

Abstract
High tibial osteotomy becomes increasingly important in the treatment of cartilage damage or osteoarthritis of the medial compartment with concurrent varus deformity. HTO produces a postoperative valgus limb alignment with shifting the load-bearing axis of the lower limb laterally. However, maximizing procedural success and postoperative knee function still possess many difficulties. The key to improve the postoperative satisfaction and long-term survival is the understanding of the vital biomechanics of HTO in essence. This review article discussed the alignment principles, surgical technique, and fixation plate of HTO as well as the postoperative gait, musculoskeletal dynamics, and contact mechanics of the knee joint. We aimed to highlight the recent findings and progresses on the biomechanics of HTO. The biomechanical studies on HTO are still insufficient in the areas of gait analysis, joint kinematics, and joint contact mechanics. Combining musculoskeletal dynamics modelling and finite element analysis will help comprehensively understand in vivo patient-specific biomechanics after HTO.
1. High Tibial Osteotomy
Knee joint is a very complex and important joint for load and motion, including the tibiofemoral (TF) joint and the patellofemoral (PF) joint. The stability of the knee joint is mainly dependent on the interaction by ligamentous and cartilaginous structures, meniscus as well as several muscles and tendons. Loads imposed on the tibiofemoral joint are over a few times the body weight (BW) during daily activities. And average peak resultant forces were highest during stair descending (346% BW), followed by stair ascending (316% BW) and level walking (261% BW) [1]. The medial-lateral force distribution is dependent on the tibiofemoral alignment and varies within different weight-bearing tasks. During a walking gait, the medial-lateral load distribution is changing on the tibia [2, 3]. And approximately 75% of the joint load passes through the medial tibial plateau during single-leg stance [4].
Osteoarthritis (OA) is nowadays the most common disease of joints in adults around the world [5]. OA is characterized by a progressive loss of articular cartilage accompanied by new bone formation and, often, synovial proliferation that may culminate in pain, loss of joint function, and disability [6]. Symptomatic OA is characterized by radiographic evidence along with persistent joint pain or stiffness [7]. Most common pattern of symptomatic OA within the knee is articular cartilage degeneration predominantly in the medial compartment [8, 9]. The joint degeneration further results in a varus deformity with increasing load transmission through the already degenerate compartment [4]. Furthermore, knee joint loading and kinematics have been found to be altered in patients with early knee OA during gait [10].
A literature search was conducted using electric databases including the PubMed for English-language studies with full text from January 2008 to December 2018. When the search parameter used for PubMed database was “high tibial osteotomy” with full text for humans, 777 papers were identified. Most of them were to examine the functional clinical outcome after operations and analyze the determinants. What we need is biomechanics analyses of HTO. Hence, we excluded them, and we removed those studies about patella and ligament reconstruction. After screening, there were 76 related literature studies. Then seven papers about the comparative studies between HTO and UKA or TKA were included. So did the 13 highly cited papers ten years ago. Figure 1 illustrates the flow chart of papers to explain the inclusion/exclusion criteria of studies.
Figure 1.
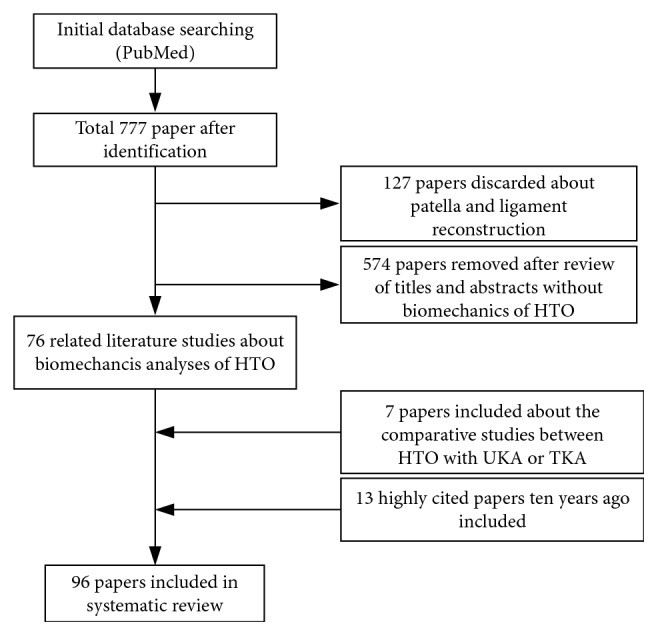
Flow chart.
Many conservative treatments of knee OA have been reported, such as medical treatment, foot orthoses, knee braces, and muscle strengthening. Those treatments can prevent or slow the progression of medial knee OA [11]. However, no conclusive evidences have been confirmed in many previous studies on the effectiveness of any braces and orthoses for patients with medial knee osteoarthritis [12]. And the optimal choice for an orthosis remains unclear, and long-term implications are lacking [13]. On the contrary, total knee arthroplasty (TKA) has been established as a very successful and commonly performed procedure for primary and secondary osteoarthritis. However, compared to medial unicompartmental knee arthroplasty (UKA) and high tibial osteotomy (HTO), active and demanding activities seem more unlikely after TKA [14, 15]. HTO showed an improved indication for active patients with a good range of motion of the knee [14, 16]. Although there are no significant differences in the clinical outcome between UKA and HTO at 12 months and 2-year follow-up, the advantages of HTO is the preservation of the knee joint as long as possible, a large corrective effect of the mechanical axis, and the avoidance or postponement of knee replacement [17–19]. The main indications for HTO and UKA are summarized and listed in Table 1 [20]. Most HTO patients returned to sport and work after knee osteotomy. From 10 to 22 weeks, almost all patients returned to the same or a higher workload [21].
Table 1.
Indications for UKA, HTO, and overlaps between treatments.
| UKA | HTO or UKA | HTO | |
|---|---|---|---|
| Age | >55 years | 55–65 years | <65 years |
| Activity level | Low demands | Moderately active | Active |
| Weight (BMI) | <30 | Any | |
| Alignment | 0–5° | 5–10° | 5–15° |
| AP instability | No to grade I | No to grade I | Any |
| ML instability | No to grade I | No to grade I | No to grade II |
| ROM | Arc 90° and <5° flexion contracture | Arc 100° and <5° flexion contracture | Arc 120° and <5° flexion contracture |
| Arthrosis severity | Any | Ahlback II | Ahlback I-II |
UKA = medial unicompartmental knee arthroplasty; HTO = high tibial osteotomy; BMI = body mass index; AP instability = anteroposterior instability; ML instability = mediolateral instability; instability grading: according to the American Medical Association (grade I = 0–5 mm; grade II = 5–10 mm; grade III = >10 mm; no hard stop); arthrosis severity = medial compartment arthrosis according to Ahlback classification, assuming that lateral and patellofemoral compartments are intact.
Selection of the ideal patient is an important factor in achieving good results with HTO. Based on the previous findings, the ideal candidate for an HTO is a young patient (<60 years of age), with no severe articular destruction (Ahlback grade III or more according to the Ahlback classification), isolated medial osteoarthritis, and good range of motion and without ligamentous instability [22]. The contraindication is ≥15° of flexion contracture, joint instability together with ≥1 cm lateral tibial thrust, ≥20° of correction, rheumatoid arthritis, and advanced patellofemoral arthritis [23]. With the improvements in soft-tissue preparation, advances in surgical techniques, neither the patients' weight and age nor the genesis of deformity has been found to influence the rate of complication from a large number of postoperative databases [24–26].
Although HTO has recently become advocated and used to treat osteoarthritis around the knee, it still causes some complications such as nonunion, tibial plateaus fracture, lateral cartilage degeneration, plate breakage, and so on. Stiffness is uncommon if preoperative motion is satisfactory [27]. Furthermore, a small percentage of patients treated with HTO (4% to 26%) do not have satisfactory pain relief, and this is the primary reason for revision to TKA [28–30]. Ultimately, majority of complications and dissatisfaction are closely related to the biomechanics of HTO. The key to improve the postoperative satisfaction and long-term survival is the understanding of the vital biomechanics of HTO.
2. Alignment Principle
The ideal mechanical axis passes from the center of the hip, through the knee, to the center of the tibiotalar joint [31]. The orientation of the normal anatomic axis of the knee is 5° to 7° valgus [32]. In addition, the articular surface of the tibia averages 3° varus and that of the femur 2° to 3° of valgus relative to the mechanical axis [33]. Schematic limb alignment assessment is shown in Figure 2. In neutral alignment, the knee moment in the coronal plane causes approximately 55 ∼ 70% of knee load to be transmitted on the medial compartment during the stance phase of gait [34]. With varus alignment, this imbalance is exacerbated so that a deviation of 1° varus from the neutral alignment increased the medial load by 5% [35]. Analyses of interindividual variations revealed a linear correlation with limb alignment [35]. In a longitudinal observational study, the varus alignment of more than 2° considerably increased the probability of developing OA in a rather short period of time [36].
Figure 2.
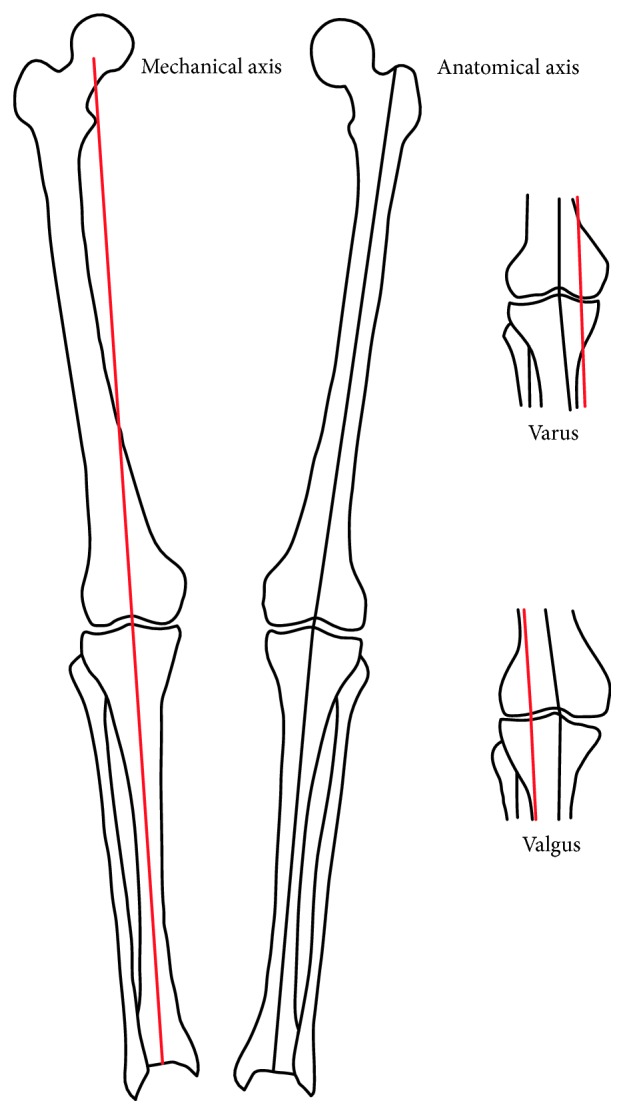
Radiographic lower limb alignment assessment. The mechanical axis of the limb (red line) is defined by a line from the center of the femoral head to the medial tibial spine and a line from the medial tibial spine to the center of the ankle. The weight-bearing line (also represented by the red line, as this knee has normal alignment of 0°) is defined by a line from the center of the femoral head to the center of the ankle joint. The anatomic axis of the limb (black line) is defined by mid-diaphyseal lines in the femur and tibia. In a varus knee, the weight-bearing axis passes medial to the medial tibial spine. In a neutral knee, the weight-bearing axis passes through the medial tibial spine. In a valgus knee, the weight-bearing axis passes lateral to the medial tibial spine [32].
The biomechanical objective of HTO is to realign the weight-bearing line (WBL) in the coronal plane. The aim is to achieve the shift of the weight-bearing line from the arthritic compartment to the opposite tibiofemoral healthy compartment [37]. Overall, leg alignment is a crucial factor for the force distribution in the knee joint [38]. The decrease of load in the diseased compartment of the tibial plateau reduces knee joint pain and delays progression of osteoarthritis [39, 40].
The reported success rates of HTO are inconsistent with the long-term survivals and satisfaction of this procedure. Although a consensus is that ideal opening wedge HTO produces a decompression of the medial joint compartment, optimal amount of alignment correction of the lower limb remains unknown, which may result in the discrepancies among the surgeries [10]. Fujisawa et al. [36, 41] recommended to align the WBL of HTO through the 65%–70% coordinate of the width of the tibial plateau, which has been refined recently to 62.5% (range 62% ∼ 66%). An average overcorrection of 3° valgus was supported by previous studies long ago. However, excessive overcorrection would lead to worse functional outcomes and degeneration in the lateral compartment, while undercorrection could not relieve the pain of the medial compartment [36, 42, 43].
The accurate correct angle is dependent on the patient's physical condition and the severity of arthritis generally. The reason why overcorrected knees are applied widely is that patients with a valgus angle of 3° and more had the best outcome and highest postoperative survival rate [37, 44]. However, this recommendation is only based on one noncomparative retrospective study, and the recommendations based on higher evidence levels do not exist. There is no reasonable way to evaluate the optimal angle of osteotomy before operation, which is the most important for limb alignment and long-term results. Furthermore, there are no significant differences in terms of the ratio of cartilage repair in the medial compartment of the tibiofemoral joint between 17 overcorrected knees with mean tibiofemoral angle of 165° ± 1° and 54 moderately corrected knees with mean tibiofemoral angle of 170° ± 2° after open-wedge HTO [45].
Compared to the two-dimensional (2D) alignment in the coronal plane, the three-dimensional (3D) alignment is a potential method to achieve better results in short and long terms after HTO surgery [46]. The 3D alignment method shows better correction on the knee load bearing, and the most important factor in HTO is observing the WBL in a 3D environment. The posterior tibial slope angle may be increased without the consideration of the change in the sagittal plane. The 3D alignment method can effectively avoid such postoperative complication, and it is worthy of further study and clinical verification. 3D printing technique has been introduced recently in HTO, and good radiological results have also been obtained [47].
Specogna et al. [48] reported the effects of the dynamic measurement on the tibiofemoral angle (TFA) during the gait cycle, which is different from the static alignment. Furthermore, standing full-length alignment (SFLA) and supine radiographs alignment were compared. The measured TFA by single-limb standing radiographs was significantly greater (−8.7° ± 4.0°) than that by double-limb standing radiographs (−7.1° ± 3.8°) and by supine radiographs (−5.5° ± 2.8°) [49]. Hence, the standing alignment may be better than the supine radiographs alignment, and the dynamic alignment may be superior to static measures.
3. Open-Wedge or Closed-Wedge HTO
Open-wedge (OW) and closed-wedge (CW) HTO are different osteotomy techniques (Figure 3). The advantages and disadvantages in clinical results between OWHTO and CWHTO are compared in Table 2. Recent studies have shown that OWHTO has several advantages over CWHTO, including higher accuracy of correction, better survival at ten years, wider range of motion, less soft-tissue dissection, and more reserve of the proximal tibiofibular joint [19, 53, 54, 56]. However, OWHTO also increases the posterior slope angle and limb length and decreases the patellar height [19, 51, 54, 55]. Besides, autologous iliac bone graft is unnecessary for patients in whom the opening wedge is <12.5 mm [50, 57]. CWHTO trend led to a higher incidence of opposite cortical fracture [19].
Figure 3.

Schematic of open-wedge HTO (a) and closed-wedge HTO (b) of a knee with varus deformity.
Table 2.
Comparison of the clinical results between open-wedge (OWHTO) and closed-wedge (CWHTO).
| Year | Papers | Patients | OWHTO | CWHTO | |
|---|---|---|---|---|---|
| OW | CW | ||||
| 2014 | Duivenvoorden et al. [50] | 45 | 47 | More complications | More early conversions to total knee arthroplasty with six years |
| 2014 | Van Egmond [51] | 25 | 25 | Patella baja leads to patellofemoral complaints and worse results | Better satisfactory and score with an average of 7.9 years |
| 2014 | Deie et al. [52] | 9 | 12 | Reduced knee varus moment and lateral thrust | Little effect on reducing lateral thrust |
| 2015 | Duivenvoorden et al. [53] | 112 | 354 | Higher survival ratio, 15% serious adverse events, 13% adverse events | 13% serious adverse events, 6% adverse events |
| 2016 | Sun et al. [19] | 740 | 743 | Increased the posterior slope angle and limb length; decreased the patellar height; higher accuracy of correction | Higher incidence of opposite cortical fracture |
| 2017 | Wu et al. [54] | 1274 | 1308 | Wider range of motion; greater posterior tibial slope angle; lesser patellar height | No significant difference in HKA and mean angle of correction |
| 2018 | Lee et al. [55] | 127 | 175 | The increase in leg length had a positive correlation with the degree of correction | The decrease in leg length was negligible |
Prodromos and Andriacchi [58] found that patients with a low knee adductor moment had better clinical results according to gait analysis after HTO. Deie et al. [52] reported that OWHTO reduced knee varus moment and lateral thrust, whereas CWHTO had little effect on reducing lateral thrust. According to their results, opening the depressed medial proximal tibia is thought be a more reasonable procedure in terms of correcting the deformed lesion than closing the intact lesion of the proximal tibia from a biomechanical aspect. Hence, medial OWHTO has been an effective and appealing surgical procedure intended to treat medial compartment osteoarthritis in young and active patients with proximal varus knees [59].
4. Fixation Plate
HTO results in a highly unstable structure of the proximal tibia, which is the potential source of mechanical failure of plates and screws. Consequently, use of the fixation devices and optimal designs are essential to the success of HTO, especially for overweight or full weight-bearing patients.
Majority of studies have investigated the fixation plate design of HTO. Currently, the commercial implants for the treatment of medial knee joint osteoarthritis are TomoFix small stature, TomoFix standard, Contour Lock, iBalance, and second-generation PEEKPower [60]. The use of locking screws can stabilize the construct and decrease the implant and bone stresses [61]. The one-leg system with locking screws can be used for the majority of the patients without heavy bodyweight and poor bone quality. For the shape design, a two-leg system is suggested for the patients with heavy load demands and greater proximal tibial size. T- and I-shaped plates can provide a wider base for supporting the HTO wedge even without the use of locking screws, thus significantly enhancing construct stiffness and suppressing wedge fracture [62]. A more concave tibial profile and/or reduced distraction angle necessitates a higher compressive load to elastically deform the plate, thereby deteriorating the lateral-hinge fracture risk [63]. A precontoured plate is recommended by surgeons when the proximal tibia is highly concave, and the distraction angle is insufficient to stretch the tibial profile. Diffo Kaze et al. [60] reported a novel anatomically contoured implant called “Activmotion” which can provide a better mechanical stability and strength. Ideal implants with a metaphyseal slope should adapt to the tibia anatomy and position more anteriorly on the medial compartment of the proximal tibia. Furthermore, the position on the proximal tibia of the fixation plate is also important. More comparable performance was found when TomoFix plate was placed more medially than the T- and I-shaped plates [62]. Therefore, if a single plate and a smaller incision are considered, the medial implant position of the TomoFix plate is appropriate as a better alternative for stabilizing the medial HTO wedge [62]. In addition, the difference of having a drill hole or not at the end of a horizontal osteotomy was investigated, and the effect on reducing the risk of lateral cortex fracture was not significant, especially for older patients [64]. A cadaveric experiment produces similar conclusions that there was no significant difference in the strains on the lateral cortex during OWHTO between the pilot hole and no-hole conditions [65].
The present findings about the biomechanics of the fixation plate showed that implant position and the geometry are vital parameters to maintain stability. The current plate design should be modified to the surface geometry of the postcorrection for the proper fitting [66]. As the correction degree increases, the plate should be bent at both ends of the opening gap in the coronal plane [67]. Patient-specific design of the fixation plate of HTO may be an alternation in future.
5. Kinematics
Medial compartment OA with varus deformity leads to the changes in kinematics of gait and joint movement. In addition to restoring the normal alignment of the lower limb, HTO is also successful in modifying the osteoarthritic gait [68]. However, there are some discrepancies in analyses about subjects, methodologies, and outcomes. Furthermore, the changes in gait could have diverse effects on the trunk, nonoperated limb, and hip and ankle joint in the operated limb after HTO [69]. Recent kinematical studies in gait are summarized in Table 3. HTO does not alter the time-distance parameters of gait at one year postoperatively; however, patients have improved perception of their walking ability [10]. Walking speed and stride length were increased after HTO [68, 70]. The range of motion of the knee joint was increased and maintained for 5 years after HTO with anterior cruciate ligament (ACL) reconstruction [71]. The corrected approximately neutral alignment in HTO produced substantial changes in dynamic loading and function of knee joint [73]. HTO presented positive results in joint kinematics after postoperative 6 months, not only in the coronal plane but also in the sagittal and axial planes [72]. Leitch et al. [70] found medial OWHTO resulted in decreased flexion and internal rotation during both level walking and stair ascent. In addition, gait modifications are an important approach to reduce the knee adduction moment (KAM) without necessarily decreasing the medial compartment force [74]. However, in general, few studies are performed to investigate the gait modification and joint movement after HTO.
Table 3.
Changes in kinematics after HTO.
| Year | Author | Patients | Duration | Gait parameter |
|---|---|---|---|---|
| 2013 | Lind et al. [68] | 11 male patients with medial OA | Before 12 months and after medial OWHTO | (1) Mean maximum varus angle during stance was reduced from 13.5° to 5.4°(normal 6.8°) (2) Walking speed increased significantly postoperatively. (3) Maximum knee flexion increased significantly (4) Stride length increased from 1.37 m preoperatively to 1.48 m postoperatively (5) The mean radiological mechanical alignment was changed (pre-op: 172°, post-op: 180°) |
|
| ||||
| 2015 | Leitch et al. [70] | 14 patients with varus alignment and OA | Before 6 and 12 months after OWHTO | (1) Speed increased after surgery. (2) The peak external rotation angle was increased after surgery |
|
| ||||
| 2015 | Marriott et al. [71] | 33 patients with varus | Before 2 and 5 years after ACL reconstruction and HTO | (1) The means of valgus, flexion, and internal rotation angle increased by 7.79°, 3.80°, and 7.07°, respectively, with 5 years (2) The means of extension and external rotation angle decreased by 2.14° and 5.88°, respectively, with 5 years |
|
| ||||
| 2017 | Da Silva et al. [72] | 21 patients with OWHTO compared to the control group (16) | Short-term results of HTO of 6 months | (1) No significant changes in stride length and speed were observed in the post-op period (2) The foot external rotation angle decreased significantly in the axial plane (25.5°–11.5°) (3) Knee varus angle significantly reduced in the coronal plane (pre-op: 11.6°; post-op: 4.3°) |
|
| ||||
| 2017 | Morin et al. [10] | 21 HTO patients | Preoperatively and at 1 year postoperatively | (1) The preoperative median of 7° varus (1–11°) was corrected to 3° valgus (0–6°) (2) Time-distance gait parameters, such as step width and walking speed, did not change 1 year after surgery (3) The patients' subjective perception of their walking ability improved |
6. Knee Joint Moment and Force
Balancing loads between medial and lateral compartments is an important factor in improving the long- or short-term survival rates of HTO. Ideally, an appropriate correction achieves a minimum overcorrection from baseline alignment necessary for adequate medial unloading, whilst avoiding overloading on the lateral compartment cartilage. The current research studies reported that KAM and knee flexion moment (KFM) after HTO of the surgical knee were decreased significantly [68, 70–72, 75, 76] and medial OWHTO resulted in a decrease in the KAM during both level walking and stair ascent [70]. However, in coronal, sagittal, and transversal planes, the change of the KAM is inconsistent in different reports [72]. Recent knee moment studies in gaits are shown in Table 4.
Table 4.
Changes in knee moment after HTO.
| Year | Author | Patients | Duration | Force or moment analysis | The influence of nonsurgical limb |
|---|---|---|---|---|---|
| 2010 | Bhatnagar and Jenkyn [76] | 30 HTO patients | Pre-HTO, 6 and 12 months post-HTO | (1) ML and MLR were reduced significantly by 0.56% BW and 1.0, respectively (2) First peak of an EKAM during stance phase was reduced significantly by 1.70% BW ∗ ht (3) No significant difference was observed between 6 and 12 months post-HTO |
— |
|
| |||||
| 2013 | Meyer et al. [75] | A single subject: Implanted with a tibial prosthesis | — | (1) Total contact force may be changing (2) KAM is not a suitable indicator of medial contact force in situations |
— |
|
| |||||
| 2013 | Lind et al. [68] | 11 male patients with medial OA | Before 12 months and after OWHTO | (1) Mean maximum KAM reduced from 3.9 to 2.7 (% Bw ∗ ht) (2) Maximum of EKFM increased significantly |
KAM increased postoperatively from 3.3 to 4.1 (% Bw ∗ ht) |
|
| |||||
| 2015 | Leitch et al. [70] | 14 patients with varus and OA | Before, 6 and 12 months after OWHTO | The peak KAM, KFM, and IRM all decreased significantly after HTO during walking and stair ascent with sustained (12 months) changes in all three orthogonal planes | IRM was higher during stair ascent, while the peak KAM was lower |
|
| |||||
| 2015 | Marriott et al. [71] | 33 patients with varus | Before, 2 and 5 years after ACL reconstruction and HTO | (1) The EKAM and KFM in the surgical limb decreased significantly in the peak. (2) Substantial improvements were maintained at 5 years in all 3 planes during walking. |
(1) KAM increase slightly. (2) KFM decreased. |
|
| |||||
| 2017 | Da Silva et al. [72] | 21 patients with OWHTO | Short-term results of HTO of 6 months | (1) The peak of KAM and KFM was reduced and close to the values of the control group in the coronal plane (2) The peak KFM and the KEM was increased significantly in the sagittal plane |
— |
Although KAM was a surrogate for knee contact force (KCF), it well suited to predict the medial force ratio throughout the whole stance phase or medial force during the early stance phase [77]. However, KAM was not sufficient to predict joint loading at the end of the stance, where external KAM contributed substantially to the loading, especially in early OA [78, 79]. Some findings suggested that the KCF predicted by a novel musculoskeletal simulation routine provides a more helpful metric than the KAM [75]. Lerner et al. [80] found that each 1° of TF alignment deviation altered the first peak medial KCF by 51 N, whilst each 1 mm of medial-lateral translation of the compartment contact point position altered the first peak medial KCF by 41 N. KCF can be used to identify early knee OA development prior to the onset of radiographic evidences [81]. However, currently, the tolerance of the in vivo joint cartilage to stress and the relationship between joint loading and the osteoarthritis pain and disease progression remain in dispute, which induces a challenge for determining appropriate loading for any individual.
Some studies analyzed the biomechanical effects of varus knee deformity on the stress distribution in the articular cartilage. Martay et al. [82] supposed the contact stresses on the medial compartment were already “too high” for HTO patients, and it was necessary to decrease the medial contact stresses and maintain relatively lower lateral contact stresses to avoid damaging the lateral tissues. They proposed correcting the weight-bearing axis to 55% tibial width (1.7°–1.9° valgus) optimally distributes medial and lateral contact stresses [82]. Nakayama et al. [83] found a large amount of correction in OWHTO with a resultant joint-line obliquity of 5° or more may induce excessive shear stress to the articular cartilage. Zheng et al. [84] also found that balanced loading occurred at angles of 4.3° and 2.9° valgus for the femoral and tibial cartilage, respectively. The study of Trad et al. [85] suggested that a balanced stress distribution between two compartments was achieved under a valgus hypercorrection angle of 4.5. The main conclusions of current relative studies are shown in Table 5. However, there are quite a few research studies related to the influence of limb alignment on medial-lateral loading and the effect of axis correction angle on stress distribution on the tibial plateau after HTO. How much the contact stresses on medial compartment cartilage should be reduced to prevent progression is still unknown, while what a threshold is beyond resulting in increasing contact stresses on lateral compartment also is unclear.
Table 5.
Knee contact mechanics of HTO.
| Year | Author | Data | Conclusion | Limitation | |
|---|---|---|---|---|---|
| 2017 | Nakayama et al. [83] | (1) The 3D bone model was derived from human bone digital anatomy media and only included the distal femur and proximal tibia | (1) The obliquity angle increases laterally directed shear stress (2) An obliquity angle of 5° or more increases shear stress in the medial compartment; the maximum shear stress value in the medial cartilage increased from 1.6 MPa for the normal knee to 3.3, 5.2, and 7.2 MPa in the joint-line obliquity models with 5°, 7.5°, and 10° of obliquity, respectively |
(1) Due to the data source, these results cannot be generalized and applied to all patients with osteoarthritis undergoing osteotomy (2) The knee model used for the FEA omitted meniscus and unfirming the thickness of cartilage to avoid excessive complexity in calculation |
|
|
| |||||
| 2017 | Zheng et al. [84] | (1) MRI data of a healthy participant. (2) Gait analysis and force-platforms data during ten walking trials |
(1) Providing a platform for noninvasive, patient-specific preoperative planning of the osteotomy for medial compartment knee osteoarthritis (2) Balanced loading occurred at angles of 4.3° and 2.9° valgus for the femoral and tibial cartilage, respectively |
(1) Did not consider the whole gait cycle (2) Did not apply muscle forces within their individual lines of action. (3) Simulation on a healthy knee with intact menisci. |
|
|
| |||||
| 2018 | Trad et al. [85] | The 3D model of the right lower limb was extracted from a 3D anonymous human skeleton | (1) The model agreed with the experimental and numerical results (2) By changing the correction angle from 0 to 10 valgus, the von Mises and the shear stresses decreased in the medial compartment and increased in the lateral compartment (3) A balanced stress distribution between two compartments was achieved under a valgus hypercorrection angle of 4.5 |
(1) The use of the geometry of a knee model artificially created and not the one specifically developed for a pathological knee (2) Without studying the dynamic behavior (3) Neglecting the cancellous bone and the muscle forces (4) All the knee components were considered as linearly homogeneous isotropic material |
|
|
| |||||
| 2018 | Martay et al. [82] | (1) MRI data of three healthy subjects. 2. Marker trajectory data and GRF data during level walking | Correcting the weight-bearing axis to 55% tibial width (1.7°–1.9° valgus) optimally distributes medial and lateral stresses/pressures | (1) Simulation on healthy knees (2) Using simple material behaviors (3) Validating their model creation method using porcine specimens (4) Without studying the dynamic behavior |
|
Some researchers found that knee joint with exposed bone was concluded to be partially or entirely covered by newly regenerated cartilage after HTO [86, 87]. However, one study reported no significant differences in terms of the ratio of cartilage repair in the medial compartment of the tibiofemoral joint between the overcorrected knees and corrected knees after OWHTO [45]. It is unclear whether the “safety corrective range” or the golden standard for the OA exists. The effect of excessive stress on soft-tissue wear or repair and the remodeling process after corrective osteotomy is still unknown. There remains a lack of quantitative research about the change in knee contact mechanics of HTO.
7. Research Method
Gait analysis, musculoskeletal modelling, and finite element analysis (FEA) are the main research methods for investigating the biomechanics of HTO in the above-mentioned study. Joint kinematics can be mainly measured using two techniques. In vivo joint kinematics and gait pattern are most commonly determined using a marker-based 3D motion-capture system during walking, stair ascent, and squat activities [71, 88]. But the subjects with high BMI are not suitable for this technology because soft-tissue motion relative to bony landmarks can introduce errors [89]. Dual fluoroscopy is more accurate with excellent precision than marker-based 3D motion capture [90–92]. Dual fluoroscopy captures 3D joint kinematics by registering 3D surface reconstructions to the 2D images acquired using fluoroscopes. The primary disadvantages of this technique are the technical challenge and radiation exposure. In spite of existing limitations, both techniques provided an approach to investigate a subject's gait pattern and in vivo joint kinematics of HTO.
An array of available musculoskeletal modelling software, for example, Anybody [89] and OpenSim [93], has been used to obtain in vivo biomechanics of the human body. The kinematical data from gait analysis was the important input condition for inverse kinematic analysis and inverse dynamics analysis of the musculoskeletal multibody dynamics model. Musculoskeletal models could estimate subject's muscles forces, joint moments, and joint reaction forces as well as joint kinematics by solving the muscle redundancy problem. The biomechanics information of joint loading and motion were the vital boundary condition of FEA. The musculoskeletal modelling method would afford a wealth of understanding on the influence of gait patterns on muscles and joint force magnitudes, a strong platform of quantifying the biomechanics of HTO. Hu et al. [94] and Chen et al. [3] investigated the biomechanics of the natural knee joint and total knee replacement using subject-specific musculoskeletal multibody dynamics models. Therefore, the musculoskeletal modelling method is easily used to investigate the biomechanics of HTO under musculoskeletal dynamics environment.
FEA of joint contact mechanics has already provided insight into the mechanical causes of OA [7]. Subject-specific FEA of joint contact mechanics also provides noninvasive, patient-specific recommendations of HTO correction angle. But few studies have investigated the effect of HTO correction angle on the stress distribution of the articular cartilage in the knee joint [82–85]. Zheng et al. [84] introduced a platform for noninvasive, patient-specific preoperative planning of the osteotomy for medial knee osteoarthritis using CAD and FEA. Multiobjective optimization could be used to identify the final alignment that balanced medial-lateral compressive and shear forces. However, limitations of simple materials' parameters for intact cartilage or meniscus were adopted in all the aforementioned studies. Saarakkala. et al. [95] found that maximum principal stresses and strains within the articular cartilage of the knee joint during walking are highly sensitive to the material parameters of the cartilage. However, the biphasic mechanics of the articular cartilage was rarely considered in FEA of HTO. The study of Meng et al. [96] took into account the complex biphasic contact interactions of the cartilage and menisci to characterize the time-dependent contact behavior of the tibiofemoral joint under body weight. Furthermore, most FE models only applied static loading and omitted joint kinetics during motion. Because many orthopedic pathologies altered the joint motion and force, those changes should be incorporated into the FE model as accurately as possible [7]. In the future, with the advantages of gait analysis, musculoskeletal modelling, and FEA, the “safety corrective range” of HTO can be determined.
8. Conclusion
The patient's gait pattern after HTO is modified based on the limb alignment, which would further influence the knee adduction moment and medial-lateral contact forces and consequently the contact stresses of the cartilage on the medial-lateral compartments of the tibiofemoral joint. Biomechanical environment of HTO is crucial for understanding the complications of HTO, and improving surgical accuracy. However, biomechanical studies on HTO are still insufficient on gait analysis, joint kinematics, and joint contact mechanics. The biomechanical relationships between the alignment and plate breakage, cartilage degeneration, nonunion, and others are still unclear. The “safety corrective range” is still unknown. Integration of gait analysis, musculoskeletal dynamics modelling, and FEA will help comprehensively understand in vivo patient-specific biomechanics information of HTO.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (51323007, 51775460, and 51508031), the Natural Science Foundation of Shaanxi Province of China (2017M5020 and 2018JQ5064), and the Fundamental Research Funds for the Central Universities (300102258501 and 300102258202).
Conflicts of Interest
The authors declare that there are no conflicts of interest.
References
- 1.Kutzner I., Heinlein B., Graichen F., et al. Loading of the knee joint during activities of daily living measured in vivo in five subjects. Journal of Biomechanics. 2010;43(11):2164–2173. doi: 10.1016/j.jbiomech.2010.03.046. [DOI] [PubMed] [Google Scholar]
- 2.Fraysse F., Arnold J., Thewlis D. A method for concise reporting of joint reaction forces orientation during gait. Journal of Biomechanics. 2016;49(14):3538–3542. doi: 10.1016/j.jbiomech.2016.08.005. [DOI] [PubMed] [Google Scholar]
- 3.Chen Z., Zhang X., Ardestani M. M., et al. Prediction of in vivo joint mechanics of an artificial knee implant using rigid multi-body dynamics with elastic contacts. Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine. 2014;228(6):564–575. doi: 10.1177/0954411914537476. [DOI] [PubMed] [Google Scholar]
- 4.Jin P. M., Holloway E. S. The young osteoarthritic knee: dilemmas in management. BMC Medicine. 2013;11(1):p. 14. doi: 10.1186/1741-7015-11-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pereira D., Ramos E., Branco J. Osteoarthritis. Acta Médica Portuguesa. 2014;28(1):99–106. doi: 10.20344/amp.5477. [DOI] [PubMed] [Google Scholar]
- 6.Abramson S. B., Attur M. Developments in the scientific understanding of osteoarthritis. Arthritis Research & Therapy. 2009;11(3):p. 227. doi: 10.1186/ar2655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Henak C. R., Anderson A. E., Weiss J. A. Subject-specific analysis of joint contact mechanics: application to the study of osteoarthritis and surgical planning. Journal of Biomechanical Engineering. 2013;135(2) doi: 10.1115/1.4023386.021003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mina C., Garrett W. E., Jr., Pietrobon R., Glisson R., Higgins L. High tibial osteotomy for unloading osteochondral defects in the medial compartment of the knee. The American Journal of Sports Medicine. 2008;36(5):949–955. doi: 10.1177/0363546508315471. [DOI] [PubMed] [Google Scholar]
- 9.Messner K., Maletius W. The long-term prognosis for severe damage to weight-bearing cartilage in the knee: a 14-year clinical and radiographic follow-up in 28 young athletes. Acta Orthopaedica Scandinavica. 1996;67(2):165–168. doi: 10.3109/17453679608994664. [DOI] [PubMed] [Google Scholar]
- 10.Morin V., Pailhe R., Duval B. R., et al. Gait analysis following medial opening-wedge high tibial osteotomy. Knee Surgery, Sports Traumatology, Arthroscopy. 2017;26(6):1838–1844. doi: 10.1007/s00167-017-4421-1. [DOI] [PubMed] [Google Scholar]
- 11.Reeves N. D., Bowling F. L. Conservative biomechanical strategies for knee osteoarthritis. Nature Reviews Rheumatology. 2011;7(2):113–122. doi: 10.1038/nrrheum.2010.212. [DOI] [PubMed] [Google Scholar]
- 12.Mine K., Nakayama T., Milanese S., Grimmer K. The effectiveness of braces and orthoses for patients with knee osteoarthritis: a systematic review of Japanese-language randomised controlled trials. Prosthetics and Orthotics International. 2017;41(2):115–126. doi: 10.1177/0309364616640926. [DOI] [PubMed] [Google Scholar]
- 13.Duivenvoorden T., Brouwer R. W., van Raaij T. M., Verhagen A. P., Verhaar J. A., Bierma-Zeinstra S. M. Braces and orthoses for treating osteoarthritis of the knee. Cochrane Database of Systematic Reviews. 2015;125(1) doi: 10.1002/14651858.cd004020.pub3.CD004020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Takeuchi R., Umemoto Y., Aratake M., et al. A mid term comparison of open wedge high tibial osteotomy vs unicompartmental knee arthroplasty for medial compartment osteoarthritis of the knee. Journal of Orthopaedic Surgery and Research. 2010;5(1):p. 65. doi: 10.1186/1749-799x-5-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Saito S., Gouttebarge V., Kuijer P. P. F. M., van Geenen R. C. I., Poolman R. W., Kerkhoffs G. M. M. J. Return to sports and physical activity after total and unicondylar knee arthroplasty: a systematic review and meta-analysis. Sports Medicine. 2016;46(2):269–292. doi: 10.1007/s40279-015-0421-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cao Z., Mai X., Wang J., Feng E., Huang Y. Unicompartmental knee arthroplasty vs high tibial osteotomy for knee osteoarthritis: a systematic review and meta-analysis. Journal of Arthroplasty. 2017;33(3):952–959. doi: 10.1016/j.arth.2017.10.025. [DOI] [PubMed] [Google Scholar]
- 17.Jeon Y. S., Ahn C. H., Kim M. K. Comparison of HTO with articular cartilage surgery and UKA in unicompartmental OA. Journal of Orthopaedic Surgery. 2017;25(1) doi: 10.1177/2309499016684092.2309499016684092 [DOI] [PubMed] [Google Scholar]
- 18.Santoso M. B., Wu L. Unicompartmental knee arthroplasty, is it superior to high tibial osteotomy in treating unicompartmental osteoarthritis? A meta-analysis and systemic review. Journal of Orthopaedic Surgery and Research. 2017;12(1):p. 50. doi: 10.1186/s13018-017-0552-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sun H., Zhou L., Li F., Duan J. Comparison between closing-wedge and opening-wedge high tibial osteotomy in patients with medial knee osteoarthritis: a systematic review and meta-analysis. The Journal of Knee Surgery. 2017;30(2):158–165. doi: 10.1055/s-0036-1584189. [DOI] [PubMed] [Google Scholar]
- 20.Dettoni F., Bonasia D. E., Castoldi F., Bruzzone M., Blonna D., Rossi R. High tibial osteotomy versus unicompartmental knee arthroplasty for medial compartment arthrosis of the knee a review of the literature. Iowa Orthopaedic Journal. 2010;30:131–140. [PMC free article] [PubMed] [Google Scholar]
- 21.Hoorntje A., Witjes S., Kuijer P. P. F. M., et al. High rates of return to sports activities and work after osteotomies around the knee: a systematic review and meta-analysis. Sports Medicine. 2017;47(11):2219–2244. doi: 10.1007/s40279-017-0726-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Aglietti P., Rinonapoli E., Stringa G., Taviani A. Tibial osteotomy for the varus osteoarthritic knee. Clinical Orthopaedics and Related Research. 1983;(176):239–251. doi: 10.1097/00003086-198306000-00035. [DOI] [PubMed] [Google Scholar]
- 23.Amendola A., Bonasia D. E. Results of high tibial osteotomy: review of the literature. International Orthopaedics. 2010;34(2):155–160. doi: 10.1007/s00264-009-0889-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Osti M., Gohm A., Schlick B., Benedetto K. P. Complication rate following high tibial open-wedge osteotomy with spacer plates for incipient osteoarthritis of the knee with varus malalignment. Knee Surgery, Sports Traumatology, Arthroscopy. 2015;23(7):1943–1948. doi: 10.1007/s00167-013-2757-8. [DOI] [PubMed] [Google Scholar]
- 25.Woodacre T., Ricketts M., Evans J. T., et al. Complications associated with opening wedge high tibial osteotomy—a review of the literature and of 15years of experience. The Knee. 2016;23(2):276–282. doi: 10.1016/j.knee.2015.09.018. [DOI] [PubMed] [Google Scholar]
- 26.Elson D. W., Dawson M., Wilson C., Risebury M., Wilson A. The UK knee osteotomy registry (UKKOR) The Knee. 2015;22(1):1–3. doi: 10.1016/j.knee.2014.10.004. [DOI] [PubMed] [Google Scholar]
- 27.Prodromos C. C., Amendola A., Jakob R. P. High tibial osteotomy: indications, techniques, and postoperative management. Instructional Course Lectures. 2015;64:555–565. [PubMed] [Google Scholar]
- 28.Hui C., Salmon L. J., Kok A., et al. Long-term survival of high tibial osteotomy for medial compartment osteoarthritis of the knee. The American Journal of Sports Medicine. 2011;39(1):64–70. doi: 10.1177/0363546510377445. [DOI] [PubMed] [Google Scholar]
- 29.Schallberger A., Jacobi M., Wahl P., Maestretti G., Jakob R. P. High tibial valgus osteotomy in unicompartmental medial osteoarthritis of the knee: a retrospective follow-up study over 13–21 years. Knee Surgery, Sports Traumatology, Arthroscopy. 2011;19(1):122–127. doi: 10.1007/s00167-010-1256-4. [DOI] [PubMed] [Google Scholar]
- 30.Saragaglia D., Blaysat M., Inman D., Mercier N. Outcome of opening wedge high tibial osteotomy augmented with a biosorb wedge and fixed with a plate and screws in 124 patients with a mean of ten years follow-up. International Orthopaedics. 2011;35(8):1151–1156. doi: 10.1007/s00264-010-1102-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Amis A. A. Biomechanics of high tibial osteotomy. Knee Surgery, Sports Traumatology, Arthroscopy. 2013;21(1):197–205. doi: 10.1007/s00167-012-2122-3. [DOI] [PubMed] [Google Scholar]
- 32.Uquillas C., Rossy W., Nathasingh C. K., Strauss E., Jazrawi L., Gonzalez-Lomas G. Osteotomies about the knee. The Journal of Bone and Joint Surgery-American Volume. 2014;96(24):p. e199. doi: 10.2106/jbjs.n.00270. [DOI] [PubMed] [Google Scholar]
- 33.Bellemans J., Colyn W., Vandenneucker H., Victor J. The Chitranjan ranawat award: is neutral mechanical alignment normal for all patients?: the concept of constitutional varus. Clinical Orthopaedics and Related Research. 2012;470(1):45–53. doi: 10.1007/s11999-011-1936-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Schipplein O. D., Andriacchi T. P. Interaction between active and passive knee stabilizers during level walking. Journal of Orthopaedic Research. 1991;9(1):113–119. doi: 10.1002/jor.1100090114. [DOI] [PubMed] [Google Scholar]
- 35.Andriacchi A., Kutzner I., Graichen F., Heinlein B., Beier A., Bergmann G. Influence of limb alignment on mediolateral loading in total knee replacement. The Journal of Bone and Joint Surgery-American Volume. 2012;94(11):1023–1029. doi: 10.2106/jbjs.k.00927. [DOI] [PubMed] [Google Scholar]
- 36.Dugdale T. W., Noyes F. R., Styer D. Preoperative planning for high tibial osteotomy. The effect of lateral tibiofemoral separation and tibiofemoral length. Clinical Orthopaedics and Related Research. 1992;(274):248–264. doi: 10.1097/00003086-199201000-00025. [DOI] [PubMed] [Google Scholar]
- 37.Bergmann G., Klinger H., Harth P., Hofmann G. Knorpelregeneration nach valgisierender tibiakopfosteotomie. Ergebnisse einer arthroskopischen studie. Zeitschrift für Orthopädie und Unfallchirurgie. 2012;150(3):272–279. doi: 10.1055/s-0031-1298388. [DOI] [PubMed] [Google Scholar]
- 38.Kutzner I., Bender A., Graichen F., et al. Mediolateral force distribution at the knee joint shifts across activities and is driven by tibiofemoral alignment. The Bone & Joint Journal. 2017;99(6):779–787. doi: 10.1302/0301-620x.99b6.bjj-2016-0713.r1. [DOI] [PubMed] [Google Scholar]
- 39.Black M. S., d’Entremont A. G., McCormack R. G., Hansen G., Carr D., Wilson D. R. The effect of wedge and tibial slope angles on knee contact pressure and kinematics following medial opening-wedge high tibial osteotomy. Clinical Biomechanics. 2017;51:17–25. doi: 10.1016/j.clinbiomech.2017.10.021. [DOI] [PubMed] [Google Scholar]
- 40.Song S. J., Bae D. K. Computer-assisted navigation in high tibial osteotomy. Clinics in Orthopedic Surgery. 2016;8(4):349–357. doi: 10.4055/cios.2016.8.4.349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Fujisawa Y., Masuhara K., Shiomi S. The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. The Orthopedic Clinics of North America. 1979;10(3):585–608. [PubMed] [Google Scholar]
- 42.Coventry M. B., Ilstrup D. M., Wallrichs S. L. Proximal tibial osteotomy. A critical long-term study of eighty-seven cases. The Journal of Bone & Joint Surgery. 1993;75(2):196–201. doi: 10.2106/00004623-199302000-00006. [DOI] [PubMed] [Google Scholar]
- 43.Hernigou P., Medevielle D., Debeyre J., Goutallier D. Proximal tibial osteotomy for osteoarthritis with varus deformity. A ten to thirteen-year follow-up study. The Journal of Bone & Joint Surgery. 1987;69(3):332–354. doi: 10.2106/00004623-198769030-00005. [DOI] [PubMed] [Google Scholar]
- 44.Antonescu D. N. Is knee osteotomy still indicated in knee osteoarthritis? Acta Orthopaedica Belgica. 2000;66(5):421–432. [PubMed] [Google Scholar]
- 45.Tsukada S., Wakui M. Is overcorrection preferable for repair of degenerated articular cartilage after open-wedge high tibial osteotomy? Knee Surgery, Sports Traumatology, Arthroscopy. 2017;25(3):785–792. doi: 10.1007/s00167-015-3655-z. [DOI] [PubMed] [Google Scholar]
- 46.Saveh A. H., Kazemi S. M., Zali A. R., et al. The plane radiograph of the knee for high tibial osteotomy assessment is in contrast to standing alignment virtually elaborated handling based pre-operation planning. Biomedical Engineering: Applications, Basis and Communications. 2017;29(1) doi: 10.4015/s1016237217500016.1750001 [DOI] [Google Scholar]
- 47.Gammada H. J., Park J., Shin J. Y., Park I. H., Park K. H., Kyung H. S. More accurate correction can be obtained using a three-dimensional printed model in open-wedge high tibial osteotomy. Knee Surgery, Sports Traumatology, Arthroscopy. 2018;26(11):3452–3458. doi: 10.1007/s00167-018-4927-1. [DOI] [PubMed] [Google Scholar]
- 48.Specogna A. V., Birmingham T. B., Hunt M. A., et al. Radiographic measures of knee alignment in patients with varus gonarthrosis. The American Journal of Sports Medicine. 2007;35(1):65–70. doi: 10.1177/0363546506293024. [DOI] [PubMed] [Google Scholar]
- 49.Winter A., Ferguson K., Syme B., McMillan J., Holt G. Pre-operative analysis of lower limb coronal alignment—a comparison of supine MRI versus standing full-length alignment radiographs. The Knee. 2014;21(6):1084–1087. doi: 10.1016/j.knee.2014.05.001. [DOI] [PubMed] [Google Scholar]
- 50.Duivenvoorden T., Brouwer R. W., Baan A., et al. Comparison of closing-wedge and opening-wedge high tibial osteotomy for medial compartment osteoarthritis of the knee. The Journal of Bone and Joint Surgery-American Volume. 2014;96(17):1425–1432. doi: 10.2106/jbjs.m.00786. [DOI] [PubMed] [Google Scholar]
- 51.Van Egmond N., van Grinsven S., van Loon C. J. M., Gaasbeek R. D., van Kampen A. Better clinical results after closed- compared to open-wedge high tibial osteotomy in patients with medial knee osteoarthritis and varus leg alignment. Knee Surgery, Sports Traumatology, Arthroscopy. 2016;24(1):34–41. doi: 10.1007/s00167-014-3303-z. [DOI] [PubMed] [Google Scholar]
- 52.Deie M., Hoso T., Shimada N., et al. Differences between opening versus closing high tibial osteotomy on clinical outcomes and gait analysis. The Knee. 2014;21(6):1046–1051. doi: 10.1016/j.knee.2014.04.007. [DOI] [PubMed] [Google Scholar]
- 53.Duivenvoorden T., van Diggele P., Reijman M., et al. Adverse events and survival after closing- and opening-wedge high tibial osteotomy: a comparative study of 412 patients. Knee Surgery, Sports Traumatology, Arthroscopy. 2015;25(3):895–901. doi: 10.1007/s00167-015-3644-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Wu L., Lin J., Jin Z., Cai X., Gao W. Comparison of clinical and radiological outcomes between opening-wedge and closing-wedge high tibial osteotomy: a comprehensive meta-analysis. PLoS One. 2017;12(2) doi: 10.1371/journal.pone.0171700.e0171700 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Lee O. S., Ahn S., Lee Y. S. Comparison of the leg-length change between opening- and closing-wedge high tibial osteotomy: a systematic review and meta-analysis. The Journal of Knee Surgery. 2018;32(4):372–379. doi: 10.1055/s-0038-1641176. [DOI] [PubMed] [Google Scholar]
- 56.Kim J. H., Kim H. J., Lee D. H. Survival of opening versus closing wedge high tibial osteotomy: a meta-analysis. Scientific Reports. 2017;7(1):p. 7296. doi: 10.1038/s41598-017-07856-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Zorzi A. R., da Silva H. G. P. V., Muszkat C., Marques L. C., Cliquet Jr A., Jr., de Miranda J. B. Opening-wedge high tibial osteotomy with and without bone graft. Artificial Organs. 2011;35(3):301–307. doi: 10.1111/j.1525-1594.2010.01058.x. [DOI] [PubMed] [Google Scholar]
- 58.Prodromos C. C., Andriacchi T. P., Galante J. O. A relationship between gait and clinical changes following high tibial osteotomy. The Journal of Bone & Joint Surgery. 1985;67(8):1188–1194. doi: 10.2106/00004623-198567080-00007. [DOI] [PubMed] [Google Scholar]
- 59.Galante S., Shibakawa A., Takizawa T., Yamazaki I., Horiuchi H. The long-term outcome of high tibial osteotomy. The Journal of Bone and Joint Surgery. British Volume. 2008;90(5):592–596. doi: 10.1302/0301-620x.90b5.20386. [DOI] [PubMed] [Google Scholar]
- 60.Diffo Kaze A., Maas S., Belsey J., Hoffmann A., Pape D. Static and fatigue strength of a novel anatomically contoured implant compared to five current open-wedge high tibial osteotomy plates. Journal of Experimental Orthopaedics. 2017;4(1):p. 39. doi: 10.1186/s40634-017-0115-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Chu-An Luo S.-Y. H., Lin S.-C., Chen C.-M., Tseng C.-S. Stress and stability comparison between different systems for high tibial osteotomies. BMC Musculoskeletal Disorders. 2013;14(1):2–8. doi: 10.1186/1471-2474-14-110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Luo C. A., Hwa S. Y., Lin S. C., Chen C. M., Tseng C. S. Placement-induced effects on high tibial osteotomized construct-biomechanical tests and finite-element analyses. BMC Musculoskeletal Disorders. 2015;16:p. 235. doi: 10.1186/s12891-015-0630-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Weng P.-W., Chen C.-H., Luo C.-A., et al. The effects of tibia profile, distraction angle, and knee load on wedge instability and hinge fracture: a finite element study. Medical Engineering & Physics. 2017;42:48–54. doi: 10.1016/j.medengphy.2017.01.007. [DOI] [PubMed] [Google Scholar]
- 64.Kaze A.D., Maas S., Hoffmann A., Pape D. Mechanical strength assessment of a drilled hole in the contralateral cortex at the end of the open wedge for high tibial osteotomy. Journal of Experimental Orthopaedics. 2017;4(1):p. 23. doi: 10.1186/s40634-017-0098-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Bujnowski K., Getgood A., Farr J., Dunning C., Burkhart T. A. A pilot hole does not reduce the strains or risk of fracture to the lateral cortex during and following a medial opening wedge high tibial osteotomy in cadaveric specimens. Bone & Joint Research. 2018;7(2):166–172. doi: 10.1302/2046-3758.72.bjr-2017-0337.r1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Kaze A.D., Maas S., Waldmann D., Zilian A., Dueck K., Pape D. Biomechanical properties of five different currently used implants for open-wedge high tibial osteotomy. Journal of Experimental Orthopaedics. 2015;2(1):p. 14. doi: 10.1186/s40634-015-0030-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Yoo O. S., Lee Y. S., Lee M. C., Park J. H., Kim J. W., Sun D. H. Morphologic analysis of the proximal tibia after open wedge high tibial osteotomy for proper plate fitting. BMC Musculoskeletal Disorders. 2016;17(1):p. 423. doi: 10.1186/s12891-016-1277-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Lind M., McClelland J., Wittwer J. E., Whitehead T. S., Feller J. A., Webster K. E. Gait analysis of walking before and after medial opening wedge high tibial osteotomy. Knee Surgery, Sports Traumatology, Arthroscopy. 2013;21(1):74–81. doi: 10.1007/s00167-011-1496-y. [DOI] [PubMed] [Google Scholar]
- 69.Kim Y. H., Dorj A., Han A., Kim K., Nha K. W. Improvements in spinal alignment after high tibial osteotomy in patients with medial compartment knee osteoarthritis. Gait & Posture. 2016;48:131–136. doi: 10.1016/j.gaitpost.2016.05.001. [DOI] [PubMed] [Google Scholar]
- 70.Leitch K. M., Birmingham T. B., Dunning C. E., Giffin J. R. Medial opening wedge high tibial osteotomy alters knee moments in multiple planes during walking and stair ascent. Gait & Posture. 2015;42(2):165–171. doi: 10.1016/j.gaitpost.2015.05.005. [DOI] [PubMed] [Google Scholar]
- 71.Marriott K., Birmingham T. B., Kean C. O., Hui C., Jenkyn T. R., Giffin J. R. Five-year changes in gait biomechanics after concomitant high tibial osteotomy and ACL reconstruction in patients with medial knee osteoarthritis. The American Journal of Sports Medicine. 2015;43(9):2277–2285. doi: 10.1177/0363546515591995. [DOI] [PubMed] [Google Scholar]
- 72.da Silva H., Zorzi A. R., da Silva H. P. V., de Miranda J. B. Gait analysis in short-term follow-up of medial opening wedge high tibial osteotomy. European Journal of Orthopaedic Surgery & Traumatology. 2017;28(5):939–946. doi: 10.1007/s00590-017-2099-1. [DOI] [PubMed] [Google Scholar]
- 73.Birmingham T. B., Giffin J. R., Chesworth B. M., et al. Medial opening wedge high tibial osteotomy: a prospective cohort study of gait, radiographic, and patient-reported outcomes. Arthritis & Rheumatism. 2009;61(5):648–657. doi: 10.1002/art.24466. [DOI] [PubMed] [Google Scholar]
- 74.Sritharan P., Lin Y.-C., Pandy M. G. Muscles that do not cross the knee contribute to the knee adduction moment and tibiofemoral compartment loading during gait. Journal of Orthopaedic Research. 2012;30(10):1586–1595. doi: 10.1002/jor.22082. [DOI] [PubMed] [Google Scholar]
- 75.Meyer A. J., D’Lima D. D., Besier T. F., Lloyd D. G., Colwell C. W., Jr., Fregly B. J. Are external knee load and EMG measures accurate indicators of internal knee contact forces during gait? Journal of Orthopaedic Research. 2013;31(6):921–929. doi: 10.1002/jor.22304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Bhatnagar T., Jenkyn T. R. Internal kinetic changes in the knee due to high tibial osteotomy are well-correlated with change in external adduction moment: an osteoarthritic knee model. Journal of Biomechanics. 2010;43(12):2261–2266. doi: 10.1016/j.jbiomech.2010.05.001. [DOI] [PubMed] [Google Scholar]
- 77.Kutzner I., Trepczynski A., Heller M. O., Bergmann G. Knee adduction moment and medial contact force - facts about their correlation during gait. PLoS One. 2013;8(12) doi: 10.1371/journal.pone.0081036.e81036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Meireles S., De Groote F., Reeves N. D., et al. Knee contact forces are not altered in early knee osteoarthritis. Gait & Posture. 2016;45:115–120. doi: 10.1016/j.gaitpost.2016.01.016. [DOI] [PubMed] [Google Scholar]
- 79.Richards R. E., Andersen M. S., Harlaar J., van den Noort J. C. Relationship between knee joint contact forces and external knee joint moments in patients with medial knee osteoarthritis: effects of gait modifications. Osteoarthritis and Cartilage. 2018;26(9):1203–1214. doi: 10.1016/j.joca.2018.04.011. [DOI] [PubMed] [Google Scholar]
- 80.Lerner Z. F., DeMers M. S., Delp S. L., Browning R. C. How tibiofemoral alignment and contact locations affect predictions of medial and lateral tibiofemoral contact forces. Journal of Biomechanics. 2015;48(4):644–650. doi: 10.1016/j.jbiomech.2014.12.049. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Meireles S., Wesseling M., Smith C. R., Thelen D. G., Verschueren S., Jonkers I. Medial knee loading is altered in subjects with early osteoarthritis during gait but not during step-up-and-over task. PLoS One. 2017;12(11) doi: 10.1371/journal.pone.0187583.e0187583 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Martay J. L., Palmer A. J., Bangerter N. K., et al. A preliminary modeling investigation into the safe correction zone for high tibial osteotomy. The Knee. 2018;25(2):286–295. doi: 10.1016/j.knee.2017.12.006. [DOI] [PubMed] [Google Scholar]
- 83.Nakayama H., Schroter S., Yamamoto C., et al. Large correction in opening wedge high tibial osteotomy with resultant joint-line obliquity induces excessive shear stress on the articular cartilage. Knee Surgery, Sports Traumatology, Arthroscopy. 2017;26(6):1873–1878. doi: 10.1007/s00167-017-4680-x. [DOI] [PubMed] [Google Scholar]
- 84.Zheng K., Scholes C. J., Chen J., Parker D., Li Q. Multiobjective optimization of cartilage stress for non-invasive, patient-specific recommendations of high tibial osteotomy correction angle—a novel method to investigate alignment correction. Medical Engineering & Physics. 2017;42:26–34. doi: 10.1016/j.medengphy.2016.11.013. [DOI] [PubMed] [Google Scholar]
- 85.Trad Z., Barkaoui A., Chafra M., Tavares J. M. R. Finite element analysis of the effect of high tibial osteotomy correction angle on articular cartilage loading. Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine. 2018;232(6):553–564. doi: 10.1177/0954411918770706. [DOI] [PubMed] [Google Scholar]
- 86.Okahashi K., Fujisawa Y., Sugimoto K., Tanaka Y. Cartilage regeneration of knee oa after high tibial osteotomy. Techniques in Knee Surgery. 2010;9(2):95–100. doi: 10.1097/btk.0b013e3181e0a0b0. [DOI] [Google Scholar]
- 87.Koshino T., Wada S., Ara Y., Saito T. Regeneration of degenerated articular cartilage after high tibial valgus osteotomy for medial compartmental osteoarthritis of the knee. The Knee. 2003;10(3):229–236. doi: 10.1016/s0968-0160(03)00005-x. [DOI] [PubMed] [Google Scholar]
- 88.Saito B. J., Besier T. F., Lloyd D. G., et al. Grand challenge competition to predict in vivo knee loads. Journal of Orthopaedic Research. 2012;30(4):503–513. doi: 10.1002/jor.22023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Damsgaard M., Rasmussen J., Christensen S. T., Surma E., de Zee M. Analysis of musculoskeletal systems in the anybody modeling system. Simulation Modelling Practice and Theory. 2006;14(8):1100–1111. doi: 10.1016/j.simpat.2006.09.001. [DOI] [Google Scholar]
- 90.Akbarshahi M., Fernandez J. W., Schache A. G., Pandy M. G. Subject-specific evaluation of patellofemoral joint biomechanics during functional activity. Medical Engineering & Physics. 2014;36(9):1122–1133. doi: 10.1016/j.medengphy.2014.06.009. [DOI] [PubMed] [Google Scholar]
- 91.Saveh A. H., Katouzian H. R., Chizari M. Measurement of an intact knee kinematics using gait and fluoroscopic analysis. Knee Surgery, Sports Traumatology, Arthroscopy. 2011;19(2):267–272. doi: 10.1007/s00167-010-1190-5. [DOI] [PubMed] [Google Scholar]
- 92.Papaioannou G., Nianios G., Mitrogiannis C., Fyhrie D., Tashman S., Yang K. H. Patient-specific knee joint finite element model validation with high-accuracy kinematics from biplane dynamic Roentgen stereogrammetric analysis. Journal of Biomechanics. 2008;41(12):2633–2638. doi: 10.1016/j.jbiomech.2008.06.027. [DOI] [PubMed] [Google Scholar]
- 93.Delp S. L., Anderson F. C., Arnold A. S., et al. OpenSim: open-source software to create and analyze dynamic simulations of movement. IEEE Transactions on Biomedical Engineering. 2007;54(11):1940–1950. doi: 10.1109/tbme.2007.901024. [DOI] [PubMed] [Google Scholar]
- 94.Hu J., Chen Z., Xin H., Zhang Q., Jin Z. Musculoskeletal multibody dynamics simulation of the contact mechanics and kinematics of a natural knee joint during a walking cycle. Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine. 2018;232(5):508–519. doi: 10.1177/0954411918767695. [DOI] [PubMed] [Google Scholar]
- 95.Saarakkala S., Nieminen M., Korhonen R., Klets O. Subject-Specific Finite Element Modeling of the Knee Joint to Study Osteoarthritis Development and Progression. Oulu, Finland: Universitatis Ouluensis; 2018. Ph.D. dissertation. [Google Scholar]
- 96.Meng Q., Jin Z., Wilcox R., Fisher J. Computational investigation of the time-dependent contact behaviour of the human tibiofemoral joint under body weight. Proceedings of the Institution of Mechanical Engineers, Part H: Journal of Engineering in Medicine. 2014;228(11):1193–1207. doi: 10.1177/0954411914559737. [DOI] [PMC free article] [PubMed] [Google Scholar]