

Abstract
Background: Measurement of wrist range of motion (ROM) is important to all aspects of treatment and rehabilitation of upper extremity conditions. Recently, gyroscopes have been used to measure ROM and may be more precise than manual evaluations. The purpose of this study was to evaluate the use of the iPhone gyroscope application and compare it with use of a goniometer, specifically evaluating its accuracy and ease of use. Methods: A cross-sectional study evaluated adult Caucasian participants, with no evidence of wrist pathology. Wrist ROM measurements in 306 wrists using the 2 methods were compared. Demographic information was collected including age, sex, and occupation. Analysis included mixed models and Bland-Altman plots. Results: Wrist motion was similar between the 2 methods. Technical difficulties were encountered with gyroscope use. Age was an independent predictor of ROM. Conclusions: Correct measurement of ROM is critical to guide, compare, and evaluate treatment and rehabilitation of the upper extremity. Inaccurate measurements could mislead the surgeon and harm patient adherence with therapy or surgeon instruction. An application used by the patient could improve adherence but needs to be reliable and easy to use. Evaluation is necessary before utilization of such an application. This study supports revision of the application on the iPhone to improve ease of use.
Keywords: iPhone, goniometer, gyroscope, wrist motion, measurement
Introduction
Measurements of wrist range of motion (ROM) are ubiquitously utilized in diagnosing pathology, establishing prognosis, and following the progress of treatment and rehabilitation of the upper extremity. Traditionally, these measurements have been performed using a goniometer. Accurate methods for using the goniometer have been established.3 Carter et al found that a dorsal-volar placement of the goniometer obtained the most accurate measurements of wrist flexion, extension, and ulnar and radial deviation.3 In addition, single measurements have been found to be sufficient and accurate, even by multiple users.5-7 In recent years, gyroscopes, like the DynaPort MiniMod and TriGyro, have entered clinical use for measuring ROM and have been found to be more precise.4,8,12,13 However, devices like this are often expensive and scarce. Furthermore, despite the availability of new technology, it is not always easy to adapt it to the clinical setting. Recent developments with smartphone technology have begun utilizing the phone’s internal gyroscope and accelerometer. These have resulted in the development of free or inexpensive applications that have the potential to accurately measure ROM in the clinic or even at home. Previous studies have evaluated the smartphone gyroscope for use in the assessment of limb motion. LeMoyne and Mastroianni evaluated the application and found that it has considerable accuracy and consistency for quantification of the patella tendon reflex response.10 Another study evaluated categories of physical activity such as walking and jogging concluding that the gyroscope was able to recognize motion with high accuracy when onboard the iPhone.16 Kim et al evaluated the utility of the iPhone gyroscope in the measurement of wrist motion. They concluded that the application was easy to use and can be used outside of the clinical setting.8 The viability of such applications has not yet been well established.8
The purpose of this study was to evaluate the use of the gyroscope application on the iPhone as compared with a goniometer, specifically the application’s accuracy and ease of use. We hypothesized that the gyroscope application is an accurate device that will be easier to use.
Materials and Methods
Institutional review board (IRB) approval was obtained prior to study commencement, and participants signed a consent form prior to evaluation. A cross-sectional study was performed. Inclusion criteria included adult (between 18 and 80 years of age) Caucasian participants, with no history of wrist pain or symptoms. We evaluated Caucasians because that is the majority of our population. Race has been shown to affect parameters such as grip strength, generalized joint mobility, and palm size. Consequently, though differences in wrist motion have not been specifically studied, it may also affect motion of the wrist. We therefore included only Caucasian participants to examine a homogeneous normal population without innate differences that may influence the measurements, thus correcting for potential confounding factors.11,14,16-18 Exclusion criteria included a history of injury, surgery, congenital, or any history of pain or other symptoms in the hand or wrist. Demographic information was collected including age, sex, occupation, and body mass index (BMI). BMI was calculated based on stated heights and weights of participants and not directly measured.
ROM was measured using a goniometer and a gyroscope. Measurements took place in public places to be able to evaluate the ease of use outside the clinical setting. Total evaluation time for each participant was about 10 minutes.
Measurement of ROM Using the Goniometer
The arm was positioned at 90° with the elbow supported on a table. The forearm was placed in neutral rotation. The measurement was performed dorsally along the joint line of the wrist which is more reliable according to a recent study.3 The goniometer was centered over the capitate. One limb was placed along the dorsal surface of the third metacarpal bone while the other limb was placed parallel to the axis of the ulna.
Measurement of ROM Using the Gyroscope
The gyroscope is a free application for iPhone 4 and above and can measure differences in height, rotation, slope, and acceleration. Direction is expressed as roll, pitch, and yaw in degrees. To perform the measurements, the back of the iPhone was placed on the back of the hand, with the left bottom corner touching the extensor pollicis longus (EPL) in the anatomic snuffbox. The motions of the wrist were then measured using the pitch (for flexion and extension) and yaw (for ulnar and radial deviation).
A total of 306 normal wrists in 171 participants were evaluated. The demographics of our population are described in Table 1.
Table 1.
Description of Our Participant Population.
| Caucasian | |
|---|---|
| Sex (males), % | 50 |
| Age, y, mean (SD) | 45.9 (20.2) |
| Body mass index, mean (SD) | 25.8 (5.6) |
| Occupation (manual labor), % | 8.4 |
| Dominance (right handed), % | 89.7 |
| Height, m, mean (SD) | 170 (0.11) |
Note. We distinguished between heavy labor and more sedentary occupations as this distinction has been shown to affect wrist motion.
Data Analysis
Linear mixed models were used because our measurements included continuous variables. These models allow analysis of data in the presence of multiple observations from the same participant. In this case, they account for the use of data from both normal hands in the same individual. This analysis assesses the relative contribution of the different variables on the outcome measure of ROM while controlling for age, sex, occupation, hand (right or left), and BMI.10 These variables (age, sex, occupation, etc.) are fixed effects that may affect wrist ROM and were therefore corrected for while comparing the measurements performed with the goniometer with those performed by the gyroscope.9 All occupations were documented, but we distinguished between heavy labor and more sedentary occupations as this distinction has been shown to affect wrist motion.9 All P values were 2-sided, and statistical significance was defined as P < .05. Data analysis was performed using IBM SPSS statistical package version 22.0 (SPSS Inc, Chicago, Illinois).
The Bland-Altman plot,1,2 or difference plot, is a graphical method to compare 2 measurement techniques. This was used to identify any inherent bias (if one measurement consistently measures differently in a certain direction than the other measurement—for example, if method 1 measures a smaller angle than method 2 on a regular basis) and to reveal any relationship between the differences between the 2 measurements and the magnitude of the measurements (Figure 1).
Figure 1.
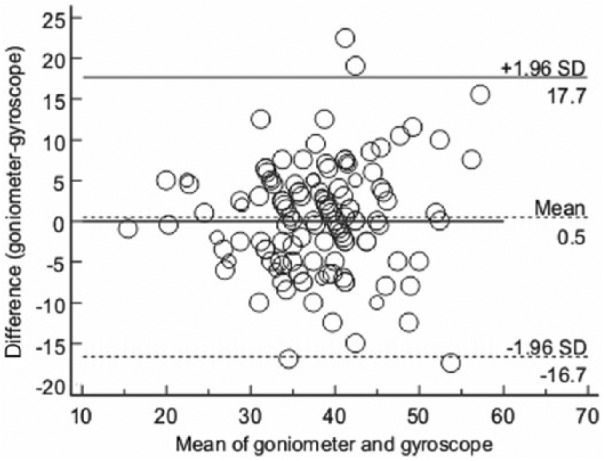
Bland-Altman plot for wrist extension, flexion, ulnar deviation, radial deviation, plotting the difference between measurements with the gyroscope and the goniometer.
Note. The graph displays a scatter diagram of the differences plotted against the averages of the 2 measurements. Horizontal lines are drawn at the mean difference, and at the limits of agreement, which are defined as the mean difference plus and minus 1.96 times the standard deviation of the differences. The resulting plot demonstrates a random distribution (thus no systemic bias) and the mean coinciding with 0 value.
Results
The average ROM as measured by both methods is described in Table 2. The agreement between the goniometer and the gyroscope in flexion, extension, radial deviation, and ulnar deviation as described by the Bland-Altman plot did not reveal any bias inherent to the measurements. Figure 1 is a Bland-Altman plot with multiple measurements per participant (using both hands). There was a statistically significant difference in flexion between the 2 methods of measurement, but the difference was of 1° on average. One degree of motion is difficult to measure and likely has no effect on function.
Table 2.
Values for Wrist Motion as Measured by the Goniometer and the Gyroscope.
| Goniometer | Gyroscope | P | |
|---|---|---|---|
| Flexion (±SD) | 74.03 ± 13.0 | 72.98 ± 13.7 | .02 |
| Extension (±SD) | 66.71 ± 14.1 | 66.42 ± 14.9 | .58 |
| Radial deviation (±SD) | 28.84 ± 10.8 | 25.57 ± 11.6 | .13 |
| Ulnar deviation (±SD) | 39.40 ± 11.8 | 38.97 ± 12.5 | .37 |
Note. Values of range of motion are in degrees. Mixed models were used to estimate marginal means and standard deviation adjusting for age, sex, occupation, side (right or left), and body mass index. There is a normal range in all wrist movements. The values found in our population were similar to other published data. The table also illustrates that the standard deviations were similar between the 2 methods of measurement.
Using mixed model analysis to correct for the use of both hands in the same individual, age was found to affect ROM (flexion, extension, and radial and ulnar deviation) as an independent variable (P = .001) while sex did not (P = .4).
Qualitatively, when compared with measurement of wrist ROM with the goniometer, the use of the application was more time-consuming and more complex (eg, the examiner had to subtract the initial angle from the measured angle). The technical difficulties we noted with the use of the iPhone gyroscope application subsisted despite the good agreement between the methods of measurement found in the study.
Specifically, the application includes an intrinsic setting angle for which pitch and roll should be 0. This means that the gyroscope compares the angle of the patient’s hand relative to a known value for horizontal, while the goniometer always measures the angle of the patient’s hand relative to their forearm no matter how their arm is positioned in space. Unless starting the application on a flat surface, therefore, often the pitch and roll do not start at 0. For instance, when you lay the phone on a flat table, it tends to start closer to 0, giving minimal error. However, when you open the application with the phone placed on a patient’s hand, if there is any angle of the patient’s forearm relative to the flat 0° set point, the pitch and roll will show an initial nonzero reading.
As there is no reset or zero option within the open application, any changes related to the horizon line need to be calculated into the measurements at all times. For example, with use of the gyroscope application to measure flexion and extension, the final reading after flexion and extension must be subtracted from the initial reading to obtain the true angle of movement.
Also, any movement of the forearm while measuring will not be accounted for because the gyroscope only has one frame of reference at any one point in time. If the forearm moves during the measurement, the angle of movement will be included in the final measurement of the angle of wrist movement. The only way to prevent this complication was by carefully stabilizing the forearm to prevent any motion. This made the measurement more difficult to perform. With use of the goniometer, this is not an issue because it includes 2 frames of reference, always measuring the hand relative to the forearm simultaneously.
Discussion
This study aimed to evaluate the gyroscope application for its ease of use in the clinic and at home. There was good agreement between the 2 methods of measurement for wrist ROM. Kim et al performed a study using the iPhone gyroscope and found wrist ROM measurements that were similar to those found in our population.8 When the iPhone gyroscope was used in a setting in which there was proper stabilization of the forearm, the phone was secured to the dorsal aspect of the hand, and there was professional oversight, the application was found to be very accurate and useful.8 They concluded that the application could be used easily by the patients outside of the clinic situation. Our results differed from those of Kim et al in the variability of the measurements. Our standard deviations were higher than those measured in the Kim et al article.8 However, they were lower than in other studies evaluating wrist motion.15 This perhaps can be explained by differences in population (variability of race, age, etc). We also differed from the Kim article in that that we found that use of the application was more complicated than expected. This was mostly due to the specific position requirements and the special considerations needed to get accurate readings as outlined above. These difficulties may have been due to the fact that we were using this application for the measurement of wrist motion for the first time and were inexperienced with its use. However, we believe that some of these include intrinsic problems with application itself. Despite the application being easily accessible and free, it would require a significant effort and diligence on the part of the patient to perform the measurements appropriately. Furthermore, inaccurate measurements could potentially harm patient adherence with therapy or surgeon instruction. Therefore, for patients to utilize the application, they would need instruction while in therapy and then to be adherent enough to follow directions carefully to minimize the sources of error found in this study. They may also need to purchase any accessory equipment needed to aid them in proper measurement.
Although the gyroscope was found to be accurate (closely associated to the gold standard of goniometric measurement), this study has led us to reject our hypothesis in that we found the gyroscope to be more difficult to use than the goniometer. Based on our findings, there are a few recommendations for adjustments of the application to make it more suitable or applicable as a tool for use in therapy. One such feature could be the addition of a reset button that could re-zero the values for pitch, yaw, and roll, while the application is in use. Similarly, it would be beneficial to change the application’s intrinsic understanding of pitch and roll, having pitch and roll defined as zero in the position in which the application is opened instead of having a preset understanding of zero for these parameters. Also, our measurements were taken by simply holding the iPhone carefully in position by hand. Movement of the phone could be a source of error in the final measurement. More comfortable methods of phone stabilization for a patient self-measuring, such as a strap, which holds the phone to the dorsal aspect of the hand, would be preferable and may make the measurement easier.
In summary, this study identified some challenges with the use of the iPhone gyroscope. Some changes in the design may improve its manageability enabling its use in the clinical setting. Further study is necessary to refine the application and to evaluate the results, as well as to trial the gyroscope on other joints and in a rehabilitation population.
Footnotes
Ethical Approval: This study was approved by our institutional review board.
Statement of Human and Animal Rights: All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008.
Statement of Informed Consent: Informed consent was obtained from all individual participants included in the study.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1(8476):307-310. [PubMed] [Google Scholar]
- 2. Bland JM, Altman DG. Measuring agreement in method comparison studies. Stat Methods Med Res. 1999;8(2):135-160. [DOI] [PubMed] [Google Scholar]
- 3. Carter TI, Pansy B, Wolff AL, et al. Accuracy and reliability of three different techniques for manual goniometry for wrist motion: a cadaveric study. J Hand Surg Am. 2009;34(8):1422-1428. [DOI] [PubMed] [Google Scholar]
- 4. El-Zayat BF, Efe T, Heidrich A, et al. Objective assessment of shoulder mobility with a new 3D gyroscope—a validation study. BMC Musculoskelet Disord. 2011;12:168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Ferriero G, Sartorio F, Foti C, et al. Reliability of a new application for smartphones (DrGoniometer) for elbow angle measurement. PM R. 2011;3(12):1153-1154. [DOI] [PubMed] [Google Scholar]
- 6. Ferriero G, Vercelli S, Sartorio F, et al. Reliability of a smartphone-based goniometer for knee joint goniometry. Int J Rehabil Res. 2013;36(2):146-151. [DOI] [PubMed] [Google Scholar]
- 7. Franchignoni F, Giordano A, Sartorio F, et al. Suggestions for refinement of the Disabilities of the Arm, Shoulder and Hand Outcome Measure (DASH): a factor analysis and Rasch validation study. Arch Phys Med Rehabil. 2010;91(9):1370-1377. [DOI] [PubMed] [Google Scholar]
- 8. Kim TS, Park DD, Lee YB, et al. A study on the measurement of wrist motion range using the iPhone 4 gyroscope application. Ann Plast Surg. 2014;73(2):215-218. [DOI] [PubMed] [Google Scholar]
- 9. Klum M, Wolf MB, Hahn P, et al. Normative data on wrist function. J Hand Surg Am. 2012;37(10):2050-2060. [DOI] [PubMed] [Google Scholar]
- 10. LeMoyne R, Mastroianni T. Implementation of a smartphone as a wireless gyroscope application for the quantification of reflex response. Conf Proc IEEE Eng Med Biol Soc. 2014;2014:3654-3657. [DOI] [PubMed] [Google Scholar]
- 11. Remvig L, Jensen DV, Ward RC. Epidemiology of general joint hypermobility and basis for the proposed criteria for benign joint hypermobility syndrome: review of the literature. J Rheumatol. 2007;34(4):804-809. [PubMed] [Google Scholar]
- 12. Rothstein JM, Miller PJ, Roettger RF. Goniometric reliability in a clinical setting. Elbow and knee measurements. Phys Ther. 1983;63(10):1611-1615. [DOI] [PubMed] [Google Scholar]
- 13. Van Hees VT, Slootmaker SM, De Groot G, et al. Reproducibility of a triaxial seismic accelerometer (DynaPort). Med Sci Sports Exerc. 2009;41(4):810-817. [DOI] [PubMed] [Google Scholar]
- 14. Watanabe H, Ogata K, Amano T, et al. [The range of joint motions of the extremities in healthy Japanese people—the difference according to the age (author’s transl)]. Nihon Seikeigeka Gakkai Zasshi. 1979;53(3):275-261. [PubMed] [Google Scholar]
- 15. Wollstein R, Kirk Watson H, Poultsides G, et al. Range of movement in the wrist as a diagnostic tool in radial-sided wrist pain. Scand J Plast Reconstr Surg Hand Surg. 2006;40(4):230-233. [DOI] [PubMed] [Google Scholar]
- 16. Wu SW, Wu SF, Liang HW, et al. Measuring factors affecting grip strength in a Taiwan Chinese population and a comparison with consolidated norms. Appl Ergon. 2009;40(4):811-815. [DOI] [PubMed] [Google Scholar]
- 17. Wu W, Dasgupta S, Ramirez EE, et al. Classification accuracies of physical activities using Smartphone motion sensors. J Med Internet Res. 2012;14(5):e130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Zhang Y, Yao Z, Wang S, et al. Motion analysis of Chinese normal knees during gait based on a novel portable system. Gait Posture. 2015;41(3):763-768. [DOI] [PubMed] [Google Scholar]