

Abstract
Background:
Workplace acts as an efficient target for health promotion activities. Pedometer can act as a motivator and monitor of physical activity.
Aims:
The aim of the study was to assess the effect of pedometer usage in increasing physical activity and the level of adherence among employees of a software company in Puducherry.
Methods:
An interventional study was conducted with a prepost design. A single group of software company employees (n = 46), age ≥30 years selected by simple random sampling, was included in the study. Intervention consisted of health education program on physical activity, goal setting, and instructions regarding the use of pedometers for 1 week. Physical activity levels were measured at baseline and endline using global physical activity questionnaire.
Results:
Out of the 46 participants, 93% of the participants used the pedometer for at least 6 days. The difference between maximum observed step count during the week (median 9834 steps) and at baseline (6963 steps) was significant. Overall, 93.5% found pedometers to be useful for improving physical activity. Proportion of individuals with adequate physical activity based on Metabolic equivalents (MET) minutes increased from 41.3% (n = 19) at baseline to 69.6% at endline (n = 32) (P = 0.004).
Conclusions:
This study shows that a pedometer-driven walking intervention in the workplace setting is feasible and effective in increasing physical activity over a short term. Further research is required to test the effect of supportive strategies and long-term effectiveness of pedometer use.
Keywords: Exercise, fitness tracker, health promotion, walking, workplace
Introduction
Regular physical activity plays a role in the prevention of several chronic diseases such as cardiovascular disease, obesity, cancer, depression, hypertension, diabetes, and osteoporosis.[1] Physical inactivity has been identified as the fourth leading risk factor for global mortality causing an estimated 3.2 million deaths globally.[2] World Health Organization recommends that adults aged 18–64 should do at least 150 min of moderate-intensity aerobic physical activity throughout the week.[2]
Pedometers are modern tools which help keep track of daily ambulatory activity and acts both as a motivator and monitor of activity. Ten thousand steps a day is a widely accepted goal used worldwide. The workplace is considered as an efficient target of intervention as substantial number of working population can be reached aiming to alter multiple levels of behavior.[3] Workplace interventions based on pedometers have been done among various work groups around the world including hospital staff,[4] university employees,[5] social services’ company employees,[6] and meat processing workers.[7] A systematic review conducted in 2013 reported that workplace physical activity intervention using pedometers is more effective than those which do not.[8] However, very few pedometer-based intervention studies have been done in India.
Sedentary office work often limits the amount of physical exercise, especially among workers in software industries. Physical activity profile in a study conducted in a selected industry in South India revealed 75.2% to have a sedentary nature of work.[9] This project studies the effect of pedometer-based intervention in a novel setting of a software company in South India.
Methods
Study design
This was an interventional study using a prepost design with no control group. Approval was obtained from the Scientific and Institutional Ethics Committee.
Study setting and participants
One of the oldest and largest of the software companies in Puducherry (ISO 9001:2015 certified) was selected. A healthy workplace committee has been formed, and health promotion is ongoing for the past 3 years. Employees aged more than 30 years, working in managerial position or as team heads were included in the study, and those already using pedometers and those with orthopedic conditions limiting physical activity were excluded from the study.
Sample size and sampling
Earlier study done in this population showed the prevalence of sedentary behavior as 75%.[9] Assuming a reduction of sedentary behavior from 75% to 50% at the end of the intervention, sample size was estimated to be 45. Calculations were done using nMaster software Version 2.0, (Vellore, India) with 95% confidence limits and power of 80%.
Pilot study and instrument validation
Pilot study was conducted among six willing individuals chosen from a different setting. Wrist-worn fitness band activity tracker (Titan Fastrack Reflex) was chosen and validation of the tool was done before starting the study. This was worn along with a previously validated instrument (Omron HJ-325 pedometer) for 1 h as part of their routine activity. There was a maximum difference of 150 steps between the two pedometers with 1600 steps recorded during 1 h. All the pedometers used in the intervention passed the 20-step test and variation in readings ranged from (5%–7%) during the 1 h free-living activity test. Data on the use of pedometer over 1 week was retrieved by pairing it to mobile application through Bluetooth. Difficulties with the use of the pedometer and test recording of steps using the mobile application were done to formulate instructions and methods for intervention.
Study procedure
Baseline assessment
Participants were selected by simple random sampling from the list of employees fulfilling the eligibility criteria, and written informed consent was obtained. A self-administered questionnaire was used to collect information on sociodemographic details, presence of chronic morbidity, and anthropometry such as height and weight. Their baseline physical activity levels were assessed using global physical activity questionnaire (GPAQ).[10]
Intervention
Following baseline assessment, the participants were divided into groups of 10–12 each. The intervention was based on self-regulation theory with goal setting, feedback (display of step count on the pedometer), step calendar, and educational material. During the awareness program, topics such as role of physical activity in disease prevention, goal setting, and use of pedometers were discussed. Participants were provided with pedometers and instructed to wear it on the wrist for 7 days during all waking hours. They were asked to observe their step counts on day 1 without any additional increase in physical activity. They were asked to gradually increase the activity levels by 5%–10% from the previous day's target to reach the goal of 10,000 steps per day. General instructions regarding the use and care of the pedometer were demonstrated by the investigators.
Endline assessment
At the end of the intervention, objective data on step counts, calories burned, distance travelled, and peak hours of usage were obtained from the pedometers by connecting it to the mobile application. Feedback on the use of the pedometer and challenges faced was collected. GPAQ was administered again to assess the change in physical activity over the past 7 days.
Statistical analysis
Data were entered in Excel and analyzed using SPSS version 21 (IBM Corp, Armonk, NY: IBM Corp, 2012). Primary outcome measures were daily step counts and adherence to pedometer use. Secondary outcome measures such as minimum and maximum step counts and baseline and endline step counts were expressed as median and interquartile range (IQR). GPAQ scores were converted to MET minutes based on total time spent in physical activity during a typical week. MET minutes in the work and recreation domain were multiplied by MET values based on the intensity of activity (4 for moderate intensity and 8 for vigorous intensity). MET minutes in the transport domain were multiplied with a factor of 4. This was categorized as adequacy of physical activity if the value was more than 600 MET minutes.
Participants who used the pedometer on four or more days were classified as compliant to pedometer usage and included in analysis. Change in step counts from baseline to maximum step counts was analyzed using Wilcoxon Signed-Rank Test. Change in proportion of patients with adequate physical activity levels from pre to postintervention was done using McNemar Chi-square test. Per protocol analysis was done and P < 0.05 was set as statistical significance.
Results
Out of the 46 participants who were enrolled, 61% were females, 89% had completed graduation, and all were working in managerial position or as team heads. The mean age (standard deviation) of participants was 35 years (3.2). Around 76% were overweight (body mass index [BMI] >23) or obese (BMI >25) and 6.5% had comorbidities such as diabetes mellitus and hypertension. Only 41% had adequate physical activity at baseline with an average sedentary period of 8 h per day (IQR = 7–10) [Table 1].
Table 1.
Baseline characteristics of the study participants (n=46)
| Characteristics | Number of participants, n (%) |
|---|---|
| Gender | |
| Female | 28 (60.9) |
| Male | 18 (39.1) |
| Age | |
| 30-39 | 42 (91.3) |
| 40-49 | 4 (8.7) |
| Education | |
| Higher secondary | 1 (2.2) |
| Diploma | 4 (8.7) |
| Graduate | 20 (43.4) |
| Postgraduate | 21 (45.7) |
| Years of experience (years) | |
| ≤5 | 9 (19.5) |
| 6-10 | 16 (34.8) |
| >10 | 21 (45.7) |
| BMI | |
| Underweight | 4 (8.7) |
| Normal | 7 (15.2) |
| Obese | 25 (54.3) |
| Overweight | 10 (21.7) |
| Comorbidity | |
| Diabetes | 1 (2.2) |
| Hypertension | 2 (4.3) |
| Normal | 43 (93.5) |
| Physical activity at baseline | |
| Adequate (≥600 MET min) | 19 (41.3) |
| Inadequate (<600 MET min) | 27 (58.7) |
| Total | 46 (100) |
BMI=Body mass index
None of the participants dropped out of the study. The change in step counts was analyzed for 44 participants, who used it for at least 4 days. Step count at baseline was 6963 and the maximum recording during the week was 9834 (P < 0.001) [Table 2]. However, the daily step count over the week showed a decline during day 3 and day 7 [Figure 1]. Self-reported physical activity at endline improved to 70% compared to 41% at baseline (P = 0.004) [Figure 2].
Table 2.
Step counts, distance covered, and calories burned by the participants during the intervention (n=44)
| Characteristics | Median (IQR) |
|---|---|
| Step counts | |
| Day 1 | 6963 (5702-9193) |
| Minimum step count during the week | 3641 (1761-5558) |
| Maximum count during the week | 9834 (7295-13,023) |
| Day 7 | 5621 (4467-8977) |
| Distance covered (km) | |
| Day 1 | 5 (4-6) |
| Maximum during the week | 6.9 (5-9.1) |
| Day 7 | 3.9 (3.1-6.3) |
| Calories burned (calories) | |
| Day 1 | 329.5 (270.3-436) |
| Maximum during the week | 465.5 (345.3-617.3) |
| Day 7 | 266 (211-425) |
IQR=Interquartile range
Figure 1.
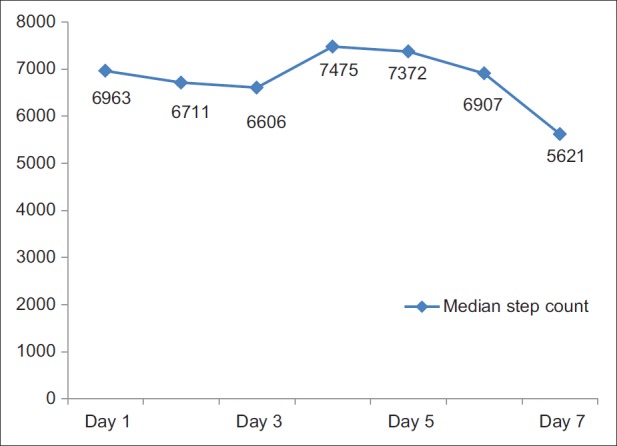
Trend of average step counts of participants during the intervention (n = 44)
Figure 2.
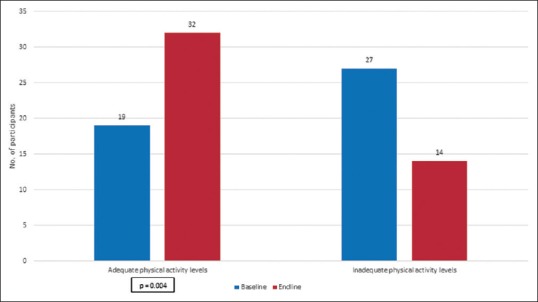
Comparison of adequate physical activity from baseline to endline (n = 46)
Around 93% of the participants used pedometer for at least 6 days during the week for 10–12 h per day. Around 94% felt that pedometer helped improve their physical activity. Common changes made by participants on pedometer use include walking (57.5%) and use of stairs (30%) [Table 3].
Table 3.
Adherence and perception regarding pedometer among the study participants (n=46)
| Characteristics | n (%) |
|---|---|
| Number of days used | |
| 2 | 2 (1.3) |
| 4 | 3 (4.1) |
| 5 | 1 (1.7) |
| 6 | 7 (14.3) |
| 7 | 33 (78.6) |
| Pedometer was useful in improving physical activity | |
| Yes | 43 (93.5) |
| No | 2 (4.3) |
| Not sure | 1 (2.2) |
| Changes made to improve physical activity | |
| Walking* | 26 (57.5) |
| Use stairs | 14 (30) |
| Daily exercise | 1 (2.5) |
| No change | 5 (10) |
*Leisure time activity, walking to office, shops, and parks are all include in walking
Discussion
Our findings suggest that pedometers are feasible and acceptable tools in improving physical activity in a workplace setting. There was a significant increase in physical activity levels and step counts during the intervention and this is consistent with other studies. However, the overall step counts showed a negative trend on comparing day 7 with baseline which has been observed in similar workplace interventions promoting pedometer use.[6] This could be due to the absence of constant reminder such as E-mails or phone calls in our study. Another reason could be due to Hawthorne effect where the participants engaged in physical activity after enrollment in excess of their normal pattern. It is possible that, in our study, attributes of their occupation such as meetings or long working hours could have influenced the findings.
Participants showed higher adherence compared to other studies (77%–91%).[7,11] This could be due to shorter period of intervention compared to 3–6 months in other studies. Majority found pedometer to be useful in improving physical activity as it helped in motivation, goal setting, and daily tracking. Similar studies[12] reported pedometers to be useful in increasing awareness of physical activity levels and motivation.
This is one of the first studies on workplace wellness from India using pedometers to improve physical activity. This interventional study has practical implications of increasing the awareness of participants about their baseline physical activity, sensitizing them to use of technology in health promotion, and promoting goal setting attitude. Other strengths include objective and subjective measurement of physical activity and minimal dropout rate. Absence of a control group and short duration of intervention were major limitations. We could not use research grade actigraphs or accelerometers in this study due to cost considerations. Inaccuracy in step counts while riding two-wheelers was another limitation. Other factors that need to be addressed in future studies include pattern of working and nonworking days and possibility of blinding.
Conclusions
This study has demonstrated that a pedometer-based walking intervention in the workplace setting is feasible and acceptable in increasing physical activity over a short term. Strategies such as goal setting, feedback, and educational intervention were helpful in improving overall adherence. Further research is required to test the effect of supportive strategies and long-term effectiveness of pedometer use.
Financial support and sponsorship
This was a short term research award for UG students – GJ – STRAUS 2016-17.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
The author thanks the management of INTEGRA, Puducherry, for the permission to conduct the study and the employees for having participated in the study.
References
- 1.Warburton DE, Nicol CW, Bredin SS. Health benefits of physical activity: The evidence. CMAJ. 2006;174:801–9. doi: 10.1503/cmaj.051351. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Physical Activity. World Health Organization. 2017. [Last accessed on 2016 Oct 27]. Available from: http://www.who.int/dietphysicalactivity/pa/en .
- 3.Quintiliani L, Sattelmair J, Sorensen G The Workplace as a Setting for Interventions to Improve Diet and Promote Physical Activity. [Last accessed on 2016 Oct 27]. Available from: http://www.who.int/dietphysicalactivity/Quintiliani-workplace-as-setting.pdf .
- 4.Croteau KA. Using pedometers to increase the non-workday steps of hospital nursing and support staff: A pilot study. Workplace Health Saf. 2017;65:452–6. doi: 10.1177/2165079916665399. [DOI] [PubMed] [Google Scholar]
- 5.Baghianimoghaddam MH, Bakhtari-Aghdam F, Asghari-Jafarabadi M, Allahverdipour H, Dabagh-Nikookheslat S, Nourizadeh R, et al. The effect of a pedometer-based program improvement of physical activity in Tabriz university employees. Int J Prev Med. 2016;7:50. doi: 10.4103/2008-7802.177897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.De Cocker KA, De Bourdeaudhuij IM, Cardon GM. The effect of a multi-strategy workplace physical activity intervention promoting pedometer use and step count increase. Health Educ Res. 2010;25:608–19. doi: 10.1093/her/cyp052. [DOI] [PubMed] [Google Scholar]
- 7.Mansi S, Milosavljevic S, Tumilty S, Hendrick P, Baxter GD. Use of pedometer-driven walking to promote physical activity and improve health-related quality of life among meat processing workers: A feasibility trial. Health Qual Life Outcomes. 2013;11:185. doi: 10.1186/1477-7525-11-185. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.To QG, Chen TT, Magnussen CG, To KG. Workplace physical activity interventions: A systematic review. Am J Health Promot. 2013;27:e113–23. doi: 10.4278/ajhp.120425-LIT-222. [DOI] [PubMed] [Google Scholar]
- 9.Kar SS, Subitha L, Kalaiselvi S, Archana R. Development and implementation of healthy workplace model in a selected industry of Puducherry, South India. Indian J Occup Environ Med. 2015;19:25–9. doi: 10.4103/0019-5278.157003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bull FC, Maslin TS, Armstrong T. Global physical activity questionnaire (GPAQ): Nine country reliability and validity study. J Phys Act Health. 2009;6:790–804. doi: 10.1123/jpah.6.6.790. [DOI] [PubMed] [Google Scholar]
- 11.Aittasalo M, Rinne M, Pasanen M, Kukkonen-Harjula K, Vasankari T. Promoting walking among office employees-evaluation of a randomized controlled intervention with pedometers and e-mail messages. BMC Public Health. 2012;12:403. doi: 10.1186/1471-2458-12-403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lauzon N, Chan CB, Myers AM, Tudor-Locke C. Participant experiences in a workplace pedometer-based physical activity program. J Phys Act Health. 2008;5:675–87. doi: 10.1123/jpah.5.5.675. [DOI] [PubMed] [Google Scholar]