

Abstract
Although HIV infection can mimic the manifestations of various autoimmune disorders, the coexistence of HIV and systemic lupus erythematosus (SLE) has been rarely reported. The exact impact of HIV on SLE and vice versa is unclear. We report an HIV-seropositive female on highly active antiretroviral therapy presenting with features of SLE. Herein, an attempt has been made to discuss the various complex clinical and therapeutic implications along with the influence on disease course and prognosis.
Key words: AIDS, autoimmune diseases, immune reconstitution inflammatory syndrome, lupus erythematosus
INTRODUCTION
Systemic lupus erythematosus (SLE) can affect persons irrespective of age or gender with predilection for females of child-bearing age.[1] It is an autoimmune multisystem disorder causing microvascular inflammation with generation of numerous antinuclear autoantibodies (ANA).[2] The occurrence of a particular autoimmune disease in an HIV-seropositive individual depends on the degree of immunosuppression.[3] There is limited literature elaborating the coexistence and interaction of HIV and SLE.
CASE REPORT
A 47-year-old female presented with erythematous-violaceous scaly plaques on the malar and other photoexposed areas [Figures 1 and 2] with bulla over the left arm [Figure 3] and buccal erosions for 1 month with fatigue, anorexia, and weight loss. She was a known HIV seropositive (baseline CD4 706) on TLE (tenofovir 300 mg, lamivudine 300 mg, and efavirenz [600 mg])-based antiretroviral therapy (ART) for 6 months. General examination revealed pallor. Systemic and musculoskeletal examination was unremarkable. Differential diagnoses of photoallergic dermatitis, drug-induced lichenoid eruption, polymorphic light eruption, lupus erythematosus, and immune reconstitution inflammatory syndrome (IRIS) were considered. She was anemic (hemoglobin – 7.8 g%) with leukopenia (3400 cells/ml) and thrombocytopenia, elevated erythrocyte sedimentation rate, and CD4 count 309 cells/dl. 24-h urinary protein was normal. Venereal Disease Research Laboratory titer was negative. Radiological investigations were noncontributory. ANA was positive (titer: 3.08). Skin histopathology was consistent with lupus erythematosus [Figure 4]. A final diagnosis of SLE was reached on fulfillment of Systemic Lupus International Collaborating Clinics Criteria (two clinical, one laboratory, and immunological with characteristic histopathology).
Figure 1.

Clinical picture showing malar rash
Figure 2.

Clinical picture showing hyperpigmented atrophic plaques over extensors aspect of the upper limb
Figure 3.

Bullous lesion over the left arm
Figure 4.
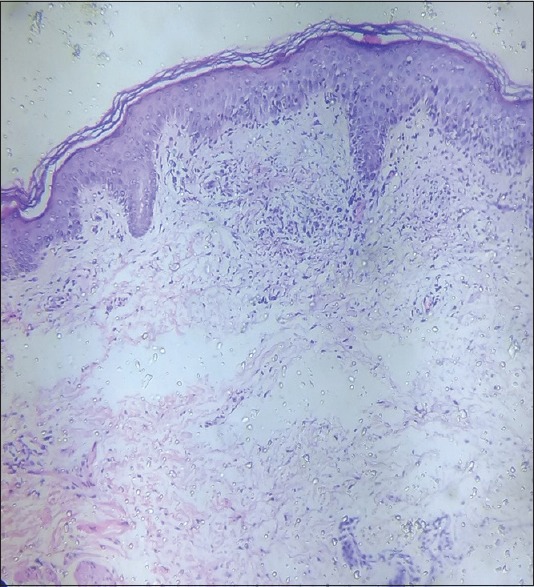
Histopathology showing hyperkeratosis, irregular acanthosis, focal hydropic degeneration in the basal layer. Dermal perivascular mononuclear cell infiltrate with fibrinoid deposits
She was restarted on highly active ART (HAART) and prednisolone 1 mg/kg (tapered over 6 weeks) with hydroxychloroquine 400 mg/day. Strict photoprotection was advised with sunscreen lotion (SPF 50) and fluocinolone acetonide cream. The patient responded with complete resolution of all cutaneous lesions within 6–8 weeks with maintenance on tablet 200 mg/day and sunscreen. She is currently under stringent monitoring.
DISCUSSION
Although HIV infection is often associated with several autoimmune diseases, its coexistence with SLE is uncommon.[4] Retroviral infections including HIV have been proposed as etiologies in SLE and Sjogren's syndrome due to antibodies to retroviral proteins or viable/dead organisms. HIV causes a state of immunodeficiency and is responsible for several serum abnormalities. The resultant immune dysregulation facilitates the development of autoimmune diseases.[5]
Autoimmunity in HIV patients may present as IRIS or late manifestations of HIV. ART initiation leads to the recovery of CD4+ T-cells with restoration of protective immunity and reduced occurrence of opportunistic infections. However, in a subset of patients, dysregulated immune response leads to the phenomenon of IRIS.[6] Although our patient developed inflammatory rash within 5 months of starting ART, evidence of immune restoration was lacking. Thus, only one major criterion was fulfilled, thereby precluding IRIS.
Diagnosis of SLE in HIV may pose difficulty as they share common features such as photosensitivity, oral ulceration, sicca syndrome, arthritis, fever, hypergammaglobulinemia, cytopenias, neuropathies, and ANA positivity.[7] It is still uncertain whether autoimmunity in HIV-positive patients has any bearing on course or prognosis. Although generally HIV-related immunosuppression improves LE symptoms,[8] ART may trigger flares subsequent to increase in CD4 count.
While some authors have paradoxically suggested that the presence of autoimmune diseases like SLE may be protective for HIV,[6] others believe that like HIV, SLE also affects the immune system, compromising the ability to combat infection.[7] Consequently, the coexistence may predispose to opportunistic infections.
Treatment of SLE in an HIV-infected individual is more challenging, as the usual armamentarium may potentially worsen immunosuppression. HAART should be resumed or continued unless ART toxicity is the main differential. Hydroxychloroquine/chloroquine has immunomodulatory and anti-inflammatory properties useful in T-cell-mediated immune diseases such as SLE and steroid-resistant graft versus host disease. These antimalarials interfere with cell activation pathways (major histocompatibility complex Class II antigen presentation and T-cell receptor-mediated intracellular calcium signaling). They demonstrate anti-HIV properties (in vitro and in vivo) by inhibiting posttranslational modification of gp120. Hydroxychloroquine is a safe, cost-effective oral once-daily treatment option for HIV–SLE coexistence.[9]
This case emphasizes the importance of serological screening for LE in HIV patients with a photosensitive rash. HIV has now probably replaced syphilis as the great imitator which justifies screening for HIV while evaluating suspected autoimmune diseases.[5]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that names and initials will not be published and due efforts will be made to conceal identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.D'Cruz DP, Khamashta MA, Hughes GR. Systemic lupus erythematosus. Lancet. 2007;369:587–96. doi: 10.1016/S0140-6736(07)60279-7. [DOI] [PubMed] [Google Scholar]
- 2.Cojocaru M, Cojocaru IM, Silosi I, Vrabie CD. Manifestations of systemic lupus erythematosus. Maedica (Buchar) 2011;6:330–6. [PMC free article] [PubMed] [Google Scholar]
- 3.Roszkiewicz J, Smolewska E. Kaleidoscope of autoimmune diseases in HIV infection. Rheumatol Int. 2016;36:1481–91. doi: 10.1007/s00296-016-3555-7. [DOI] [PubMed] [Google Scholar]
- 4.Calza L, Manfredi R, Colangeli V, D'Antuono A, Passarini B, Chiodo F, et al. Systemic and discoid lupus erythematosus in HIV-infected patients treated with highly active antiretroviral therapy. Int J STD AIDS. 2003;14:356–9. doi: 10.1258/095646203321605585. [DOI] [PubMed] [Google Scholar]
- 5.Kaliyadan F. HIV and lupus erythematosus: A diagnostic dilemma. Indian J Dermatol. 2008;53:80–2. doi: 10.4103/0019-5154.41652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sharma SK, Soneja M. HIV and immune reconstitution inflammatory syndrome (IRIS) Indian J Med Res. 2011;134:866–77. doi: 10.4103/0971-5916.92632. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Virot E, Duclos A, Adelaide L, Miailhes P, Hot A, Ferry T, et al. Autoimmune diseases and HIV infection: A cross-sectional study. Medicine (Baltimore) 2017;96:e5769. doi: 10.1097/MD.0000000000005769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zandman-Goddard G, Shoefield Y. HIV and autoimmunity review article. Autoimmune Rev. 2002;1:329–37. doi: 10.1016/s1568-9972(02)00086-1. [DOI] [PubMed] [Google Scholar]
- 9.Paton NI, Goodall RL, Dunn DT, Franzen S, Collaco-Moraes Y, Gazzard BG, et al. Effects of hydroxychloroquine on immune activation and disease progression among HIV-infected patients not receiving antiretroviral therapy: A randomized controlled trial. JAMA. 2012;308:353–61. doi: 10.1001/jama.2012.6936. [DOI] [PMC free article] [PubMed] [Google Scholar]