

Abstract
Purpose
In this study, we investigated the role of neutrophil to lymphocyte ratio (NLR) as a predictor of tumor response and as a prognostic factor in patients with rectal cancer who had undergone curative surgery after neoadjuvant chemoradiation therapy (nCRT).
Methods
Between January 2009 and July 2016, we collected 140 consecutive patients who had undergone curative intent surgery after nCRT due to rectal adenocarcinoma. We obtained the pre- and post-nCRT NLR by dividing the neutrophil count by the lymphocyte count. The cutoff value was obtained using receiver operating characteristic analysis for tumor response and using maximally selected rank analysis for recurrence-free survival (RFS). The relationship among NLR, tumor response, and RFS was assessed by adjusting the possible clinico-pathological confounding factors.
Results
The possibility of pathologic complete response (pCR) was significantly decreased in high pre- (>2.77) and postnCRT NLR (>3.23) in univariate regression analysis. In multivariate analysis, high post-nCRT NLR was an independent negative predictive factor for pCR (adjusted odds ratio, 0.365; 95% confidence interval [CI], 0.145–0.918). The 5-year RFS of all patients was 74.6% during the median 37 months of follow-up. Patients with higher pre- (>2.66) and post-nCRT NLR (>5.21) showed lower 5-year RFS rates (53.1 vs. 83.3%, P = 0.006) (69.2 vs. 75.7%, P = 0.054). In multivariate Cox analysis, high pre-nCRT NLR was an independent poor prognostic factor for RFS (adjusted hazard ratio, 2.300; 95% CI, 1.061–4.985).
Conclusion
Elevated NLR was a negative predictive marker for pCR and was independently associated with decreased RFS. For confirmation, a large-scale study with appropriate controls is needed.
Keywords: Neutrophile lymphocyte ratio, Rectal neoplasms, Chemoradiotherapy, Biomarkers, Prognosis
INTRODUCTION
Neoadjuvant chemoradiation therapy (nCRT) has been a standard treatment for locally advanced rectal cancer [1] and has contributed to improved local tumor control and superior survival rates [2]. However, the benefits of nCRT are not consistent for all patients with rectal cancer. About 50% of rectal cancers experience tumor regression and downstaging, while others remain in advanced stages [2].
Radiosensitivity depends on biological tumor characteristics. However, the tumor microenvironment and systemic inflammatory response (SIR) are also important to tumor regression after radiation [3, 4]. Intensive lymphocyte infiltration into the tumor is a well-known prognostic factor for various solid tumors [5]. In addition, the prognostic importance of several SIR indicators, such as C-reactive protein, white blood cell count, and modified Glasgow prognostic score, have frequently been reported [6-8]. The neutrophil to lymphocyte ratio (NLR), which can be obtained from a routine laboratory full blood count test, is emerging as a predictor of treatment response and prognosis [8-12].
The present study attempted to clarify the relationship of NLR to tumor response after nCRT and its influence on prognosis in rectal cancer cases.
METHODS
Patients
Between January 2009 and July 2016, we collected 140 consecutive patients who had undergone curative intent surgery after nCRT due to rectal adenocarcinoma at the Korea Cancer Center Hospital, Seoul, Korea.
All patients were identified from the institutional colorectal cancer database. We included patients with lower tumor border located below the sacral promontory on sagittal view of pelvic magnetic resonance imaging (MRI). We excluded patients with any acute infectious conditions at initiation of nCRT or rectal cancers associated with inflammatory bowel disease, hereditary cancer, familial adenomatous polyposis or other multiple polyposis syndromes, or recurrent or metastatic cancer. Institutional Review Board of Korea Cancer Center Hospital approved this retrospective study (K-1608-002-025) and exempted the informed consent.
Clinical staging, treatment, and postoperative follow-up
All patients underwent a preoperative staging work up including rectal MRI, computed tomography (CT) of the chest, abdomen, and pelvis, and a positron emission tomography scan.
Radiotherapy was performed with a dose of 50.4 Gy in 28 fractions. The concurrent chemotherapy regimen consisted of 3 cycles of 5-fluorouracil (425 mg/m2)/leucovorin (20 mg/m2) (FL) for 5 days with a 21-day interval. Two cycles were administered during the first and fifth weeks of radiotherapy, and the remaining cycle was administered during the resting period before surgery. The operation was performed 6–7 weeks after completion of radiotherapy. All operations were performed by 2 colorectal surgeons under the principle of total mesorectal excision with sharp and meticulous circumferential and longitudinal dissections along the mesorectal fascia to maintain the integrity of the mesorectal envelope. Adjuvant chemotherapy was recommended for all medically fit patients more than 4 weeks after radical resection with 3 additional cycles of the same FL regimen performed preoperatively. Postoperative follow-up consisted of a routine physical examination with CEA measurement every 3 to 6 months along with proctoscopy and a CT of the chest, abdomen, and pelvis every 6 to 12 months for 5 years.
Pathologic evaluation and blood count data
Standard pathologic tumor staging of the resected specimen was performed and recorded using the American Joint Committee on Cancer 7th edition TNM classification [13]. Pathologic response after nCRT was evaluated with the tumor regression grade (TRG) system suggested by the Gastrointestinal Pathology Study Group of the Korean Society of Pathologists [14]. Pathologic complete response (pCR) was defined as the absence of viable adenocarcinoma cells in the surgical specimen (ypT0N0).
We collected full blood count data from a pair of blood samples obtained prior to initiation of nCRT and just before surgery. The NLR was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count.
Statistical analysis
To compare categorical variables, chi-square or Fisher exact test was used. For continuous variables, independent or paired t-test and Wilcoxon rank-sum or signed-rank tests were used as appropriate. The optimal NLR cutoff values for tumor response and survival analyses were determined using receiver operating characteristic (ROC) analysis and maximally selected rank tests, respectively. Logistic regression was used to identify predictive factors for tumor response after nCRT. For survival analysis and comparison, the Kaplan-Meier and log-rank tests were used. For recurrence-free survival (RFS) analysis, events were defined as any type of recurrence or any cause of death. Cox proportional hazard regression analysis was performed for uni- and multivariate comparisons. Variables with P < 0.1 in univariate analysis were selected for multivariate regression. For multivariate regression, a backward stepwise elimination method was used. All tests were two-sided, and P < 0.05 was considered significant. Statistical analyses were performed using R ver. 3.5.0 (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
Baseline patient and tumor characteristics
Table 1 summarizes baseline characteristics and tumor information of 140 patients. The median age of the study population was 62.5 years (interquartile range [IQR], 55–72 years), and men were predominant. Lower tumor borders were frequently located below peritoneal reflection (85%).
Table 1.
Patient characteristics
| Characteristic | Value |
|---|---|
| Men | 93 (66.4) |
| Age (yr) | 62.5 (55.0–72.0) |
| ASA PS classification | |
| I | 10 (7.1) |
| II | 104 (74.3) |
| III | 26 (18.6) |
| CEA (ng/mL) | 3.6 (2.0–6.8) |
| Tumor location | |
| RA | 21 (15.0) |
| RB | 119 (85.0) |
| Perforation, yes | 3 (2.1) |
| Obstruction, yes | 11 (7.9) |
| Pre-nCRT NLR | 2.1 (1.7–2.9) |
| Post-nCRT NLR | 3.5 (2.5–4.5) |
| Clinical stage | |
| cT2 | 19 (13.6) |
| cT3 | 109 (77.9) |
| cT4a | 3 (2.1) |
| cT4b | 9 (6.4) |
| cN0 | 27 (19.3) |
| cN+ | 113 (80.7) |
| Delay after RT (wk) | 7.0 (6.0–7.0) |
| Operation | |
| APR | 32 (22.9) |
| Exenteration | 1 (0.7) |
| LAR | 52 (37.1) |
| uLAR | 55 (39.3) |
| Resection margin | |
| CRM involved | 2 (1.4) |
| DRM involved | 1 (0.7) |
| Pathologic stage | |
| ypT | |
| T0 | 29 (20.7) |
| T1 | 7 (5.0) |
| T2 | 35 (25.0) |
| T3 | 60 (42.9) |
| T4a | 3 (2.1) |
| T4b | 6 (4.3) |
| ypN | |
| N0 | 117 (83.6) |
| N1 | 15 (10.7) |
| N2 | 8 (5.7) |
| AJCC stage | |
| 0 (pCR) | 29 (20.7) |
| I | 39 (27.9) |
| II | 49 (35.0) |
| III | 23 (16.4) |
| Total retrieved LN | 9.0 (6.0–12.0) |
| Vascular invasion, yes | 10 (7.1) |
| Perineural invasion, yes | 25 (17.9) |
| Lymphatic invasion, yes | 7 (5.0) |
| Adjuvant chemotherapy, yes | 126 (90.0) |
Values are presented as number (%) or median (interquartile range).
ASA PS, American Society of Anesthesiologists physical status; CEA, carcinoembryonic antigen; RA, above peritoneal reflection; RB, below peritoneal reflection; nCRT, neoadjuvant chemoradiation therapy; NLR, neutrophil to lymphocyte ratio; RT, radiotherapy; APR, abdominoperineal resection; (u)LAR, (ultra) low anterior resection; CRM, circumferential resection margin; DRM, distal resection margin; AJCC, American Joint Committee on Cancer; pCR, pathologic complete response; LN, lymph node.
Eleven patients presented with obstruction; 7 of these had complete obstruction and underwent a stoma operation before nCRT. Four patients with intermittent and partial occlusion were treated with nCRT under careful observation without stoma.
About 9% of patients had clinical T4 stage, and about 80% of patients had clinical T3 stage. Surgeries were performed at a median of 7 weeks (IQR, 6.0–7.0 weeks) after completion of radiotherapy. Laparoscopic-assisted TME was used in 26 cases (18.6%). In this population, the sphincter sparing rate was 76.4%. Tumor perforation by traction force during operation occurred in 3 patients.
Pathologic examination identified 29 cases of total regression (20.7%) (pCR, ypT0N0). Stratification by TRG resulted in 20 cases of near total regression (14.3%), 60 cases of moderate regression (49.3%), and 22 cases of minimal or no regression (15.7%). By pathologic staging, 72 cases (51.4%) remained advanced stage (stage II/III), and 3 cases showed resection margin involvement. The median number of total examined lymph nodes was 9 (IQR, 6–12). The median values of pre- and post-nCRT NLR was 2.1 (IQR, 1.7–2.9) and 3.5 (IQR, 2.5–4.5), respectively.
NLR and tumor response after nCRT
In a descriptive analysis comparing pCR and non-pCR groups, the median value of pre-nCRT NLR was significantly higher in the non-pCR group (2.1 [IQR, 2.2–7.4] vs. 1.8 [IQR, 1.8–3.6], P = 0.042). Post-nCRT NLR was also higher in the non-pCR group, but the difference was not significant (P = 0.093). After ROC analysis to determine the optimal NLR cutoff value for pCR, pre-nCRT NLR of 2.77, and post-nCRT NLR of 3.23 were determined as optimal cutoffs. The frequency of pre-nCRT NLR >2.77 was significantly higher in the non-pCR group (36% vs. 13.8%, P = 0.038), and post-nCRT NLR was significantly higher in the non-pCR group (62.2% vs. 37.9%, P = 0.033). The median pre-nCRT CEA level of the non-pCR group was significantly higher (4.1 ng/mL [IQR, 2.2-7.4 ng/mL] vs. 2.4 ng/mL [IQR, 1.8–3.6 ng/mL], P = 0.008), as was the rate of clinical node positive (cN+) status (86.5% vs. 58.6%) (Table 2).
Table 2.
Descriptive analysis of pCR-related factors
| Variable | pCR (n = 29) | Non-pCR (n = 111) | P-value |
|---|---|---|---|
| Men | 19 (65.5) | 74 (66.7) | 1 |
| Age (yr) | 60.0 (55.0–68.0) | 65.0 (55.5–72.0) | 0.385 |
| CEA (ng/mL) | 2.4 (1.8–3.6) | 4.1 (2.2–7.4) | 0.008 |
| Pre-nCRT NLR | 1.8 (1.5–2.6) | 2.1 (1.7–3.0) | 0.042 |
| Post-nCRT NLR | 3.0 (2.5–3.8) | 3.7 (2.6–4.9) | 0.093 |
| Delay after RT (wk) | 7.0 (6.0–7.0) | 7.0 (6.0–7.0) | 0.641 |
| Tumor differentiation | 1 | ||
| Well/moderate | 28 (96.6) | 105 (94.6) | |
| Poor/mucinous | 1 (3.4) | 6 (5.4) | |
| cT4, yes | 0 (0) | 12 (10.8) | 0.139 |
| cN1, yes | 17 (58.6) | 96 (86.5) | 0.002 |
| Tumor location | 1 | ||
| RA | 4 (13.8) | 17 (15.3) | |
| RB | 25 (86.2) | 94 (84.7) | |
| Perforation, yes | 0 (0) | 3 (2.7) | 0.861 |
| Obstruction, yes | 1 (3.4) | 10 (9.0) | 0.546 |
| Pre-nCRT NLR > 2.77 | 4 (13.8) | 40 (36.0) | 0.038 |
| Post-nCRT NLR > 3.23 | 11 (37.9) | 69 (62.2) | 0.033 |
Values are presented as number (%) or median (interquartile range).
pCR, pathologic complete response; CEA, carcinoembryonic antigen; nCRT, neoadjuvant chemoradiation therapy; NLR, neutrophil to lymphocyte ratio; RT, radiotherapy; RA, above peritoneal reflection; RB, below peritoneal reflection.
Logistic regression regarding the association of pCR and other variables revealed that cN+ status, elevated CEA level, pre-nCRT NLR >2.77, and post-nCRT NLR >3.23 were all negative predictive factors for pCR by univariate analysis. After multivariate analysis, post-nCRT NLR >3.23 remained an independent negative predictive factor for pCR (adjusted odds ratio [OR], 0.365; 95% confidence interval [CI], 0.145–0.918) (Table 3).
Table 3.
Predictive factors for pathologic complete response using logistic regression analysis
| Variable | Univariate analysis |
Multivariate analysis |
||||
|---|---|---|---|---|---|---|
| OR | 95% CI | P-value | OR | 95% CI | P-value | |
| Age | 0.984 | 0.946–1.023 | 0.418 | |||
| Male sex | 0.950 | 0.401–2.248 | 0.907 | |||
| RB location | 1.130 | 0.349–3.660 | 0.838 | |||
| cT4 | 0.000 | 0.000–∞ | 0.989 | |||
| cN+ | 0.221 | 0.099–0.554 | 0.001 | 0.244 | 0.091–0.651 | 0.005 |
| PD/MUC | 0.625 | 0.072–5.407 | 0.669 | |||
| Delay after RT | 0.975 | 0.747–1.274 | 0.854 | |||
| CEA> 3.3 ng/mL | 0.250 | 0.102–0.615 | 0.003 | 0.284 | 0.109–0.783 | 0.010 |
| pre-nCRT NLR > 2.77 | 0.296 | 0.096–0.913 | 0.034 | |||
| post-nCRT NLR > 3.23 | 0.372 | 0.160–0.864 | 0.021 | 0.365 | 0.145–0.918 | 0.032 |
OR, odds ratio; CI, confidence interval; RB, below peritoneal reflection; RT, radiotherapy; CEA, carcinoembryonic antigen; nCRT, neoadjuvant chemoradiation therapy; NLR, neutrophil to lymphocyte ratio.
NLR and RFS
During the median 37-month (IQR, 19.5–58.0) follow-up, there were 29 RFS events. Recurrence was identified in 27 patients and occurred most frequently in the lung (n = 12), followed by liver and distant lymph node metastasis. The 5-year RFS of all patients was 74.6%.
Using maximally selected rank analysis, the optimal NLR cutoff value for RFS was obtained; pre-nCRT NLR was 2.66 and post-nCRT NLR was 5.21. Patients with pre-nCRT NLR >2.66 showed significantly worse 5-year RFS than patients with pre-nCRT NLR ≤2.66 (83.3% vs. 55.2%, P = 0.014) (Fig. 1). The 5-year RFS of the group with post-nCRT NLR >5.21 showed a lower 5-year RFS (69.2 vs. 76.7%, P = 0.038) (Fig. 2).
Fig. 1.
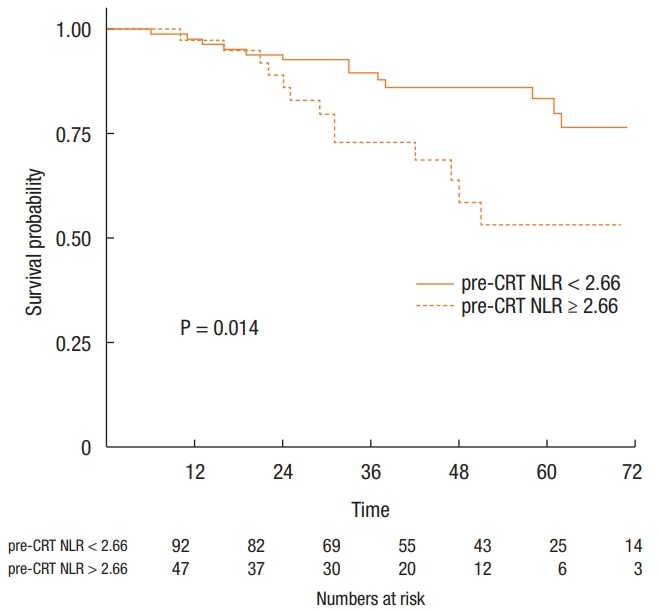
Recurrence-free survival according to pre-nCRT NLR using Kaplan-Meier analysis. Group with pre-CRT NLR >2.66 showed lower 5-year RFS (55.2% vs. 83.3%, P = 0.014). nCRT, neoadjuvant chemoradiation therapy; NLR, neutrophil to lymphocyte ratio; RFS, recurrence-free survival.
Fig. 2.
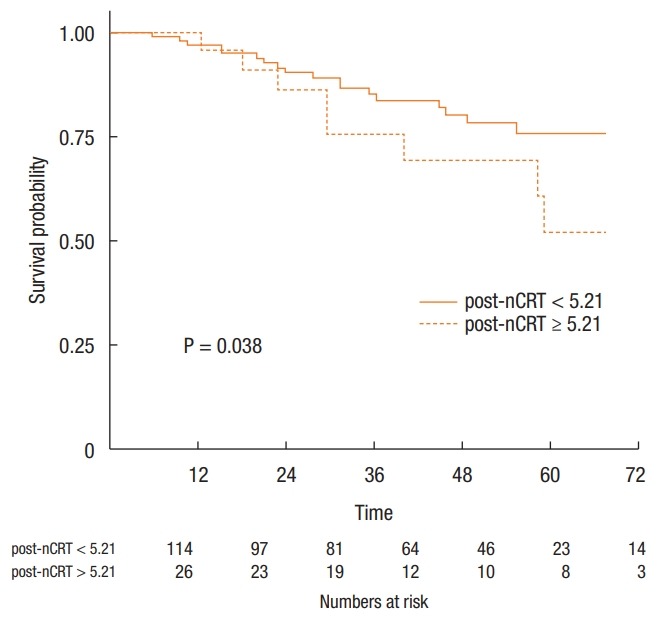
Recurrence-free survival according to post-nCRT NLR using Kaplan-Meier analysis. Group with post-nCRT >5.21 showed lower 5-year RFS (69.2 vs. 76.7%, P = 0.038). nCRT, neoadjuvant chemoradiation therapy; NLR, neutrophil to lymphocyte ratio; RFS, recurrence-free survival.
In univariate Cox regression analysis, increased pre- (hazard ratio [HR], 2.750; 95% CI, 1.304–5.799) and post-nCRT NLR (HR, 2.160; 95% CI, 0.969–4.816) were associated with poor prognosis. In multivariate Cox analysis with other significant factors in univariate analysis, pre-nCRT NLR >2.77 remained a poor independent prognostic factor for RFS (adjusted HR, 2.300; 95% CI, 1.061–4.985) (Table 4).
Table 4.
Prognostic factors associated with recurrence-free survival using Cox regression analysis
| Variable | Univariate |
Multivariate |
||||
|---|---|---|---|---|---|---|
| HR | 95% CI | P-value | HR | 95% CI | P-value | |
| Male | 2.314 | 0.875–6.117 | 0.091 | 2.301 | 0.707–7.482 | 0.166 |
| Age | 1.008 | 0.973–1.044 | 0.668 | |||
| ASA PS classifcation ≥ III | 0.906 | 0.341–2.409 | 0.843 | |||
| pre-nCRT NLR >2.66 | 2.750 | 1.304–5.799 | 0.008 | 2.300 | 1.061–4.985 | 0.035 |
| post-nCRT NLR >5.21 | 2.160 | 0.969–4.816 | 0.060 | |||
| CEA | 1.010 | 1.001–1.019 | 0.038 | 1.013 | 1.000–1.026 | 0.047 |
| cN1, yes | 1.201 | 0.457–3.162 | 0.710 | |||
| APR, yes | 2.066 | 0.967–4.413 | 0.061 | |||
| ypStage II/III | 3.937 | 1.595–9.720 | 0.003 | 2.761 | 0.978–7.792 | 0.055 |
| PD/MUC | 1.444 | 0.341–6.119 | 0.618 | |||
| Obstruction | 4.530 | 1.662–12.344 | 0.003 | 2.694 | 0.935–7.759 | 0.066 |
| N. of total retrieved LN | 0.987 | 0.932–1.046 | 0.669 | |||
| Lymphatic invasion, yes | 0.465 | 0.062–3.480 | 0.456 | |||
| Perineural invasion, yes | 4.812 | 2.227–10.398 | <0.001 | 2.592 | 1.063–6.320 | 0.036 |
| Vascular invasion, yes | 5.384 | 2.258–12.835 | <0.001 | |||
| pT4, yes | 9.063 | 2.663–30.849 | 0.003 | |||
| R1 resection | 4.425 | 1.646–11.896 | <0.001 | |||
| Adjuvant chemotherapy | 1.128 | 0.338–3.767 | 0.845 | |||
HR, hazard ratio; CI, confidence interval; ASA PS, American Society of Anesthesiologists physical status; CEA, carcinoembryonic antigen; APR, abdominoperineal resection; LN, lymph node.
DISCUSSION
In this study, increased preoperative NLR was significantly related to poor radiation response and RFS. Although multivariate regression with stepwise elimination methods showed that elevated post-nCRT NLR was independently associated with tumor response, and pre-nCRT NLR was independently associated with RFS, both factors were significantly associated with tumor response and RFS in univariate analyses.
The use of NLR as a prognostic indicator for SIR was originally described in a critically ill patient in the intensive care unit [15]. However, it has also been considered a predictive factor for survival outcome in a variety of cancers due to its performance and availability [8, 16].
NLR reflects the balance of host immunity between pro- and anti-tumor activities. A high circulating neutrophil count is considered to have pro-tumor properties because inflammatory cytokines released from neutrophils induce angiogenesis and provoke tumor growth [17]. Previous studies have shown that neutrophils can suppress T-cell response through production of reactive oxygen species, nitric oxide, and arginase. Lymphocytes, especially CD4+ or CD8+ T cells, are thought to play a key role in anti-tumor host immunity [18] by inducing tumor cell apoptosis. Intensive lymphocyte infiltration into tumor cells indicates a positive prognosis [5], and the positive relationship between circulating lymphocyte count and degree of tumor regression has been previously described [19]. Thus, high NLR suggests a pro-tumor status and higher possibility of poor radiation response, while low NLR suggests anti-tumor status and a higher possibility of positive tumor response and survival [9, 12, 19, 20]. In this study, patients with a high NLR showed poor tumor response after nCRT and a decreased survival outcome, in accordance with previous findings.
In addition to NLR, other SIR markers derived from the complete blood count (CBC) have been investigated for their prognostic roles [21-24]. Chan et al. [24] reported that elevated lymphocyte to monocyte ratio (LMR) was associated with increased overall survival, but independent association of the NLR and platelet to lymphocyte ratio (PLR) was not found in colorectal cancer. Jung et al. reported that patients with rectal cancer and high LMR, high PLR, or low NLR were associated with increased RFS, and high PLR was an independent marker for RFS after surgery following nCRT. However, no relationship to tumor response was found [23]. In the current study, we analyzed the relationships between PLR and treatment outcomes (tumor response, RFS) but did not find an association. Due to the negative results, we excluded this analysis from this manuscript.
Various cutoff values have been used to define elevated NLR groups in previous studies. However, the NLR cutoff values used in previous studies of patients with rectal cancer that underwent nCRT were inconsistent. Some studies used historical values from other primary or metastatic cancers [12, 20, 25], and other studies used cutoff values calculated by statistical methods [23, 26, 27]. In the current study, cutoff values were determined after calculation by statistical methods. ROC analysis was used for tumor response, and maximally selected rank analysis was used for RFS. The latter method included time as a variable, and we suggest this test might be more appropriate for survival analysis. To our knowledge, only three studies used calculated cutoffs in this setting [23, 26, 27]. Shen et al. [27] used ROC analysis to determine a pretreatment NLR cutoff of 2.8 for overall survival, which was similar to our pre-CRT NLR cutoff of 2.66 for RFS. The maximally selected rank analysis used in our study is the same statistical method used by Sung et al. [26]. Cutoff values were 1.75 for pre-CRT NLR and 5.14 for post-CRT NLR. In the largest retrospective study carried out prior to the current study, the cutoff was determined by log rank test using the Contal and O’Quigley method [23]. Their pretreatment NLR cutoff was 1.7, and higher NLR showed decreased RFS. The calculated cutoff can be influenced by size, characteristics of the sample population, and outcome variables, so interstudy discrepancies may exist. To obtain optimized generally acceptable cutoff values, a well-controlled large-scale study is needed.
As a limitation of this study, the sample size was small and provided insufficient data to draw confirmative results. Due to the retrospective study design, unmeasured confounding factors may exist. Additionally, underlying inflammatory conditions may influence CBC composition. Although patients with documented acute infectious or other inflammatory conditions were not included in the study, it is possible that patients with undocumented infectious conditions were included.
Selection bias might contribute to our relatively high pCR rate (20.7%). The relatively long interval between termination of nCRT or operation and additional consolidation chemotherapy treatment are possible contributors to higher pCR rates. However, the high proportion of cT2N+ patients in the current study cannot be ignored. To obtain confirmative results and establish the role of CBC-based markers, a large-scale study with clinical stage subgroup analysis is necessary.
In conclusion, in our small cohort of patients with rectal cancer treated with nCRT followed by surgery, elevated NLR was a negative predictive marker for pCR and was independently associated with decreased RFS, despite previously mentioned limitations. A future well-controlled, large-scale prospective study is needed to gather further comprehensive information on the role of CBC-derived biomarkers.
Footnotes
No potential conflict of interest relevant to this article was reported.
REFERENCES
- 1.Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, Fietkau R, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004;351:1731–40. doi: 10.1056/NEJMoa040694. [DOI] [PubMed] [Google Scholar]
- 2.Park IJ, You YN, Agarwal A, Skibber JM, Rodriguez-Bigas MA, Eng C, et al. Neoadjuvant treatment response as an early response indicator for patients with rectal cancer. J Clin Oncol. 2012;30:1770–6. doi: 10.1200/JCO.2011.39.7901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Barcellos-Hoff MH, Park C, Wright EG. Radiation and the microenvironment - tumorigenesis and therapy. Nat Rev Cancer. 2005;5:867–75. doi: 10.1038/nrc1735. [DOI] [PubMed] [Google Scholar]
- 4.Prise KM, Schettino G, Folkard M, Held KD. New insights on cell death from radiation exposure. Lancet Oncol. 2005;6:520–8. doi: 10.1016/S1470-2045(05)70246-1. [DOI] [PubMed] [Google Scholar]
- 5.Sato E, Olson SH, Ahn J, Bundy B, Nishikawa H, Qian F, et al. Intraepithelial CD8+ tumor-infiltrating lymphocytes and a high CD8+/regulatory T cell ratio are associated with favorable prognosis in ovarian cancer. Proc Natl Acad Sci U S A. 2005;102:18538–43. doi: 10.1073/pnas.0509182102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.McMillan DC. Systemic inflammation, nutritional status and survival in patients with cancer. Curr Opin Clin Nutr Metab Care. 2009;12:223–6. doi: 10.1097/MCO.0b013e32832a7902. [DOI] [PubMed] [Google Scholar]
- 7.Smith RA, Bosonnet L, Raraty M, Sutton R, Neoptolemos JP, Campbell F, et al. Preoperative platelet-lymphocyte ratio is an independent significant prognostic marker in resected pancreatic ductal adenocarcinoma. Am J Surg. 2009;197:466–72. doi: 10.1016/j.amjsurg.2007.12.057. [DOI] [PubMed] [Google Scholar]
- 8.Malietzis G, Giacometti M, Kennedy RH, Athanasiou T, Aziz O, Jenkins JT. The emerging role of neutrophil to lymphocyte ratio in determining colorectal cancer treatment outcomes: a systematic review and meta-analysis. Ann Surg Oncol. 2014;21:3938–46. doi: 10.1245/s10434-014-3815-2. [DOI] [PubMed] [Google Scholar]
- 9.Kim IY, You SH, Kim YW. Neutrophil-lymphocyte ratio predicts pathologic tumor response and survival after preoperative chemoradiation for rectal cancer. BMC Surg. 2014;14:94. doi: 10.1186/1471-2482-14-94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kishi Y, Kopetz S, Chun YS, Palavecino M, Abdalla EK, Vauthey JN. Blood neutrophil-to-lymphocyte ratio predicts survival in patients with colorectal liver metastases treated with systemic chemotherapy. Ann Surg Oncol. 2009;16:614–22. doi: 10.1245/s10434-008-0267-6. [DOI] [PubMed] [Google Scholar]
- 11.Templeton AJ, McNamara MG, Šeruga B, Vera-Badillo FE, Aneja P, Ocaña A, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014;106:dju124. doi: 10.1093/jnci/dju124. [DOI] [PubMed] [Google Scholar]
- 12.Carruthers R, Tho LM, Brown J, Kakumanu S, McCartney E, McDonald AC. Systemic inflammatory response is a predictor of outcome in patients undergoing preoperative chemoradiation for locally advanced rectal cancer. Colorectal Dis. 2012;14:e701–7. doi: 10.1111/j.1463-1318.2012.03147.x. [DOI] [PubMed] [Google Scholar]
- 13.Edge SB, Bytd DR, Compton CC, Fritz AG, Greene FL, Trotti A. American Joint Committee on Cancer, Colon and rectum, AJCC cancer staging manual. New York: Springer; 2009. [Google Scholar]
- 14.Chang HJ, Park CK, Kim WH, Kim YB, Kim YW, Kim HG, et al. A standardized pathology report for colorectal cancer. Korean J Pathol. 2006;40:193–203. [Google Scholar]
- 15.Zahorec R. Ratio of neutrophil to lymphocyte counts--rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102:5–14. [PubMed] [Google Scholar]
- 16.Guthrie GJ, Charles KA, Roxburgh CS, Horgan PG, McMillan DC, Clarke SJ. The systemic inflammation-based neutrophil-lymphocyte ratio: experience in patients with cancer. Crit Rev Oncol Hematol. 2013;88:218–30. doi: 10.1016/j.critrevonc.2013.03.010. [DOI] [PubMed] [Google Scholar]
- 17.McCourt M, Wang JH, Sookhai S, Redmond HP. Proinflammatory mediators stimulate neutrophil-directed angiogenesis. Arch Surg. 1999;134:1325–31. doi: 10.1001/archsurg.134.12.1325. [DOI] [PubMed] [Google Scholar]
- 18.Badoual C, Hans S, Rodriguez J, Peyrard S, Klein C, Agueznay Nel H, et al. Prognostic value of tumor-infiltrating CD4+ T-cell subpopulations in head and neck cancers. Clin Cancer Res. 2006;12:465–72. doi: 10.1158/1078-0432.CCR-05-1886. [DOI] [PubMed] [Google Scholar]
- 19.Kitayama J, Yasuda K, Kawai K, Sunami E, Nagawa H. Circulating lymphocyte number has a positive association with tumor response in neoadjuvant chemoradiotherapy for advanced rectal cancer. Radiat Oncol. 2010;5:47. doi: 10.1186/1748-717X-5-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Krauthamer M, Rouvinov K, Ariad S, Man S, Walfish S, Pinsk I, et al. A study of inflammation-based predictors of tumor response to neoadjuvant chemoradiotherapy for locally advanced rectal cancer. Oncology. 2013;85:27–32. doi: 10.1159/000348385. [DOI] [PubMed] [Google Scholar]
- 21.Szkandera J, Pichler M, Absenger G, Stotz M, Arminger F, Weissmueller M, et al. The elevated preoperative platelet to lymphocyte ratio predicts decreased time to recurrence in colon cancer patients. Am J Surg. 2014;208:210–4. doi: 10.1016/j.amjsurg.2013.10.030. [DOI] [PubMed] [Google Scholar]
- 22.Tan D, Fu Y, Su Q, Wang H. Prognostic role of platelet-lymphocyte ratio in colorectal cancer: a systematic review and meta-analysis. Medicine (Baltimore) 2016;95:e3837. doi: 10.1097/MD.0000000000003837. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Jung SW, Park IJ, Oh SH, Yeom SS, Lee JL, Yoon YS, et al. Association of immunologic markers from complete blood counts with the response to preoperative chemoradiotherapy and prognosis in locally advanced rectal cancer. Oncotarget. 2017;8:59757–65. doi: 10.18632/oncotarget.15760. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chan JC, Chan DL, Diakos CI, Engel A, Pavlakis N, Gill A, et al. The Lymphocyte-to-monocyte ratio is a superior predictor of overall survival in comparison to established biomarkers of resectable colorectal cancer. Ann Surg. 2017;265:539–46. doi: 10.1097/SLA.0000000000001743. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Nagasaki T, Akiyoshi T, Fujimoto Y, Konishi T, Nagayama S, Fukunaga Y, et al. Prognostic impact of neutrophil-to-lymphocyte ratio in patients with advanced low rectal cancer treated with preoperative chemoradiotherapy. Dig Surg. 2015;32:496–503. doi: 10.1159/000441396. [DOI] [PubMed] [Google Scholar]
- 26.Sung S, Son SH, Park EY, Kay CS. Prognosis of locally advanced rectal cancer can be predicted more accurately using pre- and post-chemoradiotherapy neutrophil-lymphocyte ratios in patients who received preoperative chemoradiotherapy. PLoS One. 2017;12:e0173955. doi: 10.1371/journal.pone.0173955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Shen L, Zhang H, Liang L, Li G, Fan M, Wu Y, et al. Baseline neutrophil-lymphocyte ratio (≥2.8) as a prognostic factor for patients with locally advanced rectal cancer undergoing neoadjuvant chemoradiation. Radiat Oncol. 2014;9:295. doi: 10.1186/s13014-014-0295-2. [DOI] [PMC free article] [PubMed] [Google Scholar]