

Abstract
Background
Acute necrotizing encephalopathy (ANE) is a rare, but potentially life threatening neurological condition in children. This study aimed to investigate its clinical spectrum, diagnostic and therapeutic dilemma, and prognosis.
Methods
Twelve children with ANE were included in the study. The diagnosis was made by clinical and radiological characteristics from January 1999 to December 2017 and their clinical data were retrospectively analyzed.
Results
A total of 12 children aged 6 to 93 months at onset (5 male: 7 female) were evaluated. The etiology was found in 4 of them (influenza A, H1N1; coxsackie A 16; herpes simplex virus; and RANBP2 gene/mycoplasma). The most common initial presentations were seizures (67%) and altered mental status (58%). The majority of the subjects showed elevation of aspartate aminotransferase/alanine aminotransferase with normal ammonia and increased cerebrospinal fluid protein without pleocytosis. Magnetic resonance imaging revealed increased T2 signal density in bilateral thalami in all patients, but the majority of the subjects (67%) also had lesions in other areas including tegmentum and white matter. Despite the aggressive immunomodulatory treatments, the long-term outcome was variable. One child and two sisters with genetic predisposition passed away.
Conclusion
ANE is a distinctive type of acute encephalopathy with diverse clinical spectrum. Even though the diagnostic criteria are available, they might not be watertight. In addition, treatment options are still limited. Further studies for better outcome are needed.
Keywords: Encephalopathy, Children, RAN Binding Protein 2
Graphical Abstract
INTRODUCTION
Acute necrotizing encephalopathy (ANE) is a rare, acute encephalopathy characterized by seizures or alteration of consciousness with multiple symmetrical lesions of the thalami and brain stem tegmentum and other areas after various viral illnesses. The condition was first proposed by Mizuguchi et al.1 in 1995 and was initially believed to occur in children, predominantly in countries such as Japan, Korea, Taiwan, and etc.2,3 However, a number of cases were later reported in western countries including adults, suggesting that ethnic propensity is less likely to be present.4,5,6,7,8,9 Over time, recurrent or familial forms of ANE (ANE1) were reported and the missense mutations in the gene encoding the nuclear pore protein called RAN binding protein 2 (RANBP2) were found.10,11,12,13,14,15 This unique condition is becoming more familiar, but the pathogenesis and guidelines for diagnosis and treatment remain unresolved. The aim of this study was to evaluate its various clinical spectrum, therapeutic dilemma, and prognosis.
METHODS
A total of 12 children who were admitted at Kyungpook National University Children's Hospital from January 1999 to December 2017 were included in the study and their data regarding clinical characteristics, laboratory findings, radiological features, treatment modalities and outcome were retrospectively evaluated.
The subjects consisted of 5 boys and 7 girls, aged 6 months to 93 months at onset. Based on diagnostic criteria for ANE, proposed by Mizuguch et al.1 and Neilson11 the diagnosis was made by clinico-radiological characteristics and laboratory results. Along with complete blood count (CBC) and routine blood chemistry, liver function tests, ammonia, blood glucose, polymerase chain reaction (PCR)/multiplex PCR for viruses or mycoplasma were done at the time of admission. Lumbar puncture was done within a day after hospitalization depending on the patient's clinical condition. Initial and follow-up magnetic resonance imaging (MRI) was performed on each of the subjects. The mean interval between the onset of ANE and initial MRI, and that of follow-up MRI was 2.1 days and 39.6 days respectively. Various MR pulse sequences with different orientations were obtained. However, axial T1-weighted images, axial and coronal T2-weighted images, fluid-attenuated inversion recovery (FLAIR) images, and axial and coronal contrast enhanced T1-weighted images were available for 11 out of 12 subjects. Diffusion weighted images were available in 2 of them. Computed tomography (CT) scan was done in a girl who came in with unconsciousness (case 12).
To elucidate the genetic propensity or find out other clinically plausible host factors, genomic typing of human leukocyte antigen (HLA) using PCR-sequence-specific oligonucleotide probes/sequence specific primers technique with gel immune-electrophoresis was done in 3 children, mitochondrial DNA studies were screened in 6 children and direct sequencing and next generation sequencing of entire coding regions of RANBP2 gene were conducted for a child and her parents suspicious of having ANE1.
With respect to treatment, dexamethasone or methylprednisolone was given as initial treatment in all of the subjects and IV immunoglobulin (IVIG) was added depending on the patient's condition. Dexamethasone was given 1 mg/kg/day in 4 divided doses for 5 days, methylprednisolone was given 30 mg/kg/day for 5 days and IVIG was administered 1 g/kg/day for 2 days or 0.4 g/kg/day for 5 days.
Ethics statement
This study was approved by Internal Review Board of Kyungpook National University Hospital, Ethical Committee (2019-01-021) and the informed consents for all the genetic tests were taken from the legal guardians.
RESULTS
A total of 12 children aged 6 months to 93 months at onset (male:female, 5:7) were evaluated. They all had normal developmental milestones. The condition was preceded by febrile viral illnesses in all children. Besides fever, prodromal symptoms included signs of upper respiratory infections and gastroenteritis, and various skin lesions due to different viral infections. During the acute phase, the most common neurological presentations were seizures (67%) and change of mental status (58%) (Table 1). Furthermore, three of them (25%) presented with impending shock. The majority of the subjects showed elevation of serum aminotransferases and 2 of the subjects (17%) presented with fulminant hepatitis. However, blood ammonia remained normal or borderline. In addition, two out of 12 children revealed laboratory findings indicative of disseminated intravascular coagulation without clinical signs. Abnormal variations in plasma glucose levels occurred in 5 of them (42%). Even though it was mild, cerebrospinal fluid (CSF) pleocytosis was present in one of them and CSF protein was elevated in 4 of them (33%), which may suggest blood brain barrier breakdown (Table 2).
Table 1. Demographic and clinical characteristics of the subjects with ANE.
| No. | Age, mon | Sex | Preceding illness | Clinical presentation | Involvement site |
|---|---|---|---|---|---|
| 1 | 19 | M | URI | stupor/stiffness | TT |
| 2 | 68 | M | NSFI | drowsiness/ataxia | TT |
| 3 | 88 | M | URI | stupor/seizure | TT |
| 4 | 93 | F | NSFI | diplopia | P, TT, CL |
| 5 | 40 | F | NSFI | stupor/seizure | P, T |
| 6 | 73 | F | NSFI | stupor/seizure | TT, CL (Hm) |
| 7 | 50 | M | HFMD | stupor | P, T |
| 8 | 6 | M | flu | seizure | T, P, WM |
| 9 | 39 | F | HFMD | seizure | TT, CL, WM (Hm) |
| 10 | 53 | F | NSFI | seizure | TT, WM, CL |
| 11a | 13 | F | NSFI | stupor/seizure | TT, MB, CL, WM. (Hm) |
| 12b | 25 | F | NSFI | seizure | T |
ANE = acute necrotizing encephalopathy, M = male, F = female, URI = upper respiratory infection, NSFI = nonspecific febrile illness, HFMD = hand foot mouth disease, TT = thalmotegmental, P = putamen, CL = cerebellum, Hm = hemorrhage, WM = white matter, MB = mammillary body, T = thalamus.
aProband of familial ANE; bElder sister of proband.
Table 2. Laboratory findings of the subjects with ANE.
| No. | AST/ALT, U/L | Ammonia, µ/dL | Glucose, mg/dL | CSF | ||
|---|---|---|---|---|---|---|
| Cell count, µL | Protein, mg/dL | Glucose, mg/dL | ||||
| 1 | 114/42 | 32 | 85 | 0 | 39 | 76 |
| 2 | 34/15 | 24 | 85 | 66 | 40 | 61 |
| 3 | 7,725/2,910 | 56 | 108 | 0 | 46 | 61 |
| 4 | 26/9 | 14 | 145 | 0 | 29 | 83 |
| 5 | 7,000/4,354 | 48 | 96 | 0 | 30 | 65 |
| 6 | 128/44 | 24 | 135 | 0 | 43 | 90 |
| 7 | 21/12 | 35 | 85 | 0 | 25 | 69 |
| 8 | 43/28 | 51 | 110 | 0 | 143 | 81 |
| 9 | 759/315 | 35 | 197 | 0 | 22 | 112 |
| 10 | 123/52 | 24 | 87 | 0 | 75 | 50 |
| 11a | 43/15 | 62 | 175 | 0 | 270 | 63 |
| 12b | 60/22 | 78 | 282 | 0 | 110 | 65 |
ANE = acute necrotizing encephalopathy, AST/ALT = aspartate aminotransferase/alanine aminotransferase, CSF = cerebrospinal fluid.
aProband of familial ANE; bElder sister of proband.
Various magnetic resonance (MR) images showed increased T2 signal density in bilateral thalami in all patients, but the majority of them (67%) had lesions in tegmentum, putamen of basal ganglia, periventricular white matter, cerebellar medulla, mammillary bodies, and so on (Table 1). Patients who took the apparent diffusion coefficient (ADC) imaging and diffusion weighted imaging (DWI) showed typical tricolor pattern in thalamic lesions and two cases with poor prognosis (17%) showed diffuse cerebral atrophy on follow-up MR images (Fig. 1).
Fig. 1. Radiological findings in a child with ANE. (A) The ADC imaging shows typical tricolor pattern in thalamic lesions: hemorrhage and necrosis in the center, cytotoxic edema in the middle and vasogenic edema in the outermost part. (B, C) DWI and T2 weighted MRI shows multifocal, fairly symmetric lesions involving bilateral thalami and periventricular white matter. (D, E) Follow-up ADC and DWI imaging reveals disappearance of swelling with hemosiderin deposition in thalami (E, F) T2 weighted imaging shows mild, but diffuse cerebral atrophy with incomplete resolution of previous lesions.

ANE = acute necrotizing encephalopathy, ADC = apparent diffusion coefficient, DWI = diffusion weighted imaging, MRI = magnetic resonance imaging.
Environmental and host factors for etiology were investigated. The triggering factors were found in 4 of them (33%), which include influenza A, H1N1; coxsackie A 16, herpes simplex virus, and mycoplasma. One child clinically had hand foot mouth disease (HFMD), but viral PCR was not done in this case. With respect to host factors, HLA-DRB1*1401, HLA-DRB3*0202, HLA-DQB1*0502 appear to be significant when known allele frequencies and haplotypic associations in Korean are considered (Table 3). Based on characteristic MRI findings and family history, we performed next generation sequencing (NGS) followed by direct sequencing for RANBP2-specific cDNA which revealed a heterozygous mutation in the gene (c.1754C>T: p.Thr585Met) in a girl (case 11) and her father (Fig. 2).
Table 3. Etiology of the subjects with ANE.
| No. | Provocative factor | Genetic factor | Mt DNA mutation |
|---|---|---|---|
| 1 | (−) | ND | (−) |
| 2 | (−) | DRB1 1101 1401 | ND |
| DRB3 0202 | |||
| DQB1 0301 0502 | |||
| 3 | (−) | ND | ND |
| 4 | (−) | ND | (−) |
| 5 | (−) | DRB1 0701 1401 | ND |
| DRB3 0202 | |||
| DQB1 0303 0502 | |||
| 6 | (−) | DRB1 0101 1302 | ND |
| DRB3 0301 | |||
| DQB1 0501 0609 | |||
| 7 | HFMD | ND | (−) |
| 8 | H1N1 | ND | ND |
| 9 | Coxsackie virus A16 | ND | (−) |
| 10 | (−) | ND | (−) |
| 11a | Mycoplasma | RANBP2 (+) | (−) |
| 12b | HSV | ND | ND |
ANE = acute necrotizing encephalopathy, HFMD = hand foot mouth disease, HSV = herpes simplex virus, ND = not done, RANBP2 = RAN binding protein 2.
aProband of familial ANE; bElder sister of proband.
Fig. 2. Sanger sequencing for RANBP2-specific cDNA shows c.1754C>T mutation in the proband (case 11) and her father, but not in her mother.

RANBP2 = RAN binding protein 2.
With respect to treatment, steroids have been used in all of the subjects. IVIG was additionally given in 4 of them (33%). The long-term outcome was variable. Only one patient (8%) showed excellent outcome without any neurological sequelae. Three of them (25%) had greater than 75% resolution on follow-up MRI and they were able to walk alone with almost no cognitive difficulties. Another 3 children (25%) showed 50%–75% resolution on follow-up MRI, but they had some difficulties with ambulation and cognition. Two out of 12 children (17%) ended up with severe neurological sequelae with poor radiological resolution and three children (25%) passed away despite the intensive treatment (Table 4).
Table 4. Treatment and their neurological outcome in the subjects with ANE.
| Patient No. | Treatment | Follow-up MRI | Long-term outcome |
|---|---|---|---|
| 1 | DEX | 50%–75% resolution | Fair |
| 2 | MPS pulse | > 75% resolution | Good |
| 3 | DEX | ND | Expired |
| 4 | MPS pulse | Complete resolution | Excellent |
| 5 | DEX | 50%–75% resolution | Fair |
| 6 | MPS pulse | < 50% resolution | Poor |
| 7 | MPS pulse | > 75% resolution | Good |
| 8 | MPS pulse/IVIG | 50%–75% resolution | Fair |
| 9 | MPS pulse | < 50% resolution | Poor |
| 10 | MPS pulse/IVIG | 50%–75% resolution | Good |
| 11a | MPS pulse/IVIG | ND | Expired |
| 12b | MPS pulse/IVIG | ND | Expired |
ANE = acute necrotizing encephalopathy, DEX = dexamethasone, MPS = methylprednisolone, IVIG = intravenous immunoglobulin, MRI = magnetic resonance image, ND = not done.
aProband of familial ANE; bElder sister of proband.
DISCUSSION
ANE is a rare, but unique and devastating neurological condition, mainly occurring in children. The purpose of this study is to investigate its clinical spectrum, diagnostic and therapeutic dilemma, and prognosis. Even though two reliable diagnostic criteria are available,1,11 they are mainly based on clinical and radiological features and might not be perfect. Furthermore, treatment options are still limited. We therefore inquired into its spectrum closely and tried to fill in the blanks.
As we know, ANE was first proposed as a new neurological disease in children by Mizuguchi et al.1 in 1995. As time passed on, we came to know that the condition can occur globally, at all ages, and can be recurrent or familial.6,12,16,17,18,19 With our limited experiences, ANE looks very diverse in many aspects.
It is not surprising that prodromal symptoms were diversiform due to various virus infections in this study. In addition, three of them presented with systemic inflammatory response syndrome like shock and multiple organ failure.
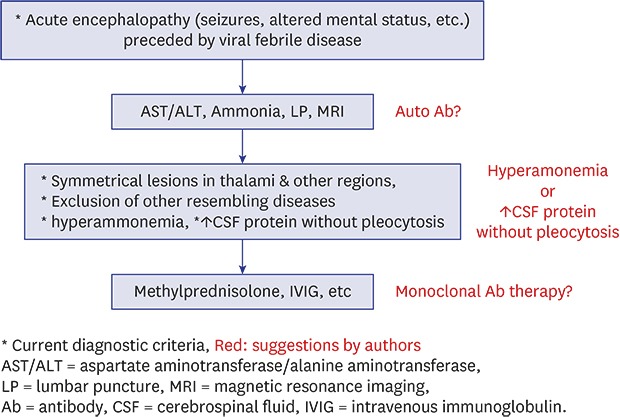
The radiological hallmark of ANE is multiple symmetric lesions involving thalami, tegmentum of upper brainstem and other regions. In this study, all of the subjects showed increased T2 signal density in bilateral thalami and the majority of them had lesions in the tegmentum of midbrain and pons, putamen of basal ganglia, periventricular white matter, cerebellar medulla, mammillary bodies, and so on. Children who took ADC imaging and DWI showed typical tricolor pattern in thalamic lesions. Based on the result, it seems that thalamic lesions can be pathognomonic for ANE. With respect to laboratory findings, four out of 12 cases (33%) showed borderline or mild elevation of ammonia with a variable degree of serum aminotransferase and a child showed mild pleocytosis without increased protein of CSF, which might be against the diagnostic criteria. However, they had characteristic radiological findings for ANE. We therefore propose that the current diagnostic criteria be revised on the base of major or minor clinical features.1,11 For example, major criteria include acute encephalopathy preceded by viral febrile disease, neuroradiologic findings for symmetrical brain lesions involving bilateral thalami and other regions, and exclusion of resembling other diseases. Minor criteria include increased cerebrospinal protein without pleocytosis and elevation of serum aminotransferase level to a variable degree without hyperammonemia. We think that each minor criteria might not be as important as the major criteria. It cannot be specific for ANE and just be a reactive process of any acute illness. There are also interpersonal variations in laboratory values. We therefore propose that a patient with three major criteria and any two minor criteria can be diagnosed with ANE.
ANE seems to develop secondary to a variety of different viruses including influenza virus and human herpesvirus 6.19,20,21,22,23,24,25 Etiologic agents in this study include novel influenza A (H1N1), Coxsackie virus A16, Mycoplasma pneumoniae, and herpes simplex virus (Table 3).
To this day, the etiology and the pathogenesis of ANE remain unclear. Aberrant immune responses on individual HLA genotypes may contribute to ANE. HLA-DRB1*1401, HLA-DRB3*0202, HLA-DQB1*0502 appear to be significant in our study, which might not be in accord with those of a Japanese study.26 However, further studies are needed to elucidate it due to very small sample size. One of our patients was a girl who presented with lethargy and flurries of seizures, which turned out to be familial ANE (case 11). Her elder sister (case 12) passed away from the same condition two months prior to her admission. We undertook NGS followed by direct sequencing of entire coding regions of RANBP2-specific cDNA which revealed a heterozygous mutation in the gene (c.1754C>T: p.Thr585Met) in her and her father, but not in her mother. This was the first case in Northeast Asia. It was postulated that hypercytokinemia or cytokine storm results in systemic response such as hepatic dysfunction or shock in ANE.23,27,28 There is an interesting study that ephrin type B receptor 2, expressed by human brain microvascular endothelial cells can be a target of autoantibody in a patient with ANE from systemic lupus erythematosus.29 Even though major antibodies have not yet been identified, we believe that ANE might be a spectrum of autoimmune neurological diseases. Because they have predilection sites in the brain and they can respond to immunotherapy. If we can find clinically plausible autoantibodies, diagnostic and therapeutic modalities will certainly be changed.
Even though various immunomodulatory treatments are available, the overall long-term outcome appears bad. Despite the relatively early and intensive treatment, about two-thirds of the subjects became disabled or passed away in our study. Results of this study correspond well with those of earlier studies.28,30,31,32 If ANE is a spectrum of autoimmune neurological diseases or any autoantibodies are found, as we mentioned earlier, monoclonal antibody therapy can be an alternative option in the near future.
This study has a limitation stemming from retrospective analysis and its small sample size.
In conclusion, ANE is a rare, but devastating neurological condition with various presentations. We think the pathogenesis and guidelines for diagnosis and treatment remain partially resolved. The discovery of neuronal autoantibodies may lead to a paradigm shift in diagnostic and therapeutic approach. However, many challenges remain.
Footnotes
Disclosure: The authors have no potential conflicts of interest to disclose.
- Conceptualization: Kwon S.
- Data curation: Lee YJ, Hwang SK.
- Formal analysis: Lee YJ, Hwang SK.
- Validation: Lee YJ, Hwang SK.
- Writing - original draft: Kwon S.
- Writing - review & editing: Lee YJ, Hwang SK.
References
- 1.Mizuguchi M, Abe J, Mikkaichi K, Noma S, Yoshida K, Yamanaka T, et al. Acute necrotising encephalopathy of childhood: a new syndrome presenting with multifocal, symmetric brain lesions. J Neurol Neurosurg Psychiatry. 1995;58(5):555–561. doi: 10.1136/jnnp.58.5.555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mizuguchi M. Acute necrotizing encephalopathy of childhood: a novel form of acute encephalopathy prevalent in Japan and Taiwan. Brain Dev. 1997;19(2):81–92. doi: 10.1016/s0387-7604(96)00063-0. [DOI] [PubMed] [Google Scholar]
- 3.Wang HS. Reports of acute encephalopathy with bilateral thalamotegmental involvement. AJNR Am J Neuroradiol. 1996;17(2):398–399. [PMC free article] [PubMed] [Google Scholar]
- 4.Aydin H, Ozgul E, Agildere AM. Acute necrotizing encephalopathy secondary to diphtheria, tetanus toxoid and whole-cell pertussis vaccination: diffusion-weighted imaging and proton MR spectroscopy findings. Pediatr Radiol. 2010;40(7):1281–1284. doi: 10.1007/s00247-009-1498-9. [DOI] [PubMed] [Google Scholar]
- 5.Komur M, Okuyaz C, Arslankoylu AE, Kara E, Atici A. Acute necrotizing encephalopathy associated with novel influenza A (H1N1) virus in Turkey. J Pak Med Assoc. 2011;61(12):1237–1239. [PubMed] [Google Scholar]
- 6.Lyon JB, Remigio C, Milligan T, Deline C. Acute necrotizing encephalopathy in a child with H1N1 influenza infection. Pediatr Radiol. 2010;40(2):200–205. doi: 10.1007/s00247-009-1487-z. [DOI] [PubMed] [Google Scholar]
- 7.Mariotti P, Iorio R, Frisullo G, Plantone D, Colantonio R, Tartaglione T, et al. Acute necrotizing encephalopathy during novel influenza A (H1N1) virus infection. Ann Neurol. 2010;68(1):111–114. doi: 10.1002/ana.21996. [DOI] [PubMed] [Google Scholar]
- 8.Mastroyianni SD, Gionnis D, Voudris K, Skardoutsou A, Mizuguchi M. Acute necrotizing encephalopathy of childhood in non-Asian patients: report of three cases and literature review. J Child Neurol. 2006;21(10):872–879. doi: 10.1177/08830738060210101401. [DOI] [PubMed] [Google Scholar]
- 9.Yildizdaş D, Kendirli T, Arslanköylü AE, Horoz OO, Incecik F, Ince E, et al. Neurological complications of pandemic influenza (H1N1) in children. Eur J Pediatr. 2011;170(6):779–788. doi: 10.1007/s00431-010-1352-y. [DOI] [PubMed] [Google Scholar]
- 10.Gika AD, Rich P, Gupta S, Neilson DE, Clarke A. Recurrent acute necrotizing encephalopathy following influenza A in a genetically predisposed family. Dev Med Child Neurol. 2010;52(1):99–102. doi: 10.1111/j.1469-8749.2009.03405.x. [DOI] [PubMed] [Google Scholar]
- 11.Neilson DE. The interplay of infection and genetics in acute necrotizing encephalopathy. Curr Opin Pediatr. 2010;22(6):751–757. doi: 10.1097/MOP.0b013e3283402bfe. [DOI] [PubMed] [Google Scholar]
- 12.Singh RR, Sedani S, Lim M, Wassmer E, Absoud M. RANBP2 mutation and acute necrotizing encephalopathy: 2 cases and a literature review of the expanding clinico-radiological phenotype. Eur J Paediatr Neurol. 2015;19(2):106–113. doi: 10.1016/j.ejpn.2014.11.010. [DOI] [PubMed] [Google Scholar]
- 13.Sondhi V, Chakrabarty B, Kumar A, Kohli S, Saxena R, Verma IC, et al. RANBP2 mutation in an Indian child with recurrent acute necrotizing encephalopathy. Brain Dev. 2016;38(10):937–942. doi: 10.1016/j.braindev.2016.05.007. [DOI] [PubMed] [Google Scholar]
- 14.Wolf K, Schmitt-Mechelke T, Kollias S, Curt A. Acute necrotizing encephalopathy (ANE1): rare autosomal-dominant disorder presenting as acute transverse myelitis. J Neurol. 2013;260(6):1545–1553. doi: 10.1007/s00415-012-6825-7. [DOI] [PubMed] [Google Scholar]
- 15.Lee YJ, Hwang SK, Lee SM, Kwon S. Familial acute necrotizing encephalopathy with RANBP2 mutation: the first report in Northeast Asia. Brain Dev. 2017;39(7):625–628. doi: 10.1016/j.braindev.2017.02.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Martin A, Reade EP. Acute necrotizing encephalopathy progressing to brain death in a pediatric patient with novel influenza A (H1N1) infection. Clin Infect Dis. 2010;50(8):e50–2. doi: 10.1086/651501. [DOI] [PubMed] [Google Scholar]
- 17.Neilson DE, Adams MD, Orr CM, Schelling DK, Eiben RM, Kerr DS, et al. Infection-triggered familial or recurrent cases of acute necrotizing encephalopathy caused by mutations in a component of the nuclear pore, RANBP2. Am J Hum Genet. 2009;84(1):44–51. doi: 10.1016/j.ajhg.2008.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Denier C, Balu L, Husson B, Nasser G, Burglen L, Rodriguez D, et al. Familial acute necrotizing encephalopathy due to mutation in the RANBP2 gene. J Neurol Sci. 2014;345(1-2):236–238. doi: 10.1016/j.jns.2014.07.025. [DOI] [PubMed] [Google Scholar]
- 19.Ochi N, Takahashi K, Yamane H, Takigawa N. Acute necrotizing encephalopathy in an adult with influenza A infection. Ther Clin Risk Manag. 2018;14:753–756. doi: 10.2147/TCRM.S160111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mungaomklang A, Chomcheoy J, Wacharapluesadee S, Joyjinda Y, Jittmittraphap A, Rodpan A, et al. Influenza virus-associated fatal acute necrotizing encephalopathy: role of nonpermissive viral infection? Clin Med Insights Case Rep. 2016;9:99–102. doi: 10.4137/CCRep.S40610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Okumura A, Abe S, Kidokoro H, Mizuguchi M. Acute necrotizing encephalopathy: a comparison between influenza and non-influenza cases. Microbiol Immunol. 2009;53(5):277–280. doi: 10.1111/j.1348-0421.2009.00124.x. [DOI] [PubMed] [Google Scholar]
- 22.Samanta D. Influenza B-associated acute necrotizing encephalopathy of childhood: a report from North America. Acta Neurol Belg. 2016;116(3):383–385. doi: 10.1007/s13760-015-0573-2. [DOI] [PubMed] [Google Scholar]
- 23.Tabarki B, Thabet F, Al Shafi S, Al Adwani N, Chehab M, Al Shahwan S. Acute necrotizing encephalopathy associated with enterovirus infection. Brain Dev. 2013;35(5):454–457. doi: 10.1016/j.braindev.2012.07.001. [DOI] [PubMed] [Google Scholar]
- 24.Ventura E, Summa A, Ormitti F, Picetti E, Crisi G. Influenza A H1N1 related acute necrotizing encephalopathy: radiological findings in adulthood. Neuroradiol J. 2012;25(4):397–401. doi: 10.1177/197140091202500401. [DOI] [PubMed] [Google Scholar]
- 25.Wu X, Wu W, Pan W, Wu L, Liu K, Zhang HL. Acute necrotizing encephalopathy: an underrecognized clinicoradiologic disorder. Mediators Inflamm. 2015;2015:792578. doi: 10.1155/2015/792578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hoshino A, Saitoh M, Miyagawa T, Kubota M, Takanashi JI, Miyamoto A, et al. Specific HLA genotypes confer susceptibility to acute necrotizing encephalopathy. Genes Immun. 2016;17(6):367–369. doi: 10.1038/gene.2016.32. [DOI] [PubMed] [Google Scholar]
- 27.Yoshida T, Tamura T, Nagai Y, Ueda H, Awaya T, Shibata M, et al. MRI gadolinium enhancement precedes neuroradiological findings in acute necrotizing encephalopathy. Brain Dev. 2013;35(10):921–924. doi: 10.1016/j.braindev.2012.11.011. [DOI] [PubMed] [Google Scholar]
- 28.Kansagra SM, Gallentine WB. Cytokine storm of acute necrotizing encephalopathy. Pediatr Neurol. 2011;45(6):400–402. doi: 10.1016/j.pediatrneurol.2011.09.007. [DOI] [PubMed] [Google Scholar]
- 29.Shirai T, Fujii H, Ono M, Watanabe R, Shirota Y, Saito S, et al. A novel autoantibody against ephrin type B receptor 2 in acute necrotizing encephalopathy. J Neuroinflammation. 2013;10(1):128. doi: 10.1186/1742-2094-10-128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Mizuguchi M. Acute necrotizing encephalopathy. Nihon Rinsho. 2011;69(3):465–470. [PubMed] [Google Scholar]
- 31.Skelton BW, Hollingshead MC, Sledd AT, Phillips CD, Castillo M. Acute necrotizing encephalopathy of childhood: typical findings in an atypical disease. Pediatr Radiol. 2008;38(7):810–813. doi: 10.1007/s00247-008-0823-z. [DOI] [PubMed] [Google Scholar]
- 32.Okumura A, Mizuguchi M, Kidokoro H, Tanaka M, Abe S, Hosoya M, et al. Outcome of acute necrotizing encephalopathy in relation to treatment with corticosteroids and gammaglobulin. Brain Dev. 2009;31(3):221–227. doi: 10.1016/j.braindev.2008.03.005. [DOI] [PubMed] [Google Scholar]