

Abstract
Background
Caregiver burden is present in many clients managing illness in a companion animal, but current assessment tools are time‐consuming and lack normative reference values.
Objectives
Statistical reduction of items in a measure of caregiver burden to create an abbreviated version, validation of the abbreviated version, and calculation of reference values.
Animals
None.
Methods
This study was conducted using observational methods. Owners of an ill cat or dog were recruited through social media (n = 429). Veterinary clients with an ill (n = 459) or healthy (n = 961) cat or dog were recruited through a general veterinary and an academic hospital with multiple specialties. The study was conducted in 3 stages: (a) reduction of the Zarit Burden Interview (ZBI) adapted for use in pets via factor and item analyses, (b) psychometric validation of the abbreviated instrument, and (c) standardization of the abbreviated (7 items) and full (18 items) measures.
Results
A 7‐item measure showed high correlations with the full measure (r = 0.88‐0.93) and good internal consistency (α = .71‐.75) across samples of veterinary clients with an ill cat or dog. This abbreviated measure correlated significantly (P < .001) and positively with stress (r = 0.40‐0.75) and negatively with quality of life (r = −0.32 to −0.56). Reference values derived from clients with a healthy companion animal suggest “normal” burden ranges of 0 to 17 on the full measure and 0 to 8 on the abbreviated version.
Conclusions and Clinical Importance
For situations precluding full assessment of client caregiver burden, this brief 7‐item version can be used with good internal consistency and validity. Reference values can help determine if a client's caregiver burden is increased.
Keywords: caregiver strain, companion animal, measure, reference values
Abbreviations
- PSS
Perceived Stress Scale
- Q‐LES‐Q‐SF
Quality of Life Enjoyment and Satisfaction Questionnaire‐Short Form
- ZBI
Zarit Burden Interview
1. INTRODUCTION
Caregiver burden, a response of strain in the context of providing care for a loved one with an illness,1, 2 is qualitatively reported by pet caregivers,3 with approximately half of owners providing care for seriously ill companion animals demonstrating quantitatively increased levels of burden.4 This caregiver burden is correlated with clinically meaningful clinical signs of depression and reduced quality of life in samples of social media‐recruited companion animal owners4 and small animal veterinary clinic clients,5 with owners of a chronically or terminally ill cat or dog being about twice as likely to describe increased clinical signs of depression and high stress levels compared to owners of a healthy pet.
Although the animal's condition is of primary focus in veterinary medicine, the client's experience is important to consider. Work in human medicine suggests patients are more effectively managed when a health care provider understands the affect underlying patient behavior.6 Qualitative work in veterinary medicine demonstrates the importance of understanding the client's perspective in the context of decision‐making for a companion animal's treatment choices.7 Awareness of caregiver burden offers the veterinarian greater ability to understand the client's perspective and appropriately tailor communications, potentially optimizing treatment.
To date, assessment of caregiver burden in the veterinary client has been conducted using the Zarit Burden Interview (ZBI)1 adapted for use with pets.4, 5, 8 However, at 18 items, this measure might not be feasible to include in a busy practice or in clinical trials where multiple assessment measures must be completed in a short amount of time. Accordingly, the goal of the present study was to (a) statistically reduce adapted ZBI items in a large sample of owners of ill companion animals, (b) validate the abbreviated version in samples of veterinary clients (both general hospital clients and clients of a large specialty hospital with multiple services) with an ill companion animal by examining correlations with the full measure and previously established measures of stress and quality of life, and (c) provide reference values for normative caregiver burden based on a large sample of veterinary clients with a healthy companion animal to aid in interpretation of these measures.
2. MATERIALS AND METHODS
2.1. Participants
This item reduction and psychometric validation study took place using 2 phases of data collection that were then separated into 3 study stages. The first phase involved data collection of adapted ZBI responses from a large general sample of owners of an ill cat or dog recruited through social media, followed by collection of responses on the adapted ZBI as well as measures of stress and quality of life across samples of veterinary clientele of a private general small animal veterinary hospital in the Midwestern region of the United States and a large academic veterinary medical hospital in the Northeastern region of the United States through mass email, waiting room recruitment, and hospital website prompts. Greater participant detail is included below.
2.1.1. Stage 1: Item reduction sample
In the first stage, owners of an ill cat or dog were recruited via social media for an online study with inclusion criteria of: minimum 18 years of age, able to read and comprehend English, owning and currently residing with a living dog or cat that has an illness endorsed by the respondent as “chronic or terminal,” and utilization of veterinary services for that animal. The social media post promoting this study had a reach (ie, number of people whose screen displayed the post) of 6508. Of the 506 responses received, 429 (84.8%) were included in the final analytic sample (see Figure 1 for enrollment and exclusion).
Figure 1.
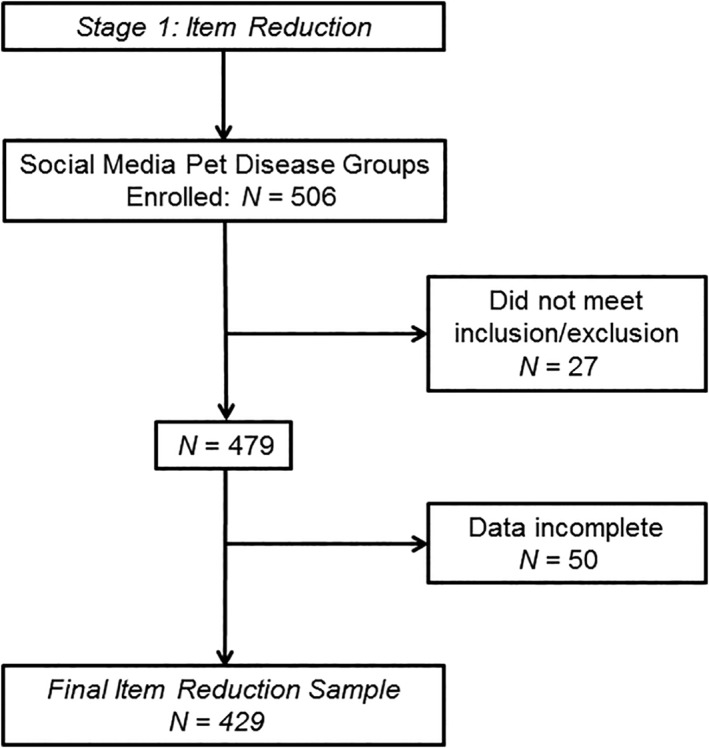
Stage 1—enrollment and inclusion/exclusion
2.1.2. Stage 2: Validation samples
In the second stage, questionnaires were administered across a private small animal general veterinary hospital and a large academic specialty veterinary center (see the Procedure section for greater details). The same inclusion/exclusion criteria as Stage 1 were utilized. Of the 910 general veterinary hospital responses received, 118 (13.0%) met study criteria and were included in the final sample (Figure 2). Of the 828 academic specialty hospital responses received, 341 (41.2%) met inclusion criteria, including 144 from internal medicine, 49 from oncology, and 148 from other specialties (Figure 2).
Figure 2.
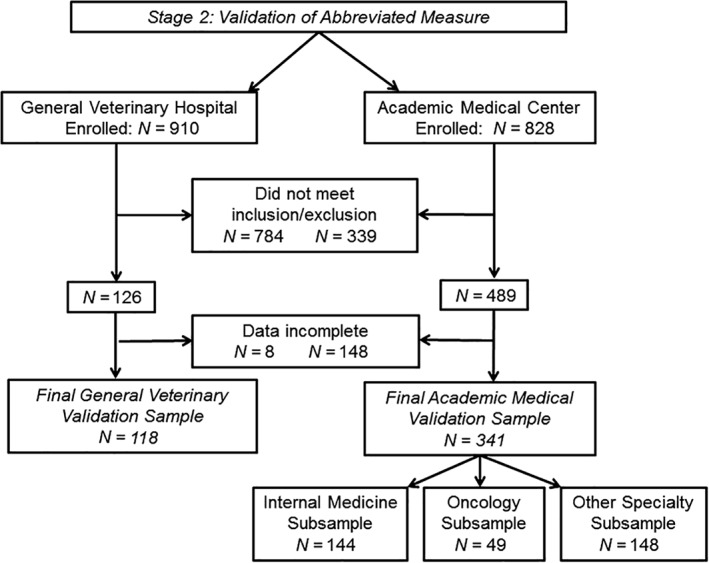
Stage 2—enrollment and inclusion/exclusion
2.1.3. Stage 3: Normative data sample
The third stage utilized data collected through the same private small animal general veterinary clinic and large academic specialty veterinary center described in Stage 2; however, in this case, those reporting on a dog or cat with an illness were removed, leaving only healthy companion animals in the sample. Of the 1738 total responses received from the general and academic hospitals, the final sample was 961 (55.3% of responses) veterinary clients with a healthy dog or cat (Figure 3).
Figure 3.

Stage 3—enrollment and inclusion/exclusion
2.2. Measures
2.2.1. Caregiver burden
The ZBI1 adapted for use with pet owners4 and small animal veterinary clients5 was the measure of focus for item reduction and creation of an abbreviated scale of pet caregiver burden. This 18‐item self‐report inventory assesses the client's experience of providing care for a sick companion animal on a 5‐point scale (“never” to “nearly always”), with items tapping into the practical impact of caregiving on the client's life (eg, “Do you feel that because of the time you spend with your pet that you don't have enough time for yourself?”) as well as affective experiences (eg, “Do you feel angry when you are around your pet?”). Higher adapted ZBI scores suggest greater caregiver burden. Psychometric properties of the adapted ZBI include internal consistency (Cronbach's α = .90‐.92)4, 5 and construct validity supported by correlation with a measure of companion animal treatment adherence that taps into difficulty providing care (r = 0.51‐0.69),4, 5 measures of the client's affective state including stress (r = 0.51‐0.56),4, 5 and a negative correlation with a quality of life measure (r = −0.54 to −0.59).4, 5
2.2.2. Perceived stress
The Perceived Stress Scale (PSS),9 a measure of stress perception, is a 10‐item scale that addresses degree of current stress and feeling that life is unpredictable or overloaded on a 5‐point scale (“never” to “very often”). Higher PSS scores indicate greater current stress, with items such as “In the last month, how often have you felt nervous and ‘stressed’?” Psychometric properties of internal consistency and convergent validity including prediction of anxiety and anger have been previously demonstrated.10
2.2.3. Quality of life
The Quality of Life Enjoyment and Satisfaction Questionnaire‐Short Form (Q‐LES‐Q‐SF)11, 12 is a 16‐item measure of quality of life which asks the respondent to indicate level of satisfaction across multiple domains (eg, mood, work, social life, and so forth) on a 5‐point scale (“very poor” to “very good”). Two items were omitted as these are not included in total scoring; a third item was removed from the current protocol because of sensitive content (ie, satisfaction with sex life) considered irrelevant to the research question. Higher scores reflect better quality of life with evidence of acceptable psychometric properties.12
2.2.4. Additional data
Participants self‐reported demographic information, specifically client age, race, and sex, and companion animal age and species. In the social media and general hospital samples, nature of primary disease was collected through participant‐reported disease with subsequent categorization by a veterinarian on our team (M.D.C.). In the academic hospital sample, nature of primary disease was collected through participant report of specialty service utilized.
2.3. Procedure
The current work was conducted and reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology criteria for cross‐sectional studies. Study protocols were approved by the Institutional Review Boards of Kent State University and Tufts University. An inductive scale reduction technique with an iterative approach13 was used, with initial item reduction conducted in a large sample of sick pet owners recruited through social media followed by validation in veterinary hospitals.
In Stage 1, a large sample of sick pet owners was recruited through social media in effort to conduct initial item reduction in a broad sample without geographic limitation. A publicly posted link to the study protocol was placed in social media pet disease groups between May 4 and 22, 2018, with group administrator or moderator approval. The post requested that individuals participate in a study to “understand how experiences of owning a cat or dog with chronic health problems or terminal illness relate to decisions, thoughts, feelings, and behaviors in the context of the pet's health care.” The protocol began with a consent page, informing the participant of the study purpose, the participant's right to discontinue at any time, Institutional Review Board approval status, and contact details for the lead investigator (M.B.S.) and local review board. Participants provided consent by advancing to the next page. Respondents were asked to report companion animal health status from a multiple choice response format that included “Healthy;” “Curable disease” (a disease that can be effectively cured and will not limit life expectancy); “Chronic disease” (a disease that lasts longer than 3 months and cannot be cured, but will not necessarily limit life expectancy); and “Terminal disease” (a progressive disease that cannot be reversed or cured, and will limit life expectancy). Because of the topic of study, only owners reporting a “Chronic” or “Terminal” disease were retained in analyses. Participants were permitted to complete the study anonymously or to provide contact information to be entered to win a gift card for an online retailer.
For Stages 2 and 3, questionnaires were administered across a small animal general veterinary hospital and a large academic veterinary medical center. These stages were conducted in veterinary hospitals to ensure that results would apply in the types of settings the abbreviated measure is expected to be most used. Data collection was conducted online between March 9, 2017, and August 15, 2018. For the private small animal general veterinary hospital, an email blast requesting participation for the study was sent to active clients and a single social media message was posted on the veterinary hospital's homepage to boost recruitment. The response rate was 13.27% of the hospital's clientele. For the academic veterinary medical center, messages were posted to the center's social media outlets and flyers about the study were distributed in the hospital waiting room. The response rate was 7.01% of the hospital's social media followers. In both cases, clients were requested to participate in a study to better understand how a pet's illness affects the owner; however, owners of both healthy and ill companion animals were encouraged to participate. Those describing experiences related to an ill dog or cat were assigned to Stage 2, whereas those reporting a healthy dog or cat were assigned to Stage 3. Participants provided consent on the first page of the survey, and then clicked to advance to the study protocol. Only clients providing informed consent were enrolled, and only those with completed protocols were included in analyses. Participants providing contact information were entered in a drawing for the chance to win a gift card for an online retailer.
All data were collected using a Qualtrics online survey platform.
2.4. Statistical analyses
Statistical analyses were conducted using SPSS version 22.0 (IBM Corp, Armonk, New York). First, demographic information was characterized for all samples using descriptive statistics.
Analyses for Stage 1 began by evaluating the adapted ZBI for normality using histograms and skewness/kurtosis values to ensure these were acceptable. Adapted ZBI responses were then examined in Stage 1 participants (ie, social media pet disease group members) in order to statistically reduce items. Participant responses to the first 17 adapted ZBI items were subjected to principal components analysis with varimax rotation and examination of multiple factor solutions. The final item (reflecting overall burden) was omitted. A factor solution was chosen based on examination of the scree plot, factor loadings, and conceptual fit. Internal consistency for each scale (ie, items included in each factor) was then examined for contribution of individual items to each scale. Items for the abbreviated scale were determined according to the highest factor loadings on each scale with number of selected items matching the proportion of variance explained by each factor. Finally, the abbreviated measure was compared to the full adapted ZBI measure using Pearson bivariate correlation and the full and abbreviated measures were examined for internal consistency (Cronbach's alpha).
Analyses for Stage 2 (ie, veterinary clients reporting an ill companion animal) began by evaluating measures (full and abbreviated adapted ZBI, PSS, and Q‐LES‐Q‐SF) for normality using histograms and skewness/kurtosis values; these were found to be acceptable. To examine the relationship between individual factors derived during Stage 1 and the full adapted ZBI, PSS, and Q‐LES‐Q‐SF, Pearson bivariate correlation was conducted. Next, Pearson bivariate correlation between the abbreviated and full adapted ZBI measures was conducted in the academic (by specialty service) and general hospital clients reporting an ill dog or cat, followed by examination of the abbreviated measure for internal consistency (Cronbach's alpha) across these samples. To examine for evidence of construct validity, Pearson bivariate correlations were conducted between the abbreviated adapted ZBI and the total scores for the PSS and Q‐LES‐Q‐SF.
Analyses for Stage 3 (ie, veterinary clients reporting a healthy companion animal) began by evaluating measures for normality using histograms and skewness/kurtosis values. Non‐normal distributions were transformed using Templeton's approach14 for transforming continuous variables to normalize distributions while leaving the original units intact. Using normalized means and SDs, score‐based normative categories for both versions of the adapted ZBI were calculated.
3. RESULTS
3.1. Stage 1: Item reduction to create abbreviated adapted ZBI
Participants were composed primarily of Caucasian women reporting on a dog. The majority of companion animal illnesses reported were related to the internal medicine domain. See Table 1 for participant demographics.
Table 1.
Stage 1—sample demographic characteristics from owners of sick dogs or cats recruited through social media pet disease groups, and who provided responses to an online research protocol including the first 17 items of the Zarit Burden Interview (ZBI) adapted for use with pets
| Social media companion animal owners (n = 429) | |
|---|---|
| Clients | |
| Age (median, min‐max) | 49 (20‐81) |
| Race (N, % Caucasian) | 396 (92.5%) |
| Sex (N, % female) | 421 (98%) |
| Animals | |
| Age (median/min‐max) | 10 (1‐20) |
| Species (N, %) | |
| Dog | 308 (72%) |
| Cat | 121 (28%) |
| Nature of primary disease (N, %) | |
| Cardiologic | 48 (11%) |
| Dermatologic | 16 (4%) |
| Internal medicine | 256 (60%) |
| Oncologic | 43 (10%) |
| Ophthalmological | 3 (<1%) |
| Orthopedic | 11 (3%) |
| Neurologic | 52 (12%) |
Scales for the adapted ZBI were first identified through principal components analysis with varimax rotation of the first 17 items. Factor analysis supported a 3‐factor solution, with factor 1 (“General Strain”) explaining approximately 23% of the variance, followed by 16% each for factors 2 (“Affect/Relational Discomfort”) and 3 (“Guilt/Uncertainty”). Item‐total correlations were computed and are shown in Table 2, ranked from the highest to lowest for each factor. Items for the abbreviated version of the adapted ZBI were selected by examining both factor loadings and item‐total correlations. To proportionally represent variance accounted for by each factor, 3 items were selected from factor 1, whereas 2 items were selected from both factors 2 and 3 (Table 2). Cronbach's alpha for the abbreviated scale was α = .76. Range of scores on the full adapted ZBI was 2‐61 (M = 24.42 ± 11.33). Range of scores on the abbreviated adapted ZBI was 0‐24 (M = 9.38 ± 4.58). Correlation of the abbreviated version with the adapted ZBI was r = 0.91.
Table 2.
Stage 1—corrected item correlation with factor ranked from the highest to lowest for each factor derived from a sample of owners of sick dogs or cats recruited through social media pet disease groups, and who provided responses to an online research protocol including the first 17 items of the Zarit Burden Interview (ZBI) adapted for use with pets
| Adapted ZBI item | r |
|---|---|
| Factor 1—general strain | |
| *Do you feel that because of the time you spend with your pet that you don't have enough time for yourself? | 0.73 |
| *Do you feel stressed between caring for your pet and trying to meet other responsibilities for your family or work? | 0.70 |
| *Do you feel you have lost control of your life since your pet's illness? | 0.69 |
| Do you feel your health has suffered because of your involvement with your pet? | 0.68 |
| Do you feel that your social life has suffered because you are caring for your pet? | 0.66 |
| Do you feel strained when you are around your pet? | 0.55 |
| Factor 2—affect/relational discomfort | |
| *Do you feel angry when you are around your pet? | 0.57 |
| *Do you feel embarrassed over your pet's behavior? | 0.56 |
| Do you feel that your pet currently affects your relationships with other family members or friends in a negative way? | 0.54 |
| Do you feel uncomfortable about having friends over because of your pet? | 0.52 |
| Do you wish you could leave the care of your pet to someone else? | 0.40 |
| Factor 3—guilt/uncertainty | |
| *Do you feel you should be doing more for your pet? | 0.63 |
| *Do you feel you could do a better job in caring for your pet? | 0.56 |
| Do you feel uncertain about what to do about your pet? | 0.53 |
| Do you feel that you will be unable to take care of your pet much longer? | 0.51 |
| Do you feel that you don't have enough money to take care of your pet in addition to the rest of your expenses? | 0.40 |
| Are you afraid of what the future holds for your pet? | 0.36 |
Note: Asterisk (*) indicates item is included on 7‐item abbreviated version.
3.2. Stage 2: Validation in veterinary clients with an ill cat or dog
Participants in both general and specialty hospital samples were also composed primarily of Caucasian women reporting on a dog. More clients reported companion animal illnesses or services within the domain of internal medicine than any other domain. See Table 3 for participant demographics results.
Table 3.
Stage 2—sample demographic characteristics from veterinary clients recruited through a small animal general veterinary hospital and a large academic hospital with specialty services who reported ownership of a sick dog or cat and provided responses to an online research protocol including the Zarit Burden Interview (ZBI) adapted for use with pets, the Perceived Stress Scale (PSS), and the Quality of Life Enjoyment and Satisfaction Questionnaire‐Short Form (Q‐LES‐Q‐SF)
| General hospital (n = 118) | Academic hospital (n = 341) | |
|---|---|---|
| Clients | ||
| Age (median, min‐max) | 52 (21‐74) | 45‐54 (18‐24; 75+) |
| Race (N, % Caucasian) | 115 (98%) | 310 (91%) |
| Sex (N, % female) | 108 (92%) | 306 (90%) |
| Animals | ||
| Age (median/min‐max) | 12 (1‐21) | 10 (1‐15) |
| Species (N, %) | ||
| Dog | 78 (66%) | 258 (76%) |
| Cat | 40 (34%) | 83 (24%) |
| Nature of primary disease (N, %) | ||
| Behavioral | 2 (2%) | 5 (2%) |
| Cardiologic | 8 (7%) | 27 (8%) |
| Dermatologic | 32 (27%) | 1 (<1%) |
| Internal medicine | 35 (30%) | 144 (42%) |
| Oncologic | 25 (21%) | 49 (14%) |
| Ophthalmological | 6 (5%) | 8 (2%) |
| Orthopedic | 7 (6%) | 25 (7%) |
| Neurologic | 2 (3%) | 27 (8%) |
| Unspecified | ‐ | 55 (16%) |
Note: “Unspecified” nature of primary disease includes those reporting on a “sick” pet but omitting category of illness.
Pearson bivariate correlations in the full sample demonstrated that 3 individual ZBI factors were each significantly related to the full adapted ZBI, PSS, and Q‐LES‐Q‐SF (P < .001 for all). For further detail, please see table included in the Supporting Information.
Pearson bivariate correlation between the abbreviated and 18‐item ZBI measures demonstrated internal consistency (Cronbach's alpha) for each sample of veterinary clients reporting an ill companion animal and construct validity between the abbreviated adapted ZBI and the PSS and Q‐LES‐Q‐SF. See Table 4 for results of validation across veterinary clinic samples.
Table 4.
Stage 2—validation of the abbreviated adapted Zarit Burden Interview (ZBI) across samples of veterinary clients recruited through a small animal general veterinary hospital and a large academic hospital with specialty services who reported ownership of a sick dog or cat and provided responses to an online research protocol including the ZBI adapted for use with pets, the Perceived Stress Scale (PSS), and the Quality of Life Enjoyment and Satisfaction Questionnaire‐Short Form (Q‐LES‐Q‐SF)
| Validation sample | N | Full ZBI | Abbreviated ZBI | r with abbreviated ZBI | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M (SD) | Range | Cronbach's α | M (SD) | Range | Cronbach's α | Full ZBI | PSS | Q‐LES‐Q‐SF | ||
| General veterinary | 118 | 18.84 (9.85) | 0‐56 | .86 | 7.57 (4.16) | 0‐22 | .73 | 0.93 | 0.40 | −0.34 |
| Specialty internal med | 144 | 17.14 (9.56) | 0‐48 | .86 | 7.10 (4.20) | 0‐20 | .75 | 0.88 | 0.57 | −0.42 |
| Oncology | 49 | 16.67 (10.43) | 2‐46 | .88 | 5.92 (4.11) | 0‐14 | .71 | 0.90 | 0.75 | −0.56 |
| Other specialty | 148 | 15.45 (9.78) | 0‐50 | .86 | 6.17 (4.06) | 0‐19 | .71 | 0.91 | 0.57 | −0.32 |
Note: “Other Specialty” includes orthopedics, neurology, cardiology, behavior, dermatology, and ophthalmology. Correlations between the abbreviated adapted ZBI and PSS/Q‐LES‐Q‐SF were all significant, P < .001.
3.3. Stage 3: Developing reference values in veterinary clients with a healthy dog or cat
The sample of participants recruited from the general and specialty hospitals who were reporting on a healthy companion animal was also composed primarily of Caucasian women reporting on a dog. See Table 5 for participant demographics. Normalized data demonstrated M = 9.73 ± 6.95 for the 18‐item adapted ZBI and M = 4.83 ± 3.29 for the 7‐item adapted ZBI. See Table 6 for raw to standardized score conversion and interpretation.
Table 5.
Stage 3—sample demographic characteristics from veterinary clients recruited through a small animal general veterinary hospital and a large academic hospital with specialty services who reported ownership of a healthy dog or cat and provided responses to an online research protocol including the Zarit Burden Interview (ZBI) adapted for use with pets
| Veterinary clients with a healthy companion animal (n = 961) | |
|---|---|
| Clients | |
| Age (median, min‐max) | 45‐54 (18‐24; 75+) |
| Race (N, % | 914 (95%) |
| Sex (N, % female) | 881 (92%) |
| Animals | |
| Age (median, mix‐max) | 7 (1‐15) |
| Species (N, %) | |
| Dog | 702 (73%) |
| Cat | 259 (27%) |
| Recruitment location | |
| General hospital | 669 (70%) |
| Academic center | 292 (30%) |
Table 6.
Stage 3—raw score interpretation for 18‐ and 7‐item Zarit Burden Interview (ZBI) adapted for use with pets derived from veterinary clients recruited through a small animal general veterinary hospital and a large academic hospital with specialty services who reported ownership of a healthy dog or cat and provided responses to an online research protocol including the ZBI adapted for use with pets
| Raw score interpretation based on SD from mean | ||||
|---|---|---|---|---|
| Average | Mild elevation | Moderate elevation | Severe elevation | |
| <1 SD | 1‐2 SD | >2‐3 SD | >3 SD | |
| <84th percentile | 85‐98th percentile | 99‐99.9th percentile | >99.9th percentile | |
| Adapted ZBI: 18‐item raw score | <17 | 18‐24 | 25‐31 | >31 |
| Adapted ZBI: 7‐item raw score | <8 | 9‐11 | 12‐15 | >15 |
4. DISCUSSION
The goal of the present study was to statistically reduce the ZBI adapted for pets to create an abbreviated version of the measure, to demonstrate psychometric properties of this abbreviated version across samples of veterinary clients with an ill companion animal, and to provide reference values for interpretation of the abbreviated and full length adapted ZBI. A 7‐item scale was created through factor analysis of responses from a large group of owners of seriously ill companion animals, proportionally representing the variance of each factor with the items most strongly contributing to their respective factors. This abbreviated scale showed high correlations with the original measure and good internal consistency across several samples of veterinary clients with an ill companion animal recruited from general and academic medical center hospitals. The abbreviated measure correlated positively with a measure of stress and negatively with a measure of quality of life, providing evidence of construct validity. Reference values derived from a large sample of general veterinary hospital and academic medical center clients reporting on a healthy companion animal indicate “normal” burden ranges from a summed score of 0 to 17 on the full measure and 0 to 8 on the abbreviated version.
An abbreviated measure of client caregiver burden could facilitate efficient gathering of information regarding the impact of companion animal disease on client functioning. This brief, 7‐item scale can easily be completed during an office visit, lending itself to use as a quick secondary outcome measure for clinical trials. It might also be of use in standard practice as a tool to facilitate client communications, as greater understanding of the client's experience while caring for a seriously ill companion animal could help the veterinarian better appreciate the client's perspective. The present study also expands the utility of the full adapted ZBI in veterinary medicine by providing reference values. In the absence of normative data from healthy samples, measurement of caregiver burden is limited to direct comparison with a healthy sample or assessment over time to examine for change. The reference values provided in the current work allow interpretation of caregiver burden assessment at a single timepoint, which may be of particular use for case studies or clinical work. Additionally, these reference values provide the opportunity for researchers to determine if, as a secondary outcome measure, a patient treatment reduces caregiver burden to a reference range for the client. Of note, prior work in a smaller sample tentatively proposed a cut score of 18 for the full adapted ZBI4; using a much larger normative sample, the current study similarly suggests a raw score of 18 as the lower end of increased caregiver burden for veterinary clients, and extends to suggest a raw score of 9 as the lower end of increased burden using the abbreviated measure. Continued examination of the full and abbreviated adapted ZBI in other samples and geographical regions might help determine if there are circumstances for which the proposed cutoffs do not apply.
Although significantly correlated in the expected directions with measures used to establish construct validity, correlations between the abbreviated adapted ZBI and constructs related to caregiver burden ranged in magnitude. Moderate to high correlations15 were observed for stress, which is consistent with past work.4, 5 In contrast, a somewhat lower strength of relationship was noted for quality of life. Interestingly, these correlations were lowest in the general hospital and “other specialty” academic hospital client samples. Variability in demographic characteristics not captured in the current study, including specific clinical issues of the companion animals, might contribute lower psychometric stability of the abbreviated adapted ZBI in these broad groups. An alternative explanation could be that several items that would overlap with specific domains assessed in examination of quality of life, including health, social, and financial strain, were removed in the abbreviation process because of low factor loadings. These “high overlap” items may drive stronger correlations with quality of life when using the full adapted ZBI. If this is the case, the abbreviated adapted ZBI could actually represent a more pure reflection of the construct of caregiver burden, as research demonstrates that caregiver burden and quality of life are separate, though typically strongly linked constructs.16 Continued work is needed to examine the theoretical underpinnings of caregiver burden in this population in order to further investigate this question.
Limitations of the current work are present. All participants were recruited through convenience sampling; hospital‐based recruitment methods consisted of voluntary participation rather than data collected from consecutively served clients, and participants were presented with the opportunity to win a gift card. These methods could have introduced selection bias in that participants were motivated to report their experiences. Additionally, although a strength of this study is the inclusion of companion animal owners from diverse settings (online social media pet disease group owners, clients of a general veterinary hospital, and clients of a large academic medical center hospital), still broader sampling might be of benefit. Stages 2 and 3 of the study (validation stages) were conducted in just 2 hospitals (1 general, 1 specialty) and represented just 2 geographical regions of the United States with median household income in the range of $62‐68 000.17 Participants were fairly homogeneous in terms of race and sex, with overrepresentation of females and Caucasians relative to the census data for these locations.17 Similar to prior work,4, 5, 8, 16, 18 the overrepresentation of Caucasian females could lead to bias in that these individuals might experience burden differently from other groups. Although this is possible, it is also likely that the demographic make‐up of our sample is representative of the target population, that is, veterinary clients who choose caregiving over euthanasia when faced with significant illness in a companion animal. Additionally, the current work included only owners of a cat or dog. Clients with other types of companion animal may experience similar burden, but it is not clear if results will generalize. Finally, regarding reference values, because caregiver burden is conceptually due to the burden of providing care during illness,1, 2 it could be argued that veterinary clients with a healthy companion animal are a suboptimal reference point. However, the present study and prior work demonstrate that when examining self‐reported caregiver burden, a summed total of “0” is actually not typical for owners of a healthy companion animal.4, 5, 8, 16 In the same way that it is necessary to know the range of values greater than “0” that could be still be considered negative for a given bloodwork titer, it is essential to establish reference values for “normal” burden associated with owning a healthy companion animal.
Future research should examine the utility of this abbreviated measure relative to the full adapted ZBI in other specialty samples to ensure robustness of findings. In the current work, recruitment in several specialty fields (eg, orthopedic, neurologic, and dermatologic) yielded samples too small to conduct stable correlational analyses; as such, these areas were combined into a single sample of “other” primary disease specialties. However, it is possible that caregiver burden would show differences in these groups, and this should be investigated as a primary question. The interaction between burden and financial stress, as well as other owner‐related characteristics (eg, personality, mental health), should be also explored in future research. Work to examine if a still further abbreviated (ie, “screener”) version of the measure might also be of benefit. In the current study, a decision was made to reduce to 7 items in order to preserve proportional representation of the adapted ZBI factors while reducing items on the measure by more than half. Further reduction of the measure might facilitate use, but could cause greater psychometric instability, and would need to be undertaken with caution. Additionally, work examining the relationship between owner burden and outcomes related to animal health, such as treatment compliance and animal quality of life, is much needed.
This study provides an abbreviated version of the ZBI adapted for use with pets. Results show this abbreviated version correlates strongly with the full measure, exhibits good internal consistency, and shows evidence of construct validity across samples recruited from general and specialty animal hospitals, though confirmation of psychometric properties in broad and representative samples is recommended. Reference values derived from a large sample of clients with healthy companion animals may be used to aid in interpretation, whether using the full or brief version. With just 7 items, the new abbreviated measure could be easily incorporated into a busy practice or clinical trials to better understand the experience of the client while providing care for an ill companion animal.
CONFLICT OF INTEREST DECLARATION
Authors declare no conflict of interest.
OFF‐LABEL ANTIMICROBIAL DECLARATION
Authors declare no off‐label use of antimicrobials.
INSTITUTIONAL ANIMAL CARE AND USE COMMITTEE (IACUC) OR OTHER APPROVAL DECLARATION
Authors declare no IACUC or other approval was needed.
HUMAN ETHICS APPROVAL DECLARATION
Human Ethics Approval was granted through the Kent State University Institutional Review Board (#16506 and #18215) and the Tufts University Social‐Behavioral‐Educational Research Institutional Review Board (#1806048).
Supporting information
Supporting Table. Stage 2—Independent factor correlations for the full adapted Zarit Burden Interview (ZBI), Perceived Stress Scale (PSS), and Quality of Life Enjoyment and Satisfaction Questionnaire‐Short Form (Q‐LES‐Q‐SF) in a combined sample of veterinary clients recruited through a small animal general veterinary hospital and a large academic hospital with specialty services, who reported ownership of a sick dog or cat in an online research protocol.
Spitznagel MB, Mueller MK, Fraychak T, Hoffman AM, Carlson MD. Validation of an abbreviated instrument to assess veterinary client caregiver burden. J Vet Intern Med. 2019;33:1251–1259. 10.1111/jvim.15508
Funding information Tufts Cummings Seed Grant
REFERENCES
- 1. Zarit SH, Reever KE, Bach‐Peterson J. Relatives of the impaired elderly: correlates of feelings of burden. Gerontol. 1980;20:649‐655. [DOI] [PubMed] [Google Scholar]
- 2. Tremont G, Davis JD, Spitznagel MB. Understanding and managing caregiver burden in cerebrovascular disease In: Paul RH, Cohen R, Ott BR, Salloway S, eds. Vascular Dementia: Cerebrovascular Mechanisms and Clinical Management. Totowa, NJ: Humana Press; 2005:305‐321. [Google Scholar]
- 3. Christiansen SB, Kristensen AT, Sandoe P, et al. Looking after chronically ill dogs: impact on the caregiver's life. Anthrozoos. 2013;26:519‐533. [Google Scholar]
- 4. Spitznagel MB, Jacobson DM, Cox MD, et al. Caregiver burden in owners of a sick companion animal: a cross‐sectional observational study. Vet Rec. 2017;181:381‐387. [DOI] [PubMed] [Google Scholar]
- 5. Spitznagel MB, Cox MD, Jacobson DM, et al. Assessment of caregiver burden and associations with psychosocial function, veterinary service use, and factors related to treatment plan adherence among owners of dogs and cats. J Am Vet Med Assoc. 2019;254:133‐144. [DOI] [PubMed] [Google Scholar]
- 6. Banez ME. Responding effectively to the angry patient. Medsurg Nurs. 1996;5:461‐468. [PubMed] [Google Scholar]
- 7. Christiansen SB, Kristensen AT, Lassen J, et al. Veterinarians' role in client's decision‐making regarding seriously ill companion animal patients. Acta Vet Scand. 2016;58:30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Spitznagel MB, Jacobson DM, Cox MD, Carlson MD. Predicting caregiver burden in general veterinary clients: contribution of companion animal clinical signs and behavior problems. Vet J. 2018;236:23‐30. [DOI] [PubMed] [Google Scholar]
- 9. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24:386‐396. [PubMed] [Google Scholar]
- 10. Perera MJ, Brintz CE, Birnbaum‐Weitzman O, et al. Factor structure of the Perceived Stress Scale‐10 (PSS) across English and Spanish language responders in the HCHS/SOL sociocultural ancillary study. Psychol Assess. 2017;29:320‐328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Endicott J, Nee J, Harrison W, Blumenthal R. Quality of Life Enjoyment and Satisfaction Questionnaire: a new measure. Psychopharmacol Bull. 1993;29:321‐326. [PubMed] [Google Scholar]
- 12. Stevanovic D. Quality of life enjoyment and satisfaction questionnaire‐short form for quality of life assessments in clinical practice: a psychometric study. J Psychiatr Ment Health Nurs. 2011;18(8):744‐750. [DOI] [PubMed] [Google Scholar]
- 13. Ben‐Porath YS. Self‐report inventories: assessing personality and psychopathology In: Graham JR, Naglieri J, eds. Handbook of Assessment Psychology. Vol X 2nd ed. New York, NY: Wiley; 2013:622‐644. [Google Scholar]
- 14. Templeton GF. A two‐step approach for transforming continuous variables to normal: implications and recommendations for IS research. Commun Assoc Inform Syst. 2011;28:4. [Google Scholar]
- 15. Hinkle DE, Wiersma W, Jurs SG. Applied Statistics for the Behavioral Sciences. 5th ed. Boston, MA: Houghton Mifflin; 2003. [Google Scholar]
- 16. Spitznagel MB, Solc M, Chapman KR, Updegraff J, Albers AL, Carlson MD. Caregiver burden in the veterinary dermatology client: comparison to healthy controls relationship to quality of life. Vet Dermatol. 2018;30:3‐e2. 10.1111/vde.12696. [DOI] [PubMed] [Google Scholar]
- 17. U.S. Census Bureau Quickfacts [Internet]. Washington, D.C. United States Department of Commerce. https://www.census.gov/quickfacts/. Accessed January 8, 2019.
- 18. Spitznagel MB, Ben‐Porath YS, Rishniw M, et al. Development and validation of a Burden Transfer Inventory measure for predicting veterinarian stress related to client behavior. J Am Vet Med Assoc. 2019;254:124‐132. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supporting Table. Stage 2—Independent factor correlations for the full adapted Zarit Burden Interview (ZBI), Perceived Stress Scale (PSS), and Quality of Life Enjoyment and Satisfaction Questionnaire‐Short Form (Q‐LES‐Q‐SF) in a combined sample of veterinary clients recruited through a small animal general veterinary hospital and a large academic hospital with specialty services, who reported ownership of a sick dog or cat in an online research protocol.