

Abstract
Background
Thrombolytic therapy is usually reserved for patients with clinically serious or massive pulmonary embolism (PE). Evidence suggests that thrombolytic agents may dissolve blood clots more rapidly than heparin and may reduce the death rate associated with PE. However, there are still concerns about the possible risk of adverse effects of thrombolytic therapy, such as major or minor haemorrhage. This is the third update of the Cochrane review first published in 2006.
Objectives
To assess the effects of thrombolytic therapy for acute pulmonary embolism.
Search methods
The Cochrane Vascular Information Specialist searched the Cochrane Vascular Specialised Register, CENTRAL, MEDLINE, Embase, and CINAHL databases and the World Health Organization International Clinical Trials Registry Platform and ClinicalTrials.gov trials registers to 16 April 2018. We undertook reference checking to identify additional studies.
Selection criteria
We included randomised controlled trials (RCTs) that compared thrombolytic therapy followed by heparin versus heparin alone, heparin plus placebo, or surgical intervention for patients with acute PE. We did not include trials comparing two different thrombolytic agents or different doses of the same thrombolytic drug.
Data collection and analysis
Two review authors (JY, QH) assessed the eligibility and quality of trials and extracted data. We calculated effect estimates using the odds ratio (OR) with 95% confidence interval (CI) or the mean difference (MD) with 95% CI. We assessed the quality of the evidence using GRADE criteria.
Main results
We identified no new studies for inclusion in this 2018 update. We included in the review 18 trials with a total of 2197 participants. We were not able to include one study in the meta‐analysis because it provided no data that we could extract. Most of the studies carried a high risk of bias because of high or unclear risk related to randomisation and blinding. Meta‐analysis showed that, compared with heparin alone, or heparin plus placebo, thrombolytics plus heparin can reduce the odds of death (OR 0.57, 95% CI 0.37 to 0.87, 2167 participants, P = 0.01, low‐quality evidence) and recurrence of PE (OR 0.51, 95% CI 0.29 to 0.89, 1898 participants, P = 0.02, low‐quality evidence). Effects on mortality weakened when we excluded from analysis four studies at high risk of bias (OR 0.66, 95% CI 0.42 to 1.06, 2054 participants, P = 0.08). The incidence of major and minor haemorrhagic events was higher in the thrombolytics group than in the control group (OR 2.90, 95% CI 1.95 to 4.31, 1897 participants, P < 0.001, low‐quality evidence; OR 3.09, 95% CI 1.58 to 6.06, 1553 participants, P = 0.001, very low‐quality evidence, respectively). We downgraded the quality of the evidence to low or very low because of design limitations, potential influence of pharmaceutical companies, and small sample sizes. Length of hospital stay (mean difference (MD) ‐0.89, 95% CI ‐3.13 to 1.34) and quality of life were similar between the two treatment groups. Limited information from a small number of trials indicated that thrombolytics may improve haemodynamic outcomes, perfusion lung scanning, pulmonary angiogram assessment, echocardiograms, pulmonary hypertension, coagulation parameters, clinical outcomes, and survival time to a greater extent than heparin alone. However, the heterogeneity of the studies and the small number of participants involved warrant caution when results are interpreted. Similarily, fewer participants from the thrombolytics group required escalation of treatment. None of the included studies reported on post‐thrombotic syndrome or compared the costs of different treatments.
Authors' conclusions
Low‐quality evidence suggests that thrombolytics reduce death following acute pulmonary embolism compared with heparin. The included studies used a variety of thrombolytic drugs. Thrombolytic therapy may be helpful in reducing the recurrence of pulmonary emboli but may cause major and minor haemorrhagic events and stroke. More high‐quality, blinded randomised controlled trials assessing safety and cost‐effectiveness of therapies for pulmonary embolism are required.
Plain language summary
Drugs to dissolve pulmonary embolism (blood clot in the lungs)
Background
A pulmonary embolus is a potentially fatal blood clot that lodges in the main artery of the lungs, straining the right side of the heart and affecting blood circulation. Patients with this condition are at risk for new emboli forming (recurrence). In the case of a massive pulmonary embolism, treatment to restore blood flow is urgently required. Heparin thins the blood, but newer drugs that actively break up the clots (thrombolytics) may act more quickly and may be more effective. These newer drugs include streptokinase, urokinase, and recombinant tissue‐type plasminogen activator. The major complication of this treatment is bleeding.
Key results
Review authors searched the literature and included 18 studies in this update (evidence current to 16 April 2018). These trials involved 2197 adult participants with pulmonary embolism, who were randomly assigned to a thrombolytic agent followed by heparin versus heparin alone or heparin plus placebo or surgical procedure. We were able to combine data from 17 clinical trials with a total of 2167 patients. Thrombolytics seemed to lower the likelihood of death or recurrence of blood clots over heparin. However, after exclusion of four very low‐quality studies, this benefit disappeared. On the other hand, thrombolytics caused more side effects, including major and minor bleeding events (haemorrhagic events) and stroke, than heparin alone. Limited information from five trials shows that thrombolytics were better at improving blood flow through the lungs; seven included studies show that they can improve heart function.
Quality of the evidence
The quality of the evidence is low because of several important design limitations, potential influence of pharmaceutical companies, and small sample sizes. We need more large and rigorous trials to examine whether thrombolytic therapy is truly beneficial for pulmonary embolism.
Summary of findings
Summary of findings for the main comparison. Thrombolytic therapy versus heparin: primary outcome measures for pulmonary embolism.
| Thrombolytic therapy versus heparin: primary outcome measures for pulmonary embolism | |||||
| Patient or population: patients with acute pulmonary embolism Setting: hospital Intervention: thrombolytic therapy Comparison: heparin | |||||
| Outcomes (duration of follow‐up: from 7 days to 12 months) | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No. of participants (RCTs) | Quality of the evidence (GRADE) | |
| Assumed risk | Corresponding risk | ||||
| Heparin | Thrombolytic therapy | ||||
| Death from all causes | Study population | OR 0.57 (0.37 to 0.87) | 2167 (17) | ⊕⊕⊝⊝ lowa | |
| 49 per 1000 | 28 per 1000 (19 to 43) | ||||
| Moderate | |||||
| 50 per 1000 | 29 per 1000 (19 to 44) | ||||
| Recurrence of pulmonary emboli | Study population | OR 0.51 (0.29 to 0.89) | 1898 (10) | ⊕⊕⊝⊝ lowa | |
| 39 per 1000 | 20 per 1000 (12 to 35) | ||||
| Moderate | |||||
| 42 per 1000 | 22 per 1000 (13 to 38) | ||||
| Major haemorrhagic events | Study population | OR 2.9 (1.95 to 4.31) | 1897 (12) | ⊕⊕⊝⊝ lowa | |
| 38 per 1000 | 102 per 1000 (71 to 145) | ||||
| Moderate | |||||
| 31 per 1000 | 85 per 1000 (59 to 121) | ||||
| Minor haemorrhagic events | Study population | OR 3.03 (1.60 to 5.73) | 1553 (10) | ⊕⊝⊝⊝ very lowa,b | |
| 101 per 1000 | 253 per 1000 (152 to 391) | ||||
| Moderate | |||||
| 107 per 1000 | 266 per 1000 (161 to 407) | ||||
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: confidence interval; OR: odds ratio; RCT: randomised controlled trial. | |||||
| GRADE Working Group grades of evidence. High quality: further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: we are very uncertain about the estimate. | |||||
aDowngraded by two levels for very serious risk of bias (due to high risk of selection, performance, and detection bias in most included studies). bDowngraded by one level for serious inconsistency (due to substantial heterogeneity; I² = 57%).
Background
Description of the condition
A pulmonary embolus, or a blood clot in the artery of the lungs, is a life‐threatening condition known as 'pulmonary embolism (PE)' that is accompanied by significant morbidity and mortality. Massive and submassive PEs are subtypes of PE that are often encountered in the literature, even though the definitions of these subtypes are often vague and can lead to ambiguity (Goldhaber 2002). Because the severity and prognosis of PE vary widely, risk stratification after PE diagnosis is essential. The American Heart Association defines massive PE, submassive PE, and low‐risk PE based on associated clinical deterioration and short‐term mortality (Table 2; Jaff 2011; Sista 2017). Submassive or massive PE has been used interchangeably with the term intermediate‐risk or high‐risk PE, respectively (Gupta 2018).
1. American Heart Association definitions of massive, submassive, and low‐risk PE.
| Risk classification | Definition | Short‐term mortality |
| Massive PE | Acute PE with haemodynamically unstable manifestations such as sustained hypotension (systolic blood pressure < 90 mmHg for at least 15 minutes or requiring inotropic support, not due to a cause other than PE, such as arrhythmia, hypovolaemia, sepsis, or left ventricular dysfunction), lack of pulse, or persistent profound bradycardia (heart rate < 40 beats per minute (bpm) with signs or symptoms of shock) | 25% to 65% |
| Submassive PE | Haemodynamically stable (without systemic hypotension (systolic blood pressure > 90 mmHg)) patients who present with either right ventricular dysfunction or myocardial necrosis (RV dysfunction (CT, BPN/proBNP, ECG changes) or myocardial necrosis (elevated troponins)) | 3% |
| Low‐risk PE | Absence of hypotension, RV dysfunction, and myocardial necrosis | < 1% |
BPN: B‐type natriuretic peptide CT: computed tomography ECG: electrocardiography PE: pulmonary embolism RV: right ventricular
Several options are available for the management of PE. Anticoagulation therapy forms the foundation of PE management (Hepburn‐Brown 2018). In massive or high‐risk PE, where restoration of pulmonary arterial flow is urgently required due to right ventricular failure, prompt therapeutic intervention is imperative. In such cases, thrombolysis (peripheral or catheter‐directed) or surgical embolectomy should be considered (Hepburn‐Brown 2018; Tapson 2017).
Description of the intervention
Although the thrombotic origin of PE has been well documented for almost two centuries, anticoagulation (anti‐clotting drugs) as treatment for venous thromboembolism (VTE) dates back less than a century, and thrombolysis was initiated only relatively recently. In 1962, Browse and James reported that streptokinase could lyse (break up) pulmonary emboli in dogs and humans. Four patients treated with different dosage regimens experienced striking clinical improvement (Browse 1962). Additional studies show that patients who had hypotension (low blood pressure) responded quickly to streptokinase therapy, and their lung scans returned almost completely to normal (Bottiger 1994; Browse 1962; Chesterman 1969). However, improvement was less marked in those with associated cardiopulmonary disease and recurrent emboli (Hirsh 1971; Meneveau 2006).
The findings of four clinical studies of urokinase for PE indicate that improvement with urokinase was more dramatic than with heparin alone (Genton 1968; Sasahara 1967; Sautter 1967; Tow 1967). Based on this promising experience, the National Heart and Lung Institute organised a multi‐institutional randomised controlled trial (RCT) to evaluate thrombolytic agents for treatment of PE. Results of Phase I (the Urokinase Pulmonary Embolism Trial ‐ UPET) show that a 12‐hour infusion of urokinase followed by heparin and oral anticoagulants, compared to heparin and oral anticoagulants alone, increased the resolution rate of pulmonary thromboemboli (Hyers 1970). Phase II (the Urokinase‐Streptokinase Pulmonary Embolism Trial ‐ USPET), completed in 1973, shows comparable results for two additional thrombolytic regimens ‐ 24 hours of streptokinase and 24 hours of urokinase. Increasing the duration of urokinase administration to 24 hours conferred little benefit, and the distinction between 24 hours of urokinase and 24 hours of streptokinase was not clear (UPET Study Group 1974). These trials did not document actual improvement in survival; however, patients with massive embolism did derive major physiological benefit. Therefore, thrombolytic agents may be useful for severely ill patients with massive embolism or submassive embolism, especially when accompanied by shock.
In the late 1980s, recombinant tissue‐type plasminogen activator (rt‐PA) was introduced for treatment of acute PE, and an RCT reported its faster action and greater safety in comparison with urokinase (Goldhaber 1988). One multi‐centre study shows that rt‐PA decreased mean pulmonary arterial pressure (Meyer 1992). Effects of intravenous rt‐PA on arterial blood gases and right ventricular function were compared with the effect of heparin treatment in acute PE. Results show that rt‐PA is more effective for acute PE than heparin alone, and that a high dose of rt‐PA leads to rapid improvement in arterial blood gases and lung perfusion images with no clinical episodes of recurrent PE (Goldhaber 1993; Yamasawa 1992). The collaborative PIOPED study suggested that rt‐PA given over two hours has little effect on angiographic clot burden but may produce some improvement in haemodynamics. However, this treatment is not without risk (Tapson 2017). Until now, the effectiveness of thrombolytic therapy in PE remains under discussion (Eberle 2018; Hepburn‐Brown 2018).
Why it is important to do this review
Although good evidence shows that thrombolytic agents are superior to heparin alone in accelerating the lysis of pulmonary emboli, restoring normal pulmonary circulation, and decreasing strain on the right side of the heart, few data are available on their long‐term benefits for PE (Chatterjee 2014). Studies of long‐term benefit of thrombolytic therapy for patients with PE suggest that thrombolytic therapy preserves the normal haemodynamic response to exercise and maintains cardiac output during long‐term follow‐up, possibly preventing recurrence of VTE and development of pulmonary hypertension (Sharma 2000).
Although it is difficult to prove that thrombolytic agents decrease mortality from pulmonary emboli, one large registry shows that thrombolytic treatment was associated with a 50% reduction in death risk among clinically stable patients with right ventricular enlargement (Konstantinides 1999), and another prospective RCT shows that thrombolytic therapy reduced the mortality rate of massive acute PE (Jerjes‐Sánchez 1995).
Different thrombolytic agents ‐ rt‐PA, alteplase, streptokinase, and urokinase ‐ are almost equally efficacious in dissolving clots. However, these agents are not without risk, sometimes leading to frequent massive bleeding, including intracranial haemorrhage (Chatterjee 2014; Dalla‐Volta 1992). Other studies show that bleeding and fever were increased in streptokinase‐treated patients, but both were generally controllable, with most bleeding occurring at the puncture site (Goldhaber 1993; Sasahara 1973). Several recent meta‐analyses conducted to assess the efficacy and safety of thrombolytic therapy for treatment of PE show no obvious differences in mortality nor in risk of PE relapse between the group of patients receiving thrombolytic agents and the group not receiving them (Cao 2014; Gao 2015; Liu 2014; Marti 2014; Nakamura 2014). However, they reveal substantial differences between these two groups with regard to the risk of bleeding events (Chatterjee 2014; Gao 2015).
Although most studies agree that thrombolytic agents are superior to heparin alone in accelerating the lysis of pulmonary thromboemboli, their benefits in terms of reduced death rate from PE and influence on survival and risks of associated haemorrhagic complications remain unclear, especially for patients with submassive, or intermediate‐risk, PE. This review will attempt to ascertain the efficacy of thrombolytic agents for treatment of PE. This is the third update of a review first published in 2006.
Objectives
To assess the effects of thrombolytic therapy for acute pulmonary embolism.
Methods
Criteria for considering studies for this review
Types of studies
We included all randomised controlled trials (RCTs) that compared thrombolytic therapy (e.g. streptokinase, urokinase, recombinant tissue plasminogen activator (rt‐PA), alteplase) followed by heparin versus heparin alone, heparin plus placebo, or surgical intervention (e.g. embolectomy) for people with acute pulmonary embolism (PE). We did not include trials that compared two different thrombolytic agents or different doses of the same thrombolytic drug.
Types of participants
We included participants who had symptoms or signs of PE, confirmed by pulmonary angiography, ventilation/perfusion lung scan, or another validated measurement.
Types of interventions
We included any type of thrombolytic drug (e.g. streptokinase, urokinase, rt‐PA, alteplase) followed by heparin versus heparin alone, heparin plus placebo, or surgical intervention (e.g. embolectomy).
Types of outcome measures
We analysed the following clinical outcome measures on an intention‐to‐treat (ITT) basis.
Primary outcomes
Death from all causes
Recurrence of pulmonary emboli
-
Haemorrhagic events
Major haemorrhagic events: a decreased haemoglobin concentration > 2 g/dL; retroperitoneal or intracranial bleeding; transfusion of two or more units of blood, which may or may not lead to discontinuation of anticoagulant treatment
Minor haemorrhagic events: other bleeding events not meeting the criteria for major bleeding
Secondary outcomes
Haemodynamic improvement and thrombolysis: immediate clinical, haemodynamic, angiographic, perfusion lung scanning, or echocardiographic outcomes or the rapidity of resolution of PE as judged by the change in total pulmonary resistance (TPR) over the initial hours
Chronic thromboembolic pulmonary hypertension after three months, six months, and one year, and at the end of the follow‐up period
Differences in coagulation parameters over time
Post‐thrombotic syndrome (PTS): complications after deep vein thrombosis (DVT) may include persistent oedema (swelling), pain, purpura (bleeding into the skin), increased skin pigmentation, eczematoid (eczema‐like) dermatitis, pruritus (itchiness), ulceration, and cellulitis (bacterial infection just below the skin). All of these complications result from impaired return of blood through the veins of the lower leg to the heart. This is determined by using any validated measurement for PTS
Escalation of treatment
Hospital stay
Survival time
Composite clinical outcome: sum per participant of mortality, recurrent PE, and major and minor haemorrhagic events
Quality of life (QoL)
Healthcare cost comparison
Search methods for identification of studies
Electronic searches
The Cochrane Vascular Information Specialist conducted systematic searches of the following databases for randomised controlled trials and controlled clinical trials without language, publication year, or publication status restrictions.
Cochrane Vascular Specialised Register via the Cochrane Register of Studies (CRS‐Web, searched on 16 April 2018).
Cochrane Central Register of Controlled Trials (CENTRAL), in the Cochrane Library, and Cochrane Register of Studies Online (CRSO; 2018, Issue 3).
MEDLINE (Ovid MEDLINE® Epub Ahead of Print, In‐Process & Other Non‐Indexed Citations, Ovid MEDLINE® Daily, and Ovid MEDLINE®) (searched from 1 January 2017 to 16 April 2018).
Embase Ovid (searched from 1 January 2017 to 16 April 2018).
Cumulative Index to Nursing and Allied Health Literature (CINAHL) Ebsco (searched from 1 January 2017 to 16 April 2018).
Allied and Complementary Medicine Database (AMED) Ovid (searched from 1 January 2017 to 16 April 2018).
The Information Specialist modelled search strategies for other databases on the search strategy designed for CENTRAL. When appropriate, we combined these strategies with adaptations of the highly sensitive search strategy designed by Cochrane for identifying randomised controlled trials and controlled clinical trials (as described in the Cochrane Handbook for Systematic Reviews of Interventions, Chapter 6; Lefebvre 2011). We have provided the search strategies used for major databases in Appendix 1.
The Information Specialist searched the following trials registries on 16 April 2018.
World Health Organization International Clinical Trials Registry Platform (who.int/trialsearch).
ClinicalTrials.gov (clinicaltrials.gov).
Searching other resources
For this update, review authors searched all references from included studies.
Data collection and analysis
Selection of studies
Two review authors (JY, QH) independently assessed the titles and abstracts of all trial reports identified by the searches. Whenever possible, we obtained the full‐text hard copies for studies that appeared to fulfil the selection criteria. Each review author had a list of selected papers and duplicate sets of the papers for independent analyses. To ascertain that the study met the inclusion criteria, we used a standard form to collect information concerning type of study, types of participants, and types of interventions, and we resolved disagreements through discussion.
Data extraction and management
Two review authors (JY, QH) independently extracted information on participants, methods, interventions, outcomes, and results using a pre‐tested form, resolving disagreements through discussion.
Assessment of risk of bias in included studies
We recorded data regarding the methodological criteria employed by investigators in all included studies. We have presented in the review a narrative summary in the 'Risk of bias' tables and have discussed these details in the text where relevant. Two review authors (JY, QH) independently assessed trials for risk of bias with regard to adequate sequence generation; allocation concealment; blinding of participants, personnel, and outcomes assessors; attrition bias (i.e. whether all participants were accounted for in the analysis (intention‐to‐treat, or ITT)); selective reporting; and other types of bias. We graded each domain as 'low risk of bias', 'high risk of bias', or 'unclear risk of bias' according to the guidelines provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Sequence generation
Examples of randomisation methods falling into each risk of bias category for generation of the allocation sequence include the following.
Low risk of bias: adequate generation of allocation sequence encompasses randomisation methods such as computer‐generated numbers, a table of random numbers, shuffling of cards or envelopes, coin or dice tossing, and drawing of lots.
High risk of bias: inadequate generation of allocation sequence refers to group allocations by case record number; date of birth; day, month, or year of admission; judgement of the clinician or the participant; laboratory test or series of tests; and availability of the intervention.
Unclear risk of bias: study authors reported generation of the allocation sequence unclearly.
Allocation concealment
Examples of methods used for allocation concealment that fall into each category include the following.
Low risk of bias: adequate allocation concealment was achieved through central randomisation (including telephone, web‐based, and pharmacy‐controlled randomisation; sealed opaque containers administered serially to participants).
High risk of bias: inadequate allocation concealment occurred via any procedure that was transparent before allocation.
Unclear risk of bias: trials provided insufficient information to allow a judgement on risk of bias.
Blinding
Double‐blinding methods include masking the clinician (person delivering treatment), the participant, and the outcomes assessor to treatment allocation. We determined risk of bias in line with the following examples.
Low risk of bias: we considered masking of both participants and the results assessor as carrying low risk of performance and detection bias. We did not consider blinding necessary for mortality or other outcomes not influenced by blinding.
High risk of bias: non‐blinded assessment outcomes such as quality of life (QoL) carry high risk of bias; for objective outcomes (e.g. death), we did not consider this necessary.
Unclear risk of bias: studies did not provide sufficient information for a judgement of 'yes' or 'no'. We considered single‐blinding of the results assessor to carry moderate risk of performance bias, detection bias, or both. If single‐blinding was performed on participants but not on the results assessor, we considered the outcomes to carry high risk of detection bias.
Incomplete outcome data
'Incomplete outcome data' refers to a mismatch between the number of randomised participants and the number included in the main analysis. Examples of the three risk categories include the following.
Low risk of bias: trials are not missing outcome data or note few exclusions and attrition; an ITT analysis is possible.
High risk of bias: the rate of exclusion, attrition, or both is higher than 15%, or there are wide differences in exclusions between intervention group and control group, whichever ITT analysis is used.
Unclear risk of bias or moderate risk of bias: trials report the rate of exclusion or attrition (or both) as higher than 10%, whichever ITT analysis is used.
Selective reporting
If the protocol of the included study was available, we compared outcomes in the protocol versus those in the published report. If the protocol was not available, we compared outcomes listed in the Methods section of the study against those presented in the Results.
Other bias
We assessed potential factors affecting the precision of an estimate of included studies.
All quality criteria met: low risk of bias.
One or more of the quality criteria met in part: unclear risk of bias.
One or more criteria not met: high risk of bias.
We resolved disagreements about whether or not a trial fulfilled certain quality criteria through discussion with a third review author (BD). We have detailed all quality criteria ratings and supporting information in the 'Risk of bias' tables (see Characteristics of included studies).
Measures of treatment effect
We analysed the data using RevMan 5.3 (Review Manager 2014). We summarised dichotomous data as odds ratio (OR) and continuous data as mean difference (MD), using 95% confidence intervals (CIs) throughout.
Unit of analysis issues
For multiple‐arm trials, we included the intervention group of interest according to the objective in our review. We took care to avoid double‐counting of participants when we included multiple‐arm trials. For cross‐over trials, we planned to include the first period of the trial and to exclude the subsequent period to prevent interference with previous drugs, even if the trial reported a washout period. For cluster RCTs, we planned to calculate the effective sample size both in the intervention group and in the control group based on the numbers of clusters and participants, and then, when necessary, to use the generic inverse variance method to pool this type of data according to recommendations provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Dealing with missing data
We contacted trial authors for missing data. For this review, we analysed outcome measures on an ITT basis.
Assessment of heterogeneity
For detecting heterogeneity across studies, we used the Chi² test with a 10% level of statistical significance, establishing a P value of 0.1 as the cutoff value to determine statistical significance. We used the I² statistic to estimate total variation across studies. We considered an I² value less than 40% to represent low‐level heterogeneity, 40% to 50% as representing a moderate level of heterogeneity, 50% to 90% as showing a substantial level of heterogeneity, and 75% to 100% as indicating considerable heterogeneity (Higgins 2011).
Within each subgroup, we used Chi² analyses to test for statistical evidence of heterogeneity among studies, and we used I² to measure the degree of inconsistency across studies. When Chi² analysis was significant and I² values were in excess of 50%, we analysed differences in participant selection, baseline values, risk of bias, design, and methods that could possibly explain the heterogeneity.
Assessment of reporting biases
Funnel plots have a limited role when used with small numbers of studies (< 10) in a meta‐analysis. Our review included only a few studies (< 10) in each subgroup, so we did not use this approach to assess reporting bias. In the future, if we can include more studies in a subgroup, we will use a funnel plot to assess the presence of publication bias. However, we did attempt to access the protocols of the included studies to assess selective reporting bias.
Data synthesis
We used a random‐effects model for pooled analysis of heterogeneous data (I² = 40% to 100%) and a fixed‐effect model for individual study data and pooled analyses of homogeneous data (I² < 40%). We used the Mantel‐Haenszel method to synthesise dichotomous data and the inverse variance method to synthesise continuous data. We summarised dichotomous data as odds ratio (OR) and continuous data as mean difference (MD) and used 95% confidence intervals (CIs) throughout. When it was not possible to undertake meta‐analyses, we described a systematic approach to synthesising the findings of multiple studies.
Subgroup analysis and investigation of heterogeneity
We analysed subgroups according to the different types of interventions included in the review. We also performed a subgroup analysis according to different types of PE (massive/submassive) for the primary outcomes. We analysed studies of submassive PE that used an ultrasound‐assisted, catheter‐directed thrombolysis system (USAT (rt‐PA)) separately from other studies investigating submassive PE because USAT (rt‐PA) is a new and different intervention from traditional thrombolytic therapy. For studies that included both massive and other unknown PE types, we categorised participants as 'type of PE unknown'. We used the interaction test (whereby an I² statistic is computed for heterogeneity across subgroup results) for subgroup differences in Review Manager 2014 as the basis for interpreting subgroup analyses. For future updates, and if the necessary data become available, we plan to analyse subgroups according to different doses and durations of intervention.
Sensitivity analysis
We performed a sensitivity analysis according to the methodological quality of included studies. We excluded very low‐quality studies from the pooled meta‐analysis. In this review, we defined very low‐quality studies as having high risk in two or more risk of bias domains.
'Summary of findings' table
In this review, we included only RCTs. We used the GRADE profiler to help us create Table 1 and reported the primary outcomes of death from all causes; recurrence of pulmonary emboli; and major and minor haemorrhagic events based on an ITT population (GRADEpro GDT 2015). We downgraded the evidence from 'high quality' by one or two levels for serious or very serious study limitations (risk of bias), indirectness and inconsistency of evidence, imprecision of effect estimates, or potential publication bias according to recommendations provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011).
Results
Description of studies
Results of the search
We included no new studies in this 2018 update. We identified one additional report for an already included study (Meyer 2014). We excluded nine new additional studies (Alexandru Ion 2017; Barrios 2017; Carroll 2018; Jing 2018; Lehnert 2017; NCT00680628; NCT00968929; Xu 2016; Yilmazel 2018). We had previously listed one study as ongoing (NCT00680628). We identified three new ongoing studies (EUCTR2017‐005075‐91‐DK; NCT02604238; NCT03218410). See Figure 1.
1.
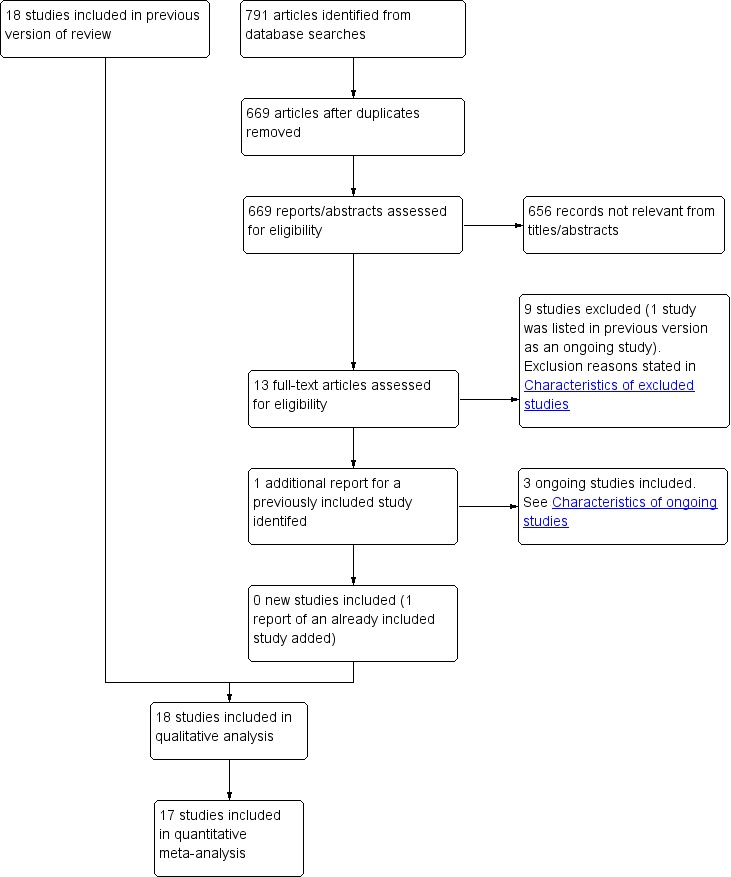
Study flow diagram.
Included studies
We included a total of 18 studies with 2197 participants (Becattini 2010; Dalla‐Volta 1992; Dotter 1979; Fasullo 2011; Goldhaber 1993; Jerjes‐Sánchez 1995; Kline 2014; Konstantinides 2002; Kucher 2014; Levine 1990; Ly 1978; Marini 1988; Meyer 2014; PIOPED 1990; Sharifi 2013; Taherkhani 2014; Tibbutt 1974; UPETSG 1970). We were able to use 17 of the included trials (2167 participants) in the meta‐analysis; the other study lacked outcome data (Marini 1988).
Design
All included RCTs used a parallel design and included two study arms (apart from Marini 1988, which had three arms). Nine were multi‐centre RCTs (Becattini 2010; Dalla‐Volta 1992; Kline 2014; Konstantinides 2002; Kucher 2014; Levine 1990; Meyer 2014; PIOPED 1990; UPETSG 1970); one was a two‐centre study (Tibbutt 1974); and the remainder were single‐centre studies (Dotter 1979; Fasullo 2011; Goldhaber 1993; Jerjes‐Sánchez 1995; Ly 1978; Marini 1988; Sharifi 2013; Taherkhani 2014).
Participants
All trials focussed on adults aged 18 or over. Trials took place in Italy (Becattini 2010; Dalla‐Volta 1992; Fasullo 2011), the United States (Dotter 1979; Goldhaber 1993; Kline 2014; PIOPED 1990; UPETSG 1970), Canada (Levine 1990), Norway (Ly 1978), Germany (Konstantinides 2002), Germany and other European countries (Kucher 2014; Meyer 2014), Iran (Taherkhani 2014), and the United Kingdom (Tibbutt 1974). Three studies did not describe the study setting or country (Jerjes‐Sánchez 1995; Marini 1988; Sharifi 2013). All trials stated baseline data and analysed comparability. Eleven trials included participants with submassive PE (Becattini 2010; Dalla‐Volta 1992; Fasullo 2011; Goldhaber 1993; Kline 2014; Konstantinides 2002; Kucher 2014; Levine 1990; Meyer 2014; Sharifi 2013; Taherkhani 2014), and only one study included only participants with massive PE (Jerjes‐Sánchez 1995). We were unable to identify the type of PE in six studies (Dotter 1979; Ly 1978; Marini 1988; PIOPED 1990; Tibbutt 1974; UPETSG 1970).
Interventions
Studies involved different types of thrombolytics, including alteplase, urokinase, streptokinase, rt‐PA, ultrasound‐assisted catheter‐directed thrombolysis system, and tenecteplase, usually followed by heparin. The control intervention was heparin alone in 11 included trials (Dalla‐Volta 1992; Dotter 1979; Goldhaber 1993; Jerjes‐Sánchez 1995; Kucher 2014; Ly 1978; Marini 1988; Sharifi 2013; Taherkhani 2014; Tibbutt 1974; UPETSG 1970). The remaining seven trials used placebo plus heparin (Becattini 2010; Fasullo 2011; Kline 2014; Konstantinides 2002; Levine 1990; Meyer 2014; PIOPED 1990). No studies compared thrombolytics versus surgical intervention.
Outcome measures
Investigators reported a variety of outcome measures. Most trials reported overall mortality, recurrence of PE, and haemorrhagic events. Main outcome measures also included perfusion lung scanning, haemodynamic outcomes, and angiographic score. Two trials that performed perfusion lung scanning reported data at several time points (first, third, and seventh days post treatment) (Levine 1990; UPETSG 1970). Three trials reported haemodynamic outcomes in nine subgroups (PIOPED 1990; Tibbutt 1974; UPETSG 1970). Four other trials reported length of hospital stay or hospitalised status of the participant, including rate of rehospitalisation (Kucher 2014; Meyer 2014; Sharifi 2013; Taherkhani 2014). Kline 2014 reported on functional capacity and quality of life (using the Venous Insufficiency Epidemiological and Economic Study, or VEINES, questionnaire and score). None of the trials assessed healthcare costs.
See the Characteristics of included studies table for further details.
Ongoing studies
We identified three new ongoing studies for this update (EUCTR2017‐005075‐91‐DK; NCT02604238; NCT03218410), bringing the total number of ongoing studies to six (EUCTR2017‐005075‐91‐DK; EudraCT: 2005‐001070‐27; NCT01531829; NCT02604238; NCT03218410). See Characteristics of ongoing studies for further details.
Excluded studies
For this 2018 update, we identified and excluded nine additional studies (Alexandru Ion 2017; Barrios 2017; Carroll 2018; Jing 2018; Lehnert 2017; NCT00680628; NCT00968929; Xu 2016; Yilmazel 2018). One study was previously listed as ongoing, but we excluded it from this update because the study was terminated (NCT00680628), bringing the total to 56 excluded studies (Abdelsamad 2011; Agnelli 1997; Alexandru Ion 2017; Barrios 2017; Bell 1974; Bell 1976; Bell 1977; Bhardwaj 2010; Carroll 2018; Charbonnier 1984; Chen 2009; Comerota 2009; De Takats 1973; Erkan 2002; Francois 1986; Goldhaber 1989; Goldhaber 1992; Goldhaber 1994; IRCT201104245625N2; Jin 2012; Jing 2018; Konstantinides 1998; Lehnert 2017; Liu 2012; Marder 1978; Meneveau 1997; Meneveau 1998; Meyer 1992; Miller 1971; Muhl 2007; NCT00968929; NCT00680628; NCT01956955; Ohayon 1986; Palla 1997; Pang 2007; Prandoni 1985; Research Group on Urokinase and PE 1984; Saponjski 2002; Sasahara 1975; Sharma 2000; Sors 1994; Tebbe 1999; Tebbe 2009; UKEP Study Group 1987; UPET Study Group 1974; Verstraete 1988; Wang 2006; Wang 2009; Wang 2010; Wu 2010; Xu 2016; Yang 2007; Yang 2011; Yilmazel 2018; Zhu 2008). See the Characteristics of excluded studies table for further details.
Risk of bias in included studies
We deemed all included studies to be at low or unclear risk for allocation and reporting bias. Two studies each were at high risk of selection bias (Jerjes‐Sánchez 1995; Ly 1978), performance and detection bias (Goldhaber 1993; Taherkhani 2014), and attrition bias (Ly 1978; Tibbutt 1974), and seven studies were at high risk of other bias (Dotter 1979; Jerjes‐Sánchez 1995; Kline 2014; Kucher 2014; Meyer 2014; Taherkhani 2014; Tibbutt 1974). Only Meyer 2014 provided sufficient detail for assessment of all domains as having low or high risk of bias, and Marini 1988 and Sharifi 2013 did not provide enough information on any domain to allow a clear determination of risk. Furthermore, for four studies, all domains had either unclear or high risk of bias (Dotter 1979; Kucher 2014; Ly 1978; Tibbutt 1974).
All in all, we identified for inclusion in this review four studies with high risk of overall bias, that is, two or more assessment domains carried high risk of bias (Jerjes‐Sánchez 1995; Ly 1978; Taherkhani 2014; Tibbutt 1974). We therefore conducted a sensitivity analysis that excluded these studies. See Figure 2 and Figure 3 for a summary of the general risk of bias of included studies.
2.

Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
3.
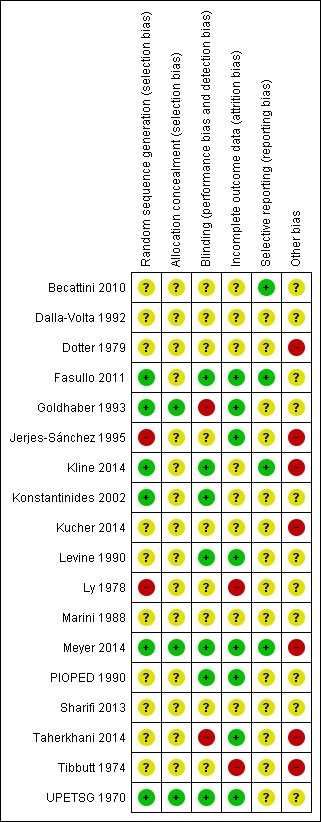
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
Six trials clearly described appropriate random sequence generation (Fasullo 2011; Goldhaber 1993; Kline 2014; Konstantinides 2002; Meyer 2014; UPETSG 1970), and nine trials did not (Becattini 2010; Dalla‐Volta 1992; Dotter 1979; Kucher 2014; Levine 1990; PIOPED 1990; Sharifi 2013; Taherkhani 2014; Tibbutt 1974). Although two studies used the appropriate method to generate the sequence, Ly 1978 did not randomise five included participants (four in the streptokinase group, one in the heparin group), and numbers were unbalanced between the intervention group and the control group at the onset of PE in Jerjes‐Sánchez 1995. Therefore, we judged these two studies as having high risk for selection bias.
Only three of the 18 trials described adequate allocation concealment (Goldhaber 1993; Meyer 2014; UPETSG 1970). Twelve trials poorly reported methods, mainly by omitting any mention of allocation concealment (Becattini 2010; Dalla‐Volta 1992; Dotter 1979; Fasullo 2011; Jerjes‐Sánchez 1995; Konstantinides 2002; Kucher 2014; Levine 1990; Marini 1988; PIOPED 1990; Taherkhani 2014; Tibbutt 1974). Three trials reported using sealed envelopes during concealment, but their descriptions were not detailed enough (sequential numbering and opaqueness) to allow a definitive judgement (Kline 2014; Ly 1978; Sharifi 2013). We contacted trial authors for further clarification but received no response.
Blinding
Seven trials reported single blinding (Becattini 2010; Dalla‐Volta 1992; Kucher 2014; Ly 1978; Sharifi 2013; Taherkhani 2014; Tibbutt 1974), and seven trials used double‐blinding (Fasullo 2011; Kline 2014; Konstantinides 2002; Levine 1990; Meyer 2014; PIOPED 1990; UPETSG 1970). Three trials did not document blinding (Dotter 1979; Jerjes‐Sánchez 1995; Marini 1988), and one trial was non‐blinded (Goldhaber 1993). Taherkhani 2014 reported that blinding was broken, so we assigned it high risk of bias.
Incomplete outcome data
Apart from Dalla‐Volta 1992 and Dotter 1979, all trials either described the withdrawal rate or provided sufficient information for this to be calculated. Withdrawal rates varied from 0% in Fasullo 2011, Jerjes‐Sánchez 1995, Levine 1990, PIOPED 1990, Taherkhani 2014, and UPETSG 1970, to 45% in Ly 1978 (among participants with an angiographic response to 72 hours of treatment in the heparin group) and 63% in Tibbutt 1974 (for long‐term follow‐up at six months; data unstable between different follow‐up periods). The remaining two studies described post‐randomisation exclusions well (Goldhaber 1993; Meyer 2014).
Selective reporting
Four studies had low reporting bias according to their study protocols (Becattini 2010; Fasullo 2011; Kline 2014; Meyer 2014). We were unable to access the protocols of the remaining included studies, so we could not assess their risk of selective reporting bias.
Other potential sources of bias
We judged seven trials to be at high risk of other bias, and the rest carried unclear risk. Reasons included small sample size, potential conflicts of interest, inconsistent randomisation, and non‐ITT methods of analysing outcome data. First, all included studies had relatively small sample sizes. The largest sample size in the included studies was 1006 participants (Meyer 2014), and the smallest was only eight (Jerjes‐Sánchez 1995). The limited number of participants could introduce a potential sources of bias. Likewise, pharmaceutical companies funded some studies, which may constitute a conflict of interest, even though some study authors state there was no influence from these companies during the whole study period (Dotter 1979; Kline 2014; Kucher 2014; Meyer 2014). Taherkhani 2014 included a small sample size, and although 59 participants had submassive pulmonary thromboembolism, only 50 participants were randomised. In the same way, Tibbutt 1974 included a small sample size, and two participants were transferred from the control group to the treatment group; moreover, investigators did not analyse outcome data on an ITT basis. Therefore, we assessed these studies as having high risk of other potential bias.
Effects of interventions
See: Table 1
Of the 18 trials that matched the inclusion criteria of this review, we were not able to include one trial in the meta‐analysis because it provided no data that we could extract (Marini 1988). Therefore, our meta‐analysis included 17 trials with a total of 2167 participants. We analysed primary outcome measures on an ITT basis. We analysed all participants who dropped out of the study according to their original group, regardless of whether or not they completed or received that treatment.
Primary outcome measures
Death from all causes
The 17 trials included in the meta‐analysis reported a total of 83 deaths: 30 in the thrombolytics group and 53 in the heparin group. Pooled analyses show that across all studies, giving thrombolytics reduced the incidence of death (OR 0.57, 95% CI 0.37 to 0.87, 2167 participants, P = 0.01, low‐quality evidence; Analysis 1.1). The analysis showed that statistical heterogeneity between studies was at a low level (Chi² = 12.08, P = 0.74, I² = 0%). However, after we excluded the studies at high risk of bias as part of the sensitivity analysis (Jerjes‐Sánchez 1995; Ly 1978; Taherkhani 2014; Tibbutt 1974), we found no clear evidence to support a difference between the two groups for mortality (OR 0.66, 95% CI 0.42 to 1.06, 2054 participants, P = 0.08; Analysis 2.1). The analysis still shows that statistical heterogeneity between studies was at a low level (Chi² = 6.76, P = 0.87, I² = 0%). Because some studies carried high risk of bias, we downgraded the quality of evidence for this outcome from high to low (Table 1). We also performed a subgroup analysis according to different types of PE (massive/submassive/unknown types of PE) and found no clear subgroup effects between subgroups (P = 0.31). Only the massive PE subgroup showed that thrombolytic therapy may have an effect on death (Analysis 3.1). We found no clear evidence to support a difference between thrombolytic therapy and heparin for death in the other subgroups.
1.1. Analysis.
Comparison 1 Thrombolytic therapy versus heparin: primary outcome measures, Outcome 1 Death from all causes.
2.1. Analysis.
Comparison 2 Thrombolytic therapy versus heparin: primary outcome measures (sensitivity analysis according to study quality), Outcome 1 Death from all causes.
3.1. Analysis.
Comparison 3 Thrombolytic therapy versus heparin: primary outcome measures (subgroup analysis according to types of PE), Outcome 1 Death from all causes.
An additional report of Meyer 2014 included for this 2018 update described long‐term mortality rates for patients with intermediate‐risk PE. Researchers in this study followed about 70% of participants over two years (median 37.8 months) and reported that tenecteplase treatment did not affect long‐term mortality rates compared to placebo and heparin. We were unable to include the data in our meta‐analysis as the other included studies reported short‐term mortality (follow‐up period less than three months for most studies). Further analyses may be possible for future updates.
Recurrence of pulmonary emboli
Ten studies reported on the recurrence of pulmonary emboli (Becattini 2010; Dalla‐Volta 1992; Dotter 1979; Fasullo 2011; Goldhaber 1993; Konstantinides 2002; Levine 1990; Meyer 2014; Sharifi 2013; UPETSG 1970). Pooled data comparing thrombolytics versus heparin show that the thrombolytics group experienced less recurrence than the heparin group (OR 0.51, 95% CI 0.29 to 0.89, 1898 participants, P = 0.02, low‐quality evidence; Analysis 1.2). Analyses show that statistical heterogeneity between studies was at a low level (Chi² = 5.27, P = 0.73, I² = 0%). We did not perform a sensitivity analysis, as the studies identified as having high risk of bias did not report this outcome. However, for most included studies, we downgraded the quality of evidence for this outcome from high to low for high risk of selection, performance, and detection bias (Table 1). We also performed a subgroup analysis according to different types of PE (submassive/unknown types of PE) and found no conclusive evidence showing a difference between subgroups (P = 0.33). The 'unknown types of PE' subgroup provided no clear evidence to support a difference between thrombolytic therapy and heparin (Analysis 3.2).
1.2. Analysis.
Comparison 1 Thrombolytic therapy versus heparin: primary outcome measures, Outcome 2 Recurrence of pulmonary emboli.
3.2. Analysis.
Comparison 3 Thrombolytic therapy versus heparin: primary outcome measures (subgroup analysis according to types of PE), Outcome 2 Recurrence of pulmonary emboli.
Major and minor haemorrhagic events
Major haemorrhagic events
Twelve studies reported on major haemorrhagic events (Becattini 2010; Dalla‐Volta 1992; Fasullo 2011; Goldhaber 1993; Kline 2014; Konstantinides 2002; Levine 1990; Ly 1978; Meyer 2014; PIOPED 1990; Tibbutt 1974; UPETSG 1970). The total number of these events was 134: 98 in the thrombolytics group and 36 in the heparin group. Pooled analyses show that across 12 studies comparing thrombolytics versus heparin, more major bleeding events occurred after treatment with thrombolytics (OR 2.90, 95% CI 1.95 to 4.31, 1897 participants, P < 0.0001, low‐quality evidence; Analysis 1.3). The result was not changed even after Ly 1978 and Tibbutt 1974 were excluded for high risk of bias (OR 3.00, 95% CI 1.99 to 4.53, 1842 participants, P < 0.0001; Analysis 2.2). Analysis shows low levels of statistical heterogeneity between studies both before (Chi² = 10.70, P = 0.38, I² = 7%) and after (Chi² = 10.16, P = 0.25, I² = 21%) the sensitivity analysis. We downgraded the quality of evidence for this outcome from high to low for possible bias (Table 1). We also performed a subgroup analysis according to different types of PE (submassive/unknown types of PE) and found no subgroup effects between subgroups (P = 0.27; Analysis 3.3).
1.3. Analysis.
Comparison 1 Thrombolytic therapy versus heparin: primary outcome measures, Outcome 3 Major haemorrhagic events.
2.2. Analysis.
Comparison 2 Thrombolytic therapy versus heparin: primary outcome measures (sensitivity analysis according to study quality), Outcome 2 Major haemorrhagic events.
3.3. Analysis.
Comparison 3 Thrombolytic therapy versus heparin: primary outcome measures (subgroup analysis according to types of PE), Outcome 3 Major haemorrhagic events.
Minor haemorrhagic events
Ten studies reported on minor haemorrhagic events (Becattini 2010; Dalla‐Volta 1992; Fasullo 2011; Kucher 2014; Levine 1990; Ly 1978; Meyer 2014; Taherkhani 2014; Tibbutt 1974; UPETSG 1970). Pooled analyses comparing thrombolytics versus heparin show more minor haemorrhagic events in the thrombolytics group (OR 3.03, 95% CI 1.60 to 5.73, 1553 participants, P < 0.001, very low‐quality evidence; Analysis 1.4). Analyses show that statistical heterogeneity between the included studies was at a substantial level (Chi² = 20.71, P = 0.01, I² = 57%), so we used a random‐effects model for the pooled analysis. After excluding the three studies at high risk of bias (Ly 1978; Taherkhani 2014; Tibbutt 1974), we still observed this difference between the two groups (OR 4.05, 95% CI 2.17 to 7.54, 1448 participants, P < 0.01; Analysis 2.3). We downgraded the quality of evidence for this outcome from high to very low for possible bias and large heterogeneity (Table 1). We also performed a subgroup analysis according to different types of PE (submassive/unknown types of PE) and found a subgroup effect between subgroups (P = 0.007); we found a difference between the two groups in the 'submassive PE' subgroup but not in the 'unknown types of PE' subgroup (Analysis 3.4).
1.4. Analysis.
Comparison 1 Thrombolytic therapy versus heparin: primary outcome measures, Outcome 4 Minor haemorrhagic events.
2.3. Analysis.
Comparison 2 Thrombolytic therapy versus heparin: primary outcome measures (sensitivity analysis according to study quality), Outcome 3 Minor haemorrhagic events.
3.4. Analysis.
Comparison 3 Thrombolytic therapy versus heparin: primary outcome measures (subgroup analysis according to types of PE), Outcome 4 Minor haemorrhagic events.
Secondary outcome measures
Haemodynamic improvement and thrombolysis
Pulmonary arterial systolic pressure improvement
One study compared urokinase versus heparin in 147 participants at 24 hours after treatment (UPETSG 1970), and one study compared streptokinase versus heparin in 21 participants at 72 hours after treatment (Tibbutt 1974); both show that thrombolytic treatment had a small effect on pulmonary arterial systolic pressure improvement (mean difference (MD) ‐4.41 mmHg, 95% CI ‐4.62 to ‐4.20; MD ‐11.60 mmHg, 95% CI ‐20.81 to ‐2.39, respectively; Analysis 4.1). Although not pooled, these results indicate that thrombolytics may decrease pulmonary arterial systolic pressure to a greater extent than heparin, and that the effect is similar for various thrombolytics. However, the high risk of bias attached to Tibbutt 1974 warrants caution when results are interpreted.
4.1. Analysis.
Comparison 4 Thrombolytic therapy versus heparin: haemodynamic outcomes, Outcome 1 Pulmonary arterial systolic pressure improvement (mmHg).
Mean pulmonary arterial pressure improvement
Three studies comparing thrombolytics versus heparin show contradictory results in the improvement in mean pulmonary arterial pressure (PIOPED 1990; Tibbutt 1974; UPETSG 1970). Although rt‐PA versus heparin at 1.5 hours shows no clear effect for thrombolytic treatment according to PIOPED 1990 (MD ‐3.00 mmHg, 95% CI ‐16.91 to 10.91; Analysis 4.2), the remaining two studies reported a small effect on mean pulmonary arterial pressure improvement at 24 and 72 hours in favour of thrombolytic treatment (MD ‐4.41 mmHg, 95% CI ‐4.62 to ‐4.20; MD ‐7.50 mmHg, 95% CI ‐12.80 to ‐2.20, respectively; Analysis 4.2).
4.2. Analysis.
Comparison 4 Thrombolytic therapy versus heparin: haemodynamic outcomes, Outcome 2 Mean pulmonary arterial pressure improvement (mmHg).
Right ventricular end‐diastolic pressure improvement
Two studies show contradictory results with regards to right ventricular end‐diastolic pressure improvement. UPETSG 1970 compared urokinase versus heparin in 142 participants, and after 24 hours, noted a small difference in right ventricular end‐diastolic pressure improvement in favour of thrombolytic treatment (MD ‐2.21 mmHg, 95% CI ‐2.35 to ‐2.07; Analysis 4.3). On the other hand, Tibbutt 1974 compared streptokinase versus heparin in 19 participants, observing no clear difference after 72 hours (MD 1.20 mmHg, 95% CI ‐2.59 to 4.99; Analysis 4.3). However, we judged Tibbutt 1974 to be at high risk of bias in this review, so results must be interpreted with caution.
4.3. Analysis.
Comparison 4 Thrombolytic therapy versus heparin: haemodynamic outcomes, Outcome 3 Right ventricular end‐diastolic pressure improvement (mmHg).
Total pulmonary resistance improvement
UPETSG 1970 compared urokinase versus heparin in 113 participants, finding a small difference in favour of urokinase at 24 hours after treatment (MD ‐0.33 dyn·s·cm‐5, 95% CI ‐0.35 to ‐0.31; Analysis 4.4). Tibbutt 1974 compared streptokinase versus heparin in 12 participants at 72 hours after treatment, finding no clear difference between treatment and control (MD 0.30 dyn·s·cm‐5, 95% CI ‐0.83 to 1.43; Analysis 4.4). PIOPED 1990 compared rt‐PA versus heparin in 13 participants at 1.5 hours after treatment, and although these results favour rt‐PA, no clear difference between the two groups is evident (MD ‐180.00 dyn·s·cm‐5, 95% CI ‐883.55 to 523.55; Analysis 4.4). Again, high risk of bias for Tibbutt 1974 warrants caution when results are interpreted.
4.4. Analysis.
Comparison 4 Thrombolytic therapy versus heparin: haemodynamic outcomes, Outcome 4 Total pulmonary resistance improvement (dyn·s·cm‐5).
Cardiac index improvement (L/min/m²)
Two studies show contradictory results for cardiac index improvement (Tibbutt 1974; UPETSG 1970). Tibbutt 1974 compared streptokinase versus heparin in 13 participants, observing a small difference in cardiac index improvement in favour of heparin (MD ‐0.60, 95% CI ‐1.05 to ‐0.15; Analysis 4.5). UPETSG 1970, which compared urokinase versus heparin in 115 participants, reported a small difference in cardiac index improvement in favour of urokinase (MD 0.20, 95% CI 0.15 to 0.25; Analysis 4.5). Results for Tibbutt 1974 must be interpreted with caution due to high risk of bias.
4.5. Analysis.
Comparison 4 Thrombolytic therapy versus heparin: haemodynamic outcomes, Outcome 5 Cardiac index improvement (L/min/m²).
Other haemodynamic outcomes
UPETSG 1970, with 160 participants, compared urokinase versus heparin at 24 hours after treatment, showing small differences in favour of urokinase in right ventricular systolic pressure (MD ‐6.90 mmHg, 95% CI ‐7.25 to ‐6.55; Analysis 4.6), right arterial mean pressure (MD ‐1.94 mmHg, 95% CI ‐2.05 to ‐1.83; Analysis 4.7), arterial‐venous oxygen difference (MD ‐0.31 vol %, 95% CI ‐0.37 to ‐0.25; Analysis 4.8), and arterial PO₂ (MD 8.45 mmHg, 95% CI 7.84 to 9.06; Analysis 4.9).
4.6. Analysis.
Comparison 4 Thrombolytic therapy versus heparin: haemodynamic outcomes, Outcome 6 Right ventricular systolic pressure improvement (mmHg) at 24 hours.
4.7. Analysis.
Comparison 4 Thrombolytic therapy versus heparin: haemodynamic outcomes, Outcome 7 Right arterial mean pressure improvement (mmHg) at 24 hours.
4.8. Analysis.
Comparison 4 Thrombolytic therapy versus heparin: haemodynamic outcomes, Outcome 8 Arterial‐venous oxygen difference (vol %) at 24 hours.
4.9. Analysis.
Comparison 4 Thrombolytic therapy versus heparin: haemodynamic outcomes, Outcome 9 Arterial PO₂ (mmHg) improvement at 24 hours.
Perfusion lung scanning
UPETSG 1970 compared urokinase versus heparin, expressing perfusion defects as a percentage of total normal perfusion of both lungs. At days 1 and 2, results show a difference in favour of urokinase (day 1: MD 3.50%, 95% CI 1.32 to 5.68; Analysis 5.1; day 2: MD 3.10%, 95% CI 0.15 to 6.05; Analysis 5.2). Subsequent results include the following: at day 5: MD 2.00% (95% CI ‐1.60 to 5.60; Analysis 5.3); at day 14: MD 0.20% (95% CI ‐4.26 to 4.66; Analysis 5.5); and at one year MD ‐1.10% (95% CI ‐7.57 to 5.37; Analysis 5.7). These results show that on days 1 and 2 after treatment, either the total normal perfusion of both lungs or the proportion of lung not perfused in those treated with thrombolytics was greater than in those treated with heparin, and on days 5 and 14 and at one year follow‐up, there was no clear effect for urokinase. A second study comparing rt‐PA versus heparin (Goldhaber 1993), in which perfusion defects were expressed as the proportion of lung not perfused, also shows a small effect in favour of rt‐PA at day 1 (MD 0.13%, 95% CI 0.05 to 0.21; Analysis 5.1).
5.1. Analysis.
Comparison 5 Thrombolytic therapy versus heparin: perfusion lung scanning (absolute resolution), Outcome 1 Day 1.
5.2. Analysis.
Comparison 5 Thrombolytic therapy versus heparin: perfusion lung scanning (absolute resolution), Outcome 2 Day 2.
5.3. Analysis.
Comparison 5 Thrombolytic therapy versus heparin: perfusion lung scanning (absolute resolution), Outcome 3 Day 5.
5.5. Analysis.
Comparison 5 Thrombolytic therapy versus heparin: perfusion lung scanning (absolute resolution), Outcome 5 Day 14.
5.7. Analysis.
Comparison 5 Thrombolytic therapy versus heparin: perfusion lung scanning (absolute resolution), Outcome 7 Absolute resolution (1‐year follow‐up).
Dalla‐Volta 1992 compared alteplase plus heparin versus heparin alone, showing no clear effect on total lung score between the two groups at day 7 (MD 1.70, 95% CI ‐1.04 to 4.44; Analysis 5.4); however, results show a small difference in favour of alteplase at day 30 after treatment (MD 2.80, 95% CI 0.35 to 5.25; Analysis 5.6). Comparison of scores in terms of change from baseline in both groups provides no clear evidence to support a difference between the two groups at day 7 or at day 30 (day 7: MD 1.80, 95% CI ‐0.51 to 4.11; Analysis 5.4; day 30: MD 0.70, 95% CI ‐1.37 to 2.77; Analysis 5.6). These results show that alteplase plus heparin and heparin alone can improve total lung scores with similar effect, but at day 30, the score in the alteplase plus heparin group was higher than the score in the heparin alone group.
5.4. Analysis.
Comparison 5 Thrombolytic therapy versus heparin: perfusion lung scanning (absolute resolution), Outcome 4 Day 7.
5.6. Analysis.
Comparison 5 Thrombolytic therapy versus heparin: perfusion lung scanning (absolute resolution), Outcome 6 Day 30.
Levine 1990 compared rt‐PA plus heparin versus placebo plus heparin, showing no difference in the number of participants with greater than 50% improvement on lung scan at 24 hours after treatment (OR 3.84, 95% CI 0.94 to 15.73; Analysis 6.1). We could not estimate this in the PIOPED 1990 study.
6.1. Analysis.
Comparison 6 Thrombolytic therapy versus heparin: number of patients with greater than 50% improvement on lung scan, Outcome 1 Day 1.
Pulmonary angiogram assessment
Researchers evaluated pulmonary angiograms using the Miller index (Miller 1971). The overall total score for pulmonary angiograms in the Dalla‐Volta 1992 study shows a small reduction in the alteplase plus heparin group (MD ‐3.4, 95% CI ‐4.72 to ‐2.08; Analysis 7.1).
7.1. Analysis.
Comparison 7 Thrombolytic therapy versus heparin: pulmonary angiogram assessment, Outcome 1 Change from baseline at 2 hours.
Ly 1978 and Tibbutt 1974 compared streptokinase versus heparin, and, when pooled, results show a small difference in angiographic score changes from baseline to 72 hours in favour of streptokinase (MD ‐9.3, 95% CI ‐12.81 to ‐5.78; Analysis 7.2). This indicates that changes in angiographic score from baseline to 72 hours after treatment were greater in participants treated with streptokinase than in those treated with heparin. These results must be interpreted with caution, because both studies carried high risk of bias according to our review criteria.
7.2. Analysis.
Comparison 7 Thrombolytic therapy versus heparin: pulmonary angiogram assessment, Outcome 2 Change from baseline at 72 hours.
Echocardiograms
Five studies performed echocardiograms (Becattini 2010; Fasullo 2011; Goldhaber 1993; Kucher 2014; Taherkhani 2014). Goldhaber 1993 compared rt‐PA plus heparin versus heparin alone; panellists decided by consensus whether right ventricular wall motion was normal or mildly (1+), moderately (2+), or severely (3+) hypokinetic. Tricuspid regurgitation was visually assessed according to the size of the largest colour doppler jet as absent, mild (1+), moderate (2+), or severe (3+). This study shows that the rt‐PA group had increased numbers of participants with improved right ventricular wall movement (OR 2.90, 95% CI 0.98 to 8.60 at 3 hours; OR 3.20, 95% CI 1.20 to 8.57 at 24 hours; Analysis 8.1) and tricuspid regurgitation (OR 6.35, 95% CI 1.90 to 21.17 at 3 hours; OR 3.20, 95% CI 1.20 to 8.57 at 24 hours; Analysis 8.2).
8.1. Analysis.
Comparison 8 Thrombolytic therapy versus heparin: echocardiograms, Outcome 1 Right ventricular wall movement improvement.
8.2. Analysis.
Comparison 8 Thrombolytic therapy versus heparin: echocardiograms, Outcome 2 Tricuspid regurgitation improvement.
Fasullo 2011 compared alteplase plus heparin versus heparin alone, assessing inferior vein cava, doppler acceleration time, paradoxical systolic septal motion, tricuspid annular plane systolic excursion, and B‐type natriuretic peptide (BNP) values (at baseline; at 24, 48, and 72 hours; at six days; at discharge; and at three months and six months). Investigators found earlier improvement in the thrombolytics group in comparison with the placebo group, with evident differences after 24 hours that lasted throughout hospitalisation and during the follow‐up period. Another study compared USAT (rt‐PA) plus heparin versus heparin alone (Kucher 2014), reporting the right‐to‐left ventricular dimension (RV/LV) ratio at 24 hours and at three months as a primary outcome. Results show a difference between the two groups at 24 hours, but at three months, they show no clear effect for the rt‐PA group (P = 0.36). This study also shows that USAT (rt‐PA) had better outcomes at 24 hours than at three months in terms of tricuspid annular systolic excursion, right ventricular‐to‐left ventricular pressure gradient, and minimum inferior vena cava diameter. Taherkhani 2014 compared alteplase or streptokinase plus enoxaparin versus enoxaparin alone. This study reported no clear effect differences between the two groups in normalisation of the RV.
In this review, we found that after treatment, most echocardiogram parameters were better in the thrombolytics group than in the control group. For example, Fasullo 2011 reported the paradoxical systolic septal motion (OR 0.24, 95% CI 0.07 to 0.82 at 24 hours; OR 0.35, 95% CI 0.13 to 0.92 at 48 hours; OR 0.29, 95% CI 0.10 to 0.88 at 72 hours; OR 0.12, 95% CI 0.01 to 2.49 at six days; Analysis 8.3); Fasullo 2011 and Kucher 2014 reported right‐to‐left ventricular ratio at 24 hours after treatment (MD ‐0.13, 95% CI ‐0.16 to ‐0.11); and Fasullo 2011 reported additional time points: 48 hours (MD ‐0.19, 95% CI ‐0.20 to ‐0.18), 72 hours (MD ‐0.14, 95% CI ‐0.15 to ‐0.13), six days (MD ‐0.22, 95% CI ‐0.23 to ‐0.21), discharge (MD ‐0.33, 95% CI ‐0.34 to ‐0.32), three months (MD ‐0.14, 95% CI ‐0.34 to 0.05; pooled Fasullo 2011 and Kucher 2014), and six months (MD ‐0.21, 95% CI ‐0.22 to ‐0.20) (see Analysis 8.4). Researchers reported similar time points for tricuspid annular plane systolic excursion: 24 hours (MD 0.45, 95% CI ‐1.18 to 2.07; pooled Fasullo 2011 and Kucher 2014), 48 hours (MD 1.00, 95% CI ‐0.13 to 2.13), 72 hours (MD 1.80, 95% CI 0.67 to 2.93), six days (MD 2.50, 95% CI 1.57 to 3.43), discharge (MD 2.00, 95% CI 0.75 to 3.25), three months (MD 0.33, 95% CI ‐3.18 to 3.85; pooled Fasullo 2011 and Kucher 2014), and six months (MD 1.30, 95% CI 0.28 to 2.32) (see Analysis 8.5). Kucher 2014 reported the right ventricular‐to‐right atrial pressure gradient (MD ‐6.30, 95% CI ‐13.06 to 0.46 at 24 hours; MD 3.20, 95% CI ‐4.77 to 11.17 at three months; Analysis 8.6) and the minimum inferior vena cava diameter (MD ‐6.60, 95% CI ‐9.36 to ‐3.84 at 24 hours; MD ‐0.50, 95% CI ‐2.79 to 1.79 at three months; Analysis 8.7).
8.3. Analysis.
Comparison 8 Thrombolytic therapy versus heparin: echocardiograms, Outcome 3 Paradoxical systolic septal motion.
8.4. Analysis.
Comparison 8 Thrombolytic therapy versus heparin: echocardiograms, Outcome 4 Right ventricle‐to‐left ventricle ratio.
8.5. Analysis.
Comparison 8 Thrombolytic therapy versus heparin: echocardiograms, Outcome 5 Tricuspid annular plane systolic excursion.
8.6. Analysis.
Comparison 8 Thrombolytic therapy versus heparin: echocardiograms, Outcome 6 Right ventricular‐to‐right atrial pressure gradient.
8.7. Analysis.
Comparison 8 Thrombolytic therapy versus heparin: echocardiograms, Outcome 7 Minimum inferior vena cava diameter.
BNP values show faster reduction in the thrombolytics group than in the placebo group during hospitalisation at six days after admission. Becattini 2010 also reported reduction in echocardiography parameters and found small differences in decreases in both right ventricle end‐diastolic dimension and the right‐to‐left end‐diastolic dimension ratio at 24 hours in favour of tenecteplase, but the difference was not maintained during the seven‐day follow‐up period (data were unavailable). These figures indicate that treatment with thrombolytics plus heparin results in more participants with improved right ventricular wall movement and tricuspid regurgitation than treatment with heparin alone.
Chronic thromboembolic pulmonary hypertension
Only three studies compared thrombolytic therapy plus heparin versus heparin alone in terms of pulmonary hypertension (Fasullo 2011; Sharifi 2013; Taherkhani 2014). Fasullo 2011 reported that participants in the thrombolytics group had lower pulmonary hypertension than participants in the heparin group at 24 hours (MD ‐8.00, 95% CI ‐14.76 to ‐1.24). Fasullo 2011 and Sharifi 2013 reported the outcome at 48 hours (MD ‐7.37, 95% CI ‐9.20 to ‐5.53), and Fasullo 2011 reported the outcome at 72 hours (MD ‐8.00, 95% CI ‐11.74 to ‐4.26). Fasullo 2011 and Taherkhani 2014 reported at six days (MD ‐5.69, 95% CI ‐9.37 to ‐2.02); Fasullo 2011 at discharge (MD ‐8.00, 95% CI ‐9.78 to ‐6.22) and at three months (MD ‐7.00, 95% CI ‐17.18 to 3.18); Fasullo 2011 and Sharifi 2013 at six months (MD ‐11.95, 95% CI ‐23.71 to ‐0.19); and Sharifi 2013 at 28 months (MD ‐15.00, 95% CI ‐17.32 to ‐12.68) (see Analysis 8.8).
8.8. Analysis.
Comparison 8 Thrombolytic therapy versus heparin: echocardiograms, Outcome 8 Pulmonary hypertension.
Differences in coagulation parameters over time
Fibrinogen
Two studies comparing thrombolytic versus heparin treatment at less than three hours after treatment show a small difference in fibrinogen levels in favour of thrombolytics (total MD ‐2.68 g/L, 95% CI ‐4.36 to ‐1.00; Analysis 9.1; Dalla‐Volta 1992; PIOPED 1990). However, we found no clear evidence to support a difference between the two groups at 24 hours (MD ‐1.61 g/L, 95% CI ‐3.99 to 0.76) nor at 48 hours (MD ‐0.60 g/L, 95% CI ‐1.40 to 0.20) after treatment (see Analysis 9.1). This indicates that thrombolytic treatment results in a lower level of fibrinogen than heparin treatment. Levine 1990 also reported this comparison; however, we could not extract the data from this study, as it reported changes in mean fibrinogen levels in a figure, showing that the thrombolytics group had a lower level of fibrinogen than the placebo group.
9.1. Analysis.
Comparison 9 Thrombolytic therapy versus heparin: haemocoagulation variables, Outcome 1 Fibrinogen (g/L).
D‐dimer
As a molecular marker of haemostatic activation, D‐dimer indicates fibrin turnover both from intravascular fibrin formation and from subsequent lysis of a fibrin clot. Results show a difference between participants treated with thrombolytics plus heparin and those treated with heparin alone in two studies at two hours after treatment (MD 21.04 µg/mL, 95% CI ‐4.60 to 46.69; Analysis 9.2; Dalla‐Volta 1992; PIOPED 1990), and in one study at 24 hours after treatment (MD 5.30 µg/mL, 95% CI 2.12 to 8.48; Analysis 9.2; Dalla‐Volta 1992). These results show that D‐dimer concentrations were higher in the thrombolytics plus heparin group than in the heparin alone group.
9.2. Analysis.
Comparison 9 Thrombolytic therapy versus heparin: haemocoagulation variables, Outcome 2 D‐dimer (µg/mL).
Plasminogen
Dalla‐Volta 1992 reported a difference in concentrations of plasminogen at two hours (MD ‐60.30%, 95% CI ‐71.92 to ‐48.68) and at 24 hours (MD ‐36.00%, 95% CI ‐48.06 to ‐23.94) after treatment in favour of alteplase (see Analysis 9.3). This shows that treatment with alteplase plus heparin results in a lower plasminogen concentration than treatment with heparin alone.
9.3. Analysis.
Comparison 9 Thrombolytic therapy versus heparin: haemocoagulation variables, Outcome 3 Plasminogen (%).
Post‐thrombotic syndrome
No data were available for this outcome. If data become available, we will include them in future updates.
Escalation of treatment
Two studies reported the number of participants who needed escalation of treatment after receiving thrombolytics versus heparin (Konstantinides 2002; Taherkhani 2014). Konstantinides 2002 compared alteplase plus heparin versus heparin alone, finding that fewer participants in the alteplase plus heparin group needed escalation of treatment for in‐hospital events compared with the heparin alone group. Pooling these data with data from alteplase or streptokinase plus enoxaparin versus enoxaparin alone (Taherkhani 2014), we found that results still show a small difference in favour of alteplase (OR 0.32, 95% CI 0.16 to 0.64, P = 0.001; Analysis 10.1).This indicates that fewer participants required rescue thrombolysis in the thrombolytic plus heparin group than in the heparin alone group.
10.1. Analysis.
Comparison 10 Thrombolytic therapy versus heparin: other outcomes, Outcome 1 Escalation of treatment.
Hospital stay
Three studies that compared thrombolytics versus heparin reported length of hospital stay (Kucher 2014; Sharifi 2013; Taherkhani 2014). Analyses show that statistical heterogeneity between included studies was at a considerable level (Chi² = 45.89, P < 0.001, I² = 96%), and given the heterogeneity of the interventions, we used a random‐effects model for the pooled analysis. Regarding the delivery technique for the thrombolytic drug, one study used the USAT system (Kucher 2014), whereas a second study delivered a 'safe dose' of rt‐PA through intravenous injection (Sharifi 2013), and the last study used alteplase or streptokinase (Taherkhani 2014). Pooled analysis of the three studies yielded no clear evidence to support a difference between the two groups in length of hospital stay (MD ‐0.89, 95% CI ‐3.13 to 1.34; Analysis 10.2).
10.2. Analysis.
Comparison 10 Thrombolytic therapy versus heparin: other outcomes, Outcome 2 Hospital stay.
Survival time
Duration of follow‐up varied, and researchers reported deaths up to 72 hours (Tibbutt 1974), 10 days (Levine 1990), 14 days (Goldhaber 1993; Ly 1978; UPETSG 1970), 19 days (PIOPED 1990), 30 days (Dalla‐Volta 1992; Konstantinides 2002), and 180 days after randomisation (Fasullo 2011). Fasullo 2011 and Konstantinides 2002 show a beneficial effect of thrombolytics over control in clinical event‐free survival time. The other studies did not report this outcome. However, we could not extract available data from the two studies to conduct a pooled analysis because they provided only a figure for survival time. Thus we cannot draw a specific conclusion on survival time nor on thrombolytic effects on death.
Composite clinical outcome
Two studies reported the important composite clinical outcome (Kline 2014; Meyer 2014). Meyer 2014 reported all‐cause death or haemodynamic decompensation, and Kline 2014 reported recurrent venous thromboembolism (VTE), poor functional capacity, and low perception of wellness as measured by the 36‐item Short Form Health Survey (SF‐36). Analysis shows more death and haemodynamic decompensation events in the placebo group than in the thrombolytics group (OR 0.44, 95% CI 0.23 to 0.87; Analysis 10.3). However, we found no clear evidence to support a difference between the two groups in terms of other outcomes. As Kline 2014 and Meyer 2014 reported different composite clinical outcomes, it is not appropriate to pool these composite results.
10.3. Analysis.
Comparison 10 Thrombolytic therapy versus heparin: other outcomes, Outcome 3 Composite clinical outcome.
Quality of life
One study reported participants' quality of life (QoL) in the follow‐up period (Kline 2014). Kline 2014 reported the number of participants who remained in the intensive care unit on day 2 and the QoL as measured by the VEINES QoL score and SF‐36. This study shows that QoL was similar between the two treatment groups.
Healthcare cost comparison
None of the included trials reported on cost comparison. If data become available, we will report this information in future updates.
Discussion
Summary of main results
We have described the main results in Table 1.
Outcomes analysed
Overall, results for included outcomes were unsatisfactory and susceptible to bias due to the fact that most outcomes in the subgroups were extracted from only one or two studies. Most studies included small sample sizes, and some had low methodological quality. Upon assessing all of the included studies in this update, we found only three studies with four or more bias domains assessed as having low risk of bias (Fasullo 2011; Meyer 2014; UPETSG 1970). However, Meyer 2014 received funds from several companies, which may have caused conflicts of interest. In addition, some trials did not assess the most important outcomes defined in this review or did not evaluate the potential complications of thrombolytic therapy.
Clinical interpretation of the data
Thrombolytic agents showed benefit in terms of death compared with heparin (OR 0.57, 95% CI 0.37 to 0.87, P = 0.01) and reduced the odds ratio for recurrence of PE (OR 0.51, 95% CI 0.29 to 0.89, P = 0.02). However, upon excluding four studies at high risk of bias, we found no clear evidence to support a difference between the two groups in risk of death (OR 0.66, 95% CI 0.42 to 1.06, P = 0.08). Results show more major and minor haemorrhagic events in the thrombolytics group than in the control group (OR 2.90, 95% CI 1.95 to 4.31, P < 0.001; OR 3.03, 95% CI 1.60 to 5.73, P < 0.001, for major and minor haemorrhagic events, respectively) even after exclusion of trials at high risk of bias for these outcomes. One study reported on stroke, which occurred more often in the thrombolytics group than in the control group (OR 12.10, 95% CI 1.57 to 93.39). The total number of deaths was 83, and the total number of major haemorrhagic events was 56 among 2116 participants over all studies. From the confidence intervals, we can see a relatively precise estimate of treatment effect for recurrence of PE and for major and minor haemorrhagic events. However, the treatment effect for mortality was influenced by exclusion of studies at high risk of bias from the sensitivity analysis, even though only slight alterations in the confidence intervals were evident. Thus, additional studies are needed before firm conclusions can be drawn.
Many of the results for the secondary outcome measures of this review are based on only one or two studies. In addition, studies used different follow‐up periods and interventions, entailing some unavoidable heterogeneity. The very limited results indicate that thrombolytic therapy was better than heparin in terms of improving haemodynamic outcomes, perfusion lung scanning, pulmonary angiogram assessment, and echocardiograms. Given the risk of bias in the included studies and the inconsistent results, we cannot draw a strong conclusion about the benefit of thrombolytic agents versus heparin in this review.
Overall completeness and applicability of evidence
We assessed the effectiveness and safety of thrombolytic therapy for people with acute pulmonary embolism. We found that thrombolytic therapy was better than comparison treatments in reducing the odds ratio of death and recurrence of PE, and it improved some composite clinical outcomes and haemodynamic parameters (perfusion lung scanning, pulmonary angiogram assessment, and echocardiograms). All participants in the included studies were adults aged 18 or over, with a mean age of about 60. However, the included trials did not include strict subgroups of elderly participants. Only Meyer 2014 included a subgroup for participants over 75, and results of this study provide no clear evidence to support a difference between the two groups in death or haemodynamic decompensation (OR 0.63, 95% CI 0.24 to 1.66). On the other hand, tenecteplase increased the odds ratio of major extracranial bleeding (OR 20.38, 95% CI 2.69 to 154.53). Any differences between adults and elderly people therefore need further investigation.
Based on data from Konstantinides 2002, Perlroth 2007 pointed out that the heparin group required treatment escalation approximately three times more often than the thrombolytics group, but researchers observed no difference in the risk of death from PE. Investigators also found that treatment with heparin alone was more effective and less costly than treatment with alteplase plus heparin among participants with submassive PE and right ventricular dysfunction. However, we were not able to show any differences between thrombolytic therapy and the comparison treatment in terms of healthcare costs and post‐thrombotic syndrome, as no included studies reported on these outcomes. In clinical practice, haemodynamic parameters and the age of patients with PE must be considered, especially for haemodynamically unstable patients and patients over 75.
The included studies involved different types of thrombolytics, including alteplase, urokinase, streptokinase, rt‐PA, ultrasound‐assisted catheter‐directed thrombolysis system, and tenecteplase, usually followed by heparin. The control intervention was heparin alone or placebo plus heparin. No studies compared thrombolytics versus surgical intervention.
In this update, we included one additional report of a previously included study (Meyer 2014). The researcher in this study followed about 70% of participants over two years (median 37.8 months) and found that tenecteplase treatment did not affect long‐term mortality among patients with intermediate‐risk PE. This report also provided echocardiography data for only about 30% of participants (144/506 (28.5%) in the tenecteplase group and 146/499 (28.9%) in the control group) with long‐term follow‐up (at least 24 months), showing that tenecteplase treatment did not reveal clear differences in residual pulmonary hypertension nor in RV dysfunction. We could not use these data in our meta‐analysis because the other included studies reported only short‐term (follow‐up period less than three months for most studies) mortality. Using data from this report in the meta‐analysis would have increased heterogeneity too much. Thus, future studies should further investigate the effect of thrombolytic treatment with long‐term follow‐up on mortality.
Thrombolytics for massive PE (haemodynamically unstable patients)
It is clinically very important to differentiate haemodynamically stable and unstable patients (massive PE). However, we have identified only one study to date that compared thrombolytic therapy versus heparin in patients with massive PE (Jerjes‐Sánchez 1995). Four studies included both massive and unknown PE types (Dotter 1979; Ly 1978; Tibbutt 1974; UPETSG 1970). The proportion of massive PE varied, standing at 8% in Ly 1978, 9% in UPETSG 1970, 23% in Tibbutt 1974, and 71% in Dotter 1979. As we did not know the types of PE for all participants included in these studies, we decided to include these four studies in the 'type of PE unknown' group. In PIOPED 1990, all included participations had an unclear PE type. Therefore, we included this study in the same group.
Jerjes‐Sánchez 1995 shows unbalanced allocation in the two groups at onset of PE, so we judged this study as having high risk of bias due to the high risk of selective reporting and the very small sample size. In this RCT, eight participants received 1,500,000 IU of streptokinase in one hour through a peripheral vein followed by heparin or heparin alone. The four participants who were randomised to streptokinase (mean time of onset of symptoms of the first event of PE: 2.5 hours) improved in the first hour after treatment, survived, and over two years of follow‐up did not present with pulmonary arterial hypertension. All four participants treated with heparin alone (mean time of onset of symptoms for the first event of PE: 34.75 hours) died within one to three hours after arrival to the emergency department. We excluded this study along with another three studies at high risk of bias from the sensitivity analysis (Ly 1978; Taherkhani 2014; Tibbutt 1974), and this appreciably influenced the results for all‐cause death between the two groups. Thus, the data from Jerjes‐Sánchez 1995 had a big influence on the pooled analysis. Even though we performed a subgroup analysis according to different types of PE (massive/submassive/unknown types of PE) for the primary outcomes, these results cannot be extrapolated to massive PE due to the limitations of Jerjes‐Sánchez 1995.
Quality of the evidence
We have described the main results in Table 1.
Randomisation and blinding
Only three studies reported both appropriate random sequence generation and allocation concealment (Goldhaber 1993; Meyer 2014; UPETSG 1970), and seven reported satisfactory blinding (Fasullo 2011; Kline 2014; Konstantinides 2002; Levine 1990; Meyer 2014; PIOPED 1990; UPETSG 1970). Goldhaber 1993 reported no blinding, and Taherkhani 2014 indicated that blinding was broken. Although two studies used the appropriate method to generate the random sequence, Ly 1978 included five participants who were not randomised, and Jerjes‐Sánchez 1995 reported unbalanced numbers between intervention and control groups at the onset of PE. The remaining trials did not provide clear details about random sequence generation, allocation concealment, or blinding. Two studies were unclear in all items for risk of bias assessment (Marini 1988; Sharifi 2013), and in four studies, all risk of bias domains were at unclear or high risk (Dotter 1979; Kucher 2014; Ly 1978; Tibbutt 1974). This could have biased study results in favour of treatment.
Sample size
Only one or two studies reported any of the outcome measures, so some effect sizes have a confidence interval over 95% (such as for incidence of stroke). For some outcomes, we may not have been able to detect any real effects of thrombolytics because of small sample size.
Conflicts of interest
Four included studies were funded by related pharmaceutical companies (Dotter 1979; Kline 2014; Kucher 2014; Meyer 2014), and some study authors worked for these companies (Meyer 2014). This could potentially result in conflicts of interest in drafting and reporting results of the study, even though study authors stated there was no influence over the whole study period.
Heterogeneity
Within each subgroup, we used Chi² analyses to test for statistical evidence of heterogeneity among studies, and we used I² to measure the degree of inconsistency across studies. When Chi² analysis was significant and I² values were in excess of 50%, we analysed differences in participant selection, baseline values, risk of bias, design, and methods that could possibly explain the heterogeneity.
Heterogeneity in responses did not appear to result from differences in methods used for most of the primary outcomes (including overall mortality, recurrence of pulmonary emboli, and major haemorrhagic events) nor for some of the secondary outcomes (mean pulmonary arterial pressure improvement, pulmonary angiogram assessment (72 hours after treatment), and echocardiograms). We obtained dynamic measurements from studies comparing thrombolytics versus heparin, showing a similar effect on those outcomes listed above. We found no dose‐related or time‐related relationships in these dynamic analyses.
We noted moderate heterogeneity in dynamic analysis of minor bleeding in studies comparing thrombolytics versus heparin (Becattini 2010; Dalla‐Volta 1992; Fasullo 2011; Kucher 2014; Levine 1990; Ly 1978; Meyer 2014; Taherkhani 2014; Tibbutt 1974; UPETSG 1970), and we found a difference between the two therapies. Therefore, when we use this result in clinical practice, we must consider heterogeneity in the meta‐analysis. A great degree of heterogeneity was present in the dynamic analysis for D‐dimer concentration at two hours after treatment (Dalla‐Volta 1992; PIOPED 1990), pulmonary artery systolic pressure (Fasullo 2011; Sharifi 2013; Taherkhani 2014), and right ventricle‐to‐left ventricle ratio (Fasullo 2011; Kucher 2014), showing differences between the two treatment groups. This may be a consequence of the different types of thrombolytics and heparin used in the two studies (see Characteristics of included studies table).
Due to the above issues, the overall quality of evidence presented in this review is low.
Potential biases in the review process
We analysed outcomes on an ITT basis, using a random‐effects model for pooled analysis of heterogeneous data (I² = 40% to 100%). We did this to reduce the bias of estimated intervention effects.
We classified studies as having high risk of overall bias if two or more risk of bias domains carried high risk of bias. We conducted a sensitivity analysis by excluding these studies to assess the effects of this exclusion on the estimated intervention effect.
Agreements and disagreements with other studies or reviews
Almost all studies show that thrombolytic therapy can reduce the primary outcomes defined by the study, especially echocardiographic parameters. Our meta‐analysis of all included studies shows beneficial results for thrombolysis in terms of death from all causes. However, the sensitivity analysis, from which we which removed studies labelled as having high risk of bias, provides no clear evidence to support a difference between the two groups in terms of death. Results from Jerjes‐Sánchez 1995 show apparent benefit for the thrombolytics group, and removing this study from the sensitivity analysis may explain the changes in results.
In a meta‐analysis in Chatterjee 2014, study authors reported that theirs was the first analysis of thrombolysis in PE with sufficient statistical power to detect associations with a meaningful mortality reduction. However, these investigators included the data from Jerjes‐Sánchez 1995, which we labelled as carrying high risk of bias, Furthermore, Chatterjee 2014 did not perform a sensitivity analysis according to the quality of included studies and did not assess conflicts of interest in the included trials, which also may introduce bias to the review process. According to theCochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), the Peto OR works well when individual odds ratios are close to one (i.e. intervention effects are small), and when events are not particularly common (the ideal event rate is below 1%). In Chatterjee 2014, the range of the OR was 0.03 to 5.80 and the maximum event rate was 100% (4/4) in the control group. Thus, the Peto OR method used by Chatterjee 2014 to pool data may not be the most appropriate way to analyse the data.
Our review included different subgroup analyses compared with Chatterjee 2014 and published guidelines (NICE 2012). In our review, we placed studies that included participants with unclear types of PE into the 'type of PE unknown' group, which was more precise than subgroups used by Chatterjee 2014 and NICE 2012 (namely, unstable/massive and stable/submassive). The National Institute for Health and Care Excellence (NICE) guideline did not reveal obvious reductions in overall mortality in the unstable/massive and stable/submassive PE subgroups (OR 0.52, 95% CI 0.24 to 1.15; OR 0.67, 95% CI 0.30 to 1.51, respectively). Four other reviews did not report obvious reductions in overall mortality, especially for patients with submassive PE or haemodynamically stable patients (Cao 2014; Liu 2014; Marti 2014; Nakamura 2014). Therefore, larger clinical trials focussing on this association are needed.
Authors' conclusions
Implications for practice.
Low‐quality evidence suggests that thrombolytics reduce death following acute pulmonary embolism compared with heparin. The thrombolytic therapies included in this review are heterogeneous. Thrombolytic therapy may be helpful in reducing the recurrence of PE but may cause more major and minor haemorrhagic events and stroke, including intracranial haemorrhage. Trial results show a three‐fold increase in major bleeding, and these results appear robust and not sensitive to the exclusion of lower‐quality studies. We also note that most of the studies included in this review considered patients with submassive PE. Only one study focussed on patients with massive PE, finding an apparent benefit for thrombolysis. More high‐quality double‐blind RCTs are needed to assess the safety and cost‐effectiveness of thrombolytic therapy for patients with acute PE.
Implications for research.
Investigators planning future randomised trials should:
use a study design that incorporates double‐blinding and adequate concealment of treatment allocation;
focus their assessment on common outcomes (e.g. mortality, haemorrhagic events (especially for intracranial haemorrhage), escalation of treatment);
plan and evaluate measures of cost‐effectiveness and quality of life;
define the different types of PE to differentiate clinical subgroups; and
assess differences between different age groups.
What's new
| Date | Event | Description |
|---|---|---|
| 20 September 2018 | New citation required but conclusions have not changed | Searches were rerun. One article related to an included study was identified. Three new ongoing studies were added, and nine additional studies were excluded. No change was made to conclusions |
| 20 September 2018 | New search has been performed | Searches were rerun. One article related to an included study was identified. Three new ongoing studies were added, and nine additional studies were excluded |
History
Protocol first published: Issue 4, 2002 Review first published: Issue 2, 2006
| Date | Event | Description |
|---|---|---|
| 1 September 2015 | New search has been performed | Searches were rerun. Ten additional studies were included, and 15 additional studies were excluded. Three new ongoing studies were added |
| 1 September 2015 | New citation required but conclusions have not changed | Searches were rerun. Ten additional studies were included, and 15 additional studies were excluded. Three new ongoing studies were added. Review text was updated in keeping with Cochrane policy including 'Risk of bias' assessments and 'Summary of findings' tables. Conclusions were not changed |
| 20 April 2010 | New search has been performed | No new trials were found that met the review inclusion criteria. Ten additional trials were excluded. Minor amendments were made, and minor errors were corrected |
| 11 May 2009 | New citation required but conclusions have not changed | Qiukui Hao was added as a review author, and Qin Wang was removed as a review author |
| 8 July 2008 | Amended | Review was converted to new review format |
Notes
The protocol for this review was developed and published under the auspices of the Cochrane Airways Collaborative Review Group. As the scope of treatment of pulmonary embolism was considered to be better suited to the Peripheral Vascular Diseases (PVD) Group, whose scope already included prevention of pulmonary embolism, this review was passed over to the PVD Group. The PVD Group was renamed Cochrane Vascular in July 2015.
The published protocol did not specify methods used for statistical analysis. We have added details of the analysis to the full review. In addition, we have clarified the review objectives.
Acknowledgements
We thank the editorial base and team, including the review group co‐ordinators and editors of Cochrane Vascular, for their advice during the writing of this review.
Appendices
Appendix 1. Database searches
| Source | Search strategy | Hits retrieved |
| CENTRAL via CRSO | #1 MESH DESCRIPTOR Pulmonary Embolism EXPLODE ALL TREES 784 #2 ((lung or pulmonary) near (embol* or clot*) ):TI,AB,KY 3388 #3 MESH DESCRIPTOR Thrombolytic Therapy EXPLODE ALL TREES 1582 #4 MESH DESCRIPTOR Fibrinolytic Agents EXPLODE ALL TREES 11397 #5 MESH DESCRIPTOR Plasminogen Activators EXPLODE ALL TREES 2302 #6 MESH DESCRIPTOR Fibrinolysis EXPLODE ALL TREES 964 #7 (streptokinase or urokinase or alteplase ):TI,AB,KY 2846 #8 (9 thromboly* or fibrinoly* ):TI,AB,KY 5077 #9 (avelizin or awelysin or celiase or distreptase or kabikinase or kabivitrum or streptase or streptodecase or apsac or anistreplase or monteplase or apsac):TI,AB,KY 216 #10 (avelizin or awelysin or celiase or distreptase or kabikinase or kabivitrum or streptase or streptodecase or apsac or anistreplase or monteplase or apsac):TI,AB,KY 216 #11 (activase or saruplase or retavase or abbokinase or abbokinase or renokinase or u‐pa ):TI,AB,KY 94 #12 ((clot* or thrombus) near3 (lyse or lysis or dissolv* or dissolution)):TI,AB,KY 1149 #13 (tPA or t‐PA or rtPA or rt‐PA or plasminogen or plasmin or alteplase or actilyse):TI,AB,KY 5649 #14 (anistreplase or streptodornase or pro‐urokinase or prourokinase or pro‐uk or lumbrokinase or duteplase or lanoteplase or pamiteplase or reteplase or saruplase or staphylokinase or streptase or tenecteplase or desmoteplase or retevase):TI,AB,KY 720 #15 #1 OR #2 3388 #16 #3 OR #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 18011 #17 #15 AND #16 852 #18 01/01/2015 TO 16/04/2018:CD 301940 #19 #17 AND #18 130 |
130 |
| Clinicaltrials.gov | Pulmonary Embolism | Thrombolytic Therapy OR Fibrinolytic Agents OR Plasminogen Activators OR Fibrinolysis | Last update posted from 01/01/2015 to 04/16/2018 | 54 |
| ICTRP Search Portal | Pulmonary Embolism | Thrombolytic Therapy OR Fibrinolytic Agents OR Plasminogen Activators OR Fibrinolysis | Last update posted from 01/01/2015 to 04/16/2018 | 2 |
| MEDLINE | 1 exp Pulmonary Embolism/ 36003 2 ((lung or pulmonary) adj2 (embol* or clot*)).ti,ab. 35371 3 exp Thrombolytic Therapy/ 22206 4 exp Fibrinolytic Agents/ 160854 5 exp Plasminogen Activators/ 38114 6 exp FIBRINOLYSIS/ 20624 7 (streptokinase or urokinase or alteplase).ti,ab. 21720 8 (thromboly* or fibrinoly*).ti,ab. 62774 9 (avelizin or awelysin or celiase or distreptase or kabikinase or kabivitrum or streptase or streptodecase or apsac or anistreplase or monteplase or apsac).ti,ab. 606 10 (activase or saruplase or retavase or abbokinase or abbokinase or renokinase or u‐pa).ti,ab. 1981 11 ((clot* or thrombus) adj3 (lyse or lysis or dissolv* or dissolution)).ti,ab. 3704 12 (tPA or t‐PA or rtPA or rt‐PA or plasminogen or plasmin or alteplase or actilyse).ti,ab. 63992 13 (anistreplase or streptodornase or pro‐urokinase or prourokinase or pro‐uk or lumbrokinase or duteplase or lanoteplase or pamiteplase or reteplase or saruplase or staphylokinase or streptase or tenecteplase or desmoteplase or retevase).ti,ab. 2539 14 1 or 2 50623 15 or/3‐13 243510 16 14 and 15 9731 17 randomized controlled trial.pt. 458772 18 controlled clinical trial.pt. 92329 19 randomized.ab. 408806 20 placebo.ab. 188173 21 drug therapy.fs. 2009606 22 randomly.ab. 288659 23 trial.ab. 424894 24 groups.ab. 1784447 25 or/17‐24 4182932 26 exp animals/ not humans.sh. 4446637 27 25 not 26 3615036 28 16 and 27 5424 29 (2017* or 2018*).ed. 1223989 30 28 and 29 250 |
250 |
| EMBASE | 1 exp lung embolism/ 67294 2 ((lung or pulmonary) adj2 (embol* or clot*)).ti,ab. 41964 3 1 or 2 73248 4 exp fibrinolytic therapy/ 19279 5 exp fibrinolytic agent/ 88683 6 exp plasminogen activator/ 52157 7 exp fibrinolysis/ 47735 8 (streptokinase or urokinase or alteplase).ti,ab. 16492 9 (thromboly* or fibrinoly).ti,ab. 39427 10 (avelizin or awelysin or celiase or distreptase or kabikinase or kabivitrum or streptase or streptodecase or apsac or anistreplase or monteplase or apsac).ti,ab. 154 11 (activase or saruplase or retavase or abbokinase or abbokinase or renokinase or u‐pa).ti,ab. 1367 12 ((clot* or thrombus) adj3 (lyse or lysis or dissolv* or dissolution)).ti,ab. 3633 13 (tPA or t‐PA or rtPA or rt‐PA or plasminogen or plasmin or alteplase or actilyse).ti,ab. 56227 14 (anistreplase or streptodornase or pro‐urokinase or prourokinase or pro‐uk or lumbrokinase or duteplase or lanoteplase or pamiteplase or reteplase or saruplase or staphylokinase or streptase or tenecteplase or desmoteplase or retevase).ti,ab. 2024 15 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 148573 16 3 and 15 11379 17 randomized controlled trial/ 450402 18 controlled clinical trial/ 414396 19 random$.ti,ab. 1155905 20 randomization/ 69465 21 intermethod comparison/ 223864 22 placebo.ti,ab. 220739 23 (compare or compared or comparison).ti. 331992 24 ((evaluated or evaluate or evaluating or assessed or assess) and (compare or compared or comparing or comparison)).ab. 1600366 25 (open adj label).ti,ab. 61988 26 ((double or single or doubly or singly) adj (blind or blinded or blindly)).ti,ab. 156621 27 double blind procedure/ 122146 28 parallel group$1.ti,ab. 19377 29 (crossover or cross over).ti,ab. 71409 30 ((assign$ or match or matched or allocation) adj5 (alternate or group$1 or intervention$1 or patient$1 or subject$1 or participant$1)).ti,ab. 246607 31 (assigned or allocated).ti,ab. 287439 32 (controlled adj7 (study or design or trial)).ti,ab. 259032 33 (volunteer or volunteers).ti,ab. 170768 34 trial.ti. 211866 35 or/17‐34 3442314 36 16 and 35 1938 37 (2017* or 2018*).em. 3287804 38 36 and 37 343 39 from 38 keep 1‐343 343 |
343 |
| CINAHL | S33 S31 AND S32 11 S32 EM 2017 OR EM 2018 316,418 S31 S17 AND S30 347 S30 S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 337,738 S29 (MH "Random Assignment") 37,749 S28 (MH "Single‐Blind Studies") or (MH "Double‐Blind Studies") or (MH "Triple‐Blind Studies") 32,593 S27 (MH "Crossover Design") 11,101 S26 (MH "Factorial Design") 913 S25 (MH "Placebos") 8,343 S24 (MH "Clinical Trials") 93,075 S23 TX "multi‐centre study" OR "multi‐center study" OR "multicentre study" OR "multicenter study" OR "multi‐site study" 4,382 S22 TX crossover OR "cross‐over" 14,383 S21 AB placebo* 27,963 S20 TX random* 216,161 S19 TX trial* 247,115 S18 TX "latin square" 141 S17 S3 AND S16 1,371 S16 S4 OR S5 OR S6 OR S7 OR S8 OR S9 OR S10 OR S11 OR S12 OR S13 OR S14 OR S15 17,925 S15 TX anistreplase or streptodornase or pro‐urokinase or prourokinase or pro‐uk or lumbrokinase or duteplase or lanoteplase or pamiteplase or reteplase or saruplase or staphylokinase or streptase or tenecteplase or desmoteplase or retevase 225 S14 TX tPA or t‐PA or rtPA or rt‐PA or plasminogen or plasmin or alteplase or actilyse 5,223 S13 TX ((clot* or thrombus) n3 (lyse or lysis or dissolv* or dissolution)) 255 S12 TX ((clot* or thrombus) n3 (lyse or lysis or dissolv* or dissolution)) 255 S11 TX activase or saruplase or retavase or abbokinase or abbokinase or renokinase or u‐pa 54 S10 TX avelizin or awelysin or celiase or distreptase or kabikinase or kabivitrum or streptase or streptodecase or apsac or anistreplase or monteplase or apsac 46 S9 TX thromboly* or fibrinoly* 10,638 S8 TX streptokinase or urokinase or alteplase 1,353 S7 (MH "Fibrinolysis") 586 S6 (MH "Plasminogen Activators+") 3,570 S5 (MH "Fibrinolytic Agents+") 11,616 S4 (MH "Thrombolytic Therapy") 4,436 S3 S1 OR S2 6,617 S2 (lung or pulmonary) n3(embol* or clot*) 6,617 S1 (MH "Pulmonary Embolism") 4,693 |
11 |
| AMED | 1 ((lung or pulmonary) adj2 (embol* or clot*)).ti,ab. 126 2 exp fibrinolytic agent/ 7 3 exp fibrinolysis/ 16 4 (streptokinase or urokinase or alteplase).ti,ab. 14 5 (thromboly* or fibrinoly).ti,ab. 56 6 (avelizin or awelysin or celiase or distreptase or kabikinase or kabivitrum or streptase or streptodecase or apsac or anistreplase or monteplase or apsac).ti,ab. 0 7 (activase or saruplase or retavase or abbokinase or abbokinase or renokinase or u‐pa).ti,ab. 3 8 ((clot* or thrombus) adj3 (lyse or lysis or dissolv* or dissolution)).ti,ab. 6 9 (tPA or t‐PA or rtPA or rt‐PA or plasminogen or plasmin or alteplase or actilyse).ti,ab. 188 10 (anistreplase or streptodornase or pro‐urokinase or prourokinase or pro‐uk or lumbrokinase or duteplase or lanoteplase or pamiteplase or reteplase or saruplase or staphylokinase or streptase or tenecteplase or desmoteplase or retevase).ti,ab. 6 11 or/2‐10 253 12 1 and 11 2 13 exp CLINICAL TRIALS/ 3720 14 RANDOM ALLOCATION/ 314 15 DOUBLE BLIND METHOD/ 650 16 Clinical trial.pt. 1210 17 (clinic* adj trial*).tw. 5347 18 ((singl* or doubl* or trebl* or tripl*) adj (blind* or mask*)).tw. 2804 19 PLACEBOS/ 583 20 placebo*.tw. 3084 21 random*.tw. 17338 22 PROSPECTIVE STUDIES/ 1065 23 or/13‐22 22298 24 12 and 23 0 |
0 |
Data and analyses
Comparison 1. Thrombolytic therapy versus heparin: primary outcome measures.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Death from all causes | 17 | 2167 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.37, 0.87] |
| 1.1 rt‐PA vs heparin | 4 | 293 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.16, 2.06] |
| 1.2 Streptokinase vs heparin | 4 | 94 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.24 [0.06, 0.93] |
| 1.3 Urokinase vs heparin | 1 | 160 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.26, 2.50] |
| 1.4 Tenecteplase vs heparin | 3 | 1147 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.35, 1.47] |
| 1.5 Alteplase vs heparin | 3 | 364 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.23, 1.65] |
| 1.6 USAT (rt‐PA) vs heparin | 1 | 59 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.31 [0.01, 7.96] |
| 1.7 Streptokinase or alteplase vs enoxaparin heparin | 1 | 50 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.13 [0.01, 2.58] |
| 2 Recurrence of pulmonary emboli | 10 | 1898 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.51 [0.29, 0.89] |
| 2.1 rt‐PA vs heparin | 3 | 280 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.11 [0.01, 0.91] |
| 2.2 Urokinase vs heparin | 1 | 160 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.31, 1.65] |
| 2.3 Tenecteplase vs heparin | 2 | 1063 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.07, 1.66] |
| 2.4 Alteplase vs heparin | 3 | 364 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.25, 2.30] |
| 2.5 Streptokinase vs heparin | 1 | 31 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.33 [0.01, 8.83] |
| 3 Major haemorrhagic events | 12 | 1897 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.90 [1.95, 4.31] |
| 3.1 rt‐PA vs heparin | 3 | 172 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.90 [0.43, 19.30] |
| 3.2 Streptokinase vs heparin | 2 | 55 | Odds Ratio (M‐H, Fixed, 95% CI) | 1.64 [0.34, 8.07] |
| 3.3 Urokinase vs heparin | 1 | 160 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.23 [1.00, 4.99] |
| 3.4 Tenecteplase vs heparin | 3 | 1146 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.95 [2.71, 9.04] |
| 3.5 Alteplase vs heparin | 3 | 364 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.23, 2.16] |
| 4 Minor haemorrhagic events | 10 | 1553 | Odds Ratio (M‐H, Random, 95% CI) | 3.03 [1.60, 5.73] |
| 4.1 rt‐PA vs heparin | 1 | 58 | Odds Ratio (M‐H, Random, 95% CI) | 20.00 [2.41, 165.71] |
| 4.2 Streptokinase vs heparin | 2 | 55 | Odds Ratio (M‐H, Random, 95% CI) | 0.64 [0.17, 2.43] |
| 4.3 Urokinase vs heparin | 1 | 160 | Odds Ratio (M‐H, Random, 95% CI) | 1.52 [0.64, 3.63] |
| 4.4 Tenecteplase vs heparin | 2 | 1063 | Odds Ratio (M‐H, Random, 95% CI) | 7.94 [1.97, 32.02] |
| 4.5 Alteplase vs heparin | 2 | 108 | Odds Ratio (M‐H, Random, 95% CI) | 2.90 [1.26, 6.66] |
| 4.6 USAT (rt‐PA) vs heparin | 1 | 59 | Odds Ratio (M‐H, Random, 95% CI) | 3.11 [0.30, 31.79] |
| 4.7 Streptokinase or Alteplase vs enoxaparin heparin | 1 | 50 | Odds Ratio (M‐H, Random, 95% CI) | 2.09 [0.18, 24.61] |
Comparison 2. Thrombolytic therapy versus heparin: primary outcome measures (sensitivity analysis according to study quality).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Death from all causes | 13 | 2054 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.42, 1.06] |
| 1.1 rt‐PA vs heparin | 4 | 293 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.16, 2.06] |
| 1.2 Streptokinase vs heparin | 1 | 31 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.5 [0.04, 6.17] |
| 1.3 Urokinase vs heparin | 1 | 160 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.80 [0.26, 2.50] |
| 1.4 Tenecteplase vs heparin | 3 | 1147 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.35, 1.47] |
| 1.5 Alteplase vs heparin | 3 | 364 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.61 [0.23, 1.65] |
| 1.6 USAT (rt‐PA) vs heparin | 1 | 59 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.31 [0.01, 7.96] |
| 2 Major haemorrhagic events | 10 | 1842 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.00 [1.99, 4.53] |
| 2.1 rt‐PA vs heparin | 3 | 172 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.90 [0.43, 19.30] |
| 2.2 Urokinase vs heparin | 1 | 160 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.23 [1.00, 4.99] |
| 2.3 Tenecteplase vs heparin | 3 | 1146 | Odds Ratio (M‐H, Fixed, 95% CI) | 4.95 [2.71, 9.04] |
| 2.4 Alteplase vs heparin | 3 | 364 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.71 [0.23, 2.16] |
| 3 Minor haemorrhagic events | 7 | 1448 | Odds Ratio (M‐H, Random, 95% CI) | 4.05 [2.17, 7.54] |
| 3.1 rt‐PA vs heparin | 1 | 58 | Odds Ratio (M‐H, Random, 95% CI) | 20.00 [2.41, 165.71] |
| 3.2 Urokinase vs heparin | 1 | 160 | Odds Ratio (M‐H, Random, 95% CI) | 1.52 [0.64, 3.63] |
| 3.3 Tenecteplase vs heparin | 2 | 1063 | Odds Ratio (M‐H, Random, 95% CI) | 7.94 [1.97, 32.02] |
| 3.4 Alteplase vs heparin | 2 | 108 | Odds Ratio (M‐H, Random, 95% CI) | 2.90 [1.26, 6.66] |
| 3.5 USAT (rt‐PA) vs heparin | 1 | 59 | Odds Ratio (M‐H, Random, 95% CI) | 3.11 [0.30, 31.79] |
Comparison 3. Thrombolytic therapy versus heparin: primary outcome measures (subgroup analysis according to types of PE).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Death from all causes | 17 | 2167 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.57 [0.37, 0.87] |
| 1.1 Submassive PE | 10 | 1841 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.60 [0.36, 1.01] |
| 1.2 Submassive PE (USAT (rt‐PA) vs heparin) | 1 | 59 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.31 [0.01, 7.96] |
| 1.3 Massive PE | 1 | 8 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.01 [0.00, 0.77] |
| 1.4 Type of PE unknown | 5 | 259 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.28, 1.62] |
| 2 Recurrence of pulmonary emboli | 10 | 1898 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.51 [0.29, 0.89] |
| 2.1 Submassive PE | 8 | 1707 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.39 [0.17, 0.86] |
| 2.2 Type of PE unknown | 2 | 191 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.68 [0.31, 1.52] |
| 3 Major haemorrhagic events | 12 | 1897 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.90 [1.95, 4.31] |
| 3.1 Submassive PE | 8 | 1669 | Odds Ratio (M‐H, Fixed, 95% CI) | 3.35 [2.06, 5.45] |
| 3.2 Type of PE unknown | 4 | 228 | Odds Ratio (M‐H, Fixed, 95% CI) | 2.07 [1.03, 4.18] |
| 4 Minor haemorrhagic events | 10 | 1553 | Odds Ratio (M‐H, Random, 95% CI) | 3.03 [1.60, 5.73] |
| 4.1 Submassive PE | 6 | 1279 | Odds Ratio (M‐H, Random, 95% CI) | 4.91 [2.93, 8.22] |
| 4.2 Submassive PE (USAT (rt‐PA) vs heparin) | 1 | 59 | Odds Ratio (M‐H, Random, 95% CI) | 3.11 [0.30, 31.79] |
| 4.3 Type of PE unknown | 3 | 215 | Odds Ratio (M‐H, Random, 95% CI) | 1.18 [0.57, 2.44] |
Comparison 4. Thrombolytic therapy versus heparin: haemodynamic outcomes.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Pulmonary arterial systolic pressure improvement (mmHg) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.1 Urokinase vs heparin at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Streptokinase vs heparin at 72 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Mean pulmonary arterial pressure improvement (mmHg) | 3 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2.1 Urokinase vs heparin at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 Streptokinase vs heparin at 72 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.3 rt‐PA vs heparin at 1.5 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Right ventricular end‐diastolic pressure improvement (mmHg) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.1 Urokinase vs heparin at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Streptokinase vs heparin at 72 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Total pulmonary resistance improvement (dyn·s·cm‐5) | 3 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4.1 Urokinase vs heparin at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Streptokinase vs heparin at 72 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.3 rt‐PA vs heparin at 1.5 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Cardiac index improvement (L/min/m²) | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1 Streptokinase vs heparin at 72 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5.2 Urokinase vs heparin at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Right ventricular systolic pressure improvement (mmHg) at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7 Right arterial mean pressure improvement (mmHg) at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 8 Arterial‐venous oxygen difference (vol %) at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 9 Arterial PO₂ (mmHg) improvement at 24 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected |
Comparison 5. Thrombolytic therapy versus heparin: perfusion lung scanning (absolute resolution).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Day 1 | 2 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.1 Urokinase vs heparin | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 rt‐PA vs heparin | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Day 2 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 2.1 Urokinase vs heparin | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Day 5 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.1 Urokinase vs heparin | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Day 7 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 4.1 Alteplase vs heparin (total lung score) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4.2 Change from baseline | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 5 Day 14 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 5.1 Urokinase vs heparin | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6 Day 30 | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.1 Alteplase vs heparin (total lung score) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 Change from baseline | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 Absolute resolution (1‐year follow‐up) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.1 Urokinase vs heparin | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 6. Thrombolytic therapy versus heparin: number of patients with greater than 50% improvement on lung scan.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Day 1 | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.1 rt‐PA vs heparin | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Day 7 | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.1 rt‐PA vs heparin | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
6.2. Analysis.
Comparison 6 Thrombolytic therapy versus heparin: number of patients with greater than 50% improvement on lung scan, Outcome 2 Day 7.
Comparison 7. Thrombolytic therapy versus heparin: pulmonary angiogram assessment.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Change from baseline at 2 hours | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 1.1 Alteplase vs heparin (overall total score) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 Alteplase vs heparin (left lung) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 Alteplase vs heparin (right lung) | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Change from baseline at 72 hours | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 Streptokinase vs heparin | 2 | 47 | Mean Difference (IV, Fixed, 95% CI) | ‐9.30 [‐12.81, ‐5.78] |
Comparison 8. Thrombolytic therapy versus heparin: echocardiograms.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Right ventricular wall movement improvement | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 1.1 3 hours after treatment | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.2 24 hours after treatment | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 1.3 End of first week | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2 Tricuspid regurgitation improvement | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 2.1 3 hours after treatment | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 2.2 24 hours after treatment | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3 Paradoxical systolic septal motion | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.1 24 hours after treatment | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 48 hours after treatment | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.3 72 hours after treatment | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.4 6 days after treatment | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 4 Right ventricle‐to‐left ventricle ratio | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 4.1 24 hours after treatment | 2 | 131 | Mean Difference (IV, Random, 95% CI) | ‐0.13 [‐0.16, ‐0.11] |
| 4.2 48 hours after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | ‐0.19 [‐0.20, ‐0.18] |
| 4.3 72 hours after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | ‐0.14 [‐0.15, ‐0.13] |
| 4.4 6 days after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | ‐0.22 [‐0.23, ‐0.21] |
| 4.5 Discharge after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | ‐0.33 [‐0.34, ‐0.32] |
| 4.6 3 months after treatment | 2 | 131 | Mean Difference (IV, Random, 95% CI) | ‐0.14 [‐0.34, 0.05] |
| 4.7 6 months after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | ‐0.21 [‐0.22, ‐0.20] |
| 5 Tricuspid annular plane systolic excursion | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 5.1 24 hours after treatment | 2 | 131 | Mean Difference (IV, Random, 95% CI) | 0.45 [‐1.18, 2.07] |
| 5.2 48 hours after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | 1.0 [‐0.13, 2.13] |
| 5.3 72 hours after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | 1.80 [0.67, 2.93] |
| 5.4 6 days after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | 2.5 [1.57, 3.43] |
| 5.5 Discharge after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | 2.0 [0.75, 3.25] |
| 5.6 3 months after treatment | 2 | 131 | Mean Difference (IV, Random, 95% CI) | 0.33 [‐3.18, 3.85] |
| 5.7 6 months after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | 1.30 [0.28, 2.32] |
| 6 Right ventricular‐to‐right atrial pressure gradient | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 6.1 24 hours after treatment | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 6.2 3 months after treatment | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7 Minimum inferior vena cava diameter | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 7.1 24 hours after treatment | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 7.2 3 months after treatment | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 8 Pulmonary hypertension | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 8.1 24 hours after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | ‐8.0 [‐14.76, ‐1.24] |
| 8.2 48 hours after treatment | 2 | 193 | Mean Difference (IV, Random, 95% CI) | ‐7.37 [‐9.20, ‐5.53] |
| 8.3 72 hours after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | ‐8.0 [‐11.74, ‐4.26] |
| 8.4 6 days after treatment | 2 | 122 | Mean Difference (IV, Random, 95% CI) | ‐5.69 [‐9.37, ‐2.02] |
| 8.5 Discharge after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | ‐8.0 [‐9.78, ‐6.22] |
| 8.6 3 months after treatment | 1 | 72 | Mean Difference (IV, Random, 95% CI) | ‐7.0 [‐17.18, 3.18] |
| 8.7 6 months after treatment | 2 | 193 | Mean Difference (IV, Random, 95% CI) | ‐11.95 [‐23.71, ‐0.19] |
| 8.8 28 months after treatment | 1 | 121 | Mean Difference (IV, Random, 95% CI) | ‐15.0 [‐17.32, ‐12.68] |
Comparison 9. Thrombolytic therapy versus heparin: haemocoagulation variables.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Fibrinogen (g/L) | 3 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 1.1 Less than 3 hours after treatment | 2 | 45 | Mean Difference (IV, Random, 95% CI) | ‐2.68 [‐4.36, 1.00] |
| 1.2 24 hours after treatment | 2 | 114 | Mean Difference (IV, Random, 95% CI) | ‐1.61 [‐3.99, 0.76] |
| 1.3 48 hours after treatment | 1 | 83 | Mean Difference (IV, Random, 95% CI) | ‐0.60 [‐1.40, 0.20] |
| 2 D‐dimer (µg/mL) | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 2.1 Less than 3 hours after treatment | 2 | 45 | Mean Difference (IV, Random, 95% CI) | 21.04 [‐4.60, 46.69] |
| 2.2 24 hours after treatment | 1 | 31 | Mean Difference (IV, Random, 95% CI) | 5.30 [2.12, 8.48] |
| 3 Plasminogen (%) | 1 | Mean Difference (IV, Fixed, 95% CI) | Totals not selected | |
| 3.1 2 hours after treatment | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 24 hours after treatment | 1 | Mean Difference (IV, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Comparison 10. Thrombolytic therapy versus heparin: other outcomes.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Escalation of treatment | 2 | 306 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.32 [0.16, 0.64] |
| 2 Hospital stay | 3 | 230 | Mean Difference (IV, Random, 95% CI) | ‐0.89 [‐3.13, 1.34] |
| 2.1 USAT (rt‐PA) vs heparin | 1 | 59 | Mean Difference (IV, Random, 95% CI) | 0.30 [‐1.57, 2.17] |
| 2.2 rt‐PA vs heparin | 1 | 121 | Mean Difference (IV, Random, 95% CI) | ‐2.7 [‐2.94, ‐2.46] |
| 2.3 Streptokinase or alteplase vs enoxaparin heparin | 1 | 50 | Mean Difference (IV, Random, 95% CI) | 0.0 [‐0.83, 0.83] |
| 3 Composite clinical outcome | 2 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 3.1 All‐cause death or haemodynamic decompensation | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.2 Recurrent VTE and poor functional capacity and low perception of wellness | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.3 Poor functional capacity and low perception of wellness | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] | |
| 3.4 Recurrent VTE and low perception of wellness | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | 0.0 [0.0, 0.0] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Becattini 2010.
| Methods |
Study design: multi‐centre, double‐blind, randomised, placebo‐controlled study Method of randomisation: not described Blinding: blind for assessment of efficacy of tenecteplase Duration: July 2006 to December 2006 Exclusions post randomisation: not clearly stated Losses to follow‐up: 7 participants |
|
| Participants |
Country: Italy Setting: 15 Italian centres No. of participants: 58: 28 in tenecteplase + heparin group, 30 in placebo + heparin group Age (mean ± SD): 72.1 ± 1.2 tenecteplase + heparin group, 64.5 ± 2.5 placebo + heparin group. Sex: 13 males, 15 females in tenecteplase + heparin group; 10 males, 20 females in placebo + heparin group Inclusion criteria: aged between 18 and 85 years with objective diagnosis of PE and onset of symptoms no more than 10 days before randomisation, normal blood pressure (SBP ≥ 100 mmHg), and RVD at echocardiography performed within 24 hours from the diagnosis of PE. The diagnosis of PE was to be done by multi‐detector CT scan, pulmonary angiography, or lung scan Exclusion criteria: chronic pulmonary hypertension, severe COPD, hypertension (SBP > 180 mmHg, DBP > 110 mmHg, or both), clinically relevant bleeding within the last 6 months, a haemorrhagic diathesis, active peptic ulcer, arterial aneurysm, arterial/venous malformation, cancer at increased risk for bleeding, history of stroke, intracranial or spinal surgery. Major surgery, biopsy, or trauma in the 2 months preceding admission were additional criteria for exclusion. Patients were excluded if they had received therapeutic doses of heparin (unfractionated or low‐molecular‐weight heparin) for longer than 72 hours before randomisation, thrombolytic treatment within the previous 4 days, or glycoprotein IIb/IIIa antagonists within the preceding 7 days; if they were on oral anticoagulation or had prolonged cardiopulmonary resuscitation (> 10 minutes) in the last 2 weeks. Severe hepatic or renal failure and subacute bacterial endocarditis were additional criteria for exclusion. Women were excluded in case of pregnancy, lactation, or delivery in the 30 days before randomisation |
|
| Interventions | All participants received UFH and VKA Treatment group: Tenecteplase was given as an IV weight‐adjusted bolus at a dose ranging from 30 to 50 mg, with a 5‐mg step every 10 kg from < 60 to ≥ 90 kg. Maximum bolus dose allowed was of 5000 IU (4000 IU for participants with bodyweight < 67 kg) Control group: placebo instead of tenecteplase Length of follow‐up: follow‐up at 24 hours, 7 days after inclusion; at or before hospital discharge for the outcome echocardiography assessment; at 7 days or before discharge for the outcome clinical deterioration; at 30 days from randomisation for the outcome recurrence of PE and death; at 7 days from randomisation or before discharge for the outcome adverse events |
|
| Outcomes |
|
|
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Blinding for assessment of efficacy of tenecteplase; no other information provided |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | About 12% of participants lost to follow‐up |
| Selective reporting (reporting bias) | Low risk | Reported all outcomes |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
Dalla‐Volta 1992.
| Methods |
Study design: multi‐centre, open, randomised, controlled, parallel study Method of randomisation: not described Blinding: single‐blind for evaluation of angiography and lung scan Duration: October 1988 to November 1990 Exclusions post randomisation: not clearly stated Losses to follow‐up: not stated |
|
| Participants |
Country: Italy Setting: hospital No. of participants: 36: 20 in alteplase + heparin group, 16 in heparin alone group Age (mean ± SD): 65.7 ± 10.9 in alteplase + heparin group, 63.4 ± 14.5 in heparin alone group Sex: 7 males, 13 females in alteplase group; 5 males, 11 females in heparin alone group Inclusion criteria: aged 18 to 80 years, clinical signs and symptoms indicating PE, within 10 days of onset; pulmonary angiogram showing vascular obstruction > 30% corresponding to Miller index score > 11 Exclusion criteria: cardiogenic shock defined by SBP < 90 mmHg and urinary output < 20 mL/h; surgical procedure or organ biopsy in previous 7 days; gastrointestinal or genitourinary bleeding during previous 3 months; stroke or transient ischaemic attack in previous 3 months; puncture of non‐compressible vessels; uncontrolled hypertension; haematological disorders and contraindication to use of heparin; severe hepatic or renal insufficiency; pregnancy or lactation |
|
| Interventions |
Treatment group: alteplase 100 mg (10 mg bolus + 50 mg IV for 1 hour + 40 mg in 2 hours), then heparin IV (continuous) Control group: heparin 1750 IU/h IV for 7 to 10 days Length of follow‐up: at 2 hours and 24 hours after end of infusion (blood coagulation tests), at 7 to 30 days (lung scan) |
|
| Outcomes |
|
|
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Single‐blind for evaluation of angiography and lung scan |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No information provided |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
Dotter 1979.
| Methods |
Study design: randomised parallel study Method of randomisation: not described Blinding: not described Duration: not described Exclusions post randomisation: not clearly stated Losses to follow‐up: not stated |
|
| Participants |
Country: USA Setting: hospital (University of Oregon Medical School Clinical Research Center or intensive care unit) No. of participants: 31: 15 in streptokinase group, 16 in heparin alone group Age (range): 18 to 85 years old Gender: 12 males, 19 females Inclusion criteria: positive pulmonary angiogram (following initial diagnosis on the basis of chest x‐ray, ECG, lung scan, and laboratory test) Exclusion criteria: haemorrhagic diathesis, severe systemic hypertension (grade Ⅲ or Ⅳ), streptococcal infection, active tuberculosis, serious liver disease with bleeding, cerebrovascular accident in previous 6 months, suspected carotid artery thrombosis, atrial fibrillation, major surgery in previous 10 days, pregnancy at any stage or the postpartum period, hepatic or renal biopsy in previous 10 days, translumbar aortography in previous 2 weeks |
|
| Interventions |
Treatment group: streptokinase administered by constant peripheral vein infusion as a loading dose of 250,000 IU over a 20‐ to 30‐minute period, followed by maintenance dosage of not less than 100,000 IU/h for 18 to 72 hours. The rate of infusion of the maintenance dose was adjusted on the basis of the TT at periodic intervals during treatment, followed by heparin and oral anticoagulants (1200 ± 300 units/h by infusion) Control group: Loading dose of 1500 units of heparin per kilogram of body weight followed by a similar constant rate infusion, monitored by Lee‐White clotting times or activated clotting times at 4‐hour intervals during the first 24 hours, and subsequently at 12‐hour intervals Length of follow‐up: not clearly stated; may be 2 hours, 4 hours, 8 hours, 12 hours, 16 hours, 20 hours, 24 hours, 72 hours, and 7 days |
|
| Outcomes |
|
|
| Notes | This study provides just a comparison, with no report of the method of randomisation used, how treatment allocation was concealed, analysis methods used, or numbers of post‐randomisation dropouts or withdrawals. Study was supported in part by Hoechst‐Roussel Pharmaceuticals, Inc. This study had previously been excluded and was reassessed and included in this update according to strict criteria for included studies in the Cochrane Handbook for Systematic Reviews of Interventions | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | No information provided |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No information provided |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | High risk | Small sample size may be a source of other bias. This study was supported in part by Hoechst‐Roussel Pharmaceuticals, Inc. |
Fasullo 2011.
| Methods |
Study design: double‐blind, randomised, placebo‐controlled study Method of randomisation: preliminary computer algorithm Blinding: blinded for assessment of outcomes and assignment of all participants Duration: January 2005 to June 2009 Exclusions post randomisation: not clearly stated Losses to follow‐up: none |
|
| Participants |
Country: Italy Setting: hospital No. of participants: 72: 37 in alteplase + heparin group, 35 in placebo + heparin alone group Age (mean ± SD): 55 ± 16.7 in alteplase + heparin group, 57 ± 15.5 in placebo ± heparin alone group Sex: 21 males, 16 females in alteplase + heparin group; 20 males, 15 females in placebo + heparin alone group Inclusion criteria: symptom onset within previous 6 hours for first episode of acute SPE; normal blood pressure SBP > 100 mmHg; RVD at echocardiogram; positive lung spiral computed tomography and dyspnoea; chest pain; tachypnoea; hypoxaemia PO₂ ≤ 75 mmHg; PCO₂ < 40 mmHg; oxygen saturation < 90% in room air; D‐dimer elevation; electrocardiography with S1‐Q3‐T3 pattern; inversion of T waves in V1 to V4; right bundle branch block or right axis deviation Exclusion criteria: active internal bleeding, recent intracranial bleeding, intracranial tumour or seizure history, ischaemic stroke in previous 2 months, neurosurgery during last month, surgery in previous 10 days, puncture of incompressible vessel in previous 10 days, trauma in previous 15 days, uncontrolled hypertension (SBP > 180 mmHg and DBP > 110 mmHg), haemorrhagic disorder of thrombocytopaenia (< 100,000), severe impaired hepatic or renal function, gastrointestinal bleeding in previous 10 days, pregnancy, > 75 years of age. Also excluded were those with arterial aneurysm or arterial/venous malformation and cancer at increased risk for bleeding and patients with chronic pulmonary hypertension or severe COPD; those who had received therapeutic doses of heparin (UFH or LMWH) for longer than 72 hours before randomisation, thrombolytic treatment within the previous 4 days, or glycoprotein IIb/IIIa antagonists within the preceding 7 days; and those taking oral anticoagulation |
|
| Interventions |
Before randomisation: IV bolus of 5000 IU of UFH Treatment group: alteplase 100 mg (Actilyse as a 10‐mg bolus, followed by a 90‐mg intravenous infusion over a period of 2 hours), then heparin and warfarin (continuous) Control group: matching placebo, heparin, and warfarin Length of follow‐up: every week for the first month, every 2 weeks for the subsequent 3 months, and every month successively for the next 6 months (recurrence of PE). At every follow‐up, clinical, ECG, echocardiographic, and laboratory assessments were performed. In addition, spiral CT and lower abdominal CT and Doppler echography of the inferior limbs were repeated 3 and 6 months after thrombolytic treatment |
|
| Outcomes |
|
|
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Preliminary computer algorithm |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Blinding for assessment of outcomes and assignment of all participants |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Low risk | Reported all outcomes |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
Goldhaber 1993.
| Methods |
Study design: single‐centre, randomised controlled trial Method of randomisation: consecutively numbered sealed envelopes generated by permuted block random number sequences Blinding: non‐blinded Duration: November 1988 to July 1991 Exclusions post randomisation: 1 Losses to follow‐up: 1 |
|
| Participants |
Country: USA Setting: hospital No. of participants: 101: 46 in rt‐PA group, 55 in heparin group Age (mean): 58 in alteplase group, 59 in heparin only group Sex: 16 males, 30 females in rt‐PA group; 28 males, 27 females in heparin group Inclusion criteria: aged 18 years or over; symptoms and signs of PE within 14 days; PE confirmed by high‐probability ventilation‐perfusion lung scans, pulmonary angiograms, or both within 24 hours of randomisation; abnormal but not high‐probability scans were considered eligible if angiograms demonstrated pulmonary arterial thrombus Exclusion criteria: major internal bleeding in previous 6 months; intracranial or intraspinal disease; operation or biopsy in previous 10 days (or open heart surgery within previous 14 days); occult blood in stool; platelet count < 100,000/µL; SBP > 200 mmHg or DBP > 110 mmHg; severe impairment in hepatic function; pregnancy; active infective endocarditis; haemorrhagic retinopathy; or any concurrent condition considered to limit survival to within 1 month |
|
| Interventions |
Treatment group: rt‐PA 100 mg by infusion over 2 hours (50 mg/h), then administered 1000 IU/h heparin, when PTT or TT was < 2 times control. Subsequent heparin dose achieved PTT = 1.5 to 2.5 times the upper limit of normal Control group: heparin, initial dose 5000 IU bolus followed by 1000 IU/h continuous IV, 4 hours after the dose of heparin according to PTT. Target PTT = 1.5 to 2.5 times upper limit of normal Participants received heparin for at least 5 days and were given oral anticoagulants Length of follow‐up: echocardiography at 3 hours and 24 hours; perfusion lung scan at 24 hours after treatment started. Adverse events followed up for 14 days or longer |
|
| Outcomes |
|
|
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Generated by permuted block random number sequences |
| Allocation concealment (selection bias) | Low risk | Consecutively numbered sealed envelopes |
| Blinding (performance bias and detection bias) All outcomes | High risk | Non‐blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Intention‐to‐treat; 1 loss to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
Jerjes‐Sánchez 1995.
| Methods |
Study design: single‐centre, prospective, randomised controlled trial Method of randomisation: "withdrawal of a sealed envelope from a closed box that initially contained 40 envelopes numbered consecutively from 1 to 40; even numbers were assigned to SK + heparin and odd numbers to heparin"; no information provided for concealment of the sequence Blinding: not described Duration: not described Exclusions post randomisation: none Losses to follow‐up: none |
|
| Participants |
Country: not described Setting: not described No. of participants: 8: 4 in streptokinase group, 4 in heparin alone group Age (mean ± SD): 51 ± 22.89 in streptokinase group, 46.5 ± 10.28 in heparin alone group Sex: 3 males, 1 female in streptokinase group; 2 males, 2 females in heparin alone group Inclusion criteria: patient age ≥ 15 years; previously healthy patients; PE diagnosis sustained by high clinical suspicion; PE proven by high‐probability V/Q lung scan, suggestive echocardiogram, or radionuclide venogram; massive PE, defined as > 9 obstructed segments on V/Q lung scan with or without cardiogenic shock, < 9 obstructed segments on V/Q lung scan but with RVD, extensive DVT, or both; symptoms or signs of PE within 14 days after onset of symptoms Exclusion criteria: previous PE; < 3 segmental defects on V/Q lung scan, with normal echocardiogram and without DVT; absolute contraindication for thrombolytic therapy |
|
| Interventions |
Treatment group: streptokinase group received 1,500,000 IU of SK over 1 hour by the peripheral vein, followed by a bolus of 10,000 IU of heparin, then a constant infusion of 1000 IU/h of heparin titrated to a partial thromboplastin time of 2.0 to 2.5 times control Control group: heparin group followed the same regimen, but without streptokinase Length of follow‐up: no information provided |
|
| Outcomes | Mortality | |
| Notes | This study had previously been excluded and was reassessed and included in this update according to strict criteria for included studies provided in the Cochrane Handbook for Systematic Reviews of Interventions | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | "The patients were randomised to streptokinase followed by heparin or to heparin alone by withdrawal of a sealed envelope from a closed box that initially contained 40 envelopes numbered consecutively from 1 to 40; even numbers were assigned to SK plus heparin and odd numbers to heparin" |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | No information provided |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | High risk | Small sample size; baseline imbalanced (especially for onset of PE ‐ 2.5 hours in thrombolytics group vs 34.75 hours in heparin group) |
Kline 2014.
| Methods |
Study design: multi‐centre, randomised, placebo‐controlled trial Method of randomisation: study statistician prepared the sequence of randomisation and linked it to a unique study ID number; sequence was concealed with a sealed envelope Blinding: double‐blind; investigator and outcomes assessors were blinded Duration: June 2008 to October 2012 Exclusions post randomisation: none Losses to follow‐up: 7 participants at 3 months |
|
| Participants |
Country: USA Setting: 8 academic medical centres No. of participants: 83: 40 in single bolus tenecteplase group, 43 in placebo group Age (mean ± SD): 57 ± 14 tenecteplase group, 54 ± 14 placebo group Sex: 20 males, 20 females in tenecteplase group; 29 males, 14 females in placebo group Inclusion criteria: age > 17 years; PE diagnosed on computed tomographic pulmonary angiography performed within 24 hours; normal arterial SBP with evidence of right ventricular strain Exclusion criteria: systolic hypotension (< 90 mmHg), inability to walk, contraindications to fibrinolysis, end‐stage conditions |
|
| Interventions | All participants were treated with full‐dose LMWH. Research pharmacist prepared placebo or tenecteplase in 0.9% saline in an opaque syringe. A site investigator injected the syringe contents as soon as practical. Decisions about long‐term anticoagulant therapy were made at the discretion of the clinical care team Treatment group: tiered‐dose tenecteplase (Genentech Inc., San Francisco, CA, USA) + LMWH Control group: placebo + LMWH Length of follow‐up: 5 days and 3 months |
|
| Outcomes |
Primary outcomes:
Secondary outcomes:
|
|
| Notes | The trial was terminated early because the principal investigator relocated to a new hospital, which led to insoluble problems in transferring contracts. This study was funded by an investigator‐initiated grant from Genentech, Inc. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | The sequence of randomisation was prepared by the study statistician and was linked to a unique study ID number |
| Allocation concealment (selection bias) | Unclear risk | Study author just stated: "concealment was conducted using sealed envelopes" |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blinded: investigator and outcomes assessors were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | About 8.4% of participants lost to follow‐up |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
| Other bias | High risk | The study was funded by an investigator‐initiated grant from Genentech, Inc. |
Konstantinides 2002.
| Methods |
Study design: multi‐centre, randomised, controlled trial Method of randomisation: adequate according to a standard randomisation programme Blinding: double‐blind Duration: September 1997 to August 2001 Exclusions post randomisation: not stated Losses to follow‐up: not described |
|
| Participants |
Country: Germany Setting: 49 medical centres No. of participants: 256: 118 in heparin + alteplase group, 138 in heparin + placebo group Age (mean ± SD): 61.2 ± 10.1 males and 64.4 ± 9.5 females in alteplase group, 60.5 ± 9.7 males and 62.2 ± 12.4 females in placebo group Sex: 54 males, 64 females in alteplase group; 68 males, 70 females in placebo group Inclusion criteria: acute PE and pulmonary hypertension or RVD detected by ECG, precapillary pulmonary hypertension based on catheterisation of right side of heart followed by confirmation of PE, electrocardiographic signs of right ventricular strain followed by confirmation of PE Exclusion criteria: aged over 80 years, haemodynamic instability defined as persistent arterial hypotension (SBP below 90 mmHg) with or without signs of cardiogenic shock, onset of symptoms more than 96 hours before diagnosis, thrombolytic treatment, major surgery or biopsy within previous 7 days, major trauma within previous 10 days, stroke, transient ischaemic attack, craniocerebral trauma, neurological surgery within previous 6 months, gastrointestinal bleeding within previous 3 months, uncontrolled hypertension, known bleeding disorder, intolerance to alteplase, diabetic retinopathy, current oral anticoagulant therapy, pregnancy or lactation, life expectancy less than 6 months, planned use of thrombolytic agents for DVT |
|
| Interventions |
Treatment group: 100 mg alteplase given as 10‐mg bolus followed by 90‐mg IV infusion over 2 hours Control group: matching placebo Both groups also received IV heparin at 1000 IU/h, and rate was adjusted to maintain APTT of 2.0 to 2.5 times the upper limit of normal Oral anticoagulation was started on day 3 after randomisation for all participants Duration of treatment: mean duration in hospital 16.7 ± 8.4 days (range 2 to 70) Length of follow‐up: up to 30 days |
|
| Outcomes |
|
|
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | According to a standard randomisation programme |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Intention‐to‐treat |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
Kucher 2014.
| Methods |
Study design: randomised, parallel study Method of randomisation: not described for concealment; randomisation performed in blocks of 3 without stratification Blinding: open‐label and outcomes assessors were blinded Duration: November 2010 to January 2013 Exclusions post randomisation: not clearly stated Losses to follow‐up: 4 participants |
|
| Participants |
Countries: Germany and Switzerland Setting: 8 tertiary care hospitals No. of participants: 59: 30 in ultrasound‐assisted catheter‐directed thrombolysis (USAT) group, 29 in heparin alone group Age (mean ± SD): 63 ± 14 years Sex: 53% were women Inclusion criteria: acute symptomatic PE confirmed by contrast‐enhanced CT with embolus located in at least 1 main or proximal lower lobe pulmonary artery; RV/LV ratio ≥ 1 obtained from the echocardiographic apical 4‐chamber view Exclusion criteria: age < 18 or > 80 years; index PE symptom duration > 14 days; insufficient echocardiographic image quality in the apical 4‐chamber view that prohibited measurement of the RV/LV ratio; known significant bleeding risk; administration of thrombolytic agents within previous 4 days; active bleeding; known bleeding diathesis; known coagulation disorder; platelet count < 100,000/µL; previous use of VKA with INR > 2.5 on admission; history of any intracranial or intraspinal surgery or trauma or intracranial/intraspinal bleeding; intracranial neoplasm, arteriovenous malformation, or aneurysm; gastrointestinal bleeding < 3 months; internal eye surgery or haemorrhagic retinopathy < 3 months; major surgery, cataract surgery, trauma, obstetrical delivery, cardiopulmonary resuscitation, or other invasive procedure < 10 days; allergy, hypersensitivity, or thrombocytopaenia from heparin, rt‐PA; severe contrast allergy to iodinated contrast; known right‐to‐left cardiac shunt; large (> 10 mm) right atrial or right ventricular thrombus; haemodynamic decompensation defined as the need for cardiopulmonary resuscitation, or systolic blood pressure < 90 mmHg for at least 15 minutes, or drop in systolic blood pressure by at least 40 mmHg for at least 15 minutes with signs of end‐organ hypoperfusion, or need for catecholamine administration to maintain adequate organ perfusion and systolic blood pressure > 90 mmHg; severe hypertension on repeated readings; pregnancy, lactation, or parturition < 30 days; participation in any other investigational drug or device study; life expectancy < 90 days; inability to comply with study assessments |
|
| Interventions |
Treatment group: all participants were treated via USAT called EkoSonic MACH4e Endovascular Systems (EKOS Corporation, Bothell, WA, USA). A continuous infusion of rt‐PA at 1 mg/h and saline coolant at 35 mL/h per catheter and intravascular ultrasound delivery were then initiated. After 5 hours of treatment, the infusion rate of rt‐PA was reduced to 0.5 mg/h per catheter for 10 hours. Maximum rt‐PA dose was 20 ± 1 mg for participant with bilateral device placement and 10 ± 0.5 mg for participant with unilateral device placement. At 15 ± 1 hour, rt‐PA infusion and ultrasound delivery were discontinued Control group: UFH was administered immediately after randomisation as an intravenous bolus of 80 IU/kg, followed by an infusion of 18 IU/kg/h (with a maximum initial infusion rate of 1800 IU/h). The intervention for participants already receiving UFH, LMWH, or fondaparinux was adjusted according to different conditions and APTT. The minimum suggested duration of anticoagulation therapy was 3 months Length of follow‐up: 90 days |
|
| Outcomes |
|
|
| Notes | The outcome was analysed based on per‐protocol population. This study was funded by EKOS Corporation (Bothell, WA, USA). Dr. Kucher reports being a consultant for EKOS Corp and having received honoraria from Sanofi‐Aventis, Boehringer Ingelheim, Pfizer, Bristol‐Myers Squibb, and Bayer | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details provided |
| Allocation concealment (selection bias) | Unclear risk | No details provided |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Open‐label, but outcome assessors were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 6.7% of participants lost to follow‐up |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | High risk | Small sample size may be a source of other bias; possible conflicts of interest |
Levine 1990.
| Methods |
Study design: multi‐centre, randomised controlled trial Method of randomisation: unclear Blinding: double‐blind Duration: not described Exclusions post randomisation: none Losses to follow‐up: none |
|
| Participants |
Country: Canada Setting: hospital No. of participants: 58: 33 in rt‐PA group, 25 in placebo group Age (mean ± SD): 61.5 ± 2.7 years in rt‐PA group, 59.6 ± 3.6 years (range 56 to 63) in placebo group Sex: 18 males, 15 females in rt‐PA group; 11 males, 14 females in placebo group Inclusion criteria: acute symptomatic PE documented by pulmonary angiography or ventilation perfusion lung scan, plus DVT confirmed by venography or B‐mode ultrasonography Exclusion criteria: active bleeding process, active peptic ulcer disease, bleeding diathesis, platelet count < 100,000 µL, recent cerebrovascular accident (within previous 2 months), major surgery within previous 10 days, obstetrical delivery or organ biopsy, severe hypertension (SBP > 200 mmHg), pregnancy, clinical symptoms suggestive of PE or longer than 2 weeks in duration, received parenteral heparin for longer than 72 hours, massive PE with hypotension and haemodynamic instability |
|
| Interventions |
Treatment group: rt‐PA 0.6 mg/kg of ideal body weight reconstituted in 50 mL sterile water as bolus injection over 2 minutes Control group: placebo (saline solution) following the same procedure as for treatment group Both groups received initial heparin bolus of 5000 IU, then 30,000 IU for first 24 hours continuous infusion, interrupted only for the duration of the study drug infusion Duration of study period: 10 days Length of follow‐up: 24 hours and 7 days post treatment |
|
| Outcomes |
|
|
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind for primary outcome measure |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
Ly 1978.
| Methods |
Study design: single‐centre, randomised, controlled trial Method of randomisation: sealed envelopes on the basis of random numbers Blinding: single‐blind for interpretation of pulmonary angiographs Duration: not described Exclusions post randomisation: 1 (heparin group) Losses to follow‐up: not described |
|
| Participants |
Country: Norway Setting: Ulleval Hospital No. of participants: 25: 14 in streptokinase group, 11 in heparin group Mean age (range): 56 (23 to 70) in heparin group, 51 (37 to 68) in streptokinase group Sex: 3 males, 8 females in streptokinase group; 8 males, 6 females in heparin group Inclusion criteria: symptoms (< 5 days) of acute major PE, confirmed by angiography Exclusion criteria: minor embolism affecting less than 1 lobar artery, known bleeding tendency or recent gastrointestinal or urogenital bleeding, major surgery within last 10 days, recent cerebrovascular episodes, severe hypertension, severe renal or hepatic insufficiency, pregnancy, recent delivery or known malignant disease, aged > 70 years |
|
| Interventions |
Treatment group: streptokinase (Streptase) 250,000 IU loading dose + 0.9% saline 20 mL IV in 20 minutes, then 100,000 IU/h maintenance dose continuous IV for 72 hours, then oral warfarin. If TT < 2 times normal control value, heparin 10,000 to 30,000 IU/d Control group: heparin (Apotekernes Laboratorium, Oslo, Norway) 15,000 IU initial dose IV followed by 30,000 IU/day continuous IV. Dose of heparin was adjusted by TT. Daily dose varied from 30,000 to 60,000 IU Length of follow‐up: not stated |
|
| Outcomes |
Angiographic scores were analysed with and without the 5 non‐randomised participants (see Notes) |
|
| Notes | 5 included participants were NOT randomised (4 in streptokinase group, 1 in heparin group). The decision to include these participants was made before the start of treatment Of streptokinase‐treated participants, 1 with massive PE was transferred from another hospital for fibrinolytic treatment; 1 was considered to be a candidate for pulmonary embolectomy but the physician decided to treat him with streptokinase instead; 1 had a history of 10 days (angiographic score 24) and 1 probably had the first of 2 embolic episodes 3 weeks earlier (angiographic score 16) Participant allocated to heparin had ulcerative colitis (angiographic score 20) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Random numbers. 5 included participants were not randomised (4 in streptokinase group, 1 in heparin group). The decision to include these participants was made before the start of treatment |
| Allocation concealment (selection bias) | Unclear risk | Used sealed envelopes |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Single‐blind for interpretation of pulmonary angiographs |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 45% of participants in the heparin group were withdrawn with an angiographic response to 72 hours of treatment |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
Marini 1988.
| Methods |
Study design: single‐centre, prospective, randomised, controlled trial Method of randomisation: not described Blinding: not described Duration: not described Exclusions post randomisation: none Losses to follow‐up: none |
|
| Participants |
Country: not described Setting: not described No. of participants: 30: 10 in urokinase 800,000 IU/12 h for 3 days group; 10 in heparin 30,000 IU/12 h for 7 days group; 10 in urokinase single dose of 3,300,000 IU in 12 hours group Mean age: 52 in urokinase 800,000 IU/12 h for 3 days group; 47 years in heparin 30,000 IU/12 h for 7 days group; 60 years in urokinase single dose of 3,300,000 IU in 12 hours group Sex: 5 males in urokinase 800,000 IU/12 h for 3 days group; 7 males in heparin 30,000 IU/12 h for 7 days group; 6 males in urokinase single dose of 3,300,000 IU in 12 hours group Inclusion criteria: younger than 72 years; > 9 unperfused lung segments; clinically identified embolic episode within previous 7 days; fibrinogen plasma concentration, Lee‐White clotting time, platelet count, PTT within normal plasma level Exclusion criteria: contraindication for thrombolytic therapy, angiographic procedure, or both |
|
| Interventions |
Treatment group: Urokinase 800,000 IU/12 h a day for 3 days or single dose of 3,300,000 IU in 12 hours Control group: Heparin 30,000 IU in a day for 7 days group Length of follow‐up: 24 hours; 3, 7, and 30 days; 6 and 12 months |
|
| Outcomes |
|
|
| Notes | No data could be extracted. Therefore, this study was not included in the meta‐analysis. This study had previously been excluded and was reassessed and included in this update according to strict criteria for included studies in the Cochrane Handbook for Systematic Reviews of Interventions | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | No information provided |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | No information provided |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
Meyer 2014.
| Methods |
Study design: multi‐centre, randomised, placebo‐controlled trial Method of randomisation: computer‐generated randomisation scheme; concealment of the sequence was sufficient (via the Internet), and treatment allocation was concealed from all investigators Blinding: double‐blind; participants and all investigators were blinded Duration: November 2007 to July 2012 Exclusions post randomisation: 4 in tenecteplase group, 2 in placebo group Losses to follow‐up: none |
|
| Participants |
Country: 12 countries: Austria, Belgium, France, Germany, Greece, Hungary, Israel, Italy, Poland, Portugal, Slovenia, Spain Setting: hospital No. of participants: 1006: 506 in tenecteplase group, 500 in placebo group Age (mean ± SD): 66.5 ± 14.7 in tenecteplase group, 65.8 ± 15.9 in placebo group Sex: 47.8% males in tenecteplase group, 46.3% males in placebo group Inclusion criteria: aged ≥ 18, objectively confirmed acute PE with onset of symptoms 15 days or less before randomisation, RVD confirmed by echocardiography or spiral CT of the chest, myocardial injury confirmed by a positive test for troponin I or troponin T Exclusion criteria: haemodynamic collapse at presentation; known significant bleeding risk; administration of thrombolytic agents within previous 4 days; vena cava filter insertion or pulmonary thrombectomy within previous 4 days; uncontrolled hypertension; treatment with an investigational drug under another study protocol in the previous 7 days (or more, according to local requirements); previous enrolment in this study; known hypersensitivity to tenecteplase, alteplase, unfractionated heparin, or any of the excipients; pregnancy, lactation, or parturition within previous 30 days; known coagulation disorder; any other condition that the investigator feels would place the patient at increased risk if investigational therapy is initiated |
|
| Interventions | All participants received UFH, except participants who had already received LMWH or fondaparinux Treatment group: a single weight‐based intravenous bolus (given over a period of 5 to 10 seconds) of the fibrinolytic agent tenecteplase. Doses ranged from 30 to 50 mg, depending on body weight. Control group: placebo; a single intravenous bolus of the same volume and appearance as the bolus of tenecteplase Length of follow‐up: 7, 30, and 180 days |
|
| Outcomes |
Primary outcomes: Clinical composite of death from any cause or haemodynamic decompensation (or collapse) within 7 days after randomisation Secondary outcomes:
|
|
| Notes | Some study authors were employed by or received funds or personal fees from related companies | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation scheme |
| Allocation concealment (selection bias) | Low risk | Via the Internet; treatment allocation concealed from all investigators |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind: participants and all investigators were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Only 6 participants were excluded in the period post randomisation |
| Selective reporting (reporting bias) | Low risk | All outcomes reported |
| Other bias | High risk | Although study authors state: "None of the trial funders had any role in the design or conduct of the trial, the analysis of the data, or the preparation of the manuscript", some study authors were employed by or received funds or personal fees from related companies |
PIOPED 1990.
| Methods |
Study design: multi‐centre, randomised, controlled trial Method of randomisation: not described Blinding: double‐blind Duration: November 1986 to June 1987 Exclusions post randomisation: none Losses to follow‐up: none |
|
| Participants |
Country: USA Setting: 6 participating hospitals No. of participants: 13: 9 in rt‐PA group, 4 in placebo group Age (range): 20 to 78 years Sex: 9 males, 4 females Inclusion criteria: acute PE Exclusion criteria: not reported |
|
| Interventions |
Treatment group: rt‐PA 40 to 80 mg administered IV at a rate of approximately 1 mg/min, in combination with heparin Control group: matching placebo + heparin Length of follow‐up: 1.5 hours, 3 hours, 7 days |
|
| Outcomes |
|
|
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
Sharifi 2013.
| Methods |
Study design: single‐centre, open, prospective, randomised, controlled trial Method of randomisation: generation of randomised sequence not described; sequence concealed by sealed envelopes Blinding: outcomes assessors Duration: May 2008 to March 2010 Exclusions post randomisation: none Losses to follow‐up: 3 in tPA group, 4 in control group |
|
| Participants |
Country: not described Setting: not described No. of participants: 121: 61 in tPA group, 60 in control group Age (mean ± SD): 58 ± 9 in tPA group, 59 ± 10 in control group Sex: 46% M in tPA group, 45% M in control group Inclusion criteria: adult patients presenting with signs and symptoms suggestive of PE plus imaging documentation on computed tomographic angiography or ventilation/perfusion scanning; patients meeting the criteria of 'moderate' PE with ≥ 2 new signs and symptoms Exclusion criteria: onset of symptoms > 10 days; > 8 hours since the start of parenteral anticoagulation; systemic arterial SBP < 95 or ≥ 200/100 mmHg; eligibility for full‐dose thrombolysis; contraindication to UFH or LMWH; severe thrombocytopaenia; major bleeding within < 2 months requiring transfusion; surgery or major trauma within < 2 weeks; brain mass; neurological surgery, intracerebral haemorrhage, or subdural haematoma within < 1 year; end‐stage illness and conditions; inability to perform echocardiography |
|
| Interventions | All participants received either UFH or subcutaneous enoxaparin Treatment group: tPA + anticoagulation The dose of tPA was 50% of the standard dose (100 mg) commonly used for treatment of PE, termed 'safe dose' thrombolysis Control group: anticoagulation alone Length of follow‐up: 28 ± 5 days |
|
| Outcomes |
Primary outcomes:
Secondary outcomes:
|
|
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | Study author just stated: "concealment was conducted using sealed envelope" |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Only outcome assessors were blinded |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 5.5% losses in follow‐up |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
Taherkhani 2014.
| Methods |
Study design: single‐centre, randomised, controlled trial Method of randomisation: via a computerised system; randomisation performed in blocks Blinding: single‐blind Duration: April 2011 to November 2013 Exclusions post randomisation: not stated Losses to follow‐up: not described |
|
| Participants |
Country: Iran Setting: Loghman Hakim Hospital No. of participants: 50: 25 in enoxaparin + alteplase or streptokinase group, 25 in enoxaparin alone group Age (mean ± SD): 54.8 ± 14.1 in enoxaparin + alteplase or streptokinase group, 56.6 ± 10.5 in enoxaparin alone group Sex: 10 males, 15 females in enoxaparin + alteplase or streptokinase group; 10 males, 15 females in enoxaparin alone group Inclusion criteria: patients with submassive pulmonary thromboembolism whose diagnosis was confirmed by multi‐slice computed tomography angiography; patients fulfilling at least 1 of the following criteria: echocardiographically detected RV dysfunction or RV enlargement without left ventricular or mitral valve disease and echocardiographically detected pulmonary artery hypertension, defined as a tricuspid regurgitant jet velocity greater than 2.8 m/s Exclusion criteria: age > 80 or < 18 years; haemodynamic instability, defined as persistent arterial hypotension (i.e. systolic pressure below 90 mmHg), with or without signs of cardiogenic shock; major surgery or biopsy within preceding 7 days; major trauma within preceding 10 days; stroke, transient ischaemic attack, craniocerebral trauma, or neurological surgery within preceding 6 months; gastrointestinal bleeding within preceding 3 months; uncontrolled hypertension; known bleeding disorder; current therapy with an oral anticoagulant; current pregnancy or lactation; life expectancy less than 6 months because of underlying disease; planned use of thrombolytic agents for extensive DVT |
|
| Interventions |
Treatment group (enoxaparin + alteplase or streptokinase group): enoxaparin (1 mg/kg subcutaneous twice a day) + alteplase (100 mg/90 min) or streptokinase (1,500,000 IU/2 h) Control group (enoxaparin alone group): enoxaparin (1 mg/kg subcutaneous twice a day) Both groups also received oral anticoagulant therapy, starting on day 3 after randomisation, and the warfarin dosage was adjusted to maintain an international normalised ratio of 2.5 to 3.5 Length of follow‐up: 1 month |
|
| Outcomes |
|
|
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | According to a computerised system; randomisation performed in blocks (no details of the blocks) |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | High risk | Single‐blind; blinding was broken |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | High risk | Small sample size. In this study, 59 participants had submassive pulmonary thromboembolism; however, the researcher selected only 50 participants for randomisation |
Tibbutt 1974.
| Methods |
Study design: 2‐centre, randomised, controlled trial Method of randomisation: not described Blinding: single‐blind analysis of angiographs; not possible to use double‐blinding due to recognisable physical characteristics of streptokinase in solution Duration: not described Exclusions post randomisation: 5 in treatment group, 2 in control group Losses to follow‐up: 10 in streptokinase group, 9 in heparin group |
|
| Participants |
Country: UK Setting: Brompton Hospital (n = 21) and Radcliffe Infirmary (n = 9) No. of participants: 30: 17 in treatment group, 13 in control group Age (range): mean 51 (29 to 71) in streptokinase group, 47 (25 to 63) in heparin group Sex: 4 males, 9 females in streptokinase group; 11 males, 6 females in heparin group Inclusion criteria: acute or progressive life‐threatening PE verified by angiography Exclusion criteria: recent surgery, gastrointestinal disease, malignant hypertension, recent cerebrovascular episode, pregnancy, recent delivery |
|
| Interventions |
Treatment group: loading dose of streptokinase (600,000 IU in 100 mL normal saline or 5% glucose solution) + 100 mg hydrocortisone infused over 30 minutes through pulmonary artery catheter. Followed by 100,000 IU/h streptokinase IV for 72 hours Control group: 5000 IU heparin (in 100 mL normal saline or 5% glucose solution) + 100 mg hydrocortisone infused over 30 minutes through pulmonary artery catheter. Followed by 2500 IU for 72 hours At 60 hours from start of infusion, warfarin given at 25 mg and continued with laboratory control for next 6 months Dose adjusted according to coagulation test (protamine heparin titration, fibrinogen titre, PTT) Length of follow‐up: 72 hours and 6 months |
|
| Outcomes |
|
|
| Notes | 2 participants transferred from control group to treatment group | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No information provided |
| Allocation concealment (selection bias) | Unclear risk | No information provided |
| Blinding (performance bias and detection bias) All outcomes | Unclear risk | Single‐blind analysis for angiographs. Not possible to use double‐blinding due to recognisable physical characteristics of streptokinase in solution |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 63% losses in long‐term follow‐up |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | High risk | Two participants transferred from control group to treatment group and data were not analysed as ITT; small sample size may be a source of other bias |
UPETSG 1970.
| Methods |
Study design: multi‐centre, randomised controlled trial Method of randomisation: telephone to Drug Assignment Center Blinding: double‐blind Duration: October 1968 to August 1970 Exclusions post randomisation: 1 Losses to follow‐up: 1 |
|
| Participants |
Country: USA Setting: 14 centres No. of participants: 160: 82 in urokinase group, 78 in heparin group Age (years): not clearly stated Sex: 47 males, 35 females in urokinase group; 45 males, 33 females in heparin group Inclusion criteria: well‐documented clinical episode suggesting PE had occurred within 5 days of institution of therapy Exclusion criteria: recent operation, contraindication to use of anticoagulant or thrombolytic therapy |
|
| Interventions |
Treatment group: 2 brands of urokinase ‐ Urokinase (Abbott) and Winkinase (Sterling‐Winthrop) ‐ were given randomly by 12‐hour infusion. Loading dose of 2000 CTA IU/lb in 10 minutes, then 2000 CTA IU/lb for 12 hours via infusion pump Control group: heparin; loading dose of 75 IU/lb, then 10 IU/lb/h for 12‐hour infusion Both groups then received heparin for a minimum of 5 days, followed by heparin or warfarin therapy for a total of 14 days. Dosage not clear Follow‐up: 6 to 18 hours after completion of test drug infusion, then at 2 weeks and 3, 6, and 12 months |
|
| Outcomes |
|
|
| Notes | — | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Drug Assignment Center |
| Allocation concealment (selection bias) | Low risk | Telephone to Drug Assignment Center |
| Blinding (performance bias and detection bias) All outcomes | Low risk | Double‐blind |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No missing data |
| Selective reporting (reporting bias) | Unclear risk | No information provided |
| Other bias | Unclear risk | Small sample size may be a source of other bias |
APTT: activated partial thromboplastin time. BP: blood pressure. COPD: chronic obstructive pulmonary disease. CT: computed tomography. CTA: Committee on Thrombolytic Agents. DBP: diastolic blood pressure. DVT: deep vein thrombosis. ECG: electrocardiogram. INR: international normalised ratio. ITT: intention‐to‐treat. IU: international units. IV: intravenous. LMWH: low‐molecular‐weight heparin. LV: left ventricle. PE: pulmonary embolism. PTT: prothrombin time. rt‐PA: recombinant tissue plasminogen activator. RVD: right ventricle dysfunction. RV/LV: right‐to‐left ventricular dimension ratio. SBP: systolic blood pressure. SD: standard deviation. SK: streptokinase. SPE: submassive pulmonary embolism. TT: thrombin time. UFH: unfractionated heparin. USAT: ultrasound‐assisted catheter‐directed thrombolysis system. VKA: vitamin K antagonists. V/Q: ventilation/perfusion (lung scan). VTE: venous thromboembolism.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Abdelsamad 2011 | Compared different doses of streptokinase |
| Agnelli 1997 | Compared 2 kinds of rt‐PA |
| Alexandru Ion 2017 | Not a true RCT |
| Barrios 2017 | Not a true RCT |
| Bell 1974 | Compared 2 thrombolytics |
| Bell 1976 | Compared streptokinase to urokinase |
| Bell 1977 | Compared 3 doses of thrombolytic |
| Bhardwaj 2010 | Not a true RCT |
| Carroll 2018 | Not a true RCT |
| Charbonnier 1984 | Compared defibrase to heparin |
| Chen 2009 | Compared different doses of rt‐PA |
| Comerota 2009 | Study focusses on acute DVT |
| De Takats 1973 | Not randomised |
| Erkan 2002 | Thrombolytic drugs were given to all groups. Thrombolytics were compared |
| Francois 1986 | Compared 2 thrombolytics |
| Goldhaber 1989 | Compared rt‐PA to streptokinase |
| Goldhaber 1992 | Compared rt‐PA to urokinase |
| Goldhaber 1994 | Compared different doses of the same thrombolytic drug |
| IRCT201104245625N2 | Compared different use types of thrombolytic regimens |
| Jin 2012 | Compared different thrombolytic regimens |
| Jing 2018 | Not a true RCT |
| Konstantinides 1998 | Not a true RCT |
| Lehnert 2017 | Not a true RCT |
| Liu 2012 | Not a true RCT |
| Marder 1978 | Compared biochemical effects of 2 types of urokinase (tissue culture urokinase with urinary source urokinase); no comparison with heparin or placebo |
| Meneveau 1997 | Compared rt‐PA to streptokinase |
| Meneveau 1998 | Compared streptokinase to alteplase |
| Meyer 1992 | Compared streptokinase to alteplase |
| Miller 1971 | No mention of method of randomisation; only the last 8 participants were randomly allocated to either streptokinase or heparin |
| Muhl 2007 | Compared 2 thrombolytics |
| NCT00680628 | This trial was terminated, as the principal investigator changed institutions, and it was not possible to solve issues with contracts |
| NCT00968929 | Compared different types of thrombolytic regimens |
| NCT01956955 | Compared LMWH and UFH in combination with thrombolytic treatment |
| Ohayon 1986 | Compared different doses of urokinase and compared urokinase vs streptokinase |
| Palla 1997 | Not a true RCT |
| Pang 2007 | Not a true RCT |
| Prandoni 1985 | Not a true RCT |
| Research Group on Urokinase and PE 1984 | Compared different doses of urokinase |
| Saponjski 2002 | Not randomised |
| Sasahara 1975 | Compared 2 thrombolytics |
| Sharma 2000 | Not a true RCT |
| Sors 1994 | Compared bolus vs infusion of alteplase |
| Tebbe 1999 | Compared reteplase vs alteplase |
| Tebbe 2009 | Compared 2 thrombolytics |
| UKEP Study Group 1987 | Compared 2 doses of thrombolytic |
| UPET Study Group 1974 | Compared 3 doses of thrombolytic |
| Verstraete 1988 | Compared intrapulmonary vs intravenous administration of rt‐PA |
| Wang 2006 | Compared 2 thrombolytics |
| Wang 2009 | Compared different thrombolytic regimens |
| Wang 2010 | Compared different times of urokinase and different doses of rt‐PA |
| Wu 2010 | Compared different doses of rt‐PA |
| Xu 2016 | Not a true RCT |
| Yang 2007 | Comparison of local and systemic thrombolytics |
| Yang 2011 | Compared 2 thrombolytics |
| Yilmazel 2018 | Compared 2 thrombolytics |
| Zhu 2008 | Not randomised |
DVT: deep vein thrombosis. LMWH: low‐molecular‐weight heparin. RCT: randomised controlled trial. rt‐PA: recombinant tissue plasminogen activator. UFH: unfractionated heparin.
Characteristics of ongoing studies [ordered by study ID]
EUCTR2017‐005075‐91‐DK.
| Trial name or title | Low dose thrombolysis, ultrasound assisted thrombolysis or heparin for intermediate high risk PE |
| Methods | Randomised controlled trial with open‐label and 3 arms |
| Participants | Participants with acute PE, intermediate high risk (visible impact on right ventricular structure and function, and biochemical markers of myocardial damage according to ESC Guidelines) Inclusion criteria:
Exclusion criteria:
|
| Interventions |
Treatment group: Alteplase: low‐dose thrombolysis Alteplase: ultrasound‐assisted thrombolysis Control group: UFH IV or LMWH (usual care) |
| Outcomes |
Primary outcomes are evaluated within 96 hours from randomisation
Secondary outcomes are evaluated within 3 months from randomisation
|
| Starting date | 2018 |
| Contact information | Telephone number: 4535453545 Fax number: 4535453519 Email: jesper.kjaergaard.05@regionh.dk |
| Notes | ‐ |
EudraCT: 2005‐001070‐27.
| Trial name or title | Open, randomised, mono‐site pilot trial for comparison of thrombolytic efficacy of tenecteplase and alteplase in patients with acute PE |
| Methods | Randomised controlled pilot trial with open‐label and parallel‐group design |
| Participants | N = 20; patients with acute PE and indication for thrombolytic therapy are included in the study |
| Interventions | Tenecteplase and alteplase |
| Outcomes | — |
| Starting date | 7 July 2005 |
| Contact information | — |
| Notes | No further details on trial methods available |
NCT01531829.
| Trial name or title | Low dose rt‐PA for acute normotensive PE with RVD |
| Methods | Randomised controlled trial with open‐label and parallel‐group design |
| Participants | N = 460; both sexes; ≥ 18 and ≤ 75 years of age |
| Interventions |
Treatment group: low‐dose (50 mg/2 h) rt‐PA + LMWH regimen Control group: LMWH |
| Outcomes |
Primary outcome measures:
Secondary outcome measures:
|
| Starting date | July 2009 |
| Contact information | Chen Wang, PhD, MD; cyh‐birm@263.net |
| Notes | No further, recent details available |
NCT02604238.
| Trial name or title | Efficacy and safety of half dose alteplase added to heparin in patients with moderate PE (MONALYSE) |
| Methods | Prospective, randomised, open‐label, controlled trial (parallel assignment) |
| Participants | 130 participants with PE (age: 18 to 65 years old) Inclusion criteria:
Exclusion criteria:
|
| Interventions |
Treatment group: administered a "safe dose" of Alteplase (IV infusion of 40 mg within 2 hours (for patients weighing < 50 kg, a loading dose of bolus of 0.5 mg in 1 minute, followed by IV infusion of 40 mg in 2 hours); infusion will be adjusted to maintain the value of aPTT between 50 and 70 seconds (1.5 to 2.5 times the reference value). All participants are treated with LMWH according to Guidelines ESC2014 heparin; in addition, participants are administered a "safe dose" of Alteplase Control group: all participants are treated with LMWH according to Guidelines ESC2014 heparin; no treatment added |
| Outcomes | Primary outcome: pulmonary hypertension reduction documented on ECG Secondary outcomes: incidence of recurrent PE fatal or non‐fatal; incidence of haemodynamic shock; incidence of hospital death from all causes Other outcomes: bleeding extracranial minor and major |
| Starting date | Not yet recruiting |
| Contact information | Alberto Conti (aaaconti@hotmail.com) or Lorella Magnani (lorella.magnani@usl1.toscana.it) |
| Notes | ‐ |
NCT03218410.
| Trial name or title | Surgical pulmonary embolectomy versus catheter‐directed thrombolysis in the treatment of PE: a non‐inferiority study (Lungembolism) |
| Methods | Monocentric, randomised, open‐label, controlled, clinical, non‐inferiority trial |
| Participants | Acute symptomatic PE (18 years to 80 years) Inclusion criteria:
Exclusion criteria:
|
| Interventions |
Treatment group: surgical pulmonary embolectomy Control group: CDT |
| Outcomes |
Primary outcome: Difference in RV/LV ratio by contrast‐enhanced chest CT Secondary outcome: Difference in pulmonary occlusion score by contrast‐enhanced chest CT |
| Starting date | 2017 |
| Contact information | Lars Englberger (+41‐31‐6322111; lars.englberger@insel.ch) |
| Notes | ‐ |
aPTT: activated partial thromboplastin time. BNP: B‐type natriuretic peptide. CDT: catheter‐directed thrombolysis. COPD: chronic obstructive pulmonary disorder. CPR: cardiopulmonary resuscitation. CT: computed tomography. CTA: Committee on Thrombolytic Agents. CTEPH: chronic thromboembolic pulmonary hypertension. ECG: echocardiogram. ESC: European Society of Cardiology. hCG: human chorionic gonadotropin. INR: international normalised ratio. IV: intravenous. LMWH: low‐molecular‐weight heparin. LV: left ventricle. NTproBNP: N‐terminal pro‐brain natriuretic peptide. PAD: pulmonary arterial disease. PE: pulmonary embolism. ptl: platelets. rt‐PA: recombinant tissue plasminogen activator. RV: right ventricle. RVD: right ventricle dysfunction. SBP: systolic blood pressure. SF‐36: Short Form‐36. TAPSE: tricuspid annular plane systolic excursion. VTE: venous thromboembolism. UFH: unfractionated heparin. USAT: ultrasound‐assisted thrombolysis. VTE: venous thromboembolism.
Differences between protocol and review
In the previous version, we revised the methods of 'Assessment of risk of bias in included studies' according to the new version of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). We added the secondary outcomes of 'Escalation of treatment' and 'Hospital stay' because of their clinical importance in the treatment of acute pulmonary embolism with thrombolytics. We reordered the outcomes of survival time, composite clinical outcome, QoL, and healthcare cost comparison from primary to secondary outcomes due to clinical importance. We added a subgroup analysis for massive/submassive PE because of its clinical importance in the treatment of acute pulmonary embolism. We used GRADE to assess the overall quality of the evidence according to instructions provided in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), and we summarised this information in a 'Summary of findings' table.
Contributions of authors
Qiukui Hao: screened studies for eligibility, assessed the quality of trials, extracted and analysed data, and drafted the review. Birong Dong: developed the protocol and assessed the quality of trials. Jirong Yue: screened studies for eligibility, searched the reference lists of included studies, and assessed the quality of trials. Taixiang Wu: ensured that the correct method was used during data extraction and analysis. Guan Jian Liu: assisted with data extraction and analysis.
Sources of support
Internal sources
Chinese Cochrane Center, West China Hospital of Sichuan University, Chinese Medical Board of New York (CMB), China.
External sources
-
Chief Scientist Office, Scottish Government Health Directorates, The Scottish Government, UK.
The Cochrane Vascular editorial base is supported by the Chief Scientist Office.
Declarations of interest
Qiukui Hao: none known. Birong Dong: none known. Jirong Yue: none known. Taixiang Wu: none known. Guan Jian Liu: none known.
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Becattini 2010 {published data only}
- Becattini C, Agnelli G, Salvi A, Grifoni S, Pancaldi LG, Enea I, et al. Bolus tenecteplase for right ventricle dysfunction in hemodynamically stable patients with pulmonary embolism. Thrombosis Research 2010;125(3):e82‐6. [DOI] [PubMed] [Google Scholar]
Dalla‐Volta 1992 {published data only}
- Dalla‐Volta S, Palla A, Santolicandro A, Giuntini C, Pengo V, Visioli O, et al. PAIMS2: Alteplase combined with heparin versus heparin in the treatment of acute pulmonary embolism. Plasminogen activator Italian multicenter study 2. Journal of the American College of Cardiology 1992;20(3):520‐6. [DOI] [PubMed] [Google Scholar]
Dotter 1979 {published data only}
- Dotter CT, Seamon AJ, Rosch J, Porter J. Streptokinase and heparin in the treatment of major pulmonary embolism: a randomised comparison. Vascular Surgery 1979;13(1):42‐52. [Google Scholar]
Fasullo 2011 {published data only}
- Fasullo S, Scalzo S, Maringhini G, Ganci F, Cannizzaro S, Basile I, et al. Six‐month echocardiographic study in patients with submassive pulmonary embolism and right ventricle dysfunction: comparison of thrombolysis with heparin. American Journal of the Medical Sciences 2011;341(1):33‐9. [DOI] [PubMed] [Google Scholar]
Goldhaber 1993 {published data only}
- Goldhaber SZ, Haire WD, Fekdstein ML, Miller M, Toltzis R, Smith JL, et al. Alteplase versus heparin in acute pulmonary embolism: randomised trial assessing right‐ventricular function and pulmonary perfusion. The Lancet 1993;341(8844):507‐11. [DOI] [PubMed] [Google Scholar]
Jerjes‐Sánchez 1995 {published data only}
- Jerjes‐Sánchez C, Ramírez‐Rivera A, Lourdes‐García M, Arriaga‐Nava R, Valencia S, Rosado‐Buzzo A, et al. Streptokinase and heparin versus heparin alone in massive pulmonary embolism: a randomized controlled trial. Journal of Thrombosis and Thrombolysis 1995;2(3):227‐9. [DOI] [PubMed] [Google Scholar]
Kline 2014 {published data only}
- Kline J, Hernandez J, Kabrhel C, Courtney DM, Jones AE, Nordenholtz K, et al. Randomized trial of tenecteplase or placebo with low molecular weight heparin for acute submassive pulmonary embolism: assessment of patient‐oriented cardiopulmonary outcomes at three months. Journal of the American College of Cardiology 2013;61(10 Suppl 1):E2074. [Google Scholar]
- Kline JA, Hernandez J, Hogg MM, Jones AE, Courtney DM, Kabrhel C, et al. Rationale and methodology for a multicentre randomised trial of fibrinolysis for pulmonary embolism that includes quality of life outcomes. Emergency Medicine Australasia 2013;25(6):515‐26. [DOI: 10.1111/1742-6723.12159] [DOI] [PubMed] [Google Scholar]
- Kline JA, Hernandez J, Kabrhel C, Courtney DM, Nordenholtz KE, Diercks DB, et al. Randomized trial of tenecteplase or placebo with low molecular weight heparin for acute submassive pulmonary embolism: assessment of patient‐oriented cardiopulmonary outcomes at three months. Academic Emergency Medicine 2013;20(5 Suppl 1):S7. [Google Scholar]
- Kline JA, Nordenholz KE, Courtney DM, Kabrhel C, Jones AE, Rondina MT, et al. Treatment of submassive pulmonary embolism with tenecteplase or placebo: cardiopulmonary outcomes at 3 months: multicenter double‐blind, placebo‐controlled randomized trial. Journal of Thrombosis and Haemostasis 2014;12(4):459‐68. [NCT00680628] [DOI] [PubMed] [Google Scholar]
Konstantinides 2002 {published data only}
- Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. New England Journal of Medicine 2002;347(15):1143‐50. [DOI] [PubMed] [Google Scholar]
Kucher 2014 {published data only}
- Kucher N, Boekstegers P, Muller O, Kupatt C, Beyer‐Westendorf J, Heitzer T, et al. Randomized controlled trial of ultrasound‐assisted catheter‐directed thrombolysis for acute intermediate‐risk pulmonary embolism. Circulation 2014;129(4):479‐86. [NCT01166997] [DOI] [PubMed] [Google Scholar]
Levine 1990 {published data only}
- Levine M, Hirsh J, Weitz J, Cruickshank M, Neemeh J, Turpie AG, et al. A randomized trial of a single bolus dosage regimen of recombinant tissue plasminogen activator in patients with acute pulmonary embolism. Chest 1990;98(6):1473‐9. [DOI] [PubMed] [Google Scholar]
Ly 1978 {published data only}
- Arnesen BLH, Eie H, Hol R. A prospective study of streptokinase and heparin in the treatment of major pulmonary embolism. Acta Medica Scandinavica Supplement 1978; Vol. 621:15. [DOI] [PubMed]
- Ly B, Arneson H, Eie H, Hol R. A controlled clinical trial of streptokinase and heparin in the treatment of major pulmonary embolism. Acta Medica Scandinavica 1978;203(6):465‐70. [DOI] [PubMed] [Google Scholar]
Marini 1988 {published data only}
- Giuntini C, Marini C, Ricco G, Palla R, Giacomelli V, Rindi M. A controlled clinical trial on the effect of heparin infusion and two regimens of urokinase in acute pulmonary embolism. Giornale Italiano di Cardiologia 1984;14(Suppl 1):26‐9. [PubMed] [Google Scholar]
- Marini C, Ricco G, Rossi G, Rindi M, Palla R, Giuntini C. Fibrinolytic effects of urokinase and heparin in acute pulmonary embolism: a randomized clinical trial. Respiration 1988;54(3):162‐73. [DOI] [PubMed] [Google Scholar]
Meyer 2014 {published data only}
- Konstantinides SV, Vicaut E, Danays T, Becattini C, Bertoletti L, Beyer‐Westendorf J, et al. Impact of thrombolytic therapy on the long‐term outcome of intermediate‐risk pulmonary embolism. Journal of the American College of Cardiology 2017;69(12):1536‐44. [DOI] [PubMed] [Google Scholar]
- Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer‐Westendorf J, et al. Fibrinolysis for patients with intermediate‐risk pulmonary embolism. New England Journal of Medicine 2014;370(15):1402‐11. [NCT00639743] [DOI] [PubMed] [Google Scholar]
- NCT00639743. PEITHO Pulmonary Embolism Thrombolysis Study. http://clinicaltrials.gov/ct2/show/NCT00639743?term=thrombolysis&rank=14 (accessed April 2009).
- PEITHO Steering Committee. Single‐bolus tenecteplase plus heparin compared with heparin alone for normotensive patients with acute pulmonary embolism who have evidence of right ventricular dysfunction and myocardial injury: rationale and design of the Pulmonary Embolism Thrombolysis (PEITHO) trial. American Heart Journal 2012; Vol. 163, issue 1:33‐8. [NCT00639743] [DOI] [PubMed]
PIOPED 1990 {published data only}
- PIOPED Investigation Committee. Tissue plasminogen activator for the treatment of acute pulmonary embolism. A collaborative study by the PIOPED investigators. Chest 1990;97(3):528‐33. [DOI] [PubMed] [Google Scholar]
Sharifi 2013 {published data only}
- Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M. Moderate pulmonary embolism treated with thrombolysis (from the "mOPETT" Trial). American Journal of Cardiology 2013;111(2):273‐7. [DOI] [PubMed] [Google Scholar]
Taherkhani 2014 {published data only}
- Taherkhani M, Taherkhani A, Hashemi SR, Langroodi TF, Sadeghi R, Beyranvand M. Thrombolytic‐plus‐anticoagulant therapy versus anticoagulant‐alone therapy in submassive pulmonary thromboembolism (TVASPE study): a randomized clinical trial. Journal of Tehran University Heart Center 2014;9(3):104‐8. [PMC free article] [PubMed] [Google Scholar]
Tibbutt 1974 {published data only}
- Tibbutt DA, Davies JA, Anderson JA, Fletcher EW, Hamill J, Thomas ML, et al. Comparison by controlled clinical trial of streptokinase and heparin in treatment of life‐threatening pulmonary embolism. British Medical Journal 1974;1(904):343‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
UPETSG 1970 {published data only}
- Sasahara AA, Hyers TM, Cole CM, Ederer F, Murray JA, Wenger NK, et al. The urokinase pulmonary embolism trial. Circulation 1973;47(2 Suppl):7‐21. [Google Scholar]
- Sharma GVRK, Burleson VA, Sasahara AA. Effect of thrombolytic therapy on pulmonary‐capillary blood volume in patients with pulmonary embolism. New England Journal of Medicine 1980;303(15):842‐5. [DOI] [PubMed] [Google Scholar]
- UPET. Urokinase pulmonary embolism trial. Phase 1 results: a co‐operative study. JAMA 1970;214(12):2163‐71. [PubMed] [Google Scholar]
References to studies excluded from this review
Abdelsamad 2011 {published data only}
- Abdelsamad AA, El‐Morsi AS, Mansour AE. Efficacy and safety of high dose versus low dose streptokinase for treatment of submassive pulmonary embolism. Egyptian Heart Journal 2011;63:67‐72. [Google Scholar]
Agnelli 1997 {published data only}
- Agnelli G, Iorio A, Parise P, Goldhaber SZ, Levine MN. Fibrinogenolysis and thrombin generation after reduced dose bolus or conventional rt‐PA for pulmonary embolism. The Coagulation Project Investigators of the Bolus Alteplase Pulmonary Embolism Group. Blood Coagulation and Fibrinolysis 1997;8(4):216‐22. [DOI] [PubMed] [Google Scholar]
Alexandru Ion 2017 {published data only}
- Alexandru Ion A, Andrei C, Raducan M, Sinescu C. The bleeding risk in thrombolysed patients with intermediary‐high risk pulmonary embolism. European Journal of Heart Failure 2017;19(Suppl 1):34‐5. [Google Scholar]
Barrios 2017 {published data only}
- Barrios D, Chavant J, Rosa‐Salazar V, Muriel A, Viallon A, Yusen RD, et al. Treatment of right heart thrombi associated with acute pulmonary embolism. American Journal of Medicine 2017;130:588‐95. [DOI] [PubMed] [Google Scholar]
Bell 1974 {published data only}
- Bell WR, Simon TL, Stengle JM, Sherry S. The urokinase‐streptokinase pulmonary embolism trial (phase II) results. Circulation 1974;50(6):1070‐1. [DOI] [PubMed] [Google Scholar]
Bell 1976 {published data only}
- Bell WR. Streptokinase and urokinase in the treatment of pulmonary thromboemboli; from a national co‐operative study. Thrombosis and Haemostasis 1976;35(1):57‐69. [PubMed] [Google Scholar]
Bell 1977 {published data only}
- Bell WR. Thrombolytic therapy: differences between streptokinase and urokinase. Vascular Surgery 1977;11:378‐83. [DOI] [PubMed] [Google Scholar]
Bhardwaj 2010 {published data only}
- Bhardwaj S, Krishna CK, Mukherjee N, Sambi RS, Aggarwal KK, Kapoor N, et al. Treatment of massive pulmonary embolism by tenecteplase. Indian Heart Journal 2010;62(5):454‐5. [PubMed] [Google Scholar]
Carroll 2018 {published data only}
- Carroll BJ, Goldhaber SZ, Liu PY, Piazza G. Catheter‐directed, ultrasound‐facilitated fibrinolysis in obese patients with massive and submassive pulmonary embolism. Journal of Thrombosis and Thrombolysis 2018;45:257‐63. [DOI] [PubMed] [Google Scholar]
Charbonnier 1984 {published data only}
- Charbonnier B, Raynaud P, Griguier P, Brochier M. Potentializing effects of a defibrillating agent on therapeutic thrombolysis in pulmonary embolism [Effets potentialisateurs d'un agent defibrinant sur la thrombolyse therapeutique dans l'embolie pulmonaire]. Archives des Maladies du Coeur et des Vaisseaux 1984; Vol. 77:1426.
Chen 2009 {published data only}
- Chen Z. Evaluation of effect of rt‐PA therapy and different dose in acute pulmonary embolism [Abstract]. American Thoracic Society 2009 International Conference; 2009 May 15‐20; San Diego. American Journal of Respiratory and Critical Care Medicine. 2009; Vol. 179 (Meeting Abstracts):A3294.
Comerota 2009 {published data only}
- Comerota AJ. The ATTRACT trial: rationale for early intervention for iliofemoral DVT. Perspectives in Vascular Surgery and Endovascular Therapy 2009;21:221‐4. [DOI] [PubMed] [Google Scholar]
De Takats 1973 {published data only}
- Takats G. The urokinase pulmonary embolism trial. American Journal of Surgery 1973;126(3):311‐3. [DOI] [PubMed] [Google Scholar]
Erkan 2002 {published data only}
- Erkan L, Findik S, Atici AG, Uzun O. Thrombolytic therapy in massive pulmonary thromboembolism. European Respiratory Journal 2002; Vol. 20:237s.
Francois 1986 {published data only}
- Francois G, Charbonnier B, Raynaud P, Garnier LF, Griguer P, Brochier M. Treatment of acute pulmonary embolism with urokinase compared with the combination plasminogen‐urokinase. 67 cases [Traitemente de l'embolie pulmonaire aigue par urokinase comparee a l'association plasminogene‐urokinase. A propos de 67 cas]. Archives des Maladies du Coeur et des Vaisseaux 1986;79(4):435‐42. [PubMed] [Google Scholar]
Goldhaber 1989 {published data only}
- Goldhaber SZ. TPA versus urokinase in acute pulmonary embolism: results of a randomized controlled trial. Vasa ‐ Supplementum 1989;27:292‐4. [PubMed] [Google Scholar]
- Goldhaber SZ. Tissue plasminogen activator in acute pulmonary embolism. Chest 1989;95(5 Suppl):282S‐9S. [DOI] [PubMed] [Google Scholar]
Goldhaber 1992 {published data only}
- Goldhaber SZ, Kessler CM, Heit JA, Elliot CG. Recombinant tissue‐type plasminogen activator versus a novel dosing regimen of urokinase in acute pulmonary embolism: a randomized controlled multicenter trial. Journal of the American College of Cardiology 1992;20(1):24‐30. [DOI] [PubMed] [Google Scholar]
Goldhaber 1994 {published data only}
- Goldhaber SZ, Agnelli G, Levine MN. Reduced dose bolus alteplase versus conventional alteplase infusion for pulmonary embolism thrombolysis: an international multicenter randomised trial. Chest 1994;106(3):718‐24. [DOI] [PubMed] [Google Scholar]
IRCT201104245625N2 {published data only}
- IRCT201104245625N2. Comparative efficacy and complications of two‐hour versus 24‐hour regimen of streptokinase in acute pulmonary embolism In Tehran Heart Center. en.irct.ir/trial/6153 (first posted 28 August 2011).
Jin 2012 {published data only}
- Jin J, Ding WB, Yuan RF. Thrombolytic treatment of acute pulmonary thromboembolism: comparison between catheter‐directed thrombolysis and venous thrombolysis. Journal of Interventional Radiology 2012;21:667‐71. [Google Scholar]
Jing 2018 {published data only}
- Jing X, Zhang G, Zhang B, Dai L, Wang X, Jia L, et al. Efficacy and safety of low‐dose urokinase for the treatment of hemodynamically stable AECOPD patients with acute pulmonary thromboembolism. Clinical Respiratory Journal 2018;12:1882‐90. [DOI] [PubMed] [Google Scholar]
Konstantinides 1998 {published data only}
- Konstantinides S, Tiede N, Geibel A, Olschewski M, Just H, Kasper W. Comparison of alteplase versus heparin for resolution of major pulmonary embolism. American Journal of Cardiology 1998;82(8):966‐70. [DOI] [PubMed] [Google Scholar]
Lehnert 2017 {published data only}
- Lehnert P, Moller CH, Mortensen J, Kjaergaard J, SkovOlsen P, Carlsen J, et al. Surgical embolectomy compared to thrombolysis in acute pulmonary embolism: Morbidity and mortality. European Journal of Cardio‐thoracic Surgery 2017;51:354‐61. [DOI] [PubMed] [Google Scholar]
Liu 2012 {published data only}
- Liu FY, Wang MQ, Duan F, Wang ZJ, Song P, Wang Y, et al. Management of acute massive with interventional techniques. Zhonghua Yi Xue Za Zhi 2012;92(19):1343‐5. [PubMed] [Google Scholar]
Marder 1978 {published data only}
- Marder VJ, Donahoe JF, Bell WR, Cranley JJ, Kwaan HC, Sashara AA, et al. Changes in the plasma fibrinolytic system during urokinase therapy: comparison of tissue culture urokinase with urinary source urokinase in patients with pulmonary embolism. Journal of Laboratory Clinical Medicine 1978;92(5):721‐9. [PubMed] [Google Scholar]
Meneveau 1997 {published data only}
- Meneveau N, Schiele F, Vuillemenot A, Valette B, Grollier G, Bernard Y, et al. Streptokinase vs alteplase in massive pulmonary embolism. A randomized trial assessing right heart haemodynamics and pulmonary vascular obstruction. European Heart Journal 1997;18(7):1141‐8. [DOI] [PubMed] [Google Scholar]
Meneveau 1998 {published data only}
- Meneveau N, Schiele F, Metz D, Valette B, Attali P, Vuillemenot A, et al. Comparative efficacy of a two‐hour regimen of streptokinase versus alteplase in acute massive pulmonary embolism: immediate clinical and hemodynamic outcome and one‐year follow‐up. Journal of the American College of Cardiology 1998;31(5):1057‐63. [DOI] [PubMed] [Google Scholar]
Meyer 1992 {published data only}
- Meyer G, Sors H, Charbonnier B, Kasper W, Bassand JP, Kerr IH, et al. Comparison of the effect of an intravenous infusion of urokinase or alteplase on total pulmonary resistance in acute massive pulmonary embolism. A European, multi‐center, double‐blind study [Vergleich der wirkung einer intravenosen infusion von urokinase oder alteplase auf den pulmonalen en gesamtwiderstand bei akuter massiver lungenembolie. Eine Europapaische multicenter‐doppelblindestudie]. Intensivmedizin und Notfallmedizin 1992;29:339‐47. [Google Scholar]
- Meyer G, Sors H, Charbonnier B, Kasper W, Bassand JP, Kerr IH, et al. Effects of intravenous urokinase versus alteplase on total pulmonary resistance in acute massive pulmonary embolism: a European multicenter double‐blind trial. The European Cooperative Study Group for Pulmonary Embolism. Journal of the American College of Cardiology 1992;19(2):239‐45. [DOI] [PubMed] [Google Scholar]
Miller 1971 {published data only}
- Miller GAH, Sutton GC, Kerr IH, Gibson RV, Honey M. Comparison of streptokinase and heparin in treatment of isolated acute massive pulmonary embolism. British Medical Journal 1971;763(2):681‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
Muhl 2007 {published data only}
- Muhl D, Furedi R, Gecse K, Ghosh S, Falusi B, Bogar L, et al. Time course of platelet aggregation during thrombolytic treatment of massive pulmonary embolism. Blood Coagulation and Fibrinolysis 2007;18(7):661‐7. [DOI] [PubMed] [Google Scholar]
NCT00680628 {published data only}
- NCT00680628. Randomized trial of tenecteplase to treat severe submassive pulmonary embolism. http://clinicaltrials.gov/ct2/show/NCT00680628?cond=pulmonary+embolism&rank=42 (accessed January 2015).
NCT00968929 {published data only}
- NCT00968929. Recombinant streptokinase versus urokinase in pulmonary embolism in China (RESUPEC). clinicaltrials.gov/ct2/show/NCT00968929 (first posted 31 August 2009).
NCT01956955 {published data only}
- NCT01956955. Comparison of low‐molecular‐weight heparin (LMWH) and unfractionated heparin (UFH) in combination with thrombolytic treatment of acute massive pulmonary thromboembolism. clinicaltrials.gov/ct2/show/NCT01956955 (first posted 8 October 2013).
Ohayon 1986 {published data only}
- Ohayon J, Colle JP, Tauzin‐Fin P, Lorient‐Roudaut MF, Besse P. Hemodynamic course during fibrinolysis in severe pulmonary embolism [Évolution hémodynamique au cours des fibrinolyses de l'embolie pulmonaire grave]. Archives des Maladies du Coeur et des Vaisseaux 1986;79(4):445‐53. [PubMed] [Google Scholar]
Palla 1997 {published data only}
- Palla A, Pazzagli M, Manganelli D, Nitto P, Marini C, Rossi G, et al. Resolution of pulmonary embolism: effect of therapy and putative age of emboli. Respiration 1997;64(1):50‐3. [DOI] [PubMed] [Google Scholar]
Pang 2007 {published data only}
- Pang BS, Wang C, Lu Y, Yang YH, Xing GH, Mao YL, et al. Changes of blood coagulative and fibrinolytic system and function of pulmonary vascular endothelium after therapy in patients with acute pulmonary thromboembolism. Zhonghua Yi Xue Za Zhi 2007;87:3074‐8. [PubMed] [Google Scholar]
Prandoni 1985 {published data only}
- Prandoni P, Zambon G, Scatigna M. Diagnostic approaches and results in the medical treatment of pulmonary thromboembolism [Aspetti diagnostici e risultati della terapia medica nella tromboembolia polmonare]. Minerva Medica 1985;76(38):1727‐37. [PubMed] [Google Scholar]
Research Group on Urokinase and PE 1984 {published data only}
- Research Group on Urokinase and Pulmonary Embolism. Multicenter study of 2 urokinase protocols in severe pulmonary embolism [Étude multicentrique sur deux protoocles d'ukokinase dans l'embolie pulmonaire grave]. Archives des Maladies du Coeur et des Vaisseaux 1984;77(7):773‐81. [PubMed] [Google Scholar]
Saponjski 2002 {published data only}
- Saponjski JD, Saponjski MD, Vukcevic VP. Massive pulmonary embolism and thrombolysis in the first week after major surgery. European Respiratory Journal 2002;20(Suppl 38):239s. [Google Scholar]
Sasahara 1975 {published data only}
- Sasahara AA, Bell WR, Simon TL, Stengle JM, Sherry S. The phase II urokinase‐streptokinase pulmonary embolism trial: a national cooperative study. Thrombosis et Diathesis Haemorrhagica 1975;33(3):464‐76. [PubMed] [Google Scholar]
Sharma 2000 {published data only}
- Sharma GV, Folland ED, McIntyre KM, Sasahara AA. Long‐term benefit of thrombolytic therapy in patients with pulmonary embolism. Vascular Medicine 2000;5(2):91‐5. [DOI] [PubMed] [Google Scholar]
Sors 1994 {published data only}
- Sors H, Pacouret G, Azarian R, Meyer G, Charbonnier B, Simonneau G. Hemodynamic effects of bolus vs 2‐h infusion of alteplase in acute massive pulmonary embolism. A randomized controlled multicenter trial. Chest 1994;106(3):712‐7. [DOI] [PubMed] [Google Scholar]
Tebbe 1999 {published data only}
- Tebbe U, Graf A, Kamke W, Zahn R, Forycki F, Kratzsch G, et al. Hemodynamic effects of double bolus reteplase versus alteplase infusion in massive pulmonary embolism. American Heart Journal 1999;138(7):39‐44. [DOI] [PubMed] [Google Scholar]
Tebbe 2009 {published data only}
- Tebbe U, Bramlage P, Graf A, Lechleitner P, Bode C, Riess FC, et al. Desmoteplase in acute massive pulmonary thromboembolism. Thrombosis and Haemostasis 2009;101:557‐62. [PubMed] [Google Scholar]
UKEP Study Group 1987 {published data only}
- The UKEP Study Research Group. The UKEP Study: multicentre clinical trial on two local regimes of urokinase in massive pulmonary embolism. European Heart Journal 1987;8(1):2‐10. [PubMed] [Google Scholar]
UPET Study Group 1974 {published data only}
- The Urokinase Pulmonary Embolism Trial Study Froup. Urokinase streptokinase embolism trial. Phase 2 results. A co‐operative study. Journal of the American Medical Association 1974;229:1606‐13. [Google Scholar]
Verstraete 1988 {published data only}
- Verstraete M, Miller GA, Bounameaux H, Charbonnier B, Colle JP, Lecorf G, et al. Intravenous and intrapulmonary recombinant tissue‐type plasminogen activator in the treatment of acute massive pulmonary embolism. Circulation 1988;77(2):353‐60. [DOI] [PubMed] [Google Scholar]
Wang 2006 {published data only}
- Wang C. The clinical features of 516 patients with acute pulmonary thromboembolism. Zhonghua Yi Xue Za Zhi 2006;86(31):2161‐5. [PubMed] [Google Scholar]
- Yang YH, Zhai ZG, Wang F, Xie WM, Wang C. Changes in deep venous thrombosis after thrombolytic anticoagulant therapies in acute pulmonary thromboembolism. Chinese Journal of Internal Medicine 2009;48:371‐4. [PubMed] [Google Scholar]
Wang 2009 {published data only}
- Wang Y, Yang Y, Wu Y, Wang C. The echocardiographic changes of pre and after treatments of recombinant streptokinase and urokinase on pulmonary embolism [Abstract]. Respirology 2009;14:A137. [Google Scholar]
Wang 2010 {published data only}
- Wang C, Zhai Z, Yang Y, Wu Q, Cheng Z, Liang L, et al. Efficacy and safety of low dose recombinant tissue‐type plasminogen activator for the treatment of acute pulmonary thromboembolism: a randomized, multicenter, controlled trial. Chest 2010;137:254‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang C, Zhai Z, Yang Y, Yuan Y, Cheng Z, Liang L, et al. Efficacy and safety of 2‐hour urokinase regime in acute pulmonary embolism: a randomized controlled trial [Abstract]. Respiratory Research 2009;10:128. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wu 2010 {published data only}
- Wu YQ, Tao LB, Lu C, Hu YH. An economic evaluation of low dose recombinant human tissue‐type plasminogen activator for the treatment of acute pulmonary thromboembolism. Zhonghua Yi Xue Za Zhi 2010;90:103‐6. [PubMed] [Google Scholar]
Xu 2016 {published data only}
- Xu, QH, Li WL, Cai ZM, Lin YC, Huang SP. Effect of 50 mg alteplase to intermediate‐risk pulmonary embolism with right ventricular dysfunction [阿替普酶50mg方案对伴右心功能不全的中危肺栓塞患者的疗效]. Chung Hua I Hsueh Tsa Chih 2016;96:3062‐6. [DOI] [PubMed] [Google Scholar]
Yang 2007 {published data only}
- Yang D, Zhao G, Wu H, Zhou H, Ji Y, Zhang Z. Comparison of local and systemic thrombolytic treatment for acute massive pulmonary embolism [Abstract]. European Respiratory Journal 2007;30:544s. [Google Scholar]
Yang 2011 {published data only}
- Yang Y, Wang Y, Ma Z, Qiu C, Wu H, Zhang X, et al. Efficacy and safety of two‐hour regimen of recombinant streptokinase versus urokinase in massive and submassive pulmonary embolism [Abstract]. Respirology 2011;16:309. [Google Scholar]
Yilmazel 2018 {published data only}
- Yilmazel U, Araz EO, Kerget B, Yilmaz N, Akgun M, Saglam L. Comparison of long‐term outcomes of 50 and 100 mg rt‐PA in the management of acute pulmonary thromboembolism. Clinical Respiratory Journal 2018;12:1628–34. [DOI] [PubMed] [Google Scholar]
Zhu 2008 {published data only}
- Zhu L, Wang C, Yang Y, Wu Y, Zhai Z, Dai H, et al. Value of transthoracic echocardiography in therapy regimens evaluation in pulmonary embolism. Journal of Thrombosis and Thrombolysis 2008;26:251‐6. [DOI] [PubMed] [Google Scholar]
References to ongoing studies
EUCTR2017‐005075‐91‐DK {published data only}
- EUCTR2017‐005075‐91. Low dose thrombolysis, ultrasound assisted thrombolysis or heparin for intermediate high risk pulmonary embolism. clinicaltrialsregister.eu/ctr‐search/trial/2017‐005075‐91/DK (first posted 25 May 2018).
EudraCT: 2005‐001070‐27 {published data only}
- EudraCT 2005‐001070‐27. Open, randomised, monosite pilot trial for comparison of thrombolytic efficacy of tenecteplase and alteplase in patients with acute pulmonary embolism. clinicaltrialsregister.eu/ctr‐search/search?query=eudract_number:2005‐001070‐27 (first posted 7 July 2005).
NCT01531829 {published data only}
- NCT01531829. Low dose Rt‐PA for acute normotensive pulmonary embolism with RVD. clinicaltrials.gov/ct2/show/NCT01531829 (first posted 13 February 2012).
NCT02604238 {published data only}
- NCT02604238. Efficacy and safety of half dose alteplase added to heparin, in patients with moderate pulmonary embolism (MONALYSE). clinicaltrials.gov/ct2/show/NCT02604238 (first posted 13 November 2015).
NCT03218410 {published data only}
- NCT03218410. Surgical pulmonary embolectomy versus catheter‐directed thrombolysis in the treatment of pulmonary embolism: a non‐inferiority study (Lungembolism). clinicaltrials.gov/ct2/show/NCT03218410 (first posted 14 July 2017).
Additional references
Bottiger 1994
- Bottiger BW, Bohrer H, Bach A, Motsch J, Martin E. Bolus injection of thrombolytic agents during cardiopulmonary resuscitation for massive pulmonary embolism. Resuscitation 1994;28(1):45‐54. [DOI] [PubMed] [Google Scholar]
Browse 1962
- Browse NL, James DC. Streptokinase and pulmonary embolism. The Lancet 1962;2:1039. [DOI] [PubMed] [Google Scholar]
Cao 2014
- Cao Y, Zhao H, Gao W, Wang Y, Cao J. Systematic review and meta‐analysis for thrombolysis treatment in patients with acute submassive pulmonary embolism. Patient Preference and Adherence 2014;28(8):275‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
Chatterjee 2014
- Chatterjee S, Chakraborty A, Weinberg I, Kadakia M, Wilensky RL, Sardar P, et al. Thrombolysis for pulmonary embolism and risk of all‐cause mortality, major bleeding, and intracranial hemorrhage: a meta‐analysis. Journal of the American Medical Association 2014;311(23):2414‐21. [DOI] [PubMed] [Google Scholar]
Chesterman 1969
- Chesterman CN, Biggs JC, Morgan J, Hickie JB. Streptokinase therapy in acute major pulmonary embolism. Medical Journal of Australia 1969;2(22):1096‐100. [DOI] [PubMed] [Google Scholar]
Eberle 2018
- Eberle H, Lyn R, Knight T, Hodge E, Daley M. Clinical update on thrombolytic use in pulmonary embolism: a focus on intermediate‐risk patients. American Journal of Health‐system Pharmacy 2018;75(17):1275‐85. [DOI] [PubMed] [Google Scholar]
Gao 2015
- Gao GY, Yang P, Liu M, Ding M, Liu GH, Tong YL, et al. Thrombolysis for acute intermediate‐risk pulmonary embolism: a meta‐analysis. Thrombosis Research 2015;136(5):932‐7. [DOI] [PubMed] [Google Scholar]
Genton 1968
- Genton E, Wolf P. Urokinase therapy in pulmonary thromboembolism. American Heart Journal 1968;76(5):628‐37. [DOI] [PubMed] [Google Scholar]
Goldhaber 1988
- Goldhaber SZ, Kessler CM, Heit J, Markis J, Sharma GVRK, Dawley D, et al. Randomised controlled trial of recombinant tissue plasminogen activator versus urokinase in the treatment of acute pulmonary embolism. The Lancet 1988;2(8606):293‐8. [DOI] [PubMed] [Google Scholar]
Goldhaber 2002
- Goldhaber SZ. Thrombolysis for pulmonary embolism. New England Journal of Medicine 2002;347(15):1131‐2. [DOI] [PubMed] [Google Scholar]
GRADEpro GDT 2015 [Computer program]
- McMaster University (developed by Evidence Prime). GRADEpro GDT. Version accessed 6 November 2018. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015.
Gupta 2018
- Gupta R, Fortman DD, Morgenstern DR, Cooper CJ. Short‐ and long‐term mortality risk after acute pulmonary embolism. Current Cardiology Reports 2018;20(12):135. [DOI] [PubMed] [Google Scholar]
Hepburn‐Brown 2018
Higgins 2011
- Higgins JP, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org. Wiley‐Blackwell.
Hirsh 1971
- Hirsh J, McDonald IG, Hale GA, O'Sullivan EF, Jelinek VM. Comparison of the effects of streptokinase and heparin on the early rate of resolution of major pulmonary embolism. Canadian Medical Association Journal 1971;104(6):488‐91. [PMC free article] [PubMed] [Google Scholar]
Hyers 1970
- Hyers TM, Stengle JM, Sherry S. Treatment of pulmonary embolism with urokinase. Results of clinical trial (phase 1). Circulation 1970;42(6):979‐80. [DOI] [PubMed] [Google Scholar]
Jaff 2011
- Jaff MR, McMurtry MS, Archer SL, Cushman M, Goldenberg, Goldhaber SZ, et al. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation 2011;123(16):1788‐830. [DOI] [PubMed] [Google Scholar]
Konstantinides 1999
- Konstantinides S, Geibel A, Kasper W. Submassive and massive pulmonary embolism: a target for thrombolytic therapy?. Thrombosis and Haemostasis 1999;82(Suppl 1):104‐8. [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Liu 2014
- Liu Y, Lu Y, Song J, Li D, Liu H, Yang J, et al. Recombinant tissue plasminogen activator for hemodynamically stable patients experiencing an acute pulmonary embolism: a meta‐analysis. Thrombosis Research 2014;134(1):50‐6. [DOI] [PubMed] [Google Scholar]
Marti 2014
- Marti C, John G, Konstantinides S, Combescure C, Sanchez O, Lankeit M, et al. Systemic thrombolytic therapy for acute pulmonary embolism: a systematic review and meta‐analysis. European Heart Journal 2014;36(10):605‐14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Meneveau 2006
- Meneveau N, Séronde MF, Blonde MC, Legalery P, Didier‐Petit K, Briand F, et al. Management of unsuccessful thrombolysis in acute massive pulmonary embolism. Chest 2006;129(4):1043‐50. [DOI] [PubMed] [Google Scholar]
Nakamura 2014
- Nakamura S, Takano H, Kubota Y, Asai K, Shimizu W. Impact of the efficacy of thrombolytic therapy on the mortality of patients with acute submassive pulmonary embolism: a meta‐analysis. Journal of Thrombosis and Haemostasis 2014;12(7):1086‐95. [DOI] [PubMed] [Google Scholar]
NICE 2012
- National Institute for Health and Clinical Excellence. Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing. nice.org.uk/guidance/cg144 2012 (accessed August 2015).
Perlroth 2007
- Perlroth DJ, Sanders GD, Gould MK. Effectiveness and cost‐effectiveness of thrombolysis in submassive pulmonary embolism. Archives of Internal Medicine 2007;167(1):74‐80. [DOI] [PubMed] [Google Scholar]
Review Manager 2014 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Sasahara 1967
- Sasahara AA, Cannilla JE, Belko JS, Morse RL, Criss AJ. Urokinase therapy in clinical pulmonary embolism. A new thrombolytic agent. New England Journal of Medicine 1967;277(22):1168‐73. [DOI] [PubMed] [Google Scholar]
Sasahara 1973
- Sasahara AA, Hyers TM, Cole CM, Ederer F, Murray JA, Wenger NK, et al. The urokinase pulmonary embolism trial: a national co‐operative study. Circulation 1973;47(2 Suppl):7‐21. [PubMed] [Google Scholar]
Sautter 1967
- Sautter RD, Emanuel RA, Fletcher FW, Wenzel FJ, Matson JI. Urokinase for the treatment of acute pulmonary thromboembolism. Journal of the American Medical Association 1967;202(3):215‐8. [PubMed] [Google Scholar]
Sista 2017
- Sista AK, Kuo WT, Schiebler M, Madoff DC. Stratification, imaging, and management of acute massive and submassive pulmonary embolism. Radiology 2017;284(1):5‐24. [DOI] [PubMed] [Google Scholar]
Tapson 2017
- Tapson VF, Friedman O. Systemic thrombolysis for pulmonary embolism: who and how. Techniques in Vascular and Interventional Radiology 2017;20(3):162‐74. [DOI] [PubMed] [Google Scholar]
Tow 1967
- Tow DE, Wagner HN Jr, Holmes RA. Urokinase in pulmonary embolism. New England Journal of Medicine 1967;277(22):1161‐7. [DOI] [PubMed] [Google Scholar]
Yamasawa 1992
- Yamasawa F, Okada Y, Asano K, Mori M, Fujita H, Hasegawa N, et al. The role of recombinant human tissue‐type plasminogen activator in the treatment of acute pulmonary thromboembolism. Internal Medicine 1992;31(7):885‐8. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Dong 2002
- Dong B, Pineo G, Mulrooney T. Thrombolytic therapy for pulmonary embolism. Cochrane Database of Systematic Reviews 2002, Issue 3. [DOI: 10.1002/14651858.CD004437] [DOI] [Google Scholar]
Dong 2006
- Dong BR, Yue J, Liu GJ, Wang Q, Wu T. Thrombolytic therapy for pulmonary embolism. Cochrane Database of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD004437.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Dong 2009
- Dong BR, Hao Q, Yue J, Wu T, Liu GJ. Thrombolytic therapy for pulmonary embolism. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD004437.pub3] [DOI] [PubMed] [Google Scholar]
Hao 2015
- Hao Q, Dong BR, Yue J, Wu T, Liu GJ. Thrombolytic therapy for pulmonary embolism. Cochrane Database of Systematic Reviews 2015, Issue 9. [DOI: 10.1002/14651858.CD004437.pub4] [DOI] [PubMed] [Google Scholar]