

Abstract
Background:
Attention deficit hyperactivity disorder (ADHD) is considered the most common neurodevelopmental disorder of childhood and can continue through adolescence and adulthood. Global impairment in children with ADHD increases with increasing number of concurrent disorders. The presence of ADHD in childhood increases the likelihood of additional difficulties in academic performance, social interactions, and low self-esteem developing into adolescents and young adults.
Aims:
The study aims to (i) to determine the prevalence of ADHD among schoolchildren at selected schools in Kancheepuram district, (ii) to find the agreement between parent and teacher reports, and (iii) to associate the prevalence of ADHD among schoolchildren with their selected demographic variables.
Settings and Design:
A quantitative research approach with cross-sectional research design was adopted for the study. The study focused on primary schoolchildren from the selected schools in Kancheepuram district.
Materials and Methods:
Totally 3253 children aged between 8 and 11 years were enumerated from the selected six schools in Kancheepuram district after obtaining informed consent from their caregivers. The presence of ADHD was assessed using Conners’ Teacher–Parent Rating Scale given to caregivers and teachers and confirmed with the Diagnostic and Statistical Manual of Mental Disorders-5 criteria for ADHD.
Results:
The analysis revealed the overall prevalence of ADHD to be 8.8%. The subtypes of ADHD were categorized as 124 (43.3%) for inattentive type, 124 (43.3%) for hyperactive type, and 38 (13.2%) for combined type of ADHD.
Conclusion:
The present study shows a high prevalence of ADHD among primary schoolchildren.
Keywords: Attention deficit hyperactivity disorder, Conners’ Teacher–Parent Rating Scale, Diagnostic and Statistical Manual of Mental Disorders-5 criteria, prevalence, schoolchildren
INTRODUCTION
Children in this modern era are forced to be victims of psychological disorder. They are grown up with undue pressures from the school, social, and cultural environment. The surging trends in the family and society indirectly affect the psychological development of the children. The recent advancements in technology had also made the children aloof from their environment. The perception of the world in the children's mind keeps changing often and they struggle to keep up to its expectations. The commercial influences of the media that exerts pressure on the schooling systems and the extraordinary advancements in digital technology had led to the increase in the psychological disorders in childhood. Attention deficit hyperactivity disorder (ADHD) is one of such disorders that are prevalent worldwide.
ADHD is one of the most prevalent chronic mental health conditions affecting school-aged children. ADHD is characterized by an age-inappropriate hyperactivity, impulsiveness, and inattention. Scahill and Schwab-Stone[1] reviewed 19 community-based studies with an estimate of prevalence from 2% to 17% and also the prevalence was found to be 5%–10% in school-aged children based on the review. The prevalence rate of ADHD was found to be 3.66% among school-going children in a part of rural India.[2] In a cross-sectional study over a period of 1 year, ADHD was assessed with checklist, parents’ report, and clinical interview of the child. The results showed a prevalence of 15.5%. The inattention subtype was predominant, and male-to-female ratio was 6.4:1.[3]
There is a lack of awareness of ADHD among parents, teachers, and educationists. There are limited researches done on the prevalence of ADHD in our community. Therefore, the investigator felt the need to conduct a study to determine the prevalence of ADHD in primary schoolchildren in Kancheepuram district and to sensitize the caregivers, teachers, and educationists about the need to rule out the symptoms of ADHD at an earlier stage and to refer them to the health-care system. The study aimed to determine the prevalence of ADHD among the schoolchildren. The objectives of the study were (i) to determine the prevalence of ADHD among schoolchildren at selected schools in Kancheepuram district, (ii) to find the agreement between parent and teacher reports, and (iii) to associate the prevalence of ADHD among schoolchildren with their demographic variables.
MATERIALS AND METHODS
Quantitative research approach with cross-sectional research design was adopted. The study was conducted in selected state board and CBSE schools in Kancheepuram district. The population of the study comprised schoolchildren between 8 and 11 years’ age groups, and the sample included those who fulfill the inclusion criteria at the selected settings. The cross-sectional study involved 3253 schoolchildren aged 8–11 years who gave consensus for the study. The investigator first allotted a code number to the personal data sheet and screening tool with the help of attendance register. Color coding was used to differentiate the classes such as green – III, yellow – IV, and orange –V standard.
Sample size
Sample size has been calculated taking the prevalence of ADHD among school-going children as 9% (where prevalence has been given as 5%–10%) at 5% significance level and 1% allowable error. The sample size required is 3144. Taking 5% nonresponse rate, the required sample size increased to 3302.
Sampling technique
The study was conducted in Kancheepuram district with the initial survey of the schools in Kancheepuram district done based on records. The blocks of Kancheepuram district were randomly selected based on lottery method. The schools in these blocks were categorized into state board (government and matriculation schools) and CBSE board. The investigator selected six schools in total with three schools in each block. The three schools in Kattankulathur block were selected for study group and three schools in St. Thomas block for control group. As the sample selection followed randomization, the representative population was chosen for the study to screen the children aged 8–11 years.
Description of the tool
The following instruments were used for collection of data:
Section A: Structured questionnaire to elicit demographic and clinical variables: This is a questionnaire designed for the current study. It was given to the parents of the children to elicit their demographic profile
Section B: Conners’ ADHD Diagnostic Teacher–Parent Rating Scale: Conner's Rating Scale rated by parents and teachers were used to identify behavioral parameters for the identification of ADHD
Section C: Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria for ADHD to confirm ADHD based on interview from the parent–teacher report.
The instruments in English were translated into Tamil by bilingual experts in literature and were back translated into English. Test–retest method was computed by the researcher to assess reliability, and content validity index was calculated for both relevance and linguistic clarity. Reliability of the Conner's ADHD Diagnostic Teacher–Parent Rating Scale was 0.81 established by Cronbach's alpha method, and the tool was found feasible and reliable.
Data collection procedure
The schools in Kancheepuram district were listed and they were selected at random from each cluster. All the students in the age group of 8–11 years in selected cluster were enumerated. The children were chosen from state board and CBSE schools. Ethical clearance for the study was obtained from the Institutional Ethical Committee. The investigator got formal permission from the schools for data collection and through the school; the information was given to the caregivers. The primary caregivers of the children involved in data collection were given informed consent while they came to leave and take the children from school and others were given the informed consent through school diary and the parents returned after signing it.
The primary caregivers were requested to participate voluntarily in the study and were informed about the nature of the study. Before signing the informed consent, the purpose of the study to assess the symptoms related to ADHD was explained, and it was informed that the study involves no risks. Confidentiality of the information shared was assured, and the primary caregivers were explained about the option to refuse to participate in the study without any further questions or implications. The primary caregiver either the mother or father, grandparents, guardian who is taking care of the child and knows the child for the past 6 months and willing to participate in the research reported the symptoms and filled the questionnaire. The primary caregivers who had difficulty in comprehending and scoring were interviewed in person by the investigator of the study with the questionnaire, and their responses were recorded by the investigator. After the parents completed filling the information, the researcher obtained the completed data collection sheets. The teachers who are held responsible as class teacher and know the children for a period of 6 months scored the tool of the children based on the behavior observed at class settings.
Children who scored positive for ADHD in both teacher and parent rating scales were further assessed by the investigator along with the children and parents by means of clinical interview using DSM-5 criteria for confirming ADHD in the selected setting. The Statistical Package for the Social Sciences (SPSS) 16 software (IBM SPSS Statistics, India) was used for statistical analysis. Chi-square test was used to test for the association between ADHD and variables. The parents and the teachers were sensitized about ADHD through PowerPoint presentation that enhanced their knowledge on ADHD and created awareness on the need for early identification and prompt medical treatment.
RESULTS
Section A: Analysis of frequency and percentage distribution of demographic variables among schoolchildren between 8 and 11 years’ age group
With regard to age distribution, 1087 (33.4%) children were in the age group of 8 years, 967 (29.7%) children were in the age group of 9 years, 715 (21.9%) children were aged 10 years, and 484 (14.8) were 11 years old. With regard to gender, 1772 (54.5%) children were male and 1481 (45.5%) children were female.
Considering standard, 1247 (38.3%) children were in the third standard, 1148 (35.3%) children were in the fourth standard, and 858 (26.4%) children were in the fifth standard. Considering the religion, 1483 (45.6%) children were Hindu, 821 (25.2%) children were Muslim, 815 (25.1%) children were Christian, and 134 (4.1%) belonged to other religions.
Considering birth order, 1811 (55.7%) children were the first child, 973 (29.9%) children were the second child, 463 (14.2%) children were the third child, and 6 (0.2%) children were the fourth child.
2484 (76.4%) children had mother as the primary caregiver, 530 (16.3%) children's primary caregiver was their father, 202 (6.2%) children were taken care by the grandparents, and 35 (1.1%) had guardian as their caregiver. With regard to primary caregivers’ educational status, 95 (2.9%) of them did not have formal education, 1967 (60.5%) of them had completed until their school education, and 1191 (36.6%) of them are graduate and above.
Considering family income, 336 (10.3%) of them earn <8019/-, 355 (10.9%) of them earn between 8020/- and 14,019/-, 855 (26.3%) of them earn between 14,020/- and 20,019/-, 933 (28.7%) of them earn between 20,020/- and 26,019/-, and 774 (23.8%) earn >26,020/. Considering the school, 242 (7.4%) of them were from government schools, 792 (24.3%) of them were from CBSE schools, and 2219 (68.2%) of them were from matriculation schools.
With regard to the previous diagnosis of ADHD, 17 (0.5%) of them were diagnosed earlier with ADHD and 3236 (99.5%) of them did not have previous diagnosis of ADHD. Thirty-four (1%) of them had a family history of ADHD and 3219 (99%) of them did not have a family history of ADHD.
Section B: Determination of prevalence of attention deficit hyperactivity disorder among schoolchildren
The presence of ADHD symptoms was confirmed based on the DSM-5 criteria. 2967 (91.2%) students were categorized as normal and 286 (8.8%) children had symptoms of ADHD. The overall prevalence of ADHD was 8.8%.
Considering the subtypes of ADHD based on the prevalence, 124 (43.3%) had inattentive symptoms, 124 (43.3%) had hyperactive symptoms, and 38 (13.2%) had combined type of symptoms. This is pictorially represented in Figure 1.
Figure 1.
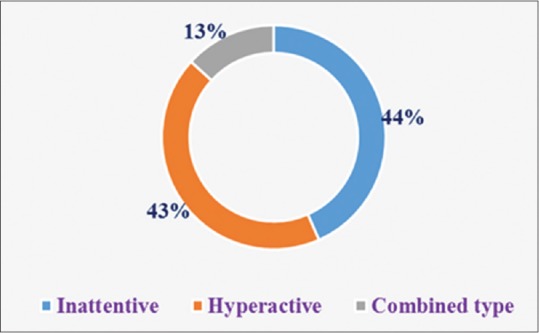
Prevalence of attention deficit hyperactivity disorder among schoolchildren based on subtypes
Section C: Agreement between the parent and teacher reports of attention deficit hyperactivity disorder
In regard to the prevalence of ADHD based on the parent report, 2878 (88.5%) students were categorized as normal and 375 (11.5%) children had symptoms of ADHD. The prevalence of ADHD based on the teacher report suggests a total of 2912 (89.5%) students categorized as normal and 341 (10.5%) children had symptoms of ADHD. Hence, the overall prevalence of ADHD as with teacher report was 11.5% and from parent report was 10.5%.
The measures of agreement on the prevalence of ADHD from the parent and teacher reports were analyzed based on κ value. κ = 0.774 showed a strong agreement between the parent scoring and the teacher scoring with P = 0.000.
Section D: Association of prevalence of attention deficit hyperactivity disorder among schoolchildren with the selected demographic variable
The analysis reveals that there was a significant association with the demographic variables such as age, standard of education, religion, birth order, primary caregiver, family income, previously diagnosed ADHD, and family history of ADHD at P < 0.05 with Chi-square values of 13.3, 20.8, 20.8, 20.55, 37.8, 206.2, 41.5, and 291.3, respectively. There was no significant association with respect to other demographic variables such as gender and caregivers’ educational status and school. This is represented in Table 1.
Table 1.
Association of prevalence of attention deficit hyperactivity disorder among schoolchildren with the selected demographic variables
| Demographic variables | Frequency (%) | χ2, df, P | |||
|---|---|---|---|---|---|
| Normal | ADHD | ||||
| Age (years) | |||||
| 8 | 1012 | 93.1 | 75 | 6.8 | 12.57, 3, 0.005 (S)* |
| 9 | 859 | 88.8 | 108 | 11.1 | |
| 10 | 658 | 92 | 57 | 8 | |
| 11 | 438 | 90.4 | 46 | 9.5 | |
| Gender | |||||
| Male | 1621 | 91.5 | 151 | 8.5 | 0.35, 1, 0.55 (NS) |
| Female | 1346 | 90.9 | 135 | 9.1 | |
| Standard of education | |||||
| III | 1129 | 90.5 | 118 | 9.5 | 20.8, 2, 0.000 (S)* |
| IV | 1024 | 89.2 | 124 | 10.8 | |
| V | 814 | 94.9 | 44 | 5.1 | |
| Religion | |||||
| Hindu | 1333 | 89.9 | 150 | 10.1 | 20.08, 3, 0.000 (S)* |
| Muslim | 736 | 89.6 | 85 | 10.4 | |
| Christian | 769 | 94.4 | 46 | 5.6 | |
| Others | 129 | 96.3 | 5 | 3.7 | |
| Birth order | |||||
| First child | 1648 | 91 | 163 | 9 | 20.55, 3, 0.000 (S)* |
| Second child | 868 | 89.2 | 105 | 10.8 | |
| Third child | 446 | 96.3 | 17 | 3.7 | |
| Fourth child | 5 | 83.3 | 1 | 16.7 | |
| Caregiver | |||||
| Both parents | 2303 | 92.7 | 181 | 7.3 | 37.8, 3, 0.000 (S)* |
| Mother/father | 465 | 87.7 | 65 | 12.3 | |
| Grandparents | 174 | 86.1 | 28 | 13.9 | |
| Guardian | 25 | 71.4 | 10 | 28.6 | |
| Caregivers’ educational status | |||||
| No formal education | 87 | 91.6 | 8 | 8.4 | 0.029, 2, 0.986 (NS) |
| School education | 1793 | 91.2 | 174 | 8.8 | |
| Graduate and above | 1087 | 91.3 | 104 | 8.7 | |
| Family income (Rs.) | |||||
| <8019 | 244 | 72.6 | 92 | 27.4 | 206.2, 4, 0.000 (S)* |
| 8020-14019 | 302 | 85.1 | 53 | 14.9 | |
| 14020-20019 | 790 | 92.4 | 65 | 7.6 | |
| 20020-26019 | 881 | 94.4 | 52 | 5.6 | |
| >26020 | 750 | 96.9 | 24 | 3.1 | |
| School | |||||
| Government school | 220 | 90.9 | 22 | 9.1 | 0.68, 2, 0.708 (NS) |
| CBSE school | 717 | 90.5 | 75 | 9.5 | |
| Matriculation school | 2030 | 91.5 | 189 | 8.5 | |
| Previously diagnosed ADHD | |||||
| Yes | 8 | 47.1 | 9 | 52.9 | 41.5, 1, 0.000 (S)* |
| No | 2959 | 91.4 | 277 | 8.6 | |
| Family history of ADHD | |||||
| Yes | 8 | 23.5 | 26 | 76.5 | 291.3, 2, 0.000 (S)* |
| No | 2959 | 92.2 | 260 | 7.8 | |
ADHD – Attention deficit hyperactivity disorder; NS – Not significant; (S)* – Significant
The analysis reveals that there was a significant association with the demographic variables such as the age, standard of education, religion, birth order, caregiver, family income, previously diagnosed ADHD, and family history of ADHD at P < 0.05 with Chi-square values of 12.57 for age, 20.08 for education, 20.08 for religion, 20.55 for birth order, 37.8 for child's relation to caregiver, 206.2 for child's family income, 41.5 for previously diagnosed ADHD, and 291.3 for family history of ADHD. There was no significant association with respect to other demographic variables.
DISCUSSION
ADHD is a highly prevalent condition among children. This study indicates the importance of early identification and intervention of this neurodevelopmental disorder. The prevalence of ADHD in this study is quite high, with a trend for increase in prevalence among school-aged children. With more literature search and survey, ADHD in the schoolchildren can be brought to light and can change the perception of society. The misconceptions can be eradicated, thereby increasing awareness of early identification and prompt treatment.
The results of the present study are consistent with the study conducted by Srignanasoundari et al.[4] to assess the prevalence of ADHD among primary schoolchildren. The sample consisted of 865 children with the age group of 4–10 years from five different primary schools using Modified Conners’ Teacher Rating Scale. Results showed that out of 865 children, the total number of males was 407 and females was 458. The study concluded with the prevalence of ADHD from 3% to 12% and worldwide prevalence of ADHD was approximately 3%. The study reported that 6.3% of primary schoolchildren were with symptoms of ADHD.
The current study was undertaken to estimate the prevalence of ADHD and to associate ADHD with various sociodemographic variables. The prevalence of ADHD in primary schoolchildren was found to be 286 (8.8%). The finding is similar to that of a study done to examine the prevalence of ADHD in 1250 preschool children to be 12.2%.[5]
There was an almost equal proportion of ADHD prevalence across gender which was also supported by Rucklidge,[6] where he contradicted the view from ligature supports. Review of gender differences across the lifespan was analyzed. Males and females with ADHD are almost the same than it is different. The review concludes stating ADHD profiles as not sex specific.
Venkata and Panicker[7] conducted a cross-sectional study to assess the prevalence of ADHD in school-aged children in Coimbatore district. Children aged between 6 and 11 years were selected and screened with Conners’ Abbreviated Rating Scale. The prevalence of ADHD was found to be 11.32%. The prevalence among lower socioeconomic group was found to be 16.33% and that among middle socioeconomic group was 6.84%. The prevalence was highest in the age group of 9–11 years. This was in line with the present study where the prevalence rate goes higher with lesser economic status and also there is a concurrence with the age group between 8 and 9 years where the highest incidence of ADHD was noted.
The measures of agreement on the prevalence of ADHD from the parent and teacher reports were analyzed based on κ value. κ = 0.774 showed a strong agreement between the parent scoring and the teacher scoring. This is supported by a meta-analytic study at the UAE among schoolchildren aged 5–16 years. The rate of ADHD was 4.1% as per the parent report and 3.4% as per the teacher report.[8]
Majority of the children had inattentive and hyperactive symptoms whereas only 2% had combined type of ADHD which again is in concurrence with the study by Pham et al.[9] The study determined the prevalence of ADHD in primary schoolchildren using the ADHD Rating Scale-IV for parents/caregivers and teachers. The prevalence rate of ADHD was 7.7%. The rate of the predominantly inattentive type, predominantly hyperactive type, and combined type was 1.7%, 5%, and 1%, respectively. The difference in genders was not significant across all subtypes.
There was a significant association between the demographic variables such as the age, standard of education, birth order, primary caregiver, monthly income, history of ADHD in family, and previously diagnosed ADHD. This was supported by Kurlan et al.[10] where they performed a cross-sectional study in the United States of America. Children aged 7–14 years were diagnosed based on the DSM IV criteria. Data were collected from primary caregivers and from the clinical interview of the children. The study showed a significant association between gender, age, socioeconomic status, and parental support.
The primary caregivers and teachers were sensitized on ADHD through educational session and through PowerPoint presentation. They were given with the awareness about identification and initiating the treatment for ADHD. Yewatkar et al.[11] performed a cross-sectional study to determine the prevalence of ADHD. The study findings revealed most of the children to be boys, and the prevalence rate of ADHD was 6.4%. The study concluded emphasizing the need for early identification and treatment in the identified children.
CONCLUSION
ADHD is one of the best-investigated child mental health disorders. ADHD has received a great deal of clinical, scientific, and public attention in recent years. The overall prevalence of ADHD is 286 (8.8%). The findings of the study enable us to conclude that ADHD is found to be more prevalent in schoolchildren, and this prevalence constitutes a major public health problem. Our findings point to the importance of screening of this vulnerable population and taking appropriate interventional measures.
Limitations
The limitations of this study were as follows:
Inclusion of only those children and caregivers who can understand English or Tamil
Inclusion of only selected schools.
Financial support and sponsorship
The source of financial grants and other funding was done by the author herself.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Scahill L, Schwab-Stone M. Epidemiology of ADHD in school-age children. Child Adolesc Psychiatr Clin N Am. 2000;9:541–55, vii. [PubMed] [Google Scholar]
- 2.Naik A, Patel S, Biswas DA. Prevalence of ADHD in a rural Indian population. Innov J Med Health Sci. 2016;11:45–6. [Google Scholar]
- 3.Mukhopadhyay M, Misra S, Mitra T, Niyogi P. Attention deficit hyperactivity disorder. Indian J Pediatr. 2003;70:789. doi: 10.1007/BF02723796. [DOI] [PubMed] [Google Scholar]
- 4.Srignanasoundari E, Vijayalakshmi S, Vijayaragavan R. A study to assess the prevalence of attention deficit hyperactivity disorder among primary school children at selected schools of Kancheepuram district in Tamil Nadu. Int J Health Sci Res. 2016;6:201–6. [Google Scholar]
- 5.Suvarna BS, Kamath A. Prevalence of attention deficit disorder among preschool age children. Nepal Med Coll J. 2009;11:1–4. [PubMed] [Google Scholar]
- 6.Rucklidge JJ. Gender differences in attention-deficit/hyperactivity disorder. Psychiatr Clin North Am. 2010;33:357–73. doi: 10.1016/j.psc.2010.01.006. [DOI] [PubMed] [Google Scholar]
- 7.Venkata JA, Panicker AS. Prevalence of attention deficit hyperactivity disorder in primary school children. Indian J Psychiatry. 2013;55:338–42. doi: 10.4103/0019-5545.120544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Eapen V, Mabrouk AA, Zoubeidi T, Sabri S, Yousef S, Al-Ketbi J, et al. Epidemiological study of attention deficit hyperactivity disorder among school children in the United Arab Emirates. Ham Med J. 2009;3:119–27. [Google Scholar]
- 9.Pham HD, Nguyen HB, Tran DT. Prevalence of ADHD in primary school children in Vinh Long, Vietnam. Pediatr Int. 2015;57:856–9. doi: 10.1111/ped.12656. [DOI] [PubMed] [Google Scholar]
- 10.Kurlan R, Como PG, Miller B, Palumbo D, Deeley C, Andresen EM, et al. The behavioral spectrum of tic disorders: A community-based study. Neurology. 2002;59:414–20. doi: 10.1212/wnl.59.3.414. [DOI] [PubMed] [Google Scholar]
- 11.Yewatkar DV, Pande DP, Bangde LA, Joshi T. Prevalence of attention deficit hyperactivity disorder in an urban school of a developing country. Int J Res Med Sci. 2017;3:3759–62. [Google Scholar]