

Abstract
Clear cell odontogenic carcinoma (CCOC) is a rare, low-grade malignant epithelial neoplasm, occurring in the jawbones, mainly affecting the mandible of elderly patients. In addition to hyalinizing clear cell carcinoma of the salivary gland, it is one of the epithelial neoplasms known to harbor an EWSR1-ATF1 fusion. Therefore, a link between these tumors seems plausible. We describe six cases of CCOC showing EWSR1 rearrangements, with two cases being positive for the ATF1 partner gene using FISH analysis. In one case, an EWSR1-CREB1 fusion was identified using RT-PCR, which we report for the first time in this tumor type. The other three cases investigated by FISH were negative for ATF1, CREB1 and CREB3L2. In conclusion, our data show that EWSR1-CREB1 is an alternative fusion gene to EWSR1-ATF1 in CCOC.
Keywords: Clear cell odontogenic carcinoma, EWSR1-CREB1, EWSR1-ATF1, Gene fusion, RT-PCR, FISH
Introduction
Clear cell odontogenic carcinoma (CCOC) is a rare, usually low-grade malignant epithelial neoplasm, occurring in the jawbones, with predilection for the mandible. The age range of patients is broad, however, the tumor is most often diagnosed in the 6th decade [1].
Clinically, an expansion of the affected part of the jaw is often obvious and loosening of teeth may be concomitantly present. Recurrences and metastases (lymph nodes, lung) after resection with clear margins are rare [1].
Radiological findings are not distinct from other malignant odontogenic tumors, demonstrating an ill-defined radiolucency variably associated with dental root resorption [1].
Microscopically, three different patterns have been described: biphasic, monomorphic and ameloblastomatous. The biphasic pattern shows arrangements of clear cells in a linear architecture with peripheral palisading of hyperchromatic polygonal cells with eosinophilic cytoplasm; the ameloblastomatous pattern is composed of islands of clear cells with peripheral columnar cells and the monomorphic pattern is characterized by a hyalinized to fibrocellular stroma [1]. Co-occurrence of these patterns may be present.
Based on the morphological resemblance to clear cell carcinoma of the salivary gland, genetic similarities were assumed and subsequently confirmed by the presence of the EWSR1-ATF1 fusion gene [2].
In our index case, however, we found an EWSR1-CREB1 fusion using RT-PCR. Since this is an unreported finding for CCOC, we aimed to analyze a series of CCOC using RT-PCR and FISH.
Materials and Methods
The cases were collected from the authors’ (referral) files. Clinical details were obtained from the referring physicians. The study was conducted in accordance with the Code of Conduct of the Federation of Medical Scientific Societies in the Netherlands (http://www.federa.org).
In all cases, the tissue was fixed in 4% buffered formalin, routinely processed including decalcification if needed and embedded in paraffin; 2–4 µm thick sections were stained with hematoxylin and eosin.
Two cases (i.e. case 1 and 2) were collected from the authors’ laboratory file, four cases (i.e. case 3–6) were collected from referral files.
Immunohistochemistry was performed for diagnostic purposes using standard protocols with an indirect biotin-free system based on polymer (Ultraview universal DAB kit, Ventana Medical Systems Inc.). Used primary antibodies are EMA (clone E29, 1:250, Dako, Agilent, Santa Clara, USA), Pan-cytokeratin MNF116 (1:500, DAKO, Glostrup, Denmark), Pan-cytokeratin clone AE1/3 (1:50, Cell Marque, Sanbio, Uden, The Netherlands), CK7 (clone OV-TL 12/30, 1:400, Immunologic, VWR International, Radnor, USA), CK14 (clone LL002, 1:200, Immunologic, VWR International, Radnor, USA), S-100 (polyclonal, 1:2500, Dako, Agilent, Santa Clara, USA) p63 (clone 4A4, 1:3000, Immunologic, VWR International, Radnor, USA), and p40 (clone BC28, 1:20, Biocare Medical, VWR International, Radnor, USA).
For case 1 and 2, antigen retrieval was performed using EDTA buffer, pH 9.0 for 10 min at 95 °C and 10 min blocking with 3% H2O2 in methanol. The primary antibodies were added for 1 h at room temperature. Secondary antibody Poly-HRP Gam/R/Ra; (Immunologic, VWR International, Radnor, USA) was applied for 30 min at room temperature. The substrate Bright DAB; Immunologic (Immunologic, VWR International, Radnor, USA) was applied for 7 min at room temperature. Similar protocols were used for referral cases 3–6.
Appropriate positive and negative controls were used throughout.
RNA was extracted from formalin-fixed and paraffin-embedded tissues (FFPE) using RNA-Bee-RNA isolation reagent (Bio-Connect BV, Huissen, the Netherlands) according to standard procedures. RNA quantity and quality were determined by a NanoDrop measurement (Fisher Scientific, Landsmeer, the Netherlands) and RNA extracts were subjected to RT-PCR for EWSR1-ATF1/CREB1.
Translocation-Specific PCR
cDNA synthesis was performed in a 24 µl reaction containing 1 µg of RNA, 1 µg of random hexamers (Promega Benelux, Leiden, the Netherlands) and 20 nmol dNTPs (Invitrogen Life Technologies Europe, Bleiswijk, the Netherlands) and heated at 65 °C for 5 min. Next 2 µl of RNasin (Promega Benelux, Leiden, the Netherlands), 8 µl of 5x first strand buffer (Invitrogen Life Technologies Europe, Bleiswijk, the Netherlands), 4 µl of 0.1 M DTT (Invitrogen Life Technologies Europe, Bleiswijk, the Netherlands) and 2 µl of Superscript II (Invitrogen Life Technologies Europe, Bleiswijk, the Netherlands) were added and the sample heated accordingly: 10 min at 20 °C, 60 min at 42 °C and 3 min at 95 °C. cDNA was stored at − 20 °C.
Potential translocation-specific EWSR1-ATF1/CREB1 fusion products were detected using primers targeting EWSR1 (exon 7: TCCTACAGCCAAGCTCCAAGTC and exon 8: GATTTGATCGTGGAGGCATGAG, RefSeq: NM_005243.1), ATF1 (exon 5: GTACTCCATCTGTGCCTGG, RefSeq: NM_005171.2) and CREB1 (exon 7: GTACCCCATCGGTACCATTGT and exon 8: CAATAGTGCTAGTGGGTGCTGTGC, RefSeq: NM_ 134442.3).
DNA amplification was performed in duplicate in a PTC 200 Thermal Cycler (MJ Research, Waltham, USA). The PCR was started with 10 min at 95 °C and followed with 38 cycles of denaturation at 95 °C for 30 s, annealing at 58 °C for 30 s and extension at 72 °C for 60 s, followed by a final extension at 72 °C for 7 min and cooling down for 5 min at 20 °C. PCR products were analyzed by 2% agarose gel electrophoresis.
Fluorescence In Situ Hybridization (FISH) Analysis
For the detection of an EWSR1 gene rearrangement (22q12), a directly ZyGreen/ZyOrange -labeled break apart probe (ZYTVZ-2096, VWR International, Radnor, USA) was used. The EWSR1-positive tumors were further tested with custom SpectrumOrange and SpectrumGreen differentially labeled break-apart probes by bacterial artificial chromosomes (BAC) flanking ATF1 (12q13), CREB1 (2q34) and CREB3L2 (7q33) genes. Probes were produced and labeled as previously described [3].
FISH was performed on 4 µm sections of formalin-fixed, paraffin-embedded tissue after baking at 56 °C for 45 min, deparaffinization with xylene and dehydration with ethanol. All tissue sections were pretreated with 10 mM sodium citrate (pH = 6.0) at 96 °C (10 min). After cooling down and rinsing in demineralised water, slides were treated with 0.01 M HCL (5 min) followed by pepsin digestion at 37 °C (15 min). After rinsing in 0.01 M HCL and subsequently PBS, slides were fixated in 1% formaldehyde/PBS (5 min). The slides were dehydrated in increasing ethanol series and air-dried. The probes were applied to the sections and the covered slides were sealed with rubber cement, heat-denatured at 80 °C for 10 min and hybridised at 37 °C overnight. Following rinsing successively in 2× sodium salt citrate (SCC) at 42 °C (5 min) and 0.3% NP-40 at 73 °C (respectively 2 and 1 min), 2× SCC at room temperature (5 min) and demineralised water; then, slides were again dehydrated in increasing ethanol solutions and air-dried. Finally, the slides were mounted with a solution containing both DAPI and Vectashield (Vector, Brunschwig, Amsterdam, the Netherlands). FISH signals were scored using a Leica DMRBE (Leitz) fluorescence microscope. A case was confirmed as positive for rearrangement of a given gene when > 15% of the nuclei examined showed a break-apart signal pattern.
Results
Clinical data are summarized in Table 1.
Table 1.
Clinical data
| Case # | Age/sex | Site | Therapy |
|---|---|---|---|
| 1 | 48/f | Mandible (34–37) | Resection R0; LN no metastases |
| 2 | 78/f | Mandible (median) | Resection R1; LN no metastases |
| 3 | 72/f | Mandible (38) | NA |
| 4 | 68/m | Maxilla (26) | Resection R0; LN no metastases |
| 5 | 71/f | Mandible | Resection R0; LN status unknown |
| 6 | 76/m | Mandible | Resection R0; LN status unknown |
f female, m male, R0 clear resection margins, R1 histologically positive margins, LN lymph nodes, NA not available
Of the six patients, four were female and two were male. The age ranged from 48 to 78 years. All tumors except one were located in the mandible. Surgical resection was performed in all cases where information was available (5/6). Clear margins were reported in four out of five cases. The remaining case showed microscopically positive margins of the mucosa, whereas bone margins were negative. In three cases, lymph node dissection was documented without presence of metastases.
Histologically, lesions were composed of sheets, trabeculae and/or strands of slightly pleomorphic cells with round to oval nuclei having open chromatin and prominent nucleoli (Fig. 1a, d). Mitotic figures were scarce or absent. There was abundant clear cytoplasm in five cases and mainly eosinophilic cytoplasm in one case. The stromal reaction varied from fibromyxoid, cellular to scarce with prominent vascularization. Coarse collagen bundles were seen in three cases (Fig. 1c). An inflammatory reaction was present in one case. In three cases extension into soft tissue was obvious.
Fig. 1.
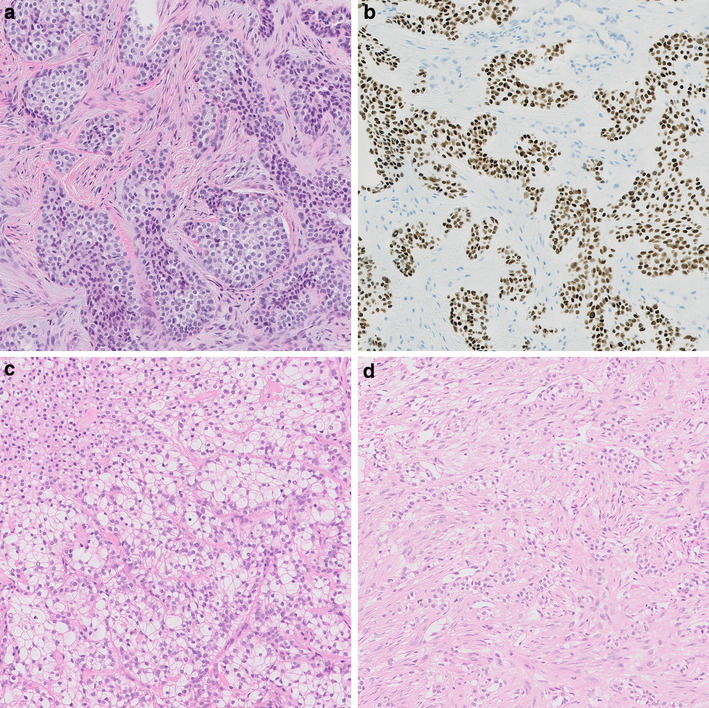
Case 1 (a index case) showed sheets of slightly polymorphic cells with clear to eosinophilic cytoplasm and positive nuclear staining for P63 (b). Case 3 (c) showed clear cells with intervening collagenic bundles and case 5 (d) was composed of strands and trabeculae of clear cells. HE, 20× (a, c, d). P63, clone 4A4, 1:3000, Immunologic, VWR International, Radnor, USA, 20x (b)
Immunohistochemical staining results are shown in Table 2.
Table 2.
Immunohistochemical staining results
| Case # | CK AE1/3 | CK MNF116 | P63 | P40 | CK7 | CK14 | EMA | S100 |
|---|---|---|---|---|---|---|---|---|
| 1 | + | nd | + | + | foc | nd | nd | nd |
| 2 | + | nd | + | nd | foc | + | + | foc |
| 3 | nd | + | nd | nd | foc | + | − | − |
| 4 | nd | + | nd | nd | nd | + | nd | − |
| 5 | nd | nd | nd | nd | nd | + | nd | − |
| 6 | + | nd | nd | nd | nd | nd | + | − |
foc focal expression, nd not done
Cases were positive with pankeratin AE1/3 (n = 3/3) and MNF116 (n = 2/2). CK14 showed a positive reaction in all four cases analysed (4/4). CK7 was focally expressed in three (3/3) cases. P63 and p40 were nuclear positive in two and one case tested, respectively (Fig. 1b). EMA reactivity was present in two out of three samples (2/3). S100 was only focally positive in one out of five cases (1/5).
Molecular test results are summarized in Table 3.
Table 3.
Molecular test results
| Casec | RT-PCRa | EWSR1 FISH | ATF1/CREB1/CREB3L2 FISH |
|---|---|---|---|
| 1 | EWSR1-CREB1 | + | NAb |
| 2 | Negative | + | − |
| 3 | Failed | + | ATF1+ |
| 4 | NAc | + | ATF1+ |
| 5 | NAc | + | − |
| 6 | NAc | + | − |
a EWSR1-ATF, EWSR1-CREB1
bNo sufficient tissue left
cNo tissue blocks available for RT-PCR
By RT-PCR, the index case presented an EWSR1-CREB1 fusion gene (Fig. 2); another case tested was negative for both fusion genes (ATF1 and CREB1) and one case failed for analysis due to insufficient RNA quality. Of three cases, only unstained tissue slides were available for FISH analysis.
Fig. 2.
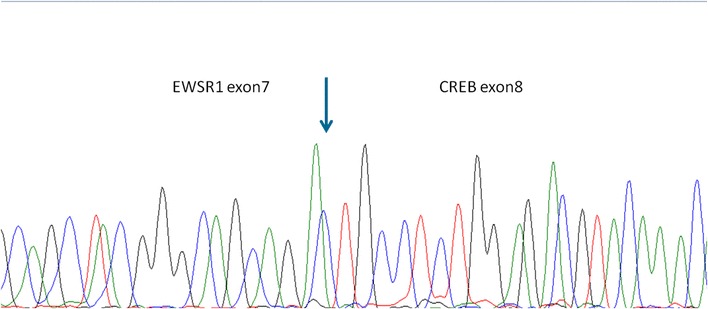
EWSR1-CREB1 fusion—index case 1
By FISH, all cases (6/6) showed an EWSR1 rearrangement and two cases were positive for ATF1 rearrangement. None of the tested cases (3/3) revealed CREB1/CREB3L2 involvement.
Discussion
There is a growing number of entities showing EWSR1-ATF1/CREB1 fusion genes including angiomatoid fibrous histiocytoma, clear cell sarcoma, clear cell sarcoma-like tumor of the gastrointestinal tract, myoepithelial tumor of soft tissue, intrapulmonary and intracranial myxoid tumors, clear cell carcinoma of the salivary gland and clear cell odontogenic carcinoma [4–6]. EWSR1 is a prototypical gene showing capability for fusing with a lot of different genes and showing rearrangements in several mesenchymal and non-mesenchymal neoplasms [7]. ATF1, CREB1 and CREB3L2 belong to the cAMP response element binding protein (CREB) transcription factor gene family and are functionally related [5]. The exact mechanisms by which EWSR1-ATF/CREB gene fusions contribute to oncogenesis are not well understood, but they are considered very early events in tumorigenesis and additional genetic or epigenetic events are considered to play an additional role in generating the different phenotypes [5, 7]. This fact reconfirms the stem cell/precursor cell concept in fusion gene associated neoplasms [8–10]. Whether some of these tumors represent a common spectrum of lesions is still under debate [2, 4].
Depending on the clinicopathological context, EWSR1-ATF1/CREB1 confirmation is a diagnostic aid to the corresponding histopathological diagnosis.
Apparently, as in other entities, ATF1 can be substituted by CREB1 in CCOC as identified in one of our cases tested by RT-PCR. Unfortunately, presence of CREB1 as fusion partner to EWSR1 in the index case could not be confirmed by FISH because no sufficient tissue was left for analysis.
All other cases in our cohort investigated using FISH, harbored EWSR1 rearrangement, with two cases showing a fusion with AFT1. The EWSR1-ATF1 fusion could not be confirmed by RT-PCR because of insufficient RNA quality in case 3. In case 4 we only had unstained tissue slides for FISH analysis, so RT-PCR could not be done for confirmation. None of the remaining cases (n = 3) were positive for CREB1 or CREB3L2, the latter as another member of the CREB transcription factor family.
CCOC shows overlapping histopathological and immunohistochemical characteristics with clear cell carcinoma of salivary glands. Additional molecular analysis corroborated this hypothesis. Both tumors are low-grade malignant neoplasms and are the first epithelial derived tumors with the mentioned fusion genes [2, 11].
In terms of immunohistochemistry, our cases confirm the findings reported by others [11, 12].
Differential diagnoses of CCOC are central (intraosseous) squamous cell carcinoma, clear cell variant of calcifying epithelial odontogenic tumor, myoepithelial tumors, central (intraosseous) mucoepidermoid carcinoma and sclerosing odontogenic carcinoma.
Even if there is immunohistochemical overlap with squamous cell carcinoma with positivity for high molecular weight keratin, p63 and p40 expression, the fusion gene seems to be specific to CCOC. Furthermore, pleomorphic nuclei, which are easily identified in SCC are usually not a prominent feature of CCOC. However, squamous metaplasia can occur in CCOC and, vice versa, clear cell changes can be present in SCC [11].
Clear cell variant of calcifying epithelial odontogenic tumor is a benign neoplasm and is, like CCOC, composed of nests of polygonal cells with a prominent stroma. The nuclei are more polymorphic in comparison to CCOC. Evidence of stromal amyloid and concentric calcification distinguishes this tumor type from CCOC [11].
Myoepithelial tumors may occur in the bone and may show clear cell morphology. However, more variable cytomorphology within a lesion and expression of S100 or GFAP are distinctive features. EWSR1 rearrangements can occur in these lesions [11, 13].
Central mucoepidermoid carcinoma (MEC) is the most common malignant salivary gland tumor of the jaw bones and a mimicker of CCOC when clear cells are present. However, epidermoid cells with abundant cytoplasm and goblet cells lining cysts or forming clusters are absent in CCOC. The hyalinized stroma may be present in both entities. Immunohistochemically, there is overlap of positive markers for CK5/6, p40, p63 and CK7 [14]. Evidence of the fusion gene might be a diagnostic aid in difficult cases with MEC harboring MAML2 fusions. A metastatic lesion originating from salivary gland should be ruled out [15–17].
Sclerosing odontogenic carcinomas are characterized by infiltrating single files of polyhedral epithelial cells with bland looking nuclei and large cytoplasmic vacuoles. The dense sclerotic stroma is a hallmark of this tumor. Involvement of adjacent muscle and nerves are often seen. The immunohistochemical profile does not differ from CCOC with expression of CK5/6, CK7 and p63. These tumors do not harbor EWSR1 rearrangement [12].
Metastases of renal cell carcinoma and melanoma can be mimics of CCOC and can be ruled out by immunohistochemistry with PAX8 expression for the former and positive melanoma markers for the latter [11].
Surgical resection seems to be the gold standard therapy [1]. Long term follow-up is necessary for these patients since late metastases and subsequent death are occasionally observed [12].
In conclusion, we report a series of CCOC showing EWSR1 rearrangement in all cases. For the first time, we showed that CREB1 is an alternative fusion partner of EWSR1 in CCOC.
Acknowledgements
We are grateful to the pathologists of the laboratories in Zwolle, Dordrecht and Roermond, the Netherlands, for providing case material.
Conflict of interest
All authors declare that there are no conflict of interest.
Ethical Approval
The study was conducted in accordance with the Code of Conduct of the Federation of Medical Scientific Societies in the Netherlands (http://www.federa.org).
References
- 1.Loyola AM, Cardoso SV, de Faria PR, Servato JP, Barbosa de Paulo LF, Eisenberg AL, et al. Clear cell odontogenic carcinoma: report of 7 new cases and systematic review of the current knowledge. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120(4):483–496. doi: 10.1016/j.oooo.2015.06.005. [DOI] [PubMed] [Google Scholar]
- 2.Bilodeau EA, Weinreb I, Antonescu CR, Zhang L, Dacic S, Muller S, et al. Clear cell odontogenic carcinomas show EWSR1 rearrangements: a novel finding and a biological link to salivary clear cell carcinomas. Am J Surg Pathol. 2013;37(7):1001–1005. doi: 10.1097/PAS.0b013e31828a6727. [DOI] [PubMed] [Google Scholar]
- 3.Antonescu CR, Katabi N, Zhang L, Sung YS, Seethala RR, Jordan RC, et al. EWSR1-ATF1 fusion is a novel and consistent finding in hyalinizing clear-cell carcinoma of salivary gland. Genes Chromosomes Cancer. 2011;50(7):559–570. doi: 10.1002/gcc.20881. [DOI] [PubMed] [Google Scholar]
- 4.Bale TA, Oviedo A, Kozakewich H, Giannini C, Davineni PK, Ligon K, et al. Intracranial myxoid mesenchymal tumors with EWSR1-CREB family gene fusions: myxoid variant of angiomatoid fibrous histiocytoma or novel entity? Brain Pathol. 2018;28(2):183–191. doi: 10.1111/bpa.12504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kao YC, Sung YS, Zhang L, Chen CL, Vaiyapuri S, Rosenblum MK, et al. EWSR1 fusions with CREB family transcription factors define a novel myxoid mesenchymal tumor with predilection for intracranial location. Am J Surg Pathol. 2017;41(4):482–490. doi: 10.1097/PAS.0000000000000788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sciot R, Jacobs S, Calenbergh FV, Demaerel P, Wozniak A, Debiec-Rychter M. Primary myxoid mesenchymal tumour with intracranial location: report of a case with a EWSR1-ATF1 fusion. Histopathology. 2018;72(5):880–883. doi: 10.1111/his.13437. [DOI] [PubMed] [Google Scholar]
- 7.Thway K, Fisher C. Tumors with EWSR1-CREB1 and EWSR1-ATF1 fusions: the current status. Am J Surg Pathol. 2012;36(7):e1–e11. doi: 10.1097/PAS.0b013e31825485c5. [DOI] [PubMed] [Google Scholar]
- 8.Vogelstein B, Kinzler KW. Cancer genes and the pathways they control. Nat Med. 2004;10(8):789–799. doi: 10.1038/nm1087. [DOI] [PubMed] [Google Scholar]
- 9.Tirode F, Laud-Duval K, Prieur A, Delorme B, Charbord P, Delattre O. Mesenchymal stem cell features of Ewing tumors. Cancer Cell. 2007;11(5):421–429. doi: 10.1016/j.ccr.2007.02.027. [DOI] [PubMed] [Google Scholar]
- 10.Taylor BS, Barretina J, Maki RG, Antonescu CR, Singer S, Ladanyi M. Advances in sarcoma genomics and new therapeutic targets. Nat Rev Cancer. 2011;11(8):541–557. doi: 10.1038/nrc3087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bilodeau EA, Hoschar AP, Barnes EL, Hunt JL, Seethala RR. Clear cell carcinoma and clear cell odontogenic carcinoma: a comparative clinicopathologic and immunohistochemical study. Head Neck Pathol. 2011;5(2):101–107. doi: 10.1007/s12105-011-0244-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Richardson MS, Muller S. Malignant odontogenic tumors: an update on selected tumors. Head Neck Pathol. 2014;8(4):411–420. doi: 10.1007/s12105-014-0584-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Song W, Flucke U, Suurmeijer AJH. Myoepithelial tumors of bone. Surg Pathol Clin. 2017;10(3):657–674. doi: 10.1016/j.path.2017.04.010. [DOI] [PubMed] [Google Scholar]
- 14.Sato K, Akiba J, Nakamura K, Abe H, Kawahara A, Aso T, et al. Mucoepidermoid carcinoma of the sublingual gland harboring a translocation of the MAML2 gene: a case report. Oncol Lett. 2017;14(3):2970–2974. doi: 10.3892/ol.2017.6550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tonon G, Modi S, Wu L, Kubo A, Coxon AB, Komiya T, et al. t(11;19)(q21;p13) translocation in mucoepidermoid carcinoma creates a novel fusion product that disrupts a Notch signaling pathway. Nat Genet. 2003;33(2):208–213. doi: 10.1038/ng1083. [DOI] [PubMed] [Google Scholar]
- 16.Hsieh MS, Wang H, Lee YH, Ko JY, Chang YL. Reevaluation of MAML2 fusion-negative mucoepidermoid carcinoma: a subgroup being actually hyalinizing clear cell carcinoma of the salivary gland with EWSR1 translocation. Hum Pathol. 2017;61:9–18. doi: 10.1016/j.humpath.2016.06.029. [DOI] [PubMed] [Google Scholar]
- 17.de Souza LL, Pontes FSC, Pontes HAR, Neto NC, de Carvalho WRS, Guimaraes DM. Central mucoepidermoid carcinoma: an up-to-date analysis of 147 cases and review of prognostic factors. J Craniomaxillofac Surg. 2018;46(1):162–167. doi: 10.1016/j.jcms.2017.10.020. [DOI] [PubMed] [Google Scholar]