 38/32): 0.014‐inch superelastic NiTi (Sentalloy, GAC) Brackets used and placement of brackets and arch wires were standardised. Type of full arch edgewise fixed appliance was not specified. Operators: 8 dentists (6 postgraduates and 2 orthodontists, instructors in the postgraduate programme) |
|
| Outcomes | Pain: intensity of pain measured on a 100 mm VAS, hourly for first 11 hours then daily for 2‐7 days | |
| Notes |
Sample size calculation: not stated Baseline comparability: group A: male/female 28/35, mean age 12.5 years; group B: male/female 28/37, mean age 12.6 years Other information: we could not contact study authors |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk |
Quote: "randomly assigned" Comment: unclear risk. Method of sequence generation not stated |
| Allocation concealment (selection bias) | Unclear risk | Comment: allocation concealment not stated |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Unclear risk | Comment: blinding of participants and personnel not stated |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Unclear risk | Comment: blinding of outcome assessment not stated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comment: some data missing at some time points, especially at 11 hours (24 participants in Group A and 25 participants in Group B, totally 49 participants, 38.3%) |
| Selective reporting (reporting bias) | Low risk | Comment: planned outcomes reported |
| Other bias | Low risk | Comment: no other sources of bias identified |
Jones 1992.
| Methods |
Study design: RCT, 2 parallel groups Location: Cardiff, Wales, UK Setting: the Orthodontic Clinic at the University of Wales College of Medicine Number of centres: 1 Study period: not stated Funding source: not stated |
|
| Participants |
Inclusion criteria: participant required extraction of at least one premolar tooth and the placement of a full arch edgewise fixed appliance, 0.018 x 0.030‐inch standard (triple control) preadjusted bioprogressive brackets (Rocky Mountain Orthodontics, Denver, Colo.); no relevant medical history to affect the dental extraction under local anaesthesia; no molar band, palatal arch, Nance button, or quadhelix present on entry to trial were either active or causing discomfort; no extraoral traction was to be used over the period of the study; participant was < 17 years; informed and witnessed consent was obtained from patients, parents/guardian and the general dental practitioner who originally referred each participant Exclusion criteria: not stated Number randomised: 45 participants (45 arches) Number evaluated: 43 participants (43 arches, upper/lower 21/22) (male/female 23/20; aged from 113‐202 months) (group A: median age 158.0 months; group B: median age 159.5 months) |
|
| Interventions |
Comparison: multistrand stainless steel vs superelastic NiTi Group A (n = 21): 0.015‐inch multistrand steel (Twistflex, Unitek) Group B (n = 22): 0.014‐inch superelastic alloy (heavy Japanese NiTi, GAC) All participants had full arch edgewise fixed appliance, with 0.018 x 0.030‐inch standard (triple control) preadjusted bioprogressive brackets (Rocky Mountain Orthodontics) Operators: not stated |
|
| Outcomes | Pain: intensity of pain measured on a 100 mm VAS daily for the first 7 days | |
| Notes |
Sample size calculation: "as a part of this process the necessary sample size was selected on the basis of calculations from the results for a previous study by one of the authors". Baseline comparability: "On initial analysis of the data, the groups undergoing examination were found to be well matched for sex, age, social class, and degree of initial crowding". Group A: median age 158.0 months; group B: median age 159.5 months Other information: no further information obtained from study authors |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk |
Quote: "Subsequent to the random allocation of an initial arch wire in 43 patients." Comment: method of sequence generation not stated |
| Allocation concealment (selection bias) | Unclear risk | Comment: allocation concealment not stated |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Unclear risk | Comment: blinding of participants and personnel not stated |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Unclear risk | Comment: blinding of outcome assessment not stated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk |
Quote: "Of the 45 patients originally admitted to the study, two failed to return any questionnaires and therefore were excluded. Of the 43 remaining, one patient failed to return a stage II questionnaire and another a stage III questionnaire." Comment: 3 participants (6.7%) excluded from analysis at stage II (first arch wire) |
| Selective reporting (reporting bias) | Low risk | Comment: planned outcomes reported |
| Other bias | Low risk | Comment: no other sources of bias identified |
O'Brien 1990.
| Methods |
Study design: RCT, 2 parallel groups Location: Manchester UK Setting: University Dental Hospital of Manchester Number of centres: 1 Study period: not stated Funding source: "the assistance of Thomas Bolton & Johnson Limited, Stoke‐on‐Trent, England, for supplying the archwires" |
|
| Participants |
Inclusion criteria: patients attending university dental hospital clinic for routine Edgewise fixed appliance therapy Exclusion criteria: not stated Number randomised: 40 participants (40 arches, upper/lower 40/0) (group A: mean age 13.4 ± 3.12 years, aged from 11.5‐17.5 years; group B: male/female: 9/11, mean age 12.95 ± 3.2 years, aged from 11‐16.5 years) Number evaluated: not stated |
|
| Interventions |
Comparison: conventional NiTi vs superelastic NiTi Group A (n = 20, upper/lower 20/0): 0.016‐inch conventional work hardened NiTi, Nitinol (Unitek Corp) Group B (n = 20, upper/lower 20/0): 0.016‐inch superelastic NiTi, Titanol (Forestadent) They were all fitted with identical edgewise brackets. The archwire was tied with ligatures into the brackets, the operator attempting to achieve complete engagement where clinically possible. Operators: not stated |
|
| Outcomes | Alignment rate: tooth movement till next arch wire (indirectly) | |
| Notes |
Sample size calculation: not stated Baseline comparability: for initial tooth displacement, there was no significant difference between the two groups (P > 0.05). Other information: the following completed data were acquired by personal communication: 1) participants were followed to the second data collection stage at 35 days; 2) slot size of the bracket was "probably 0.018 inch". |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The sequence was generated by a random number generator" from personal email |
| Allocation concealment (selection bias) | Low risk | Quote: "We put the arch wires into envelopes which were in a box on the clinic. The operator then took the next sequential arch wire" from personal email |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Unclear risk | Comment: blinding of participants and personnel not stated |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Low risk | Quote: "When I recorded the tooth movement from the study casts, I did not know which group the patients had been allocated, I was therefore blinded" from personal email |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: number of participants included in the evaluation of outcomes not stated |
| Selective reporting (reporting bias) | High risk |
Quote: "We attempted to record pain data but this was not sufficiently reliable for analysis" from personal email Comments: not all prespecified primary outcomes reported |
| Other bias | Low risk | Comment: no other sources of bias identified |
Pandis 2009.
| Methods |
Study design: double‐blind RCT, 2 parallel groups Location: Corfu, Greece Setting: private orthodontic office of Nikolaos Pandis Number of centres: 1 Study period: December 2006‐March 2008 Funding source: not stated |
|
| Participants |
Inclusion criteria: non‐extraction treatment on the mandible; eruption of all mandibular teeth; no spaces in the mandibular arch; no crowding in the posterior segments; mandibular irregularity index > 2 mm; no therapeutic intervention planned involving intermaxillary or other intraoral or extraoral appliances including intra‐arch or interarch elastics, lip bumpers, maxillary expansion appliances, or headgears Exclusion criteria: not stated Number randomised: 60 participants (male/female 14/46; mean age 13.1 ± 1.8 years, age 10‐18 years) Number evaluated: 60 participants (60 arches, upper/lower 0/60) (group A: male/female 5/25, mean age 12.8 ± 1.7 years; group B: male/female 9/21, mean age 13.4 ± 1.8 years) |
|
| Interventions |
Comparison: conventional NiTi vs copper thermoactive NiTi Group A (n = 30, upper/lower 0/30): 0.016‐inch NiTi (Modern Arch) Group B (n = 30, upper/lower 0/30): 0.016‐inch copper thermoactive NiTi 35ºC (Ormco) All participants were bonded with In‐Ovation‐R self ligating brackets with 0.022 in slot (GAC). All first and second molars (when present) were bonded with bondable tubes (Speed System Orthodontics). Bracket bonding, arch wire placement and treatment were performed by the same clinician. Operators: 1 clinician |
|
| Outcomes | Time to alignment of the mandibular anterior dentition (for participants not aligned after 6‐month treatment, the remaining crowding was recorded) | |
| Notes |
Sample size calculation: "The planned sample of 60 subjects was based on a time‐to‐event analysis, with a power of 80% to detect a 45% difference in effect (hazard ratio) and for type I error of 0.05." Baseline comparability: "No variable was identified to discriminate the 2 samples, thus verifying the random allocation of the intervention to the 2 wire groups." Other information: further information was requested from the study authors but there was no reply. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was done using random permuted blocks of size 6." |
| Allocation concealment (selection bias) | Low risk | Quote: "Opaque envelopes were used to allocate treatment." "Allocation was concealed from the operator and participants during the observation period" |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Low risk | Quote: "Double blind investigation" |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Low risk | Quote: "Double blind investigation" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: no withdrawals |
| Selective reporting (reporting bias) | Low risk | Comment: planned outcomes reported |
| Other bias | Low risk | Comment: no other sources of bias identified |
Quintão 2005.
| Methods |
Study design: RCT, 4 parallel groups Location: Brazil Setting: Postgraduate orthodontic clinic of the Dental School of the State University of Rio de Janeiro Number of centres: 1 Study period: not stated Funding source: not stated |
|
| Participants |
Inclusion criteria: presence of all permanent teeth except second and third molars; absence of previous orthodontic treatment and absence of previous palatal expansion device; absence of previous relevant expansion device; overjet and overbite that would allow for fixing lower anterior teeth without creating occlusal interferences; crowding degree and dental position that would allow for full insertion of archwire into the bracket; good oral hygiene and periodontal status Exclusion criteria: not stated Number randomised: 45 participants (male/female 17/28; mean age: 13.2 ± 1.2 years for male and 12.8 ± 1.2 years for female participants) Number evaluated: 45 participants (90 arches, upper/lower 45/45) |
|
| Interventions |
Comparison: stainless steel vs multistranded steel vs superelastic NiTi vs thermoactivated NiTi Group A (n = 22 arches, upper/lower 11/11): 0.014‐inch stainless steel (SS GLD, GAC) Group B (n = 22 arches, upper/lower 11/11): 0.0155‐inch multistranded stainless steel (SS Pentacat, GAC) Group C (n = 26 arches, upper/lower 13/13): 0.016‐inch superelastic nickel‐titanium (Sentalloy, GAC) Group D (n = 20 arches, upper/lower 10/10): 0.016‐inch thermoactivated nickel‐titanium (Thermal, G&H) A preadjusted edgewise system, with brackets and slot ring tubes 0.022 × 0.028 inch (GAC) was used in every case Operators: 1 operator |
|
| Outcomes | Alignment rate: tooth movement measured on LII at 8 weeks (indirectly) | |
| Notes |
Sample size calculation: not stated Baseline comparability: not stated |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Using a randomised numbering system" |
| Allocation concealment (selection bias) | Unclear risk | Comment: allocation concealment not described |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Unclear risk | Comment: blinding of participants and personnel not described |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Unclear risk | Comment: blinding of outcome assessors not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: no withdrawals |
| Selective reporting (reporting bias) | Low risk | Comment: planned outcomes reported |
| Other bias | Low risk | Comment: no other sources of bias identified |
Sandhu 2013.
| Methods |
Study design: double‐blind RCT, 2 parallel groups Location: India Setting: not stated Number of centres: 1 Study period: December 2010‐June 2012 Funding source: not stated |
|
| Participants |
Inclusion criteria: 11‐17‐year‐old boys and girls who required fixed orthodontic treatment; moderate‐severe crowding (4‐9 mm) in the mandibular anterior segment that was not severe enough to prevent bracket engagement, patients with severe crowding related to 1 or 2 teeth (such as blocked out lateral incisors) were not included; eruption of all mandibular anterior teeth; no history of medical problems/medication that could influence pain perception; informed and witnessed consent from the minor participant and their parent/guardian Exclusion criteria: presence of a severe deep bite that could affect bracket placement on the mandibular anterior teeth; malocclusion correction required treatment procedures other than continuous arch wire mechanics; participants taking pain medications for chronic pain; participants with a positive history of dental pain or pain in the orofacial region; a medical condition that precluded the use of a fixed orthodontic appliance Number randomised: 96 participants (96 arches, upper/lower 0/96) (age 11‐17 years) Number evaluated: 85 participants (85 arches, upper/lower 0/85) (male/female 42/43; mean age 14.1 ± 2.0 years) (group A: male/female 21/22, mean age 13.9 ± 2.0 years; group B: male/female 21/21, mean age 14.2 ± 1.9 years) |
|
| Interventions |
Comparison: multistranded stainless steel vs superelastic NiTi Group A (n = 43, upper/lower 0/43): 0.0175‐inch multistranded stainless steel (Six‐stranded, 3M) Group B (n = 42, upper/lower 0/42): 0.016‐inch superelastic nickel‐titanium (austenitic active, Unitek) Preadjusted Edgewise Appliances with 0.022 x 0.028‐inch slot twin brackets (Roth prescription, Unitek) were bonded directly to the mandibular dentition using light‐cure composite resin (Transbond XT, Unitek). Operators: 2 qualified orthodontists |
|
| Outcomes | Pain: intensity of pain measured on a 100 mm VAS at 1, 2, 4, 6 and 12 hours for first 12 hours, then 3 times (morning, afternoon and bedtime) daily on days 1‐7, day 10 and day 14 | |
| Notes |
Sample size calculation: "Sample size was based on power analysis (Stata/SE 10.0 software, College Station, TX, USA) for a repeated measure design with 1 baseline and 32 follow‐up repeated measurements (r=0.15) to detect a 3‐mm (SD 10 for each group, Cohen’s effect size 0.3) mean difference on a 100‐mm VAS. The sample size determining assumptions, such as effect size and correlation coefficient (r) between follow‐up repeated measurement, were based on pilot study results. We determined that 42 participants per group (84 in total) were required to achieve 90% power with a significance level of 0.05. Considering possible drop out of 10–15% during follow up, it was decided to enrol at least 95 participants." Baseline comparability: baseline demographic and clinical characteristics data shown in a table about age, sex, initial crowding and extractions |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The randomization schedule was prepared by using ralloc procedure (Stata/SE 10.0 software) to enrol 96 participants into superelastic NiTi and multistranded stainless steel groups using stratified block (size 4) randomization." |
| Allocation concealment (selection bias) | Low risk | Quote: "A statistician generated the random allocation sequence, and the dental assistant helped enrol and conceal participant allocation using the opaque sealed envelope method." |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Low risk | Quote: "double‐blind" |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Low risk | Quote: "The VAS score was measured by trained dental assistants (blinded to the study) using a manual 0.1mm calibrated Vernier caliper (manual type)." |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: 11 participants (11.5%) excluded from analysis |
| Selective reporting (reporting bias) | Low risk | Comment: planned outcomes reported |
| Other bias | Low risk | Comment: no other sources of bias identified |
Sebastian 2012.
| Methods |
Study design: double‐blind RCT, 2 parallel groups Location: India Setting: not stated Number of centres: 1 Study period: not stated Funding source: not stated |
|
| Participants |
Inclusion criteria: female participants in postmenarche period between 13 and 15 years of age with crowding in the lower anterior segment and having a mandibular irregularity index > 6; class I skeletal pattern; nonextraction treatment in mandibular arch; eruption of all mandibular teeth with no spacing between them; no relevant medical history; no recent history of intake of drugs such as nonsteroidal anti‐inflammatory drugs (NSAIDs); patients who may have experienced periodontal disease and hence loss of attachment was avoided; no previous active orthodontic treatment; full arch mechanics, preadjusted edgewise appliance therapy; no therapeutic intervention planned involving intermaxillary or other intraoral or extraoral appliances during the study period Exclusion criteria: intake of medication during study period Number randomised: 24 participants (male/female: 0/24) Number evaluated: 24 participants (24 arches, upper/lower 0/24) (group A: mean age 13.8 ± 0.7 years; group B: mean age 13.6 ± 0.6 years) |
|
| Interventions |
Comparison: coaxial superelastic NiTi vs single‐stranded superelastic NiTi Group A (n = 12, upper/lower 0/12): 0.016‐inch coaxial superelastic wire (Regular 7 Stranded Supercable Wire, Speed System Orthodontics) Group B (n = 12, upper/lower 0/12): 0.016‐inch single‐stranded superelastic wire (Rematitan Lite Wire, Dentauram) All participants were bonded with 0.022 x 0.028‐inch slot MBT prescription brackets (Victory Series, Unitek). The arch wires were ligated with elastomeric modules usually or steel ties. Operators: 1 clinician |
|
| Outcomes | Alignment rate: tooth movement measured on LII at 4, 8 and 12 weeks (indirectly) | |
| Notes |
Sample size calculation: "For an alpha error of 0.05 and power of 95%, assuming that the change in measurements at 4 weeks for the Rematitan and Supercable groups was 1.5 mm and 2.5 mm, respectively, with a standard deviation (SD) of 0.60 (based on the pilot study), the minimum sample size required was estimated to be 10 for each of the two groups." Baseline comparability: "No variable was identified to differentiate the two samples with the use of t‐tests, thus verifying the random allocation of interventions to the two wire groups." |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomisation was done using computer software generated numbers" |
| Allocation concealment (selection bias) | Low risk | Quote: "Opaque envelopes were used to allocate the arch wires to 2 groups, each consisting of 12 participants. Allocation thus was concealed from the investigator and from participants during the study." |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Low risk | Quote: "double‐blind"; "Allocation thus was concealed from the investigator and from participants during the study." |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Low risk | Quote: "All readings were measured by an expert single operator who was not aware of the arch wire specimen used for the arches being measured." |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: no withdrawals |
| Selective reporting (reporting bias) | Low risk | Comment: planned outcomes reported |
| Other bias | Low risk | Comment: no other sources of bias identified |
West 1995.
| Methods |
Study design: RCT, 2 parallel groups Location: Cardiff, Wales, UK Setting: the orthodontic clinic at the University of Wales College of Medicine Number of centres: 1 Study period: not stated Funding source: not stated |
|
| Participants |
Inclusion criteria: no previous orthodontic treatment; no quadhelix or other palatal expansion device present; no relevant medical history; full arch mechanics, straight wire appliance to be used; patients with previously fitted palatal arches or extraoral traction could be included in the study. Exclusion criteria: not stated Number randomised: 62 participants (74 arches) (male/female 21/41) (group A: mean age 14.9 ± 4.3 years; group B: mean age 15.4 ± 5.2 years) Number evaluated: not stated |
|
| Interventions |
Comparison: multistrand stainless steel vs superelastic NiTi Group A (n = 38 arches): 0.0155‐inch multiple flex steel (Dentaflex, Optident) Group B (n = 36 arches): 0.014‐inch superelastic NiTi (NiTi, Armoco) No definite instructions were given regarding system of ligation; clinicians followed usual practice. Ligation systems and slot sizes not reported Operators: 5 clinicians |
|
| Outcomes | Alignment rate: tooth movement measured at close to 6 weeks (indirectly) | |
| Notes |
Sample size calculation: "It was estimated that a study involving 74 arch wires would be adequate to demonstrate an alignment difference of 1.3 mm between the two types of wire at 6 weeks, with a discriminative power of 80% at the 5% level of confidence." Baseline comparability: group A: mean age 14.9 ± 4.3 years; group B: mean age 15.4 ± 5.2 years Other information: MScD dissertation reported: 1. randomly assigned by means of a table; 2. fixed orthodontic appliances were Roth prescription 0.022 Straight Wire Appliance (Johnston and Johnston). No additional information available from authors |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk |
Quote: MScD dissertation reported: "randomly assigned by means of a table" Comment: random sequence generation by random number table |
| Allocation concealment (selection bias) | Unclear risk | Comment: allocation concealment not stated |
| Blinding of participants and personnel (performance bias) Patient reported outcomes | Unclear risk | Comment: blinding of participants or personnel not stated |
| Blinding of outcome assessment (detection bias) Clinician assessed outcomes | Unclear risk | Comment: blinding of outcome assessors not stated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comment: no information on the number of participants or arch wires included in the outcome evaluation |
| Selective reporting (reporting bias) | High risk | Comment: ITA reported graphically only. No mean/median reported for each type of wire |
| Other bias | Unclear risk | Comment: ligation systems and slot sizes were not reported, which might have biased the results. |
n = number; h = hour; d = day; LII: Little's irregularity index; NiTi = nickel‐titanium; RCT = randomised controlled trial; SD = standard deviation; VAS = visual analogue scale
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Abdelrahman 2015b | Not an RCT |
| AlQabandi 1999 | Not a comparison of initial arch wires |
| Bernhold 2001 | Published as abstract and identified as ongoing study in the first version of the review. Attempt to contact study author in 2012 unsuccessful and no subsequent publications found. Insufficient information in abstract to include this study |
| Bloom 1998 | Published as abstract only and no subsequent full publication identified. Insufficient information to include in review |
| Campos 2013 | Not a comparison of initial arch wires |
| Chekay 1999 | Published as abstract only and no subsequent full publication identified. Insufficient information to include in review |
| Dalstra 2004 | Not an RCT. All participants received the same arch wire |
| Farzanegan 2012 | Not a comparison of initial arch wires |
| Fleming 2009a | Not a comparison of initial arch wires |
| Fleming 2009b | Not a comparison of initial arch wires |
| Huffman 1983 | Not an RCT |
| Jones 1984 | Case series |
| Jones 1990 | Not an RCT |
| Kuftinec 1980 | Not an RCT |
| Lew 1988 | Not an RCT |
| Mandall 2006 | Comparison of arch wire sequences and not individual arch wires |
| Marković 2015 | Not an RCT |
| Ong 2011 | Study evaluates initial arch wire sequence |
| Pandis 2007 | Not a comparison of initial arch wires |
| Sandhu 2012 | Not an RCT |
| Weiland 2003 | A CCT split‐mouth study |
CCT = controlled clinical trial RCT = randomised controlled trial
Differences between protocol and review
Changes to authorship
Change to title from 'Initial arch wires for alignment of crooked teeth with fixed orthodontic braces' to 'Initial arch wires for tooth alignment during orthodontic treatment with fixed appliances'.
Changes to results: we revised some of our 'Risk of bias' judgements in the nine studies included in the previous version (Jian 2013), especially for blinding and selective outcome reporting.
Updated methods: 'Risk of bias' tables have been updated and expanded and 'Summary of findings' tables have been added to the review.
Contributions of authors
Yan Wang was responsible for designing and writing the review, screening search results, extracting data and contacting authors of the papers for additional information.
Chang Liu was responsible for screening search results, assessing risk of bias, extracting data and data analysis.
Fan Jian and Joy Hickman were responsible for updating the background section and checking the manuscript.
Declan Millet and Grant McIntyre were responsible for editing the manuscript.
Wenli Lai organised the retrieval of papers and assessed risk of bias.
Sources of support
Internal sources
School of Dentistry, The University of Manchester; Manchester Academic Health Sciences Centre (MAHSC); NIHR Manchester Biomedical Research Centre, UK.
External sources
-
National Institute for Health Research (NIHR), UK.
This project was supported by the NIHR, via Cochrane Infrastructure funding to Cochrane Oral Health. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health.
-
Cochrane Oral Health Global Alliance, Other.
The production of Cochrane Oral Health reviews has been supported financially by our Global Alliance since 2011 (ohg.cochrane.org/partnerships‐alliances). Contributors over the past year have been the American Association of Public Health Dentistry, USA; AS‐Akademie, Germany; the British Association for the Study of Community Dentistry, UK; the British Society of Paediatric Dentistry, UK; the Canadian Dental Hygienists Association, Canada; the Centre for Dental Education and Research at All India Institute of Medical Sciences, India; the National Center for Dental Hygiene Research & Practice, USA; New York University College of Dentistry, USA; and the Swiss Society for Endodontology, Switzerland.
Declarations of interest
Yan Wang: no conflict of interest Chang Liu: no conflict of interest Fan Jian: no conflict of interest Grant T McIntyre: no conflict of interest Declan T Millett: no conflict of interest Joy Hickman: I receive occasional remuneration for fulfilling teaching and training commitments in my areas of clinical expertise with the Tip‐Edge Appliance and combined treatments involving orthognathic surgery. Wenli Lai: no conflict of interest
New search for studies and content updated (conclusions changed)
References
References to studies included in this review
Abdelrahman 2015a {published data only}
- Abdelrahman RSh, Al‐Nimri KS, Al Maaitah EF. A clinical comparison of three aligning archwires in terms of alignment efficiency: a prospective clinical trial. Angle Orthodontist 2015;85(3):434‐9. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cioffi 2012 {published data only}
- Cioffi I, Piccolo A, Tagliaferri R, Paduano S, Galeotti A, Martina R. Pain perception following first orthodontic archwire placement‐‐thermoelastic vs superelastic alloys: a randomized controlled trial. Quintessence International 2012; Vol. 43, issue 1:61‐9. [PubMed]
Cobb 1998 {published data only}
- Cobb NW 3rd, Kula KS, Phillips C, Proffit WR. Efficiency of multi‐strand steel, superelastic Ni‐Ti and ion‐implanted Ni‐Ti archwires for initial alignment. Clinical Orthodontics and Research 1998;1(1):12‐9. [PUBMED: 2821491] [DOI] [PubMed] [Google Scholar]
Evans 1998 {published data only}
- Evans TJ. A Clinical Comparison and Performance Perspective of Three Aligning Archwires [MScD dissertation]. Cardiff, UK: University of Wales, 1996. [Google Scholar]
- Evans TJ, Jones ML, Newcombe RG. Clinical comparison and performance perspective of three aligning arch wires. American Journal of Orthodontics and Dentofacial Orthopedics 1998;114(1):32‐9. [EMBASE: 2821493] [DOI] [PubMed] [Google Scholar]
Fernandes 1998 {published data only}
- Fernandes LM, Øgaard B, Skoglund L. Pain and discomfort experienced after placement of a conventional or a superelastic NiTi aligning archwire. A randomized clinical trial [Schmerzen und beschwerden nach eingliederung eines herkömmlichen und eines superelastischen NiTi‐nivellierungsbogens]. Journal of Orofacial Orthopedics 1998;59(6):331‐9. [DOI] [PubMed] [Google Scholar]
Jones 1992 {published data only}
- Chan LSC. Pain and Discomfort Experienced During Orthodontic Treatment: a Randomised Controlled Clinical Trial of Two Initial Aligning Archwires [MScD dissertation]. Cardiff, UK: University of Wales, 1990. [Google Scholar]
- Jones M, Chan C. The pain and discomfort experienced during orthodontic treatment: a randomized controlled clinical trial of two initial aligning arch wires. American Journal of Orthodontics and Dentofacial Orthopedics 1992;102(4):373‐81. [DOI] [PubMed] [Google Scholar]
- Jones ML, Staniford H, Chan C. Comparison of superelastic NiTi and multistranded stainless steel wires in initial alignment. Journal of Clinical Orthodontics. 1990/10/01 1990; Vol. 24, issue 10:611‐3. [PubMed]
O'Brien 1990 {published data only}
- O'Brien K, Lewis D, Shaw W, Combe E. A clinical trial of aligning archwires. European Journal of Orthodontics 1990;12(4):380‐4. [DOI] [PubMed] [Google Scholar]
- O'Brien KD. A randomized controlled clinical trial of aligning archwires. British Journal of Orthodontics 1987;14:315. [Google Scholar]
- Wang Y. Could you help us [personal communication]. Email to: K O'Brien 19 March 2009.
Pandis 2009 {published data only}
- Pandis N, Polychronopoulou A, Eliades T. Alleviation of mandibular anterior crowding with copper‐nickel‐titanium vs nickel‐titanium wires: a double‐blind randomized control trial. American Journal of Orthodontics and Dentofacial Orthopedics 2009;136(2):152‐3. [DOI] [PubMed] [Google Scholar]
Quintão 2005 {published data only}
- Gravina MA, Brunharo IH, Fraga MR, Artese F, Campos MJ, Vitral RW, et al. Clinical evaluation of dental alignment and leveling with three different types of orthodonticwires. Dental Press Journal of Orthodontics 2013;18(6):31‐7. [PUBMED: 24351147] [DOI] [PubMed] [Google Scholar]
- Quintão CCA, Jones ML, Menezes LM, Koo D, Elias CN. A prospective clinical trial to compare the performance of four initial orthodontic archwires. Korean Journal of Orthodontics 2005;35(5):381‐7. [CENTRAL: CN‐01015767] [Google Scholar]
Sandhu 2013 {published data only}
- Sandhu SS, Sandhu J. A randomized clinical trial investigating pain associated with superelastic nickel‐titanium and multistranded stainless steel archwires during the initial leveling and aligning phase of orthodontic treatment. Journal of Orthodontics 2013;40(4):276‐85. [PUBMED: 24297959] [DOI] [PMC free article] [PubMed] [Google Scholar]
Sebastian 2012 {published data only}
- Sebastian B. Alignment efficiency of superelastic coaxial nickel‐titanium vs superelastic single‐stranded nickel‐titanium in relieving mandibular anterior crowding: a randomized controlled prospective study. Angle Orthodontist 2012;82(4):703‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
West 1995 {published data only}
- West AE. A Clinical Comparison of Two Initial Aligning Archwires [MScD dissertation]. Cardiff, UK: University of Wales, 1992. [Google Scholar]
- West AE, Jones ML, Newcombe RG. Multiflex versus superelastic: a randomized clinical trial of the tooth alignment ability of initial arch wires. American Journal of Orthodontics and Dentofacial Orthopedics 1995;108(5):464‐71. [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Abdelrahman 2015b {published data only}
- Abdelrahman RSh, Al‐Nimri KS, Al Maaitah EF. Pain experience during initial alignment with three types of nickel‐titanium archwires: a prospective clinical trial. Angle Orthodontist 2015;85(6):1021‐6. [PUBMED: 26516711] [DOI] [PMC free article] [PubMed] [Google Scholar]
AlQabandi 1999 {published data only}
- AlQabandi AK, Sadowsky C, BeGole EA. A comparison of the effects of rectangular and round arch wires in levelling the curve of Spee. American Journal of Orthodontics and Dentofacial Orthopedics 1999;116(5):522‐9. [DOI] [PubMed] [Google Scholar]
Bernhold 2001 {published data only}
- Bernhold M, Bondemark L. Superelastic nickel‐titanium heat‐activated archwires for tooth movement ‐ a prospective randomized study of apical root resorption. Swedish Dental Journal 2001;25:177. [Google Scholar]
Bloom 1998 {published data only}
- Bloom KL, Bhatia SN. Comparison of copper NiTi and nitinol archwires in initial alignment. European Journal of Orthodontics 1998;20:614. [Google Scholar]
Campos 2013 {published data only}
- Campos MJ, Fraga MR, Raposo NR, Ferreira AP, Vitral RW. Assessment of pain experience in adults and children after bracket bonding and initial archwire insertion. Dental Press Journal of Orthodontics 2013;18(5):32‐7. [PUBMED: 24352385] [DOI] [PubMed] [Google Scholar]
Chekay 1999 {published data only}
- Chekay BA, Killiany DM, Purcell MV, Frost RA. Apical root resorption: a comparison of wire materials. Journal of Dental Research 1999;78 Special Issue:202 (Abs No 776). [Google Scholar]
Dalstra 2004 {published data only}
- Dalstra M, Melsen B. Does the transition temperature of Cu‐NiTi archwires affect the amount of tooth movement during alignment?. Orthodontics & Craniofacial Research 2004;7(1):21–5. [DOI] [PubMed] [Google Scholar]
Farzanegan 2012 {published data only}
- Farzanegan F, Zebarjad SM, Alizadeh S, Ahrari F. Pain reduction after initial archwire placement in orthodontic patients: a randomized clinical trial. American Journal of Orthodontics and Dentofacial Orthopedics 2012;141(2):169‐73. [PUBMED: 22284284] [DOI] [PubMed] [Google Scholar]
Fleming 2009a {published data only}
- Fleming PS, Dibiase AT, Sarri G, Lee RT. Pain experience during initial alignment with a self‐ligating and a conventional fixed orthodontic appliance system. A randomized controlled clinical trial. The Angle Orthodontist 2009;79(1):46‐50. [DOI] [PubMed] [Google Scholar]
Fleming 2009b {published data only}
- Fleming PS, DiBiase AT, Sarri G, Lee RT. Comparison of mandibular arch changes during alignment and leveling with 2 preadjusted edgewise appliances. American Journal of Orthodontics and Dentofacial Orthopedics 2009;136(3):340‐7. [DOI] [PubMed] [Google Scholar]
Huffman 1983 {published data only}
- Huffman DJ, Way DC. A clinical evaluation of tooth movement along arch wires of two different sizes. American Journal of Orthodontics 1983;83(6):453‐9. [PubMed] [Google Scholar]
Jones 1984 {published data only}
- Jones ML. An investigation into the initial discomfort caused by placement of an archwire. European Journal of Orthodontics 1984;6(1):48‐54. [DOI] [PubMed] [Google Scholar]
Jones 1990 {published data only}
- Jones ML, Staniford H, Chan C. Comparison of superelastic NiTi and multistranded stainless steel wires in initial alignment. Journal of Clinical Orthodontics 1990;24(10):611‐3. [PubMed] [Google Scholar]
Kuftinec 1980 {published data only}
- Kuftinec MM, Inman GO. A comparison of plain versus multilooped arch wires in stage I of Begg therapy. American Journal of Orthodontics 1980;78(1):81‐8. [DOI] [PubMed] [Google Scholar]
Lew 1988 {published data only}
- Lew K. A comparison of archwires used for initial alignment in Begg treatment. Australian Orthodontic Journal 1988;10(3):180‐2. [PubMed] [Google Scholar]
Mandall 2006 {published data only}
- Mandall N, Lowe C, Worthington H, Sandler J, Derwent S, Abdi‐Oskouei M, et al. Which orthodontic archwire sequence? A randomized clinical trial. European Journal of Orthodontics 2006;28(6):561‐6. [DOI] [PubMed] [Google Scholar]
Marković 2015 {published data only}
- Marković E, Fercec J, Šćepan I, Glišić B, Nedeljković N, Juloski J, et al. The correlation between pain perception among patients with six different orthodontic archwires and the degree of dental crowding. Srpski Arhiv Za Celokupno Lekarstvo 2015;143(3‐4):134‐40. [PUBMED: 26012120] [DOI] [PubMed] [Google Scholar]
Ong 2011 {published data only}
- Ong E, Ho C, Miles P. Alignment efficiency and discomfort of three orthodontic archwire sequences: a randomized clinical trial. Journal of Orthodontics 2011;38(1):32‐9. [DOI] [PubMed] [Google Scholar]
Pandis 2007 {published data only}
- Pandis N, Polychronopoulou A, Eliades T. Self‐ligating vs conventional brackets in the treatment of mandibular crowding: a prospective clinical trial of treatment duration and dental effects. American Journal of Orthodontics and Dentofacial Orthopedics 2007;132(2):208‐15. [DOI] [PubMed] [Google Scholar]
Sandhu 2012 {published data only}
- Sandhu SS, Shetty VS, Mogra S, Varghese J, Sandhu J, Sandhu JS. Efficiency, behavior, and clinical properties of superelastic NiTi versus multistranded stainlesssteel wires: a prospective clinical trial. The Angle Orthodontist 2012;82(5):915‐21. [PUBMED: 22225530] [DOI] [PMC free article] [PubMed] [Google Scholar]
Weiland 2003 {published data only}
- Weiland F. Constant versus dissipating forces in orthodontics: the effect on initial tooth movement and root resorption. European Journal of Orthodontics 2003;25(4):335‐42. [DOI] [PubMed] [Google Scholar]
Additional references
Ballard 2009
- Ballard DJ, Jones AS, Petocz P, Darendeliler MA. Physical properties of root cementum: part 11. Continuous vs intermittent controlled orthodontic forces on root resorption. A microcomputed‐tomography study. American Journal of Orthodontics and Dentofacial Orthopedics 2009;136(1):1‐8; discussion 8‐9. [DOI] [PubMed] [Google Scholar]
Bellini 2016
- Bellini H, Moyano J, Gil J, Puigdollers A. Comparison of the superelasticity of different nickel‐titanium orthodontic archwires and the loss of their properties by heat treatment. Journal of Materials Science. Materials in Medicine 2016;27(10):158. [DOI: 10.1007/s10856-016-5767-5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Burstone 1981
- Burstone CJ. Variable‐modulus orthodontics. American Journal of Orthodontics 1981;80(1):1‐16. [DOI] [PubMed] [Google Scholar]
Burstone 1985
- Burstone CJ, Qin B, Morton JY. Chinese NiTi wire‐‐a new orthodontic alloy. American Journal of Orthodontics 1985;87(6):445‐52. [DOI] [PubMed] [Google Scholar]
Deeks 2011
- Deeks JJ, Higgins JPT, Altman DG (editors). Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Egger 1997
- Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;315(7109):629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Erdinç 2004
- Erdinç E, Dinçer B. Perception of pain during orthodontic treatment with fixed appliances. European Journal of Orthodontics 2004;26(1):79‐85. [DOI] [PubMed] [Google Scholar]
Evans 1996
- Evans TJ, Durning P. Aligning archwires, the shape of things to come?‐‐a fourth and fifth phase of force delivery. British Journal of Orthodontics 1996;23(3):269‐75. [DOI] [PubMed] [Google Scholar]
Firestone 1999
- Firestone AR, Scheurer PA, Bürgin WB. Patients' anticipation of pain and pain‐related side effects, and their perception of pain as a result of orthodontic treatment with fixed appliances. European Journal of Orthodontics 1999;21(4):387‐96. [DOI] [PubMed] [Google Scholar]
GRADE 2004
- The GRADE Working Group. Grading quality of evidence and strength of recommendations. BMJ 2004;328(7454):1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011a
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
HSCIC 2015
- Health and Social Care Information Centre. Children's Dental Health Survey 2013. Report 4: The Burden of Dental Disease in Children: England, Wales and Northern Ireland. Health and Social Care Information Centre, 2015. [ISBN: 978‐1‐78386‐323‐5] [Google Scholar]
Kapila 1989
- Kapila S, Sachdeva R. Mechanical properties and clinical applications of orthodontic wires. American Journal of Orthodontics and Dentofacial Orthopedics 1989;96(2):100‐9. [DOI] [PubMed] [Google Scholar]
Keim 2014
- Keim RG, Gottlieb EL, Vogels DS 3rd, Vogels PB. 2014 JCO study of orthodontic diagnosis and treatment procedures, Part 1: results and trends. Journal of Clinical Orthodontics 2014;48(10):607‐30. [PubMed] [Google Scholar]
Kusy 1997
- Kusy RP. A review of contemporary archwires: their properties and characteristics. Angle Orthodontist 1997;67(3):197‐207. [DOI] [PubMed] [Google Scholar]
Kusy 2007
- Kusy RP, Whitley JQ. Thermal and mechanical characteristics of stainless steel, titanium‐molybdenum, and nickel‐titanium archwires. American Journal of Orthodontics and Dentofacial Orthopedics 2007;131(2):229‐37. [DOI] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Linge 1991
- Linge L, Linge BO. Patient characteristics and treatment variables associated with apical root resorption during orthodontic treatment. American Journal of Orthodontics and Dentofacial Orthopedics 1991;99(1):35‐43. [DOI] [PubMed] [Google Scholar]
Little 1975
- Little RM. The irregularity index: a quantitative score of mandibular anterior alignment. American Journal of Orthodontics 1975;68(5):554‐63. [DOI] [PubMed] [Google Scholar]
Manzanera 2009
- Manzanera D, Montiel‐Company JM, Almerich‐Silla JM, Gandía JL. Orthodontic treatment need in Spanish schoolchildren: an epidemiological study using the Index of Orthodontic Treatment Need. European Journal of Orthodontics 2009;31(2):180‐3. [DOI] [PubMed] [Google Scholar]
Marques 2007
- Marques CR, Couto GB, Orestes Cardoso S. Assessment of orthodontic treatment needs in Brazilian schoolchildren according to the Dental Aesthetic Index (DAI). Community Dental Health 2007;24(3):145‐8. [PubMed] [Google Scholar]
Moher 2005
- Moher D, Schulz KF, Altman D, CONSORT Group. The CONSORT Statement: revised recommendations for improving the quality of reports of parallel‐group randomized trials 2001. Explore (New York, NY) 2005;1(1):40‐5. [DOI] [PubMed] [Google Scholar]
Ng'ang'a 1997
- Ng'ang'a PM, Stenvik A, Ohito F, Ogaard B. The need and demand for orthodontic treatment in 13‐ to 15‐year‐olds in Nairobi, Kenya. Acta Odontologica Scandinavica 1997;55(5):325‐8. [DOI] [PubMed] [Google Scholar]
Ngan 1989
- Ngan P, Kess B, Wilson S. Perception of discomfort by patients undergoing orthodontic treatment. American Journal of Orthodontics and Dentofacial Orthopedics 1989;96(1):47‐53. [DOI] [PubMed] [Google Scholar]
O'Brien 1993
- O'Brien KD, Shaw WC, Roberts CT. The use of occlusal indices in assessing the provision of orthodontic treatment by the hospital orthodontic service of England and Wales. British Journal of Orthodontics 1993;20(1):25‐35. [DOI] [PubMed] [Google Scholar]
Proffit 2000
- Proffit WR. Contemporary Orthodontics. St Louis: CV Mosby Cooperation, 2000. [Google Scholar]
Quintão 2009
- Quintão CC, Cal‐Neto JP, Menezes LM, Elias CN. Force‐deflection properties of initial orthodontic archwires. World Journal of Orthodontics 2009;10(1):29‐32. [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Richmond 1993
- Richmond S, Shaw WC, Stephens CD, Webb WG, Roberts CT, Andrews M. Orthodontics in the general dental service of England and Wales: a critical assessment of standards. British Dental Journal 1993;174(9):315‐29. [DOI] [PubMed] [Google Scholar]
Riley 2009
- Riley M, Bearn DR. A systematic review of clinical trials of aligning archwires. Journal of Orthodontics 2009;36(1):42‐51. [DOI] [PubMed] [Google Scholar]
Santoro 2001a
Santoro 2001b
Scheurer 1996
- Scheurer PA, Firestone AR, Bürgin WB. Perception of pain as a result of orthodontic treatment with fixed appliances. European Journal of Orthodontics 1996;18(4):349‐57. [DOI] [PubMed] [Google Scholar]
Schünemann 2011
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and ‘Summary of findings' tables. In: Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Van Wyk 2005
- Wyk PJ, Drummond RJ. Orthodontic status and treatment need of 12‐year‐old children in South Africa using the Dental Aesthetic Index. Journal of the South African Dental Association 2005;60(8):334‐6, 338. [PubMed] [Google Scholar]
Whiting‐O'Keefe 1984
- Whiting‐O'Keefe QE, Henke C, Simborg DW. Choosing the correct unit of analysis in Medical Care experiments. Medical Care 1984;22(12):1101‐14. [DOI] [PubMed] [Google Scholar]
Worthington 2015
- Worthington H, Clarkson J, Weldon J. Priority oral health research identification for clinical decision‐making. Evidence‐based Dentistry 2015;16(3):69‐71. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Jian 2013
- Jian F, Lai W, Furness S, McIntyre GT, Millett DT, Hickman J, et al. Initial arch wires for tooth alignment during orthodontic treatment with fixed appliances. Cochrane Database of Systematic Reviews 2013, Issue 4. [DOI: 10.1002/14651858.CD007859.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Wang 2010
- Wang Y, Jian F, Lai W, Zhao Z, Yang Z, Liao Z, et al. Initial arch wires for alignment of crooked teeth with fixed orthodontic braces. Cochrane Database of Systematic Reviews 2010, Issue 4. [DOI: 10.1002/14651858.CD007859.pub2] [DOI] [PubMed] [Google Scholar]