

Abstract
Murine pharmacokinetics (PK) represents the absorption, distribution, metabolism, and elimination of drugs from the body, which helps to guide clinical studies, ultimately resulting in more effective drug treatment. The purpose of this protocol is to describe a serial bleeding protocol, obtaining blood samples at six time points from single mouse to yield a complete PK profile. This protocol has proved to be rapid, highly repeatable, and relatively easy to acquire. Comparing with the conventional PK studies, this method not only dramatically reduces animal usage, but also decreases sample variation obtained from different animals.
Keywords: Blood, Plasma, Pharmacokinetic, Submandibular vein, Orbital venous plexus, Cardiac puncture
Background
Pharmacokinetic, from ancient Greek pharmakon “drug” and kinetikos “movement”, studies how the body handle drugs. In vivo murine PK studies are crucial to ensure compounds have appropriate PK properties in preclinical pharmacology and toxicity studies. The drug concentration can be measured in the blood, plasma, urine or other easily sampled fluids. However, in vivo PK studies have been traditionally low-throughput experiments: 6-12 terminal blood samples per compound in triplicate, requires 18-36 mice per study. The high animal usage and labor-intensive sampling are main hurdle for this conventional assay. With the improving sensitivity of bioanalytical method, efforts to increase the PK throughout have been reported including the use of cassette dosing ( Berman et al., 1997 , Korfmacher et al., 2001 ), Snapshot PK method ( Liu et al., 2008 ) and more recently, Fast PK ( Reddy et al., 2012 ). We have established a serial bleeding protocol, in which six blood samples can be collected from same mice by a submandibular vein (cheek) bleed, the orbital bleed and a cardiac puncture (terminal bleed) at a very narrow time window after administration of drugs. The protocol ensures collection of blood at specific time point and decreases variability among multiple subjects with dramatically decreased animal usage. This method is extremely valuable for the murine pharmacokinetics study with limited number of animals, and compounds with short half-life or fast clearance property.
Materials and Reagents
Syringe: BD 1 ml Syringe with 27 G x 1/2 in needle (BD, catalog number: 309623)
Capillary (Fisher Scientific, FisherbrandTM, catalog number: 22-362566)
Oral gavage needle (Reusable Small Animal Feeding Needles) (Cadence Science, catalog number: 7905)
Eppendorf tubes (Eppendorf® Safe-Lock microcentrifuge tubes) (Eppendorf, catalog number: 022363611)
Non-sterile cotton gauze sponges (Fisher Scientific, FisherbrandTM, catalog number: 22-362178)
Tubes to collect blood obtained from cardiac puncture (SARSTEDT, catalog number: 2022-07-31)
Oatp1b2 KO and wild-type DBA mice (between 8 and 12 weeks of age, see Procedure for details)
Nilotinib (Chemietek, catalog number: CT-NL001)
Paclitaxel (LC Laboratories, catalog number: P-9600)
Saline (Hospira, NDC:0409-4888-02)
Hydroxypropyl methylcellulose (HPMC) (Sigma-Aldrich, catalog number: 09963-25G)
Cremophor EL (Sigma-Aldrich, catalog number: 238470-1SET)
Ethyl alcohol (Sigma-Aldrich, catalog number: E7023)
Pipet rubber bulb for capillary tubes (Globe Scientific, catalog number: 51674)
Isoflurane (Henry Schein, NDC 11695-7667-1)
0.5% (m/v) HPMC (see Recipes)
Equipment
Lancet, Goldenrod 4 or 5 mm (MEDIpoint, catalog number: Goldenrod ANIMAL LANCET 4MM)
Pipettes, 200 μl and 20 μl single channel pipette4 (Mettler-Toledo, ShopRAININ, model: Pipet-Lite XLS+, catalog numbers: 17014391 and 17014392)
Red lamp (UL E187949F, 250V, 660W)
Scout Pro Balance (OHAUS, model: SP202)
Tail vein injection platform (in low tail injection platform) (AIMS, catalog number: IL300)
Centrifuge (Eppendorf, Mini spin plus, model: 5453)
Sonicator (QSONICA, model: Q55)
Vaporstick anesthesia Machine (Smiths Medical, Surgivet, model: V7015)
Classic T3Vaporizer (Smiths Medical, Surgivet, model: VCT302)
Digital vortex mixer (Fisher Scientific, FisherbrandTM, catalog number: 02-215-370)
Software
WinNonlin 6.2 software (Pharsight, Leblanc et al., 2018 )
Graph Pad prism 6.0
Procedure
-
Mice
The plasma pharmacokinetic study of single-dose of paclitaxel (PTX) pretreated with nilotinib or vehicle were performed on Oatp1b2 KO and wild-type DBA mice. These mice were provided by Richard B. Kim (Western University, London, Ontario, Canada) and Jeffrey L. Stock (Pfizer Inc., Groton, Connecticut, USA). Mice between 8 and 12 weeks of age, were housed in a temperature-controlled environment with a 12-h light/dark cycle. All mice received a standard diet and water ad libitum, accordance with the Institutional Animal Care and Use Committee of The Ohio State University and all studies were performed in accordance with national animal protection laws.
-
Preparation
Depends on the number of the mice and the PK time points involved in the PK study, the preparation of the work can be done the day before or on the same day of the PK study. We separated mice with two mice per cage to ensure the easy accessibility and smooth transaction to each team participants during the study. We weighed the mice, numbered the mice on the tail, calculated the drug volume based on the body weight. Label two sets of 0.5 ml sample collection tubes, for blood and serum samples respectively. The mice information, drug injection volume, drug injection and collection time points were summarized in the Table 1. On the day of the PK study, team member performed their assigned duty according to the instruction. Videos 1 and 5 show the layout of the blood collection and process platforms.
Video 1. Blood collection platform.
Download video file (1.2MB, mp4)
-
Drug preparation
Drugs are prepared on the day of PK experiment at room temperature. Dissolve Nilotinib in 0.5% (w/v) HPMC (hydroxypropyl methylcellulose), sonicate to make working suspension at 10 mg/ml within 1 h of administration. Paclitaxel was formulated in Cremophor EL/ethanol (1:1) at 6 mg/ml and diluted in normal saline, vortexed to make 2 mg/ml working solution right before injection.
-
Drug administration
Paclitaxel is given by intra-venous bolus in the tail vein at a dose of 10 mg/kg, 100 mg/kg nilotinib or an equivalent volume of vehicle control (0.5% HPMC) given by oral gavage 30 min before paclitaxel (Table 1).
Administer Nilotinib by oral gavage.
Expose the mouse a few minutes before the scheduled i.v. injection to the red lamp.
Place the mouse in the tail vein injection platform.
Inject the drug intra-venous bolus in the tail vein.
Note: The precise dosing of the drug at the specific time point is critical.
-
Blood collection
As illustrated in Figure 1, we collect blood samples (30 μl each) from individual mice at selected time points: 5, 10, and 15 min from the submandibular vein using a lancet. At 30 and 60 min time points, we anesthetize the mouse using isoflurane, collect blood from the retro-orbital venous plexus using a heparinized capillary. At 120 min, collect blood by cardiac puncture using a syringe and needle.
-
Blood collection by the cheek bleeding (Video 2)
-
Proper restrain mice with one hand, which will apply adequate pressure to the maxillary vein.
Note: This step is critical for the success of the cheek bleeding procedure, avoid holding too tight around the area of ears, which would cause unexpected bleeding from ears or nose and ultimately death of the animal.
-
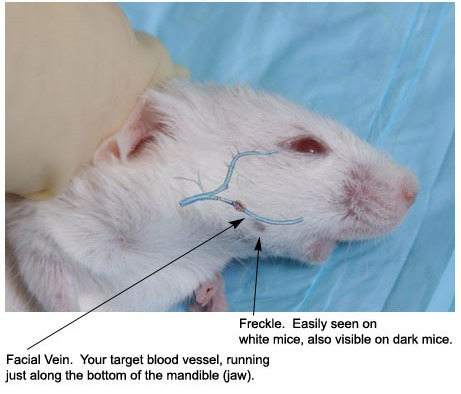
Visualize landmarks. FVB mice have a convenient landmark in the area of the maxillary vein as shown in Figure 2. Often viewed as a small bald spot or hair whorl (freckle), you can find this along the curvature of the mandible; the vein is just above this mark in the groove past the jawbone. Darker mice have the same spot but it may be more difficult to see.
Note: You can also align a lancet caudal to the angle of the mandible, extending to the ear. Location of the puncture site is at the midway point of the lancet.
-
Using the point of a lancet, apply firm pressure at the point, caudal to the eye and ventral to the ear, where the submandibular vein is located, then release until blood flows.
Note: Avoid the jawbone, the puncture will induce bleeding where the retro-orbital and submandibular veins join the jugular vein. In case of puncture of ear canal due to improper technique, apply pressure with gauze until bleeding stops.
-
Collect the blood (30 μl per mouse and time point) with heparinized capillary and transfer into a pre-labeled 0.5 ml microcentrifuge tube using a pipet rubber bulb.
Note: Depends on how many time points you will collect blood from one mice, the volume from each time point could vary, however, the total volume of blood collected has to be allowed by IACUC Guidelines.
Apply gentle pressure with gauze to stop the bleeding. The bleeding will stop in seconds.
Release the mouse that will self-groom.
-
Rotate the side of cheek bleeding for the next time point. For example, we performed the 5 min time point bleeding on the right cheek, the 10 min on the left cheek and the 15 min on the right cheek again.
Note: If symptoms of distress were observed due to restraint or blood loss, release restraint, gently stimulate the mouse until it recovers.
-
-
Blood collection by the retro-orbital venous plexus (Video 3)
Anesthetize the mouse with 3% isoflurane carried in oxygen.
Verify the absence of corneal blink and movement after noxious stimulus prior to the procedure.
Place the mouse on lateral recumbency position and scruff it with thumb and forefinger.
Insert a collection capillary in the medial canthus of the eye under the nictitating membrane, at 30-degree angle to the nose.
Slightly rotate the capillary with a slight pressure to puncture the sinus tissue, and the blood will flow in the capillary.
Withdraw the capillary and apply a clean pad on the eye will stop the bleeding.
Check the eye 30 min after the procedure.
-
Perform the blood collection on the right eye for 30 min time point and then rotate on the left eye for 60 min time point.
Note: Retro-orbital bleeding is relatively safe and easy to perform in PK study, however, mice might be under stress after several serial cheek bleeding, especially within a short time window. In this case, sometimes it would be difficult to obtain blood from retro-orbital bleeding. We found that intraperitoneal injection of 1-2 ml of normal saline would help.
-
Blood collection by cardiac puncture (Video 4)
The cardiac puncture is performed as a terminal procedure.
-
Euthanize the mouse in a CO2 chamber.
Note: Depends on IACUC approval, cardiac puncture could be performed while mice are under anesthesia.
-
After absence of vital sign, immediately perform the posterior cardiac puncture procedure.
Note: It would be very difficult to get blood from cardiac puncture if you wait too long after euthanizing the mice.
Place the mouse on dorsal recumbency position, spray with 70% ethanol.
Insert the needle through the chest wall, under the xiphoid, and puncture the diaphragm. Maintain the needle parallel to the spine, and insert it underneath the ribs.
When the heart is punctured at the level of the elbow, apply back pressure on the syringe. If the needle is in the heart, the syringe will fill up with blood. If not, re-position the needle and try again to back pressure the needle.
-
Add more backpressure once the syringe is filled with blood.
Note: We typically obtain blood as much as we can to ensure the sufficient volume for analytical measurement of the drug. Typically, the drug concentration is the lowest one comparing with all the earlier time points; it is also a good practice to remove as much as blood from circulation to minimize the blood contamination in the tissue if you are also interested in collecting the tissues for further examination.
Transfer blood into a 1.3 ml microtube with heparin, gently invert 2-3 times, allow the heparin released into the blood.
-
-
Blood sample process (Video 5)
Centrifuge blood samples at 1,500 × g for 5 min.
Carefully transfer the translucent yellowish supernatant (plasma) without any carryover of the blood cells into a pre-labeled corresponding time-point tube.
Store plasma samples at -80 °C until analysis.
-
Determination of drug levels
Paclitaxel is quantified by a validated method based on reversed-phase liquid chromatography coupled to tandem mass-spectrometric detection (LC/MS/MS, Leblanc et al., 2018 ).
Table 1. Paclitaxel PK study dosing and sampling information sheet.

Figure 1. Time scheme of drug administration and blood collection.

Video 2. Cheek bleeding.

(This video was made at The Ohio State University according to guidelines from The Ohio State University on Animal Care and Use Committee of The Ohio State University, and approved by the Animal Research Ethics Board of The Ohio State University under protocol #2015A10000101.)
Figure 2. Visualized landmark for mice cheek bleeding.
Video 3. Retro Orbital bleeding.
(This video was made at The Ohio State University according to guidelines from The Ohio State University on Animal Care and Use Committee of The Ohio State University, and approved by the Animal Research Ethics Board of The Ohio State University under protocol #2015A10000101.)
Video 4. Cardiac puncture.

(This video was made at The Ohio State University according to guidelines from The Ohio State University on Animal Care and Use Committee of The Ohio State University, and approved by the Animal Research Ethics Board of The Ohio State University under protocol #2015A10000101).
Video 5. Blood process platform.

Data analysis
Noncompartmental pharmacokinetic parameters (Cmax, Tmax, AUC, clearance, half-life) were calculated using WinNonlin 6.2 software (Pharsight, Leblanc et al., 2018 ). The elimination rate constant (Kel) was estimated from the slope of the terminal phase of the log plasma concentration-time curve fitted by the method of least squares, and the terminal half-life (T1/2) was calculated as 0.693/Kel. The peak plasma concentration (Cmax) and the time to reach peak plasma concentration (Tmax) were obtained by visual inspection of the data from the concentration-time curve. The area under the plasma concentration-time curve (AUC) was calculated according to the linear trapezoidal rule up to the last time point with measurable concentrations of the analyte of interest. Significant differences from the corresponding vehicle control group or baseline mice (P < 0.05) was evaluated with an unpaired 2-sided Student’s t-test with Welch’s correction. Typical plasma concentration-time curve is shown in Figure 3, and pharmacokinetic parameters of paclitaxel (PTX) is shown in Table 2: the area under the curve in plasma for paclitaxel only modestly increased in Oatp1b2 KO mice, and the plasma levels of paclitaxel were not affected by pretreatment with nilotinib.
Figure 3. Plasma concentration-time curves of paclitaxel after paclitaxel administration (10 mg/kg; i.v.) pretreated with nilotinib (100 mg/kg; p.o.) or vehicle (n = 5 per group).

Table 2. Pharmacokinetic parameters of paclitaxel (10 mg/kg) in mice given with or without nilotinib (100 mg/kg).
| Paclitaxel + vehicle | Paclitaxel + nilotinib | ||
| WT | AUCLast (µg·h/ml) | 16.62 ± 4.075 | 16.90 ± 6.434 |
| AUCinf (µg·h/ml) | 22.01 ± 3.939 | 21.61 ± 9.004 | |
| Cmax (µg/ml) | 28.86 ± 7.272 | 32.02 ± 10.71 | |
| CL (L/h/kg) | 0.4662 ± 0.0839 | 0.5271 ± 0.2388 | |
| T1/2 (h) | 1.129 ± 0.253 | 0.985 ± 0.313 | |
| KO | AUCLast (µg·h/ml) | 30.02 ± 9.827 | 28.40 ± 13.73 |
| AUCinf (µg·h/ml) | 49.31 ± 15.48 | 52.53 ± 26.14 | |
| Cmax (µg/ml) | 40.07 ± 15.06 | 44.03 ± 11.88 | |
| CL (L/h/kg) | 0.2293 ± 0.1081 | 0.2650 ± 0.2055 | |
| T1/2 (h) | 1.340 ± 0.143 | 1.857 ± 0.919 |
Abbreviations: AUC, area under the plasma concentration-time curve; Cmax, maximum plasma concentration; CL, systemic clearance; T1/2, half-life of the terminal phase; WT, wild-type; KO, OATP1B2 (-/-).
Notes
Careful planning and thorough preparation of the study are critical for ensuring the smooth completion of the PK study. Two mice per cage is especially important for PK study involving multiple drug dosing, tight bleeding schedule. The time point of PK study is designed based on the individual drug property in certain species. For the drug we studied in this manuscript, paclitaxel, it is eliminated out of body very fast, that’s why we have Time-Concentration curve ended at 2 h. The time/volume of each bleeding as well as total volume of blood is adjusted and approved according to Institution IACUC approval. For drugs with longer half-life, you have to adjust the time and volume of blood withdrawal schedule based on IACUC guideline.
Three minutes interval between each bleeding is adjustable, totally depends on the comfort level of the PK team.
Determination of sample size for each treatment group is largely dependent on individual drug property, experimental variation handed by individual study group. It is typically considered to be using the minimum # of mice to reach the scientific statistical significance. With our experience, 5 mice from each treatment group is the optimal # for most of PK study, including paclitaxel.
The PK study is teamwork, make sure everyone involved in the study is well informed with his/her responsibilities, and well trained and skilled to perform their duties on time.
Document every detail step and have a second person to check the calculation of the drug preparation and procedure.
Recipes
-
0.5% (m/v) HPMC
0.5 g Hydroxypropyl methylcellulose
100 ml Millipore H2O
Acknowledgments
This protocol is adapted from Leblanc et al. (2018). This work was supported by NIH grants R01CA187176. The funding agency had no role in the preparation of the manuscript.
Competing interests
The authors do not have any potential conflicts of interest to declare.
Ethics
All animals were housed and handled in according with the Institutional Animal Care and Use Committee of The Ohio State University, and all studies were performed in accordance with national animal protection laws.
Citation
Readers should cite both the Bio-protocol article and the original research article where this protocol was used.
References
- 1. Berman J., Halm K., Adkison K. and Shaffer J.(1997). Simultaneous pharmacokinetic screening of a mixture of compounds in the dog using API LC/MS/MS analysis for increased throughput. J Med Chem 40(6): 827-829. [DOI] [PubMed] [Google Scholar]
- 2. Korfmacher W. A., Cox K. A., Ng K. J., Veals J., Hsieh Y., Wainhaus S., Broske L., Prelusky D., Nomeir A. and White R. E.(2001). Cassette-accelerated rapid rat screen: a systematic procedure for the dosing and liquid chromatography/atmospheric pressure ionization tandem mass spectrometric analysis of new chemical entities as part of new drug discovery. Rapid Commun Mass Spectrom 15(5): 335-340. [DOI] [PubMed] [Google Scholar]
- 3. Leblanc A. F., Sprowl J. A., Alberti P., Chiorazzi A., Arnold W. D., Gibson A. A., Hong K. W., Pioso M. S., Chen M., Huang K. M., Chodisetty V., Costa O., Florea T., de Bruijn P., Mathijssen R. H., Reinbolt R. E., Lustberg M. B., Sucheston-Campbell L. E., Cavaletti G., Sparreboom A. and Hu S.(2018). OATP1B2 deficiency protects against paclitaxel-induced neurotoxicity. J Clin Invest 128(2): 816-825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Liu B., Chang J., Gordon W. P., Isbell J., Zhou Y. and Tuntland T.(2008). Snapshot PK: a rapid rodent in vivo preclinical screening approach . Drug Discov Today 13(7-8): 360-367. [DOI] [PubMed] [Google Scholar]
- 5. Reddy J., Madishetti S. and Vachaspati P. R.(2012). Fast mouse PK(Fast PK): a rapid screening method to increase pharmacokinetic throughput in pre-clinical drug discovery. Eur J Pharm Sci 47(2): 444-450. [DOI] [PubMed] [Google Scholar]