

Abstract
Introduction:
A multitude of modalities are available for the treatment of chronic rhinosinusitis, however, each has its side effects and compliance issues. Bhramari pranayama, which is a breathing exercise in the practice of yoga, offers an inexpensive and free from side effect modality in this regard.
Objective:
The objective of this study was to evaluate the efficacy of Bhramari pranayama in relieving the symptoms of chronic sinusitis.
Methodology:
A total of 60 patients with chronic sinusitis were randomly divided into two groups, one received conventional treatment of chronic sinusitis and the other group was in addition taught to practice yogic breathing exercise Bhramari pranayama. The patients were advised to practice this breathing exercise twice a day and were followed up at 1, 4, and 12 weeks using the Sino-Nasal Outcome Test (SNOT-22 score).
Results:
The mean SNOT-22 score in the group following the Bhramari pranayama breathing exercise using the ANOVA test improved from 39.13 ± 9.10 to 24.79 ± 8.31 (P = 0.0002), this improvement was seen by the end of 4 weeks itself and continued until the 12th week of assessment.
Conclusion:
Integrating regular practice of Bhramari pranayama along with the conventional management of chronic rhinosinusitis is more effective than conventional management alone.
Keywords: Chronic rhinosinusitis, complementary therapies, nose diseases, paranasal sinus diseases, yoga
Introduction
Chronic rhinosinusitis is a common clinical condition affecting the general population. Changing lifestyles, increased pollution, rapid urbanization, and increase in resistance to antibiotics are responsible for the increased prevalence of upper respiratory tract infections and sinusitis. The reported incidence in developing countries being as high as 12%–15%.[1] Chronic rhinosinusitis not only causes morbidity but also decreases the quality of life resulting in reduced work performance.[2]
The main principle in management is to improve the ventilation and drainage of the sinuses. Although various medical and surgical modalities exist for managing chronic rhinosinusitis, still none have proven to be completely effective. We are still a long way to find the ideal treatment of chronic sinusitis. Initial management includes medications such as antihistaminics, nasal decongestants, and antibiotics such as amoxicillin-clavulanic acid and steroid nasal sprays.[3] All these medications are used in various permutations and combinations. However, all of them have side effects which reduce the compliance and lead to the recurrence of symptoms. The medical treatment for chronic sinusitis is expensive and not free from side effects. Furthermore, the frequent use of antibiotics leads to the development of drug resistance.
Surgery is done for refractory cases but is more often not completely successful in relieving the patient's symptoms and has its own complications.[4]
Nasal irrigation using yogic techniques, such as Jal Neti, have already been proven to be safe and effective adjunct in the management of various clinical conditions in ear-, nose-, and throat (ENT)-like allergic rhinitis.[5] Bhramari pranayama is a yogic breathing technique which relieves anxiety; it is safe and easy to do. The vibrations produced during the humming sound may help in the ventilation and drainage of the sinuses by dislodging the mucous and reducing mucosal edema.[6] The pranayama is to be practiced for 5 min twice daily.
The literature regarding the efficacy of Bhramari pranayama in relieving symptoms of chronic sinusitis is sparse. Therefore, we carried out a study to prove the efficacy of Bhramari pranayama in the management of chronic rhinosinusitis.
Methodology
Subjects
The randomized trial was approved by the Institute Review Board and the Institute Ethics Committee (ICMR-STS/2016/04) and was carried out on 60 patients with chronic rhinosinusitis in the Department of ENT of our institute from August to September 2016. The patients, who were willing for the study, aged above 18 years and had clinical and radiological evidence of chronic sinusitis, were included in the study, the diagnosis of chronic sinusitis was based on the American Academy of Otolaryngology–Head-and-Neck Surgery adult sinusitis guidelines.[7] Patients with nasal polyps, gross septal deviation, nasal tumors, previous nasal surgery, acute sinusitis, and patients who smoke were excluded from the study.
After obtaining ethical committee clearance and informed consent, the selected patients underwent thorough history taking and clinical examination which was recorded in the pro forma. The patients underwent a nasal endoscopic examination and preoperative computed tomography (CT) scan for assessing the severity of the sinusitis. The Lund-Mackay scoring system was used for assessing the severity on the CT scan. These patients were then randomized by the investigator using computer-generated random numbers into two study groups. Group A had 30 patients and received conventional medical treatment for chronic rhinosinusitis which included fluticasone propionate steroid nasal spray and saline nasal irrigations for 14–21 days where indicated.
Group B having 30 patients received the same conventional treatment and were taught Bhramari pranayama in the yoga outpatient department and were asked to practice it daily.
Bhramari pranayama
Bhramari pranayama derives its name from the black Indian bee called Bhramari and pranayama meaning breathing technique. The exercise is performed by sitting comfortably in a calm place with the eyes closed. The patient is asked to place his thumb in the ear canal or on tragal cartilage to gently block the ear canal. The index finger is placed over the eyebrow, and the rest of the fingers are used to close the eyes. The patient is then asked to take a deep breath and exhale slowly through his nose making a loud humming sound and focusing his attention on the areas between the eyebrows. The process is repeated 5 times/session. The patient is taught the pranayama and asked to perform the pranayama in front of the investigator. The patients were advised to practice the pranayama twice daily for 15 min each. The compliance was monitored by the principal investigator by telephonic conversation.
Outcomes
Outcomes were recorded and evaluated pre- and post-procedure using the Sino-Nasal Outcome Test score (SNOT-22) at 1, 4, and 12 weeks' interval by a blinded investigator to reduce the bias. The results were analyzed at the end of the study by another blinded investigator.
Statistics
All quantitative variables were estimated using measurements of central location (i.e., mean and median) and measurements of dispersion (i.e., standard deviation).
The SNOT-22 scores were analyzed using the paired t-test and independent t-test and one-way ANOVA test. The Chi-square test was used for comparisons of the gender distribution of the groups. P < 0.05 was considered as statistically significant.
Results
A total of 30 patients were taken in each group, however, two patients in Group A and one patient in Group B were lost to follow-up; therefore, the sample size in Group A became 28 and in Group B became 29. One patient in Group A shifted to another city, and we could not follow him up. The other two patients, one from Group A and other from Group B were not reachable on the phone; hence, we lost them to follow-up.
Patient population
No statistically significant differences were found between groups regarding age (32.6 ± 8.2 and 33.1 ± 11.6, respectively) and gender (13 females and 15 males, 15 females and 14 males, respectively) (P = 0.08 and P = 0.09, respectively). A summary of the patient demographics is given in Table 1. There was no difference in the preintervention Lund-Mackay CT scan scores between the groups (7.4 ± 2.7 and 7.8 ± 2.2) (P = 0.651).
Table 1.
Patient characteristics in the conventional treatment group (Group A) and the Bhramari pranayama group (Group B)
| Group A (n=28) | Group B (n=29) | Statistical difference (P) | |
|---|---|---|---|
| Average age (SD) | 32.64 (8.22) | 33.31 (11.68) | 0.08 |
| Female (%) | 13 (46.43) | 15 (51.72) | 0.09 |
| Male (%) | 15 (53.57) | 14 (48.28) |
SD=Standard deviation
Sino-Nasal Outcome Test-22 scores
The mean baseline SNOT-22 score in Group A was 37.89 ± 10.8, and Group B was 39.13 ± 9.10. There was no statistical difference between the baseline scores of both the groups (P = 0.313) [Table 2].
Table 2.
Comparison of the Sino-Nasal Outcome Test-22 scores at baseline, 1, 4 and 12 weeks of both the groups
| Mean (SD) |
P | ||
|---|---|---|---|
| Group A | Group B | ||
| Baseline SNOT score | 37.89±10.08 | 39.13±9.10 | 0.313 |
| SNOT score at 1 week | 34.39±10.08 | 35.68±8.41 | 0.29 |
| SNOT score at 4 weeks | 32.07±7.90 | 29.79 (8.59 | 0.151 |
| SNOT score at 12 weeks | 28.21±7.73 | 24.79±8.31 | 0.019 |
| P | 0.003 | 0.0002 | |
SD=Standard deviation, SNOT=Sino-Nasal Outcome Test
There was a statistically significant reduction in the SNOT-22 scores in both the groups. In Group A, the SNOT-22 score reduced from 37.89 ± 10.08 to 28.21 ± 7.73 (P = 0.004). In Group B, the SNOT-22 score reduced from 39.13 ± 9.10 to 24.79 ± 8.31 (P = 0.0002). The distribution of the SNOT-22 scores and the statistical analysis in both the groups over the study period is given in Figure 1 and Table 2, respectively.
Figure 1.
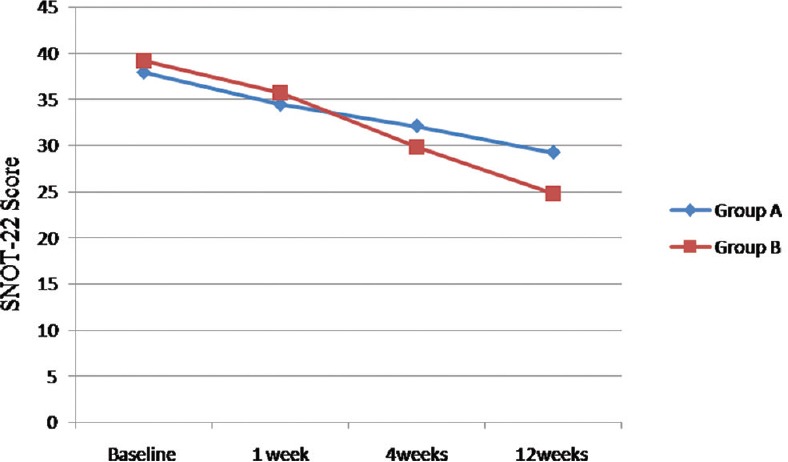
Distribution of the Sino-Nasal Outcome Test-22 scores in both the groups over the study period
The analysis of the SNOT-22 scores in both the groups at 1st, 4th, and 12th weeks was done. It was seen that there was no difference between the SNOT scores at 1st and 4th weeks, however, there was a significant difference in the SNOT scores at the 12th week (P = 0.021) [Table 2].
We also analyzed the individual SNOT-22 scores in Group B (yoga group) at 1st, 4th, and 12th weeks and compared them with baseline SNOT scores using the paired t-test. We found that there was a statistically significant improvement in the scores by the 4th week (P = 0.00008) and it continued until the 12th week (P < 0.00001) [Table 3].
Table 3.
Comparison of the baseline Sino-Nasal Outcome Test-22 scores and at 1st, 4th and 12th weeks of Group B
| Mean (SD) |
P | |
|---|---|---|
| SNOT score at baseline | SNOT score | |
| 39.13±9.10 | 1st week=35.68±8.41 | 0.069 |
| 4th week=29.79±8.59 | 0.00008 | |
| 12th week=24.79±8.31 | <0.00001 | |
SD=Standard deviation, SNOT=Sino-Nasal Outcome Test
Discussion
A variety of medications, such as nasal sprays, nasal decongestants, and oral steroids, are available for the treatment of chronic rhinosinusitis be completely effective.[8,9,10,11] Besides this, most medications have side effects, and there is a problem of development of antibiotic resistance. The search for an ideal treatment for chronic sinusitis is far from over, and in recent years, a variety of ancillary treatments for the management of chronic sinusitis have been described.
The most commonly used and scientifically proved ancillary treatment is hypertonic saline irrigation. Rudmik et al.,[12] in an evidence-based review, have recommended the use of hypertonic saline in chronic sinusitis. A study by Heatley et al.,[13] in the University of Wisconsin, has shown that daily nasal irrigation using a bulb syringe, nasal irrigation pot, and daily reflexology massage were equally efficacious and resulted in improvement in the symptoms of chronic sinusitis in over 70% of subjects. Medication usage was decreased in approximately one-third of the participants regardless of intervention.
Kosugi et al.[14] evaluated the efficacy of high-volume budesonide nasal irrigations and found them to be effective and well tolerated in the management of chronic sinusitis.
Yoga, the ancient healing art of India, has recently become popular as a therapeutic adjuvant to modern scientific medicine. Pranayama is an ancient Indian practice concerned with controlling one's breathing. Research has shown that it can relieve symptoms diseases such as anxiety and depression and has a number of benefits such as improving blood circulation, improves concentration, and increasing the quality of life. One such technique is the Bhramari pranayama (the humming bee breath).
There are several mechanism by which humming is supposed to relieve the symptoms of sinusitis. The first mechanism as described by Eby[15] is that humming acts as a sonic cleanser. Humming creates sound vibrations that encourage air to move back and forth between the sinuses and nasal passage. This air movement helps open the blocked ostia of the sinuses, allowing the sinuses to ventilate and drain properly. This mechanism also helps to prevent microbes and allergens from settling down in the sinuses and creates a healthy environment within them. The second mechanism is by increasing the nitric oxide levels. It has been proven that humming increases the endogenous generation of nitric oxide level by 15-fold as compared with the quiet exhalation.[16] Nitric oxide is a vasodilator and can regulate the filling of nasal capacitance vessels which in turn improves the nasal mucosal temperature and humidification, resulting in more effective air conditioning of the sinuses and respiratory passage. This, in turn, improves the ciliary movement and results in better drainage of the nose and paranasal sinuses. A third mechanism by which Bhramari pranayama may be useful is by reducing anxiety and other psychological symptoms, which are often seen in patients with chronic sinusitis. The regular practice of yoga has been proven to be effective in reducing anxiety and depression and improving the quality of life.
Our study found a definite and statistically significant improvement in the symptom score of patient's practicing bhramari pranayama, and this significance was seen as early as in 2 weeks (P < 0.05) of starting the pranayama and continued until the end of 4 weeks (P < 0.00001). The reduction in the SNOT-22 scores is significant not only statistically but also in accordance with the minimal clinically important difference for SNOT score which is 9.[17]
The strength of the present study is the randomized design and blind data collection and assessment. The small sample size and short follow-up of the patients limited the study power. Lack of a tool to assess compliance for performing the pranayama is another limitation of the study. There also another limitation that the conventional medical therapy was not entirely standardized and was tailored to each patient, although all patients had a common core usage of topical fluticasone propionate nasal sprays. Another improvement in the study design would be the use of other scoring tools such as the chronic sinusitis survey score, the short form 36 score, Lund-Kennedy endoscopic score, etc., to assess the patients in both the arms; the use of these standard tools can add more scientific evidence to the study.
Conclusion
In this study, we conclude that Bhramari pranayama is an effective complementary modality in the treatment of chronic sinusitis. Bhramari pranayama helps by ventilating the sinuses by its mechanical cleaning and anti-inflammatory effects. Such practices of yoga are inexpensive, without side effects, and can improve the symptoms in patients with chronic sinusitis.
Financial support and sponsorship
Partial funding was obtained from Indian Council of Medical Research, India.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Halawi AM, Smith SS, Chandra RK. Chronic rhinosinusitis: Epidemiology and cost. Allergy Asthma Proc. 2013;34:328–34. doi: 10.2500/aap.2013.34.3675. [DOI] [PubMed] [Google Scholar]
- 2.Marambaia PP, Lima MG, Santos KP, Gomes Ade M, de Sousa MM, Marques ME, et al. Evaluation of the quality of life of patients with chronic rhinosinusitis by means of the SNOT-22 questionnaire. Braz J Otorhinolaryngol. 2013;79:54–8. doi: 10.5935/1808-8694.20130010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rudmik L, Soler ZM. Medical therapies for adult chronic sinusitis: A Systematic review. JAMA. 2015;314:926–39. doi: 10.1001/jama.2015.7544. [DOI] [PubMed] [Google Scholar]
- 4.Mascarenhas JG, da Fonseca VM, Chen VG, Itamoto CH, Silva CA, Gregório LC, et al. Long-term outcomes of endoscopic sinus surgery for chronic rhinosinusitis with and without nasal polyps. Braz J Otorhinolaryngol. 2013;79:306–11. doi: 10.5935/1808-8694.20130055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Barham HP, Harvey RJ. Nasal saline irrigation: Therapeutic or homeopathic. Braz J Otorhinolaryngol. 2015;81:457–8. doi: 10.1016/j.bjorl.2015.07.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bauman A. Sinusitis survival: Vibrations created from chanting Om can help clear your sinuses and ward off infections. Yoga J. 2003;3:34. [Google Scholar]
- 7.Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, Brook I, Ashok Kumar K, Kramper M, et al. Clinical practice guideline (update): Adult sinusitis. Otolaryngol Head Neck Surg. 2015;152:S1–39. doi: 10.1177/0194599815572097. [DOI] [PubMed] [Google Scholar]
- 8.DeConde AS, Soler ZM. Chronic rhinosinusitis: Epidemiology and burden of disease. Am J Rhinol Allergy. 2016;30:134–9. doi: 10.2500/ajra.2016.30.4297. [DOI] [PubMed] [Google Scholar]
- 9.Bhattacharyya N. Functional limitations and workdays lost associated with chronic rhinosinusitis and allergic rhinitis. Am J Rhinol Allergy. 2012;26:120–2. doi: 10.2500/ajra.2012.26.3752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kennedy JL, Borish L. Chronic rhinosinusitis and antibiotics: The good, the bad, and the ugly. Am J Rhinol Allergy. 2013;27:467–72. doi: 10.2500/ajra.2013.27.3960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ocak E, Acar B, Kocaöz D. Medical adherence to intranasal corticosteroids in adult patients. Braz J Otorhinolaryngol. 2016:pii: S1808-8694 (16) 30136-7. doi: 10.1016/j.bjorl.2016.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rudmik L, Hoy M, Schlosser RJ, Harvey RJ, Welch KC, Lund V, et al. Topical therapies in the management of chronic rhinosinusitis: An evidence-based review with recommendations. Int Forum Allergy Rhinol. 2013;3:281–98. doi: 10.1002/alr.21096. [DOI] [PubMed] [Google Scholar]
- 13.Heatley DG, McConnell KE, Kille TL, Leverson GE. Nasal irrigation for the alleviation of sinonasal symptoms. Otolaryngol Head Neck Surg. 2001;125:44–8. doi: 10.1067/mhn.2001.115909. [DOI] [PubMed] [Google Scholar]
- 14.Kosugi EM, Moussalem GF, Simões JC, Souza Rde P, Chen VG, Saraceni Neto P, et al. Topical therapy with high-volume budesonide nasal irrigations in difficult-to-treat chronic rhinosinusitis. Braz J Otorhinolaryngol. 2016;82:191–7. doi: 10.1016/j.bjorl.2015.03.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Eby GA. Strong humming for one hour daily to terminate chronic rhinosinusitis in four days: A case report and hypothesis for action by stimulation of endogenous nasal nitric oxide production. Med Hypotheses. 2006;66:851–4. doi: 10.1016/j.mehy.2005.11.035. [DOI] [PubMed] [Google Scholar]
- 16.Maniscalo M. Humming, nitric oxide and paranasal sinuses ventilation. Eur Respir J. 2003;22:3239. [Google Scholar]
- 17.Hopkins C, Gillett S, Slack R, Lund VJ, Browne JP. Psychometric validity of the 22-item sinonasal outcome test. Clin Otolaryngol. 2009;34:447–54. doi: 10.1111/j.1749-4486.2009.01995.x. [DOI] [PubMed] [Google Scholar]