

Abstract
Results of previous studies about the effect of Kangaroo Mother Care (KMC) on hospital management indicators (HMIs) (length of stay [LOS], readmission to hospital, parent satisfaction, and parent's preference for same postdelivery care) had high confusions. The aim of this study was to conduct a systematic review and meta-analysis of randomized controlled trials on the effect of KMC on HMI in comparison with the conventional neonatal care (CNC). In this systematic review and meta-analysis study, required data were collected by searching the following keywords: “length of stay,” “readmission to hospital,” satisfaction,” same post-delivery,” “hospital management,” indicators, “skin-to-skin,” “Kangaroo Mother Care,” randomized trial. The following databases were searched: Google Scholar, PubMed, EMBASE, Scopus, and Cochrane. To estimate the hospital management indicators, computer software Comprehensive Meta-Analysis 2 was used. Finally, 18 articles were included to analysis. The overall LOS standard different between groups (KMC vs. CNC) was − 0.91 days (95% confidence interval [CI], −2.14–0.32, Q = 25.6, df = 10, P = 0.004, I2 = 60.98). The overall readmission to hospital standard different between groups was − 1.78% (95% CI, −1.21%–0.86%, Q = 0.024, df = 1, P = 0.87, I2 = 0.00). The overall parent satisfaction standard different between groups was 5.3% (95% CI, −32.4%–43%, Q = 0.052, df = 2, P = 0.97, I2 = 0.00). The overall standard different between groups was 16.2% (95% CI, −24.7%–57.1%, Q = 0.040, df = 1, P = 0.84, I2 = 0.00). KMC improves HMI but not significantly. According to the current study result and other studies that report positive effect of KMC on health status of the newborns and parents, implemented of KMC in low- and middle-income countries recommended.
Keywords: Conventional neonatal care, hospital management indicators, Kangaroo Mother Care, skin-to-skin
Introduction
Among the existing groups in the community, babies’ health has a higher priority in receiving health services because of a direct connection with public health, which requires the government and communities to pay more attention to this issue.[1,2,3]
Healthy babies are the real wealth of societies that their survival and health are considered community-driven development, in addition to their importance as the human and individual right.[4] Due to certain physical circumstances and the rapid growth and influence of various environmental factors, etc., babies are considered the most vulnerable segments of society and they need appropriate health care and treatment with high quality.[5,6,7,8,9,10]
One of the most important factors in care of neonatal is midwifery care and interventions, including mother–neonate separation immediately after birth, which can lead to adverse impacts on infants and their parents.[11] To alleviate this issue, Kangaroo Mother Care (KMC) technique has been recommended by the WHO. It is a type of neonatal care practice, in which the neonate is carried while having skin-to-skin contact with their parent.[12]
Evidence and records of the studies introduce the effectiveness of KMC's criteria in reducing babies’ mortality, complications, reinforce breastfeeding, growth, and heat protection of baby and improving other physiological parameters.[12,13,14,15,16,17,18,19,20,21] In addition to the impact of the KMC on the babies and their parents, the studies’ results show the effect of this method on some indicators of hospital management.[22,23,24,25,26,27]
Results of previous studies about the effect of KMC on hospital management indicators (HMIs) (length of stay [LOS], readmission to hospital, parent satisfaction, and parent's preference for same postdelivery care) had high confusions. In this regard, the aim of this study was to conduct a systematic review and meta-analysis of randomized controlled trials on the effect of KMC on HMI in comparison with the conventional neonatal care (CNC).
Methods
Current systematic review and meta-analysis study were conducted in 2016, using the approach of systematic review adopted from the book entitled, “A Systematic Review to Support Evidence-Based Medicine.”[28] Also in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses.[29,30,31]
Inclusion and excluded criteria
The eligibility criteria for inclusion or exclusion of articles are summarized in Table 1.
Table 1.
Inclusion and excluded criteria for selection of KMC studies
| Inclusion criteria (PICOTS) | Excluded criteria |
|---|---|
| Population: LBW and VLBW baby pairs and their parents | Articles published in non-English language |
| Intervention: KMC (skin-to-skin contact) | Community-based articles |
| Comparison: CNC | Pilots study articles |
| Outcome: HMI (length of stay, readmission to hospital, parent satisfaction and parents preference for same postdelivery care) | Articles with <10 sample size |
| Time: 0 day-18 month after intervention | Articles published earlier than January 1, 2000 |
| Study design: randomized controlled trial studies | Specific kind of articles (conference presentations, case reports and qualitative studies) |
CNC=Conventional neonatal care, LBW=Low birth weight, VLBW=Very LBW, HMI=Hospital management indicators, KMC=Kangaroo Mother Care
Information sources and search strategy
Required data were collected by searching the following keywords: “length of stay,” “readmission to hospital,” satisfaction,” same post-delivery,” “hospital management,” indicators, “skin-to-skin,” “Kangaroo Mother Care,” “randomized trial.” The complete search strategy for PubMed databases is shown in Table 2. The search of databases was done through two of the researcher who had enough experience in search (J.M and D.N).
Table 2.
Complete search strategy for PubMed databases
| Search | Recent queries in PubMed | Item found |
|---|---|---|
| #1 | (((((“satisfaction”[Title/Abstract]) OR “hospital management”[Title/Abstract]) OR “hospital performanc”[Title/Abstract]) OR “indicator*”[Title/Abstract]) OR “index “[Title/Abstract]) OR “Length of Stay”[Title/Abstract]) OR ”Readmission to hospital”[Title/Abstract]) OR “same post-delivery”[Title/Abstract] | 958,452 |
| #2 | (“skin-to-skin”[Title/Abstract]) OR “KMC”[Title/Abstract] | 1367 |
| #3 | #1 AND #2 | 21* |
*Filters activated: Clinical Trial, English. KMC=Kangaroo Mother Care
The following databases were searched: Google Scholar, PubMed, EMBASE, Scopus, and Cochrane Central Register of Controlled Trials. Furthermore, manual search was conducted by two authors (J.M and D.N) in some of the relevant journals and websites. These authors also reviewed and selected articles reference of reference, grey literature, and expert contact also were done. Two authors (P.H and A.Z) independently assessed the relevant full-text articles for eligibility according to the predefined criteria. Any disagreements between investigators were resolved through discussing with third and fourth investigator (F.F and P.H).
Review process
Two authors (J.M and F.F) who had enough experience and knowledge were responsible for independent extraction of the data. Two extraction tables were designed in the first phase of the review process which included the following items:
Characteristics of studies
Name of first author, article published year, country, sample size, gestational age (week), birth weight (g), delivery type (% of cesarean), KMC duration per day (hours), KMC start time.
Hospital management indicators
First author's name, study publish year, LOS, readmission to hospital, parent satisfaction, and parent's preference for the same postdelivery care. Validity of the designed tables improved using three hospital managers’, four obstetricians’, and five midwifery experts’ opinion. A pilot study was conducted to more improvement of the tables.
Assessment of risk of bias
The risk of bias of included articles was evaluated with the criteria outlined in the Cochrane Handbook.[32] These criteria included six dimensions of risk of bias: sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other sources of bias. The result of risk of bias assessment with this tool included low risk of bias, high risk of bias, and unclear or unknown.
Data analysis
Computer software Comprehensive Meta-Analysis 2 (Englewood, NJ, USA) was employed to estimate the HMI. Forest plot was used for reporting the indicators. Sample size is shown in the forest plot by the size of each square. Confidence interval (CI) is shown by lines on each side of the square. HMIs were calculated based on fixed and random effect model with 95% CI. Heterogeneity between studies was assessed using I2 (I2≥50% indicates heterogeneity). Funnel plot was used to assess the possibility of publication bias.
Results
Of 290 identified articles, finally, 18 articles included in the analysis [Figure 1]. As seen in Figure 1, 156 studies excluded due to duplication. In the next phase, 98 articles were excluded in abstracts and titles screening and seven further articles excluded in full-text review phase.
Figure 1.
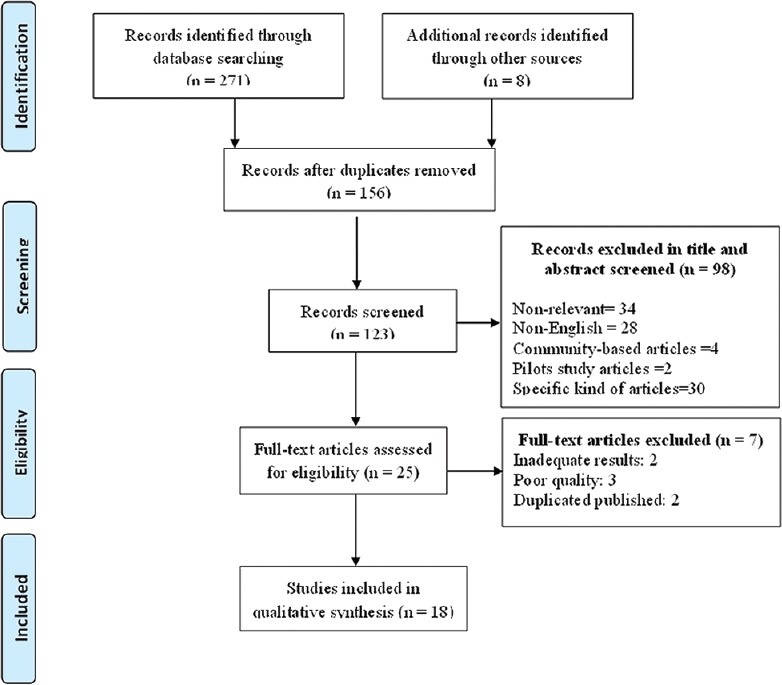
Searches and inclusion process
Characteristics of included studies and HMI results are summarized in Tables 3 and 4, respectively. Studies reviewed in the current study had been conducted in 11 countries, mainly in India (7 studies). 1190 (66.1 people/per study) participants in the KMC group and 1157 (64.2 people/per study) participants in the CNC group were examined. The average gestational age of participants in KMC group was 34.9 weeks and in CNC group was 35 weeks. The mean birth weight was 2060.2 ± 928.1 g and 2028 ± 890.6 g in the KMC and CNC groups, respectively. Cesarean contains 53.8% of deliveries type. The mean length of KMC was nearly 4 h per day. In eight studies, KMC was initiated immediately.
Table 3.
Characteristics of included studies
| Author: Year | Country | Participants (n) | Gestational age (week) | Birth weight (g) | Delivery type (percentage of cesarean) | SSC duration per day (h) | SSC start | |||
|---|---|---|---|---|---|---|---|---|---|---|
| KMC | CNC | KMC | CNC | KMC | CNC | |||||
| Roberts et al., 2000[25] | Australia | 16 | 14 | 31.7 | 31.2 | 1562 | 1481 | 77 | 1.6 | - |
| Carfoot et al., 2005[33] | UK | 102 | 102 | >38 | >38 | - | - | 28 | - | Immediately |
| Dehghani et al., 2015[34] | Iran | 27 | 26 | 34.4 | 35 | 2268.8 | 2192.2 | - | 1 h each day for 3 days | - |
| Charpak et al., 2001[35] | France | 382 | 364 | ≤32:36 ≥32:64 |
≤32:30 ≥32:70 |
1705 | 1735 | 68 | 24 h/day | - |
| Swarnkar and Vagha, 2016[18] | India | 30 | 30 | 35.4 | 35.9 | 1815.5 | 1859 | - | 8 h | Immediately |
| Gathwala et al.[36] | India | 50 | 50 | 35.4 | 35 | 1690 | 1690 | - | 6 h | - |
| Mahmood et al., 2011[37] | Pakistan | 80 | 80 | 38.9 | 38.9 | 3058 | 3036 | 0 | - | - |
| Srivastava et al., 2014[38] | US | 10 | 10 | 39.8 | 39.7 | 3734 | 3341 | - | 2 h | Immediately |
| Suman et al., 2008[39] | India | 103 | 103 | 35.3 | 35.9 | 1683.4 | 1723.6 | - | 1-2 h | Immediately |
| Ghavane et al., 2012[40] | India | 68 | 68 | 30.8 | 30.7 | 1170 | 1198 | 86 | 8 h | - |
| Nagai et al., 2011[41] | Madagascar | 29 | 26 | 36.8 | 36 | 2082.2 | 2074.3 | 25.3 | - | Immediately |
| Ramanathan et al., 2001[42] | India | 14 | 14 | 30.4 | 30.9 | 1219 | 1270.9 | 46.4 | 4 h | - |
| Acharya et al., 2014[22] | Nepal | 63 | 63 | 32.2 | 32.5 | 1385.8 | 1458.5 | - | 6 h | Immediately |
| Gouchon et al., 2010[43] | Italy | 17 | 17 | 38.6 | 38.6 | 3409 | 3305 | 100 | 2 h | Not immediately |
| Boo and Jamli, 2007[23] | Malaysia | 64 | 62 | - | - | <1501 | <1501 | - | 2.5 h | Immediately |
| Ali et al., 2009[44] | India | 58 | 56 | 33.1 | 33.6 | 1607 | 1615 | 0 | 1 h | Immediately |
| Kadam et al., 2005[24] | India | 44 | 45 | 33.3 | 34 | 1467 | 14611 | - | 9.8 h | - |
| Rojas et al., 2003[26] | US | 33 | 27 | 26.6 | 27.2 | 906 | 939 | - | 8 h | - |
KMC=Kangaroo Mother Care, CNC=Conventional neonatal care
Table 4.
Effect of Kangaroo Mother Care on hospital management indicators
| Author: Year | LOS (mean±SD) | Readmission to hospital (%) | Parent satisfaction | Parents preference for same postdelivery care | ||||
|---|---|---|---|---|---|---|---|---|
| KMC | CNC | KMC | CNC | KMC | CNC | KMC | CNC | |
| Roberts et al., 2000[25] | 48±28 | 46±19 | - | - | - | - | - | - |
| Carfoot et al., 2005[33] | - | - | - | - | 100 | 97 | 100 | 81 |
| Dehghani et al., 2015[34] | 12.7±6.4 | 11±7.8 | - | - | - | - | - | - |
| Charpak et al., 2001[35] | - | - | 4 | 5.9 | - | - | - | - |
| Swarnkar and Vagha, 2016[18] | 11.4±1.7 | 12.5±2.6 | - | - | - | - | - | - |
| Gathwala et al.[36] | - | - | - | - | 94 | - | ||
| Mahmood et al., 2011[37] | - | - | - | - | 97.5 | 85 | 92.5 | 64.8 |
| Srivastava et al., 2014[38] | - | - | - | - | 99 | 72 | - | - |
| Suman et al., 2008[39] | 12.7±6.2 | 12.8±5.7 | - | - | - | - | - | - |
| Ghavane et al., 2012[40] | 25.5±12.3 | 26.0±13.0 | - | - | - | - | - | - |
| Nagai et al., 2011[41] | - | - | 13.9 | 13.9 | - | - | - | - |
| Ramanathan et al., 2001[42] | 27.2±7 | 34.6±7 | - | - | - | - | - | - |
| Acharya et al., 2014[22] | 16.1±5.8 | 13.1±7.6 | - | - | - | - | - | - |
| Gouchon et al., 2010[43] | - | - | - | - | 100 | - | - | - |
| Boo and Jamli, 2007[23] | 17.9±12.3 | 24.2±10.7 | ||||||
| Ali et al., 2009[44] | 13.7±8.9 | 15±10.34 | ||||||
| Kadam et al., 2005[24] | 8.5±4.4 | 9.3±4.5 | ||||||
| Rojas et al., 2003[26] | 61±28 | 61±33 | ||||||
KMC=Kangaroo Mother Care, CNC=Conventional neonatal care
The overall LOS standard different between groups (KMC vs. CNC) was −0.91 days (95% CI, −2.14–0.32, Q = 25.6, df = 10, P = 0.004, I2 = 60.98). This difference was not significant (P < 0.05). Difference between groups in low birth weight (LBW) was −0.72 days (95% CI, −2.54–1.11, Q = 4.39, df = 4, P = 0.35, I2 = 8.93). Difference between groups in very LBW (VLBW) was −1.07 days (95% CI, −2.73–0.60, Q = 21.16, df = 5, P = 0.001, I2 = 76.37) [Figure 2].
Figure 2.
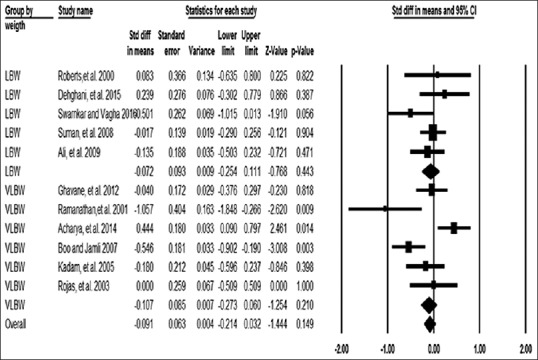
Length of stay standard different between KMC and CNC. KMC = Kangaroo Mother Care, CNC = Conventional neonatal care
Only two studies find that report readmission to hospital different between groups (KMC vs. CNC) in LBW infant. According to results of these studies, the overall readmission to hospital standard different between groups was −1.78% (95% CI, −1.21%–0.86%, Q = 0.024, df = 1, P = 0.87, I2 = 0.00) [Figure 3]. This difference was not significant (P < 0.05).
Figure 3.
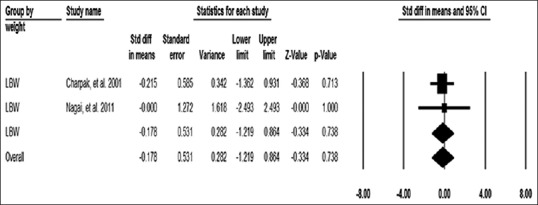
Readmission to hospital standard different between KMC and CNC in LBW infant. KMC = Kangaroo Mother Care, CNC = Conventional neonatal care, LBW = Low birth weight
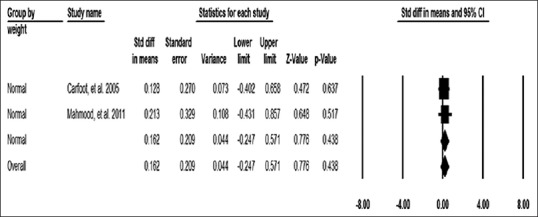
Parent satisfaction different between groups (KMC vs. CNC) in normal weight infant were reported in four studies that three studies result included to analysis (in one study parent satisfaction was not report in CNC group). According to the results of these studies, the overall parent satisfaction standard different between groups was 5.3% (95% CI, −32.4%–43%, Q = 0.052, df = 2, P = 0.97, I2 = 0.00) [Figure 4]. This difference was not significant (P < 0.05).
Figure 4.
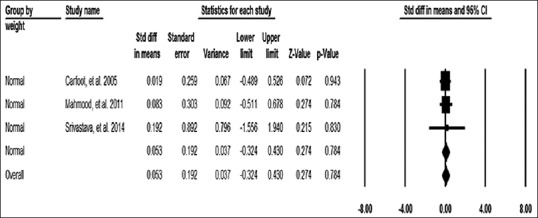
Parent satisfaction standard different between KMC and CNC in normal weight infant. KMC = Kangaroo Mother Care, CNC = Conventional neonatal care
Parents preference for same postdelivery care different between groups (KMC vs. CNC) in normal weight infant was reported in three studies, but the results of two studies included to analysis (in one study, preference for same postdelivery care was not report in CNC group). According to results of these studies, the overall standard different between groups was 16.2% (95% CI, −24.7%–57.1%, Q = 0.040, df = 1, P = 0.84, I2 = 0.00) [Figure 5]. This difference was not significant (P < 0.05).
Figure 5.
Parent preference for same postdelivery care standard different between KMC and CNC in normal weight infant. KMC = Kangaroo Mother Care, CNC = Conventional neonatal care
The result from the risk of bias evaluation showed that many of studies had high risk of bias (8 studies) [Table 5]. Four studies had low risk of bias and six studies had unclear risk of bias.
Table 5.
Result from the risk of bias assessment
| Reference | Sequence generation | Allocation concealment | Blinding | Incomplete outcome data | Selective outcome reporting | Other sources of bias | Result |
|---|---|---|---|---|---|---|---|
| Roberts et al., 2000[25] | Yes: ■ No: Unclear: |
Yes: No: ■ Unclear: |
Yes: No: Unclear:■ |
Yes: No: ■ Unclear: |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Low risk: Unclear: High risk:■ |
| Carfoot et al., 2005[33] | Yes: ■ No: Unclear: |
Yes: ■ No: Unclear: |
Yes: No: Unclear:■ |
Yes: No: ■ Unclear: |
Yes: No: ■ Unclear: |
Yes: No: Unclear:■ |
Low risk: ■ Unclear: High risk: |
| Dehghani et al., 2015[34] | Yes: No: Unclear:■ |
Yes: No: Unclear:■ |
Yes: No: Unclear:■ |
Yes: No: ■ Unclear: |
Yes: No: ■ Unclear: |
Yes: No: Unclear:■ |
Low risk: Unclear: High risk: ■ |
| Charpak et al., 2001[35] | Yes:■ No: Unclear: |
Yes: ■ No: Unclear: |
Yes: No: Unclear:■ |
Yes: No: ■ Unclear: |
Yes: No: ■ Unclear: |
Yes: No: Unclear:■ |
Low risk:■ Unclear: High risk: |
| Swarnkar and Vagha, 2016[18] | Yes: No: Unclear: ■ |
Yes: No: Unclear: ■ |
Yes: No: Unclear: ■ |
Yes: No: Unclear: ■ |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Low risk: Unclear: High risk: ■ |
| Gathwala et al.[36] | Yes:■ No: Unclear: |
Yes: No: Unclear:■ |
Yes: No: ■ Unclear: |
Yes: No: Unclear:■ |
Yes: No: ■ Unclear: |
Yes: No: Unclear:■ |
Low risk: Unclear: ■ High risk: |
| Mahmood et al., 2011[37] | Yes:■ No: Unclear: |
Yes: ■ No: Unclear: |
Yes: No: Unclear:■ |
Yes: No: Unclear:■ |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Low risk: Unclear: ■ High risk: |
| Srivastava et al., 2014[38] | Yes: ■ No: Unclear: |
Yes: ■ No: Unclear: |
Yes: No: ■ Unclear: |
Yes: No: Unclear:■ |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Low risk: Unclear: ■ High risk: |
| Suman et al., 2008[39] | Yes: ■ No: Unclear: |
Yes: ■ No: Unclear: |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Yes: No:■ Unclear: |
Yes: No: ■ Unclear: |
Low risk: Unclear: ■ High risk: |
| Ghavane et al., 2012[40] | Yes: ■ No Unclear: |
Yes: ■ No: Unclear: |
Yes: No:■ Unclear: |
Yes: No:■ Unclear: |
Yes: No: ■ Unclear: |
Yes: No: Unclear: ■ |
Low risk: ■ Unclear: High risk: |
| Nagai et al., 2011[41] | Yes: ■ No: Unclear: |
Yes: No: Unclear: ■ |
Yes: No: ■ Unclear: |
Yes: No: Unclear: ■ |
Yes: No: ■ Unclear: |
Yes: No: Unclear: ■ |
Low risk: Unclear: High risk: ■ |
| Ramanathan et al., 2001[42] | Yes: ■ No: Unclear: |
Yes: No: Unclear:■ |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Yes: No: Unclear:■ |
Yes: No: Unclear:■ |
Low risk: Unclear: High risk: ■ |
| Acharya et al., 2014[22] | Yes: ■ No: Unclear: |
Yes: No: Unclear:■ |
Yes: No: ■ Unclear: |
Yes: No: Unclear:■ |
Yes: No: ■ Unclear: |
Yes: No: Unclear:■ |
Low risk: Unclear: High risk: ■ |
| Gouchon et al., 2010[43] | Yes: ■ No: Unclear: |
Yes: ■ No: Unclear: |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Yes: No: Unclear:■ |
Yes: No: Unclear:■ |
Low risk: Unclear:■ High risk: |
| Boo and Jamli, 2007[23] | Yes: ■ No: Unclear: |
Yes: ■ No: Unclear: |
Yes: No:■ Unclear: |
Yes: No:■ Unclear: |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Low risk: ■ Unclear: High risk: |
| Ali et al., 2009[44] | Yes: ■ No: Unclear: |
Yes: No: Unclear: ■ |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Yes: No: Unclear:■ |
Yes: No: Unclear:■ |
Low risk: Unclear: High risk: ■ |
| Kadam et al., 2005[24] | Yes: ■ No: Unclear: |
Yes: No: Unclear: ■ |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Yes: No:■ Unclear: |
Yes: No: Unclear:■ |
Low risk: Unclear: High risk:■ |
| Rojas et al., 2003[26] | Yes: ■ No: Unclear: |
Yes: ■ No: Unclear: |
Yes: No: ■ Unclear: |
Yes: No: Unclear: ■ |
Yes: No: Unclear:■ |
Yes: No: Unclear:■ |
Low risk: Unclear:■ High risk: |
■: Confirms this case
Discussion
The overall LOS standard different between groups (KMC vs. CNC) was −0.91 days (95% CI, −2.14-0.32, Q = 25.6, df = 10, P = 0.004, I2 = 60.98). The overall readmission to hospital standard different between groups was −1.78% (95% CI, −1.21%–0.86%, Q = 0.024, df = 1, P = 0.87, I2 = 0.00). The overall parent satisfaction standard different between groups was 5.3% (95% CI, −32.4%–43%, Q = 0.052, df = 2, P = 0.97, I2 = 0.00). The overall standard different between groups was 16.2% (95% CI, −24.7%–57.1%, Q = 0.040, df = 1, P = 0.84, I2 = 0.00). Result from the risk of bias evaluation showed that the many of studies had high risk of bias.
As mentioned, the results of this study showed that although KMC reduced LOS, this reduction was not statistically significant. This finding is consistent with the systematic review findings of Boundy et al., who have examined the results of 12 observational and interventional studies.[45] However, the systematic review results of Conde-Agudelo et al. in 2011 that have assessed the results of nine clinical trials showed that KMC has a significant effect in reducing LOS.[46] In addition, the results of some other studies indicate the significant effect of KMC in reducing the LOS.[47,48] The difference results of these studies could be in the inclusion and exclusion criteria of articles, the number and the time of reviewing articles, and babies’ identification. Anyway, like most hospital indicators, LOS influenced by many factors and KMC alone cannot determine LOS in babies. The important thing to note is that, in none of the reviewed studies, other factors that could affect the LOS of babies have not considered and the results of studies in this area have not adjusted. Therefore, it is recommended that the researchers pay attention to this issue in future studies.
However, the rate of readmission was lower in the KMC, but this difference was not statistically significant. This finding is consistent with the study results of Sloan et al.[49] Since the main target group of KMC in babies has been LBW and VLBW. In this study, the majority of babies were in this group, and these babies are facing with many complications after discharge from the hospital. Evaluating potential readmission criteria can be along with many protections, and therefore, researchers must be careful in calculating the index.
Parental satisfaction with the group of KMC was higher than the CNC group. Different studies have shown that KMC has a large positive impact on morale, comfort and in the total satisfaction of parents.[50,51,52] As noted, babies KMC main target group is LBW and VLBW. Mothers who have babies with these features often blame themselves for their newborns’ conditions and are experiencing many mental health problems. In the KMC, mothers feel that they have an important role in the recovery of their baby and have a close relationship with their baby and are more satisfied. However, studies in the field of parental consent from KMC are limited and require further studies in this field.
Limitation
The main limitation of this study was incomplete reported data in reviewed articles. The importance of these incomplete reported data was type of delivery, length of KMC, and KMC initiation time, which imposed limitation to some subgroup analyses. Due to the limitations of this study, it is suggested to use the consort guideline for studies such as randomized clinical trials. It is also suggested that the editors and reviewers at journals have been more sensitive to the format of the report and the appropriateness of the results of the articles.
Conclusion
This study results showed that despite the HMI improvement by KMC, the rate of improvement was not statistically significant. However, given the high importance and effectiveness of the HMI, influence, though a little, in these indexes can contain many other results. Thus, according to the results of this study and the results of other studies that show the positive impact of KMC in clinical and physiological indices of babies and the parents, the development of KMC in hospitals, especially in countries with limited health care resources, is recommended.
Financial support and sponsorship
This study was financially supported by Iran University of Medical Sciences.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We wish to acknowledge Dr. Hojat Gharaee and Dr. Ramin Rezapour for helpful consultation.
References
- 1.Clothing and health of infants. JAMA. 2016;315:2022. doi: 10.1001/jama.2015.17085. [DOI] [PubMed] [Google Scholar]
- 2.Shrivastava SR, Shrivastava PS, Ramasamy J. Inequality in health for women, infants, and children: An alarming public health concern. Int J Prev Med. 2016;7:10. doi: 10.4103/2008-7802.173906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Azami-Aghdash S, Ghojazadeh M, Dehdilani N, Mohammadi M, Asl Amin Abad R. Prevalence and causes of cesarean section in Iran: Systematic review and meta-analysis. Iran J Public Health. 2014;43:545–55. [PMC free article] [PubMed] [Google Scholar]
- 4.Ghojazadeh M, Velayati A, Mallah F, Azami-Aghdash S, Mirnia K, Piri R, et al. Contributing death factors in very low-birth-weight infants by path method analysis. Niger Med J. 2014;55:389–93. doi: 10.4103/0300-1652.140378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Chavda P, Misra S. Evaluation of input and process components of quality of child health services provided at 24 × 7 primary health centers of a district in central gujarat. J Family Med Prim Care. 2015;4:352–8. doi: 10.4103/2249-4863.161315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.McMillen JC, Raffol M. Characterizing the quality workforce in private U.S. Child and family behavioral health agencies. Adm Policy Ment Health. 2016;43:750–9. doi: 10.1007/s10488-015-0667-4. [DOI] [PubMed] [Google Scholar]
- 7.Miller NP, Amouzou A, Hazel E, Degefie T, Legesse H, Tafesse M, et al. Assessing the quality of sick child care provided by community health workers. PLoS One. 2015;10:e0142010. doi: 10.1371/journal.pone.0142010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Shah AY, LLanos K, Dougherty D, Cha S, Conway PH. State challenges to child health quality measure reporting and recommendations for improvement. Healthc (Amst) 2016;4:217–24. doi: 10.1016/j.hjdsi.2016.03.001. [DOI] [PubMed] [Google Scholar]
- 9.Sharma A, Rana SK, Prinja S, Kumar R. Quality of health management information system for maternal & child health care in Haryana state, India. PLoS One. 2016;11:e0148449. doi: 10.1371/journal.pone.0148449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tabrizi JS, Farahbakhsh M, Shahgoli J, Rahbar MR, Naghavi-Behzad M, Ahadi HR, et al. Designing excellence and quality model for training centers of primary health care: A Delphi method study. Iran J Public Health. 2015;44:1367–75. [PMC free article] [PubMed] [Google Scholar]
- 11.Forster DA, McLachlan HL. Breastfeeding initiation and birth setting practices: A review of the literature. J Midwifery Womens Health. 2007;52:273–80. doi: 10.1016/j.jmwh.2006.12.016. [DOI] [PubMed] [Google Scholar]
- 12.Chan GJ, Valsangkar B, Kajeepeta S, Boundy EO, Wall S. What is kangaroo mother care? Systematic review of the literature. J Glob Health. 2016;6:6. doi: 10.7189/jogh.06.010701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Castral TC, Warnock F, Leite AM, Haas VJ, Scochi CG. The effects of skin-to-skin contact during acute pain in preterm newborns. Eur J Pain. 2008;12:464–71. doi: 10.1016/j.ejpain.2007.07.012. [DOI] [PubMed] [Google Scholar]
- 14.Johnston CC, Filion F, Campbell-Yeo M, Goulet C, Bell L, McNaughton K, et al. Kangaroo mother care diminishes pain from heel lance in very preterm neonates: A crossover trial. BMC Pediatr. 2008;8:13. doi: 10.1186/1471-2431-8-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Chan GJ, Labar AS, Wall S, Atun R. Kangaroo mother care: A systematic review of barriers and enablers. Bull World Health Organ. 2016;94:130–41J. doi: 10.2471/BLT.15.157818. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chiu SH, Anderson GC. Effect of early skin-to-skin contact on mother-preterm infant interaction through 18 months: Randomized controlled trial. Int J Nurs Stud. 2009;46:1168–80. doi: 10.1016/j.ijnurstu.2009.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Dezhdar S, Jahanpour F, Firouz Bakht S, Ostovar A. The effects of kangaroo mother care and swaddling on venipuncture pain in premature neonates: A Randomized clinical trial. Iran Red Crescent Med J. 2016;18:e29649. doi: 10.5812/ircmj.29649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Swarnkar K, Vagha J. Effect of kangaroo mother care on growth and morbidity pattern in low birth weight infants. J Krishna Inst Med Sci Univ. 2016;5:91–9. [Google Scholar]
- 19.Maleki D, Ghojazadeh M, Mahmoudi SS, Mahmoudi SM, Pournaghi-Azar F, Torab A, et al. Epidemiology of oral cancer in Iran: A Systematic review. Asian Pac J Cancer Prev. 2015;16:5427–32. doi: 10.7314/apjcp.2015.16.13.5427. [DOI] [PubMed] [Google Scholar]
- 20.Azami-Aghdash S, Ghojazadeh M, Sheyklo SG, Daemi A, Kolahdouzan K, Mohseni M, et al. Breast cancer screening barriers from the womans perspective: A Meta-synthesis. Asian Pac J Cancer Prev. 2015;16:3463–71. doi: 10.7314/apjcp.2015.16.8.3463. [DOI] [PubMed] [Google Scholar]
- 21.Ghojazadeh M, Hajebrahimi S, Pournaghi-Azar F, Mohseni M, Derakhshani N, Azami-Aghdash S, et al. Effect of kangaroo mother care on successful breastfeeding: A systematic review and meta-analysis of randomised controlled trials. Rev Recent Clin Trials. 2019;14:31–40. doi: 10.2174/1574887113666180924165844. [DOI] [PubMed] [Google Scholar]
- 22.Acharya N, Singh RR, Bhatta NK, Poudel P. Randomized control trial of kangaroo mother care in low birth weight babies at a tertiary level hospital. J Nepal Paediatr Soc. 2014;34:18–23. [Google Scholar]
- 23.Boo NY, Jamli FM. Short duration of skin-to-skin contact: Effects on growth and breastfeeding. J Paediatr Child Health. 2007;43:831–6. doi: 10.1111/j.1440-1754.2007.01198.x. [DOI] [PubMed] [Google Scholar]
- 24.Kadam S, Binoy S, Kanbur W, Mondkar JA, Fernandez A. Feasibility of kangaroo mother care in Mumbai. Indian J Pediatr. 2005;72:35–8. doi: 10.1007/BF02760578. [DOI] [PubMed] [Google Scholar]
- 25.Roberts KL, Paynter C, McEwan B. A comparison of kangaroo mother care and conventional cuddling care. Neonatal Netw. 2000;19:31–5. doi: 10.1891/0730-0832.19.4.31. [DOI] [PubMed] [Google Scholar]
- 26.Rojas MA, Kaplan M, Quevedo M, Sherwonit E, Foster L, Ehrenkranz RA, et al. Somatic growth of preterm infants during skin-to-skin care versus traditional holding: A randomized, controlled trial. J Dev Behav Pediatr. 2003;24:163–8. doi: 10.1097/00004703-200306000-00006. [DOI] [PubMed] [Google Scholar]
- 27.Mohseni M, Alikhani M, Tourani S, Azami-Aghdash S, Royani S, Moradi-Joo M, et al. Rate and causes of discharge against medical advice in Iranian hospitals: A Systematic review and meta-analysis. Iran J Public Health. 2015;44:902–12. [PMC free article] [PubMed] [Google Scholar]
- 28.SKhan K, Kunz R, Kleijnen J, Antes G. Crc Press; 2011. Feb 25, Systematic Reviews to Support Evidence-Based Medicine. [Google Scholar]
- 29.Moher D, Liberati A, Tetzlaff J, Altman DG PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann Intern Med. 2009;151:264–9, W64. doi: 10.7326/0003-4819-151-4-200908180-00135. [DOI] [PubMed] [Google Scholar]
- 30.Moher D, Liberati A, Tetzlaff J, Altman DG PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Moher D, Liberati A, Tetzlaff J, Altman DG PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Open Med. 2009;3:e123–30. [PMC free article] [PubMed] [Google Scholar]
- 32.Higgins JP, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions. Version 5.0.2.: The Cochrane Collaboration. 2009 [Google Scholar]
- 33.Carfoot S, Williamson P, Dickson R. A randomised controlled trial in the north of england examining the effects of skin-to-skin care on breast feeding. Midwifery. 2005;21:71–9. doi: 10.1016/j.midw.2004.09.002. [DOI] [PubMed] [Google Scholar]
- 34.Dehghani K, Movahed Z, Dehghani H, Nasiriani K. A randomized controlled trial of kangaroo mother care versus conventional method on vital signs and arterial oxygen saturation rate in newborns who were hospitalized in neonatal intensive care unit. J Clin Neonatol. 2015;4:26–31. [Google Scholar]
- 35.Charpak N, Ruiz-Pelaez JG, Figueroa de C Z, Charpak Y. A randomized, controlled trial of kangaroo mother care: Results of follow-up at 1 year of corrected age. Pediatrics. 2001;108:1072–9. doi: 10.1542/peds.108.5.1072. [DOI] [PubMed] [Google Scholar]
- 36.Gathwala G, Singh B, Singh J. Effect of kangaroo mother care on physical growth, breastfeeding and its acceptability. Trop Doct. 2010;40:199–202. doi: 10.1258/td.2010.090513. [DOI] [PubMed] [Google Scholar]
- 37.Mahmood I, Jamal M, Khan N. Effect of mother-infant early skin-to-skin contact on breastfeeding status: A randomized controlled trial. J Coll Physicians Surg Pak. 2011;21:601–5. doi: 10.2011/JCPSP.601605. [DOI] [PubMed] [Google Scholar]
- 38.Srivastava S, Gupta A, Bhatnagar A, Dutta S. Effect of very early skin to skin contact on success at breastfeeding and preventing early hypothermia in neonates. Indian J Public Health. 2014;58:22–6. doi: 10.4103/0019-557X.128160. [DOI] [PubMed] [Google Scholar]
- 39.Suman RP, Udani R, Nanavati R. Kangaroo mother care for low birth weight infants: A randomized controlled trial. Indian Pediatr. 2008;45:17–23. [PubMed] [Google Scholar]
- 40.Ghavane S, Murki S, Subramanian S, Gaddam P, Kandraju H, Thumalla S, et al. Kangaroo mother care in kangaroo ward for improving the growth and breastfeeding outcomes when reaching term gestational age in very low birth weight infants. Acta Paediatr. 2012;101:e545–9. doi: 10.1111/apa.12023. [DOI] [PubMed] [Google Scholar]
- 41.Nagai S, Yonemoto N, Rabesandratana N, Andrianarimanana D, Nakayama T, Mori R, et al. Long-term effects of earlier initiated continuous kangaroo mother care (KMC) for low-birth-weight (LBW) infants in madagascar. Acta Paediatr. 2011;100:e241–7. doi: 10.1111/j.1651-2227.2011.02372.x. [DOI] [PubMed] [Google Scholar]
- 42.Ramanathan K, Paul VK, Deorari AK, Taneja U, George G. Kangaroo mother care in very low birth weight infants. Indian J Pediatr. 2001;68:1019–23. doi: 10.1007/BF02722345. [DOI] [PubMed] [Google Scholar]
- 43.Gouchon S, Gregori D, Picotto A, Patrucco G, Nangeroni M, Di Giulio P, et al. Skin-to-skin contact after cesarean delivery: An experimental study. Nurs Res. 2010;59:78–84. doi: 10.1097/NNR.0b013e3181d1a8bc. [DOI] [PubMed] [Google Scholar]
- 44.Ali SM, Sharma J, Sharma R, Alam S. Kangaroo mother care as compared to conventional care for low birth weight babies. Dicle Med J. 2009;36:3. [Google Scholar]
- 45.Boundy EO, Dastjerdi R, Spiegelman D, Fawzi WW, Missmer SA, Lieberman E, et al. Kangaroo mother care and neonatal outcomes: A meta-analysis. Pediatrics. 2016;137(1):e20152238. doi: 10.1542/peds.2015-2238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Conde-Agudelo A, Díaz-Rossello JL. Kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Cochrane Database Syst Rev. 2014;4:CD002771. doi: 10.1002/14651858.CD002771.pub3. [DOI] [PubMed] [Google Scholar]
- 47.Jafari M, Bayat Mokhtari A, Kermansaravi A. The effect of kangaroo mother care on weight gain, stay lengthh and controlling temperature of preterm neonates with low birth weight in neonatal intensive care units of selected hospitals in Mashhad. Surg Nurs J. 2014;3:32–7. [Google Scholar]
- 48.Mohammadzadeh A, Farhat A, Jafarzadeh M, Hasanzadeh L, Esmaeli H. Advantages of kangaroo mother care in less than 2000 grams low birth weight neonates. Med J Islamic Repub Iran. 2011;25:11–5. [Google Scholar]
- 49.Sloan NL, Camacho LW, Rojas EP, Stern C. Kangaroo mother method: Randomised controlled trial of an alternative method of care for stabilised low-birthweight infants. Maternidad Isidro Ayora study team. Lancet. 1994;344:782–5. doi: 10.1016/s0140-6736(94)92341-8. [DOI] [PubMed] [Google Scholar]
- 50.Marlow N. Family friendly care. BMJ. 2004;329:1182. doi: 10.1136/bmj.329.7475.1182. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.de Macedo EC, Cruvinel F, Lukasova K, D’Antino ME. The mood variation in mothers of preterm infants in kangaroo mother care and conventional incubator care. J Trop Pediatr. 2007;53:344–6. doi: 10.1093/tropej/fmm076. [DOI] [PubMed] [Google Scholar]
- 52.Tallandini MA, Scalembra C. Kangaroo mother care and mother-premature infant dyadic interaction. Infant Ment Health J. 2006;27:251–75. doi: 10.1002/imhj.20091. [DOI] [PubMed] [Google Scholar]