Abstract
Objective To define the major epidemiological features of upper limb penetrating injuries, as well as to identify the causes and the frequency of these lesions at the Instituto de Ortopedia e Traumatologia, a hand surgery center in the city of São Paulo, state of São Paulo, Brazil.
Methods The present study was based on a sample of consecutive patients from our orthopedics and traumatology institute from May 2014 to May 2016. Data were collected by telephone, and a prestructured questionnaire regarding data and features of the lesions was applied. Descriptive statistics and proportions comparison with the chi-squared test were performed with a p -value < 5% considered as statistically significant.
Results At first, 1,648 records were considered and, after applying the exclusion criteria and eliminating duplicate records, 598 records were included in the present study. Most of the patients were male (77.8%), right-handed (95.82%), with an average age of 37.27 years old. Manual laborers were the most injured individuals (50.00%), and fingers were the most affected site (51.84%). Glass was the most frequent etiologic agent (33.77%). The prevalence of amputation was higher in industrial machinery injuries ( p < 0.05) when compared with other causes. Younger patients (< 18 years old) had more glass-related injuries, while older patients (≥ 60 years old) had more traumas caused by power tools ( p < 0.05). Women had more injuries resulting from razors and glass ( p < 0.05). Manual laborers had a higher frequency of power tools and industrial machinery-related injuries ( p < 0.05) and a higher prevalence of amputations ( p < 0.05).
Conclusion The most frequent etiology was glass, especially in individuals < 18 years old. Women and older patients (> 60 years old) presented a high frequency of traumas caused by razors and power tools, respectively. More severe injuries were caused by machinery and were related with work activity.
Keywords: wounds, penetrating; hand injuries; cross-sectional studies
Introduction
The upper limb is one of the anatomic regions that are most affected by injuries and wounds, due to the frequent interaction with the environment and to the direct contact with harmful agents 1 The hand is considered a complex tool to perform several types of work, executing precision and accuracy activities, as well as strength and repetition movements.
Several etiologic agents may be related to penetrating wounds with distinct trauma mechanisms, such as crushing, avulsions, or cuts. These injuries are frequent in the work environment and are mainly related to industrial machines. 2 However, domestic accidents, automobile accidents, sports practice, and aggressions are also important causes. 3
The structures that commonly sustain penetrating injuries include musculotendinous structures, neurovascular bundles, bones, and amputations at various levels. 4 A thorough evaluation, with the definition of the trauma mechanism and of the causal agent, and a specific physical examination may guide the diagnosis of associated lesions, facilitating patient referral or treatment by a specialized team.
The socioeconomic impact of these conditions is high, since they affect mainly young and economically active patients, 5 6 require an extensive rehabilitation period, and possibly cause sequelae with transient or permanent functional restriction. The economic burden can be direct, related to the multidisciplinary care, or indirect, due to compensation for accidents, sickness, and temporary or permanent disability. 5 The literature reports that between 20 and 50% of the compensation claims by workers are related to hand injuries. 7
Knowledge on the prevalence and etiological agents of penetrating wounds in the upper limb may help to understand frequently encountered injuries, in addition to guide the development of prevention and awareness strategies. The present study aims to define the main epidemiological features of these lesions, as well as to identify the cause and frequency of penetrating injuries in the upper limbs in patients presented at the Discipline of Hand and Upper Limb Surgery of the Instituto de Ortopedia e Traumatologia between May 2014 and May 2016.
Materials and Methods
The methodology of the present study was approved by the local ethics committee under the number CAAE 61257216.1.0000.5505, report number 1.849.563. The manuscript was prepared according to the strengthening the reporting of observational studies in epidemiology (STROBE) statement.
Population
Convenience sample of consecutive patients presented at the Instituto de Ortopedia e Traumatologia of the Universidade Federal de São Paulo, São Paulo, state of São Paulo, Brazil, from May 2014 to May 2016. The patients were independently recruited by two researchers who performed a research of the medical records available at the digital platform of the hospital, the Electronic Patient Record (PEP, in the Portuguese acronym), and identified through a diagnostic registry by the International Classification of Diseases (ICD-10).
Inclusion Criteria
Patients diagnosed with upper limb injuries (S61, S51, S41, according to the ICD-10 classification), upper limb trauma (T11 and subitems), flexor and extensor tendon injuries (S66, S56 and subitems), neural trauma (S64, S54, S44 and subitems), radial, ulnar, and medial nerves lesions (G56.1, G56.2, G56.3), amputations (S56, S58, S48), sequelae from amputation stump (T87), sequelae from upper limb injuries (T92, excluding subitems 1, 2 and 3). The ICD-10-recognized diagnosis was compared to the clinical admission history to ratify the clinical condition.
Exclusion Criteria
Patients whose electronic records did not provide relevant information for research (contact information, clinical history or nonconcordant ICD registry) were excluded. In addition, patients whose medical record showed a closed (noncutting) mechanism of injury and burn-related injuries were excluded. Patients who could not be located after 3 telephone contact attempts with a 1-week interval were excluded, as well as those who did not wish to answer the questionnaire.
Data Collection and Extraction Method
The identification of multiple ICDs for each patient was performed as follows: each patient was considered a single analytic unit, despite the existence of several ICDs for the same individual.
After listing the patients who were candidates for evaluation, relevant data was collected by telephone using a prestructured questionnaire ( Annex 1 ). After verbal consent, the following data were obtained: gender, dominant hand, age at the time of the accident, occupation, lesion topography, and etiological agent.
Annex 1. Prestructured questionnaire.
| QUESTIONNAIRE – PENETRATING WOUNDS ON UPPER LIMBS |
|---|
| NAME:_______________________________________________ RH:_____________________________ GENDER: __M __F DYNAMIC: __ R __L AGE WHEN THE ACCIDENT OCCURRED: _________ OCCUPATION: ______________________________ OCCUPATIONAL HAZARD? __Y __N LOCAL OF THE WOUND (WHERE ON THE BODY IS THE WOUND?) ______________________________________________________________ ETIOLOGY (HOW HAVE YOU BEEN INJURED?) ______________________________________________________________ ______________________________________________________________ |
In order to group data for analysis, occupation at the time of the trauma was divided into eight categories: 1—manual laborer, 2—retail worker, 3—office/services worker, 4—technicians, 5—farmers, 6—craftsmen, 7—students, and 8—retired/unemployed individuals ( Annex 2 ).
Annex 2. Occupation categories.
| Occupation | Description |
|---|---|
| Manual labor | mason, construction assistant, metallurgical |
| Retail worker | salesperson, street marketer, clerk |
| Offices/services | administrative assistant, secretary, butcher, receptionist |
| Technician | electrician, electronics technician, nursing technician |
| Farmer | seeding, catcher |
| Craftsmen | weaver, carpenter, cobbler |
| Student | student |
| Retired/unemployed | retired or unemployed at the moment of the injury |
After preparing a spreadsheet with all of the extracted data, the selected patients were grouped according to gender, occupation, and age (< 18 years old and ≥ 60 years old) to analyze the importance of different etiological agents in more homogeneous populational subgroups.
Statistical Methods
The statistical analysis of all the collected information was initially performed descriptively, through mean, minimum and maximum values, absolute and relative frequencies (percentage), dispersion measures (standard deviation [SD]) and graphic methods.
For the inferential statistical analysis, dichotomous categorical variables of interest were compared using the chi-squared test with a p value < 5%. The test criterion was the minimum presence of 5 events per cell in a 2 × 2 contingency table.
Results
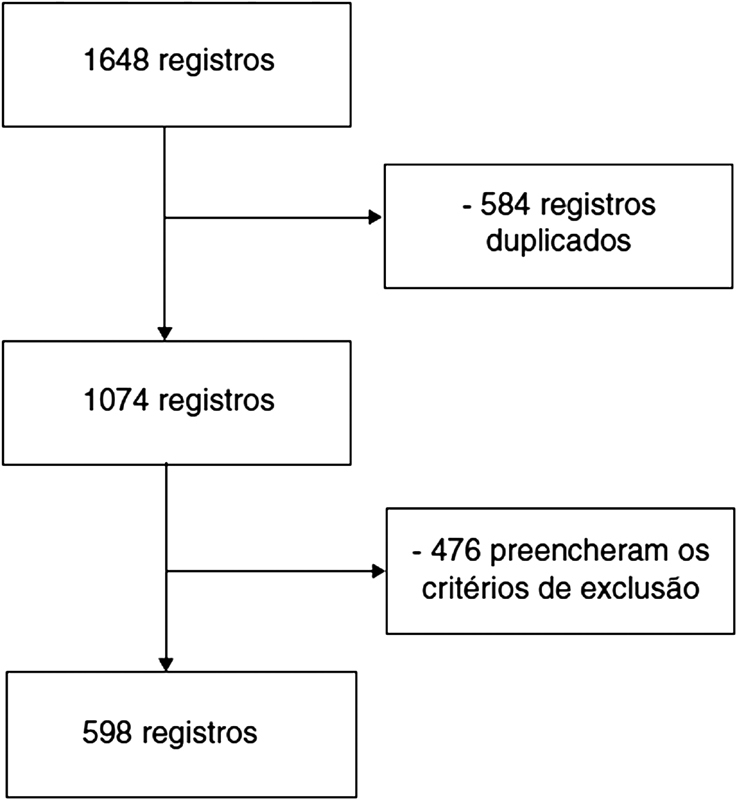
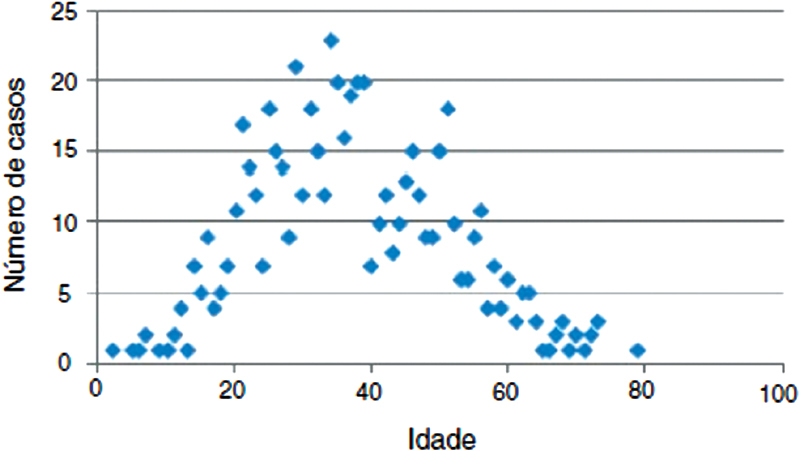
After researching the selected ICDs, 1,648 records were initially considered. Of these records, 584 duplicates (patients with more than 1 ICD at the medical record) were excluded, leaving 1,074 records. Next, 476 records were excluded according to the predetermined criteria. Reasons leading to exclusion were the following: 212 for closed trauma, 258 for the lack of information in the medical record, and 6 for burn-related injuries. For the final analysis, 598 patients remained ( Fig. 1 ). Demographic features of the included patients are shown in Table 1 , and the distribution of the lesions by age is show in Fig. 2 .
Fig. 1.
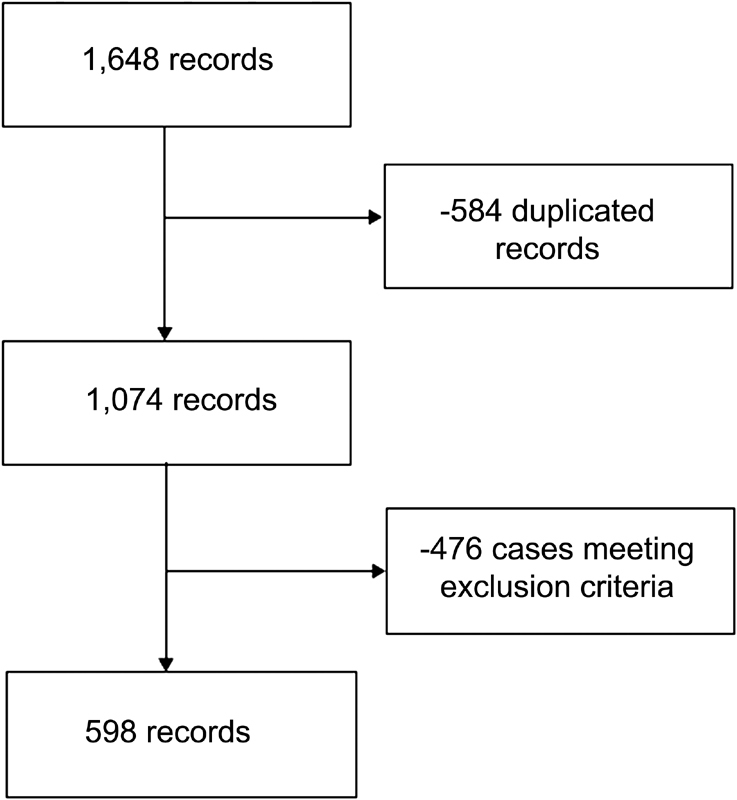
Patients selection organizational chart.
Table 1. Epidemiological features.
| Feature | Quantitative variable | Qualitative variable |
|---|---|---|
| Gender | 77.80% (male) | |
| Age | Average, 37.27 years old (2-79 years old; SD: 13.9) |
|
| Dominance | 95.82% (right-handed) | |
| Laterality | 52.84% (dominant) 46.98% (non-dominant) 0.84% (bilateral) |
Abbreviations: SD, standard deviation.
Fig. 2.
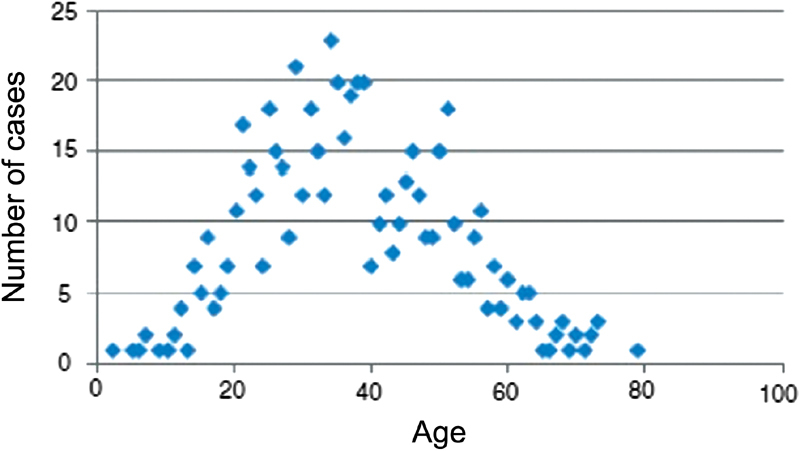
Number of cases per age.
Manual laborers accounted for 299 cases (50.00%), followed by office and services workers, with 134 cases (22.40%) ( Table 2 ).
Table 2. Occupational activity of the included patients.
| Occupation at the time of the trauma | Number of cases | % |
|---|---|---|
| Manual laborer | 299 | 50.00 |
| Offices/services | 134 | 22.40 |
| Retired/unemployed individuals | 50 | 8.36 |
| Students | 46 | 7.69 |
| Retail workers | 42 | 7.04 |
| Craftsmen | 13 | 2.17 |
| Technicians | 8 | 1.34 |
| Farmers | 6 | 1.00 |
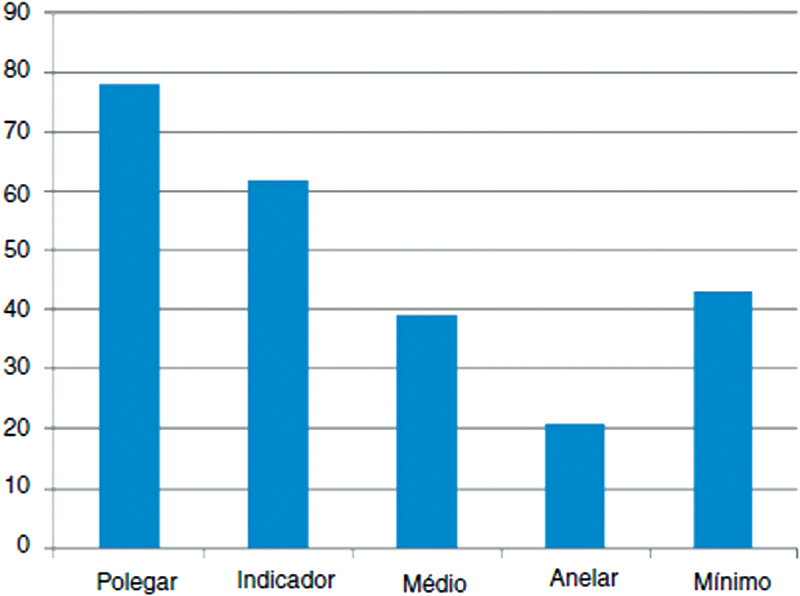
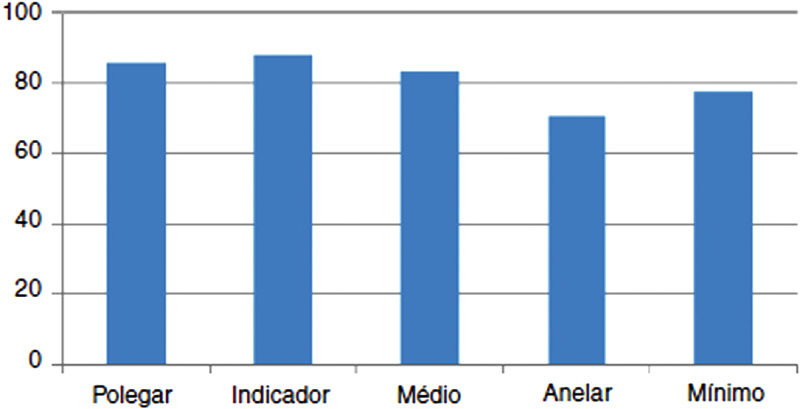
The distribution of the number of patients according to the affected anatomical region is shown in Table 3 . Out of 598 patients, 310 had injuries affecting the fingers, with 406 injured fingers; 243 patients (78.39%) had wounds in a single finger, and 67 (21.61%) presented with injuries in ≥ 2 fingers. From 243 cases of single-finger injury, the most affected finger was the thumb (78), followed by the index finger (62), the minimum finger (43), the middle finger (39), and the ring finger (21) ( Fig. 3 ). Considering these 406 fingers, the most affected finger was the index finger (88), followed by the thumb (86), the middle finger (83), the minimum finger (78), and the ring finger (71) ( Fig. 4 ).
Table 3. Lesion topography per patient.
| Topography | Number of cases | % |
|---|---|---|
| Arm | 13 | 2.18 |
| Elbow | 6 | 1.00 |
| Forearm | 144 | 24.08 |
| Wrist | 39 | 6.52 |
| Hand | 86 | 14.38 |
| Fingers | 310 | 51.84 |
Fig. 3.
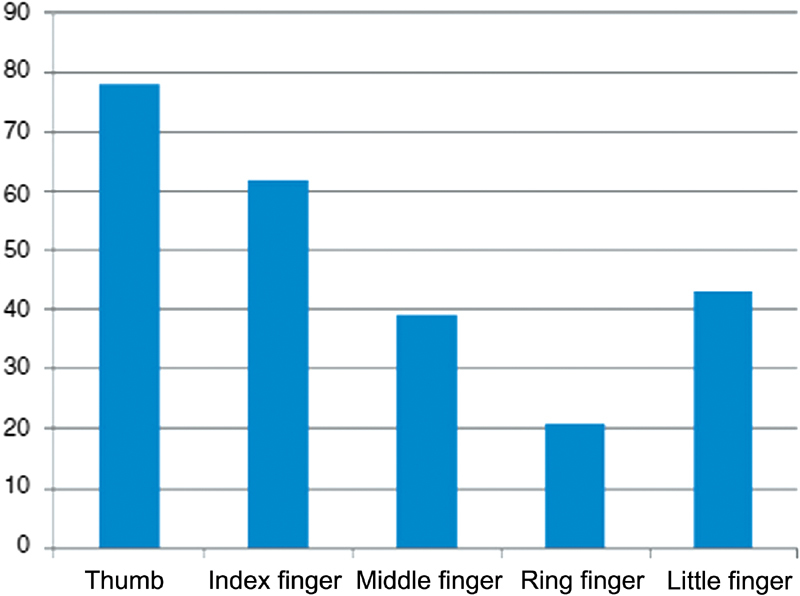
Number of lesions per finger in isolated injury cases.
Fig. 4.
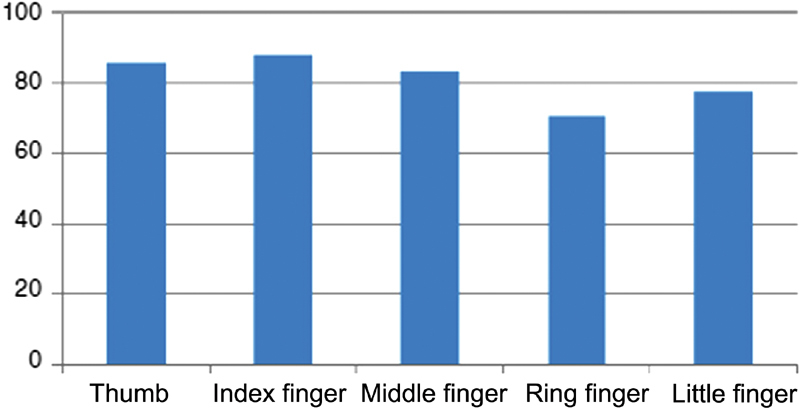
Number of lesions per finger in total injured fingers.
A total of 13 etiological agents were identified: traffic accidents, explosives, gunshot wounds, razor, kite string, power tools, industrial machine, automotive material, construction material, bites, other work-related objects, household objects, and glass ( Table 4 ). Among these etiological agents, glass produced 202 injuries (33.77%), followed by power tools, with 136 (22.74%), and razor, with 119 injuries (19.90%). Together, these 3 etiological agents accounted for 75.4% of the injuries.
Table 4. Lesion etiology from included events.
| Etiological agent | Number of cases | % |
|---|---|---|
| Glass | 202 | 33.78 |
| Power tools | 136 | 22.74 |
| Razors | 119 | 19.90 |
| Building material | 27 | 4.51 |
| Industrial machine | 26 | 4.35 |
| Work-related object | 24 | 4.01 |
| Traffic accidents | 19 | 3.18 |
| Bites | 12 | 2.01 |
| Gunshot wounds | 12 | 2.01 |
| Household objects | 9 | 1.50 |
| Automotive material | 6 | 1.00 |
| Explosives | 5 | 0.84 |
| Kite string | 1 | 0.17 |
Amputations were more prevalent in industrial machine injuries when compared to other etiological agents (26.42% vs. 2.20%; X 2 = 68.094; p < 0.05). Younger patients present a higher frequency of glass-related injuries (64.10% versus 31.66%; X 2 = 17.150 ; p < 0.05). Women presented a higher frequency of glass-related (47.37%% versus 29.89%; X 2 = 14.120 ; p < 0.05) and razor-related injuries (30.83% vs. 16.77%; X 2 = 12.813; p < 0.05) when compared with other etiological agents. The most frequent worker class in the sample, manual laborers, had a higher prevalence of power tools (34.11% vs. 11.37%; X 2 = 44.009 ; p < 0.05) and industrial machines-related injuries (7.02% versus 1.67%; X 2 = 10.294; p < 0.05), compared to other occupational classes, in addition to a higher prevalence of amputations (12.37% vs. 5.35%; X 2 = 9.130; p < 0.05).
Discussion
This populational sample presented at a hand surgery specialized center showed that patients most commonly treated in this service due to upper limb wounds are males, with an average age of 37.27 years old, and right-handed; in addition, injuries occur mainly in the dominant limb. This result is consistent with national and international studies reported in the literature. 3 5 8 Men from the economically-active age group are more exposed to causal agents of injuries, either in labor or household activities, such as minor repairs or renovations. The dominant hand is often the most affected, since it is the most exposed to etiological agents.
Since the literature reports that men are much more affected by upper limb injuries, these lesions are not valued and further analyzed in women. The present study found that razors and glass were much more significant as etiological agents in females, accounting for more than three quarters of these lesions. In our society, women typically do not handle power tools and building materials, in addition to being less affected by urban violence; as such, these etiological agents are less prevalent, with glass and razor standing out.
Regarding the location, most patients injured their fingers. The thumb was the most affected finger in isolated lesions. Cases with the involvement of multiple fingers showed no digital predominance or involvement pattern. These data are in agreement with the literature, with some studies reporting that the thumb is the most affected finger in isolated injuries 2 ; however, it is difficult to find literary studies regarding the frequency of finger involvement in lesions involving multiple digits.
Among the causative agents, glass injuries are prominent, resulting in approximately one-third of the lesions. As an etiological agent, glass becomes even more important when analyzing the proportion of the population < 18 years old, accounting for more than half of the injuries. Frequently, people from this age group are not exposed to other important etiological agents, such as power tools and industrial machines, so glass-related injuries may be more common. In similar literature studies, glass was not shown as the main etiological agent of upper limb injuries, lagging behind machine-induced lesions 8 9 and traffic accidents. 3 This difference may be explained by the selection of the patients according to penetrating injuries-related diagnoses rather than by closed traumas and fractures.
Manual laborers were the most affected by penetrating injuries, accounting for half of the sample, consistent with the literature. 5 In addition, these workers had a higher frequency of machine injuries and amputations, indicating more severe, higher energy lesions, possibly related to occupational activities.
Another relevant relationship demonstrated by the present study was the high prevalence of finger injuries caused by machines. Since young people are generally not exposed to other important etiological agents, such as power tools and industrial machines, glass may stand out. In similar literature studies, glass has not been shown to be the main etiological agent of upper limb injuries, lagging behind machine-induced lesions. 3 This difference may be explained by the selection of the patients according to penetrating injuries-related diagnoses rather than by closed traumas and fractures.
Manual laborers were the most affected by penetrating injuries, accounting for half of the sample, consistent with the literature. 5 In addition, these workers had a higher frequency of machine injuries and amputations, indicating more severe, higher energy lesions, possibly related to occupational activities.
Another relevant relationship demonstrated by the present study was the high prevalence of power tools-related injuries in patients in their 6 th decade of life or older. This data was not found in other literary studies, perhaps because this age group is not the most analyzed. Despite being more experienced, the elderly present reduced reflexes and abilities compared to younger people, which may explain the increased power tool-related lesions in this age group.
The present study is relevant because it represents an expressive population presented at a referral hand surgery service in a large Brazilian urban center caring for patients from different regions. Penetrating wounds are relatively frequent injuries with a significant social and economic impact. Knowing the most common etiological agents and the population most afflicted by a certain type of injury is of paramount importance to prepare more effective prevention strategies, which are the best way to address this issue. Therefore, we can conclude that we should focus more on strategies to prevent glass-related injuries in young people, razor- and glass-related injuries in women, and power tools-related wounds in the elderly and manual laborers. Since this is a retrospective study, it has a memory bias; in addition, because it was performed at a referral center, patients with penetrating wounds treated in primary and secondary services were not included in the analysis.
Conflitos de interesse Os autores declaram não haver conflitos de interesse.
Trabalho desenvolvido na Disciplina de Cirurgia da Mão e do Membro Superior, Departamento de Ortopedia e Traumatologia, Escola Paulista de Medicina, Universidade Federal de São Paulo, São Pulo, SP, Brasil. Publicado originalmente por Elsevier Ltda.
Work developed at Discipline of Hand and Upper Limb Surgery, Orthopedics and Traumatology Department of the Escola Paulista de Medicina of the Universidade Federal de São Paulo, São Paulo, SP, Brazil.
References
- 1.Burke F D, Dias J J, Lunn P G, Bradley M. Providing care for hand disorders: trauma and elective. The Derby Hand Unit experience (1989-1990) J Hand Surg [Br] 1991;16(01):13–18. doi: 10.1016/0266-7681(91)90119-9. [DOI] [PubMed] [Google Scholar]
- 2.Frank M, Lange J, Napp M, Hecht J, Ekkernkamp A, Hinz P.Accidental circular saw hand injuries: trauma mechanisms, injury patterns, and accident insurance Forensic Sci Int 2010198(1-3):74–78. [DOI] [PubMed] [Google Scholar]
- 3.Fonseca M RC, Mazzer N, Barbieri C H, Ellui V MC. Traumas da mão: estudo retrospectivo. Rev Bras Ortop. 2006;41(05):181–186. [Google Scholar]
- 4.Perera J. The pattern of tissue damage in occupational trauma. Ceylon Med J. 1996;41(01):15–18. [PubMed] [Google Scholar]
- 5.Trybus M, Lorkowski J, Brongel L, Hladki W. Causes and consequences of hand injuries. Am J Surg. 2006;192(01):52–57. doi: 10.1016/j.amjsurg.2005.10.055. [DOI] [PubMed] [Google Scholar]
- 6.Pardini A G, Jr, Tavares K E, Fonseca Neto J A. Lesöes da mäo em acidentes do trabalho: análise de 1.000 casos. Rev Bras Ortop. 1990;25(05):119–124. [Google Scholar]
- 7.O'Sullivan M E, Colville J. The economic impact of hand injuries. J Hand Surg [Br] 1993;18(03):395–398. doi: 10.1016/0266-7681(93)90072-n. [DOI] [PubMed] [Google Scholar]
- 8.Davas Aksan A, Durusoy R, Ada S, Kayalar M, Aksu F, Bal E. Epidemiology of injuries treated at a hand and microsurgery hospital. Acta Orthop Traumatol Turc. 2010;44(05):352–360. doi: 10.3944/AOTT.2010.2372. [DOI] [PubMed] [Google Scholar]
- 9.Souza M AP, Cabral L HA, Sampaio R F, Mancini M C. Acidentes de trabalho envolvendo mãos: casos atendidos em um serviço de reabilitacão. Fisioter Pesqui. 2008;15(01):64–71. [Google Scholar]