

Abstract
Background
The goal of this study was to evaluate the relationship between body mass index (BMI) and early complications of total hip replacement (THR) and total knee replacement (TKR).
Methods
This is a retrospective study of patients who underwent primary THR and TKR between January 2011 and December 2015. We included patients between 18 and 90 years of age with BMI less than 40 kg/m2 with a minimal postoperative follow-up time of 45 days. The primary outcomes were the presence of infection, mechanical complications (dislocation, fractures, arthrofibrosis, or neuropraxia), and thromboembolic events. Overweight and obesity were defined as a BMI of 25–29.9 kg/m2 and ≥ 30 kg/m2, respectively.
Results
In total 750 patients were included (THR, 268; TKR, 482) with a mean age of 65.0 ± 12.4 years. The percentage of patients with normal weight, overweight, and obesity was 24.9% (n = 187), 41.7% (n = 313), and 33.4% (n = 250), respectively. The early complication rate was 8.9% (95% confidence interval [CI], 7.1% to 11.2%). Infection and mechanical complications were most prevalent. There was no statistically significant relationship between the incidence of complications and BMI (obesity vs. normal weight: hazard ratio [HR], 1.49; 95% CI, 0.72 to 3.06; p = 0.282); however, there was a tendency toward a greater risk of infectious complications in the patients with obesity (HR, 6.08; 95% CI, 0.75 to 49.16; p = 0.090). Patients with diabetes mellitus (DM) had more risk of infectious complications than those without DM (HR, 2.60; 95% CI, 1.00 to 6.79).
Conclusions
There was no statistical relationship between BMI and early complications of THR and TKR. Nonetheless, there was a tendency toward a higher risk of infection in patients with some degree of obesity.
Keywords: Arthroplasty, Complications, Hip, Knee, Obesity
Articular replacement performed in patients with body mass index (BMI) above 30 kg/m2 has shown to be a successful and reproducible procedure with decreased pain and improvement of function and quality of life.1) However, these benefits are affected by the increased risk of perioperative complications.2,3,4,5) Surgery in obese patients is technically challenging and has suboptimal clinical and functional results;6) therefore, there is reluctance of the orthopedic surgeons to perform an elective joint replacement in patients with a high BMI, particularly above 40 kg/m2.
Several authors have described a higher risk of complications in obese patients.7,8,9) For example, Lubbeke et al.7) reported the risk of infection doubled in 9,061 patients with BMI greater than 35 kg/m2 after total hip replacement (THR) and total knee replacement (TKR) during 6.5 years of follow-up. Other studies have reported no difference in the rate of complications.5,10,11,12,13,14,15) Despite these findings, at this point there is no evidence to contraindicate articular replacement in a patient based on BMI.8)
Considering that the evidence in relation to a greater rate of complications related to joint replacement in obese patients is not conclusive, the goal of this study was to evaluate the relation between BMI and early postoperative complications (first 45 days) in patients with overweight or obesity, in comparison to patients with normal weight that underwent TKR and THR.
METHODS
Design and Study Population
We conducted a retrospective study of patients who underwent primary THR and TKR from Institute of Osteoarticular Diseases, Centro Médico Imbanaco in Cali, Colombia between January 1, 2011 and December 31, 2015. The institutional joint replacement registry was reviewed to identify patients with BMI less than 40 kg/m2 and minimal postoperative follow-up time of 45 days. The cases were operated if they had signs and symptoms of severe osteoarthritis. We conducted this study in compliance with the principals of the declaration of Helsinki. The study was approved by Institutional Review Board of Centro Médico Imbanaco (No. IRB00008539). Informed consent was not obtained for retrospective designs.
The patients were operated by three orthopedic surgeons (WS, AE, JCP) with more than 20 years of experience in joint replacement surgery, following a standardized surgical protocol. To evaluate the relationship between BMI and complication rate, patients were classified into three groups according to the BMI categories defined by the World Health Organization: normal weight (≤ 24.9 kg/m2), overweight (25–29.9 kg/m2), and obesity (≥ 30 kg/m2).
Result Variables
The BMI, demographical data, comorbidities, such as hypertension (HT), diabetes, hypothyroidism, pulmonary and cardiovascular diseases, and intra- and postoperative early complication data were gathered from the clinical record. The primary outcomes were the presence of superficial or deep infection, mechanical complications defined as dislocation, fractures, arthrofibrosis or neuropraxia, non-infectious complications of the surgical wound, thromboembolic events and other complications within the following 45 postoperative days. In order to avoid bias in the data collection, a systematic search for complications was done in every case, decreasing the risk of over- or underestimation.
Statistical Analysis
The quantitative variables were described by central tendency (mean, median) and dispersion (standard deviation, interquartile range) measures. The qualitative variables were reported as frequencies and proportions. The incidence rate of early infections was estimated using the Wilson method according to the type of joint replacement with a 95% confidence interval (CI).
To evaluate the relationship between BMI and early complications, a Cox regression model adjusted for confounding variables, such as age, sex, replacement type, diabetes mellitus (DM) and arterial HT, was used. The reference category was the normal weight group. The hazard ratio (HR) and corresponding 95% CI were reported. The Kaplan-Meier method was used to describe the occurrence of complications during the first 45 postoperative days. All analyses were carried out with Stata ver. 13.0 (StataCorp., College Station, TX, USA).
RESULTS
During the study period, 781 procedures were performed, 23 cases were excluded because they did not have a complete documentation of the study variables and eight cases for BMI ≥ 40 kg/m2. Finally, 750 cases were analyzed (THR, 268 cases; TKR, 482 cases) with postoperative follow-up at 45 days. Their average age was 65.0 ± 12.4 years, and 530 (70.7%) were females. The average BMI was 28.0 ± 4.2 kg/m2 at the time of the intervention: 187 (24.9%) had a BMI < 24.9 kg/m2; 313 (41.7%) had a BMI 25 to 29.9 kg/m2; and 250 (33.4%) had a BMI 30 to 39.9 kg/m2. Forty-eight percent (n = 367) of the individuals had been diagnosed with HT and 96 (12.8%) were diabetic. The proportion of cases with DM in normal weight, overweight, and obesity group was 9.1%, 14.7%, and 13.6%, respectively, and the HT percentage was 34.2%, 50.8%, and 58.1%, respectively. The characteristics of the patients according to the type of replacement are described in Table 1.
Table 1. Characteristics of the Patients Undergoing THR or TKR.
| Variable | THR (n = 268) | TKR (n = 482) |
|---|---|---|
| Age (yr) | 60.2 ± 14.6 | 67.6 ± 10.1 |
| Sex | ||
| Female | 165 (61.6) | 365 (75.7) |
| Male | 103 (38.4) | 117 (24.3) |
| BMI (kg/m2) | 26.4 ± 4.0 | 28.9 ± 4.0 |
| ≤ 24.9 | 103 (38.4) | 84 (17.4) |
| 25–29.9 | 109 (40.7) | 204 (42.3) |
| 30–39.9 | 56 (20.9) | 194 (40.2) |
| Comorbidity | ||
| Diabetes mellitus | 29 (10.8) | 67 (13.9) |
| Hypertension | 103 (38.4) | 264 (54.8) |
| Others | 30 (11.1) | 60 (12.4) |
Values are presented as mean ± standard deviation or number (%).
THR: total hip replacement, TKR: total knee replacement, BMI: body mass index.
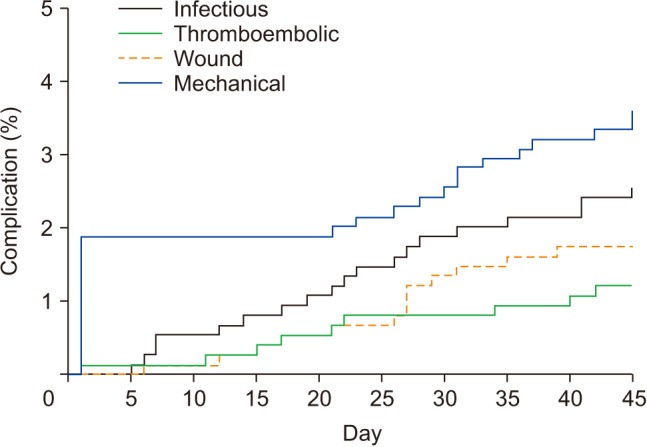
The percentage of early complications was 8.9% and there were no differences between the two types of joint replacement (Table 2). Infectious and mechanical complications were most frequent in this cohort with a percentage of 2.5% and 3.5%, respectively. The patients that underwent THR had a greater incidence of mechanical complications (6.3%), while the group that underwent TKR had a higher risk of infection (3.3%). Fig. 1 describes the occurrence of different complication types over time.
Table 2. Incidence of Early Complications According to the Type of Replacement.
| Complication | Total | THR | TKR |
|---|---|---|---|
| Total | 8.9 (7.1–11.2) | 8.9 (6.1–12.9) | 8.9 (6.8–11.9) |
| Infectious | 2.5 (1.6–3.9) | 1.1 (3.8–3.2) | 3.3 (2.0–5.2) |
| Wound | 1.7 (1.0–2.9) | 0.4 (0.06–2.1) | 2.5 (1.4–4.2) |
| Thromboembolic | 1.2 (0.6–2.2) | 0.7 (0.2–2.7) | 1.5 (0.7–2.9) |
| Mechanical | 3.5 (2.4–5.1) | 6.3 (3.9–9.9) | 1.9 (1.1–3.7) |
Values are presented as percentage (95% confidence interval).
THR: total hip replacement, TKR: total knee replacement.
Fig. 1. Kaplan-Meier curve for the percentage of complications during postoperative follow-up.
After adjusting for possible confounding variables, no relationship was found between BMI and early complications (Table 3). However, there was a slight tendency of a higher risk of infection in the obese patients: they were six times more likely to have an infection than normal weight patients (p = 0.090). Patients with DM had more risk of infectious complications than those without (HR, 2.60; 95% CI, 1.00 to 6.79).
Table 3. Early Complications According to BMI.
| Complication | BMI | HR* (95% CI) | p-value* |
|---|---|---|---|
| Total | Normal | Reference | |
| Overweight | 1.57 (0.79–3.10) | 0.193 | |
| Obesity | 1.49 (0.72–3.06) | 0.282 | |
| Infectious | Normal | Reference | |
| Overweight | 4.35 (0.53–35.38) | 0.169 | |
| Obesity | 6.08 (0.75–49.16) | 0.090 | |
| Wound | Normal | Reference | |
| Overweight | 2.91 (0.34–24.73) | 0.328 | |
| Obesity | 2.81 (0.32–24.51) | 0.349 | |
| Mechanical | Normal | Reference | |
| Overweight | 0.91 (0.37–2.24) | 0.832 | |
| Obesity | 0.68 (0.23–2.01) | 0.488 |
BMI: body mass index, HR: hazard ratio, CI: confidence interval.
*Adjusted for age, sex, replacement type, and comorbidities.
DISCUSSION
The results of this study suggest that there was no statistical relationship between BMI and early complications in patients who underwent THR and TKR. However, there was a tendency towards a higher risk of postsurgical infection in obese patients; this finding also has been shown in other studies.16,17) The probability of a higher risk of infection in obese patients could be related to the low vascularity and the thick layer of adipose tissue, which makes the surgical approach more challenging and subsequently prolongs the operative time. In addition, there might be an association with abnormal growth factor and hormonal levels.18)
There is a high prevalence of obesity in patients with an indication of elective orthopedic surgery, particularly in those that require TKR. In this study, the results were similar to those reported elsewhere in literature,19) with a frequency of overweight or obesity of 75.1%.
We found a high rate of comorbidities, especially HT and DM; these were more frequent among the patients with higher BMI. Other pathologies, such as rheumatoid arthritis, hypothyroidism, neurological and psychiatric comorbidities and others, did not show any statistical relation with early complications. After adjusting for possible confounding variables, there was an incidence of complications of 8.9% and mortality of 0% at 45 days after the procedure, without any difference between the types of joint replacement; these findings are similar to those in previous studies.20,21)
A higher rate of mechanical complications was observed in the THR group (6.3%): among 17 cases, the most frequent complication was the intraoperative periprosthetic fracture (11 cases), followed by dislocation (three cases) and neuropraxia (three cases). We did not find a relationship between BMI and the development of mechanical complications; multiples studies have shown an increase in the rate of hip dislocation in obese patients.16,22) The incidence of periprosthetic fracture in our study was higher (4.1%) than the estimates by Singh et al.23) who described a rate of 0.7% in 14,065 procedures at 1 year after surgery without differences between obese and nonobese patients.
Similar to other studies, we found a close relationship between the presence of DM and infection risk after THR or TKR. Maradit Kremers et al.24) reported an increased risk of prosthetic joint infections in 20,171 THR or TKR patients with a diagnosis of DM or hyperglycemia (glucose level > 180 mg/dL). However, they found no association between hemoglobin A1c levels and the risk of infection. In patients with DM, there has been a higher risk of postoperative wound infection after TKR (odds ratio, 6.07; 95% CI, 1.12 to 33.0).25) Although the diagnosis of DM has been recognized as a major risk factor for infectious complications, this association has been explained due to a close relationship with obesity and other comorbidities.24,26)
Although based on record review, the main strength of this study is the quality of information, because the follow-up in these patients is part of the routine perioperative care. Because of the close relationship between the incidence of complications with other factors such as age, the presence of diabetes or inflammatory articular disease, statistical methods were used to adjust for these variables and avoid overestimation of the effect of BMI. Prior to joint replacement, all patients with BMI ≥ 40 kg/m2 are treated with a multidisciplinary approach to encourage weight loss including diet, exercise and behavioral modifications according to institutional protocols.
Severe arthrosis is one of the main consequences of obesity. Obese patients with severe arthrosis could benefit from articular replacement and the procedure might be a cost-effective intervention to improve their quality of life. Our results showed THR or TKR in patients with BMI ≤ 29.9 kg/m2 did not increase the complication rate. Therefore, it is important to take preventive measures to decrease the risk of infection and maintain close follow-up after THR or TKR so that these procedures can be conducted in patients with BMI > 30 kg/m2 without increasing the risk of complications.
Further studies with a larger sample size are required to extrapolate these results to patients with morbid obesity and to prove if there is a higher risk of infection and other perioperative complications in this population. The tendency found in our study suggests that there is a relationship between obesity and a higher risk of infection, which we want to be validated in future studies involving a larger sample.
In summary, patients with BMI 25 to 29.9 kg/m2 undergoing THR or TKR do not have a higher risk of complications than patients with normal weight. Nonetheless, there was a tendency toward a higher risk of infection in patients with some degree of obesity (BMI > 30 kg/m2). Therefore, we believe it is necessary to highlight the importance of a close postoperative follow-up, a multidisciplinary treatment for obesity and other preventive measures to decrease the probability of an infectious process, minimizing the risk in patients with BMI > 30 kg/m2. A greater sample size may be required to increase the statistical power in further research due to the low incidence of postoperative complications.
ACKNOWLEDGEMENTS
We appreciate the Research Institute of Centro Médico Imbanaco, Cali, Colombia, for its support during the development of this project.
Footnotes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
References
- 1.Busato A, Roder C, Herren S, Eggli S. Influence of high BMI on functional outcome after total hip arthroplasty. Obes Surg. 2008;18(5):595–600. doi: 10.1007/s11695-007-9412-8. [DOI] [PubMed] [Google Scholar]
- 2.Dowsey MM, Choong PF. Obese diabetic patients are at substantial risk for deep infection after primary TKA. Clin Orthop Relat Res. 2009;467(6):1577–1581. doi: 10.1007/s11999-008-0551-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jain NB, Guller U, Pietrobon R, Bond TK, Higgins LD. Comorbidities increase complication rates in patients having arthroplasty. Clin Orthop Relat Res. 2005;(435):232–238. doi: 10.1097/01.blo.0000156479.97488.a2. [DOI] [PubMed] [Google Scholar]
- 4.Winiarsky R, Barth P, Lotke P. Total knee arthroplasty in morbidly obese patients. J Bone Joint Surg Am. 1998;80(12):1770–1774. doi: 10.2106/00004623-199812000-00006. [DOI] [PubMed] [Google Scholar]
- 5.Suleiman LI, Ortega G, Ong'uti SK, et al. Does BMI affect perioperative complications following total knee and hip arthroplasty? J Surg Res. 2012;174(1):7–11. doi: 10.1016/j.jss.2011.05.057. [DOI] [PubMed] [Google Scholar]
- 6.Wang JL, Gadinsky NE, Yeager AM, Lyman SL, Westrich GH. The increased utilization of operating room time in patients with increased BMI during primary total hip arthroplasty. J Arthroplasty. 2013;28(4):680–683. doi: 10.1016/j.arth.2012.06.037. [DOI] [PubMed] [Google Scholar]
- 7.Lubbeke A, Zingg M, Vu D, et al. Body mass and weight thresholds for increased prosthetic joint infection rates after primary total joint arthroplasty. Acta Orthop. 2016;87(2):132–138. doi: 10.3109/17453674.2015.1126157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Issa K, Harwin SF, Malkani AL, Bonutti PM, Scillia A, Mont MA. Bariatric orthopaedics: total hip arthroplasty in superobese patients (those with a BMI of ≥50 kg/m2) J Bone Joint Surg Am. 2016;98(3):180–185. doi: 10.2106/JBJS.O.00474. [DOI] [PubMed] [Google Scholar]
- 9.Alvi HM, Mednick RE, Krishnan V, Kwasny MJ, Beal MD, Manning DW. The effect of BMI on 30 day outcomes following total joint arthroplasty. J Arthroplasty. 2015;30(7):1113–1117. doi: 10.1016/j.arth.2015.01.049. [DOI] [PubMed] [Google Scholar]
- 10.Wallace G, Judge A, Prieto-Alhambra D, de Vries F, Arden NK, Cooper C. The effect of body mass index on the risk of post-operative complications during the 6 months following total hip replacement or total knee replacement surgery. Osteoarthritis Cartilage. 2014;22(7):918–927. doi: 10.1016/j.joca.2014.04.013. [DOI] [PubMed] [Google Scholar]
- 11.Moran M, Walmsley P, Gray A, Brenkel IJ. Does body mass index affect the early outcome of primary total hip arthroplasty? J Arthroplasty. 2005;20(7):866–869. doi: 10.1016/j.arth.2005.02.008. [DOI] [PubMed] [Google Scholar]
- 12.Patel AD, Albrizio M. Relationship of body mass index to early complications in hip replacement surgery: study performed at Hinchingbrooke Hospital, Orthopaedic Directorate, Huntingdon, Cambridgeshire. Int Orthop. 2007;31(4):439–443. doi: 10.1007/s00264-006-0222-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jiganti JJ, Goldstein WM, Williams CS. A comparison of the perioperative morbidity in total joint arthroplasty in the obese and nonobese patient. Clin Orthop Relat Res. 1993;(289):175–179. [PubMed] [Google Scholar]
- 14.Deshmukh RG, Hayes JH, Pinder IM. Does body weight influence outcome after total knee arthroplasty? A 1-year analysis. J Arthroplasty. 2002;17(3):315–319. doi: 10.1054/arth.2002.30776. [DOI] [PubMed] [Google Scholar]
- 15.Perka C, Arnold U, Buttgereit F. Influencing factors on perioperative morbidity in knee arthroplasty. Clin Orthop Relat Res. 2000;(378):183–191. doi: 10.1097/00003086-200009000-00028. [DOI] [PubMed] [Google Scholar]
- 16.Wagner ER, Kamath AF, Fruth KM, Harmsen WS, Berry DJ. Effect of body mass index on complications and reoperations after total hip arthroplasty. J Bone Joint Surg Am. 2016;98(3):169–179. doi: 10.2106/JBJS.O.00430. [DOI] [PubMed] [Google Scholar]
- 17.Haverkamp D, Klinkenbijl MN, Somford MP, Albers GH, van der Vis HM. Obesity in total hip arthroplasty: does it really matter? A meta-analysis. Acta Orthop. 2011;82(4):417–422. doi: 10.3109/17453674.2011.588859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Felson DT. Weight and osteoarthritis. Am J Clin Nutr. 1996;63(3 Suppl):430S–432S. doi: 10.1093/ajcn/63.3.430. [DOI] [PubMed] [Google Scholar]
- 19.Namba RS, Paxton L, Fithian DC, Stone ML. Obesity and perioperative morbidity in total hip and total knee arthroplasty patients. J Arthroplasty. 2005;20(7 Suppl 3):46–50. doi: 10.1016/j.arth.2005.04.023. [DOI] [PubMed] [Google Scholar]
- 20.Selvan D, Donnelly T, McNicholas M. Management of complications of primary total knee replacement. Orthop Trauma. 2013;27(6):355–363. [Google Scholar]
- 21.Nutt JL, Papanikolaou K, Kellett CF. Complications of total hip arthroplasty. Orthop Trauma. 2013;27(5):272–276. [Google Scholar]
- 22.Liu W, Wahafu T, Cheng M, Cheng T, Zhang Y, Zhang X. The influence of obesity on primary total hip arthroplasty outcomes: a meta-analysis of prospective cohort studies. Orthop Traumatol Surg Res. 2015;101(3):289–296. doi: 10.1016/j.otsr.2015.01.011. [DOI] [PubMed] [Google Scholar]
- 23.Singh JA, Jensen MR, Harmsen SW, Lewallen DG. Are gender, comorbidity, and obesity risk factors for postoperative periprosthetic fractures after primary total hip arthroplasty? J Arthroplasty. 2013;28(1):126–131. doi: 10.1016/j.arth.2012.03.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Maradit Kremers H, Lewallen LW, Mabry TM, Berry DJ, Berbari EF, Osmon DR. Diabetes mellitus, hyperglycemia, hemoglobin A1C and the risk of prosthetic joint infections in total hip and knee arthroplasty. J Arthroplasty. 2015;30(3):439–443. doi: 10.1016/j.arth.2014.10.009. [DOI] [PubMed] [Google Scholar]
- 25.Han HS, Kang SB. Relations between long-term glycemic control and postoperative wound and infectious complications after total knee arthroplasty in type 2 diabetics. Clin Orthop Surg. 2013;5(2):118–123. doi: 10.4055/cios.2013.5.2.118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lenguerrand E, Beswick AD, Whitehouse MR, Wylde V, Blom AW. Outcomes following hip and knee replacement in diabetic versus nondiabetic patients and well versus poorly controlled diabetic patients: a prospective cohort study. Acta Orthop. 2018;89(4):399–405. doi: 10.1080/17453674.2018.1473327. [DOI] [PMC free article] [PubMed] [Google Scholar]