

A 50-year-old male presented with a 6-month-old growth on the left upper thigh. The lesion had begun as a small reddish papule that evolved into a large lobulated mass in a few months with central resolution and peripheral extension. The lesion regressed over time, but a part of it persisted at the periphery. Examination revealed an 8 × 4 cm atrophic depigmented patch with marginal hyperpigmented rim and specks of hyperpigmentation within. A 1.5 × 1 cm dome-shaped pinkish nodule topped with yellowish thick scales and a similar 1 × 1 cm lesion without scaling were noted near the margins of the patch [Figure 1].
Figure 1.

An 8 × 4 cm atrophic depigmented patch surrounded by a hyperpigmented margin showing a 1.5 × 1 cm pinkish nodule with yellowish adherent scales (black arrow) and another pinkish 1 × 1 cm nodule (blue arrow) near the margin
Dermoscopy of the scaly nodule revealed central thick yellowish-white scales (keratin) surrounded by multiple grayish-white circles, lines, and structureless zones on a pinkish background. The grayish-white circles were seen surrounding central whitish structure. Also noted were the red globules interspersed with the whitish zones [Figure 2a]. Dermoscopy of the non-scaly nodule revealed multiple whitish globules and lines on an erythematous background [Figure 2b]. On dermoscopy, the hyperpigmented margin revealed multiple dark globules and irregular pigment network, and the atrophic region showed milky white area interspersed with fine telangiectatic vessels [Figure 3].
Figure 2.
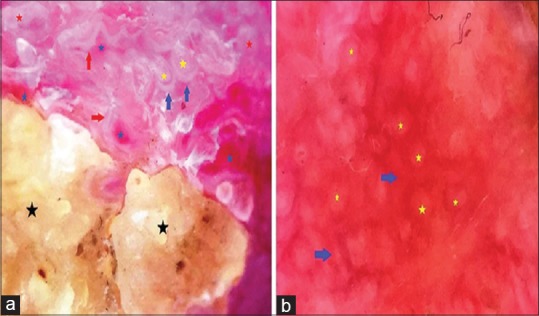
Non-contact dermoscopy of scaly nodule under polarized mode using DermLite™ DL3 shows thick yellowish-white keratin (black stars) and multiple grayish-white circles (blue arrows), lines (red arrows), and structureless zones (red stars) on a pinkish background. The grayish-white circles are seen surrounding central whitish structure (yellow stars). Also seen are red globules (blue stars) in between the whitish zones (a). Dermoscopy of the non-scaly nodule shows multiple whitish globules (yellow stars) and lines (blue arrows) on an erythematous background (b). (original magnification ×10)
Figure 3.
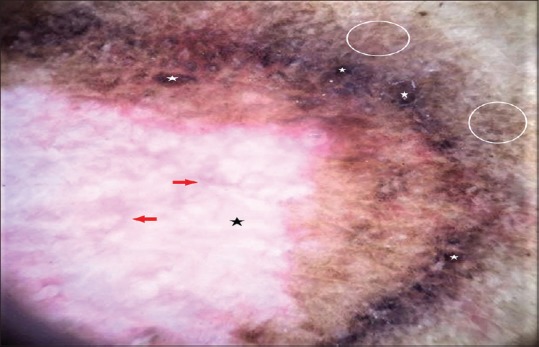
Non-contact dermoscopy of the marginal area under polarized mode using DermLite™ DL3 shows dark globules (white stars) and irregular pigment network (white circles) surrounding a milky white area (black star) interspersed with fine telangiectatic vessels (red arrows) (original magnification ×10)
Biopsy from the nodule with scaling revealed large invaginating masses of well-differentiated keratinocytes with overlying compact orthokeratotic hyperkeratosis, hypergranulosis, and acanthosis. Also noted were acanthosis and hypergranulosis of the epithelium of a dilated follicular infundibulum [Figure 4]. The clinical and histological features were characteristic of keratoacanthoma (centrifugum marginatum type).
Figure 4.
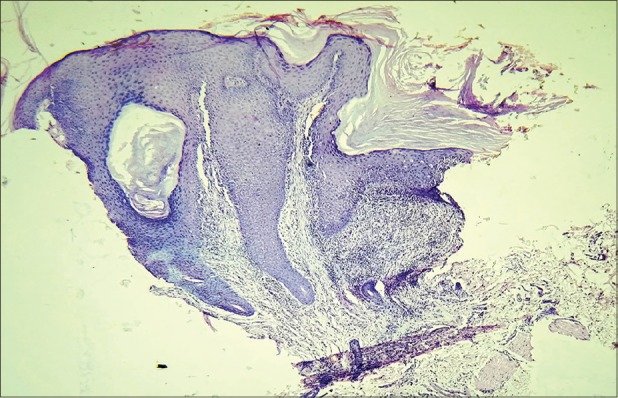
Photomicrograph showing large invaginating masses of keratinocytes with overlying compact hyperkeratosis, hypergranulosis, and acanthosis. Also note the dilated follicular infundibulum with acanthosis and hypergranulosis of its epithelium (hematoxylin and eosin, original magnification ×5)
A typical keratoacanthoma is a rapidly enlarging solitary papule that evolves into a circumscribed crateriform nodule with a keratotic plug within a few weeks, and then gradually involutes over months to leave behind an atrophic scar. Most of the lesions affect the elderly and involve the sun-exposed areas. Several other clinical forms including keratoacanthoma centrifugum marginatum are described as well. The latter is a rare type characterized by progressive peripheral growth with central clearing. Histopathologically, keratoacanthoma shows a crateriform pattern with an endoexophytic proliferation of normal keratinocytes. In the growing phase, invaginating masses of keratinocytes are seen with a keratin-filled crater. In regressing lesions, a prominent central keratin plug with “lipping” or “buttressing” of the edges of the lesion over the central crater is typical.[1,2]
Rosendahl et al. characterized keratin, surface scales, white circles, white structureless zones, and blood spots as dermoscopic criteria common to keratoacanthoma and squamous cell carcinoma (SCC) by retrospective analysis of 60 cases of invasive SCC and 43 cases of keratoacanthoma. After statistically re-evaluating the significance of these criteria with 206 non-pigmented raised lesions, they concluded that the keratin, white circles, and blood spots serve as useful clues to differentiate SCC and keratoacanthoma from other raised non-pigmented lesions. Keratin had the highest sensitivity, and white circles showed highest specificity for keratoacanthoma and SCC.[3] The dermoscopic–histopathologic correlation in our case [Figure 5] was in concordance with those delineated by Rosendahl et al. [Table 1].
Figure 5.

Dermoscopic–histopathologic correlation. The yellowish-white scales on dermoscopy correspond to the compact hyperkeratosis (black stars), the white circles to acanthosis and hypergranulosis of the infundibular epithelium (red stars), the whitish structure inside the circles correspond to the dilated infundibulum with keratin plug (blue stars), and the red globules to the microhemorrhage in the keratin (black circles) (dermoscopy, original magnification ×10; hematoxylin and eosin, original magnification ×5)
Table 1.
Dermoscopic-histopathologic correlation in keratoacanthoma (also see Figure 5)
| Dermoscopic findings | Corresponding histopathologic findings |
|---|---|
| Central yellowish-whitish scaling (keratin) | Compact orthokeratotic hyperkeratosis |
| White circles | Acanthosis and hypergranulosis of infundibular epithelium, indicative of follicular invasion |
| Whitish structure within the circles | Dilated follicular infundibulum with keratin plug |
| Whitish lines and structureless areas | Keratinizing tumor cell masses |
| Red globules within white areas | Microhemorrhage (blood spots) within the keratin |
The role of dermoscopy in keratoacanthoma appears to be mostly limited to differentiate it, together with SCC, from other raised non-pigmented lesions based on findings like keratin, white circles, and blood spots. Although not absolutely specific to SCC and keratoacanthoma, the significance of these findings lies in the fact that they were found to occur much more frequently in these two lesions. Hence, their presence in any raised non-pigmented skin lesion should prompt a biopsy. Although central keratin was shown to be more common in keratoacanthoma than in SCC, unequivocal differentiation between the two is not possible with dermoscopy alone and requires correlation with clinical and histological findings.[3]
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Soyer HP, Rigel DS, Wurm EMT. Actinic keratosis, basal cell carcinoma and squamous cell carcinoma. In: Bolognia JL, Jorizzo JL, Schaffer JV, editors. Dermatology. 3rd ed. London: Elsevier; 2012. pp. 1773–93. [Google Scholar]
- 2.Weedon D. Tumors of the epidermis. In: Weedon D, editor. Weedon's Skin Pathology. 3rd ed. Edinburgh: Churchill Livingstone Elsevier; 2010. pp. 668–708. [Google Scholar]
- 3.Rosendahl C, Cameron A, Argenziano G, Zalaudek I, Tschandl P, Kittler H. Dermoscopy of squamous cell carcinoma and keratoacanthoma. Arch Dermatol. 2012;148:1386–92. doi: 10.1001/archdermatol.2012.2974. [DOI] [PubMed] [Google Scholar]