

Abstract
Context:
HIV/AIDS individuals have problems relating to immune system, quality of life (QOL), and cognitive functions (CFs). Yoga is found to be useful in similar conditions. Hardly, any work is reported on yoga for HIV-positive adults/adolescents. Hence, this study is important.
Aim:
The aim of the study is to determine the effect of yoga on immune parameters, CFs, and QOL of HIV-positive children/adolescents.
Settings and Design:
Single-group, pre–post study with 4-month yoga intervention.
Methods:
The study had 18 children from an HIV/AIDS rehabilitation center for children/adolescents. CD4, CD8, CD4/CD8 ratio, and viral loads were studied. CF tests included six letter cancellation test, symbol digit modalities test, digit-span forward backward test, and Stroop tests. QOL was assessed using PedsQL-QOL and fatigue questionnaire. Depression was assessed using CDI2-SR.
Statistical Analysis Used:
t-test and Wilcoxon signed-rank tests, as applicable.
Results:
The study included 18 children/adolescents. There was improvement in general health of the participants. There was statistically significant increase in CD4 cells counts (p = 0.039) and significant decrease in viral load (p = 0.041). CD4/CD8 ratio moved to normal range. QOL significantly improved. CFs had mixed results with improved psychomotor performance (PP) and reduced executive functions.
Conclusions:
There was improvement in general health and immune parameters. While depression increased, QOL improved. CFs showed mixed results with improved PP and reduced executive functions.
Keywords: Children/adolescents, HIV/AIDS, immune system, quality of life, yoga
Introduction
HIV/AIDS still remains to be one of the challenging and prevailing diseases of the modern times. The HIV/AIDS individuals have issues with general health owing to poor immune system leading to several opportunistic infections. The quality of life (QOL) is also rated to be poor among HIV/AIDS adults[1] and is attributed to reasons such as stigma, depression, and cultural beliefs.[2,3] Depression and cognitive disorders are also a prevalent comorbid mental disorders in HIV positives.[4,5,6,7] Depression is reported in up to 45% of HIV/AIDS patients.[8] Bhargav et al.[9] have reported that yoga could promote the health of HIV-infected mothers, enhance the efficacy of antiretroviral therapy (ART) in preventing vertical progression of HIV (mother-to-child transmission of HIV), and help reduce ART-related side effects. The mechanisms of action explained in the report also indicate that yoga would help any HIV-positive individual in general. Other reports also show that yoga helps in improving immune system functioning.[10] Bhargav et al.[11] describe the importance and mechanism of working of yoga on HIV-positive individuals and also recommend a theoretical comprehensive yoga module for HIV positives. However, they do not provide any empirical evidence. In spite of the clue that yoga can improve immune functioning, not many studies are reported on immune parameters in specific owing to the cost of blood tests.[12] A pilot randomized controlled trial study reports that 1-month yoga intervention showed improvement in CD4 count and depression among adult age group.[13] Yet, another single-group pre–post study has shown improvement in immunity, depression, and anxiety management of HIV adults.[14] Yoga has shown improvement in cognitive functions (CFs) of normal school children.[15] Yoga, in general, is known to also helpful in alleviating depression and improving QOL in several diseased conditions.[13] However, there are hardly any reports on the effect of yoga on children/adolescents with HIV. The current study is an attempt to determine the effect of yoga practice on the immune system, CFs, and QOL of HIV-positive children/adolescents.
Methods
This study is a part of larger study to determine the effect of yoga on the immune system, CFs, and QOL of HIV-positive children/adolescents. The design is a single-group pre–post study conducted on HIV-positive children/adolescents in an HIV/AIDS rehabilitation center (RC). The RC had 22 children/adolescents, both males and females, at the time of the start of the study. Although all 22 were included in the study, for CF tests where the ability to read English was inevitable, only such of those having the appropriate abilities had to be considered. Further, for answering questionnaires, assistance was provided to the participants in the local language by research volunteers. Four participants had left the RC at the time of final data collection, and hence, the net number of participants were 18. The RC had voluntarily provided consent for the study.
The yoga intervention largely based on a potential yoga module for HIV-positive individuals[11] included 1-h daily practice primarily involving loosening and breathing exercises, āsanas (Sūryanamaskāra - six rounds, Padmāsana, Vajrāsana, Varvāṇgāsana, Bhujangāsana, Ardhakati Ćakrásana, Uśtrāsana, Ardha Ćakrásana, Paśćimottanāsana, and Shavāsana) and prāṇāyāma (Kapālabāti (Kriya), Bhāstrika, Nāḍiśodhana, and Brāmari). Yoga was taught by a professional yoga teacher. Duration of intervention was 6 months. The daily routine of the participants was not disturbed, except for one hour yoga. Routine medical care too was not disturbed, and all the participants continued the standard medical care and checkups as per norms/schedules. All the participants were under the first-line ART routine as part of the standard medical care.
For the study of immune parameters, health status, and related issues, the data were collected from the medical files proactively maintained by the RC as per norms. CD4 and CD3 counts and viral load were available. CD8 counts were computed using the formula CD8 = CD3 − CD4, and the CD4/CD8 ratio was calculated. Health-related QOL (HRQOL) was assessed with the help of PedsQL QOL questionnaire which has four subscales, namely, (a) health and general activities, (b) feelings, (c) getting along with others, and (d) about school. Fatigue-related QOL (FRQOL) was assessed through the PedsQL fatigue questionnaire which has three subscales (a) general fatigue (b) sleep fatigue, and (c) cognitive fatigue. The depression level of the candidates was assessed through self-reported child depression inventory, version 2 (CDI2-SR) questionnaire. The CFs were assessed through digit-span forward-backward (DSFB) test, symbol digit modalities test (SDMT), six letter cancellation test (SLCT), and Stroop test (ST). While SLCT and SDMT test for the psychomotor performance (PP), DSFB and ST test the executive functioning (EF) aspect of CF. Standard test procedures were used for the assessment in all tests. The statistical programming language R3.5.0 (with appropriate add-on packages) was used, and suitable codes were written for statistical computations and for graphical representation of data. t-test and Wilcoxon signed-rank test (WSRT) were used for determining the differences in the parameters for data with normal distribution and not with normal distribution, respectively.
Results
Sociodemographic data
The participants included 18 children/adolescents of age between 8 and 18 years. The mean age was 13.5 ± 2.46 years (mean ± standard deviation). Of 18 participants, 14 were males and 4 were female.
General health
At the beginning of the study, the participants had several opportunistic infections and health issues, namely, skin infection, eye, and ear problems, all of which were significantly reduced at the time of final data collection. These general health conditions are as reported by the physician during routine medical checkup.
Immune parameters
The mean CD4 cell counts significantly increased from 571.1 ± 238.0 cells/mm3 before yoga to 717.4 ± 241.7 cells/mm3 after yoga (p = 0.039), with typically the values at the baseline being in tune with that reported by an earlier study.[9] The average CD8 cell counts decreased from 1389.18 ± 572.88 cells/mm3 before yoga to 1338.82 ± 471.12 cells/mm3 after yoga, which was not statistically significant (p = 0.477, WSRT). Mean CD4/CD8 ratio increased from 0.814 to 1.016 although the median difference between pre- and post-values was not statistically significant (p = 0.091; WSRT). The average viral load significantly reduced from 55487.5 ± 56996.4 copies/mL before yoga to 5755.4 ± 6539.3 copies/mL after yoga (p = 0.041; WSRT). Table 1 shows the summary of the immune parameters along with the general medical issues. Figures 1 and 2 show the distribution of CD4 and viral load, respectively, along with the change in the parameters case to case between pre- and post-yoga.
Table 1.
General health of participants along and immune parameters
| ID | General medical issues |
CD4 |
CD4/CD8 |
Viral load |
||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | Pre | Post | |
| A01 | Swelling below ears | Reduced | 346 | 600↑ | 0.23 | 0.49↑ | 77455 | 310↓ |
| A03 | NA | NA | 356 | 952↑ | 0.20 | 0.57↑ | 145662 | 4188↓ |
| A04 | Skin infection | Nil | 712 | 777↑ | 0.81 | 0.88↑ | 5676 | 7029↑ |
| A05 | Blood from nose | Nil | 543 | 439↓ | 0.29 | 0.30↑ | 18008 | 310↓ |
| A06 | Liquid discharge from ear | Reduced | 403 | 397↓ | 0.45 | 0.39↓ | 126009 | 15468↓ |
| A12 | Skin infection, stomach pain, and tiredness | Nil | 624 | 753↑ | 0.71 | 0.68↑ | 2567 | 9153↑ |
| A13 | Skin infection | Reduced | 348 | 710↑ | 0.12 | 0.28↑ | 137511 | 310↓ |
| A14 | Tiredness due | Nil | 829 | 1081↑ | 0.74 | 1.01↑ | 304 | 7234↑ |
| A15 | Chest pain, mesenteric lymphadenitis, and skin infection | Nil | 317 | 364↑ | 0.24 | 0.33↑ | 50461 | 310↓ |
| A16 | Eye infection | Reduced | 997 | 911↓ | 0.69 | 0.54↓ | 10121 | 18687↑ |
| A22 | Skin infection and blood from nose | Nil | 807 | 907↑ | 0.81 | 0.83↑ | 36589 | 310↓ |
↑=Increased compared to pre, ↓=Decreased compared to pre, NA=Not available
Figure 1.
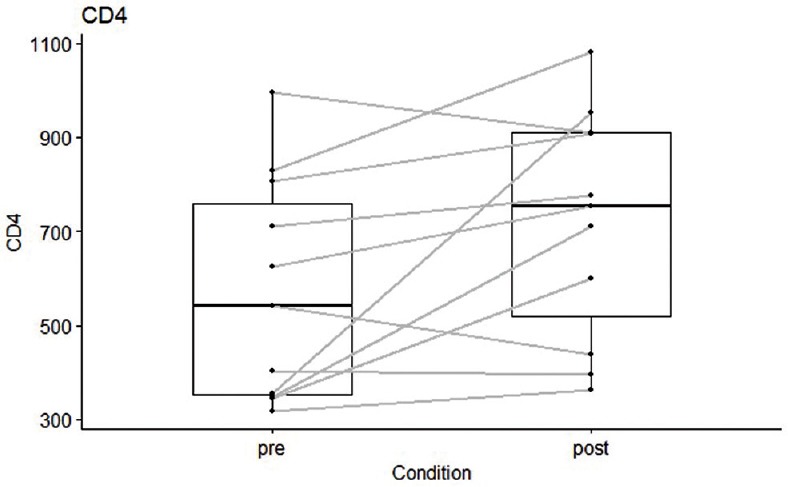
Change in CD4 cell counts between pre and post yoga intervention
Figure 2.
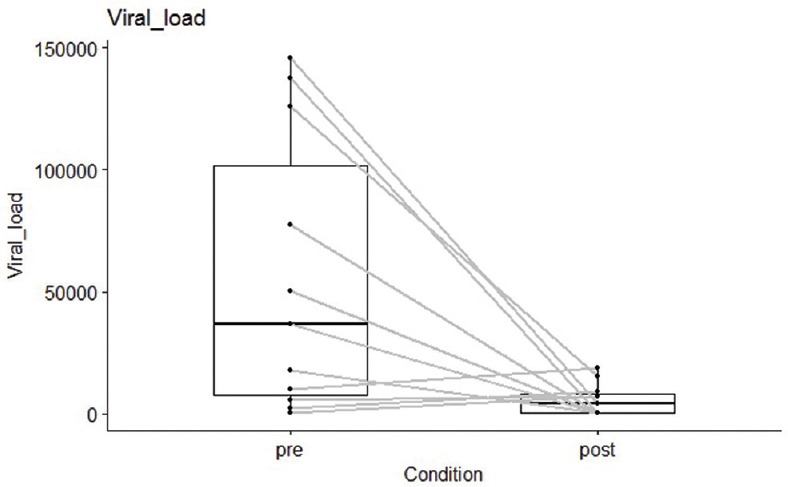
Change in viral load between pre and post yoga intervention
Quality-of-life parameters
The HRQOL had an average pre score of 1439.7 ± 346.22 and an average post score of 1677.1 ± 280.57 which was statistically significant (p = 0.013). All the four subscales indicated improvement in the post scores when compared to the pre scores. Of the four subscales, physical functioning subscale score had statistical significance (p = 0.004). Emotional, social, and school functioning scores showed only improvement but no statistical significance (p = 0.068, 0.123, and 0.212, respectively). The FRQOL of the participants showed significant improvement, with an average of 1024.3 ± 331.87 before yoga and 1208.9 ± 344.13 after yoga (p = 0.033). All the three subscales showed an increase in average fatigue QOL scores, which means that the fatigue levels reduced. Of the three subscales, while general fatigue and cognitive fatigue scales indicated no statistical significance (p = 0.203 and 0.136, respectively), sleep fatigue scores indicated statistical significance (p = 0.022). Table 2 shows the summary of HRQOL and FRQOL results.
Table 2.
Summary of quality-of-life results
| Pre |
Post |
P | |||
|---|---|---|---|---|---|
| Count | Mean±SD | Count | Mean±SD | ||
| HRQOL | |||||
| Physical_functioning_score | 18 | 482.9±166.04 | 18 | 595.8↑±96.35 | 0.004** |
| Emotional_functioning_score | 18 | 295.1±84.36 | 18 | 337.5↑±79.64 | 0.068 |
| Social_functioning_score | 18 | 363.2±87.08 | 18 | 406.3↑±81.6 | 0.123 |
| School_functioning_score | 18 | 298.4±74.79 | 18 | 337.5↑±111.56 | 0.212 |
| Score_psysoc | 18 | 956.8±201.23 | 18 | 1081.3↑±211.97 | 0.04* |
| Total_HRQOL_score | 18 | 1439.7±346.22 | 18 | 1677.1↑±280.57 | 0.013* |
| FRQOL | |||||
| General fatigue | 18 | 417.4±108.05 | 18 | 458.3↑±105.37 | 0.203 |
| School fatigue score | 18 | 301.4±125.87 | 18 | 392.2↑±137.68 | 0.022* |
| Cognitive fatigue | 18 | 305.6±155.13 | 18 | 358.3↑±150.24 | 0.136 |
| Total_FRQOL_score | 18 | 1024.3±331.87 | 18 | 1208.9↑±344.13 | 0.033* |
*p<0.05, **p < 0.01, ↑=Increased compared to pre, ↓=Decreased compared to pre, HRQOL=Health-related quality of life, FRQOL=Fatigue-related quality of life, SD=Standard deviation
The CDI2-SR-T scores were calculated as per the guidelines are given in the CDI-SR user manual.[16] Results revealed that the average of the total CDI-T-scores significantly increased from 55.7 ± 8.42 before yoga to 61.1 ± 10.33 after yoga (p = 0.029). Similarly, all the subscales and the sub-subscales showed increase in the average T-scores. This means that the depression has increased. CDI2-SR classifies depression status into four categories, (1) very elevated, (2) elevated, (3) high average, and (4) average or lower.[16] Although there is an increase in the depression of the children, it has only moved from higher range of lower depression state (lower depression range = 40–59) to lower range of high depression range (high depression range = 60–64). Both raw scores and T-scores indicated similar performance. Table 3 shows the summary of the results of various CDI parameters.
Table 3.
Results of child depression inventory subscales and sub-subscales
| CDI parameter |
Pre |
Post |
P |
||
|---|---|---|---|---|---|
| Count |
Mean±SD |
Count |
Mean±SD |
||
| Raw scores | |||||
| CDI-raw-Total | 18 | 10.7±4.98 | 18 | 14.8↑±6.63 | 0.015* |
| CDI-raw-EP | 18 | 5.7±2.43 | 18 | 7.7↑±3.74 | 0.039* |
| CDI-raw-NMPS | 18 | 5.1±2.07 | 18 | 5.2↑±2.85 | 0.887 |
| CDI-raw-NSE | 18 | 0.6±1.14 | 18 | 2.6↑±1.62 | 0*** |
| CDI-raw-FP | 18 | 5.1±3.59 | 18 | 7.1↑±3.67 | 0.082 |
| CDI-raw-INE | 18 | 3.2±2.29 | 18 | 4.9↑±2.55 | 0.032* |
| CDI-raw-IP | 18 | 1.8±1.73 | 18 | 2.1↑±1.97 | 0.571 |
| T-scores | |||||
| CDI-T-Total | 18 | 55.7±8.42 | 18 | 61.1↑±10.33 | 0.029* |
| CDI-T-EP | 18 | 56.1±6.66 | 18 | 61.4↑±9.77 | 0.041* |
| CDI-T-NMPS | 18 | 57.3±15.11 | 18 | 61.2↑±11.3 | 0.203 |
| CDI-T-NSE | 18 | 46.8±6.43 | 18 | 58.2↑±9.22 | 0*** |
| CDI-T-FP | 18 | 54.4±11.14 | 18 | 56.4↑±16.44 | 0.631 |
| CDI-T-INE | 18 | 51.3±8.78 | 18 | 57.3↑±10.2 | 0.041* |
| CDI-T-IP | 18 | 57.2±14.97 | 18 | 59.5↑±15.97 | 0.632 |
*p<0.05, **p < 0.01, ***p < 0.001, ↑=Increased compared to pre, ↓=Decreased compared to pre, CDI=Child depression inventory, EP=Emotional problem, FP=Functional problem, NMPS=Negative mood physical symptoms, NSE=Negative self-esteem, INE=Ineffectiveness, IP=Interpersonal, SD=Standard deviation
Cognitive functions
The results of the CF tests are summarized in Table 4. It might be noted that the number of participants in each of the test differs due to English reading ability, especially for ST. Another reason is that some children did not want to take some tests.
Table 4.
Results of cognitive tests
| Pre |
Post |
P (t-test) | |||
|---|---|---|---|---|---|
| Count | Mean±SD | Count | Mean±SD | ||
| DSF | 13 | 7.2±1.77 | 13 | 6↓±2.27 | 0.059 |
| DSB | 13 | 1.8±1.46 | 13 | 4.1↑±3.2 | 0.009* |
| DSFB | 13 | 9±2.89 | 13 | 10.1↑±4.35 | 0.266 |
| Stroop_WS | 9 | 40.9±23.18 | 9 | 55.3↑±33.42 | 0.051 |
| Stroop_CS | 9 | 33.1±7.15 | 9 | 37.1↑±19.17 | 0.574 |
| Stroop_CWS | 9 | 25.4±8.79 | 9 | 21↓±11.92 | 0.458 |
| SDMT | 15 | 20.1±10.91 | 16 | 43.3↑±12.21 | 0*** |
| SLCT | 15 | 23.4±11.54 | 17 | 27.6↑±10.81 | 0.01** |
*p<0.05, **p < 0.01, ***p < 0.001, ↑=Increased compared to pre, ↓=Decreased compared to pre, DSF=Digit-span forward, DSB=Digit-span backward, DSFB=Digit-span forward backward, Stroop_WS=Stroop Word score, Stroop_CS=Stroop Color score, Stroop_CWS=Stroop Color-Word score, SDMT=Symbol Digit Modalities Test, SLCT=Six letter cancellation test, SD=Standard deviation
The average DSFB total score had no statistically significant improvement (p = 0.266). A split-up of the score indicated that DSF score decreased with no statistical significance (p = 0.059) and the DSB score had a statistically significant increase (p = 0.009). There was improvement in average Stroop Word score and Stroop Color score although not statistically significant. The average Stroop Color-Word score decreased but not statistically significant (p = 0.458). There was statistically significant increase in the scores of SDMT (p = 0) and SLCT (p = 0.01).
Discussion
There has been a significant improvement in the general health condition of the participants, as reported by the physicians during their routine checkup. Skin infection in the participants is either reduced or nullified in all the participants. For want of control group in the study, the improvement cannot be attributed purely to yoga intervention. However, sūryanamaskāra, kapālabāti (Kriya), bhāstrika, and nāḍiśodhana prānāyāma in the yoga intervention are known to be excellent practices for participants having skin diseases.[17] Hence, yoga could have played a role in improving the status.
The major point that was demonstrated through this study is that there was improvement in the immune parameters. The CD4 cells are the major marker for HIV/AIDS increased by 36.63% which is also statistically significant. Further, at the baseline, the counts were well matching with the ones reported in one of the earlier studies. The CD4/CD8 ratio improved by 42.05%. The normal CD4/CD8 ratio is 1–4[18] and the average ratio shifted from a lower value (0.814) to normal (1.016), also indicating improvement in the immune system. This is further supported by the decrease in the viral load by an average of 178.5%. Figure 3 shows the relationship between changes in viral load against changes in CD4. It can be observed that in most the cases where there is a massive drop in the viral load, they are characterized by large increase in the CD4 cell counts.
Figure 3.
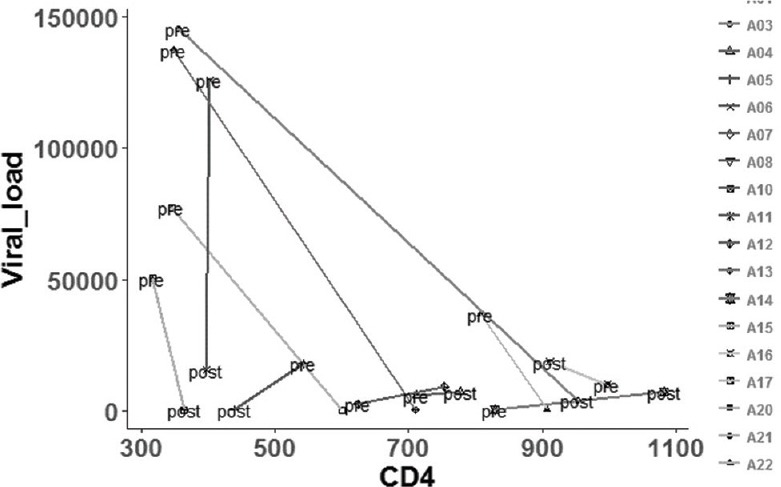
Case-wise relation between viral load and CD4 cell counts, pre and post yoga intervention
The case-to-case observation indicated that yoga greatly helped those participants whose viral loads were very high. It can be noted that participants with a viral load >18,000 cells/mm3 showed a more significant decrease in viral load (p = 0.018, WSRT). Considering such cases, the CD4 counts and CD4/CD8 ratio cell count increased although not significantly (p = 0.128 and p = 0.063, WSRT). Overall, it can be noted that yoga has helped candidates even with high levels of viral loads. Perhaps, yoga seems to have an attribute of addressing the crucial problems first by prioritizing. Although in this study, the changes in immune parameters cannot be completely attributed to yoga program since this study does not have a control group; another 1-month yoga intervention study reports that there is a significant increase in CD4 cell counts among adults against the control group.[13] Thus, this study shows that yoga can help to HIV positives in increasing the CD4 cells and reducing the viral load in children/adolescents. However, there was no change in ART status recommended by the physicians.
In the current study, there was mixed response to CFs. SLCT showed improvement in the result. Normative data for SLCT on healthy school children indicate a mean score of 24.04, for the age group of 9–16 years.[19] In the current study, the mean scores were 23.4 and 27.6 before and after yoga, respectively. Thus, at the baseline, the scores were lesser than that of normal and improved to normal after yoga. Similarly, SDMT also showed significant improvement (p~0). DSFB test which is a test for EF showed a nonsignificant improvement. Stroop tasks which also require good working memory and is a test of EF[20] also showed show improvement but not significant. Thus, in the current study, CFs pertaining PP showed significant improvement while that of EF did not. With reference to DSFB test while the participants showed improvement in DSB, there was difficulty with DSF test. Supporting this phenomenon, another study on large group of children with specific learning disabilities also showed similar results which are attributed to more requirement of working memory in DSF than in DSB.[20] It is also known that depression has a negative impact on working memory,[21] thus resulting in poor executive function. Incidentally, in the current study, the participants' depression level also showed an increase. Overall, the current study could not improve EFs of the participants owing to depression which also could not be improved.
There was an overall significant improvement in the QOL although not statistically significant in all the subscales. The physical functioning score had good significance since yoga is known to improve the flexibility of the body. The fatigue factors assessed through the PedsQL fatigue questionnaire also showed improvement. Of the three subscales, sleep/rest fatigue showed significant improvement. However, although not statistically significant, there was improvement in general fatigue and cognitive fatigue subscales. Improvement in sleep/rest fatigue state is an important aspect since HIV-positive individuals are known to have issues in sleep.[6]
CDI total score had increased significantly (p < 0.05). The total score comprises emotional problem (EP) and the functional problem (FP). Of these, the increase in EP is statistically significant (p = 0.039), and FP is not statistically significant (p = 0.082). EP has two components, negative mood physical symptoms (NMPSs) and negative self-esteem (NSE). Of these, NMPS is not statistically significant (p = 0.887>>0.05), whereas NSE has a high statistical significance (p~0). Thus, the participants have statistically significant NSE. Looking into the components of NSE in the questionnaire, it can be understood that there is a need to address the issues such as “things not working out well with” (Q.2r [question 2; r indicating reverse scoring]), “blaming themselves for the faults that happen” (Q.7r), and “sometimes being disgusted” (Q.8). However, for the participants, “liking themselves” (Q.6r) was not an issue although they had an issue about “somebody else loving them” (Q.24r). This means that in the current study, yoga could not address these issues but largely physical issues.
Similarly, FP has two sub components ineffectiveness (INE) and interpersonal (IP). The IP has no statistical significance (p = 0.571). However, with INE, there is a statistically significant increase (p = 0.032). A detailed analysis of the INE reveals through the component questionnaire that there are issues with “making up mind to do things” (Q.12r), “having fun at school” (Q.20r), and “feeling good relative to others” (Q.23). It can also be noted that the participants on an average that they do have any issues with “having fun” (Q.4) in general (although not at school), “to make time to do school-related things” (Q.14r, Q.22), and “remembering things” (Q.28). Although the EF tests indicated poor working memory, CDI is not sensitive to tap the difference between different types of memories. However, this also explains the improvement in other CFs which require memory. The component on issues related to going to school has been positive in spite of it being a component of INE which had overall negative effect. This is further supported by the improvement in the school functioning subscale of PedsQL QOL questionnaire. Overall, the yoga program needs to be improved to address psychosocial issues, which can be improved with the addition of yogic games which help children involve better with others and proper counseling.
Conclusions
In the current study, the six months yoga program could significantly improve the immune parameters of the HIV-positive children/adolescents. CD4 and viral load significantly improved, with CD4 cells increasing and viral load reducing. CD4/CD8 ratio moved to a normal range. Yoga could also improve the QOL of the children/adolescents. In an overall sense, yoga could not improve, in the current study, the depression of the children/adolescents. However, several sub components of the depression showed improvement or were not affected. With reference to CFs, PP improved while executive functions did not improve owing to depression among the participants. The major issue is with mentally preparing the children/adolescents to think more positively about themselves. Improvement in the yoga program by introducing yogic games, more of prānāyāmas, and the introduction of counseling could improve the situation.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank research volunteers who participated in data collection.
References
- 1.Kumar A, Girish H, Nawaz A, Balu P, Kumar B. Determinants of quality of life among people living with HIV/AIDS: A cross sectional study in central Karnataka, India. Int J Med Sci Public Health. 2014;3:1413. [Google Scholar]
- 2.Holzemer WL, Human S, Arudo J, Rosa ME, Hamilton MJ, Corless I, et al. Exploring HIV stigma and quality of life for persons living with HIV infection. J Assoc Nurses AIDS Care. 2009;20:161–8. doi: 10.1016/j.jana.2009.02.002. [DOI] [PubMed] [Google Scholar]
- 3.Aranda-Naranjo B. Quality of life in the HIV-positive patient: Implications and consequences. J Assoc Nurses AIDS Care. 2004;15:20S–27S. doi: 10.1177/1055329004269183. [DOI] [PubMed] [Google Scholar]
- 4.Masiello A, De Guglielmo C, Giglio S, Acone N. Beyond depression: Assessing personality disorders, alexithymia and socio-emotional alienation in patients with HIV infection. Infez Med. 2014;22:193–9. [PubMed] [Google Scholar]
- 5.Goldberg RE, Short SE. What do we know about children living with HIV-infected or AIDS-ill adults in sub-saharan africa? A systematic review of the literature. AIDS Care. 2016;28(Suppl 2):130–41. doi: 10.1080/09540121.2016.1176684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Chaponda M, Aldhouse N, Kroes M, Wild L, Robinson C, Smith A, et al. Systematic review of the prevalence of psychiatric illness and sleep disturbance as co-morbidities of HIV infection in the UK. Int J STD AIDS. 2018;29:704–13. doi: 10.1177/0956462417750708. [DOI] [PubMed] [Google Scholar]
- 7.Nichols SL, Montepiedra G, Farley JJ, Sirois PA, Malee K, Kammerer B, et al. Cognitive, academic, and behavioral correlates of medication adherence in children and adolescents with perinatally acquired HIV infection. J Dev Behav Pediatr. 2012;33:298–308. doi: 10.1097/DBP.0b013e31824bef47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tymchuk S, Gomez D, Koenig N, Gill MJ, Fujiwara E, Power C, et al. Associations between depressive symptomatology and neurocognitive impairment in HIV/AIDS. Can J Psychiatry. 2018;63:329–36. doi: 10.1177/0706743717737029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bhargav H, Huilgol V, Metri K, Sundell IB, Tripathi S, Ramagouda N, et al. Evidence for extended age dependent maternal immunity in infected children: Mother to child transmission of HIV infection and potential interventions including sulfatides of the human fetal adnexa and complementary or alternative medicines. J Stem Cells. 2012;7:127–53. [PubMed] [Google Scholar]
- 10.Falkenberg RI, Eising C, Peters ML. Yoga and immune system functioning: A systematic review of randomized controlled trials. J Behav Med. 2018;41:467–82. doi: 10.1007/s10865-018-9914-y. [DOI] [PubMed] [Google Scholar]
- 11.Bhargav H, Raghuram N, Rao NH, Tekur P, Koka PS. Potential yoga modules for treatment of hematopoietic inhibition in HIV-1 infection. J Stem Cells. 2010;5:129–48. [PubMed] [Google Scholar]
- 12.Field T. Yoga clinical research review. Complement Ther Clin Pract. 2011;17:1–8. doi: 10.1016/j.ctcp.2010.09.007. [DOI] [PubMed] [Google Scholar]
- 13.Naoroibam R, Metri KG, Bhargav H, Nagaratna R, Nagendra HR. Effect of integrated yoga (IY) on psychological states and CD4 counts of HIV-1 infected patients: A randomized controlled pilot study. Int J Yoga. 2016;9:57–61. doi: 10.4103/0973-6131.171723. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Koar WH. Meditation, T-cells, anxiety, depression and HIV infection. Subtle Energies Energy Med J Arch. 1995;6:89–97. [Google Scholar]
- 15.Telles S, Singh N, Bhardwaj AK, Kumar A, Balkrishna A. Effect of yoga or physical exercise on physical, cognitive and emotional measures in children: A randomized controlled trial. Child Adolesc Psychiatry Ment Health. 2013;7:37. doi: 10.1186/1753-2000-7-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kovacs M. (CDI 2) Technical Manual. 2nd ed. Multi-Health Systems Inc.; 2012. Children's Depression Inventory. [Google Scholar]
- 17.Mayer A. Yoga for Skin Diseases. Mysore. 2014. [Last accessed on 2018 Jul 10]. Available from: https://www.yogaindea.wordpress.com/2014/01/14/yoga-for-skin-diseases/
- 18.Bosire EM, Nyamache AK, Gicheru MM, Khamadi SA, Lihana RW, Okoth V, et al. Population specific reference ranges of CD3, CD4 and CD8 lymphocyte subsets among healthy Kenyans. AIDS Res Ther. 2013;10:24. doi: 10.1186/1742-6405-10-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Pradhan B, Nagendra HR. Normative data for the letter-cancellation task in school children. Int J Yoga. 2008;1:72–5. doi: 10.4103/0973-6131.43544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Giofrè D, Stoppa E, Ferioli P, Pezzuti L, Cornoldi C. Forward and backward digit span difficulties in children with specific learning disorder. J Clin Exp Neuropsychol. 2016;38:478–86. doi: 10.1080/13803395.2015.1125454. [DOI] [PubMed] [Google Scholar]
- 21.Christopher G, MacDonald J. The impact of clinical depression on working memory. Cogn Neuropsychiatry. 2005;10:379–99. doi: 10.1080/13546800444000128. [DOI] [PubMed] [Google Scholar]