

Abstract
Background
Cognitive behavioural therapy (CBT) is a psychosocial treatment that aims to help individuals re‐evaluate their appraisals of their experiences that can affect their level of distress and problematic behaviour. CBT is now recommended by the National Institute for Health and Care Excellence (NICE) as an add‐on treatment for people with a diagnosis of schizophrenia. Other psychosocial therapies that are often less expensive are also available as an add‐on treatment for people with schizophrenia. This review is also part of a family of Cochrane Reviews on CBT for people with schizophrenia.
Objectives
To assess the effects of CBT compared with other psychosocial therapies as add‐on treatments for people with schizophrenia.
Search methods
We searched the Cochrane Schizophrenia Group's Study Based Register of Trials (latest 6 March, 2017). This register is compiled by systematic searches of major resources (including AMED, BIOSIS CINAHL, Embase, MEDLINE, PsycINFO, PubMed, and registries of clinical trials) and their monthly updates, handsearches, grey literature, and conference proceedings, with no language, date, document type, or publication status limitations for inclusion of records into the register.
Selection criteria
We selected randomised controlled trials (RCTs) involving people with schizophrenia who were randomly allocated to receive, in addition to their standard care, either CBT or any other psychosocial therapy. Outcomes of interest included relapse, global state, mental state, adverse events, social functioning, quality of life and satisfaction with treatment. We included trials meeting our inclusion criteria and reporting useable data.
Data collection and analysis
We reliably screened references and selected trials. Review authors, working independently, assessed trials for methodological quality and extracted data from included studies. We analysed dichotomous data on an intention‐to‐treat basis and continuous data with 60% completion rate. Where possible, for binary data we calculated risk ratio (RR), for continuous data we calculated mean difference (MD), all with 95% confidence intervals (CIs). We used a fixed‐effect model for analyses unless there was unexplained high heterogeneity. We assessed risk of bias for the included studies and used the GRADE approach to produce a 'Summary of findings' table for our main outcomes of interest.
Main results
The review now includes 36 trials with 3542 participants, comparing CBT with a range of other psychosocial therapies that we classified as either active (A) (n = 14) or non active (NA) (n = 14). Trials were often small and at high or unclear risk of bias. When CBT was compared with other psychosocial therapies, no difference in long‐term relapse was observed (RR 1.05, 95% CI 0.85 to 1.29; participants = 375; studies = 5, low‐quality evidence). Clinically important change in global state data were not available but data for rehospitalisation were reported. Results showed no clear difference in long term rehospitalisation (RR 0.96, 95% CI 0.82 to 1.14; participants = 943; studies = 8, low‐quality evidence) nor in long term mental state (RR 0.82, 95% CI 0.67 to 1.01; participants = 249; studies = 4, low‐quality evidence). No long‐term differences were observed for death (RR 1.57, 95% CI 0.62 to 3.98; participants = 627; studies = 6, low‐quality evidence). Only average endpoint scale scores were available for social functioning and quality of life. Social functioning scores were similar between groups (long term Social Functioning Scale (SFS): MD 8.80, 95% CI ‐4.07 to 21.67; participants = 65; studies = 1, very low‐quality evidence), and quality of life scores were also similar (medium term Modular System for Quality of Life (MSQOL): MD ‐4.50, 95% CI ‐15.66 to 6.66; participants = 64; studies = 1, very low‐quality evidence). There was a modest but clear difference favouring CBT for satisfaction with treatment ‐ measured as leaving the study early (RR 0.86, 95% CI 0.75 to 0.99; participants = 2392; studies = 26, low quality evidence).
Authors' conclusions
Evidence based on data from randomised controlled trials indicates there is no clear and convincing advantage for cognitive behavioural therapy over other ‐ and sometimes much less sophisticated and expensive ‐ psychosocial therapies for people with schizophrenia. It should be noted that although much research has been carried out in this area, the quality of evidence available is mainly low or of very low quality. Good quality research is needed before firm conclusions can be made.
Plain language summary
Is Cognitive behavioural therapy as effective as other psychosocial treatments for people with schizophrenia
Background
People with serious mental illnesses such as schizophrenia can experience severe disturbances in their thought processes, which may lead to delusions (beliefs that are not based on reality) and hallucinations (seeing and hearing things that are not really there). The standard care for people with schizophrenia is antipsychotic medication, but these medications are not always successful on their own and additional treatments such as psychosocial therapies (including cognitive behavioural therapy (CBT)) are recommended for people with schizophrenia. CBT aims to help people re‐evaluate their views of their symptoms. This process is thought to help reduce distress and change behaviours. It is often used to help people with illnesses such as anxiety and depression. However, CBT is expensive and the evidence for its effectiveness is not clear, particularly for people with schizophrenia.
Searches
The Information Specialist of Cochrane Schizophrenia searched their specialised register for trials that allocated people with schizophrenia to receive either CBT or another type of psychosocial treatment, up to March 2017. These searches found 4117 records. The review authors inspected and screened these records.
Main results
Thirty‐six randomised controlled trials, randomising in total 3542 people with schizophrenia could be included. The quality of evidence from these trials is very low to low. For important outcomes such as relapse, rehospitalisation, mental state, death, social functioning, quality of life no real differences were found between CBT compared with other psychosocial treatments. The number of participants leaving the study early was used as an indirect measure for satisfaction with treatment. Slightly more people allocated to other psychosocial treatments groups left early compared to CBT groups. Results were not robust enough to make firm conclusions.
Conclusions
No firm conclusions can be made regarding the effectiveness of CBT compared to other psychosocial treatments for people with schizophrenia until results from further good‐quality trials are available.
Summary of findings
Summary of findings for the main comparison. CBT compared to ALL OTHER PSYCHOLOGICAL THERAPIES for schizophrenia.
| CBT compared to OTHER PSYCOSOCIAL THERAPIES for people with schizophrenia | ||||||
|
Patient or population: people with schizophrenia Setting: inpatients and outpatients Intervention: CBT+ standard care Comparison: Other psychological therapies + standard care | ||||||
| Outcomes | Anticipated absolute effects* (95% CI) | Relative effect (95% CI) | № of participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Risk with ALL OTHER PSYCHOLOGICAL THERAPIES | Risk with CBT | |||||
| Global state: relapse follow‐up: range 8 weeks to 12 months | Study population | RR 1.05 (0.85 to 1.29) | 375 (5 RCTs) | ⊕⊕⊝⊝ LOW 1,2 | ||
| 463 per 1,000 | 486 per 1,000 (393 to 597) | |||||
| Global state: rehospitalisation* follow‐up: range 70 days to 5 years | Study population | RR 0.96 (0.82 to 1.14) | 943 (8 RCTs) | ⊕⊕⊝⊝ LOW 1,2 | Data for pre‐defined outcome 'clinically important change' not reported. | |
| 375 per 1,000 | 360 per 1,000 (307 to 427) | |||||
| Mental state: General ‐ clinically important change (no improvement) follow‐up: range 12 months to 5 years | Study population | RR 0.82 (0.67 to 1.01) | 249 (4 RCTs) | ⊕⊕⊝⊝ LOW 1,2 | ||
| 636 per 1,000 | 522 per 1,000 (426 to 643) | |||||
| Adverse effect/event: death ‐ any cause follow‐up: range 70 days to 24 months | Study population | RR 1.57 (0.62 to 3.98) | 627 (6 RCTs) | ⊕⊕⊝⊝ LOW 3,4 | ||
| 16 per 1,000 | 25 per 1,000 (10 to 64) | |||||
| Functioning ‐ average scores (Social Functioning Scale, high = good) follow‐up: mean 12 months * | The mean functioning ‐ average scores (Social Functioning Scale, high = good, long term) was 128.5 | MD 8.80 higher (4.07 lower to 21.67 higher) | ‐ | 65 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 2, 5, 6 | Data for pre‐defined outcome 'clinically important change' not reported. |
| Quality of life: average scores (MSQOL, high = good, medium term) follow‐up: mean 6 months * | The mean quality of life: average scores (MSQOL, high = good, medium‐term) was 60.9 | MD 4.50 lower (15.66 lower to 6.66 higher) | ‐ | 64 (1 RCT) | ⊕⊝⊝⊝ VERY LOW 2,6 ,7 | Data for pre‐defined outcome 'clinically important change' not reported. |
| Satisfaction with treatment ‐ leaving the study early for any reason | Study population | RR 0.86 (0.75 to 0.99) | 2392 (26 RCTs) | ⊕⊕⊝⊝ LOW 1,9 | ||
| 247 per 1,000 | 217 per 1,000 (192 to 256) | |||||
| *The risk in the intervention group (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; MD: mean difference; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: We are very confident that the true effect lies close to that of the estimate of the effect Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect | ||||||
1 Downgraded by one level due to risk of bias: some studies had unclear or high risk of bias with blinding of participants and outcome assessments, as well as attrition issues.
2 Downgraded by one level due to imprecision: small sample size and wide confidence interval.
3 Downgraded by one level due to risk of bias: majority of the included studies had unclear risk of blinding of participants and outcome assessments.
4 Downgraded by one level due to imprecision: small event rate and wide confidence interval around effect estimate.
5 Downgraded by one level due to risk of bias: high risk of detection bias due to unblinded assessment.
6 Downgraded by one level due to indirectness: scores from scale were employed as a surrogate index of the intended outcome.
7 Downgraded by one level due to risk of bias: high risk of allocation concealment bias, and unclear risk around blinding.
8 Downgraded by one level due to imprecision: small sample size and wide confidence interval which included appreciable benefit and no effect.
9 Downgraded one level due to indirectness: leaving the study early used to predict satisfaction with treatment
Background
Description of the condition
Schizophrenia is a serious mental illness. It appears in all countries and societies with a rate of approximately 0.5%. Variations occur with men being more affected along with ethnic minorities. Onset is usually in young adulthood. The course is worse if there is an early or insidious onset, if negative symptoms are dominant, or if there is a history of substance abuse (Castle and Morgan 2008). Some of those affected have difficulties with their thoughts, making illogical associations and developing false and sometimes bizarre false explanations (i.e. delusions) for their experiences or symptoms. Problems with false perceptions may occur, for example, hearing voices or seeing visions (hallucinations). Difficulties with concentration, attention and motivation may also lead to poor social and occupational functioning. The range of emotional expression, capacity to think and act may be reduced, together with an inability to experience pleasure. It is customary to view the symptoms of schizophrenia as falling into two broad categories: (i) 'positive' symptoms, which are unusual by their presence (for example, hearing voices); and (ii) 'negative' symptoms, which are unusual by their absence (for example, restricted range and intensity of emotional expression).
Description of the intervention
Medication is the mainstay of treatment for schizophrenia but 5% to 25% of people continue to experience symptoms in spite of medication (Christison 1991; Davis 1977; Meltzer 1992) and may experience side effects that are unwanted and unpleasant.
Talking therapies are often used in addition to medication. In cognitive behaviour therapy (CBT), links are made between the person's feelings and patterns of thinking which underpin their distress. The participant is encouraged to take an active part by using the following techniques.
People are encouraged to establish links between their thoughts, feelings or actions and their current or past symptoms, and/or functioning. It should promote re‐evaluation of people's perceptions, beliefs or reasoning related to the target symptoms and include at least one of the following: people monitoring their own thoughts, feelings or behaviours with respect to their symptoms or recurrence of symptoms promoting alternative ways of coping with the target symptom reducing distress improving functioning.
Examining and disputing the evidence for and against the problematic and/or distressing beliefs and reasons for maintaining problematic behaviours.
Using reasoning abilities and personal experience to develop rational, useful and personally acceptable alternative explanations and interpretations (Alford 1994); and to test these alternative explanations and abandon associated safety behaviours in real‐world situations. Tarrier 1993 has also stressed the beneficial effects of enhancing coping strategies and general problem‐solving skills.
We note that the above description of CBT is consistent with that within the National Institute for Health and Care Excellence (NICE) guidance for CBT‐P (NICE 2014). NICE guidance proposes that CBT should be delivered on a one‐to‐one basis over at least 16 planned sessions and follow a treatment manual.
During the evolution of CBT for schizophrenia, a variety of interventions have been labelled as CBT. We note that not all of these interventions specifically target beliefs (e.g. psychoeducation, relapse prevention, symptom‐focused coping strategies, etc), and it is difficult to provide a single, unambiguous definition of the interventions which can be included under the rubric of CBT. Many of the trials of CBT for psychosis have incorporated additional active therapeutic elements (e.g. psychoeducation and relapse prevention, etc) that would be considered adjunctive to techniques which are specifically targeted at eliciting beliefs and behavioural changes (e.g. guided discovery or behavioural experiments). In recognition, the review authors have constructed criteria that are felt to be workable and to capture the elements of good practice in CBT. These criteria are described below.
How the intervention might work
Cognitive behavioural therapy (CBT) aims to reduce distressing emotional experiences or problematic behaviour by changing the way in which the individual appraises, interprets and evaluates their experiences. CBT encourages the person to identify and challenge unhelpful and distressing interpretations of their experiences. Many CBT programmes (e.g. A ‐ Garety 2008), are based upon a stress‐vulnerability model of symptom onset and relapse. The empirical evidence for the stress‐vulnerability model has been questioned (McKenna 2007). Alternatively, in a theoretical review of the potential change processes that CBT for psychosis might possess, Birchwood 2006 distinguishes between "quasi‐neuroleptic" effects of CBT upon psychotic symptoms (e.g. hallucination) and the emotional and behavioural consequences of such experiences or their treatment. Accordingly, Birchwood 2006 distinguishes between psychotic symptomatology and the emotional distress or problem behaviours that may result from such symptomatology. Birchwood 2006 asserts that, similar to the focus of CBT in affective disorders, the appropriate goal of the CBT intervention is to reduce emotional distress and problem behaviours. Specifically, Birchwood 2006 suggests that CBT might focus upon the following.
Reduction of distress and/or problem behaviour associated with beliefs about psychotic symptomatology.
The emotional and interpersonal difficulty in individuals at high risk of developing psychosis.
Relapse prodromes to prevent relapse in psychosis.
Comorbid depression and social anxiety, including the patient’s appraisal of the diagnosis and its stigmatising consequences.
General stress reactivity, thereby increasing resilience to life stress and preventing psychotic relapse.
Increasing self‐esteem and social confidence in people with psychosis.
Nevertheless, many of the current trials of CBT for psychosis have defined their outcomes in terms of psychotic symptomatology (e.g. hallucinatory and delusional experiences,) rather than in terms of distress, problem behaviour or stigma and self‐esteem. In clinical practice, interventions are often broad and multifaceted, but when applied to clinical trials such approaches may not specifically address the psychological mechanisms purported by CBT theory to underpin the individuals distress and problem behaviour.
Similarly, more recent developments in psychological therapies have incorporated some of the principles of CBT. However these therapies,such as Acceptance and Committment Therapy and Compassion Focused Therapy do not explicitly target beliefs regarding psychotic experiences and their implications. Rather, the focus is on accepting mental experience and developing compassion with greater focus on modifying affect rather than cognition. These therapies, which are often referred to as "third wave therapies", address mental events and distress more broadly and focus on beliefs about mental life in general (rather than specific beliefs related to symptoms).
Why it is important to do this review
Despite national treatment guidelines recommending CBT as an adjunct therapy for serious mental illness (NICE 2014), CBT is still not as widely available for people with schizophrenia as it is for people with other disorders (for example, depression and panic disorder).
The first case report of CBT for delusional beliefs in 1952, reported by Beck 2005, did not lead to widespread development of CBT for schizophrenia or its symptoms. Psychological interventions have become more widely accepted over the past two decades and are now seen as part of a comprehensive set of routine interventions in the treatment and management of schizophrenia (NICE 2014). However, the availability of CBT and other evidence‐based therapies on the NHS is extremely limited. The 2012 National Audit reveals that 34% had not been offered psychological therapy with 20% waiting over a year (Royal College of Psychiatrists 2012). The delivery of CBT to people with schizophrenia also depends upon having a commitment from health service managers to support and facilitate training and supervision (Turkington 2004).
Since the publication of the original Cochrane Review of Cognitive behavioural therapy for schizophrenia (Jones 2004), there has been a substantial increase in the number of published and relevant randomised controlled trials (RCTs), and a refinement in the definition and working models of CBT. In addition, there has also been a diversification of research, with trials not only assessing overall effectiveness of CBT but investigating more specific aspects of CBT. It was necessary to update and split the original review of CBT to create a family of CBT reviews (Jones 2009a and Jones 2009b) to incorporate and address these new more diverse data. This particular review provides information about CBT's relative effectiveness compared with other similar adjunct psychosocial therapies.
Objectives
To assess the effects of cognitive behavioural therapy (CBT) compared with other psychosocial therapies as add‐on treatments for people with schizophrenia.
Methods
Criteria for considering studies for this review
Types of studies
All relevant randomised controlled trials (RCTs). We excluded quasi‐randomised trials, such as those where allocation is undertaken on surname. If a trial had been described as double‐blind, but it was implied it had been randomised, we would have included these trials in a sensitivity analysis (see Sensitivity analysis). If identified, we would have included randomised cross‐over studies, but only used data up to the point of first cross‐over because of the instability of the outcomes and the likely carry‐over effects of all treatments.
As CBT requires the person to actively engage and participate in the therapy, it may not be possible to blind the participant to treatment condition (that is, it may not be possible to provide a placebo control condition to reduce the effects of an anticipated outcome on behalf of the participant). However, it is both possible and desirable to blind the researcher to condition (that is, the person collecting outcome data is unaware of the allocation of the individual participant). Accordingly, single‐blind trials are considered of appropriate methodological quality for the assessment of this type of intervention.
We would have compared the outcomes of trials that described a single‐blind procedure with trials that did not describe any blinding procedure. If there was no substantive difference within primary outcomes (see Types of outcome measures), when these non‐blinded studies were added, then we would have included them in the final analysis. If there was a substantive difference, we would have used only single‐blinded randomised trials and the results of the sensitivity analysis would have been described in the text.
Types of participants
People with a current diagnosis of schizophrenia, diagnosed by any criteria, irrespective of gender or race. We did not include participants who had very late onset of illness (onset after the age of 60 years) or those with other psychotic disorders such as bipolar affective disorder, substance‐induced psychosis, significant physical or sensory difficulties or people with co‐existing developmental disorders and/or learning disabilities. If studies randomised people with schizophrenia and those with the above disorders, we only included trials where more than 50% of the participants had a diagnosis of schizophrenia.
This review does not include trials that report outcomes from participants deemed to be "at‐risk" of developing schizophrenia in the future.
We are interested in making sure that information is as relevant as possible to the current care of people with schizophrenia, so aimed to highlight the current clinical state clearly (acute, early post‐acute, partial remission, remission), as well as the stage (prodromal, first episode, early illness, persistent), and whether the studies primarily focused on people with particular problems (for example, negative symptoms, treatment‐resistant illnesses).
Types of interventions
1. Cognitive behavioural therapy (CBT)
The label cognitive behavioural therapy has been applied to a variety of interventions, accordingly, is difficult to provide a single, unambiguous definition. Recognising this, the review authors constructed criteria that were felt to be both workable and to capture the elements of good practice in CBT.
In order to be classified as 'well‐defined', the intervention must clearly demonstrate the following components:
a discrete psychological intervention, which is in addition to, and separate from, other therapeutic interventions (for example, behavioural family therapy) and
recipients establish links between their symptoms, thoughts and beliefs, and consequent distress or problem behaviour and
the re‐evaluation of their perceptions, beliefs or reasoning relating to the target symptoms; this may include the re‐evaluation of situation specific "inferential" beliefs or more global "evaluative" beliefs.
All therapies that did not meet these criteria (or that provided insufficient information) but were labelled as 'CBT' or 'Cognitive Therapy' were included as 'less‐well‐defined CBT'. We conducted a sensitivity analysis on the primary outcomes of this review(seeTypes of outcome measures) in order to investigate whether a 'well‐defined' implementation of this therapy presents with differential outcomes.
In addition, for primary outcomes, we undertook sensitivity analyses between studies that employed experienced CBT therapists compared with relatively inexperienced CBT therapists. Experienced CBT therapists were defined as:
persons possessing appropriate professional qualifications for the provision of CBT (e.g. British Association of Behavioural and Cognitive Psychotherapy (BABCP) accreditation, Diploma in CBT, or other professionally‐accredited qualifications involving CBT as major part of training (e.g. Clinical or Counselling Psychologist)) or
in situations where the qualifications of the therapist are unclear but they appear to have received training in CBT or specific training for the trial and there is clear evidence of the use a thorough adherence protocol.
Unqualified CBT therapists may be defined as persons not possessing appropriate professional qualifications or with no appropriate accreditation, report of training and use of an adherence protocols.
2. Other psychosocial treatments
Other psychosocial treatments includes standard care that has been supplemented by additional psychological or social interventions, or both, such as supportive therapy, psychoeducation, family therapy and other 'talking therapies'.
This review distinguishes between trials that described 'active' psychosocial interventions (e.g. family therapy) aimed at a meaningful symptom reduction and those trials which have used 'non active' psychosocial interventions (e.g, unstructured conversations), which act as merely a control for the non‐specific effects of therapy (e.g. time spent with a therapist). Study labels are prefaced with an "A‐" or an "NA‐" to indicate whether an active or non active intervention was used as a comparison condition and the pooled effect of these trials is also presented.
3. Standard care
The care a person with schizophrenia would normally receive had they not been involved in the trial. This normally includes a biological, psychological and social approach to care including antipsychotic medication, and utilisation of services including hospital stay, day hospital attendance and community psychiatric nursing involvement.
Types of outcome measures
Outcomes can be categorised as being of short‐, medium‐ or long duration. A short‐term outcome is defined as occurring within the period typically associated with active treatment. The National Institute for Health and Care Excellence (NICE) asserts that "for it to make a difference, [the patient] should have CBT treatment for more than 16 planned sessions" (NICE 2014). Accordingly, in this review, we have grouped outcomes into those measured in the short term (within 24 weeks of the onset of therapy), medium term (within 24 to 52 weeks of the onset of therapy) and long term (over 52 weeks since the onset of therapy).
Outcomes can also be grouped into broad areas (Table 2).
1. Outcome categories.
| Category | Description |
| General functioning | These relate to meaningful changes in symptomatology and general clinical condition, recovery and well‐being. |
| Mental state | These refer to presence or absence of symptoms of psychosis as well as continuous measures relating to characteristics of psychotic symptoms (e.g. preoccupation; conviction; frequency; duration; intensity, loudness; perceived interference with daily living) and insight. Measures of general affect are also considered (e.g. anxiety, depression, shame, hopelessness, anger; self‐esteem) and symptom‐related affect measures (e.g. voice‐related distress; delusional distress).The presence or frequency of problematic behaviours are included (such as suicide attempts; deliberate self‐harm; violence to others, etc) and functional and adaptive behaviours (e.g. increased coping strategies) . |
| Adverse outcomes | All health interventions have the capacity for unintended and unwanted side effects. To‐date there has been a paucity of studies that have attempted to identify adverse effects of psychological therapies. Such outcomes might include dependency, increased distress, increased family dysfunction and disengagement from mental health services. |
| Service utilisation | The measurement of service utilisation and functional outcomes may convey important information regarding health economic benefits, as well as provide indirect markers of personal independence. Such outcomes might include number of acute hospital or inpatient days, number of acute hospital admissions or equivalent (e.g. home treatment/crisis team intervention; respite admissions), changes in legal status under mental health legislation (Department of Health 1983), changes in level of care (including accommodation type and intensity of service (Assertive Outreach Team versus Community Mental Health Team)). |
| Functional outcomes | These outcomes might include changes in employment, occupational and educational status, level of received social security benefits or social welfare, perceived quality of life and level of social functioning. |
| Pharmacological treatment | These outcomes would include alterations in the degree of compliance with the prescribed medication regimen, as well as alterations to the prescribed medication including changes in type of medication and prescribed dosage. Unwanted side effects will also be assessed. |
| Economic outcomes | These outcomes would include both the direct costs of CBT (e.g. costs relating to the provision of therapy) and the indirect costs of CBT (e.g. reduction in medication, reduction in relapse, etc). |
CBT: Cognitive behavioural therapy
We aimed to report binary outcomes recording clear and clinically meaningful degrees of change (e.g. global impression of much improved, or more than 50% improvement on a rating scale ‐ as defined within the trials) before any others. Thereafter, we listed other binary outcomes and then those that are continuous.
* see Differences between protocol and review.
Primary outcomes
1. Global state
1.1 Relapse 1.2 Clinically important change ‐ as defined by the individual studies (for example, global impression much improved, or less than 50% reduction on a specified rating scale) ‐ short‐, medium‐ and long term.
2. Mental state
2.1 Clinically important change ‐ as defined by the individual studies (for example, mental state much improved, or less than 50% reduction on a specified rating scale) ‐ short‐, medium‐ and long term.
Secondary outcomes
1. Global state
1.1 Hospitalisation. 1.2 Healthy days. 1.3 Average endpoint/change score global state scale.
2. Mental state
2.1 Any change in general mental state. 2.2 Average endpoint general mental state score. 2.3 Average change in general mental state scores. 2.4 Clinically important change in specific symptoms. 2.5 Any change in specific symptoms. 2.6 Average endpoint specific symptom score. 2.7 Average change in specific symptom scores.
3. Adverse effect/event(s)
3.1 Any adverse effect/event(s) 3.2 Average endpoint general adverse effect score. 3.3 Average change in general adverse effect scores. 3.4 Clinically important adverse effect/event ‐ as defined by individual studies. 3.5 Any specific adverse effects. 3.6 Average endpoint specific adverse effects. 3.7 Average change in specific adverse effects.
4. Functioning
4.1 Average endpoint general functioning score. 4.2 Average change in general functioning scores. 4.3 Clinically important change in specific aspects of functioning, such as social or life skills. 4.4 Any change in specific aspects of functioning, such as social or life skills. 4.5 Average endpoint specific aspects of functioning, such as social or life skills. 4.6 Average change in specific aspects of functioning, such as social or life skills.
5. Quality of life
5.1 Clinically important change in quality of life ‐ as defined by individual studies. 5.2 Any change in quality of life. 5.3 Average endpoint quality of life score. 5.4 Average change in quality of life scores. 5.5 Clinically important change in specific aspects of quality of life ‐ as defined by individual studies. 5.6 Any change in specific aspects of quality of life. 5.7 Average endpoint specific aspects of quality of life. 5.8 Average change in specific aspects of quality of life.
6. Satisfaction with treatment
6.1 Leaving the study early: specific reason 6.2 Recipient of care satisfied with treatment. 6.3 Recipient of care average satisfaction score. 6.4 Recipient of care average change in satisfaction scores. 6.5 Carer satisfied with treatment. 6.6 Carer average satisfaction score. 6.7 Carer average change in satisfaction scores.
7. Engagement with services
7.1 Clinically important engagement ‐ as defined by individual studies. 7.2 Any engagement. 7.3 Average endpoint engagement score. 7.4 Average change in engagement scores. 7.5 Compliance with medication/treatment.
8. Economic
8.1 Direct costs. 8.2 Indirect costs.
'Summary of findings' tables
We used the GRADE approach to interpret findings (Schünemann 2011); and used GRADEpro GDT to export data from our review to create a 'Summary of findings' table. These tables provide outcome‐specific information concerning the overall certainty of evidence from each included study in the comparison, the magnitude of effect of the interventions examined, and the sum of available data on all outcomes we rate as important to patient care and decision making. We selected the following main outcomes for inclusion in the 'Summary of findings' table.
Global state: relapse
Global state: clinically important change ‐ as defined by individual studies
Mental state: general ‐ clinically important change ‐ as defined by individual studies
Adverse effect: clinically important adverse effect/event ‐ as defined by individual studies
Functioning: clinically important change in social functioning
Quality of life: clinically important change
Satisfaction with treatment ‐ leaving the study early for any reason
If data were not available for these pre‐specified outcomes but were available for ones that are similar, we presented the closest outcome to the pre‐specified one in the table but took this into account when grading the finding.
Search methods for identification of studies
Electronic searches
1. Electronic searches
1.1 The Cochrane Schizophrenia Group's Register (March 2010 to 6 March 2017)
This was searched by the Information Specialist of the Cochrane Schizophrenia Group, Samantha Roberts, using the phrase:
{[(*cogniti* AND (*behavio* or therap*)) OR (*cogniti* and (*technique* or *restructur* or *challeng*)) OR (*self* and (*instruct* or *management* or *attribution*)) OR (*rational* and *emotiv*) in title, abstract, index terms of REFERENCE] or [Cognitive* in interventions of STUDY]}
This register is compiled by systematic searches of major databases, handsearches and conference proceedings (see group module).
2. Details of previous searches for previous CBT review
For search details used in previous versions, please see Appendix 1.
Searching other resources
1. Reference lists
We searched all references of included articles for further relevant trials.
2. Authors
For this update, we did not contact the first author of each of the included papers to request additional published and unpublished materials.
Data collection and analysis
Below are methods used for 2015 and 2017 searches. Previous methods can be seen in Appendix 2.
Selection of studies
Review authors (JX, SZ, DH, and CJ) independently inspected all identified citations. When disputes arose as to which category a citation should be allocated, resolution was achieved by either discussion with the other review authors, or obtaining a full report of the citation. Review authors (JX, SZ, DH and CJ) obtained and independently inspected full reports of citations meeting the review inclusion criteria. When disputes arose as to whether an full report should be included or excluded from the review, JX, SZ, DH and CJ resolved by discussion. If it had not been possible to resolve by discussion, we would have asked another review author (CI) to read the full report and to make a final judgement.
Data extraction and management
1. Extraction
Review authors JX, SZ, DH and CJ extracted data from all included studies. We resolved disputes by discussion. When it was not possible to extract data or if further information was needed, we attempted to contact the authors in order to obtain missing information or for clarification whenever necessary. Where multi‐centre studies reported outcomes separately for each component centre, we extracted data relevant to each component centre and reported these separately.The reporting of data from component centres was only undertaken when this procedure did not bias the overall sample size for the statistical tests.
2. Management
2.1 Forms
We extracted data onto standard, simple forms.
2.2 Scale‐derived data
We included continuous data from rating scales only if:
the psychometric properties of the measuring instrument have been described in a peer‐reviewed journal (Marshall 2000);
the measuring instrument has not been written or modified by one of the trialists for that particular trial; and
the instrument should be a global assessment of an area of functioning and not sub‐scores which are not, in themselves, validated or shown to be reliable.
It should be noted that some sub‐scale scores were included in this review (for instance, we did include sub‐scores from mental state scales measuring positive and negative symptoms of schizophrenia), however, in all cases the sub‐scale scores were well‐validated and are in common use within the empirical literature.
Ideally, the measuring instrument would either be i. a self‐report or ii. completed by an independent rater or relative (not the therapist). We realise that this is not often reported clearly; in Description of studies, where possible, we noted if this was the case or not.
2.3 Endpoint versus change data
There are advantages of both endpoint and change data: change data can remove a component of between‐person variability from the analysis; however, calculation of change needs two assessments (baseline and endpoint) that can be difficult to obtain in unstable and difficult‐to‐measure conditions such as schizophrenia. We preferred to use endpoint data throughout.
2.4 Skewed data
Continuous data on clinical and social outcomes are often not normally distributed. To avoid the pitfall of applying parametric tests to non‐parametric data, we applied the following standards to relevant continuous endpoint data before inclusion.
For endpoint data from studies including fewer than 200 participants:
a) when a scale starts from the finite number zero, we subtracted the lowest possible value from the mean, and divided this by the standard deviation (SD). If this value was lower than one, it strongly suggests that the data are skewed and we excluded these data. If this ratio was higher than one but less than two, there is suggestion that the data are skewed: we entered these data and tested whether their inclusion or exclusion would change the results substantially. If the data changed results, we presented them as 'other' data. Finally, if the ratio was larger than two, we included these data, because it is less likely they are skewed (Altman 1996; Higgins 2011).
b) if a scale starts from a positive value (such as the Positive and Negative Syndrome Scale (PANSS), which can have values from 30 to 210 (Kay 1986)), we modified the calculation described above to take the scale starting point into account. In these cases skewed data are present if 2 SD > (S − S min), where S is the mean score and 'S min' is the minimum score.
Please note: we entered all relevant data from studies of more than 200 participants in the analysis irrespective of the above rules, because skewed data posed less of a problem in large studies.
2.5 Common measure
To facilitate comparison between trials, where possible, we converted variables that were reported in different metrics, such as days in hospital (mean days per year, per week or per month) to a common metric (e.g. mean days per month).
2.6 Conversion of continuous to binary
Where possible, we converted continuous outcome measures to dichotomous data. This could be done by identifying cut‐off points on rating scales and dividing participants accordingly into 'clinically improved' or 'not clinically improved'. It is generally assumed that if there had been a 50% reduction in a scale‐derived score such as the Brief Psychiatric Rating Scale (BPRS, Overall 1962) or the PANSS (Kay 1987), this can be considered as a clinically significant response (Leucht 2005a; Leucht 2005b). If data based on these thresholds were not available, we used the primary cut‐off presented by the original authors.
2.7 Direction of graphs
We aimed to enter data in such a way that the area to the left of the line of no effect indicates a favourable outcome for CBT.
Assessment of risk of bias in included studies
Review authors (JX, SZ DH and CJ) assessed risk of bias using the tool described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011a). This tool encourages consideration of how the randomisation sequence was generated, how allocation was concealed, the integrity of blinding at outcome measurement, the completeness of outcome data, selective reporting and other biases. We excluded studies where sequence generation was at a high risk of bias or where allocation was clearly not concealed. If disputes arose as to the correct category for a trial, this was resolved through discussion and, if necessary, adjudication by the other review authors (AM, CI and IC). If this was not possible because further information was necessary, we intended not to enter the data but to allocate the trial to the list of those awaiting assessment. Review authors were not blinded to the names of the authors, institutions, journal of publication, or results of the trials.
Measures of treatment effect
We adopted P = 0.05 as the conventional level of a clear difference (statistically significant), but we were especially cautious where results were only slightly below this, and in these situations we reported 95% confidence intervals (CI) in preference to P values.
1. Binary data
For binary outcomes, we calculated a standard estimation of the risk ratio (RR) and its 95% CI as it has been shown that RR is more intuitive than odds ratios (Boissel 1999); and that odds ratios tend to be interpreted as RR by clinicians (Deeks 2000). Although the number needed to treat for an additional beneficial outcome (NNTB) and the number needed to treat for an additional harmful outcome (NNTH), with their CIs, are intuitively attractive to clinicians, they are problematic to calculate and interpret in meta‐analyses (Hutton 2009). For binary data presented in the 'Summary of findings' table(s) where possible, we calculated illustrative comparative risks.
2. Continuous data
For continuous outcomes we estimated mean differences (MD) and the 95% CI between groups. We preferred not to calculate effect size measures (standardised mean difference (SMD)). However, if scales that are very similar had been used, we would have presumed there is a small difference in measurement, and we would have calculated effect size and transform the effect back to the units of one or more of the specific instruments.
Unit of analysis issues
1. Cluster trials
Studies increasingly employ 'cluster randomisation' (such as randomisation by clinician or practice), but analysis and pooling of clustered data poses problems. Firstly, authors often fail to account for intra‐class correlation in clustered studies, leading to a 'unit of analysis' error (Divine 1992), whereby P values are spuriously low, CIs unduly narrow and statistical significance overestimated. This causes type I errors (Bland 1997; Gulliford 1999).
Where clustering was not accounted for in primary studies, we had planned to present data in a table, with a (*) symbol to indicate the presence of a probable unit of analysis error. In subsequent versions of this review, if such data are reported, we will seek to contact first authors of studies to obtain intra‐class correlation coefficients (ICCs) for their clustered data and to adjust for this by using accepted methods (Gulliford 1999). Where clustering has been incorporated into the analysis of primary studies, we will present these data as if from a non‐cluster randomised study, but adjust for the clustering effect.
We have sought statistical advice and been advised that the binary data presented in a report should be divided by a 'design effect'. This is calculated using the mean number of participants per cluster (m) and the ICC [Design effect = 1+(m‐1)*ICC] (Donner 2002). If the ICC is not reported, it is assumed to be 0.1 (Ukoumunne 1999).
If cluster studies had been appropriately analysed taking into account ICCs and relevant data documented in the report, synthesis with other studies would have been possible using the generic inverse variance technique.
2. Cross‐over trials
A major concern of cross‐over trials is the carry‐over effect. It occurs if an effect (e.g. pharmacological, physiological or psychological) of the treatment in the first phase is carried over to the second phase. As a consequence, on entry to the second phase, the participants can differ systematically from their initial state despite a wash‐out phase. For the same reason cross‐over trials are not appropriate if the condition of interest is unstable (Elbourne 2002). As both effects are very likely in severe mental illness, we planned to use only the data from the first phase of the study.
3. Studies with multiple treatment groups
Where a study involves more than two treatment arms, if relevant, we presented the additional treatment arms in comparisons. If data were binary we simply added these and combine within the two‐by‐two table. If data were continuous, we combined data following the formula in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011). Where additional treatment arms are not relevant, we did not reproduce these data.
Dealing with missing data
1. Overall loss of credibility
At some degree of loss to follow‐up, the findings of a trial must lose credibility (Xia 2009). We were forced to make a judgment where the level of loss to follow‐up was too great for short‐term trials to be included in this review. If more than 40% of data were unaccounted for at eight weeks, we did not use these data within the analyses.
2. Binary
If attrition for a binary outcome was between 0% and 40% and if the outcomes of these participants were described, we included these data as reported. Where these data were not clearly described for the primary outcome, we assumed the worst for each person who was lost to follow‐up, and for adverse effects, we assumed rates similar to those among participants who continued to have their data recorded.
3. Continuous
3.1 Attrition
We have reported data where attrition for a continuous outcome was between 0% and 40% and completer‐only data were reported in the study.
3.2 Standard deviations
We first tried to obtain the missing values from the authors. If not available, where there were missing measures of variance for continuous data but an exact standard error (SE) and CI were available for group means, and either 'P' value or 't' value were available for differences in mean, we noted these, and in future versions of this review we will calculate them according to the rules described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011): When only the SE is reported, standard deviations (SDs) can be calculated by the formula SD = SE * square root (n). Chapters 7.7.3 and 16.1.3 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011) present detailed formulae for estimating SDs from P values, t or F values, CIs, ranges or other statistics. If these formulae do not apply, in the future we will calculate SDs according to a validated imputation method which is based on the SDs of the other included studies (Furukawa 2006). Some of these imputation strategies can introduce error. The alternative would be to exclude a given study’s outcome and thus to lose information. We will examine the validity of the imputations in a sensitivity analysis excluding imputed values.
3.3 Assumptions about participants who left the trials early or were lost to follow‐up
Various methods are available to account for participants who left the trials early or were lost to follow‐up. Some trials just present the results of study completers; others use the method of last observation carried forward (LOCF); while more recently, methods such as multiple imputation or mixed‐effects models for repeated measurements (MMRM) have become more of a standard. While the latter methods seem to be somewhat better than LOCF (Leon 2006), we feel that the high percentage of participants leaving the studies early and differences between groups in their reasons for doing so is often the core problem in randomised schizophrenia trials. Therefore, we did not exclude studies based on the statistical approach used. However, by preference we used the more sophisticated approaches, i.e. we preferred to use MMRM or multiple‐imputation to LOCF, and we only presented completer analyses if some kind of intention‐to‐treat (ITT) data were not available at all. Moreover, we addressed this issue in the item 'Incomplete outcome data' of the 'Risk of bias' tool.
Assessment of heterogeneity
1. Clinical heterogeneity
We considered all included studies initially, without seeing comparison data, to judge clinical heterogeneity. We simply inspected all studies for clearly outlying situations or people which we had not predicted would arise. When such situations or participant groups arose, these were fully discussed.
2. Methodological heterogeneity
We considered all included studies initially, without seeing comparison data, to judge methodological heterogeneity. We simply inspected all studies for clearly outlying methods which we had not predicted would arise. When such methodological outliers arose, these were fully discussed.
3. Statistical heterogeneity
3.1 Visual inspection
We visually inspected graphs to investigate the possibility of statistical heterogeneity.
3.2 Employing the I2 statistic
Heterogeneity between studies was investigated by considering the I2 method alongside the Chi2 'P' value. The I2 provides an estimate of the percentage of inconsistency thought to be due to chance (Higgins 2003). The importance of the observed value of I2 depends on i. magnitude and direction of effects and ii. strength of evidence for heterogeneity (e.g. 'P' value from Chi2 test, or a CI for I2). We interpreted an I2 estimate greater than or equal to 75% accompanied by a statistically significant Chi2 statistic as evidence of substantial levels of heterogeneity (Deeks 2011). When substantial levels of heterogeneity were found in the primary outcome, we explored reasons for heterogeneity (Subgroup analysis and investigation of heterogeneity).
Assessment of reporting biases
Reporting biases arise when the dissemination of research findings is influenced by the nature and direction of results (Egger 1997 ). These are described in section 10.1 of the Cochrane Handbook for Systematic reviews of Interventions (Sterne 2011).
1. Protocol versus full study
We attempted to locate protocols of included randomised trials. If the protocol was available, we compared outcomes in the protocol and in the published report. If the protocol was not available, we compared outcomes listed in the methods section of the trial report with actually reported results.
2. Funnel plot
We are aware that funnel plots may be useful in investigating reporting biases but are of limited power to detect small‐study effects. We did not use funnel plots for outcomes where there were 10 or fewer studies, or where all studies were of similar size. In other cases, where funnel plots were possible, we sought statistical advice in their interpretation.
Data synthesis
We understand that there is no closed argument for preference for use of fixed‐effect or random‐effects models. The random‐effects method incorporates an assumption that the different studies are estimating different, yet related, intervention effects. To us, this often seems to be true and the random‐effects model takes into account differences between studies, even if there is no statistically significant heterogeneity. There is, however, a disadvantage to the random‐effects model: it puts added weight onto small studies, which often are the most biased ones. Depending on the direction of effect, these studies can either inflate or deflate the effect size. We chose to use fixed‐effect for all analyses, except where if was high heterogeneity where the source of heterogeneity could not be identified.
Subgroup analysis and investigation of heterogeneity
1. Subgroup analyses
We anticipated subgroup analyses to test the hypothesis that CBT may be highlighted to have different effects when compared with the following.
1.1 Active versus non active control therapies
Active psychological treatments as opposed to inactive ones.
We aimed to undertake the analysis for only the primary outcomes of this review or the nearest we could find to them (see Types of outcome measures), and if data were available discussed the findings.
2. Investigation of methodological heterogeneity
We considered all included studies initially, without seeing comparison data, to judge methodological heterogeneity. We simply inspected all studies for clearly outlying methods which we had not predicted would arise and would have discussed any such methodological outliers if they had arisen.
3. Investigation of statistical heterogeneity
3.1 Visual inspection
We inspected graphs visually to investigate statistical heterogeneity.
3.2 Employing the I² statistic
We investigated statistical heterogeneity between studies by considering the I² statistic alongside the Chi² P value. The I² statistic provides an estimate of the percentage of inconsistency thought to be due to chance (Higgins 2003). The importance of the observed value of I² depends on the magnitude and direction of effects as well as the strength of evidence for heterogeneity (e.g. P value from Chi²¬test, or a confidence interval for I²). We interpreted an I² estimate greater than or equal to 50% and accompanied by a statistically significant Chi² statistic as evidence of substantial heterogeneity (Chapter 9. Cochrane Handbook for Systematic Reviews of Interventions)(Deeks 2011). When substantial levels of heterogeneity were found, we explored reasons for heterogeneity and discussed the findings.
Where unanticipated clinical or methodological heterogeneity were obvious, we simply stated hypotheses regarding these for future reviews or versions of this review. We did not anticipate undertaking additional analyses relating to these.
Sensitivity analysis
If there were substantial differences in the direction or precision of effect estimates in any of the sensitivity analyses listed below, we would not have added data from the lower‐quality studies to the results of the higher‐quality trials, but would have presented these data within a subcategory. If their inclusion did not result in a substantive difference, they remained in the analyses.
1. Implication of randomisation
We planned to include trials in a sensitivity analysis if they were described in some way as to imply randomisation. For the primary outcomes, if there was no substantive difference when the implied randomised studies were added to those studies with better description of randomisation, we would have included these studies.
2. Blinding
We planned to include trials in a sensitivity analysis if they were described in a way that suggested they were blinded for assessment of outcome as opposed to not blinding at all.
3. Well‐defined CBT versus less‐well‐defined CBT
For the primary outcomes, we compared findings for trials meeting our criteria for 'well‐defined' CBT as opposed to those studies that labelled the therapy as CBT, but either did not contain the 'inferential' and 'evaluative' component or which did not provide enough information for this discrimination to be made (see Types of interventions).
4. Therapist experience
For the primary outcomes, we compared findings for trials meeting the criteria for experienced CBT therapists compared with trials using relatively inexperienced CBT therapists or who did not provide enough information for this discrimination to be made (see Types of interventions).
5. Assumptions for lost binary data
Where assumptions had to be made regarding people lost to follow‐up (see Dealing with missing data), we compared the findings of the primary outcomes when we used our assumption and where we compared with completer data only. If there was a substantial difference, we reported these results and discussed them, but continued to employ our assumption.
If assumptions had to be made regarding missing SDs (see Dealing with missing data), we compared the findings on primary outcomes when we use our assumption compared with completer data only. We would have undertaken a sensitivity analysis to test how prone results were to change when 'completer' data only were compared to the imputed data using the above assumption. If there was a substantial difference, we would have reported results and discussed them, but would have continued to employ our assumption.
6. Risk of bias
For the primary outcomes, we analysed the effects of excluding trials that had at high risk of bias across one or more of the domains (see Assessment of risk of bias in included studies).
7. Imputed values
We would have undertaken a sensitivity analysis to assess the effects of including data from trials where we had used imputed values for ICC in calculating the design effect in cluster‐randomised trials.
8. Fixed‐ and random‐effects
For the primary outcomes, we synthesised data using a random‐effects model to evaluate whether this altered the significance of the results.
Results
Description of studies
Thirty‐six studies with 3542 participants are included. Three of these studies (NA ‐ Lewis 2002 (L); NA ‐ Lewis 2002 (M); NA ‐ Lewis 2002 (N)) were actually specific sites of a multicentre trial, NA ‐ Lewis 2002. As some outcome data were only reported with respect to the specific sites, rather than lose these data we have included their outcomes as individual studies.
A summary of the included studies is provided in Characteristics of included studies, and a summary of the excluded studies is provided in Characteristics of excluded studies. Those studies awaiting classification or are ongoing are described in Characteristics of studies awaiting classification and Characteristics of ongoing studies, respectively.
Results of the search
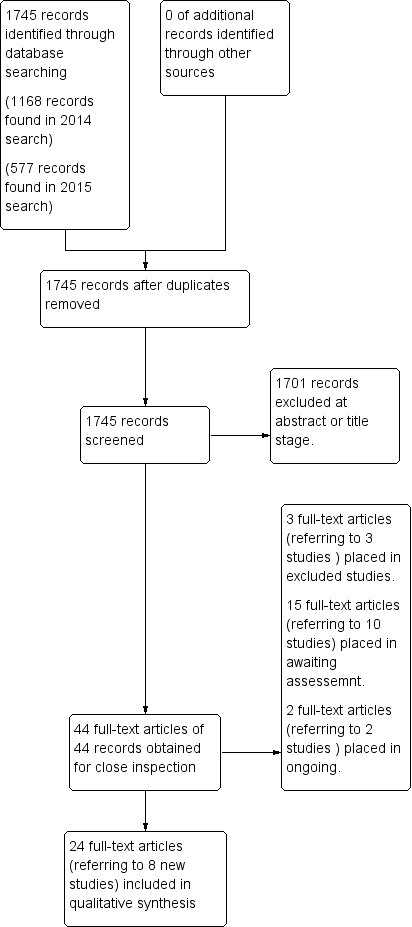
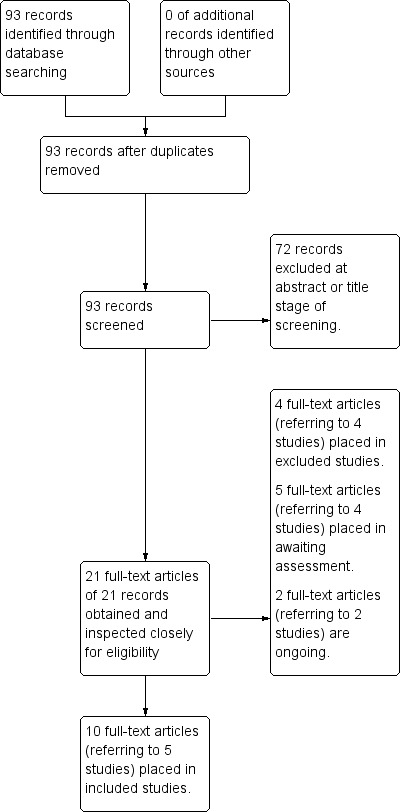
For this update, we ran searches in 2014 (1168 results), 2015 (577 results), and 2017 (93 studies), see Figure 1 and Figure 2.
1.
Study selection from 2014 and 2015 searching
2.
Study selection from 2017 searching
For the previous version of this review (Jones 2012), electronic searches identified 2279 references. Seventy‐four of these reports (62 studies) did not meet the inclusion criteria (see Characteristics of excluded studies) and 31 full‐text reports (referring to 20 studies) were placed in included studies. For this update, searches were carried out in 2014, 2015 and 2017. We have added 13 new studies to the included studies table. One multicentre trial had three sites, resulting in 36 studies contributing data for analyses.
2014 and 2015 searches
One thousand seven hundred and forty‐five additional records were identified; 1701 of these records were excluded at the first screening stage and 44 full‐text articles were obtained for further assessment. Twenty‐four of these full‐text articles (referring to eight studies) were relevant to the review and placed in the included studies table. (A ‐ Granholm 2013; A ‐ Granholm 2014; A ‐ Jiang 2010; A ‐ Lecomte 2008; A ‐ Ma 2012; A ‐ Velligan 2014; A ‐ Wittorf 2010; NA ‐ Davis 2008). Three full‐text articles (referring to three studies) were excluded. Fifteen full‐text articles (referring to 10 studies) were awaiting assessment. Two studies were ongoing. See Figure 1.
2017 search
In this search, 93 additional records were identified. Seventy two of these records were excluded at first screening stage and 21 full‐text articles were obtained for further screening. Ten of these full‐text articles (referring to five studies) were relevant to the review and placed in the included studies table (A ‐ Li 2014; A ‐ Li 2015; A ‐ Li 2015b; NA ‐ Li 2015; NA ‐ Zhang 2015). Four full‐text articles (referring to four studies) were excluded. Five full‐text articles (referring to four studies) are awaiting assessment. Two further studies were placed in the ongoing studies table.SeeFigure 2.
Overall, review authors for this review have screened 4117 records so far and 3950 records have been excluded at the first screening stage. One hundred and sixty‐seven full‐text articles have been obtained for further screening, of which, 69 studies from 81 full‐text reports did not meet the inclusion criteria. Sixteen studies from 21 full‐text articles are awaiting assessment; six of these studies were not printed in English (Chung 2001; Delahaye 2009; Klingberg 2001; Lee 1999; Mirabella 2009; Wu 2008) and the remaining 10 studies are awaiting publication of outcome data (Clarke 2011; D'Souza 2002; ISRCTN60855021 2009; Klingberg 2013; Lystad 2013; NCT00980252 2009; NCT01139502 2010; Penades 2006; Valmaggia 2003; Jones 2012). Four studies are ongoing trials (NCT02170051 2014; NCT02349880 2015; NCT01992913 2014; Xu 2008). Thirty‐six studies are now included in this review Characteristics of included studies. See Figure 3
3.
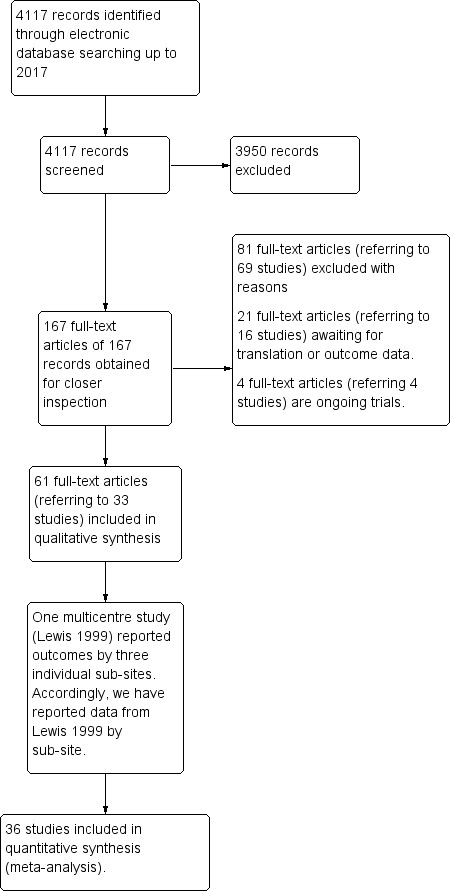
Merged study flow diagrams for all searching up to March 2017
Included studies
1. Duration of trial
The trial duration ranged from six weeks (A ‐ Levine 1998) to 24 months (A ‐ Haddock 1999). In 16 studies, the duration of the trial was within six months (A ‐ Bechdolf 2004; A ‐ Cather 2005; NA ‐ Davis 2008; NA ‐ Haddock 2009; NA ‐ Jackson 2008; A ‐ Jiang 2010; A ‐ Levine 1998; A ‐ Lecomte 2008; A ‐ Li 2015b; NA ‐ Li 2015; A ‐ Ma 2012; A ‐ Penn 2009; A ‐ Pinto 1999; NA ‐ Turkington 2000; NA ‐ Valmaggia 2005; A ‐ Wittorf 2010); For another nine studies, the treatment duration was between six to 12 months (A ‐ Buchkremer 1997; A ‐ Durham 2003; A ‐ Garety 2008;A ‐ Granholm 2013; A ‐ Granholm 2014; A ‐ Klingberg 2012; NA ‐ Sensky 2000; A ‐ Velligan 2014; NA ‐ Zhang 2015 ), and the remaining eight studies observed the effect of a long‐term CBT which is more than 12 months (NA ‐ Drury 2000; A ‐ Haddock 1999; NA ‐ Kemp 1998; NA ‐ Lewis 2002; A ‐ Li 2014; A ‐ Li 2015; NA ‐ O'Donnell 2003; A ‐ Tarrier 1999).
2. Participants
People in these studies were aged between 18 and 65. Participants were selected from in‐patient and out‐patient populations, at varying phases of illness (from acute phase to relatively stable but with treatment resistant symptoms), and with a range of typical co‐morbidities. However, many trials excluded people with co‐morbid substance misuse, evidence of organic brain disorder, learning disability or marked thought disorder and/or conceptual disorganisation.
All 36 trials focused on people with psychosis, whether schizophrenia, delusional disorder or schizoaffective disorder, and all employed operational criteria for diagnoses (DSM III‐R, DSM IV, DSM‐IV TR or ICD‐10). Many people were reported to have co‐morbid mental disorders, such as depression or anxiety disorder.
NA ‐ Jackson 2008 report outcomes for participants with a first episode psychosis. The 28 trials included participants with a representative range of duration of illness. For example, NA ‐ Jackson 2008 reports outcomes from participants with approximate two years length of illness, whereas NA ‐ Drury 2000, A ‐ Bechdolf 2004, A ‐ Garety 2008 and NA ‐ Kemp 1998 included participants with an average of five to 10 years length of illness. A ‐ Durham 2003 and A ‐ Cather 2005 included participants with an average duration of illness in excess of 10 years. A ‐ Cather 2005, A ‐ Buchkremer 1997 included participants with an approximate average of 22.9 years length of illness. Ten studies (NA ‐ Davis 2008; A ‐ Jiang 2010; A ‐ Ma 2012; A ‐ Velligan 2014; A ‐ Wittorf 2010; NA ‐ Haddock 2009; A ‐ Klingberg 2012; NA ‐ O'Donnell 2003; NA ‐ Sensky 2000; NA ‐ Valmaggia 2005) did not report the length of illness of participants.
Participants were recruited from inpatient or outpatients settings from the UK (NA ‐ Drury 2000; A ‐ Durham 2003; A ‐ Garety 2008; A ‐ Haddock 1999; NA ‐ Kemp 1998; NA ‐ O'Donnell 2003; NA ‐ Sensky 2000; A ‐ Tarrier 1999; NA ‐ Turkington 2000), Germany (A ‐ Bechdolf 2004; A ‐ Buchkremer 1997; A ‐ Klingberg 2012; NA ‐ Lewis 2002; A ‐ Wittorf 2010), the USA (A ‐ Cather 2005; A ‐ Penn 2009; A ‐ Pinto 1999; A ‐ Velligan 2014; A ‐ Granholm 2013; A ‐ Granholm 2014), China (A ‐ Jiang 2010; A ‐ Ma 2012), India (NA ‐ Davis 2008), Australia(NA ‐ Jackson 2008), Israel (A ‐ Levine 1998), Belgium (NA ‐ Valmaggia 2005), and Canada (A ‐ Lecomte 2008). It should be noted that several studies were conducted over 10 years ago.
All participants received standard care in addition to CBT or other adjunctive therapies. Standard care would typically include antipsychotic medication. For example, A ‐ Cather 2005 only included participants treated with olanzapine for at least six months, whereas A ‐ Pinto 1999 intentionally selected people with medication‐resistant symptoms.
3. Interventions
3.1 CBT
3.1.1 CBT with other therapeutic activities
In addition to cognitive restructuring, hypothesis testing and behavioural experiments, most CBT interventions commonly included other therapeutic activities such as psychoeducation, relapse prevention, coping strategy enhancement, problem‐solving strategies or relaxation training. Some CBT interventions were administered on a group basis (A ‐ Bechdolf 2004; A ‐ Levine 1998; A ‐ Granholm 2013; A ‐ Granholm 2014; A ‐ Lecomte 2008; A ‐ Penn 2009), whereas others utilised individual therapy (NA ‐ Lewis 2002; NA ‐ Jackson 2008; NA ‐ Valmaggia 2005). NA ‐ Drury 2000, and NA ‐ Davis 2008 employed a combination of both group and individual therapy.
The CBT interventions varied with regard to both the target of the therapy and the degree of specificity of the focus of the intervention. For example, NA ‐ Kemp 1998 and NA ‐ O'Donnell 2003 used a CBT intervention focused specifically on medication compliance, whereas the CBT intervention described by A ‐ Bechdolf 2004 had a wider focus incorporating auditory hallucinations and delusions, anxiety, depression, relapse prevention and enhancing medication compliance. Most trials targeted positive symptoms of psychosis, some with an explicit focus on auditory hallucinations (A ‐ Bechdolf 2004; NA ‐ Haddock 2009; NA ‐ Jackson 2008; A ‐ Penn 2009; NA ‐ Valmaggia 2005; A ‐ Ma 2012; A ‐ Wittorf 2010), and/or delusions (A ‐ Garety 2008; NA ‐ Haddock 2009; NA ‐ Jackson 2008; NA ‐ Valmaggia 2005; A ‐ Ma 2012; A ‐ Wittorf 2010). It was less common for the CBT intervention to target negative symptoms of psychosis (A ‐ Klingberg 2012; A ‐ Ma 2012). Strategies for relapse prevention were a common component in the CBT intervention and a specific focus in some trials (e.g. A ‐ Garety 2008). Emotional distress (A ‐ Bechdolf 2004; NA ‐ Sensky 2000) and self‐esteem (A ‐ Bechdolf 2004; A ‐ Penn 2009), either in general or specifically related to the experience of psychosis, was a target in some trials that also targeted other symptoms. Finally, one trial, NA ‐ Haddock 2009, focused specifically on psychotic symptoms and anger relating to aggression and violence.
3.1.2 CBT arm does not include other active therapies
In 23 trials, the CBT arm was not 'contaminated' by other contemporaneous active psychological therapies, which would not normally be a standard component of CBT for psychosis. However, A ‐ Buchkremer 1997 reported a CBT intervention which variously included medication‐management training or key‐person counselling, or both. The differential effects of the CBT and the medication management training or key‐person counselling were not evaluated. NA ‐ Drury 2000 reported a CBT intervention that consisted of both individual and group cognitive therapy as well as family engagement (aimed at developing familial coping strategies). In addition, it included a structured activity programme (cooking, creative therapy and discussion groups) for an average of five hours per week. Thus, in NA ‐ Drury 2000, the intervention incorporates CBT within a broader rehabilitation framework. The differential effects of the CBT and the rehabilitation were not evaluated. A ‐ Granholm 2013 and A ‐ Granholm 2014 used CBT that consisted of thought‐challenging, social skills training, and problem‐solving training. Finally, A ‐ Pinto 1999 included social skills training in the CBT arm of the trial and also included psychoeducation in the control arm of the trial. Accordingly, the differential effects of these interventions cannot be evaluated.
3.1.3 Well‐defined CBT
All studies employed a cognitive behavioural intervention in addition to standard care. In order to be classified as 'well‐defined' the intervention had to clearly demonstrate the components outlined above (Types of interventions). Only 12 trials met our criteria for 'well‐defined CBT' (A ‐ Bechdolf 2004; A ‐ Cather 2005; NA ‐ Drury 2000; A ‐ Garety 2008; A ‐ Haddock 1999; NA ‐ Haddock 2009; NA ‐ Lewis 2002; A ‐ Pinto 1999; NA ‐ Turkington 2000; NA ‐ Valmaggia 2005; A ‐ Velligan 2014; A ‐ Wittorf 2010) in that they clearly reported a therapeutic focus on belief change or re‐evaluating the subjective meaning of symptoms.
A ‐ Durham 2003 and A ‐ Buchkremer 1997 describe their intervention as CBT and for this reason are included in this review. However, the therapeutic focus appears to be on problem‐solving skills and the development of coping strategies rather than on the re‐evaluation of the subjective symptoms. A ‐ Klingberg 2012 was unique in having a specific focus on negative symptoms, however, reflecting this focus, the intervention incorporated goal setting, initiation, planning and increasing activity levels. Accordingly, the re‐evaluation of the subjective symptoms was not clearly a focus in this intervention. A ‐ Penn 2009 focused on CBT for auditory hallucinations based on Wykes 2004 treatment protocol. The authors, however, acknowledge that their intervention in the CBT arm emphasised the development of coping skills and de‐emphasised cognitive restructuring.
3.1.4 CBT provided by qualified therapists
We defined qualified CBT therapists as:
persons possessing appropriate professional qualifications for the provision of CBT (for example, BABCP accreditation, Diploma in CBT, or other professionally‐accredited qualifications involving CBT as major part of training (for example, Clinical or Counselling Psychologist)); or
in situations were the qualifications of the therapist are unclear but they appear to have received training in CBT or specific training for the trial, and there is a thorough adherence to the protocol.
According to these criteria, 20 trials (71%) met the criteria for qualified CBT therapists, with the remaining studies not providing sufficient information to assess this. There was wide variation in the way in which trials fulfilled this criterion with some having a clearly specified a priori protocol to which adherence was assessed in a structured fashion, whilst others appear to have only a broad CBT‐based agenda and to assess compliance by audio‐taping samples of sessions (NA ‐ Turkington 2000), or by ensuring regular supervision.
3.2 Other psychosocial therapies
In all trials, the other psychosocial therapy arm of the trial was in addition to standard care. The comparison arm of the trials employed a variety of interventions. We characterised interventions aimed at meaningful symptom or distress reduction as active comparison therapy, whereas psychosocial interventions which act as merely a control for the non‐specific effects of therapy (for example, time spent with therapist) were characterised as non active comparison therapy. Some interventions such as supportive psychotherapy or counselling varied in the degree to which they were used as an active and structured therapy. In such cases, allocation to the active or non active conditions was dependent upon whether the authors had made reference to the intervention as a control for the non‐specific effects of therapy. Table 3 describes the interventions in each trial in more detail than is possible in Characteristics of included studies.
2. More detailed description of interventions in the included studies.
| Cognitive Behavioural Therapy | Control therapy | |||||
| No other active therapies | Experienced therapists | Well‐defined CBT | Comments | Active | Nonactive | |
| A ‐ Bechdolf 2004 | √ | √ | √ |
CBT administered by trained psychiatrist or psychologist. CBT strategies included: formulation, guided recovery, symptom monitoring, exposure/focusing strategies for managing voices, hypothesis/reality testing, re‐framing attributions, rational responding, coping strategy enhancement, distraction techniques, role play, anxiety management, depression and self‐esteem work, medication compliance/motivational interviewing, schema work, relapse prevention and keeping well strategies. |
Psychoeducation | |
| A ‐ Buchkremer 1997 | ✗ | ? | ✗ |
CBT included Key Working and Psychoeducation. CBT not provided as a discrete psychological intervention and it is not explicit whether the recipients of the therapy established links between their symptoms, thoughts and beliefs, and consequent distress or problem behaviour· Insufficient information provided regarding the experience of the therapists. |
Psychoeducation regarding medication and structured free time activity | |
| A ‐ Cather 2005 | √ | √ | √ |
No indication other active therapies In the CBT arm of the trial. Treatment was delivered by nine therapists with an average of 7.8 years (SD = 4.77) of experience conducting CBT. Well‐defined CBT: cognitive restructuring, goal setting and coping skills enhancement. |
Psychoeducation | |
| NA ‐ Drury 2000 | ✗ | ? | √ |
CBT included family engagement sessions + structured activity + self‐care skills. Insufficient information provided regarding the experience of the therapists. CBT involved challenging and testing key beliefs. |
Recreation support, leisure and social activities | |
| A ‐ Durham 2003 | √ | √ | ✗ |
The CBT was delivered by five clinical nurse specialists with extensive professional experience of severe mental disorder. All had completed a recognised post‐registration training on standard CBT. All were registered as therapists with the British Association of Behavioural and Cognitive Psychotherapy (BABCP). CBT included: initial emphasis on engagement, education and building a therapeutic alliance; functional analysis of key symptoms, leading to a formulation and problem list; development of a normalising rationale for the patient’s psychotic experiences; exploration and enhancement of current coping strategies; acquisition of additional coping strategies for hallucinations and delusions; and focus on accompanying affective symptomatology using relaxation training, personal effectiveness training and problem‐solving as appropriate. |
Supportive Psychotherapy | |
| NA ‐ Davis 2008 | √ | ? | ✗ | Content: The weekly 1‐hour CBT group therapy intervention includes presentation of didactic material, exercises designed to apply didactic material to participants' experiences at work and work feedback. The weekly 30‐45 minute individual CBT sessions offer personalised application of group material. | supportive group | |
| A ‐ Garety 2008 | √ | √ | √ |
Clinical psychologists employed full time on the trial, provided CBT for 96 individuals (72% of the total). A further 37 participants were seen by a mix of doctoral clinical psychologists and nurses who had received specialist training in CBT. A CBT adherence protocol was used. |
Family Intervention | |
| A ‐ Granholm 2013 | ✗ | √ | ✗ | Group based intervention included thought Challenging, Social Skills Training, and Problem‐Solving Training. Cognitive therapy was combined with role‐play practice of communication skills and problem‐solving training. | Goal‐Focused Supportive Contact | |
| A ‐ Granholm 2014 | ✗ | √ | ✗ | Group based intervention included thought Challenging, Social Skills Training, and Problem‐Solving Training. Cognitive therapy was combined with role‐play practice of communication skills and problem‐solving training. | Goal‐Focused Supportive Contact | |
| A ‐ Haddock 1999 | √ | √ | √ |
CBT was provided by clinical psychologists with expertise in CBT for psychosis. CBT involved formulation, guided discovery, symptom monitoring, exposure/focusing, hypothesis/ reality testing reframing attributions and coping strategy enhancement. |
Supportive counselling and Psychoeducation | |
| NA ‐ Haddock 2009 | √ | √ | √ |
Therapists processed BABCP minimum standards for practice of CBT and were experienced at applying CBT to psychosis. A CBT adherence protocol was used. A therapy manual for each treatment was developed and audio tapes of sessions were assessed by supervisors using the Cognitive Therapy Scale for Psychosis. |
Social activities therapy | |
| NA ‐ Jackson 2008 | √ | √ | ? | Authors reports that CBT was adapted from Kingdon and Turkington (1994), however, insufficient detail is given with regard to specific procedures. | Befriending | |
| A ‐ Jiang 2010 | √ | ? | ✗ | CBT involves remediation of the participants' false cognition; remediation of the harmful behaviour; relaxation training; promote the participants getting involved in recreational activities. | Health education | |
| NA ‐ Kemp 1998 | √ | √ | ? |
No indication of other active therapy in the CBT arm of the trial. The therapists were trained in cognitive‐behavioural psychotherapy. Regular supervision was undertaken to ensure consistency with regard to the delivery of the intervention. Compliance therapy did not make explicit to links between beliefs and affective states, rather beliefs about medication and illness were identified and explored. |
Non‐specific counselling | |
| A ‐ Klingberg 2012 | √ | ? | ✗ |
CBT involved case formulation, goal setting, homework assignments, role play. Focus on initiative and planning, social activity, emotional participation and expression and speech activity. CBT strategies designed specifically to reduce negative symptoms. |
Cognitive Remediation therapy | |
| A ‐ Lecomte 2008 | √ | √ | ✗ | Content: The manual is built in 4 parts: (1) stress: how it affects me; (2) testing hypotheses and looking for alternatives, (3) drugs, alcohol, and how I feel; and (4) coping and competence. | Group social skill training | |
| A ‐ Levine 1998 | √ | ? | √ |
Therapists were previously trained in inducing "cognitive dissonance in person with paranoia". CBT involved identifying relationships between beliefs and behaviours and generating alternative explanations. Insufficient information provided about the experience of the therapists. |
Supportive therapy | |
| NA ‐ Lewis 2002 | √ | √ | √ |
All therapists were eligible for accreditation as cognitive behaviour therapists by the BABCP. CBT involved identifying relationships between beliefs and behaviours and generating alternative explanations. |
Supportive therapy | |
| A ‐ Li 2014 | √ | √ | √ | The trial protocol for using CBT to treat schizophrenia was compiled in Chinese and based on the principles and practice developed by Kingdon & Turkington (2004). | Supportive Therapy | |
| A ‐ Ma 2012 | √ | √ | ? | The CBT therapy referred to Kingdon D et. al's (Kingdon 2005) CBT handbook. The CBT mainly involves therapies for hallucination, delusion, negative symptoms or emotional symptoms, medication compliance and prevention of relapse.Trainee CBT therapists conducted the CBT. | supportive therapy | |
| NA ‐ O'Donnell 2003 | √ | ? | ? |
No indication of other active therapy in the CBT arm of the trial. insufficient details provided regarding the qualifications of the therapist. Compliance therapy did not make explicit to links between beliefs and affective states, rather beliefs about medication and illness were identified and explored. |
Non‐specific counselling | |
| A ‐ Penn 2009 | √ | √ | ✗ |
The therapists included a clinical psychologist, a psychiatrist, a social work graduate student, and doctoral students in clinical psychology with the equivalent of at least a Master's degree in psychology. Adherence measured by rating of audio taped sessions. CBT emphasised coping skills enhancement rather than cognitive restructuring. |
Enhanced supportive therapy | |
| A ‐ Pinto 1999 | ✗ | ? | √ |
CBT arm included individual CBT + social skills training + standard care. Insufficient details provided regarding the qualifications of the therapists. CBT emphasised the "disputation of irrational belief relating to delusions and hallucinations as well as reality testing". |
Supportive therapy | |
| NA ‐ Sensky 2000 | √ | √ | ? |
CBT conducted by experienced psychiatric nurses, who underwent recognised training in CBT, and were registered as therapists by the United Kingdom Council for Psychotherapies. The therapy including "developing a normalizing rationale, treating coexisting anxiety or depression, and generating a shared case formulation. Thereafter, specific techniques were used with positive psychotic symptoms. Thereafter, Socratic questioning was used, and for grandiose or systematised delusions, linked underlying beliefs were identified using inference chaining (the downward arrow technique)". |
Befriending | |
| A ‐ Tarrier 1999 | √ | √ | ✗ |
The therapists were all clinical psychologists. CBT is described as including coping strategies, problem‐solving and relapse prevention. The description of CBT does not include establishing explicit links between beliefs and affective states. |
Supportive counselling | |
| NA ‐ Turkington 2000 | √ | ? | √ |
The CBT arm does not have any other active therapies. insufficient details provided regarding the qualifications of the therapists. CBT is described as "disputation of irrational belief relating to delusions and hallucinations as well as reality testing". |
Befriending | |
| NA ‐ Valmaggia 2005 | √ | √ | √ |
CBT was provided by psychologists specialising in CBT and who were experienced in working with patients with schizophrenia. Treatment fidelity was assessed. CBT "begins with an engagement phase emphasising collaboration and focuses upon delusional distress. In the second phase a shared case formulation is identified, specific techniques are used for symptom and distress reduction. With auditory hallucinations the aim is to change the beliefs about the origin, power and dangerousness of voices. In delusions, the focus is on challenging the dysfunctional beliefs and learning to make more balanced conclusions. In the last phase of therapy, treatment focuses on relapse prevention strategies". |
Supportive counselling | |
| A ‐ Velligan 2014 | √ | √ | √ |
CBTp is a talk therapy designed to treat persistent symptoms of psychosis and the accompanying distress. A 9‐month treatment manual was developed based upon Kingdon and Turkington and included simple handouts and homework assignments based on the work of Granhom et al. The focus of the sessions was on patient identified problems, particularly those that interfered with daily functioning or were distressing, normalizing symptoms, and using CBT techniques to develop alternative explanatory models of event. The CBT was delivered by experienced therapists. |
Cognitive adaptation training | |
| A ‐ Wittorf 2010 | √ | √ | √ |
In collaboration with the patient an individual treatment plan including behaviour analyses is established and treatment goals are retrieved. This process of a ease formulation should be completed until session 9. Afterward, specific cognitive disputing strategies such as work on delusions (e.g. debating persecutory delusions; testing beliefs), hallucinations (e.g. use of a voice diary; work on reattribution with the patient's explanation of voice hearing, and test it out), and cognitive schemata (e.g. linking defectiveness schema to the content of the voices; confronting the patient with evidence that discredits the schema) are the central part of the CBT. The CBT was conducted by 7 specifically trained female clinical psychologists. A mixture of trainees and experienced therapists. |
Supportive therapy | |
| NA ‐ Li 2015 | ? | ? | ? |
The author did not state who delivered CBT the content of CBT includes: patients information and baseline condition was comprehensively collected and evaluated to pave the way for establishment of treatment plan. Towards hallucination, reasonable explanation was developed with patients to ease their anxiety; diary was kept for voices they heard; individual coping strategy was established. Similar process was followed to deal with delusion. Therapists generally adopted the process of identifying problem, establish a rational explanation, reinforce correct perception |
Standard psychological support + pharmacological therapy | |
| A ‐ Li 2015 | ? | ? | ? |
Content: through analysis of underlying causes and developing problem‐solving models to correct patients negative/problematic behaviour, as well as improving patients understanding of the condition. Re‐build behavioural model that is beneficial to patient cognitive ability, reduces social conflict, improve medication compliance and reduce symptoms. Delivered by: psychiatrists taking part in the present study's institution. |
Family intervention or occupational therapy | |
| A ‐ Li 2015b | ? | ? | ? |
Content: three stages and each with distinctive therapeutic goals. Therapy programme was developed with clear focus of each stage and homework was allocated. Initially therapeutic relationship was established by investigating patients feeling towards illness stigma and their perception of the illness. During second stage, CBT techniques were employed to correct the misconception and to incept positive thought model and coping strategy. In final stage, previous learning was reinforced and consolidated. Delivered by: not stated. |
Supportive therapy + pharmacological therapy | |
√ = criteria fulfilled; ✗ = criteria not fulfilled; ? = unclear. BABCP: British Association of Behavioural and Cognitive Psychotherapy; CBT: Cognitive behavioural therapy
Fifteen trials compared CBT with non active control therapies (NA ‐ Davis 2008; NA ‐ Drury 2000; NA ‐ Haddock 2009; NA ‐ Jackson 2008; NA ‐ Kemp 1998; NA ‐ Lewis 2002; NA ‐ Lewis 2002 (L); NA ‐ Lewis 2002 (M); NA ‐ Lewis 2002 (N); NA ‐ Li 2015; NA ‐ O'Donnell 2003; NA ‐ Sensky 2000; NA ‐ Turkington 2000; NA ‐ Valmaggia 2005; NA ‐ Zhang 2015). Twenty‐one trials described active comparison therapies (A ‐ Bechdolf 2004; A ‐ Buchkremer 1997; A ‐ Cather 2005; A ‐ Durham 2003; A ‐ Garety 2008; A ‐ Granholm 2013; A ‐ Granholm 2014; A ‐ Haddock 1999; A ‐ Jiang 2010; A ‐ Klingberg 2012; A ‐ Lecomte 2008; A ‐ Levine 1998; A ‐ Li 2014; A ‐ Li 2015; A ‐ Li 2015b; A ‐ Ma 2012; A ‐ Penn 2009; A ‐ Pinto 1999; A ‐ Tarrier 1999; A ‐ Velligan 2014; A ‐ Wittorf 2010), the most common being psychoeducation and supportive therapy or counselling. Notably, two trials used particularly well‐defined non CBT interventions. A ‐ Garety 2008 reported outcomes compared with family therapy and A ‐ Klingberg 2012 reported outcomes compared with cognitive remediation therapy.
4. Outcomes
4.1 Global state outcomes
Relapse data were reported in seven trials (A ‐ Bechdolf 2004; NA ‐ Drury 2000; A ‐ Garety 2008; A ‐ Haddock 1999; NA ‐ Lewis 2002; A ‐ Tarrier 1999; NA ‐ Valmaggia 2005). However, different studies used varied criteria for relapse. For example, A ‐ Garety 2008 defined relapse as "the re‐emergence of, or significant deterioration in, positive psychotic symptoms of at least moderate degree persisting for at least 2 weeks", whereas A ‐ Bechdolf 2004 defined relapse as "a rating of at least 5 and a 2‐point increase compared with the previous assessment in at least one of the items of the Positive Syndrome Subscale of the PANSS".
Eight trials reported data relating to rehospitalisation (A ‐ Bechdolf 2004; A ‐ Buchkremer 1997; NA ‐ Drury 2000; NA ‐ Jackson 2008; A ‐ Klingberg 2012; NA ‐ Lewis 2002; A ‐ Penn 2009; NA ‐ Sensky 2000).
A few trials also used scales to report global state outcomes. Brief descriptions of these scales are below.
The Global Assessment Scale (GAS) (Endicott 1976)
This scale rates people from zero to 100 on a continuum from psychological or psychiatric sickness to health (high = good). A ‐ Durham 2003 used this scale and reported useable data.
The Global Assessment of Functioning (GAF) (Greenberg 2005)
GAF is a 90‐point rating scale that assesses psychological, social and occupational functioning. A high score indicates a better outcome. Three trials used this scale (NA ‐ Haddock 2009; NA ‐ Kemp 1998; NA ‐ O'Donnell 2003) and reported useable data.
4.2 Mental state outcomes
Seven trials reported important or reliable change in mental health (A ‐ Bechdolf 2004; A ‐ Cather 2005; NA ‐ Drury 2000; A ‐ Durham 2003; A ‐ Garety 2008; NA ‐ Sensky 2000; A ‐ Tarrier 1999). The definitions of important or reliable change varied between the trials. For example, A ‐ Bechdolf 2004 defined clinically important change as greater than two standard deviations on the Positive and Negative Syndrome Scale (PANSS) global score and a statistically significant Reliable Change Index (RCI), A ‐ Cather 2005 defined important or reliable change as a clinically significant reduction of positive symptoms, which is a 20% reduction in PANSS positive factor score, and A ‐ Garety 2008 defined important or reliable change as partial or full remission of symptoms without further episode. NA ‐ Sensky 2000 defined reliable change as greater than 50% improvement and reported outcomes at 18 months from the Comprehensive Psychiatric Rating Scale (CPRS) (CBT 29/46, Befriending 17/44), Montgomery Asberg Depression Rating Scale (MADRS) (CBT 31/46, Befriending 22/44) and the Scale for the Assessment of Negative Symptoms (SANS) (CBT 23/46, Befriending 23/44). For the purpose of this review, the frequency of reliable change was averaged across these three outcome measures.
It was common for trialists to report continuous measures of mental state outcomes. Brief descriptions of scales used by the trials to report mental state outcomes are below.
Brief Psychiatric Rating Scale ‐ BPRS (Overall 1962)
The BPRS is a brief rating scale used to assess the severity of a range of psychiatric symptoms, including psychotic symptoms. The most commonly used version of the scale has 18 items, which are rated from one if not present to seven with high scores indicating poorer functioning. Each item can be defined on a seven‐point scale varying from 'not present' to 'extremely severe'. A ‐ Haddock 1999, A ‐ Lecomte 2008; NA ‐ Kemp 1998 and A ‐ Pinto 1999 reported useable data from the BPRS. NA ‐ Jackson 2008 reported the positive symptoms sub‐scale of the BPRS, but these data were skewed and were not pooled within the meta‐analysis.
Positive and Negative Syndrome Scale (PANSS) (Kay 1987)
This scale is designed to assess the positive symptoms (i.e. delusions, conceptual disorganisation, hallucinations, hyperactivity, grandiosity, suspiciousness/persecution and hostility), negative symptoms (i.e. blunted affect, emotional withdrawal, poor rapport, passive/apathetic social withdrawal, difficulty in abstract thinking, lack of spontaneity and flow of conversation, stereotyped thinking), and general psychopathology (i.e. somatic concern, anxiety, depression, guilt, tension, mannerisms and posture, motor retardation, unco‐operativeness, unusual thought content, disorientation, attentional problems, lack of judgement and insight, disturbance of volition, poor impulse control, preoccupation and active social avoidance). This scale was used by A ‐ Bechdolf 2004, A ‐ Cather 2005, NA ‐ Haddock 2009, A ‐ Levine 1998, NA ‐ Lewis 2002, A ‐ Penn 2009, NA ‐ Valmaggia 2005, A ‐ Garety 2008, A ‐ Granholm 2013, A ‐ Granholm 2014, A ‐ Durham 2003, NA ‐ O'Donnell 2003, and a Chinese version was used by A ‐ Li 2014 and NA ‐ Li 2015. A ‐ Levine 1998 reported the positive symptoms sub‐scale of the PANSS, but these data were skewed and were not pooled within the meta‐analysis.
Comprehensive Psychiatric Rating Scale ‐ CPRS (Asberg 1978)
The Comprehensive Psychiatric Rating Scale is a general psychiatric rating scale. NA ‐ Sensky 2000 used this scale and reported useable data.
Psychotic Symptom Rating Scale ‐ PSYRATS (Haddock 1999b)
This scale is used to assess dimensions of hallucinations and delusions. PSYRATS consists of two scales designed to rate auditory hallucinations and delusions. The items are rated on a five‐point ordinal scale (zero to four).The auditory hallucinations are on an 11‐item scale. Items include frequency, duration, severity and intensity of distress, controllability, loudness, location, beliefs about origin of voices. This scale was used by A ‐ Cather 2005, A ‐ Durham 2003, NA ‐ Haddock 2009, NA ‐ Lewis 2002, and A ‐ Penn 2009. The delusions sub‐scale is a six‐item scale that assesses dimensions of delusions. The items include preoccupation, distress, duration, conviction, intensity of distress and disruption. NA ‐ Lewis 2002 reported useable data from this scale. This scale was also used by A ‐ Cather 2005, A ‐ Durham 2003, NA ‐ Haddock 2009, and A ‐ Penn 2009 used this scale but reported skewed data.
Scale for the Assessment of Positive Symptoms (SAPS) (Andreasen 1984)
SAPS is a rating scale to measure positive symptoms in schizophrenia. The scale is split into four domains, and within each domain separate symptoms are rated from zero (absent) to five (severe). Higher score indicates worse outcome.
Scale for the Assessment of Negative Symptoms (SANS) (Andreasen 1984)
The SANS is designed to assess the negative symptoms of schizophrenia. This six‐point scale gives a global rating of the following negative symptoms: alogia, affective blunting, avolition‐apathy, anhedonia‐asociality and attention impairment. Higher scores indicate more symptoms. A ‐ Pinto 1999 and A ‐ Tarrier 1999 reported useable data from this scale. NA ‐ Jackson 2008 and NA ‐ Sensky 2000 used this scale but reported skewed data.
Symptom Checklist 90 (SCL ‐ 90) (Derogatis 1975)
SCL ‐ 90 is a relatively brief self‐report psychometric instrument (questionnaire). It consists of 90 items, yielding nine scores along primary symptom dimensions and three scores among global distress indices. The primary symptom dimensions that are assessed are somatisation, obsessive‐compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, psychoticism, and a category of "additional items" which helps clinicians assess other aspect of the clients symptoms. A ‐ Li 2015 used this scale and reported useable data.
Beck Depression Inventory (BDI) (Beck 1961)
This is a 21‐item, self‐report questionnaire which measures the intensity of depressive symptoms. A ‐ Granholm 2013, A ‐ Granholm 2014, A ‐ Garety 2008 and A ‐ Penn 2009 used this scale but reported skewed data.
Montgomery Asberg Depression Rating Scale (MADRS) (Montgomery 1979)
This depression rating scale is designed to be sensitive to change. It was developed using a 65‐item comprehensive psychopathology scale to identify the 17 most commonly occurring symptoms in primary depressive illness. Ratings are on 10 items, with higher score indicating poor outcome. Maximum score is 30. NA ‐ Sensky 2000 used this scale, but reported skewed data.
Hamilton Rating Scale for Depression (HAMD) (Hamilton 1967)
The HAMD is 17‐item scale used to assess the severity of depression. Each item was rated on three‐ or five‐point scale. Higher score indicates severe depression. A ‐ Li 2015b used this scale and reported useable data.
Rosenberg Self‐Esteem Scale (RSES) (Rosenberg 1965)
This is a 10‐item, self‐rated measure of self‐esteem. A ‐ Penn 2009 and A ‐ Lecomte 2008 used this scale, but A ‐ Lecomte 2008 reported skewed data.
Stigma Scale for Mental Illness (SSMI) (King 2007)
SSMI is a 28‐item scale to assess the stigma in mental illness. Each item was rated on five‐point scale (from zero to four), with higher score indicating poor self‐esteem. A ‐ Li 2015b used this scale and reported useable data.
Beck Anxiety Inventory (BAI) (Beck 1988)
This is a 21‐item, self‐report questionnaire which measures the intensity of depressive symptoms. A ‐ Garety 2008 and A ‐ Granholm 2013 used this scale, but reported skewed data.
Hamilton Anxiety Rating Scale (HAMA) (Hamilton 1976
The HAMA is a 14‐item psychological questionnaire to assess the severity of anxiety. Each item was rated on five‐point scale, with a possible total score varying from zero to 56. Higher score indicates severe anxiety. A ‐ Jiang 2010 used this scale and reported useable data.
Self‐Rating Anxiety Scale (SARS) (Zung 1971)
SARS is a 20 items self‐report scale to measure the level of anxiety. Four groups of symptoms were rated: central nervous system, motor, cognitive, and automatic symptoms. The overall score ranged from 20 to 80, with higher score indicating more severe anxiety. Useable data from this scale were reported by A ‐ Li 2015b.
Yale‐Brown Obsessive Compulsive Scale (Y‐BOCS) (Goodman 1989)
This is a 10‐item, clinician‐rated scale, which measures the severity of symptoms of obsessive‐compulsive disorder. Each item was rated from zero (no symptoms) to four (extreme symptoms). A ‐ Jiang 2010 used this scale and reported useable data.
Novaco Anger Scale (NAS) (Novaco 2003)
This is a 48‐item, self‐report questionnaire measuring cognitive, behaviour and arousal aspects of anger. NA ‐ Haddock 2009 used this scale and reported useable data.
Novaco Provocation Inventory (NPI) (Novaco 2003)
This is a 25‐item, self‐report questionnaire measuring triggers or provocations to anger. NA ‐ Haddock 2009 used this scale but reported skewed data.
Ward Anger Rating Scale (WARS) (NA ‐ Haddock 2009)
Part A consists of 18 dichotomous, weekly ratings regarding verbal and physical behaviours associated with anger and aggression. Part B consists of seven items regarding affective–behavioural attributes related to anger. NA ‐ Haddock 2009 used this scale but reported skewed data.
Historical Clinical Risk Management ‐ 20 (HCR ‐ 20) (Webster 1997)
This 20‐item, clinician‐rated scale consists of three sub‐scales (i.e. historical factors; clinical factors; and risk factors in relation to the future) relating to risk of violence. NA ‐ Haddock 2009 used this scale but reported skewed data.
4.3 Adverse effects/events
Mortality was only reported in six trials (A ‐ Durham 2003; NA ‐ Lewis 2002; NA ‐ Jackson 2008; NA ‐ O'Donnell 2003; A ‐ Tarrier 1999; A ‐ Klingberg 2012), with NA ‐ Lewis 2002 and NA ‐ Jackson 2008 specifically reporting suicides.
Klingberg 2009 reported rates for 'No adverse effects'. Twenty trials provided information on participants who left the study early (A ‐ Bechdolf 2004; A ‐ Cather 2005; NA ‐ Drury 2000; A ‐ Durham 2003; A ‐ Garety 2008; A ‐ Haddock 1999; NA ‐ Jackson 2008; A ‐ Jiang 2010; NA ‐ Kemp 1998; A ‐ Klingberg 2012; NA ‐ Lewis 2002; A ‐ Ma 2012; NA ‐ O'Donnell 2003; A ‐ Penn 2009; A ‐ Pinto 1999; NA ‐ Sensky 2000; A ‐ Tarrier 1999; NA ‐ Valmaggia 2005; A ‐ Velligan 2014 and A ‐ Wittorf 2010).
4.4 Functioning outcomes
These important outcomes were not reported in binary form (able to look after self, able to hold employment). Scales were employed by a few trials for social and cognitive functioning plus life skills.
Social Functioning Scale (SFS) (Birchwood 1990)
This scale measures social role and behavioural functioning across seven basic areas of community functioning: social engagement, interpersonal behaviour, prosocial activities, recreation, independence, employment. A ‐ Penn 2009 used this scale and reported useable data.
Personal and Social Performance scale (PSP)Morosini 2000
The PSP is a scale to measure social and individual performance, which includes four domains socially useful activities, personal and social relationships, self‐care, disturbing and aggressive behaviours. The overall score ranged from one to 100, with higher scores represent better personal and social functioning. A ‐ Li 2014 used this scale and reported useable data.
Maryland Assessment of Social Competence (MASC) (Bellack 2006)
MASC is a structural behavioural assessment that was used as to measure the functional capacity domain of social competence through conversation. A ‐ Granholm 2014 used this scale and reported useable data.
Social and Occupational Functioning Assessment Scale (SOFAS) (Brambilla 2000)
This is a clinician‐rated measure of social and occupational functioning on a continuum from excellent to grossly impaired functioning. NA ‐ Jackson 2008 and A ‐ Garety 2008 used this scale and reported useable data.
Schedule for Assessment of Insight (SAI) (David 1990)
The SAI measures three separate dimensions of insight: treatment compliance (scale of zero to four), recognition of illness (scale of zero to six), and re‐labelling of psychotic phenomena (scale of zero to four). Higher SAI scores indicate greater insight. A ‐ Li 2014 and NA ‐ O'Donnell 2003 used this scale and reported useable data.
The Insight Scale (Birchwood 1994)
The Insight Scale is a brief eight‐item scale that determines the level of acceptance of a psychiatric condition. A ‐ Lecomte 2008 used this scale and reported useable data.
Beck Cognitive Insight Scale (BCIS) (Beck 2004)
This is a 15‐item, self‐report measure of self‐reflectiveness and over confidence in the interpretation of experiences. A ‐ Penn 2009 and NA ‐ Kemp 1998 used this scale but reported skewed data.
Comprehensive Module Test (CMT) (Liberman 1994)
The CMT is a assess factual knowledge about skills and the application of skills in vignettes, however, it was adapted to assess mastery of the specific content trained in Cognitive Behavioral Social Skills Training (CBSST) in the study A ‐ Granholm 2013 and A ‐ Granholm 2014. The total score ranged from 0 to 33 with higher score indicating better CBSST skill acquisition.
4.5 Quality of life outcomes
Again, few trials reported on quality of life outcomes. Brief description of scales used to report quality of life outcomes are below.
Life Satisfaction Index (LSI) (Wallace 2002)
The LSI measures the overall life satisfaction, which incorporates several domain on well‐being, with higher score indicating more life satisfaction. A ‐ Granholm 2013 used this scale and reported useable data.
European Quality of Life Questionnaire (Brazier 1993).
This is also known as the EuroQoL or the EQ‐5D. This is a self‐rated measure of five dimensions of health‐related quality of life (mobility, self‐care, usual activities, pain/discomfort, anxiety/depression). A ‐ Garety 2008 used this scale and reported useable data.
The Quality of Life Scale (QLS) (Heinrichs 1984a)
The QLS is used to assess deficit symptoms, and is a 21‐item based, semi‐structured interview scale. NA ‐ O'Donnell 2003 used this scale and reported useable data.
Modular System for Quality of Life (MSQoL) (Pukrop 2000)
The MSQoL is a 47‐item based scale that consists of six domains: physical health, vitality, psychosocial relationships, material resources, affect, and leisure time. A ‐ Bechdolf 2004 used this scale and reported useable data.
4.6 Engagement with services
A few attitudes to medication outcomes were reported. Descriptions of the scales used to report these are below.
Attitude to Medication Questionnaire (AMQ)(NA ‐ Kemp 1998)
The AMQ is a 14‐item based scale, with total score ranges from zero to 28. Higher scores indicating more positive attitudes. NA ‐ Kemp 1998 used this scale and reported useable data.
Drug Attitude Inventory (DAI) (Hogan 1983)
The DAI reflects the participants' subjective response to neuroleptics and attitude toward medication, with total score ranges from zero to 30. NA ‐ O'Donnell 2003 used this scale and reported useable data.
Excluded studies
We excluded 69 studies (81 reports) from this review.
1. Issues relating to methods
We excluded 19 studies because they were not randomised controlled trials (RCTs) (Arlow 1997; Bechdolf 2005b; Bouchaud 1996; Buchanan 1992; Chadwick 1994; Garety 1994; Hartman 1983; Hodel 1994; Hogarty 1991; Jackson 1998; Kemp 1996b; Kingdon 1991; Kuipers 1996; May 1984; Perris 1992; Shon 2002; Spaulding 1992; Xie 2010).
2. Issues relating to participants
Two studies reported outcome on individuals at‐risk of psychosis (McGorry 2002; Morrison 2002), and were therefore excluded as they do not apply directly to people with a diagnosis of schizophrenia.
3. Issues relating to comparison
A large number of papers reported CBT compared with standard care (Barrowclough 2001; Barrowclough 2006; Bradshaw 2000; Castle 2002; Daniels 1998; England 2007; Garety 1998; Granholm 2005; Gumley 2003; Jackson 2001; Kuipers 2004; Lysaker 2009; Rector 2003; Sellwood 2001; Startup 1998; Startup 2006; Turkington 2002; Turkington 2006; Wykes 2003), and were therefore excluded from this review as they do not involve an adjunctive comparison therapy.
4. Issues relating to intervention
Several studies reported CBT interventions as part of a broader treatment package where it was not possible to identify the effect of the CBT elements (Edwards 2003; Evins 2001; Haldun 2002; Hayward 1995; Herz 2000). In particular, Anzai 2002 reported comparisons of different types of services (community re‐entry model versus occupational rehabilitation) in which CBT had greater or lesser involvement.
Several studies employed therapeutic strategies that did not meet our criteria for CBT (Bach 2002; Bellucci 2002; Bradshaw 1993; Claghorn 1974; Drake 1993; Fritze 1988; Gaudiano 2006; Hayward 2009; Hogarty 1997; Hogarty 2004; MacPherson 1996; Olbrich 1990; Roder 2002; Tarrier 1993; Van Der Gaag 2003; Velligan 2002; Wykes 2002). Notably, Tarrier 1993 employed coping strategy enhancement which, although a commonly used component of CBT, would not in itself meet our criteria for CBT. The same applied to acceptance and commitment therapy (Bach 2002; Gaudiano 2006), which, like CBT, has a focus on cognitions. However, it aims to help patients respond differently to their thoughts rather than directly challenge or test out their validity. Patients are encouraged to accept and experience their internal events non‐judgmentally. Accordingly, this treatment would not meet our criteria for CBT. Personal therapy (Hogarty 1997), like CBT, aims to prevent relapse and promote personal and social adjustment. However, personal therapy differs from CBT in that it consists of psychoeducation awareness of early signs, supportive therapy techniques, social skills training, the teaching of coping strategies, without an explicit focus on beliefs and cognitive restructuring. Accordingly, this treatment would not meet our criteria for CBT. A ‐ Lecomte 2008 investigated a group‐based CBT intervention, but which did not meet our criteria. Grawe 2006 reported a integrated treatment involving CBTand skill training, which we did not consider eligible.
Seven papers (Bellucci 2002; Fritze 1988; Hogarty 2004; Olbrich 1990; Van Der Gaag 2003; Velligan 2002; Wykes 2002) reported the use of therapeutic strategies designed to overcome intellectual and memory deficits associated with schizophrenia rather than psychotic symptoms, beliefs or cognitive distortions.
5. Issues relating to outcome data
A paper by Wirshing 1992 was excluded because the author did not report data in each group separately .
Risk of bias in included studies
For graphical representation please see Figure 4 and Figure 5.
4.
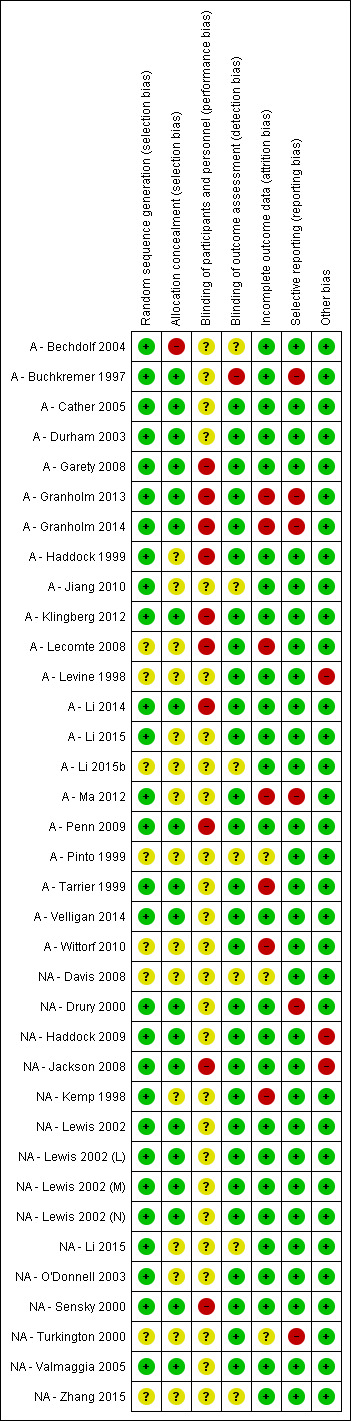
'Risk of bias' summary: review authors' judgements about each 'Risk of bias' item for each included study.
5.
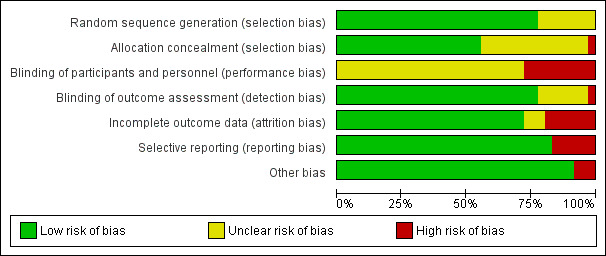
'Risk of bias' graph: review authors' judgements about each 'Risk of bias' item presented as percentages across all included studies.
Allocation
All of the 33 included trials reported some form of randomisation. Twenty‐five reported adequate sequence generation, whist the remaining trial provided insufficient information to rate this particular bias.
Allocation was concealed in 17 studies, with the remaining studies not providing enough information to rate this bias.
Blinding
With respect to blinding of participants and personnel (performance bias) three trials (NA ‐ Drury 2000; NA ‐ Haddock 2009; NA ‐ Turkington 2000) reported attempts at blinding. As noted previously, it is extremely difficult to blind participants and personnel in interventions that require active engagement and participation. Accordingly, the success of these trials to blinding for performance bias remains unclear.
Twenty‐five trials attempted to reduce any detection bias by employing raters who were naive to allocation (A ‐ Cather 2005; A ‐ Durham 2003; A ‐ Garety 2008; A ‐ Granholm 2013; A ‐ Granholm 2014; A ‐ Haddock 1999; A ‐ Klingberg 2012; A ‐ Lecomte 2008; A ‐ Levine 1998; A ‐ Li 2014; A ‐ Li 2015; A ‐ Ma 2012; A ‐ Penn 2009; A ‐ Tarrier 1999; A ‐ Velligan 2014; A ‐ Wittorf 2010; NA ‐ Drury 2000; NA ‐ Haddock 2009; NA ‐ Jackson 2008; NA ‐ Kemp 1998; NA ‐ Lewis 2002; NA ‐ O'Donnell 2003; NA ‐ Sensky 2000; NA ‐ Turkington 2000; NA ‐ Valmaggia 2005). One trial (A ‐ Buchkremer 1997) reported that "Data recorded by trained project staff who were not blind with respect to the group of allocation". The remaining trials did not provide sufficient information and were rated as "unclear risk".
Incomplete outcome data
Seven studies were rated as high risk regarding incomplete data (A ‐ Granholm 2013; A ‐ Granholm 2014; A ‐ Lecomte 2008; A ‐ Ma 2012;A ‐ Tarrier 1999; A ‐ Wittorf 2010; NA ‐ Kemp 1998). In the study NA ‐ Kemp 1998, overall, 35% of participants were lost to follow‐up; 28% from the compliance therapy group and 43% from the control group. Of the 200 participants randomised in the trial by A ‐ Ma 2012, 32 participants left the study early and 48 participants were excluded from the final analysis due to invalid data. Thirty three out of seventy seven participants dropped out from the study by A ‐ Wittorf 2010, and ninty‐two participants (61.7%) left the study early in A ‐ Granholm 2014.
Selective reporting
A ‐ Buchkremer 1997 failed to report a large number, but not all, of their outcomes by individual groups and data were aggregated in a manner which rendered data unsuitable for meta‐analysis. We were unable to use the Psychiatric Assessment Scale (PAS) used by NA ‐ Drury 2000 as the data were only reported in graphical form. The measure of compliance reported in NA ‐ Kemp 1998 was not peer‐reviewed and therefore could not be included. A ‐ Ma 2012 did not report the PANSS and IBS (Irrational Beliefs Scale) scores. A ‐ Granholm 2013 and A ‐ Granholm 2014 measured the mental state by the PANSS scale, however only reported data on a modified version of the positive symptoms scale and the total score of PANSS; as well, the other sub‐scale scores (such as negative symptoms and general psychopathology) were not reported. NA ‐ Turkington 2000 reported many continuous outcomes without standard deviations (SDs) and therefore it was not possible to use these data.
Other potential sources of bias
NA ‐ Haddock 2009 is one of the few trials to report outcome data with regard to problem behaviours. However, a potential source of bias in these data may result from the inclusion of a mixed sample of in‐patients and out‐patients, with a greater opportunity to observe and record aggressive behaviour in the in‐patient sample. A ‐ Levine 1998 contained only six participants in each of the two arms of the trial. Such a small trial could not guarantee that randomisation would be adequate to control for idiosyncratic participant characteristics. NA ‐ Jackson 2008 was rated as high risk of other bias due to the imbalanced baseline characteristics.
Effects of interventions
See: Table 1
Comparison 1: Cognitive behavioural therapy (CBT) versus all other PSYCHOSOCIAL THERAPIES
1. Global state
Four outcomes were reported as indicators of global state; relapse, rehospitalisation, Global Assessment of Functioning (GAF) Scale, and Global Assessment Scale (GAS).
1.1.Global state: 1. Relapse
Seven trials reported data on relapse. (Analysis 1.1)
1.1. Analysis.
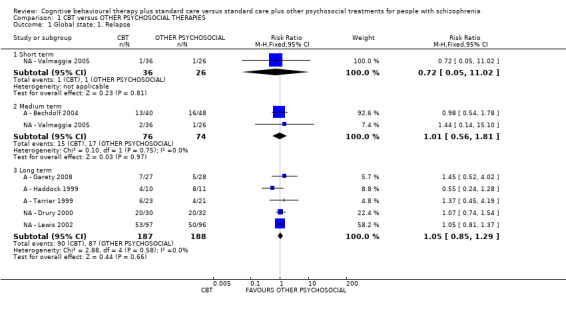
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 1 Global state: 1. Relapse.
1.1.1 Short term
NA ‐ Valmaggia 2005 reported relapse at short‐term follow‐up. No clear difference between CBT and a non active psychosocial therapy was observed in the short term (risk ratio (RR) 0.72, 95% confidence interval (CI) 0.05 to 11.02; participants = 62; studies = 1).
1.1.2 Medium term
A ‐ Bechdolf 2004 and NA ‐ Valmaggia 2005 reported relapse at medium‐term follow‐up. No clear difference between CBT and other psychosocial therapies was observed (RR 1.01, 95% CI 0.56 to 1.81; participants = 150; studies = 2).
1.1.3 Long term
Five studies (NA ‐ Drury 2000; A ‐ Garety 2008; A ‐ Haddock 1999; NA ‐ Lewis 2002; A ‐ Tarrier 1999) reported relapse at long‐term follow‐up . No clear difference between CBT and other psychosocial therapies was observed (RR 1.05, 95% CI 0.85 to 1.29; participants = 375; studies = 5; low‐quality evidence).
1.2 Global state: 2. Average endpoint score (various scales, high = good)
Four trials reported global state data as endpoint scores from the GAS and the GAF scales. (Analysis 1.2).
1.2. Analysis.
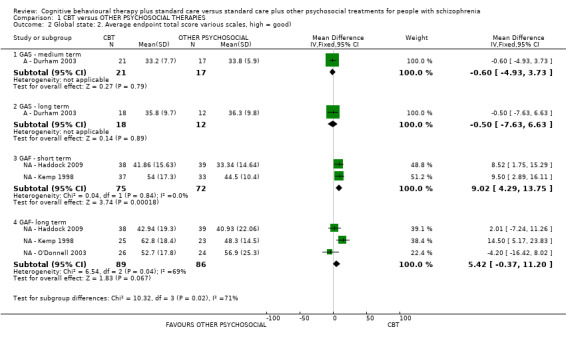
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 2 Global state: 2. Average endpoint total score various scales, high = good).
1.2.1 GAS ‐ medium term
A ‐ Durham 2003 reported medium‐term data. No clear differences between CBT and an active other psychosocial therapy was observed (mean difference (MD) ‐0.60, 95% CI ‐4.93 to 3.73; participants = 38; studies = 1).
1.2.2 GAS ‐ long term
A ‐ Durham 2003 also reported long‐term data. No clear differences between CBT and an active other psychosocial therapy was observed (MD ‐0.50, 95% CI ‐7.63 to 6.63; participants = 30; studies = 1).
1.2.3 GAF ‐ short term
NA ‐ Haddock 2009 and NA ‐ Kemp 1998 reported short‐term data. When compared with inactive psychosocial therapies, a positive effect favouring CBT was observed (MD 9.02, 95% CI 4.29 to 13.75; participants = 147; studies = 2).
1.2.4 GAF ‐ long term
NA ‐ Haddock 2009, NA ‐ Kemp 1998 and NA ‐ O'Donnell 2003 reported long‐term data from the GAF. No effect was observed with long‐term data (MD 5.42, 95% CI ‐0.37 to 11.20; participants = 175; studies = 3; I2 = 69%). These long‐term data have moderate levels of heterogeneity (Chi2 = 6.54; df = 2; P = 0.04; I2 = 69%). The outlier, was the only trial detecting a positive effect for CBT (NA ‐ Kemp 1998). When data from this trial were removed, from the meta‐analysis, homogeneity was restored and the result remained the same.
1.3 Global state: 3. Rehospitalisation
Eight trials reported data for rehospitalisation. (Analysis 1.3).
1.3. Analysis.
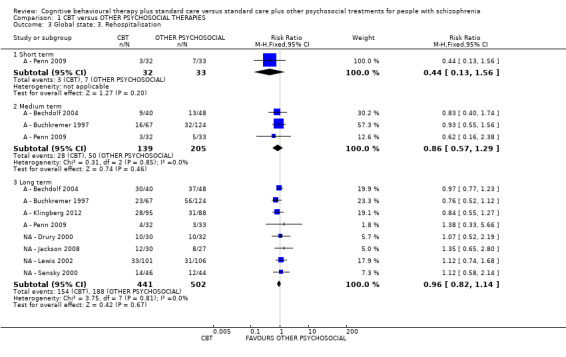
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 3 Global state: 3. Rehospitalisation.
1.3.1 Short term
A ‐ Penn 2009 reported rehospitalisation at short‐term follow‐up. No difference between CBT and an active other psychosocial therapy was observed (RR 0.44, 95% CI 0.13 to 1.56; participants = 65; studies = 1).
1.3.2 Medium term
A ‐ Bechdolf 2004, A ‐ Buchkremer 1997 and A ‐ Penn 2009 reported rehospitalisation at medium‐term follow‐up. No difference between CBT and active other psychosocial therapies was observed (RR 0.86, 95% CI 0.57 to 1.29; participants = 344; studies = 3).
1.3.3 Long term
Eight studies (A ‐ Bechdolf 2004; A ‐ Buchkremer 1997; NA ‐ Drury 2000; NA ‐ Jackson 2008; A ‐ Klingberg 2012; NA ‐ Lewis 2002A ‐ Penn 2009; NA ‐ Sensky 2000) reported rehospitalisation at long‐term follow‐up. No clear difference between CBT and other psychosocial therapies was observed (RR 0.96, 95% CI 0.82 to 1.14; participants = 943; studies = 8, low‐quality evidence).
Mental state
Four outcomes were reported as indicators of general mental state: clinically important change ‐ no improvement (defined by each study, see Characteristics of included studies), average endpoint total scores from British Psychiatric Rating Scale (BPRS), Positive and Negative Symptom Scale (PANSS), and the Comprehensive Psychiatric Rating Scale (CPRS).
1.4 Mental state: 1. General ‐ clinically important change (no improvement)
1.4.1 Short term
The two trials reporting useable data for no improvement in the short term used only active therapies as their control (psychoeducation (A ‐ Cather 2005), and supportive counselling (A ‐ Tarrier 1999)). A positive effect was observed for CBT (RR 0.75, 95% CI 0.58 to 0.99; participants = 87; studies = 2; Analysis 1.4).
1.4. Analysis.
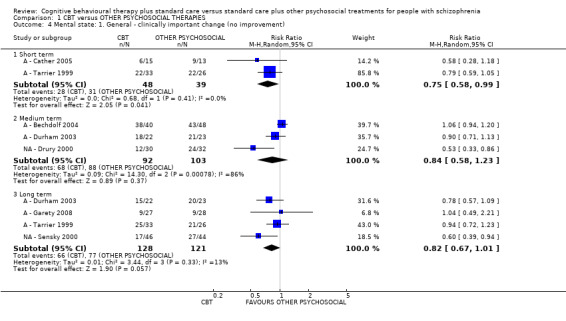
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 4 Mental state: 1. General ‐ clinically important change (no improvement).
1.4.2 Medium term
Medium‐term data were reported by three trials, where both active and non active therapies were used. No difference between CBT and other psychosocial therapies was observed (RR 0.84, 95% CI 0.58 to 1.23; participants = 195; studies = 3; I2 = 86%; Analysis 1.4). This subgroup also had important levels of heterogeneity. The source of heterogeneity could not be identified, so we used a random‐effects model for analyses of these data.
1.4.3 Long term
Long‐term data were reported by four trials where both active and non active therapies were used as control interventions. (n = 249). Again, no clear difference between CBT and other psychological therapies was observed (RR 0.82, 95% CI 0.67 to 1.01; participants = 249; studies = 4; low‐quality evidence; Analysis 1.4).
1.5 Mental state: 2. General (average endpoint total score various scales, high = poor)
Seven trials reported on general mental state by measuring endpoint total scores using the BPRS, the PANSS, and the (CPRS. (Analysis 1.5)
1.5. Analysis.
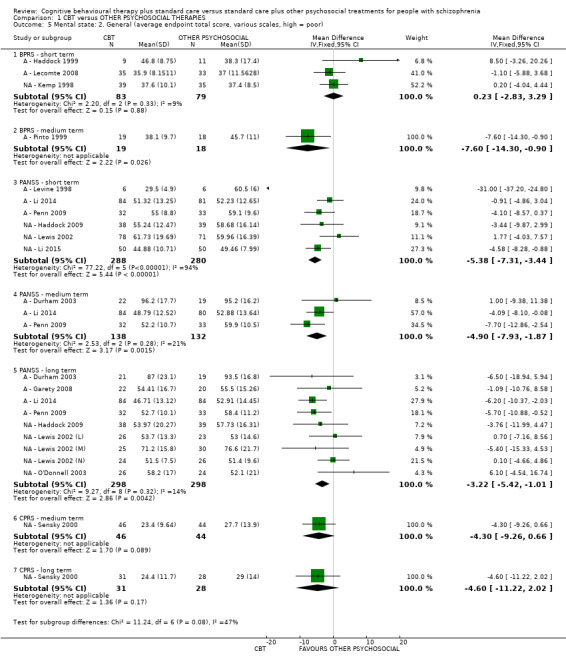
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 5 Mental state: 2. General (average endpoint total score, various scales, high = poor).
1.5.1 BPRS ‐ short term
A ‐ Haddock 1999, A ‐ Lecomte 2008 and NA ‐ Kemp 1998 reported short‐term data. No difference between CBT and other psychosocial therapies (active and non active) was observed (MD 0.23, 95% CI ‐2.83 to 3.29; participants = 162; studies = 3).
1.5.2 BPRS ‐ medium term
A ‐ Pinto 1999 compared CBT with an active therapy (supportive counselling) found a positive effect for CBT in the medium term (MD ‐7.60, 95% CI ‐14.30 to ‐0.90; participants = 37; studies = 1).
1.5.3 PANSS ‐ short term
A ‐ Levine 1998, A ‐ Li 2014, A ‐ Penn 2009, NA ‐ Haddock 2009, NA ‐ Lewis 2002, and NA ‐ Li 2015 reported short‐term data. CBT was compared with both active and non active psychosocial therapies in these trials. A positive effect for CBT was observed (MD ‐5.38, 95% CI ‐7.31 to ‐3.44; participants = 568; studies = 6; I2 = 94%), The short‐term result had an important level of heterogeneity (Heterogeneity: Chi2 = 77.22; df = 5; P < 0.00001; I2 = 94%). This heterogeneity appears to be induced by a very small study (A ‐ Levine 1998), after removing this trial from the meta‐analysis, homogeneity was restored and the result remains the same.
1.5.4 PANSS ‐ medium term
A ‐ Durham 2003, A ‐ Li 2014, and A ‐ Penn 2009 reported medium‐term data. CBT was compared with active psychosocial therapies in these trials. A positive effect for CBT was observed (MD ‐4.90, 95% CI ‐7.93 to ‐1.87; participants = 270; studies = 3)
1.5.5 PANSS ‐ long term
Nine trials comparing CBT with both active and non active psychosocial therapies reported long‐term data. A positive effect was found for CBT (MD ‐3.22, 95% CI ‐5.42 to ‐1.01; participants = 596; studies = 9).
1.5.6 CPRS ‐ medium term
NA ‐ Sensky 2000 reported medium‐term data using the CPRS. No clear difference between CBT and a non active psychosocial therapy was observed (MD ‐4.30, 95% CI ‐9.26 to 0.66; participants = 90; studies = 1)
1.5.7 CPRS long term
NA ‐ Sensky 2000 also reported long‐term data using the CPRS. No clear difference between CBT and a non active psychosocial therapy was observed (MD ‐4.60, 95% CI ‐11.22 to 2.02; participants = 59; studies = 1).
1.6 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS sub scale, high = poor)
Twelve trials reported average endpoint scores from positive symptom sub‐scale of the PANSS (Analysis 1.6).
1.6. Analysis.
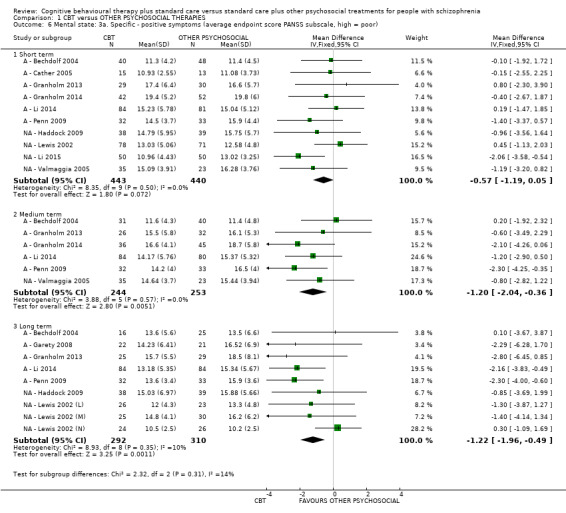
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 6 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS subscale, high = poor).
1.6.1 Short term
Ten trials comparing CBT with both active and non active psychosocial therapies reported short‐term data. No clear difference was observed (MD ‐0.57, 95% CI ‐1.19 to 0.05; participants = 883; studies = 10).
1.6.2. Medium term
Six trials comparing CBT with both active and non active psychosocial therapies reported medium‐term data. A positive effect for CBT was observed (MD ‐1.20, 95% CI ‐2.04 to ‐0.36; participants = 497; studies = 6)
1.6.3 Long term
Nine trials comparing CBT with both active and non active psychosocial therapies reported long‐term data. A positive effect for CBT was observed (MD ‐1.22, 95% CI ‐1.96 to ‐0.49; participants = 602; studies = 9).
1.7 Mental state: 3b. Specific ‐ positive symptoms (average endpoint score various scales, high = poor) ‐ skewed data
A ‐ Levine 1998 reported data showing an advantage for CBT in the short‐term improvement of positive symptoms. However, these data were skewed, and we did not include in analyses, but presented as 'Other data'. (Analysis 1.7).
1.7. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 7 Mental state: 3b. Specific ‐ positive symptoms (average endpoint score various subscales, high = poor) ‐ skewed data.
| Mental state: 3b. Specific ‐ positive symptoms (average endpoint score various subscales, high = poor) ‐ skewed data | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| PANSS ‐ short term | |||||
| A ‐ Levine 1998 | CBT | 7 | 4.6 | 6 | Reporetd as favouring CBT |
| A ‐ Levine 1998 | Other treatments | 13.7 | 2.5 | 6 | |
| SAPS ‐ medium term | |||||
| A ‐ Pinto 1999 | CBT | 17.9 | 17 | 19 | Reported as favouring CBT |
| A ‐ Pinto 1999 | Other treatments | 29.9 | 12.1 | 18 | |
| BPRS ‐ short term | |||||
| NA ‐ Jackson 2008 | CBT | 7.45 | 4.05 | 31 | No difference |
| NA ‐ Jackson 2008 | Other treatments | 7.65 | 4.03 | 31 | |
| BPRS ‐ long term | |||||
| NA ‐ Jackson 2008 | CBT | 7.20 | 4.08 | 31 | No difference |
| NA ‐ Jackson 2008 | Other treatments | 7.55 | 4.76 | 31 | |
1.8 Mental state: 3c. Specific ‐ positive symptoms (average endpoint score BPRS, high = poor) ‐ short term
A ‐ Lecomte 2008 reported short‐term endpoint scores from the positive symptom sub‐scale of the BPRS . No clear difference between the two treatment groups was observed (MD ‐0.10, 95% CI ‐0.45 to 0.25; participants = 68; studies = 1).
1.9 Mental state: 4a. Specific ‐ hallucinations (average endpoint score PANSS, high = poor)
Five trials (A ‐ Penn 2009; A ‐ Cather 2005; A ‐ Durham 2003; NA ‐ Haddock 2009; NA ‐ Lewis 2002) reported on hallucinations using the PANSS sub scale . (Analysis 1.9).
1.9. Analysis.
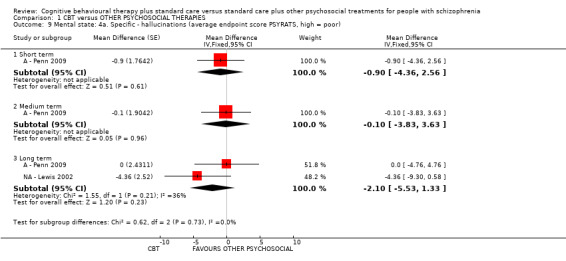
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 9 Mental state: 4a. Specific ‐ hallucinations (average endpoint score PSYRATS, high = poor).
1.9.1 Short term
One study (A ‐ Penn 2009) reported short‐term data, no difference between CBT and an active psychosocial therapy was observed (MD ‐0.90, 95% CI ‐4.36 to 2.56; participants = 0; studies = 1).
1.9 2 Medium term
A ‐ Penn 2009 also reported medium‐term data, again, no difference between CBT and an active psychosocial therapy was observed. (MD ‐0.10, 95% CI ‐3.83 to 3.63; participants = 0; studies = 1).
1.9.3 Long term
Two trials (A ‐ Penn 2009; NA ‐ Lewis 2002) reported long‐term data, and there was no clear difference between CBT and other psychosocial therapies (MD ‐2.10, 95% CI ‐5.53 to 1.33; participants = 0; studies = 2).
1.10 Mental sate: 4b. Specific ‐ hallucinations (average endpoint score Psychotic Symptom Rating Scale (PSYRATS), high = poor) ‐ skewed data
Data reported by other trials for this outcome were skewed and are presented as 'Other data', no clear differences were observed at the individual trial level (Analysis 1.10).
1.10. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 10 Mental state: 4b. Specific ‐ hallucinations (average endpoint score PSYRATS, high = poor) ‐ skewed data.
| Mental state: 4b. Specific ‐ hallucinations (average endpoint score PSYRATS, high = poor) ‐ skewed data | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| Short term | |||||
| A ‐ Cather 2005 | CBT | 18.11 | 11.36 | 15 | Reported no difference |
| A ‐ Cather 2005 | Other treatments | 20.52 | 12.57 | 13 | |
| NA ‐ Haddock 2009 | CBT | 9.74 | 13.92 | 38 | Reported no difference |
| NA ‐ Haddock 2009 | Other treatments | 11.38 | 15.13 | 39 | |
| NA ‐ Lewis 2002 | CBT | 6.15 | 10.31 | 47 | Reported no difference |
| NA ‐ Lewis 2002 | Other treatments | 6.41 | 10.61 | 41 | |
| Medium term | |||||
| A ‐ Durham 2003 | CBT | 17.9 | 13.2 | 21 | Reported no difference |
| A ‐ Durham 2003 | Other treatments | 20.6 | 12.3 | 19 | |
| Long term | |||||
| A ‐ Durham 2003 | CBT | 18.5 | 12.8 | 20 | Reported no difference |
| A ‐ Durham 2003 | Other treatments | 18.0 | 12.2 | 19 | |
| NA ‐ Haddock 2009 | CBT | 9.36 | 12.72 | 38 | Reported no difference |
| NA ‐ Haddock 2009 | Other treatments | 10.38 | 16.63 | 39 | |
1.11 Mental state: 5a. Specific ‐ delusions (average endpoint score PSYRATS, high = poor) ‐ long term
Five trials reported endpoint scores from the delusions sub scale of the PSYRATS, but data were useable from one trial only. NA ‐ Lewis 2002 show no clear difference between CBT and a non active psychosocial therapies at long term (MD ‐1.04, 95% CI ‐3.27 to 1.19; participants = 0; studies = 1; Analysis 1.11).
1.11. Analysis.
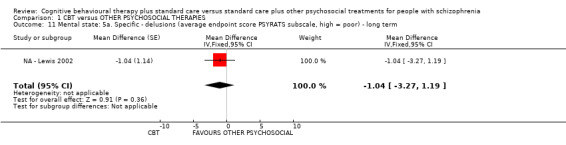
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 11 Mental state: 5a. Specific ‐ delusions (average endpoint score PSYRATS subscale, high = poor) ‐ long term.
1.12 Mental sate: 5b. Specific ‐ delusions (average endpoint score PSYRATS, high = poor) ‐ skewed data
Four trials reported skewed data for this outcome. No clear differences between CBT and other psychosocial therapies in the short term (four RCTs), medium term (two RCTs) or long term (three RCTs) were observed at the individual trial level. (Analysis 1.12).
1.12. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 12 Mental state: 5b. Specific ‐ delusions (average endpoint score PSYRATS subscale, high = poor) ‐ skewed data.
| Mental state: 5b. Specific ‐ delusions (average endpoint score PSYRATS subscale, high = poor) ‐ skewed data | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| Short term | |||||
| A ‐ Cather 2005 | CBT | 10.69 | 6.49 | 15 | Reported as no difference |
| A ‐ Cather 2005 | Other treatments | 10.15 | 7.48 | 13 | |
| A ‐ Penn 2009 | CBT | 8.6 | 7.0 | 32 | Reported as no difference |
| A ‐ Penn 2009 | Other treatments | 10.0 | 6.3 | 33 | |
| NA ‐ Haddock 2009 | CBT | 4.9 | 6.55 | 38 | Reported as favouring CBT |
| NA ‐ Haddock 2009 | Other treatments | 11.04 | 6.7 | 39 | |
| NA ‐ Lewis 2002 | CBT | 6.95 | 7.66 | 74 | Reported as no difference |
| NA ‐ Lewis 2002 | Other treatments | 6.13 | 6.98 | 67 | |
| Medium term | |||||
| A ‐ Durham 2003 | CBT | 13.3 | 5.4 | 22 | Reported as no difference |
| A ‐ Durham 2003 | Other treatments | 11.8 | 6.2 | 19 | |
| A ‐ Penn 2009 | CBT | 8.0 | 7.7 | 32 | Reported as no difference |
| A ‐ Penn 2009 | Other treatments | 10.4 | 5.9 | 33 | |
| Long term | |||||
| A ‐ Durham 2003 | CBT | 11.1 | 5.8 | 21 | Reported as no difference |
| A ‐ Durham 2003 | Other treatments | 9.7 | 6.1 | 19 | |
| A ‐ Penn 2009 | CBT | 6.9 | 7.0 | 32 | Reported as no difference |
| A ‐ Penn 2009 | Other treatments | 9.0 | 6.8 | 33 | |
| NA ‐ Haddock 2009 | CBT | 7.6 | 8.25 | 38 | Reported as no difference |
| NA ‐ Haddock 2009 | Other treatments | 8.38 | 8.03 | 39 | |
1.13 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS, high = poor)
Eleven trials reported endpoint scores using the Negative Symptom sub scale of the PANSS. (Analysis 1.13).
1.13. Analysis.
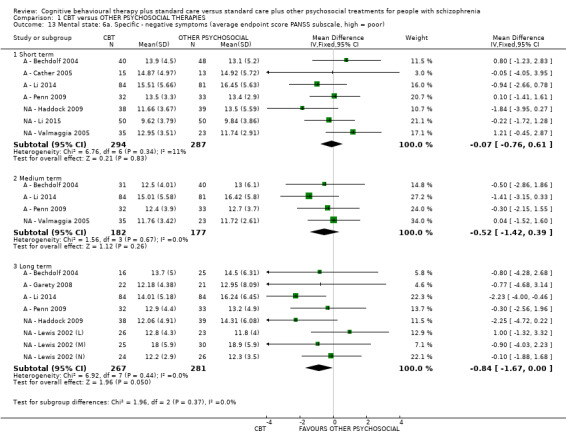
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 13 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor).
1.13.1 Short term
No clear difference between CBT and other psychosocial therapies was observed in the short term (MD ‐0.07, 95% CI ‐0.76 to 0.61; participants = 581; studies = 7)
1.13.2 Medium term
No clear difference between CBT and other psychosocial therapies was observed in the medium term (MD ‐0.52, 95% CI ‐1.42 to 0.39; participants = 359; studies = 4)
1.13.3 Long term
No clear difference between CBT and other psychosocial therapies was observed in the long term (MD ‐0.84, 95% CI ‐1.67 to 0.00; participants = 548; studies = 8).
1.14 Mental state: 6b. Specific ‐ negative symptoms (average endpoint score PANSS, high = poor) ‐ skewed data
A ‐ Levine 1998 also measured negative symptoms by using PANSS sub scale, and found a positive effect for CBT; however, we did not include this very small trial in the meta‐analysis due to skewed data.
1.15 Mental state: 6c. Specific ‐ negative symptoms ‐ average endpoint score (Scale for the Assessment of Negative Symptoms (SANS), high = poor)
Four trials (NA ‐ Jackson 2008; A ‐ Pinto 1999; NA ‐ Sensky 2000; A ‐ Tarrier 1999) reported endpoint scores on the SANS. Two studies reported useable data. (Analysis 1.15)
1.15. Analysis.
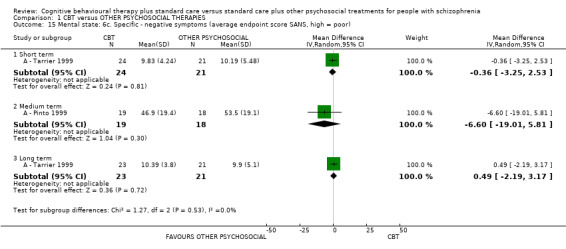
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 15 Mental state: 6c. Specific ‐ negative symptoms (average endpoint score SANS, high = poor).
1.15.1 Short term
No clear difference between CBT and an active psychosocial therapy was observed for this outcome in the short term (MD ‐0.36, 95% CI ‐3.25 to 2.53; participants = 45; studies = 1).
1.15.2 Medium term
No clear difference between CBT and an active psychosocial therapy was observed for this outcome in the medium term (MD ‐6.60, 95% CI ‐19.01 to 5.81; participants = 37; studies = 1).
1.15.3 Long term
No clear difference between CBT and an active psychosocial therapy was observed for this outcome in the long term (MD 0.49, 95% CI ‐2.19 to 3.17; participants = 44; studies = 1).
1.16 Mental state: 6d. Specific ‐ negative symptoms (average endpoint score SANS, high = poor) ‐ skewed data
Skewed data on negative symptoms were reported by two studies (NA ‐ Jackson 2008; NA ‐ Sensky 2000) and are presented as 'Other data' (Analysis 1.16).
1.16. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 16 Mental state: 6d. Specific ‐ negative symptoms (average endpoint score SANS, high = poor) ‐ skewed data.
| Mental state: 6d. Specific ‐ negative symptoms (average endpoint score SANS, high = poor) ‐ skewed data | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| Short term | |||||
| NA ‐ Jackson 2008 | CBT | 17.67 | 10.19 | 31 | Reported no difference |
| NA ‐ Jackson 2008 | Other treatments | 22.88 | 12.87 | 31 | |
| Medium term | |||||
| NA ‐ Sensky 2000 | CBT | 24.7 | 14.0 | 46 | Reported no difference |
| NA ‐ Sensky 2000 | Other treatments | 24.7 | 19.0 | 44 | |
| Long term | |||||
| NA ‐ Jackson 2008 | CBT | 14.66 | 10.9 | 31 | Reported no difference |
| NA ‐ Jackson 2008 | Other treatments | 19.55 | 14.79 | 31 | |
| NA ‐ Sensky 2000 | CBT | 22.8 | 14.5 | 31 | Reported as favouring CBT |
| NA ‐ Sensky 2000 | Other treatments | 33.1 | 22.6 | 28 | |
1.17 Mental state: 6e. Specific ‐ negative symptoms (average endpoint score BPRS sub scale, high = poor) ‐ short term
A ‐ Lecomte 2008 reported short‐term data for this outcome; no difference between treatment groups was observed (MD 0.10, 95% CI ‐0.31 to 0.51; participants = 68; studies = 1; Analysis 1.17).
1.17. Analysis.
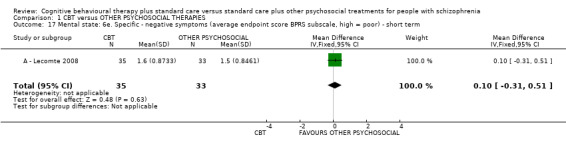
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 17 Mental state: 6e. Specific ‐ negative symptoms (average endpoint score BPRS subscale, high = poor) ‐ short term.
1.18 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS sub scale, high = poor)
Eight trials reported endpoint scores from the general psychopathology sub scale of the PANSS. (Analysis 1.18
1.18. Analysis.
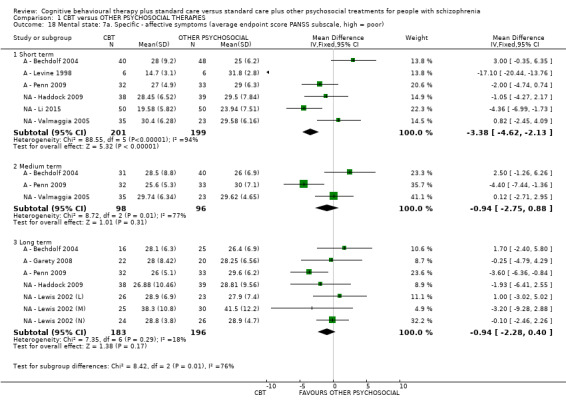
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 18 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor).
1.18.1 Short term
Six trials compared CBT with active and non active psychosocial therapies. A positive effect for CBT was observed at short term (MD ‐3.38, 95% CI ‐4.62 to ‐2.13; participants = 400; studies = 6). This short‐term effect had an important level of heterogeneity (Chi² = 88.55; df = 5; P <0.00001; I2 = 94%). This heterogeneity appears to be induced by a very small study (A ‐ Levine 1998). After removing this trial from the meta‐analysis, the result changed to no clear difference between treatment groups.
1.18.2 Medium term
Three trials compared CBT with active and non active psychosocial therapies. No clear difference was observed at medium term (MD ‐0.94, 95% CI ‐2.75 to 0.88; participants = 194; studies = 3).
1.18.3 Long term
Seven trials compared CBT with active and non active psychosocial therapies. No clear difference was observed at long term (MD ‐0.94, 95% CI ‐2.28 to 0.40; participants = 379; studies = 7).
1.19 Mental state: 7b. Specific ‐ affective symptoms (average endpoint score Symptom Checklist (SCL)90, total, high = poor) ‐ long term
A ‐ Li 2014 reported long‐term endpoint scores from SCL90. A positive effect, favouring the control groups (active psychosocial therapies of family intervention and occupational therapy) was observed (MD 8.26, 95% CI 1.77 to 14.74; participants = 134; studies = 1). (Analysis 1.19).
1.19. Analysis.
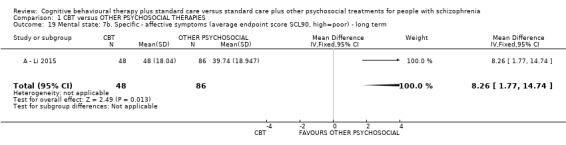
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 19 Mental state: 7b. Specific ‐ affective symptoms (average endpoint score SCL90, high=poor) ‐ long term.
1.20 Mental state: 8a. Specific ‐ depression (average endpoint score BDI, high = poor) ‐ skewed data
Three trials reported outcomes using the Beck Depression Scale (BDI). CBT was compared with enhanced supportive therapy (A ‐ Penn 2009), and group goal‐focused supportive contact (A ‐ Granholm 2013; A ‐ Granholm 2014). However, as data were skewed we did not pool them in the meta‐analysis but presented as 'Other data'. No clear difference between CBTand other therapies was observed in the individual studies. (Analysis 1.20).
1.20. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 20 Mental state: 8a. Specific ‐ depression (average endpoint score BDI, high = poor).
| Mental state: 8a. Specific ‐ depression (average endpoint score BDI, high = poor) | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| Short term | |||||
| A ‐ Granholm 2013 | CBT | 17.2 | 12.3 | 30 | Reported as no difference |
| A ‐ Granholm 2013 | Other treatments | 13.8 | 11.2 | 30 | |
| A ‐ Granholm 2014 | CBT | 17.1 | 11.2 | 42 | Reported as no difference |
| A ‐ Granholm 2014 | Other treatments | 16.7 | 13.6 | 52 | |
| A ‐ Penn 2009 | CBT | 11.4 | 7.6 | 32 | Reported as no difference |
| A ‐ Penn 2009 | Other treatments | 12.6 | 10.2 | 33 | |
| Medium term | |||||
| A ‐ Granholm 2013 | CBT | 15.0 | 12.6 | 26 | Reported as no difference |
| A ‐ Granholm 2013 | Other treatments | 14.3 | 14.0 | 32 | |
| A ‐ Granholm 2014 | CBT | 13.8 | 10.4 | 45 | Reported as no difference |
| A ‐ Granholm 2014 | Other treatments | 14.0 | 10.2 | 36 | |
| A ‐ Penn 2009 | CBT | 10.5 | 8.5 | 32 | Reported as no difference |
| A ‐ Penn 2009 | Other treatments | 13.9 | 10.7 | 33 | |
| Long term | |||||
| A ‐ Garety 2008 | CBT | 15.54 | 10.91 | 22 | Did not report whether there is a significant statistical difference |
| A ‐ Garety 2008 | Other treatments | 21.39 | 13.87 | 18 | |
| A ‐ Granholm 2013 | CBT | 14.4 | 10.2 | 25 | Reported as no difference |
| A ‐ Granholm 2013 | Other treatments | 11.1 | 11.2 | 29 | |
| A ‐ Penn 2009 | CBT | 11.5 | 9.4 | 32 | Reported as no difference |
| A ‐ Penn 2009 | Other treatments | 17.9 | 13.6 | 33 | |
1.21. Mental state: 8b. Specific ‐ depression (average endpoint score Montgomery‐Asberg Depression Rating Scale (MADRS), high = poor)
NA ‐ Sensky 2000 measured depressive symptomatology using the MADRS and compared CBT with a non active control therapy. We could not use these data in analyses as they were skewed and we presented as 'Other data'. (Analysis 1.21).
1.21. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 21 Mental state: 8b. Specific ‐ depression (average endpoint score MADRS, high = poor).
| Mental state: 8b. Specific ‐ depression (average endpoint score MADRS, high = poor) | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| Medium term | |||||
| NA ‐ Sensky 2000 | CBT | 4.9 | 3.5 | 46 | Reported as favouring CBT |
| NA ‐ Sensky 2000 | Other treatments | 7.4 | 4.6 | 44 | |
| Long term | |||||
| NA ‐ Sensky 2000 | CBT | 5.5 | 4.3 | 31 | Reported as no difference |
| NA ‐ Sensky 2000 | Other treatments | 7.0 | 4.6 | 28 | |
1.22 Mental state: 8c. Specific ‐ depression (average endpoint score Hamilton Rating Scale for Depression (HAMD), high = poor) ‐ short term
One trial, compared CBT with an active control, and reported endpoint scores from the HAMD an effect favouring CBT that was observed in the short term (1 RCT, N = 95, MD ‐3.92, CI ‐4.96 to ‐2.88; Analysis 1.22).
1.22. Analysis.
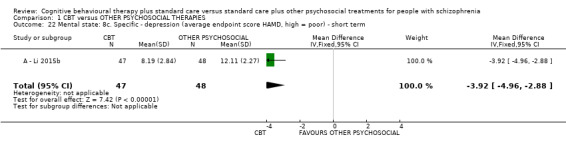
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 22 Mental state: 8c. Specific ‐ depression (average endpoint score HAMD, high = poor) ‐ short term.
1.23 Mental state: 9a. Specific ‐ self‐esteem (average endpoint score Rosenberg Self‐Esteem Scale (RSES), high = poor)
A ‐ Penn 2009 presented data for self‐esteem using the RSES. (Analysis 1.23).
1.23. Analysis.
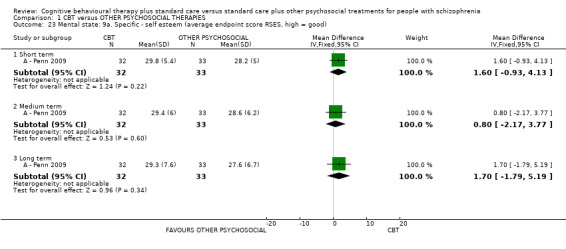
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 23 Mental state: 9a. Specific ‐ self esteem (average endpoint score RSES, high = good).
1.23.1 Short term
No clear difference between CBT and an active psychosocial therapy was observed at short term (MD 1.60, 95% CI ‐0.93 to 4.13; participants = 65; studies = 1).
1.23.2 Medium term
No clear difference between CBT and an active psychosocial therapy was observed at medium term (MD 0.80, 95% CI ‐2.17 to 3.77; participants = 65; studies = 1).
1.23.3 Long term
No clear difference between CBT and an active psychosocial therapy was observed at long term (MD 1.70, 95% CI ‐1.79 to 5.19; participants = 65; studies = 1).
1.24. Mental state: 9b. Specific ‐ self‐esteem (average endpoint score RSES, high = poor) ‐ skewed data
A ‐ Lecomte 2008 also presented self‐esteem data from RSES, but these were skewed and are presented as 'Other data' (Analysis 1.24).
1.24. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 24 Mental state: 9b. Specific ‐ self esteem (average endpoint score RSES, high = good) ‐ short term, skewed data.
| Mental state: 9b. Specific ‐ self esteem (average endpoint score RSES, high = good) ‐ short term, skewed data | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| A ‐ Lecomte 2008 | CBT | 15.4 | 20.66 | 35 | No difference between groups |
| A ‐ Lecomte 2008 | Other treatments | 17.1 | 22.56 | 33 | |
1.25. Mental health: 10. Specific ‐ self‐stigma (average endpoint score Stigma Scale for Mental Illness (SSMI), high = poor) ‐ short term
One study reported endpoint scores from the SSMI. An effect favouring CBT was observed in the short term (MD ‐8.64, CI ‐11.86 to ‐5.42; participants = 95; studies = 1; Analysis 1.25).
1.25. Analysis.
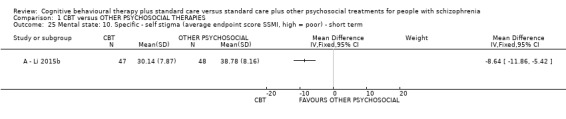
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 25 Mental state: 10. Specific ‐ self stigma (average endpoint score SSMI, high = poor) ‐ short term.
1.26. Mental state: 11a. Specific ‐ anxiety (average endpoint score Beck Anxiety Inventory (BAI), high = poor) ‐ skewed data
Two studies reported skewed data from the BAI for this outcome, and are presented as 'Other data' (Analysis 1.26).
1.26. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 26 Mental state: 11a. Specific ‐ anxiety (average endpoint score BAI, high = poor) ‐ long term, skewed data.
| Mental state: 11a. Specific ‐ anxiety (average endpoint score BAI, high = poor) ‐ long term, skewed data | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| A ‐ Garety 2008 | CBT | 15.82 | 14.67 | 22 | Did not report whether there is a significant statistical difference |
| A ‐ Garety 2008 | Other treatments | 16.41 | 12.79 | 18 | |
| A ‐ Granholm 2013 | CBT | 11.5 | 10.1 | 25 | Reported as no difference |
| A ‐ Granholm 2013 | Other treatments | 10.4 | 11.0 | 29 | |
1.27 Mental state: 11b. Specific ‐ anxiety (average endpoint score Hamilton Anxiety Scale (HAMA), high = poor) ‐ short term
One trial compared CBT with an active psychosocial therapy and measured anxiety using the HAMA. A positive effect was observed for CBT at short tem (MD ‐5.78, 95% CI ‐8.79 to ‐2.77; participants = 65; studies = 1; Analysis 1.27)
1.27. Analysis.
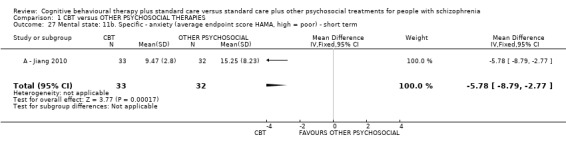
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 27 Mental state: 11b. Specific ‐ anxiety (average endpoint score HAMA, high = poor) ‐ short term.
1.28 Mental state: 11c. Specific ‐ anxiety (average endpoint score Self Rating Anxiety Scale (SRAS), high = poor) ‐ long term
A ‐ Li 2015b measured anxiety using the SRAS, a positive effect for CBT was observed at long term (MD ‐2.89, 95% CI ‐4.53 to ‐1.25; participants = 95; studies = 1; Analysis 1.28).
1.28. Analysis.
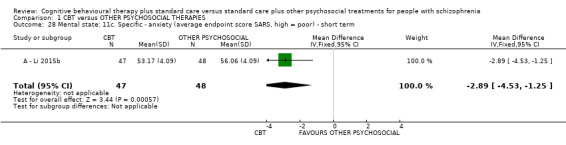
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 28 Mental state: 11c. Specific ‐ anxiety (average endpoint score SARS, high = poor) ‐ short term.
1.29 Mental state: 12a. Specific ‐ clinically important change ‐ Obsessive Compulsive Disorder
A ‐ Jiang 2010 observed a positive effect for CBT at short term (RR 0.29, 95% CI 0.12 to 0.68; participants = 65; studies = 1). (Analysis 1.29).
1.29. Analysis.
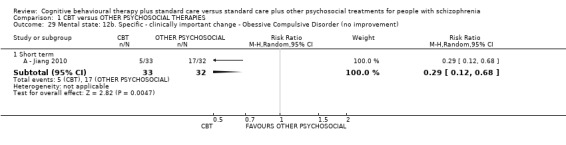
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 29 Mental state: 12b. Specific ‐ clinically important change ‐ Obessive Compulsive Disorder (no improvement).
1.30 Mental state: 12a. Specific ‐ Obessive Compulsive Disorder (average endpoint score Yale‐Brown Obsessive Compulsive Scale (Y‐BOCS), high = poor) ‐ short term
A ‐ Jiang 2010 also presented average endpoint scores for Obsessive Compulsive Disorder using the Y‐BOCS. A positive effect for CBT was observed (MD ‐13.55, 95% CI ‐15.43 to ‐11.67; participants = 65; studies = 1; Analysis 1.30 ).
1.30. Analysis.
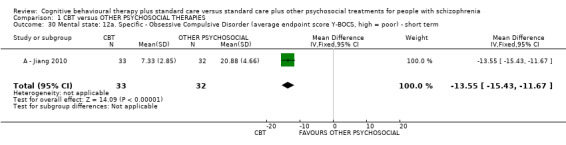
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 30 Mental state: 12a. Specific ‐ Obsessive Compulsive Disorder (average endpoint score Y‐BOCS, high = poor) ‐ short term.
1.31 Mental state: 13. Specific ‐ anger/aggression (Novaco Anger Scale (NAS), high = poor)
A ‐ Haddock 1999 presented endpoint scores for anger/aggression using the NAS. (Analysis 1.31).
1.31. Analysis.
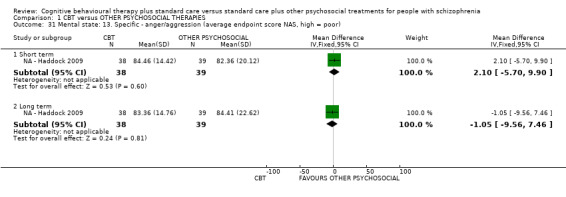
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 31 Mental state: 13. Specific ‐ anger/aggression (average endpoint score NAS, high = poor).
1.31.1 Short term
No clear differences between CBT and an active psychosocial therapy was observed at short term (MD 2.10, 95% CI ‐5.70 to 9.90; participants = 77; studies = 1).
1.31.2 Long term
No clear differences between CBT and an active psychosocial therapy was observed at long term (MD ‐1.05, 95% CI ‐9.56 to 7.46; participants = 77; studies = 1).
1.32 Mental state: 14. Specific ‐ problem behaviours (endpoint scores various scales, high = poor) ‐ skewed data
Skewed data for this outcome were reported from the NPI, the Ward Anger Rating Scale (WARS), and the Historical Clinical Risk Management–20 scale They are presented as 'Other data'. (Analysis 1.32).
1.32. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 32 Mental state: 14. Specific ‐ problem behaviours (average endpoint score various scales, high = poor) ‐ skewed data.
| Mental state: 14. Specific ‐ problem behaviours (average endpoint score various scales, high = poor) ‐ skewed data | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| Novaco Provocation Inventory ‐ short term | |||||
| NA ‐ Haddock 2009 | CBT | 4.03 | 4.19 | 38 | Reported as no difference |
| NA ‐ Haddock 2009 | Other treatment | 6.36 | 6.79 | 39 | |
| Novaco Provocation Inventory ‐ long term | |||||
| NA ‐ Haddock 2009 | CBT | 4.2 | 4.65 | 38 | Reported as no difference |
| NA ‐ Haddock 2009 | Other treatment | 6.3 | 8.0 | 39 | |
| Ward Anger Rating Scale ‐ long term | |||||
| NA ‐ Haddock 2009 | CBT | 4.2 | 4.65 | 38 | Reported as no difference |
| NA ‐ Haddock 2009 | Other treatment | 6.3 | 8.0 | 39 | |
| Ward Anger Rating Scale ‐ short term | |||||
| NA ‐ Haddock 2009 | CBT | 4.03 | 4.19 | 38 | Reported as no difference |
| NA ‐ Haddock 2009 | Other treatment | 6.36 | 6.79 | 39 | |
| HCR‐20 risk management ‐ long term | |||||
| NA ‐ Haddock 2009 | CBT | 4.0 | 3.96 | 38 | Reported as no difference |
| NA ‐ Haddock 2009 | Other treatment | 4.23 | 2.83 | 39 | |
1.33 Mental state: 15. Specific ‐ thought disturbances (average endpoint score PANSS sub scale, high = poor) ‐ skewed data
Skewed data for this outcome are presented as 'Other data' (Analysis 1.33).
1.33. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 33 Mental state: 15. Specific ‐ thought disturbances (average endpoint score PANSS subscale, high = poor).
| Mental state: 15. Specific ‐ thought disturbances (average endpoint score PANSS subscale, high = poor) | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| A ‐ Levine 1998 | CBT | 3.5 | 3.3 | 6 | Reported as no difference |
| A ‐ Levine 1998 | Other treatment | 7.8 | 2.1 | 6 | |
Adverse Effects
Adverse effect reporting was limited with trials providing useable data for only two outcomes.
1.34 Adverse effect/event (s): 1. Number of events
A ‐ Ma 2012 and A ‐ Klingberg 2012 reported incidence of adverse events. Analysis 1.34
1.34. Analysis.
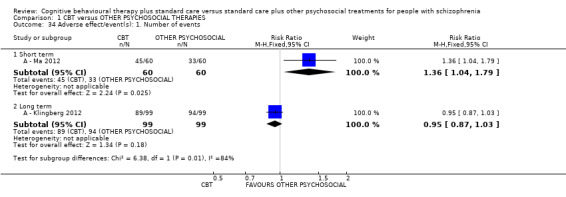
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 34 Adverse effect/event(s): 1. Number of events.
1.34.1 Short term
Participants in the CBT group experienced fewer adverse events in the short term (RR 1.36, 95% CI 1.04 to 1.79; participants = 120; studies = 1).
1.34.2 Long term
There was no clear difference between CBT and active psychosocial therapies in the long term (RR 0.95, 95% CI 0.87 to 1.03; participants = 198; studies = 1).
As short ‐and long‐term outcomes were derived from separate studies it was not possible to separate the effect of trial methodology from true longitudinal differences.
1.35 Adverse effect/event (s): 2. Death ‐ any cause
Six studies reported 14 deaths, with NA ‐ Lewis 2002 and NA ‐ Jackson 2008 specifically reporting suicides. Others reported natural or accidental deaths (A ‐ Durham 2003; A ‐ Klingberg 2012; NA ‐ O'Donnell 2003; A ‐ Tarrier 1999). There were nine deaths in the CBT intervention groups and five deaths in other psychosocial therapies groups, with no clear difference observed between the two treatments (RR 1.57, 95% CI 0.62 to 3.98; participants = 627; studies = 6, low‐quality evidence) (Analysis 1.35).
1.35. Analysis.
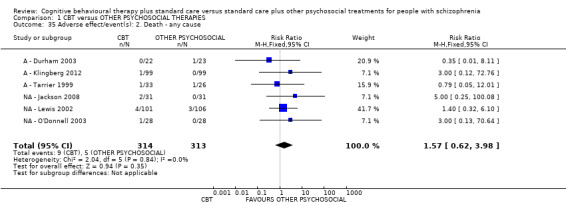
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 35 Adverse effect/event(s): 2. Death ‐ any cause.
Functioning
Studies reported data for social functioning, cognitive functioning and life skills.
1.36 Functioning: 1a. Social functioning (average endpoint scores various scales, high = good)
Two studies reported average endpoint scores from the Social Functioning Scale (SFS) and Social and Occupational Functioning Assessment Scale (SOFAS). (Analysis 1.36).
1.36. Analysis.
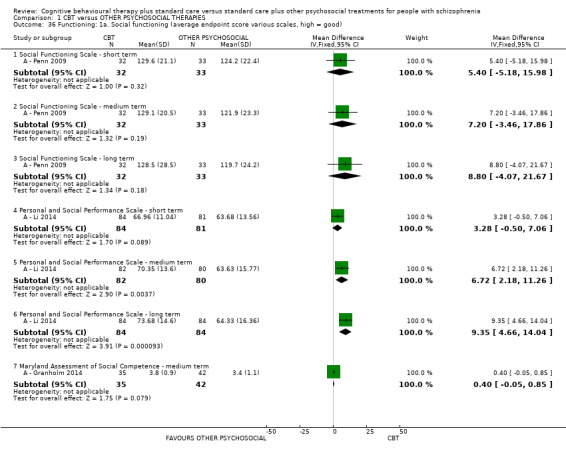
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 36 Functioning: 1a. Social functioning (average endpoint score various scales, high = good).
1.36 1. SFS ‐ short term
A ‐ Penn 2009 reported data from the SFS and observed no clear difference between CBT and an active psychosocial therapy in the short term (MD 5.40, 95% CI ‐5.18 to 15.98; participants = 65; studies = 1).
1.36 2. SFS ‐ medium term
A ‐ Penn 2009 reported data from the SFS and observed no clear difference between CBTand an active psychosocial therapy in the medium term for this outcome (MD 7.20, 95% CI ‐3.46 to 17.86; participants = 65; studies = 1).
1.36 .3 SFS ‐ long term
A ‐ Penn 2009 reported data from the SFS and observed no clear difference between CBT and an active psychosocial therapy in the long term for this outcome (MD 8.80, 95% CI ‐4.07 to 21.67; participants = 65; studies = 1; very low‐quality evidence).
1.36.4 Personal and Social Performance Scale (PSP) ‐ short term
A ‐ Li 2014 reported average endpoint scores from SOFAS. There was no observable difference between CBT and an active psychosocial therapy in the short term (MD 3.28, 95% CI ‐0.50 to 7.06; participants = 165; studies = 1).
1.36.5 PSPS ‐ medium term
A ‐ Li 2014 reported average endpoint scores from SOFAS. A positive effect for CBT was observed in the medium term (MD 6.72, 95% CI 2.18 to 11.26; participants = 162; studies = 1).
1.36.6 ‐ long term
A ‐ Li 2014 reported average endpoint scores from SOFAS. A positive effect for CBT was observed in the long term (MD 9.35, 95% CI 4.66 to 14.04; participants = 168; studies = 1).
1.37 Functioning: 1b. Social functioning (average endpoint score Social and Occupational Functioning Assessment Scale (SOFAS), high = poor)
Three studies reported social functioning data using SOFAS (Analysis 1.37.
1.37. Analysis.
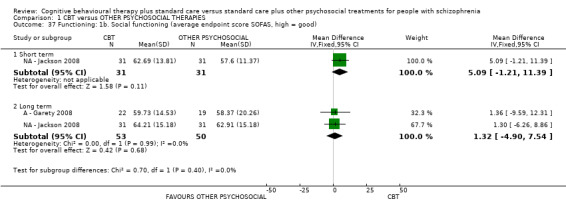
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 37 Functioning: 1b. Social functioning (average endpoint score SOFAS, high = good).
1.37.1 short term
NA ‐ Jackson 2008 observed no clear difference between CBT and a non active psychosocial therapy at short term (MD 5.09, 95% CI ‐1.21 to 11.39; participants = 62; studies = 1) .
1.37.2 long term
A ‐ Garety 2008 and NA ‐ Jackson 2008 also found no observable difference between CBT and other psychosocial therapies for this outcome (MD 1.32, 95% CI ‐4.90 to 7.54; participants = 103; studies = 2).
1.38 Functioning: 2a. Cognitive ‐ insight (average endpoint scores various scales, high = good)
Two trials (A ‐ Li 2014; NA ‐ O'Donnell 2003) reported data from the Schedule for Assessing Insight (SAI) and A ‐ Lecomte 2008 reported data using the Insight Scale (IS) (Analysis 1.38)
1.38. Analysis.
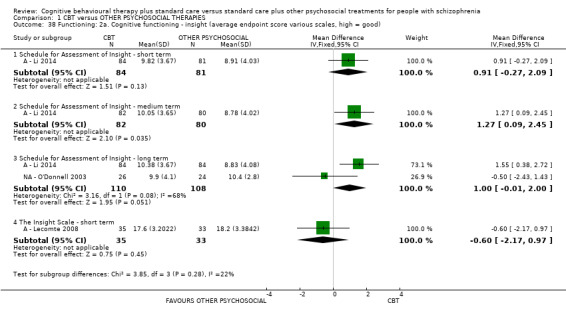
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 38 Functioning: 2a. Cognitive functioning ‐ insight (average endpoint score various scales, high = good).
1.38.1 SAI ‐ short term
No difference between CBT and an active psychosocial therapy was observed in the short term (MD 0.91, 95% CI ‐0.27 to 2.09; participants = 165; studies = 1).
1.38.2 SAI ‐ medium term
A ‐ Li 2014 observed a positive effect for CBT in the medium term (MD 1.27, 95% CI 0.09 to 2.45; participants = 162; studies = 1).
1.38.3 SAI ‐ long term
No difference between CBT and other psychosocial therapies was observed in the long term (MD 1.00, 95% CI ‐0.01 to 2.00; participants = 218; studies = 2).
1.38.4 IS ‐ short term
No difference between CBT and an active psychosocial therapy was observed on the IS scale (MD ‐0.60, 95% CI ‐2.17 to 0.97; participants = 68; studies = 1).
1.39 Functioning: 2b. Cognitive ‐ insight (average endpoint scores Beck Cognitive Insight Scale (BCIS), average endpoint score SAI, high = good) ‐ skewed data
One trial (A ‐ Penn 2009) reported skewed data from the BCIS and another trial (NA ‐ Kemp 1998) reported skewed data from the SAI These data are presented as 'Other data' (Analysis 1.39).
1.39. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 39 Functioning: 2b. Cognitive functioning ‐ insight (average endpoint score BCIS / SAI, high = good) ‐ skewed data.
| Functioning: 2b. Cognitive functioning ‐ insight (average endpoint score BCIS / SAI, high = good) ‐ skewed data | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| Short term | |||||
| A ‐ Penn 2009 | CBT | 6.7 | 6.3 | 32 | Reported as no difference |
| A ‐ Penn 2009 | Other treatment | 6.0 | 5.8 | 33 | |
| NA ‐ Kemp 1998 | CBT | 63 | 23.6 | 39 | Reported as in favour of CBT group |
| NA ‐ Kemp 1998 | Other treatment | 40.6 | 31.2 | 35 | |
| Medium term | |||||
| A ‐ Penn 2009 | CBT | 4.2 | 6.6 | 32 | Reported as no difference |
| A ‐ Penn 2009 | Other treatment | 4.7 | 5.4 | 33 | |
| Long term | |||||
| A ‐ Penn 2009 | CBT | 4.4 | 5.6 | 32 | Reported as no difference |
| A ‐ Penn 2009 | Other treatment | 3.7 | 4.4 | 33 | |
| NA ‐ Kemp 1998 | CBT | 70.7 | 24.4 | 16 | Reported as in favour of CBT group |
| NA ‐ Kemp 1998 | Other treatment | 55.3 | 42.5 | 15 | |
1.40 Functioning 3. Life skills ‐ skills acquisition (average endpoint score Comprehensive Module Test (CMT), high = good) ‐ skewed data
Two trials (A ‐ Granholm 2013; A ‐ Granholm 2014) reported data on skills acquisition using CMT These data are skewed and are presented as 'Other data' (Analysis 1.40).
1.40. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 40 Functioning: 3. Life skills ‐ skills acquisition ‐ (average endpoint score CMT, high = good) ‐ skewed data.
| Functioning: 3. Life skills ‐ skills acquisition ‐ (average endpoint score CMT, high = good) ‐ skewed data | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| Short term | |||||
| A ‐ Granholm 2013 | CBT | 8.6 | 5.6 | 30 | Reported as in favour of CBT group |
| A ‐ Granholm 2013 | Other treatment | 6.2 | 5.1 | 30 | |
| A ‐ Granholm 2014 | CBT | 8.1 | 4.4 | 42 | Reported as in favour of CBT group |
| A ‐ Granholm 2014 | Other treatment | 5.8 | 4.0 | 52 | |
| Medium term | |||||
| A ‐ Granholm 2013 | CBT | 12.0 | 7.1 | 26 | Reported as in favour of CBT group |
| A ‐ Granholm 2013 | Other treatment | 5.5 | 4.1 | 32 | |
| A ‐ Granholm 2014 | CBT | 10.4 | 5.7 | 36 | Reported as in favour of CBT group |
| A ‐ Granholm 2014 | Other treatment | 6.5 | 3.9 | 44 | |
| Long term | |||||
| A ‐ Granholm 2013 | CBT | 11.2 | 7.2 | 24 | Reported as in favour of CBT group |
| A ‐ Granholm 2013 | Other treatment | 5.8 | 3.8 | 28 | |
Quality of life
Three trials measured quality of life (general) using the Life Satisfaction Index (LSI), European Quality of Life Questionnaire (EuroQoL) and the Quality of Life Scale (QoL) scales. (Analysis 1.41).
1.41. Analysis.
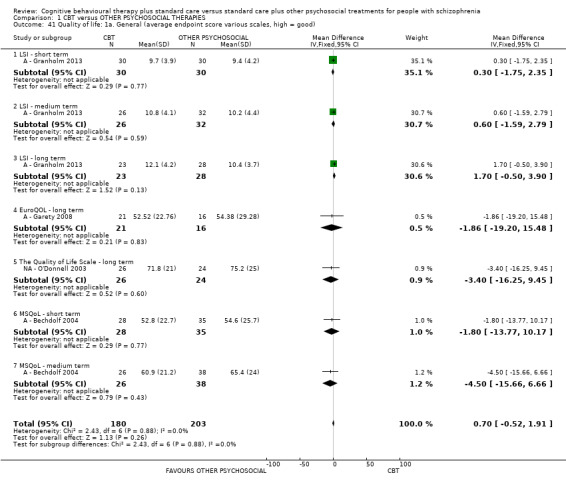
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 41 Quality of life: 1a. General (average endpoint score various scales, high = good).
1.41 Quality of life: 1a. General (average endpoint scores, various scales, high = good)
1.41.1 LSI ‐ short term
A ‐ Granholm 2013 did not observe any difference between CBT and an other active psychosocial therapy for this outcome in the short term (MD 0.30, 95% CI ‐1.75 to 2.35; participants = 60; studies = 1).
1.41.2 LSI ‐ medium term
A ‐ Granholm 2013 did not observe any difference between CBT and an other active psychosocial therapy for this outcome in the medium term (MD 0.60, 95% CI ‐1.59 to 2.79; participants = 58; studies = 1).
1.41.3 LSI ‐ long term
A ‐ Granholm 2013 did not observe any difference between CBT and an other active psychosocial therapy for this outcome in the long term (MD 1.70, 95% CI ‐0.50 to 3.90; participants = 51; studies = 1).
1.41.4 EuroQoL ‐ long term
A ‐ Garety 2008 reported on changes in general quality of life using average endpoint scores from the EuroQOL. There was no clear differences in EuroQOL scores between CBT and an other active psychosocial therapy in the long term (MD ‐1.86, 95% CI ‐19.20 to 15.48; participants = 37; studies = 1).
1.41.5 The QoL scale ‐ long term
NA ‐ O'Donnell 2003 reported on changes in general quality of life using average endpoint scores using the QoL scale. There was no clear difference between CBT and a non active psychosocial therapy for this outcome (MD ‐3.40, 95% CI ‐16.25 to 9.45; participants = 50; studies = 1).
1.41.6 Modular System for Quality of Life (MSQoL) ‐ short term
A ‐ Bechdolf 2004 reported changes in general quality of life using average endpoint scores from the MSQoL scale, no differences were observed at short term (MD ‐1.80, 95% CI ‐13.77 to 10.17; participants = 63; studies = 1).
1.41.7 MSQoL ‐ medium term
A ‐ Bechdolf 2004 reported changes in general quality of life using average endpoint scores from the MSQoL scale, no differences were observed at medium term (MD ‐4.50, 95% CI ‐15.66 to 6.66; participants = 64; studies = 1; very low quality)
1.42 Quality of life: 2a. Specific (average endpoint score MSQoL, high = good) ‐ short term
A ‐ Bechdolf 2004 reported short‐term data for specific aspects of quality of life, using the MSQoL. (Analysis 1.42).
1.42. Analysis.
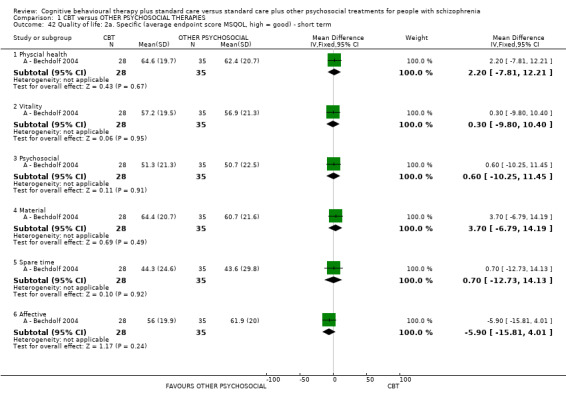
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 42 Quality of life: 2a. Specific (average endpoint score MSQOL, high = good) ‐ short term.
1.42.1 physical health
No clear difference was observed between CBT and an active psychosocial therapy for this outcome (MD 2.20, 95% CI ‐7.81 to 12.21; participants = 63; studies = 1).
1.42.2. vitality
No clear difference was observed between CBT and an active psychosocial therapy for this outcome (MD 0.30, 95% CI ‐9.80 to 10.40; participants = 63; studies = 1).
1.42.3 psychosocial
No clear difference was observed between CBT and an active psychosocial therapy for this outcome (MD 0.60, 95% CI ‐10.25 to 11.45; participants = 63; studies = 1).
1.42.4 material
No clear difference was observed between CBT and an active psychosocial therapy for this outcome (MD 3.70, 95% CI ‐6.79 to 14.19; participants = 63; studies = 1).
1.42.5 spare time
No clear difference was observed between CBT and an active psychosocial therapy for this outcome (MD 0.70, 95% CI ‐12.73 to 14.13; participants = 63; studies = 1).
1.42.6 affective
No clear difference was observed between CBT and an active psychosocial therapy for this outcome (MD ‐5.90, 95% CI ‐15.81 to 4.01; participants = 63; studies = 1).
1.43 Quality of life: 2a. Specific (average endpoint score MSQoL, high = good) ‐ short term
A ‐ Bechdolf 2004 reported medium‐term data for specific aspects of quality of life, again using the MSQoL. (Analysis 1.43).
1.43. Analysis.
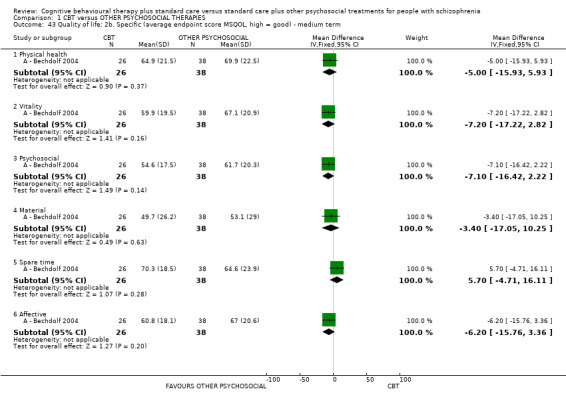
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 43 Quality of life: 2b. Specific (average endpoint score MSQOL, high = good) ‐ medium term.
1.43.1 physical health
No clear difference was observed between CBT and an active psychosocial therapy (MD ‐5.00, 95% CI ‐15.93 to 5.93; participants = 64; studies = 1).
1.43.2. vitality
No clear difference was observed between CBT and an active psychosocial therapy (MD ‐7.20, 95% CI ‐17.22 to 2.82; participants = 64; studies = 1).
1.43.3 psychosocial
No clear difference was observed between CBT and an active psychosocial therapy (MD ‐7.10, 95% CI ‐16.42 to 2.22; participants = 64; studies = 1).
1.43.4 material
No clear difference was observed between CBT and an active psychosocial therapy (MD ‐3.40, 95% CI ‐17.05 to 10.25; participants = 64; studies = 1).
1.43.5 spare time
No clear difference was observed between CBT and an active psychosocial therapy (MD 5.70, 95% CI ‐4.71 to 16.11; participants = 64; studies = 1).
1.43.6 affective
No clear difference was observed between CBT and an active psychosocial therapy (MD ‐6.20, 95% CI ‐15.76 to 3.36; participants = 64; studies = 1).
1.44 Satisfaction with treatment: 1. Leaving the study early
Twenty‐six trials reported data on participants leaving the trial early and a clear difference, favouring CBT was observed (RR 0.86, 95% CI 0.75 to 0.99; participants = 2392; studies = 26; low‐quality evidence; Analysis 1.44 and Figure 6).
1.44. Analysis.
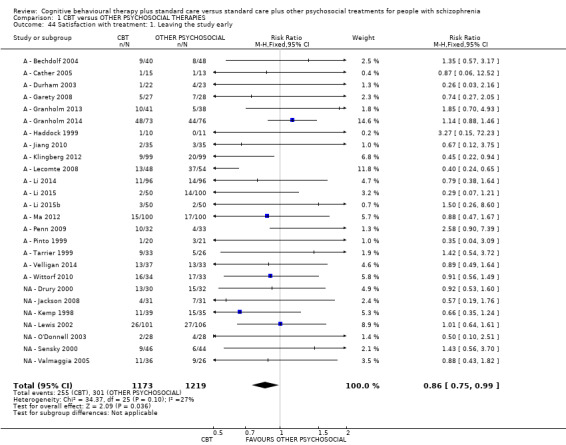
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 44 Satisfaction with treatment: 1. Leaving the study early.
6.
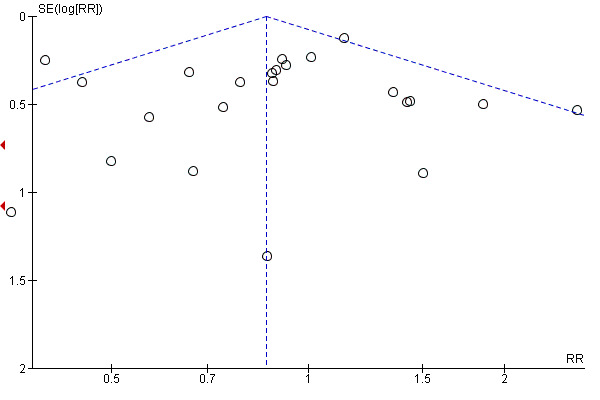
Funnel plot of comparison: 1 CBT versus ALL OTHER PSYCHOLOGICAL THERAPIES, outcome: 1.50 Satisfaction with treatment: 2. Leaving the study early.
1.45 Engagement with services: 1. Compliance (favourable) with medication ‐ long term
Three trials observed no clear effect for CBT compared to other psychosocial therapies (active and inactive) for this outcome (RR 1.01, 95% CI 0.93 to 1.11; participants = 354; studies = 3; Analysis 1.45).
1.45. Analysis.
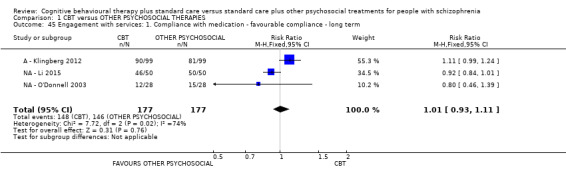
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 45 Engagement with services: 1. Compliance with medication ‐ favourable compliance ‐ long term.
1.46 Engagement with services: 2. Attitude to medication (average endpoint score various scales, high = good)
Attitude to medication was measured by two trials; NA ‐ Kemp 1998 used the Attitue to Medication Questionnaire and NA ‐ O'Donnell 2003 used the DAI. (Analysis 1.46).
1.46. Analysis.
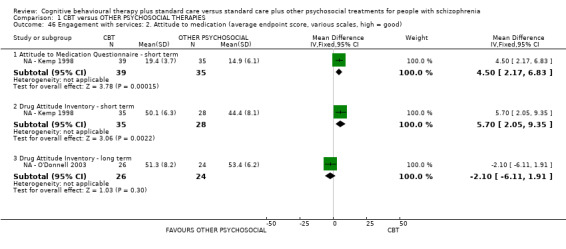
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 46 Engagement with services: 2. Attitude to medication (average endpoint score, various scales, high = good).
1.46.1 Attitude to Medication Questionnaire ‐ short term
One trial compared CBT with a non active psychosocial therapy and a positive effect was observed for CBT (MD 4.50, 95% CI 2.17 to 6.83; participants = 74; studies = 1).
1.46.2 DAI ‐ short term
One trial compared CBT with a non active psychosocial therapy and a positive effect was observed for CBT (MD 5.70, 95% CI 2.05 to 9.35; participants = 63; studies = 1).
1.46.3 DAI ‐ long term
One trial compared CBT with a non active psychosocial therapy and no effect was observed (MD ‐2.10, 95% CI ‐6.11 to 1.91; participants = 50; studies = 1).
2. SUBGROUP 2: Cognitive behavioural therapy (CBT) versus ACTIVE PSYCHOSOCIAL THERAPIES
We performed subgroup analyses for outcomes where both inactive and non active therapies were used as control interventions. We then tested these outcomes for subgroup differences.
2.1 Global state: 1. Relapse
There was no clear difference between CBT and active psychosocial therapies at both medium (RR 0.97, 95% CI 0.54 to 1.78; participants = 88; studies = 1) and long term (RR 1.02, 95% CI 0.58 to 1.78; participants = 120; studies = 3) follow‐up.
2.2 Global state: 2. Rehospitalistaion
There was no clear difference between CBT and active psychosocial therapies at long‐term follow‐up (RR 0.87, 95% CI 0.71 to 1.06; participants = 527; studies = 4).
2.3 Mental state: 1. General ‐ clinically important change (no improvement)
No difference between CBT and active psychosocial therapies was observed at medium (RR 1.02, 95% CI 0.91 to 1.14; participants = 133; studies = 2) or long term (RR 0.96, 95% CI 0.77 to 1.21; participants = 158; studies = 3).
2.4 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor)
There was no clear difference between CBT and active psychosocial therapies at short term (MD ‐0.25, 95% CI ‐1.09 to 0.60; participants = 499; studies = 6), but a positive effect was observed for CBT at medium term (MD ‐1.29, 95% CI ‐2.21 to ‐0.36; participants = 439; studies = 5), and long term (MD ‐2.10, 95% CI ‐3.15 to ‐1.05; participants = 371; studies = 5) follow‐up.
2.5 Mental state: 4a. Specific ‐ hallucinations (average endpoint score Positive Symptoms Rating Scale (PSRS), high = poor)
There was no clear difference between CBT and active psychosocial therapy at long term (MD 0.00, 95% CI ‐4.76 to 4.76; participants = 0; studies = 1).
2.6 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS sub scale, high = poor)
There was no clear difference between CBT and active psychosocial therapy at short (MD ‐0.08, 95% CI ‐1.04 to 0.89; participants = 346; studies = 4) or medium term (MD ‐0.80, 95% CI ‐1.92 to 0.31; participants = 301; studies = 3), but a clear effect favouring CBT at long term .(MD ‐1.34, 95% CI ‐2.57 to ‐0.11; participants = 317; studies = 4).
2.7 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS sub scale, high = poor)
At short term there was a clear difference, favouring CBT, between CBT and active psychosocial therapies (MD ‐4.90, 95% CI ‐6.69 to ‐3.11; participants = 165; studies = 3; I2 = 97%); there was high heterogeneity for this outcome, when the outlier A ‐ Levine 1998 was removed, homogeneity was restored and the result changed to show no effect; medium term (MD ‐1.68, 95% CI ‐4.04 to 0.69; participants = 136; studies = 2); and at long term (MD ‐1.61, 95% CI ‐3.65 to 0.44; participants = 148; studies = 3) results also showed no difference between these treatment groups.
2.8 Adverse effect/event(s) ‐ death
There was no clear difference between CBT and active psychosocial therapies for the outcome of death (RR 0.94, 95% CI 0.19 to 4.56; participants = 302; studies = 3).
2.9 Functioning: 1b. Social functioning (average endpoint score SOFAS, high = good)
There was no clear difference between CBT and active psychosocial therapy at long term (MD 1.36, 95% CI ‐9.59 to 12.31; participants = 41; studies = 1).
2.10 Functioning: 2a. Cognitive functioning ‐ insight (average endpoint score various scales, high = good)
There was a favourable effect for CBT compared to active psychosocial therapy for this outcome at long term ((MD 1.55, 95% CI 0.38 to 2.72; participants = 168; studies = 1).
2.11 Satisfaction with treatment: 1. Leaving the study early ‐ for any reason
There was no clear difference between numbers of participants leaving the study early from the CBT groups compared to numbers leaving early from the active psychosocial therapy groups ((RR 0.85, 95% CI 0.72 to 1.01; participants = 1779; studies = 19).
2.12 Engagement with services: 1. Compliance with medication ‐ favourable compliance ‐ long term
There was no clear difference between CBT and active psychosocial therapy at long term (RR 1.11, 95% CI 0.99 to 1.24; participants = 198; studies = 1).
3. SUBGROUP 3: Cognitive behavioural therapy (CBT) versus NON ACTIVE PSYCHOSOCIAL THERAPIES
3.1 Global state: 1. Relapse
There was no clear difference between CBT and non active psychosocial therapies for relapse at medium (RR 1.44, 95% CI 0.14 to 15.10; participants = 62; studies = 1) or long term (RR 1.05, 95% CI 0.85 to 1.31; participants = 255; studies = 2) follow‐up.
3.2 Global state: 2. Rehospitalistaion
There was no clear difference between CBT and non active psychosocial therapies at long‐term follow‐up (RR 1.14, 95% CI 0.86 to 1.52; participants = 416; studies = 4).
3.3 Mental state: 1. General ‐ clinically important change (no improvement)
There was a clear effect, favouring CBT compared to non active psychosocial therapies at medium (RR 0.53, 95% CI 0.33 to 0.86; participants = 62; studies = 1) and long term (RR 0.60, 95% CI 0.39 to 0.94; participants = 90; studies = 1).
3.4 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor)
There was a clear difference between CBT and non active psychosocial therapies at short term (MD ‐0.93, 95% CI ‐1.84 to ‐0.03; participants = 384; studies = 4), but no effect was observed for CBT at medium term (MD ‐0.80, 95% CI ‐2.82 to 1.22; participants = 58; studies = 1) or long term (MD ‐0.36, 95% CI ‐1.40 to 0.68; participants = 231; studies = 4) follow‐up.
3.5 Mental state: 4a. Specific ‐ hallucinations (average endpoint score PSRS, high = poor)
There was no clear difference between CBT and non active psychosocial therapy at long term (MD ‐4.36, 95% CI ‐9.30 to 0.58; participants = 0; studies = 1).
3.6 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS sub scale, high = poor)
There was no clear difference between CBT and non active psychosocial therapy at short term (MD ‐0.07, 95% CI ‐1.06 to 0.91; participants = 235; studies = 3), medium term (MD 0.04, 95% CI ‐1.52 to 1.60; participants = 58; studies = 1) and long term (MD ‐0.40, 95% CI ‐1.54 to 0.74; participants = 231; studies = 4).
3.7 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS sub scale, high = poor)
At short term there was a clear difference, favouring CBT, between CBT and non active psychosocial therapies (MD ‐1.95, 95% CI ‐3.68 to ‐0.22; participants = 235; studies = 3). There was no effect observed at medium term (MD 0.12, 95% CI ‐2.71 to 2.95; participants = 58; studies = 1), and long term (MD ‐0.44, 95% CI ‐2.21 to 1.34; participants = 231; studies = 4) follow‐up.
3.8 Adverse effect/event(s) ‐ death
There was no clear difference between CBT and non active psychosocial therapies for the outcome of death (RR 2.06, 95% CI 0.63 to 6.75; participants = 325; studies = 3).
3.9 Functioning: 1b. Social functioning (average endpoint score SOFAS, high = good)
There was no clear difference between CBT and non active psychosocial therapy at long term (MD 1.30, 95% CI ‐6.26 to 8.86; participants = 62; studies = 1).
3.10 Functioning: 2a. Cognitive functioning ‐ insight (average endpoint score various scales, high = good)
There no effect observed between CBT and non active psychosocial therapy for this outcome at long term (MD ‐0.50, 95% CI ‐2.43 to 1.43; participants = 50; studies = 1).
3.11 Satisfaction with treatment: 1. Leaving the study early ‐ for any reason
There was no clear difference between numbers of participants leaving the study early from the CBT groups compared to numbers leaving early from the non active psychosocial therapy groups (RR 0.88, 95% CI 0.68 to 1.15; participants = 613; studies = 7)
3.12 Engagement with services: 1. Compliance with medication ‐ favourable compliance ‐ long term
There was no clear difference between CBT and non active psychosocial therapy at long term (RR 0.89, 95% CI 0.78 to 1.03; participants = 156; studies = 2).
4. SUBGROUP DIFFERENCE TESTS
We tested for subgroup differences between active and non active psychosocial therapies. Overall, there was no evidence that CBT had different effects when compared with active or non active therapies.The only outcomes where there was some evidence are presented below.
4.4 ‐ 4.5 Mental state: General ‐ clinically important change
At medium term there was no evidence of a difference between CBT and an active therapy, but there was a favourable effect for CBT when compared with non active therapies (Analysis 4.4); this difference in effect was significant: Test for subgroup differences: Chi² = 6.60, df = 1 (P = 0.01), I² = 84.8% This effect remained at long term (Analysis 4.5): Test for subgroup differences: Chi² = 3.39, df = 1 (P = 0.07), I² = 70.5%.
4.4. Analysis.
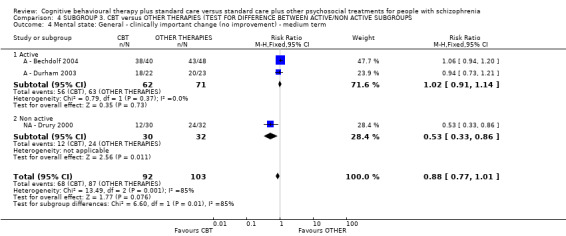
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 4 Mental state: General ‐ clinically important change (no improvement) ‐ medium term.
4.5. Analysis.
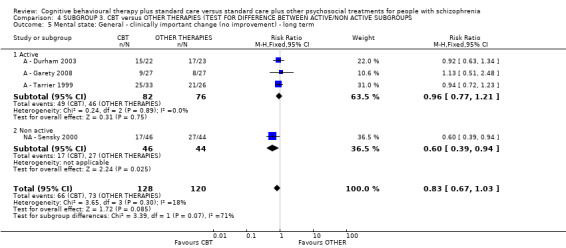
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 5 Mental state: General ‐ clinically important change (no improvement) ‐ long term.
4.8 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS sub scale, high = poor)
Long‐term results from the PANSS sub scale for positive symptoms showed a favourable effect CBT when compared with active therapies but no difference when compared with non active therapies (Analysis 4.8), this difference in effect was significant: Test for subgroup differences: Chi² = 5.36, df = 1 (P = 0.02), I² = 81.4%.
4.8. Analysis.
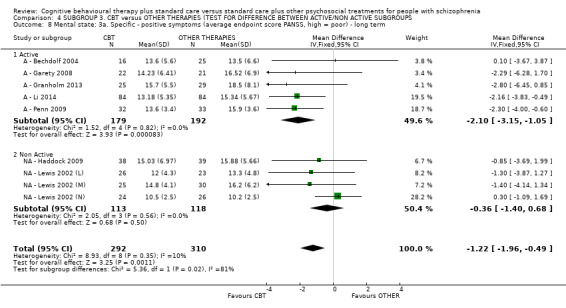
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 8 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor) ‐ long term.
4.13 Mental state: 6a. Specific ‐ affective symptoms (average endpoint score PANSS sub scale, high = poor) ‐ long term
Short‐term data showed a difference between subgroups Test for subgroup differences: Chi² = 5.39, df = 1 (P = 0.02), I² = 81.5%, but the data for active comparison were highly skewed, when the outlier is removed, there are no subgroup differences for this outcome. Test for subgroup differences: Chi² = 1.97, df = 1 (P = 0.16), I² = 49.2%. (Analysis 4.13).
4.13. Analysis.
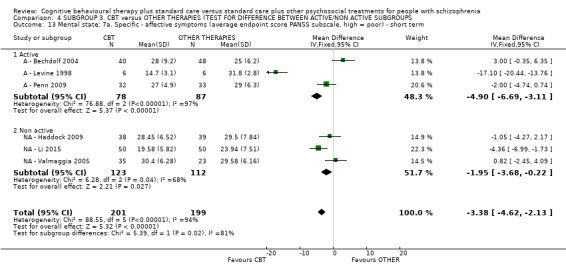
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 13 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor) ‐ short term.
Sensitivity analysis
1. Implication of randomisation
As we did not include any study that implied randomisation, we were unable to carry out a sensitivity analyses.
2. Blinding
As no study clearly stated that the outcome assessor was non‐blinded, we did not perform sensitivity analysis for this domain.
3. Well‐defined CBT versus less‐well‐defined CBT
No clear difference in results were found when trials with less‐well‐defined CBT were excluded from the meta‐analyses of the primary outcomes (Analysis 5.1; Analysis 5.2; Analysis 5.3; Analysis 5.4).
5.1. Analysis.
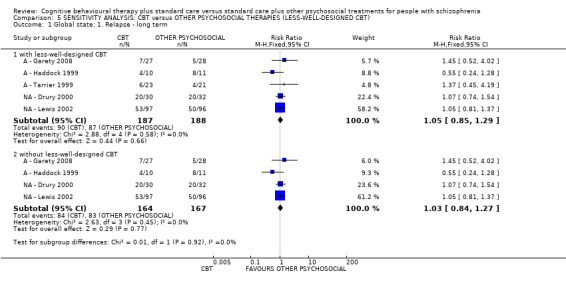
Comparison 5 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (LESS‐WELL‐DESIGNED CBT), Outcome 1 Global state: 1. Relapse ‐ long term.
5.2. Analysis.
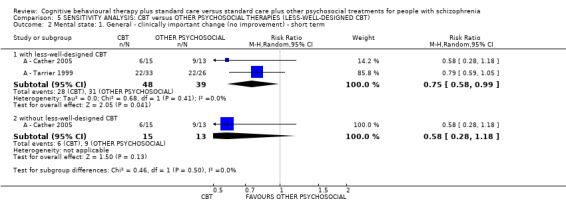
Comparison 5 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (LESS‐WELL‐DESIGNED CBT), Outcome 2 Mental state: 1. General ‐ clinically important change (no improvement) ‐ short term.
5.3. Analysis.
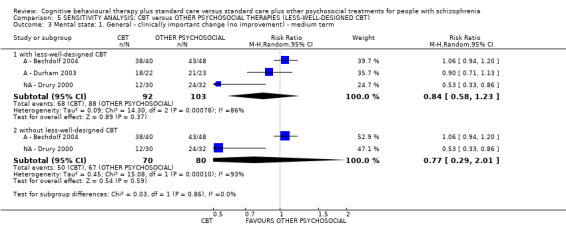
Comparison 5 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (LESS‐WELL‐DESIGNED CBT), Outcome 3 Mental state: 1. General ‐ clinically important change (no improvement) ‐ medium term.
5.4. Analysis.
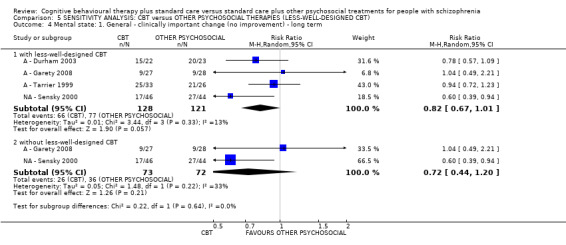
Comparison 5 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (LESS‐WELL‐DESIGNED CBT), Outcome 4 Mental state: 1. General ‐ clinically important change (no improvement) ‐ long term.
4. Therapist experience
No clear difference in results were found when trials with 'less experienced' therapists were excluded from the meta‐analyses of the primary outcome(Analysis 6.1; Analysis 6.2).
6.1. Analysis.
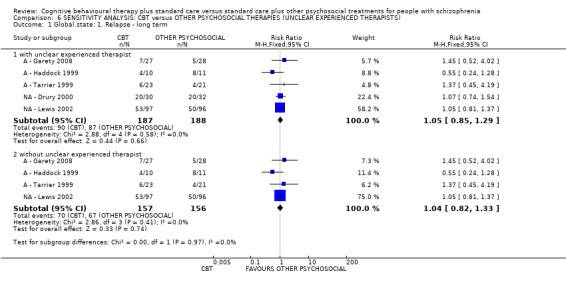
Comparison 6 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (UNCLEAR EXPERIENCED THERAPISTS), Outcome 1 Global state: 1. Relapse ‐ long term.
6.2. Analysis.
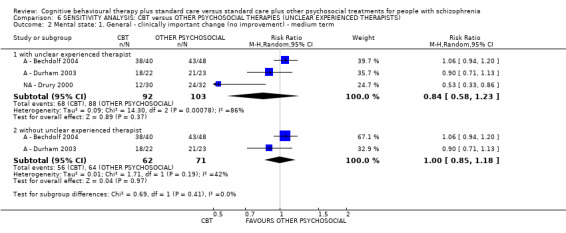
Comparison 6 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (UNCLEAR EXPERIENCED THERAPISTS), Outcome 2 Mental state: 1. General ‐ clinically important change (no improvement) ‐ medium term.
5. Assumptions for lost binary data
We made assumptions for lost binary data (see Dealing with missing data). Sensitivity analysis showed that there was no substantial difference between results using our assumption and results from completers only (Analysis 7.1; Analysis 7.2; Analysis 7.3; Analysis 7.4).
7.1. Analysis.
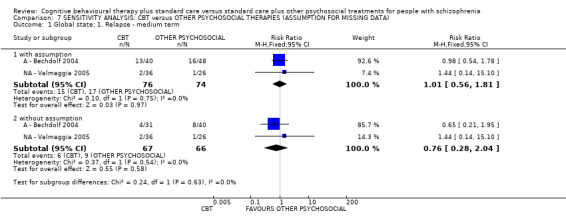
Comparison 7 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (ASSUMPTION FOR MISSING DATA), Outcome 1 Global state: 1. Relapse ‐ medium term.
7.2. Analysis.
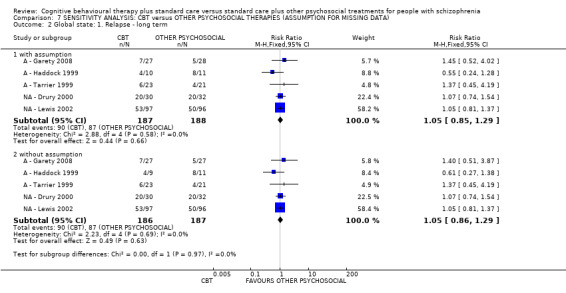
Comparison 7 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (ASSUMPTION FOR MISSING DATA), Outcome 2 Global state: 1. Relapse ‐ long term.
7.3. Analysis.
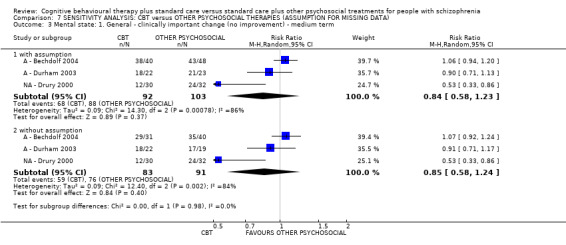
Comparison 7 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (ASSUMPTION FOR MISSING DATA), Outcome 3 Mental state: 1. General ‐ clinically important change (no improvement) ‐ medium term.
7.4. Analysis.
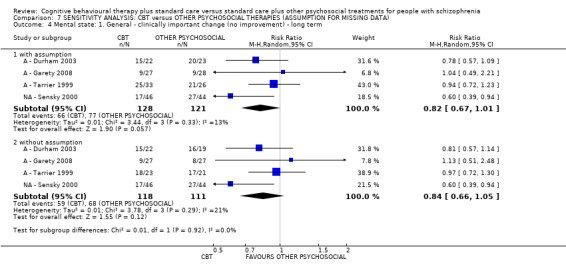
Comparison 7 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (ASSUMPTION FOR MISSING DATA), Outcome 4 Mental state: 1. General ‐ clinically important change (no improvement) ‐ long term.
6. Risk of bias
No substantive difference in results were found when trials with a high risk of bias were excluded from meta‐analyses of the primary outcomes (Analysis 8.1; Analysis 8.2; Analysis 8.3; Analysis 8.4; Analysis 8.5).
8.1. Analysis.
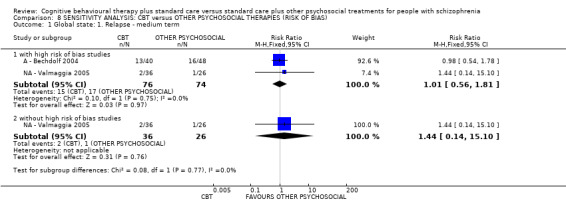
Comparison 8 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (RISK OF BIAS), Outcome 1 Global state: 1. Relapse ‐ medium term.
8.2. Analysis.
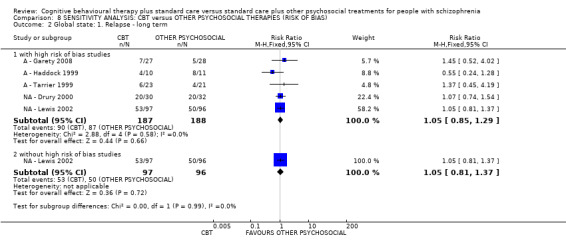
Comparison 8 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (RISK OF BIAS), Outcome 2 Global state: 1. Relapse ‐ long term.
8.3. Analysis.

Comparison 8 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (RISK OF BIAS), Outcome 3 Mental state: 1. General ‐ clinically important change (no improvement) ‐ short term.
8.4. Analysis.
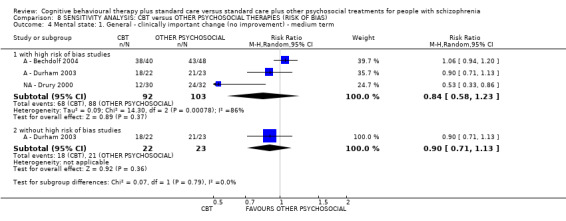
Comparison 8 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (RISK OF BIAS), Outcome 4 Mental state: 1. General ‐ clinically important change (no improvement) ‐ medium term.
8.5. Analysis.
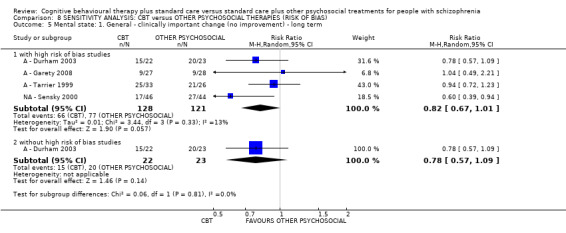
Comparison 8 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (RISK OF BIAS), Outcome 5 Mental state: 1. General ‐ clinically important change (no improvement) ‐ long term.
7. Imputed values
We did not carry out a sensitivity analysis for imputed values as no cluster‐randomised trials are included in the review.
8. Fixed‐ and random‐effects
No substantive difference in results were found when we combined data using a random‐effects model for the primary outcome Analysis 9.1.
9.1. Analysis.
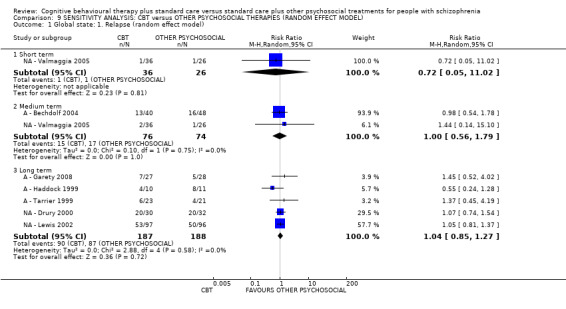
Comparison 9 SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (RANDOM EFFECT MODEL), Outcome 1 Global state: 1. Relapse (random effect model).
Discussion
Summary of main results
1. Comparison 1. Cognitive behavioural therapy (CBT) versus other psychosocial therapies
The conclusions of this review should be read in conjunction with another Cochrane Review of the efficacy of cognitive behavioural therapy relative to standard care. It should be noted that the outcomes reported for this review compare CBT with other psychosocial therapies that were designed to achieve meaningful symptom reduction. Accordingly, these outcomes are not measures of overall efficacy of CBT for people with schizophrenia, but rather should be interpreted as measures of the relative advantage of CBT specifically compared with other psychosocial interventions.
1.1 Global state
No advantage was found for CBT over other psychological therapies with respect to rate of relapse or rehospitalisation. No differential effect of CBT was observed on global state when measured using the Global Assessment Scale (GAS). In contrast, there was a consistent positive effect for CBT when global state was measured using the Globals Assessment of Functioning (GAF); this effect was based on data from two studies and only observed in the short term and may be a chance finding.
When CBT was compared specifically active psychosocial therapies, the lack of effect on rate of relapse or rehospitalisation remained, and results were also unchanged when CBT was compared specifically with non active therapies.
1.2 Mental state
We found a positive effect for CBT over other psychosocial therapies with respect to important change in general mental state in the short term (based on two studies with a total 87 participants) but no difference was observed in the medium term (based on three studies with a total of 195 participants) or long term (based on four studies with a total of 249 participants).
For general mental state measured in terms of endpoints scores on the Brief Psychiatric Rating Scale (BPRS), no effect was found in the short or long term. A small advantage for CBT was found in the medium term, but this was observed in only a single small trial (A ‐ Pinto 1999), which compared CBT with an active therapy (supportive counselling).
When general mental state was measured using endpoints scores on the Positive and Negative Syndrome Scale (PANSS), a positive effect for CBT in the short, medium and long term was found. This relatively modest advantage of CBT is a reduction in the PANSS total score by an average of five points in the short term reducing to an average of approximately three points in the long term. There were important levels of heterogeneity for this result but the positive effect for CBT was maintained when the outlier, A ‐ Levine 1998, was removed and heterogeneity was reduced to 11%.
Much of the CBT‐based interventions for psychosis focus on specific symptoms. With respect to positive symptoms on the PANSS, no clear difference between CBTand other psychosocial therapies was observed in the short term. However, there was a small but reliable effect in favour of CBT of approximately one point reduction in PANSS positive symptom score in the medium term and long term,
When more specific measures of mental state such hallucinations were measured no advantage was found for CBT at any duration of treatment outcome. With respect to delusions as measured by the sub‐scale of the PANSS across nine trials, there was also no clear difference between CBT and other therapies in the short, medium‐or long term. Five trials reported outcomes for delusions, four trials reported skewed data with only one trial reported short‐term positive effects for CBT (NA ‐ Haddock 2009). No other studies reported significant effects, although the failure to demonstrate an effect may also reflect the lack of trials reporting this outcome and the preponderance of skewed data. Therefore accordingly there is no systematic evidence of a treatment effect on these outcome measures.
No consistent effect was found for the differential impact of CBT on negative symptoms at any treatment duration.
With respect to affective symptoms, no positive effect for CBT was observed on the General Psychopathology scale of the PANSS. Symptoms of depression were measured on the Montgomery Asberg Depression Rating Scale (MADRS), Beck Depression Inventory (BDI) and the Hamilton Depression Scale (HAMD). The data for outcomes on the MADRS and BDI were skewed, however a medium‐term advantage for CBT was observed on the MADRS and a short‐term advantage was observed on the HADS. Accordingly, there is inconsistent evidence of a treatment effect for depressive symptoms.
Anxiety was measured using the Beck Anxiety scale (BAI), the Hamilton Anxiety scale (HAMA)and the Self Rating Anxiety Scale (SARS) . There was an advantage for CBT in the short term on the HAMA and the SARS but not the BAI. Accordingly, there is inconsistent evidence of a treatment effect for anxiety symptoms.
On the basis of data from one trial (NA ‐ Haddock 2009), no advantage was observed on the Novaco Anger scale (NAS) in the short or long term and no difference was observed on the Novaco Provocation Inventory (NPI) in the short or long term.
One study (A ‐ Li 2015b) reported short‐term improvement for CBT on the Stigma Scale for Mental Illness (SSMI). However, when self‐esteem was measured using the Rosenberg Self‐Esteem scale (RSES), no advantage for CBT was observed in the short, medium or long term.
With respect to problem behaviours, no advantage was observed for CBT on the Ward Anger Rating Scale (WARS) or the risk management sub scale of the HCR20.
These findings provide only weak and inconsistent support for the assertion by Birchwood 2006 that CBT when correctly applied should effect change in emotional distress and/or problematic behaviours rather than psychotic symptomatology. However, it should be noted that the trials reporting outcomes in this category have not specifically included interventions that have targeted the affective response to psychotic symptomatology and have generally not measured specific belief‐related distress (or has been measured on scales with psychometric propetries that were not compatible with meta‐analytic synthesis). Similarly, it should be noted that these data compare CBT with other psychological therapies, it is possible that the interventions in the control arm may also exert an effect on symptom‐related distress and thus obscure any treatment effect related to CBT per se.
1.3 Adverse effect/events
CBT did not show an advantage with respect to avoidance of death by natural causes or suicide, although it should be noted that the overall numbers were small with only six studies reporting deaths.
Only two trials reported adverse effect data. One of these trials (A ‐ Ma 2012) found participants in the CBT group experienced less adverse effects in the short term in comparison with supportive therapy, whereas the other study (Klingberg 2009) reported no difference in adverse outcomes between CBT and Cognitive Remediation Training in the long term.
Many of the included studies do not report adverse effects of this therapy. If such treatment is potentially to be recommended for wide adoption, routine recording and reporting of adverse effects should be expected within evaluative studies.
1.4 Functioning
No advantage for CBT was observed on the Social Functioning Scale (SFS) or the Social and Occupational Functioning Assessment Scale (SOFAS). On the Personal and Social Performance Scale (PSP), a positive effect for CBT was observed in the medium term and long term.
On the Schedule for Assessing Insight (SAI), no difference was observed in the short term or long term and no advantage for CBT was reported from skewed data for the Beck Cognitive Insight Scale (BCIS). However, a positive effect for CBT was observed in the medium term from one trial on the SAI. Overall, there is no consistent evidence of an advantage for CBT with regard to promoting insight.
No clear difference was observed on the SFS when CBT was compared with an active psychosocial therapy (enhanced supportive therapy (A ‐ Penn 2009) at any duration of outcome. Similarly, when CBT was compared with a non active psychosocial therapy (befriending), no advantage was observed using the SOFAS by A ‐ Garety 2008 and NA ‐ Jackson 2008 in the short or long term.
This important outcome is not often measured but there is no indication that the addition of CBT to standard care has any convincing generalised effect.
1.5 Quality of life
There is no evidence of an advantage for CBT on general or specific measures of Quality of Life.
1.6 Satisfaction with treatment
One trial (NA ‐ Kemp 1998) reported an advantage for CBT in the short term on the Attitude to Medication Questionnaire (AMQ)and the Drug Attitude Inventory (DAI), although no effect in the long term was reported by NA ‐ O'Donnell 2003.
Twenty‐six studies contributed data to leaving the study early. CBT had a moderate effect for keeping people in the study more than other psychosocial therapies. Whether this is directly due to 'satisfaction with care' is unclear.
1.7 Engagement with service
No advantage for CBT was observed in three trials reporting compliance with medication.
2. SUBGROUP DIFFERENCES: ACTIVE or NON ACTIVE PSYCHOSOCIAL THERAPIES
When we tested for subgroup differences between active and non active psychosocial therapies, in general there was no evidence that CBT had different effects when compared with active or non active therapies, except in the following analyses. At medium term there was no evidence of a difference between CBT and an active therapy, but there was a favourable effect for CBT when compared with non active therapies (Analysis 4.4), this difference in effect between subgroups was significant (Chi² = 6.60, df = 1 (P = 0.01), I² = 84.8%). In addition, long‐term results from the PANSS sub‐scale showed a favourable effect of CBT when compared with active therapies but no difference when compared with non active therapies (Analysis 4.8), this difference in effect for the subgroups was significant: Chi² = 5.36, df = 1 (P = 0.02), I² = 81.4%.
Overall completeness and applicability of evidence
1. Completeness
There has been an improvement in the reporting of the main outcomes (relapse, hospitalisation, mental state, adverse event) since the last update of this review. At the time of the last update, even the most replete of the outcomes contained less than 300 participants, and this has improved since this update. For rehospitalisation, the current review reports outcomes from eight trials involving 943 participants.
Nevertheless, the trials were often small and often undertaken by pioneers of CBT. There is a poverty of measurement of certain outcomes and none on others. For example, there are two trials reporting any adverse event and six trials reporting deaths.
2. Applicability
2.1 Participants
The included studies involved people with schizophrenia or psychosis as derived from recognised diagnostic criteria from a wide range of settings, including both in‐patients and out‐patients. The results of this review could thus be said to be valid for people with a diagnosis of a psychotic disorder whose illness has taken a chronic course whether treated on an in‐patient or out‐patient basis.
The exclusion criteria were such that this review is of less relevance to people with other psychotic disorders such as bipolar disorder, substance‐induced psychosis, significant physical or sensory difficulties or people with acquired brain injury or co‐existing developmental learning disabilities. It should be noted that people who were described as in the category of "at risk" of psychosis but not yet diagnosed were not included in this review.
2.2 Interventions
Eleven trials meet our criteria for ‘well‐defined CBT’. The period of active therapy varied between studies. For example, A ‐ Bechdolf 2004 provided up to eight weeks of individual CBT, whilst NA ‐ Drury 2000 gave both individual and group cognitive therapy over the course of recovery (which did not exceed nine months) as well as family engagement, aimed at developing familial coping strategies and a structured activity programme (for an average of five hours per week) including cooking, creative therapy and discussion groups. On the other hand, NA ‐ Kemp 1998 reported that their intervention consisted of four to six sessions of therapy aimed at increasing medication compliance.
The CBT interventions varied in both the target of the therapy and the degree of specificity of the focus of the intervention. For example,NA ‐ Kemp 1998 and NA ‐ O'Donnell 2003 used a CBT intervention focused specifically on medication compliance, whereas the CBT intervention described by A ‐ Bechdolf 2004 had a wider focus and targeted auditory hallucinations and delusions, anxiety, depression, relapse prevention and enhancing medication compliance. Most trials targeted positive symptoms of psychosis, some with an explicit focus on auditory hallucinations A ‐ Bechdolf 2004; A ‐ Haddock 1999; NA ‐ Jackson 2008; A ‐ Penn 2009; NA ‐ Valmaggia 2005) and/or delusions A ‐ Garety 2008; A ‐ Haddock 1999; NA ‐ Jackson 2008; NA ‐ Valmaggia 2005). It was less common for the CBT intervention to target negative symptoms of psychosis (Klingberg 2009). Strategies for relapse prevention were a common component in the CBT intervention and a specific focus in some trials (e.g. A ‐ Garety 2008). Emotional distress A ‐ Bechdolf 2004; NA ‐ Sensky 2000) and self‐esteem (A ‐ Bechdolf 2004; A ‐ Penn 2009), either in general or specifically related to the experience of psychosis, was a target in some trials that also targeted other symptoms. Finally, A ‐ Haddock 1999 focused specifically on psychotic symptoms and anger relating to aggression and violence.
The present review has adopted a tiered definition of CBT. Cognitive behavioural therapy in clinical practice typically includes a number of components: cognitive restructuring, hypothesis testing, behavioural experiments, psychoeducation, relapse prevention, coping strategy enhancement, problem‐solving strategies, with or without, relaxation training. In this respect, many of the current trials reflect common clinical practice. However, this multi‐component approach is not necessarily helpful in identifying the active components of CBT because the control arms of the trials are often not balanced in terms of component therapies. Trials generally include a range of interventions in the same treatment arm and in many the intervention is described as “CBT” without a clear indication that the active element of therapy involves explicit manipulation of beliefs. In addition, cognitive therapy for psychosis, as reflected in current trials, has become increasingly distanced from its basis in CBT for non‐psychotic mood disorders where the focus is on the emotional and behavioural consequences of dysfunctional thinking patterns and the intervention is clearly designed to address cognitions and beliefs. This point has been identified by Birchwood 2006 who has noted that CBT for psychosis has often been treated as if it were a 'quasi‐neuroleptic' where the focus of outcome measurement has been on global symptoms with the expectation that CBT should reduce psychotic symptoms directly as opposed to eliciting emotional and behavioural changes. More recent trials of CBT in relation to standard care are more clearly based on theoretical models of psychotic symptoms (e.g. Trower 2004). Such trials have a clear focus on the specificity of the beliefs addressed (e.g. power beliefs about voices) and outcome measures which are sensitive to belief change as the mediator of emotional and behavioural change.
Overall, interventions did vary considerably but the findings were consistent. When well‐implemented CBT is given, for long or short periods, with various foci of treatment, there is no convincing difference between CBT and other psychosocial interventions in relation to psychotic symptomatology and broad measures of functioning (Table 1). However, there are some promising preliminary findings with respect to the effect of CBT on symptoms of depression. At present, it remains unclear, but it is interesting to speculate as to the relative benefits for CBT for psychosis compared with CBT which is specifically focused upon depression in this group of patients.
Quality of the evidence
This is an attempt to quantitatively summarise the effects of cognitive behavioural therapy for schizophrenia. This has not been an easy task and the review authors will be pleased to hear from readers in order to improve this work for future issues of the Cochrane Library. The methodological quality of the included studies is summarised in Figure 5. There still are too few trials. Studies are too small. Outcomes are often reported in such a way that leaves presentation in a systematic review, difficult or impossible. In addition, rating scales are often used to measure outcomes that are not directly relevant to psychological therapy: i.e. they do not measure belief‐mediated distress or behaviour.
There has, however, been a general improvement in methodological rigor of the more recent trials. Several trials had relatively large sample sizes (A ‐ Buchkremer 1997; A ‐ Garety 2008; Klingberg 2009; NA ‐ Lewis 2002, all exceeded 100 participants). All 33 included studies which report some form of randomisation, with 21 describing adequate sequence generation. Allocation was concealed in 18 studies and 25 of the 36 trials employed raters blinded to the treatment condition.
One of the key issues, which is a limiting factor in interpreting current trial data, is the wide variation in the targets of treatment and there is little agreement on how these targets and key outcomes should be operationalised. Studies frequently measure different outcomes or measure the same outcome using different measures. The differences in the psychometric properties of these measures make it difficult to interpret the variability of the outcomes reported in the trials. It would be invaluable to future trials to receive direction regarding a common consensus on the most reliable, valid and clinically‐relevant outcome measures for CBT for psychosis. In the view of the authors this is likely to require the design and validation of new outcome measures both for specific aspects of positive symptoms (e.g. beliefs, preoccupation and conviction), as well as key emotional and behavioural outcomes including anxiety, depression and more specific symptom‐related distress. For example, current state‐of‐the‐art measures of these dimensions are not fully adequate to assess the efficacy of CBT. The Psychotic Symptom Rating Scale(PSYRATS), for example, includes only a single four‐point measure of delusional or voice‐related distress and the Beliefs About Voices Questionnaire includes measures of emotional response to voices which are not clearly delineated from other variables, such as the person's behaviour in relation to the voice. In addition, the ultimate aim of clinical intervention is to improve functioning and trials should include primary outcomes relating to this including, return to work, social functioning and quality of life. It would seem important to also report on some economic outcomes.
Finally, a welcome addition to some of the newer trials is the introduction of protocols to assess adherence to CBT methods, though there remains a lack of consensus across trials as to how this is implemented. In addition, a recent government focus in the UK on making psychological therapies more widely available is likely to mean that a broader range of expertise is employed in the delivery of CBT for psychosis. At present, the experience of therapists in trials is not always clearly described and this renders it difficult to undertake a sensitivity analysis of the effect of therapist expertise.
Potential biases in the review process
One of the review authors (AM) is actively engaged in the evaluation of the efficacy of CBT for psychosis.
Agreements and disagreements with other studies or reviews
There are few reviews of CBT that have made comparisons with other psychological therapies. However, in a meta‐analysis of eight trials with 528 patients, Pilling 2002 reported that CBT did not show an advantage over other active therapies (i.e. supportive counselling, and a problem‐solving group) although positive effects of CBT were reported relative to standard care.
Authors' conclusions
Implications for practice.
1. For people with schizophrenia
The use of cognitive behavioural therapy (CBT) has been associated with some reduction in symptoms of psychosis, particularly the positive symptoms of schizophrenia. However, there is considerable variability in the findings of the various studies and effect sizes tend to be quite modest. Therefore, at present, it is not possible to assert any substantial benefit for CBT in contrast to other psychological therapies.
2. For clinicians
Currently, CBT for people with schizophrenia is a scarce commodity, often provided by highly‐skilled and experienced therapists. These data are not convincing of clear benefit over other ‐ and sometimes less sophisticated ‐ therapies for people with schizophrenia. There is some indication that CBT may help the positive symptoms of schizophrenia and there is mixed and inconsistent evidence for the benefit of CBT for psychosis on secondary anxiety and depression.
3. For policy makers
Cognitive behavioural therapy may provide a useful add‐on to traditional treatment of people with schizophrenia. The nature of the randomised controlled trials of CBT included in this review and their small sample sizes demands caution until such time as data from larger, more methodologically coherent randomised controlled trials are available to supplement these findings.
Implications for research.
1.General
1.1 Study design
More, large, generally applicable, clinically‐meaningful trials are needed. More comparisons of CBT with supportive approaches would seem of particular interest. Further research should address the issue of the use of CBT in specific settings and contexts (e.g. tertiary psychiatric services, long‐stay institutions, and day hospitals). If all of the trials within this review had conformed to the suggestions within the CONSORT statement on trials reporting (Begg 1996; Moher 2001), much more may be known on the effect of CBT for people with schizophrenia.
1.2 Randomisation
Allocation concealment is a fundamental part of trial methodology. If readers are to be reassured that selection bias was minimised then the randomisation process should be clearly described.
1.3 Blinding
Double‐blind evaluation of the outcomes of a psychosocial intervention is extremely difficult, and probably impossible. Trialists should, however, take every precaution to minimise the effect of biases by using blinded or independent raters (quoting inter‐rater reliability and measuring their blindness) and, probably more importantly, using 'harder' outcomes such as relapse, self‐harm, and relapse or admission rather than scale data.
1.4 Withdrawals
Intention‐to‐treat analysis is preferable. If possible, all trials should describe from which groups withdrawals came, why they occurred and what was their outcome.
2. Specific to cognitive behavioural therapy trials
For a suggested design of future study (see Table 4), modified from that included in the full version of the Cochrane psychoeducation review (Zhao 2015).
3. Suggested design of study.
| Methods | Allocation: randomised, fully explicit description of methods of randomisation and allocation concealment. Blinding: single, tested. Setting: community rather than hospital. Duration: 12 weeks treatment, and then follow‐up to at least 52 weeks. |
| Participants | Diagnosis: schizophrenia (ICD). N = 300.* Age: adults. Sex: both. |
| Interventions | 1. Cognitive behaviour therapy + standard care. N = 150. Content:
Delivered by: experienced therapists. 2. Other psychosocial therapy + standard care . N = 150. |
| Outcomes | General: time to all‐cause treatment failure marked by its discontinuation, relapse/rehospitalisation, general impression of clinician (CGI), career/other, compliance with treatment. Mental state: BPRS and PANSS. Global state: CGI (Clinical Global Impression). Quality of life. QOL (Quality of Life Questionnaire). Social functioning: return to everyday living for 80% of time.* Economic outcomes. |
| Notes | * Powered to be able to identify a difference of ˜ 20% between groups for primary outcome with adequate degree of certainty. |
BPRS: Brief Psychiatric Rating Scale; ICD: International Classification of Diseases; PANSS: Positive and Negative Syndrome Scale
2.1 The issue of practitioners
Cognitive behavioural therapy holds the promise of providing a valuable adjunct to traditional treatments for people with psychotic disturbances. Despite the fact that it may be an effective therapy, it is currently inaccessible to large numbers of those with schizophrenia, even within well‐resourced care services. This situation will remain until either the basic skills of cCBTcan be generalised to other healthcare professionals; or there can be increased availability of specialists specifically practising CBT for those with schizophrenia.
2.2 Power
Estimates of statistical power based on data obtained from this review indicate that using data from within this review for the outcome of 'no important improvement' about 70 people per group are required to show a statistically clear difference in the outcome over a period of at least six months (alpha 0.05, beta 0.8). This computation assumes that the difference in proportions is ‐0.29 (specifically, 0.58 versus 0.87). Given an attrition rate of approximately 30%, researchers should aim for a minimal sample size of 100 persons per intervention.
2.3 Outcomes measured
Outcomes should be clear and clinically useful, but if authors are to persist in using continuous scale‐derived data, these tools should be standardised, and peer‐reviewed (Marshall 2000). Trialists often did not present clear measures of association between intervention and outcome, for example, risk ratios, odds ratios, risk or mean difference, as well as the raw data. Wherever possible, binary outcomes should be reported in preference to continuous scale‐derived data as they are easier to interpret and clinically relevant. If P values are used, the exact value should be reported.
Concrete outcomes of disturbance such as 'disturbed episode', 'use of detention order', 'use of special nursing observation' or, for those in the community, 'avoiding hospitalisation' would be of interest. Data on quality of life, social functioning, occupational status, general impression of carer or other, unwanted effects, such as anxiety, depression and dependence on the relationship with the therapist, staff fatigue and economic outcomes would be very welcome.
The present data provide little indication of how effective CBT procedures might be when they are applied by less experienced practitioners and in routine clinical settings. It would be useful to know whether the effects of CBT are sustained after the therapy course has finished, whether booster sessions are beneficial, and whether continued (long‐term) therapy is required to sustain the treatment effect. A cost/benefit analysis would enable clinicians and purchasers to manage service provision and make best use of resources.
Feedback
Twitter comment, 11 November 2012
Summary
A twitter comment posted re Sensky trial data http://topsy.com/twitter/clinpsych_11?nohidden=1&offset=60&om=aaaaaa&page=7
Reply
Authors have amended review in response to this twitter.
Contributors
Twitter comment: Paul Hutton.
Author responding: Chris Jones.
Feedback received, 14 June 2015
Summary
Rory Bryne provided feedback regarding possible errors in data extraction and trial selection for this review.
Reply
We would like to thank Rory Byrne for his feedback. The review authors are investigating these comments and will respond in full as soon as possible. If necessary, they will amend the review. Please note, this review is currently being updated. Readers should be aware that some results may change with the publication of this update.
Contributors
Feedback: Rory Byrne
Reply: Claire Irving, Managing Editor Cochrane Schizophrenia Group.
Full response to feedback (June 2015), 25 September 2015
Summary
The authors thank Rory for his feedback and have provided responses to individual comments below. Most of the data entry errors noted by Rory have been corrected and these amendments have not substantially changed the review results or conclusions. Other comments need further investigation and will be addressed in the update of this review which is underway.
Trials missed by searching
1. Comment: Failure to extract data from Lecomte 2008 (1) and Grawe 2006 (2). Both are favourable to CBT over control treatments, but both are not even listed in excluded studies (not identified by reviewers?).
Author Response: Thank you for highlighting this issue – we will investigate this omission and check how they had been missed in the first place to ensure completeness of the searches for the impending full update. Both these publications will be screened for inclusion/exclusion in the forthcoming update.
Management of data
2. Comment: Reviewers did not impute missing values for relapse data for Bechdolf 2004 (3, 4), which goes against the review’s stated methodology.
Author response: Data have been changed for outcome 1.23 rehospitalisationin outcome, and sensitivity analysis. This correction does not make any substantive difference to the results or conclusions.
3. Comment: Relapse data for Tarrier 1999 looks wrong (5), in that long‐term N for counselling is 29 but only 26 were randomised in original study. Also unclear why reviewers did not use 3‐month relapse data (zero in both groups) in their ‘short term outcome’. Author response: the first issue is a typo that has been corrected. The short termrelapse data (zero in both groups) has been added and both amendments do not make any substantive difference to the results or conclusions.
4. Comment: Unclear why Cochrane review did not use relapse or response rate data from Valmaggia 2005 (6) (data available on request). Author response: data were embedded in a table and missed in data extraction. We have now added these data, no substantive difference to results or conclusions.
5. Comment: Cochrane review ignores time spent in hospital as outcome, although suggests it will use this in protocol. This outcome favours CBT in several publications. Author response: the protocol stated it would use relapse and hospitalisation which is recorded as rehospitalisation in the review. Time spent in hospital data are highly problematic and often impossible to synthesise but we will address this issue in the impending full update.
6. Comment: The review makes error with input of Lewis 2002 (7) relapse data, erroneously favouring CBT. It appears to use rehospitalisation data for CBT, and relapse data for supportive counselling. Fixing this means the data are less favourable to CBT. Author response: The data will be corrected to reflect that reported in Tarrier 2004 ( a follow‐up study of Lewis 2002)
“Re‐hospitalisation and relapse
Data were available for 307 (99%) participants for hospital admission and 285 (92%) for relapse. Rates of re‐hospitalisationwere: CBT, 33/101 (33%); supportive counselling, 31/106 (29%); treatment as usual, 37/102 (36%). Rates of relapse were: CBT, 53/97 (54.6%); supportive counselling, 50/96 (52.1%); treatment as usual, 47/92 (51.1%). There was no clear differencein number or survival times (Cox’s regression) for either re‐hospitalisation or relapse between the groups.”
The final sample consisted of 309 participants, of whom 101 were allocated to CBT, 106 to supportive counselling and 102 to treatment as usual. At the 18‐month follow‐up assessment, 225 patients (73% of those randomised) were interviewed: of these, 75 had received CBT, 79 supportive counselling and 71 treatment as usual.
7. Comment: Cochrane review also fails to use equivocal re‐hospitalisation data from Lewis 2002 (7) and Sensky 2000
Author response: data in these papers have been checked, findings are below
Lewis 2002
Length of hospital admission, duration 42 to 70 days
“A secondary analysis was performed for length of index hospital admission. There was no difference between the treatment groups, with median lengths of stay of 48 days for CBT, 53 for supportive counselling and 47 for routine care.” (Page 95)
Not used in review. Duration of hospitalisation data were not included in this review but will be added to subsequent editions of this review.
1.1 Tarrier 2004 ( is linked with Lewis 2002 in review as is an 18 month follow‐up of Lewis 2002)
“Participant hospital data were available for assessment of re‐hospitalisation in 307 (99% of the sample) and case notes for assessment of relapse in 295 (95%). The median number of days until assessment (with interquartile range) was, for each group: CBT, 575 (IQR 557–616), supportive counselling, 571 (557–617) and treatment as usual, 582 (554–640).” (Page 233)
Not used in review. Duration of hospitalisation data were not included in this review but will be added to subsequent editions of this review.
“Data were available for 307 (99%) participants for hospital admission and 285 (92%) for relapse. Rates of re‐hospitalisationwere: CBT, 33/101 (33%); supportive counselling, 31/106 (29%); treatment as usual, 37/102 (36%).” (Page 234)
Used in review 1.23.6 re‐hospitalisationlong term (please note that figures in the review have been corrected for intention‐to‐treat)
“Rates of relapse were: CBT, 53/97 (54.6%); supportive counselling, 50/96 (52.1%); treatment as usual, 47/92 (51.1%). There was no clear differencein number or survival times (Cox’s regression) for either re‐hospitalisation or relapse between the groups.” (Page 234)
Used in review 1.23.3 relapse long term (please note that figures in the review have been corrected for intention‐to‐treat)
Sensky 2000
No data regarding relapse or re‐hospitalisationwere identified.
2.1 Turkington 2008 (linked with Sensky 2000 in review as is a 5 year follow‐up to Sensky 2000)
“3.5. Hospitalisation results over 5 years
“There was no clear difference between the two groups available for study on the number of re‐hospitalisations or total days spent in hospital. There was a trend in favour of CBT (CBT total days hospitalised=1323, BF total days hospitalised=2947). The hospitalisation data were heavily skewed. Analysis was undertaken using log transformation and then with non‐parametric methodology. The actual number of patients admitted was 26 (CBT=14, BF=12) with the total number of admissions being 41 (CBT=22, BF=19).” (Pages 4 and 5)
The following data should be added to 1.23.6 re‐hospitalisationlong term
CBT Control: Sensky 2000 14/46 12/44
This will be add to the next review
7. Comment: extraction of re‐hospitalisation data from Buchkremer 1997 (9) is suspect in Cochrane review. Unclear which groups they extracted data from, or why (study had a complex design, and not clear how to categorise as CBT or control). Author response: we agree this is a complex design. We had tried to be as fair as possible to these difficult data. We have now made things more simple in that we have pooled groups 2 and 2a (CBT) and groups 1 and 1a for the control group. In doing this results and conclusions are not substantively changed.
Long term outcomes (one year) should be based on pooling group II and group IIa ((0.15*33)+(0.32*34))/(33+34)) for CBT and pooling group I and group Ia ((0.31*32)+(0.27*35))/(32+35)) for OPT
Interpretation/Presentation
8. Comment: Medium‐term non‐response data are heterogenous (50%), but demonstrate a significant trend in favour of CBT (RR of non‐response 0.78 [0.61, 1.00], p=.047). Unclear why the Cochrane review reports this as ‘no difference’, and reports only the equivocal results from long‐term non‐response rate data in the abstract. Author response: We undertake no statistical test for trend. The reader states that there is a significant trend in favour of CBT. He may have undertaken this statistical test but this is not routine in Cochrane reviews and for this outcome, being one of three focusing on this finding, there is the danger of over analysing weak data. We note that in the 2012 version we state “As neither short‐term or long‐term effects for “no important or reliable change” showed a clear effect it was considered appropriate to interpret this ambiguous finding (i.e., CI 0.61 to 1.00) as non‐significant. This conclusion is further supported by the observation that two of the three studies contributing to this effect did not show significant results.” We recognise that readers may differ on this issue but it was one that was not ignored in the 2012 version.
9. Comment: In other Cochrane reviews (e.g., haloperidol review), effect sizes with wider confidence intervals were interpreted as favourable but not statistically significant (e.g., haloperidol vs placebo: numbers leaving early at 6‐24 weeks, 8 RCTS, RR 0.56 [0.30, 1.04]). The wide confidence intervals in the CBT review probably reflect the limited number of studies and limited number of participants (i.e., low statistical power).
Author response: We recognise the need to be even‐handed across all reviews. The Cochrane editors have noted this helpful comment and we will encourage all authors to ensure that findings that are not falling within the conventional boundaries of statistical significance are noted as such in the same way.
10. Comment: Failing to consider whether the results are robust to different statistical approaches: One way of reducing heterogeneity is to examine whether it persists when different statistical methods are used (10). If we calculate the odds ratio for the medium term non‐response data, the results clearly favour CBT, and heterogeneity is 0% (OR of non‐response 0.29 [0.13, 0.64]). This translates to a numbers needed to treat of 5 (95% CI 3‐25). [This figure does not include equivocal data from Valmaggia 2005 , or CBT‐favourable data from Lecomte 2008. The OR for the analysis with these studies included is 0.34 [0.19, 0.62], with an associated NNT of 7 (3‐ infinity)].
Author response: Thank you for pointing this out. This is one important result of many within the review. This one finding is clearly unstable and it is important that this is considered when any additional data are added from the above studies in the impending full update.
11. Comment: Failure to include all relevant studies and failure to consider dose: The Cochrane review also fails to include long‐term data from Grawe 2006 in their analysis of long‐term non‐response rates. If we include this study, then the random‐effects analysis begins to favour CBT. The original RR of 0.84 [0.64, 1.09] becomes 0.79 [0.62, 1.01]. However heterogeneity is still substantial (48%) and significant (p=0.10), meaning the studies might be too different to meaningfully combine in a meta‐analysis. Indeed, removing the lowest dose study (Tarrier 1999), leads to 0% heterogeneity and an estimate of 0.71 [0.57, 0.89], favouring CBT. The NNT for CBT in this analysis is 5 (3‐14). Moreover, the odds‐ratio estimate favoured CBT regardless of whether we included Grawe 2006 or excluded Tarrier 1999 (original OR 0.54 [0.30, 0.96]).
12. Author response: Thank you for giving this consideration to the trials. As this trial has not yet been screened or data extracted by review authors, this issue will be considered when any additional data are added from the above studies in the impending full update.
References
1. Lecomte T, Leclerc C, Corbiere M, Wykes T, Wallace CJ, Spidel A. Group cognitive behavior therapy or social skills training for individuals with a recent onset of psychosis? Results of a randomized controlled trial. J Nerv Ment Dis. 2008 Dec;196(12):866‐75.
2. Grawe RW, Falloon IRH, Widen JH, Skogvoll E. Two years of continued early treatment for recent‐onset schizophrenia: a randomised controlled study. Acta Psychiatrica Scandinavica. 2006;114(5):328‐36.
3. Bechdolf A, Knost B, Kuntermann C, Schiller S, Klosterkotter J, Hambrecht M, et al. A randomized comparison of group cognitive‐behavioural therapy and group psychoeducation in patients with schizophrenia. Acta Psychiatr Scand. 2004 Jul;110(1):21‐8.
4. Bechdolf A, Kohn D, Knost B, Pukrop R, Klosterkotter J. A randomized comparison of group cognitive‐behavioural therapy and group psychoeducation in acute patients with schizophrenia: outcome at 24 months. Acta Psychiatr Scand. 2005 Sep;112(3):173‐9.
5. Tarrier N, Yusupoff L, Kinner C, McCarthy E, Gladhill A, Haddock G, et al. A randomized controlled trial of intense cognitive behaviour therapy for chronic schizophrenia. British Medical Journal. 1998;317:303‐7.
6. Valmaggia LR, van der Gaag M, Tarrier N, Pijnenborg M, Slooff CJ. Cognitive‐behavioural therapy for refractory psychotic symptoms of schizophrenia resistant to atypical antipsychotic medication. Randomised controlled trial. Br J Psychiatry. 2005 Apr;186:324‐30.
7. Tarrier N, Lewis S, Haddock G, Bentall R, Drake R, Kinderman P, et al. Cognitive‐behavioural therapy in first‐episode and early schizophrenia. 18‐month follow‐up of a randomised controlled trial. Br J Psychiatry. 2004 Mar;184:231‐9.
8. Turkington D, Sensky T, Scott J, Barnes TR, Nur U, Siddle R, et al. A randomized controlled trial of cognitive‐behavior therapy for persistent symptoms in schizophrenia: a five‐year follow‐up. Schizophr Res. 2008 Jan;98(1‐3):1‐7.
9. Buchkremer G, Klingberg S, Holle R, Schulze Monking H, Hornung WP. Psychoeducational psychotherapy for schizophrenic patients and their key relatives or care‐givers: results of a 2‐year follow‐up. Acta Psychiatr Scand. 1997 Dec;96(6):483‐91.
10. Higgins JPT, Green S, Collaboration C. Cochrane handbook for systematic reviews of interventions. Chichester, England ; Hoboken, NJ: Wiley‐Blackwell; 2011. Available from: http://www.cochrane‐handbook.org.
Reply
Replies are above.
Contributors
Chris Jones (review author)
Clive Adams and Claire Irving: editorial team Cochrane Schizophrenia Group.
What's new
| Date | Event | Description |
|---|---|---|
| 4 June 2019 | Amended | Correction to article metadata; no impact on article content. |
History
Protocol first published: Issue 9, 2010 Review first published: Issue 4, 2012
| Date | Event | Description |
|---|---|---|
| 8 April 2019 | Amended | Minor spelling corrections made. |
| 10 May 2017 | New search has been performed | Results of update searching added to review, 16 new trials added to included studies table. New data added to analyses. Methods and text updated. |
| 10 May 2017 | New citation required but conclusions have not changed | New data do not change the overall conclusions from previous versions of this review. |
| 25 September 2015 | Amended | Author response added to feedback received June 2015. See Feedback 3. |
| 9 July 2015 | Amended | New feedback has been received (see Feedback). |
| 20 March 2014 | Amended | Title changed to Cognitive Behavioural Therapy versus other psychosocial treatments for schizophrenia |
| 2 April 2013 | Amended | Outcomes from paper Turkington 2008 added to NA ‐ Sensky 2000. Also see Feedback section. |
| 17 April 2012 | Amended | Reference correction (Birchwood 2006). |
Notes
None.
Acknowledgements
Cochrane Schizophrenia maintain a template for the methods section of their reviews, we have used and adapted this template.
Clive Adams, for invaluable editorial support and encouragement. We would also like to thank Sujoy Ray for his help with data extraction from several papers.
We thank for peer reviewing this update.
Appendices
Appendix 1. Previous searches
1. Detail of previous searches
1.1 The Cochrane Schizophrenia Group's Register (January 2004) was searched using the phrase:
{[(*cogniti* AND (*behavio* or therap*)) OR (*cogniti* and (*technique* or *restructur* or *challeng*)) OR (*self* and (*instruct* or *management* or *attribution*)) OR (*rational* and *emotiv*) in title, abstract, index terms of REFERENCE] or [Cognitive* in interventions of STUDY]}
The Schizophrenia Groups trials register is based on regular searches of BIOSIS Inside; CENTRAL; CINAHL; EMBASE; MEDLINE and PsycINFO; the hand searching of relevant journals and conference proceedings, and searches of several key grey literature sources. A full description is given in the Group's module.
2. Details of previous searches:
2.1 Biological Abstracts (January 1980 ‐ January 1998) was searched using the Cochrane Schizophrenia Groups search for randomised controlled trials and schizophrenia (please see Cochrane Schizophrenia Group Module) combined with:
[and (COGNITIV* and BEHAVIO* and THERAP*) or (COGNITI* and (TECHNIQUE* or THERAP* or RESTRUCTUR* or CHALLENG*)) or (ATTRIBUTION* or (SELF and (INSTRUCT* or MANAGEMENT* or ATTRIBUTION*))) or (RET or (RATIONAL and EMOTIV*))]
2.2 CINAHL (January 1982 ‐ January 1998) was searched using the Cochrane Schizophrenia Group's search for randomised controlled trials and schizophrenia (please see Cochrane Schizophrenia Group Module) combined with:
[and (COGNITIV* and BEHAVIO* and THERAP*) or (COGNITI* and (TECHNIQUE* or THERAP* or RESTRUCTUR* or CHALLENG*)) or (ATTRIBUTION* or (SELF and (INSTRUCT* or MANAGEMENT* or ATTRIBUTION*))) or (RET or (RATIONAL and EMOTIV*)) or "COGNITIVE‐THERAPY"/ all topical subheadings / all age subheadings]
2.3 The Cochrane Library (Issue 2, 1998) CENTRAL Register was searched using the phrase:
[<me> COGNITIVE THERAPY or <me> PSYCHOTHERAPY RATIONAL EMOTIVE or (COGNITI* and (TECHNIQUE* or THERAP* or RESTRUCTUR* or CHALLENG*)) or (SELF and ( INSTRUCT* or MANAGEMENT* or ATTRIBUTION*)) or ATTRIBUTION* or (COGNITIV* and BEHAVIO* and THERAP*) or RET or ( RATIONAL and EMOTIV*)]
2.4 The Cochrane Schizophrenia Group's Register of Trials (August 1998) was searched using the phrase:
[(COGNITIV* and BEHAVIO* and THERAP*) or (COGNITI* and (TECHNIQUE* or THERAP* or RESTRUCTUR* or CHALLENG*)) or (ATTRIBUTION* or (SELF and (INSTRUCT* or MANAGEMENT* or ATTRIBUTION*))) or (RET or (RATIONAL and EMOTIV*)) or #42=142]
2.5 The Cochrane Schizophrenia Groups' Register of Trials (January 2001) was searched using the phrase:
[(COGNITIV* and BEHAVIO* and THERAP*) or (COGNITI* and (TECHNIQUE* or THERAP* or RESTRUCTUR* or CHALLENG*)) or (ATTRIBUTION* or (SELF and (INSTRUCT* or MANAGEMENT* or ATTRIBUTION*))) or (RET or (RATIONAL and EMOTIV*))]
This register now encompasses all other of the databases and many more (see Group Module).
2.6 EMBASE (1980 ‐ January 1998) was searched using the Cochrane Schizophrenia Group's search for randomised controlled trials and schizophrenia (please see Cochrane Schizophrenia Group Module) combined with:
[and (COGNITIV* and BEHAVIO* and THERAP*) or (COGNITI* and (TECHNIQUE* or THERAP* or RESTRUCTUR* or CHALLENG*)) or (ATTRIBUTION* or (SELF and (INSTRUCT* or MANAGEMENT* or ATTRIBUTION*))) or (RET or (RATIONAL and EMOTIV*)) or "COGNITIVE‐THERAPY"/ all subheadings]
2.7 MEDLINE (1966 ‐ January 1998) was searched using the Cochrane Schizophrenia Group's search for randomised controlled trials and schizophrenia (please see Cochrane Schizophrenia Group Module) combined with:
[and (COGNITIV* and BEHAVIO* and THERAP*) or (COGNITI* and (TECHNIQUE* or THERAP* or RESTRUCTUR* or CHALLENG*)) or (ATTRIBUTION* or (SELF and (INSTRUCT* or MANAGEMENT* or ATTRIBUTION*))) or (RET or (RATIONAL and EMOTIV*)) or "COGNITIVE‐THERAPY"/ all subheadings]
2.8 PsycLIT (1887 January 1998) was searched using the Cochrane Schizophrenia Group's search for randomised controlled trials and schizophrenia (please see Cochrane Schizophrenia Group Module) combined with:
[and (COGNITIV* and BEHAVIO* and THERAP*) or explode "COGNITIVE‐TECHNIQUES" or (COGNITI* and (TECHNIQUE* or THERAP* or RESTRUCTUR* or CHALLENG*)) or (ATTRIBUTION* or (SELF and (INSTRUCT* or MANAGEMENT* or ATTRIBUTION*))) or (RET or (RATIONAL near2 EMOTIV*)) or explode "RATIONAL‐EMOTIVE‐THERAPY" or explode "SELF‐HELP‐TECHNIQUES" or explode "INDIVIDUALIZED‐INSTRUCTION" or explode "SELF‐INSTRUCTIONAL‐TRAINING"]
2.9 SIGLE (1990 ‐ January 1998) was searched using the Cochrane Schizophrenia Group's search for randomised controlled trials and schizophrenia (please see Cochrane Schizophrenia Group Module) combined with:
[and (COGNITIV* and BEHAVIO* and THERAP*) or (COGNITI* and (TECHNIQUE* or THERAP* or RESTRUCTUR* or CHALLENG*)) or (ATTRIBUTION* or (SELF and (INSTRUCT* or MANAGEMENT* or ATTRIBUTION*))) or (RET or (RATIONAL and EMOTIV*))]
2.10 Sociofile (1980 ‐ January 2001) was searched using the Cochrane Schizophrenia Group's search for randomised controlled trials and schizophrenia (please see Cochrane Schizophrenia Group Module) combined with:
[and (COGNITIV* and BEHAVIO* and THERAP*) or (COGNITI* and (TECHNIQUE* or THERAP* or RESTRUCTUR* or CHALLENG*)) or (ATTRIBUTION* or (SELF and (INSTRUCT* or MANAGEMENT* or ATTRIBUTION*))) or (RET or (RATIONAL and EMOTIV*)) or explode "PSYCHOTHERAPY"]
Searching other resources
1. Reference Lists All references of included articles were searched for further relevant trials.
2. Authors When appropriate, the first author of each of the included papers was contacted and additional published and unpublished materials were requested.
Appendix 2. Previous data collection and analyses
Data collection and analysis
Selection of studies
Three review authors (AM, DH & CAJ) independently inspected all identified citations. When disputes arose as to which category a citation should be allocated, resolution was attempted by discussion. When this was not possible, we acquired the full article. Two review authors (DH, CAJ) independently inspected all articles identified in this way. When disputes arose as to whether an article was indeed relevant to this review, we attempted resolution by discussion. When this was not possible, we asked another review authors (CI) to read the article and decide. IR, AM and CI reviewed 30% of the citations and articles, included and excluded by DH and CAJ, to check the use of inclusion criteria.
Data extraction and management
1. Extraction
Review authors DH and CAJ extracted data from all included studies. In addition, to ensure reliability, CI independently extracted data from a random sample of these studies, comprising 10% of the total. We resolved disputes by discussion and adjudication from the other review authors (AM, CI and IC) if necessary. When it was not possible to extract data or if further information was needed, we attempted to contact the authors. We extracted data presented only in graphs and figures whenever possible, but the data were included only if two review authors independently had the same result. We attempted to contact authors through an open‐ended request in order to obtain missing information or for clarification whenever necessary. Where possible, we extracted data relevant to each component centre of multi‐centre studies separately.
2. Management
2.1 Forms
We extracted data onto standard, simple forms.
2.2 Scale‐derived data
We included continuous data from rating scales only if: a. the psychometric properties of the measuring instrument had been described in a peer‐reviewed journal (Marshall 2000); and b. the measuring instrument was not written or modified by one of the trialists for that particular trial; and c. the measuring instrument was either i. a self‐report or ii. completed by an independent rater or relative (not the therapist).
2.3 Endpoint versus change data
There are advantages of both endpoint and change data. Change data can remove a component of between‐person variability from the analysis. On the other hand, calculation of change needs two assessments (baseline and endpoint) which can be difficult in unstable and difficult to measure conditions such as schizophrenia. We decided to primarily use endpoint data and only use change data if the former were not available. We combined endpoint and change data in the analysis as we used mean differences rather than standardised mean differences throughout (Higgins 2009 ).
2.4 Skewed data
Continuous data on clinical and social outcomes are often not normally distributed. To avoid the pitfall of applying parametric tests to non‐parametric data, we aimed to apply the following standards to all data before inclusion: a) standard deviations and means are reported in the paper or obtainable from the authors; b) when a scale starts from the finite number zero, the standard deviation (SD), when multiplied by two, is less than the mean (as otherwise the mean is unlikely to be an appropriate measure of the centre of the distribution, (Altman 1996); c) if a scale started from a positive value (such as Positive and Negative Syndrome Scale (PANSS) which can have values from 30 to 210), the calculation described above was modified to take the scale starting point into account. In these cases skew is present if 2 SD > (S‐S min), where S is the mean score and S min is the minimum score. Endpoint scores on scales often have a finite start and end point and these rules can be applied. When continuous data are presented on a scale that includes a possibility of negative values (such as change data), it is difficult to tell whether data are skewed or not. We planned to enter skewed data from studies of less than 200 participants in additional tables rather than into an analysis. Skewed data pose less of a problem when looking at means if the sample size is large and such data were entered into syntheses.
2.5 Common measure
To facilitate comparison between trials, we intended to convert variables that can be reported in different metrics, such as days in hospital (mean days per year, per week or per month) to a common metric (e.g. mean days per month).
2.6 Conversion of continuous to binary
Where possible, efforts were made to convert outcome measures to dichotomous data. This could be done by identifying cut‐off points on rating scales and dividing participants accordingly into 'clinically improved' or 'not clinically improved'. It was generally assumed that if there had been a 50% reduction in a scale‐derived score such as the Brief Psychiatric Rating Scale (BPRS, Overall 1962) or the PANSS (Kay 1987), this could be considered as a clinically significant response (Leucht 2005a; Leucht 2005b). If data based on these thresholds were not available, we used the primary cut‐off presented by the original authors.
2.7 Direction of graphs
Where possible, we entered data in such a way that the area to the left of the line of no effect indicates a favourable outcome for CBT.
2.8 Summary of findings table
We anticipated including the following short‐ or medium term outcomes in a 'Summary of findings' table.
1. Global state
1.1 Relapse 1.2 Rehospitalisation 1.3 Healthy days
2. Mental state
2.1 Improved to an important extent
3. Adverse effect
3.1 Any adverse event
4. Social functioning
4.1 Employed
5. Quality of life
5.1 Not improved to an important extent
Assessment of risk of bias in included studies
Two review authors (DH and CAJ) assessed risk of bias using the tool described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2009). This tool encourages consideration of how the randomisation sequence was generated, how allocation was concealed, the integrity of blinding at outcome measurement, the completeness of outcome data, selective reporting and other biases. We excluded studies where sequence generation was at a high risk of bias or where allocation was clearly not concealed. If disputes arose as to the correct category for a trial, this was resolved through discussion and adjudication by the other review authors (AM, CI and IC) if necessary. If this was not possible because further information was necessary, we intended not to enter the data but to allocate the trial to the list of those awaiting assessment. Review authors were not blinded to the names of the authors, institutions, journal of publication, or results of the trials.
Measures of treatment effect
We adopted P = 0.05 as the conventional level of statistical significance but we were especially cautious where results were only slightly below this, and we reported 95% confidence intervals (CI) in preference to P values.
1. Binary data
For binary outcomes, we calculated a standard estimation of the risk ratio (RR) and its 95% CI. It has been shown that RR is more intuitive (Boissel 1999) than odds ratios (OR) and that (OR) tend to be interpreted as RR by clinicians (Deeks 2000). For statistically significant results, we had planned to calculate the number needed to treat to provide benefit /to induce harm statistic (NNTB/H), and its 95% CI using Visual Rx (http://www.nntonline.net/) taking account of the event rate in the control group, but this has been superseded by the Summary of findings table 1.
2. Continuous data
For continuous outcomes, we estimated mean difference (MD) between groups. We preferred not to calculate effect size measures (standardised mean difference SMD). However, had scales of very considerable similarity been used, we would have presumed there was a small difference in measurement, and we would have calculated effect size and transformed the effect back to the units of one or more of the specific instruments.
Unit of analysis issues
1. Cluster trials
Studies increasingly employ 'cluster randomisation' (such as randomisation by clinician or practice) but analysis and pooling of clustered data poses problems. Firstly, authors often fail to account for intra‐class correlation in clustered studies, leading to a 'unit of analysis' error (Divine 1992) whereby P values are spuriously low, CIs unduly narrow and statistical significance overestimated. This causes type I errors (Bland 1997; Gulliford 1999).
Where clustering was not accounted for in primary studies, we had planned to present data in a table, with a (*) symbol to indicate the presence of a probable unit of analysis error. In subsequent versions of this review we will seek to contact first authors of studies to obtain intra‐class correlation coefficients for their clustered data and to adjust for this by using accepted methods (Gulliford 1999). Where clustering has been incorporated into the analysis of primary studies, we will present these data as if from a non‐cluster randomised study, but adjust for the clustering effect.
We have sought statistical advice and been advised that the binary data presented in a report should be divided by a 'design effect'. This is calculated using the mean number of participants per cluster (m) and the intra‐class correlation coefficient (ICC) [Design effect = 1+(m‐1)*ICC] (Donner 2002). If the ICC is not reported it is assumed to be 0.1 (Ukoumunne 1999).
If cluster studies had been appropriately analysed taking into account ICCs and relevant data documented in the report, synthesis with other studies would have been possible using the generic inverse variance technique.
2. Cross‐over trials
A major concern of cross‐over trials is the carry‐over effect. It occurs if an effect (e.g. pharmacological, physiological or psychological) of the treatment in the first phase is carried over to the second phase. As a consequence, on entry to the second phase, the participants can differ systematically from their initial state despite a wash‐out phase. For the same reason cross‐over trials are not appropriate if the condition of interest is unstable (Elbourne 2002). As both effects are very likely in severe mental illness, had we found any cross‐over trials, we planned to use only the data from the first phase of the study.
3. Studies with multiple treatment groups
Where a study involved more than two treatment arms, if relevant, we presented the additional treatment arms in the comparisons. Where the additional treatment arms were not relevant, we did not report these data.
Dealing with missing data
1. Overall loss of credibility
At some degree of loss of follow‐up, the findings of a trial must lose credibility (Xia 2009). We were forced to make a judgment where this was for the very short term trials likely to be included in this review. We decided that if more than 40% of data were unaccounted for at eight weeks, we would not reproduce these data or use them within analyses.
2. Binary
If attrition for a binary outcome was between 0% and 40% and outcomes of these people were described, we included these data as reported. Where these data were not clearly described for the primary outcome, we assumed the worst for each person who was lost, and for adverse effects, we assumed rates similar to those among patients who did continue to have their data recorded.
3. Continuous
3.1 Attrition
In the case where attrition for a continuous outcome was between 0% and 40% and completer‐only data were reported, we have reproduced these.
3.2 Standard deviations
We first tried to obtain the missing values from the authors. If not available, where there were missing measures of variance for continuous data but an exact standard error (SE) and CI were available for group means , and either 'P' value or 't' value were available for differences in mean, we noted these, and in future versions of this review we will calculate them according to the rules described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2009): When only the SE is reported, standard deviations (SDs) can be calculated by the formula SD = SE * square root (n). Chapters 7.7.3 and 16.1.3 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2009) present detailed formula for estimating SDs from P values, t or F values, CIs, ranges or other statistics. If these formula do not apply, we, in the future will calculate SDs according to a validated imputation method which is based on the SDs of the other included studies (Furukawa 2006). Some of these imputation strategies can introduce error. The alternative would be to exclude a given study’s outcome and thus to lose information. We will examine the validity of the imputations in a sensitivity analysis excluding imputed values.
3.3 Last observation carried forward
We anticipated that in some studies the method of Last Observation Carried Forward (LOCF) would be employed within the study report. As with all methods of imputation to deal with missing data, LOCF introduces uncertainty about the reliability of the results. Therefore, where LOCF data have been used in the trial, if less than 40% of the data had been assumed, we reproduced these data and indicated that they are the product of LOCF assumptions.
Assessment of heterogeneity
1. Clinical heterogeneity
We considered all included studies initially, without seeing comparison data, to judge clinical heterogeneity. We simply inspected all studies for clearly outlying situations or people which we had not predicted would arise. When such situations or participant groups arose, these were fully discussed.
2. Methodological heterogeneity
We considered all included studies initially, without seeing comparison data, to judge methodological heterogeneity. We simply inspected all studies for clearly outlying methods which we had not predicted would arise. When such methodological outliers arose these were fully discussed.
3. Statistical heterogeneity
3.1 Visual inspection
We visually inspected graphs to investigate the possibility of statistical heterogeneity.
3.2 Employing the I2 statistic
Heterogeneity between studies was investigated by considering the I2 method alongside the Chi2 'P' value. The I2 provides an estimate of the percentage of inconsistency thought to be due to chance (Higgins 2003). The importance of the observed value of I2depends on i. magnitude and direction of effects and ii. strength of evidence for heterogeneity (e.g. 'P' value from Chi2 ¬test, or a CI for I2). We interpreted an I2 estimate greater than or equal to 75% accompanied by a statistically significant Chi2 statistic as evidence of substantial levels of heterogeneity (Higgins 2009). When substantial levels of heterogeneity were found in the primary outcome, we explored reasons for heterogeneity (Subgroup analysis and investigation of heterogeneity).
Assessment of reporting biases
Reporting biases arise when the dissemination of research findings is influenced by the nature and direction of results (Egger 1997). These are described in section 10.1 of the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2009). We are aware that funnel plots may be useful in investigating reporting biases but are of limited power to detect small‐study effects. We did not use funnel plots for outcomes where there were 10 or fewer studies, or where all studies were of similar sizes. In other cases, where funnel plots were possible, we sought statistical advice in their interpretation.
Data synthesis
We understand that there is no closed argument for preference for use of fixed‐effect or random‐effects models. The random‐effects method incorporates an assumption that the different studies are estimating different, yet related, intervention effects. The random‐effects model takes into account differences between studies, even if there is no statistically significant heterogeneity. There is, however, a disadvantage to the random‐effects model. It puts added weight onto small studies which often are the most biased ones. Depending on the direction of effect, these studies can either inflate or deflate the effect size.
Subgroup analysis and investigation of heterogeneity
1. Subgroup analyses
We anticipated subgroup analyses to test the hypothesis that CBT may be highlighted to have different effects when compared with:
1.1 Active versus non active control therapies
Active psychological treatments as opposed to inactive ones.
1.2 Rigorous criteria for diagnosing schizophrenia as opposed to more loose criteria
We defined 'rigorous' as involving operational criteria.
1.3 Rigorous criteria for describing CBT as opposed to a more loose description
We defined 'rigorous' as outlined this in Types of interventions.
1.4 People in first episode of illness versus those at a later stage of illness
For each of the above subgroups, we aimed to undertake the analysis for only the primary outcomes of this review or the nearest we could find to them (see Types of outcome measures) and if data were available discussed the findings in the Effects of interventions..
2. Investigation of heterogeneity
If inconsistency was high, this was reported. First, we investigated whether data had been entered correctly. Second, if data were correct, we visually inspected the graph and studies outside of the company of the rest were successively removed to see if heterogeneity was restored. When this occurred with no more than 10% of the data being excluded, we presented the data. If not, we did not pool data and discussed the issues.
Where unanticipated clinical or methodological heterogeneity were obvious, we simply stated hypotheses regarding these for future reviews or versions of this review. We did not anticipate undertaking analyses relating to these.
Sensitivity analysis
1. Implication of randomisation
We aimed to include trials in a sensitivity analysis if they were described in some way as to imply randomisation. For the primary outcomes, we included these studies and if there was no substantive difference when the implied randomised studies were added to those with better description of randomisation, then we used all the data from these studies.
2. Blinding
We aimed to include trials in a sensitivity analysis if they were described in some way that suggested they blinded for assessment of outcome as opposed to not blinding at all. For the primary outcomes, we compared findings of blinded and non‐blinded studies.
3. Well‐defined CBT versus less‐well‐defined CBT
We aimed to include trials in a sensitivity analysis if they meet the criteria for 'well‐defined' CBT as opposed to those studies that labelled the therapy as CBT but either did not contain the 'inferential' and 'evaluative' component or who did not provide enough information for this discrimination to be made (see Types of interventions). For the primary outcomes, we compared findings of well‐defined CBT and less‐well‐defined CBT.
Appendix 3. Changes from protocol to first version of the review
1. Methods from the protocol could not be implemented.
1.1 Trial search
For the trial search, we did not contact the first author of each of the included papers and requested additional published and unpublished materials in the update review process.
1.2 Data extraction and management
For the data extraction and management, we did not encounter change data, therefore only endpoint data were used. We did not convert continuous data to binary. We did not encounter data from cross‐over or cluster‐randomised controlled trials. The attrition rate was between 0% to 40% in all studies with missing data, therefore, we included data as reported. Due to the sparse data, we did not test other subgroup hypotheses excluding the subgroup "active" versus "non active" control analysis.
1.3 'Summary of findings' table
In the full review, we included short‐term relapse and rehospitalisation, mental state: clinically important change, death, adverse event, social function and long‐term quality of life in our 'Summary of findings' table. We did not encounter any study reporting healthy days and no improvement of quality of life.
Data and analyses
Comparison 1. CBT versus OTHER PSYCHOSOCIAL THERAPIES.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Global state: 1. Relapse | 7 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 Short term | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.72 [0.05, 11.02] |
| 1.2 Medium term | 2 | 150 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.56, 1.81] |
| 1.3 Long term | 5 | 375 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.85, 1.29] |
| 2 Global state: 2. Average endpoint total score various scales, high = good) | 4 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 2.1 GAS ‐ medium term | 1 | 38 | Mean Difference (IV, Fixed, 95% CI) | ‐0.60 [‐4.93, 3.73] |
| 2.2 GAS ‐ long term | 1 | 30 | Mean Difference (IV, Fixed, 95% CI) | ‐0.5 [‐7.63, 6.63] |
| 2.3 GAF ‐ short term | 2 | 147 | Mean Difference (IV, Fixed, 95% CI) | 9.02 [4.29, 13.75] |
| 2.4 GAF‐ long term | 3 | 175 | Mean Difference (IV, Fixed, 95% CI) | 5.42 [‐0.37, 11.20] |
| 3 Global state: 3. Rehospitalisation | 8 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Short term | 1 | 65 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.44 [0.13, 1.56] |
| 3.2 Medium term | 3 | 344 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.57, 1.29] |
| 3.3 Long term | 8 | 943 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.82, 1.14] |
| 4 Mental state: 1. General ‐ clinically important change (no improvement) | 7 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 4.1 Short term | 2 | 87 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.58, 0.99] |
| 4.2 Medium term | 3 | 195 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.58, 1.23] |
| 4.3 Long term | 4 | 249 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.67, 1.01] |
| 5 Mental state: 2. General (average endpoint total score, various scales, high = poor) | 17 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 5.1 BPRS ‐ short term | 3 | 162 | Mean Difference (IV, Fixed, 95% CI) | 0.23 [‐2.83, 3.29] |
| 5.2 BPRS ‐ medium term | 1 | 37 | Mean Difference (IV, Fixed, 95% CI) | ‐7.60 [‐14.30, ‐0.90] |
| 5.3 PANSS ‐ short term | 6 | 568 | Mean Difference (IV, Fixed, 95% CI) | ‐5.38 [‐7.31, ‐3.44] |
| 5.4 PANSS ‐ medium term | 3 | 270 | Mean Difference (IV, Fixed, 95% CI) | ‐4.90 [‐7.93, ‐1.87] |
| 5.5 PANSS ‐ long term | 9 | 596 | Mean Difference (IV, Fixed, 95% CI) | ‐3.22 [‐5.42, ‐1.01] |
| 5.6 CPRS ‐ medium term | 1 | 90 | Mean Difference (IV, Fixed, 95% CI) | ‐4.30 [‐9.26, 0.66] |
| 5.7 CPRS ‐ long term | 1 | 59 | Mean Difference (IV, Fixed, 95% CI) | ‐4.60 [‐11.22, 2.02] |
| 6 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS subscale, high = poor) | 14 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 Short term | 10 | 883 | Mean Difference (IV, Fixed, 95% CI) | ‐0.57 [‐1.19, 0.05] |
| 6.2 Medium term | 6 | 497 | Mean Difference (IV, Fixed, 95% CI) | ‐1.20 [‐2.04, ‐0.36] |
| 6.3 Long term | 9 | 602 | Mean Difference (IV, Fixed, 95% CI) | ‐1.22 [‐1.96, ‐0.49] |
| 7 Mental state: 3b. Specific ‐ positive symptoms (average endpoint score various subscales, high = poor) ‐ skewed data | Other data | No numeric data | ||
| 7.1 PANSS ‐ short term | Other data | No numeric data | ||
| 7.2 SAPS ‐ medium term | Other data | No numeric data | ||
| 7.3 BPRS ‐ short term | Other data | No numeric data | ||
| 7.4 BPRS ‐ long term | Other data | No numeric data | ||
| 8 Mental state: 3c. Specific ‐ positive symptoms (average endpoint BPRS subscale, high = poor) ‐ short term | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | ‐0.10 [‐0.45, 0.25] |
| 9 Mental state: 4a. Specific ‐ hallucinations (average endpoint score PSYRATS, high = poor) | 2 | Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 9.1 Short term | 1 | Mean Difference (Fixed, 95% CI) | ‐0.90 [‐4.36, 2.56] | |
| 9.2 Medium term | 1 | Mean Difference (Fixed, 95% CI) | ‐0.1 [‐3.83, 3.63] | |
| 9.3 Long term | 2 | Mean Difference (Fixed, 95% CI) | ‐2.10 [‐5.53, 1.33] | |
| 10 Mental state: 4b. Specific ‐ hallucinations (average endpoint score PSYRATS, high = poor) ‐ skewed data | Other data | No numeric data | ||
| 10.1 Short term | Other data | No numeric data | ||
| 10.2 Medium term | Other data | No numeric data | ||
| 10.3 Long term | Other data | No numeric data | ||
| 11 Mental state: 5a. Specific ‐ delusions (average endpoint score PSYRATS subscale, high = poor) ‐ long term | 1 | Mean Difference (Fixed, 95% CI) | ‐1.04 [‐3.27, 1.19] | |
| 12 Mental state: 5b. Specific ‐ delusions (average endpoint score PSYRATS subscale, high = poor) ‐ skewed data | Other data | No numeric data | ||
| 12.1 Short term | Other data | No numeric data | ||
| 12.2 Medium term | Other data | No numeric data | ||
| 12.3 Long term | Other data | No numeric data | ||
| 13 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) | 11 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 13.1 Short term | 7 | 581 | Mean Difference (IV, Fixed, 95% CI) | ‐0.07 [‐0.76, 0.61] |
| 13.2 Medium term | 4 | 359 | Mean Difference (IV, Fixed, 95% CI) | ‐0.52 [‐1.42, 0.39] |
| 13.3 Long term | 8 | 548 | Mean Difference (IV, Fixed, 95% CI) | ‐0.84 [‐1.67, 0.00] |
| 14 Mental state: 6b. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) ‐ short term, skewed data | Other data | No numeric data | ||
| 15 Mental state: 6c. Specific ‐ negative symptoms (average endpoint score SANS, high = poor) | 2 | Mean Difference (IV, Random, 95% CI) | Subtotals only | |
| 15.1 Short term | 1 | 45 | Mean Difference (IV, Random, 95% CI) | ‐0.36 [‐3.25, 2.53] |
| 15.2 Medium term | 1 | 37 | Mean Difference (IV, Random, 95% CI) | ‐6.60 [‐19.01, 5.81] |
| 15.3 Long term | 1 | 44 | Mean Difference (IV, Random, 95% CI) | 0.49 [‐2.19, 3.17] |
| 16 Mental state: 6d. Specific ‐ negative symptoms (average endpoint score SANS, high = poor) ‐ skewed data | Other data | No numeric data | ||
| 16.1 Short term | Other data | No numeric data | ||
| 16.2 Medium term | Other data | No numeric data | ||
| 16.3 Long term | Other data | No numeric data | ||
| 17 Mental state: 6e. Specific ‐ negative symptoms (average endpoint score BPRS subscale, high = poor) ‐ short term | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | 0.10 [‐0.31, 0.51] |
| 18 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor) | 10 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 18.1 Short term | 6 | 400 | Mean Difference (IV, Fixed, 95% CI) | ‐3.38 [‐4.62, ‐2.13] |
| 18.2 Medium term | 3 | 194 | Mean Difference (IV, Fixed, 95% CI) | ‐0.94 [‐2.75, 0.88] |
| 18.3 Long term | 7 | 379 | Mean Difference (IV, Fixed, 95% CI) | ‐0.94 [‐2.28, 0.40] |
| 19 Mental state: 7b. Specific ‐ affective symptoms (average endpoint score SCL90, high=poor) ‐ long term | 1 | 134 | Mean Difference (IV, Fixed, 95% CI) | 8.26 [1.77, 14.74] |
| 20 Mental state: 8a. Specific ‐ depression (average endpoint score BDI, high = poor) | Other data | No numeric data | ||
| 20.1 Short term | Other data | No numeric data | ||
| 20.2 Medium term | Other data | No numeric data | ||
| 20.3 Long term | Other data | No numeric data | ||
| 21 Mental state: 8b. Specific ‐ depression (average endpoint score MADRS, high = poor) | Other data | No numeric data | ||
| 21.1 Medium term | Other data | No numeric data | ||
| 21.2 Long term | Other data | No numeric data | ||
| 22 Mental state: 8c. Specific ‐ depression (average endpoint score HAMD, high = poor) ‐ short term | 1 | 95 | Mean Difference (IV, Fixed, 95% CI) | ‐3.92 [‐4.96, ‐2.88] |
| 23 Mental state: 9a. Specific ‐ self esteem (average endpoint score RSES, high = good) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 23.1 Short term | 1 | 65 | Mean Difference (IV, Fixed, 95% CI) | 1.60 [‐0.93, 4.13] |
| 23.2 Medium term | 1 | 65 | Mean Difference (IV, Fixed, 95% CI) | 0.80 [‐2.17, 3.77] |
| 23.3 Long term | 1 | 65 | Mean Difference (IV, Fixed, 95% CI) | 1.70 [‐1.79, 5.19] |
| 24 Mental state: 9b. Specific ‐ self esteem (average endpoint score RSES, high = good) ‐ short term, skewed data | Other data | No numeric data | ||
| 25 Mental state: 10. Specific ‐ self stigma (average endpoint score SSMI, high = poor) ‐ short term | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 26 Mental state: 11a. Specific ‐ anxiety (average endpoint score BAI, high = poor) ‐ long term, skewed data | Other data | No numeric data | ||
| 27 Mental state: 11b. Specific ‐ anxiety (average endpoint score HAMA, high = poor) ‐ short term | 1 | 65 | Mean Difference (IV, Fixed, 95% CI) | ‐5.78 [‐8.79, ‐2.77] |
| 28 Mental state: 11c. Specific ‐ anxiety (average endpoint score SARS, high = poor) ‐ short term | 1 | 95 | Mean Difference (IV, Fixed, 95% CI) | ‐2.89 [‐4.53, ‐1.25] |
| 29 Mental state: 12b. Specific ‐ clinically important change ‐ Obessive Compulsive Disorder (no improvement) | 1 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 29.1 Short term | 1 | 65 | Risk Ratio (M‐H, Random, 95% CI) | 0.29 [0.12, 0.68] |
| 30 Mental state: 12a. Specific ‐ Obsessive Compulsive Disorder (average endpoint score Y‐BOCS, high = poor) ‐ short term | 1 | 65 | Mean Difference (IV, Fixed, 95% CI) | ‐13.55 [‐15.43, ‐11.67] |
| 31 Mental state: 13. Specific ‐ anger/aggression (average endpoint score NAS, high = poor) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 31.1 Short term | 1 | 77 | Mean Difference (IV, Fixed, 95% CI) | 2.10 [‐5.70, 9.90] |
| 31.2 Long term | 1 | 77 | Mean Difference (IV, Fixed, 95% CI) | ‐1.05 [‐9.56, 7.46] |
| 32 Mental state: 14. Specific ‐ problem behaviours (average endpoint score various scales, high = poor) ‐ skewed data | Other data | No numeric data | ||
| 32.1 Novaco Provocation Inventory ‐ short term | Other data | No numeric data | ||
| 32.2 Novaco Provocation Inventory ‐ long term | Other data | No numeric data | ||
| 32.3 Ward Anger Rating Scale ‐ long term | Other data | No numeric data | ||
| 32.4 Ward Anger Rating Scale ‐ short term | Other data | No numeric data | ||
| 32.5 HCR‐20 risk management ‐ long term | Other data | No numeric data | ||
| 33 Mental state: 15. Specific ‐ thought disturbances (average endpoint score PANSS subscale, high = poor) | Other data | No numeric data | ||
| 34 Adverse effect/event(s): 1. Number of events | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 34.1 Short term | 1 | 120 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.36 [1.04, 1.79] |
| 34.2 Long term | 1 | 198 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.95 [0.87, 1.03] |
| 35 Adverse effect/event(s): 2. Death ‐ any cause | 6 | 627 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.57 [0.62, 3.98] |
| 36 Functioning: 1a. Social functioning (average endpoint score various scales, high = good) | 3 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 36.1 Social Functioning Scale ‐ short term | 1 | 65 | Mean Difference (IV, Fixed, 95% CI) | 5.40 [‐5.18, 15.98] |
| 36.2 Social Functioning Scale ‐ medium term | 1 | 65 | Mean Difference (IV, Fixed, 95% CI) | 7.20 [‐3.46, 17.86] |
| 36.3 Social Functioning Scale ‐ long term | 1 | 65 | Mean Difference (IV, Fixed, 95% CI) | 8.80 [‐4.07, 21.67] |
| 36.4 Personal and Social Performance Scale ‐ short term | 1 | 165 | Mean Difference (IV, Fixed, 95% CI) | 3.28 [‐0.50, 7.06] |
| 36.5 Personal and Social Performance Scale ‐ medium term | 1 | 162 | Mean Difference (IV, Fixed, 95% CI) | 6.72 [2.18, 11.26] |
| 36.6 Personal and Social Performance Scale ‐ long term | 1 | 168 | Mean Difference (IV, Fixed, 95% CI) | 9.35 [4.66, 14.04] |
| 36.7 Maryland Assessment of Social Competence ‐ medium term | 1 | 77 | Mean Difference (IV, Fixed, 95% CI) | 0.40 [‐0.05, 0.85] |
| 37 Functioning: 1b. Social functioning (average endpoint score SOFAS, high = good) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 37.1 Short term | 1 | 62 | Mean Difference (IV, Fixed, 95% CI) | 5.09 [‐1.21, 11.39] |
| 37.2 Long term | 2 | 103 | Mean Difference (IV, Fixed, 95% CI) | 1.32 [‐4.90, 7.54] |
| 38 Functioning: 2a. Cognitive functioning ‐ insight (average endpoint score various scales, high = good) | 3 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 38.1 Schedule for Assessment of Insight ‐ short term | 1 | 165 | Mean Difference (IV, Fixed, 95% CI) | 0.91 [‐0.27, 2.09] |
| 38.2 Schedule for Assessment of Insight ‐ medium term | 1 | 162 | Mean Difference (IV, Fixed, 95% CI) | 1.27 [0.09, 2.45] |
| 38.3 Schedule for Assessment of Insight ‐ long term | 2 | 218 | Mean Difference (IV, Fixed, 95% CI) | 1.00 [‐0.01, 2.00] |
| 38.4 The Insight Scale ‐ short term | 1 | 68 | Mean Difference (IV, Fixed, 95% CI) | ‐0.60 [‐2.17, 0.97] |
| 39 Functioning: 2b. Cognitive functioning ‐ insight (average endpoint score BCIS / SAI, high = good) ‐ skewed data | Other data | No numeric data | ||
| 39.1 Short term | Other data | No numeric data | ||
| 39.2 Medium term | Other data | No numeric data | ||
| 39.3 Long term | Other data | No numeric data | ||
| 40 Functioning: 3. Life skills ‐ skills acquisition ‐ (average endpoint score CMT, high = good) ‐ skewed data | Other data | No numeric data | ||
| 40.1 Short term | Other data | No numeric data | ||
| 40.2 Medium term | Other data | No numeric data | ||
| 40.3 Long term | Other data | No numeric data | ||
| 41 Quality of life: 1a. General (average endpoint score various scales, high = good) | 4 | 383 | Mean Difference (IV, Fixed, 95% CI) | 0.70 [‐0.52, 1.91] |
| 41.1 LSI ‐ short term | 1 | 60 | Mean Difference (IV, Fixed, 95% CI) | 0.30 [‐1.75, 2.35] |
| 41.2 LSI ‐ medium term | 1 | 58 | Mean Difference (IV, Fixed, 95% CI) | 0.60 [‐1.59, 2.79] |
| 41.3 LSI ‐ long term | 1 | 51 | Mean Difference (IV, Fixed, 95% CI) | 1.70 [‐0.50, 3.90] |
| 41.4 EuroQOL ‐ long term | 1 | 37 | Mean Difference (IV, Fixed, 95% CI) | ‐1.86 [‐19.20, 15.48] |
| 41.5 The Quality of Life Scale ‐ long term | 1 | 50 | Mean Difference (IV, Fixed, 95% CI) | ‐3.40 [‐16.25, 9.45] |
| 41.6 MSQoL ‐ short term | 1 | 63 | Mean Difference (IV, Fixed, 95% CI) | ‐1.80 [‐13.77, 10.17] |
| 41.7 MSQoL ‐ medium term | 1 | 64 | Mean Difference (IV, Fixed, 95% CI) | ‐4.50 [‐15.66, 6.66] |
| 42 Quality of life: 2a. Specific (average endpoint score MSQOL, high = good) ‐ short term | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 42.1 Physcial health | 1 | 63 | Mean Difference (IV, Fixed, 95% CI) | 2.20 [‐7.81, 12.21] |
| 42.2 Vitality | 1 | 63 | Mean Difference (IV, Fixed, 95% CI) | 0.30 [‐9.80, 10.40] |
| 42.3 Psychosocial | 1 | 63 | Mean Difference (IV, Fixed, 95% CI) | 0.60 [‐10.25, 11.45] |
| 42.4 Material | 1 | 63 | Mean Difference (IV, Fixed, 95% CI) | 3.70 [‐6.79, 14.19] |
| 42.5 Spare time | 1 | 63 | Mean Difference (IV, Fixed, 95% CI) | 0.70 [‐12.73, 14.13] |
| 42.6 Affective | 1 | 63 | Mean Difference (IV, Fixed, 95% CI) | ‐5.90 [‐15.81, 4.01] |
| 43 Quality of life: 2b. Specific (average endpoint score MSQOL, high = good) ‐ medium term | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 43.1 Physical health | 1 | 64 | Mean Difference (IV, Fixed, 95% CI) | ‐5.0 [‐15.93, 5.93] |
| 43.2 Vitality | 1 | 64 | Mean Difference (IV, Fixed, 95% CI) | ‐7.20 [‐17.22, 2.82] |
| 43.3 Psychosocial | 1 | 64 | Mean Difference (IV, Fixed, 95% CI) | ‐7.10 [‐16.42, 2.22] |
| 43.4 Material | 1 | 64 | Mean Difference (IV, Fixed, 95% CI) | ‐3.40 [‐17.05, 10.25] |
| 43.5 Spare time | 1 | 64 | Mean Difference (IV, Fixed, 95% CI) | 5.70 [‐4.71, 16.11] |
| 43.6 Affective | 1 | 64 | Mean Difference (IV, Fixed, 95% CI) | ‐6.20 [‐15.76, 3.36] |
| 44 Satisfaction with treatment: 1. Leaving the study early | 26 | 2392 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.75, 0.99] |
| 45 Engagement with services: 1. Compliance with medication ‐ favourable compliance ‐ long term | 3 | 354 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.93, 1.11] |
| 46 Engagement with services: 2. Attitude to medication (average endpoint score, various scales, high = good) | 2 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 46.1 Attitude to Medication Questionnaire ‐ short term | 1 | 74 | Mean Difference (IV, Fixed, 95% CI) | 4.50 [2.17, 6.83] |
| 46.2 Drug Attitude Inventory ‐ short term | 1 | 63 | Mean Difference (IV, Fixed, 95% CI) | 5.70 [2.05, 9.35] |
| 46.3 Drug Attitude Inventory ‐ long term | 1 | 50 | Mean Difference (IV, Fixed, 95% CI) | ‐2.10 [‐6.11, 1.91] |
1.8. Analysis.
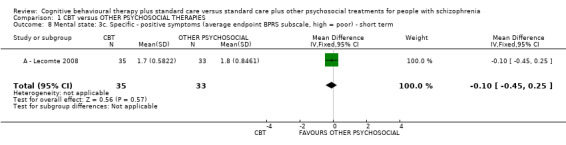
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 8 Mental state: 3c. Specific ‐ positive symptoms (average endpoint BPRS subscale, high = poor) ‐ short term.
1.14. Analysis.
Comparison 1 CBT versus OTHER PSYCHOSOCIAL THERAPIES, Outcome 14 Mental state: 6b. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) ‐ short term, skewed data.
| Mental state: 6b. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) ‐ short term, skewed data | |||||
|---|---|---|---|---|---|
| Study | Intervention | Mean | SD | N | Notes |
| A ‐ Levine 1998 | CBT | 7.8 | 4.0 | 6 | Reported favouring CBT |
| A ‐ Levine 1998 | Other treatments | 15.0 | 1.5 | 6 | |
Comparison 2. SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Global state: 1. Relapse | 4 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 Medium term | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.54, 1.78] |
| 1.2 Long term | 3 | 120 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.58, 1.78] |
| 2 Global state: 2. Rehospitalisation | 4 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 Long term | 4 | 527 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.71, 1.06] |
| 3 Mental state: 1. General ‐ clinically important change (no improvement) | 4 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Medium term | 2 | 133 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.91, 1.14] |
| 3.2 Long term | 3 | 158 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.77, 1.21] |
| 4 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor) | 7 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 4.1 Short term | 6 | 499 | Mean Difference (IV, Fixed, 95% CI) | ‐0.25 [‐1.09, 0.60] |
| 4.2 Medium term | 5 | 439 | Mean Difference (IV, Fixed, 95% CI) | ‐1.29 [‐2.21, ‐0.36] |
| 4.3 Long term | 5 | 371 | Mean Difference (IV, Fixed, 95% CI) | ‐2.10 [‐3.15, ‐1.05] |
| 5 Mental state: 4a. Specific ‐ hallucinations (average endpoint score PSRS, high = poor) | 1 | Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 5.1 Long term | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [‐4.76, 4.76] | |
| 6 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) | 5 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 Short term | 4 | 346 | Mean Difference (IV, Fixed, 95% CI) | ‐0.08 [‐1.04, 0.89] |
| 6.2 Medium term | 3 | 301 | Mean Difference (IV, Fixed, 95% CI) | ‐0.80 [‐1.92, 0.31] |
| 6.3 Long term | 4 | 317 | Mean Difference (IV, Fixed, 95% CI) | ‐1.34 [‐2.57, ‐0.11] |
| 7 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor) | 4 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 7.1 Short term | 3 | 165 | Mean Difference (IV, Fixed, 95% CI) | ‐4.90 [‐6.69, ‐3.11] |
| 7.2 Medium term | 2 | 136 | Mean Difference (IV, Fixed, 95% CI) | ‐1.68 [‐4.04, 0.69] |
| 7.3 Long term | 3 | 148 | Mean Difference (IV, Fixed, 95% CI) | ‐1.61 [‐3.65, 0.44] |
| 8 Adverse effect/event(s): 2. Death ‐ any cause | 3 | 302 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.19, 4.56] |
| 9 Functioning: 1b. Social functioning (average endpoint score SOFAS, high = good) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.1 Long term | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | 1.36 [‐9.59, 12.31] |
| 10 Functioning: 2a. Cognitive functioning ‐ insight (average endpoint score various scales, high = good) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.1 Schedule for assessment of insight ‐ long term | 1 | 168 | Mean Difference (IV, Fixed, 95% CI) | 1.55 [0.38, 2.72] |
| 11 Satisfaction with treatment: 1. Leaving the study early ‐ for any reason | 19 | 1779 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.72, 1.01] |
| 12 Engagement with services: 1. Compliance with medication ‐ favourable compliance ‐ long term | 1 | 198 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.99, 1.24] |
2.1. Analysis.
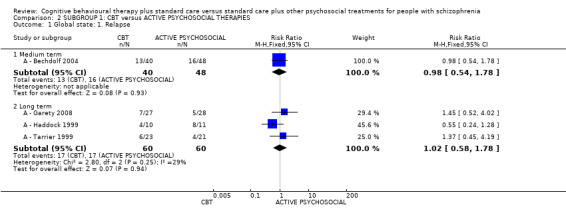
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 1 Global state: 1. Relapse.
2.2. Analysis.
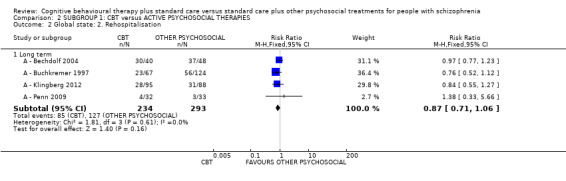
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 2 Global state: 2. Rehospitalisation.
2.3. Analysis.
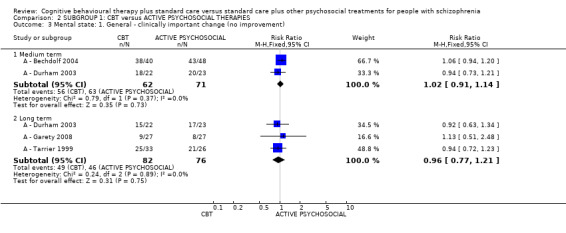
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 3 Mental state: 1. General ‐ clinically important change (no improvement).
2.4. Analysis.
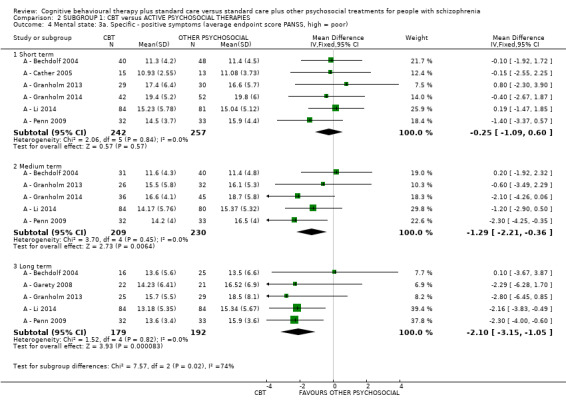
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 4 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor).
2.5. Analysis.
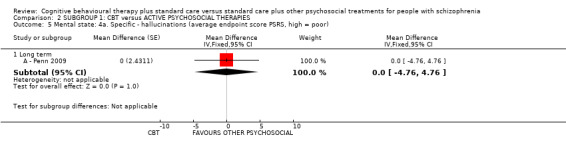
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 5 Mental state: 4a. Specific ‐ hallucinations (average endpoint score PSRS, high = poor).
2.6. Analysis.
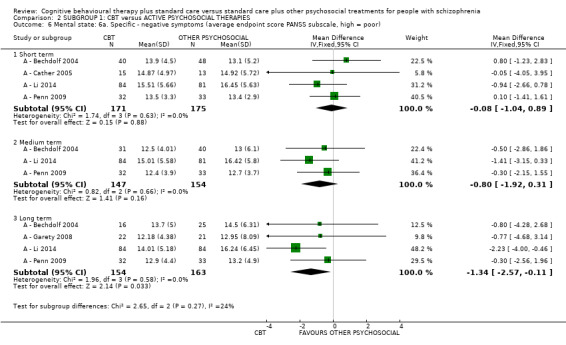
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 6 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor).
2.7. Analysis.
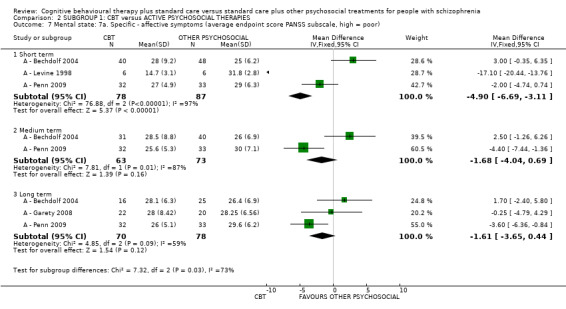
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 7 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor).
2.8. Analysis.
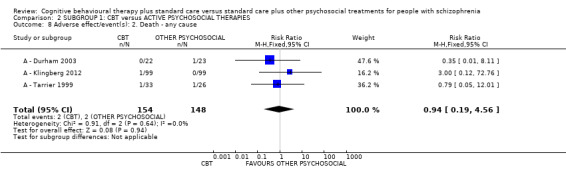
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 8 Adverse effect/event(s): 2. Death ‐ any cause.
2.9. Analysis.
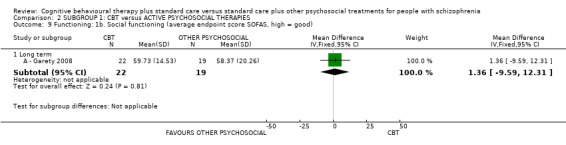
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 9 Functioning: 1b. Social functioning (average endpoint score SOFAS, high = good).
2.10. Analysis.
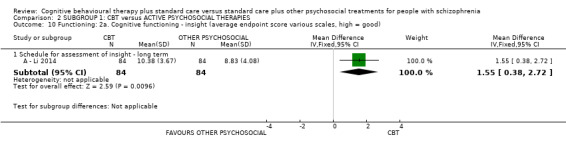
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 10 Functioning: 2a. Cognitive functioning ‐ insight (average endpoint score various scales, high = good).
2.11. Analysis.
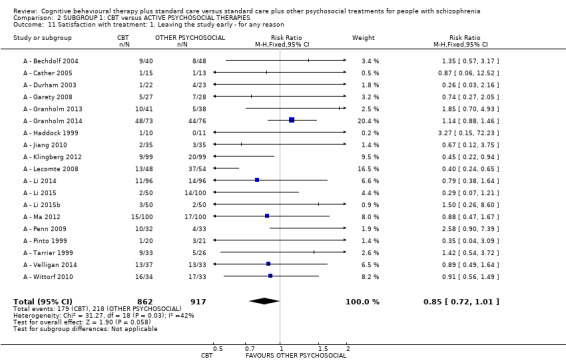
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 11 Satisfaction with treatment: 1. Leaving the study early ‐ for any reason.
2.12. Analysis.
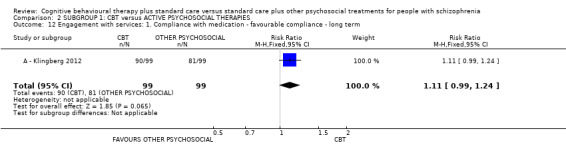
Comparison 2 SUBGROUP 1: CBT versus ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 12 Engagement with services: 1. Compliance with medication ‐ favourable compliance ‐ long term.
Comparison 3. SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Global state: 1. Relapse | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 Medium term | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.44 [0.14, 15.10] |
| 1.2 Long term | 2 | 255 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.85, 1.31] |
| 2 Global state: 2. Rehospitalisation | 4 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 Long term | 4 | 416 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.86, 1.52] |
| 3 Mental state: 1. General ‐ clinically important change (no improvement) | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 3.1 Medium term | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.53 [0.33, 0.86] |
| 3.2 Long term | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.60 [0.39, 0.94] |
| 4 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor) | 7 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 4.1 Short term | 4 | 384 | Mean Difference (IV, Fixed, 95% CI) | ‐0.93 [‐1.84, ‐0.03] |
| 4.2 Medium term | 1 | 58 | Mean Difference (IV, Fixed, 95% CI) | ‐0.80 [‐2.82, 1.22] |
| 4.3 Long term | 4 | 231 | Mean Difference (IV, Fixed, 95% CI) | ‐0.36 [‐1.40, 0.68] |
| 5 Mental state: 4a. Specific ‐ hallucinations (average endpoint score PSRS, high = poor) | 1 | Mean Difference (Fixed, 95% CI) | Subtotals only | |
| 5.1 Long term | 1 | Mean Difference (Fixed, 95% CI) | ‐4.36 [‐9.30, 0.58] | |
| 6 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) | 6 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 6.1 Short term | 3 | 235 | Mean Difference (IV, Fixed, 95% CI) | ‐0.07 [‐1.06, 0.91] |
| 6.2 Medium term | 1 | 58 | Mean Difference (IV, Fixed, 95% CI) | 0.04 [‐1.52, 1.60] |
| 6.3 Long term | 4 | 231 | Mean Difference (IV, Fixed, 95% CI) | ‐0.40 [‐1.54, 0.74] |
| 7 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor) | 6 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 7.1 Short term | 3 | 235 | Mean Difference (IV, Fixed, 95% CI) | ‐1.95 [‐3.68, ‐0.22] |
| 7.2 Medium term | 1 | 58 | Mean Difference (IV, Fixed, 95% CI) | 0.12 [‐2.71, 2.95] |
| 7.3 Long term | 4 | 231 | Mean Difference (IV, Fixed, 95% CI) | ‐0.44 [‐2.21, 1.34] |
| 8 Adverse effect/event(s): 2. Death ‐ any cause | 3 | 325 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.06 [0.63, 6.75] |
| 9 Functioning: 1b. Social functioning (average endpoint score SOFAS, high = good) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 9.1 Long term | 1 | 62 | Mean Difference (IV, Fixed, 95% CI) | 1.30 [‐6.26, 8.86] |
| 10 Functioning: 2a. Cognitive functioning ‐ insight (average endpoint score various scales, high = good) | 1 | Mean Difference (IV, Fixed, 95% CI) | Subtotals only | |
| 10.1 Schedule for assessment of insight ‐ long term | 1 | 50 | Mean Difference (IV, Fixed, 95% CI) | ‐0.5 [‐2.43, 1.43] |
| 11 Satisfaction with treatment: 1. Leaving the study early | 7 | 613 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.68, 1.15] |
| 12 Engagement with services: 1. Compliance with medication ‐ favourable compliance ‐ long term | 2 | 156 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.78, 1.03] |
3.1. Analysis.
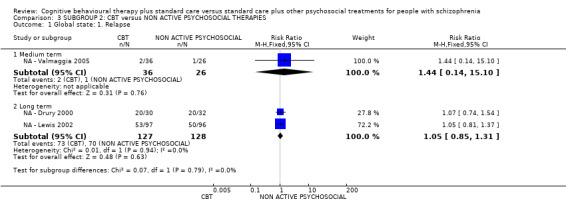
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 1 Global state: 1. Relapse.
3.2. Analysis.
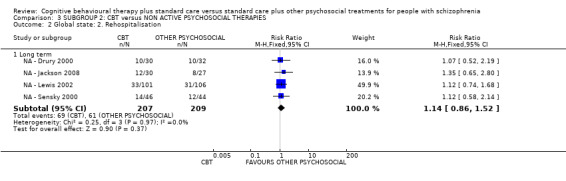
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 2 Global state: 2. Rehospitalisation.
3.3. Analysis.
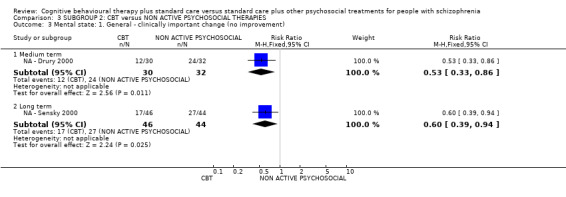
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 3 Mental state: 1. General ‐ clinically important change (no improvement).
3.4. Analysis.
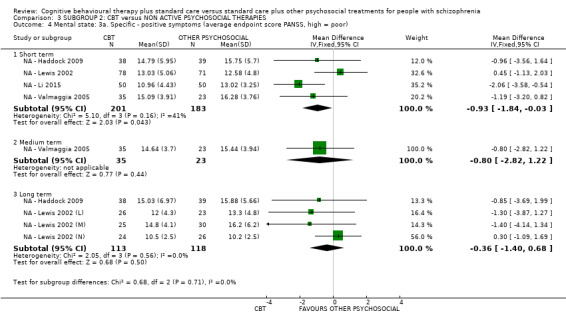
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 4 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor).
3.5. Analysis.
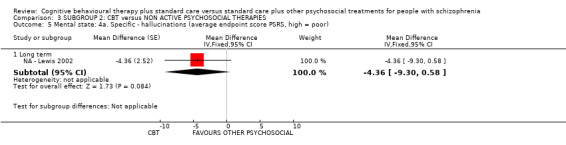
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 5 Mental state: 4a. Specific ‐ hallucinations (average endpoint score PSRS, high = poor).
3.6. Analysis.
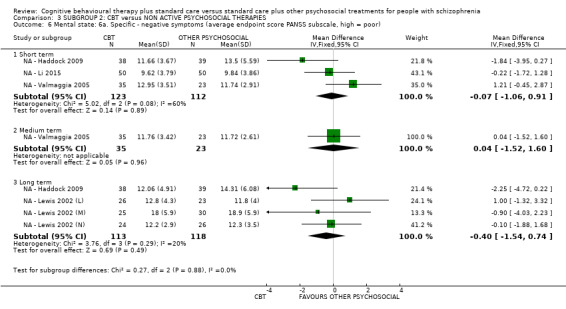
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 6 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor).
3.7. Analysis.
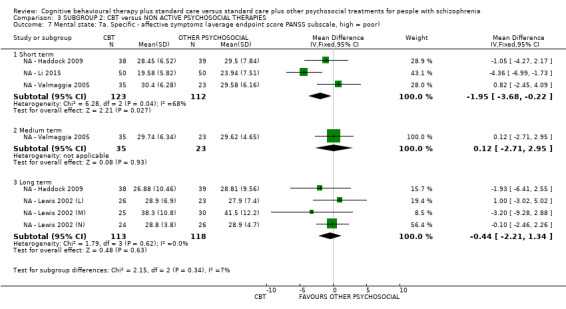
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 7 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor).
3.8. Analysis.
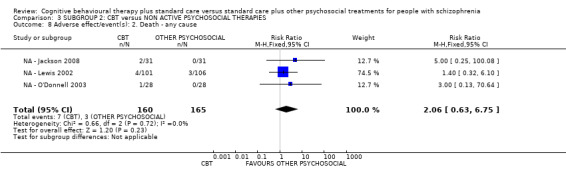
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 8 Adverse effect/event(s): 2. Death ‐ any cause.
3.9. Analysis.
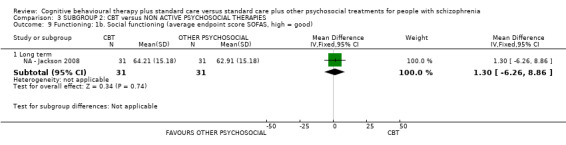
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 9 Functioning: 1b. Social functioning (average endpoint score SOFAS, high = good).
3.10. Analysis.
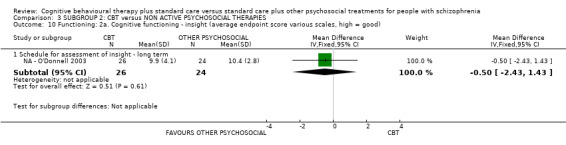
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 10 Functioning: 2a. Cognitive functioning ‐ insight (average endpoint score various scales, high = good).
3.11. Analysis.
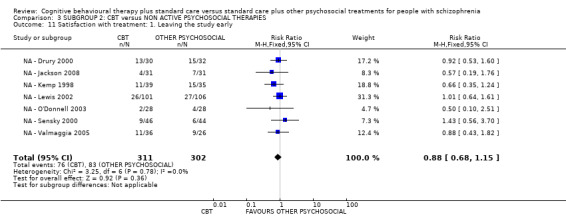
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 11 Satisfaction with treatment: 1. Leaving the study early.
3.12. Analysis.
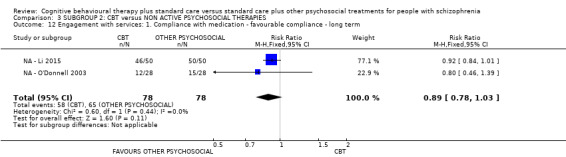
Comparison 3 SUBGROUP 2: CBT versus NON ACTIVE PSYCHOSOCIAL THERAPIES, Outcome 12 Engagement with services: 1. Compliance with medication ‐ favourable compliance ‐ long term.
Comparison 4. SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Global state: 1. Relapse ‐ medium term | 2 | 150 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.56, 1.81] |
| 1.1 Active | 1 | 88 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.98 [0.54, 1.78] |
| 1.2 Non active | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.44 [0.14, 15.10] |
| 2 Global state: 1. Relapse ‐ long term | 5 | 375 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.85, 1.29] |
| 2.1 Active | 3 | 120 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.58, 1.78] |
| 2.2 Non active | 2 | 255 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.85, 1.31] |
| 3 Global state: 2. Rehospitalisation ‐ long term | 8 | 943 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.82, 1.14] |
| 3.1 Active | 4 | 527 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.87 [0.71, 1.06] |
| 3.2 Non active | 4 | 416 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.14 [0.86, 1.52] |
| 4 Mental state: General ‐ clinically important change (no improvement) ‐ medium term | 3 | 195 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.77, 1.01] |
| 4.1 Active | 2 | 133 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.02 [0.91, 1.14] |
| 4.2 Non active | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.53 [0.33, 0.86] |
| 5 Mental state: General ‐ clinically important change (no improvement) ‐ long term | 4 | 248 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.83 [0.67, 1.03] |
| 5.1 Active | 3 | 158 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.96 [0.77, 1.21] |
| 5.2 Non active | 1 | 90 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.60 [0.39, 0.94] |
| 6 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor) ‐ short term | 6 | 998 | Mean Difference (IV, Fixed, 95% CI) | ‐0.25 [‐0.84, 0.35] |
| 6.1 Active | 6 | 499 | Mean Difference (IV, Fixed, 95% CI) | ‐0.25 [‐1.09, 0.60] |
| 6.2 Non active | 6 | 499 | Mean Difference (IV, Fixed, 95% CI) | ‐0.25 [‐1.09, 0.60] |
| 7 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor) ‐ medium term term | 6 | 497 | Mean Difference (IV, Fixed, 95% CI) | ‐1.20 [‐2.04, ‐0.36] |
| 7.1 Active | 5 | 439 | Mean Difference (IV, Fixed, 95% CI) | ‐1.29 [‐2.21, ‐0.36] |
| 7.2 Non Active | 1 | 58 | Mean Difference (IV, Fixed, 95% CI) | ‐0.80 [‐2.82, 1.22] |
| 8 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor) ‐ long term | 9 | 602 | Mean Difference (IV, Fixed, 95% CI) | ‐1.22 [‐1.96, ‐0.49] |
| 8.1 Active | 5 | 371 | Mean Difference (IV, Fixed, 95% CI) | ‐2.10 [‐3.15, ‐1.05] |
| 8.2 Non Active | 4 | 231 | Mean Difference (IV, Fixed, 95% CI) | ‐0.36 [‐1.40, 0.68] |
| 9 Mental state: 4a. Specific ‐ hallucinations (average endpoint score PSYRATS, high = poor) ‐ long term | 2 | Mean Difference (Fixed, 95% CI) | ‐2.10 [‐5.53, 1.33] | |
| 9.1 Active | 1 | Mean Difference (Fixed, 95% CI) | 0.0 [‐4.76, 4.76] | |
| 9.2 Non active | 1 | Mean Difference (Fixed, 95% CI) | ‐4.36 [‐9.30, 0.58] | |
| 10 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) ‐ short term | 7 | 581 | Mean Difference (IV, Fixed, 95% CI) | ‐0.07 [‐0.76, 0.61] |
| 10.1 Active | 4 | 346 | Mean Difference (IV, Fixed, 95% CI) | ‐0.08 [‐1.04, 0.89] |
| 10.2 Non active | 3 | 235 | Mean Difference (IV, Fixed, 95% CI) | ‐0.07 [‐1.06, 0.91] |
| 11 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) ‐ medium term | 4 | 359 | Mean Difference (IV, Fixed, 95% CI) | ‐0.52 [‐1.42, 0.39] |
| 11.1 Active | 3 | 301 | Mean Difference (IV, Fixed, 95% CI) | ‐0.80 [‐1.92, 0.31] |
| 11.2 Non active | 1 | 58 | Mean Difference (IV, Fixed, 95% CI) | 0.04 [‐1.52, 1.60] |
| 12 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) ‐ long term | 8 | 548 | Mean Difference (IV, Fixed, 95% CI) | ‐0.84 [‐1.67, 0.00] |
| 12.1 Active | 4 | 317 | Mean Difference (IV, Fixed, 95% CI) | ‐1.34 [‐2.57, ‐0.11] |
| 12.2 Non active | 4 | 231 | Mean Difference (IV, Fixed, 95% CI) | ‐0.40 [‐1.54, 0.74] |
| 13 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor) ‐ short term | 6 | 400 | Mean Difference (IV, Fixed, 95% CI) | ‐3.38 [‐4.62, ‐2.13] |
| 13.1 Active | 3 | 165 | Mean Difference (IV, Fixed, 95% CI) | ‐4.90 [‐6.69, ‐3.11] |
| 13.2 Non active | 3 | 235 | Mean Difference (IV, Fixed, 95% CI) | ‐1.95 [‐3.68, ‐0.22] |
| 14 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor) ‐ medium term | 3 | 194 | Mean Difference (IV, Fixed, 95% CI) | ‐0.94 [‐2.75, 0.88] |
| 14.1 Active | 2 | 136 | Mean Difference (IV, Fixed, 95% CI) | ‐1.68 [‐4.04, 0.69] |
| 14.2 Non active | 1 | 58 | Mean Difference (IV, Fixed, 95% CI) | 0.12 [‐2.71, 2.95] |
| 15 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor) ‐ long term | 7 | 379 | Mean Difference (IV, Fixed, 95% CI) | ‐0.94 [‐2.28, 0.40] |
| 15.1 Active | 3 | 148 | Mean Difference (IV, Fixed, 95% CI) | ‐1.61 [‐3.65, 0.44] |
| 15.2 Non active | 4 | 231 | Mean Difference (IV, Fixed, 95% CI) | ‐0.44 [‐2.21, 1.34] |
| 16 Adverse effects: 1b. Adverse effect/event(s) ‐ death | 6 | 627 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.57 [0.62, 3.98] |
| 16.1 Active | 3 | 302 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.94 [0.19, 4.56] |
| 16.2 Non active | 3 | 325 | Risk Ratio (M‐H, Fixed, 95% CI) | 2.06 [0.63, 6.75] |
| 17 Functioning: 1b. Social functioning (average endpoint score SOFAS, high = good) ‐ long term | 2 | 103 | Mean Difference (IV, Fixed, 95% CI) | 1.32 [‐4.90, 7.54] |
| 17.1 Active | 1 | 41 | Mean Difference (IV, Fixed, 95% CI) | 1.36 [‐9.59, 12.31] |
| 17.2 Non active | 1 | 62 | Mean Difference (IV, Fixed, 95% CI) | 1.30 [‐6.26, 8.86] |
| 18 Functioning: 2a. Cognitive functioning ‐ insight (average endpoint score SAI, high = good) ‐ long term | 2 | 218 | Mean Difference (IV, Fixed, 95% CI) | 1.00 [‐0.01, 2.00] |
| 18.1 Active | 1 | 168 | Mean Difference (IV, Fixed, 95% CI) | 1.55 [0.38, 2.72] |
| 18.2 Non active | 1 | 50 | Mean Difference (IV, Fixed, 95% CI) | ‐0.5 [‐2.43, 1.43] |
| 19 Satisfaction with treatment: 1. Leaving the study early | 26 | 2392 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.75, 0.99] |
| 19.1 Active | 19 | 1779 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.85 [0.72, 1.01] |
| 19.2 Non active | 7 | 613 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.88 [0.68, 1.15] |
| 20 Engagement with services: 1. Compliance with medication ‐ favourable compliance ‐ long term | 3 | 354 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.93, 1.11] |
| 20.1 Active | 1 | 198 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.11 [0.99, 1.24] |
| 20.2 Non active | 2 | 156 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.89 [0.78, 1.03] |
4.1. Analysis.
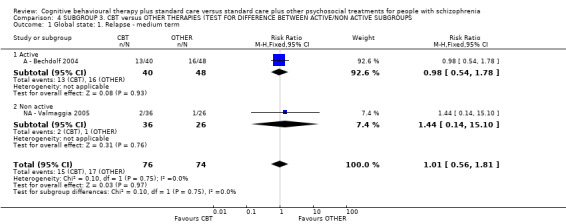
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 1 Global state: 1. Relapse ‐ medium term.
4.2. Analysis.
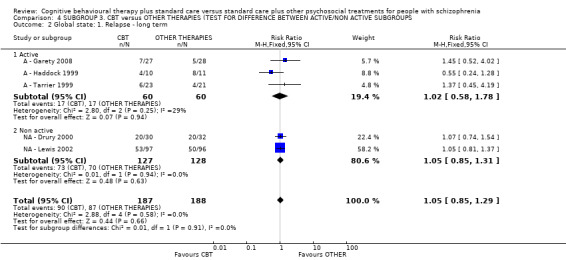
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 2 Global state: 1. Relapse ‐ long term.
4.3. Analysis.
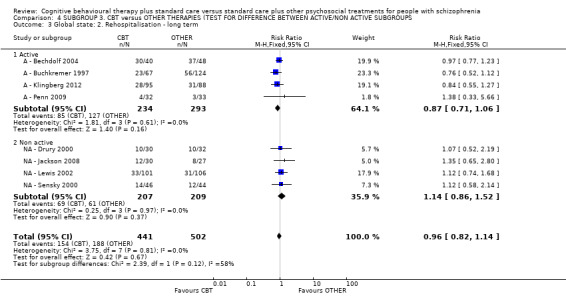
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 3 Global state: 2. Rehospitalisation ‐ long term.
4.6. Analysis.
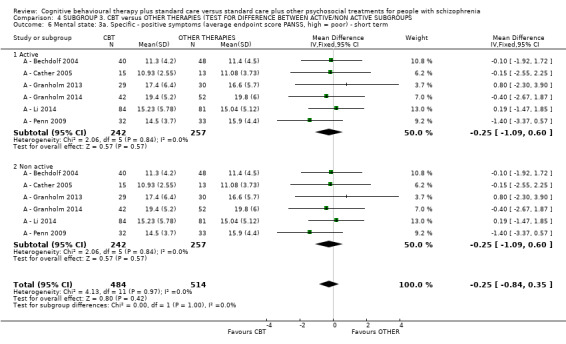
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 6 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor) ‐ short term.
4.7. Analysis.
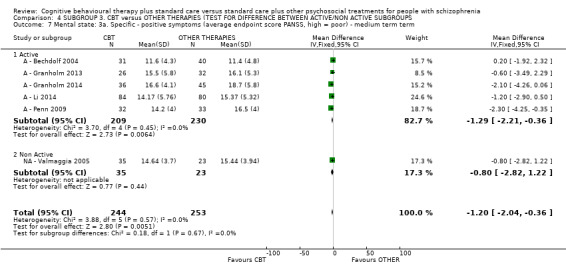
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 7 Mental state: 3a. Specific ‐ positive symptoms (average endpoint score PANSS, high = poor) ‐ medium term term.
4.9. Analysis.
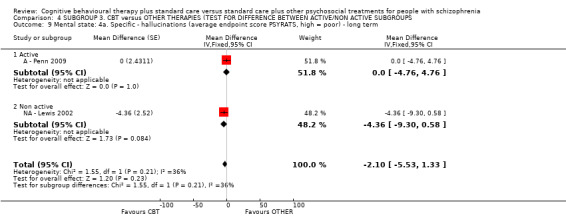
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 9 Mental state: 4a. Specific ‐ hallucinations (average endpoint score PSYRATS, high = poor) ‐ long term.
4.10. Analysis.
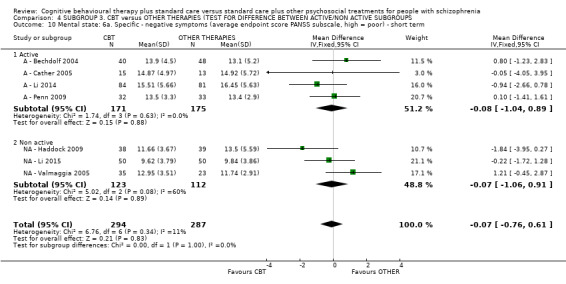
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 10 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) ‐ short term.
4.11. Analysis.
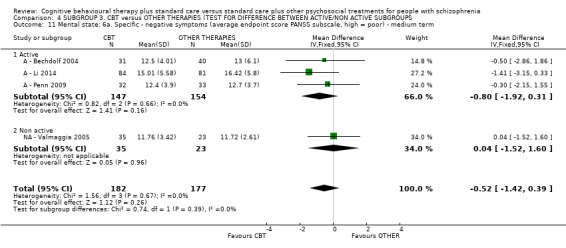
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 11 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) ‐ medium term.
4.12. Analysis.
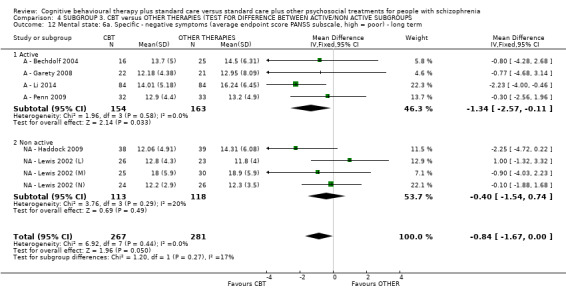
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 12 Mental state: 6a. Specific ‐ negative symptoms (average endpoint score PANSS subscale, high = poor) ‐ long term.
4.14. Analysis.
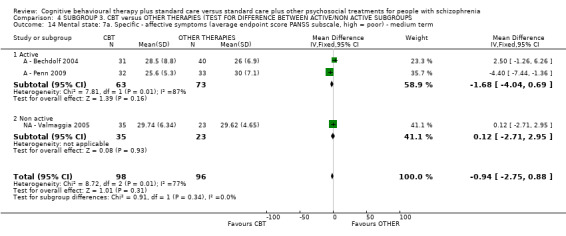
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 14 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor) ‐ medium term.
4.15. Analysis.
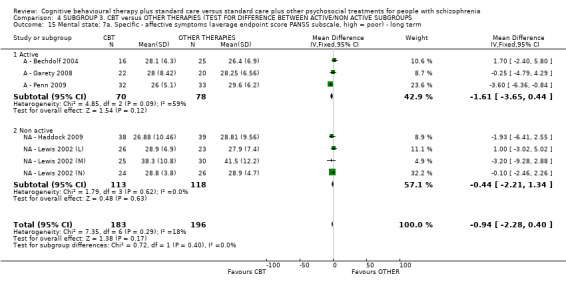
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 15 Mental state: 7a. Specific ‐ affective symptoms (average endpoint score PANSS subscale, high = poor) ‐ long term.
4.16. Analysis.
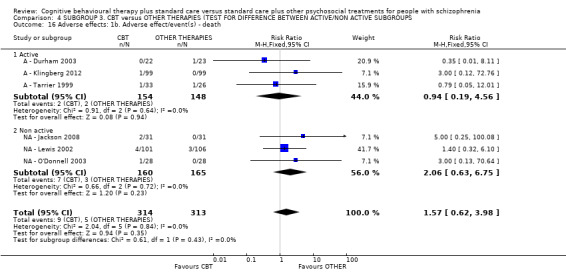
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 16 Adverse effects: 1b. Adverse effect/event(s) ‐ death.
4.17. Analysis.
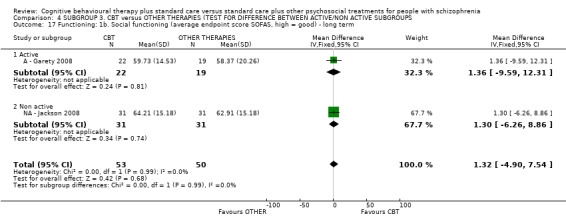
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 17 Functioning: 1b. Social functioning (average endpoint score SOFAS, high = good) ‐ long term.
4.18. Analysis.
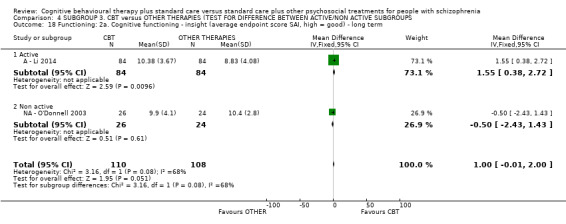
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 18 Functioning: 2a. Cognitive functioning ‐ insight (average endpoint score SAI, high = good) ‐ long term.
4.19. Analysis.
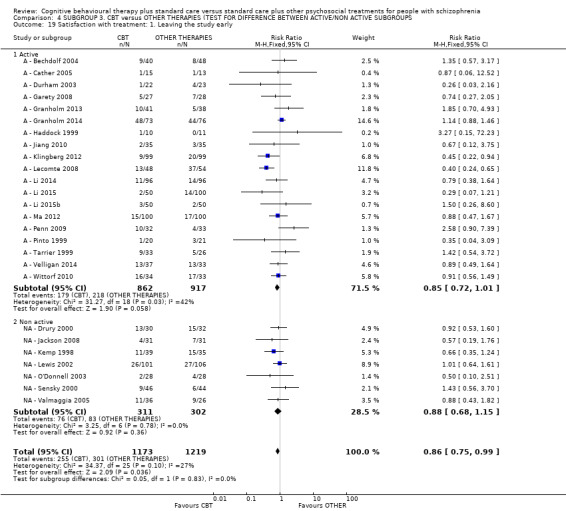
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 19 Satisfaction with treatment: 1. Leaving the study early.
4.20. Analysis.
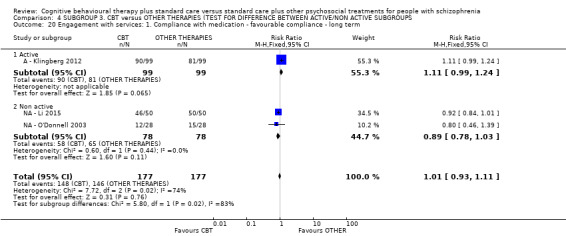
Comparison 4 SUBGROUP 3. CBT versus OTHER THERAPIES (TEST FOR DIFFERENCE BETWEEN ACTIVE/NON ACTIVE SUBGROUPS, Outcome 20 Engagement with services: 1. Compliance with medication ‐ favourable compliance ‐ long term.
Comparison 5. SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (LESS‐WELL‐DESIGNED CBT).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Global state: 1. Relapse ‐ long term | 5 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 with less‐well‐designed CBT | 5 | 375 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.85, 1.29] |
| 1.2 without less‐well‐designed CBT | 4 | 331 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.03 [0.84, 1.27] |
| 2 Mental state: 1. General ‐ clinically important change (no improvement) ‐ short term | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2.1 with less‐well‐designed CBT | 2 | 87 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.58, 0.99] |
| 2.2 without less‐well‐designed CBT | 1 | 28 | Risk Ratio (M‐H, Random, 95% CI) | 0.58 [0.28, 1.18] |
| 3 Mental state: 1. General ‐ clinically important change (no improvement) ‐ medium term | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 3.1 with less‐well‐designed CBT | 3 | 195 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.58, 1.23] |
| 3.2 without less‐well‐designed CBT | 2 | 150 | Risk Ratio (M‐H, Random, 95% CI) | 0.77 [0.29, 2.01] |
| 4 Mental state: 1. General ‐ clinically important change (no improvement) ‐ long term | 4 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 4.1 with less‐well‐designed CBT | 4 | 249 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.67, 1.01] |
| 4.2 without less‐well‐designed CBT | 2 | 145 | Risk Ratio (M‐H, Random, 95% CI) | 0.72 [0.44, 1.20] |
Comparison 6. SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (UNCLEAR EXPERIENCED THERAPISTS).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Global state: 1. Relapse ‐ long term | 5 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 with unclear experienced therapist | 5 | 375 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.85, 1.29] |
| 1.2 without unclear experienced therapist | 4 | 313 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.04 [0.82, 1.33] |
| 2 Mental state: 1. General ‐ clinically important change (no improvement) ‐ medium term | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 2.1 with unclear experienced therapist | 3 | 195 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.58, 1.23] |
| 2.2 without unclear experienced therapist | 2 | 133 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.85, 1.18] |
Comparison 7. SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (ASSUMPTION FOR MISSING DATA).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Global state: 1. Relapse ‐ medium term | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 with assumption | 2 | 150 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.56, 1.81] |
| 1.2 without assumption | 2 | 133 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.76 [0.28, 2.04] |
| 2 Global state: 1. Relapse ‐ long term | 5 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 with assumption | 5 | 375 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.85, 1.29] |
| 2.2 without assumption | 5 | 373 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.86, 1.29] |
| 3 Mental state: 1. General ‐ clinically important change (no improvement) ‐ medium term | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 3.1 with assumption | 3 | 195 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.58, 1.23] |
| 3.2 without assumption | 3 | 174 | Risk Ratio (M‐H, Random, 95% CI) | 0.85 [0.58, 1.24] |
| 4 Mental state: 1. General ‐ clinically important change (no improvement) ‐ long term | 4 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 4.1 with assumption | 4 | 249 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.67, 1.01] |
| 4.2 without assumption | 4 | 229 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.66, 1.05] |
Comparison 8. SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (RISK OF BIAS).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Global state: 1. Relapse ‐ medium term | 2 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 1.1 with high risk of bias studies | 2 | 150 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.01 [0.56, 1.81] |
| 1.2 without high risk of bias studies | 1 | 62 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.44 [0.14, 15.10] |
| 2 Global state: 1. Relapse ‐ long term | 5 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 2.1 with high risk of bias studies | 5 | 375 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.85, 1.29] |
| 2.2 without high risk of bias studies | 1 | 193 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.05 [0.81, 1.37] |
| 3 Mental state: 1. General ‐ clinically important change (no improvement) ‐ short term | 2 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 3.1 with high risk of bias studies | 2 | 87 | Risk Ratio (M‐H, Random, 95% CI) | 0.75 [0.58, 0.99] |
| 3.2 without high risk of bias studies | 1 | 28 | Risk Ratio (M‐H, Random, 95% CI) | 0.58 [0.28, 1.18] |
| 4 Mental state: 1. General ‐ clinically important change (no improvement) ‐ medium term | 3 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 4.1 with high risk of bias studies | 3 | 195 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.58, 1.23] |
| 4.2 without high risk of bias studies | 1 | 45 | Risk Ratio (M‐H, Random, 95% CI) | 0.90 [0.71, 1.13] |
| 5 Mental state: 1. General ‐ clinically important change (no improvement) ‐ long term | 4 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 5.1 with high risk of bias studies | 4 | 249 | Risk Ratio (M‐H, Random, 95% CI) | 0.82 [0.67, 1.01] |
| 5.2 without high risk of bias studies | 1 | 45 | Risk Ratio (M‐H, Random, 95% CI) | 0.78 [0.57, 1.09] |
Comparison 9. SENSITIVITY ANALYSIS: CBT versus OTHER PSYCHOSOCIAL THERAPIES (RANDOM EFFECT MODEL).
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Global state: 1. Relapse (random effect model) | 7 | Risk Ratio (M‐H, Random, 95% CI) | Subtotals only | |
| 1.1 Short term | 1 | 62 | Risk Ratio (M‐H, Random, 95% CI) | 0.72 [0.05, 11.02] |
| 1.2 Medium term | 2 | 150 | Risk Ratio (M‐H, Random, 95% CI) | 1.00 [0.56, 1.79] |
| 1.3 Long term | 5 | 375 | Risk Ratio (M‐H, Random, 95% CI) | 1.04 [0.85, 1.27] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
A ‐ Bechdolf 2004.
| Methods | Allocation: randomised.
Blinding: not reported. Location: inpatient, Germany. Length of follow‐up: after treatment, 6 months, 24 months. (p.145). |
|
| Participants | Diagnosis: episode of schizophrenia, schizoaffective or other psychotic disorder (ICD‐10). N = 88. Sex: 40M, 48F. Age: mean ˜ 32.2 years, SD ˜ 9.9 years. History: length of illness: mean ˜ 56.7months, SD ˜ 65.4 months. Excluded: primary diagnosis of drug or alcohol dependence, organic brain disease, learning disability or hearing impairment. |
|
| Interventions | 1. CBT plus standard care: N = 40. Content: the group CBT treatment was based on the approach by Tarrie and colleagues (Tarrier 1993a), who used coping strategy enhancement, problem‐solving and relapse prevention in patients with psychosis. Delivered by: two therapists: an experienced and CBT‐trained psychiatrist and a clinical psychologist. Frequency: the intervention included 16 sessions in 8 weeks. Sessions followed a semi‐structured format and lasted between 60 and 90 minutes, interrupted by a 5‐ to 10‐minute break. 2. Psychoeducation group: N = 48. Content: the PE programme was developed by Hornung and colleagues (Hornung 1996; Hornung 1999). It covered the following topics: symptoms of psychosis, models of psychosis, effects and side effects of medication, maintenance medication, early symptoms of relapse, relapse prevention. The approach was primarily didactic and included the following strategies: formulation, guided discovery and motivational interviewing. Frequency: the programme included eight sessions in 8 weeks. Sessions followed a semi‐structured format and lasted between 60 and 90 minutes, occasionally interrupted by a 5‐ to 10‐minute break. Treatment duration: 8 weeks. All interventions were an adjunct to routine hospital care and patients remained under the medical supervision of the responsible consultant psychiatrist. |
|
| Outcomes | Global state: relapse (rating > 5 also 2‐point increase on previous assessment in > 1 item of positive syndrome sub‐scale of PANSS); rehospitalisation (36‐hour full hospitalisation or 5‐day partial hospitalisation because of exacerbation of acute psychotic symptoms). Mental state: clinically significant change*, PANSS. Quality of life: physical health (the Modular System for Quality of Life,MsQoL), vitality (MsQoL), Material QOL (MsQoL), Spare time QOL (MsQoL), Affective QoL (MsQoL), general QoL (MsQoL). Satisfaction with treatment: leaving the study early. Unable to use ‐ Engagement with services: compliance with medication (4‐point rating scale was not peer‐reviewed). |
|
| Notes | * Defined as (i) improvement of PANSS global score >2 SD beyond the mean of the intake sample at follow‐up and (ii) reliable change index (RCI) exceeds 1.96. RCI was calculated by dividing the absolute magnitude of change by the SE of the change score (follow‐up minus pretest) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was conducted by computer‐generated random numbers for blocks of eight participants…The results were placed in sealed envelopes and opened at the time of treatment allocation." (p.145). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | High risk | Quote: "Randomization was conducted by computer‐generated random numbers for blocks of eight participants…The results were placed in sealed envelopes and opened at the time of treatment allocation." (p.145). Comments: participants and investigators enrolling participants could foresee assignment because the allocation assignment was opened before treatment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of outcome assessor. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "In the CBT group 9/40 subjects (22.5%) and in the PE group 8/48 patients (16.7%) were lost to follow up." (p.146). Comments: missing outcome data balanced in numbers across intervention groups. |
| Selective reporting (reporting bias) | Low risk | Comments: the author did not report the outcome ‐ compliance with medication. |
| Other bias | Low risk | Comments: this work was supported by grant from the Koln Fortune Program; other bias was not obvious. |
A ‐ Buchkremer 1997.
| Methods | Allocation: randomised.
Blinding: maybe non‐blind. Location: outpatients, nine psychiatric hospitals in Germany. Length of follow‐up: 8 months, 12 months, and 24 months. |
|
| Participants | Diagnosis: schizophrenia (DSM‐III‐R).
N = 191. Sex: 111M, 80F. Age: mean ˜31.3 years, SD ˜7 years. History: length of illness mean 22.9 years, SD 5.8 years. I. schizophrenia diagnosed according to DSM‐III‐R 295 with the exception of 295.7 (exclusion of schizoaffective disturbances); II. at least two acute psychotic episodes within the past 5 years; III. at least 4 weeks of psychopathological stabilisation; IV. indication for long‐term neuroleptic medication on an out‐patient basis; V. no secondary psychiatric diagnosis. Excluded not reported. |
|
| Interventions | 1. CBT group: N = 34. Content: psychoeducational medication management training + cognitive psychotherapy*. Delivered by: not reported. Frequency: 10 sessions of psychoeducational training plus unknown sessions of cognitive psychotherapy. 2. Intergrated CBT group: N = 33. Content: psychoeducational medication management training** + cognitive therapy + key person counselling. Delivered by: not reported. Frequency: 10 sessions of psychoeducational training plus 20 sessions of key‐person counselling***. The author did not report the number of sessions of cognitive therapy. 3. Psychoeducation group: N = 32. Content: psychoeducational medication training. Content: improving knowledge of schizophrenia and its treatment, promoting medication and crisis‐management skills. Delivered by: not reported. Frequency: five weekly sessions following with five 14‐day‐interval sessions. 4. Intergrated psychoeducation group: N = 35. Content: psychoeducational medication training + key person counselling. Delivered by: not reported. Frequency: 10 sessions of psychoeducational training plus 20 sessions of key‐person counselling. 5. Non active control group: N = 57. Content: structured free‐time activity. Content: regular leisure‐time activities. Delivered by: students of psychology or educational sociology. Frequency: not reported. Treatment duration: 8 months. |
|
| Outcomes | Global state: rehospitalisation****. Unable to use ‐ Global state: SCPI, MPS (data not reported by individual groups). Mental state: BPRS, SANS (data not reported by individual groups), IRA (data not reported by individual groups). Global state: GAS (data not reported by individual groups). Satisfaction with treatment: leaving the study early (data not reported by individual groups). |
|
| Notes | * Cognitive psychotherapy ‐ designed to mediate problem‐solving skills and to improve coping strategies. Structured coping with stress situations (definition of a problem, setting of goals and systematic selection of steps towards attainment of goals) and more adequate coping with everyday stress were to be learned as a means of reducing general stress levels. ** Psychoeducational medication training (PMT) ‐ individualised information about schizophrenia and its treatment, patients trained to recognise and react to early signs of relapse. *** Key‐person counselling (KC) ‐ targeted at relatives/care‐givers ‐ given information about schizophrenia and its treatment, and recognition of impending relapses discussed, together with coping strategies, dealing with day‐to‐day problems involved in living with schizophrenia, aimed to transfer to self‐help group. **** Data are presented for two CBT groups (Groups 1 and 2, see above) and two other psychological therapy groups (groups 3 and 4, see above). Data were pooled for this outcome. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "At each location the structural homogeneity of the treatment groups was ensured by applying a randomisation technique in which the prognostic factors...were balanced by preliminary matching." (p.3). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomization was carried out by an independent institution..."(p.3). Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Quote: "Data recorded by trained project staff who were not blind with respect to the group of allocation." (p.3). Comments: the outcome assessor was not blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: modified intention‐to‐treat approach all who attended > 1 group session included in main analysis. |
| Selective reporting (reporting bias) | High risk | Comments: data for BPRS, SANS, GAS and others were reported by individual groups only. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Cather 2005.
| Methods | Allocation: randomised.
Blinding: maybe single‐blind. Location: two sites in Boston, USA. Length of follow‐up: 16 weeks. |
|
| Participants | Diagnosis: schizophrenia (61%) or schizoaffective disorder (39%).
N = 30. Sex: 18M, 12F. Age: 18 ‐ 65 years (mean 40.4 years, SD 11.96 years). History: length of illness: mean 18 years, SD 13 years, English speaking, treated with olanzapine for > 6 months and at stable dose > 30 days, and exhibiting residual psychotic symptoms. Excluded: evidence of organic brain disorder, recent substance use disorder , a conceptual disorganisation rating on the PANSS of moderate or higher, or previous exposure to CBT. |
|
| Interventions | 1. CBT group: N = 15. Content: inclusive of cognitive restructuring, goal setting and coping strategy enhancement, with focus on addressing specific functional goals in relation to social and occupational functioning. Delivered by: nine therapists with an average of 7.8 years of experience conducting CBT. Frequency: weekly 1‐hour individual sessions for 16 weeks 2. Psychoeducation group: N = 13. Content: supportive elements of therapy and psychoeducation in a manualised intervention delivered by experienced therapists. Frequency: weekly 1‐hour individual sessions for 16 weeks. Treatment duration: 16 weeks. |
|
| Outcomes | Mental state: general ‐ clinically important change*, PANSS positive/negative***, hallucinations (PSYRATS), delusions (PSYRATS). Satisfaction with treatment: leaving the study early. Unable to use ‐ Global state: average endpoint score in social functioning: SFS.** Mental state: PANSS dysphoria scale: no standard scoring of the general psychopathology scale. |
|
| Notes | *Defined as a reduction in PANSS positive factor score from pre‐ to post‐ treatment less than 20%. ** SFS is designed to assess functioning over the past 3 months. In this study it was used to assess functioning over a one‐week period. Accordingly, this non‐standard use of the SFS invalidates comparison with other studies. *** This study is unclear whether the negative and positive sub scales of the PANSS were scored using standard scoring procedures. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomised ‐ stratified by severity of symptoms (PANNS < 63) and gender ‐ no further details." (p.203). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "Allocation carried out by an "independent member of the research team" (p.203). Comments: participants and investigators enrolling participants could not foresee assignment because the randomisation was conducted by an independent member. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comments: rater blind to allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "of the two participants (1 in CBT and 1 in PE) received fewer than four sessions and were considered drop‐outs and excluded from the analyses. Attrition rates did not differ significantly between the fCBT(6%) and PE(7%) groups." (p.203). Comments: missing outcome data balanced in numbers across intervention groups. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but there is no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Durham 2003.
| Methods | Allocation: randomised.
Blinding: maybe single‐blind. Location: two adjacent mental health services in Tayside and Fife (Scotland). Length of follow‐up: 9 month, 12 months. |
|
| Participants | Diagnosis: schizophrenia, schizoaffective and delusional disorder (ICD‐10 and DSM ‐IV).
N = 66. Sex: 45M, 21F. Age: mean ˜ 36 years. History: length of illness: mean ˜ 13 years. Psychosis and a diagnosis of schizophrenia, schizoaffective disorder or delusional disorder, affective disorder or delusional disorder aged 16–65 years who are known to the psychiatric services as having persistent and distressing positive symptoms of hallucinations or delusions, or both, and who have been stabilised on anti‐psychotic medication for at least a 6‐month period medication under the care of a consultant psychiatrist. Excluded: primary diagnosis of alcoholism or drug misuse, evidence of organic brain disease and history of violence. |
|
| Interventions | 1. CBT group: N = 22. Content: individual CBT + standard care. Delivered by: five clinical nurse specialists with extensive five clinical nurse specialists with extensive professional experience of severe mental professional experience of severe mental disorder. Frequency: a maximum of 20 therapy sessions of approximately half an hour in length of approximately half an hour in length over a 9‐month period. 2. Supportive psychotherapy group: N = 23. Content: individual psychotherapy + standard care. Delivered by: not reported. Frequency: a maximum of 20 therapy sessions of approximately half an hour in length of approximately half an hour in length over a 9‐month period 3. Standard care group: N = 21. Content: routine care, case management & medication. Delivered by: not reported. Frequency: a maximum of 20 therapy sessions of approximately half an hour in length of approximately half an hour in length over a 9‐month period Treatment duration: 9 months. |
|
| Outcomes | Global state: GAS.
Mental state: clinically important change ‐ no improvement*, PANSS, PSYRATS (skewed data). Adverse effect/event: death. Satisfaction with treatment: leaving the study early. |
|
| Notes | * Defined as the decrease rate of PANSS score < 25%. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The randomisation procedure (sealed envelope technique) was devised by the project statistician (Cathy Hau) and project statistician (Cathy Hau) and administered centrally by the non‐clinical administered centrally. It was carried out separately within each treatment centre using randomised permuted blocking. " (p.303). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "...administered centrally by the non‐clinical project coordinator...."(p.303) Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Organisation and administration of the work of the independent assessors and therapists were kept strictly separate in order to maintain the blindness of the assessor. (p.304). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: analyses repeated with missing values replaced either with previous values carried forward or with group means, and the same pattern of significance was found. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Garety 2008.
| Methods | Allocation: randomised.
Blinding: single‐blind.
Location: five local mental health services in London. Length of follow‐up: 3, 6, 12, and 24 months. |
|
| Participants | Diagnosis: non‐affective psychosis (ICD‐10 and DSM‐IV) with at least one positive symptom of moderate severity on the PANSS.
N = 301* Sex: 211M, 90F. Age: mean ˜37.1 years, SD ˜10.9 years. History: length of illness: ˜9.9 years, SD ˜ 8.7 years. 1. Current diagnosis of psychosis; 2. Non‐affective (International Statistical Classification of Diseases and Related Health Problems, Tenth edition [ICD‐10], F20); 3. Age 18 to 65 years; 4. Second or subsequent episode, which started not more than three months before entry; 5. Rated at least four (moderate severity) on the PANSS on at least one positive psychotic symptom. Excluded criteria were: primary diagnosis of alcoholism or drug misuse, evidence of alcoholism or drug misuse, evidence of organic brain disease and history of organic brain disease and history of violence. |
|
| Interventions | Pathway 1 (participants without carers) 1. CBT group: N = 106. Content: CBT + standard care. Targeted at relapse prevention, done by exploring people's understanding of triggers and risks of relapse and by developing new model of disorder emphasising alternatives to delusional thinking, targets often included persistent negative beliefs about self and others, characteristic reasoning styles such as jumping to conclusions and distressing emotional reactions to events and anomalous experiences; administered by skilled practitioners (doctorial level clinical psychologists) and treatment fidelity assessed using the Cognitive Therapy for Psychosis Adherence Scale. Delivered by: five clinical nurse specialists with extensive five clinical nurse specialists with extensive professional experience of severe mental professional experience of severe mental disorder. Frequency: 12 to 20 sessions within 9 months. 2. Standard care group: N = 112. Treatment duration: 9 months. Pathway 2 (participants with carers) 3. CBT group: N = 27. Content: targeted at relapse prevention, done by exploring people's understanding of triggers and risks of relapse and by developing new model of disorder emphasising alternatives to delusional thinking, targets often included persistent negative beliefs about self and others, characteristic reasoning styles such as jumping to conclusions and distressing emotional reactions to events and anomalous experiences; administered by skilled practitioners (doctorial level clinical psychologists) and treatment fidelity assessed using the Cognitive Therapy for Psychosis Adherence Scale. Delivered by: five clinical nurse specialists with extensive five clinical nurse specialists with extensive professional experience of severe mental professional experience of severe mental disorder. Frequency: 12 to 20 sessions within 9 months. 4. Family intervention group: N = 28. Content: emphasis on improving communication, offering discussion of up‐to‐date information about psychosis, problem‐solving, reducing criticism and conflict, improving activity, and emotional processing of grief, loss and anger. Delivered by: 16 mental health professionals. Frequency: not reported. 5. Standard care group: (N = 28). Treatment duration: 9 months. |
|
| Outcomes | Global state: relapse***. Mental state: clinically important change ‐ no improvement**, PANSS, BDI (skewed data), BAI (skewed data). Functioning: Social and occupational functioning (SOFAS). Quality of life: European Quality of life measure (EuroQoL). Satisfaction with treatment: leaving the study early. Unable to use ‐ Mental state: specific symptoms ‐ PSYRATS (trial did not report the score on delusion and hallucination) |
|
| Notes | * Only used data derived from the CBT group and family intervention group for Pathway 2 (the participants with carers). N = 55. ** Number of participants did not experience partial or full remission. *** Defined as the number of participants relapse after partial or full remission from initial episode. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "...using randomised permuted blocks with a block size randomly varying between two and ten for the no carer pathway and three and nine for the carer pathway..."(p.413). Comments: the investigators described a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomisation schedules were independently generated by a trial randomisation service in a separate location from all trial centres.." (p.413). Comments:participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Trial research assessors were independent of treatment delivery and every effort was made to ensure they were kept masked to allocation." (p.415). Comments: participants and therapists knew the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Trial research assessors were independent of treatment delivery and every effort was made to ensure they were kept masked to allocation." (p.415). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: intention‐to‐treat analysis was undertaken. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Granholm 2013.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: outpatient residential and treatment settings, San Diego, USA. Length of follow‐up: 4.5, 9, 13.5 and 18‐ months. |
|
| Participants | Diagnosis: schizophrenia or schizoaffective disorder (SCID‐I).
N = 79. Sex: 44 M , 35 F. Age: mean 55 years, SD 6.6 years. History: schizophrenia or schizoaffective disorder based on the Structured Clinical Interview for the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (SCID‐I). Excluded: prior exposure to CBT during the previous five years, level of care required at baseline that would interfere outpatient therapy groups (e.g. hospitalisations for medical, psychiatric, or substance abuse problems), or disabling medical problems that would interfere with therapy or testing. |
|
| Interventions | 1. Group CBT group: N = 41. Content: group based intervention included thought Challenging, Social Skills Training, and Problem‐Solving Training. Cognitive therapy was combined with role‐play practice of communication skills and problem‐solving training Delivered by: two doctoral‐level or masters‐level therapists with at least two years of CBT experience Frequency: twice, for a total of 36 weekly sessions. 2. Goal‐Focused Supportive Contact group: N = 38. Content: enhanced supportive contact that included a primary focus, like CBSST, on setting and achieving functioning goals (e.g. living, learning, working and socialising) Delivered by: the same therapists with CBT group. Frequency: a total of 36 weekly sessions. |
|
| Outcomes | Mental state: positive symptoms ‐ PANSS, BDI (skewed data), BAI (skewed data) Functioning: life skills ‐ Comprehensive Module Test (skewed data). Quality of life: Life Satisfaction Index. Satisfaction with treatment: leaving the study early. Unable to use ‐ Defeatist Attitudes: Defeatist Performance Attitude Scale (not predefined in our protocol). Functioning: independent living skills survey (data are not available to use, the reported result is average of available domain scores). Mental state: SANS, Self Esteem Rating Scale‐Short Form ‐ SERS (only sub scale scores were available, no total score). |
|
| Notes | Trial Registry: NCT00237796 This study was funded by National Institute of Mental Health (NIMHRO1MH071410) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "participants were randomly assigned by an independent statistician"(p.3). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "participants were randomly assigned by an independent statistician"(p.3). Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "single‐blind...Assessors were blind to treatment allocation" (p.3). Comments: participants and personnel knew the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "single‐blind...Assessors were blind to treatment allocation" (p.3). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comments: 10 participants from the CBT group and five participants from the active control group left the study early. High proportion of dropout. |
| Selective reporting (reporting bias) | High risk | Comments: the total score of PANSS was not reported as well as other sub scale score such as negative symptoms and general psychopathology. The total score of SANS was not reported. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Granholm 2014.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: a variety of community settings throughout San Diego, USA. Length of follow‐up: 4.5, 9, 15, 21‐months. |
|
| Participants | Diagnosis: schizophrenia or schizoaffective disorder (DSM ‐ IV).
N = 149. Sex: 99 M, 50 F. Age: mean ˜ 41.6 years, SD ˜ 9.2 years. History: length of illness: mean˜ 21.4 years, SD˜ 10.6 years. Excluded: (a) prior exposure to CBT or SST during the previous 5 years, and (b) level of care required at baseline that would interfere with participation in outpatient therapy groups or assessments. |
|
| Interventions | 1. Group CBT group: N = 73. Content: group‐based intervention included thought Challenging, Social Skills Training, and Problem‐Solving Training. Cognitive therapy was combined with role‐play practice of communication skills and problem‐solving training Delivered by: two doctoral‐level or masters‐level therapists with at least two years of CBT experience Frequency: a total of 36 weekly sessions (9 months) with monthly booster sessions for 12 months follow‐up 2. Goal‐Focused Supportive Contact group: N = 76. Content: enhanced supportive contact that included a primary focus, like CBSST, on setting and achieving functioning goals (e.g. living, learning, working and socialising) Delivered by: the same therapists with CBT group. Frequency: a total of 36 weekly sessions (9 months) with monthly booster sessions for 12 months follow‐up |
|
| Outcomes | Mental state: positive symptoms ‐ PANSS scores*, Beck Depression Inventory (BDI, skewed data)*. Functioning: life skills ‐ Comprehensive Module Test (CMT, skewed data)*, Maryland Assessment of Social Competence (MASC)*. Satisfaction with treatment: leaving the study early. Unable to use ‐ Psychosocial Rehabilitation Toolkit ‐ PSR Toolkit (the author did not report the data of this outcome). Mental state: SANS (only sub scale scores were available, no total score). Defeatist Performance Attitude Scale ‐ DPAS (not predefined in our protocol). |
|
| Notes | * Long‐term outcome not included due to greater than 40% attrition. Short‐term data were also not reported for MASC. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "An independent statistician allocated participants to treatments according to a computer‐generated randomisation list."(p.2). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "An independent statistician allocated participants to treatments according to a computer‐generated randomisation list."(p.2). Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Assessors were blinded to treatment allocation, and therapists and the study coordinator, who were aware of treatment allocation, did not complete any outcome assessments."(p.2). Comments: participants and therapists knew the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Assessors were blinded to treatment allocation, and therapists and the study coordinator, who were aware of treatment allocation, did not complete any outcome assessments."(p.2). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comments: 48 participants from the CBT group and 44 participants from the active control group left the study early. High proportion of dropout. |
| Selective reporting (reporting bias) | High risk | Comments: the total score of PANSS was not reported as well as other sub scale score such as negative symptoms and general psychopathology. The total score of SANS was not reported. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Haddock 1999.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: inpatients, UK. Length of follow‐up: 2 years. |
|
| Participants | Diagnosis: schizophrenia (DSM‐IV) or schizoaffective disorder confirmed by an independent psychiatrist attached to the project.
N = 21.
Sex: 19 M, 2 F.
Age: mean ˜28 years, SD ˜7 years. History: length of illness < 5 years. Excluded: not reported. |
|
| Interventions | 1. CBT group: N = 10. Content: short‐term individual CBT + standard care. Delivered by: two clinical psychologists with expertise in the CBT. Frequency: not reported. 2. Supportive counselling group: N = 11. Content: supportive counselling and psychoeducation + standard care. Delivered by: not reported. Frequency: not reported. Treatment duration: 5 weeks with booster sessions at 1, 2, 3, and 4 months after discharge. |
|
| Outcomes | General state: relapse.
Mental state: BPRS score.
Satisfaction with treatment: leaving the study early. Unable to use ‐ Mental state: PSYRATS (only P values were reported, no usable data ) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomised ‐ no further details." (p.255) Comments: the author used computer‐generated randomisation procedure in another study (NA ‐ Haddock 2009) |
| Allocation concealment (selection bias) | Unclear risk | Comments: insufficient information. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: " ward staff and responsible medical officers were informed that patients were taking part in the study, but were not informed of the treatment allocation."(p.255). Comments: it is likely that the participants and personnel would know the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Independent assessment was carried out by the project psychiatrist, who was blind to the treatment allocation. Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: completer data (less than 5% drop out). |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Jiang 2010.
| Methods | Allocation: randomised.
Blinding: not reported. Location: Inpatients, China. Length of follow‐up: 3, 6‐months. |
|
| Participants | Diagnosis: chronic schizophrenia (CCMD‐3) with obsessive‐compulsive symptoms (total score of Yale‐Brown Obsessive‐Compulsive Scale (Y‐BOCS) >16). N = 70* . Sex: 36 M, 29 F. Age: 25 ‐ 70 years, mean ˜ 39.13 years, SD ˜ 14.12years. Excluded: other psychotic disorder, obvious physical disorder, nervous system disease, pregnancy, breast feeding women. |
|
| Interventions | 1. CBT group: N = 35. Content: remediation of the participants' false cognition; remediation of the harmful behaviour; relaxation training; promote the participants getting involved in recreational activities. Delivered by: not reported. Frequency: not reported. 2. Health education: N = 35. Content: general health education and standard psychological nursing care. Delivered by: not reported. Frequency: not reported. Treatment duration: 6 months. Both groups continued to receive antipsychotics. |
|
| Outcomes | Mental state: no clinical response on obsessive‐compulsive disorder**, Yale‐Brown Obsessive Compulsive Scale (Y‐BOCS), anxiety (HAMA). Satisfaction with treatment: leaving the study early. |
|
| Notes | * 5 participants left the study early. ** defined by the decreased rate of Y‐BOCS score<25%. Funding source: not reported. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomisation based on random number table" (p.227). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Unclear risk | Comments: the author did not report the allocation concealment. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not report the blinding.Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comments: the author did not report the blinding. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: two participants left the study early in the CBT group and three participants left the study early in health education group. |
| Selective reporting (reporting bias) | Low risk | Comments: all measured outcomes were reported. |
| Other bias | Low risk | Comments: none obvious. |
A ‐ Klingberg 2012.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: 3 study centres, Germany. Length of follow‐up: 6 and 12 months. |
|
| Participants | Diagnosis: DSM‐IV) confirmed by a structured clinical interview (SCID‐I). N = 198. Sex:111 M, female 87 F. Age: mean 36.9 years, SD 9.9 years. History: outpatient, fluent speaker in German language; willingness to give informed consent. Excluded: any PANSS positive symptom (P1–P7) ≥ 6; severe depression as indicated by PANSS G6 ≥ 6; any extrapyramidal symptom of at least moderate intensity as assessed with the Udvalg for Klinske Undersøgelser (UKU) side‐effect rating scale; age < 18 or > 55; verbal IQ < 80 assessed by a German multiple‐choice vocabulary test; organic brain disease; diagnosis of substance abuse or substance dependence according to DSM‐IV/SCID‐I as primary clinical problem including the intention to initiate treatment of substance abuse/ dependence; travel time to the study centre ≥ 1 hour. |
|
| Interventions | 1. CBT group: N = 99. Content: applies general principles of cognitive behaviour therapy (e.g. case formulation based on a cognitive model, goal setting, discussion of cognitive processes, homework assignments, role‐play) for the treatment of negative symptoms. The treatment concept of the CBT has been described in detail elsewhere(Klingberg 2008; Klingberg 2009). Delivered by: five specifically trained clinical psychologists. Frequency (times): 20 sessions in 9 months. 2. Cognitive Remediation (CR) group: N = 99. Content: the program follows the principles of errorless learning, overlearning, and immediate positive feedback (verbal), which are combined with alternative cognitive strategies such as systematic elaboration of information, verbalization, self‐instruction, and structuring of information. The CR has been adapted from an earlier study (Wolwer 2005). Delivered by: five specifically trained clinical psychologists. Frequency (times): 20 sessions in 9 months. Treatment duration (weeks): 9 months. All patients received routine psychiatric outpatient care outside of the study including antipsychotic medication and regular visits with a psychiatrist. |
|
| Outcomes | Global state: rehospitalisation Adverse events: death (due to accident), no events/effects. Satisfaction with treatment: leaving the study early. Engagement with service: compliance with medication‐number of participants with favourable or adequate medication compliance*. Unable to use ‐ Number of participants receiving antipsychotics at baseline, 6‐ and 12‐month (not predefined in our protocol). Mental state: Clinical Global Impression Scale (CGI), PANSS, SANS, Calgary Depression Rating Scale for Schizophrenia (CDSS) and specific symptom score‐SCL‐90‐R‐GSI (Global severity index) (these outcomes were reported as effect size that can not be transformed and used). Global state: Global assessment of functioning (GAF) (these outcomes were reported as effect size effect size that can not be transformed and used). |
|
| Notes | * Data were reported at 6 months. As 6 months and 12 months are both medium‐outcome data, therefore, we only used data reported at 12 months). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: " ...generated by the Institute for Medical Biometry using a computerized algorithm and was stored by CenTrial"(p.S102). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: " ...generated by the Institute for Medical Biometry using a computerized algorithm and was stored by CenTrial"(p.S102). Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "Assessor blind regarding the study condition"(p.S102) "the result of the randomisation only to the therapist in order to keep the assessor blind regarding the study condition. The therapist then gives the information about treatment allocation to the patient." (p.S102). Comments: participants and therapists knew the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: " Blinded assessment"(p.S100) "assessor blind regarding the study condition"(p.S102) "the result of the randomisation only to the therapist in order to keep the assessor blind regarding the study condition. The therapist then gives the information about treatment allocation to the patient." (p.S102). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: 9 and 20 participants dropped out from the CBT group and CR group, respectively, however, the intention‐to‐treat sample includes all randomised patients. |
| Selective reporting (reporting bias) | Low risk | Comments: all measured outcomes were reported. |
| Other bias | Low risk | Funding source: This study was funded publicly by the German Research Foundation (Deutsche Forschungsgemeinschaft, grants Kl 1179/2‐1 and Kl 1179/3‐1). Comments: none obvious. |
A ‐ Lecomte 2008.
| Methods | Allocation: randomised. Blinding: single‐blind. Location: community mental health clinics in Quebec and British Columbia, Canada. Length of follow‐up: 3, 12 months. |
|
| Participants | Diagnosis: schizophrenia spectrum, n = 71; others, n = 58. N = 129. Sex: 36 M, 93 F. Age: 18 ‐ 35 years; mean ˜ 24.92 years. History: currently presenting with persistent or fluctuating psychotic symptoms (defined as delusions or hallucinations appearing occasionally, such as in periods of stress), having consulted for the first time a mental health professional for psychotic symptoms in the past 2 years, and being followed by a psychiatrist (and therefore receiving antipsychotic medication). Individuals only recruited once they had been discharged from the hospital and considered 'stabilised' by their psychiatrist. Nonaffective psychosis was preferred but individuals with unclear diagnoses at the time of the referral were also accepted. Excluded: organic disorder, having already received one of the interventions, and not being able to give informed consent. Capacity to give informed consent verified by a true‐false questionnaire given after the study and consent form were explained. |
|
| Interventions | 1. Group CBT: N = 48. Content: the manual is built in 4 parts: (1) stress: how it affects me; (2) testing hypotheses and looking for alternatives, (3) drugs, alcohol, and how I feel; and (4) coping and competence. Frequency: 24 sessions, twice a week, for 3 months. Delivered by: 2 therapists and none had previous training in CBT. Treatment duration: 3 months. 2. Group social skill training: N = 54. Content: teaching skills such as symptom management and relapse prevention. Treatment duration: 3 months. 3. Waiting‐list control group: N= 27*. Content: On waiting list . Treatment duration: 3 months. |
|
| Outcomes | Mental state: BPRS total score, positive and negative score, Self‐esteem ‐ Self‐Esteem Rating Scale (skewed data). Fucntioning: Insight ‐ The Insight Scale. Satisfaction with the treatment: leaving the study early. Unable to use ‐ Coping with stress: Cybernetic Coping Scale (CCS) ‐ invalidate data, only data from sub scales (CCS active and CCS passive) were reported, however the validity of the sub‐scale was not tested. The addiction severity index (ASI) ‐ data were not reported. Belief about Voices Questionnaire (BAVQ) ‐ only data in CBT group at 1 year follow‐up were reported. Maudsley Assessment of Delusion schedule ‐ only data in CBT group at 1 year follow‐up were reported. The social provision scale (SPS) ‐ not predefined in our protocol. Mental state: Beck Depression Index (BDI) ‐ only data in CBT group at 1‐year follow‐up were reported. |
|
| Notes | *We only used data from CBT group and social skill training group. We did not use data from this trial at 15‐month follow‐up as the attrition rate exceeded 50%. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "Participants were randomly assigned..." (p.868) Comments:iInsufficient information about the sequence generation process to permit judgement of 'Low risk' or 'High risk'. |
| Allocation concealment (selection bias) | Unclear risk | Comments: the method of concealment is not described. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comments: single‐blinded, only outcome assessor was blinded, |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "...single blinded, the assessors were blinded." (p.868) |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comments: 13 participants from the CBT group and 37 participants from the control group left the study early at 9 months follow‐up. High proportion of dropped out. |
| Selective reporting (reporting bias) | Low risk | Comments: all measured outcomes were reported. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Levine 1998.
| Methods | Allocation: randomised.
Blinding: maybe single‐blind. Location: Israel. Length of follow‐up: 6, 10 weeks. |
|
| Participants | Diagnosis: paranoid schizophrenia diagnosis according to DSM‐III‐R criteria
N = 12. Sex: not reported. Age: range 20‐45 years. History: length of illness > 5 years. Inclusion criteria: education: 8 years of schooling and more; active delusional system; no change of antipsychotic drugs given in standard dosage in the last 3 months. Excluded: alcohol and/or drug abuse; chronic physical condition; Orthodox religious conviction. |
|
| Interventions | 1. CBT group: N = 6. Content: group based, six weekly sessions + standard care. Delivered by: all researchers taking part in the present study were previously trained in inducing cognitive dissonance in paranoid patients. Frequency: six sessions, once weekly for 50 minutes. 2. Supportive therapy group: N = 6. Content: group based, six weekly sessions + standard care. Delivered by: all researchers taking part in the present study were previously trained in inducing cognitive dissonance in paranoid patients. Frequency: 50 minutes weekly for 6 weeks. Treatment duration: 6 weeks. |
|
| Outcomes | Mental state: PANSS total score. Unable to use ‐ PANSS ‐ positive (skewed data), PANSS ‐ negative (skewed data), thought disturbance (skewed data). |
|
| Notes | None. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comments: reports random allocation ‐ no detail provided. |
| Allocation concealment (selection bias) | Unclear risk | Comments: insufficient details provided. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comments: raters unaware of allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: no dropouts. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | High risk | Comments: sample size of only 6 participants per group. |
A ‐ Li 2014.
| Methods | Allocation: randomised. Blinding: single‐blind. Location: inpatient and out‐patients in three psychiatric hospitals in Beijing, China. Length: 84 weeks. |
|
| Participants | Diagnosis: schizophrenia (72.9% in the CBT group and 77.1% in the ST group were characterised as paranoid type, and 27.1% in the CBT group 22.9% in the ST group were classed as having undifferentiated schizophrenia. N = 96. Sex: 72 M, 24 F. Age: 18–60 years *. History: PANSS total score greater than 60 indicating at least a mild level of psychiatric symptoms; on an adequate dose of an antipsychotic medication for at least the prior 4 weeks; capable of providing written informed consent. Excluded: a co‐morbid diagnosis of mental retardation or primary substance dependence; a score of 55 (worse) of conceptual disorganisation according to the PANSS, which included those who could not communicate, had poor rapport, or lack of spontaneity and flow of conversation; had received electroconvulsive therapy within the past 6 months prior to entry into the study; currently receiving other types of systematic psychotherapy. |
|
| Interventions | 1. CBT group: N = 96. Quote "CBT is a manual‐based treatment. In this study, it was delivered by therapists to patients who were allocated to the CBT group. There were 12 sessions in the first 12 weeks followed by three booster sessions in the subsequent 12 weeks. Each session lasted for about 40– 50 min and flexibility on time was given depending on the attention, tolerance level and mental state of the participants. The trial protocol for using CBT to treat schizophrenia was compiled in Chinese and based on the principles and practice developed by Kingdon & Turkington (Kingdon 2004). This training manual was written in Chinese and translated to English before it was used as the training material for review by Kingdon and Turkington, and three CBT specialists in Hong Kong, Beijing and Changsha of China. Its cultural relevance and acceptability were tested on 10 patients with schizophrenia. The first four sessions were delivered twice a week and focused on the introduction of the treatment, building a therapeutic alliance, psychoeducation about the cognitive–behavioural model of psychosis and normalization of the experience of psychosis. The next six sessions in the intermediate stage were offered once a week. These sessions involved cognitive–behavioural work with delusions, hallucinations, negative symptoms and anxiety/depression. Homework was also assigned in a flexible manner after each session to consolidate what was learned in the session. The two sessions in the final phase were delivered once every 2 weeks. They included a discussion of attitudes to medication and relapse prevention work. Finally, three booster sessions were offered once monthly for reviewing patients' progress and consolidating what patients had learned of CBT strategies for coping" (p 1896). Quote "The eight therapists were experienced psychiatrists or psychologists with 5 to 20 years experience using psychotherapy in hospitals on patients with a mental disorder. They had been trained and supervised in the application of cognitive therapy for psychosis by experienced cognitive – behavioural therapists, and had special expertise in the application of CBT for psychosis using a translated Kingdon and Turkington manual" Kingdon 2004 (p.1898). 2. Supportive Therapy group: N = 96. Quote "ST was also in the form of manual‐based treatment and comprised 12 sessions in the first 12 weeks followed by three consolidated sessions in the subsequent 12 weeks. Each session lasted for about 40 – 50 min. This intervention is based on supportive models of psychotherapy and has been reported to be the most widely practised form of individual psychotherapy in psychiatric services (Winston et al. 2004 ). The primary goal of the ST in the first 12 sessions was to provide patients with emotional support, knowledge of mental disorders, and provide suggestions to patients on preventing a relapse of the disease. Similar to the CBT approach, ST also focused on developing and maintaining therapeutic alliance and providing psychoeducation to patients. However, ST did not have a therapeutic component and did not have a treatment structure. For example, patients could select session topics such as discussing interests, personal experiences and expressing feelings. Therapists were nondirective but used reflective listening and summarizing techniques to support patients in coping with current life events and in relapse prevention. No homework was given and no specific CBT." (p1896) Treatment duration: 24 weeks. |
|
| Outcomes | Mental state: PANSS general, positive, negative scores Functioning: Personal and Social Performance Scale scores, Schedule for Assesing Insight scores. Satisfaction with treatment: leaving the study early. |
|
| Notes | * The groups were evenly matched in terms of demographics, with the exception of age. The ST group was significantly older (mean age was 33.44 years) than the CBT group (mean age was 29.27 years). Age was therefore treated as a confounding factor in subsequent analyses. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomly allocated to the CBT group or the ST group (1:1 randomization). Block randomization was conducted by computer‐generated, random numbers to allocate the eligible participants to either of the two groups, stratified according to study site and performed at a geographically remote and independent location." Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "..., stratified according to study site and performed at a geographically remote and independent location." Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comments: single‐blinded study, only outcome assessor was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comments: five independent trained raters were blind to the allocation status of the participants. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: 25 or 96 participants left the study early. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: none obvious. |
A ‐ Li 2015.
| Methods | Allocation: randomised.
Blinding: maybe single‐blind. Location: China. Length of follow‐up: 1 year. |
|
| Participants | Diagnosis: schizophrenia, diagnosed with CCMD‐3.
N = 200. Sex: 92 M, 86 F*. Age: range 18‐60 years. History: length of illness > 5 years, illness condition relatively stable and living with relatives to maintain pharmacological therapy. Excluded: people with tardive dyskinesia; severe physical impairment; pregnant or lactating women. |
|
| Interventions | 1. CBT group: N = 50. Content: through analysis of underlying causes and developing problem‐solving models to correct patients negative/problematic behaviour, as well as improving patients understanding of the condition. Re‐build behavioural model that is beneficial to patient cognitive ability, reduces social conflict, improve medication compliance and reduce symptoms. Delivered by: psychiatrists taking part in the present study's institution. Frequency: twice/month for the first 6 months, once/month for the last 6 months. 50 minutes each session. Frequency: 50 minutes each session. 2. Family intervention group: N = 50. Content: psychoeducation directed to carers to improve their understanding of the condition and skills on family intervention/care. Carers was trained on emotional expression, ability to recognise early warning signs and dealing with conflicts. Delivered by: twice/month for the first 6 months, once/month for the last 6 months. 50 minutes each session. Frequency: 50 minutes each session. Treatment duration: 6 weeks. 3. Occupational therapy group: N = 50. Content: participants past work experience, current skills and development potential was evaluated at the start of the therapy to inform the individual occupational therapy planning, which includes the following content: work target, individual strength and weakness, means of achieving target, change perception (e.g. housework is also work). Encouragement was given and systemic psychological care was also provided. Delivered by: twice/month for the first 6 months, once/month for the last 6 months. 50 minutes each session. Frequency: 50 minutes each session. Treatment duration: 6 weeks. 4. Standard care group: N = 50. This group received the usual care they would have received on the ward. |
|
| Outcomes | Mental state: SCL‐90 total score. Satisfaction with treatment: leaving the study early. Unable to use ‐ Functioning: Family Burden Scale score was reported, however the study author did not provide the full name or reference for the scale and it appears the scale was not validated or peer‐reviewed. |
|
| Notes | * Twenty‐two participants dropped out from the trial. We only used data from the first three groups, and combined data from family intervention group and occupational therapy group into one single group data. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: random number table was employed to achieve random sequence generation. |
| Allocation concealment (selection bias) | Unclear risk | Comment: the author did not describe this information. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comment: another clinician unaware of the group allocations performed outcome evaluation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: a small number of participants dropped out in each of the four groups, but the distribution of dropout was balanced between groups and had minimal affect on the SCL‐90 average score (which is the main usable outcome of this study). |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comment: none obvious. |
A ‐ Li 2015b.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: China. Length of follow‐up: 12 weeks. |
|
| Participants | Diagnosis: schizophrenia, diagnosed with ICD‐10.
N = 100. Sex: 46 M, 40 F*. Age: range 18‐60 years. History: length of illness > 5 years: PANSS score <70; HAMD score > 17 <24; SAS score > 51 < 69; SSMI‐C score > 50 ; illness condition relatively stable in the past 6 months; educated to middle school level or above. Exclusded: severe physical impairment; pregnant or lactating women; abnormal lab tests |
|
| Interventions | 1. CBT group: N = 50. Content: three stages and each with distinctive therapeutic goals. Therapy programme was developed with clear focus of each stage and homework was allocated. Initially therapeutic relationship was established by investigating patients feeling towards illness stigma and their perception of the illness. During second stage, CBT techniques were employed to correct the misconception and to incept positive thought model and coping strategy. In final stage, previous learning was reinforced and consolidated. Delivered by: not stated. Frequency: 50 to 60 minutes each session, 8 sessions in total. Once/week for the first 8 weeks and once/fortnight for the last 4 weeks. Treatment duration: 12 weeks. 2. Supportive therapy group: N = 50. Content: psychoeducation to improve patients understanding of the condition and importance of medication, as well as the side effects expected. Delivered by: not stated. Frequency: 50 to 60 minutes each session, 8 sessions in total. Once/week for the first 8 weeks and once/fortnight for the last 4 weeks. Treatment duration: 12 weeks. |
|
| Outcomes | Mental state: SSMI‐C total score, HAMD score, SAS score. Satisfaction with treatment: leaving the study early. |
|
| Notes | * Five participants dropped out from the trial. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: the author stated the group assignment as randomly assigned. No details about the randomisation method were reported. |
| Allocation concealment (selection bias) | Unclear risk | Comment: the author did not describe this information. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: the author stated single‐blind, but we are unclear who was blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: the author stated single‐ blind, but we are unclear who was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: dropout rate was small and balanced between groups without having had any significant on the scale score average. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comment: none obvious. |
A ‐ Ma 2012.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: inpatients and outpatients, three hospitals in China. Length of follow‐up: 12, 24 weeks. |
|
| Participants | Diagnosis: schizophrenia, DSM‐IV. N = 200. Sex: 51 M, 69 F*. Age: 18‐60 years; mean ˜ 29 years, SD ˜ 10 years. History: middle‐school education or higher; PANSS total score ≥ 60; receiving one type of antipsychotics; consistent dosage and type of antipsychotics use for at least 2 weeks; carers has signed the informed consent. Excluded: have other psychotic disorder; the item score 'dissociation' in PANSS scale≥5; the item score 'Poor rapport' in PANSS scale≥5; the item score 'Lack of spontaneity & flow of conversation' in PANSS scale≥5; did not receive modified electroconvulsive therapy one month before randomisation; receiving other psychological therapies at present; with any severe or unstable physical disorder. |
|
| Interventions | 1. CBT group: N = 100. Content: the CBT therapy referred to Kingdon D et. al's (Kingdon 2005) CBT handbook. The CBT mainly involves therapies for hallucination, delusion, negative symptoms or emotional symptoms, medication compliance and prevention of relapse. Delivered by: trainee CBT therapists. Frequency: during the first 24‐week treatment period, participants received 15 sessions in total involving: two sessions per week for 2 weeks; one session per week for 6 weeks; four biweekly sessions, and three once‐per‐month sessions. 2. Supportive Therapy group: N = 100. Content: a supportive therapy handbook was established, which mainly involves basic psychological treatment strategies such as unconditional positive regards, positive regards, support, acceptance, encouragement, health education relevant to schizophrenia, etc. Delivered by: not reported. Frequency: during the first 24‐week treatment period, participants received 15 sessions in total involving: two sessions per week for 2 weeks; one session per week for 6 weeks; four biweekly sessions, and three once‐per‐month sessions. Treatment duration: 24 weeks. |
|
| Outcomes | Adverse effects: no events Satisfaction with treatment: leaving the study early. Unable to use ‐ Coping style Qustionaire: invalidate data, only data from sub scales (such as problem‐solving, self‐accusation) were reported, however the validity of sub scale was not tested. Mental state: PANSS, IBS score: not reported in the study results. Quality of life: Physical health (WHOQOL‐BREF); psychological (WHOQOL‐BREF); social relationships (WHOQOL‐BREF); environment (WHOQOL‐BREF) at 12‐, 24‐week (outliers, data in two treatment groups were exactly the same). |
|
| Notes | * 32 participants left the study early, 48 participants were excluded from the final analysis due to invalid questionnaire. Funding sources: funded by the Beijing municipal science and technology research and development projects: D0906001040391. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomisation based on random number table" (p.802). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Unclear risk | Comments: the author did not describe this information. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants or personnel.Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comments: outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comments: 32 participants left the study early, 48 participants were excluded from the final analysis due to invalid questionnaire. |
| Selective reporting (reporting bias) | High risk | Comments: the author did not report the PANSS score and IBS score. |
| Other bias | Low risk | Comments: none obvious. |
A ‐ Penn 2009.
| Methods | Allocation: randomised.
Blinding: single‐blind.
Location: outpatient clinic at a local hospital and local community mental health centres, central North Carolina, USA. Length of follow‐up: post treatment, 3, 12 months follow‐up. |
|
| Participants | Diagnosis: schizophrenia, schizoaffective disorder.
N = 65. Sex: 33 M, 32 F. Age: 18 ‐ 65 years. History: presence of current persistent auditory hallucinations of at least moderate severity (rating of at least 4 PANSS); attending at least two pharmacological trials, one of which being an atypical antipsychotic or clozapine for 8 weeks prior to randomisation. Excluded: meeting criteria for mental retardation (based on both IQ and functional impairment criteria) or having current substance dependence. |
|
| Interventions | 1. CBT group: N = 32. Content: based upon New Reference protocols, focused on auditory hallucinations (content behavioural analysis, and coping strategies) ‐ more emphasising coping skills rather than cognitive restructuring; and de‐emphasising self‐esteem work than New Reference. Delivered by: a clinical psychologist, a psychiatrist, a social work graduate student, and doctoral students Frequency: 12 one‐hour weekly sessions. 2. Enhanced supportive therapy group: N = 33. Content: divided into 3 phases: i. establishing therapeutic alliance, ii. agreeing on interpersonal goals (for each group member); and iii. focusing on social integration (i.e. identifying steps to achieve those interpersonal goals) ‐ direct approach to solving problems relying on advice from therapists and other group members (unlike CBT, group leaders provided direct advice for client questions/problems, and solicited advice and suggestions from group members). Delivered by: other competent therapists. Frequency: 12‐week manual‐based intervention. Each session lasted about 1 hour. Treatment duration: 12 weeks. |
|
| Outcomes | Global state: hospitalisation. Mental state: PANSS, PSYRATS, BDI, RSES scores. Functioning: social ‐ SFS scores, cognitive ‐ BCIS. Satisfaction with treatment: leaving the study early. Unable to use ‐ The Belief about Voices Questionnaire‐Revised (BAVQ) ‐ invalidate data, only data from sub scales (malevolence, benevolence, resistance, engagement, and omnipotence) were reported, however the validity of the sub‐scale was not tested. |
|
| Notes | None. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was stratified by gender to ensure equal numbers across groups using a computer randomisation generator. " (p.54). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomization to treatment condition (with condition being designated by a random number), was conducted by a research associate blind to the correspondence between random number and treatment group."(p.54). Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "... Experimental blindness was maintained by asking participants not to talk to the RAs about their treatment." (p.54). Comments: Participants and therapists knew the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "All recruitment procedures and research evaluations were conducted by two research assistants (RAs) who were blind to treatment assignment." (p.54). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: intention‐to‐treat analysis. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Pinto 1999.
| Methods | Allocation: randomised.
Blinding: not reported. Location: inpatients and outpatients, North America. Length of follow‐up: 6 months |
|
| Participants | Diagnosis: schizophrenia (DSM IV).
N = 41. Sex: 28 M, 13 F. Age: mean ˜ 33.9 years, SD ˜ 10.1 years. History: length of illness mean ˜ 11.6 years, SD ˜ 7.9 years, no evidence of current substance abuse or organic pathology, treatment‐refractory psychosis, able to provide informed consent. Exclusded: not reported. |
|
| Interventions | 1. CBT group: N = 20. Content: individual CBT + social skills training + standard care. Delivered by: not reported. Frequency: not reported. 2. Supportive counselling: N = 21. Content: included psychoeducation about nature and treatment of schizophrenia, active listening, empathy and reassurance, health promotion, crisis management, advocacy + standard care. Delivered by: well‐trained psychiatrist or psychologist. Frequency: not reported. Monthly support meetings for family members were available for the families of clients in both groups. Treatment duration: 6 months. |
|
| Outcomes | Mental state: BPRS, SAPS (skewed data), SANS. Satisfaction with treatment: leaving the study early. | |
| Notes | None. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comments: the author reported random allocation but did not describe more details. |
| Allocation concealment (selection bias) | Unclear risk | Comments: the author did not describe this information. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of outcome assessor. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comments: the author did not describe this information. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Tarrier 1999.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: National Health Service trusts in Greater Manchester Lenght of follow‐up: 10 weeks, 12, 24 months. |
|
| Participants | Diagnosis: schizophrenia, schizoaffective psychosis, delusional disorder (DSM III R).
N = 87. Sex: 69 M, female 18 F. Age: 16 ‐ 65 years, mean ˜ 39 years, SD ˜ 11 years. History: median length illness 11 years; experiencing psychotic symptoms (i.e. hallucinations or delusions) for at least six months which did not appear to be responding further to medication; no evidence of organic pathology which could have explained the psychopathology; receiving regular and stable antipsychotic medication. |
|
| Interventions | 1. CBT group: N = 33. Content: coping strategy enhancement, training in problem‐solving, strategies to reduce relapse + standard care. Delivered by: three experienced clinical psychologists and followed a protocol manual. Frequency: six hourly sessions, each of which were followed by two summary sessions. Sessions were carried out twice a week and 20 sessions of treatment were carried out over 10 weeks. After post‐treatment assessment, four booster sessions were given once a month for four months. 2. Supportive counselling group: N = 26. Content: emotional support, unconditional regard, general counselling + standard care. Delivered by: three experienced clinical psychologists and followed a protocol manual. Frequency: 20 one‐hour sessions twice a week with four booster sessions after post‐treatment assessment. 3. Standard care group: N = 28. Content: standard psychiatric management with medication, monitoring outpatient follow‐up and care programme approach. Delivered by: Three experienced clinical psychologists and followed a protocol manual. Frequency: not available. Treatment duration: 10 weeks treatment plus 4 months booster session. |
|
| Outcomes | Global state: relapse. Mental state: clinically important change*, negative symptoms ‐ SANS. Adverse effect/event: death. Satisfaction with treatment: leaving the study early. Unable to use ‐ Mental state: positive symptoms(calculated by combining PSE and BPRS scores ‐ log transformed data). |
|
| Notes | * Less than 50% improvement in positive symptoms sub scale of BPRS in both severity and number of symptoms. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comments: stratified block randomisation procedure. |
| Allocation concealment (selection bias) | Low risk | Comments: allocation contained in sealed envelopes ‐ undertaken by independent third party. Participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comments: raters blind to treatment condition. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comments: completer data reported. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
A ‐ Velligan 2014.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: "public mental health clinics in 2 counties in Texas"(p.2). Length of follow‐up: 3, 6, 9, 12, 15 months follow‐up. (p.2). |
|
| Participants | Diagnosis: schizophrenia or schizoaffective disorder. N = 166. Sex: 74 M, 92 F. Age: 18 ‐ 60 years; mean˜ 43.47 years, SD˜ 10.7 years. History: fluent English speakers between the ages of 18 and 60 years; receiving ongoing treatment with an oral antipsychotic; persisting positive symptoms as evidenced by a score of ≥ 4 on BPRS expanded version ratings of delusions, hallucinations, and/or suspiciousness; functional impairment as evidenced by a score of < 70 on the social and occupational functioning scale; stable residence; able to understand and complete assessments. Excluded: documented history of significant head trauma, seizure disorder, or mental retardation; history of substance abuse or dependence in the past month; history of violence in the past 6 months (as a safety measure for staff making home visits). |
|
| Interventions | 1. CBT Group: N = 37. Content: CBTp is a talk therapy designed to treat persistent symptoms of psychosis and the accompanying distress. A 9‐month treatment manual was developed based upon Kingdon and Turkington and included simple handouts and homework assignments based on the work of Granhom et al. The focus of the sessions was on patient identified problems, particularly those that interfered with daily functioning or were distressing, normalizing symptoms, and using CBT techniques to develop alternative explanatory models of event. Delivered by: experienced therapists (p.3). Frequency: CBT was delivered weekly for 9 months for up to 38 visits during the treatment period. Sessions lasted for ˜1 hour. 2. Cognitive Adaptation Training (CAT) Group: N = 33. Content: CAT is a series of manual‐driven compensatory strategies and environmental supports (signs, checklists, electronic cueing devices) established and maintained on weekly home visits by a CAT therapist/trainer. Delivered by: experienced therapists. Frequency (times): CAT was delivered weekly for 9 months for up to 38 visits during the treatment period. Sessions lasted for ˜1 hour. 3. CBT+CAT group: N = 40. * Content: CBT combined with CAT. Delivered by: experienced therapists 4. Standard care group: N = 42.* TAU consisted of case management and medication follow‐up appointments provided by the local community mental health centre. Delivered by: Experienced therapists Treatment duration: 9 months. |
|
| Outcomes | Outcomes Satisfaction with treatment: leaving the study early. Unable to use ‐ Mental state: BPRS, Hallucination Rating Scale (AHRS), the Delusion Rating Scale (DRS). (only P values were reported). Function: the Multnomah Community Ability Scale (MCAS) (only P values were reported). |
|
| Notes | Funding source: National Institute of Mental Health (5R01MH082793). * We only used data from CBT and CAT group, according to the inclusion criteria in our protocol, we did not use data from CBT+ CAT group and TAU group. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was stratified by gender and age using a computer generated algorithm created by the study statistician who had no patient contact." (p.2) Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomization was stratified by gender and age using a computer generated algorithm created by the study statistician who had no patient contact." (p.2) Comments: participants and investigators enrolling participants could not foresee assignment because the allocation assignment was conducted by an independent statistics. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "All raters were blind to treatment condition"(p.4). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: 13 patients in the CBT group and 13 patients in the CAT group dropped from the study. Intention‐to‐treat analysis was conduct when analysing the data. |
| Selective reporting (reporting bias) | Low risk | Comments: all measured outcomes were reported. |
| Other bias | Low risk | Comments: none obvious. |
A ‐ Wittorf 2010.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: inpatients and outpatients departments of psychiatry and psychotherapy of the Universities of Tuebingen, Frankfurt, Duesseldorf, Bonn, Cologne, and Essen, Germany. Length of follow‐up: session‐3, 6, 9 and 12. (p.479). |
|
| Participants | Diagnosis: schizophrenia (DSM‐IV), schizophreniform disorder (DSM‐IV, 295.4), schizoaffective disorder (DSM‐IV 295.7), or delusional disorder (DSM‐IV 297.1), confirmed by a structured clinical interview (SCID‐I). N = 100* Sex: 35 M, 32 F. Age: 18 ‐59 years; mean 37.78 years, SD 8.44 years. History: presence of delusions or hallucinations of at least moderate intensity according to the PANSS items (P1 or P3 2:4); persistence of positive symptoms for at least 3 months with or without compliance regarding antipsychotic medication; no diagnosis of substance abuse or substance dependence according to DSM‐IV/ SCID‐I as primary clinical problem implying the intention of the institution responsible for treatment to initiate a specialised treatment of substance abuse/dependence; IQ > 80 according to the Mehrfachwahl‐Wortschatztest (MWT‐B; Lehrl, 1992), a German multiple‐choice vocabulary test measuring the premorbid intellectual level; no organic brain disease (other than schizophrenia) according to standard patient examination procedures; fluency regarding the German language; and travel time to the study centre of less than 1 hour. Excluded: not reported. |
|
| Interventions | 1. CBT group: N = 34. Content: in collaboration with the patient an individual treatment plan including behaviour analyses is established and treatment goals are retrieved. This process of a ease formulation should be completed until session 9. Afterward, specific cognitive disputing strategies such as work on delusions (e.g. debating persecutory delusions; testing beliefs), hallucinations (e.g. use of a voice diary; work on reattribution with the patient's explanation of voice hearing, and test it out), and cognitive schemata (e.g. linking defectiveness schema to the content of the voices; confronting the patient with evidence that discredits the schema) are the central part of the CBT. Delivered by: conducted by 7 specifically trained female clinical psychologists. A mixture of trainees and experienced therapists. Frequency: 7 weekly session followed by 13 biweekly sessions. 50 minutes for individual sessions. Treatment duration (weeks): 12 session**. 2. Support therapy group: N = 33. Content: implicit problem‐solving, activation of external resources (social network), Stering of self‐confidence, and advice and instruction by the therapist to enhance a functional social behaviour. Delivered by: conducted by 7 specifically trained female clinical psychologists. A mixture of trainees and experienced therapists. Frequency: 7 weekly session followed by 13 biweekly sessions. 50 minutes for individual sessions. Treatment duration (weeks): 12 session. |
|
| Outcomes | Outcomes Satisfaction with treatment: leave the study early. Unable to use ‐ Therapeutic alliance: Patient Session Questionnaire (PSQ) , Therapist Session Questionnaire (TSQ) ‐ not predefined in our protocol. |
|
| Notes | Funding sources: the study was funded by the German Federal Ministry of Education and Research, project number 01GV0618. * only data from 67 completers were reported. * *The author of this review decided not to include therapy sessions beyond session 12 to our analyses as the treatment manuals do not bring new treatment interventions or techniques into focus in these later phases of treatment. Further, patient attrition was another reason to discontinue data analyses after the 12th session (p.479). |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote "randomly assigned" (p.479). Comments: insufficient information about the sequence generation process to permit judgement of 'Low risk' or 'High risk'. |
| Allocation concealment (selection bias) | Unclear risk | Comments: the author did not report the method. Insufficient information about the sequence generation process to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not report the method. Insufficient information about the sequence generation process to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote "Eight clinical psychologists who had been trained to sufficient reliability and were blind to treatment condition administered the PANSS" (p.480). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comments: 16 participants in CBT group and 17 participants in the ST group dropped out from the study. |
| Selective reporting (reporting bias) | Low risk | Comments: all measured outcomes were reported. |
| Other bias | Low risk | Comments: none obvious. |
NA ‐ Davis 2008.
| Methods | Allocation: randomised.
Blinding: not reported. Location: outpatient psychiatry service, India. Length of follow‐up: 12 months. |
|
| Participants | Diagnosis: Schizophrenia or schizoaffective disorder. Total: N = 45. Sex: Not reported. Age: Mean 47 years, SD 6.15 years. Length of illness: not reported. Inclusion criteria: not reported. Exclusion criteria: not reported. |
|
| Interventions | 1. Group and individual CBT group: (N = 25). Content: the weekly 1‐hour CBT group therapy intervention includes presentation of didactic material, exercises designed to apply didactic material to participants' experiences at work and work feedback. The weekly 30‐ to 45‐minute individual CBT sessions offer personalised application of group material. Delivered by: not reported. Frequency (times): once peer week. 2. Support group: (N = 19). Content: weekly support group that lasts up to an hour and offers support and discussion of work‐related issues brought up by participants. Delivered by: not reported. Frequency (times): once peer week. Treatment duration: 6 months. |
|
| Outcomes | Unable to use ‐ Satisfaction with treatment: recipient of care average satisfaction score‐Client satisfaction Questionaire‐8 (CSQ‐8). The author did not report the number of participants contributed data for this assessment. the Program Satisfaction Interview (PSI). we will use peer‐reviewed scale only. The PSI is an interview developed by the study authors using evaluation questionnaires as a model. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "a randomised controlled feasibility study."(p.55). Comments: the author did not describe the method of randomisation. |
| Allocation concealment (selection bias) | Unclear risk | Comments: insufficient information about the sequence generation process to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of outcome assessor. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comments: the author did not report number of participants leaving the study early. |
| Selective reporting (reporting bias) | Low risk | Comments: the author reported all measured outcomes. |
| Other bias | Low risk | Comments: none obvious. |
NA ‐ Drury 2000.
| Methods | Allocation: randomised.
Blinding: double‐blind. Location: inpatients, All Saint Hospital in Biringham. Length of follow‐up: 4 years. |
|
| Participants | Diagnosis: schizophrenia, schizoaffective, or delusional disorder (DSM‐IV).
N = 62. Sex: 25 M, 15 F, 22 unknown. Age: mean ˜ 30 years, SD ˜ 9, range 20‐55. History: length of illness ˜ 6.1 years, SD ˜ 8.3 years. Excluded: medication non compliance, first episode, not reporting psychotic symptoms . |
|
| Interventions | 1. CBT group: N = 30. Content: individual, challenging and testing key beliefs, group cognitive therapy, family engagement and coping strategy enhancement + standard care. Delivered by: not reported. Frequency: individual cognitive therapy and group cognitive therapy were administered for an average of 3 hours per week with daily input; family engagement and a structured activity programme required an average 5 hours per week. 2. Recreation and support group: N = 32. * Content: leisure and social activities away from ward + standard care. Delivered by: not reported. Frequency: not reported. Treatment Duration: 18 months. |
|
| Outcomes | General state: relapse, rehospitalisation
Mental state: no clinically important change ( personal recovery from positive symptoms (using definition 2 above), recovery of insight (score >9 on the Insight Scale and a score of < 30 on the Early Signs Scale‐ a validated scale of non‐specific prepsychotic symptoms).
Satisfaction with treatment: leaving the study early. Unable to use ‐ Mental state: specific symptoms‐PAS (data reported were derived from ANOVAs analysis with baseline variable as covariate, no extractable data) Average use of antipsychotic medication (data skewed). |
|
| Notes | * Review authors consider recreation and support to be a non active therapy. Authors contacted for further data. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comments: random allocation, using stratified sampling technique. |
| Allocation concealment (selection bias) | Low risk | Quote: "Randomisation was conducted by an independent member of the research team." (p.8). Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Neither patients nor consultants were aware of group allocation other than that they would be receiving a supportive recovery programme." (p.595) Comments: participants and therapists did not know the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Measures were administered either by an assistant psychologist who was not involved in the original trail, or by the first author. Neither patients nor consultants were aware of treatment group, but both were blind to relapse and rehospitalization." (p.9). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: completer analysis of outcomes. No intention to treat analysis of people who left early. |
| Selective reporting (reporting bias) | High risk | Comments: the data were only reported in graphical form. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
NA ‐ Haddock 2009.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: 19 outpatients, 58 inpatients, five National Health Service trusts in the North West of England. Length of follow‐up: 6 weeks, and 12‐months. |
|
| Participants | Diagnosis: schizophrenia or schizoaffective disorder (DSM‐IV).
N = 77. Sex: 66 M,11 F. Age: mean˜ 35.7 years, SD ˜12.5 years. Histroy: history of violent behaviour defined as follows: either (i) at least two recorded incidents of violence to property or others in 12 months prior to trial entry, or (ii) at least three recorded incidents of verbal aggression threatening violence to property or others in 12 months prior to trial entry, or (iii) for participants in secure care, one recorded violent index offence plus an indication that the individual was at risk of further violence without the protective effect of the treatment setting . This was rated by the responsible medical officer or care co‐ordinator using the Security, Dependency, Treatment and Political Needs Assessment Scale; experiencing persistent hallucinations and/or delusions scoring four or more on the relevant PANSS sub‐scales (P1 and P3); receiving antipsychotic medication (dose between 400 mg and 1000 mg chlorpromazine or equivalent) ascertained from detailed case‐note review. Excluded: not reported. |
|
| Interventions | 1. CBT group: N = 38. Content: motivational strategies to aid engagement, to reduce severity and distress of psychotic symptoms and severity of anger linked to aggression and violence. Delivered by: therapists who carried out the CBT programme met the British Association of Behavioural and Cognitive Psychotherapies' Minimum Training Standards for the practice of CBT and had prior experience of applying CBT for people with psychosis. Frequency: 25 sessions. 2. Social activities therapy group: N = 39. Content: helping identify and carry out enjoyable activities. Delivered by: trained therapists. Frequency: 25 sessions. Treatment duration: 6 months. |
|
| Outcomes | Global state: GAF scores. Mental state: PANSS, PSYRATS, NAS, PI, WARS, HCR‐20. | |
| Notes | Therapy manual developed for each treatment. Audio tapes of sessions assessed by supervisors using the Cognitive Therapy Scale for Psychosis, SAT tapes also rated to ensure no CBT used by presence of non‐specific therapeutic quality standards. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: " Randomised with computer‐generated sequences." (p.153). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "Independent allocation". (p.153). Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Masking maintained by ensuring therapists and assessors were housed in separate accommodation, therapy files were kept separately from data and clinical staff was repeatedly instructed not to disclose any knowledge of therapy group to assessors.". (p.153). Comments: participants and personnel were blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Masking maintained by ensuring therapists and assessors were housed in separate accommodation, therapy files were kept separately from data and clinical staff was repeatedly instructed not to disclose any knowledge of therapy group to assessors.". (p.153). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: intention‐to‐treat analysis undertaken. |
| Selective reporting (reporting bias) | Low risk | Comments: We did not have the study protocol but see no indication of selective reporting. |
| Other bias | High risk | Comments: different samples (i.e. inpatient and outpatient) and therefore opportunities to observe base rates of violent behaviour will vary as a function of sample. |
NA ‐ Jackson 2008.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: Early Psychosis Prevention and Intervention Centre, Melbourne, Australia. Length of follow‐up: 14 weeks, 1 year. |
|
| Participants | Diagnosis: people experiencing a first episode of psychosis.
N = 62. Sex: 45 M, 17 F. Age: mean ˜ 22 years, SD ˜ 3‐4 years. History: length of illness: CBT = 83 (untreated) days, befriending = median 107 (untreated) days. Excluded: unable to speak English, IQ < 70, psychosis due to medical condition, change to non‐psychotic diagnosis, treatment from private psychiatrist/psychologist, participating in first‐episode mania trial, exhibiting violent behaviour, or being incarcerated. |
|
| Interventions | 1. CBT group: N = 31. Content: manualised ‐ assessment and formulation of relationship between psychotic and non‐psychotic complaints and participants' life history, treatment prioritised in order of the following; risk, distressing positive symptoms, comorbidity, negative symptoms, issues of identity and relapse prevention. Delievered by: the therapists received 3 months of training in the treatments and were supervised throughout the trial. Frequency: a maximum of 20 X 45‐minute sessions over 14 weeks. 2. Befriending group: N = 31. Content: based on NA ‐ Sensky 2000 ‐ a non active therapist contact control, "befriending aims to control for time in therapy, participant expectations and positive experiences of therapy". Delievered by: the therapists received 3 months of training in the treatments and were supervised throughout the trial. Frequency: not reported. Treatment duration: 14 weeks. |
|
| Outcomes | Gobal state: rehospitalisation. Mental state: Psychotic sub‐scale of SANS (skewed data), positive symptoms ‐ BPRS (skewed data). Social functioning: SOFAS. Adverse effect/event: death. Satisfaction with treatment: leaving the study early. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Randomization was stratified according to affective and non‐affective psychotic diagnosis to ensure equal distribution across therapists and treatment conditions." (p.727). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "Allocation was conducted by independent statistician."(p.727). Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Quote: "participants who were aware of the therapy condition to which they had been allocated." (p.282). Comments: participants knew the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comments: single ‐ raters blind to allocated treatment. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Quote: "Missing values in each of the outcome measures for any individual at time points subsequent to baseline were assumed to have occurred at random, given observed pretreatment scores. Multiple Imputation was used to compensate for missing data." (p.729). Comments: measures were taken to deal with the missing data. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | High risk | Imbalanced baseline: the participant group contained fewer patients with schizophreniform disorder (40.3%) than expected by chance (refusers = 62.7%). There were also significantly more patients with schizoaffective disorder in the participant group (11.3%) than in the refuser group (1.6%). |
NA ‐ Kemp 1998.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: a ward of the Maudsdey Hospital, London. Length of follow‐up: post intervention, three and 18 months after discharge. |
|
| Participants | Diagnosis: schizophrenia, schizoaffective, delusional disorder (DSM III‐R).
N = 74. Sex: 23 M, 24 F, 27 unclear. Age: 18 ‐ 65 years; mean ˜ 35 years, SD ˜ 12 years. History: length of illness: mean ˜8.4 years, SD ˜6.4 years (data were based on 47 patients). acute psychosis over eight months, admitted to a ward of the Maudsley Hospital. Excluded: non‐English speakers, learning disability, deaf, organic brain disease. |
|
| Interventions | 1. CBT group: N = 39. Content: psychoeducation + compliance therapy + standard care. Compliance therapy: In the first two sessions of compliance therapy patients were invited to review their history of illness and conceptualise the problem. In the next two sessions discussion became more specific, focusing on symptoms and the side effects of treatment. In the last two sessions, the stigma of drug treatment was tackled by considering that drugs are a freely chosen strategy to enhance the quality of life. Delivered by: a research psychiatrist with additional help from a clinical psychologist. Frequency: 4‐6 sessions (mean 5.1) of compliance therapy, lasting 20‐60 minutes roughly twice a week. 2. Control group: N = 35. Content: non‐specific counselling + standard care. Delivered by: a research psychiatrist with additional help from a clinical psychologist. Frequency: 4‐6 sessions. Treatment duration: 2‐3 weeks intervention plus boosters till 12 months. |
|
| Outcomes | Global state: GAF score. Mental state: BPRS score. Satisfaction with treatment: Drug Attitude Inventory (DAI), Attitudes to Medication Questionnaire (AMQ), leaving the study early. Unable to use ‐ Insight: Shedule for Assessment of Insight (SAI) (skewed data). Compliance measure (scale not peer‐reviewed). |
|
| Notes | The main focus of the intervention was on medication compliance. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Patients were randomly assigned by means of a table of random numbers to compliance therapy or control treatment." (p.3). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Unclear risk | Comments: no information reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "The evaluations at six months were carried out by an independent assessor blinded to the intervention." (p.5). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Comments: overall, 35% were lost during the follow‐up period (28%) from the compliance therapy group and 15 from the control group (43%). |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
NA ‐ Lewis 2002.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: Manchester/Salford, Liverpool and north Nottinghamshire, in England. Length of follow‐up: at 70 days, and 18‐months. |
|
| Participants | Diagnosis: schizophrenia, schizophreniform disorder, schizoaffective disorder or delusional disorder (DSM IV).
N = 309.* Sex: 216 M, 93 F. Age: mean ˜ 27.4 years. History: in acute phase, first or second acute admission; positive psychotic symptoms for 4 weeks or more; score of 4 or more (moderate or severe) on the PANSS target item either (P1) or hallucinations (P3); neither substance misuse nor organic disorder judged to be the major cause of psychotic symptoms. Excluded: not reported. |
|
| Interventions | 1. CBT group: N = 101. Content: CBT + routine care. Delivered by: five therapists trained in CBT in psychosis. Frequency: the delivery was to aim for 15–20 hours within a 5‐week treatment envelope, plus 'booster' sessions at a further 2 weeks and 1, 2 and 3 months. 2. Supportive counselling group: N = 106. Content: supportive counselling + routine care. Delivered by: not reported. Frequency: it was delivered in the same 5‐week format with three boosters. 3. Routine care group: N = 102. Content: routine care. Treatment duration: 5 weeks plus further 3‐month booster. |
|
| Outcomes | Global state: relapse, rehospitalisation.
Mental state: PANSS, hallucination ‐ PSYRATS, delusional ‐ PSYRATS (skewed data). Adverse effect/event: death. Satisfaction with treatment: leaving the study early. |
|
| Notes | * 315 participants were randomised, however, six people were excluded after randomisation. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "Independent, concealed randomisation ofIndependent, concealed randomisation of individuals with minimisation was then individuals with minimisation was then performed by a trial administrator at each performed by a trial administrator at each centre. " (p. s92). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Comments: described as "concealed". |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comments: raters blind to treatment allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: intention‐to‐treat regressional analysis. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
NA ‐ Lewis 2002 (L).
| Methods | see NA ‐ Lewis 2002. | |
| Participants | Diagnosis: schizophrenia (DSM IV). N = 114. | |
| Interventions | see NA ‐ Lewis 2002. | |
| Outcomes | Global state: hospital admission* Mental state: PANSS, delusional sub scale ‐ PSYRATS* Adverse effect/event: death. Satisfaction with treatment: leaving the study early. |
|
| Notes | This is one centre in the NA ‐ Lewis 2002 study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | see NA ‐ Lewis 2002. |
| Allocation concealment (selection bias) | Low risk | see NA ‐ Lewis 2002. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | see NA ‐ Lewis 2002. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | see NA ‐ Lewis 2002. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | see NA ‐ Lewis 2002. |
| Selective reporting (reporting bias) | Low risk | see NA ‐ Lewis 2002. |
| Other bias | Low risk | see NA ‐ Lewis 2002. |
NA ‐ Lewis 2002 (M).
| Methods | see NA ‐ Lewis 2002. | |
| Participants | Diagnosis: schizophrenia (DSM IV). N = 112. | |
| Interventions | see NA ‐ Lewis 2002. | |
| Outcomes | Global state: hospital admission*. Adverse effect/event:dDeath*. Mental state: PANSS. Satisfaction with treatment: leaving the study early*. | |
| Notes | * This is one centre in the NA ‐ Lewis 2002a study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | see NA ‐ Lewis 2002. |
| Allocation concealment (selection bias) | Low risk | see NA ‐ Lewis 2002. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | see NA ‐ Lewis 2002. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | see NA ‐ Lewis 2002. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | see NA ‐ Lewis 2002. |
| Selective reporting (reporting bias) | Low risk | see NA ‐ Lewis 2002. |
| Other bias | Low risk | see NA ‐ Lewis 2002. |
NA ‐ Lewis 2002 (N).
| Methods | see NA ‐ Lewis 2002. | |
| Participants | Diagnosis: schizophrenia (DSM IV). N = 83. | |
| Interventions | see NA ‐ Lewis 2002. | |
| Outcomes | Global state: hospital admission*
Mental state: PANSS, PSYRATS (delusional scale)*. Adverse effect/event: death*. Satisfaction with treatment: leaving the study early.* |
|
| Notes | This is one centre in the NA ‐ Lewis 2002a study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | see NA ‐ Lewis 2002. |
| Allocation concealment (selection bias) | Low risk | see NA ‐ Lewis 2002. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | see NA ‐ Lewis 2002. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | see NA ‐ Lewis 2002. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | see NA ‐ Lewis 2002. |
| Selective reporting (reporting bias) | Low risk | see NA ‐ Lewis 2002. |
| Other bias | Low risk | see NA ‐ Lewis 2002. |
NA ‐ Li 2015.
| Methods | Allocation: randomised with random number table.
Blinding: unclear. Location: China . Length of follow‐up: 8 weeks. |
|
| Participants | Diagnosis: schizophrenia, diagnosed with ICD‐10.
N = 100. Sex: male and female (numbers not reported). Age: 18 ‐ 60 years. History: length of illness 3 month to 10 years, average around 5 years; illness condition and drug dosage relatively stable for at least two weeks; educated to middle‐school level or above; able to give informed consent. |
|
| Interventions | 1. CBT group: N = 50. Content: patients information and baseline condition was comprehensively collected and evaluated to pave the way for establishment of treatment plan. Towards hallucination, reasonable explanation was developed with patients to ease their anxiety; diary was kept for voices they heard; individual coping strategy was established. Similar process was followed to deal with delusion. Therapists generally adopted the process of identifying problem, establish a rational explanation, reinforce correct perception. Delivered by: not stated. Frequency: 30 to 40 minutes each session, 12 sessions in total. Twice/week for the first 4 weeks and once/week for the last 4 weeks. Treatment duration: 8 weeks. 2. Standard psychological support: N = 50. Content: patients' general information was obtained and changes in condition was monitored. They were allowed to communicate with nursing and clinical staff for 30 to 40 minutes each day. General psychoeducation was given. Delivered by: not clearly stated, but seems to be by nursing and ward clinicians. Frequency: 30 to 40 minutes each session, 12 sessions in total. Twice/week for the first 4 weeks and once/week for the last 4 weeks. Treatment duration: 8 weeks. |
|
| Outcomes | Mental state: PANSS positive, negative, general pathology and total scale score. Engagement with services: medication compliance. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comment: random number table was used. |
| Allocation concealment (selection bias) | Unclear risk | Comment: not stated. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: Not reported. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: not reported. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: no dropout. |
| Selective reporting (reporting bias) | Low risk | Comment: we did not have original study protocol, but there was no obvious selective reporting. |
| Other bias | Low risk | Comment: none obvious. |
NA ‐ O'Donnell 2003.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: St John of God Hospital, Dublin. Length of follow‐up: 12 months. |
|
| Participants | Diagnosis: schizophrenia (DSM III R).
N = 56. Sex: not reported Age: 18 ‐ 65 years; mean 32 years, SD 9 years. History: IQ greater than 80; fluent English speakers, no evidence of organic disturbance. Excluded: not reported. |
|
| Interventions | 1. CBT group: N = 28. Content: compliance therapy ‐ techniques adapted from motivational interviewing and other cognitive therapies as well as psychoeducation (based on manual from NA ‐ Kemp 1998a); Delivered by: unclear. Frequency: comprised five 30 to 60 minute sessions. 2. Non‐specific counselling group: N = 28. Content: if patients raised matters relating to medication, they were asked to discuss them with their treating teams. Freqency: five 30 to 60 minute sessions. Treatment duration: 5 sessions. |
|
| Outcomes | Global state: GAF score. Mental state: PANSS score. Adverse effect/event: death. Cognitive functioning: schedule for assessment of insight (SAI). Quality of life: the quality of life scale (Heinrichs 1984). Satisfaction: leaving the study early, satisfaction with treatment: attitude to medication. Engagement with service: compliance with medication*. |
|
| Notes | * Compliance with medication was assessed based on a four‐point‐scale: 1 (0% to 24% compliance = non‐ compliant or consistently irregular), 2 (25% to 49% compliance ‐ frequently irregular), 3 (50% to 74% compliance ‐ irregular), and 4 (75% to 100% compliance ‐ regular). The author of trial defined an optimal compliance as any participant who scored > 3. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "...randomly allocated consenting patients to compliance therapy or control groups using odd and even digits from a standard table of random numbers..." (p.2). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Unclear risk | Comments: insufficient details provided. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "A researcher who was blind to the type of intervention delivered repeated the assessments." (p.2). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: completer data reported. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
NA ‐ Sensky 2000.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: five clinical services, 2 in West London and 3 in the north of England Length of follow‐up: 9 months, 5 years. |
|
| Participants | Diagnosis: schizophrenia (ICD‐10 & DSM IV).
N = 90. Sex: 53 M, 37 F. Age: 16 ‐ 60 years. History: symptom(s) causing distress and/or dysfunction that had persisted for at least 6 months despite adequate trials of antipsychotic medication. Excluded: primary diagnosis of alcohol or drug abuse; current abuse of drugs or alcohol warranting specific clinical intervention, such as attendance at a specialist substance misuse clinic; exclusively negative symptoms; or not complaining of any positive symptoms or of depression. |
|
| Interventions | 1. CBT group: N= 46. Content: CBT + standard care. Delivered by: two experienced nurses who received regular supervision. Frequency: 20 sessions during 9 months period with 45 minutes per session . 2. Befriending group: N = 44. Content: non active therapist contact, focus is upon leisure activity + standard care. Delivered by: two experienced nurses who received regular supervision. Frequency: 20 sessions during 9‐month period with 45 minutes per session . Treatment duration: 9 months. |
|
| Outcomes | Global state: rehospitalisation. Mental state: clinically important change*, Comprehensive Psychiatric Rating Scale (CPRS), Montgomery‐Asburg Depression Rating Scale (MADRS), Scale for the Assessment of Negative Symptoms (SANS) Satisfaction with treatment: leaving the study early. |
|
| Notes | * Defined as the improvement between baseline and follow‐up evaluation of less than 50% in CPRS scores. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "The randomisation was conducted by members of the research team not involved with either the assessments or the treatments. " (p.166). "Randomisation for Insight trial was conducted from a remote centre by computer generated blocks of six random numbers and was stratified by the centre." (p.653). Comments: the investigators describe a random component in the sequence generation process. |
| Allocation concealment (selection bias) | Low risk | Quote: "The results were placed in sealed envelopes and only opened at the time of the treatment allocation. " (p.653). Comments: participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | High risk | Comments: only raters were blind to treatment condition. Participants and therapists knew the group assignment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comments: raters blind to treatment condition. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: intention‐to‐treat analysis undertaken. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
NA ‐ Turkington 2000.
| Methods | Allocation: randomised.
Blinding: double‐blind. Location: Sheffield Bassetlaw Hospital. Length of follow‐up: 6 months. |
|
| Participants | Diagnosis: schizophrenia (ICD‐10 & DSM III‐R).
N = 18.
Sex: 9 M, 9 F. Age: 16 ‐ 65 years. History: length of illness: mean 9.2˜13 years. Excluded: not reported. |
|
| Interventions | 1. CBT group: N = 12. Content: CBT + standard care. Delivered by: a psychiatrist. Frequency: sSix sessions for 2 months, each session lasted 20 to 40 minutes. 2. Befriending: N = 6. Cotent: non‐directive discussion around neutral topics + standard care. Treatment duration: 2 months. |
|
| Outcomes | Unable to use ‐
Mental state: MADRS (no SD).
Length of time in hospital (no SD). Mental state: CPRS (no SD). |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comments: reported random allocation, no detail provided. |
| Allocation concealment (selection bias) | Unclear risk | Comments: not reported. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Quote: "Patients assessor and clinical team remain blinded to the treatment allocation. " (p.103). Comments: participants and personnel were blinded. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Quote: "Patients assessor and clinical team remain blinded to the treatment allocation. " (p.103). Comments: the outcome assessor was blinded. |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Comments: no details provided. |
| Selective reporting (reporting bias) | High risk | Comments: data unable to be used due to failure to report SDs. |
| Other bias | Low risk | Comments: no clear indication of other bias. |
NA ‐ Valmaggia 2005.
| Methods | Allocation: randomised.
Blinding: single‐blind. Location: various mental health hospitals across the Netherlands and in one in Belgium. Length of follow‐up: Baseline, at 23 weeks, 6 month after intervention. |
|
| Participants | Diagnosis: schizophrenia (DSM‐IV).
N = 62. Sex: 41 M, female 21 F. Age: 18 ‐ 70 years. History: residual delusions or auditory hallucinations experienced for at least 3 months; a stable medication regimen (last medi‐cation change more than 6 weeks prior to recruitment). Excluded: conceptual disorganisation; stereotypic thinking; disorientation, measured by the Positive and Negative Syndrome Scale (PANSS), item P2 >=4, N7>=3, G10>=2; drug or alcohol addiction as a primary diagnosis (patients using drugs or alcohol below the level of this criterion were included); mental retardation (premorbid IQ<80); organic conditions; cognitive–behavioural therapy given for persistent psychotic symptoms in the past. |
|
| Interventions | 1. CBT group: N = 36. Content: Manualised, therapy begins with engagement phase emphasising collaboration, focuses on delusional distress; second phase ‐ shared case formulation is identified, specific techniques used for symptom and distress reduction. With auditory hallucinations aim is to change beliefs about origin, power and dangerousness of voices. In delusions, focus is on challenging dysfunctional beliefs and learning to make more balanced conclusions; last phase ‐ treatment focuses on relapse prevention strategies. * Delivered by: Experienced psychologists. Frequency: Sessions 1‐12 took place once a week, sessions 13‐15 every 2place once a week, sessions 13‐15 every 2 weeks and session 16 after 4 weeks. 2. Supportive counselling group: N = 26. Content: conventional method previously used in other studies (e.g., NA ‐ Lewis 2002a). Treatment duration: 22 weeks. |
|
| Outcomes | Global state: relapse. Mental state: PANSS score. Satisfaction: leaving the study early. |
|
| Notes | * The therapist shows non‐critical acceptance, warmth, genuineness and empathy. Focus of intervention was preferably identified by patient, however if patient experiences difficulties identifying therapeutic targets then therapist could ask questions about current living circumstances, illness and current problems, daily routine, social contacts, family, and personal history. In addition, intervention offered patients psychoeducation about schizophrenia. The authors state that "To control for non‐specific therapy and therapist effects, cognitive–behavioural therapy was compared with supportive counselling plus psycho‐education". Accordingly, this use of supportive counselling was considered as an non active therapy. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Comments: Randomisation was based on drawing lots. |
| Allocation concealment (selection bias) | Low risk | Quote: "To ensure the anonymity of participants, each individual was given a code, and coordinator used form to communicate results of random assignment to local therapist." Comments: Participants and investigators enrolling participants could not foresee assignment. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comments: The author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Comments: Raters blind to allocation. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comments: Intention‐to‐treat analysis undertaken. |
| Selective reporting (reporting bias) | Low risk | Comments: We did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comments: No clear indication of other bias. |
NA ‐ Zhang 2015.
| Methods | Allocation: randomised.
Blinding: not report. Location: China. Length of follow‐up: 24 weeks. |
|
| Participants | Diagnosis: schizophrenia, diagnosed with ICD‐10.
N = 198. Sex: male and female (numbers not reported). Age: 18 ‐ 60 years. History: length of illness > 5 years. PANSS score > 60 HAMD score >17 <24; ability to give informed consent; educated to middle school level or above. Excluded: severe physical impairment; certain PANSS sub scale score is higher than 5; received ECT in the 30 minutes prior to CBT session. |
|
| Interventions | 1. CBT group: N = 99. Content: three stages and each with distinctive therapeutic goals. Therapy programme was developed with clear focus of each stage and homework was allocated. Initially therapeutic relationship was established by investigating patients feeling towards illness stigma and their perception of the illness. During second stage, CBT techniques were employed to correct the misconception and to incept positive thought model and coping strategy. In final stage, previous learning was reinforced and consolidated. Delivered by: trained psychiatrist provided CBT training to therapists in the study ( a total of 140 hours of systematic training). Frequency: 46 minutes to 1 hour per session, 15 therapy sessions delivered in 24 weeks. . Treatment duration: 24 weeks. 2. Supportive therapy: N = 99. Content: not stated Delivered by: trained psychiatrist provided CBT training to therapists in the study ( a total of 140 hours of systematic training). Frequency: 46 minutes to 1 hour per session, 15 therapy sessions delivered in 24 weeks. . Treatment duration: 24 weeks. |
|
| Outcomes | Unable to use‐ CSQ score was reported, but the scale was not peer‐reviewed or validated. |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Comment: randomised, no further detail. |
| Allocation concealment (selection bias) | Unclear risk | Comment: the author did not describe the allocation concealment. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Comment: the author did not describe the blinding of participants and personnel. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Comment: the author did not describe the blinding of outcome assessor. Insufficient information to permit judgement of 'Low risk' or 'High risk'. |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Comment: 14 patients and 14 patients dropped out of CBT and supportive therapy group respectively, but the number who dropped out was balanced and did not affect on the CSQ average score significantly. |
| Selective reporting (reporting bias) | Low risk | Comments: we did not have the study protocol but see no indication of selective reporting. |
| Other bias | Low risk | Comment: none obvious. |
BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory; BPRS: Brief Psychiatric Rating Scale; CBSST: Cognitive Behavioral Social Skills Training; CBT: Cognitive behavioural therapy; DSM IV: Diagnostic and Statistical Manual, 4th edition; GAF: Global Assessment of Functioning; GAS: Global Assessment Scale; HAMD: Hamilton Rating Scale for Depression; ICD 10: International Classification of Diseases; KC: Key‐person counselling; MADRS:Montgomery‐Asberg Depression Rating Scale; PANSS: Positive and Negative Syndrome Scale; PAS: Psychiatric Assessment Scale; PMT: Psychoeducational medication training; PSRS: Psychotic Symptom Rating Scale; RSES: Rosenberg Self‐Esteem Scale; SANS: Scale for the Assessment of Negative Symptoms; SD: standard deviation; SE: standard error; SFS: Social Functioning Scale; SOFAS: Social and occupational functioning; WARS: Ward Anger Rating Scale.
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Anzai 2002 | Allocation: randomised. Participants: people with schizophrenia. Intervention: community re‐entry model versus conventional occupational rehabilitation program, not CBT. |
| Arlow 1997 | Allocation: not randomised, case series. |
| Bach 2002 | Allocation: randomised. Participants: people with schizophrenia. Intervention: Acceptance and Commitment Therapy compared with treatment as usual; no other psychological therapy. |
| Barrowclough 2001 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Barrowclough 2006 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Bechdolf 2005b | Allocation: uncontrolled prospective design with pre‐ and post‐treatment measures. |
| Bellucci 2002 | Allocation: randomised. Participants: people with schizophrenia. Intervention: computer‐assisted cognitive rehabilitation versus a 'wait‐list' control group, not CBT. |
| Bouchaud 1996 | Allocation: not randomised trial, review. |
| Bradshaw 1993 | Allocation: randomised. Participants: people with schizophrenia. Intervention: Coping‐skills training versus problem‐solving approach, not CBT. |
| Bradshaw 2000 | Allocation: randomised.
Participants: people with schizophrenia.
Intervention: Day Treatment Program plus CBT versus Day Treatment Program The Day Treatment Program incorporated active psychological treatments (e.g., social skills training, independent living skills groups, goal groups, occupational and recreational therapy, prevocational employment training and medication management). However, these active treatments in the comparison condition were also mirrored in the CBT condition, such that the study did not provide a differential test of CBT versus other psychological therapies. |
| Browning 2013 | Study design: patients were sequentially allocated to treatment groups. |
| Buchanan 1992 | Allocation: not randomised, case series. |
| Castle 2002 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT versus waiting list controls. |
| Chadwick 1994 | Allocation: not randomised, case series and review. |
| Claghorn 1974 | Allocation: randomised. Participants: people with schizophrenia. Interventions: group dynamic therapy + chlorpromazine or thiothixene versus chlorpromazine or thiothixene ‐ not described as cognitive therapy. |
| Daniels 1998 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Drake 1993 | Allocation: not randomised; review article. Participants: mixed diagnostic categories. Intervention: social network treatment versus treatment as usual, not CBT. |
| Edwards 2003 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT + thioridazine versus clozapine. |
| England 2007 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Evins 2001 | Allocation: randomised. Participants: People with schizophrenia. Interventions: CBT + bupropion versus CBT. |
| Fritze 1988 | Allocation: randomised. Participants: people with schizophrenia. Interventions: rehabilitation of intellectual disabilities versus standard care, not CBT. |
| Garety 1994 | Allocation: not randomised. |
| Garety 1998 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Gaudiano 2006 | Allocation: randomised. Participants: people with schizophrenia. Intervention: Acceptance and Commitment Therapy compared with treatment as usual; no other psychological therapy. |
| Granholm 2005 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Grawe 2006 | Study design: randomised controlled trial. Participants: schizophrenia or schizophrenia disorder. Intervention: integrated treatment involving skill training, CBT and standard treatment versus standard treatment. |
| Gumley 2003 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Haldun 2002 | Allocation: randomised. Participants: people with schizophrenia Intervention: CBT + family therapy + case management + education + medication versus medication + education. |
| Hartman 1983 | Allocation: not randomised. |
| Hayward 1995 | Allocation: randomised. Participants: people with schizophrenia. Intervention: medication self‐management using motivational interviewing versus standard care. Not CBT. |
| Hayward 2009 | Allocation: randomised.
Participants: people with schizophrenia. Intervention: Alliance Enhancement Therapy (AET) + psychoeducation + clozapine versus psychoeducation + clozapine. |
| Herz 2000 | Allocation: randomised Participants: outpatients with schizophrenia Intervention: Program for Relapse Prevention (PRP) is more effective than treatment as usual (TAU). Not CBT. |
| Hodel 1994 | Allocation: not randomised. |
| Hogarty 1991 | Allocation: not randomised. |
| Hogarty 1997 | Allocation: randomised.
Participants: persons with schizophrenia.
Intervention: personal T therapy, not CBT. |
| Hogarty 2004 | Allocation: randomised. Participants: people with schizophrenia. Intervention: cognitive remediation for cognitive (intellectual) deficits, not CBT. |
| Jackson 1998 | Allocation: not randomised. |
| Jackson 2001 | Allocation: randomised. Participants: people with schizophrenia. Intervention: cognitive therapy versus treatment as usual. |
| Kemp 1996b | Allocation: not randomised, case series. |
| Kingdon 1991 | Allocation: not randomised, case series. |
| Kuipers 1996 | Allocation: not randomised, review. |
| Kuipers 2004 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Kukla 2014 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT versus a control condition on work performance. Outcomes: no usable data. |
| Lecompte 1996 | Allocation: randomised. Participants: people with schizophrenia. Intervention: medication compliance versus unstructured conversations. Outcomes: no usable data. |
| Lysaker 2009 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| MacPherson 1996 | Allocation: randomised. Participants: people with schizophrenia. Intervention: education programme based on bibliotherapy versus standard care, not CBT. |
| May 1984 | Allocation: not randomised trial, review. |
| McGorry 2002 | Allocation: randomised. Participants: people at risk of developing schizophrenia. Intervention: needs‐based intervention with no antipsychotic versus specific intervention of CBT + risperidone, not CBT alone. |
| Morrison 2002 | Allocation: randomised. Participants: people at incipient risk of psychosis, not schizophrenia |
| O'Connor 2007 | Allocation: randomised. Participants: people with delusional disorder. |
| Olbrich 1990 | Allocation: randomised. Participants: people with schizophrenia. Intervention: skills training aimed at cognitive deficits versus standard care, not CBT. |
| Perris 1992 | Allocation: not randomised, case series. |
| Rector 2003 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Roder 2002 | Allocation: not randomised. Participants: mixed diagnoses of schizophrenia and schizoaffective disorder Intervention: residential social skills training versus vocational social skills training versus recreational social skills training versus general social skills training, not CBT. |
| Sellwood 2001 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Shawyer 2012 | Allocation: randomised. Participants: schizophrenia or related condition based on DSM‐IV criteria with command hallucination. Interventions: CBT + Acceptance and Commitment Therapy + mindfulness exercise versus befriending. |
| Shon 2002 | Allocation: not randomised, ABA design. |
| Spaulding 1992 | Allocation: not randomised, case series. |
| Startup 1998 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Startup 2006 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Tarrier 1993 | Allocation: randomised. Participants: people with schizophrenia. Interventions: problem‐solving (CBT focusing on social disability + daily living difficulties) + standard care versus coping strategy enhancement (CBT focusing on positive symptoms) + standard care; in addition, also allocated within group to waiting list or not. No control arm. Outcomes: leaving the study early, mental state (BPRS, PAS), self‐perception, completer data only ‐ numbers initially allocated to each group not reported. Authors are being contacted. |
| Turkington 2002 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Turkington 2006 | Allocation: randomised. Participants: people with schizophrenia. Intervention: CBT compared with treatment as usual; no other psychological therapy. |
| Van Der Gaag 2003 | Allocation: randomised. Participants: people with schizophrenia. Intervention: cognitive remediations program versus participation in a leisure program, not CBT. |
| Velligan 2002 | Allocation: randomised. Participants: people with schizophrenia. Intervention: cognitive adaption training versus, patient environmental changes versus treatment as usual, not CBT. |
| Wirshing 1992 | Allocation: randomised. Participants: people with schizophrenia. Interventions: CBT + standard care (cognitive restructuring, behavioural rehearsal/role play, coping‐strategy enhancement, problem‐solving) versus group psychotherapy + standard care (insight oriented psychotherapy group + education re schizophrenia). Outcomes: leaving the study early, mental state (BPRS, SANS). ‐ data presented for 41 people who completed 12 months ‐ numbers initially allocated to each group not reported. |
| Wykes 2002 | Allocation: randomised. Participants:people with schizophrenia. Intervention: rehabilitation of intellectual disabilities, not CBT. |
| Wykes 2003 | Allocation: randomised. Participants: people with schizophrenia. Intervention: group CBT versus standard care, not other psychological therapy. |
| Xie 2010 | Study design: randomised controlled trial. Participants: schizophrenia. Intervention: cognitive therapy + antipsychotic versus standard psychological treatment + antipsychotics. |
BPRS: Brief Psychiatric Rating Scale; CBT: Cognitive behavioural therapy; DSM IV: Diagnostic and Statistical Manual, 4th edition; PAS: Premorbid Adjustment Scale; PRP: program for relapse prevention; SANS: Scale for the Assessment of Negative Symptoms; TAU: treatment as usual.
Characteristics of studies awaiting assessment [ordered by study ID]
Chung 2001.
| Methods | Awaiting for translation (Korean). |
| Participants | Awaiting for translation (Korean). |
| Interventions | Awaiting for translation (Korean). |
| Outcomes | Awaiting for translation (Korean). |
| Notes | Awaiting for translation (Korean). |
Clarke 2011.
| Methods | Allocation: Quote "randomly assigned" (p.1) Blinding:Quote " All patients were rated fortnightly by an independent rater..." (p.1). Duration: Quote "10 weeks" (p.1). Location: not reported. Length of follow‐up: not reported.. |
| Participants | Diagnosis: schizophrenia with symptoms of depression and hopelessness and who rated spirituality as important to them. Total: N = 42. Sex: not reported. Age: not reported. Length of illness: not reported. Inclusion criteria: not reported. Exclusion criteria: not reported. |
| Interventions | CBT Group: a clinician trained in using Spiritually Augmented Cognitive Behaviour Therapy (SACBT) Case management Group: a case manager who offered supportive case management. All patients were prescribed atypical antipsychotic medication. Both groups were seen for 14 sessions over 10 weeks. |
| Outcomes | MADRS instrument. Quality of Life in Depression instrument. Treatment attitude, beliefs and adherence were monitored fortnight. |
| Notes | Awaiting for full texts. |
D'Souza 2002.
| Methods | Allocation: randomly assigned.
Blinding: Quote: " All patients were rated fortnightly by an independent rater..." (p.1).
Duration:10 weeks. Location: not reported. Length of follow‐up: not stated. |
| Participants | Diagnosis: schizophrenia with symptoms of depression and hopelessness and who rated spirituality as important to them. Total: N = 42. Sex: not reported. Age: not reported. Length of illness: not reported. Inclusion criteria: not reported. Exclusion criteria: not reported. |
| Interventions | Awaiting for full texts. |
| Outcomes | Awaiting for full texts. |
| Notes | Author's name: R. D' Souza, D. Rich, I. Diamond, K. Godfery Insititute: Centre for Excellence in Remote and Rural Psychological Medicine. Address: University of Sydney Broken Hill Base Hospital, Australia Email: unclear. |
Delahaye 2009.
| Methods | Awaiting for translation. |
| Participants | Awaiting for translation. |
| Interventions | Awaiting for translation. |
| Outcomes | Awaiting for translation. |
| Notes | Awaiting for translation. |
ISRCTN60855021 2009.
| Methods | Allocation: Quote:" single centre randomised interventional treatment pilot/feasibility study"(p.1).
Blinding: not reported.
Duration: not reported. Location: not reported. Length of follow‐up: 6 months. |
| Participants | Diagnosis: psychosis. Total: N = 48. Sex: not reported. Age: not reported. Length of illness: not reported. Inclusion criteria: 1. Score above 30 on the Social Interaction Anxiety Scale (SIAS); 2. Early Intervention Service user; 3. Aged 14 years and above, either sex Exclusion criteria: current acute psychotic episode |
| Interventions | Standard therapy group. Enhanced behavioural therapy group. |
| Outcomes | Social Anxiety Interaction Scale Paranoia Scale Brief Core Schema Scale |
| Notes | Awaiting for full text. Contact author for clarification about patients and interventions. Author's name: Dr Ruth Turner Insititute: Address: Norfolk and Waveney Mental Health NHS Foundation Trust 80 St. Stephens Road. NR1 3RE Email: ruth.turner@nwmhp.nhs.uk |
Jones 2012.
| Methods | Allocation: randomised.
Blinding: not reported.
Duration: not reported. Location: not reported. Length of follow‐up: not reported. |
| Participants | Diagnosis: schizophrenia. Total: N = 48. Sex: not reported. Age: not reported. Length of illness: not reported. Inclusion criteria: a diagnosis of schizophrenia as determined with the Structured Clinical Interview Patient Version (SCID‐P16) for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM‐IV) which should have been obtained a maximum of 5 years before commencement of the study. Exclusion criteria: participants will be excluded from the study if they exhibit current DSM‐IV substance abuse or dependence (other than nicotine) and/or a current or past neurological condition or disorder including epilepsy or head trauma with loss of consciousness. |
| Interventions | Awaiting for more information. |
| Outcomes | Social Anxiety Interaction Scale. Paranoia Scale. Brief Core Schema Scale. |
| Notes | Contact information University of Cambridge Department of Psychiatry Herchel Smith Buidling for Brain & Mind Sciences, Forvie Site, Robinson Way Cambridge CB2 0SZ UNITED KINGDOM Tel: 01223 336 798 Email: gjs46@medschl.cam.ac.uk |
Klingberg 2001.
| Methods | Awaiting for translation (Germany). |
| Participants | Awaiting for translation (Germany). |
| Interventions | Awaiting for translation (Germany). |
| Outcomes | Awaiting for translation (Germany). |
| Notes | Awaiting for translation (Germany). |
Klingberg 2013.
| Methods | Allocation: Quote: " Allocation sequence will be generated by the Institute for Medical Biometry (IMB) applying a permuted block design with random blocks stratified by study centre and medication compliance" (p.5).
Blinding: Quote: " The therapist will open the envelope and will find the treatment condition to be conducted in this patient…The therapist then gives the information about treatment allocation to the patient…. randomisation will be conducted by CenTrial in order to keep the data management and the statistician blind against the study condition…. the raters will instruct the patient not to reveal their treatment condition and not to talk about details of their treatment.." (p.5). Duration: 36 weeks. Location: inpatient and outpatient. Length of follow‐up: 9 months. |
| Participants | Diagnosis: schizophrenia (DSM‐IV 295.1, 295.2, 295.3, 295.6, 295.9), schizophreniform disorder (DSM IV, 295.4), schizoaffective disorder (DSM‐IV 295.7), or delusional disorder (DSM IV 297.1). Total: N = 330. Sex: not reported. Age: not reported. Length of illness: not reported. Inclusion criteria: schizophrenia (DSM‐IV 295.1, 295.2, 295.3, 295.6, 295.9), schizophreniform disorder (DSM IV, 295.4), schizoaffective disorder (DSM‐IV 295.7), or delusional disorder (DSM IV 297.1), confirmed by a structured clinical interview (SCID‐I). Essential for inclusion is moderate or severe symptom intensity, i.e., a score of 4 or more, on the PANSS‐items “Delusions” (P1) or “Hallucinations” (P3). Furthermore, the presence of positive symptoms for at least three months with or without compliance regarding antipsychotic education is necessary. Other inclusion criteria are fluency regarding the German language, age between 18 and 59, a verbal IQ > 80 assessed by a multiple choice vocabulary test, and willingness to give informed consent. Exclusion criteria: any kind of organic brain diseases (other than schizophrenia) according to standard patient examination procedures and diagnosis of substance abuse or substance dependence according to DSM‐IV/SCID‐I as primary clinical problem. |
| Interventions | 1. CBT Group: (N = 165). Content: engagement (strategies to foster motivation for treatment participation); Assessment (regarding symptoms and social problems); Developing understanding of psychotic symptoms using a normalising' style of providing information ); Case formulation and treatment planning; Specific techniques designed to address delusions and hallucinations; Specific techniques designed to address dysfunctional beliefs and schemata; Specific techniques designed to improve social functioning. Delivered by: specifically trained psychotherapists on the basis of a treatment manual. Frequency (times) : 7 sessions in the first seven weeks, followed by 13 fortnightly sessions. Treatment duration (weeks): 36 weeks. Follow‐up: 36 weeks. 2. Control group: (N = 165). Content: engagement; assessment of social problems and interests of the patient; treatment planning; focus on housing, work, leisure time, hobbies, and events, as adequate; Delivered by: specifically trained psychotherapists on the basis of a treatment manual. Frequency (times): not stated. Treatment duration (weeks): sessions in the first seven weeks, followed by 13 fortnightly sessions. Follow‐up: post treatment, 6 months, 12 months |
| Outcomes |
‐‐Unable to use: The author did not report these outcomes. PANSS. Death caused by suicide. Suicide attempt. Suicidal crisis. Calgary Depression Rating Scale. Clinical Global Impression Scale. Distress: PSYRATS. Delusions: AMDP. Insight: SUMD. Symptoms Checklist: SCL‐90‐R. Self‐concept: Frankfurt Self‐Concept Scales. The Brief Core Schema Scales. |
| Notes | Awaiting for full texts. Author's name: Stefan Klingberg Insititute: Department of Psychiatry and Psychotherapy, University of Tuebingen, Address: Germany Email: stefan.klingberg@med.uni‐tuebingen.de |
Lee 1999.
| Methods | Awaiting translation. |
| Participants | Awaiting translation. |
| Interventions | Awaiting translation. |
| Outcomes | Awaiting translation. |
| Notes | Awaiting translation. |
Lystad 2013.
| Methods | Multi‐site study, randomised control trial. |
| Participants | Diagnosis: schizophrenia spectrum disorders |
| Interventions | CBT‐related technique group. Cognitive remediation (CRT ) group. |
| Outcomes | PANSS score. |
| Notes | Awaiting for full text. |
Mirabella 2009.
| Methods | Awaiting translation. |
| Participants | Awaiting translation. |
| Interventions | Awaiting translation. |
| Outcomes | Awaiting translation. |
| Notes | Awaiting translation. |
NCT00980252 2009.
| Methods | Allocation: randomised. Blinding: not reported. Duration: not reported |
| Participants | Diagnosis: clinical diagnosis of schizophreniform disorder, schizophrenia, or schizoaffective disorder in last 6 months
N = not reported. Age: range 16 to 45 years. Length of illness: not reported. |
| Interventions | 1. CBT: cognitive behavioural therapy + standard care. 2. Psychoeducation + standard care. |
| Outcomes | Acceptance of therapeutic intervention as measured by number of sessions attended. Difference in adherence behaviour as measured by duration of antipsychotic treatment during follow‐up. Differences in adherence attitudes. |
| Notes | Awaitting for full text. |
NCT01139502 2010.
| Methods | Allocation: Quote: " Randomized" (p.2).
Blinding: Quote: "Open Label" (p.2).
Duration: not reported. Location: Quote " nine different counties in Norway" (p.1) Length of follow‐up: not reported. |
| Participants | Diagnosis: schizophrenia spectrum disorders. Total: N = 160 Sex: not reported. Age: not reported. Length of illness: not reported. Inclusion criteria: persons with schizophrenia spectrum disorders Exclusion criteria: IQ < 70; neurological disease diagnosis; active suicidal; severe drug abuse. |
| Interventions | 1. CBT Group: (N = 80). Content: two weekly meetings in which participant and work consultant discuss problems interfering with work and social interaction. Home work related to these problems is assigned between the meetings. Delivered by: not reported. Frequency (times): not reported. Treatment duration (weeks): not reported. Follow‐up: not reported. 2. Cognitive training Group: (N = 80). Content: work rehabilitation with the addition of cognitive training Work rehabilitation with the addition of two hours weekly training of concentration, memory, and executive function. Delivered by: not reported. Frequency (times): not reported. Treatment duration (weeks): not reported. Follow‐up: not reported. |
| Outcomes | Outcomes Primary Outcome Measures: The Work Behavior Inventory The Global Assessment of Function The Positive and Negative Symptom Scale (PANSS) The Apathy Evaluation Scale The Alcohol Use Disorder Identification Test The Drug Use Disorder Identification Test The Measurement and Treatment Research to Improve Cognitive Function in Schizophrenia |
| Notes | Awaiting for full text. Author’s name: Erik Falkum, MD, PhD Insititute: Department of Research and Development, clinic for Mental Health, Oslo University Hospital, Oslo, Norway Address: Department of Research and Development, clinic for Mental Health, Oslo University Hospital, Oslo, Norway Email: erik.falkum@medisin.uio.no Tel: +47 22 92 34 59 Author's name: Torill Ueland, PhD Insititute: Department of Research and Development, clinic for Mental Health, Oslo University Hospital, Oslo, Norway Address: Department of Research and Development, clinic for Mental Health, Oslo University Hospital, Oslo, Norway Email: torill.ueland@medisin.uio.no Tel: +47 91 72 53 39 |
Penades 2006.
| Methods | Allocation: randomised controlled trial.
Blinding: not reported.
Duration:not reported. Location: not reported. Length of follow‐up:6 months. (p.1) |
| Participants | Diagnosis: DSM‐IV schizophrenia disorder, cognitive impairments and prominent negative symptoms. Total: N = 40 Sex: not reported. Age: not reported. Length of illness: not reported. Inclusion criteria:not reported. Exclusion criteria:not reported. |
| Interventions | 1. Standard medication + CBT group. 2. Standard medication + CRT group. |
| Outcomes | Outcomes: not reported. |
| Notes | Awaiting for full text. Author's Name: R. Penade. Insititute: Hospital Clinic, Barcelona, Spain Address: VILLARROEL, 170, 08036 BARCELONA, Spain. Email: rpenades@clinic.ub.es Tel: +34 2275477. Fax.: +34 2275477. |
Valmaggia 2003.
| Methods | Allocation: randomised controlled trial.
Blinding: blind assessment took place at baseline, after treatment and at 6 months follow‐up.
Duration:not reported. Location: not reported. Length of follow‐up: 6 months. |
| Participants | Diagnosis: refractory schizophrenia. Sex: not reported. Age: not reported. Length of illness: not reported. Inclusion criteria:not reported. Exclusion criteria:not reported. |
| Interventions | 1. CBT group: 16 sessions. 2. Supportive therapy plus psychoeducation group: 16 sessions. |
| Outcomes | Outcomes: not reported. |
| Notes | Awaiting for full text. Author's name: L. R. Valmaggia, Insititute: ept. ofPsychotic Disorders, GGZ‐Drenthe, Assen, Netherlands. Address: None. Email: None. |
Wu 2008.
| Methods | Awaiting translation. |
| Participants | Awaiting translation. |
| Interventions | Awaiting translation. |
| Outcomes | Awaiting translation. |
| Notes | Awaiting translation. |
CBT: Cognitive behavioural therapy; DSM IV: Diagnostic and Statistical Manual, 4th edition; MADRS:Montgomery‐Asberg Depression Rating Scale; PANSS: Positive and Negative Syndrome Scale; PSYRATS: Psychotic Symptom Rating Scale
Characteristics of ongoing studies [ordered by study ID]
NCT01992913 2014.
| Trial name or title | Integrated cognitive behavior therapy to improve work outcomes in schizophrenia. |
| Methods | Allocation: randomised. Blindling: single‐blind (outcome assessor) Location: not reported. Duration: not reported. Follow‐up: not reported. |
| Participants | Diagnosis: schizophrenia. Inclusion Criteria: Diagnosis of DSM‐IV schizophrenia or schizoaffective disorder (SCID); severe/extreme functional disability [World Health Organization Disability Assessment Scale (WHODAS) score > 50]; stabilised in the community (3 months since last hospitalisation); receiving treatment at the Veterans Administration; minimal engagement in psychiatric rehabilitation services (just psychiatrist and therapist/case management in the last 6 months); eligible for and willing to be enrolled in Supported Employment program; age 18 to 65; proficient in English Able to give informed consent. Exclusion Criteria: neurologic disease or damage that would make the diagnosis of schizophrenia questionable; Current opioid or stimulant dependence (SCID); |
| Interventions | Group 1: Intergrated CBT with computerised cognitive remediation. Group 2: Psychoeducation. |
| Outcomes | Primary Outcome Measures: Work force Participation Measures. Secondary Outcome Measures: specific Levels of Functioning Work Behavior Inventory |
| Starting date | Not reported. |
| Contact information | Not reported. |
| Notes | Not reported. |
NCT02170051 2014.
| Trial name or title | Improving negative symptoms of psychosis In real‐world environments |
| Methods | Allocation:randomised. Blindling: single‐blinded. Location: Califonia. Duration: not stated. Follow‐up: not stated. |
| Participants | Diagnosis: schizophrenia Inclusion Criteria
Exclusion Criteria
|
| Interventions | Group 1: Cognitive Behavioral Social Skills Training‐Compensatory Cognitive Training. Group 2: goal‐focused supportive contact. |
| Outcomes | Change in Clinical Assessment Interview for Negative Symptoms (CAINS) at 4.5 months. Change in MATRICS Consensus Cognitive Battery (MCCB) at 4.5 months. Change in UCSD Performance‐based Skills Assessment‐Brief at 4.5 months. Change in Social Skills Performance Assessment at 4.5 months. Change in Specific Levels of Functioning Scale at 4.5 months. Change in Independent Living Skills Survey at 4.5 months. Change in Defeatist Performance Attitudes Scale at 4.5 months. |
| Starting date | July 2014. |
| Contact information | Name: Barbara Johnson Tel: 619‐543‐6486 Email: b4johnson@ucsd.edu <b4johnson@ucsd.edu> |
| Notes |
NCT02349880 2015.
| Trial name or title | A shared decision‐making training for inpatients with schizophrenia |
| Methods | Allocation: randomised controlled trial.
Blinding: open‐label. Duration: not reported. Location: not reported. Length of follow‐up: 12 months. (p.1) |
| Participants | Diagnosis: DSM‐IV schizophrenia disorder, Schizo‐affective Disorder. Total: N = 240. Sex: not reported. Age: not reported. Length of illness: not reported. Inclusion criteria:
Exclusion criteria: debility. |
| Interventions | 1. CBT Group 2. Cognitive training Group |
| Outcomes | Outcomes: not reported. |
| Starting date | January 23, 2015 |
| Contact information | No contact information provided. |
| Notes | None. |
Xu 2008.
| Trial name or title | A randomised controlled trial of cognitive‐behavioral therapy for schizophrenia. |
| Methods | Allocation: Quote" Block randomizations"(p.2)
Blinding: Quote" Results assessor: Blind"(p.2)
Duration:Quote"24 weeks"(p.2) Location: Quote"Beijing, China"(p.2) Length of follow‐up: 24 weeks. (p.2) |
| Participants | Diagnosis: Schizophrenia, DSM‐IV. Total: N = 200. Sex: not reported. Age: not reported. Length of illness: not reported. Inclusion criteria: aged between 18 and 60 years; Schizophrenia diagnosis according to DSM‐IV criteria; PANSS total score greater than 60; Using stable antipsychotic medication for at least 2 weeks prior to entering the study; Received only one antipsychotic medication; Patients and one of their parents signed informed consent; The educational background higher than junior middle school (including junior middle school) . Exclusion criteria: Other primary or co‐primary psychiatric disorder; In the PANSS sub scale: conceptual disorganiSation ≥ 4,poor rapport ≥ 4,lack of spontaneity and flow of conversation ≥ 5; Undergoing MECT at the latest 1 month; Suffering from serious physical disease. |
| Interventions | 1. CBT + medication group: (N = 100). Content: From the first to 12th week, 12 sessions of CBT are conducted weekly; 3 sessions are conducted to promote maintenance every 3 week from the 16th to 24th week, and the remaining 60 weeks is follow‐up period. Delivered by: not reported. Frequency (times): not reported. Treatment duration (weeks): not reported. Follow‐up: not reported. 2. Supportive psychotherapy+ medication group: (N = 100). Content: From the first to12th week, 12 sessions of supportive psychotherapy are conducted weekly; 3 sessions are conducted to promote maintenance every 3 week from the 16th to 24th week, and the remaining 60 weeks is follow‐up period. Delivered by: not reported. Frequency (times): not reported. Treatment duration (weeks): not reported. Follow‐up: not reported. |
| Outcomes | Outcomes Coping Questionnaire, The Psychotic Symptom Rating Scales (PSYRATS). Personal and social performance scale (PSP). The positive and negative symptoms of schizophrenia Scale (PANSS). Irrational beliefs Scale (IBS). Schizophrenic symptoms attribution questionnaire (SAQS), The Clinical Global Impressions (CGI) scale. The World Health Organization Quality of Life Questionnaire—Brief Version (WHOQOL‐BREF). Insight questionnaire. |
| Starting date | April, 2008. |
| Contact information | Author's name: Ziyan Xu Insititute: Beijing Anding hospital affiliated to capital medical university Address: NO.5, Ankang hutong, Dewai main street, Xicheng District, Beijing Email: yzxu22@163.com Tel: +86 0 13521805471 |
| Notes | Funding source: Beijing Municipal Science &Technology Commission. |
CBT: Cognitive behavioural therapy; DSM IV: Diagnostic and Statistical Manual, 4th edition; ICD 10 ‐ International Classification of Diseases; PANSS: Positive and Negative Syndrome Scale
Differences between protocol and review
For previous changes please see Appendix 3
For the 2018 update
1. Outcomes
The outcomes have been re‐ordered to reflect the order of outcomes reported in the 'Summary of findings' table. We have separated global state and general functioning outcomes for clarity. We have also made a post hoc decision regarding the importance of 'death' as a primary outcome for psychological interventions. We feel evidence regarding the global state of participants and their satisfaction with treatment are better outcomes by which to evaluate the effectiveness of CBT rather than an event that rarely occurs with psychological therapies. Death is now part of adverse events outcomes. We have also changed outcomes from 'no' clinically important change to clinically important change to avoid the use of confusing double negatives. We have also used the longest follow‐up time point available for presenting in the 'Summary of findings' table..
2. Interventions
We have renamed the control intervention from 'treatment as usual' to 'standard care'.
3. Methods update
We have updated the methods to reflect latest changes in Cochrane Schizophrenia's template.
4. Subgroup analyses
Due to lack of data, we decided not to anticipate subgroup analysis for people in first episode of illness versus those at a later stage of illness.
The subgroup analyses for comparing CBT with active and inactive psychotherapies should not read 'versus' each other (as in previously published protocol) but should read 'Active or non active control therapies'.
Contributions of authors
Chris Jones ‐ protocol formulation, searching, trial selection, data extraction, report writing (all versions)
David Hacker ‐ protocol formulation, searching, trial selection, data extraction, report writing (all versions)
Alan Meaden ‐ protocol formulation, searching, trial selection, data extraction, report writing (all versions)
Irene Cormac ‐ protocol formulation, report writing (all versions)
Claire Irving ‐ protocol formulation, trial selection, report checking and writing (all versions)
Jun Xia ‐ report writing, trial selection, data extraction, report writing (2018 version)
Sai Zhao ‐ trial selection, data extraction, report writing (2018 version)
Chunhu Shi ‐ trial selection, data extraction (2018 version)
Jue Chen: help with trial selection, help with data extraction, checking of discussion (2018 version)
Sources of support
Internal sources
South Warwickshire Mental Health Trust, UK.
University of Birmingham, UK.
Nottinghamshire Healthcare NHS Trust, UK.
External sources
No sources of support supplied
Declarations of interest
Chris Jones is a Clinical Psychologist who specialises in neuropsychology.
David Hacker is a Clinical Psychologist who specialises in neuropsychology.
Alan Meaden is a Clinical Psychologist who works with persons with psychosis.
Irene Cormac is a Forensic Psychiatrist ‐ no declarations of interest.
Claire Irving is the Managing Editor Cochrane Schizophrenia ‐ no declarations of interest.
Jun Xia runs a company Systematic Review Solutions that specialises in writing and completing systematic reviews ‐ no declarations of interest.
Sai Zhao is an employee of Systematic Review Solutions ‐ no declarations of interest.
Chunhu is an employee of Systematic Review Solutions ‐ no declarations of interest.
Jue Chen is an employee of Systematic Review Solutions ‐ no declarations of interest.
Edited (no change to conclusions)
References
References to studies included in this review
A ‐ Bechdolf 2004 {published data only}
- Bechdolf A, Knost B, Kuntermann C, Schiller S, Klosterkotter J, Hambrecht M, et al. A randomized comparison of group cognitive‐behavioural therapy and group psychoeducation in patients with schizophrenia. Acta Psychiatrica Scandinavica 2004;110(1):21‐8. [CSzG: Ref11268] [DOI] [PubMed] [Google Scholar]
- Bechdolf A, Knost B, Nelson B, Schneider N, Veith V, Yung AR, et al. Randomized comparison of group cognitive behaviour therapy and group psychoeducation in acute patients with schizophrenia: effects on subjective quality of life. Australian and New Zealand Journal of Psychiatry 2010;44:144‐50. [CSzG: Ref19694] [DOI] [PubMed] [Google Scholar]
- Bechdolf A, Kohn D, Knost B, Pukrop R, Klosterkotter J. A randomized comparison of group cognitive‐behavioural therapy and group psychoeducation in acute patients with schizophrenia: outcome at 24 months. Acta Psychiatrica Scandinavica 2005;112(3):172‐9. [CSzG: Ref18491] [DOI] [PubMed] [Google Scholar]
- Munk‐Jorgensen P. Erratum. Acta Psychiatrica Scandinavica 2004;110:483. [CSzG: Ref18577] [Google Scholar]
A ‐ Buchkremer 1997 {published data only}
- Buchkremer G, Klingberg S, Holle R, Schulze Monking H, Hornung W. Psychoeducational psychotherapy for schizophrenic patients and their key relatives or care‐givers: Results of a two year follow‐up. Acta Psychiatrica Scandinavica 1997;96(6):483‐91. [CSzG: Ref602] [DOI] [PubMed] [Google Scholar]
- Klingberg S, Buchkremer G, Holle R, Monking H, Hornung W. Differential therapy effects of psychoeducational psychotherapy for schizophrenic patients ‐ results of 2‐year follow‐up. European Archives of Psychiatry and Clinical Neuroscience 1999;249:66‐72. [CSzG: Ref5104] [DOI] [PubMed] [Google Scholar]
A ‐ Cather 2005 {published data only}
- Cather C, Penn D, Otto MW, Yovel I, Mueser KT, Goff DC. A pilot study of functional cognitive behavioral therapy (fCBT) for schizophrenia. Schizophrenia Research 2005;74(23):201‐9. [CSzG: Ref12184] [DOI] [PubMed] [Google Scholar]
A ‐ Durham 2003 {published data only}
- Durham RC, Guthrie M, Morton RV, Reid DA, Treliving LR, Fowler D, et al. Tayside‐Fife clinical trial of cognitive‐behavioural therapy for medication‐resistant psychotic symptoms. British Journal of Psychiatry 2003;182:303‐11. [CSzG: Ref9545] [DOI] [PubMed] [Google Scholar]
A ‐ Garety 2008 {published data only}
- Garety PA, Fowler DG, Freeman D, Bebbington P, Dunn G, Kuipers E. Cognitive‐behavioural therapy and family intervention for relapse prevention and symptom reduction in psychosis: randomised controlled trial. British Journal of Psychiatry 2008;192(6):412‐23. [CSzG: Ref16445] [DOI] [PubMed] [Google Scholar]
A ‐ Granholm 2013 {published data only}
- Granholm E, Holden J, Link P. Randomized clinical trial of cognitive behavioral social skills training (cbsst) for older people with schizophrenia: Replication and role of defeatist attitudes. Schizophrenia Bulletin 2011;37:304. [CSzG: Ref22776] [Google Scholar]
A ‐ Granholm 2014 {published data only}
- Granholm E, Holden J, Link PC, McQuaid JR. Randomized clinical trial of cognitive behavioral social skills training for schizophrenia: improvement in functioning and experiential negative symptoms. Journal of Consulting and Clinical Psychology 2014;82(6):1173‐85. [CSzG: Ref29118] [DOI] [PMC free article] [PubMed] [Google Scholar]
A ‐ Haddock 1999 {published data only}
- Haddock G, Tarrier N, Morrison AP, Hopkins R, Drake R, Lewis S. A pilot study evaluating the effectiveness of individual inpatient cognitive‐behavioural therapy in early psychosis. Social Psychiatry and Psychiatric Epidemiology 1999;34(5):254‐8. [CSzG: Ref8475] [DOI] [PubMed] [Google Scholar]
A ‐ Jiang 2010 {published data only}
- Jiang Y, Wang H, Wang J. Effect of cognitive behavioral therapy in patients with chronic schizophrenia to obsessive‐compulsive symptoms. Sichuan Mental Health [四川精神卫生] 2010;23:227‐9. [CSzG: Ref24094] [Google Scholar]
A ‐ Klingberg 2012 {published data only}
- Cantero MD, Duque A, Valiente C, Fuentenebro F, Villavicencio P, Mehl S, et al. Social cognitive biases as moderators and mediators of successful cognitive behavioural therapy in schizophrenia – results of the positive study. Schizophrenia Research 2012;136(April):1088‐5. [Google Scholar]
- Klingberg S, Herrlich J, Wiedemann G, Wolwer W, Meisner C, Engel C, et al. Adverse effects of cognitive behavioral therapy and cognitive remediation in schizophrenia: results of the treatment of negative symptoms study. Journal of Nervous and Mental Disease 2012;200:569‐76. [CSzG: Ref24444] [DOI] [PubMed] [Google Scholar]
- Klingberg S, Wittorf A, Herrlich J, Wiedemann G, Meisner C, Buchkremer G, et al. Cognitive behavioural treatment of negative symptoms in schizophrenia patients: study design of the TONES study, feasibility and safety of treatment. European Archives of Psychiatry and Clinical Neuroscience 2009;259(Suppl 2):S149‐54. [CSzG: Ref20607] [DOI] [PubMed] [Google Scholar]
- Klingberg S, Wolwer W, Engel C, Wittorf A, Herrlich J, Meisner C, et al. Negative symptoms of schizophrenia as primary target of cognitive behavioral therapy: results of the randomized clinical tones study. Schizophrenia Bulletin 2011;37(Suppl 2):98‐110. [CSzG: Ref23239] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klingberg S, Wolwer W, Engel C, Wittorf A, Herrlich J, Meisner C, et al. The role of cognitive behavioral therapy and cognitive remediation for the treatment of negative symptoms. European Archives of Psychiatry and Clinical Neuroscience 2011;261:S36. [CSzG: Ref23741] [DOI] [PubMed] [Google Scholar]
A ‐ Lecomte 2008 {published data only}
- Beauchamp MC, Lecomte T, Lecomte C, Leclerc C, Corbiere M. Personality traits in early psychosis: relationship with symptom and coping treatment outcomes. Early Intervention in Psychiatry 2011;5(1):33‐40. [CSzG: Ref22697] [DOI] [PubMed] [Google Scholar]
- Lecomte T, Leclerc C, Corbiere M, Wykes T, Wallace CJ, Spidel A. Group cognitive behavior therapy or social skills training for individuals with a recent onset of psychosis? Results of a randomized controlled trial. Journal of Nervous and Mental Disease 2008;196:866‐75. [CSzG: Ref17174] [DOI] [PubMed] [Google Scholar]
- Lecomte T, Leclerc C, Wykes T, Spidel A. Group CBT for early psychosis ‐ are there still benefits 1 year later?. Early Intervention in Psychiatry 2010;4(Suppl 1):150. [CSzG: Ref23485] [Google Scholar]
A ‐ Levine 1998 {published data only}
- Levine J, Barak Y, Granek I. Cognitive group therapy for paranoid schizophrenics: applying cognitive dissonance. Journal of Cognitive Psychotherapy 1998;12(1):3‐12. [CSzG: Ref7252] [Google Scholar]
A ‐ Li 2014 {published data only}
- Li ZJ, Guo ZH, Wang N, Xu ZY, Qu Y, Wang XQ, et al. Cognitive–behavioural therapy for patients with schizophrenia: a multicentre randomized controlled trial in Beijing, China. Psychological Medicine 2015;45(9):1893‐905. [DOI] [PubMed] [Google Scholar]
A ‐ Li 2015 {published data only}
- Li H, Shu J, Huang C, Sun H, Zhu Y, Wang S. Comparative study of effects of community comprehensive rehabilitation on family burden and psychological health of their main caregivers of patients the chronic schizophrenia [社区综合康复对慢性精神分裂症患者的家庭负担及照料者心理健康的对比研究]. Medical Journal of Chinese People's Health [中国民康医学] 2015;27(9):1‐4+7. [CSzG: Ref34296] [Google Scholar]
A ‐ Li 2015b {published data only}
- Li Y, Xiong A, Hou L, Zhao Y, Hou C. Effects of behavior treatment for schizophrenia patients during recovery stage [精神分裂症患者恢复期应用行为治疗的作用分析]. Journal of Hainan Medical University [海南医学院学报] 2015;21(3):430‐2. [CSzG: Ref31686] [Google Scholar]
A ‐ Ma 2012 {published data only}
- Ma Y, Li Z, Xu Z, Guo Z, Qu Y, Wang X, et al. Effects of cognitive behavioral therapy on coping style for patients with schizophrenia [认知行为治疗对精神分裂症患者应对方式的影响]. Chinese Journal of Clinical Psychology [中国临床心理学杂志] 2013;21(3):455‐7. [CSzG: Ref28418] [Google Scholar]
- Ma Y, Li Z, Xu Z, Guo Z, Qu Y, Wang X, et al. Effects of cognitive behavioral therapy on quality of life in patients with schizophrenia: a single blind randomized controlled study [认知行为治疗改善精神分裂症患者生活质量的随机单盲对照试验]. Chinese Mental Health Journal [Zhongguo Xin Li Wei Sheng Za Zhi; 中国心理卫生杂志] 2012;26(11):801‐7. [CSzG: Ref27002] [Google Scholar]
A ‐ Penn 2009 {published data only}
- Penn DL, Meyer PS, Evans E, Wirth RJ, Cai K, Burchinal M. A randomized controlled trial of group cognitive‐behavioral therapy vs. enhanced supportive therapy for auditory hallucinations. Schizophrenia Research 2009;109:52‐9. [CSzG: Ref18213] [DOI] [PubMed] [Google Scholar]
A ‐ Pinto 1999 {published data only}
- Pinto A, LaPia S, Mennella R, Giorgio D, DeSimone L. Cognitive‐behavioural therapy and clozapine for clients with treatment refactory schizophrena. Psychiatric Services 1999;50(7):901‐4. [CSzG: Ref5215] [DOI] [PubMed] [Google Scholar]
A ‐ Tarrier 1999 {published data only}
- Tarrier N, Beckett R, Harwood S, Baker A, Yusupoff L, Ugarteburu I. A trial of two cognitive‐behavioural methods of treating drug‐resistant residual psychotic symptoms in schizophrenic patients: I. outcome. British Journal of Psychiatry 1993;162:524‐32. [CSzG: Ref2814] [DOI] [PubMed] [Google Scholar]
- Tarrier N, Kinney C, McCarthy E, Humphreys L, Wittkowski A, Morris, J. Two‐year follow‐up of cognitive behavioral therapy and supportive counselling in the treatment of persistent symptoms in chronic schizophrenia. Journal of Consulting and Clinical Psychology 2000;68(5):917‐22. [CSzG: Ref5396] [PubMed] [Google Scholar]
- Tarrier N, Wittkowski A, Kinney C, McCarthy E, Morris J, Humpherys L. Durability of the effects of cognitive‐behavioural therapy in the treatment of chronic schizophrenia: 12‐month follow‐up. British Journal of Psychiatry 1999;174:500‐4. [CSzG: Ref3681] [DOI] [PubMed] [Google Scholar]
- Tarrier N, Yusupoff L, Kinney C, McCarthy E, Gledhill A, Haddock G, et al. Randomised controlled trial of intensive cognitive behavioural therapy for patients with chronic schizophrenia. BMJ 1998;317:303‐7. [CSzG: Ref3682] [DOI] [PMC free article] [PubMed] [Google Scholar]
A ‐ Velligan 2014 {published data only}
- NCT01915017. Interventions to improve functional outcome and persistent symptoms in schizophrenia. Clinicaltrials.gov/show/NCT01915017 (first received 26 July 2013). [CSzG: Ref27937]
- Velligan DI, Tai S, Roberts DL, Maples‐Aguilar N, Brown M, Mintz J, et al. A randomized controlled trial comparing cognitive behavior therapy, cognitive adaptation training, their combination and treatment as usual in chronic schizophrenia. Schizophrenia Bulletin 2015;41(3):597‐603. [CSzG: Ref29077] [DOI] [PMC free article] [PubMed] [Google Scholar]
A ‐ Wittorf 2010 {published data only}
- Wittorf A, Jakobi UE, Bannert KK, Bechdolf A, Muller BW, Sartory G, et al. Does the cognitive dispute of psychotic symptoms do harm to the therapeutic alliance?. Journal of Nervous and Mental Disease 2010;198:478‐85. [CSzG: Ref21349] [DOI] [PubMed] [Google Scholar]
- Wittorf A, Klingberg S. The therapeutic alliance in CBT for pychoses: course and predictive value for outcome. European Archives of Psychiatry and Clinical Neuroscience 2011;261:S13‐S4. [CSzG: Ref23759] [Google Scholar]
NA ‐ Davis 2008 {published data only}
- Davis LW, Ringer JM, Strasburger AM, Lysaker PH. Participant evaluation of a CBT program for enhancing work function in schizophrenia. Psychiatric Rehabilitation Journal 2008;32:55‐8. [CSzG: Ref16644] [DOI] [PubMed] [Google Scholar]
NA ‐ Drury 2000 {published data only}
- Drury V, Birchwood M, Cochrane R. Cognitive therapy and recovery from acute psychosis: a controlled trial. British Journal of Psychiatry 2000;177:8‐14. [CSzG: Ref4107] [DOI] [PubMed] [Google Scholar]
- Drury V, Brichwood M, Cochrane R, Macmillan F. Cognitive therapy and recovery from acute psychosis: a controlled trial. I. Impact on psychotic symptoms. British Journal of Psychiatry 1996;169:593‐601. [CSzG: Ref1476] [DOI] [PubMed] [Google Scholar]
- Drury V, Brichwood M, Cochrane R, Macmillan F. Cognitive therapy and recovery from acute psychosis: a controlled trial. II. Impact on recovery time. British Journal of Psychiatry 1996;169:602‐7. [CSzG: Ref1477] [DOI] [PubMed] [Google Scholar]
NA ‐ Haddock 2009 {published data only}
- Haddock G, Barrowclough C, Shaw JJ, Dunn G, Novaco RW, Tarrier N. Cognitive‐behavioural therapy v. social activity therapy for people with psychosis and a history of violence: randomised controlled trial. British Journal of Psychiatry 2009;194(2):152‐7. [CSzG: Ref18298] [DOI] [PubMed] [Google Scholar]
NA ‐ Jackson 2008 {published data only}
- Allott K, Alvarez‐Jimenez M, Killackey EJ, Bendall S, McGorry PD, Jackson HJ. Patient predictors of symptom and functional outcome following cognitive behaviour therapy or befriending in first‐episode psychosis. Schizophrenia Research 2011;132(2‐3):125‐30. [CSzG: Ref23404] [DOI] [PubMed] [Google Scholar]
- Allott KA, Alvarez‐Jimenez M, Bendall S, Killackey EJ, McGorry PD, Jackson HJ. Predictors of functional outcome following CBT in first‐episode psychosis. Schizophrenia Bulletin 2011;37:258. [CSzG: Ref22824] [DOI] [PubMed] [Google Scholar]
- Bendall S, Allott K, Jovev M, Marois M, Killackey E, Gleeson J, et al. Therapy contamination as a measure of therapist treatment adherence in a trial of cognitive behaviour therapy versus befriending for psychosis. Behavioural and Cognitive Psychotherapy 2015;43:314‐27. [CSzG: Ref29748] [DOI] [PubMed] [Google Scholar]
- Bendall S, Jackson HJ, Killackey E, Allott K, Johnson T, Harrigan S, et al. The credibility and acceptability of befriending as a control therapy in a randomized controlled trial of cognitive behaviour therapy for acute first episode psychosis. Behavioural and Cognitive Psychotherapy 2006;34:277‐91. [CSzG: Ref18494] [Google Scholar]
- Jackson HJ, McGorry PD, Killackey E, Bendall S, Allott K, Dudgeon P, et al. Acute‐phase and 1‐year follow‐up results of a randomized controlled trial of CBT versus befriending for first‐episode psychosis: the ACE project. Psychological Medicine 2008;38(5):725‐35. [CSzG: Ref16107] [DOI] [PubMed] [Google Scholar]
NA ‐ Kemp 1998 {published data only}
- Kemp R, Hayward P, Applewhaite G, Everitt B, David A. Compliance therapy in psychotic patients: a randomised controlled trial. BMJ 1996;312:345‐9. [CSzG: Ref1308] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kemp R, Kirov G, Everitt B, Hayward P, David A. Randomised controlled trial of compliance therapy. British Journal of Psychiatry 1998;172:413‐9. [CSzG: Ref3499] [DOI] [PubMed] [Google Scholar]
NA ‐ Lewis 2002 {published data only}
- Lewis S, Tarrier N, Haddock G, Bentall R, Kinderman P, Kingdon D, et al. Randomised controlled trial of cognitive‐behavioural therapy in early schizophrenia: acute‐phase outcomes. British Journal of Psychiatry 2002;181(S43):S91‐7. [CSzG: Ref8736] [DOI] [PubMed] [Google Scholar]
- Tarrier N, Lewis S, Haddock G, Bentall R, Drake R, Kinderman P, et al. Cognitive‐behavioural therapy in first‐episode and early schizophrenia. British Journal of Psychiatry 2004;184:231‐9. [CSzG: Ref10096] [DOI] [PubMed] [Google Scholar]
NA ‐ Lewis 2002 (L) {published data only}
- Lewis S, Tarrier N, Haddock G, Bentall R, Kinderman P, Kingdon D, et al. Randomised controlled trial of cognitive‐behavioural therapy in early schizophrenia: acute‐phase outcomes. British Journal of Psychiatry 2002;181(S43):S91‐7. [CSzG: Ref8736] [DOI] [PubMed] [Google Scholar]
- Tarrier N, Lewis S, Haddock G, Bentall R, Drake R, Kinderman P, et al. Cognitive‐behavioural therapy in first‐episode and early schizophrenia. British Journal of Psychiatry 2004;184:231‐9. [CSzG: Ref10096] [DOI] [PubMed] [Google Scholar]
NA ‐ Lewis 2002 (M) {published data only}
- Lewis S, Tarrier N, Haddock G, Bentall R, Kinderman P, Kingdon D, et al. Randomised controlled trial of cognitive‐behavioural therapy in early schizophrenia: acute‐phase outcomes. British Journal of Psychiatry 2002;181(S43):S91‐7. [CSzG: Ref8736] [DOI] [PubMed] [Google Scholar]
- Tarrier N, Lewis S, Haddock G, Bentall R, Drake R, Kinderman P, et al. Cognitive‐behavioural therapy in first‐episode and early schizophrenia. British Journal of Psychiatry 2004;184:231‐9. [CSzG: Ref10096] [DOI] [PubMed] [Google Scholar]
NA ‐ Lewis 2002 (N) {published data only}
- Lewis S, Tarrier N, Haddock G, Bentall R, Kinderman P, Kingdon D, et al. Randomised controlled trial of cognitive‐behavioural therapy in early schizophrenia: acute‐phase outcomes. British Journal of Psychiatry 2002;181(S43):S91‐7. [CSzG: Ref8736] [DOI] [PubMed] [Google Scholar]
- Tarrier N, Lewis S, Haddock G, Bentall R, Drake R, Kinderman P, et al. Cognitive‐behavioural therapy in first‐episode and early schizophrenia. British Journal of Psychiatry 2004;184:231‐9. [CSzG: Ref10096] [DOI] [PubMed] [Google Scholar]
NA ‐ Li 2015 {published data only}
- Li Y, Li Z, Xin L, Hou L, Zhao Y, Hou C. The efficacy of special cognitive‐behavior approaches on schizophrenia during acute‐phase [特定认知行为技术对急性期精神分裂症的干预效果]. Hebei Medicine [河北医学] 2015;21(06):1018‐20. [CSzG: Ref33920] [Google Scholar]
NA ‐ O'Donnell 2003 {published data only}
- O'Donnell C, Donohoe G, Sharkey L, Owens N, Migone M, Harries R, et al. Compliance therapy: a randomised controlled trial in schizophrenia. BMJ 2003;327(7419):834. [CSzG: Ref9883] [DOI] [PMC free article] [PubMed] [Google Scholar]
NA ‐ Sensky 2000 {published data only}
- Sensky T, Turkington D, Kingdon D, Scott JL, Scott J, Siddle R, et al. A randomized controlled trial of cognitive‐behavioural therapy for persistent symptoms in schizophrenia resistant to medication. Archives of General Psychiatry 2000;57:165‐72. [CSzG: Ref5259] [DOI] [PubMed] [Google Scholar]
- Turkington D, Sensky T, Scott J, Barnes T, Nur U, Siddle R, et al. A randomized controlled trial of cognitive‐behavior therapy for persistent symptoms in schizophrenia: a five‐year follow‐up. Schizophrenia Research 2008;98:1‐7. [CSzG: Ref15582] [DOI] [PubMed] [Google Scholar]
NA ‐ Turkington 2000 {published data only}
- Turkington D, Kingdon D. Cognitive‐behavioural techniques for general psychiatrists in the management of patients with psychoses. British Journal of Psychiatry 2000;177:101‐6. [CSzG: Ref5385] [DOI] [PubMed] [Google Scholar]
NA ‐ Valmaggia 2005 {published data only}
- Valmaggia LR, Gaag MVD, Tarrier N, Pijnenborg M, Slooff CJ. Cognitive‐behavioural therapy for refractory psychotic symptoms of schizophrenia resistant to atypical antipsychotic medication. Randomised controlled trial. British Journal of Psychiatry 2005;186:324‐30. [CSzG: Ref11462] [DOI] [PubMed] [Google Scholar]
NA ‐ Zhang 2015 {published data only}
- Zhang Y. Effect of cognitive behavior on coping style in patients with schizophrenia. World Latest Medicine Information [世界最新医学信息文摘] 2015;13(72):63. [CSzG: Ref34641] [Google Scholar]
References to studies excluded from this review
Anzai 2002 {published data only}
- Anzai N, Yoneda S, Kumagai N, Nakamura Y, Ikebuchi E, Liberman R. Training persons with schizophrenia in illness self‐management: a randomised controlled trial in Japan. Psychiatric Services 2002;53(5):545‐7. [DOI] [PubMed] [Google Scholar]
Arlow 1997 {published data only}
- Arlow PB, Moran ME, Bermanzohn PC, Stronger R, Siris SG. Cognitive‐behavioural treatment of panic attacks in chronic schizophrenia. Journal of Psychotherapy Practice and Research 1997;6:145‐50. [PMC free article] [PubMed] [Google Scholar]
Bach 2002 {published data only}
- Bach P, Hayes SC. The use of acceptance and commitment therapy to prevent the rehospitalization of psychotic patients: a randomized controlled trial. Journal of Consulting and Clinical Psychology 2002;70(5):1129‐39. [DOI] [PubMed] [Google Scholar]
Barrowclough 2001 {published data only}
- Barrowclough C, Haddock G, Tarrier N, Lewis SW, Moring J, O'Brien R, et al. Randomized controlled trial of motivational interviewing, cognitive behavior therapy, and family intervention for patients with comorbid schizophrenia and substance use disorders. American Journal of Psychiatry 2001;158(10):1706‐13. [DOI] [PubMed] [Google Scholar]
- Haddock G, Barrowclough C, Tarrier N, Moring J, O'Brien R, Schofield N, et al. Cognitive‐behavioural therapy and motivational intervention for schizophrenia and substance misuse. 18‐month outcomes of a randomised controlled trial. British Journal of Psychiatry 2003;183:418‐26. [DOI] [PubMed] [Google Scholar]
Barrowclough 2006 {published data only}
- Barrowclough C, Haddock G, Lobban F, Jones S, Siddle R, Roberts C, et al. Group cognitive‐behavioural therapy for schizophrenia. Randomised controlled trial. British Journal of Psychiatry 2006;189:527‐32. [DOI] [PubMed] [Google Scholar]
Bechdolf 2005b {published data only}
- Bechdolf A, Veith V, Schwarzer D, Schormann M, Stamm E, Janssen B, et al. Cognitive‐behavioral therapy in the pre‐psychotic phase: an exploratory study. Psychiatry Research 2005;136(2‐3):251‐5. [DOI] [PubMed] [Google Scholar]
Bellucci 2002 {published data only}
- Bellucci DM, Galberman K, Haslam N. Computer assisted cognitive rehabilitation reduces negative symptoms in the severely mentally ill. Schizophrenia Research 2002;59:225‐32. [DOI] [PubMed] [Google Scholar]
Bouchaud 1996 {published data only}
- Bouchaud S, Vallieres A, Roy M, Maziade M. Cognitive restructuring in the treatment of psychotic symptoms in schizophrenia: a critical analysis. Behavior Therapy 1996;27:257‐77. [Google Scholar]
Bradshaw 1993 {published data only}
- Bradshaw W. Coping‐skills, training versus a problem‐solving approach with schizophrenic patients. Hospital and Community Psychiatry 1993;44(5):491‐500. [DOI] [PubMed] [Google Scholar]
Bradshaw 2000 {published data only}
- Bradshaw W. Integrating cognitive‐behavioral psychotherapy for persons with schizophrenia into a psychiatric rehabilitation program: results of a three year trial. Community Mental Health Journal 2000;36(5):491‐500 . [DOI] [PubMed] [Google Scholar]
Browning 2013 {published data only}
- Browning S, Corrigall R, Garety P, Emsley R, Jolley S. Psychological interventions for adolescent psychosis: a pilot controlled trial in routine care. European Psychiatry 2013;28:423‐6. [DOI] [PubMed] [Google Scholar]
Buchanan 1992 {published data only}
- Buchanan A. A two year prospective study of treatment compliance in patients with schizophrenia. Psychological Medicine 1992;22(3):787‐97. [DOI] [PubMed] [Google Scholar]
Castle 2002 {published data only}
- Castle D, Nathan P, Kingser P, Halprin S, Drummand P, Jeffreys L. Treating social anxiety in schizophrenia: a group based cognitive behaviour therapy approach. 155th Annual Meeting of the American Psychiatric Association; 2002 May 18‐23; Philadelphia, Pennsylvania, USA. 2002.
Chadwick 1994 {published data only}
- Chadwick P, Birchwood M. The omnipotence of voices: a cognitive approach to auditory hallucinations. British Journal of Psychiatry 1994;164:190‐201. [DOI] [PubMed] [Google Scholar]
- Chadwick P, Lowe C. A cognitive approach to measuring and modifying delusions. Behavioural Research Therapy 1994;32(3):355‐67. [DOI] [PubMed] [Google Scholar]
Claghorn 1974 {published data only}
- Clagthorn JL, Johnstone EE, Cook TH, Itschner L. Group therapy and maintenance treatment of schizophrenics. Archives of General Psychiatry 1974;31:361‐5. [DOI] [PubMed] [Google Scholar]
Daniels 1998 {published data only}
- Daniels L. A group cognitive‐behavioural and process‐oriented approach to treating the social impairment and negative symptoms associated with chronic mental illness. Journal of Psychotherapy Practice and Research 1998;7:167‐76. [PMC free article] [PubMed] [Google Scholar]
Drake 1993 {published data only}
- Drake RE, Bebout RR, Roach JP. A research evaluation of social network case management for homeless persons with dual disorders. Social Network Research 1993;1:83‐98. [Google Scholar]
Edwards 2003 {published data only}
- Edwards J, Wong L, Bernett P, Harrigan SM, McGorry PD, Wade D, et al. Enduring positive symptoms in first episode psychosis: a randomised controlled trial of clozapine and CBT. International Congress on Schizophrenia Research 2003;60:321. [DOI] [PMC free article] [PubMed] [Google Scholar]
England 2007 {published data only}
- England M. Efficacy of cognitive nursing intervention for voice hearing. Perspectives in Psychiatric Care 2007;42(2):69‐76. [DOI] [PubMed] [Google Scholar]
- England M. Significance of cognitive intervention for voice hearers. Perspectives in Psychiatric Care 2008;44(1):40‐7. [DOI] [PubMed] [Google Scholar]
Evins 2001 {published data only}
- Evins AE, Mays VK, Rigotti NA, Tisdale T, Cather C, Goff D. A pilot trial of bupropion added to cognitive behavioural therapy for smoking cessation in schizophrenia. Nicotine and Tobacco Research 2001;3:397‐403. [DOI] [PubMed] [Google Scholar]
Fritze 1988 {published data only}
- Fritze J, Forthner B, Schmitt B, Thaler U. Cognitive training adjunctive to pharmacotherapy in schizophrenia and depression: a pilot study on the lateralization hypothesis of schizophrenia and depression and on cognitive therapy as adjunctive to pharmacotherapy. Neuropsychobiology 1988;19:45‐50. [DOI] [PubMed] [Google Scholar]
Garety 1994 {published data only}
- Garety PA, Kuiper L, Fowler D, Chamberlin F, Dunn G. Cognitive behavioural therapy for drug‐resistant psychosis. British Journal of Medical Psychology 1994;67:259‐71. [DOI] [PubMed] [Google Scholar]
Garety 1998 {published data only}
- Garety P, Fowler D, Kuipers E, Freeman D, Dunn G, Bebbington P, et al. London East‐Anglia randomised controlled trial of cognitive behavioural therapy for psychosis: II. Predictors of outcome. British Journal of Psychiatry 1994;171:420‐6. [DOI] [PubMed] [Google Scholar]
- Kuipers E, Fowler D, Garety P, Chisholm D, Freeman D, Dunn G, et al. London East‐Anglia randomised control trial of cognitive behavioural therapy for psychosis III: Follow‐up and economic evaluation at 18 months. British Journal of Psychiatry 1998;173:61‐8. [DOI] [PubMed] [Google Scholar]
- Kuipers E, Garety P, Fowler D, Dunn G, Freeman D, Bebbington P, et al. London East‐Anglia randomised controlled trial of cognitive behavioural therapy for psychosis: I. Effects of the treatment phase. British Journal of Psychiatry 1997;171:319‐27. [DOI] [PubMed] [Google Scholar]
Gaudiano 2006 {published data only}
- Gaudiano BA, Herbert JD. Acute treatment of inpatients with psychotic symptoms using acceptance and commitment therapy: pilot results. Behaviour Research and Therapy 2006;44(3):415‐37. [DOI] [PubMed] [Google Scholar]
Granholm 2005 {published data only}
- Granholm E, McQuaid JR, McClure FS, Auslander LA, Perivoliotis D, Pedrelli P, et al. A randomized, controlled trial of cognitive behavioral social skills training for middle‐aged and older outpatients with chronic schizophrenia. American Journal of Psychiatry 2005;162(3):520‐9. [DOI] [PubMed] [Google Scholar]
- Granholm E, McQuaid JR, McClure FS, Link PC, Perivoliotis D, Gottlieb JD, et al. Randomized controlled trial of cognitive behavioral social skills training for older people with schizophrenia: 12‐month follow‐up. Journal of Clinical Psychiatry 2007;68(5):730‐7 . [DOI] [PubMed] [Google Scholar]
Grawe 2006 {published data only}
- Grawe RW, Falloon IR, Widen JH, Skogvoll E. Two years of continued early treatment for recent‐onset schizophrenia: a randomised controlled study. Acta Psychiatrica Scandinavica 2006;114:328‐36. [DOI] [PubMed] [Google Scholar]
Gumley 2003 {published data only}
- Gumley A, O'Grady M, McNay L, Rilley J, Power K, Norrie J. Early intervention for relapse in schizophrenia: results of a twelve month randomized controlled trial of cognitive behavioural therapy. Psychological Medicine 2003;33:419‐31. [DOI] [PubMed] [Google Scholar]
Haldun 2002 {published data only}
- Haldun S, Mehmet S, Perhan G, Ilkten C, Besti U. Optimal treatment of schizophrenia. 12th World Congress of Psychiatry; 2002 Aug 24‐29; Yokohama, Japan. 2002.
Hartman 1983 {published data only}
- Hartman LM, Cashman FE. Cognitive‐behavioral and psychopharmacological treatment of delusional symptoms: a preliminary report. Behavioural Psychotherapy 1983;11:50‐61. [Google Scholar]
Hayward 1995 {published data only}
- Hayward P, Chan N, Kemp R, Youle S, David A. Medication self‐management: a preliminary report on an intervention to improve medication compliance. Journal of Mental Health 1995;4:511‐7. [Google Scholar]
Hayward 2009 {published data only}
- Hayward P, David AS, Green N, Rabe‐Hesketh S, Haworth E, Thompson N, et al. Promoting therapeutic alliance in clozapine users: an exploratory randomized controlled trial. Clinical Schizophrenia and Related Psychoses 2009;3(3):127‐32. [Google Scholar]
Herz 2000 {published data only}
- Herz MI, Lamberti JS, Mintz J, Scott R, O'Dell SP, McCartan L, et al. A program for relapse prevention in schizophrenia: a controlled study. Archives of General Psychiatry 2000;57(3):277‐83. [DOI] [PubMed] [Google Scholar]
Hodel 1994 {published data only}
- Hodel B, Brenner HD. Cognitive therapy with schizophrenic patients: conceptual basis, present state, future directions. Acta Psychiatrica Scandinavica 1994;90S:108‐15. [DOI] [PubMed] [Google Scholar]
Hogarty 1991 {published data only}
- Hogarty GE, Anderson CM, Reiss DF, Kornblith SJ, Greenwald DP, Ulrich RF, et al. Family psychoeducation, social skills training, and maintenance chemotherapy in the aftercare treatment of schizophrenia: II. Two year effects of a controlled study on relapse and adjustment. Archives of General Psychiatry 1991;48:340‐7. [DOI] [PubMed] [Google Scholar]
Hogarty 1997 {published data only}
- Hogarty G, Cornblith S, Greenwald D, DiBarry A, Cooley S, Ulrich R, et al. Three‐year trials of personal therapy among schizophrenic patients living with or independent of family. I. Description of study and effects on relapse rates. American Journal of Psychiatry 1997;154(11):1504‐13. [DOI] [PubMed] [Google Scholar]
- Hogarty G, Greenwald D, Ulrich R, Cornblith S, DiBarry A, Cooley S, et al. Three‐year trials of personal therapy among schizophrenic patients living with or independent of family. II: Effects on adjustment of patients. American Journal of Psychiatry 1997;154(11):1514‐24. [DOI] [PubMed] [Google Scholar]
Hogarty 2004 {published data only}
- Hogarty GE, Flesher S, Ulrich R, Carter M, Greenwald D, Pogue‐Geile M, et al. Cognitive enhancement therapy for schizophrenia: effects of a 2‐year randomized trial on cognition and behavior. Archives of General Psychiatry 2004;61(9):866‐76. [DOI] [PubMed] [Google Scholar]
Jackson 1998 {published data only}
- Jackson H, McGorry P, Edwards J, Hulbert C, Henry L, Francey S, et al. Cognitively oriented psychotherapy for early psychosis (COPE): priminary results. British Journal of Psychiatry 1998;172(Suppl 33):93‐100. [PubMed] [Google Scholar]
Jackson 2001 {published data only}
- Jackson C. Promoting personal recovery from psychosis: a randomised control trial in first episode schizophrenia. National Research Register 2001.
Kemp 1996b {published data only}
- Kemp R, David A. Compliance therapy: an intervention targeting insight and treatment adherence in psychotic patients. Behavioural and Cognitive Psychotherapy 1996;24:331‐50. [Google Scholar]
Kingdon 1991 {published data only}
- Kingdon D, Turkington D. The use of cognitive behavior therapy with a normalizing rationale in schizophrenia. Journal of Nervous and Mental Disease 1991;179(4):207‐11. [DOI] [PubMed] [Google Scholar]
Kuipers 1996 {published data only}
- Kuipers E. The management of difficult to treat patients with schizophrenia, using non‐drug therapies. British Journal of Psychiatry 1996;169:41‐51. [PubMed] [Google Scholar]
Kuipers 2004 {published data only}
- Kuipers E, Holloway F, Rabe‐Hesketh S, Tennakoon L. An RCT of early intervention in psychosis: Croydon outreach and assertive support team (COAST). Social Psychiatry and Psychiatric Epidemiology 2004;39(5):358‐63. [DOI] [PubMed] [Google Scholar]
Kukla 2014 {published data only}
- Kukla M, Davis LW, Lysaker PH. Cognitive behavioral therapy and work outcomes: correlates of treatment engagement and full and partial success in schizophrenia. Behavioural and Cognitive Psychotherapy 2014;42(05):577‐92. [DOI] [PubMed] [Google Scholar]
Lecompte 1996 {published data only}
- Lecompte D, Pelc I. A cognitive‐behavioral program to improve compliance with medication in patients with schizophrenia. International Journal of Mental Health 1996;25(1):51‐6. [Google Scholar]
Lysaker 2009 {published data only}
- Lysaker PH, Davis LW, Bryson GJ, Bell MD. Effects of cognitive behavioral therapy on work outcomes in vocational rehabilitation for participants with schizophrenia spectrum disorders. Schizophrenia Research 2009;107:186‐91 . [DOI] [PubMed] [Google Scholar]
MacPherson 1996 {published data only}
- MacPherson R, Jerrom B, Hughes A. A controlled study of education about drug treatment of schizophrenia. British Journal of Psychiatry 1996;168:709‐17. [DOI] [PubMed] [Google Scholar]
May 1984 {published data only}
- May PR. A step forward in research on psychotherapy of schizophrenia. Schizophrenia Bulletin 1984;10:604‐7. [DOI] [PubMed] [Google Scholar]
McGorry 2002 {published data only}
- McGorry P, Yung A, Phillips L, Yuen H, Francey S, Cosgrave E, et al. Randomised controlled trial of interventions designed to reduce the risk of progression to first‐episode psychosis in a clinical sample with subthreshold symptoms. Archives of General Psychiatry 2002;59:921‐8. [DOI] [PubMed] [Google Scholar]
Morrison 2002 {published data only}
- Morrison AP, Bentall RP, French P, Walford L, Kilcommons A, Knight A, et al. Randomised controlled trial of early detection and cognitive therapy for preventing transition to psychosis in high‐risk individuals. British Journal of Psychiatry 2002;181(43):78‐84. [DOI] [PubMed] [Google Scholar]
O'Connor 2007 {published data only}
- O’Connor K, Stip E, Pélissier MC, Aardema F, Guay S, Gaudette G, et al. Treating delusional disorder: a comparison of cognitive behavioural therapy and attention placebo control. Canadian Journal of Psychiatry 2007;52(3):182‐90. [DOI] [PubMed] [Google Scholar]
Olbrich 1990 {published data only}
- Olbrich R, Mussgay L. Reducton of schizophrenic deficits by cognitive training: an evaluative study. European Archives of Psychiatry and Neurological Sciences 1990;239:366‐9. [DOI] [PubMed] [Google Scholar]
Perris 1992 {published data only}
- Perris C. A cognitive‐behavioral treatment program for patients with a schizophrenic disorder. New Directions for Mental Health Services 1992;53:21‐32. [DOI] [PubMed] [Google Scholar]
Rector 2003 {published data only}
- Rector NA, Seeman MV, Segal ZV. Cognitive therapy for schizophrenia: a preliminary randomized controlled trial. Schizophrenia Research 2003;63:1‐11. [DOI] [PubMed] [Google Scholar]
Roder 2002 {published data only}
- Roder V, Brenner HD, Muller D, Lachler M, Zorn P, Reisch T, et al. Development of specific social skills training programmes for schizophrenia patients: results of a multi‐centre study. Acta Psychiatrica Scandinavica 2002;105:363‐71. [DOI] [PubMed] [Google Scholar]
Sellwood 2001 {published data only}
- Sellwood W, Barrowclough C, Tarrier N, Quinn J, Mainwaring J, Lewis S. Needs‐based cognitive‐behavioural family intervention for carers of patients suffering from schizophrenia: 12‐month follow‐up. Acta Psychiatrica Scandinavica 2001;104(5):346‐55. [DOI] [PubMed] [Google Scholar]
- Sellwood W, Wittkowski A, Tarrier N, Barrowclough C. Needs‐based cognitive‐behavioural family intervention for patients suffering from schizophrenia: 5‐year follow‐up of a randomized controlled effectiveness trial. Acta Psychiatrica Scandinavica 2007;116(6):447‐52. [DOI] [PubMed] [Google Scholar]
Shawyer 2012 {published data only}
- Shawyer F, Farhall J, Mackinnon A, Trauer T, Sims E, Ratcliff K, et al. A randomised controlled trial of acceptance‐based cognitive behavioural therapy for command hallucinations in psychotic disorders. Behaviour Research and Therapy 2012;50:110‐21. [DOI] [PubMed] [Google Scholar]
Shon 2002 {published data only}
- Shon K, Park S. Medication and symptom management education program for the rehabilitation of psychiatric patients in Korea: the effects of promoting schedule on self‐efficacy theory. Yonsei Medical Journal 2002;43(5):579‐89. [DOI] [PubMed] [Google Scholar]
Spaulding 1992 {published data only}
- Spaulding WD. Design prerequisites for research on cognitive therapy for schizophrenia. Schizophrenia Bulletin 1992;18:139‐42. [DOI] [PubMed] [Google Scholar]
Startup 1998 {unpublished data only}
- Startup M, Jackson M. A controlled trial of cognitive behaviour therapy for schizophrenia and related disorders. Wales Office of Research and Development for Health and Social Care 2003. [Grant number: RC012]
- Wales Office of Research and Development for Heatlh and Social Care. A controlled trial of cognitive behaviour therapy for schizophrenia and related disorders. dialspace.dial.pipex.com/word/ (accessed prior to 01 June 2017).
Startup 2006 {published data only}
- Startup M, Jackson MC, Startup S. Insight and recovery from acute psychotic episodes: the effects of cognitive behavior therapy and premature termination of treatment. Journal of Nervous and Mental Disorders 2006;194(10):740‐5. [DOI] [PubMed] [Google Scholar]
Tarrier 1993 {published data only}
- Tarrier N, Beckett R, Harwood S, Baker A, Yusupoff L, Ugarteburu I. A trial of two cognitive behavioural methods of treating drug‐resistant residual psychotic symptoms in schizophrenic patients: I. Outcome. British Journal of Psychiatry 1993;162:524‐32. [DOI] [PubMed] [Google Scholar]
- Tarrier N, Sharpe L, Beckett R, Harwood S, Baker A, Yusopoff L. A trial of two cognitive behavioural methods of treating drug resistant residual psychotic symptoms in schizophrenic patients: II. Treatment specific changes in coping and problem solving skills. Social Psychiatry and Psychiatric Epidemiology 1993;28:5‐10. [DOI] [PubMed] [Google Scholar]
Turkington 2002 {published data only}
- Turkington D, Kingdon D, Turner T. Effectiveness of a brief cognitive behavioural therapy intervention in the treatment of schizophrenia. British Journal of Psychiatry 2002;180:523‐7. [DOI] [PubMed] [Google Scholar]
Turkington 2006 {published data only}
- Turkington D, Kingdon D, Rathod S, Hammond K, Pelton J, Mehta R. Outcomes of an effectiveness trial of cognitive‐behavioural intervention by mental health nurses in schizophrenia. British Journal of Psychiatry 2006;189:36‐40. [DOI] [PubMed] [Google Scholar]
Van Der Gaag 2003 {published data only}
- Gaag M, Kern RS, Bosch RJ, Liberman RP. A controlled trial of cognitive remediation in schizophrenia. Schizophrenia Bulletin 2003;28:167‐76. [DOI] [PubMed] [Google Scholar]
Velligan 2002 {published data only}
- Velligan DI, Prihoda TJ, Ritch JL, Maples M, Bow‐Thomas CC, Dassori A. A randomized single blind pilot study of compensatory strategies in schizophrenia out‐patients. Schizophrenia Bulletin 2002;28(2):283‐92. [DOI] [PubMed] [Google Scholar]
Wirshing 1992 {published data only}
- Eckman TA, Wirshing WC, Marder SR, Liberman RP, Johnston‐Cronk K, Zimmerman K, et al. Technique for training schizophrenic patients in illness self‐management: a controlled trial. American Journal of Psychiatry 1992;149:1549‐55. [DOI] [PubMed] [Google Scholar]
- Wirshing WC, Marder SR, Eckman T, Liberman RP, Mintz J. Acquisition and retention of skills training methods in chronic schizophrenic outpatients. Psychopharmacology Bulletin 1992;28:241‐5. [PubMed] [Google Scholar]
Wykes 2002 {published data only}
- Wykes T. The effectiveness of cognitive remediation therapy (CRT) for patients with schizophrenia. National Research Register 2002.
Wykes 2003 {published data only}
- Wykes T, Thompson N, Green N, Surgaldze S, Hayward P. Changing voices: a randomised control trial of group cognitive behavioural treatment. Schizophrenia Research 2003;60:331. [Google Scholar]
- Wykes T, Thompson N, Hyward P. Changing voices: a randomised control trial of group cognitive treatment. Schizophrenia Research 2002;53(Suppl 1):12. [DOI] [PubMed] [Google Scholar]
Xie 2010 {published data only}
- Xie H, Li R. Cognitive therapy to medication compliance in first‐episode schizophrenia patients [认知治疗对首发精神分裂症患者服药依从性的影响]. Attend to Practice and Research [护理实践与研究] 2010;7(22):17‐8. [Google Scholar]
References to studies awaiting assessment
Chung 2001 {published data only}
- Chung YC, Kim JH, Eun HB, Hwang IK. Effect of cognitive‐behavioral therapy on the delusion in schizophrenic patients. Journal of the Korean Neuropsychiatric Association 2001;40(1):63‐71. [Google Scholar]
Clarke 2011 {published data only}
- Clarke S. A randomised control trial comparing the effectiveness of acceptance and commitment therapy with treatment as usual, cognitive behavioural therapy, with treatment resistant participants. public.ukcrn.org.uk (accessed prior to 02 June 2016).
D'Souza 2002 {published data only}
- D'Souza R, Rich D, Diamond I, Godfery K. A open randomized control study using a spiritually augmented cognitive behaviour therapy for demoralization and treatment adherence in patients with schizophrenia. Australian and New Zealand Journal of Psychiatry 2002;36(6):A9‐A. [Google Scholar]
Delahaye 2009 {published data only}
- Delahaye N, Pieters G. Cognitive behavior therapy and family therapy for relapse prevention and symptom reduction in psychosis: randomized controlled efficacy study. Tijdschrift voor Psychiatrie Netherlands 2009;51(10):779‐80. [Google Scholar]
ISRCTN60855021 2009 {published data only}
- ISRCTN60855021. Social anxiety research clinic: an exploratory randomised controlled trial of standard versus enhanced cognitive behavioural therapy for social anxiety in early psychosis. www.isrctn.com/ISRCTN60855021 (retrospectively received 21 October 2010).
Jones 2012 {published data only}
- Jones P. Cts: cognitive training for schizophrenia. public.ukcrn.org.uk/Search/StudyDetail.aspx?StudyID=11571. (accessed prior to 01 June 2017).
Klingberg 2001 {published data only}
- Klingberg S, Wiedemann G, Buchkremer G. Cognitive‐behavioural therapy for schizophrenic patients ‐ design and preliminary results of a randomised effectiveness trial. Zeitschrift Für Klinische Psychologie Und Psychotherapie 2001;30(4):259‐67. [Google Scholar]
Klingberg 2013 {published data only}
- Klingberg S, Wittorf A, Meisner C, Wolwer W, Wiedemann G, Bechdolf A, et al. Specific efficacy of cognitive behavioral therapy for the treatment of persistent positive symptoms in schizophrenia patients. Schizophrenia Bulletin 2013;39:S338‐9. [Google Scholar]
- Klingberg S, Wittorf A, Meisner C, Wolwer W, Wiedemann G, Herrlich J, et al. Cognitive behavioral therapy versus supportive therapy for persistent positive symptoms in psychotic disorders: major results of the positive study. European Archives of Psychiatry and Clinical Neuroscience 2011;261:S13. [Google Scholar]
- Klingberg S, Wittorf A, Meisner C, Wolwer W, Wiedemann G, Herrlich J, et al. Cognitive behavioural therapy versus supportive therapy for persistent positive symptoms in psychotic disorders: the positive study, a multicenter, prospective, single‐blind, randomised controlled clinical trial. Trials 2010;11:123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Konnopka A, Stuhldreher N, Klingberg S, Wittorf A, Bechdolf A, Muller B, et al. Costs of psychotic disorders and cost‐effectiveness of cognitive behavioural therapy compared to supportive treatment. Journal of Mental Health Policy and Economics 2013;16:S19. [Google Scholar]
- Wagner M. Cognitive biases and cognitive deficits in patients with positive symptoms: relationship with symptoms and with symptom change during psychotherapy. European Archives of Psychiatry and Clinical Neuroscience 2011;261:S14. [Google Scholar]
- Wittorf A, Klingberg S. The therapeutic alliance in CBT for pychoses: course and predictive value for outcome. European Archives of Psychiatry and Clinical Neuroscience 2011;261:S13‐S4. [Google Scholar]
Lee 1999 {published data only}
- Lee HS, Hyun MH, Cho HS, Lee YH, Kim TY, Chang SA, et al. Effects of cognitive differentiation training of intergrated psychological therapy to the basic cognitive functions in schizophrenic patients. Journal of the Korean Neuropsychiatric Association 1998;37:801‐10. [Google Scholar]
- Lee MH, Lee HS, Cho HS, An SK, Hyun MH, Kim TY, et al. Development of a cognitive rehabilitation program for patients with schizophrenia. Journal of the Korean Neuropsychiatric Association 1999;38:375‐88. [Google Scholar]
Lystad 2013 {published data only}
- Lystad JU, Bull HC, Ueland T, Falkum E. A randomized clinical trial of cognitive remediation versus cognitive behavioral therapy techniques in vocational rehabilitation for adults with schizophrenia spectrum disorders ‐ sample characteristics of the first 40 participants in each intervention. Schizophrenia Bulletin 2013;39:S297. [Google Scholar]
Mirabella 2009 {published data only}
- Mirabella F, Rosicarelli ML, Broccoli G, Leoncini L, Marchesini N, Morosini P. Effectiveness assessment of a structured cognitive‐behavioural group therapy on psychiatric inpatients in day centres. Psicoterapia Cognitiva e Comportamentale 2009;15:329‐52. [Google Scholar]
NCT00980252 2009 {published data only}
- NCT00980252. Medication adherence in schizophrenia: development of a CBT‐based intervention. www.clinicaltrials.gov/show/NCT00980252 (first received 18 September 2009).
NCT01139502 2010 {published data only}
- NCT01139502. Cognitive behaviour therapy and cognitive training in work rehabilitation for persons with severe mental illness. ClinicalTrials.gov/show/NCT01139502 Vol. (first received 2 June 2 2010).
Penades 2006 {published data only}
- Penades R, Catalan R, Salamero M, Gasto C. Randomised controlled trial of cognitive remediation therapy for outpatients with chronic schizophrenia. 13th Biennial Winter Workshop on Schizophrenia Research; 2006 Feb 4‐10; Davos, Switzerland. Davos, SWITZERLAND: Elsevier Science Bv, 2006:102‐3.
Valmaggia 2003 {published data only}
- Valmaggia LR, Gaag M. A randomised controlled trial of cognitive behaviour therapy for treatment refractory schizophrenia. 9th International Congress on Schizophrenia Research; 2003 Mar 29‐Apr 2; Colorado Spings, Colorado, USA. Colorado Spings, Colorado: Elsevier Science Bv, 2003:305.
Wu 2008 {published data only}
- Wu N, Wang Q, Kong L. A controlled study of cognitive behaviour therapy in chronic schizophrenia. Journal of Clinical Psychosomatic Diseases 2008;14(3):206. [Google Scholar]
References to ongoing studies
NCT01992913 2014 {published data only}
- NCT01992913. Integrated cognitive behavior therapy to improve work outcomes in schizophrenia. Clinicaltrials.gov/show/NCT01992913 (first received 01 November 2013).
NCT02170051 2014 {published data only}
- NCT02170051. Improving negative symptoms of psychosis in real‐world environments. http://Clinicaltrials.gov/show/NCT02170051 (first received 18 June 2014).
NCT02349880 2015 {published data only}
- NCT02349880. A shared decision‐making training for inpatients with schizophrenia. https://Clinicaltrials.gov/ct2/show/NCT02349880 (first received 23 January 2015).
Xu 2008 {published data only}
- Xu Z, Li Z. A randomized controlled trial of cognitive‐behavioral therapy for schizophrenia. www.chictr.org/ (accessed prior to 02 June 2017).
Additional references
Alford 1994
- Alford BA, Beck AT. Cognitive therapy of delusional beliefs. Behaviour Research and Therapy 1994;32:369‐80. [DOI] [PubMed] [Google Scholar]
Altman 1996
- Altman DG, Bland JM. Detecting skewness from summary information. BMJ 1996;313:1200. [DOI] [PMC free article] [PubMed] [Google Scholar]
Andreasen 1984
- Andreasen NC. Scale for the Assessment of Negative Symptoms (SANS). University of Iowa, 1984. [PubMed] [Google Scholar]
Asberg 1978
- Asberg M, Montgomery S, Perris C, Shalling D, Sedvall G. A comprehensive psychopathological rating scale. Acta Psychiatrica Scandinavicia 1978;271:5‐27. [DOI] [PubMed] [Google Scholar]
Beck 1961
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Archives General Psychiatry 1961;4:561‐71. [DOI] [PubMed] [Google Scholar]
Beck 1988
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. Journal of Consulting and Clinical Psychology 1988;56(6):893‐7. [DOI] [PubMed] [Google Scholar]
Beck 2004
- Beck AT, Baruch E, Balter JM, Steer RA, Warman DM. A new instrument for measuring insight: the Beck cognitive insight scale. Schizophrenia Research 2004;68(2):319‐30. [DOI] [PubMed] [Google Scholar]
Beck 2005
- Beck AT. The current state of cognitive therapy. Archives of General Psychiatry 2005;62:953‐9. [DOI] [PubMed] [Google Scholar]
Begg 1996
- Begg C, Cho M, Eastwood S, Horton R, Moher D, Olkin I, et al. Improving the quality of randomized controlled trials. The CONSORT statement. JAMA 1996;276:637‐9. [DOI] [PubMed] [Google Scholar]
Bellack 2006
- Bellack A S, Brown C H, Thomas‐Lohrman S. Psychometric characteristics of role‐play assessments of social skill in schizophrenia. Behavior Therapy 2006;37(4):339‐52. [DOI] [PubMed] [Google Scholar]
Birchwood 1990
- Birchwood M, Smith J, Cochrane R, Wetton C, Copestake S. The social functioning scale: the development and validation of a new scale of social adjustment for use in family intervention programmes with schizophenic patients. British Journal of Psychiatry 1990;157:853‐9. [DOI] [PubMed] [Google Scholar]
Birchwood 1994
- Birchwood M, Smith J, Drury V, Healy J, Macmillan F, Slade M. A self‐report Insight Scale for psychosis: reliability, validity and sensitivity to change. Acta Psychiatrica Scandinavica 1994;89(1):62‐7. [DOI] [PubMed] [Google Scholar]
Birchwood 2006
- Birchwood M, Trower P. The future of cognitive–behavioural therapy for psychosis: not a quasi‐neuroleptic. British Journal of Psychiatry 2006;188:107‐8. [DOI] [PubMed] [Google Scholar]
Bland 1997
- Bland JM. Statistics notes. Trials randomised in clusters. BMJ 1997;315:600. [DOI] [PMC free article] [PubMed] [Google Scholar]
Boissel 1999
- Boissel JP, Cucherat M, Li W, Chatellier G, Gueyffier F, Buyse M, et al. The problem of therapeutic efficacy indices. 3. Comparison of the indices and their use. Therapie 1999;54(4):405‐11. [PubMed] [Google Scholar]
Brambilla 2000
- Brambilla S, Pioli R. Development, reliability and acceptability of a new version of the DSM‐IV social and occupational functioning assessment scale (SOFAS) to assess routine social funtioning. Acta Psychiatrica Scandinavica 2000;101:323‐9. [PubMed] [Google Scholar]
Brazier 1993
- Brazier J, Jones N, Kind P. Testing the validity of the EuroQol and comparing it with the SF–36 health survey questionnaire. Quality of Life Research 1993;2:169–80. [DOI] [PubMed] [Google Scholar]
Castle and Morgan 2008
- Castle David J, Morgan V. Epidemiology Chapter 2. In: Mueser K.T, Jeste D.V editor(s). Clinical Handbook of Schizophrenia. Guilford Press, 2008:14‐25. [Google Scholar]
Christison 1991
- Christison GW, Kirch DG, Wyatt RJ. When symptoms persist: choosing among alternative somatic symptoms for schizophrenia. Schizophrenia Bulletin 1991;17:217‐45. [DOI] [PubMed] [Google Scholar]
David 1990
- David AS. Insight and psychosis. British Journal of Psychiatry 1990;156:789‐808. [DOI] [PubMed] [Google Scholar]
Davis 1977
- Davis JM, Casper R. Antipsycotic drugs: clinical pharmacology and therapeutic use. Drugs 1977;14:260‐82. [DOI] [PubMed] [Google Scholar]
Deeks 2000
- Deeks J. Issues in the selection for meta‐analyses of binary data. 8th International Cochrane Colloquium; 2000 Oct 25‐28th; Cape Town, South Africa. 2000.
Deeks 2011
- Deeks JJ, Higgins JP, Altman DG. Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Green S editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Department of Health 1983
- Department of Health. Mental Health Act. www.legislation.gov.uk/ukpga/1983/20/contents (accessed prior to 02 June 2017).
Derogatis 1975
- Derogatis LR. SCL‐90‐R: Symptom Checklist‐90‐R. SCL‐90‐R: Symptom Checklist‐90‐R: Administration, Scoring, and Pprocedures Manual. NCS Pearson, 1975. [Google Scholar]
Divine 1992
- Divine GW, Brown JT, Frazier LM. The unit of analysis error in studies about physicians' patient care behavior. Journal of General Internal Medicine 1992;7(6):623‐9. [DOI] [PubMed] [Google Scholar]
Donner 2002
- Donner A, Klar N. Issues in the meta‐analysis of cluster randomized trials. Statistics in Medicine 2002;21:2971‐80. [DOI] [PubMed] [Google Scholar]
Egger 1997
- Egger M, Davey‐Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a simple graphical test. BMJ 1997;315:629‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne D, Altman DG, Higgins JPT, Curtina F, Worthingtond HV, Vaile A. Meta‐analyses involving cross‐over trials: Methodological issues. International Journal of Epidemiology 2002;31(1):140‐9. [DOI] [PubMed] [Google Scholar]
Endicott 1976
- Endicott J, Spitzer R, Fleiss J, Cohen CJ. The global assessment scale. A procedure to measuring overall severity of psychiatric disturbance. Archives of General Psychiatry 1976;33:766‐71. [DOI] [PubMed] [Google Scholar]
Furukawa 2006
- Furukawa TA, Barbui C, Cipriani A, Brambilla P, Watanabe N. Imputing missing standard deviations in meta‐analyses can provide accurate results. Journal of Clinical Epidemiology 2006;59(7):7‐10. [DOI] [PubMed] [Google Scholar]
Goodman 1989
- Goodman W K, Price L H, Rasmussen S A, et al. The Yale‐Brown Obsessive Compulsive Scale: I. development, use, and reliability. Archives of General Psychiatry 1989;46(11):1006‐11. [DOI] [PubMed] [Google Scholar]
Greenberg 2005
- Greenberg G A, Rosenheck R A. Using the GAF as a national mental health outcome measure in the Department of Veterans Affairs. Psychiatric Services 2005;56(4):420‐6. [DOI] [PubMed] [Google Scholar]
Gulliford 1999
- Gulliford MC. Components of variance and intraclass correlations for the design of community‐based surveys and intervention studies: data from the Health Survey for England 1994. American Journal of Epidemiology 1999;149:876‐83. [DOI] [PubMed] [Google Scholar]
Haddock 1999b
- Haddock G, McCarron J, Tarrier N, Faragher EB. Scales to measure dimensions of hallucinations and delusions: the psychotic symptom rating scales (PSYRATS). Psychological Medicine 1999;29(4):879‐89. [DOI] [PubMed] [Google Scholar]
Hamilton 1976
- Hamilton M. HAMA Hamilton Anxiety Scale. ECDEU Assessment Manual for Psychopharmacology 193‐8.
Hamilton 1967
- Hamilton M. Development of a rating scale for primary depressive illness. British Journal of Social and Clinical Psychology 1967;6(4):278‐96. [DOI] [PubMed] [Google Scholar]
Heinrichs 1984
- Heinrichs DW, Hanlon TE, Carpenter WT Jr. The quality of life scale: an instrument for rating the schizophrenic deficit syndrome. Schizophrenia Bulletin 1984;10:338‐98. [DOI] [PubMed] [Google Scholar]
Heinrichs 1984a
- Heinrichs DW, Hanlon TE, Carpenter W T Jr. The Quality of Life Scale: an instrument for rating the schizophrenic deficit syndrome. Schizophrenia Bulletin 1984;10(3):388‐98. [DOI] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327:557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Chapter 7: Selecting studies and collecting data. In: Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Higgins 2011a
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Hogan 1983
- Hogan TP, Awad AG, Eastwood R. A self‐report scale predictive of drugcompliance in schizophrenics: reliability and discriminative validity. Psychological Medicine 1983;13(1):177‐83. [DOI] [PubMed] [Google Scholar]
Hornung 1996
- Hornung WP, Kieserg A, Feldmann R. Psychoeducational training for schizophrenic patients: background, procedure and empirical findings. Patient Education and Counseling 1996;29:257‐68. [DOI] [PubMed] [Google Scholar]
Hornung 1999
- Hornung WP, Feldmann R, Klingberg S, Buchkremer G, Reker T. Long‐term effects of psychoeducational psychotherapeutic intervention for schizophrenic outpatients and their key‐persons: results of a five‐year follow‐up. European Archives of Psychiatry and Clinical Neuroscience 1999;29:162‐7. [DOI] [PubMed] [Google Scholar]
Hutton 2009
- Hutton JL. Number needed to treat and number needed to harm are not the best way to report and assess the results of randomised clinical trials. British Journal of Haematology 2009;146(1):27‐30. [DOI] [PubMed] [Google Scholar]
Jones 2004
- Jones C, Cormac I, Mota J, Campbell C. Cognitive behaviour therapy for schizophrenia. Cochrane Database of Systematic Reviews 2004, Issue 2. [DOI: 10.1002/14651858.CD000524.pub2] [DOI] [PubMed] [Google Scholar]
Jones 2009a
- Jones C, Cormac I, Campbell C, Meaden A, Hacker D, Irving CB. Cognitive behaviour therapy versus specific pharmacological treatments for schizophrenia. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD007965] [DOI] [Google Scholar]
Jones 2009b
- Jones C, Campbell C, Cormac I, Hacker D, Meaden A, Irving CB. Cognitive behaviour therapy versus standard care for schizophrenia. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD007964] [DOI] [Google Scholar]
Kay 1986
- Kay SR, Opler LA, Fiszbein A. Positive and Negative Syndrome Scale (PANSS) Manual. 1986. North Tonawanda, NY: Multi‐Health Systems, 1986. [Google Scholar]
Kay 1987
- Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophrenia Bulletin 1987;13(2):261‐76. [DOI] [PubMed] [Google Scholar]
King 2007
- King M, Dinos S, Shaw J, Watson R, Stevens S, Passetti F, et al. The Stigma Scale: development of a standardised measure of the stigma of mental illness. British Journal of Psychiatry 2007;190:248‐54. [DOI] [PubMed] [Google Scholar]
Kingdon 2004
- Kingdon DG, Turkington D. Cognitive Therapy of Schizophrenia (Guides to Individualized Evidence‐Based Treatment). New York: Guilford Press, 2004. [Google Scholar]
Klingberg 2008
- Klingberg S, Hesse K, Herrlich J, Kossowa, Wiedmann G, Wittorf A, et al. Cognitive behavioral therapy on negative symptoms of schizophrenia disorders—background and therapy of the TONES study. Nervenheilkunde 2008;27:997‐1006. [Google Scholar]
Klingberg 2009
- Klingberg S, Wittorf A, Herrlich J, et al. Cognitive behavioural treatment of negative symptoms in schizophrenia patients: study design of the TONES study, feasibility and safety of treatment. European Archives of Psychiatry and Clinical Neuroscience 2009;259:S149‐54. [DOI] [PubMed] [Google Scholar]
Leon 2006
- Leon AC, Mallinckrodt CH, Chuang‐Stein C, Archibald DG, Archer GE, Chartier K. Attrition in randomized controlled clinical trials: methodological issues in psychopharmacology. Biological Psychiatry 2006;59(11):1001‐5. [DOI] [PubMed] [Google Scholar]
Leucht 2005a
- Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel R. What does the PANSS mean?. Schizophrenia Research 2005;79:231‐8. [DOI] [PubMed] [Google Scholar]
Leucht 2005b
- Leucht S, Kane JM, Kissling W, Hamann J, Etschel E, Engel R. Clinical implications of Brief Psychiatric Rating Scale scores. British Journal of Psychiatry 2005;187:366‐71. [DOI] [PubMed] [Google Scholar]
Liberman 1994
- Liberman R P. Psychosocial treatments for schizophrenia. Psychiatry 1994;57(2):104‐14. [DOI] [PubMed] [Google Scholar]
Marshall 2000
- Marshall M, Lockwood A, Adams C, Bradley C, Joy C, Fenton M. Unpublished rating scales ‐ a major source of bias in randomised controlled trials of treatments for schizophrenia?. British Journal of Psychiatry 2000;176:249‐52. [DOI] [PubMed] [Google Scholar]
McKenna 2007
- McKenna PJ. Schizophrenia and Related Syndromes. 2nd Edition. London: Routledge, 2007. [Google Scholar]
Meltzer 1992
- Meltzer HY. Treatment of the neuroleptic‐nonresponsive schizophrenic patient. Schizophrenia Bulletin 1992;18:515‐42. [DOI] [PubMed] [Google Scholar]
Moher 2001
- Moher D, Schulz KF, Altman D. The CONSORT statement: revised recommendations for improving the quality of reports of parallel‐group randomized trials. JAMA 2001;285:1987‐91. [DOI] [PubMed] [Google Scholar]
Montgomery 1979
- Montgomery S, Asberg M. A new depression scale designed to be sensitive to change. British Journal of Psychiatry 1979;154:382‐9. [DOI] [PubMed] [Google Scholar]
Morosini 2000
- Morosini PL, Magliano L, Brambilla L, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM‐IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatrica Scandinavica 2000;101(4):323‐9. [PubMed] [Google Scholar]
NICE 2014
- National Institute for Clinical Excellence. Psychosis and schizophrenia in adults: prevention and management. www.nice.org.uk/guidance/cg178/chapter/1‐Recommendations (accessed on 01 January 2018. [PubMed]
Novaco 2003
- Novaco RW. The Novaco Anger Scale and Provocation Inventory (NAS‐PI). Los Angeles: Western Psychological Services, 2003. [Google Scholar]
Overall 1962
- Overall J, Gorham D. The brief psychiattric rating scale. Psychological Reports 1962;10:799‐812. [Google Scholar]
Pilling 2002
- Pilling S, Bebbington P, Kuipers E, Garety P, Geddes J, Martindale B, et al. Psychological treatments in schizophrenia : II. Meta‐analyses of randomized controlled trials of social skills training and cognitive remediation. Psychological Medicine 2002;32:783‐91. [DOI] [PubMed] [Google Scholar]
Pukrop 2000
- Pukrop R, Moller HJ, Steinmeyer EM. Quality of life in psychiatry: a systematic contribution to construct validation and the development of the integrative assessment tool "modular system for quality of life". European Archives of Psychiatry and Clinical Neuroscience 2000;250(3):120‐32. [DOI] [PubMed] [Google Scholar]
Rosenberg 1965
- Rosenberg M. The measurement of self‐esteem. Society and the Adolescent Self Image. Princeton University Press, 1965:297‐307. [Google Scholar]
Royal College of Psychiatrists 2012
- Royal College of Psychiatrists (2012). Report of the National Audit of Schizophrenia (NAS) 2012. London: Healthcare Quality Improvement Partnership.
Schünemann 2011
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and 'Summary of findings' tables. In: Higgins JPT, Green S (editors), Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Sterne 2011
- Sterne JAC, Egger M, Moher D editor(s). Chapter 10: Addressing reporting biases. In: Higgins JPT, Green S editor(s). Cochrane Handbook for Systematic Reviews of Intervention.. Available from www.handbook.cochrane.org.
Tarrier 1993a
- Tarrier N, Beckett R, Harwood S, Baker A, Yusupoff L, Ugarteburu I. A trial of two cognitive‐behavioural methods of treating drug‐resistant residual psychotic symptoms in schizophrenic patients: I. Outcome. British Journal of Psychiatry 1993;162:524‐32. [DOI] [PubMed] [Google Scholar]
Trower 2004
- Trower P, Birchwood M, Meaden A, Bryne S, Nelson A, Ross K. Cognitive therapy for command hallucinations: randomised controlled trial. British Journal of Psychiatry 2004;184:312‐20. [DOI] [PubMed] [Google Scholar]
Turkington 2004
- Turkington D, Dudley R, Warman DM, Beck AT. Cognitive‐behavioral therapy for schizophrenia: a review. Journal of Psychiatric Practice 2004;10(1):5‐16. [DOI] [PubMed] [Google Scholar]
Ukoumunne 1999
- Ukoumunne OC, Gulliford MC, Chinn S, Sterne JAC, Burney PGJ. Methods for evaluating area‐wide and organistation‐based intervention in health and health care: a systematic review. Health Technology Assessment 1999;3(5):1‐75. [PubMed] [Google Scholar]
Wallace 2002
- Wallace KA, Wheeler AJ. Reliability generalization of the life satisfaction index. Educational and Psychological Measurement 2002;62:674–684. [Google Scholar]
Webster 1997
- Webster CD, Douglas KS, Eaves D, Hart SD. HCR–20: Assessing Risk for Violence. 2nd Edition. Simon Fraser University, 1997. [Google Scholar]
Wolwer 2005
- Wolwer W, Frommann N, Halfmann S, Piaszek A, Streit M, Gaebel W. Remediation of impairments in facial affect recognition in schizophrenia: efficacy and specificity of a new training program. Schizophrenia Research 2005;80:295‐303. [DOI] [PubMed] [Google Scholar]
Wykes 2004
- Wykes T. Psychological treatment for voices in psychosis. Cognitive Neuropsychiatry 2004;9:25‐41. [DOI] [PubMed] [Google Scholar]
Xia 2009
- Xia J, Adams CE, Bhagat N, Bhagat V, Bhoopathi P, El‐Sayeh H, et al. Losing participants before the trial ends erodes credibility of findings. Psychiatric Bulletin 2009;33:254‐7. [Google Scholar]
Zhao 2015
- Zhao S, Sampson S, Xia J, Jayaram MB. Psychoeducation (brief) for people with serious mental illness. Cochrane Database of Systematic Reviews 2015, Issue 4. [DOI: 10.1002/14651858.CD010823.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Zung 1971
- Zung WW. A rating instrument for anxiety disorders. Psychosomatics 1971;12(6):371‐9. [PUBMED: 5172928] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Jones 2010
- Jones C, Hacker D, Cormac I, Meaden A, Irving CB. Cognitive behaviour therapy versus psychosocial treatments for schizophrenia. Cochrane Database of Systematic Reviews 2010, Issue 9. [DOI: 10.1002/14651858.CD008712] [DOI] [Google Scholar]
Jones 2012
- Jones C, Hacker D, Cormac I, Meaden A, Irving CB. Cognitive behavioural therapy versus other psychosocial treatments for schizophrenia. Cochrane Database of Systematic Reviews 2012, Issue 4. [DOI: 10.1002/14651858.CD008712.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]