

Abstract
Background:
Findings from previous population-based studies are in conflict regarding the relative use of tobacco products among transgender populations compared with their cisgender counterparts. The purpose of this study was to estimate the prevalence of current tobacco use among transgender persons in the United States and evaluate differences in relative use between transgender and cisgender respondents.
Methods:
This was a secondary analysis of data from the Population Assessment of Tobacco and Health (PATH) Study Wave 2 (October 2014 and October 2015). Differences in current use of cigarettes, e-cigarettes, and cigars were examined between self-identified transgender (n = 154) and cisgender (n = 27 788) respondents.
Results:
In multivariable analyses, transgender identity was not associated with any of the 3 tobacco behaviors or the summary measure of tobacco use (ie, any current use of cigarettes, e-cigarettes, or cigars). In each of the models, female binary sex (compared with male), older age, Hispanic ethnicity (compared with non-Hispanic white), higher household income, and higher educational attainment were independently associated with lower odds of current use of cigarettes, e-cigarettes, or cigars, whereas sexual minority identity (ie, gay/lesbian or bisexual) was independently associated with higher odds of use.
Conclusions:
The prevalence of the use of cigarettes, e-cigarettes, and cigar use was statistically equivalent between transgender and cisgender populations in this national study of adults in the United States, which differs from previous research showing higher rates of tobacco use among transgender individuals. Differences in tobacco use that were identified were fully explained by sociodemographic characteristics (eg, income and education) between the transgender and cisgender populations.
Keywords: gender identity, electronic nicotine products, combustible cigarettes, health disparities, cigars
Introduction
It is commonly reported in the scientific literature, or cited by community-based organizations, that lesbian, gay, bisexual, and transgender (LGBT) populations are more likely to use tobacco compared with their heterosexual, straight, and/or cisgender counterparts (ie, those whose sex assigned at birth is concordant with their current gender identity).1 However, the empirical evidence for such a broad statement is tenuous. Although a significant body of research does in fact suggest higher tobacco use among some sexual minority groups (eg, lesbian and bisexual identified women),1 other research shows large variability in tobacco use across these subgroups.2–4 In addition, researchers often confound sexual orientation and gender identity—conceptually and analytically—aggregating data from sexual minorities (eg, self-identified gay, lesbian, and bisexual persons) with populations whose gender identity is somehow different from their sex assigned at birth (eg, transgender persons). In fact, research on tobacco use among transgender populations is limited and the existing evidence regarding tobacco use disparities in these populations is equivocal.2,5–7 As such, the claim that “LGBT” populations—as a collective population—have higher tobacco use is premature and requires further investigation. Identifying the most-at-risk populations will help target tobacco control interventions and ultimately lead to a reduction of health disparities experienced by sexual and gender minority (SGM) populations—a broad term used to encompass heterogeneous LGBT populations.8
Probability-based surveys of the general population are best for obtaining nationally representative estimates of self-reported behaviors at the population level. Because gender identity is typically assessed with a binary response option (ie, male or female), most national estimates of tobacco use exclude consideration of gender minority populations. Surveys that do allow for such estimates have resulted in conflicting findings. Specifically, 3 studies have used data from recent administrations of the Behavioral Risk Factor Surveillance System (BRFSS), where optional measurement of gender identity has occurred in up to 32 states since 2014. Findings from the 2016 data suggest that gender minority identity (ie, transgender compared with cisgender) was not associated with current use of cigarettes or ever using electronic cigarettes.2 The 2 other studies have combined the 2014 and 2016 BRFSS data and have reported conflicting evidence regarding within-group differences between transgender men, women, and gender non-conforming adults.6,7 Namely, in 1 study, gender non-conforming adults reported lower cigarette use than either transgender men or women, but only in bivariate models.6 Conversely, when comparing “non-conforming transgender adults” with “gender-binary transgender adults” (ie, transgender men and women), there were no statistical differences in smoking status.7 Results from the Tobacco in Changing Media Environment Study, a probability-based sample of adults in the United States, indicated that transgender-identified adults showed higher current use of cigarettes, cigars, and electronic cigarettes compared with their cisgender peers.5
Several methodological differences in previous studies may explain their differential findings. In the Tobacco in Changing Media Environment Study, current use of each tobacco product was operationalized as any use in the past 30 days. Current use in the BRFSS study was operationalized as smoking combustible cigarettes every day or some days among established users. It is possible that this more conservative estimate of current use explains the null findings. The studies also differed in how they conducted the sampling and modeled the associations. For example, in the Tobacco in Changing Media Environment Study, the authors concluded that transgender (compared to cisgender) participants has higher tobacco use; however, the sample they used combined a random digit dial sample with a convenience sample in which transgender participants were overrepresented. This may have biased the estimates. Furthermore, the BRFSS study adjusted for additional covariates that were not included in the Tobacco in Changing Media Environmental Study, like mental health and related substance abuse. Including these covariates, which theoretically are potential mediators in the causal pathway linking transgender identity with tobacco use, may have resulted in overadjustment bias.9 Finally, to date, no study has examined the associations between gender minority status and tobacco use using a fully nationally representative sample.
To help provide a clearer understanding of tobacco use behaviors among gender minority populations, we sought to estimate tobacco use behaviors among transgender persons in a nationally representative sample of adults in the United States. We tested the following hypothesis: transgender identity is associated with a higher prevalence of tobacco use behaviors for cigarettes (H1a), e-cigarettes (H1b), and cigars (H1c). In addition, 2 exploratory research questions were examined: (R1) what are the differences in tobacco use across transgender groups (eg, male-to-female, female-to-male, gender non-conforming) and (R2) what are the differences in perceived tobacco addiction between transgender and cisgender populations?
Methods
This study was a secondary analysis of data from the restricted use file of the Population Assessment of Tobacco and Health (PATH) Study. The PATH Study is a collaborative effort between the National Institutes of Health and the Center for Tobacco Products at the Food and Drug Administration. It is a nationally representative cohort study of adults 18 years and older in the United States. Sampling was performed by the address-based, area probability methods using in-person household screening and Audio Computer-Assisted Self-Interviewing data collection. Wave 2 (N = 28 362 adults) was fielded between October 2014 and October 2015 and was the first PATH survey to include gender identity in the survey instrument. Sampling weights adjust for oversampling of tobacco users, African Americans, young adults 18 to 24 years, and non-response patterns. Detailed methodology regarding the PATH Study can be found elsewhere.10
Measures
Standard demographic variables were collected and included: age, race, household income, and educational attainment. Variables were selected and recoded to reflect the categories and tobacco products explored in previously published studies to facilitate the comparison of findings.5 Binary sex was assessed by asking “What is your sex?” with “Male” or “Female” as the 2 response options. Transgender status was assessed with 2 items. The first item, “Do you consider yourself to be transgender,” was asked of all respondents and followed this question prompt: “Some people describe themselves as transgender when they experience a different gender identity from their sex at birth. For example, a person born into a male body, but who feels female or lives as a woman would be transgender.” If a respondent identified as transgender, then that person was asked, “Do you consider yourself to be male-to-female, female-to-male, or non-conforming?” Sexual identity was assessed with 1 item that asked, “Do you consider yourself to be . . .” with the following response options: “Straight,” “Lesbian or gay,” “Bisexual,” or “Something else.”
Current tobacco use
Established current cigarette use is defined as having ever smoked at least 100 cigarettes and currently smoking “every day” or “some days.” An alternative operationalization was also used that eliminated the 100-cigarette threshold as was done in a previous study.5 Current use of electronic cigarettes (inclusive of e-cigarettes, e-cigars, e-pipes, e-hookahs, personal vaporizers, vape pens, and hookah pens) or cigars (inclusive of traditional cigars, cigarillos, and filtered cigars) was defined as any respondent who has ever tried the specific product and currently uses it “every day” or “some days.” In addition, a combined current tobacco use variable was created. Specifically, any respondent who currently used cigarettes (using the 100-cigarette threshold), e-cigarettes, or cigar was considered a current tobacco user and all other respondents were considered non-current tobacco users.
Perceived tobacco addiction
Two items were used to assess perceived addiction to tobacco. The first item (“Do you consider yourself addicted to” [tobacco product type[s] used]?) assessed perceived addiction with the following response options: “No, not at all,” “Yes, somewhat addicted,” “Yes, very addicted.” The second item (“Do you ever have strong cravings to” [tobacco product type[s] used]?) assessed perceived cravings with a “yes” or “no” response option. These items were presented to established tobacco users and analyzed in this study only among respondents who reported current use of cigarettes, e-cigarettes, or cigars as previously defined.
Statistical analysis
There were 28 362 adult respondents in PATH Wave 2. Missing data on the gender identity variable were minimal (n = 250; 0.9%). Similarly, missing data on covariates were limited except for income (n = 2136; 7.5%) and sexual orientation (n = 405; 1.4%). As a result, we modeled “missing” as a categorical level of these 2 variables. Listwise deletion was used to account for missingness on age (n = 5; 0.02%), race (n = 70; 0.3%), and education (n = 145; 0.5%). Descriptive statistics were used to identify bivariate associations between all variables of interest and gender identity using chi-square tests. Then, bivariate logistic regression models were used to identify crude associations between gender identity and current tobacco use. Separate models were created for cigarettes, e-cigarettes, and cigars. Multivariable logistic regression was used to assess the association between gender identity and current tobacco use adjusting for age, race, household income, and educational attainment. All analyses were performed using SAS 9.3 and were weighted to account for sampling scheme and to create nationally representative estimates.
Results
Approximately 0.5% of the sample identified as transgender (n = 154). This represents a population of more than 1.1 million individuals in the United States. Overall, 23.0% of transgender respondents considered themselves “male-to-female,” 13.4% identified as “female-to-male,” 11.4% as “non-conforming,” 36.4% did not identify with any of these labels, and 15.8% were unsure. The sociodemographic characteristics of transgender and cisgender respondents are provided in Table 1. There were statistically significant differences between these populations by sexual identity, race/ethnicity, household income, and educational attainment (P < .01). Whereas most of the transgender respondents identified as heterosexual or straight (62.0%), gay/lesbian, bisexual, or some other non-heterosexual identities were more commonly endorsed by transgender compared with cisgender respondents. Transgender respondents were also more likely to identity as Hispanic (38.2% vs 15.0%), to report a household income less than $25 000 a year (50.4% vs 29.6%), and to have completed less than a high school education (32.2% vs 11.1%) compared with the cisgender sample.
Table 1.
Population characteristics of transgender and cisgender respondents (N = 27 942).
| Transgender |
Cisgender |
P-value | |||
|---|---|---|---|---|---|
| n (%) | (95% CI) | n (%) | (95% CI) | ||
| Total | 154 (0.5) | (0.3-0.6) | 27 788 (99.5) | (99.4-99.7) | |
| Binary sex | |||||
| Male | 76 (50.4) | (38.2-62.7) | 13 736 (47.9) | (47.8-48.1) | .624 |
| Female | 77 (49.2) | (37.2-61.3) | 14 032 (52.0) | (51.8-52.1) | |
| Don’t know/not sure | 1 (0.3) | (0.0-1.0) | 20 (0.1) | (0.0-0.1) | |
| Sexual identity | |||||
| Heterosexual/straight | 87 (62.0) | (51.1-72.8) | 25 732 (94.2) | (93.8-94.6) | <.001 |
| Gay/lesbian | 15 (10.0) | (2.7-17.2) | 558 (1.4) | (1.2-1.6) | |
| Bisexual | 19 (8.5) | (4.6-12.3) | 889 (1.9) | (1.7-2.1) | |
| Something else | 31 (18.5) | (9.5-27.5) | 397 (1.3) | (1.1-1.5) | |
| Missing/refused | 2 (1.0) | (0.0-2.7) | 212 (1.2) | (1.0-1.4) | |
| Age | |||||
| 18-24 | 49 (14.7) | (8.4-21.1) | 8029 (12.7) | (12.6-12.9) | .122 |
| 25-44 | 62 (46.0) | (35.3-56.7) | 9695 (34.0) | (33.7-34.3) | |
| 45-64 | 34 (25.8) | (14.3-37.4) | 7379 (34.4) | (34.0-34.7) | |
| 65+ | 9 (13.4) | (3.7-23.1) | 2685 (18.9) | (18.6-19.2) | |
| Race or ethnicity | |||||
| Hispanic | 51 (38.2) | (26.7-49.7) | 4909 (15.0) | (14.8-15.1) | <.001 |
| White | 70 (45.9) | (34.8-56.9) | 16 657 (65.7) | (65.6-65.9) | |
| Black | 20 (8.3) | (4.1-12.6) | 4104 (11.6) | (11.5-11.7) | |
| Other | 13 (7.6) | (0.2-14.9) | 2118 (7.7) | (7.6-7.8) | |
| Household income | |||||
| Missing/refused | 11 (5.4) | (1.8-9.0) | 1928 (8.1) | (7.6-8.6) | <.001 |
| <$25 000 | 83 (50.4) | (39.7-61.0) | 10 535 (29.6) | (28.7-30.4) | |
| $25 000-$49 999 | 33 (26.7) | (16.1-37.3) | 5870 (21.0) | (20.2-21.7) | |
| $50 000-$74 999 | 8 (6.4) | (0.00-13.2) | 3420 (14.1) | (13.5-14.7) | |
| >$75 000 | 19 (11.1) | (3.5-18.7) | 6035 (27.3) | (26.3-28.2) | |
| Education | |||||
| <High School | 36 (32.2) | (17.8-46.5) | 3672 (11.1) | (10.6-11.5) | <.001 |
| High school or GED | 48 (23.3) | (14.6-31.9) | 8351 (28.3) | (27.7-28.8) | |
| Some college | 51 (26.3) | (17.2-35.4) | 9770 (32.1) | (31.6-32.7) | |
| Bachelor’s degree | 15 (15.1) | (5.9-24.3) | 3920 (18.1) | (17.8-18.4) | |
| Any postgraduate | 4 (3.2) | (0.00-7.8) | 2075 (10.4) | (10.2-10.7) | |
| Tobacco use behaviors | |||||
| Any cigarettes, e-cigarettes, cigars | 80 (32.6) | (24.0-41.1) | 11 933 (23.6) | (23.0-24.2) | .023 |
| Cigarettes (with 100-cigarette threshold) | 57 (22.6) | (15.9-29.4) | 9496 (18.6) | (18.1-19.2) | .202 |
| Cigarettes (no 100-cigarette threshold) | 82 (34.9) | (25.3-44.5) | 11 411 (22.4) | (21.8-23.0) | .003 |
| E-cigarettes | 33 (12.4) | (7.0-17.3) | 3559 (6.5) | (6.2-6.8) | .003 |
| Cigars | 29 (11.6) | (6.3-17.0) | 2829 (5.7) | (5.5-6.0) | .003 |
Abbreviations: CI, confidence interval; GED, general education development.
Results include unweighted frequencies and weighted percentages.
There were significant bivariate differences in reported tobacco use behaviors by gender identity (Table 1). Specifically, a larger percentage of transgender compared with cisgender respondents (32.6% vs 23.6%) reported current use of any tobacco products (ie, cigarettes, e-cigarettes, or cigars). With 1 exception, current use of specific tobacco products also differed significantly by sexual identity. Transgender (compared with cisgender) respondents reported higher current use of cigarettes (34.9% vs 22.4%, P = .003; without 100-cigarette threshold), e-cigarettes (12.4% vs 6.5%, P = .003), and cigars (11.6% vs 5.7%, P = .003). Transgender respondents were no more likely to be current established cigarette users (defined by smoking ⩾100 cigarettes over lifetime) compared with cisgender respondents (22.6% vs 18.6%; P = .20). As a result, current use of cigarettes with no lifetime threshold was modeled in subsequent regression analyses (Table 2).
Table 2.
Logistic regression models of tobacco use behaviors by gender identity, sexual orientation, and sociodemographic variables.
| Crude odds ratios | Model 1: Any cigarettes, cigars, or e-cigarettes |
Model 2: Cigarettes (no 100-cigarette threshold) |
Model 3: E-cigarettes |
Model 4: Cigars |
|---|---|---|---|---|
| OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Gender identity | ||||
| Transgender | 1.56 (1.06-2.31) | 1.86 (1.22-2.84) | 2.03 (1.24-3.33) | 2.17 (1.26-3.72) |
| Cisgender | 1.00 | 1.00 | 1.00 | 1.00 |
| AOR | AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | AOR (95% CI) |
| Gender identity | ||||
| Transgender | 1.19 (0.75-1.89) | 1.30 (0.80-2.12) | 1.42 (0.87-2.31) | 1.80 (1.00-3.22) |
| Cisgender | 1.00 | 1.00 | 1.00 | 1.00 |
| Binary sex | ||||
| Male | 1.00 | 1.00 | 1.00 | 1.00 |
| Female | 0.56 (0.53-0.60) | 0.66 (0.62-0.71) | 0.78 (0.71-0.85) | 0.21 (0.19-0.24) |
| Don’t know/not sure | 0.20 (0.03-1.26) | 0.31 (0.07-1.26) | 0.13 (0.01-1.52) | 0.09 (0.01-1.10) |
| Sexual identity | ||||
| Heterosexual/straight | 1.00 | 1.00 | 1.00 | 1.00 |
| Gay/lesbian | 1.81 (1.40-2.34) | 2.11 (1.65-2.72) | 2.61 (2.03-3.37) | 1.08 (0.74-1.57) |
| Bisexual | 2.13 (1.73-2.62) | 2.02 (1.65-2.48) | 2.13 (1.65-2.75) | 2.42 (1.79-3.28) |
| Something else | 0.59 (0.44-0.79) | 0.70 (0.51-0.94) | 0.73 (0.51-1.05) | 0.92 (0.53-1.60) |
| Missing/refused | 0.37 (0.26-0.53) | 0.39 (0.26-0.58) | 0.33 (0.17-0.66) | 0.41 (0.22-0.76) |
| Age | ||||
| 18-24 | 1.00 | 1.00 | 1.00 | 1.00 |
| 25-44 | 1.36 (1.25-1.48) | 1.43 (1.32-1.55) | 0.79 (0.70-0.89) | 0.77 (0.68-0.87) |
| 45-64 | 0.92 (0.84-1.01) | 0.94 (0.86-1.02) | 0.40 (0.36-0.46) | 0.57 (0.50-0.65) |
| 65+ | 0.27 (0.24-0.30) | 0.26 (0.23-0.30) | 0.11 (0.09-0.14) | 0.21 (0.16-0.28) |
| Race or ethnicity | ||||
| Hispanic | 0.41 (0.37-0.46) | 0.46 (0.41-0.51) | 0.52 (0.45-0.60) | 0.67 (0.58-0.77) |
| White | 1.00 | 1.00 | 1.00 | 1.00 |
| AOR | AOR (95% CI) | AOR (95% CI) | AOR (95% CI) | AOR (95% CI) |
| Black | 0.77 (0.70-0.85) | 0.87 (0.79-0.95) | 0.62 (0.54-0.72) | 1.23 (1.08-1.40) |
| Other | 0.63 (0.56-0.70) | 0.70 (0.61-0.80) | 0.88 (0.74-1.04) | 0.57 (0.48-0.67) |
| Household income | ||||
| Missing/Refused | 0.52 (0.46-0.59) | 0.54 (0.48-0.61) | 0.62 (0.51-0.75) | 0.55 (0.45-0.67) |
| <$25 000 | 1.00 | 1.00 | 1.00 | 1.00 |
| $25 000-$49 999 | 0.65 (0.58-0.72) | 0.62 (0.57-0.69) | 0.73 (0.64-0.84) | 0.67 (0.57-0.77) |
| $50 000-$74 999 | 0.48 (0.44-0.53) | 0.44 (0.40-0.49) | 0.68 (0.59-0.78) | 0.58 (0.49-0.68) |
| >$75 000 | 0.39 (0.35-0.43) | 0.33 (0.29-0.36) | 0.48 (0.41-0.57) | 0.68 (0.59-0.79) |
| Education | ||||
| <High School | 1.00 | 1.00 | 1.00 | 1.00 |
| High school or GED | 0.90 (0.80-1.01) | 0.84 (0.75-0.94) | 1.04 (0.90-1.21) | 0.97 (0.80-1.17) |
| Some college | 0.68 (0.61-0.77) | 0.58 (0.52-0.66) | 0.98 (0.84-1.14) | 1.02 (0.86-1.22) |
| Bachelor’s degree | 0.35 (0.30-0.41) | 0.28 (0.23-0.33) | 0.43 (0.34-0.53) | 0.93 (0.74-1.16) |
| Any postgraduate | 0.25 (0.21-0.30) | 0.18 (0.15-0.22) | 0.30 (0.22-0.40) | 0.85 (0.65-1.11) |
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval; GED, general education development; OR, odds ratio.
The crude odds ratios of tobacco use were higher for transgender (compared with cisgender) respondents for all the 3 tobacco products (Table 2). However, in multivariable analyses, transgender identity was not associated with any of the 3 tobacco behaviors or the summary measure of tobacco use (ie, any current use of cigarettes, e-cigarettes, or cigars). In each of the models, female binary sex (compared with male), older age, Hispanic ethnicity (compared with non-Hispanic white), higher household income, and higher educational attainment were independently associated with lower odds of current use of cigarettes, e-cigarettes, or cigars, whereas sexual minority identity (ie, gay/lesbian or bisexual) was independently associated with higher odds of use.
Although there was a variation in the type of tobacco products used by specific transgender subgroups, these differences were not statistically significant (Figure 1). For example, whereas 22.5% (95% confidence interval [CI]: 6.7-38.4) of “male-to-female” transgender respondents reported using e-cigarettes, compared with 14.8% of “female-to-male” and 9.3% of “gender non-conforming” respondents, there was a complete overlap in the error estimates with all of the other transgender subgroups. Thus, these differences were not statistically significant (P > .05).
Figure 1.

Tobacco use behaviors by transgender identity (N = 154).
Perceived addiction to tobacco was high among all users. The percentages of cisgender and transgender respondents who perceived that they were “very” or “somewhat” addicted to tobacco were statistically equivalent (Figure 2). The percentage of cisgender and transgender respondents who perceived that they had strong cravings for tobacco was statistically equivalent (Figure 3).
Figure 2.
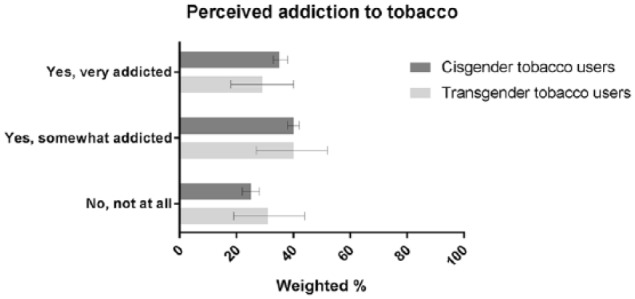
Perceived addiction to tobacco among current tobacco users by gender identity.
Figure 3.
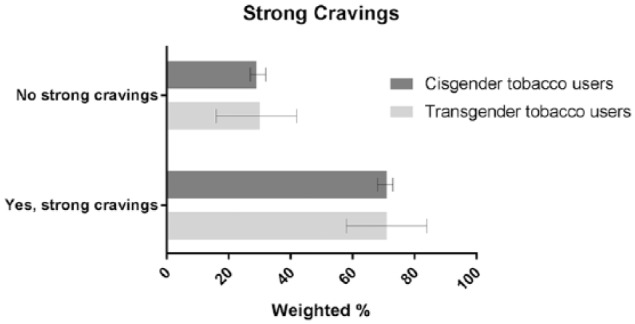
Perceived tobacco cravings among current tobacco users by gender identity.
Discussion
In this study, we estimated tobacco use behaviors among transgender persons in a nationally representative sample of adults in the United States and compared tobacco use between cisgender and transgender respondents. Although bivariate differences in cigarette, e-cigarette, and cigar use were identified—tobacco use was more prevalent among transgender respondents—these differences appear to be related to other sociodemographic characteristics (eg, educational attainment and income) rather than gender identity. Thus, the previous finding that transgender adults use tobacco at much higher rates than cisgender populations was not supported by this study (ie, Hypotheses H1a, H1b, and H1c).5
The differences in tobacco use patterns reported here appear to be related to important sociodemographic differences between transgender and cisgender populations. The transgender sample had lower socioeconomic status on indicators that are commonly associated with higher tobacco use (eg, lower educational attainment and income).11 Although bivariate differences in tobacco use were identified as in previous research,2,5 these differences were not significant after adjusting the models for those sociodemographic factors. Of the 2 other published population-based studies examining tobacco use differences by gender identity, one found similar sociodemographic differences between the transgender and cisgender samples and the other did not.2,5 These demographic differences likely reflect the sampling strategies employed by the 2 studies (ie, a web-based panel survey in the former and random digit dial in the latter). This study used a random household sample and Audio Computer-Assisted Self-Interviewing.10
We propose that these demographic differences are in fact a reflection of actual population-based differences resulting from the systematic stigma and discrimination experienced by transgender populations that limit educational and employment opportunities.12,13 There are a number of psychosocial and structural risk factors that may contribute to higher tobacco use among these populations. Social stressors associated with transgender identities, including identity development and related conflicts, can lead to increased substance use as a coping mechanism.14 Gender minority youth and adults have been shown to experience chronic levels of harassment, discrimination, and violence that are associated with substance use,13,15 as well as related mental health disorders.16 Discrimination can also influence tobacco use indirectly through limited educational attainment, in addition to structural discrimination in housing and employment.13,17 Tobacco industry marketing toward SGM communities through direct and indirect advertisings, community outreach, and sponsorships may also increase susceptibility to tobacco use.18,19 In addition, the cultural associations of tobacco use with masculinity and rebellion may be particularly salient messages for gender minorities who are actively engaged in the affirmation of their gender identieis.20
Future research is needed to test specific hypotheses about the relationship between socioeconomic status and tobacco use in transgender populations. Based on our current findings, we propose that lower socioeconomic status completely mediates the association between transgender identity and tobacco use, and that there are multilevel factors (eg, state and local policies, family acceptance, access to gender affirmative care) that are protective against gender-identity-based stigma and discrimination.
In our exploratory analyses, we found that there were no statistically significant differences in tobacco use across transgender subgroups (ie, based on transgender identities like “male-to-female” or non-binary). In qualitative research, some SGM persons endorsed tobacco products as a way of expressing gender—in particular, aspects of toughness and masculinity.21 Thus, we may expect higher tobacco use among transgender populations who are seeking a masculine gender presentation.
We also found that perceived tobacco addiction and the experience of cravings are similar between transgender and cisgender tobacco users. These findings are in contrast to what may be expected based on parallel studies of sexual minority populations, which found significantly higher levels of tobacco use disorders among gay/lesbian and bisexual individuals.22 If minority stress operates on transgender individuals in similar ways, then we can hypothesize that they would engage in similar coping behaviors like tobacco use.14,23–25
These findings should be evaluated against the limitations of this study. First, tobacco use is based on self-report and may reflect social desirability bias, and thus it is possible that current use is underestimated in this study. Second, the transgender sample was small, and, as a result, the standard errors of the estimates presented are large. This may bias the results toward the null and may reduce the reliability of the estimates. This is particularly true for the exploratory analyses of the transgender and tobacco user subsamples. Third, a dichotomous measure of transgender identity does not reflect the heterogeneity of gender identities among transgender populations. Thus, the importance of those differences (eg, differences in gender expression, experiences of discrimination, social networks) in relation to tobacco use is not fully reflected in the current analyses.
Conclusions
The prevalence of the use of 3 popular tobacco products—cigarettes, e-cigarettes, and cigars—was statistically equivalent between transgender and cisgender populations in the national study of adults in the United States. We were unable to replicate findings from previous research that showed much higher rates of tobacco use among transgender individuals. The differences in tobacco use that we did identify in bivariate analyses were fully explained by differences in sociodemographic characteristics (eg, income and education) between the transgender and cisgender populations.
Footnotes
Funding:The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ORCID iD: Christopher W Wheldon  https://orcid.org/0000-0002-0452-0252
https://orcid.org/0000-0002-0452-0252
Author Contributions: Christopher Wheldon conceptualized the study, analyzed the data, and contributed to the writing of the manuscript. Kara Wiseman contributed to conceptualization of the study and the writing of the manuscript.
References
- 1. Lee JGL, Griffin GK, Melvin CL. Tobacco use among sexual minorities in the USA, 1987 to May 2007: a systematic review. Tob Control. 2009;18:275–282. [DOI] [PubMed] [Google Scholar]
- 2. Hoffman L, Delahanty J, Johnson SE, Zhao X. Sexual and gender minority cigarette smoking disparities: an analysis of 2016 Behavioral Risk Factor Surveillance System data. Prev Med (Baltim). 2018;113:109–115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Wheldon CW, Kaufman AR, Kasza KA, Moser RP. Tobacco use among adults by sexual orientation: findings from the Population Assessment of Tobacco and Health study. LGBT Health. 2018;5:33–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Emory K, Buchting FO, Trinidad DR, Vera L, Emery SL. Lesbian, gay, bisexual, and transgender (LGBT) view it differently than non-LGBT: exposure to tobacco-related couponing, e-cigarette advertisements, and anti-tobacco messages on social and traditional media. Nicotine Tob Res. 2019;21:513–522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Buchting FO, Emory KT, Scout, et al. Transgender use of cigarettes, cigars, and E-cigarettes in a national study. Am J Prev Med. 2017;53:e1–e7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Lagos D. Looking at population health beyond “male” and “female”: implications of transgender identity and gender nonconformity for population health. Demography. 2018;55:2097–2117. [DOI] [PubMed] [Google Scholar]
- 7. Streed CG, McCarthy EP, Haas JS. Self-reported physical and mental health of gender nonconforming transgender adults in the United States. LGBT Health. 2018;5:443–448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Institute of Medicine (IOM). The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. Washington, DC: The National Academies Press, IOM; 2011. [PubMed] [Google Scholar]
- 9. Schisterman EF, Cole SR, Platf RW. Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology. 2009;20:488–495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Hyland A, Ambrose BK, Conway KP, et al. Design and methods of the Population Assessment of Tobacco and Health (PATH) Study. Tob Control. 2017;26:371–378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Hiscock R, Bauld L, Amos A, Fidler JA, Munafò M. Socioeconomic status and smoking: a review. Ann N Y Acad Sci. 2012;1248:107–123. [DOI] [PubMed] [Google Scholar]
- 12. Bradford J, Reisner SL, Honnold JA, Xavier J. Experiences of transgender-related discrimination and implications for health: results from the Virginia Transgender Health Initiative Study. Am J Public Health. 2013;103:1820–1829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Shires DA, Jaffee KD. Structural discrimination is associated with smoking status among a national sample of transgender individuals. Nicotine Tob Res. 2016;18:1502–1508. [DOI] [PubMed] [Google Scholar]
- 14. Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull. 2003;129:674–697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Reisner SL, Greytak EA, Parsons JT, Ybarra ML. Gender minority social stress in adolescence: disparities in adolescent bullying and substance use by gender identity. J Sex Res. 2015;52:243–256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Mustanski BS, Garofalo R, Emerson EM. Mental health disorders, psychological distress, and suicidality in a diverse sample of lesbian, gay, bisexual, and transgender youths. Am J Public Health. 2010;100:2426–2432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Drescher CF, Lopez EJ, Griffin JA, Toomey TM, Eldridge ED, Stepleman LM. Mental health correlates of cigarette use in LGBT individuals in the southeastern United States. Subst Use Misuse. 2018;53:891–900. [DOI] [PubMed] [Google Scholar]
- 18. Smith EA, Thomson K, Offen N, Malone RE. “If you know you exist, it’s just marketing poison”: meanings of tobacco industry targeting in the lesbian, gay, bisexual, and transgender community. Am J Public Health. 2008;98:996–1003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Stevens P, Carlson LM, Hinman JM. An analysis of tobacco industry marketing to lesbian, gay, bisexual, and transgender (LGBT) populations: strategies for mainstream tobacco control and prevention. Health Promot Pract. 2004;5:129S–134S. [DOI] [PubMed] [Google Scholar]
- 20. Remafedi G. Lesbian, gay, bisexual, and transgender youths: who smokes, and why? Nicotine Tob Res. 2007;9:65–71. [DOI] [PubMed] [Google Scholar]
- 21. Matthews AK, Cesario J, Ruiz R, Ross N, King A. A qualitative study of the barriers to and facilitators of smoking cessation among lesbian, gay, bisexual, and transgender smokers who are interested in quitting. LGBT Health. 2017;4:24–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Boyd CJ, Veliz PT, Stephenson R, Hughes TL, McCabe SE. Severity of alcohol, tobacco, and drug use disorders among sexual minority individuals and their “not sure” counterparts. LGBT Health. 2019;6:15–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Lick DJ, Durso LE, Johnson KL. Minority stress and physical health among sexual minorities. Perspect Psychol Sci. 2013;8:521–548. [DOI] [PubMed] [Google Scholar]
- 24. Meyer IH. Minority stress and mental health in gay men. J Health Soc Behav. 1995;36:38–56. [PubMed] [Google Scholar]
- 25. Meyer IH. Does an improved social environment for sexual and gender minorities have implications for a new minority stress research agenda? HHS public access. Psychol Sex Rev. 2016;7:81–90. [PMC free article] [PubMed] [Google Scholar]