

Abstract
Background
Acupuncture has a history of traditional use in China for women's health conditions including premenstrual syndrome (PMS), but its effectiveness for this condition remains unclear. This review examined the available evidence supporting the use of acupuncture or acupressure to treat PMS.
Objectives
To evaluate the effectiveness and safety of acupuncture or acupressure for women with PMS or premenstrual dysphoric disorder (PMDD).
Search methods
We searched the Cochrane Gynaecology and Fertility Specialised Register, Cochrane Central Register of Studies Online (CENTRAL CRSO), MEDLINE, Embase, AMED, PsycINFO, CINAHL (from inception to 21 September 2017), two clinical trial databases (from their inception to 21 September 2017), and four electronic databases in China (from their inception to 15 October 2017): Chinese Biomedical Literature database (CBM), China National Knowledge Infrastructure (CNKI), VIP information/ Chinese Scientific Journals database and WANFANG. Reference lists from included articles were handsearched.
Selection criteria
We included studies if they randomised women with PMS and associated disorders (PMDD and late luteal phase dysphoric disorder/LPDD) to receive acupuncture or acupressure versus sham, usual care/waiting‐list control or pharmaceutical interventions mentioned by the International Society for Premenstrual Disorders (ISPMD). If acupuncture or acupressure were combined with another therapy, these studies were also included where the additional therapy was the same in both groups. Cross‐over studies were eligible for inclusion, but only data from the first phase could be used.
Data collection and analysis
Two review authors independently selected the studies, assessed eligible studies for risk of bias, and extracted data from each study. Study authors were contacted for missing information. The quality of the evidence was assessed using GRADE. Our primary outcomes were overall premenstrual symptoms and adverse events. Secondary outcomes included specific PMS symptoms, response rate and quality of life.
Main results
Five trials (277 women) were included in this review. No trials compared acupuncture or acupressure versus other active treatments. The number of treatment sessions ranged from seven to 28. The quality of the evidence ranged from low to very low quality, the main limitations being imprecision due to small sample sizes and risk of bias related to detection bias and selective reporting.
Acupuncture versus sham acupuncture
Acupuncture may provide a greater reduction in mood‐related PMS symptoms (mean difference (MD) ‐9.03, 95% confidence interval (CI) ‐10.71 to ‐7.35, one randomised controlled trial (RCT), n = 67, low‐quality evidence) and in physical PMS symptoms (MD ‐9.11, 95% CI ‐10.82 to ‐7.40, one RCT, n = 67, low‐quality evidence) than sham acupuncture, as measured by the Daily Record of Severity of Problems scale (DRSP). The evidence suggests that if women have a mood score of 51.91 points with sham acupuncture, their score with acupuncture would be between 10.71 and 7.35 points lower and if women have a physical score of 46.11 points, their score with acupuncture would be between 10.82 and 7.4 points lower.There was insufficient evidence to determine whether there was any difference between the groups in the rate of adverse events (risk ratio (RR) 1.74, 95% CI 0.39 to 7.76, three RCTs, n = 167, I2 = 0%, very low‐quality evidence).
Specific PMS symptoms were not reported
There may be little or no difference between the groups in response rates. Use of a fixed‐effect model suggested a higher response rate in the acupuncture group than in the sham group (RR 2.59, 95% CI 1.71 to 3.92; participants = 100; studies = 2; I2 = 82%), but owing to the high heterogeneity we tested the effect of using a random‐effects model, which provided no clear evidence of benefit for acupuncture (RR 4.22, 95% CI 0.45 to 39.88, two RCTs, n = 100, I2 = 82%, very low‐quality evidence).
Acupuncture may improve quality of life (measured by the WHOQOL‐BREF) compared to sham (MD 2.85, 95% CI 1.47 to 4.23, one RCT, n = 67, low‐quality evidence).
Acupuncture versus no treatment
Due to the very low quality of the evidence, we are uncertain whether acupuncture reduces PMS symptoms compared to a no treatment control (MD ‐13.60, 95% CI ‐15.70 to ‐11.50, one RCT, n = 14).
No adverse events were reported in either group.
No data were available on specific PMS symptoms, response rate or quality of life outcomes.
Acupressure versus sham acupressure
We found low‐quality evidence that acupressure may reduce the number of women with moderate to severe PMS symptoms at the end of the trial compared to sham acupressure (RR 0.64 95% CI 0.52 to 0.79, one RCT, n = 90, low‐quality evidence). The evidence suggests that if 97 women out of 100 in the sham acupressure group had moderate to severe PMS symptoms, the number of women in the acupressure group with moderate to severe symptoms would be 50 to 76 women.
Acupressure may improve both physical (MD 24.3, 95% CI 17.18 to 31.42, one RCT, n = 90, low‐quality evidence) and mental (MD 17.17, 95% CI 13.08 to 21.26, one RCT, n = 90, low‐quality evidence) quality of life.
No data were available on adverse events, specific symptoms or response rates.
Authors' conclusions
The limited evidence available suggests that acupuncture and acupressure may improve both physical and psychological symptoms of PMS when compared to a sham control. There was insufficient evidence to determine whether there was a difference between the groups in rates of adverse events.There is no evidence comparing acupuncture or acupressure versus current ISPMD recommended treatments for PMS such as selective serotonin reuptake inhibitors (SSRIs). Further research is required, using validated outcome measures for PMS, adequate blinding and suitable comparator groups reflecting current best practice.
Plain language summary
Acupuncture and acupressure for premenstrual syndrome (PMS)
Review question
Cochrane authors reviewed the evidence on the effectiveness and safety of acupuncture or acupressure in women with premenstrual syndrome (PMS) or premenstrual dysphoric disorder.
Background
We wanted to know whether using acupuncture or acupressure therapy was better than receiving sham acupuncture, no treatment or currently recommended pharmaceutical medications for PMS such as serotonin reuptake inhibitors (SSRIs ‐ a type of anti‐depressant).
Study characteristics
We found five randomised controlled trials including 277 women that examined the effect of acupuncture or acupressure in women with PMS. The evidence is current to September 2017. We also ran a smaller search in November 2017 to see if we had missed any recently published studies. Three trials compared acupuncture with sham acupuncture, one compared acupuncture with no treatment and one compared acupressure with sham acupressure.
Key results
Acupuncture may reduce overall mood and physical PMS symptoms when compared to sham. Acupressure may reduce the number of women having moderate to severe PMS symptoms when compared to sham acupressure. There was not enough evidence to determine the safety of acupuncture or acupressure.
Quality of the evidence
The quality of the evidence ranged from low to very low.The main limitations were imprecision due to small sample sizes (too few women in the study) and risk of bias related to blinding (where researchers or participants knew what treatment they were getting).
Summary of findings
Background
Description of the condition
Premenstrual syndrome (PMS) is a clinical syndrome resulting in symptoms that occur in relation to the menstrual cycle, and can lead to interference with women's lives. Symptoms usually begin five to 11 days before menstruation, and cease when menstruation starts, or soon after (Backstorm 1991; Dickerson 2004). PMS is common, with 95% of women reported to have one or more premenstrual symptoms during their reproductive life (Hylan 1999). Symptoms are often mild, but in some women can be severe enough to substantially affect daily activities. About 5% to 8% of women thus suffer from severe PMS; most of these women also meet criteria for the associated condition of premenstrual dysphoric disorder (PMDD) (Kimberly 2008). There is evidence that raised levels of inflammatory markers may play a role in PMS (Bertone‐Johnson 2014; Gold 2016).The aetiology of PMS is still unclear.
More than 200 premenstrual symptoms have been recorded and can be classified into three broad categories:
behavioural symptoms including fatigue, insomnia, dizziness, changes in sexual interest, food cravings or overeating;
psychological symptoms including irritability, anger, depressed mood, crying and tearfulness, anxiety, tension, mood swings, lack of concentration, confusion, forgetfulness, restlessness, loneliness, decreased self‐esteem, tension;
physical symptoms including headaches, breast tenderness and swelling, back pain, abdominal pain and bloating, weight gain, swelling of extremities, water retention, nausea, muscle and joint pain (Dickerson 2004; Reid 1986).
PMDD, previously known as late luteal phase dysphoric disorder (LLPDD), is a more severe form of PMS (O'Brien 2011). PMDD is characterised by intense emotional symptoms occurring between ovulation and menstruation. Symptoms include severe depression, irritability and/or mood swings which interfere with relationships, social functioning, and work or school (Bancroft 1993; Medem 2004). According to the Diagnostic and Statistical Manual of Mental Disorders (DSM‐V) the diagnosis of PMDD requires (1) the presence of at least five luteal‐phase symptoms (panel), at least one of which must be a mood symptom (i.e. depressed mood, anxiety or tension, affect lability, or persistent anger and irritability); (2) the timing of symptoms confirmed by two cycles of daily charting; and (3) evidence of functional impairment. Finally, symptoms must not be the exacerbation of another psychiatric condition (APA 2013).The American College of Obstetrics and Gynecology (ACOG) criteria include the presence of at least one psychological or physical symptom that causes significant impairment and confirmed by means of prospective ratings (ACOG 2001).
Description of the intervention
Acupuncture is a Chinese medical treatment that has been used for more than 2000 years in China and Japan (White 2004). Acupuncture involves the insertion of fine metal needles into the skin and underlying tissues at precise points on the body. The needle can be left alone, or can be stimulated by twisting of the needle in various ways, or stimulated by electricity (electro‐acupuncture). Acupressure stimulates the same points as acupuncture using manual pressure, usually with the finger or thumb, on these points rather than the insertion of a needle (Beal 1999). Acupressure is able to be self‐delivered by the person themselves, while acupuncture is usually delivered by a trained practitioner. However, acupuncture is considered to give a greater 'dose' of treatment due to the insertion and manipulation of the needle (Armour 2016), rather than pressure alone. Acupuncture treatment is composed of needling aspects (choice of points and needling techniques), specific components relating to the style of diagnosis and treatment used, and generic needling components not specific to acupuncture such as belief, time, and attention given to the patient (Langevin 2011).
How the intervention might work
The mechanism of acupuncture remains unclear although potential mechanisms have been identified from research, and it is likely that a number of concurrent pathways may contribute to the overall therapeutic effect. Acupuncture can modulate endogenous opioids (Mayor 2013), and needling of specific acupuncture points such as SP6 may alter blood flow to the uterus and modulate prostaglandin levels (Armour 2016). Recent research has shown that acupuncture acts on a variety of inflammatory markers (McDonald 2013; McDonald 2015). Because women with PMS have elevated levels of inflammatory markers (Gold 2016), this may be a primary pathway through which acupuncture may reduce PMS symptoms.
Why it is important to do this review
Many interventions have been used to treat PMS, such as selective serotonin reuptake inhibitors (SSRIs) and hormonal interventions. Current guidelines for the treatment of PMS and PMDD from the International Society for Premenstrual Disorders (ISPMD) recommend SSRI medication as a first line of treatment (Ismaili 2016). SSRI treatments are effective for many women with PMS however the side effects are frequent and can lead to discontinuation (Marjoribanks 2013). Acupuncture may be an effective non‐pharmacological therapeutic option with a much lower rate of adverse events than SSRI medication (Witt 2009).
Objectives
To evaluate the effectiveness and safety of acupuncture or acupressure for women with premenstrual syndrome (PMS) or premenstrual dysphoric disorder (PMDD).
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials without restriction on language and publication types. Cross‐over studies were eligible for inclusion, but we planned to include only data from the first phase. We excluded non‐randomised studies (for example studies with evidence of inadequate sequence generation such as alternate days, patient numbers).
Types of participants
Inclusion
We included studies of women of any age who met the diagnostic criteria for premenstrual syndrome (PMS) or premenstrual dysphoric disorder (PMDD). Diagnosis of PMS or PMDD had to be made prior to trial inclusion by a healthcare professional such as a general practitioner using an established diagnostic tool such as the DSM‐IV (Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition) and ICD‐10 (International Statistical Classification of Diseases and Related Health Problems 10th Revision), or a validated symptom screening tool.
Exclusion
We excluded studies where there was only a self‐diagnosis of PMS.
Types of interventions
The included intervention group methods were body acupuncture, electro‐acupuncture, scalp acupuncture, ear acupuncture, acupressure, electromagnetic acupuncture, pyonex, intradermal needling, or moxibustion. However, we excluded acupoint injection. If acupuncture or acupressure were combined with another valid therapy, we included these studies if the additional therapy was the same in both groups such as acupuncture plus selective serotonin reuptake inhibitors (SSRIs) versus SSRI alone.
Control group methods were sham acupuncture or sham acupressure, no treatment, or any conventional treatments recommended by the International Society for Premenstrual Disorders (ISPMD), including SSRIs, oral contraceptives, gonadotropin‐releasing hormone agonists, danazol or estradiol.
We excluded studies which compared two different forms of acupuncture, or compared acupuncture with a herbal medicine or a conventional treatment without proven efficacy.
Types of outcome measures
Primary outcomes
Overall premenstrual symptoms, measured using a validated prospective screening tool (such as the Premenstrual Symptom Screening Tool (PSST) or Daily Record of Severity of Problems (DRST)), or by pre‐defined medical diagnostic criteria. These may be reported as an overall score or by separate sub scales such as mental and physical symptoms.
Adverse events (all adverse events, specific adverse effects, withdrawals for adverse effects).
Secondary outcomes
Specific symptoms of PMS: behavioural, psychological, physical.
Response rate (according to how response to treatment was defined in individual studies).
Quality of life, measured by a validated scale such as the Short form (SF) SF‐36 or SF‐12.
Search methods for identification of studies
We conducted a comprehensive and exhaustive search strategy to identify all relevant studies regardless of language or publication status (published, unpublished, in press, and in progress). The search was conducted in consultation with the Gynaecology and Fertility Group Information Specialist.
See Appendix 1, Appendix 2; Appendix 3; Appendix 4; Appendix 5; Appendix 6; Appendix 7 for search strategies.
Electronic searches
We searched the Cochrane Gynaecology and Fertility Specialised Register, the Cochrane Central Register of Studies (CENTRAL CRSO), MEDLINE, AMED, Embase, PsycINFO, CINAHL (from inception to 21 September 2017) and four electronic databases in China (from inception to 15 Oct 2017): Chinese Biomedical Literature database (CBM), China National Knowledge Infrastructure (CNKI), VIP information/Chinese Scientific Journals database and WANFANG database. An additional search on 2 November 2017 was undertaken using PubMed and Google Scholar to identify any recent trials not yet included in the previous databases.
Searching other resources
Other sources of trials included:
Trial registers for ongoing and registered trials: http://www.clinicaltrials.gov and WHO International Clinical Trials Registry Platform (apps.who.int/trialsearch/).
Reference lists from included articles and previous systematic reviews.
-
Additional electronic resources were searched in November 2017:
DARE – Database of Abstracts of Reviews of Effects (reference lists from non Cochrane reviews on similar topics);
ProQuest Dissertations & Theses for unpublished dissertations and theses;
Conference abstracts on the Web of Science;
OpenGrey for unpublished literature from Europe ‐ http://www.opengrey.eu/;
LILACS database for the Portuguese and Spanish speaking world ‐ http://regional.bvsalud.org/php/index.php?lang=en.
Additional electronic resources were searched in English.
Data collection and analysis
Selection of studies
Two review authors (MA and CE) screened the titles and abstracts of articles found in the search, and discarded trials that were clearly not eligible. One review author (JH) searched for and selected the trials from the Chinese databases.
One review author (JH) translated Chinese papers. MA, CE and JH independently assessed whether trials met the inclusion criteria, with disagreements resolved by discussion. If articles contained insufficient information to make a decision about eligibility, MA or CE attempted to contact authors of the original reports to obtain further details. If details of randomisation were unclear in the reporting, we contacted all trial authors to ascertain if the study was truly randomised. We made a first contact and then sent a reminder one month later.
The selection process was documented with a "PRISMA" flow chart (Figure 1).
1.
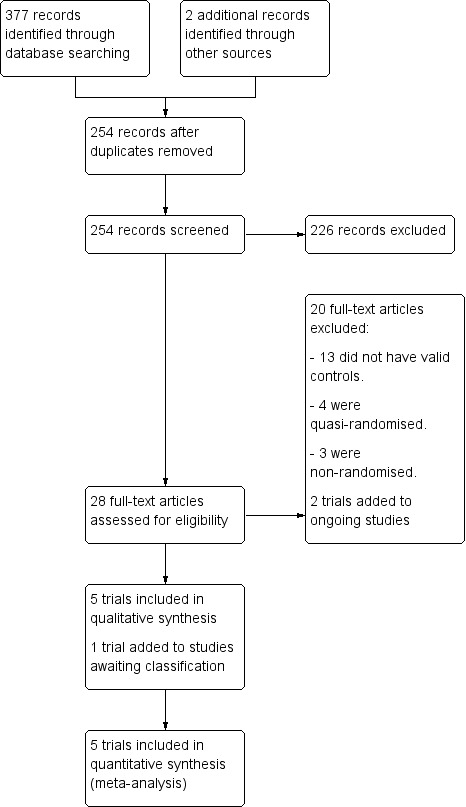
Study flow diagram.
Data extraction and management
Following an assessment for inclusion MA, CS, CE, TW and JH independently extracted data. We resolved discrepancies by discussion. For each included trial we extracted data regarding the location of the trial, the methods of the trial (as per assessment of risk of bias), the participants (age range, eligibility criteria), the nature of the interventions, and data relating to the outcomes specified above. We collected information on reported benefits and adverse effects. We extracted data and entered them onto a form sourced from the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). MA checked and entered data into Review Manager 5.3 (RevMan 2014).
Assessment of risk of bias in included studies
Two review authors (from MA, CS, CE, TW and JH) independently assessed risks of bias for each trial, using the criteria described in the Cochrane Handbook (Higgins 2011). The tool consists of seven items, with three potential responses: 'yes', 'no', and 'unclear'. In all cases a judgement of ‘yes’ indicates a low risk of bias and a judgement of ‘no’ indicates a high risk of bias. If insufficient detail was reported our judgement was usually ‘unclear’. We also made a judgement of 'unclear' if we knew what happened in the study but the risk of bias was unknown to us, or if an entry was not relevant to the study at hand (particularly for assessing blinding and incomplete outcome data, or when the outcome being assessed by the entry had not been measured in the study).
We assessed the following characteristics: sequence generation, allocation concealment, blinding (or masking) of participants, blinding (or masking) of outcome assessors, incomplete data assessment, selective outcome reporting, and other sources of bias. We resolved disagreements that arose at any stage by discussion between the review authors or with a third party, when necessary. We generated a 'Risk of bias' assessment table for each study. We assessed other aspects of trial quality including the extent of blinding (if appropriate), whether groups were comparable at baseline, the extent of losses to follow‐up, non‐compliance and whether the outcome assessment was standardised according to the Cochrane Handbook (Higgins 2011). This information is presented in the Characteristics of included studies.
Measures of treatment effect
We performed statistical analysis in accordance with the Cochrane Handbook (Higgins 2011). We performed statistical analysis using Review Manager 5 software (RevMan 2014). For dichotomous data, we expressed results for each study as summary risk ratios (RRs) with corresponding 95% confidence intervals (CIs), using the Mantel‐Haenszel method. We expressed continuous data as mean differences (MDs) with 95% CIs, or as standardised mean differences (SMDs) if outcomes were conceptually the same but measured in different ways in the different trials. A standard rule of thumb for interpreting effect sizes is that 0.2 represents a small effect, 0.5 a moderate effect and 0.8 a large effect.
Unit of analysis issues
The primary analysis was per woman randomised. We included trials with multiple arms and describe them in the Characteristics of included studies, for example, two different types of acupressure compared with sham acupressure. If there were two acupuncture or acupressure groups, we combined data from both treatment arms into one group. For studies with a sham control and no treatment control group, we divided the shared intervention evenly between groups as described in the Cochrane Handbook (Higgins 2011). Where outcomes were repeated measures, we undertook analysis of outcomes at the end of the intervention.
Dealing with missing data
We analysed data on an intention‐to‐treat basis, as far as possible. We did not impute missing data but we did report the proportion lost to follow‐up and analysed only the available data. In future updates, if more eligible studies are included, the impact of including studies with high levels of missing data in the overall assessment of treatment effect will be explored by using sensitivity analysis.
Assessment of heterogeneity
We measured inconsistency across trials in the meta‐analysis using the I² statistic. This describes the percentage of total variation across studies that is due to heterogeneity rather than chance (Higgins 2003; Higgins 2011). The interpretation of the I² statistic is as follows:
10% to 40% might not be important;
30% to 60% may represent moderate heterogeneity;
50% to 90% may represent substantial heterogeneity;
75% to 100% considerable heterogeneity.
We regarded heterogeneity as substantial if an I² was greater than 50% and either the Tau² was greater than zero, or there was a low P value (less than 0.10) in the Chi² test for heterogeneity. If we identified substantial heterogeneity (above 50%), we used a random‐effects model in the meta‐analysis.
Assessment of reporting biases
We planned to investigate potential biases of publication using the funnel plot or other analytical methods (Egger 1997). If there were 10 or more studies in the same analysis we would have investigated reporting biases (such as publication bias) using funnel plots. If visual assessment had suggested asymmetry, we would have explored possible reasons.
Data synthesis
We carried out statistical analysis using the Review Manager software (RevMan 2014). We used fixed‐effect meta‐analysis for combining data where it was reasonable to assume that studies were estimating the same underlying treatment effect: i.e. where trials were examining the same intervention, and the trials’ populations and methods were judged sufficiently similar, or if the number of studies was small (less than three).
If there was clinical heterogeneity sufficient to expect that the underlying treatment effects differed between trials, or if substantial statistical heterogeneity was detected, we used random‐effects meta‐analysis to produce an overall summary, if an average treatment effect across trials was considered clinically meaningful. The random‐effects summary was treated as the average range of possible treatment effects and we discussed the clinical implications of treatment effects differing between trials. If the average treatment effect was not clinically meaningful, we did not combine trials. Where we used random‐effects analyses, the results were presented as the average treatment effect with 95% CIs, and the estimates of Tau² and I².
An increase in the odds of a particular outcome, which may be beneficial (e.g. reduction in symptoms) or detrimental (e.g. adverse effects), will be displayed graphically in the meta‐analyses to the right of the centre‐line and a decrease in the odds of an outcome to the left of the centre‐line.
Subgroup analysis and investigation of heterogeneity
Had we identified substantial heterogeneity, we planned to investigate it using sensitivity analyses and to consider whether an overall summary was meaningful, and if it was, to undertake a random‐effects analysis.
Sensitivity analysis
We planned to conduct sensitivity analyses for the primary outcomes to determine whether the conclusions were robust to arbitrary decisions made regarding the eligibility and analysis. These analyses included consideration of whether the review conclusions would have differed if eligibility had been restricted to studies at low risk of bias (defined as studies rated as being at low risk of bias with respect to sequence generation and allocation concealment, and not rated as at high risk of bias in any of the domains assessed).
We did not perform any sensitivity analyses because each subgroup analysis did not include sufficient studies.
Overall quality of the body of evidence: 'Summary of findings' tables
We used the GRADE approach as outlined in the GRADE handbook in order to assess the quality of the body of evidence. We prepared a 'Summary of findings' table using GRADEpro (GRADEpro GDT 2015) and Cochrane methods. This table outlines the overall quality of the body of evidence for the main review outcomes (Overall premenstrual symptoms, adverse events, specific PMS symptoms, response rates and quality of life) for the main review comparison (acupuncture versus sham). We also generated 'Summary of findings' tables for the comparisons 'acupuncture versus no treatment'; and 'acupressure versus sham acupressure' for these same outcomes.
The GRADE approach uses five considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of the body of evidence for each outcome. The evidence can be downgraded from 'high quality' by one level for serious (or by two levels for very serious) limitations, depending on assessments for risk of bias, indirectness of evidence, serious inconsistency, imprecision of effect estimates or potential publication bias. Judgements were justified, documented, and incorporated into reporting of results for each outcome.
Assessment of the quality of the acupuncture intervention delivered
We assessed the quality of the acupuncture or acupressure intervention in published journal articles using the National Institute for Complementary Medicine Acupuncture Network (NICMAN) scale (Smith 2017). The NICMAN scale was developed to assess the quality of the acupuncture delivered in a clinical trial, and is designed to be used in combination with the STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) reporting guidelines (MacPherson 2010). This scale assesses and scores the following: the rationale behind the point selection, the qualifications and experience of the practitioner delivering the intervention, the adequacy of the number of treatment sessions, and the reporting of vital components of the acupuncture practice itself such as needle depth, diameter and stimulation. Higher scores indicate improved quality of the acupuncture intervention delivered, but there is no cut‐off for a 'high' versus 'low' quality score on the NICMAN scale. Each trial was independently scored out of 23 by two review authors (from CS, JH, CE, TW, YY). Any discrepancies were resolved by discussion. If this was not reached a third review author (MA) decided on the final score.
Results
Description of studies
Results of the search
The search retrieved 379 articles. Twenty‐eight studies were potentially eligible and were retrieved in full text. Five studies met our inclusion criteria. Twenty studies were excluded. One study was placed in awaiting classification due to an inability to contact the study authors. Two studies are ongoing. See study tables: Characteristics of included studies; Characteristics of excluded studies; Characteristics of studies awaiting classification; Characteristics of ongoing studies
Included studies
Study design and setting
Two hundred and seventy‐seven women with premenstrual syndrome (PMS )were included in this review. One trial was from Croatia (Habek 2002), two from China (Yu 2006; Zhang 2017), one from Korea (Shin 2009) and one from Iraq (Bazarganipour 2017). One trial (Bazarganipour 2017) reported funding support.
Two trials were undertaken in the community (Bazarganipour 2017; Shin 2009), two trials in an outpatient hospital setting (Yu 2006; Zhang 2017), and in one trial the setting was unclear (Habek 2002).
All studies were randomised controlled trials (RCTs). Two studies had a parallel two‐arm design in which participants were randomised either to acupuncture or sham acupuncture group (Habek 2002; Yu 2006). Three studies had a three‐arm design (Bazarganipour 2017; Shin 2009; Zhang 2017). For two of the three armed trials, only the appropriate arms of verum acupuncture and sham or waiting‐list control were included in the analysis (Shin 2009; Zhang 2017). One trial included two different acupressure groups, one using the acupuncture point LI4 and one using LR3 (Bazarganipour 2017). These were combined into one active group as specified in Unit of analysis issues.
Participants
Women in two trials were aged from 18 to 45 years (Bazarganipour 2017;Yu 2006), one from 18 to 40 years (Zhang 2017),one from 20 to 35 years (Shin 2009); the other only reported the mean ages of the two groups were both about 30 years (Habek 2002). Sample sizes ranged from 20 (Shin 2009) to 90 (Bazarganipour 2017).
DSM‐IV was used as diagnostic criteria in two trials (Yu 2006; Zhang 2017), ICD‐10 was used in one trial (Shin 2009), PSST scores in one trial (Bazarganipour 2017) and a patient history form was used in the other trial (Habek 2002).
Women were screened for baseline PMS symptoms for three menstrual cycles in two trials (Shin 2009; Yu 2006), two cycles in one trial (Habek 2002), and one cycle in two trials (Bazarganipour 2017; Zhang 2017).
Interventions and comparators
Three trials reported the effect between acupuncture and sham acupuncture (Habek 2002; Yu 2006; Zhang 2017), and one between acupuncture and no treatment control (Shin 2009). One of these trials (Habek 2002), combined acupuncture with auriculo‐acupuncture, which is acupuncture administered to points on the pinna of the ear, while another administered Korean hand acupuncture (Shin 2009). One trial compared acupressure and sham acupressure (Bazarganipour 2017). The type of sham acupuncture used was superficial needling on 'non‐meridian' or 'non‐acupuncture' points in two trials (Habek 2002; Yu 2006) and a non‐penetrative sham in one trial (Zhang 2017). Sham acupressure consisted of acupressure being applied to an area unrelated to PMS symptoms (Bazarganipour 2017).
Treatment frequency and total number of sessions
Acupuncture 'dose' consists of neurophysiological and cumulative dose (Armour 2016). Neurophysiological components include needle retention time, number of acupuncture points used, location of acupuncture points and type of stimulation used (manual versus electro‐acupuncture). Cumulative dose components include the frequency and total number of treatments.
The treatment frequency, timing of treatment and total number of treatments used in the included studies were very heterogenous. The number of treatments ranged from seven (Habek 2002) to 28 (Bazarganipour 2017) in total. Treatments were given throughout the menstrual cycle in two studies (Shin 2009; Zhang 2017), in the luteal phase only in two studies (Bazarganipour 2017; Habek 2002), and in the last seven days of the cycle in another study (Yu 2006). Treatment frequency varied from daily (Bazarganipour 2017), to three times per week (Zhang 2017).
The number of acupuncture points varied between studies
Duration of treatment sessions
Session durations and needle retention ranged from 15 minutes (Shin 2009) to 30 minutes (Habek 2002; Yu 2006; Zhang 2017).
Outcomes
All trials except Zhang 2017 collected their outcomes at the end of the intervention. Zhang 2017 had a one‐ and two‐month follow‐up. Data from the two‐month follow‐up were used.
Overall premenstrual symptoms
Daily symptom rating charts were used in three studies (Shin 2009, Yu 2006; Zhang 2017). The Premenstrual Daily Symptom Diary (PTSD), a four‐point scale from 'no symptom' to 'severe symptoms' on 19 items for 31 days was used in one trial (Yu 2006). It is unclear if this was a validated outcome measure. The sum of the symptoms score change between pretreatment and the third treatment month was used, 'mean rank' but not 'mean and standard deviation' was reported as the outcome, so the data were not included in the meta‐analysis (Yu 2006). The Menstrual Symptom Severity List, a five‐point scale rating symptoms from 'not present' to 'extreme' on 33 items (Mitchell 1992) was used in one trial (Shin 2009). The treatment effects were defined as the differences between the first pretreatment luteal phase (five days prior to menses) mean score and the first post‐treatment luteal phase (five days prior to menses) mean score, but only end scores were reported, so we used end scores as the outcome in this review (Shin 2009). One study (Bazarganipour 2017) used the Premenstrual Symptom Screening Tool (PSST) scores as their outcome (Steiner 2003). PSST has 19 questions in two parts, 14 questions related to mood, body, and behaviour and five questions based on the potential impact of these symptoms on an individual’s life. These data were presented as the number of women reporting no or mild PMS symptoms compared to those reporting moderate to severe at the end of the intervention. The number of women reporting moderate to severe PMS at the end of the review was presented in the analysis. One study (Zhang 2017), used a Daily Record of Severity of Problems scale (DRSP), a validated measure of PMS symptoms (Endicott 2006), and provided separate scores for mood and physical symptom components. These were reported separately in the meta‐analysis.
Adverse events
Adverse events were reported as an outcome in all acupuncture trials but not in the acupressure trial (Bazarganipour 2017). Specific adverse events reported included haematomas, pain at the site of needling and itching after needling.
Specific symptoms of PMS: psychological, physical and functional symptoms, irritability.
No studies reported on this outcome.
Response rate
Two trials reported effectiveness rate. Treatments were considered to be successful if there were no further symptoms of PMS, if acupuncture and medication treatment of PMS became unnecessary or if PMS symptoms did not occur for at least a year after the acupuncture therapy (Habek 2002). Acupuncture was considered to be effective if the improvement rate of the scores on PTSD was greater than or equal to 30% (Yu 2006).
Quality of life
Two trials reported quality of life (QoL) outcomes. One study (Bazarganipour 2017) used the SF12 and one study (Zhang 2017) used the WHO Quality of Life‐BREF scale (WHOQOL‐BREF). The SF‐12 is a 12‐item questionnaire used to assess generic health outcomes from the patient’s perspective (Ware 1996). It is based on a subset of questions from the larger SF‐36 and covers the same eight domains of health outcomes, including physical functioning (PF), role‐physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role‐emotional (RE), and mental health (MH). The WHOQOL‐BREF instrument comprises 26 items, which measure the following broad domains: physical health, psychological health, social relationships, and environment (Whoqol 1998).
Excluded studies
Twenty studies were excluded, see Characteristics of excluded studies;
Three studies were excluded because they were not randomised controlled trials (RCTs) (Li 2004; Li 2008; Wang 2003).
Four studies were excluded because they were quasi‐RCTs (Carvalho 2013; Hong 2002; Sun 2004; Jiang 2005).
Four studies were excluded because they used combined comprehensive treatment methods as control group (Xu 2006a, Xu 2006b, Xu 2011; Zhang 1994).
Two studies were excluded because they used two acupuncture methods as control group (Gu 2008; Zhao 2012).
Two studies were excluded because they used traditional Chinese medicine as control group (Hu 2010, Li 2014).
Five studies were excluded because they compared acupuncture with western medicine but that medicine was not mentioned in Types of interventions (Cao 2013; Chen 2011; Koleini 2017; Sun 2008; Zheng 2001).
Risk of bias in included studies
See Figure 2 and Figure 3. One study (Zhang 2017) was at a low risk of bias in all domains.
2.
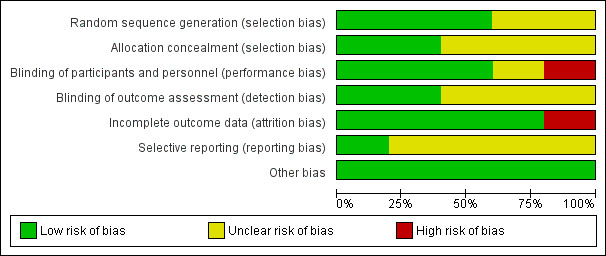
Risk of bias graph: review authors' judgments about each risk of bias item presented as percentages across all included studies.
3.
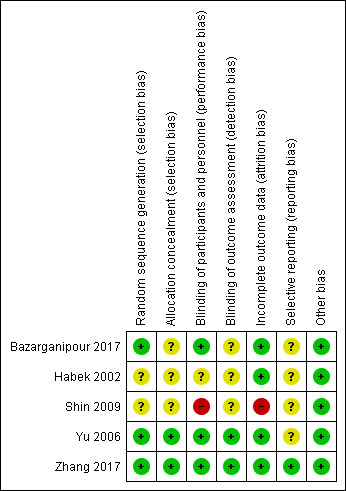
Risk of bias summary: review authors' judgments about each risk of bias item for each included study.
Allocation
Random sequence generation
The method of random sequence generation was associated with a low risk of bias in three trials (Bazarganipour 2017; Yu 2006; Zhang 2017). The two remaining trials were rated as unclear risk of bias as they did not report the methods of randomisation (Habek 2002; Shin 2009).
Allocation concealment
Two trials were rated as at low risk of bias related to allocation concealment (Yu 2006; Zhang 2017), while the other three were rated as unclear due to lack of clear reporting (Bazarganipour 2017; Habek 2002; Shin 2009).
Blinding
Sham‐acupuncture was used in three trials (Habek 2002; Yu 2006; Zhang 2017). Blinding of participants was not tested in one trial (Habek 2002) and was rated as unclear. Blinding remained intact for two trials (Yu 2006; Zhang 2017), which were rated as low risk of bias. Sham acupressure was used in one trial (Bazarganipour 2017), blinding was not tested but it is unlikely that due to the pressure used that blinding would have been unsuccessful and was rated as low risk of bias. One trial using a no treatment control did not attempt to blind (Shin 2009) and was rated as high risk of bias.
Detection bias was rated as low risk of bias in two trials (Yu 2006; Zhang 2017), where the clinicians assessing the outcomes were blinded to group allocation. Blinding was rated as unclear in the other three trials (Bazarganipour 2017; Habek 2002; Shin 2009), where the blinding status of the assessors and analysts was not reported.
Incomplete outcome data
Four trials had missing data for less than 20% of participants and were rated as at low risk of attrition bias (Bazarganipour 2017; Habek 2002; Yu 2006; Zhang 2017). One trial had data missing for over 20% of participants and was rated as at high risk of attrition bias (Shin 2009).
Selective reporting
Four trials were rated as at unclear risk of selective reporting as there was no published protocol (Bazarganipour 2017; Habek 2002; Shin 2009; Yu 2006). One trial (Zhang 2017) was rated as at low risk of bias: this was a PhD thesis and included a comprehensive protocol in the methods section.
Other potential sources of bias
No other potential source of bias was identified in any study, and all studies were rated as at low risk for this domain.
NICMAN scale scores
Three studies were analysed and NICMAN scale scores assessed (Bazarganipour 2017; Habek 2002; Shin 2009). It was not practical to perform this assessment on an entire Masters or PhD thesis so no score was generated for Yu 2006 or Zhang 2017. Scores (out of 23) ranged from 14 (Habek 2002), 16 (Bazarganipour 2017) to 19 (Shin 2009). Overall, the design of the study, including the population, intervention, comparison and outcomes was considered adequate in all three studies, however there was poor reporting on the rationale behind the acupuncture point selection and the qualifications of the therapist performing the acupuncture in both Bazarganipour 2017 and Shin 2009.
Effects of interventions
See: Table 1; Table 2; Table 3
Summary of findings for the main comparison. Acupuncture compared to sham for premenstrual syndrome.
| Acupuncture compared to sham acupuncture for premenstrual syndrome | ||||||
| Patient or population: women with PMS Setting: outpatient clinic or community Intervention: acupuncture Comparison: sham acupuncture | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with sham acupuncture | Risk with Acupuncture | |||||
| Overall premenstrual symptoms ‐ Mood at two month follow‐up. Assessed with: Daily Record of Severity of Problems (DRSP) scale. Scale range for DRSP (mood) 0‐60. Lower scores indicate less severe premenstrual symptoms |
The mean overall premenstrual symptoms‐ Mood was 51.91 | MD 9.03 lower (10.71 lower to 7.35 lower) | ‐ | 67 (1 RCT) | ⊕⊕⊝⊝ LOW 1 | Acupuncture may reduce the number of mood PMS related symptoms women have, compared to sham acupuncture. |
| Overall premenstrual symptoms ‐ Physical at two month follow‐up.Assessed with: DRSP. Scale range for DRSP (physical) 0‐66. Lower scores indicate less severe premenstrual symptoms | The mean overall premenstrual symptoms ‐ Physical was 46.11 | MD 9.11 lower (10.82 lower to 7.40 lower) | ‐ | 67 (1 RCT) | ⊕⊕⊝⊝ LOW 1 | Acupuncture may reduce the number of physical PMS related symptoms women have, compared to sham acupuncture. |
| Adverse events at up to 2 months' follow‐up | 24 per 1000 | 42 per 1000 (10 to 189) | RR 1.74 (0.39 to 7.76) | 167 (3 RCTs) | ⊕⊝⊝⊝ VERY LOW 2 3 | There was insufficient evidence to determine whether there was any difference between the groups in the rate of adverse events. |
| Specific PMS symptoms ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Response rate at end of treatment | 327 per 1000 | 1000 per 1000 (147 to 1000) | RR 4.22 (0.45 to 39.88) | 100 (2 RCTs) | ⊕⊝⊝⊝ VERY LOW 4 5 6 | There was insufficient evidence to determine whether there was any difference in response rate between the groups. |
| Quality of Life
assessed with: WHOQOL‐BREF. Scale range 0‐100. Higher scores indicate greater quality of life. |
The mean quality of life score was 73.8 | MD 2.85 higher (1.47 higher to 4.23 higher) | ‐ | 67 (1 RCT) | ⊕⊕⊝⊝ LOW 1 | Acupuncture may improve quality of life, compared to sham acupuncture. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; MD: mean difference; RCT: randomised controlled trial; RR: risk ratio | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded two levels due to very serious imprecision: small sample size (67 participants)
2 Downgraded one level due to serious risk of bias: unclear risk of blinding of both participants and assessors in one of the three trials. This may have affected adverse event reporting.
3 Downgraded two levels due to very serious imprecision: small sample size (167 participants) and rare events. 95% confidence interval covers both benefit and harm
4 Downgraded two levels due to very serious imprecision: small sample size (100 participants)
5 Downgraded one level due to serious risk of bias: unclear risk of blinding of both participants and assessors in one of the two included trials. This may be affected response rate.
6 Downgraded one level due to serious inconsistency: significant heterogeneity (I2 = 82%) due to different definitions of response rate.
Summary of findings 2. Acupuncture compared to no treatment for premenstrual syndrome.
| Acupuncture compared to no treatment for premenstrual syndrome | ||||||
| Patient or population: women with PMS Setting: community Intervention: acupuncture Comparison: no treatment | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with no treatment | Risk with Acupuncture | |||||
| Overall premenstrual symptoms at end of treatment. Assessed with the Menstrual Symptom Severity List (MSSL). Scale range 0‐33. Lower scores indicate less severe symptoms. |
The mean overall premenstrual symptom score was 17.54 | MD 13.60 lower (15.70 lower to 11.50 lower) | ‐ | 14 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 1 2 | Due to the very low quality of the evidence, we are uncertain whether acupuncture reduces PMS symptoms compared to a no treatment control |
| Adverse events at end of treatment | 0 per 1000 | 0 per 1000 (0 to 0) | not estimable | 20 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 1 3 | Neither group reported any adverse events |
| Specific PMS symptoms ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Response rate ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Quality of Life ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; MD: mean difference | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded one level due to serious risk of bias: unclear risk of bias in randomisation, high risk of bias in blinding of participants which is likely to affect patient reported outcome. High level of missing data.
2 Downgraded two levels due to very serious imprecision: very small sample size (14 participants)
3 Downgraded two levels due to very serious imprecision: very small sample size (14 participants) for rare events.
Summary of findings 3. Acupressure compared to sham acupressure for premenstrual syndrome.
| Acupressure compared to sham acupressure for premenstrual syndrome | ||||||
| Patient or population: women with PMS Setting: community Intervention: acupressure Comparison: sham acupressure | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Certainty of the evidence (GRADE) | Comments | |
| Risk with sham acupressure | Risk with Acupressure | |||||
| Overall premenstrual symptoms at end of treatment. Assessed with: number of women reporting moderate or severe PMS symptoms at the end of the intervention. Lower scores indicate more women with mild PMS or no PMS symptoms. | 97 per 100 | 62 per 100 (50 to 76) | RR 0.64 (0.52 to 0.79) | 90 (1 RCT) | ⊕⊕⊝⊝ LOW 1 | Acupressure may reduce the number of women with moderate to severe PMS symptoms at the end of the trial compared to sham acupressure |
| Adverse events ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Specific PMS symptoms ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Response rate ‐ not measured | ‐ | ‐ | ‐ | ‐ | ‐ | No studies reported on this outcome |
| Quality of Life ‐ Physical at end of treatment. Assessed with: SF‐12 Scale range 0‐100 Higher scores indicate greater quality of life |
The mean quality of Life ‐ Physical score was 67.2 | MD 24.30 higher (17.18 higher to 31.42 higher) | ‐ | 90 (1 RCT) | ⊕⊕⊝⊝ LOW 1 | Acupressure may improve physical quality of life compared to sham acupressure. |
| Quality of Life ‐ Mental at end of treatment. Assessed with: SF‐12 Scale range 0‐100 Higher scores indicate greater quality of life |
The mean quality of Life ‐ Mental score was 52.34 | MD 17.17 higher (13.08 higher to 21.26 higher) | ‐ | 90 (1 RCT) | ⊕⊕⊝⊝ LOW 1 | Acupressure may improve mental quality of life compared to sham acupressure. |
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; MD: mean difference | ||||||
| GRADE Working Group grades of evidence High certainty: We are very confident that the true effect lies close to that of the estimate of the effect Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded two levels due to very serious imprecision: small sample size (90 participants)
1 Acupuncture versus sham
One trial used 'mean rank' but not 'mean and standard deviation' as the outcome for 'Overall premenstrual symptoms', so was not included in this meta‐analysis (Yu 2006).
Primary outcomes
1.1 Overall premenstrual symptoms ‐ Mood
1.1. Analysis.
Comparison 1 Acupuncture vs sham acupuncture, Outcome 1 Overall premenstrual symptoms‐ Mood.
One trial (Zhang 2017) reported on this outcome.
Acupuncture may provide a greater reduction in mood‐related premenstrual syndrome (PMS) symptoms than sham acupuncture (mean difference (MD) ‐9.03, 95% confidence interval (CI) ‐10.71 to ‐7.35, one RCT, n = 67, low‐quality evidence), as measured by the Daily Record of Severity of Problems scale (DRSP). The evidence suggests that if women have a mood score of 51.91 points with sham acupuncture, their score with acupuncture would be between 10.71 and 7.35 points lower.
1.2 Overall premenstrual symptoms ‐ Physical
1.2. Analysis.
Comparison 1 Acupuncture vs sham acupuncture, Outcome 2 Overall premenstrual symptoms ‐ Physical.
One trial (Zhang 2017) reported on this outcome. Acupuncture may provide a greater reduction in physical PMS symptoms than sham acupuncture (MD ‐9.11, 95% CI ‐10.82 to ‐7.40, one RCT, n = 67, low‐quality evidence), as measured by the DRSP. The evidence suggests that if women have physical score of 46.11 points their score with acupuncture would be between 10.82 and 7.4 points lower.
1.3 Adverse events
1.3. Analysis.
Comparison 1 Acupuncture vs sham acupuncture, Outcome 3 Adverse events.
Three trials reported the safety of acupuncture in this comparison. Overall, there was insufficient evidence to determine if there was a difference in the adverse event rate between acupuncture and sham acupuncture (RR 1.74, 95% CI 0.39 to 7.76, three RCTs, n = 167, I2 = 0%, very low‐quality evidence)
Secondary outcomes
1.4 Response rate
1.4. Analysis.
Comparison 1 Acupuncture vs sham acupuncture, Outcome 4 Response rate.
Two trials (Habek 2002; Yu 2006) reported response rate for acupuncture versus sham acupuncture
Individually, both studies found a benefit in the intervention group, and pooling of their data supported this finding (RR 2.59, 95% CI 1.71 to 3.92; participants = 100; studies = 2; I2 = 82%). However, due to the high heterogeneity we tested the effect of using a random‐effects model, which provided no clear evidence of benefit for acupuncture (RR 4.22, 95% CI 0.45 to 39.88, two RCTs, n = 100, I2 = 82%, very low‐quality evidence). The high heterogeneity is most likely due to very heterogenous definitions of what was defined as a 'response rate' between the two studies as well as clinical heterogeneity in the intervention delivered. We concluded that owing to the very low quality of the evidence, there may be little or no difference between the groups for this outcome.
1.5 Quality of life
1.5. Analysis.
Comparison 1 Acupuncture vs sham acupuncture, Outcome 5 Quality of Life.
One trial reported quality of life outcomes using the WHOQOL‐BREF (Zhang 2017). Acupuncture may improve quality of life compared to sham acupuncture, measured at the end of the intervention (MD 2.85, 95% CI 1.47 to 4.23, one RCT, n = 67, low‐quality evidence).
1.6 Specific symptoms of PMS
No study reported this outcome.
2 Acupuncture versus no treatment
Primary outcomes
2.1. Overall premenstrual symptoms
2.1. Analysis.
Comparison 2 Acupuncture vs no treatment, Outcome 1 Overall premenstrual symptoms.
One trial reported overall premenstrual symptoms using the Menstrual Symptom Severity List (MSSL), and reported end scores for this outcome (Shin 2009). Due to the very low quality of the evidence, we are uncertain whether acupuncture reduces PMS symptoms compared to a no treatment control (MD ‐13.60, 95% CI ‐15.70 to ‐11.50, one RCT, n = 14, very low‐quality evidence)
2.2. Adverse events
2.2. Analysis.
Comparison 2 Acupuncture vs no treatment, Outcome 2 Adverse events.
One trial reported the safety of acupuncture. There were no adverse events reported in either group (Shin 2009).
Secondary outcomes
2.3 Specific symptoms of PMS
No study reported this outcome.
2.4 Response rate
No study reported this outcome.
3 Acupressure versus sham acupressure
Primary outcomes
3.1 Overall premenstrual symptoms
3.1. Analysis.
Comparison 3 Acupressure vs sham acupressure, Outcome 1 Overall premenstrual symptoms.
One trial reported overall PMS (Bazarganipour 2017). There was evidence that acupressure may reduce the number of women with moderate to severe PMS symptoms at the end of the trial compared to sham acupressure (RR 0.64 95% CI 0.52 to 0.79, one RCT, n = 90, low‐quality evidence). The evidence suggests that if 97 women out of 100 in the sham acupressure group had moderate to severe PMS symptoms, the number of women in the acupressure group with moderate to severe symptoms would be 50 to 76 women.
3.2. Adverse events
No study reported this outcome.
Secondary outcomes
3.3 Specific symptoms of PMS
No study reported this outcome.
3.4 Response rate
No study reported this outcome.
3.5 Quality of life
3.2. Analysis.
Comparison 3 Acupressure vs sham acupressure, Outcome 2 Quality of Life.
One trial reported quality of life outcomes using the SF‐12 scale (Bazarganipour 2017). The mental and physical subscale components were reported separately. There was evidence that acupressure may improve both physical (MD 24.30, 95% CI 17.18 to 31.42, one RCT, n = 90, low‐quality evidence) and mental (MD 17.17, 95% CI 13.08 to 21.26, one RCT, n = 90, low‐quality evidence) quality of life, compared to sham acupressure.
Discussion
Summary of main results
Evidence from these five trials including 277 women found that both acupuncture and acupressure may reduce overall premenstrual syndrome (PMS) symptoms. Acupuncture may reduce the overall severity of PMS symptoms as well as the number of both mood‐related and physical PMS symptoms at the end of the intervention. There was insufficient evidence to determine whether there is a difference in rates of adverse events between acupuncture and sham acupuncture. For the single acupressure trial there was a reduction in the number of women suffering from moderate or severe PMS at the end of the intervention. There are a small number of trials included within each comparison, and this limits the power of the review to detect any meaningful differences between groups.Therefore, while there may be benefits for acupuncture and acupressure, these benefits should be interpreted with caution until larger studies are undertaken.
Overall completeness and applicability of evidence
There were a small number of trials included in this review, and the outcome measures for PMS symptoms were heterogenous, limiting the ability to make meaningful meta‐analysis. The completeness and applicability of the evidence is limited due to the small number of trials, with relatively small sample sizes. The reporting on specific safety outcomes was limited in some trials, either due to a lack of reporting or due to very small sample sizes making it hard to detect these relatively rare events. All trials compared acupuncture with either sham or with no‐treatment. No trial compared acupuncture or acupressure with the current International Society for Premenstrual Disorders (ISPMD) recommended treatments.
Trials varied significantly in the frequency and total number of treatments given as well as the acupuncture points chosen and the timing of the intervention relative to menses, which may reflect differences in 'best practice' between different countries. This difference in both 'dosage' and timing around menses can potentially affect the outcome in menstrual conditions (Armour 2016), however due to the small number of trials a subgroup analysis on this factor could not be undertaken.
Quality of the evidence
The 'Risk of bias' tables (Figure 2; Figure 3) show that acupuncture and acupressure studies on PMS have not generally been undertaken to a high methodological standard. Only one trial was at a low risk of bias across all domains. The majority of studies had low risk of bias in randomisation and unclear risk of bias in allocation concealment, blinding of outcome assessors and selective reporting. In cases where it was unclear, we contacted the authors to provide additional details, however there was no response.
None of the trials' acupuncture interventions were rated highly on the National Institute for Complementary Medicine Acupuncture Network (NICMAN) scale, with issues in reporting the rationale for point selection being common. Acupuncture point selection, based on either biomedical or traditional understanding, depending on the framework chosen, should be used to guide point selection for trials, and without a clear rationale for point choice it is difficult to determine if studies are using treatments that reflect clinical practice.
Blinding of participants was at low risk of bias in three studies, however none of these reported assessments of blinding success between groups. The lack of blinding of outcome assessors, or in the case of participant‐reported outcomes, of participants themselves, may influence outcomes, and therefore, were rated as high risk of bias. Due to the small number of studies in each comparison means that while individual studies have had positive results, there is currently insufficient evidence for a consistent treatment effect.
The GRADE quality of evidence was often downgraded due to imprecision, mostly related to small sample sizes, and risk of bias particularly related to participant blinding. The overall quality of evidence for GRADE was moderate to very low for PMS symptoms and very low for adverse events (Table 1; Table 2; Table 3).
Potential biases in the review process
We attempted to minimise bias during the review process. Two review authors assessed the eligibility of studies, carried out data extraction and assessed the risk of bias. We are aware that some literature on acupuncture and acupressure may not be published in mainstream journals and therefore maybe excluded from the main databases. Our search was comprehensive and we included studies identified in languages other than English, however we did not systematically search all other language databases, for example Korean language only databases, therefore we cannot rule out the possibility that some studies may have been missed.
Agreements and disagreements with other studies or reviews
There has been only one systematic review on this topic performed in the past five years (Jang 2014). That review included eight acupuncture studies and included four trials that did not meet the inclusion criteria for this review due to the choice of control interventions (Gu 2008; Hong 2002; Xu 2006a; Xu 2006b). Overall, the authors found that physical symptoms such as breast tenderness improved while psychological symptoms did not. Our review included several more recent trials that were not included in Jang 2014 and found benefits for acupuncture for both physical and psychological symptoms.
Authors' conclusions
Implications for practice.
The limited evidence available suggests that acupuncture and acupressure may improve both physical and psychological symptoms of premenstrual syndrome (PMS) when compared to a sham control. There was insufficient evidence to determine whether there was a difference between the groups in rates of adverse events.There is no evidence comparing acupuncture or acupressure versus current International Society for Premenstrual Disorders (ISPMD) recommended treatments for PMS, such as selective serotonin reuptake inhibitors (SSRIs). Further research is required, using validated outcome measures for PMS, adequate blinding and suitable comparator groups reflecting current best practice.
Implications for research.
Very few studies included validated outcome measures for PMS and none compared acupuncture or acupressure with a currently accepted pharmaceutical or psychological intervention for PMS. We suggest future research include three‐armed trials comparing acupuncture or acupressure with a suitable sham and with an active pharmaceutical or psychological intervention suggested by current clinical guidelines. Given the issues with blinding a three‐armed trial, having blinded clinician‐rated scales as well as subjective patient‐centred outcomes should be considered. There is a need to improve the quality and reporting in future trials, especially with regards to the choice of acupuncture point selection and the rationale behind the choice of point(s) should be clear. Future trials need to improve reporting on the qualifications and experience of the practitioner delivering the acupuncture or acupressure intervention, including years of training, qualification and current registration status.
What's new
| Date | Event | Description |
|---|---|---|
| 23 August 2018 | Amended | Abstract text corrected. |
History
Protocol first published: Issue 2, 2005 Review first published: Issue 8, 2018
| Date | Event | Description |
|---|---|---|
| 28 January 2015 | Amended | Converted to new review format. |
Acknowledgements
We are grateful to the editorial board of Cochrane Menstrual Disorders and Subfertility Group (now called Cochrane Gynaecology and Fertility) for their methodological and language support and assistance with searching the literature. In particular, we are grateful to Professor Wu Taixiang from Chinese Cochrane Center in West China Hospital, Sichuan University for his professional tuition and instruction all through the procedure of the protocol and the early draft of this review.
The authors of this 2018 review acknowledge the contributions of Jinna Yu, Zhishun Liu, Baoyan Liu, Taixiang Wu, XiaoKe Wu and Vivian Welch to previous unpublished versions of this review.
Appendices
Appendix 1. Cochrane Gynaecology and Fertlity specialised register search strategy
Procite platform
Searched 21 September 2017
Keywords CONTAINS "premenstrual " or "premenstrual dysphoria" or "premenstrual aggravation" or "premenstrual dysphoric disorder" or "premenstrual pain " or "premenstrual symptoms" or "Premenstrual Syndrome‐Symptoms" or "PMS" or "dysphoria" or "PMDD" or Title CONTAINS "premenstrual " or "premenstrual dysphoria" or "premenstrual aggravation" or "premenstrual dysphoric disorder" or "premenstrual pain " or "premenstrual symptoms" or "Premenstrual Syndrome‐Symptoms" or "PMS" or "dysphoria" or "PMDD"
AND
Keywords CONTAINS "acupoint" or "acupressure" or "acupressure‐acupuncture therapy" or "acupuncture" or "electro‐acupuncture" or "electro‐magnetic" or "electroacupuncture" or "electrical stimulation" or "moxibustion" or "*acupuncture" or "auricular acupressure" or "auricular pressure" or "needle insertion" or Title CONTAINS "acupoint" or "acupressure" or "acupressure‐acupuncture therapy" or "acupuncture" or "electro‐acupuncture" or "electro‐magnetic" or "electroacupuncture" or "electrical stimulation" or "moxibustion"or "*acupuncture" or "auricular acupressure" or "auricular pressure" or "needle insertion" (10 hits)
Appendix 2. CENTRAL Register of Studies Online (CRSO) search strategy
Web platform Searched 21 September 2017
#1 MESH DESCRIPTOR Premenstrual Syndrome EXPLODE ALL TREES 385
#2 (Premenstrua* adj5 Syndrome*):TI,AB,KY 655
#3 dysphor*:TI,AB,KY 781
#4 (PMS or PMT):TI,AB,KY 558
#5 (premenstrua* adj5 tension):TI,AB,KY 75
#6 premenstrual:TI,AB,KY 845
#7 (late luteal phase adj5 disorder*):TI,AB,KY 23
#8 PMD:TI,AB,KY 75
#9 #1 OR #2 OR #3 OR #4 OR #5 OR #6 OR #7 OR #8 1828
#10 MESH DESCRIPTOR Acupuncture Therapy EXPLODE ALL TREES 3646
#11 acupuncture:TI,AB,KY 8917
#12 acupressure:TI,AB,KY 628
#13 (Electroacupunctur* or electro‐acupunctur*):TI,AB,KY 1426
#14 acupoint*:TI,AB,KY 2025
#15 meridian*:TI,AB,KY 603
#16 (non‐meridian* or trigger*):TI,AB,KY 4884
#17 (moxibustion or moxa*):TI,AB,KY 1088
#18 #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 15644
#19 #9 AND #18 42
Appendix 3. MEDLINE search strategy
Ovid platform Searched from 1946 to 21 September 2017 1 exp Premenstrual Syndrome/ (3983) 2 (Premenstrua$ adj5 Syndrome$).tw. (2446) 3 dysphor$.tw. (4926) 4 pms.tw. (4737) 5 pmt.tw. (1661) 6 (premenstrua$ adj5 tension$).tw. (503) 7 premenstrual.tw. (4795) 8 (late luteal phase adj5 disorder).tw. (85) 9 llpd$.tw. (38) 10 pmd$.tw. (4411) 11 or/1‐10 (18786) 12 exp Acupuncture/ (1506) 13 exp acupuncture therapy/ or exp acupressure/ or exp acupuncture analgesia/ or exp acupuncture, ear/ or exp electroacupuncture/ or exp meridians/ or exp moxibustion/ (21564) 14 acupuncture.tw. (18640) 15 acupressure.tw. (880) 16 exp Electroacupuncture/ (3258) 17 (Electroacupunctur$ or electro‐acupunctur$).tw. (4176) 18 acupoint$.tw. (4083) 19 meridian$.tw. (4819) 20 ((meridian or non‐meridian or trigger) adj10 point$).tw. (2478) 21 exp Moxibustion/ (1542) 22 (moxibustion or moxabustion or moxa$).tw. (3206) 23 or/12‐22 (33736) 24 11 and 23 (60) 25 randomized controlled trial.pt. (481966) 26 controlled clinical trial.pt. (96881) 27 randomized.ab. (422264) 28 randomised.ab. (82875) 29 placebo.tw. (201990) 30 clinical trials as topic.sh. (190475) 31 randomly.ab. (292311) 32 trial.ti. (190079) 33 (crossover or cross‐over or cross over).tw. (78725) 34 or/25‐33 (1236937) 35 exp animals/ not humans.sh. (4585712) 36 34 not 35 (1140717) 37 24 and 36 (29)
Appendix 4. Embase search strategy
Ovid platform Searched from 1980 to 21 September 2017 1 exp premenstrual dysphoric disorder/ or exp premenstrual syndrome/ (6019) 2 (Premenstrua$ adj5 Syndrome$).tw. (2862) 3 dysphor$.tw. (6118) 4 (pms or pmt).tw. (7991) 5 (premenstrua$ adj5 tension$).tw. (356) 6 premenstrual.tw. (5287) 7 (late luteal phase adj5 disorder).tw. (103) 8 (llpd$ or pmd$).tw. (6147) 9 or/1‐8 (24195) 10 exp acupuncture analgesia/ or exp acupuncture/ or exp acupuncture needle/ (39566) 11 exp acupressure/ (1741) 12 (acupuncture or acupressure).tw. (26239) 13 exp electroacupuncture/ (5482) 14 (Electroacupunctur$ or electro‐acupunctur$).tw. (5132) 15 acupoint$.tw. (5137) 16 meridian$.tw. (5511) 17 ((meridian or non‐meridian or trigger) adj10 point$).tw. (3607) 18 exp moxibustion/ (2335) 19 or/10‐18 (48148) 20 9 and 19 (142) 21 Clinical Trial/ (947951) 22 Randomized Controlled Trial/ (469604) 23 exp randomization/ (75622) 24 Single Blind Procedure/ (29554) 25 Double Blind Procedure/ (140190) 26 Crossover Procedure/ (53240) 27 Placebo/ (299862) 28 Randomi?ed controlled trial$.tw. (167370) 29 Rct.tw. (25692) 30 random allocation.tw. (1685) 31 randomly allocated.tw. (28302) 32 allocated randomly.tw. (2267) 33 (allocated adj2 random).tw. (784) 34 Single blind$.tw. (19787) 35 Double blind$.tw. (175378) 36 ((treble or triple) adj blind$).tw. (713) 37 placebo$.tw. (255724) 38 prospective study/ (402253) 39 or/21‐38 (1804452) 40 case study/ (49880) 41 case report.tw. (338520) 42 abstract report/ or letter/ (1010607) 43 or/40‐42 (1390853) 44 39 not 43 (1758453) 45 20 and 44 (63)
Appendix 5. PsycINFO search strategy
Ovid platform Searched from 1806 to 21 September 2017
1 exp Premenstrual Dysphoric Disorder/ (429) 2 exp Premenstrual Syndrome/ (1475) 3 (Premenstrua$ adj5 Syndrome$).tw. (1189) 4 dysphor$.tw. (5709) 5 (pms or pmt).tw. (1684) 6 (premenstrua$ adj5 tension$).tw. (172) 7 premenstrual.tw. (2479) 8 (late luteal phase adj5 disorder).tw. (112) 9 (llpd$ or pmd$).tw. (1045) 10 or/1‐9 (8817) 11 exp Acupuncture/ (1313) 12 exp Acupuncture/ (1313) 13 (acupuncture or acupressure).tw. (1882) 14 exp Electrical Stimulation/ (19571) 15 (Electroacupunctur$ or electro‐acupunctur$).tw. (308) 16 acupoint$.tw. (241) 17 meridian$.tw. (781) 18 ((meridian or non‐meridian or trigger) adj10 point$).tw. (408) 19 or/11‐18 (22509) 20 10 and 19 (40) 21 random.tw. (50922) 22 control.tw. (393763) 23 double‐blind.tw. (20962) 24 clinical trials/ (10575) 25 placebo/ (4969) 26 exp Treatment/ (694599) 27 or/21‐26 (1077010) 28 20 and 27 (35)
Appendix 6. AMED search strategy
Ovid platform Searched from 1985 to 21 September 2017 1 exp Premenstrual syndrome/ (107) 2 (Premenstrua$ adj5 Syndrome$).tw. (165) 3 dysphor$.tw. (39) 4 (pms or pmt).tw. (94) 5 (premenstrua$ adj5 tension$).tw. (7) 6 premenstrual.tw. (171) 7 (late luteal phase adj5 disorder).tw. (0) 8 (llpd$ or pmd$).tw. (20) 9 or/1‐8 (273) 10 exp Acupuncture/ (3292) 11 exp Acupressure/ or exp Acupuncture therapy/ (7689) 12 (acupuncture or acupressure).tw. (9807) 13 exp Electroacupuncture/ (878) 14 (Electroacupunctur$ or electro‐acupunctur$).tw. (1070) 15 acupoint$.tw. (1983) 16 meridian$.tw. (671) 17 ((meridian or non‐meridian or trigger) adj10 point$).tw. (554) 18 exp Moxibustion/ (537) 19 or/10‐18 (11126) 20 9 and 19 (16)
Appendix 7. CINAHL search strategy
Ebsco platform Searched from 1961 to 21 September 2017
| # | Query | Results |
| S35 | S20 AND S34 | 19 |
| S34 | S21 OR S22 or S23 or S24 OR S25 OR S26 OR S27 OR S28 OR S29 OR S30 OR S31 OR S32 OR S33 | 1,160,698 |
| S33 | TX allocat* random* | 7,195 |
| S32 | (MH "Quantitative Studies") | 16,373 |
| S31 | (MH "Placebos") | 10,354 |
| S30 | TX placebo* | 47,288 |
| S29 | TX random* allocat* | 7,195 |
| S28 | (MH "Random Assignment") | 44,035 |
| S27 | TX randomi* control* trial* | 131,386 |
| S26 | TX ( (singl* n1 blind*) or (singl* n1 mask*) ) or TX ( (doubl* n1 blind*) or (doubl* n1 mask*) ) or TX ( (tripl* n1 blind*) or (tripl* n1 mask*) ) or TX ( (trebl* n1 blind*) or (trebl* n1 mask*) ) | 906,331 |
| S25 | TX ( (trebl* n1 blind*) or (trebl* n1 mask*) ) | 210 |
| S24 | TX ( (trebl* n1 blind*) or (trebl* n1 mask*) ) | 210 |
| S23 | TX clinic* n1 trial* | 211,140 |
| S22 | PT Clinical trial | 80,028 |
| S21 | (MH "Clinical Trials+") | 221,365 |
| S20 | S9 AND S19 | 51 |
| S19 | S10 OR S11 OR S12 OR S13 OR S14 OR S15 OR S16 OR S17 OR S18 | 18,602 |
| S18 | TX (moxibustion or moxabustion or moxa*) | 1,198 |
| S17 | (MM "Moxibustion") | 264 |
| S16 | TX meridian* | 2,334 |
| S15 | TX acupoint* | 983 |
| S14 | TX (Electroacupunctur* or electro‐acupunctur*) | 1,342 |
| S13 | TX Electroacupuncture | 1,296 |
| S12 | TX acupressure | 1,193 |
| S11 | TX acupuncture | 16,542 |
| S10 | (MH "Acupuncture+") OR (MM "Acupuncture, Ear") OR (MM "Acupuncture Points") OR (MM "Acupuncturists") OR (MM "Acupuncture Anesthesia") OR (MM "Acupuncture Analgesia") | 12,300 |
| S9 | S1 OR S2 OR S3 OR S4 OR S5 OR S6 OR S7 OR S8 | 3,658 |
| S8 | TX(late luteal phase N5 disorder) | 11 |
| S7 | TX premenstrual | 1,780 |
| S6 | TX (premenstrua* N5 tension*) | 46 |
| S5 | TX pmt | 229 |
| S4 | TX pms | 1,210 |
| S3 | TX dysphor* | 1,292 |
| S2 | TX(Premenstrua* N5 Syndrome*) | 1,444 |
| S1 | (MM "Premenstrual Syndrome+") OR (MM "Premenstrual Dysphoric Disorder+") | 1,074 |
Data and analyses
Comparison 1. Acupuncture vs sham acupuncture.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Overall premenstrual symptoms‐ Mood | 1 | 67 | Mean Difference (IV, Fixed, 95% CI) | ‐9.03 [‐10.71, ‐7.35] |
| 2 Overall premenstrual symptoms ‐ Physical | 1 | 67 | Mean Difference (IV, Fixed, 95% CI) | ‐9.11 [‐10.82, ‐7.40] |
| 3 Adverse events | 3 | 167 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.74 [0.39, 7.76] |
| 4 Response rate | 2 | 100 | Risk Ratio (M‐H, Random, 95% CI) | 4.22 [0.45, 39.88] |
| 5 Quality of Life | 1 | 67 | Mean Difference (IV, Fixed, 95% CI) | 2.85 [1.47, 4.23] |
Comparison 2. Acupuncture vs no treatment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Overall premenstrual symptoms | 1 | 14 | Mean Difference (IV, Fixed, 95% CI) | ‐13.6 [‐15.70, ‐11.50] |
| 2 Adverse events | 1 | 20 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 3. Acupressure vs sham acupressure.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Overall premenstrual symptoms | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.64 [0.52, 0.79] |
| 2 Quality of Life | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Bazarganipour 2017.
| Methods | Randomised, sham controlled, single‐blind, parallel three‐armed trial comparing acupressure vs sham acupressure. | |
| Participants | Country: Iraq Site: Hormozgan University Participants: 97 university students with PMS Inclusion criteria: age 18 to 45 years, menstruation between 21 and 35 days,has moderate to severe PMS as scored by the PSST. Exclusion criteria: infectious skin diseases, lesions or dermatitis at the acupressure point locations, NSAID or other analgesics three hours prior to the intervention, severe depression or anxiety (based on HADS score), auditory or visual impairments, major external factors causing tension in the last six months (such as surgery or death in the family), heart disease, renal disorder, diabetes, asthma, thyroid conditions, respiratory disorders or genital diseases. |
|
| Interventions | Participants received two training sessions by a researcher (FB) who had been trained in acupressure techniques from a TCM specialist for 20 sessions over four months. Training of the students took place in student accomodation, and consisted of PMS pathology, treatment methods, and introducing acupressure. No description of whether self‐acupressure was observed or checked after training, nor of compliance. In both groups, the first menstrual cycle was used as a baseline measure. Acupressure group 1 (n = 32) Acupuncture point LR3 was used in the second and third cycles. Participants were instructed to start applying pressure 14 days prior to the onset of menses. Acupressure group 2 (n = 32) Acupuncture point LI4 was used in the second and third cycles. Participants were instructed to start applying pressure 14 days prior to the onset of menses. Sham acupressure (n = 33) Sham point located at the dorsal surface of the foot between the third and the fourth toes which was not in the line of the Liver meridian. In all three groups, participants sat down for 10‐15 minutes to adapt to room temperature. All windows and doors were closed and nobody was allowed to enter the room. Participants are described as being supine but it is not clear at what point they lay down. During the second and third cycle the acupressure was performed daily, and consisted of two minutes of pressure on each acupoint, then two minutes of stimulation without pressure, until a light pain occurred in the acupoint, for 20 minutes in total. It is unclear if the participant or a researcher applied the pressure during the second and third cycles, with conflicting information in the abstract vs body text. No mention of whether acupressure was given bilaterally or unilaterally. Participants were telephoned daily, in the five days leading up to menstruation, as a reminder of the timing of interventions and outcome collection. In this review acupressure group 1 and group 2 were combined and compared to sham acupressure. |
|
| Outcomes | PSST questionnaire (rates PMS severity), SF12 HRQOL, Hospital Anxiety and Depression Scale (HADS) | |
| Notes | NICMAN score: 16 Funding: by a grant from Hormozgan University of Medical Science in Iran. Conflict of Interest: not reported Date study was conducted: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Participants were randomly divided into the study groups using a table of random numbers" (pg 67) |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Quote: “Participants were blinded to their allocation to the intervention groups.” (pg 67) |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Patient‐reported outcomes, therefore blinding of participants likely to ensure outcomes not affected. Unclear if statistician or analysts blinded, researcher teaching acupressure not blind to allocation, but this is unlikely to affect outcome |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 7 dropouts, similar drop‐out rates between groups |
| Selective reporting (reporting bias) | Unclear risk | Common outcomes reported, however no protocol published |
| Other bias | Low risk | Baseline characteristics balanced between groups |
Habek 2002.
| Methods | Randomised, sham‐controlled, parallel two‐arm trial | |
| Participants | Country: Croatia Site: no details Recruitment: 35 women with PMS Inclusion: no details Exclusion: no details | |
| Interventions | Screening: two cycles screening Intervention group: (n = 18), mean age = 30.6 ± 8.4 years. Traditional acupuncture plus auriculo‐acupuncture. Traditional acupuncture points: GV20 (Baihui), bilateral LI 4 (Hegu), bilateral LR3 (Taichong), CV3 (Zhongji), CV4 (Guanyuan), CV6 (Qihai), bilateral PC6 (Neiguan), bilateral GB34 (Yanglingquan), bilateral BL23 (Shenshu). Auriculo‐acupuncture points: TF4 (auricular Shenmen). Physician (OB/GYN) inserted thin solid sterilised stainless steel needles until the de qi effect was obtained. Control group: (n = 17), mean age = 29.8 ± 7.3 years. The 17 women were treated with sham‐superficial acupuncture without the de qi effect (inserting the same type of needles at points on the lateral thighs and arms that were not on the classically described meridians. Duration: 7 days (four sessions) Timing of administration: treatments were conducted during the luteal phase of the menstrual cycle, every second day (7 days) for a period of 30 minutes a day. Summary measures: 1. success rate; 2. safety. |
|
| Outcomes | 1. Success rate: treatments were considered to be successful if PMS did not occur any more, if AP and medication treatment of PMS became unnecessary or if PMS symptoms did not occur for a year after the AP therapy. 2. Safety: adverse events were recorded (haematoma) |
|
| Notes | NICMAN score: 14 Funding: not reported Conflict of Interest: not reported Date study was conducted: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "A randomized prospective, placebo‐controlled trial included 35 women with PMS" (pg 24). Randomisation method not reported |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No dropouts in either group |
| Selective reporting (reporting bias) | Unclear risk | No protocol published |
| Other bias | Low risk | None noted |
Shin 2009.
| Methods | Randomised, non‐blinded, parallel 2‐arms trial | |
| Participants | Country: Korea
Site: the laboratory of Ewha Woman's University College of Nursing
Recruitment: 185 women were recruited through a posted advertisement placed in a university hospital, of these 30 volunteers were enrolled and randomly divided into three groups (Hand Acupuncture Therapy, Hand Moxibustion Therapy, control group) of 10 each. There were respectively 7, 8, 7 volunteers in each group completed. Hand acupuncture group versus control group were included in this review. Inclusion: women aged 20 to 35 years meeting ICD‐10 criteria for PMS. Exclusion: 1. menstrual irregularity (fewer than 20 days or more than 36 days) in the previous 3 months; 2. pregnancy or breastfeeding; hysterectomy; 3. oral contraceptive use in the previous 3 months; antidepressant, benzodiazepine, or psychotropic drug use; 4. diagnosed with thyroid disorder; and a history of depression or anxiety disorder. |
|
| Interventions | Screening: three menstrual cycles were screened prior to intervention using the Menstrual Symptom Severity Scale and used as baseline data. Intervention group: hand acupuncture therapy: (n = 10) Treatments were applied to the basic female corresponding hyuls on the Im Ki Mek of both hands: A5, A6, A8, A12, A16, A18; Liver Ki Mek N18; and Spleen Ki Mek F6, Needles were inserted into either hand at an approximate penetration depth of less than 1 mm. After needle insertion, the women were instructed to keep their hands still for 15 minutes. Control group: no treatment control group. (n = 10) Women did not receive any treatment but were contacted at the time of follow‐up assessment. Duration: 10 sessions for 4 weeks Timing of administration: 10 times treatments in the 4‐week period, once every 3 days at Ewha University Medical Center. Summary measures: score change of severity of menstrual symptoms between the first pretreatment luteal phase (5 days prior to menses) and the first post‐treatment luteal phase (5 days prior to menses) |
|
| Outcomes | The Menstrual Symptom Severity developed by Mitchell, Woods, and Lentz (1992) | |
| Notes | NICMAN score: 19 Funding: not reported Conflict of Interest: not reported Date study was conducted: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: “ Women were randomly divided into three groups (i.e., HAT, HMT, control) of 10 each” (pg 175). Method of randomisation not reported. |
| Allocation concealment (selection bias) | Unclear risk | Not reported |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | No blinding possible due to no treatment control group. Likely to affect outcome. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not reported |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 14 women completed (7 in the HAT group, and 7 in the control group). During the intervention phase, 6 women withdrew for a variety of reasons (e.g., work schedule, personal plans, wedding, school, vacation, and so forth). |
| Selective reporting (reporting bias) | Unclear risk | No protocol published |
| Other bias | Low risk | None noted |
Yu 2006.
| Methods | Randomised, single‐blind, sham‐controlled, parallel two‐arm trial | |
| Participants | Country: China
Site: acupuncture clinic in a multi‐speciality TCM hospital
Recruitment: 73 women with PMS were recruited via advertisements and from referral from affiliated psychiatric and gynaecological clinics, of these 65 were randomised. 33 into intervention group (30 completed the trial), 32 into sham‐acupuncture group (30 completed the trial). Inclusion: 1.women aged 18 to 45 years with regular menstrual cycles meeting DSM‐IV criteria for PMS; 2. course of disease: 3 months to 15 years; 3. voluntarily signed the informed consent. Exclusion: 1. women with organic diseases, such as diabetes, anaemia, endometriosis, thyroid function low; 2. women with abnormal personality or chronic mental disorders, such as depression, anxiety, dysthymia, panic, etc.; 3. women in pregnancy, lactation, peri‐menopause or prepare for pregnancy; 4. women with alcoholism or drug abuse history in the last 6 to 12 months; 5. women with oral contraceptives or hormone treatment history in the last 3 months. |
|
| Interventions | Screening: three menstrual cycles used to screen for PMS symptoms before intervention Intervention group: acupuncture group (n = 33) Mean age = 32.17 ± 8.49 years. Traditional acupuncture: DU 20 (Baihui), EX‐HN3 (Yintang), EX‐HN 3 (Taiyang), bilateral SP 6 (Sanyinjiao), bilateral SP 10 (Xuehai). Additional points according to different symptoms: add bilateral LR3 (Taichong), CV17 (Danzhong), bilateral LR 14 (Qimen) in PMS women with emotional instability, irritability or breast pain; add bilateral EX‐CA1 (Zigong), CV4 (Guanyuan), bilateral SP9 (Yinlingquan) in PMS women with headache, limbs pain or abdominal pain; add bilateral ST36 (Zusanli), CV6 (Qihai) in PMS women with fatigue or sleepiness; Add bilateral PC6 (Neiguan), bilateral HT7 (Shenmen) in PMS women with insomnia or heart palpitations; add bilateral BL23 (Shenshu), GV4 (Mingmen), bilateral KI3 (Taixi) in PMS women with waist discomfort; different depth for different points; manual manipulation every 10 minutes, retention for 30 minutes. Disposable acupuncture needles (0.30 mm x 40 mm, 0.30 mm x 25 mm were used. Control group: sham‐acupuncture group (n = 32) Mean age = 31.07 ± 7.79 years. Sham acupuncture: superficial acupuncture at non‐acupuncture points 1 cm away from the above points at 0.2 to 0.3 cun depth, no manipulation. Duration: three cycles (9 sessions). Timing of administration: 3 treatments in the 7 days before menstruation for three menstrual cycles. Summary measures: 1. score change after 3 cycles; 2. change in days with discomfort after 3 cycles; 3. response rate; 4. safety. |
|
| Outcomes |
Effective: > or = 30%, ineffective:< 30%. |
|
| Notes | NICMAN score: not applicable Funding: not applicable (masters thesis) Conflict of Interest: not applicable (masters thesis) Date study was conducted: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Central randomisation, using a computer random number generator, details unknown to investigators |
| Allocation concealment (selection bias) | Low risk | Clinical study of telephone voice response system, details unknown to investigators |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants blinded |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Data management by the third party, details unknown to investigators |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 65 were randomised, 3/33 missing from intervention group (1 due to "lack of efficacy", 1 due to pregnancy, 1 due to "have no time"); 2/32 missing from control group (1 due to "move house away", 1 due to "lack of efficacy") |
| Selective reporting (reporting bias) | Unclear risk | No protocol published |
| Other bias | Low risk | None noted |
Zhang 2017.
| Methods | Randomised, sham controlled, parallel three‐arm trial comparing acupuncture + intradermal needling, vs non‐channel superficial acupuncture + intradermal needling vs sham acupuncture and sham intradermal needling. | |
| Participants | Country: China Site: participants were recruited from Hai Kou Hospital of Traditional Chinese Medicine and Hai Nan Provincial Hospital of Traditional Chinese Medicine in Hai Kou, China from January 2015 to June 2016. Participants: 105 women aged 18‐40 years, diagnosed with PMDD Inclusion criteria
Exclusion criteria
|
|
| Interventions | Experimental intervention: acupuncture (n = 35)
Duration: 30 minutes each intervention, three times interventions a week, interval between two interventions > 24 hours, four weeks as a course, two courses in total. Follow‐up at after 2 months. Stop intervention during the first, second and third days of menstruation. Intradermal needle therapy: embedding needles in the skin 3 mm to 5 mm at BL15 (Xinshu),BL18 (Ganshu) and BL23 (Shenshu) for 2‐3 days. Duration: interventions twice a week, interval between two interventions > 72 hours, four weeks as a course, two courses in total. Follow‐up after 2 months. Stop intervention during the first, second and third days of menstruation. Control/Comparison intervention 1. Non‐acupoint superficial + intradermal needle control group 1 (n = 35)
Duration: 30 minutes each intervention, three times interventions a week, interval between two interventions > 24 hours, four weeks as a course, two courses in total. Follow‐up at after 2 months. Stop intervention during the first, second and third days of menstruation. 2. Intradermal needle therapy: Embedding needles in the skin 3‐5 mm at BL15 (Xinshu),BL18 (Ganshu) and BL23 (Shenshu) for 2 to3 days. Duration: twice interventions a week, interval between two interventions > 72 hours, four weeks as a course, two courses in total. Follow at after 2 months. Stop intervention during the first, second and third days of menstruation. 2. Acupoint non‐invasive acupuncture + non‐invasive intradermal needle control group 2 (n = 35)
Duration: 30 minutes each intervention, three times interventions a week, interval between two interventions > 24 hours, four weeks as a course, two courses in total. Follow at after 2 months. Stop intervention during the first, second and third days of menstruation. 2. Non‐invasive sham intradermal needle at BL15 (Xinshu), BL18 (Ganshu) and BL23 (Shenshu) for 2‐3 days. Duration: interventions twice a week, interval between two interventions > 72 hours, four weeks as a course, two courses in total. Follow‐up after 2 months. Stop intervention during the first, second and third days of menstruation. In this review we included the comparison of acupuncture versus control group 2 (i.e. acupuncture versus acupoint non‐invasive acupuncture + non‐invasive intradermal needle) |
|
| Outcomes | Primary: Hamilton Anxiety Scale (HAMA) Secondary: WHO Quality of Life‐BREF scale (WHOQOL‐BREF), Daily Record of Severity of Problems scale (DRSP) Adverse events reported (haematoma, pain at needle site, and itching at needle site). Endpoints: after one and two courses of intervention and at one and two months follow‐up. |
|
| Notes | NICMAN score: Not applicable Funding: Not applicable (PhD Thesis) Conflict of interest: not applicable (PhD Thesis) Date study was conducted: January 2015 to June 2016 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: “A computerized PMS3.1 software was used to generate a random number and simple randomisation was used (p28)” |
| Allocation concealment (selection bias) | Low risk | Quote: “Make grouped allocation results into cards. Put them into sealed kraft paper envelopes then sequentially numbered them. (p28) |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Participants blinded to group allocation through the use of sham control group. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: “People who participate in random allocation do not participate in intervention and data statistics. This study was designed to blind the personnel who assess outcome and analyse data" (pg 28). |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropouts balanced and unrelated to intervention group |
| Selective reporting (reporting bias) | Low risk | All outcomes stated in the PhD thesis methods reported |
| Other bias | Low risk | No baseline imbalance or other evidence of bias |
AP: acupuncture point
DSM IV: Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition
RSP: Daily Record of Severity of Problems scale
HAT: hand acupuncture therapy
HMT: hand moxibustion therapy
ICD‐10: International Statistical Classification of Diseases and Related Health Problems 10th Revision
NICMAN: National Institute for Complementary Medicine Acupuncture Network
NSAID: non‐steroidal anti‐inflammatory drug
PMDD: premenstrual dysphoric disorder
PMS: premenstrual syndrome
PSST: Premenstrual Symptoms Screening Tool
SF12 HRQOL: Short Form 12 ‐ Health Related Quality of Life.
TCM: traditional Chinese medicine
WHO: World Health Organization
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Cao 2013 | Control treatment (Celebrex) did not met the inclusion criteria. |
| Carvalho 2013 | Quasi‐randomised (assigned alternately). |
| Chen 2011 | Control treatment (Celebrex) did not met the inclusion criteria. |
| Gu 2008 | Control treatment did not met the inclusion criteria (eight methods of intelligent turtle combined with point selection treatment based on syndrome differentiation versus point selection treatment based on syndrome differentiation) |
| Hong 2002 | Quasi‐randomised (by the visiting sequence). |
| Hu 2010 | Control treatment (Xiaoyao Pill) did not met the inclusion criteria. |
| Jiang 2005 | Quasi‐randomised (by the visiting sequence). |
| Koleini 2017 | Control treatment (vitamin B6) did not meet the inclusion criteria. |
| Li 2004 | Not randomised, no control group. |
| Li 2008 | Not randomised, no control group. |
| Li 2014 | Control treatment (Xiaoyao Pill) did not met the inclusion criteria. |
| Sun 2004 | Quasi‐randomised (by the visiting sequence). Control treatment was comprehensive treatment method (medroxyprogesterone acetate and diazepam). |
| Sun 2008 | Control treatment (ibuprofen) did not met the inclusion criteria. |
| Wang 2003 | Not randomised, no control group. |
| Xu 2006a | Control treatment was comprehensive treatment method (medroxyprogesterone acetate and diazepam). |
| Xu 2006b | Control treatment was comprehensive treatment method (medroxyprogesterone acetate and diazepam). |
| Xu 2011 | Control treatment was comprehensive treatment method (Vitamin B1 and Oryzanol and Xiaoyao Pills). |
| Zhang 1994 | Control treatment was comprehensive treatment method (Ciwujia Injection combined with diazepam and Xiaoyao Pills). |
| Zhao 2012 | Control treatment did not met the inclusion criteria (fire‐needles versus ordinary needles). |
| Zheng 2001 | Control treatment (vitamin B6) did not meet inclusion criteria. |
Characteristics of studies awaiting assessment [ordered by study ID]
Kim 2005.
| Methods | Acupuncture vs placebo acupuncture |
| Participants | 20 participants with PMS screened by DRSP |
| Interventions | Experimental group received acupuncture at CV6 and SP6 plus other points based on diagnosis. Control group received acupuncture at SI5 and ST40. Up to 13 sessions over 8 weeks for both groups |
| Outcomes | Digital infrared thermal imaging (DITI), DRSP and progesterone levels. |
| Notes | Unable to contact author to determine randomisation status and group numbers. |
Kurebayashi 2013.
| Methods | A randomised clinical trial aimed at evaluating the auriculotherapy |
| Participants | 40 females aged 21 to 44 years |
| Interventions | Control group: no treatment Experimental group: Traditional Chinese medicine ear points: Kidney, Liver, Stomach, Brain Stem, Ovary and Uterus point with semi‐permanent needles once per week for 8 sessions. |
| Outcomes | Premenstrual syndrome symptoms |
| Notes | Completed July 2012. Contacted CI (Leonice Fumiko Sato Kurebayashi) in May 2018 regarding data and publications. No response |
DRSP: Daily Record of Severity of Problems scale
Characteristics of ongoing studies [ordered by study ID]
NCT02504515.
| Trial name or title | Effect of homeopathy, acupuncture or anthroposophic medicine in women's quality of life |
| Methods | A randomised clinical trial aimed to evaluating the effect of homeopathy, acupuncture or anthroposophic medicine |
| Participants | 906 females aged 18 years and over |
| Interventions | Homeopathy Acupuncture Anthroposophic medicine No further details provided |
| Outcomes | World Health Organization Bref (WHOQOL‐BREF) questionnaire |
| Starting date | April 2015 |
| Contact information | Rubens Lene Carvalho Tavares, Professor, Federal University of Minas Gerais |
| Notes | Estimated completion date December 2017 |
Differences between protocol and review
The standard of 'assessment of quality of included studies' had changed, given in the new version of theCochrane Handbook of Systematic Reviews of Interventions 5.1.0.
The method of control group of included studies had changed. In the protocol, control intervention could be Chinese medicine, western medicine, sham acupuncture , no intervention, and any other interventions, but in this review, the control group method changed to sham acupuncture, blank control (no intervention) or western medicine such as SSRIs, oral contraceptives, gonadotropin‐releasing hormone agonists, danazol or estradiol which were mentioned by ISPMD. Because if the effect of one control intervention is uncertain, it is meaningless to compare another intervention with it.
Acupressure was added as an appropriate intervention for inclusion in this review and title changed to "Acupuncture and acupressure for premenstrual syndrome" to reflect this.
NICMAN scale scores were added to provide a measure of the quality of the acupuncture or acupressure intervention delivered.
Response rates were added as a secondary outcome measure as this allowed inclusion of data not reported in a standard validated scale.
Contributions of authors
Mike Armour: performed the screening of the searches, ran the additional Google Scholar and PubMed searches, rated studies using the NICMAN scale, entered the data, performed the meta‐analysis and interpretation, generated the GRADE tables, and took the lead in writing the review.
Carolyn Ee: performed the grey literature search, searched the trial registries, assisted MA with screening, performed data extraction, rated studies using the NICMAN scale and commented on each draft of the review.
Jie Hao: searched the Chinese literature, screened Chinese language studies, performed data extraction, rated studies using the NICMAN scale and commented on the final version of the review.
Tania Wilson: performed data extraction, rated studies using the NICMAN scale and commented on the final version of the review.
Sofia Yao: performed data extraction, rated studies using the NICMAN scale and commented on the final version of the review.
Caroline A Smith: performed data extraction, rated studies using the NICMAN scale and commented on the final version of the review.
Sources of support
Internal sources
-
Mike Armour, Australia.
National Institute of Complementary Medicine, Western Sydney University
-
Carolyn Ee, Australia.
National Institute of Complementary Medicine, Western Sydney University
-
Caroline Smith, Australia.
National Institute of Complementary Medicine, Western Sydney University
External sources
No sources of support supplied
Declarations of interest
MA: is an acupuncturist recently involved in clinical practice and until recently, the director of an acupuncture clinic. As a medical research institute, NICM receives research grants and donations from foundations, universities, government agencies and industry. Sponsors and donors provide untied and tied funding for work to advance the vision and mission of the Institute.
CE: is a practising acupuncturist and the director of an integrative health centre which provides acupuncture clinical services to the general public. As a medical research institute, NICM receives research grants and donations from foundations, universities, government agencies and industry. Sponsors and donors provide untied and tied funding for work to advance the vision and mission of the Institute.
CS: none known. As a medical research institute, NICM receives research grants and donations from foundations, universities, government agencies and industry. Sponsors and donors provide untied and tied funding for work to advance the vision and mission of the Institute.
JH: is a Chinese medicine practitioner and acupuncturist.
SY: none known
TW: holds dual registration as a psychologist and acupuncturist
Edited (no change to conclusions)
References
References to studies included in this review
Bazarganipour 2017 {published data only}
- Bazarganipour F, Taghavi SA, Allan H, Beheshti F, Khalili A, Miri F, et al. The effect of applying pressure to the LIV3 and LI4 on the symptoms of premenstrual syndrome: a randomized clinical trial. Complementary Therapies in Medicine 2017;31:65‐70. [PUBMED: 28434473] [DOI] [PubMed] [Google Scholar]
Habek 2002 {published data only}
- Habek D, Habek JC, Barbir A. Using acupuncture to treat premenstrual syndrome. Archives of Gynecology and Obstetrics 2002;267(1):23‐6. [DOI] [PubMed] [Google Scholar]
Shin 2009 {published data only}
- Shin KR, Ha JY, Park HJ. The effect of hand acupuncture therapy and hand moxibustion therapy on premenstrual syndrome among Korean women. Western Journal of Nursing Research 2009;31(2):171‐86. [DOI] [PubMed] [Google Scholar]
Yu 2006 {published data only}
- Yu J, Liu B, Liu Z. Clinical Observation Based on a Systematic Review of Efficacy and Safety of Acupuncture Treatment for Premenstrual Syndrome [master's thesis]. Beijing (China): China Academy of Chinese Medical Science, 2006:1‐89. [Google Scholar]
Zhang 2017 {published data only}
- Zhang GC. Clinical study on the treatment of acupuncture for premenstrual syndrome. Clinical Study on the Treatment of Acupuncture for Premenstrual Syndrome (PhD Thesis). Guang Zhou (China): Guang Zhou University of Chinese Medicine, 2017. [Google Scholar]
References to studies excluded from this review
Cao 2013 {published data only}
- Cao L, Hou GY. Treatment of headache during menstruation with electroacupuncture and triple puncture. Journal of Clinical Acupuncture and Moxibustion 2013;29(4):21‐3. [Google Scholar]
Carvalho 2013 {published data only}
- Carvalho F, Weires K, Ebling M, Padilha Mde S, Ferrao YA, Vercelino R. Effects of acupuncture on the symptoms of anxiety and depression caused by premenstrual dysphoric disorder. Acupuncture in Medicine 2013;31(4):358‐63. [DOI] [PubMed] [Google Scholar]
Chen 2011 {published data only}
- Chen L, Zhu W, Lin Y, Huang JP, Lin F, Yuan LP, et al. Clinical study of balance acupuncture and moxibustion for treatment of women with premenstrual headache. Journal of Guangzhou University of Traditional Chinese Medicine 2011;28(4):379‐81. [Google Scholar]
Gu 2008 {published data only}
- Gu AH. Observation on eight methods of intelligent turtle combined with point selection treatment based on syndrome differentiation for 30 cases with premenstrual tension syndrome. Huna Journal of Traditional Chinese Medicine 2008;24(5):30‐1. [Google Scholar]
Hong 2002 {published data only}
- Hong YF. Clinical therapeutic effect of scalp acupuncture on premenstrual tension syndrome. Chinese Acupuncture & Moxibustion 2002;22(9):597‐8. [Google Scholar]
- Hong YF. The effect of scalp acupuncture treatment for premenstrual syndrome. Shanghai Journal of Acupuncture and Moxibustion 2002;21(3):24. [Google Scholar]
Hu 2010 {published data only}
- Fang YQ, Wu J, Hu YP, Zhou R, Yang LJ, Shi Y, et al. Observation on the tranquilizing and liver‐regulating acupuncture treatment for 47 PMS with liverqi stagnation type ‐ randomised controlled study. Guangming Journal of Chinese Medicine 2008;23(9):1308‐10. [Google Scholar]
- Hu YP, Zhou R. Observation on the tranquilizing and liver‐regulating acupuncture treatment for PMS with liver qi stagnation type. Journal of Shanxi of Traditional Chinese Medicine 2010;31(8):1047‐50. [Google Scholar]
- Wang J, Wu J. Observation on the tranquilizing and liver‐regulating acupuncture treatment for PMS with liverqi stagnation type. Journal of Sichuan of Traditional Chinese Medicine 2007;25(9):82‐3. [Google Scholar]
Jiang 2005 {published data only}
- Jiang W, Li Y, Sun J. Clinical study on treatment of premenstrual tension syndrome with auricular point sticking. Chinese Acupuncture & Moxibustion 2002;22(3):165‐7. [Google Scholar]
- Jiang W, Shan QH. Clinical study on treatment of premenstrual tension syndrome with auricular pressure pellets. International Journal of Clinical Acupuncture 2005;14(1):27‐33. [Google Scholar]
Koleini 2017 {published data only}
- Koleini S, Valiani M. Comparing the effect of auriculotherapy and vitamin B6 on the symptoms of premenstrual syndrome among the students who lived in the dorm of Isfahan University of Medical Sciences. Iranian Journal of Nursing and Midwifery Research 2017;22(5):354‐8. [PUBMED: 29033988] [DOI] [PMC free article] [PubMed] [Google Scholar]
Li 2004 {published data only}
- Li YM, Yu L, Gong DF. Observation on treatment of 46 premenstrual tension syndrome cases with auricular point sticking. Journal of Clinical Acupuncture and Moxibustion 2004;20(12):45. [Google Scholar]
Li 2008 {published data only}
- Li C. Acupuncture for 20 cases with premenstrual headache. Journal of Practical Traditional Chinese Medicine 2008;24(9):591. [Google Scholar]
Li 2014 {published data only}
- Li L, Li JF, Chen WF, Wu YX, Huang H, Lin QM. Effect of auricular point sticking on menstrual distending pains of breasts. Modern Clinical Nursing 2014;13(2):40‐2. [Google Scholar]
Sun 2004 {published data only}
- Guo SY, Sun YZ. Clinical Study on the Treatment of Premenstrual Syndrome by the Back‐shu and Front‐mu and Network Points Acupuncture [Master's thesis]. Harbin (China): Heilongjiang University of Chinese Medicine, 2004. [Google Scholar]
- Guo SY, Sun YZ. Comparison between acupuncture and medication in treatment of premenstrual syndrome. Shanghai Journal of Acupuncture and Moxibustion 2004;23(1):5‐6. [Google Scholar]
- Sun YZ, Guo SY. Comparison of therapeutic effects of acupuncture and medicine on premenstrual syndrome. Chinese Acupuncture & Moxibustion 2004;24(1):29‐30. [Google Scholar]
Sun 2008 {published data only}
- Sun ZH. Acupuncture for 42 premenstrual headache. Jiangxi Journal of Traditional Chinese Medicine 2008;5:50. [Google Scholar]
Wang 2003 {published data only}
- Wang QQ, Chen HL. Ear electro‐acupuncture for treatment of premenstrual syndrome in 49 cases. Journal of Sichuan of Traditional Chinese Medicine 2003;21(10):81‐2. [Google Scholar]
Xu 2006a {published data only}
- Xu YY. Clinical Study on the Treatment of Acupuncture of Back‐shu on Premenstrual Syndrome [Master's thesis]. Harbin: Hei Long Jiang University of Chinese Medicine, 2006. [Google Scholar]
Xu 2006b {published data only}
- Xu YY, Sun YZ. Observation on the waist penetration needling therapy for premenstrual syndrome. JCAM 2006;22(5):37‐8. [Google Scholar]
Xu 2011 {published data only}
- Xu SL. Clinical study on treatment of premenstrual syndrome by acupuncture and moxibustion. Journal of Acupuncture and Tuina Science 2011;9(5):310‐1. [Google Scholar]
Zhang 1994 {published data only}
- Zhang WF, Bei YL, Zhang WZ. The effect of acupuncture in the treatment of 60 cases with premenstrual tension syndrome. Chinese Acupuncture and Moxibustion 1994;Supplement:100‐1. [Google Scholar]
Zhao 2012 {published data only}
- Li Z. Clinical observation on fire needle for menstrual headache due to phlegm stagnation in collaterals. Shanghai Journal of Acupuncture and Moxibustion 2012;31(3):145‐6. [Google Scholar]
Zheng 2001 {published data only}
- Zheng JY, Zheng JZ. The efficacy of acupuncture in the treatment of headache during menstruation: a report of 60 cases. Hebei Journal of Traditional Chinese Medicine 2001;23(8):612‐3. [Google Scholar]
References to studies awaiting assessment
Kim 2005 {published data only}
- Kim SC, Kim SN, Lim JA, Choi CM, Shim EK, Koo ST, et al. Effects of acupuncture treatment on the premenstrual syndrome: controlled clinical trial. Journal of Korean Acupuncture and Moxibustion Society 2005;22:41‐60. [Google Scholar]
Kurebayashi 2013 {published data only}
- Kurebayashi L. Auriculotherapy in the cares to the premenstrual syndrome. https://clinicaltrials.gov/ct2/show/NCT01782040.
References to ongoing studies
NCT02504515 {published data only}
- Effect of homeopathy, acupuncture or anthroposophic medicine in women's quality of life. Ongoing study April 2015.
Additional references
ACOG 2001
- ACOG. ACOG Practice Bulletin: premenstrual syndrome. International Journal of Gynecology & Obstetrics 2001;73:183‐91. [Google Scholar]
APA 2013
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders‐DSM‐V. American Psychiatric Association. Washington DC: American Psychiatric Association, 2013. [Google Scholar]
Armour 2016
- Armour M, Smith CA. Treating primary dysmenorrhoea with acupuncture: a narrative review of the relationship between acupuncture 'dose' and menstrual pain outcomes. Acupuncture in Medicine : journal of the British Medical Acupuncture Society 2016;34(6):416‐24. [PUBMED: 27913451] [DOI] [PubMed] [Google Scholar]
Backstorm 1991
- Backstrom T, Hammarback S. Premenstrual syndrome‐psychiatric or gynaecological disorder. Annals of Medicine 1991;23(6):625‐33. [DOI] [PubMed] [Google Scholar]
Bancroft 1993
- Bancroft J. The premenstrual syndrome ‐a reappraisal of the concept and the evidence. Psychological Medicine 1993;Supplement 24:1‐47. [DOI] [PubMed] [Google Scholar]
Beal 1999
- Beal MW. Acupuncture and acupressure: applications to women’s reproductive health care. Journal of Nurse‐Midwifery 1999;44(3):217‐30. [DOI] [PubMed] [Google Scholar]
Bertone‐Johnson 2014
- Bertone‐Johnson ER, Ronnenberg AG, Houghton SC, Nobles C, Zagarins SE, Takashima‐Uebelhoer BB, et al. Association of inflammation markers with menstrual symptom severity and premenstrual syndrome in young women. Human Reproduction (Oxford, England) 2014;29(9):1987‐94. [PUBMED: 25035435] [DOI] [PubMed] [Google Scholar]
Dickerson 2004
- Dickerson LM, Mazyck PJ, Hunter MH. Premenstrual syndrome. American Family Physician 2004;57(8):1743‐52. [PubMed] [Google Scholar]
Egger 1997
- Egger Matthias, Smith George Davey, Schneider Martin, Minder Christoph. Bias in meta‐analysis detected by a simple, graphical test. BMJ 1997;315(7109):629. [DOI] [PMC free article] [PubMed] [Google Scholar]
Endicott 2006
- Endicott J, Nee J, Harrison W. Daily Record of Severity of Problems (DRSP): reliability and validity. Archives of Women's Mental Health 2006;9(1):41‐9. [PUBMED: 16172836] [DOI] [PubMed] [Google Scholar]
Gold 2016
- Gold EB, Wells C, Rasor MO. The association of inflammation with premenstrual symptoms. Journal of Women's Health 2016;25(9):865‐74. [PUBMED: 27135720] [DOI] [PMC free article] [PubMed] [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- GRADE Working Group, McMaster University. GRADEpro GDT. Version accessed on 4th Febuary 2018. Hamilton (ON): GRADE Working Group, McMaster University, 2015.
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration Available from www.cochrane‐handbook.org.
Hylan 1999
- Hylan TR, Sundell K, Judge R. The impact of premenstrual symptomatology on functioning and treatment‐seeking behavior: experience from the United States, United Kingdom, and France. Journal of Womens Health & Gender‐Based Medicine 1999;8(8):1043‐52. [DOI] [PubMed] [Google Scholar]
Ismaili 2016
- Ismaili E, Walsh S, O'Brien PMS, Backstrom T, Brown C, Dennerstein L, et al. Fourth consensus of the International Society for Premenstrual Disorders (ISPMD): auditable standards for diagnosis and management of premenstrual disorder. Archives of Women's Mental Health 2016;19(6):953‐8. [PUBMED: 27378473] [DOI] [PubMed] [Google Scholar]
Jang 2014
- Jang SH, Kim DI, Choi MS. Effects and treatment methods of acupuncture and herbal medicine for premenstrual syndrome/premenstrual dysphoric disorder: systematic review. BMC Complementary and Alternative Medicine 2014;14:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kimberly 2008
- Yonkers KA, O’Brien PMS, Eriksson E. Premenstrual syndrome. Lancet 2008;371(9619):1200‐10. [DOI] [PMC free article] [PubMed] [Google Scholar]
Langevin 2011
- Langevin HM, Wayne PM, Macpherson H, Schnyer R, Milley RM, Napadow V, et al. Paradoxes in acupuncture research: strategies for moving forward. Evidence‐Based Complementary and Alternative Medicine. England, 2011; Vol. 2011:180805. [DOI] [PMC free article] [PubMed]
MacPherson 2010
- MacPherson H, Altman DG, Hammerschlag R, Li YP, WU TX, White A, et al. Revision of standards for reporting interventions in clinical trials of acupuncture. Chinese Journal of Integrative Medicine 2010;8(9):804‐18. [DOI] [PubMed] [Google Scholar]
Marjoribanks 2013
- Marjoribanks Jane, Brown Julie, O'Brien Patrick Michael Shaughn, Wyatt Katrina. Selective serotonin reuptake inhibitors for premenstrual syndrome. Cochrane Database of Systematic Reviews 2013;6. [DOI] [PMC free article] [PubMed] [Google Scholar]
Mayor 2013
- Mayor D. An exploratory review of the electroacupuncture literature: clinical applications and endorphin mechanisms. Acupuncture in Medicine: Journal of the British Medical Acupuncture Society 2013;31(4):409‐15. [PUBMED: 23917395] [DOI] [PubMed] [Google Scholar]
McDonald 2013
- McDonald JL, Cripps AW, Smith PK, Smith CA, Xue CC, Golianu B. The anti‐inflammatory effects of acupuncture and their relevance to allergic rhinitis: a narrative review and proposed model. Evidence‐based Complementary and Alternative Medicine: eCAM 2013;2013:591796. [PUBMED: 23476696] [DOI] [PMC free article] [PubMed] [Google Scholar]
McDonald 2015
- McDonald JL, Cripps AW, Smith PK. Mediators, receptors, and signalling pathways in the anti‐inflammatory and antihyperalgesic effects of acupuncture. Evidence‐based Complementary and Alternative Medicine: eCAM 2015;2015:975632. [PUBMED: 26339274] [DOI] [PMC free article] [PubMed] [Google Scholar]
Medem 2004
- Medem Inc and American Psychiatric Association. Premenstrual dysphoric disorder (PMDD). http://www.medem.com/medlb/article_detaillb.cfm?article_ID=ZZZF9KNGTRC&sub_cat=2003 accessed at 25 July, 2004.
Mitchell 1992
- Mitchell ES, Woods NF, Lentz MJ. Recognising PMS when you see it: criteria for PMS sample selection. In: Taylor DL, Woods NF editor(s). Menstruation, Health and Illness. New York (USA): Hemisphere, 1991:89‐102. [Google Scholar]
O'Brien 2011
- O'Brien PM, Backstrom T, Brown C, Dennerstein L, Endicott J, Epperson CN, et al. Towards a consensus on diagnostic criteria, measurement and trial design of the premenstrual disorders: the ISPMD Montreal consensus. Archives of Women's Mental Health 2011;2(14):13‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Reid 1986
- Reid RL. Premenstrual syndrome: a time for introspection. American Journal of Obstetrics & Gynecology 1986;155(5):921‐6. [DOI] [PubMed] [Google Scholar]
RevMan 2014 [Computer program]
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Smith 2017
- Smith CA, Zaslawski CJ, Cochrane S, Zhu X, Zheng Z, Loyeung B, et al. Reliability of the NICMAN Scale: an instrument to assess the quality of acupuncture administered in clinical trials. Evidence‐based Complementary and Alternative Medicine : eCAM 2017;2017:5694083. [PUBMED: 28690661] [DOI] [PMC free article] [PubMed] [Google Scholar]
Steiner 2003
- Steiner M, Macdougall M, Brown E. The premenstrual symptoms screening tool (PSST) for clinicians. Archives of Women's Mental Health 2003;6(3):203‐9. [PUBMED: 12920618] [DOI] [PubMed] [Google Scholar]
Ware 1996
- Ware J, Kosinski M, Keller SD. A 12‐Item Short‐Form Health Survey: construction of scales and preliminary tests of reliability and validity. Medical Care 1996;34(3):220‐33. [DOI] [PubMed] [Google Scholar]
White 2004
Whoqol 1998
- The Whoqol Group. Development of the World Health Organization WHO QoL_BREF quality of life assessment. Psychological Medicine 1998;28(3):551‐8. [DOI] [PubMed] [Google Scholar]
Witt 2009
- Witt CM, Pach D, Brinkhaus B, Wruck K, Tag B, Mank S, et al. Safety of acupuncture: results of a prospective observational study with 229,230 patients and introduction of a medical information and consent form. Forschende Komplementarmedizin (2006) 2009;16(2):91‐7. [PUBMED: 19420954] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Yu 2005
- Yu J, Liu B, Liu Z, Welch V, Wu T, Clarke J, Smith CA. Acupuncture for premenstrual syndrome. Cochrane Database of Systematic Reviews 2005, Issue 2. [DOI: 10.1002/14651858.CD005290] [DOI] [Google Scholar]