

Abstract
Background
Multiple pharmacologic treatments have been studied for acute lung injury (ALI) and acute respiratory distress syndrome (ARDS).
Objectives
Our objective was to determine the effects of pharmacologic treatments on clinical outcomes in adults with ALI or ARDS.
Search methods
We searched OVID versions of CENTRAL (The Cochrane Library Issue 3, 2003), MEDLINE (1966 to week 2, January 2004), EMBASE (1980 to week 4, 2004), CINAHL (1982 to week 2, January 2004), and HEALTHSTAR (1995 to December 2003); proceedings from four conferences (1994 to 2003); and bibliographies of review articles and included studies.
Selection criteria
Randomized controlled trials of pharmacologic treatments compared to no therapy or placebo for established ALI or ARDS in adults admitted to an intensive care unit, with measurement of early mortality (primary outcome), late mortality, duration of mechanical ventilation, ventilator‐free days to day 28, or adverse events. We excluded trials of nitric oxide, partial liquid ventilation, fluid and nutritional interventions, oxygen, and trials in other populations reporting outcomes in subgroups of patients with ALI or ARDS.
Data collection and analysis
Two reviewers independently screened titles and abstracts, rated studies for inclusion, extracted data and assessed methodologic quality of included studies. Disagreements were resolved by consensus in consultation with a third reviewer. For each pharmacologic therapy, we quantitatively pooled the results of studies using random effects models where permitted by the available data. We contacted study authors when clarification of the primary outcome was required.
Main results
Thirty three trials randomizing 3272 patients met our inclusion criteria. Pooling of results showed no effect on early mortality of prostaglandin E1 (seven trials randomizing 697 patients; relative risk [RR] 0.95, 95% confidence interval [CI] 0.77 to 1.17), N‐acetylcysteine (five trials randomizing 239 patients; RR 0.89, 95% CI 0.65 to 1.21), early high‐dose corticosteroids (two trials randomizing 187 patients; RR 1.12, 95% CI 0.72 to 1.74), or surfactant (nine trials randomizing 1441 patients; RR 0.93, 95% CI 0.77 to 1.12). Two interventions were beneficial in single small trials; corticosteroids given for late phase ARDS reduced hospital mortality (24 patients; RR 0.20, 95% CI 0.05 to 0.81), and pentoxifylline reduced one‐month mortality (RR 0.67, 95% CI 0.47 to 0.95) in 30 patients with metastatic cancer and ARDS. Individual trials of nine additional interventions failed to show a beneficial effect on prespecified outcomes.
Authors' conclusions
Effective pharmacotherapy for ALI and ARDS is extremely limited, with insufficient evidence to support any specific intervention.
Keywords: Humans; Acetylcysteine; Acetylcysteine/therapeutic use; Adrenal Cortex Hormones; Adrenal Cortex Hormones/therapeutic use; Alprostadil; Alprostadil/therapeutic use; Pulmonary Surfactants; Pulmonary Surfactants/therapeutic use; Randomized Controlled Trials as Topic; Respiratory Distress Syndrome, Adult; Respiratory Distress Syndrome, Adult/drug therapy
There is little evidence to support the use of drugs to improve outcomes in adults with lung injury
In adults, direct lung damage or indirect damage caused by trauma, infection or other factors can result in acute lung injury, including acute respiratory distress syndrome. Patients with this syndrome require mechanical ventilation. About half of patients die, and survivors have a prolonged stay in intensive care and physical limitations afterwards. Many drugs have been studied to improve lung function and reduce inflammation in these patients. The evidence to date does not convincingly show that any drug saves lives, although some small studies have shown potential benefit.
Background
The acute respiratory distress syndrome (ARDS), first described in 1967 (Ashbaugh 1967), is characterized by diffuse inflammation of the lung's alveolar‐capillary membrane in response to various pulmonary and extrapulmonary insults (Ware 2000). These insults cause pulmonary injury by direct (for example, gastric aspiration, pneumonia, inhalational injury, pulmonary contusion) or indirect (for example, sepsis, trauma, pancreatitis, multiple transfusions of blood products) mechanisms. An American‐European Consensus Conference (AECC) (Bernard 1994) formulated a widely cited definition of ARDS as follows: an acute onset of (1) hypoxaemia, with a ratio of the partial pressure of arterial oxygen (PaO2) to the inspired fraction of oxygen (FiO2) of 200 mmHg or less, (2) bilateral infiltrates on a frontal chest radiograph, and (3) no clinical evidence of left atrial hypertension or a pulmonary artery occlusion pressure of 18 mmHg or less in the presence of a pulmonary artery catheter. Acute lung injury (ALI) includes a milder form of lung injury, with a PaO2/FiO2 ratio of 300 mmHg or less. Almost all patients with ARDS and most with ALI require mechanical ventilation to survive; all require supplemental oxygen. The mortality of ARDS is high, estimated to be between 34% and 60% (Ware 2000). In addition, survivors have a prolonged stay in the intensive care unit (ICU) and demonstrate significant functional limitations, primarily fatigue and muscle weakness, that reduce quality of life after hospital discharge (Herridge 2003).
Research on therapy for ARDS has focused on both mechanical ventilation strategies and pharmacologic interventions. Animal and clinical studies, including randomized controlled trials (RCTs), have demonstrated the role of mechanical ventilation in perpetuating lung injury (Dos Santos 2000), leading to macroscopic damage (for example, pneumothorax), diffuse ventilator‐induced lung injury, and multiple organ system failure (Murphy 2000; Ranieri 1999). Several RCTs have compared lung protective (pressure and volume limited) to traditional strategies of mechanical ventilation (Amato 1998; ARDS Network 2000a; Brochard 1998; Brower 1999; Stewart 1998). The largest and most recent study (ARDS Network 2000a) was stopped early after a planned interim analysis showed a statistically significant reduction in hospital mortality from 39.8 percent to 31.0 percent (p = 0.007) in the group receiving low compared to traditional tidal volumes. The results of this trial have convinced many clinicians and investigators that lung protective ventilation using low tidal volumes and low inflation pressures is the most important therapeutic intervention available for patients with ARDS and ALI.
The pathogenesis of ARDS, extensively reviewed elsewhere (Luce 1998; Ware 2000), provides multiple potential targets for pharmacologic interventions. Regardless of the inciting insult, the pathology of ARDS features damage to the alveolar‐capillary membrane, with leakage of protein‐rich edema fluid into alveoli. Epithelial damage involves the basement membrane and types I and II cells. Injury reduces the amount and function of surfactant produced by type II cells. This increases alveolar surface tension, decreases lung compliance, and causes atelectasis. Endothelial damage is associated with numerous inflammatory events. These include neutrophil recruitment, sequestration and activation; formation of oxygen radicals; activation of the coagulation system, leading to microvascular thrombosis with platelet‐fibrin thrombi; and recruitment of mesenchymal cells with production of procollagen (a precursor to fibrosing alveolitis). Within the alveolar space, the balance between pro‐inflammatory (for example, tumour necrosis factor [TNF] alpha and interleukins [IL] 1, 6, and 8) and anti‐inflammatory mediators (for example, IL‐1 receptor antagonist and soluble TNF receptor) favours ongoing inflammation. In summary, initial lung injury is followed by repair, remodelling, and fibrosing alveolitis.
The diversity of approaches to pharmacologic therapy for ALI and ARDS reflects the complex pathophysiology. Therapies evaluated in randomized trials in humans include corticosteroids, other anti‐inflammatory agents, immunomodulating agents, pulmonary vasodilators, antioxidants, and surfactants. These therapies have multiple proposed mechanisms of action (Brower 2001; Dos Santos 2002; Table 5). They have not been evaluated in a systematic review, with the exception of inhaled nitric oxide (Sokol 2002).
Table 1.
Proposed mechanisms of action of pharmacologic treatments for ALI and ARDS
| Pharmacotherapy | Mechanism of Action |
| Prostaglandin E1 | Pulmonary vasodilator; decreases neutrophil activation; decreases platelet aggregation |
| N‐acetylcysteine and procysteine | Antioxidant (scavenger of free radical oxygen species) |
| Corticosteroids | Multiple anti‐inflammatory pathways; prevents collagen deposition |
| Surfactant | Restores normal mechanical properties of alveoli (surface tension, alveolar opening) |
| Dazoxiben | Anti‐inflammatory agent and pulmonary vasodilator (inhibits thromboxane synthase) |
| Acyclovir | Treats herpes simplex virus, which can be found in lower respiratory tract of patients with lung injury |
| Indomethacin | Anti‐inflammatory agent (decreases thromboxane production by inhibiting cyclooxygenase) |
| Pentoxifylline | Prevents neutrophil chemotaxis and activation (phosphodiesterase inhibitor) |
| Neutrohil elastase inhibitor | Inhibits pro‐inflammatory and tissue destroying protease |
| Interleukin‐10 | Immunomodulator (anti‐inflammatory cytokine) |
| Ketoconazole | Multiple anti‐inflammatory pathways (inhibits thromboxane synthase, 5‐lipoxygenase, alveolar macrophages) |
| Lisofylline | Multiple anti‐inflammatory pathways (decreases oxidized free fatty acids and pro‐inflammatory cytokines) |
| Granulocyte‐macrophage colony‐stimulating factor | Immunomodulator (stimulates phagocytosis and functions of host defence cells) |
Another version of this review: 'Pharmacologic treatments for the acute respiratory distress syndrome and acute lung injury: systematic review and meta‐analysis' (Adhikari 2004) is in press in Treatments in Respiratory Medicine.
Objectives
1. The primary objective of this systematic review was to evaluate the effect of each pharmacologic therapy, compared to placebo or no therapy, on early all‐cause mortality (at or before three months after randomization) in adults with established ALI or ARDS. 2. Secondary objectives were to evaluate the effect of each pharmacologic therapy, compared to placebo or no therapy, on late all‐cause mortality (greater than three months after randomization), duration of ventilation, ventilator‐free days to day 28, and adverse events.
Methods
Criteria for considering studies for this review
Types of studies
We reviewed randomized controlled trials (RCTs), either published in full or in abstract form. We excluded quasi‐randomized trials. We also excluded subgroups of patients with ALI or ARDS reported in RCTs of interventions for other populations because of the methodologic limitations of subgroup analyses (Oxman 1992).
Types of participants
We included adult patients with ALI or ARDS admitted to an ICU. We used authors' definitions of adult, ALI, and ARDS.
Types of interventions
We included any pharmacologic therapy compared to placebo or no therapy for the treatment of established ALI or ARDS, including any pharmacologic therapy given for the treatment of established ALI that may prevent the development of ARDS. We did not consider studies of enteral and intravenous therapies that are either not considered to be pharmacologic by regulatory authorities (nutritional interventions) or are combined with other management strategies (fluid management). We also did not consider inhaled nitric oxide (previously reviewed [Sokol 2002]), pharmacologic therapies used as part of a strategy of mechanical ventilation (partial liquid ventilation), or medical oxygen. We excluded any pharmacologic therapy started for prophylaxis of ALI, even when continued in patients who subsequently developed ALI or ARDS. We excluded studies directly comparing two pharmacologic therapies without a no treatment or placebo group.
Types of outcome measures
Primary outcomes
The primary outcome was early all‐cause mortality (at or before three months after randomization). We considered ICU and hospital mortality to be early mortality.
Secondary outcomes
Secondary outcomes included:
late all‐cause mortality (greater than three months after randomization);
duration of mechanical ventilation (defined as the time from randomization to extubation, study withdrawal, or death);
number of ventilator‐free days to day 28 (Schoenfeld 2002);
adverse events (defined as those leading to discontinuation of the study medication). In studies with a no placebo control arm, adverse events were defined as "serious adverse events" using authors' definitions.
Search methods for identification of studies
Electronic searches
We searched the following databases: CENTRAL (The Cochrane Library, Issue 3, 2003), MEDLINE (1966 to week 2, January 2004), EMBASE (1980 to week 4, 2004), CINAHL (1982 to week 2, January 2004), and HEALTHSTAR (1995 to December 2003), using the standard methods of the Cochrane Anaesthesia Review Group (Cracknell 2003). We used OVID versions of all databases. We used a highly sensitive strategy to retrieve RCTs from MEDLINE (Robinson 2002) and modified it for other databases. No language restriction was applied.
For detailed search strategy for OVID MEDLINE, CENTRAL, CINAHL, and HEALTHSTAR see Appendix 1 and for OVID EMBASE see Appendix 2.
Searching other resources
We also reviewed the bibliographies of retrieved articles and searched for abstracts from conference proceedings published from 1994 to 2003 in American Journal of Respiratory and Critical Care Medicine,Chest,Critical Care Medicine and Intensive Care Medicine.
We searched the bibliographies of recent narrative review articles (Anzueto 2002; Bernard 1990; Bernard 1991a; Brower 1999; Chadda 2002; Conner 2000; Cranshaw 2002; Dos Santos 2000; Hite 2001; Laterre 2003; Lewis 2003; Lovat 2003; McIntyre 2000; Que 2000; Spragg 2000; Spragg 2002c; Tasaka 2002; Thompson 2003; Wiedemann 2003) and contacted content experts for additional unpublished trials.
Data collection and analysis
Two reviewers (Neill Adhikari and Karen Burns) independently screened titles and abstracts, selected studies for inclusion, extracted data and assessed methodologic quality of included studies. Disagreements in all phases were resolved by consensus in consultation with a third reviewer (Maureen Meade).
Study identification
We screened titles and abstracts and retrieved all potentially relevant studies. We rated all retrieved studies for inclusion and have listed excluded studies in the "Table of excluded studies".
Data extraction
We extracted data on participants, intervention, and outcomes for each study using a standardized form. We contacted authors if we required clarification of data for the primary outcome.
We did not systematically evaluate the mechanistic quality of the pharmacologic therapies studied (for example, whether adequate amounts of the therapeutic agent were delivered to the presumed target for sufficient time to achieve the desired biologic response).
Quality assessment
We assessed methodologic quality with respect to allocation concealment, baseline similarity of treatment and control groups, similarity of cointerventions in treatment and control groups, blinding of caregivers and outcomes assessors, analysis of the primary outcome following the intention‐to‐treat principle (patients analysed in the group to which they were assigned and not withdrawn after randomization), and completeness of follow‐up.
Data analysis
For each pharmacologic therapy, we quantitatively pooled the results of studies where permitted by the available data. We anticipated variability in the reporting of adverse events and therefore described these qualitatively. For quantitative comparisons, treatment and control groups were compared using relative risk (RR) for categorical outcomes and weighted mean difference (WMD) for continuous outcomes. For studies reporting more than one treatment arm differing in medication dose, we combined data from all doses to determine an overall outcome measure for the treatment group. In all analyses we used the random effects model (DerSimonian 1986) in Review Manager 4.2 (Review Manager 4.2) because this method generally produces more conservative estimates of the precision of the treatment effect than the fixed effect model (Montori 2002).
For each pooled comparison, homogeneity of treatment effect was estimated using the Q statistic (Cochran 1954). We considered p ≤ 0.05 to be significant for the test of overall treatment effect and p ≤ 0.10 to be significant for the test of homogeneity. When statistically significant heterogeneity was found, we aggregated results using the random effects model only if studies were clinically similar. Results of studies with major clinical dissimilarities as judged by the reviewers were not pooled but were qualitatively summarized. We also used the recently described I2 statistic when assessing the impact of statistical heterogeneity on study results (Higgins 2002). This statistic is independent of the number of studies pooled and denotes the proportion of total variance in individual study estimates of treatment effect that arises from between‐study heterogeneity. We considered values of I2 greater than 50% to represent substantial between‐study heterogeneity (Higgins 2002).
We constructed funnel plots to assess for the potential of publication bias when pooled analyses contained at least five studies.
For each pharmacologic therapy we conducted the following additional analyses for the outcomes of early mortality, late mortality, duration of mechanical ventilation, and ventilator‐free days to day 28:
Subgroup analysis of the treatment effect in patients with ALI not meeting criteria for ARDS compared to those with ARDS;
Sensitivity analysis of treatment effect in trials with adequate allocation concealment compared to all trials;
Sensitivity analysis of treatment effect in trials with balanced cointerventions (reported or applied according to protocol) in treatment and control groups compared to all trials.
For each analysis, we statistically tested the difference in estimates of treatment effect between the two groups using a z test (Fleiss 1993) and considered p ≤ 0.05 to be statistically significant.
Results
Description of studies
Overall description
Searches of electronic databases yielded 5705 citations for screening. From these citations, conference abstracts, and bibliographies of retrieved studies, we identified 75 potentially relevant publications of which 33 met our inclusion criteria. We excluded 39 publications (see "Table of characteristics of excluded studies"), in addition to two duplicate publications (Holcroft 1986b; Shoemaker 1987) and one probable duplicate publication (Wiedemann 1992).
The 33 included publications described 33 studies. Two studies of surfactant (Spragg 2002a; Spragg 2002b) were reported in one abstract. One publication (Bernard 1997a) reported a trial of patients randomized to receive N‐acetylcysteine (NAC), procysteine, or placebo. We included the patients randomized to NAC and placebo in a pooled analysis of the effect of NAC on early mortality and described the procysteine arm separately. Another study of NAC (Ortolani 2000) randomized patients to NAC, NAC plus rutin (a flavanoid antioxidant), or control. We combined data from both NAC groups in our pooled analysis and did not analyse the effect of rutin, which we classified as a nutritional supplement. Finally, one study of prostaglandin E1 (PGE1) reported mortality data in 147 randomized patients (Slotman 1992), of whom clinical outcomes in 101 patients had been previously published (Bone 1989b). We counted these two publications as one study (Bone 1989a) and extracted data on early mortality from the later publication (Slotman 1992) and data on methodology, late mortality and adverse events from the earlier publication (Bone 1989b). Two additional trials (HL 10 2004; LaSRS 2000; see "Characteristics of ongoing studies") have recently ceased patient recruitment. Neither has been published in full or in abstract form.
Published trials meeting our selection criteria randomized 3272 patients and studied a wide range of pharmacologic therapies. They included seven trials of PGE1 (Abraham 1996; Abraham 1999; Bone 1989a; Holcroft 1986a; Rossignon 1990; Shoemaker 1986; Vincent 2001), five trials of NAC (Bernard 1997a; Domenighetti 1997; Jepsen 1992; Ortolani 2000; Suter 1994), three trials of corticosteroids (Bernard 1987; Meduri 1998; Weigelt 1985), and nine trials of surfactant (Anzueto 1996; Gregory 1997; Kesecioglu 2001; Reines 1992; Spragg 2002a; Spragg 2002b; Spragg 2003; Walmrath 2000; Weg 1994). Ten additional therapies were evaluated in single studies: dazoxiben (Reines 1985), acyclovir (Tuxen 1987), indomethacin (Steinberg 1990), pentoxifylline (Ardizzoia 1993), neutrophil elastase inhibitor (ICI 200,880) (Gottlieb 1994), procysteine (Bernard 1997a), interleukin 10 (Bernard 1999), ketoconazole (ARDS Network 2000b), lisofylline (ARDS Network 2002), and granulocyte‐macrophage colony‐stimulating factor (Presneill 2002).
Studies of the same pharmacologic therapy differed with respect to patient populations and drug administration, as follows.
Studies of prostaglandin E1
All seven studies of PGE1 (Abraham 1996; Abraham 1999; Bone 1989a; Holcroft 1986a; Rossignon 1990; Shoemaker 1986; Vincent 2001) enrolled patients with predominantly ARDS, although three restricted enrolment to those with trauma, surgery, or sepsis as a risk factor (Bone 1989a; Rossignon 1990; Shoemaker 1986). They varied with respect to method of medication administration (continuous infusion [Bone 1989a; Holcroft 1986a; Rossignon 1990; Shoemaker 1986] versus intermittent boluses [Abraham 1996; Abraham 1999; Vincent 2001]), formulation (liposomal in three trials [Abraham 1996; Abraham 1999; Vincent 2001]), and dose (ranging from 7.2 μg/kg/day [Vincent 2001] to 43.2 μg/kg/day [Bone 1989a; Holcroft 1986a; Rossignon 1990; Shoemaker 1986] for seven days).
Studies of N‐acetylcysteine
The five studies of NAC included four enrolling primarily patients with ARDS (Bernard 1997a; Domenighetti 1997; Jepsen 1992; Ortolani 2000) and one that restricted enrolment to those with mild ALI (Suter 1994). Two trials used continuous infusions (Jepsen 1992; Suter 1994) and the other three used intermittent intravenous boluses (Bernard 1997a; Domenighetti 1997; Ortolani 2000). The total dose of NAC varied considerably, from 120 mg/kg (Suter 1994) to 3510 mg/kg (Jepsen 1992), delivered over three to ten days. The total dose delivered in one trial (Ortolani 2000) was unclear.
Studies of corticosteroids
The three studies of corticosteroids included two that used a high dose, short course (48 hours or less) of medication early in the course of ALI (Weigelt 1985) and ARDS (Bernard 1987). The duration of ARDS prior to randomization in both trials was less than seven days. One trial used a lower dose of methylprednisolone for a longer duration (one month) for patients with non‐resolving ARDS who had been mechanically ventilated for at least seven days (Meduri 1998).
Studies of surfactant
The nine studies of surfactant (Anzueto 1996; Gregory 1997; Kesecioglu 2001; Reines 1992; Spragg 2002a; Spragg 2002b; Spragg 2003; Walmrath 2000; Weg 1994) enrolled primarily patients with ARDS. Three restricted eligibility to patients with sepsis‐induced ALI or ARDS (Anzueto 1996; Reines 1992; Weg 1994). The surfactant preparations were variable: synthetic surfactant with phospholipids (Anzueto 1996; Reines 1992; Weg 1994), synthetic surfactant with phospholipids and protein (Spragg 2002a; Spragg 2002b; Spragg 2003; Walmrath 2000), bovine surfactant (Gregory 1997), and porcine surfactant (Kesecioglu 2001). The method of delivery (continuous aerosolization in early trials [Anzueto 1996; Reines 1992; Weg 1994] and intratracheal instillation in later trials [Gregory 1997; Kesecioglu 2001; Spragg 2002a; Spragg 2002b; Spragg 2003; Walmrath 2000]) and the delivered doses (when measured) were also variable.
Risk of bias in included studies
Methodologic features of the included studies are shown in "Table of characteristics of included studies" and summarized in Figure 1.
Figure 1.

Summary of reported methodologic characteristics of included trials
Legend (1) Baseline similarity: Yes = pre‐randomization factors (age, severity of illness, non‐pulmonary organ failures, presence of sepsis, and duration of hospitalization, ICU stay, or mechanical ventilation) were clinically similar between treatment and control groups; Yes (A) = at least one baseline factor differed but was included in an adjusted analysis. (2) Blinding: Yes = caregivers were blinded or the term "double‐blind" was used. (3) Cointerventions: Yes = at least one cointervention (including positive end‐expiratory pressure, lung protective ventilation, weaning protocols, corticosteroids, other) was standardized, or its use was documented in both groups. (4) Zero withdrawals of patients after randomization and complete follow‐up refer to the outcome of early mortality.
Allocation concealment
Ten studies described adequate concealment of allocation (Anzueto 1996; ARDS Network 2000b; ARDS Network 2002; Bernard 1987; Bernard 1997a; Bone 1989a; Presneill 2002; Shoemaker 1986; Spragg 2003; Weg 1994).
Baseline characteristics
Only four studies did not report at least one prognostically important baseline characteristic (Kesecioglu 2001; Reines 1985; Reines 1992; Walmrath 2000), of which three were reported in abstract form (Kesecioglu 2001; Reines 1992; Walmrath 2000). Of the remaining 29 studies, ten had at least one clinically important imbalance at baseline (Abraham 1996; Abraham 1999; Bernard 1999; Presneill 2002; Shoemaker 1986; Spragg 2002a; Spragg 2002b; Tuxen 1987; Vincent 2001; Weigelt 1985). Four studies conducted additional analyses adjusting for baseline imbalances (Anzueto 1996; ARDS Network 2000b; Bernard 1987; Meduri 1998).
Blinding
Twenty six studies reported blinding of at least caregivers or used the term double‐blind. Four studies did not use a placebo control and did not report blinding of study personnel (Ardizzoia 1993; Gregory 1997; Kesecioglu 2001; Spragg 2003). One study used a placebo and was described as "single‐blind" (Reines 1985). Two studies explicitly reported no blinding (Ortolani 2000; Walmrath 2000).
In blinded studies, effects of medications that may have unblinded caregivers included hypotension with PGE1 (Abraham 1996; Abraham 1999; Bone 1989a; Holcroft 1986a; Rossignon 1990; Shoemaker 1986; Vincent 2001) and dazoxiben (Reines 1985), hyperglycaemia with corticosteroids (Bernard 1987; Meduri 1998; Weigelt 1985) and reflux of surfactant into the ventilator tubing (Anzueto 1996; Reines 1992 ; Spragg 2002a; Spragg 2002b; Weg 1994).
Cointerventions
Twelve studies standardized at least one cointervention or documented its application in the treatment and control groups (Abraham 1999; ARDS Network 2000b; ARDS Network 2002; Gregory 1997; Holcroft 1986a; Jepsen 1992; Meduri 1998; Presneill 2002; Spragg 2003; Vincent 2001; Weg 1994; Weigelt 1985). The remaining studies did not describe cointerventions. No study reported imbalances in the application of cointerventions.
Post‐randomization withdrawals
All studies analysed patients according to assigned treatment group. However, eleven studies reported at least one post‐randomization withdrawal (Abraham 1999; Bernard 1997a; Bone 1989a; Domenighetti 1997; Gregory 1997; Tuxen 1987; Weigelt 1985) or did not clearly report this information (Reines 1985; Spragg 2002a; Spragg 2002b; Weg 1994). Twenty‐six studies reported no losses to follow‐up. The remaining studies had incomplete follow‐up data on fewer than 1% of randomized patients (Abraham 1999; Bone 1989a; Spragg 2002b) or did not fully describe the extent of patient follow‐up (ARDS Network 2002; Reines 1992; Walmrath 2000; Weg 1994).
Effects of interventions
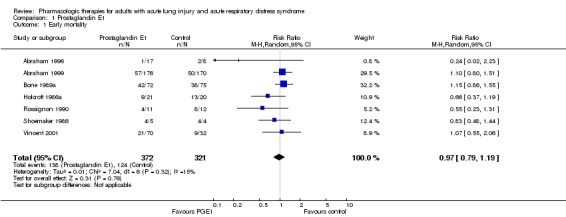
Effects of prostaglandin E1
Seven studies randomized 697 patients (Abraham 1996; Abraham 1999; Bone 1989a; Holcroft 1986a; Rossignon 1990; Shoemaker 1986; Vincent 2001). Outcomes data were available for 693 patients. The pooled analysis showed no statistically significant effect of PGE1 on early mortality (see "Graph 01/01"; relative risk [RR] 0.95, 95% confidence interval [CI] 0.77 to 1.17), without statistically significant heterogeneity (p = 0.27; I2 = 21.3%). Studies varied with respect to PGE1 dose and formulation (see "Description of included studies"), although no study individually showed a mortality benefit at a conventional level of significance (p = 0.05).
Individual trials reported more adverse events leading to study drug discontinuation in the PGE1 group (Abraham 1996; Abraham 1999; Holcroft 1986a; Rossignon 1990; Vincent 2001). These adverse events were primarily cardiopulmonary (hypotension, dysrhythmias, hypoxia) and neurological (agitation). Three trials reported other safety data (Abraham 1996; Abraham 1999; Bone 1989a), summarized in "Table of characteristics of included studies". Because of incomplete reporting, we were unable to pool data for late mortality, duration of mechanical ventilation, or ventilator‐free days to day 28.
Effects of N‐acetylcysteine
Five studies randomized 239 patients (Bernard 1997a; Domenighetti 1997; Jepsen 1992; Ortolani 2000; Suter 1994). Outcomes data were available for 235 patients. The pooled analysis showed no statistically significant effect of NAC on early mortality (see "Graph 02/01"; RR 0.89, 95% CI 0.65 to 1.21), without statistically significant heterogeneity (p = 0.63; I2 = 0%). Studies varied with respect to NAC dose and formulation (see "Description of included studies"), although no study individually showed a mortality benefit at a conventional level of significance (p = 0.05).
No control group patient experienced an adverse event leading to study drug discontinuation. One patient receiving NAC had a rash, after which NAC was stopped (Jepsen 1992). Because of incomplete reporting, we were unable to pool data for late mortality, duration of mechanical ventilation, or ventilator‐free days to day 28.
Effects of early high dose corticosteroids
There was no statistically significant effect of early high dose corticosteroids on early mortality (see "Graph 03/01"; RR 1.12, 95% CI 0.72 to 1.74) in the pooled analysis of two studies randomizing 187 patients (Bernard 1987; Weigelt 1985). These studies had outcomes data for 180 patients. There was evidence of substantial heterogeneity (I2 = 50.1%) that did not meet our criteria for statistical significance (p = 0.16). The two trials studied somewhat different populations. Patients in the multicentre trial (Bernard 1987) were sicker. They met criteria for ARDS and the control group mortality was 63%. In contrast, Weigelt enrolled patients exclusively in a single surgical ICU with ALI and not ARDS (Weigelt 1985). Mortality in the control group was much lower (31%). The two trials used similar corticosteroid regimens (methylprednisolone 30 mg/kg every 6 hours for 4 doses [Bernard 1987] or 48 hours [Weigelt 1985]). Neither study individually showed a mortality benefit at a conventional level of significance (p = 0.05). Because of incomplete reporting, we were unable to pool data for late mortality, duration of mechanical ventilation, or ventilator‐free days to day 28. The two studies did not report adverse events leading to study drug discontinuation but did report more infectious complications in the group receiving corticosteroids (see "Table of characteristics of included studies" for details).
Effects of surfactant
There was no statistically significant effect of surfactant therapy on early mortality (see "Graph 04/01"; RR 0.93, 95% CI 0.77 to 1.12) in the pooled analysis of nine studies randomizing 1441 patients (Anzueto 1996; Gregory 1997; Kesecioglu 2001; Reines 1992; Spragg 2002a; Spragg 2002b; Spragg 2003; Walmrath 2000; Weg 1994). These studies had outcomes data for 1416 patients. There was no evidence of statistically significant heterogeneity (p = 0.28; I2 = 18.7%). The surfactant preparations and delivery methods were highly variable (see "Description of included studies"). One study published in abstract form (Kesecioglu 2001) showed a statistically significant mortality benefit (RR 0.21, 95% CI 0.05 to 0.91). This study enrolled patients with ALI (including ARDS) and used intratracheal porcine surfactant. The abstract does not describe details of the surfactant's biologic effect.
Although three studies reported ventilator‐free days to day 28 (Kesecioglu 2001; Spragg 2003; Walmrath 2000) and two other studies reported no differences in this outcome (Spragg 2002a; Spragg 2002b), data limitations precluded a pooled analysis. One study (Spragg 2003) reported no adverse event leading to study drug discontinuation. Other studies reported more adverse events (primarily respiratory and haemodynamic) in the surfactant group (Anzueto 1996; Gregory 1997; Reines 1992; Weg 1994; see "Table of characteristics of included studies" for details). Because of incomplete reporting, we were unable to pool data for late mortality or duration of mechanical ventilation.
Effects of additional therapies
The effects of pharmacologic therapies evaluated in single trials are summarized in "Table of characteristics of included studies". One study enrolling 24 patients (Meduri 1998) meeting AECC criteria for ARDS (Bernard 1994) showed that administration of corticosteroids for late phase non‐resolving ARDS reduced mortality in the ICU (0/16 in methylprednisolone group versus 5/8 in placebo group; RR 0.05, 95% CI 0.00 to 0.78) and hospital (2/16 in methylprednisolone group versus 5/8 in placebo group; RR 0.20, 95% CI 0.05 to 0.81) and reduced duration of ventilation, with no increase in infectious complications. One study of 30 patients (Ardizzoia 1993) with metastatic cancer and ARDS (as defined by the authors) found that pentoxifylline reduced one month mortality (10/15 in pentoxifylline group versus 15/15 in control group; RR 0.67, 95% CI 0.47 to 0.95) with no adverse events leading to discontinuation of therapy. There was no evidence of effect of any other intervention on prespecified outcomes.
Subgroup analyses
Studies of PGE1 and surfactant enrolled patients primarily with ARDS and did not report results separately for patients meeting criteria for ALI but not ARDS. For NAC, there was no difference in effect on early mortality whether given to patients with primarily ARDS (Bernard 1997a; Domenighetti 1997; Jepsen 1992; Ortolani 2000) compared to ALI (Suter 1994) (RR 0.94, 95% CI 0.67 to 1.31 versus RR 0.63, 95% CI 0.28 to 1.45; p value for comparison = 0.38). Similarly, early high dose corticosteroids showed no differential effect (p value for comparison = 0.17) on early mortality in patients with ALI (Weigelt 1985; RR 1.49, 95% CI 0.85 to 2.62) compared to those with ARDS (Bernard 1987; RR 0.95, 95% CI 0.69 to 1.29).
Sensitivity analyses
Studies reporting adequate allocation concealment included two trials of PGE1 (Bone 1989a; Shoemaker 1986), one trial of NAC (Bernard 1997a), one trial of early high‐dose corticosteroids (Bernard 1987), and three trials of surfactant (Anzueto 1996; Spragg 2003; Weg 1994). When these trials were compared to all trials of the same pharmacologic therapy, there were no differences in treatment effect on early mortality for PGE1 (RR 0.99, 95% CI 0.67 to 1.46 versus RR 0.95, 95% CI 0.77 to 1.17; p value for comparison = 0.85), NAC (RR 0.83, 95% CI 0.32 to 2.15 versus RR 0.89, 95% CI 0.65 to 1.21; p value for comparison = 0.89), early high dose corticosteroids (RR 0.95, 95% CI 0.69 to 1.29 versus RR 1.12, 95% CI 0.72 to 1.74; p value for comparison = 0.55), or surfactant (RR 0.98, 95% CI 0.83 to 1.16 versus RR 0.93, 95% CI 0.77 to 1.12; p value for comparison = 0.68). Studies reporting any balanced cointervention between treatment and control groups included four trials of PGE1 (Abraham 1999; Holcroft 1986a; Rossignon 1990; Vincent 2001), one trial of NAC (Jepsen 1992), and three trials of surfactant (Gregory 1997; Spragg 2003; Weg 1994). When these trials were compared to all trials of the same pharmacologic therapy, there were no differences in treatment effect on early mortality for PGE1 (RR 0.90, 95% CI 0.66 to 1.24 versus RR 0.95, 95% CI 0.77 to 1.17; p value for comparison = 0.78), NAC (RR 1.06, 95% CI 0.67 to 1.70 versus RR 0.89, 95% CI 0.65 to 1.21; p value for comparison = 0.54), or surfactant (RR 0.71, 95% CI 0.45 to 1.12 versus RR 0.93, 95% CI 0.77 to 1.12; p value for comparison = 0.28).
Evaluation of publication bias
Examination of funnel plots (study precision versus treatment effect) for trials of PGE1, NAC, and surfactant therapy (Figure 2; Figure 3; Figure 4) suggested the possibility of publication bias arising from the non‐publication of small trials with equivocal or negative findings.
Figure 2.

Funnel plot of standard error (SE) of treatment effect (log relative risk [RR]) versus treatment effect (RR) for outcome of early mortality in trials of prostaglandin E1
Figure 3.

Funnel plot of standard error (SE) of treatment effect (log relative risk [RR]) versus treatment effect (RR) for outcome of early mortality in trials of N‐acetylcysteine
Figure 4.

Funnel plot of standard error (SE) of treatment effect (log relative risk [RR]) versus treatment effect (RR) for outcome of early mortality in trials of surfactant
Discussion
The principal finding of our systematic review is that no pharmacotherapy convincingly improves survival in patients with ARDS and ALI. We identified 33 RCTs of pharmacologic treatments for established ALI and ARDS enrolling 3272 patients, with the first trials published in 1985 (Reines 1985; Weigelt 1985). The median number of patients randomized per trial was low (45, range 9 to 725). Our pooled analyses had sample sizes of 180 to 1416 patients (early high‐dose corticosteroids and surfactant therapy respectively). When we combined studies, there was no effect on early mortality of PGE1, NAC, the early administration of high‐dose corticosteroids, or surfactant. With respect to adverse effects, all trials of PGE1 and early high‐dose corticosteroids and four out of five surfactant trials with safety data showed more adverse events with active therapy. However, the potential difficulty of achieving effective blinding of PGE1 and surfactant may have biased adverse event reporting in the active treatment arms. Of the miscellaneous interventions evaluated in single trials, corticosteroids given late in the course of ARDS decreased ICU and hospital mortality (Meduri 1998), and pentoxifylline decreased mortality in patients with metastatic cancer and ARDS (Ardizzoia 1993). We did not analyse the effect of rutin (Ortolani 2000), which we classified as a nutritional supplement.
In our pooled analyses, we did not find a differential effect in patients with ARDS compared to patients meeting criteria for ALI but not ARDS, although these subgroup analyses were underpowered. Similarly, the results of our analyses did not change when they were restricted to studies with definite allocation concealment or studies with balanced cointerventions. However, we did not perform a sensitivity analysis considering only trials that evaluated therapies with documented evidence of bioavailability and biologic effect.
Because the confidence intervals around pooled relative risks for PGE1, NAC, early high‐dose corticosteroids, and surfactant therapy are wide, we cannot exclude the possibility of a modest benefit or harm to patients. However, in each case the overall best estimate of relative risk suggested no effect. Clinical application of these therapies is therefore not currently justified. Any additional large trials should await preclinical and preliminary clinical studies to identify variations of dose, timing of administration, and formulation that may lead to clinical benefit. For example, a recently completed trial of HL 10 (HL 10 2004) evaluated the only surfactant preparation shown to be potentially beneficial (Kesecioglu 2001), a porcine surfactant with a high phospholipid concentration delivered by intratracheal installation.
We found that the scientific quality (Guyatt 2002) of included trials was variable. Methodologic strengths of a clear majority of studies included caregiver blinding or "double‐blinding" (Devereaux 2001), analysis of early mortality by strict intention‐to‐treat criteria (analysis according to assigned group and zero withdrawals), and complete patient follow‐up. No study documented differential application of potentially important cointerventions, although the majority provided no information about cointerventions. A minority of studies described adequate allocation concealment. About one‐half of the trials documented similarity between treatment groups for at least one prognostically important baseline characteristic. Our assessment of methodologic features was restricted to published descriptions, and we may therefore have underestimated the methodologic strength of some studies, especially those reported in abstract form (Bernard 1999; Gottlieb 1994; Kesecioglu 2001; Reines 1992; Spragg 2002a; Spragg 2002b; Walmrath 2000).
Another limitation of this systematic review is the identification of a small number of trials for each pharmacologic therapy, most of which randomized a small number of patients. Plots of study precision versus treatment effect for trials of NAC, PGE1 and surfactant therapy suggested the existence of small unpublished non‐beneficial trials. However, the inclusion of any such trials would not qualitatively change our findings of no treatment effect for these interventions. We did not search for RCTs of pharmacologic therapies for other related critically‐ill populations (such as sepsis) reporting outcomes in subgroups of patients with ALI and ARDS because of limitations in the interpretation of subgroup analyses. Strengths of this systematic review include the use of strategies to minimize bias in the selection and reporting of studies: the extensive literature search, duplicate independent screening of articles and data abstraction, and explicit criteria for methodologic assessment (Oxman 2002). We used clinical judgment to decide a priori to combine studies for which a similar direction and magnitude of treatment effect could reasonably be expected. Although aggregated studies differed with respect to eligibility criteria and study medications (formulation, method of administration, and dose), we found no statistical evidence of between study variation in trials of PGE1, NAC, and surfactant therapy. One of two statistical methods used suggested substantial heterogeneity between the two studies of early high dose corticosteroids (Bernard 1987; Weigelt 1985). However, neither study individually demonstrated a benefit, supporting the decision to pool their results. We used random effects models to aggregate data and generate conservative confidence limits for the point estimate of the pooled treatment effect (Montori 2002). We did not find statistically significant differences in treatment effect according to prespecified hypotheses concerning patient population or methodology. Effective pharmacologic therapy for established ALI and ARDS is therefore extremely limited. We identified two potentially beneficial treatments. First, prolonged corticosteroid administration for late ARDS, which may attenuate the fibroproliferative process, was evaluated in one small trial (Meduri 1998). This study randomized 24 patients with late‐phase ARDS and showed an impressive but clinically implausible point estimate of benefit, with a wide confidence interval (absolute risk reduction in ICU mortality 0.62; 95% CI, 0.30‐0.95). Methodologic strengths of this trial included blinding of caregivers, intention‐to‐treat analysis, complete follow‐up, and adjustment for baseline imbalances. The authors did not describe concealment of allocation. However, the major limitation is the method of data analysis. The investigators calculated a priori that 99 patients would be required to detect an absolute survival improvement of 30% in corticosteroid‐treated patients. Enrolment was terminated prematurely using early stopping rules based on sequential clinical trials (Whitehead 1983). This approach may inflate the treatment effect in small trials (Marras 1999) by increasing the probability of confounding by imbalances in baseline prognostic characteristics. Patients in the corticosteroid group had less organ dysfunction and pulmonary morbidity and thus may have had a better prognosis, a bias which may have persisted despite statistical adjustment and confounded the results. In addition, the crossover of four of the eight placebo‐assigned patients to corticosteroids (as per protocol) precluded an accurate evaluation of the infection risk associated with this treatment. Therefore, this trial provides important albeit preliminary evidence for the efficacy of corticosteroids for late‐phase ARDS. The recently completed Late Steroid Rescue Study, which randomized 180 patients, should provide more definitive data (LaSRS 2000).
The second potentially beneficial intervention was pentoxifylline, a phosphodiesterase inhibitor that prevents neutrophil chemotaxis and activation. This therapy was evaluated in a randomized trial enrolling 30 patients with metastatic cancer (Ardizzoia 1993). Although unclear allocation concealment and lack of blinding threaten the internal validity of this trial, the most important limitation is lack of generalizability. Eighteen of 30 randomized patients had lymphangitic metastases that may have mimicked the characteristic radiographic changes of ARDS and caused diagnostic misclassification. The mortality in this trial was higher (25 of 30 patients died at 1 month) than generally observed in patients with ARDS (Rubenfeld 2003; Ware 2000), which limits the applicability of the findings to lower‐risk patients. Finally, the severity of patients' lung injury according to AECC criteria (Bernard 1994) was not clear because the authors did not describe the oxygenation criteria used for the diagnosis of ARDS or whether patients required mechanical ventilation. In conclusion, further research is required to assess the potential role of pentoxifylline in the treatment of ALI and ARDS in patients without cancer.
There are several potential reasons to explain the large number of non‐beneficial trials of pharmacologic therapies for ALI and ARDS. These explanations overlap with insights into the design of RCTs in patients with severe sepsis (Opal 2003). First, randomized trials may have been conducted before early investigations had established the optimal dose and duration of the candidate therapy that would achieve adequate tissue levels and biologic response. Second, the definition of the clinical syndrome of ALI and ARDS, although feasible to apply in clinical settings and in research, does not have optimal reliability and validity (Ferguson 2001; Rubenfeld 2003; Villar 1999). Trials may therefore have enrolled patients unlikely to respond to candidate therapies. However, an inadequate definition of ALI and ARDS cannot be the exclusive explanation for non‐beneficial trials given the recent positive RCT of low tidal volumes in ALI patients (ARDS Network 2000a). Third, ALI and ARDS are clinically heterogeneous syndromes with various causes, genetic susceptibilities (Villar 2003) and clinical courses. Trials may thus have included responsive and non‐responsive subgroups. Fourth, there are many important non‐pulmonary determinants of outcome for patients with ALI and ARDS. Fifth, investigators may have overestimated the intrinsic therapeutic potential of candidate therapies. The latter three points may have contributed to the design of RCTs that were inadequately powered to reliably detect moderate clinical benefits.
Authors' conclusions
Our pooled analyses provide no evidence to support the routine administration of PGE1, NAC, early high‐dose corticosteroids, or surfactant in critically ill patients with ALI and ARDS. Single studies showed no evidence of treatment effect of dazoxiben, acyclovir, indomethacin, neutrophil elastase inhibitor (ICI 200,880), procysteine, interleukin 10, ketoconazole, lisofylline, or granulocyte‐macrophage colony‐stimulating factor. Single small studies have shown a potential benefit of prolonged corticosteroid administration in late‐phase ARDS and pentoxifylline in patients with metastatic cancer and ARDS. However, there is currently insufficient evidence to support the routine use of either therapy.
Preclinical research should develop novel candidate therapies for ALI and ARDS and adequately assess pharmacologic properties and biologic response prior to large randomized trials.
Subgroups of patients with ALI should be defined that share biochemical and/or genetic homogeneity and that may benefit from targeted pharmacologic interventions.
Further clinical studies are required to assess the potential benefit of pentoxifylline in ALI and ARDS patients without cancer.
Future adequately powered RCTs should implement rigorous methods to maximize internal validity. Reporting of important cointerventions would assist the assessment of performance bias, especially in trials without caregiver blinding.
Acknowledgements
We thank Elizabeth Uleryk for assistance in searching bibliographic databases, Dr Jan Friedrich and Dr Yumiko Imai for assistance in translation, and Dr Deirdre Grady for assistance in searching conference proceedings. We would also like to thank Dr John Carlisle, Prof Nathan Pace, Dr Harald Herkner, Dr Roger G. Spragg, Dr Leo Celi, Dr Palvannan Sivalingam, Dr Tom Pedersen, Janet Wale and Kathie Godfrey for their help and editorial advice during the preparation of this review.
Appendices
Appendix 1. Search strategy for OVID MEDLINE, CENTRAL, CINAHL, and HEALTHSTAR
1. randomized controlled trial.pt. 2. controlled clinical trial.pt. 3. randomized controlled trials/ 4. random allocation/ 5. double‐blind method/ 6. single‐blind method/ 7. or/1‐6 8. animal/ not human/ 9. 7 not 8 10. clinical trial.pt. 11. exp clinical trials/ 12. (clinic$ adj25 trial$).tw. 13. ((singl$ or doubl$ or trebl$ or tripl$) adj (mask$ or blind$)).tw. 14. placebos/ 15. placebo$.tw. 16. random$.tw. 17. research design/ 18. (latin adj square).tw. 19. or/10‐18 20. 19 not 8 21. 20 not 9 22. comparative study/ 23. exp evaluation studies/ 24. follow‐up studies/ 25. prospective studies/ 26. (control$ or prospectiv$ or volunteer$).tw. 27. cross‐over studies/ 28. or/22‐27 29. 28 not 8 30. 29 not (9 or 21) 31. 9 or 21 or 30 32. respiratory distress syndrome, adult/ 33. ((acute adj lung adj injur:) or (shock adj lung) or ards).tw. 34. ((acute or adult) and (respiratory adj distress)).tw. 35. or/32‐34 36. 31 and 35
Appendix 2. Search strategy for EMBASE
1. randomized controlled trial/ 2. exp controlled study/ 3. prospective study/ 4. exp clinical trial/ 5. single blind procedure/ 6. double blind procedure/ 7. comparative study/ 8. evaluation/ or follow up/ 9. (clinic$ adj25 (trial or stud:)).tw. 10. random:.tw. 11. ((singl: or doubl: or trebl: or tripl:) adj (blind: or mask:)).tw. 12. placebo.tw. 13. placebo/ 14. (control: or prospectiv:).tw. 15. ct.fs. 16. or/1‐15 17. animal/ not human/ 18. 16 not 17 19. respiratory distress syndrome, adult/ 20. ((acute adj lung adj injur:) or (shock adj lung) or ards).tw. 21. ((acute or adult) and (respiratory adj distress)).tw. 22. or/19‐21 23. 18 and 22
Data and analyses
Comparison 1.
Prostaglandin E1
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Early mortality | 7 | 693 | Risk Ratio (M‐H, Random, 95% CI) | 0.97 [0.79, 1.19] |
Analysis 1.1.
Comparison 1 Prostaglandin E1, Outcome 1 Early mortality.
Comparison 2.
N‐acetylcysteine
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Early mortality | 5 | 235 | Risk Ratio (M‐H, Random, 95% CI) | 0.89 [0.65, 1.21] |
Analysis 2.1.

Comparison 2 N‐acetylcysteine, Outcome 1 Early mortality.
Comparison 3.
Early high‐dose corticosteroids
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Early mortality | 2 | 180 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [0.72, 1.74] |
Analysis 3.1.

Comparison 3 Early high‐dose corticosteroids, Outcome 1 Early mortality.
Comparison 4.
Surfactant
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Early mortality | 9 | 1416 | Risk Ratio (M‐H, Random, 95% CI) | 0.93 [0.77, 1.12] |
Analysis 4.1.

Comparison 4 Surfactant, Outcome 1 Early mortality.
What's new
| Date | Event | Description |
|---|---|---|
| 13 December 2018 | Amended | Editorial team changed to Cochrane Emergency and Critical Care |
History
Protocol first published: Issue 4, 2003 Review first published: Issue 4, 2004
| Date | Event | Description |
|---|---|---|
| 9 June 2010 | Amended | Contact details updated. |
| 2 August 2008 | Amended | Converted to new review format. |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
| Methods | n = 25, 8 centres Allocation concealment: not described Baseline similarity: age (D), APACHE II, sepsis Blinding: caregivers Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Mechanical ventilation; bilateral CXR infiltrates, no LAH, P/F of 225 mmHg or less; duration of ARDS < 24 hours Exclusions: Recent MI; liver or renal failure; neurogenic pulmonary edema |
|
| Interventions | IV liposomal PGE1, dose titrated to 3.6 mcg/kg every 6 hours (14.4 mcg/kg/day) for 7 days, or placebo | |
| Outcomes | 28 day mortality: RR 0.24 (95% CI 0.02 to 2.23) Adverse events leading to discontinuation of therapy: treatment: 1/17 (desaturation and dysrhythmia), control: 0/8 Other safety data: any medication‐related adverse event (treatment: 14/17 patients, control: 3/8 patients); infusion site irritation, transient desaturation and agitation were reported in some treatment but no control patients; no serious adverse event in either group was considered related to study medication |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 350, 47 centres Allocation concealment: not described Baseline similarity: age (D), APACHE II, sepsis Blinding: caregivers Cointerventions: initiation of weaning standardized; corticosteroids given to 25% of treatment patients and 26% of control patients Withdrawals: treatment (1/178), control (1/172) Losses to follow‐up: treatment (1/178), control (1/172) |
|
| Participants | Inclusions: AECC definition for ARDS; duration of ARDS < 24 hours Exclusions: Recent MI; liver or renal failure; neurogenic pulmonary edema |
|
| Interventions | IV liposomal PGE1, dose titrated to 3.6 mcg/kg every 6 hours (14.4 mcg/kg/day) for 7 days, or placebo | |
| Outcomes | 28 day mortality: RR 1.10 (95% CI 0.80 to 1.51), based on data from 346 patients Duration of ventilation (median days): 16.9 (PGE1 group); 19.6 (placebo group); p = 0.94 Adverse events leading to discontinuation of therapy (mainly hypotension and hypoxia): treatment (20/178 patients), control (1/172 patients) Other safety data: drug‐related adverse events more common in treatment group (hypotension‐ treatment: 93/178 patients, control: 29/172 patients; hypoxia‐ treatment: 43/178 patients, control: 9/172 patients); no difference in incidence of serious adverse events |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 725, 63 centres Allocation concealment: central randomization Baseline similarity: age, APACHE III (A), sepsis Blinding: caregivers Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor: sepsis or sepsis syndrome present for < 96 hours; diffuse CXR infiltrates, P/F < 250 mmHg, no left ventricular failure; mechanical ventilation; duration of ARDS < 48 hours Exclusions: Chronic lung, liver or renal disease; acute liver failure; HIV with Pneumocystis carinii pneumonia; inhalational injury |
|
| Interventions | Continuously aerosolized synthetic surfactant (Exosurf) with DPPC 13.5 mg/ml) 240 ml daily for 5 days (estimated aerosolized DPPC: 112 mg/kg/d), or placebo (nebulized 0.45% saline) | |
| Outcomes | 30 day mortality: RR 1.01 (95% CI 0.84 to 1.20) Duration of ventilation: MD ‐0.40 days (95% CI ‐3.04 to 2.24) Adverse events leading to discontinuation of therapy not reported Serious adverse events: treatment: 5/364 (hypotension, barotrauma, hypoxaemia, increased peak airway pressure, respiratory arrest); control: 3/361 (hypotension, barotrauma) |
|
| Notes | Duration of ventilation was reported as 16.0 (1.0) days for the surfactant group and 16.4 (0.9) days for the placebo group. Although the authors reported the duration of ventilation as mean (standard deviation), the standard deviations were extremely small and we assumed that they were standard errors of the mean. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
| Methods | n = 30, 1 centre Allocation concealment: not described Baseline similarity: age Blinding: caregivers not blinded (no placebo) Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: metastatic cancer; diffuse CXR infiltrates, rapid fall in PaO2, and absence of congestive heart failure | |
| Interventions | IV pentoxyfylline 100 mg twice daily for 7 days, then 400 mg orally three times daily; or no pentoxifylline | |
| Outcomes | 1 month mortality: 10/15 (pentoxifylline group) and 15/15 (control group); RR 0.67 (95% CI 0.47 to 0.95) Adverse events leading to discontinuation of therapy: none |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 234, 10 centres Allocation concealment: central randomization Baseline similarity: age (A), APACHE III (A), sepsis (A) Blinding: caregivers, study coordinators, investigators Cointerventions: lung protective ventilation studied in factorial design; screening for ability to wean and weaning protocol standardized Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Mechanical ventilation; AECC definition for ALI and ARDS; duration of ALI or ARDS < 36 hours Exclusions: Neurologic disease impairing weaning; chronic lung disease; morbid obesity; liver disease; immunocompromised; burns; increased intracranial pressure |
|
| Interventions | Enteral ketoconazole, 400 mg once daily for 21 days or until 48 hours of unassisted breathing, or placebo | |
| Outcomes | Hospital mortality: RR 1.03 (95% CI 0.84 to 1.29) Ventilator free days to day 28 (median): 10 (ketoconazole group); 9 (placebo group); p = 0.89 Adverse events leading to discontinuation of therapy not reported All adverse events: no difference in incidence of liver enzyme elevations (p = 0.53); trend to more cardiovascular adverse events in ketoconazole group (p = 0.07) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
| Methods | n = 235, 10 centres Allocation concealment: central randomization Baseline similarity: age, APACHE III, sepsis Blinding: caregivers, study coordinators, investigators Cointerventions: lung protective ventilation studied in factorial design in 194 patients and applied to all patients subsequently enrolled; screening for ability to wean and weaning protocol standardized Withdrawals: none Losses to follow‐up: unclear |
|
| Participants | Inclusions: Mechanical ventilation; AECC definition for ALI and ARDS; duration of ALI or ARDS < 36 hours Exclusions: Neurologic disease impairing weaning, chronic lung disease, morbid obesity, liver disease; immunocompromised; burns; increased intracranial pressure |
|
| Interventions | IV lisofylline 3 mg/kg (maximum 300 mg) every 6 hours for 20 days or until 48 hours of unassisted breathing, or placebo | |
| Outcomes | 28 day mortality: RR 1.31 (95% CI 0.87 to 1.98) Ventilator free days to day 28 (median): 9 (lisofylline group); 11 (placebo group); p = 0.62 Adverse events leading to discontinuation of therapy not reported Severe adverse events: "no significant difference" |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
| Methods | n = 99, 7 centres Allocation concealment: sequentially numbered drug packs Baseline similarity: age (A), duration of ventilation (A), organ failures (A), sepsis Blinding: caregivers, investigating team Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor for ARDS; bilateral CXR infiltrates; PaO2 of 70 mmHg or less on FiO2 of at least 0.4, or PaO2/PAO2 of 0.3 or less; no LAH Exclusions: Hypotension; burns; some infections |
|
| Interventions | IV methylprednisolone,30 mg/kg IV every 6 hours for 4 doses, or placebo | |
| Outcomes | 45 day mortality: RR 0.95 (95% CI 0.69 to 1.29) Adverse events leading to discontinuation of therapy not reported Other safety information: infectious complications (treatment: 8/50, control: 5/49) |
|
| Notes | Mean duration of mechanical ventilation before study entry was 2.8 days (standard error 0.5 days) in the methylprednisolone group and 1.9 days (standard error 0.4 days) in the placebo group. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
| Methods | n = 48, 5 centres Allocation concealment: sequentially numbered drug packs Baseline similarity: age, APACHE II Blinding: caregivers, investigating team Cointerventions: not described Withdrawals: NAC (2/16), procysteine (none), control (none). Mortality information for one withdrawn patient who received NAC was available and included in the analysis. Losses to follow‐up: none |
|
| Participants | Inclusions: Mechanical ventilation; bilateral CXR infiltrates, no LAH, P/F of 200 mmHg or less or 225 mmHg or less if PEEP > 10 cmH2O; duration of ARDS < 24 h Exclusions: Severe acute or chronic liver disease; immunocompromised |
|
| Interventions | IV NAC, 70 mg/kg every 8 hours for 10 days (total dose 2100 mg/kg), or IV procysteine, 63 mg/kg every 8 hours for 10 days, or placebo | |
| Outcomes | 30 day mortality (NAC versus control): RR 0.83 (95% CI 0.32 to 2.15) 30 day mortality (procysteine versus control): RR 0.88 (95% CI 0.36 to 2.16) Ventilator free days to day 30 (median): 11 (NAC group); 20 (procysteine group); 3 (placebo group); differences not significant at p = 0.05 level Adverse events attributed to study medication: none |
|
| Notes | Patients (n = 48) were randomized to receive NAC (n = 16), procysteine (n = 17), or placebo (n = 15). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
| Methods | n = 60 Allocation concealment: not described Baseline similarity: "comparable" except for presence of shock (more common in treatment group) Blinding: caregivers Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Mechanical ventilation; AECC definition for ALI and ARDS; duration of ALI or ARDS < 36 hours Exclusions: Neurologic disease impairing weaning; chronic lung disease; morbid obesity; liver disease; immunocompromised; burns; increased intracranial pressure |
|
| Interventions | IV interleukin‐10, 8 mcg/kg or 20 mcg/kg IV daily for 6 days, or placebo | |
| Outcomes | 28 day mortality (both doses of interleukin‐10 versus control): RR 0.68 (95% CI 0.26 to 1.76) Ventilator free days to day 28 (not stated if mean or median): 15 (8 mcg/kg group); 6 (20 mcg/kg group); 9 (placebo group); p value not given Adverse events leading to discontinuation of therapy: none |
|
| Notes | Published only as abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 147, 13 centres Allocation concealment: central randomization Baseline similarity: age, sepsis Blinding: caregivers Cointerventions: not described Withdrawals: In Bone 1989b, 1/50 control patients died shortly after randomization but before the start of study drug infusion. This patient was included in the analyses of 30 day and 6 month mortality. No treatment patient was withdrawn. Additional withdrawals were not described in Slotman 1992. Losses to follow‐up: In Bone 1989b, one patient was lost to follow‐up before 30 days and was classified as a survivor. The treatment group of this patient was unclear and we therefore retained this patient in our analyses. Another two control patients and three treatment patients were lost to follow‐up between 30 days and six months. These patients were not included the the analysis of six month mortality. No additional losses to follow‐up are described in Slotman 1992. |
|
| Participants | Inclusions: Risk factor for ARDS: trauma, post surgery, sepsis; bilateral CXR infiltrates; P/F less than or equal to 150 mmHg on PEEP = 0 cmH2O or less than or equal to 200 mmHg on PEEP > 0 cmH2O Exclusions: Severe lung disease, liver or renal failure; severe head injury; high dose steroids |
|
| Interventions | Continuous IV PGE1, maximum dose 30 ng/kg/minute (43.2 mcg/kg/day) for 7 days, or placebo | |
| Outcomes | 30 day mortality: RR 1.15 (RR 0.86 to 1.55), based on data from 147 patients Six month mortality: RR 1.18 (95% CI 0.89 to 1.57), based on data from 96 patients Adverse events leading to discontinuation of therapy not reported Other safety information: hypotension (treatment: 10/50 patients, control: 7/51 patients); dysrhythmias (treatment: 10/50 patients, control: 5/51 patients); flushing (treatment: 2/50 patients, control: none); diarrhoea (treatment: 6/50 patients, control: 1/51 patients) |
|
| Notes | Data from 147 patients were reported in Slotman 1992, of whom data from 101 patients were reported in Bone 1989b. We counted these two publications as one study. We extracted 30 day mortality data from Slotman 1992 and six month mortality and adverse events data from Bone 1989b. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
| Methods | n = 45, 4 centres Allocation concealment: not described Baseline similarity: age, SAPS II, sepsis Blinding: caregivers Cointerventions: not described Withdrawals: treatment (1/23), control (2/22) Losses to follow‐up: none |
|
| Participants | Inclusions: AECC definition for ARDS Exclusion: Immunocompromised |
|
| Interventions | Continuous IV NAC, 190 mg/kg/day for 3 days (total dose 570 mg/kg), or placebo | |
| Outcomes | ICU mortality: RR 1.27 (95% CI 0.48 to 3.37), based on data from 42 patients Duration of ventilation: MD ‐1.2 days (95% CI ‐5.2 to 2.8), based on data from 42 patients Adverse events attributed to study medication: none |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 25 Allocation concealment: not described Baseline similarity: age, APACHE II Blinding: caregivers Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor for ARDS; diffuse CXR infiltrates, P/F ratio < 285 mmHg, no cardiogenic pulmonary edema | |
| Interventions | IV neutrophil elastase inhibitor (ICI 200,880), 350mg for up to 14 days, or placebo | |
| Outcomes | Mortalilty: RR 0.27 (95% CI 0.04 to 2.10) | |
| Notes | Published as abstract only | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 51, 5 centres (see Notes) Allocation concealment: not described Baseline similarity: age, sepsis, organ failures Blinding: caregivers not blinded (no placebo) Cointerventions: only mode of mechanical ventilation standardized during study period Withdrawals: treatment (1/27), control (none) Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor for ARDS; mechanical ventilation; bilateral CXR infiltrates, P/F less than or equal to 200 mmHg, PEEP at least 5 cmH2O, compliance less than or equal to 50 ml/cmH2O, PAOP less than or equal to 18 mmHg; duration of ARDS 48 hours or less Exclusions: Chronic lung disease; lung cancer; AIDS; cardiogenic shock; head injury |
|
| Interventions | Intratracheal bovine surfactant (Survanta), 50 mg/kg for 8 doses, or 100 mg/kg for 4 doses, or 100 mg/kg for 8 doses, or standard therapy | |
| Outcomes | 28 day mortality (see Notes): RR 0.59 (95% CI 0.25 to 1.38), based on data from 43 patients Duration of ventilation (median days): 15 (50mg/kg for 8 doses group), 10 (100 mg/kg for 8 doses), 10 (control group); difference not significant at p = 0.05 level Adverse events leading to discontinuation of therapy not reported Any adverse event: treatment: 6/27 patients, including respiratory events, haemodynamic instability, rash, decreased consciousness; control: 0/16 patients |
|
| Notes | The mortality comparison includes patients who received surfactant (50 mg/kg for 8 doses and 100 mg/kg for 8 doses) versus control. We excluded the treatment arm with 100 mg/kg of phospholipids for 4 doses because it included directly (n = 8) and randomly (n = 8) allocated patients. Outcomes were not reported separately for the 8 randomized patients. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 41, 1 centre Allocation concealment: not described Baseline similarity: age, duration of ventilation, sepsis Blinding: caregivers, investigators Cointerventions: one patient in each group received corticosteroids Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor for ARDS; mechanical ventilation; bilateral CXR infiltrates, compliance less than or equal to 50 mL/cmH2O, FiO2 at least 0.4 and PEEP at least 5 cmH2O Exclusions: Risk of intracranial haemorrhage; haemodynamic instability |
|
| Interventions | Continuous IV PGE1, maximum dose 30 ng/kg/minute (43.2 mcg/kg/day) for 7 days, or placebo | |
| Outcomes | 30 day mortality: RR 0.66 (95% CI 0.37 to 1.19) Adverse events leading to discontinuation of therapy: hypotension (treatment: 4/21 patients, control: 1/20); malaise or agitation (treatment: 2/21 patients, control: none) |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 66, 1 centre Allocation concealment: not described Baseline similarity: age Blinding: caregivers Cointerventions: corticosteroid administration "no different" between groups Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor for ARDS; PaO2 < 55 mmHg on room air or P/F < 250 mmHg; duration of intubation < 24 hours Exclusions: Chronic lung, cardiovascular, liver or renal disease |
|
| Interventions | IV NAC, bolus 150 mg/kg, then 20 mg/kg/hour continuously for 7 days (total dose 3510 mg/kg), or placebo | |
| Outcomes | 60 day mortality: RR 1.06 (95% CI 0.67 to 1.70) Adverse events leading to discontinuation of therapy: treatment: 1/32 (rash), control: 0/34 |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 36 Allocation concealment: not described Baseline similarity: not described Blinding: caregivers not blinded (no placebo) Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Patients with ALI/ARDS (not described) | |
| Interventions | Intratracheal porcine surfactant (HL10) with 100‐200 mg/kg of phospholipids, up to 4 doses, or standard therapy | |
| Outcomes | 28 day mortality: RR 0.21 (95% CI 0.05 to 0.91) Ventilator free days to day 28: MD 0.80 (95% CI ‐6.33 to 7.93) |
|
| Notes | Published only as abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 24, 4 centres Allocation concealment: not described Baseline similarity: age, MODS, sepsis; analyses adjusted for variables used to calculate severity of illness scores Blinding: caregivers Cointerventions: lung protective ventilation (limitation of plateau pressure to 35 cmH20) used in both groups Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: AECC definition for ARDS; at least 7 days of mechanical ventilation; lung injury score at least 2.5 with a reduction of less than 1 point from day 1 of ARDS Exclusions: ARDS of 3 or more weeks' duration; untreated infection; burns; recent gastrointestinal bleed |
|
| Interventions | IV methylprednisolone, 2 mg/kg/day IV for 14 days, tapering to zero over the next 18 days, or placebo | |
| Outcomes | ICU mortality: 0/16 (methylprednisolone group) and 5/8 (placebo group); RR 0.05 (95% CI 0 to 0.78) Hospital mortality: 2/16 (methylprednisolone group) and 5/8 (placebo group); RR 0.20 (95% CI 0.05 to 0.81) Duration of ventilation (median days): 11.5 (methylprednisolone group); 23 (placebo group); p = 0.001 Adverse events leading to discontinuation of therapy not reported Other safety data: infections per 100 patient‐days of treatment: 8 (methylprednisolone group); 7 (placebo group) |
|
| Notes | The mean duration of ARDS at randomization was 9.4 days (standard error 0.9 days) in the methyprednisolone group and 8.8 days (standard error 1.2 days) in the placebo group. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 36, 2 centres Allocation concealment: not described Baseline similarity: age, APACHE II score Blinding: none Cointerventions: not clearly described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Mechanical ventilation; bilateral CXR infiltrates, P/F less than or equal to 200 mmHg or less than or equal to 250 mmHg if PEEP at least 10 cm H2O Exclusions: duration of ARDS more than 24 hours; haemodynamic instability; severe heart or liver disease; "septic complications during trial" |
|
| Interventions | IV NAC, 50 mg/kg every 8 hours while mechanically ventilated, or IV NAC, 50 mg/kg every 8 hours and IV rutin, 5 mg/kg every 8 hours, both while mechanically ventilated, or control (250 mL of 5% dextrose in water) | |
| Outcomes | 30 day mortality (NAC and NAC plus rutin versus control): RR 0.64 (95% CI 0.32 to 1.30) Adverse events leading to discontinuation of therapy not reported Adverse effects on cardiac performance: none |
|
| Notes | Patients (n = 36) were randomized to receive NAC (n = 12), NAC and rutin (n = 12), or control (n = 12). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 18, 1 centre Allocation concealment: presupplied randomized drug packs Baseline similarity: age (D), APACHE II, duration of ventilation Blinding: caregivers, data collectors Cointerventions: Level of PEEP and tidal volumes similar in two groups Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor: severe sepsis; CXR infiltrate, PaO2 < 60 mmHg on room air or P/F < 287 mmHg Exclusions: Malignancy, immunosuppression |
|
| Interventions | IV GM‐CSF, 3 mcg/kg daily for 5 days, or placebo | |
| Outcomes | Hospital mortality: RR 1.33 (95% CI 0.45 to 3.96) Adverse events leading to discontinuation of therapy: treatment: 1/10 (transient oliguria), control: 0/8 |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
| Methods | n = 10 Allocation concealment: not described Baseline similarity: not described Blinding: unclear ("single‐blind", placebo used) Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor: sepsis syndrome; PaO2 < 60 mmHg or intrapulmonary shunt > 20% or radiologic evidence of ARDS Exclusions: Major cardiac, pulmonary, renal, endocrine diseases |
|
| Interventions | IV dazoxiben, 100 mg every 4 hours for 72 hours, or placebo | |
| Outcomes | Mortality: RR 2.00 (95% CI 0.26 to 15.62) Adverse events leading to discontinuation of therapy: none |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 49 Allocation concealment: not described Baseline similarity: not described Blinding: caregivers Cointerventions: not described Withdrawals: not described Losses to follow‐up: not described |
|
| Participants | Inclusion: Sepsis‐induced ARDS Exclusions: Not described |
|
| Interventions | Continuously aerosolized synthetic surfactant (Exosurf) with DPPC 40.5 mg/ml, or with DPPC 81 mg/ml, or placebo (nebulized 0.6% saline), for up to 5 days | |
| Outcomes | 14 day mortality (all surfactant doses versus control): RR 0.61 (95% CI 0.30 to 1.24) Adverse events leading to discontinuation of therapy not reported Other safety information: treatment: 2/33 patients had exhalation filter occlusion |
|
| Notes | Published only as abstract | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 23, 1 centre Allocation concealment: not described Baseline similarity: age, duration of ventilation Blinding: caregivers Cointerventions: not described (no patients received corticosteroids at time of randomization, but not specifically stated whether corticosteroids given after randomization) Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor: surgery or trauma; diffuse CXR infiltrates, PaO2 at least 60 mmHg on FiO2 at least 0.5, no left ventricular failure Exclusion: chronic obstructive pulmonary disease |
|
| Interventions | Continuous IV PGE1, dose titrated to 30 ng/kg/minute (43.2 mcg/kg/day) for 7 days, or placebo | |
| Outcomes | Mortality: RR 0.55 (95% CI 0.23 to 1.31) Duration of ventilation: MD 4 days (95% CI ‐13 to 21) Adverse events leading to discontinuation of therapy: treatment: 2/11 patients (hypotension), control: 0/12 patients |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 9, 1 centre Allocation concealment: local independent randomization Baseline similarity: age (D) Blinding: caregivers Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor: sepsis or surgery; mechanical ventilation; CXR infiltrates, PaO2 < 55 mmHg on room air or P/F ratio < 250 mmHg, no evidence of volume overload | |
| Interventions | Continuous IV PGE1, dose titrated to 30 ng/kg/minute (43.2 mcg/kg/day) for 48‐72 hours, or placebo | |
| Outcomes | Mortality: RR 0.80 (95% CI 0.52 to 1.24) | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
| Methods | n = 221 Allocation concealment: not described Baseline similarity: APACHE II (D) Blinding: caregivers (sham medication delivery in control group) Cointerventions: not described (lung protective ventilation "encouraged") Withdrawals: not described Losses to follow‐up: none |
|
| Participants | Patients with ARDS (not described) | |
| Interventions | Intratracheal synthetic surfactant (Venticute, containing 1 mg recombinant surfactant protein C and 50 mg phospholipids per ml), 1 ml/kg up to 4 doses in 12‐24 hours, or standard therapy | |
| Outcomes | 28 day mortality: RR 1.27 (95% CI 0.84 to 1.93) Ventilator‐free days to day 28: "not different between the groups" (data not reported) |
|
| Notes | Data from Spragg 2002a (North American trial) and Spragg 2002b (European/South African trial) are presented in the same abstract; neither trial has been published in full. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 227 Allocation concealment: not described Baseline similarity: APACHE II (D) Blinding: caregivers (sham medication delivery in control group) Cointerventions: not described (lung protective ventilation "encouraged") Withdrawals: not described Losses to follow‐up: treatment (1/118); control (1/109) |
|
| Participants | Patients with ARDS (not described) | |
| Interventions | Intratracheal synthetic surfactant (Venticute, containing 1 mg recombinant surfactant protein C and 50 mg phospholipids per ml), 1 ml/kg up to 4 doses in 12‐24 hours, or standard therapy | |
| Outcomes | 28 day mortality: RR 0.99 (95% CI 0.71 to 1.37), based on data from 225 patients Ventilator‐free days to day 28: "not different between the groups" (data not reported) |
|
| Notes | Data from Spragg 2002a (North American trial) and Spragg 2002b (European/South African trial) are presented in the same abstract. Neither trial has been published in full. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 40, 11 centres Allocation concealment: central randomization Baseline similarity: age, modified APACHE II, sepsis Blinding: caregivers unblinded (no placebo) Cointerventions: daily screening for ability to wean Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor for ARDS; AECC definition of ARDS; duration of ARDS not more than 48 hours; PEEP of at least 5 cmH20; at least 48 hours of antimicrobial therapy if pneumonia present Exclusions: Hemodynamic instability; severe hypoxaemia; lung cancer; AIDS |
|
| Interventions | Intratracheal synthetic surfactant (Venticute, containing 1 mg recombinant surfactant protein C and 50 mg phospholipids per ml), 1 ml/kg up to 4 doses in 24 hours, or 0.5 mL/kg up to 4 doses in 24 hours, or standard therapy | |
| Outcomes | 28 day mortality (all surfactant doses versus control): RR 0.67 (95% CI 0.26 to 1.72) Ventilator‐free days to day 28 [median (interquartile range)]: low dose: 4 (0 to 12); high dose 5 (0 to 18); control: 6 (0 to 15); differences reported to be non significant Adverse events leading to discontinuation of therapy: none Other safety data: treatment: 1/27 patients had an adverse event likely related to treatment (transient hypoxia and supraventricular tachycardia); no difference in incidence of serious adverse events |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
| Methods | n = 10, 1 centre Allocation concealment: not described Baseline similarity: age Blinding: caregivers blinded; investigators not blinded Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: bilateral infiltrates on CXR, P/F ratio less than 200 mmHg, PEEP greater than 5 cmH20, PAOP less than or equal to 18 mmHg; duration of ventilation at least 24 hours Exclusions: chronic lung disease; pneumonia; gastrointestinal bleeding |
|
| Interventions | One dose of IV indomethacin 50 mg or placebo | |
| Outcomes | Mortality: RR 0.50 (95% CI 0.06 to 3.91) Adverse events leading to discontinuation of therapy not reported Other safety data: no differences in levels of creatinine or blood urea nitrogen |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 61, 4 centres Allocation concealment: not described Baseline similarity: age, SAPS II, sepsis Blinding: caregivers Cointerventions: not described Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: Risk factor and mild‐moderate ALI (lung injury score between 0.1 and 2.5) Exclusions: Cardiogenic pulmonary edema; immunocompromised |
|
| Interventions | Continuous IV NAC, 40 mg/kg/day for 3 days (total dose 120 mg/kg), or placebo | |
| Outcomes | 1 month mortality: RR 0.63 (95% CI 0.28 to 1.45) Adverse events attributed to study medication: none |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 45, 2 centres Allocation concealment: not described Baseline similarity: age (D), sepsis Blinding: caregivers Cointerventions: not described Withdrawals: treatment (5/22); control (2/23) Losses to follow‐up: none |
|
| Participants | Inclusions: bilateral CXR infiltrates, noncardiogenic pulmonary edema, PaO2 < 80 mmHg with Fi02 at least 0.4 Exclusions: history of pulmonary disease or pulmonary trauma |
|
| Interventions | IV acyclovir, 5 mg/kg daily for 18 days or until end of mechanical ventilation, or placebo | |
| Outcomes | Mortality: RR 1.10 (95% CI 0.54 to 2.22), based on data from 38 patients Duration of ventilation: MD 6.0 days (95% CI ‐4.4 to 16.4) Adverse events (any): none |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 102, 31 centres Allocation concealment: not described Baseline similarity: age (D), SAPS II, sepsis Blinding: caregivers Cointerventions: Nitric oxide applied according to protocol Withdrawals: none Losses to follow‐up: none |
|
| Participants | Inclusions: AECC definition for ARDS; duration of ARDS < 24 hours Exclusions: Recent MI; chronic congestive heart failure; liver or renal failure; pneumonectomy; neurogenic pulmonary edema; neutropenia |
|
| Interventions | IV liposomal PGE1, dose titrated to 1.8 mcg/kg every 6 hours (7.2 mcg/kg/day) for 7 days, or placebo | |
| Outcomes | 28 day mortality: RR 1.07 (95% CI 0.55 to 2.06) Duration of ventilation (days; not stated whether median or mean): 16 (PGE1 group); 16.6 (placebo group); p = 0.94 Adverse events leading to discontinuation of therapy (details not given): treatment: 8/70, control: 2/32 |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 41, centres in Europe and South Africa (see Notes) Allocation concealment: not described Baseline similarity: not described Blinding: caregivers not blinded (no placebo) Cointerventions: not described Withdrawals: none Losses to follow‐up: not described |
|
| Participants | ARDS, not further described | |
| Interventions | Intratracheal synthetic surfactant (Venticute, containing 1 mg recombinant surfactant protein C and 50 mg phospholipids per ml), 1 ml/kg up to 4 doses in 24 hours (medium dose), or 4 ml/kg followed by up to 3 doses of 2 ml/kg within 24 hours (high dose), or standard therapy | |
| Outcomes | Mortality (medium dose surfactant versus control): RR 0.86 (95% CI 0.27 to 2.71), based on data from 26 patients. Ventilator‐free days to day 28 (median): medium dose: 14; high dose: not reported; control: 0 |
|
| Notes | Published only as abstract. Mortality data are reported only for the medium dose and standard therapy groups (n = 26). | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
| Methods | n = 51, 20 centres Allocation concealment: central randomization Baseline similarity: age, APACHE II Blinding: caregivers Cointerventions: "no difference" in use of glucocorticoids or mineralocorticoids Withdrawals: not described Losses to follow‐up: not described |
|
| Participants | Inclusions: Risk factor: sepsis or sepsis syndrome present < 18 hours; mechanical ventilation; bilateral CXR infiltrates, P/F 50‐299 mmHg Exclusions: Chronic lung, liver or renal disease; AIDS; pulmonary infection; cardiac ischaemia or left ventricular failure |
|
| Interventions | Continuously aerosolized synthetic surfactant (Exosurf) with DPPC 13.5 mg/ml, 175 ml every 4 hours for 12 hours/day or 24 hours/day for 5 days (estimated aerosolized DPPC: 21.9 and 43.5 mg/kg/day respectively), or placebo (nebulized 0.6% saline) | |
| Outcomes | 30 day mortality (all surfactant doses versus control): RR 0.81 (95% CI 0.42 to 1.57) Adverse events leading to discontinuation of therapy not reported Other safety data: treatment: pneumothorax (1/34 patients), clonus (1/34 patients); control: 0/17 patients had adverse events |
|
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Low risk | A ‐ Adequate |
| Methods | n = 88, 1 centre Allocation concealment: not described Baseline similarity: age (D), sepsis Blinding: caregivers Cointerventions: application of PEEP protocolized Withdrawals: 7/88 (group unclear) Losses to follow‐up: none |
|
| Participants | Inclusions: Mechanical ventilation with PaO2 < 100 mmHg on FiO2 = 0.4 and PaO2 < 350 mmHg on FiO2 = 1 Exclusions: Presence of ARDS (more than one of the following: PaO2 < 250 mmHg on FiO2 = 1, pulmonary shunt > 25%, diffuse interstitial edema on CXR); immunocompromised; some infections; uncontrolled diabetes mellitus |
|
| Interventions | IV methylprednisolone, 30 mg/kg IV every 6 hours for 48 hours, or placebo | |
| Outcomes | Mortality: RR 1.49 (95% CI 0.85 to 2.62), based on data from 81 patients Duration of ventilation (days): 20 (range 5 to 63) in treatment group, 18 (range 3 to 72) in placebo group Adverse events leading to discontinuation of therapy not reported Other safety information: infectious complications (treatment: 30/39 patients, control: 18/42 patients) |
|
| Notes | The duration of mechanical ventilation prior to randomization was not reported. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Allocation concealment (selection bias) | Unclear risk | B ‐ Unclear |
All included studies were randomized controlled trials. Inclusions and exclusions refer to principal selection criteria. Outcomes include those selected a priori for analysis in this review. For definition of lung injury score, see American Review of Respiratory Diesease 1988;138(3):720‐3.
Methods notes: Baseline similarity: Pre‐randomization factors assessed included age, severity of illness, non‐pulmonary organ failures, presence of sepsis, and duration of hospitalization, ICU stay, or mechanical ventilation. Factors are listed if they were clinically similar between treatment and control groups. Factors with significant clinical differences (D) between groups and included in an adjusted analysis (A) are noted. Blinding: We assessed blinding of caregivers, data collectors, and outcomes assessors and note the use of other terms. We interpreted "double‐blind" to include caregiver blinding. Cointerventions: We assessed whether the use of PEEP, a lung protective ventilation strategy, weaning protocols, corticosteroids, or other interventions were standardized or documented. Withdrawals: The number of randomized patients withdrawn from the mortality analysis. Losses to follow‐up: The number of randomized patients with incomplete follow‐up data for mortality.
Abbreviations: AECC = American‐European Consensus Conference (see Background), AIDS = acquired immunodeficiency syndrome, ALI = acute lung injury, APACHE = acute physiology and chronic health evaluation (see Critical Care Medicine 1985;13(10):818‐29 and Chest 1991;100(6):1619‐36), ARDS = acute respiratory distress syndrome, CI = confidence interval, CXR = chest radiograph, DPPC = dipalmitoylphosphatidylcholine, HIV = human immunodeficiency virus, ICU = intensive care unit, IV = intravenous, LAH = left atrial hypertension, MD = difference (mean in treatment group ‐ mean in control group), MI = myocardial infarction, MODS = multiple organ dysfunction score (see Critical Care Medicine 1995;23(10):1638‐52), n = number of randomized patients, NAC = N‐acetylcysteine, PAO2 = partial pressure of alveolar oxygen, PAOP = pulmonary artery occlusion pressure, PEEP = positive end‐expiratory pressure, P/F = ratio of partial pressure of arterial oxygen (PaO2) to fraction of oxygen in inspired gas (FiO2), PGE1=prostaglandin E1, RR = relative risk, SAPS = simplified acute physiology score (see Critical Care Medicine 1984;12(11):975‐7).
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Bernard 1989 | RCT of N‐acetylcysteine in 19 patients with ARDS; clinical outcomes not reported |
| Bernard 1991 | RCT of ibuprofen in 30 patients with sepsis; not reported to have ALI/ARDS at randomization |
| Bernard 1997b | RCT of ibuprofen in 455 patients with sepsis; not all patients had ALI/ARDS at randomization |
| Bigatello 1994 | Subgroup analysis of patients with ARDS from RCT of HA‐1A (human monoclonal antiendotoxin antibody) for patients with sepsis |
| Bone 1987 | RCT of methylprednisolone in patients at risk for ARDS; not reported to have ALI at randomization |
| Bone 1995 | RCT of monoclonal antibody to endotoxin (E5) in patients with sepsis; not all patients had ALI/ARDS at randomization |
| Bursten 1996 | RCT of lisofylline in patients at risk for ARDS; not reported to have ALI at randomization |
| Fisher 1994 | RCT of human interleukin 1 receptor antagonist for patients with sepsis; not all patients had ALI/ARDS at randomization |
| Fourrier 1993 | RCT of antithrombin III concentrates in 35 patients with septic shock; not reported to have ALI/ARDS at randomization |
| Heard 1999 | RCT of prostaglandin E1 in 28 patients with ARDS; clinical outcomes not reported |
| Kawai 1988 | Case series of ulinastatin and steroids for patients with sepsis‐induced ARDS |
| Kawai 1990 | Case series of ulinastatin and steroids for patients with sepsis‐induced ARDS |
| Konrad 1995 | RCT of N‐acetylcysteine in intubated surgical intensive care unit patients; not reported to have ALI/ARDS at randomization |
| Looareesuwan 1998 | RCT of pentoxyfylline in 45 patients with severe malaria; not reported to have ALI/ARDS at randomization |
| Lucas 1981 | Quasi‐randomized (allocation based on unit number) trial of steroids during trauma resuscitation; not reported to have ALI/ARDS at randomization |
| Luce 1988 | RCT of methylprednisolone in patients with septic shock at high risk of ARDS; not reported to have ALI at randomization |
| Marshall 2001 | Subgroup analysis of patients with ARDS from RCT of afelimomab (anti‐tumour necrosis factor antibody) for severe sepsis |
| McMichan 1976 | RCT of aprotinin in patients lower extremity or pelvic trauma and shock; did not have ALI/ARDS at randomization |
| McMichan 1982 | RCT of aprotinin in patients lower extremity or pelvic trauma and shock; did not have ALI/ARDS at randomization; same patients enrolled in McMichan 1976 |
| Nelson 1998 | RCT of filgrastim in hospitalized patients with pneumonia; ARDS was exclusion criterion and not reported to have ALI |
| Nelson 2000 | RCT of filgrastim in hospitalized patients with multilobar pneumonia; ARDS was exclusion criterion and not reported to have ALI |
| Ogawa 1996 | RCT of ONO‐5046 Na (a neutrophil elastase inhibitor) in systemic inflammatory response syndrome induced lung injury; trial did not include a placebo or no therapy control group |
| Paran 1995 | RCT of octreotide for pancreatitis; not reported to have ALI/ARDS at randomization |
| Paran 2000 | RCT of octreotide for pancreatitis; not reported to have ALI/ARDS at randomization |
| Radermacher 1988 | Non‐randomized comparison of ketanserin and sodium nitroprusside in patients with ARDS |
| Radermacher 1989 | Non‐randomized crossover comparison of nitroglycerin and prostaglandin E1 in patients with ARDS |
| Root 2003 | RCT of filgrastim for patients with pneumonia and severe sepsis; not all patients had ALI/ARDS at randomization |
| Russell 1990 | Non‐randomized comparison of prostaglandin E1 to control in patients with ARDS |
| Satoh 1998 | RCT of surfactant in patients with unilateral lung injury after thoracic aneurysm surgery |
| Schuster 2003 | RCT of platelet‐activating factor acetylhydrolase in patients with severe sepsis; excluded patients with ARDS and not reported to have ALI at randomization |
| Slotman 1988 | RCT of ketoconazole to prevent ARDS; excluded patients with ARDS and not reported to have ALI at randomization |
| Sprung 1984 | RCT of corticosteroids in patients with septic shock; not reported to have ALI/ARDS at randomization |
| Tanaka 2001 | RCT of lenograstim for patients with sepsis; majority but not all patients had mild‐moderate ALI at randomization |
| Tuxen 1986 | RCT of aprotinin to prevent ARDS in patients with trauma, sepsis, haemorrhage or surgery; excluded patients with ARDS and not reported to have ALI at randomization |
| Umberger 2002 | Cost‐effectiveness data from RCT of methylprednisolone for late phase ARDS (Meduri 1998); no new clinical outcomes reported |
| van der Merwe 1985 | Non‐randomized comparison methylprednisolone to control in patients with severe trauma; not reported to have ALI/ARDS at randomization |
| Vincent 1985 | RCT of dipyridamole for the prevention of ARDS; did not have ALI at randomization |
| Wunderink 2001 | RCT of filgrastim for patients with pneumonia and sepsis; not all patients had ALI/ARDS at randomization |
| Yu 1993 | RCT of ketoconazole to prevent ARDS in patients with sepsis; not reported to have ALI at randomization |
Abbreviations: ALI = acute lung injury, ARDS = acute respiratory distress syndrome, RCT = randomized controlled trial
Characteristics of ongoing studies [ordered by study ID]
| Trial name or title | HL 10 for treatment of ALI and ARDS |
| Methods | |
| Participants | Not known |
| Interventions | HL 10 (porcine surfactant) versus standard care |
| Outcomes | Not known |
| Starting date | Not known |
| Contact information | Dr. Brian Juel Pedersen, Information Specialist, Leo Pharma, brian.pedersen@leo‐pharma.com |
| Notes | 1) Enrolment terminated May 2004; results not yet published or presented 2) Information from Leo Pharma website, http://www.leo‐pharma.com/w‐site/leo/docs.nsf/2addbdd119e92fb08025690a004eb625/797437f3e23f3e95c1256be50024818e?OpenDocument (accessed 20 April 2004) |
| Trial name or title | Late Steroid Rescue Study: The Efficacy of Corticosteroids as Rescue Therapy for the Late Phase of Acute Respiratory Distress Syndrome |
| Methods | |
| Participants | 180 patients meeting AECC criteria for ARDS, 7‐28 days from onset of ARDS, continuing to require mechanical ventilation |
| Interventions | Methylprednisolone 2 mg/kg bolus, then 0.5 mg/kg every 6 hours for 14 days, then 0.5 mg/kg every 12 hours for 7 days, followed by a taper; or placebo |
| Outcomes | 60 day mortality; ventilator‐free days to day 28; organ failure‐free days to day 28; reduction in markers of fibroproliferation and inflammation at day 7; adverse events |
| Starting date | 1997 |
| Contact information | Study chair: Leonard Hudson MD, Harborview Medical Center, Seattle WA USA; njschwab@u.washington.edu |
| Notes | 1) Enrolment terminated; preliminary results presented at American Thoracic Society International Conference, 25 May 2004 2) Study protocol available at http://www.ardsnet.org/ards02.php (accessed 20 April 2004) |
Abbreviations: AECC = American‐European Consensus Conference (Bernard 1994), ALI = acute lung injury, ARDS = acute respiratory distress syndrome
Contributions of authors
Neill Adhikari proposed and registered the title and designed the protocol. He conducted the search, retrieved relevant articles, assessed methodologic quality of retrieved articles, and abstracted data as the primary reviewer. He analysed the data and prepared the final review.
Karen Burns conducted the search, assessed methodologic quality of retrieved articles, and abstracted data as the second reviewer. She revised the final review for important intellectual content.
Maureen Meade supervised the review and resolved disagreements about article inclusion, data extraction, and methodologic quality. She revised the final review for important intellectual content.
Sources of support
Internal sources
McMaster University, Canada.
External sources
Dr Burns is the recipient of a Canadian Lung Association/Merck Frosst Postdoctoral Fellowship, Canada.
Dr Meade is a Peter Lougheed Scholar of the Canadian Institutes of Health Research, Canada.
Declarations of interest
None known
Notes
The following minor errors and omissions have been corrected in issue 1, 2005:
1) In Spragg 2002b (in the 'Table of Comparisons', under 'Surfactant'), the treatment and control numbers of patients randomized were reversed. The review previously read surfactant: '108' and control: '117'. This has been corrected to read: surfactant '117' and control '108'.
2) In Methodological quality of included studies/Baseline characteristics, the review previously stated 'Of the remaining 30 studies, nine had at least one clinically important imbalance at baseline.' This has been corrected to read 'Of the remaining 29 studies, ten had at least one clinically important imbalance at baseline.' Weigelt 1985 has now been properly cited.
3) In Methodological quality of included studies/Cointerventions, the review previously stated 'Eleven studies standardized at least one cointervention or documented its application in the treatment and control groups.' This has been corrected to read 'Twelve studies standardized at least one cointervention or documented its application in the treatment and control groups,' and Weigelt 1985 has now been appropriately cited.
Edited (no change to conclusions)
References
References to studies included in this review
- Abraham E, Park YC, Covington P, Conrad SA, Schwartz M. Liposomal prostaglandin E1 in acute respiratory distress syndrome: a placebo‐controlled, randomized, double‐blind, multicenter clinical trial. Critical Care Medicine 1996;24(1):10‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Abraham E, Baughman R, Fletcher E, Heard S, Lamberti J, Levy H, et al. Liposomal prostaglandin E1 (TLC C‐53) in acute respiratory distress syndrome: a controlled, randomized, double‐blind, multicenter clinical trial. TLC C‐53 ARDS Study Group. Critical Care Medicine 1999;27(8):1478‐85. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Anzueto A, Baughman RP, Guntupalli KK, Weg JG, Wiedemann HP, Raventos AA, et al. Aerosolized surfactant in adults with sepsis‐induced acute respiratory distress syndrome. Exosurf Acute Respiratory Distress Syndrome Sepsis Study Group. New England Journal of Medicine 1996;334(22):1417‐21. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Ardizzoia A, Lissoni P, Tancini G, Paolorossi F, Crispino S, Villa S, et al. Respiratory distress syndrome in patients with advanced cancer treated with pentoxifylline: a randomized study. Supportive Care in Cancer 1993;1(6):331‐3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- The ARDS Network. Ketoconazole for early treatment of acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA 2000;283(15):1995‐2002. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- The ARDS Clinical Trial Network. Randomized, placebo‐controlled trial of lisofylline for early treatment of acute lung injury and acute respiratory distress syndrome. Critical Care Medicine 2002;30(1):1‐6. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bernard GR, Luce JM, Sprung CL, Rinaldo JE, Tate RM, Sibbald WJ, et al. High‐dose corticosteroids in patients with the adult respiratory distress syndrome. New England Journal of Medicine 1987;317(25):1565‐70. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bernard GR, Wheeler AP, Arons MM, Morris PE, Paz HL, Russell JA, et al. A trial of antioxidants N‐acetylcysteine and procysteine in ARDS. The Antioxidant in ARDS Study Group. Chest 1997;112(1):164‐72. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bernard GR, Wheeler AP, Naum CC, Morris PE, Nelson L, Schein R, et al. A placebo‐controlled, randomized trial of IL‐10 in acute lung injury (ALI). Chest 1999;116(4 Suppl. 2):206S. 10532494 [Google Scholar]
- Bone RC, Slotman G, Maunder R, Silverman H, Hyers TM, Kerstein MD, et al. Randomized double‐blind, multicenter study of prostaglandin E1 in patients with the adult respiratory distress syndrome. Prostaglandin E1 Study Group. Chest 1989;96(1):114‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]; Slotman GJ, Kerstein MD, Bone RC, Silverman H, Maunder R, Hyers TM, et al. The effects of prostaglandin E1 on non‐pulmonary organ function during clinical acute respiratory failure. The Prostaglandin E1 Study Group. Journal of Trauma 1992;32(4):480‐8. [MEDLINE: ] [PubMed] [Google Scholar]
- Domenighetti G, Suter PM, Schaller MD, Ritz R, Perret C. Treatment with N‐acetylcysteine during acute respiratory distress syndrome: a randomized, double‐blind, placebo‐controlled clinical study. Journal of Critical Care 1997;12(4):177‐82. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Gottlieb JE, Elmer M, Steiner R. Efficacy of intravenous ICI 200,880, a neutrophil elastase inhibitor, in the treatment of adult respiratory distress syndrome (ARDS). Chest 1994;106(2 Suppl):67S. [Google Scholar]
- Gregory TJ, Steinberg KP, Spragg R, Gadek JE, Hyers TM, Longmore WJ, et al. Bovine surfactant therapy for patients with acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine 1997;155(4):1309‐15. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Holcroft JW, Vassar MJ, Weber CJ. Prostaglandin E1 and survival in patients with the adult respiratory distress syndrome. A prospective trial. Annals of Surgery 1986;203(4):371‐8. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]; Holcroft JW, Vassar MJ, Weber CJ. Prostaglandin E1 and survival in patients with the adult respiratory distress syndrome. A prospective trial. Seminars in Respiratory Medicine 1986;7(5):40‐7. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jepsen S, Herlevsen P, Knudsen P, Bud MI, Klausen NO. Antioxidant treatment with N‐acetylcysteine during adult respiratory distress syndrome: a prospective, randomized, placebo‐controlled study. Critical Care Medicine 1992;20(7):918‐23. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Kesecioglu J, Schultz MJ, Lundberg D, Lauven PM, Lachmann B. Treatment of acute lung injury (ALI/ARDS) with surfactant. American Journal of Respiratory and Critical Care Medicine 2001;163(5 Pt. 2):A819. [Google Scholar]
- Meduri GU, Headley AS, Golden E, Carson SJ, Umberger RA, Kelso T, et al. Effect of prolonged methylprednisolone therapy in unresolving acute respiratory distress syndrome: a randomized controlled trial. JAMA 1998;280(2):159‐65. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Ortolani O, Conti A, Gaudio AR, Masoni M, Novelli G. Protective effects of N‐acetylcysteine and rutin on the lipid peroxidation of the lung epithelium during the adult respiratory distress syndrome. Shock 2000;13(1):14‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Presneill JJ, Harris T, Stewart AG, Cade JF, Wilson JW. A randomized phase II trial of granulocyte‐macrophage colony‐stimulating factor therapy in severe sepsis with respiratory dysfunction. American Journal of Respiratory and Critical Care Medicine 2002;166(2):138‐43. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Reines HD, Halushka PV, Olanoff LS, Hunt PS. Dazoxiben in human sepsis and adult respiratory distress syndrome. Clinical Pharmacology and Therapeutics 1985;37(4):391‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Reines HD, Silverman H, Hurst J, Warren J, Williams J, Rotello L, et al. Effects of two concentrations of nebulized surfactant (Exosurf) in sepsis‐induced adult respiratory distress syndrome (ARDS). Critical Care Medicine 1992;20(4 Suppl.):S61. [Google Scholar]; Wiedemann H, Baughman R, DeBoisblanc B, Schuster D, Caldwell E, Weg J, et al. A multicenter trial in human sepsis‐induced ARDS of an aerosolized synthetic surfactant (Exosurf). American Review of Respiratory Disease 1992;145(4 part 2):A184. [Google Scholar]
- Rossignon MD, Khayat D, Royer C, Rouby JJ, Jacquillat C, Viars P. Functional and metabolic activity of polymorphonuclear leukocytes from patients with adult respiratory distress syndrome: results of a randomized double‐blind placebo‐controlled study on the activity of prostaglandin E1. Anesthesiology 1990;72(2):276‐81. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Shoemaker WC. Effectiveness of prostaglandin E1 in adult respiratory distress syndrome. Progress in Clinical and Biological Research 1987;236A:361‐8. [MEDLINE: ] [PubMed] [Google Scholar]; Shoemaker WC, Appel PL. Effects of prostaglandin E1 in adult respiratory distress syndrome. Surgery 1986;99(3):275‐83. [MEDLINE: ] [PubMed] [Google Scholar]
- Spragg RG, Lewis JF, Rathgeb F, Hafner D, Seeger W. Intratracheal instillation of rSP‐C surfactant improves oxygenation in patients with ARDS. American Journal of Respiratory and Critical Care Medicine 2002;165(5 Pt. 2):A22. [Google Scholar]
- Spragg RG, Lewis JF, Rathgeb F, Hafner D, Seeger W. Intratracheal instillation of rSP‐C surfactant improves oxygenation in patients with ARDS. American Journal of Respiratory and Critical Care Medicine 2002;165(5 Pt. 2):A22. [Google Scholar]
- Spragg RG, Lewis JF, Wurst W, Hafner D, Baughman RP, Wewers MD, et al. Treatment of acute respiratory distress syndrome with recombinant surfactant protein C surfactant. American Journal of Respiratory and Critical Care Medicine 2003;167(11):1562‐6. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Steinberg SM, Rodriguez JL, Bitzer LG, Rhee JW, Kelley KA, Flint LM. Indomethacin treatment of human adult respiratory distress syndrome. Circulatory Shock 1990;30(4):375‐84. [MEDLINE: ] [PubMed] [Google Scholar]
- Suter PM, Domenighetti G, Schaller MD, Laverriere MC, Ritz R, Perret C. N‐acetylcysteine enhances recovery from acute lung injury in man. A randomized, double‐blind, placebo‐controlled clinical study. Chest 1994;105(1):190‐4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Tuxen DV, Wilson JW, Cade JF. Prevention of lower respiratory herpes simplex virus infection with acyclovir in patients with the adult respiratory distress syndrome. American Review of Respiratory Disease 1987;136(2):402‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Vincent JL, Brase R, Santman F, Suter PM, McLuckie A, Dhainaut JF, et al. A multi‐centre, double‐blind, placebo‐controlled study of liposomal prostaglandin E1 (TLC C‐53) in patients with acute respiratory distress syndrome. Intensive Care Medicine 2001;27(10):1578‐83. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Walmrath D, Vaal JB, Bruining HA, Kilian JG, Papazian L, Hohlfeld J, et al. Treatment of ARDS with a recombinant SP‐C (rSP‐C) based synthetic surfactant. American Journal of Respiratory and Critical Care Medicine 2000;161(3):A379. [Google Scholar]
- Weg JG, Balk RA, Tharratt RS, Jenkinson SG, Shah JB, Zaccardelli D, et al. Safety and potential efficacy of an aerosolized surfactant in human sepsis‐induced adult respiratory distress syndrome. JAMA 1994;272(18):1433‐8. [MEDLINE: ] [PubMed] [Google Scholar]
- Weigelt JA, Norcross JF, Borman KR, Snyder WH, III. Early steroid therapy for respiratory failure. Archives of Surgery 1985;120(5):536‐40. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
- Bernard GR, Swundell BB, Meredith MJ, et al. Glutathione (GSH) repletion by N‐acetylcysteine (NAC) in patients with the adult respiratory distress syndrome. American Review of Respiratory Disease 1989;139(4):A221. [Google Scholar]
- Bernard GR, Reines HD, Halushka PV, Higgins SB, Metz CA, Swindell BB, et al. Prostacyclin and thromboxane A2 formation is increased in human sepsis syndrome. Effects of cyclooxygenase inhibition. American Review of Respiratory Disease 1991;144(5):1095‐01. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bernard GR, Wheeler AP, Russell JA, Schein R, Summer WR, Steinberg KP, et al. The effects of ibuprofen on the physiology and survival of patients with sepsis. The Ibuprofen in Sepsis Study Group. New England Journal of Medicine 1997;336(13):912‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bigatello LM, Greene RE, Sprung CL, Panacek EA, Straube RC, Zimmerman JL, et al. HA‐1A in septic patients with ARDS: results from the pivotal trial. Intensive Care Medicine 1994;20(5):328‐34. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bone RC, Fisher CJ, Jr, Clemmer TP, Slotman GJ, Metz CA. Early methylprednisolone treatment for septic syndrome and the adult respiratory distress syndrome [published erratum appears in Chest 1988;94(2):448]. Chest 1987;92(6):1032‐6. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bone RC, Balk RA, Fein AM, Perl TM, Wenzel RP, Reines HD, et al. A second large controlled clinical study of E5, a monoclonal antibody to endotoxin: results of a prospective, multicenter, randomized, controlled trial. The E5 Sepsis Study Group. Critical Care Medicine 1995;23(6):994‐1006. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bursten SL, Federighi DA, Parsons P, Harris WE, Abraham E, Moore EE, Jr, et al. An increase in serum C18 unsaturated free fatty acids as a predictor of the development of acute respiratory distress syndrome. Critical Care Medicine 1996;24(7):1129‐36. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Fisher CJ, Jr, Dhainaut J‐F, Opal SM, Pribble JP, Balk RA, Slotman GJ, et al. Recombinant human interleukin 1 receptor antagonist in the treatment of patients with sepsis syndrome: Results from a randomized, double‐blind, placebo‐controlled trial. JAMA 1994;271(23):1836‐43. [MEDLINE: ] [PubMed] [Google Scholar]
- Fourrier F, Chopin C, Huart JJ, Runge I, Caron C, Goudemand J. Double‐bind, placebo‐controlled trial of antithrombin III concentrates in septic shock with disseminated intravascular coagulation. Chest 1993;104(3):882‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Heard SO, Longtine K, Toth I, Puyana JC, Potenza B, Smyrnios N. The influence of liposome‐encapsulated prostaglandin E1 on hydrogen peroxide concentrations in the exhaled breath of patients with the acute respiratory distress syndrome. Anesthesia and Analgesia 1999;89(2):353‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Kawai S, Kawahira M, Miura H, Kobayashi H. Effect of ulinastatin on septic ARDS. Japanese Pharmacology and Therapeutics 1988;16(8):453‐9. [MEDLINE: ] [Google Scholar]
- Kawai S, Sakayori S, Watanabe H, Kobayashi H. Usefulness of a protease inhibitor (urinastatin) in ARDS with infectious diseases. Nihon Kyobu Shikkan Gakkai Zasshi 1990;28(6):843‐51. [MEDLINE: ] [PubMed] [Google Scholar]
- Konrad F, Schoenberg MH, Wiedmann H, Kilian J, Georgieff M. The application of N‐acetylcysteine as an antioxidant and mucolytic in mechanical ventilation in intensive care patients. A prospective, randomized, placebo‐controlled, double‐blind study [Die Applikation von N‐Acetylcystein als Antioxidans und Mukolytikum bei beameten Intensivpatienten]. Anaesthesist 1995;44(9):651‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Looareesuwan S, Wilairatana P, Vannaphan S, Wanaratana V, Wenisch C, Aikawa M, et al. Pentoxifylline as an ancillary treatment for severe falciparum malaria in Thailand. American Journal of Tropical Medicine and Hygiene 1998;58(3):348‐53. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Lucas CE, Ledgerwood AM. Pulmonary response of massive steroids in seriously injured patients. Annals of Surgery 1981;194(3):256‐61. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luce JM, Montgomery AB, Marks JD, Turner J, Metz CA, Murray JF. Ineffectiveness of high‐dose methylprednisolone in preventing parenchymal lung injury and improving mortality in patients with septic shock. American Review of Respiratory Disease 1988;138(1):62‐8. [DOI] [PubMed] [Google Scholar]
- Marshall J for the Afelimomab Study Group. Effect of anti‐TNF antibody on pulmonary component of MOD score. American Journal of Respiratory and Critical Care Medicine 2001;163(5):A820. [Google Scholar]
- McMichan JC, Rosengarten DS, McNeur JC, Philipp E. Posttraumatic lung syndrome. Definition, diagnosis, and therapy. Report of a double blind study [Das posttraumatische Lungen‐Syndrom. Definition, Diagnose und Therapie]. Medizinische Welt 1976;76(48):2331‐40. [MEDLINE: ] [PubMed] [Google Scholar]
- McMichan JC, Rosengarten DS, Philipp E. Prophylaxis of post‐traumatic pulmonary insufficiency by protease‐inhibitor therapy with aprotinin: a clinical study. Circulatory Shock 1982;9(2):107‐16. [MEDLINE: ] [PubMed] [Google Scholar]
- Nelson S, Belknap SM, Carlson RW, Dale D, DeBoisblanc B, Farkas S, et al. A randomized controlled trial of filgrastim as an adjunct to antibiotics for treatment of hospitalized patients with community‐acquired pneumonia. CAP Study Group. Journal of Infectious Diseases 1998;178(4):1075‐80. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Nelson S, Heyder AM, Stone J, Bergeron MG, Daugherty S, Peterson G, et al. A randomized controlled trial of filgrastim for the treatment of hospitalized patients with multilobar pneumonia. Journal of Infectious Diseases 2000;182(3):970‐3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Ogawa M, Tamakuma S, Hirasawa H, Siba T, Nakajima M. Effect of a Specific Neutrophil Elastase Inhibitor, ONO‐5046 Na on the Lung Dysfunction Associated with SIRS (Systemic Inflammatory Response Syndrome). European Respiratory Journal 1996;9:286s. [Google Scholar]
- Paran H, Neufeld D, Mayo A, Shwartz I, Singer P, Kaplan O, et al. Preliminary report of a prospective randomized study of octreotide in the treatment of severe acute pancreatitis. Journal of the American College of Surgeons 1995;181(2):121‐4. [MEDLINE: ] [PubMed] [Google Scholar]
- Paran H, Mayo A, Paran D, Neufeld D, Shwartz I, Zissin R, et al. Octreotide treatment in patients with severe acute pancreatitis. Digestive Diseases and Sciences 2000;45(11):2247‐51. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Radermacher P, Huet Y, Pluskwa F, Herigault R, Mal H, Teisseire B, Lemaire F. Comparison of ketanserin and sodium nitroprusside in patients with severe ARDS. Anesthesiology 1988;68(1):152‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Radermacher P, Santak B, Assmann R, Falke KJ. Prostaglandin E1 and right ventricular function in ARDS. Intensive Care Medicine 1989;15(2):146‐7. [MEDLINE: ] [PubMed] [Google Scholar]
- Root RK, Lodato RF, Patrick W, Cade JF, Fotheringham N, Milwee S, et al. Multicenter, double‐blind, placebo‐controlled study of the use of filgrastim in patients hospitalized with pneumonia and severe sepsis. Critical Care Medicine 2003;31(2):367‐73. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Russell JA, Ronco JJ, Dodek PM. Physiologic effects and side effects of prostaglandin E1 in the adult respiratory distress syndrome. Chest 1990;97(3):684‐92. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Satoh D, Matsukawa S, Saishu T, Hashimoto Y. Effect of surfactant on respiratory failure associated with thoracic aneurysm surgery. Critical Care Medicine 1998;26(10):1660‐2. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Schuster DP, Metzler M, Opal S, Lowry S, Balk R, Abraham E, et al. Recombinant platelet‐activating factor acetylhydrolase to prevent acute respiratory distress syndrome and mortality in severe sepsis: Phase IIb, multicenter, randomized, placebo‐controlled, clinical trial. Critical Care Medicine 2003;31(6):1612‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Slotman GJ, Burchard KW, D'Arezzo A, Gann DS. Ketoconazole prevents acute respiratory failure in critically ill surgical patients. Journal of Trauma 1988;28(5):648‐54. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Sprung CL, Caralis PV, Marcial EH, Pierce M, Gelbard MA, Long WM, et al. The effects of high‐dose corticosteroids in patients with septic shock. A prospective, controlled study. New England Journal of Medicine 1984;311(18):1137‐43. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Tanaka H, Nishino M, Nakamori Y, Ogura H, Ishikawa K, Shimazu T, et al. Granulocyte colony‐stimulating factor (G‐CSF) stiffens leukocytes but attenuates inflammatory response without lung injury in septic patients. Journal of Trauma 2001;51(6):1110‐6. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Tuxen DV, Cade JF. Effect of aprotinin in adult respiratory distress syndrome. Anaesthesia and Intensive Care 1986;14(4):390‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Umberger R, Headley A, Waters T, Tolley E, Stentz F, Golden E, Meduri G. Cost‐effectiveness of methylprednisolone treatment (MPT) in unresolving ARDS (U‐ARDS). American Journal of Respiratory and Critical Care Medicine 2002;165(5 Pt. 2):A22. [Google Scholar]
- Merwe CJ, Louw AF, Welthagen D, Schoeman HS. Adult respiratory distress syndrome in cases of severe trauma ‐ the prophylactic value of methylprednisolone sodium succinate. South African Medical Journal 1985;67(8):279‐84. [MEDLINE: ] [PubMed] [Google Scholar]
- Vincent JL, Brimioulle S, Berre J, Kahn RJ. Prevention of the adult respiratory distress syndrome with dipyridamole. Critical Care Medicine 1985;13(10):783‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Wunderink R, Leeper K, Jr, Schein R, Nelson S, DeBoisblanc B, Fotheringham N, et al. Filgrastim in patients with pneumonia and severe sepsis or septic shock. Chest 2001;119(2):523‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Yu M, Tomasa G. A double‐blind, prospective, randomized trial of ketoconazole, a thromboxane synthetase inhibitor, in the prophylaxis of the adult respiratory distress syndrome. Critical Care Medicine 1993;21(11):1635‐42. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
References to ongoing studies
- Acute respiratory distress syndrome. http://www.leo‐pharma.com/w‐site/leo/docs.nsf/2addbdd119e92fb08025690a004eb625/797437f3e23f3e95c1256be50024818e?OpenDocument [Accessed 20 April 2004]2004.
- ARDS Clinical Network. Late steroid rescue study (LaSRS): the efficacy of corticosteroids as rescue therapy for the late phase of acute respiratory distress syndrome. http://www.ardsnet.org/documents/lasrs6200web.pdf [Accessed 20 April 2004]2000.
Additional references
- Amato MB, Barbas CS, Medeiros DM, Magaldi RB, Schettino GP, Lorenzi‐Filho G, et al. Effect of a protective‐ventilation strategy on mortality in the acute respiratory distress syndrome. New England Journal of Medicine 1998;338(6):347‐54. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Anzueto A. Surfactant supplementation in the lung. Respiratory Care Clinics of North America 2002;8(2):211‐36. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- The Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. New England Journal of Medicine 2000;342(18):1301‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. Lancet 1967;2(7511):319‐23. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bernard GR. Potential of N‐acetylcysteine as treatment for the adult respiratory distress syndrome. European Respiratory Journal Supplement 1990;11:496s‐8s. [MEDLINE: ] [PubMed] [Google Scholar]
- Bernard GR. N‐acetylcysteine in experimental and clinical acute lung injury. American Journal of Medicine 1991;91(3C):54S‐9S. [DOI] [PubMed] [Google Scholar]
- Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, et al. Report of the American‐European consensus conference on ARDS: definitions, mechanisms, relevant outcomes and clinical trial coordination. The Consensus Committee. Intensive Care Medicine 1994;20(3):225‐32. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Bone RC, Slotman G, Maunder R, Silverman H, Hyers TM, Kerstein MD, et al. Randomized double‐blind, multicenter study of prostaglandin E1 in patients with the adult respiratory distress syndrome. Prostaglandin E1 Study Group. Chest 1989;96(1):114‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Brochard L, Roudot‐Thoraval F, Roupie E, Delclaux C, Chastre J, Fernandez‐Mondejar E, et al. Tidal volume reduction for prevention of ventilator‐induced lung injury in acute respiratory distress syndrome. The Multicenter Trial Group on Tidal Volume reduction in ARDS. American Journal of Respiratory and Critical Care Medicine 1998;158(6):1831‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Brower RG, Shanholtz CB, Fessler HE, Shade DM, White P, Jr, Wiener CM, et al. Prospective, randomized, controlled clinical trial comparing traditional versus reduced tidal volume ventilation in acute respiratory distress syndrome patients. Critical Care Medicine 1999;27(8):1492‐8. [10470755] [DOI] [PubMed] [Google Scholar]
- Brower RG, Ware LB, Berthiaume Y, Matthay MA. Treatment of ARDS. Chest 2001;120(4):1347‐67. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Chadda K, Annane D. The use of corticosteroids in severe sepsis and acute respiratory distress syndrome. Annals of Medicine 2002;34(7‐8):582‐9. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Cochran W. The combination of estimates from different experiments. Biometrics 1954;10:101‐29. [Google Scholar]
- Conner BD, Bernard GR. Acute respiratory distress syndrome. Potential pharmacologic interventions. Clinics in Chest Medicine 2000;21(3):563‐87. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Cracknell J, Møller A, Pedersen T. Cochrane Anaesthesia Group module. In: The Cochrane Library, issue 1, 2003, Update Software, Oxford.
- Cranshaw J, Griffiths MJ, Evans TW. The pulmonary physician in critical care ‐ part 9: non‐ventilatory strategies in ARDS. Thorax 2002;57(9):823‐9. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7(3):177‐88. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Devereaux PJ, Manns BJ, Ghali WA, Quan H, Lacchetti C, Montori VM, et al. Physician interpretations and textbook definitions of blinding terminology in randomized controlled trials. JAMA 2001;285(15):2000‐3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Dos Santos CC, Slutsky AS. Invited review: mechanisms of ventilator‐induced lung injury: a perspective. Journal of Applied Physiology 2000;89(4):1645‐55. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Dos Santos CC, Chant C, Slutsky AS. Pharmacotherapy of acute respiratory distress syndrome. Expert Opinion in Pharmacotherapy 2002;3(7):875‐88. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Ferguson ND, Davis A, Chan CK, Slutsky AS, Detsky AS, Stewart TE. Development of a modified clinical definition of ARDS using the delphi technique. American Journal of Respiratory and Critical Care Medicine 2001;163:A449. [Google Scholar]
- Fleiss JL. The statistical basis of meta‐analysis. Statistical Methods in Medical Research 1993;2(2):121‐45. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Guyatt G, Cook D, Devereaux PJ, Meade M, Strauss S. Therapy. In: Guyatt G, Rennie D editor(s). Users' guides to the medical literature: a manual for evidence‐based clinical practice. Chicago: AMA Press, 2002:55‐80. [Google Scholar]
- Herridge MS, Cheung AM, Tansey CM, Matte‐Martyn A, Diaz‐Granados N, Al Saidi F, et al Canadian Critical Care Trials Group. One‐year outcomes in survivors of the acute respiratory distress syndrome. New England Journal of Medicine 2003;348(8):683‐93. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21:1539‐58. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Hite RD, Morris PE. Acute respiratory distress syndrome: Pharmacological treatment options in development. Drugs 2001;61(7):897‐907. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Holcroft JW, Vassar MJ, Weber CJ. Prostaglandin E1 and survival in patients with the adult respiratory distress syndrome. A prospective trial. Seminars in Respiratory Medicine 1986;7(5):40‐7. [MEDLINE: ] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laterre PF, Wittebole X, Dhainaut JF. Anticoagulant therapy in acute lung injury. Critical Care Medicine 2003;31(4 Suppl.):S329‐36. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Lewis JF, Brackenbury A. Role of exogenous surfactant in acute lung injury. Critical Care Medicine 2003;31(4 Suppl):S324‐8. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Lovat R, Preiser J‐C. Antioxidant therapy in intensive care. Current Opinion in Critical Care 2003;9(4):266‐70. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Luce JM. Acute lung injury and the acute respiratory distress syndrome. Critical Care Medicine 1998;26(2):369‐76. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Marras T, Herridge M, Mehta S. Corticosteroid therapy in acute respiratory distress syndrome. Intensive Care Medicine 1999;25(10):1191‐3. [DOI] [PubMed] [Google Scholar]
- McIntyre RC, Pulido EJ, Bensard DD, Shames BD, Abraham E. Thirty years of clinical trials in acute respiratory distress syndrome. Critical Care Medicine 2000;28(9):3314‐31. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Montori V, Guyatt G, Oxman A, Cook D. Summarizing the evidence: fixed‐effects and random‐effects models. In: Guyatt G, Rennie D editor(s). Users' guides to the medical literature: a manual for evidence‐based clinical practice. Chicago: AMA Press, 2002:539‐46. [Google Scholar]
- Murphy DB, Cregg N, Tremblay L, Engelberts D, Laffey JG, Slutsky AS, et al. Adverse ventilatory strategy causes pulmonary‐to‐systemic translocation of endotoxin. American Journal of Respiratory and Critical Care Medicine 2000;162(1):27‐33. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Opal SM. Clinical trial design and outcomes in patients with severe sepsis. Shock 2003;20(4):295‐302. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Oxman AD, Guyatt GH. A consumer's guide to subgroup analyses. Annals of Internal Medicine 1992;116(1):78‐84. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Oxman A, Guyatt G, Cook D, Montori V. Summarizing the evidence. In: Guyatt G, Rennie D editor(s). Users' guides to the medical literature: a manual for evidence‐based clinical practice. Chicago: AMA Press, 2002:155‐73. [Google Scholar]
- Que LG, Huang Y‐C. Pharmacologic adjuncts during mechanical ventilation. Seminars in Respiratory and Critical Care Medicine 2000;21(3):223‐32. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Ranieri VM, Suter PM, Tortorella C, Tullio R, Dayer JM, Brienza A, et al. Effect of mechanical ventilation on inflammatory mediators in patients with acute respiratory distress syndrome: a randomized controlled trial. JAMA 1999;282(1):54‐61. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- The Cochrane Collaboration. Review Manager (RevMan). Version 4.2 for Windows. Oxford, England: The Cochrane Collaboration, 2004.
- Robinson KA, Dickersin K. Development of a highly sensitive search strategy for the retrieval of reports of controlled trials using PubMed. International Journal of Epidemiology 2002;31:150‐3. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Rubenfeld GD. Epidemiology of acute lung injury. Critical Care Medicine 2003;31(4 Suppl):S276‐84. [DOI] [PubMed] [Google Scholar]
- Schoenfeld DA, Bernard GR. Statistical evaluation of ventilator‐free days as an efficacy measure in clinical trials of treatments for acute respiratory distress syndrome. Critical Care Medicine 2002;30(8):1772‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Shoemaker WC. Effectiveness of prostaglandin E1 in adult respiratory distress syndrome. Progress in Clinical and Biological Research 1987;236A:361‐8. [MEDLINE: ] [PubMed] [Google Scholar]
- Slotman GJ, Kerstein MD, Bone RC, Silverman H, Maunder R, Hyers TM, et al. The effects of prostaglandin E1 on non‐pulmonary organ function during clinical acute respiratory failure. The Prostaglandin E1 Study Group. Journal of Trauma 1992;32(4):480‐8. [MEDLINE: ] [PubMed] [Google Scholar]
- Sokol J, Jacobs SE, Bohn D. Inhaled nitric oxide for acute hypoxemic respiratory failure in children and adults (C. Cochrane Database of Systematic Reviews 2002, Issue 4. [DOI: 10.1002/14651858.CD002787; MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Spragg RG. Surfactant replacement therapy. Clinics in Chest Medicine 2000;21(3):531‐41. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Spragg RG. The future of surfactant therapy for patients with acute lung injury ‐ new requirements and new surfactants. Biology of the Neonate 2002;81(Suppl. 1):20‐4. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Stewart TE, Meade MO, Cook DJ, Granton JT, Hodder RV, Lapinsky SE, et al. Evaluation of a ventilation strategy to prevent barotrauma in patients at high risk for acute respiratory distress syndrome. Pressure‐ and Volume‐Limited Ventilation Strategy Group. New England Journal of Medicine 1998;338(6):355‐61. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Tasaka S, Hasegawa N, Ishizaka A. Pharmacology of acute lung injury. Pulmonary Pharmacology and Therapeutics 2002;15(2):83‐95. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Thompson BT. Glucocorticoids and acute lung injury. Critical Care Medicine 2003;31(4 Suppl):S253‐7. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Villar J, Perez‐Mendez L, Kacmarek RM. Current definitions of acute lung injury and the acute respiratory distress syndrome do not reflect their true severity and outcome. Intensive Care Medicine 1999;25(9):930‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Villar J, Flores C, Mendez‐Alvarez S. Genetic susceptibility to acute lung injury. Critical Care Medicine 2003;31(4 Suppl):S272‐5. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Ware LB, Matthay MA. The acute respiratory distress syndrome. New England Journal of Medicine 2000;342(18):1334‐49. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]
- Whitehead J, Stratton I. Group sequential clinical trials with triangular continuation regions. Biometrics 1983;39(1):227‐36. [MEDLINE: ] [PubMed] [Google Scholar]
- Wiedemann H, Baughman R, DeBoisblanc B, Schuster D, Caldwell E, Weg J, et al. A multicenter trial in human sepsis‐induced ARDS of an aerosolized synthetic surfactant (Exosurf). American Review of Respiratory Disease 1992;145(4 part 2):A184. [Google Scholar]
- Wiedemann HP, Arroliga AC, Komara JJ, Jr. Emerging systemic pharmocologic approaches in acute respiratory distress syndrome. Respiratory Care Clinics of North America 2003;9(4):419‐35. [MEDLINE: ] [DOI] [PubMed] [Google Scholar]