

Abstract
Background
There are many shortcomings in traditional prefabricated rehabilitation insoles for symptomatic flatfoot patients. This study investigated the effects of customized 3-dimensional (3D) printed insoles on pressure and comfort of the plantar foot in symptomatic flatfoot patients.
Material/Methods
Eighty patients with bilateral flatfoot participated in this study. At week 0, patients were randomly assigned into 1 of 2 groups. In the control group, the patients wore standardize shoes with prefabricated insoles; and in the experimental group the patients wore standardize shoes and customized insoles. The Footscan® system recorded peak pressure, peak force, and peak contact area in 10 areas of the sole at weeks 0 and at week 8. Patients used visual analogue scale scores at week 0 and at week 8 to assess overall comfort of insoles.
Results
At week 0, compared with the control group, the peak pressure in the metatarsal was significantly lower in the experimental group (P<0.05) while the peak pressure in the mid-foot was significantly higher than the control group (P<0.05). At week 8, in the experimental group, the peak pressures in the mid-foot were significantly higher than the control group (P<0.05). The comfort scores (measured by pain scale) reported by the experimental group were significantly lower than those reported by the control group (P<0.05).
Conclusions
Customized 3D printed insoles reduced the pressure on the metatarsals by distributed it over the mid-foot area, thus reduced the damage from symptomatic flatfoot. Customized 3D printed insoles were more effective than prefabricated insoles and offered better comfort for patients with symptomatic flatfoot.
MeSH Keywords: Flatfoot; Foot Orthoses; Imaging, Three-Dimensional; Physical and Rehabilitation Medicine
Background
Show insoles play an important part in lower limb rehabilitation [1,2]. According to biomechanical principles, insoles are designed to reduce load and correct deformities. Insoles have been used for the prevention and treatment of foot and lower limb diseases [3]. Some studies have shown that rehabilitation insoles have a positive effect on reducing lesions on the foot and improving walking function [4,5]. The formation of symptomatic flatfoot might be caused by a deformity of the position between the scaphoid and the wedge bone [6]. Patients often complain of fatigue and foot pain after walking, accompanied by knee and ankle pain [7,8]; all of these symptoms greatly reduce a person’s quality of life. The conservative treatment method consists of traditional pre-made insoles. However, there are some shortcomings in traditional rehabilitation insoles for treating flatfoot, including complicated production processes and long production times. Meanwhile, some patients are prone to feelings of inferiority when wearing traditional rehabilitation insoles [9]. Compared to traditional insoles, customized insoles tend to improve the biomechanics of the soles and even the lower extremities. By optimizing the traditional support structure, it can be more suitable for the patient’s plantar structure, thereby reducing damage and improving comfort [10,11]. However, there are currently few studies on customized insoles for patients with flatfoot symptoms, and the number of cases is small [12,13]. Researchers have overlooked the negative effects of inappropriate traditional insoles on patients with flatfoot deformity. Therefore, we decided to study the effect of customized insoles, especially 3-dimensional (3D) printed customized insoles for patients with flatfoot symptoms.
It has been suggested that 3D printing, because of its advantage of fast construction, can meet the huge demand for insoles [14,15]. Some studies have confirmed that it is feasible to make an insole using 3D printing technology [3,4,16], and because each patient’s plantar pressure distribution and contact area are different, the forces will vary. Some studies have suggested that traditional pre-made insoles do not improve motor function and comfort [5,17]. Although there are many applications for 3D printed insoles, few research studies have focused on the flatfoot deformity. Our research aimed to explore the effect of customized 3D printed insoles on the pressure and comfort of the foot in symptomatic flatfoot patients compared to traditional pre-made insoles. The authors hypothesized that patients who use customized insoles will show better plantar pressure distribution and comfort compared with patients using prefabricated insoles.
Material and Methods
General information
From April to October 2018, 90 patients with symptomatic flatfoot participated in this research from the Norman Bethune Second Hospital of Jilin University through outpatient random sampling. Subsequently, 80 patients met the study inclusion criteria. Each patient signed an agreement to participate in the study. The sample number of 80 was chosen because it was similar to related insole experiments [18–23]. Furthermore, our criteria ensured that errors would be minimized for relatively small sample sizes. The research was approved by the Ethics Committee and all participants provided informed consent.
Criteria
The inclusion criteria were as follows: age 26–55 years, history of symptomatic flexible flatfoot (pain over the foot or calf, fatigue after prolonged walking within 5 years, no lower limb treatment, foot posture index (FPI) ranging from 6 to 12, and free movement of the toes). The final 2 factors were evaluated by a physician. The FPI is a clinical diagnostic tool used to classify the foot as supination or normal. The FPI score is an integer between −12 and +12. A foot with an index higher than +6 is called a foot varus and such patients were eligible to participate in this study [24]. Participants were also required to have no history of lower limb injuries or surgeries within the previous 10 months, because lower extremity surgery and injury can affect gait [25–27]. The exclusion criteria were as follows: patients who had undergone arthroplasty and those who had used a foot orthosis in the past year.
Table 1 shows the demographic characteristics of the include patients. The experimental group and the control group had no significant differences in terms of age, body weight, body mass index, wearing time, and FPI (P>0.05). The Visual Analogue Scale (VAS) was used to compare comfort differences between different insoles within groups and between groups at different times.
Table 1.
Demographic characteristics of the participants (N=80).
| Characteristics | Experimental group | Control group | ||
|---|---|---|---|---|
| Mean (SD) | Range | Mean (SD) | Range | |
| Age (years) | 38.61 (7.41) | 26–55 | 41.52 (4.28) | 29–60 |
| Sex | 20 males, 20 females | 20 males, 20 females | ||
| Weight (kg) | 63.37 (12.52) | 48–88 | 67.18 (10.72) | 50–86 |
| BMI (kg/m2) | 26.56 (12.42) | 15.9–29.7 | 25.71 (10.41) | 17.4–28.3 |
| FPI | +7m (2.12) | +6–+8 | +7 (2.61) | +6–+9 |
| Wearing time (hours/day) | 6.7 (2.31) | 4.3–9.7 | 7.1 (3.31) | 5.31–10.72 |
| VA | P values | |||
| 0 week | 7.91 (3.11) | 8.12 (1.21) | 0.87 | |
| 8th week | 2.42 (0.13) | 5.92 (1.19) | 0.03 | |
| P values | 0.01 | 0.25 | ||
SD – standard deviation; BMI – body mass index; FPI – foot posture index; VAS – Visual Analogue Scale.
Study design
This was a single-blind randomized controlled study; an independent therapist (TM) carried out the randomization process. He used a computer-generated table of random numbers (Excel) to finish the groupings. The patients were randomly distributed to either the 3D printed customized insole-wearing group (experimental group) or the prefabricated-insole wearing group (control group). An independent assistant (RX) dealt with the data processing. Assessments were made at week 0 and week 8.
Experimental and control groups
Before the test, there was no significant difference in pain score (VAS) between the experimental group and the control group when walking barefoot (P=0.001). Flat shoes and socks were uniformly purchased by the hospital 1 month before the experiment. All participants wore standardized flat base shoes and standardized cotton socks during the test. The experimental group A wore the following: standardized shoes + customized ethylene vinyl acetate (EVA) insoles. The control group B wore the following: standardized shoes + traditional pre-made rehabilitation insoles.
Customized foot insoles are manufactured by the insole manufacturer (Bodyarch, China). A 0.5 m2 plantar pressure plate-pressure collection device was used to obtain the patient’s foot model. Then we used the Bodyarch Cloud® data analyze system to analyze the data. The Bodyarch X1 Printer® made the 3D printed insoles. Using the EVA material, each insole was cast on the front side. The printed insole and pre-made insole were respectively inserted into the corresponding participant’s shoes at week 0, and the participants were blinded to the insert status. Similar to a previous research study, the study participants were only told that the study aimed to analyze the effects of 2 types of insoles [28], which were considered to have different therapeutic mechanisms. Figure 1 shows the customized insole and the pre-made insole.
Figure 1.

(A) Customized 3D printed insole; (B) prefabricated insole.
Experimental procedures
The Footscan® 7 gait 2nd generation system (RSscan International, Olen, Belgium, 2096×472×18 mm) collected the dynamic parameters of the foot data. The Footscan system has been proven to be a good test for plantar pressure [29,30]. To provide a “full platform” of 4 meters, the platform is located in the center of the floor [31]. Before each measurement, the Footscan® system is calibrated. As described by Xu et al. [30], no walking mat is placed above the flat plate in order to obtain more accurate parameters. In our study, participants were asked to walk through the plate at a normal pace while barefoot so the software could automatically calibrate all parameters. After the correction condition was measured, the plantar pressure data was collected initially (week 0). The experimental and control groups were analyzed at random, in order to minimize potential errors.
We zeroed the system before the first walk test and inserted the insole into the shoe under each test condition. After 3 minutes of acclimatization of standing and walking, the participants completed 3 walks along each 10 m walkway. A stopwatch was used in each test to control walking speed. If the trial was not within 5% of the first walking time, the trial was repeated to minimize the effect of walking speed on plantar pressure [24]. The mean walking speed of all trials was 3.12 (±1.95) km/hour. Once the first plantar pressure was obtained, the insoles and shoes were then provided to the participants and they were asked to wear the insoles during the next 8 weeks.
During the 8 weeks of wearing the insoles, participants were instructed to wear the insoles for a same time period each day (6 to 8 hours per day). Patients didn’t receive other rehabilitation treatment during the 8 weeks of the experiment. Participants returned for a second data collection after 8 weeks. Following the same procedure as in the first data collection, participants were unaware of the specific group information of the week 8 data collection testing.
The VAS was used to assess comfort when wearing insoles [32–34]. VAS is a numerical scale with marked points at 0 and 10, in which 0 indicates no discomfort and 10 indicates the highest level of discomfort. At week 0 and week 8, by putting a vertical mark on the scale representing the level of comfort, patients were requested to score their comfort based on their initial steps (see Table 1.)
Data analysis
Using the Footscan system (Figure 2) to analyze foot parameters, the foot was divided into 10 areas by the software: the big toe (T1), toes 2–5 (T2–T5), the 1st to 5th metatarsal (M1, M2, M3, M4, and M5), medial heel (H1), lateral heel (H2), and mid-foot (MF) (Figure 3). The primary data collected points were the 3 parameters, peak pressure, peak contact area, and peak force, measured in the 10 areas, at week 0 and at week 8 were. We used the Social Science Statistics Program (SPSS) 20th Edition to perform statistical analysis. Paired t-test of variance was used to compare the statistical significance between the experiment group and the control group. We used the independent t-test to compare intergroup difference. In order to reduce the error caused by individual lower limb differences, only the left foot of each participant was selected for evaluation [35]. The statistical significance of the test was set to the conventional level of 0.05.
Figure 2.

The Footscan® system can record the peak value of pressure, force, and contact area in full cycle of gait.
Figure 3.
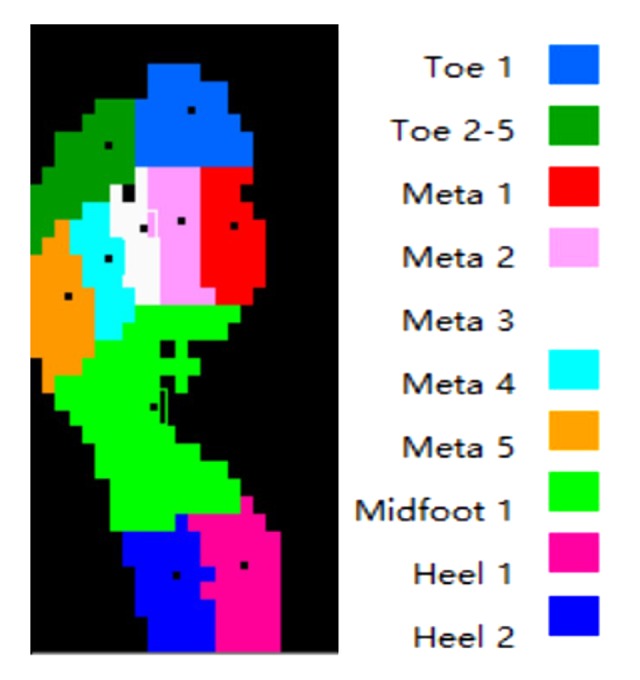
The Footscan® system divides the sole into 10 areas: the big toe (T1), toes 2–5 (T2–T5), the 1st to 5th metatarsal (M1, M2, M3, M4, and M5), midfoot (MF), medial heel (H1, MH), and lateral heel (H2, LH).
Results
Trial profile
Figure 4 summarizes the trial profile. Ninety patients were clinically prescreened and asked to participate; 10 individuals were ineligible on the basis of the inclusion criteria. All 80 individuals were randomly assigned to 1 of 2 groups and completed the study. The experiment group had 40 participants who wore the customized insoles, and the control group had 40 participants who wore the prefabricated-insoles.
Figure 4.

Flow chart of study participants, following the Consolidated Standards of Reporting Trials guidelines.
Comfort score
At week 0, there were no significant difference in VAS scores (Table 1) between the experimental group (7.91±3.11) and the control group (8.12±1.21) at week 0 (P>0.05). At week 8, all participants reported that comfort had increased, and the experimental group reported significant improvement (P<0.05). The comfort score (VAS pain score) reported by the experimental group (2.42±0.13) was significantly lower than that of the control group at week 8 (5.92±1.19, P<0.05).
Biomechanical analysis
Table 2 compares the 3 parameters of the 10 regions between the experimental group and the control group at week 0; the overall difference was small. In the experimental group, the peak pressure in the 3rd metatarsal region was significantly lower than in the control group (P=0.04), and the mid-foot pressure was higher in the experiment group (P=0.04). In the control group, the peak force in the 1st metatarsal region was significantly higher than the experimental group (P=0.01). There was no significant difference of peak pressure and peak force between the experimental group and the control group in other areas. There was no significant difference in the peak contact area between the experimental group and the control group in all areas.
Table 2.
Comparison of the experimental group and control group at week 0.
| Areas | Peak pressure (kPa) | Peak force (N) | Peak contact area (cm2) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| CI | PI | p | CI | PI | p | CI | PI | p | |
| T1 | 101.21±50.61 | 140.80±191.50 | 0.42 | 137.91±100.21 | 109.71±53.21 | 0.64 | 12.30±100.20 | 14.10±6.70 | 0.40 |
| T2–5 | 34.31±18.12 | 67.40±80.10 | 0.27 | 34.31±27.91 | 41.21±42.21 | 0.49 | 8.20±4.30 | 6.80±5.70 | 0.61 |
| M1 | 71.00±68.71 | 135.51±68.22 | 0.08 | 43.71±33.11 | 120.71±82.00 | 0.01* | 7.20±3.40 | 7.20±3.80 | 0.60 |
| M2 | 192.61±90.91 | 280.61±251.41 | 0.31 | 166.71±87.8 | 117.12±82.13 | 0.78 | 7.90±2.80 | 7.00±3.30 | 0.82 |
| M3 | 202.91±69.11 | 400.00±263.41 | 0.04* | 149.61±85.11 | 234.41±207.14 | 0.23 | 10.40±12.90 | 6.20±2.50 | 0.66 |
| M4 | 197.11±75.31 | 318.43±172.63 | 0.18 | 150.21±79.61 | 188.71±126.11 | 0.46 | 7.00±1.90 | 6.40±2.80 | 0.97 |
| M5 | 142.51±69.00 | 140.73±78.73 | 0.93 | 154.71±95.82 | 136.17±97.61 | 0.78 | 10.60±2.80 | 9.60±4.20 | 0.33 |
| MF | 113.71±22.41 | 45.33±53.23 | 0.04* | 394.12±153.31 | 220.11±321.11 | 0.46 | 33.10±10.60 | 35.40±16.90 | 0.66 |
| MH | 195.11±70.21 | 166.63±60.51 | 0.46 | 285.61±183.21 | 236.21±157.00 | 0.79 | 12.9±4.8 | 12.8±6.2 | 0.66 |
| LH | 178.71±61.92 | 167.63±88.71 | 0.87 | 221.10±130.80 | 201.11±148.90 | 0.96 | 11.2±4.1 | 11.4±5.6 | 0.56 |
p<0.05, indicating a significant difference; values are expressed as means ±standard deviations.
CI – customized insole; PI – prefabricated insole; T1 – hallux; T2–5 – toes 2–5; M1 – 1st metatarsal; M2 – 2nd metatarsal; M3 – 3rd metatarsal; M4 – 4th metatarsal; M5 – 5th metatarsal; MF – midfoot; MH – medial heel; LH – lateral heel.
Table 3 compares the 3 parameters of the 10 areas between the experimental group and the control group at week 8, the peak pressure in mid-foot of the experimental group was significantly higher than that of the same area of the control group (P=0.04). The peak force in mid-foot of the experimental group was also significantly higher than that of the same area of the control group (P=0.01). There was no significant difference in peak pressure and peak force in other areas. In the experimental group, the contact areas of the 3rd and 4th metatarsal areas were smaller than the contact area produced by the control group (M3: P=0.04, M4: P=0.04).
Table 3.
Comparison of the experimental and control groups at week 8.
| Areas | Peak pressure (kPa) | Peak force (N) | Peak contact area (cm2) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| CI | PI | p | CI | PI | p | CI | PI | p | |
| T1 | 126.21±46.61 | 105.60±109.70 | 0.89 | 153.20±80.90 | 109.71±44.91 | 0.21 | 11.10±2.50 | 14.61±6.11 | 0.36 |
| T2–5 | 56.31±27.51 | 42.20±48.50 | 0.85 | 50.70±41.90 | 34.71±34.51 | 0.84 | 8.80±5.30 | 11.51±6.21 | 0.36 |
| M1 | 118.50±152.60 | 164.00±57.31 | 0.69 | 97.41±51.81 | 145.30±100.40 | 0.25 | 7.90±3.50 | 12.41±5.21 | 0.17 |
| M2 | 176.7±56.71 | 201.60±199.30 | 0.61 | 158.20±96.70 | 177.11±64.11 | 0.62 | 7.90±3.30 | 11.61±4.11 | 0.14 |
| M3 | 239.20±100.10 | 286.41±250.61 | 0.42 | 138.00±93.60 | 225.31±95.21 | 0.13 | 6.20±2.30 | 10.11±3.41 | 0.04* |
| M4 | 144.20±60.00 | 169.51±42.61 | 0.75 | 104.30±61.20 | 143.30±79.60 | 0.61 | 6.70±2.70 | 10.22±3.31 | 0.04* |
| M5 | 113.41±56.51 | 71.31±33.71 | 0.52 | 123.50±71.40 | 86.90±58.40 | 0.68 | 9.60±3.90 | 12.31±4.61 | 0.48 |
| MF | 112.21±11.81 | 44.13±31.11 | 0.04* | 422.60±147.80 | 119.80±104.70 | 0.01* | 36.30±12.20 | 30.21±11.71 | 0.23 |
| MH | 206.71±57.21 | 161.81±78.22 | 0.87 | 293.50±149.90 | 219.2±100.50 | 0.79 | 12.90±4.80 | 14.90±5.50 | 0.47 |
| LH | 199.31±58.61 | 177.31±104.21 | 0.74 | 240.30±139.10 | 209.40±112.20 | 0.81 | 11.10±4.20 | 13.30±4.90 | 0.38 |
p<0.05, indicating a significant difference; values are expressed as means ±standard deviations.
CI – customized insole; PI – prefabricated insole; T1 – hallux; T2–5 – toes 2–5; M1 – 1st metatarsal; M2 – 2nd metatarsal; M3 – 3rd metatarsal; M4 – 4th metatarsal; M5 – 5th metatarsal; MF – midfoot; MH – medial heel; LH – lateral heel.
Table 4 compares the 3 parameters of the 10 areas in the control group between week 0 and week 8. In week 8, the peak pressures of the 4th and 5th metatarsal areas of the control group were significantly lower than the peak pressure of the same areas at week 0 (M4: P=0.04, M5: P=0.03). In week 8, the peak force of the 1st metatarsal area of the control group was significantly higher than the peak force of the same areas at week 0 (P=0.02). The peak force of the 5th metatarsal area of the control group at week 8 were significantly lower than the peak force of the same areas at week 0 (P=0.03). At week 8, the contact area of the mid-foot in the control group was higher than the same area at week 0 (P=0.03).
Table 4.
Comparison of study parameters in the control group at week 0 and week 8.
| Areas | Peak pressure (kPa) | Peak force (N) | Peak contact area (cm2) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 0PI | 8PI | p | 0PI | 8PI | p | 0PI | 8PI | p | |
| T1 | 140.81±191.52 | 105.60±109.70 | 0.45 | 109.71±53.12 | 109.72±44.91 | 0.72 | 14.10±6.70 | 14.61±6.11 | 0.55 |
| T2–5 | 67.41±80.11 | 42.20±48.50 | 0.85 | 41.21±42.21 | 34.71±34.51 | 0.69 | 6.80±5.70 | 11.51±6.22 | 0.16 |
| M1 | 135.51±68.22 | 164.00±57.31 | 0.32 | 120.71±82.00 | 145.30±100.40 | 0.02* | 7.20±3.40 | 12.41±5.22 | 0.17 |
| M2 | 280.60±251.40 | 201.60±199.30 | 0.82 | 117.20±82.30 | 177.11±64.11 | 0.34 | 7.00±3.31 | 11.61±4.11 | 0.23 |
| M3 | 400.00±263.40 | 286.41±250.61 | 0.38 | 234.41±207.42 | 225.31±95.21 | 0.61 | 6.21±2.51 | 10.11±3.41 | 0.21 |
| M4 | 318.40±172.60 | 169.51±42.61 | 0.04* | 188.71±126.11 | 143.31±79.61 | 0.17 | 6.41±2.81 | 10.22±3.31 | 0.25 |
| M5 | 140.70±78.70 | 71.31±33.71 | 0.03* | 136.71±97.61 | 86.90±58.40 | 0.03* | 9.60±4.20 | 12.31±4.62 | 0.796 |
| MF | 45.30±53.20 | 44.11±31.12 | 0.97 | 220.11±321.11 | 119.80±104.70 | 0.21 | 30.21±11.72 | 35.41±16.90 | 0.03* |
| MH | 166.60±60.50 | 161.81±78.22 | 0.59 | 236.21±157.00 | 219.20±100.50 | 0.53 | 12.81±6.21 | 14.91±5.53 | 0.84 |
| LH | 167.60±88.70 | 177.31±104.21 | 0.31 | 201.10±148.90 | 209.40±112.20 | 0.91 | 11.41±5.61 | 13.31±4.91 | 0.92 |
p<0.05, indicating a significant difference; values are expressed as means ±standard deviations.
0PI – 0 week prefabricated insole; 8PI – 8th week prefabricated insole; T1 – hallux; T2–5 – toes 2–5; M1 – 1st metatarsal; M2 – 2nd metatarsal; M3 – 3rd metatarsal; M4 – 4th metatarsal; M5 – 5th metatarsal; MF – midfoot; MH – medial heel; LH – lateral heel.
Table 5 compares the 3 parameters of the 10 areas of the experimental group between week 0 and week 8. At week 8, the peak pressure of the 2nd to 5th toe and the lateral heel area of the big toe of the experimental group was significantly higher than the peak pressure of the same area at week 0 (T1: P=0.01, T2–5: P=0.03, LH: P=0.03). The contact area of the mid-foot area in experimental group at week 8 was significantly higher than the contact area of the corresponding area at week 0 (MF: P=0.03).
Table 5.
Comparison of the study parameters in the experimental group at week 0 and week 8.
| Areas | Peak pressure (kPa) | Peak force (N) | Peak contact area (cm2) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| 0PI | 8PI | p | 0PI | 8PI | p | 0PI | 8PI | p | |
| T1 | 101.21±50.61 | 126.21±46.61 | 0.01* | 137.91±100.21 | 153.21±80.91 | 0.67 | 12.31±100.21 | 11.11±2.52 | 0.19 |
| T2–5 | 34.31±18.11 | 56.31±27.52 | 0.03* | 34.32±27.92 | 50.71±41.91 | 0.04* | 8.22±4.32 | 8.81±5.32 | 0.62 |
| M1 | 71.00±68.71 | 118.50±152.60 | 0.94 | 43.71±33.11 | 145.31±100.41 | 0.18 | 7.20±3.40 | 7.90±3.50 | 0.38 |
| M2 | 192.63±90.93 | 176.72±56.71 | 0.46 | 166.71±87.81 | 158.23±96.71 | 0.56 | 7.91±2.82 | 7.92±3.32 | 0.81 |
| M3 | 202.91±69.11 | 239.20±100.10 | 0.68 | 149.62±85.12 | 138.00±93.60 | 0.46 | 10.42±12.91 | 6.20±2.30 | 0.30 |
| M4 | 197.12±75.31 | 144.20±60.00 | 0.47 | 150.23±79.62 | 104.30±61.20 | 0.02* | 7.01±1.92 | 6.70±2.70 | 0.42 |
| M5 | 142.52±69.00 | 113.42±56.52 | 0.17 | 154.71±95.83 | 123.52±71.41 | 0.21 | 10.61±2.81 | 9.61±3.92 | 0.33 |
| MF | 113.71±22.41 | 112.21±11.81 | 0.82 | 394.11±153.31 | 422.62±147.82 | 0.35 | 33.12±10.61 | 36.32±12.22 | 0.03* |
| MH | 195.11±70.23 | 206.72±57.22 | 0.37 | 285.62±183.22 | 293.51±149.92 | 0.73 | 12.91±4.82 | 12.92±4.82 | 0.93 |
| LH | 178.72±61.91 | 199.31±58.61 | 0.07 | 221.00±130.82 | 240.31±139.13 | 0.3 | 11.21±4.11 | 11.11±4.22 | 0.81 |
p<0.05, indicating a significant difference; values are expressed as means ±standard deviations.
0PI – 0 week prefabricated insole; 8PI – 8th week prefabricated insole; T1 – hallux; T2–5 – toes 2–5; M1 – 1st metatarsal; M2 – 2nd metatarsal; M3 – 3rd metatarsal; M4 – 4th metatarsal; M5 – 5th metatarsal; MF – midfoot; MH – medial heel; LH – lateral heel.
Discussion
The purpose of designing 3D printed insoles
The aim of this study was to compare the effects of customized insoles and prefabricated insoles on the biomechanical parameters of the plantar foot in patients with symptomatic flatfoot. The purpose of insole is to increase the contact area and support the arch which can help to distribute load in the mid-foot position [24].
Comparison of biomechanical effects between customized and prefabricated insoles on patients with flatfoot
In the mid-foot area, compared with the control group, the peak pressure in the experimental group was significantly higher at week 0 and week 8, showing that the customized insole had better effect on appending the foot load and improving the joint deformity in patients with symptomatic flatfoot, and the customized insole was better than the prefabricated insole. In the intra-group comparison, the contact areas of the experimental and the control groups at week 8 were higher than at week 0. One of the main mechanisms for the effect of foot insoles is changing mid-foot pressure [36,37]. Our study findings were consistent with previous studies that found that customized insoles were better than pre-customized insoles.
In the heel area, the results in our study indicated that the customized insoles did not differ significantly from the prefabricated insoles in terms of pressure, force, and contact area. According to previous studies, the heel area is subject to the greatest pressure on the foot [38,39]. Redmond et al. found that custom insoles resulted in less pressure in the heel area, possibly related to the shape and height of the custom heel cup; although it is unclear what effect the device has on heel pressure lower peak pressure under the heel is considered to be potentially beneficial [24].
In the metatarsal area, compared with the control group, the peak pressure of the 3rd metatarsal area in the experimental group was lower than that of week 0. This might indicate that the customized insole can more effectively reduce the load on the plantar metatarsal region in comparison to the prefabricated insole. The metatarsal region has a lower load onset. Guldemond et al. found that the use of a metatarsal pad could reduce the pressure in the 1st metatarsal and increased arch support height. Although both insoles in their study had a metatarsal pad, none of them significantly affected the 1st metatarsal and other metatarsal pressures [40], which was similar to the current experiment, suggesting the need for additional time for the pressure effects of the foot insole to alter the weight line and reduce stress.
In the toe area, there was no significant difference between the 2 insoles in our study. Only in the experimental group comparison, did the customized insole showed a higher peak pressure of the 2nd to 5th toes at week 8 than week 0, possibly because of patients’ plantar lesions leading to increased pressure in the toe area. It is not possible to reduce the toe area load simply through the use of an insole, and it is thus necessary to also perform rehabilitation. Although the thickness of the customized insole in the toe region in our study was higher than the prefabricated insole, it did not achieve the intended effect in the toe region.
Level of comfort is also a factor that affects user’s feeling toward a foot insole. Uncomfortable insoles can decrease the balance of the lower limb and affect a patient’s mood [36,41], especially for the elderly. This experiment showed that customized insoles have a better comfort level than prefabricated insoles, thus, customized insoles have the potential to improve the therapeutic effect.
This study had some limitations. First, the investigated covered only the short-term effects of 2 types of foot insoles and did not assess their long-term effects. Second, although the Footscan system has been proven to be an accurate plantar pressure evaluation system [29,42], for in-shoe pressure, there remain errors in the measurement techniques, including assessment of the full underside of the foot surface when measuring the contact area.
Conclusions
Customized 3D printed insoles reduced the load of the metatarsals and distributed the load to the mid-foot area to reduce lesions of the foot in patients with symptomatic flatfoot. Customized 3D printed insoles performed better than the prefabricated insole and showed better comfort improvement. Our findings suggested that the 3D printed customized insoles used in this study can be effective in rehabilitation treatment for flatfoot patients. Further research needs to be conducted including the long-term effect from wearing insoles and changes in joint mechanics.
Footnotes
Source of support: Departmental sources
Conflicts of interest
None.
References
- 1.Dombroski CE, Balsdon ME, Froats A. The use of a low-cost 3D scanning and printing tool in the manufacture of custom-made foot orthoses: A preliminary study. BMC Res Notes. 2014;7:443. doi: 10.1186/1756-0500-7-443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kobayashi T, Orendurff MS, Hunt G, et al. An articulated ankle-foot orthosis with adjustable plantarflexion resistance, dorsiflexion resistance and alignment: A pilot study on mechanical properties and effects on stroke hemiparetic gait. Med Eng Phys. 2017;44:94–101. doi: 10.1016/j.medengphy.2017.02.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lee YC, Lin G, Wang MJ. Comparing 3D foot scanning with conventional measurement methods. J Foot Ankle Res. 2014;7:44. doi: 10.1186/s13047-014-0044-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cha YH, Lee KH, Ryu HJ, et al. Ankle-foot orthosis made by 3D printing technique and automated design software. Appl Bionics Biomech. 2017;2017 doi: 10.1155/2017/9610468. 9610468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Munteanu SE, Scott LA, Bonanno DR, et al. Effectiveness of customised foot orthoses for Achilles tendinopathy: A randomised controlled trial. Br J Sports Med. 2015;49:989–94. doi: 10.1136/bjsports-2014-093845. [DOI] [PubMed] [Google Scholar]
- 6.Meyr AJ, Sansosti LE, Ali S. A pictorial review of reconstructive foot and ankle surgery: Evaluation and intervention of the flatfoot deformity. J Radiol Case Rep. 2017;11:26–36. doi: 10.3941/jrcr.v11i6.2757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chen YC, Lou SZ, Huang CY, Su FC. Effects of foot orthoses on gait patterns of flat feet patients. Clin Biomech (Bristol, Avon) 2010;25:265–70. doi: 10.1016/j.clinbiomech.2009.11.007. [DOI] [PubMed] [Google Scholar]
- 8.Pita-Fernandez S, Gonzalez-Martin C, Alonso-Tajes F, et al. Flat foot in a random population and its impact on quality of life and functionality. J Clin Diagn Res. 2017;11:LC22–27. doi: 10.7860/JCDR/2017/24362.9697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rasenberg N, Riel H, Rathleff MS, et al. Efficacy of foot orthoses for the treatment of plantar heel pain: A systematic review and meta-analysis. Br J Sports Med. 2018;52:1040–46. doi: 10.1136/bjsports-2017-097892. [DOI] [PubMed] [Google Scholar]
- 10.Braun BJ, Pelz P, Veith NT, et al. Long-term pathological gait pattern changes after talus fractures – dynamic measurements with a new insole. Int Orthop. 2018;42:1075–82. doi: 10.1007/s00264-017-3720-y. [DOI] [PubMed] [Google Scholar]
- 11.Linberg BH, Mengshoel AM. Effect of a thin customized insole on pain and walking ability in rheumatoid arthritis: A randomized study. Musculoskeletal Care. 2018;16:32–38. doi: 10.1002/msc.1199. [DOI] [PubMed] [Google Scholar]
- 12.Barati K, Saeedi H, Hajiaghaei B, et al. The effect of hydrodynamic insole on foot kinematics in individuals with flexible flatfoot: Case series using a single-subject design. Proc Inst Mech Eng H. 2019;233:407–13. doi: 10.1177/0954411919831326. [DOI] [PubMed] [Google Scholar]
- 13.Zhai J, Wang J, Qiu Y. Whether flexible flatfoot needs the treatment? An observation of plantar pressure effects on adults with flexible flatfoot by wearing over the counter insoles when walking on level surface, upstairs and downstairs. J Am Podiatr Med Assoc. :2017. doi: 10.7547/16-103. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 14.Ligon SC, Liska R, Stampfl J, et al. Polymers for 3D printing and customized additive manufacturing. Chem Rev. 2017;117:10212–90. doi: 10.1021/acs.chemrev.7b00074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zou D, He T, Dailey M, et al. Experimental and computational analysis of composite ankle-foot orthosis. J Rehabil Res Dev. 2014;51:1525–36. doi: 10.1682/JRRD.2014-02-0046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Telfer S, Pallari J, Munguia J, et al. Embracing additive manufacture: Implications for foot and ankle orthosis design. BMC Musculoskelet Disord. 2012;13:84. doi: 10.1186/1471-2474-13-84. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gordillo-Fernandez LM, Ortiz-Romero M, Valero-Salas J, et al. Effect by custom-made foot orthoses with added support under the first metatarso-phalangeal joint in hallux limitus patients: Improving on first metatarso-phalangeal joint extension. Prosthet Orthot Int. 2016;40:668–74. doi: 10.1177/0309364615584659. [DOI] [PubMed] [Google Scholar]
- 18.Chapman GJ, Halstead J, Redmond AC. Comparability of off the shelf foot orthoses in the redistribution of forces in midfoot osteoarthritis patients. Gait Posture. 2016;49:235–40. doi: 10.1016/j.gaitpost.2016.07.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lee HJ, Lim KB, Yoo J, et al. Effect of custom-molded foot orthoses on foot pain and balance in children with symptomatic flexible flat feet. Ann Rehabil Med. 2015;39:905–13. doi: 10.5535/arm.2015.39.6.905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hahni M, Hirschmuller A, Baur H. The effect of foot orthoses with forefoot cushioning or metatarsal pad on forefoot peak plantar pressure in running. J Foot Ankle Res. 2016;9:44. doi: 10.1186/s13047-016-0176-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bok SK, Lee H, Kim BO, et al. The effect of different foot orthosis inverted angles on plantar pressure in children with flexible flatfeet. PLoS One. 2016;11:e0159831. doi: 10.1371/journal.pone.0159831. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Escalona-Marfil C, McPoil TG, Mellor R, Vicenzino B. A radiographic and anthropometric study of the effect of a contoured sandal and foot orthosis on supporting the medial longitudinal arch. J Foot Ankle Res. 2014;7:38. doi: 10.1186/s13047-014-0038-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Zhai JN, Wang J, Qiu YS. Plantar pressure differences among adults with mild flexible flatfoot, severe flexible flatfoot and normal foot when walking on level surface, walking upstairs and downstairs. J Phys Ther Sci. 2017;29:641–46. doi: 10.1589/jpts.29.641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Khodaei B, Saeedi H, Jalali M, et al. Comparison of plantar pressure distribution in CAD-CAM and prefabricated foot orthoses in patients with flexible flatfeet. Foot (Edinb) 2017;33:76–80. doi: 10.1016/j.foot.2017.07.002. [DOI] [PubMed] [Google Scholar]
- 25.Melvin JC, Smith JB, Kruse RL, Vogel TR. Risk factors for 30-day hospital re-admission with an infectious complication after lower-extremity vascular procedures. Surg Infect (Larchmt) 2017;18:319–26. doi: 10.1089/sur.2016.234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Ghanami RJ, Hurie J, Andrews JS, et al. Anesthesia-based evaluation of outcomes of lower-extremity vascular bypass procedures. Ann Vasc Surg. 2013;27:199–207. doi: 10.1016/j.avsg.2012.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Toosizadeh N, Yen TC, Howe C, et al. Gait behaviors as an objective surgical outcome in low back disorders: A systematic review. Clin Biomech (Bristol, Avon) 2015;30:528–36. doi: 10.1016/j.clinbiomech.2015.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.McCormick CJ, Bonanno DR, Landorf KB. The effect of customised and sham foot orthoses on plantar pressures. J Foot Ankle Res. 2013;6:19. doi: 10.1186/1757-1146-6-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Xu C, Wen XX, Huang LY, et al. Normal foot loading parameters and repeatability of the Footscan(R) platform system. J Foot Ankle Res. 2017;10:30. doi: 10.1186/s13047-017-0209-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Xu C, Wen XX, Huang LY, et al. Reliability of the Footscan® platform system in healthy subjects: A comparison of without top-layer and with top-layer protocols. Biomed Res Int. 2017;2017 doi: 10.1155/2017/2708712. 2708712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Xu C, Yan YB, Zhao X, et al. Pedobarographic analysis following Pemberton’s pericapsular osteotomy for unilateral developmental dysplasia of the hip: An observational study. Medicine (Baltimore) 2015;94:e932. doi: 10.1097/MD.0000000000000932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mills K, Blanch P, Vicenzino B. Influence of contouring and hardness of foot orthoses on ratings of perceived comfort. Med Sci Sports Exerc. 2011;43:1507–12. doi: 10.1249/MSS.0b013e31820e783f. [DOI] [PubMed] [Google Scholar]
- 33.Kristo I, Stift A, Staud C, et al. The type of loose seton for complex anal fistula is essential to improve perianal comfort and quality of life. Colorectal Dis. 2016;18:O194–98. doi: 10.1111/codi.13335. [DOI] [PubMed] [Google Scholar]
- 34.Lindorfer J, Kroll J, Schwameder H. Comfort assessment of running footwear: Does assessment type affect inter-session reliability? Eur J Sport Sci. 2019;19:177–85. doi: 10.1080/17461391.2018.1502358. [DOI] [PubMed] [Google Scholar]
- 35.Zammit GV, Menz HB, Munteanu SE. Reliability of the TekScan MatScan® system for the measurement of plantar forces and pressures during barefoot level walking in healthy adults. J Foot Ankle Res. 2010;3:11. doi: 10.1186/1757-1146-3-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Collins NJ, Hinman RS, Menz HB, Crossley KM. Immediate effects of foot orthoses on pain during functional tasks in people with patellofemoral osteoarthritis: A cross-over, proof-of-concept study. Knee. 2017;24:76–81. doi: 10.1016/j.knee.2016.09.016. [DOI] [PubMed] [Google Scholar]
- 37.Chen Y, Li JX, Hong Y, Wang L. Plantar stress-related injuries in male basketball players: Variations on plantar loads during different maximum-effort maneuvers. Biomed Res Int. 2018;2018 doi: 10.1155/2018/4523849. 4523849. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.van der Wilk D, Dijkstra PU, Postema K, et al. Effects of ankle foot orthoses on body functions and activities in people with floppy paretic ankle muscles: A systematic review. Clin Biomech (Bristol, Avon) 2015;30:1009–25. doi: 10.1016/j.clinbiomech.2015.09.013. [DOI] [PubMed] [Google Scholar]
- 39.Umehara J, Ikezoe T, Nishishita S, et al. Effect of hip and knee position on tensor fasciae latae elongation during stretching: An ultrasonic shear wave elastography study. Clin Biomech (Bristol, Avon) 2015;30:1056–59. doi: 10.1016/j.clinbiomech.2015.09.007. [DOI] [PubMed] [Google Scholar]
- 40.Guldemond NA, Leffers P, Schaper NC, et al. The effects of insole configurations on forefoot plantar pressure and walking convenience in diabetic patients with neuropathic feet. Clin Biomech (Bristol, Avon) 2007;22:81–87. doi: 10.1016/j.clinbiomech.2006.08.004. [DOI] [PubMed] [Google Scholar]
- 41.Bonanno DR, Landorf KB, Munteanu SE, et al. Effectiveness of foot orthoses and shock-absorbing insoles for the prevention of injury: A systematic review and meta-analysis. Br J Sports Med. 2017;51:86–96. doi: 10.1136/bjsports-2016-096671. [DOI] [PubMed] [Google Scholar]
- 42.Yuan XN, Liang WD, Zhou FH, et al. Comparison of walking quality variables between incomplete spinal cord injury patients and healthy subjects by using a footscan plantar pressure system. Neural Regen Res. 2019;14:354–60. doi: 10.4103/1673-5374.244798. [DOI] [PMC free article] [PubMed] [Google Scholar]