

Abstract
Object The consistency of pituitary macroadenomas affects the complexity of surgical resection. On T2-weighted (T2W) imaging, the intensity ratio of the tumor to the cerebellar peduncle (tumor to cerebellar peduncle T2-weighted imaging intensity [TCTI] ratio) correlates with meningioma consistency. We aimed to determine the correlation of this radiographic finding with pituitary macroadenoma consistency and to determine whether it can be used for preoperative planning.
Methods We performed a retrospective evaluation of 196 patients with macroadenomas who underwent endoscopic transsphenoidal resection from January 2012 to June 2017. Macroadenoma consistency was determined by one senior neurosurgeon at the time of surgery. Axial and coronal T2W magnetic resonance imaging images were evaluated retrospectively, and adenoma size, Knosp grade, suprasellar extension and TCTI were calculated.
Results The mean TCTI ratio was 1.70 (95% confidence interval [CI]: 1.65–1.75). Intraoperatively, 140 (71.4%) adenomas were classified as soft and 48 (24.5%) as fibrous. Gross total resection was achieved in 66.7% of fibrous adenomas and in 86.4% of soft adenomas ( p = 0.007). The mean ratio was 1.68 (95% CI: 1.62–1.74) for soft tumors and 1.76 (95%CI: 1.67–1.84) for fibrous tumors. There was no difference in the mean TCTI ratio between groups. Lactotroph and somatotroph adenomas had a lower mean TCTI ratio compared with other functioning and nonfunctioning adenomas with a mean TCTI of 1.52 compared with 1.77.
Conclusions In this retrospective cohort study, we found that the TCTI ratio does not correlate with tumor consistency. We also noted that the TCTI ratio is increased in prolactin and growth hormone-secreting adenomas.
Keywords: macroadenoma, pituitary adenoma, transsphenoidal, consistency, T2-weighted imaging intensity
Introduction
Pituitary macroadenoma consistency may affect the complexity of surgical resection. 1 2 While most macroadenomas are soft and easily aspirated, 3 ∼10% of cases are fibrous and firm adenomas for which suction is not effective. 1 4 No standardized method exists at this time to predict adenoma consistency. Among different conventional imaging modalities, T2-weighted (T2W) imaging holds promise as a method to predict adenoma collagen content and consistency. However, previous studies have provided variable and contradictory results regarding the effectiveness of this imaging modality. 4 5 6 7 8
The tumor to cerebellar peduncle T2-weighted imaging intensity (TCTI) ratio has been extensively evaluated to predict meningioma consistency. TCTI ratio strongly correlates with tumor consistency, and TCTI ratios >1.8 correlate with softer tumors. 9 10 11 A recent study demonstrated that the use of the ratio of signal intensity of pituitary adenoma to cerebellar peduncle on T2W imaging (TCTI) correlates well with tumor consistency, and all six firm tumors in their series had a TCTI <1.8. 12
We therefore sought to validate these results in a larger patient cohort. We conducted a cohort study of retrospectively reviewed preoperative images and prospectively collected operative data to determine the correlation of this radiographic finding with adenoma consistency.
Materials and Methods
Patient Population
Following institutional review board approval, we performed a retrospective evaluation of patients with pituitary macroadenomas who underwent endoscopic or transsphenoidal by the senior author (John A. Jane) between January 2012 and June 2017. Inclusion criteria included preoperative imaging consistent with pituitary macroadenomas (260 patients). Exclusion criteria included previous surgery (six patients), history of apoplexy (three patients), unavailable preoperative imaging (three patients), no prospective documentation of adenoma consistency (three patients), characterization of adenoma consistency with unclear terms including “cystic,” “liquid,” “hemorrhagic,” or “apoplectic” (seven patients), no tumor identified intraoperatively (one patient), and lesions that were found not to be macroadenomas in histopathologic analysis (six patients). Also, following initial imaging analysis 33 patients were noted to have highly cystic adenomas and were excluded from the study. Thus, a cohort of 196 patients was analyzed.
Operative Findings
Macroadenoma consistency was determined by one senior neurosurgeon at the time of surgery and prospectively reported in the operative note as “fibrous,” “intermediate,” or “soft.” The characterization was based on the ability to suction the tumor using regular suction as well as an ultrasonic surgical aspirator. Findings were entered into a prospective database shortly after surgery.
Radiographic Analysis
All patients underwent routine preoperative magnetic resonance imaging. Axial and coronal T2W MRI images were evaluated retrospectively by two of the authors (Panagiotis Mastorakos and Ajay Chatrath), who were blinded to the surgical findings using the “Carestream Health” picture archiving and communication system (Carestream Health, Rochester, New York, United States). A region of interest (ROI) was selected within the adenoma in homogenous adenomas or multiple ROIs were selected for heterogeneous lesions, and the mean intensity was calculated. An ROI from the middle cerebellar peduncle was chosen, and the mean intensity was measured ( Fig. 1A ). Thus, the TCTI ratio was calculated. The reliability coefficient between to raters was 0.8. For simplicity and to maximize the power of our comparison, we compared the TCTI ratio of “soft” and “fibrous” tumors and did not include tumors of intermediate consistency in the comparison.
Fig. 1.
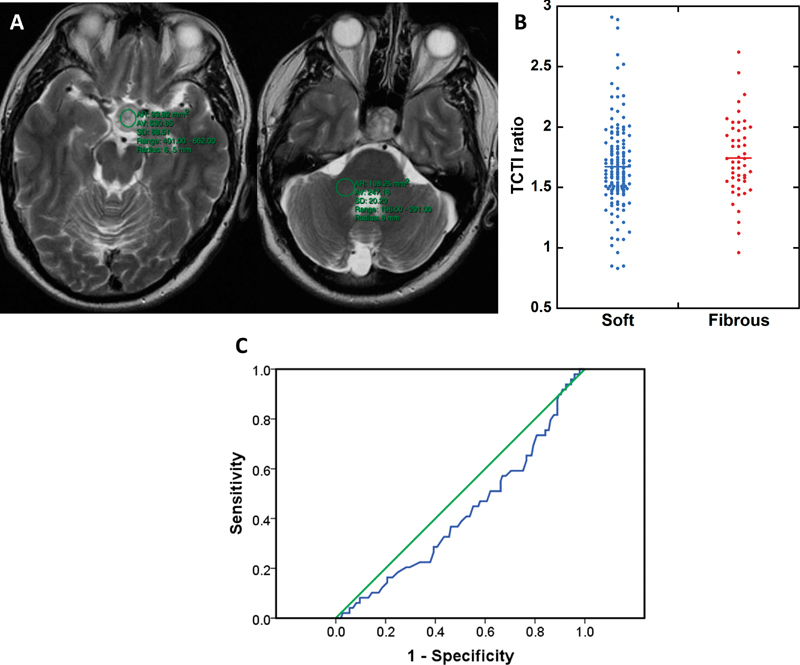
( A ) Representative MRI analysis and ROI measurement for macroadenoma and cerebellar peduncle; ( B ) dot plot of TCTI ratio for soft and fibrous adenoma, no statistically significant difference was identified ( p = 0.19); ( C ) ROC curve demonstrating lack of predictive value of the TCTI ratio for tumor consistency (AUC = 0.419 ± 0.047, p = 0.9). AUC, area under the curve; MRI, magnetic resonance imaging; ROI, region of interest; TCTI, T2-weighted imaging intensity.
Statistical Methods
Student's t -test was used to compare quantitative parameters between two groups and one-way analysis of variance (ANOVA) to compare quantitative parameters between multiple groups. Chi-square was used to compare quantitative parameters. To assess the diagnostic value of this method to predict tumor consistency, we analyzed the receiver operating characteristic (ROC) curve. IBM SPSS statistics data editor (SPSS Inc., Chicago, Illinois, United States) was used for all statistical analyses. All statistical studies were two-sided, and a p value <0.05 was deemed statistically significant. To identify a difference in TCTI ratio of 0.1 with a power of 0.9 and p < 0.05, we calculated that we would require 187 patients.
Results
Demographics
A population of 196 patients was included in this cohort, among whom 92 (47%) were female, and 104 (53%) were male. The average age of surgery was 55.5 ± 15.7 years. There was no difference in age and sex between patients with soft and fibrous adenomas ( Table 1 ).
Table 1. Demographic characteristics and imaging findings.
| Population | 202 |
| M/F (%) | 107 (53%)/95 (47%) |
| Age at surgery ± STD | 55.3 ± 15.8 |
| Adenoma diameter (mm) ± STD | 25.9 ± 10.5 |
| Knosp grade (%) | |
| 0 | 27 (13.2%) |
| 1 | 55 (27.2%) |
| 2 | 56 (27.9%) |
| 3 | 40 (19.8%) |
| 4 | 24 (11.8%) |
| Suprasellar extension (%) | |
| None | 66 (32.7%) |
| <10 mm | 81 (40%) |
| 10–20 mm | 47 (23.3%) |
| >20 mm | 8 (3.9%) |
Abbreviations: STD, standard deviation.
Imaging Analysis
The average maximum adenoma diameter was 25.9 ± 10.5 mm. In our cohort, 13.3% of adenomas were Knosp grade 0, 27% Knosp grade 1, 28% Knosp grade 2, 19.9% Knosp grade 3, and 11.7% Knosp grade 4. Also, 33.2% had no suprasellar extension, 39.8% extended <10 mm, 22.9% extended 10 to 20 mm, and 4.1% extended >20 mm ( Table 1 ). The mean cerebellar peduncle T2W intensity was 615.6, and the mean adenoma intensity was 1062.4. The mean TCTI ratio was calculated to be 1.70 (range: 0.83–2.91; 95% confidence interval [CI]: 1.65–1.75).
Operative Findings
Intraoperatively, 140 (71.4%) patients had adenomas that were classified as soft, and 48 (24.5%) patients were found to have fibrous tumors. In addition, eight (4.1%) adenomas were of intermediate consistency and could not be classified in either of two categories.
The mean TCTI ratio was 1.68 (range: 0.83–2.91; 95% CI: 1.62–1.74) for soft tumors and 1.76 (range: 0.96–2.62; 95%CI: 1.67–1.84) for fibrous tumors ( Fig. 1B , Table 2 ). The difference was not statistically significant between the two groups ( p = 0.19). The ROC curve had an area under the curve (AUC) of 0.419 ± 0.047, p value of 0.9 ( Fig. 1C ). The TCTI ratio of the adenomas of intermediate consistency was 1.82 (range: 1.03–2.41; 95%CI: 1.54–2.10). Given a TCTI difference of 0.08 between the two groups the statistical power of our comparison was 0.77.
Table 2. Correlation of tumor consistency with TCTI score and resection.
| Total | Soft | Fibrous | Intermediate | |
|---|---|---|---|---|
| Population (%) | 202 | 145 (71.8%) | 49 (24.3%) | 8 (3.9%) |
| TCTI ratio (95%CI) | 1.7 (1.65–1.74) | 1.67 (1.61–1.73) | 1.74 (1.65–1.83) | 1.82 (1.54–2.1) |
| Resection | ||||
| GTR | 162 (80.2%) | 123 (84.8%) | 32 (65.3%) | 7 (87.5%) |
| Subtotal resection | 33 (16.3%) | 19 (13.1%) | 13 (26.5%) | 1 (12.5%) |
| Partial resection | 7 (3.4%) | 3 (2%) | 4 (8.1%) | 0 |
Abbreviations: CI, confidence interval; GTR, gross total resection; TCTI, tumor to cerebellar peduncle T2-weighted imaging intensity.
Subtotal resection (estimated >80% resection); partial resection (estimated <80% resection).
Gross total resection was achieved in 160 (81.6%) patients, subtotal resection (>80% of tumor) in 32 (16.3%) patients, and partial resection in 4 (2%) of patients. Among patients with soft adenomas, 86.4% had gross total resection, 12.9% had subtotal resection (estimated resection of >80%), and in 0.7%, we completed partial resection (estimated resection of <80%). In patients with fibrous adenomas, gross total resection was completed in 66.7% of patients and subtotal and partial resection in 27.1% and 6.3%, respectively. This difference was statistically significant ( p = 0.007; Table 2 ). Of note, Knosp grade, suprasellar extension, and size did not correlate with tumor consistency with p -value of 0.35, 0.11, and 0.30, respectively.
Histopathology
Histopathologic analysis of representative fibrous adenomas demonstrated thick fibrous septa intermixed with the tumor cells due to increased perivascular fibrosis on hematoxylin and eosin stain as well as extensive degree of fibrosis on reticulin stain ( Fig. 2A and B ). Also, histopathologic analysis of representative soft adenomas demonstrated delicate vasculature on hematoxylin and eosin stain and delicate blood vessels and lack of fibrosis on reticulin stain ( Fig. 2C and D ).
Fig. 2.
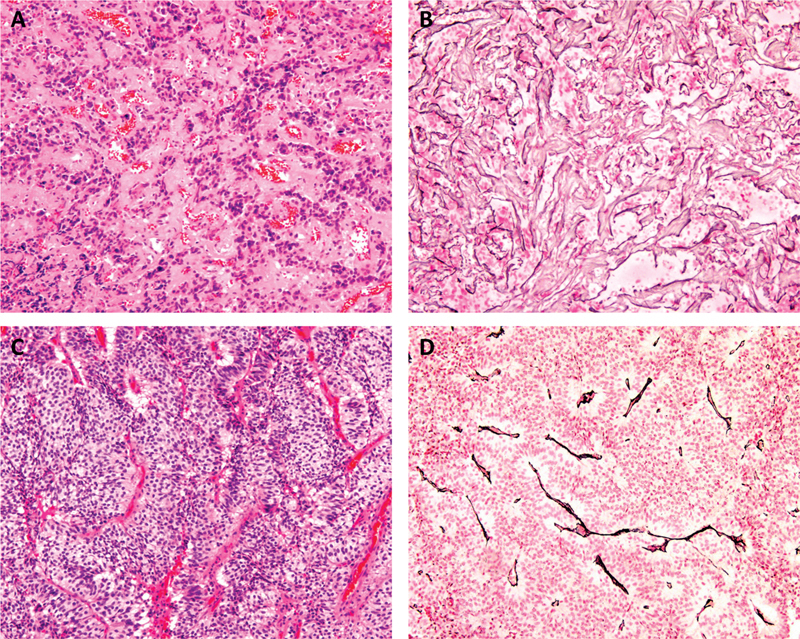
Histopathologic analysis of representative fibrous ( A and B ) and soft ( C and D ) pituitary adenomas (original magnification 100x). ( A ) H&E-stained sections show thick fibrous septa intermixed with the tumor cells due to increased perivascular fibrosis. ( B ) Reticulin Wilder's silver-stained sections demonstrate extensive degree of fibrosis of the adenoma. ( C ) H&E-stained sections show a hypercellular adenoma with delicate vasculature. ( D ) Reticulin Wilder's silver-stained sections demonstrate delicate blood vessels and lack of fibrosis within the adenoma. H&E, hematoxylin and eosin.
Histopathologic analysis demonstrated 98 (50%) nonfunctioning macroadenomas (NFMA), 23 (11.7%) somatotroph adenomas, 13 (6.6%) lactotroph adenomas, and 8 (4.1%) combined lactotroph/somatotroph adenomas, among which 3 (1.5%) were plurihormonal PIT-1 positive adenomas. There were also 13 (6.6%) corticotroph adenomas, among which 9 (4.6%) were silent, as well as 38 (19.4%) gonadotroph adenomas and 3 (1.5%) thyrotroph adenomas. There was no correlation between tumor consistency and type of macroadenoma ( p = 0.638). More specifically, for NFMA, 91.9% were soft, 4.1% were intermediate, and 4.1 were fibrous. For somatotroph adenomas, 90% were soft, 5% were intermediate, and 5% were fibrous. For combined lactotroph/somatotroph adenomas, 75% were soft, and 25% were fibrous.
The TCTI ratio was 1.77 (CI 1.70–1.83) for NFMA, 1.59 (CI 1.34–1.66) for somatotroph adenomas, 1.52 (CI 1.31–1.72) for lactotroph adenomas, 1.45 (CI 1.18–1.73) for combined lactotroph/somatotroph adenomas, 1.70 (CI 1.45–1.97) for corticotroph adenomas, and 1.76 (CI 1.65–1.88) for gonadotroph adenomas. NFMA, gonadotroph, and corticotroph adenomas had higher TCTI compared with lactotroph and somatotroph adenomas. The difference was statistically significant ( p < 0.05; Fig. 3 ).
Fig. 3.
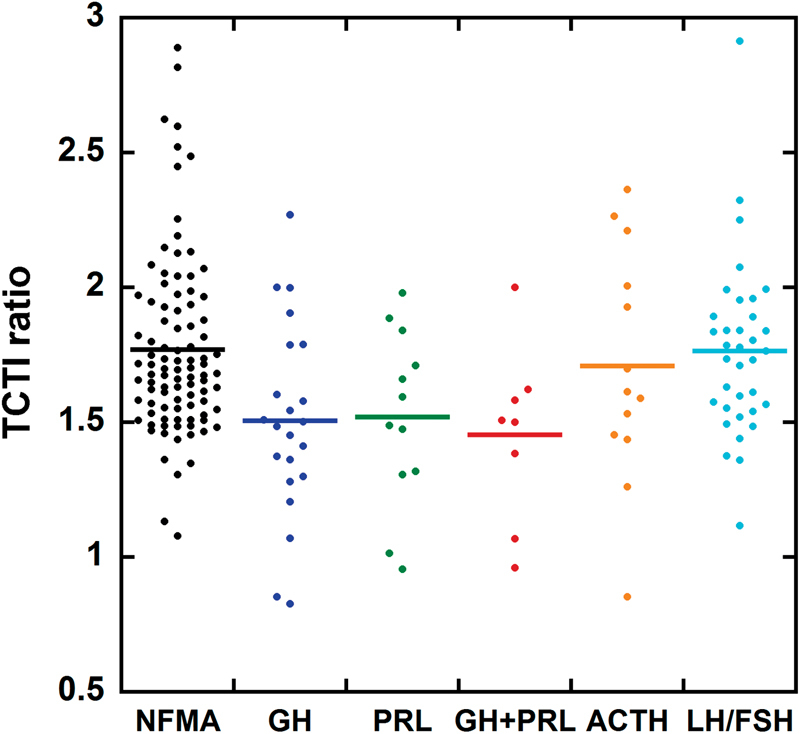
Dot plot of TCTI for different adenoma types. ACTH; FSH; GH; LH; NFMA; PRL; TCTI, T2-weighted imaging intensity.
Discussion
Preoperative knowledge of adenoma consistency may aid with surgical planning, considerations regarding duration of surgery, and patient counseling. For large lesions with suprasellar extension, tumor consistency can be a factor in deciding on the need for craniotomy. 4 Thus, a reliable preoperative predictor of the pituitary adenoma consistency would prove to be a useful biomarker for preoperative surgical planning. 13 Our result further supports this, as we demonstrated that tumor firmness as assessed by the surgeon intraoperatively correlates with decreased frequency of gross total resection and increased frequency of partial resection. This finding was independent of Knosp score, size, or suprasellar extension.
Small case series have suggested that low T2W intensity may be associated with increased collagen content in surgical specimens 5 6 and that fibrous tumors tend to be isointense to the cerebral tissue. 4 7 Bahuleyan et al reported that T2W MRI intensity did not correlate with macroadenoma consistency. 8 Similarly a case series of growth hormone-producing adenomas did not identify any correlation with tumor consistency. 14 15 The TCTI ratio offers a simple way to normalize the T2W intensity, has been extensively characterized in meningiomas, and has shown to strongly correlate with tumor consistency. 9 10 11 The use of this ratio in pituitary adenomas has offered promising results in a small cohort. 12 Using a large cohort, we show that the TCTI ratio does not correlate well with tumor consistency and does not offer predictive value in this context. Smith et al demonstrated in their series that all fibrous adenomas had a TCTI ratio <1.8. 12 However, in our cohort most tumors had a TCTI ratio lower than 1.8, and interestingly, while there was no statistically significant difference, soft pituitary adenomas had a lower mean TCTI ratio compared with fibrous tumors.
We also noted that lactotroph and somatotroph adenomas, as well as combined lactotroph/somatotroph adenomas have a lower mean TCTI ratio compared with other functioning and nonfunctioning adenomas with a mean TCTI of 1.52 compared with 1.77. Hagiwara et al have noted that on T2W-imaging, somatotroph adenomas were more often hypointense compared with non-GH-producing adenomas. This finding may be attributed to secretory granule density, as high intragranular protein concentrations might result in T2 hypointensity. 15
This is a retrospective study allowing the potential for bias. Reviewers were blinded to the surgical findings to remove any potential bias of imaging interpretation. Also, we acknowledge the subjectivity of intraoperative characterization of adenoma consistency and noted that this characterization was completed prospectively to avoid potential bias. This may also explain the discrepancy between the percentage of fibrous tumors in the literature and that in our case series.
Conclusion
Assessing adenoma consistency preoperatively is useful for surgical planning; however, in this retrospective cohort study, we found that the TCTI ratio does not correlate with tumor consistency. This negative result in a relatively large cohort allows us to conclude that T2W imaging cannot be used to predict adenoma consistency and surgery complexity. We also noted that the TCTI ratio is increased in prolactin and growth hormone-secreting adenomas.
Funding Statement
Funding This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
This work has not been previously presented or published and is not under consideration for publication by any other journal.
Footnotes
Conflicts of Interest The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
References
- 1.Naganuma H, Satoh E, Nukui H.Technical considerations of transsphenoidal removal of fibrous pituitary adenomas and evaluation of collagen content and subtype in the adenomas Neurol Med Chir (Tokyo) 20024205202–212., discussion 213 [DOI] [PubMed] [Google Scholar]
- 2.Couldwell W T.Transsphenoidal and transcranial surgery for pituitary adenomas J Neurooncol 200469(1-3):237–256. [DOI] [PubMed] [Google Scholar]
- 3.Taylor D G, Jane J A, Jr, Oldfield E H. Resection of pituitary macroadenomas via the pseudocapsule along the posterior tumor margin: a cohort study and technical note. J Neurosurg. 2018;128(02):422–428. doi: 10.3171/2017.7.JNS171658. [DOI] [PubMed] [Google Scholar]
- 4.Snow R B, Lavyne M H, Lee B C, Morgello S, Patterson R H., Jr Craniotomy versus transsphenoidal excision of large pituitary tumors: the usefulness of magnetic resonance imaging in guiding the operative approach. Neurosurgery. 1986;19(01):59–64. doi: 10.1227/00006123-198607000-00008. [DOI] [PubMed] [Google Scholar]
- 5.Iuchi T, Saeki N, Tanaka M, Sunami K, Yamaura A. MRI prediction of fibrous pituitary adenomas. Acta Neurochir (Wien) 1998;140(08):779–786. doi: 10.1007/s007010050179. [DOI] [PubMed] [Google Scholar]
- 6.Yiping L, Ji X, Daoying G, Bo Y. Prediction of the consistency of pituitary adenoma: A comparative study on diffusion-weighted imaging and pathological results. J Neuroradiol. 2016;43(03):186–194. doi: 10.1016/j.neurad.2015.09.003. [DOI] [PubMed] [Google Scholar]
- 7.Snow R B, Johnson C E, Morgello S, Lavyne M H, Patterson R H., Jr Is magnetic resonance imaging useful in guiding the operative approach to large pituitary tumors? Neurosurgery. 1990;26(05):801–803. doi: 10.1097/00006123-199005000-00011. [DOI] [PubMed] [Google Scholar]
- 8.Bahuleyan B, Raghuram L, Rajshekhar V, Chacko A G. To assess the ability of MRI to predict consistency of pituitary macroadenomas. Br J Neurosurg. 2006;20(05):324–326. doi: 10.1080/02688690601000717. [DOI] [PubMed] [Google Scholar]
- 9.Smith K A, Leever J D, Chamoun R B. Predicting consistency of meningioma by magnetic resonance imaging. J Neurol Surg B Skull Base. 2015;76(03):225–229. doi: 10.1055/s-0034-1543965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Smith K A, Leever J D, Hylton P D, Camarata P J, Chamoun R B. Meningioma consistency prediction utilizing tumor to cerebellar peduncle intensity on T2-weighted magnetic resonance imaging sequences: TCTI ratio. J Neurosurg. 2017;126(01):242–248. doi: 10.3171/2016.1.JNS152329. [DOI] [PubMed] [Google Scholar]
- 11.Yao A, Pain M, Balchandani P, Shrivastava R K. Can MRI predict meningioma consistency? A correlation with tumor pathology and systematic review. Neurosurg Rev. 2018;41(03):745–753. doi: 10.1007/s10143-016-0801-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Smith K A, Leever J D, Chamoun R B. Prediction of consistency of pituitary adenomas by magnetic resonance imaging. J Neurol Surg B Skull Base. 2015;76(05):340–343. doi: 10.1055/s-0035-1549005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Boxerman J L, Rogg J M, Donahue J E, Machan J T, Goldman M A, Doberstein C E. Preoperative MRI evaluation of pituitary macroadenoma: imaging features predictive of successful transsphenoidal surgery. AJR Am J Roentgenol. 2010;195(03):720–728. doi: 10.2214/AJR.09.4128. [DOI] [PubMed] [Google Scholar]
- 14.Chakrabortty S, Oi S, Yamaguchi M, Tamaki N, Matsumoto S. Growth hormone-producing pituitary adenomas: MR characteristics and pre- and postoperative evaluation. Neurol Med Chir (Tokyo) 1993;33(02):81–85. doi: 10.2176/nmc.33.81. [DOI] [PubMed] [Google Scholar]
- 15.Hagiwara A, Inoue Y, Wakasa K, Haba T, Tashiro T, Miyamoto T. Comparison of growth hormone-producing and non-growth hormone-producing pituitary adenomas: imaging characteristics and pathologic correlation. Radiology. 2003;228(02):533–538. doi: 10.1148/radiol.2282020695. [DOI] [PubMed] [Google Scholar]