

Key Teaching Points.
-
•
Device recapture during leadless pacemaker implant is frequently performed should the parameters be unsatisfactory. Operators need to cautiously align the delivery system with the deployed device before locking the tether.
-
•
In patients with small body habitus and right ventricular size, apical implantation of Micra pacemaker may increase the challenge of subsequent recaptures with the potential for damage to the tether owing to repeated abrasions.
-
•
Percutaneous recovery of an embolized Micra leadless pacemaker can be safely performed even with an unfavorable device orientation.
Introduction
The Micra transcatheter pacing system (Medtronic, Minneapolis, MN) is a safe and effective alternative to transvenous pacemaker in selected patients.1, 2, 3 The device was designed with full recapture capability. In 40% of cases, initial deployment of device may result in unsatisfactory electrical parameters, necessitating recapture.4 The tether in the delivery system serves as an important connection between the device and the delivery catheter, allowing multiple recaptures to be performed. This report describes an unexpected event of tether breakage during a difficult recapture attempt, leading to device embolization. Small body build of the patient and apical deployment of the device are postulated as possible contributory factors to this complication.
Case report
An 83-year-old woman with small body habitus (weight: 56 kg, height: 152 cm, body mass index [BMI]: 24.2, body surface area [BSA]: 1.52 m2) presented with symptomatic 2:1 atrioventricular block. After discussing the options of a transvenous dual-chamber pacemaker and a leadless pacemaker implant, the patient opted to proceed with the latter.
The first 2 deployments at mid and low interventricular septum resulted in high pacing thresholds steadily greater than 3.0 V at 0.24 ms, although R-wave amplitudes were more than 5 mV and impedances were within range. Device recaptures were performed uneventfully. The third implant at the right ventricle (RV) apex yielded similar results. Device retrieval from the apex, however, was more difficult owing to the unfavorable angle between the recapture cone and the Micra (Figure 1). After prolonged manipulation, the Micra was dislodged from myocardial anchorage. While the operator attempted to realign the dislodged leadless pacemaker by gently pulling the tether, there was a sudden give-way sensation and the tether was found broken. As a result, the leadless pacemaker embolized to the inferior branch of the left pulmonary artery.
Figure 1.

A: Left anterior oblique view and B: right anterior oblique (RAO) view showing apical position of the final implant attempt. C: Final deployment position in RAO view. Note the naturally upward curve of the delivery catheter, making it unfavorably aligned with the Micra transcatheter pacing system. D: RAO view showing acute angle between the deployed device and the recapture cone when tether is pulled.
To retrieve the dislodged device, a 7F multipurpose catheter (MPA1 catheter, Cordis, Fremont, CA) was placed at the left pulmonary artery. A 20 mm snare (NSnare, Cook Medical LLC, Bloomington, IN) was deployed with the aim to snare the proximal retrieval feature. However, the upside-down position of the embolized Micra meant that the snare was only able to reach the tines. The tines were snared successfully (Figure 2) and the device was gently pulled back into the RV. A second 25 mm snare (NSnare, Cook Medical LLC) was deployed railing over the first snare to secure the grasp on the deformable nitinol tines. The whole system was pulled into the inferior vena cava, where careful manipulation to reposition the Micra allowed a third snare to catch the proximal retrieval feature. The whole system was then removed from the patient’s body via the Micra delivery sheath. The patient subsequently underwent implantation of a transvenous dual-chamber pacemaker.
Figure 2.

A: Angiogram showing Micra embolized to the left pulmonary artery, without obstruction of the flow. B: Embolized device dragged to the right ventricle with a snare around the tines. C: Second snare looped around the tines for safety before pulling it to the inferior vena cava (IVC). D: Repositioning within the IVC allowed the third snare to grasp the proximal retrieval feature, with successful retrieval via the Micra delivery sheath.
The device and delivery catheter were examined after retrieval. The tether was found to be broken approximately mid length, with evidence of damage likely owing to mechanical abrasion during recapture attempts (Figure 3). We postulate that the acute angle between the recapture cone and the apically implanted Micra constituted a hinge point at the edge of the recapture cone (Figure 1D). The tether got abraded over the edge of the recapture cone during multiple recapture attempts, which caused its gradual weakening. After dislodgment from myocardial anchorage, the Micra became completely misaligned with the cone and the tether broke with additional tension.
Figure 3.
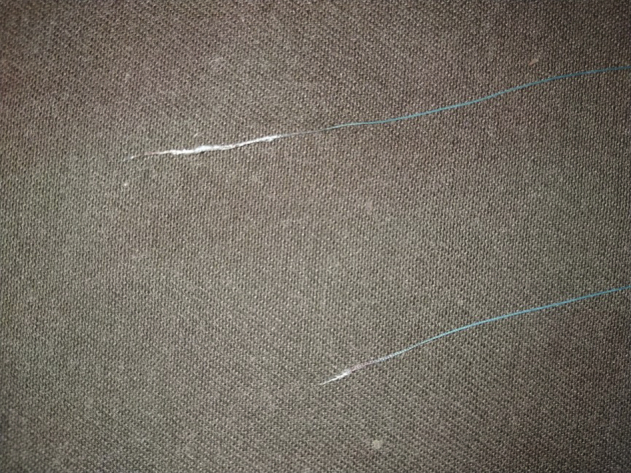
Examination of the broken tether showed damage, probably caused by abrasion.
Discussion
This case highlights the difficulties of Micra implantation in patients with small body habitus. Previous studies found that low BMI may be one of the risk factors associated with complication.1, 5 Compared to BMI, BSA may better correlate with RV cavity size and echocardiography-based RV dimensions may be smaller in women with lesser BSA.6 Previously published data including the pivotal trial1 and the Micra postapproval registry3 did not include BMI or BSA of enrolled patients. Additional studies are needed to investigate the impact of patient-related factors on procedural success and rate of complications.
Device repositioning after deployment is commonly performed to achieve adequate fixation or electrical parameters.4 To perform recapture, it is recommended to apply tension to the tether while advancing the delivery system until the recapture cone is in contact with the device.7 The operator should then make sure that the recapture cone and device are coaxial before locking the tether and retracting the device. The natural upward curvature of the delivery catheter may make this maneuver difficult in small hearts (Figure 1C). With an apically deployed device, an acute angle may form between the device and recapture cone when one pulls the tether. Repeated recapture attempt in this situation could rub the tether against the edge of the recapture cone and weaken it significantly.
The tether of the Micra leadless pacemaker is made up of polyester (polyethylene terephthalate) coated with polytetrafluoroethylene.8 According to Medtronic engineers, its tensile strength measured in preclinical testing was approximately 10 lb, which is remarkably strong, taking into account its thin caliber. However, repeated abrasion can still break it.
Device embolization is a rare but dreaded complication of a leadless pacemaker implant procedure.9 In the Micra investigational device exemption study,1 no device dislodgment or embolization was encountered. This case illustrates that even with an unfavorable orientation, the embolized leadless pacemaker can still be safely retrieved percutaneously.
Conclusion
Tether failure during Micra recapture is a rare event. Although Micra implantation is generally considered safe and effective, device recapture in patients with small body habitus may be technically challenging. Caution must be made to avoid abrasion of the tether onto the edge of the recapture cone, which can lead to breaking of the tether.
References
- 1.Reynolds D., Duray G.Z., Omar R. A leadless intracardiac transcatheter pacing system. N Engl J Med. 2016;374:533–541. doi: 10.1056/NEJMoa1511643. [DOI] [PubMed] [Google Scholar]
- 2.Duray G.Z., Ritter P., El-Chami M. Long-term performance of a transcatheter pacing system: 12-month results from the Micra Transcatheter Pacing Study. Heart Rhythm. 2017;14:702–709. doi: 10.1016/j.hrthm.2017.01.035. [DOI] [PubMed] [Google Scholar]
- 3.Roberts P.R., Clementy N., Al-Samadi F. A leadless pacemaker in the real-world setting: the Micra Transcatheter Pacing System Post-Approval Registry. Heart Rhythm. 2017;14:1375–1379. doi: 10.1016/j.hrthm.2017.05.017. [DOI] [PubMed] [Google Scholar]
- 4.Piccini J.P., Stromberg K., Jackson K.P. Long-term outcomes in leadless Micra transcatheter pacemakers with elevated thresholds at implantation: results from the Micra transcatheter pacing system global clinical trial. Heart Rhythm. 2017;14:685–691. doi: 10.1016/j.hrthm.2017.01.026. [DOI] [PubMed] [Google Scholar]
- 5.Mont L., Cunnane R., El-Chami M.F. Risk factors for cardiac perforation/effusion in leadless pacemaker patients: experience with the Micra transcatheter pacemaker [abstract] Heart Rhythm. 2018;18:S119. [Google Scholar]
- 6.Willis J., Augustine D., Shah R., Stevens C., Easaw J. Right ventricular normal measurements: time to index? J Am Soc Echocardiogr. 2012;25:1259–1267. doi: 10.1016/j.echo.2012.06.015. [DOI] [PubMed] [Google Scholar]
- 7.Medtronic Micra MC1VR01 clinician manual. Manual Document Number: M948893A001 E. http://manuals.medtronic.com/content/dam/emanuals/crdm/CONTRIB_231758.pdf Available at. Accessed March 10, 2019.
- 8.Medtronic Micra product specification. April 2016. https://www.medtronic.com/content/dam/medtronic-com/01_crhf/brady/pdfs/2018-05-micra-specification-sheet.pdf Available at. Accessed March 10, 2019.
- 9.Sundaram S., Choe W. The one that got away: a leadless pacemaker embolizes to the lungs. Heart Rhythm. 2016;13:2316. doi: 10.1016/j.hrthm.2016.09.006. [DOI] [PubMed] [Google Scholar]