

Abstract
Background
Lidocaine is a local anaesthetic that is sometimes used on the skin to treat neuropathic pain.
Objectives
To assess the analgesic efficacy of topical lidocaine for chronic neuropathic pain in adults, and to assess the associated adverse events.
Search methods
We searched CENTRAL, MEDLINE, and EMBASE from inception to 1 July 2014, together with the reference lists of retrieved papers and other reviews. We also searched ClinicalTrials.gov and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) search portal to identify additional published or unpublished data.
Selection criteria
We included randomised, double‐blind studies of at least two weeks' duration comparing any formulation of topical lidocaine with placebo or another active treatment in chronic neuropathic pain. Participants were adults aged 18 and over. We included only full journal publication articles.
Data collection and analysis
Two review authors independently extracted efficacy and adverse event data, and examined issues of study quality. We performed analysis using three tiers of evidence. First tier evidence derived from data meeting current best standards and subject to minimal risk of bias (outcome equivalent to substantial pain intensity reduction, intention‐to‐treat analysis without imputation for dropouts; at least 200 participants in the comparison, 8 to 12 weeks' duration, parallel design); second tier evidence from data that failed to meet one or more of these criteria and that we considered at some risk of bias but with adequate numbers in the comparison; and third tier evidence from data involving small numbers of participants that we considered very likely to be biased or used outcomes of limited clinical utility, or both.
Main results
We included 12 studies (508 participants) in comparisons with placebo or an active control. Six studies enrolled participants with moderate or severe postherpetic neuralgia, and the remaining studies enrolled different, or mixed, neuropathic pain conditions, including trigeminal neuralgia and postsurgical or post‐traumatic neuralgia. Four different formulations were used: 5% medicated patch, 5% cream, 5% gel, and 8% spray. Most studies used a cross‐over design, and two used a parallel‐group design. Two studies used enriched enrolment with randomised withdrawal. Seven studies used multiple doses, with one to four‐week treatment periods, and five used single applications. We judged all of the studies at high risk of bias because of small size or incomplete outcome assessment, or both.
There was no first or second tier evidence, and no pooling of data was possible for efficacy outcomes. Only one multiple‐dose study reported our primary outcome of participants with ≥ 50% or ≥ 30% pain intensity reduction. Three single‐dose studies reported participants who were pain‐free at a particular time point, or had a 2‐point (of 10) reduction in pain intensity. The two enriched enrolment, randomised withdrawal studies reported time to loss of efficacy. In all but one study, third tier (very low quality) evidence indicated that lidocaine was better than placebo for some measure of pain relief. Pooling multiple‐dose studies across conditions demonstrated no clear evidence of an effect of lidocaine on the incidence of adverse events or withdrawals, but there were few events and the withdrawal phase of enriched enrolment designs is not suitable to assess the true impact of adverse events (very low quality evidence).
Authors' conclusions
This review found no evidence from good quality randomised controlled studies to support the use of topical lidocaine to treat neuropathic pain, although individual studies indicated that it was effective for relief of pain. Clinical experience also supports efficacy in some patients. Several large ongoing studies, of adequate duration, with clinically useful outcomes should provide more robust conclusions about both efficacy and harm.
Plain language summary
Topical lidocaine for neuropathic pain in adults
Neuropathic pain is pain coming from damaged nerves. It differs from pain messages carried along healthy nerves from damaged tissue (a fall, or cut, or arthritic knee). Neuropathic pain is treated by different medicines than pain from damaged tissue. Medicines like paracetamol or ibuprofen are usually not effective in neuropathic pain, while medicines that are sometimes used to treat epilepsy or depression can be very effective in some people with neuropathic pain. Other possible treatments include the use of local anaesthetic applied to the skin.
Lidocaine is a local anaesthetic. It is available in plasters (or patches), sprays, and creams, as topical lidocaine. These contain high concentrations of lidocaine because it crosses the skin poorly. Treatment with plasters usually involves applying one, two, or three plasters for up to 12 hours a day.
In July 2014 we performed searches to look for clinical trials where topical lidocaine was used to treat neuropathic pain. We found 12 small studies of modest quality that tested topical lidocaine against topical placebo for a number of weeks. One study also tested a cream containing amitriptyline, which is an antidepressant. The 508 people in the studies had different types of neuropathic pain, with pain after herpes zoster infection the most common.
There was some indication that topical lidocaine was beneficial in these studies (very low quality evidence). There was no clear evidence of an effect of lidocaine on the incidence of adverse events or withdrawals (very low quality evidence).
A number of studies of topical lidocaine in neuropathic pain are ongoing. Several are large and of long duration. They will be of great help in working out the benefits of topical lidocaine when they are completed and results can be incorporated in this review.
Summary of findings
for the main comparison.
| Topical lidocaine (5% patch) compared with placebo for mixed peripheral neuropathic pain conditions | ||||||
|
Patient or population: adults with peripheral neuropathic pain conditions Settings: community Intervention: topical lidocaine (5% patch), multiple applications Comparison: placebo | ||||||
| Outcomes | Outcome with comparator (placebo) | Outcome with intervention | RR, NNH (95% CI) | No of participants and studies | Quality of the evidence (GRADE) | Comments |
| At least 50% reduction in pain or equivalent | 3/40 (ITT 3/58) | 12/40 (ITT 12/58) | Not calculated | 58 participants 1 study |
Very low | Small numbers of participants in 1 study, cross‐over design, 2‐week duration |
| "Moderate" benefit At least 30% reduction in pain |
3/40 (ITT 3/58) | 16/40 (ITT 16/58) | Not calculated | 58 participants 1 study |
Very low | Small numbers of participants in 1 study, cross‐over design, 2‐week duration |
| Patient Global Impression of Change much or very much improved | No data | |||||
| Adverse event withdrawals | 2/174 | 12/263 during open‐label treatment in 1 study 3/175 during double‐blind treatment |
RR 1.24 (95% CI 0.34 to 4.55) NNH not calculated |
263 participants in open‐label phase, 1 study 210 participants in double‐blind treatment, 5 studies |
Very low | Small numbers of studies and participants, includes cross‐over studies, ≤ 2‐week duration |
| Serious adverse events | 6/263 during open‐label treatment in 1 study ‐ judged unrelated to study medication No other SAE reported |
Not calculated | 263 participants in open‐label phase, 1 study 210 participants in double‐blind treatment, 5 studies |
Very low | Small numbers of studies and participants, includes cross‐over studies, ≤ 2‐week duration | |
| Death | None reported | Not calculated | 210 participants 5 studies |
No data | Small numbers of studies and participants | |
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
CI: confidence interval; ITT: intention‐to‐treat; NNH: number needed to treat to harm; RR: risk ratio; SAE: serious adverse events
Background
This review is based on a template for Cochrane systematic reviews of drugs used to relieve neuropathic pain. The aim is for all reviews to use the same methods, based on new criteria for what constitutes reliable evidence in chronic pain (Moore 2010a; Appendix 1). An earlier review of topical lidocaine for postherpetic neuralgia (Khaliq 2007) has been withdrawn from The Cochrane Library because it was out of date as several newer studies had been published; postherpetic neuralgia will be covered within the broader scope of this review.
Description of the condition
The 2011 International Association of the Study of Pain definition of neuropathic pain is "pain caused by a lesion or disease of the somatosensory system" (Jensen 2011), based on an earlier consensus meeting (Treede 2008). Neuropathic pain may be caused by nerve damage, but is often followed by changes in the central nervous system (CNS) (Moisset 2007). It is complex (Apkarian 2011; Tracey 2011), and neuropathic pain features can be found in patients with joint pain (Soni 2013). Many people with these conditions are significantly disabled, with moderate or severe pain for many years.
Chronic painful conditions comprised five of the 11 top‐ranking conditions for years lived with disability in 2010 (Vos 2012), and are responsible for considerable loss of quality of life, employment, and increased health costs (Moore 2014a).
In primary care in the UK the incidences, per 100,000 person‐years observation, have been reported as 28 (95% confidence interval (CI) 27 to 30) for postherpetic neuralgia, 27 (95% CI 26 to 29) for trigeminal neuralgia, 0.8 (95% CI 0.6 to 1.1) for phantom limb pain and 21 (95% CI 20 to 22) for painful diabetic neuropathy (Hall 2008). Estimates vary between studies, often because of small numbers of cases. The incidence of trigeminal neuralgia has been estimated at 4 in 100,000 per year (Katusic 1991; Rappaport 1994), while more recently, a study of facial pain in the Netherlands found incidences per 100,000 person‐years of 12.6 for trigeminal neuralgia and 3.9 for postherpetic neuralgia (Koopman 2009). A systematic review of chronic pain demonstrated that some neuropathic pain conditions, such as painful diabetic neuropathy, can be more common, with prevalence rates up to 400 per 100,000 person‐years (McQuay 2007), illustrating how common the condition was as well as its chronicity. The prevalence of neuropathic pain was reported as being 3.3% in Austria (Gustorff 2008), 6.9% in France (Bouhassira 2008), as high as 8% in the UK (Torrance 2006), between 7% and 10% in a systematic review of epidemiological studies in the general population (van Hecke 2014), and about 7% in a systematic review of studies published since 2000 (Moore 2014a). Some forms of neuropathic pain, such as diabetic neuropathy and postsurgical chronic pain (which is often neuropathic in origin) are increasing (Hall 2008).
Neuropathic pain is known to be difficult to treat effectively, with only a minority of individuals experiencing a clinically relevant benefit from any one intervention. A multidisciplinary approach is now advocated, with pharmacological interventions being combined with physical or cognitive interventions, or both. Conventional analgesics are usually not effective. Some patients may derive some benefit from low concentration topical capsaicin, though evidence about benefits is uncertain (Derry 2012). High concentration topical capsaicin may benefit some patients with postherpetic neuralgia (Derry 2013). Treatment is more usually by so‐called unconventional analgesics such as antidepressants like duloxetine and amitriptyline (Lunn 2009; Moore 2012; Sultan 2008), or antiepileptics like gabapentin or pregabalin (Moore 2009; Moore 2011a). An overview of treatment guidelines points out some general similarities, but also differences in approach (O'Connor 2009). The proportion of patients who achieve worthwhile pain relief (typically at least 50% pain intensity reduction (Moore 2013a)) is small, generally 10% to 25% more than with placebo, with numbers needed to treat to benefit (NNTs) usually between 4 and 10 (Moore 2013b). Neuropathic pain is not particularly different from other chronic pain in regard to a small proportion of trial participants having a good response to treatment (Moore 2013b).
Description of the intervention
Topical medications are applied externally and are taken up through the skin. They exert their effects close to the site of application, and there is no substantial systemic uptake or distribution. This compares with transdermal application, where the medication is applied externally and is taken up through the skin, but relies on systemic distribution for its effect. Where drugs are applied to the skin using an adhesive patch, the patch may be referred to as a 'patch' or a 'plaster'. In this review we have used the term 'plaster' because this is the description given by the manufacturer of the product used most often in the studies we identified. However, some studies have used the term 'patch', and we have used this term where it relates specifically to what was reported in that study.
Lidocaine is a local anaesthetic. It can be injected for dental analgesia and minor surgery, or infiltrated into wounds, but can also provide surface anaesthesia when applied topically, for example as a medicated plaster, a gel, or a spray. Lidocaine is readily absorbed from mucous membranes and through damaged skin, and from injection sites, but absorption through intact skin is poor. To be clinically useful as a topical agent, lidocaine must be formulated with a carrier to facilitate transfer across the skin.
Creams, gels, foam sprays, and solutions containing lidocaine are most often used for short‐term analgesia, for example before painful medical procedures or to treat cuts, burns, and insect bites, but may also be used in chronic conditions. The concentration of lidocaine in these formulations is usually around 2% to 5% w/w.
To treat chronic pain, lidocaine is usually applied as a plaster. The medicated plaster used in a common product (Versatis®) is a white hydrogel plaster containing adhesive material, which is applied to a non‐woven polyethylene terephthalate backing and covered with a polyethylene terephthalate film release liner (EMC 2013). A single plaster measuring 10 cm x 14 cm contains 700 mg lidocaine (5% w/w), and up to three plasters can be applied daily, for up to 12 hours, leaving plaster‐free periods of at least 12 hours. Plasters may be cut to size if necessary, and hair should be removed with scissors (not shaved) before application. Steady state plasma concentrations are established within four days (EMC 2013; Mick 2012).
Lidocaine is a potent antiarrhythmic drug with a narrow therapeutic window, and high doses can also precipitate CNS disturbances, such as psychosis. At high concentration it can lead to death. The amount of lidocaine reaching the systemic circulation following plaster use is low (of the order of 3%) and well below therapeutic antiarrythmic concentrations or toxic concentrations in individuals with good cardiac, renal, and hepatic function (Campbell 2002). Lidocaine is extensively metabolised in the liver and excreted by the kidneys. Caution is required when treating patients with severe cardiac, renal, or hepatic impairment.
As with other topical applications, localised skin reactions to the plaster or carrier in the formulation may occur.
How the intervention might work
Lidocaine is a non‐selective, voltage‐gated sodium channel inhibitor, affecting both the generation and conduction of nerve impulses. It stabilises nerve membranes, reducing ectopic activity in damaged afferent pain receptors. Other effects on keratinocytes and immune cells, or activation of irritant receptors (TRPV1 and TRPA1), may also contribute to the analgesic effect of topical lidocaine (Sawynok 2014). Long‐term use may cause a loss of epidermal nerve fibres (Wehrfritz 2011).
Lidocaine does not cross intact skin well, and when applied as a plaster, with steady controlled release of the drug, the amount of lidocaine that penetrates is enough to cause analgesia, but not anaesthesia.
Why it is important to do this review
Topical lidocaine plasters have been approved as first or second line therapy for the treatment of postherpetic neuralgia in the US, Europe, UK, and many other countries, including Latin America and the Middle East. The plaster and other formulations are also used off‐label in clinical practice to treat other localised neuropathic pain conditions. It is important to review the evidence for both benefit and harm from topical lidocaine in all painful neuropathic conditions for which it is prescribed in order to make informed treatment choices.
The standards used to assess evidence in chronic pain trials have changed substantially, with particular attention being paid to trial duration, withdrawals, and statistical imputation following withdrawal, all of which can substantially alter estimates of efficacy. The most important change is the move from using average pain scores, or average change in pain scores, to the number of patients who have a large decrease in pain (by at least 50%) and who continue in treatment, ideally in trials of 8 to 12 week or longer. Pain intensity reduction of 50% or more has been shown to correlate with improvements in comorbid symptoms, function, and quality of life. These standards are set out in the reference guide for pain studies (Cochrane PaPaS Group 2011).
This Cochrane review will assess the evidence in ways that make both statistical and clinical sense, and will use developing criteria for what constitutes reliable evidence in chronic pain (Moore 2010a). Trials included and analysed will need to meet a minimum of reporting quality (blinding, randomisation), validity (duration, dose and timing, diagnosis, outcomes, etc) and size (ideally at least 500 participants in a comparison in which the NNT is four or above (Moore 1998)). This sets a high standard and marks a departure from how reviews were done previously.
Objectives
To assess the analgesic efficacy of topical lidocaine for chronic neuropathic pain in adults, and to assess the associated adverse events.
Methods
Criteria for considering studies for this review
Types of studies
We included studies if they were randomised controlled trials (RCTs) with assessment of participant outcomes following any duration of treatment, although the emphasis of the review was on studies with eight weeks of treatment or longer. We included only double‐blind studies in the review; we sought single‐blind and open cohort studies for completeness and mentioned these in the discussion. We required full journal publication, with the exception of online clinical trial results summaries of otherwise unpublished clinical trials and abstracts with sufficient data for analysis. We did not include short abstracts (usually meeting reports). We excluded studies that were non‐randomised, studies of experimental pain, case reports, and clinical observations.
Types of participants
We included adult participants aged 18 years and above. Participants could have one or more of a wide range of chronic neuropathic pain conditions including:
painful diabetic neuropathy;
postherpetic neuralgia;
trigeminal neuralgia;
phantom limb pain;
postoperative or traumatic neuropathic pain;
complex regional pain syndrome (CRPS) Type I and Type II;
cancer‐related neuropathy;
human immunodeficiency virus (HIV) neuropathy;
spinal cord injury.
We included studies of participants with more than one type of neuropathic pain; in such cases we planned to analyse results according to the primary condition. We excluded migraine and headache studies as they are the subject of another Cochrane review (Chronicle 2004).
Types of interventions
Lidocaine at any dose, formulated for topical application, and administered for the relief of neuropathic pain and compared to placebo or any active comparator.
Types of outcome measures
We anticipated that studies would use a variety of outcome measures, with the majority using standard subjective scales (numerical rating scale (NRS) or visual analogue scale (VAS)) for pain intensity or pain relief, or both. We were particularly interested in Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials (IMMPACT) definitions for moderate and substantial benefit in chronic pain studies (Dworkin 2008). These are defined as at least 30% pain relief over baseline (moderate), at least 50% pain relief over baseline (substantial), much or very much improved on the Patient Global Impression of Change (PGIC) (moderate), and very much improved on PGIC (substantial). These outcomes are different from those used in most earlier reviews using average pain scores (Khaliq 2007), concentrating as they do on dichotomous outcomes where pain responses do not follow a normal (Gaussian) distribution. People with chronic pain desire high levels of pain relief, ideally more than 50%, and with pain not worse than mild (Moore 2013a; O'Brien 2010).
We have included a 'Summary of findings' table, which includes outcomes of at least 50% and at least 30% pain intensity reduction, PGIC, adverse event withdrawals, serious adverse events, and death.
Primary outcomes
Patient‐reported pain relief of 30% or greater
Patient‐reported pain relief of 50% or greater
PGIC much or very much improved
PGIC very much improved
Secondary outcomes
Any pain‐related outcome indicating some improvement
Withdrawals due to lack of efficacy
Participants experiencing any adverse event
-
Participants experiencing any serious adverse event, including hypersensitivity reactions, cardiac events
Serious adverse events typically include any untoward medical occurrence or effect that at any dose results in death, is life‐threatening, requires hospitalisation or prolongation of existing hospitalisation, results in persistent or significant disability or incapacity, is a congenital anomaly or birth defect, is an 'important medical event' that may jeopardise the patient, or may require an intervention to prevent one of the above characteristics/consequences
Withdrawals due to adverse events
Specific adverse events, particularly local skin reactions
Search methods for identification of studies
Electronic searches
We searched the following databases:
the Cochrane Central Register of Controlled Trials (CENTRAL) (2014, Issue 6) (via The Cochrane Library);
MEDLINE (via Ovid) (1946 to 1 July 2014);
EMBASE (via Ovid) (1974 to 1 July 2014).
The search strategies for CENTRAL, MEDLINE, and EMBASE are shown in Appendix 2, Appendix 3, and Appendix 4 respectively.
Searching other resources
We reviewed the bibliographies of randomised trials identified and review articles, and searched two clinical trial databases (ClinicalTrials.gov (http://clinicaltrials.gov/) and the World Health Organization (WHO) International Clinical Trials Registry Platform (ICTRP) search portal (http://apps.who.int/trialsearch/)) to identify additional published or unpublished data. We did not contact investigators or study sponsors.
Data collection and analysis
The intention was to perform separate analyses according to particular neuropathic pain conditions for efficacy outcomes; we would perform analyses combining different neuropathic pain conditions for exploratory purposes only. For analyses of adverse events we planned to combine data from different conditions.
Selection of studies
We determined eligibility by reading the abstract of each study identified by the search. We eliminated studies that clearly did not satisfy the inclusion criteria, and we obtained full copies of the remaining studies; two review authors made the decisions. Two review authors read these studies independently and reached agreement by discussion. We did not anonymise the studies in any way before assessment. We have included a Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) flow chart (Moher 2009) (Figure 1).
1.
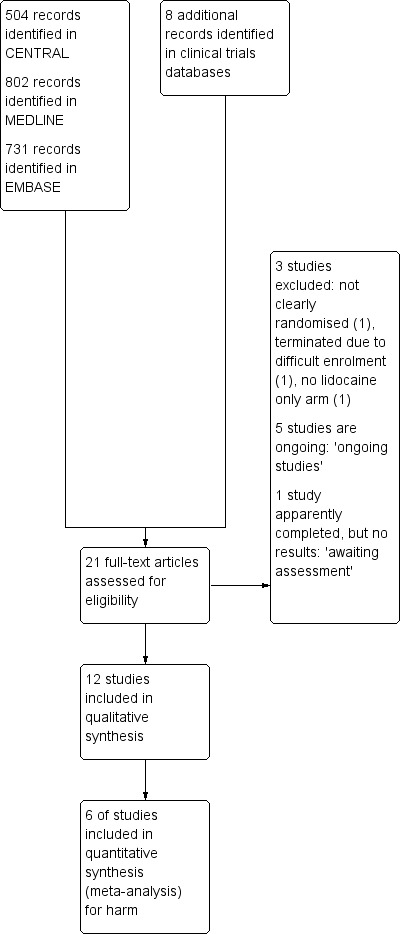
Study flow diagram.
Data extraction and management
Two review authors independently extracted data using a standard data extraction form and checked for agreement before entry into The Cochrane Collaboration's statistical software, Review Manager 2013, or any other analysis tool. We included information about the pain condition and number of participants treated, drug and dosing regimen, study design (placebo or active control), study duration and follow‐up, analgesic outcome measures and results, withdrawals, and adverse events (participants experiencing any adverse event, or serious adverse event).
Assessment of risk of bias in included studies
We used the Oxford Quality Score as the basis for inclusion, limiting inclusion to studies that were randomised and double‐blind as a minimum (Jadad 1996).
Two authors independently assessed the risk of bias for each study, using the criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011), and adapted from those used by the Cochrane Pregnancy and Childbirth Group, with any disagreements resolved by discussion.
We assessed the following for each study.
Random sequence generation (checking for possible selection bias). We assessed the method used to generate the allocation sequence as: low risk of bias (any truly random process, for example random number table; computer random number generator); unclear risk of bias (method used to generate sequence not clearly stated). We excluded studies using a non‐random process (for example, odd or even date of birth; hospital or clinic record number).
Allocation concealment (checking for possible selection bias). The method used to conceal allocation to interventions prior to assignment determines whether intervention allocation could have been foreseen in advance of, or during recruitment, or changed after assignment. We assessed the methods as: low risk of bias (for example, telephone or central randomisation; consecutively numbered, sealed, opaque envelopes); unclear risk of bias (method not clearly stated). We excluded studies that do not conceal allocation (for example, open list).
Blinding of outcome assessment (checking for possible detection bias). We assessed the methods used to blind study participants and outcome assessors from knowledge of which intervention a participant received. We assessed the methods as: low risk of bias (study stated that it was blinded and described the method used to achieve blinding, for example, identical tablets; matched in appearance and smell); unclear risk of bias (study stated that it was blinded but did not provide an adequate description of how it was achieved). We excluded studies that were not double‐blind.
Incomplete outcome data (checking for possible attrition bias due to the amount, nature, and handling of incomplete outcome data). We assessed the methods used to deal with incomplete data as: low risk (< 10% of participants did not complete the study and/or used 'baseline observation carried forward' analysis); unclear risk of bias (used 'last observation carried forward' analysis); high risk of bias (used 'completer' analysis).
Size of study (checking for possible biases confounded by small size). We assessed studies as being at low risk of bias (≥ 200 participants per treatment arm); unclear risk of bias (50 to 199 participants per treatment arm); high risk of bias (< 50 participants per treatment arm).
Measures of treatment effect
We planned to calculate NNTs as the reciprocal of the absolute risk reduction (ARR) (McQuay 1998). For unwanted effects, the NNT becomes the number needed to treat to harm (NNH) and is calculated in the same manner. We used dichotomous data to calculate risk ratio (RR) with 95% CIs using a fixed‐effect model unless significant statistical heterogeneity was found (Data synthesis). Continuous data were not used in analyses.
Unit of analysis issues
The unit of randomisation was the individual participant. We would split the control treatment arm between active treatment arms in a single study if the active treatment arms were not combined for analysis.
We included cross‐over studies and planned to use only data from the first period, where available. Where only combined data for both periods were reported we treated the study as if it was a parallel study, drawing attention to the potential bias that this confers, and interpreting the results accordingly.
Dealing with missing data
We planned to use intention‐to‐treat (ITT) analysis where the ITT population consists of participants who were randomised, took at least one dose of the assigned study medication, and provided at least one post‐baseline assessment. Missing participants were assigned zero improvement where possible.
Assessment of heterogeneity
We planned to deal with clinical heterogeneity by combining studies that examined similar conditions for efficacy analyses. We assessed statistical heterogeneity visually and with the use of the I2 statistic (L'Abbé 1987).
Assessment of reporting biases
The aim of this review was to use dichotomous data of known utility (Moore 2010c). The review did not depend on what authors of the original studies chose to report or not, though clearly difficulties arose in studies failing to report any dichotomous results. We planned to extract and use continuous data, which probably poorly reflect efficacy and utility, if useful for illustrative purposes only.
We planned to assess publication bias using a method designed to detect the amount of unpublished data with a null effect required to make any result clinically irrelevant (usually taken to mean a NNT of 10 or higher) (Moore 2008).
Data synthesis
We planned to use a fixed‐effect model for meta‐analysis, and would use a random‐effects model only if there was significant clinical heterogeneity and it was considered appropriate to combine studies.
We planned to analyse data for each painful condition in three tiers, according to outcome and freedom from known sources of bias.
The first tier would use data meeting current best standards, where studies reported the outcome of at least 50% pain intensity reduction over baseline (or its equivalent), without the use of last observation carried forward (LOCF) or other imputation method for dropouts, reported an ITT analysis, lasted eight or more weeks, had a parallel‐group design, and had at least 200 participants (preferably at least 400) in the comparison (Moore 1998; Moore 2010a; Moore 2012). These top‐tier results would be reported first.
The second tier would use data from at least 200 participants but where one or more of the above conditions were not met (for example reporting at least 30% pain intensity reduction, using LOCF or a completer analysis, or lasting four to eight weeks).
The third tier of evidence relates to data from fewer than 200 participants, or where there were expected to be significant problems because, for example, of very short duration studies of less than four weeks, where there was major heterogeneity between studies, or where there were shortcomings in allocation concealment, attrition, or incomplete outcome data. For this third tier of evidence, no data synthesis is reasonable, and may be misleading, but an indication of beneficial effects might be possible.
Subgroup analysis and investigation of heterogeneity
We planned all analyses to be according to individual painful conditions, because placebo response rates with the same outcome can vary between conditions, as can the drug‐specific effects (Moore 2009).
We would have carried out subgroup analysis for different topical formulations if there had been sufficient data.
Sensitivity analysis
We would have carried out sensitivity analysis for duration of study if there had been sufficient data.
Results
Description of studies
Results of the search
Searches of CENTRAL, MEDLINE, and EMBASE identified 504, 731, and 802 reports, and a further eight reports were identified in clinical trials databases. After screening titles and abstracts, we considered 21 reports potentially relevant and examined them in full (Figure 1).
We identified five studies that are ongoing (EudraCT 2009‐015415‐41; EudraCT 2012‐000347‐28; EudraCT 2012‐003077‐26; NCT00686127; NCT01752322), and details can be found in the Characteristics of ongoing studies table. The clinical trial reports indicate that all five studies satisfy the inclusion criteria for this review. Three of these studies plan to enrol ≥ 200 participants in parallel groups, with treatment for 12 weeks; these studies will significantly add to the body of evidence for topical lidocaine in neuropathic pain.
We identified one other study that is apparently completed, but for which there are no study results (NCT00904202). This five‐week, randomised, double‐dummy, parallel‐group study (62 participants) compared topical lidocaine plasters with oral gabapentin and placebo.
Included studies
We included 12 studies, with 508 participants, in comparisons with placebo or an active control (Binder 2009; Bischoff 2013; Cheville 2009; Galer 1999; Galer 2002; Ho 2008; Kanai 2006; Kanai 2009a; Kanai 2009b; Meier 2003; Rowbotham 1995; Rowbotham 1996). Galer 2002 was a full publication of a subset of participants from a study first published as a conference abstract.
Six studies enrolled participants with postherpetic neuralgia (Binder 2009; Galer 1999; Galer 2002; Kanai 2009a; Rowbotham 1995; Rowbotham 1996), while single studies enrolled participants with inguinal postherniorrhaphy pain (Bischoff 2013), postsurgical pain (mainly due to breast or lung cancer) (Cheville 2009), mixed peripheral neuropathic pains (postherpetic neuralgia, postsurgical neuropathic pain, peripheral neuropathy (Ho 2008), and mostly postherpetic neuropathy, postsurgical neuralgia (Meier 2003)), trigeminal neuralgia (Kanai 2009b), and post‐traumatic peripheral neuropathy (mainly following plastic surgery, thoracotomy, contused wound) (Kanai 2009b). Study size ranged from 21 to 96 participants.
The mean age of participants in the studies was 57 to 77 years (age range 20 to 90 years), and all studies included both men and women. Exclusion criteria included causes of pain other than that specified, hypersensitivity to lidocaine or amide local anaesthetics or the vehicle ingredients, inflamed or injured skin at the application site, pregnancy or lactation, and severe terminal illness or other condition that would interfere with the study. Baseline pain was moderate or severe. Pain was reported as having been present for at least three months in all studies except two (Galer 2002; Rowbotham 1995), which had inclusion criteria of pain for at least one month, but did not report the actual duration in included participants. It is likely that the majority of participants in these studies had experienced pain for at least three months (ie chronic pain), so we decided to include them with an intention to carry out a sensitivity analysis.
All studies were placebo‐controlled (plaster, cream, or gel without active ingredient, or saline spray), and one included an active treatment arm using amitriptyline 5% cream (Ho 2008). Two studies used a parallel‐group design (Binder 2009 for the randomised withdrawal phase of an enriched enrolment, randomised withdrawal study; Galer 2002), and the remainder used a cross‐over design. Studies using cross‐over designs usually had a washout period between treatment phases of between ≥ 3 and 14 days, sometimes specifying that pain had to return to ≥ 75% of pretreatment level before starting the next phase. There was no washout specified in Cheville 2009 and Galer 1999. Two studies used an enriched enrolment, randomised withdrawal design. Binder 2009 had an open‐label phase to select responders, then randomised to either continued treatment or placebo. Galer 1999 enriched for response to lidocaine at recruitment, then used a cross‐over design for continued treatment or placebo.
Studies generally allowed continued use of stable oral analgesics, but all topical medications were discontinued. In three single‐dose studies all conventional analgesics were discontinued at least 12 hours before treatment and resumed in the event of treatment failure, or when pain returned.
Excluded studies
We excluded three studies. One did not state that it was randomised (Tajti 1999), one did not use a lidocaine only treatment arm (NCT00609323), and one was terminated due to difficult enrolment and reported no results (NCT01155986).
Risk of bias in included studies
Comments on potential biases in individual studies are reported in the 'Risk of bias' section of the Characteristics of included studies table. The findings are displayed in Figure 2 and Figure 3; we undertook no sensitivity analysis. The greatest risk of bias came from small study size, which affected all included studies.
2.
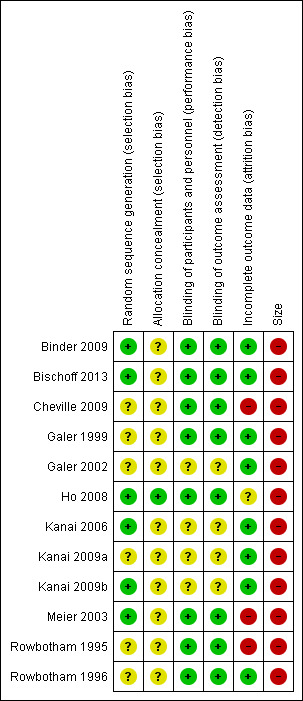
'Risk of bias' summary: review authors' judgements about each risk of bias item for each included study.
3.
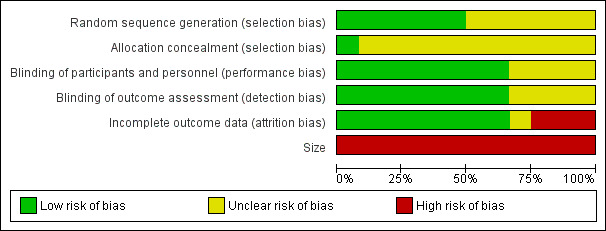
'Risk of bias' graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
Allocation
All the studies were randomised and half adequately described the method used to generate the random sequence. Only one study adequately described the method used to conceal allocation of the sequence (Ho 2008).
Blinding
All studies were double‐blind, but four did not adequately report the method used to maintain the blinding (Galer 2002; Kanai 2006; Kanai 2009a; Kanai 2009b).
Incomplete outcome data
We judged eight studies at low risk from incomplete outcome reporting. We judged one study at unclear risk due to a withdrawal rate ≥ 10% for each treatment without any mention of imputation method (Ho 2008). We judged three studies at high risk: Cheville 2009 had a withdrawal rate ≥ 10%, and carried out different imputations for missing data but did not report the results, while Meier 2003 and Rowbotham 1995 had withdrawal rates > 10% and reported completer analyses.
Other potential sources of bias
Eleven of the included studies had treatment groups with fewer than 50 participants and we judged them at high risk for this item. One study had more than 50 participants per treatment arm (58). No study had 200 or more participants per treatment arm (low risk for this item).
Effects of interventions
See: Table 1
There was no first or second tier evidence of efficacy. We downgraded the evidence primarily because of the short duration of the studies, small numbers of participants in comparisons, reporting of results only for participants who completed cross‐over studies (completer analyses), and lack of desirable primary outcomes.
Third tier evidence
Efficacy
Postherpetic neuralgia
Two studies in postherpetic neuralgia used a randomised withdrawal design.
Binder 2009 enrolled participants into an open‐label treatment phase and responders (at least moderate relief during regular use and increase in pain when plasters not worn) were then randomised to continue treatment or switched to placebo. Of the 263 participants enrolled in the open‐label phase, 71 (27%) were responders. The primary outcome in the withdrawal phase was time to exit, defined as ≥ 2‐point reduction in pain relief from randomisation on two consecutive days. The median time to exit was 13.5 days (2 to 14) with lidocaine and 9.0 days (1 to 14) with placebo. Secondary endpoints using daily and weekly pain intensity and pain relief showed a worsening of these measures in those who switched to placebo.
Galer 1999 enrolled participants from the open‐label compassionate use protocol (US FDA approved) who had previous regular use of lidocaine plasters for at least one month and were responders (as above). Participants were randomised to continue treatment or placebo in a cross‐over design. Median time to exit (as above) was greater than 14 days with lidocaine and 3.8 days with placebo. "A lot" or "complete" relief was reported on at least 5 out of 14 days in 18/32 participants with lidocaine and 6/32 with placebo.
There were four other studies in postherpetic neuralgia.
Galer 2002, in a three‐week parallel study, reported on a subset of 96 participants who satisfied the inclusion criteria using the Neuropathic Pain Scale (NPS) criteria and excluded those who had missing baseline or final visit NPS scores. Composite NPS score reductions were consistently greater in the lidocaine group than the placebo group (for example, change in NPS 10: lidocaine 15.3 (SD 17.9), placebo 7.7 (SD 14.2)).
Kanai 2009a used single applications of lidocaine 8% or saline spray in a cross‐over study. Fifteen minutes after treatment, 9/24 participants reported total pain relief with lidocaine and 0/24 with placebo, while 10/24 reported > 2‐point reduction in pain with lidocaine and 0/24 with placebo. Thirty minutes after treatment, 18/24 participants reported that pain was at least moderately better and lasted the full length of the observation with lidocaine and 1/24 with placebo. The median persistence of effect with lidocaine was 4.5 hours (range 2 to 24) and < 2 hours with placebo (one participant).
Rowbotham 1995 used single applications of lidocaine 5% gel or placebo gel in a cross‐over study, and reported on participants who completed all phases of the cross‐over (39/47). In participants treating painful areas on the head or neck, there were no consistent differences between lidocaine applied to the painful area, lidocaine applied to a remote area (placebo to painful area), or placebo. In participants treating painful areas on the torso or limbs, the mean pain intensity scores decreased in all groups initially, but this was maintained only in those treating the painful area with lidocaine.
Rowbotham 1996 used single applications of lidocaine 5% plaster or placebo plaster in a cross‐over study. Mean pain intensity and pain relief scores were better with lidocaine than with placebo or no treatment (not blinded). At four hours and six hours 7/35 participants had 'moderate' or 'a lot' of relief with lidocaine, and 3/35 had 'a lot' or 'complete' relief, using a 6‐point scale.
Other neuropathic pain conditions
The remaining studies investigated different types of neuropathic pain conditions, or mixed conditions.
Bischoff 2013 enrolled 21 participants with severe unilateral persistent inguinal postherniorrhaphy pain in a cross‐over study with two‐week treatment periods comparing topical lidocaine 5% plaster with placebo. Undefined 'pain relief' was reported in 8/21 participants with topical lidocaine, and 2/21 with placebo.
Cheville 2009 enrolled 28 participants with persistent pain with neuropathic features following surgery for cancer in a cross‐over study with four‐week treatment periods comparing topical lidocaine 5% plaster with placebo. Various scales were used to measure pain, together with interference, mood, and quality of life. Group mean data showed no difference between topical lidocaine and placebo. The study was terminated early due to slow recruitment.
Ho 2008 enrolled 35 participants with postsurgical neuropathic pain, postherpetic neuralgia, and diabetic neuropathy with allodynia or hyperalgesia, in a cross‐over study with one‐week treatment periods comparing topical lidocaine 5% cream with amitriptyline 5% cream and placebo. Pain intensity was reduced more compared with baseline by lidocaine than by amitriptyline or placebo. Patient satisfaction was rated as "good" or "excellent" following washout at the end of each treatment phase by 2/28 (ITT 2/35) participants with lidocaine, 5/30 with amitriptyline (ITT 5/35), and 7/27 (ITT 7/35) with placebo.
Kanai 2006 enrolled 25 participants with trigeminal neuralgia in a single‐dose cross‐over study of lidocaine 8% spray compared with placebo (saline spray). After 15 minutes, 10/25 participants were pain‐free with lidocaine compared with 0/25 with placebo, and 24/25 had pain reduced by ≥ 2/10 with lidocaine compared with 3/25 with placebo. The effect of lidocaine, where present, persisted for a median of 4.3 hours (range 0.5 to 24).
Kanai 2009b enrolled 31 participants with post‐traumatic peripheral neuropathy (caused by surgery or injury) in a single‐dose cross‐over study of lidocaine 8% spray compared with placebo (saline spray). After 15 minutes, 5/31 participants were pain‐free with lidocaine compared with 0/25 with placebo, and 22/31 had pain reduced by > 2/10 with lidocaine compared with 8/31 with placebo. In those with pain relief, the effect persisted for a median of five hours (range 2 to 60) with lidocaine, and < 2 hours (three participants) with placebo. A patient global evaluation reported 27/31 participants who were at least moderately better and with relief lasting the full length of the observation (probably 30 minutes) compared with 3/31 with placebo.
Meier 2003 enrolled 58 participants with peripheral neuropathic pain syndromes in a cross‐over study with two‐week treatment periods comparing topical lidocaine 5% plaster with placebo. Pain intensity was reduced by ≥ 50% in 12/40 (ITT 12/58) participants with lidocaine and 3/40 (ITT 3/58) with placebo, and by ≥ 30% in 16/40 (ITT 16/58) with lidocaine and 3/40 (ITT 3/58) with placebo.
Adverse events
Adverse events were inconsistently reported, but were mostly transient local effects of mild or moderate intensity, and did not differ between lidocaine and placebo groups. For those using patches, events were described as local skin reactions, erythema, application site reactions, rash, pruritus, and skin reddening. For creams they were described as itching, numbness, tingling, and burning, while for the spray, they were described as local irritation, and bitter taste or numbness of the throat.
Any adverse event
Only two studies reported this outcome for all treatment groups. Ho 2008 reported 10/35 participants experiencing any adverse event with lidocaine cream, 7/35 with amitriptyline cream, and 6/35 with placebo cream. Meier 2003 reported 20/58 participants experiencing any adverse event with lidocaine plaster and 17/58 with placebo patch.
Serious adverse events
The only serious adverse events reported were in the open‐label phase of Binder 2009, where there were six serious events, all judged unrelated to study medication. No deaths were reported.
Withdrawals
All cause withdrawals
Six studies provided data for this outcome and we pooled them for analysis (Binder 2009 (double‐blind phase); Bischoff 2013; Cheville 2009; Galer 1999; Ho 2008; Meier 2003). None of the cross‐over studies provided data for the first treatment period only.
Combining the studies across conditions, 32/210 (15%) of participants withdrew with topical lidocaine, and 37/209 (18%) with placebo. The RR did not reach statistical significance (RR 0.86, 95% CI 0.57 to 1.3), and the NNH was not calculated (Analysis 1.1).
1.1. Analysis.
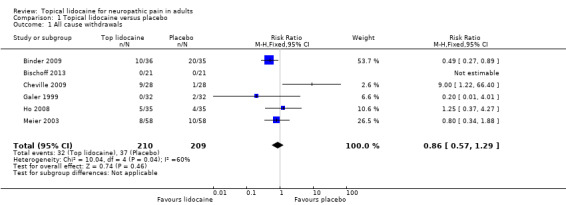
Comparison 1 Topical lidocaine versus placebo, Outcome 1 All cause withdrawals.
Galer 2002 did not provide any information about withdrawals. Of the single‐dose studies, the three using single doses of lidocaine 8% spray reported no withdrawals (Kanai 2006; Kanai 2009a; Kanai 2009b); we have not included these in the pooled analysis because they are not comparable with studies lasting one week or longer. The two using single applications of the lidocaine 5% patch did not report fully by treatment arm (Rowbotham 1995; Rowbotham 1996).
Lack of efficacy withdrawals
Four studies provided usable data for this outcome (Binder 2009 (double‐blind phase); Bischoff 2013; Galer 1999; Meier 2003). None of the cross‐over studies provided data for the first treatment period only.
Combining the studies across conditions, 10/147 (6.8%) of participants withdrew due to lack of efficacy with topical lidocaine, and 18/146 (12%) with placebo. The RR did not reach statistical significance (RR 0.55, 95% CI 0.29 to 1.05), and we did not calculate the NNH (Analysis 1.2).
1.2. Analysis.
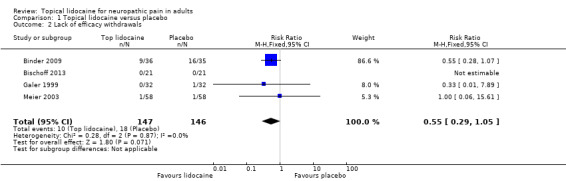
Comparison 1 Topical lidocaine versus placebo, Outcome 2 Lack of efficacy withdrawals.
Adverse event withdrawals
Five studies provided usable data for this outcome (Binder 2009 (double‐blind phase); Bischoff 2013; Cheville 2009; Galer 1999; Meier 2003). None of the cross‐over studies provided data for the first treatment period only.
Combining the studies across conditions, 3/175 (1.7%) of participants withdrew due to adverse events with topical lidocaine, and 2/174 (1.1%) with placebo. The RR did not reach statistical significance (RR 1.24, 95% CI 0.34 to 4.55)), and we did not calculate the NNH (Analysis 1.3).
1.3. Analysis.
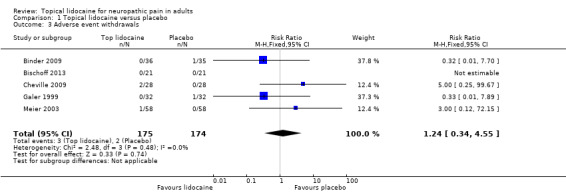
Comparison 1 Topical lidocaine versus placebo, Outcome 3 Adverse event withdrawals.
Binder 2009 reported that 12/263 participants withdrew during the open‐label phase due to adverse events, 10 of which were local skin reactions.
Death
No deaths were reported.
Discussion
Summary of main results
The review found 12 studies enrolling 508 participants with chronic neuropathic pain. In six of the studies, participants (280) had postherpetic neuropathy, while the reminder enrolled participants with various neuropathic pain conditions. Studies used different designs, including enriched enrolment, randomised withdrawal, parallel‐group, and cross‐over designs, and study duration ranged from a single dose to 12 weeks of continuous treatment. Three different formulations were studied: most used the 5% medicated plaster, but both 5% cream and 8% spray were also tested.
No first or second tier evidence was available. No pooling of data was possible, but third tier evidence in individual studies indicated some improvement in pain relief with topical lidocaine compared with placebo, although this was derived mainly from small, short duration studies where major bias is possible, and using various different outcome measures (see Appendix 1). Adverse events were mainly local application site reactions and were generally described as mild or moderate in intensity, and transient. There was no evidence of a significant increase in the frequency of adverse events with lidocaine compared with placebo, or of withdrawals for any reason, or because of lack of efficacy or adverse events.
Overall completeness and applicability of evidence
Although topical lidocaine was tested in a number of different neuropathic pain conditions, there were either diverse study designs or too few participants in any one condition to allow pooling of studies or to be confident about any effect, or size of effect. In addition, studies were of short duration, so cannot indicate whether any early response would be maintained in the longer term. This is important in chronic conditions. A long‐term, open‐label extension study in postherpetic neuralgia reports that the medicated plaster is safe when used for up to five years (including the initial study period), but of those who were satisfied with treatment and entered the extension phase, 10% discontinued due to lack of efficacy, and 9% due to adverse events (Sabatowski 2012).
We identified five ongoing studies, three of which plan to enrol between 222 to 600 participants with post‐traumatic or postoperative neuropathic pain in randomised, double‐blind, placebo‐controlled, parallel‐group studies of 12 weeks' duration. Although only one of these studies has stated that it will report the number of participants with ≥ 30% and ≥ 50% reduction in pain from baseline, all will measure pain intensity and pooled analysis may be possible. This amount of new data will overwhelm that from studies in this review.
Quality of the evidence
Reporting quality in the studies was generally poor by current standards. While all the studies were randomised and double‐blind, none provided data that met predefined criteria for first or second tier analysis. We judged all the included studies at high risk of bias due to small size and incomplete outcome data, or both.
The majority of studies used a cross‐over design and only one reported first period efficacy data separately (Cheville 2009), while one reported only on participants who provided data for both phases of treatment (Meier 2003).
Although in these small studies there was no difference between lidocaine and placebo for the incidence of adverse events and withdrawals, the studies were underpowered to show such an effect. In the two enriched studies, participants who could not tolerate lidocaine plasters were not included in the randomised phase.
Potential biases in the review process
We carried out a broad search for studies, and think it is unlikely that significant numbers of studies remain unknown to us. However, the ongoing studies we identified may provide a substantial amount of good quality data for post‐traumatic or postsurgical neuropathic pain.
The majority of studies used a cross‐over design. The degree of exaggeration of treatment effects in cross‐over trials compared to parallel‐group designs, as has been seen in some circumstances (Khan 1996), is unclear but in itself is unlikely to be the source of major bias (Elbourne 2002). However, all except one reported results for both treatment periods combined, and it was not always clear whether there was imputation for missing data.
Agreements and disagreements with other studies or reviews
There have been several reviews in the last five years of topical analgesics, or the lidocaine medicated plaster specifically, in various neuropathic pain conditions (Garnock‐Jones 2009; Mick 2012; Sawynok 2014; Snedecor 2014; Wolff 2010; Wolff 2011). These reviews have included all study designs, from case reports to randomised, double‐blind, placebo‐controlled trials. The consensus is that the medicated plaster provides relief from neuropathic pain that is superior to placebo, and that it is well tolerated; the majority of adverse events are mild to moderate local application site reactions that resolve when the plaster is removed.
These reviews are essentially in agreement with the findings of this review, but they include small amounts of data from studies at high risk of bias, both from study design (eg open‐label, complete enrichment) and method of analysis (eg completer analysis in cross‐over studies, last observation carried forward imputation). Confidence in their conclusions is therefore weakened.
An earlier Cochrane review of topical lidocaine for postherpetic neuralgia has been withdrawn because it is considered out of date since the standards now used to assess evidence in chronic pain trials have changed and more studies have been published (Khaliq 2007). That review included three studies, two of which are included using the same reports in this review (Rowbotham 1995; Rowbotham 1996). The third is a conference abstract, and we have included a full publication of a subset of participants from this study (Galer 2002). The review also excluded Galer 1999 because it had enriched enrolment and Meier 2003 because it was not limited to postherpetic neuralgia; both these studies are included in this review.
Authors' conclusions
Implications for practice.
Limited information from single studies, mainly in postherpetic neuralgia, indicates that topical lidocaine 5% plaster may be effective in treating neuropathic pain in a small number of patients, and is well tolerated, at least in the short term.
Implications for research.
With limited numbers of trials and participants, there is a clear need for large, good quality, long duration randomised studies in different neuropathic pain conditions. Several such trials are apparently being conducted and it would not be sensible to embark on a new clinical trial programme without knowledge of their results. An update of this review will be done when ongoing studies present data.
Lidocaine 8% spray may be useful for treating breakthrough pain, due to its apparent rapid onset and limited duration of action. This also represents a potentially useful research area.
Clinical practice indicates that lidocaine plasters can be helpful to carefully chosen patients with neuropathic pain limited to a defined area of superficial allodynia or hyperalgesia. For patients like this a study protocol could be generated to evaluate lidocaine plasters in individual patients. It would need to be designed carefully, with specified measurements, outcomes, and timing, and be part of a nationwide or regional assessment. There are exemplars for this in chronic pain, for example the successful assessment of tumour necrosis factor (TNF)‐antagonists for rheumatoid arthritis in clinical practice in the south of Sweden (Geborek 2002).
What's new
| Date | Event | Description |
|---|---|---|
| 29 May 2019 | Amended | Contact details updated. |
| 11 October 2017 | Review declared as stable | No new studies likely to change the conclusions are expected. |
History
Protocol first published: Issue 2, 2014 Review first published: Issue 7, 2014
| Date | Event | Description |
|---|---|---|
| 8 June 2016 | Review declared as stable | See Published notes. |
Notes
A restricted search in June 2016 did not identify any potentially relevant studies. Therefore, this review has now been stabilised following discussion with the authors and editors. If appropriate, we will update the review if new evidence likely to change the conclusions is published, or if standards change substantially which necessitate major revisions.
Acknowledgements
General institutional support is provided by the Oxford Pain Relief Trust.
CRG Funding Acknowledgement: The National Institute for Health Research (NIHR) is the largest single funder of the Cochrane Pain, Palliative and Supportive Care Review Group. Disclaimer: The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the NIHR, NHS or the Department of Health.
Appendices
Appendix 1. Methodological considerations for chronic pain
There have been several recent changes in how efficacy of conventional and unconventional treatments is assessed in chronic painful conditions. The outcomes are now better defined, particularly with new criteria of what constitutes moderate or substantial benefit (Dworkin 2008); older trials may only report participants with "any improvement". Newer trials tend to be larger, avoiding problems from the random play of chance. Newer trials also tend to be longer, up to 12 weeks, and longer trials provide a more rigorous and valid assessment of efficacy in chronic conditions. New standards have evolved for assessing efficacy in neuropathic pain, and we are now applying stricter criteria for inclusion of trials and assessment of outcomes, and are more aware of problems that may affect our overall assessment. To summarise, these are some of the recent insights that must be considered in this new review:
Pain results tend to have a U‐shaped distribution rather than a bell‐shaped distribution. This is true in acute pain (Moore 2011b; Moore 2011c), back pain (Moore 2010d), arthritis (Moore 2010b), as well as in fibromyalgia (Straube 2010); in all cases average results usually describe the experience of almost no‐one in the trial. Data expressed as averages are potentially misleading, unless they can be proven to be suitable.
As a consequence, we have to depend on dichotomous results (the individual either has or does not have the outcome) usually from pain changes or patient global assessments. The IMMPACT group has helped with their definitions of minimal, moderate, and substantial improvement (Dworkin 2008). In arthritis, trials shorter than 12 weeks, and especially those shorter than eight weeks, overestimate the effect of treatment (Moore 2010b); the effect is particularly strong for less effective analgesics, and this may also be relevant in neuropathic‐type pain.
The proportion of patients with at least moderate benefit can be small, even with an effective medicine, falling from 60% with an effective medicine in arthritis, to 30% in fibromyalgia (Moore 2009; Moore 2010b; Moore 2013b; Moore 2014b; Straube 2008; Sultan 2008). A Cochrane review of pregabalin in neuropathic pain and fibromyalgia demonstrated different response rates for different types of chronic pain (higher in diabetic neuropathy and postherpetic neuralgia and lower in central pain and fibromyalgia) (Moore 2009). This indicates that different neuropathic pain conditions should be treated separately from one another, and that pooling should not be done unless there are good grounds for doing so.
Individual patient analyses and other evidence indicate that patients who get good pain relief (moderate or better) have major benefits in many other outcomes, affecting quality of life in a significant way (Moore 2010c; Moore 2014a).
Appendix 2. Search strategy for CENTRAL
MESH DESCRIPTOR lidocaine EXPLODE ALL TREES (3655)
(lidocaine or Lidocain or Lidocaina or Lidocainum or Lidokaiini or Lidokain or Lidokaina or Lidokainas orLignocaina or Lignocaine):it,ab,kw (6406)
1 or 2 (6406)
MESH DESCRIPTOR Administration, Topical EXPLODE ALL TREES (11902)
topical*:it,ab,kw (15968)
4 or 5 (21760)
MESH DESCRIPTOR Neuralgia EXPLODE ALL TREES (565)
MESH DESCRIPTOR pain EXPLODE ALL TREES (28433)
((pain* or discomfort*) adj10 (central or complex or myofasci* or nerv* or neuralg* or neuropath*)):ti,ab,kw (2572)
((neur* or nerv*) adj6 (compress* or damag*)):ti,ab,kw (509)
7 or 8 or 9 or 10 (30133)
4 and 6 and 11 (504)
Appendix 3. Search strategy for MEDLINE via Ovid
Lidocaine/ (21225)
(lidocaine or Lidocain or Lidocaina or Lidocainum or Lidokaiini or Lidokain or Lidokaina or Lidokainas orLignocaina or Lignocaine).mp. (26612)
1 or 2 (26612)
exp Administration, Topical/ (65413)
topical*.mp. (83967)
3 or 4 (113117)
exp Pain/ (296594)
exp Neuralgia/ (12582)
((pain* or discomfort*) adj10 (central or complex or myofasci* or nerv* or neuralg* or neuropath*)).mp. (38260)
((neur* or nerv*) adj6 (compress* or damag*)).mp. (46211)
or/7‐10 (351685)
randomized controlled trial.pt. (359493)
controlled clinical trial.pt. (86909)
randomized.ab. (260696)
placebo.ab. (141221)
drug therapy.fs. (1651531)
randomly.ab. (186387)
trial.ab. (268187)
groups.ab. 1203305)
or/12‐19 (3092194)
3 and 4 and 11 and 20 (802)
Appendix 4. Search strategy for EMBASE (via Ovid)
lidocaine/ (60509)
(lidocaine or Lidocain or Lidocaina or Lidocainum or Lidokaiini or Lidokain or Lidokaina or Lidokainas or Lignocaina or Lignocaine).mp. (64380)
1 or 2 (64380)
topical drug administration/ (70281)
topical*.mp. (811936)
4 or 5 (157119)
exp pain/ (811936)
exp neuralgia/ (72654)
((pain* or discomfort*) adj10 (central or complex or myofasci* or nerv* or neuralg* or neuropath*)).mp. (85575)
((neur* or nerv*) adj6 (compress* or damag*)).mp. (68768)
7 or 8 or 9 or 10 (877953)
crossover‐procedure/ (39839)
double‐blind procedure/ (122815)
randomized controlled trial/ (369173)
random* or factorial* or crossover* or cross over* or cross‐over* or placebo* or (doubl* adj blind*) or assign* or allocat*).tw. (1218207)
12 or 13 or 14 or 15 (1302892)
3 and 6 and 11 and 16 (731)
Appendix 5. Summary of outcomes in individual studies: efficacy
| Study | Treatment | Pain outcome | Other efficacy outcome |
| Binder 2009 | Open‐label (≥ 8 weeks): All participants treated with lidocaine 5% plaster Double‐blind (2 weeks): Lidocaine 5% plaster Placebo Up to 3 plasters applied for ≥ 12 h daily |
Open‐label:
≥ moderate PR = 51.7% = 137/263
≥ 50% PR = 25.9% = 68/263
≥ 30% PR = 39.5% = 104/263
Double‐blind: Median time to exit (≥ 2/6‐point reduction in PR from randomisation on 2 consecutive days) Lidocaine 13.5 days (2 to 14) Placebo 9.0 days (1 to 14) |
Open‐label: Responders experienced improvement in all QoL domains of SF‐36 Double‐blind: Participants switching to placebo experienced worsening of secondary endpoints of pain intensity and pain relief |
| Bischoff 2013 | Lidocaine 5% plaster Placebo plaster One plaster applied for 12 h daily Cross‐over, 2 x 2‐week treatment periods |
Participants experiencing undefined "pain relief"
Lidocaine 8/21 Placebo 2/21 No difference between participants with or without thermal hyposensitivity |
SPID (before/after each treatment period) Lidocaine 2.9 (95% CI ‐0.7 to 6.5) Placebo 0.7 (‐1.4 to 2.8) |
| Cheville 2009 | Lidocaine 5% plaster Placebo plaster Up to 3 plasters, left in place for up to 18 h, removed overnight Cross‐over, 2 x 4‐week treatment periods | Mean weekly PI (average pain) for first period: Lidocaine 4.4 (SD 2.1) Placebo 4.8 (1.7) Mean weekly PI (worst pain) for first period: Lidocaine 5.8 (2.7) Placebo 6.2 (1.9) |
PGIC recorded but not reported |
| Galer 1999 | Lidocaine 5% plaster Placebo plaster Up to 3 plasters applied for ≥ 12 h daily Cross‐over, 2 x 2‐week treatment periods |
Median time to exit (≥ 2/6‐point reduction in PR from randomisation on 2 consecutive days)
Lidocaine > 14 days
Placebo 3.8 days "A lot" or "complete" relief on ≥ 5 of 14 days: Lidocaine 18/32 Placebo 6/32 |
Preference: Lidocaine 25/32 Vehicle 3/32 No preference 4/32 |
| Galer 2002 | Lidocaine 5% plaster Vehicle plaster Parallel groups, 3‐week treatment period | No usable data | |
| Ho 2008 | Lidocaine 5% cream (50 mg/ml)
Amitriptyline 5% cream
Placebo cream 3 to 5 ml applied x 2 daily 3 x 1‐week treatment periods |
Participant satisfaction (poor, fair, good, excellent), good/excellent: Lidocaine 8/28 (not ITT) Amitriptyline 5/30 Placebo 7/27 | |
| Kanai 2006 | Lidocaine 8% spray, 2 x 0.1 ml) Placebo spray Sprayed into affected nostril Cross‐over, 2 x single dose | Pain‐free at 15 minutes:
Lidocaine 10/25
Placebo 0/25 PI VAS decreased by ≥ 2/10 at 15 minutes: Lidocaine 24/25 Placebo 3/25 |
Effect of lidocaine persisted for median duration of 4.3 h (0.5 to 24) |
| Kanai 2009a | Lidocaine 8% spray
Saline spray
To cover painful site (up to 30 sprays of 0.1 ml) Cross‐over, 2 x single dose |
Pain‐free at 15 minutes:
Lidocaine 9/24
Placebo 0/24 PI VAS decreased by > 2/10 at 15 minutes: Lidocaine 10/24 Placebo 0/24 |
Participant global evaluation, 4‐point scale at 30 minutes, ≥ moderately better with relief lasting full length of observation:
Lidocaine 18/24
Placebo 1/24 Median persistence of effect in participants with relief: Lidocaine 4.5 h (2 to 24) Placebo < 2 h (1 participant) |
| Kanai 2009b | Lidocaine 8% spray
Saline spray
To cover painful site (up to 30 sprays of 0.1 ml) Cross‐over, 2 x single dose |
Pain‐free at 15 minutes:
Lidocaine 5/31
Placebo 0/31 PI VAS decreased by > 2/10 at 15 minutes: Lidocaine 22/31 Placebo 8/31 |
Participant global evaluation, 4‐point scale at 30 minutes, ≥ moderately better with relief lasting full length of observation:
Lidocaine 27/31
Placebo 3/31 Median persistence of effect in participants with relief: Lidocaine 5 h (2 to 60) Placebo < 2 h (3 participants) |
| Meier 2003 | Lidocaine 5% plaster Vehicle plaster Up to 4 plasters applied to painful area for ≥ 12 h daily Cross‐over, 2 x 7‐day treatment periods | ≥ 50% pain reduction: Lidocaine 31% = 12/40 Placebo 8.1% = 3/40 ≥ 30% pain reduction: Lidocaine 41% = 16/40 Placebo 8.6% = 3/40 | |
| Rowbotham 1995 | Lidocaine 5% gel on painful area Lidocaine gel on contralateral area Vehicle gel on both areas Gel applied over painful area and over matching contralateral area. Each participant treated painful area with active, and contralateral with active, using matching placebo gel to maintain 2 areas treated each phase Cross‐over, 3 x single application | Head/neck participants: Mean PI VAS scores over 8 h did not differ between groups Torso/limb participants: Mean VAS scores over 24 h decreased in all groups early on, but maintained only in the active applied to painful area group ‐ different from placebo |
Some reduction in allodynia scores in the active applied to painful area group |
| Rowbotham 1996 | Lidocaine 5% plaster
Vehicle plaster
Up to 3 plasters applied to painful area for 12 h
2 x sessions with active plaster, 1 with placebo plaster, and 1 with no plasters Cross‐over, 3 x single application, 1 no application (not blinded) |
Mean PI VAS reduced with lidocaine compared with vehicle (4 to 12 h) or no treatment (0.5 to 12 h) | |
| h: hours; ITT: intention‐to‐treat; PGIC: Patient Global Evaluation of Change; PI: pain intensity; PR: pain relief; QoL: quality of life; SD; standard deviation; SF‐36: Short‐Form 36; SPID: summed pain intensity difference; VAS: visual analogue scale | |||
Appendix 6. Summary of results in individual studies: adverse events and withdrawals
| Study | Treatment | Adverse events | Withdrawals |
| Binder 2009 | Open‐label (≥ 8 weeks): All participants treated with lidocaine 5% plaster Double‐blind (2 weeks): Lidocaine 5% plaster Placebo Up to 3 plasters applied for ≥ 12 h daily |
Open‐label phase Any AE: 81/263 (34 drug related) Local skin AEs: 17/263 SAE: 6/263 (judged unrelated to medication) No deaths Double‐blind phase Any AE: Lidocaine 2/35 Placebo 1/35 |
Open‐label phase AE: 12/263 (10 local skin reactions) Double‐blind phase All cause: Lidocaine 10/35 Placebo 20/35 LoE: Lidocaine 9/36 Placebo 16/35 AE: Lidocaine 0/35 Placebo 1/35 One participant from each group lost to follow‐up |
| Bischoff 2013 | Lidocaine 5% plaster Placebo plaster One plaster applied for 12 h daily Cross‐over, 2 x 2‐week treatment periods |
One participant developed erythema in treated area, which resolved soon after completion | None |
| Cheville 2009 | Lidocaine 5% plaster Placebo plaster Up to 3 plasters, left in place for up to 18 h, removed overnight Cross‐over, 2 x 4‐week treatment periods | Mild or moderate Rash/desquamatisation, dizziness, fatigue, neuromotor most common in lidocaine group | Lidocaine/placebo: 7/14 (refused further treatment 3, AE 2, alternative treatment 1, other 1) Placebo/lidocaine: 3/14 (refused further treatment 2, other 1) Nine of 10 who withdrew did so while using lidocaine patches. Withdrawals more likely to have baseline pain ≥ 7/10 |
| Galer 1999 | Lidocaine 5% plaster Placebo plaster Up to 3 plasters applied for ≥ 12 h daily Cross‐over, 2 x 2‐week treatment periods |
Application site reaction: Lidocaine 9/32 Vehicle 11/32 No difference between treatments for events in ≥ 5% of participants All AEs mild or moderate. No SAE | Lidocaine 0/32 Vehicle 2/32 (increased pain + insomnia, and erythema) |
| Galer 2002 | Lidocaine 5% plaster Vehicle plaster Parallel groups, 3‐week treatment period | No data | No data |
| Ho 2008 | Lidocaine 5% cream (50 mg/ml)
Amitriptyline 5% cream
Placebo cream 3 ml to 5 ml applied x 2 daily 3 x 1‐week treatment periods |
Any AE: Lidocaine 21.9% = 10/35 Amitriptyline 18.8% = 7/35 Placebo 16.1% = 6/35 (denominator unclear) | All cause Lidocaine 5/35 Amitriptyline 5/35 Placebo 4/35 |
| Kanai 2006 | Lidocaine 8% spray, 2 x 0.1 ml) Placebo spray Sprayed into affected nostril Cross‐over, 2 x single dose | 15/25 with lidocaine: Local irritation (15), bitter taste/numbness of throat (1) AEs with placebo not specifically mentioned No SAE No difficulties with swallowing or talking | None |
| Kanai 2009a | Lidocaine 8% spray
Saline spray
To cover painful site (up to 30 sprays of 0.1 ml) Cross‐over, 2 x single dose |
None observed or reported | None |
| Kanai 2009b | Lidocaine 8% spray
Saline spray
To cover painful site (up to 30 sprays of 0.1 ml) Cross‐over, 2 x single dose |
Lidocaine ‐ 3 participants with mild, transient local irritation and 1 with local flare | None |
| Meier 2003 | Lidocaine 5% plaster Vehicle plaster Up to 4 plasters applied to painful area for ≥ 12 h daily Cross‐over, 2 x 7‐day treatment periods | Any AE: Lidocaine 20/58 Placebo 17/58 During washout phase 3 Nearly all (38/41) mild and local sensations Most common: rash and pruritus. No difference between groups | All cause: Lidocaine 8/58 Placebo 10/58 (denominator unclear) LoE: Lidocaine 1/58 Placebo 1/58 AE: Lidocaine 1/58 Placebo 0/58 Baseline pain did not return during washout: Lidocaine 5/28 Placebo 5/30 |
| Rowbotham 1995 | Lidocaine 5% gel on painful area Lidocaine gel on contralateral area Vehicle gel on both areas Gel applied over painful area and over matching contralateral area. Each participant treated painful area with active, and contralateral with active, using matching placebo gel to maintain 2 areas treated each phase Cross‐over, 3 x single application | Mild and transient reddening of skin was most common ‐ no difference between active gel and vehicle gel 29/47 had no reddening after any application | Incorrect diagnosis (1) Used topical agents (2) Skin redness after first session (placebo) (2) Worsening of pain following first session (lidocaine), without skin reaction (1) Did not complete 3 sessions within 6 weeks (1 due to prolonged relief from second session) (2) |
| Rowbotham 1996 | Lidocaine 5% plaster
Vehicle plaster
Up to 3 plasters applied to painful area for 12 h
2 x sessions with active plaster, 1 with placebo plaster, and 1 with no plasters Cross‐over, 3 x single application, 1 no application (not blinded) |
Bruising and pain on patch removal (on systemic steroids for asthma) (1) Mild, transient skin reddening (1 vehicle, 1 lidocaine) | One participant had severe depression that interfered with obtaining reliable ratings (lidocaine) |
| AE: adverse event; h: hours; LoE: lack of effect; SAE: serious adverse event | |||
Data and analyses
Comparison 1. Topical lidocaine versus placebo.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 All cause withdrawals | 6 | 419 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.86 [0.57, 1.29] |
| 2 Lack of efficacy withdrawals | 4 | 293 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.55 [0.29, 1.05] |
| 3 Adverse event withdrawals | 5 | 349 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.24 [0.34, 4.55] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Binder 2009.
| Methods | Multicentre, enriched enrolment, randomised withdrawal study. Eight‐week open‐label phase followed by randomisation of responders to 2‐week, double‐blind, placebo‐controlled phase Up to 3 medicated plasters (to cover affected area) applied for up to 12 h per day |
|
| Participants | Postherpetic neuralgia ≥ 3 months after rash healing, PI ≥ 4/10, age ≥ 50 years Responder: regular (≥ every second day) plaster use during 4 weeks before randomisation; ≥ moderate pain relief (6‐point VRS) during week before randomisation; mean daily PI ≥ 7/10 while wearing plaster during open‐label phase, and PI increased when plaster not worn N = 263 for open‐label phase M 112, F 151 Age 73 years (SD 8.5) Baseline pain intensity 5.9/10 N = 71 for double‐blind phase M 28, F 43 Mean age 72 years (SD 8.7) Baseline pain intensity 5.7/10 |
|
| Interventions | Double‐blind phase: Lidocaine 5% plaster (Versatis ®), n = 36 Placebo plaster, n = 35 Concomitant stable analgesic therapy allowed, except topical analgesics or additional lidocaine therapy |
|
| Outcomes | Time to exit from double‐blind phase due to lack of efficacy (≥ 2‐point decrease in PR (6‐point VRS) on 2 consecutive days of plaster application compared with mean in last week of open‐label treatment) Daily and weekly: PI: NRS, 0 to 10 PR: 6‐point VRS McGill Pain Questionnaire Additional assessments for sleep, quality of life, allodynia Adverse events |
|
| Notes | Oxford Quality Score: R = 2, DB = 2, W = 1. Total = 5/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | Plasters described as "medicated" and "placebo". Codes removed from computer systems and stored in sealed envelopes until database lock |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Plasters described as "medicated" and "placebo". Codes removed from computer systems and stored in sealed envelopes until database lock |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Full analysis set analysis, no imputation |
| Size | High risk | < 50 participants per treatment arm |
Bischoff 2013.
| Methods | Single‐centre, randomised, double‐blind, placebo‐controlled cross‐over study One plaster applied to groin area for 12 h, followed by plaster‐free interval of 12 h. Each treatment period lasted 14 days, separated by a 14‐day washout |
|
| Participants | Men with severe unilateral persistent inguinal postherniorrhaphy pain > 6 months, PI > 6/10, age ≥ 18 years. Subgroups: with thermal hyposensitivity (≥ 3 increased thermal thresholds) or without thermal hyposensitivity (≤ 2 increased, normal or decreased thermal thresholds) N = 21 Mean age 57 years (SD 13) Baseline pain intensity at rest 6/10 (4 to 7) |
|
| Interventions | Lidocaine 5% plaster (Versatis ®) Placebo plaster Concomitant analgesics allowed if stable for ≥ 4 weeks and maintained |
|
| Outcomes | PI: NRS 0 to 10, twice daily on last 3 days before treatment and at end of treatment period, at rest, on movement, and during palpitation Additional assessments for sleep interference, neuropathic pain, psychological factors Adverse events |
|
| Notes | Oxford Quality Score: R = 2, DB = 2, W = 1. Total = 5/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "computer‐generated randomization list" |
| Allocation concealment (selection bias) | Unclear risk | Not described, but likely to be adequate since pharmacy packed |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "the patches appeared identical and were packed by hospital pharmacy in identical small plastic boxes" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "the patches appeared identical and were packed by hospital pharmacy in identical small plastic boxes" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants completed study and analysed |
| Size | High risk | < 50 participants per treatment arm |
Cheville 2009.
| Methods | Multicentre, randomised, double‐blind, placebo‐controlled, cross‐over study Up to 3 plasters applied to painful area on waking and left in place for 18 h or until usual bedtime. Each treatment period lasted 4 weeks, with no washout between periods |
|
| Participants | Cancer patients with postsurgical incisional pain ≥ 1 month, PI ≥ 4/10 with neuropathic features, age ≥ 18 years N = 28 M 9, F 19 Mean age 62 years (SD 9.5) Baseline pain intensity (average) 4.9/10 (SD 1.8) |
|
| Interventions | Lidocaine 5% plaster (Lidoderm ®) Placebo plaster Stable pre‐entry oral analgesic regimens continued, with increases or decreases allowed at discretion of physician |
|
| Outcomes | PI: NRS 0 to 10, weekly McGill Pain Questionnaire, Brief Pain Inventory, Neuropathic Pain Scale PGIC: 7‐point scale, weekly Additional assessments for psychological factors, quality of life Adverse events |
|
| Notes | Oxford Quality Score: R = 1, DB = 2, W = 1. Total = 4/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "supplied in identical appearing patches in a blinded fashion" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "supplied in identical appearing patches in a blinded fashion" |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Withdrawals ≥ 10%. Different imputations for missing data carried out but not reported |
| Size | High risk | < 50 participants per treatment arm |
Galer 1999.
| Methods | Two centre enriched enrolment, randomised withdrawal study. Open‐label use of lidocaine plaster for > 1 month, randomised to 2 x 2‐week double‐blind, placebo‐controlled, cross‐over with no washout Up to 3 plasters applied to painful area (as for usual open‐label plasters) |
|
| Participants | Postherpetic neuralgia (participants in previous lidocaine trials now with open‐label use, or refractory with approved compassionate use). Current pain relief from plasters rated ≥ moderate (6‐point scale) and increase in pain during plaster‐free periods N = 32 M 14, F 18 Mean age 77 years (62 to 97) Duration of pain > 8 months |
|
| Interventions | Lidocaine 5% plaster (Lidoderm ®) Placebo plaster Concomitant analgesic medication allowed |
|
| Outcomes | Time to exit from double‐blind treatment phase due to lack of efficacy (≥ 2‐point decrease in PR (6‐point VRS) on 2 consecutive days of plaster application compared with pre‐study open‐label treatment) Adverse events |
|
| Notes | Oxford Quality Score: R = 1, DB = 2, W = 1. Total = 5/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Vehicle patches are identical except for the absence of lidocaine" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Vehicle patches are identical except for the absence of lidocaine" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All treated participants included in analysis. No imputation |
| Size | High risk | < 50 participants per treatment arm |
Galer 2002.
| Methods | Two centre, randomised, double‐blind, placebo‐controlled, parallel‐group study. Treatment duration 3 weeks | |
| Participants | Postherpetic neuralgia, torso pain ≥ 1 month, with allodynia, and ≥ moderate daily pain N = 96 (subset of larger study) M 36, F 60 Mean age 74 years (SD 8.3) Baseline pain intensity > 6/10 |
|
| Interventions | Lidocaine 5% plaster (Lidoderm ®) Placebo plaster Concomitant medication not reported |
|
| Outcomes | Change from baseline to endpoint in individual and 4 composite variables derived from Neuropathic Pain Scale (post hoc analysis) | |
| Notes | Oxford Quality Score: R = 1, DB = 1, W = 1. Total = 3/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described (note post hoc analysis of subset) |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not described |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Analysis used participants with complete data sets |
| Size | High risk | < 50 participants per treatment arm |
Ho 2008.
| Methods | Single‐centre, randomised, double‐blind, placebo‐controlled, cross‐over study 3 ml to 5 ml of study drug applied as a cream to cleaned painful area twice daily. Treatment duration 3 x 7 days with 7‐day washout periods between treatments |
|
| Participants | Postsurgical neuropathic pain, postherpetic neuralgia, or diabetic neuropathy with allodynia or hyperalgesia, ≥ 6 months, refractory to treatment. Age ≥ 18 years N = 35 M 16, F 19 Mean age 57 years (SD 13.8) Baseline pain intensity 53/100 |
|
| Interventions | Lidocaine 5% cream Amitriptyline 5% cream Placebo cream Vehicle: pluronic lecithin organogel. Active ingredient dissolved and mixed with Poloxamer 30%, then combined with lecithin‐isopropyl mysterate mixture to form emulsion |
|
| Outcomes | PI: 100 mm VAS and short‐form McGill Pain Questionnaire, before and after treatment phases PI: NRS 0 to 10, twice daily Patient satisfaction: 4‐point scale, at end of washout period Rescue medication Adverse events |
|
| Notes | Oxford Quality Score: R = 2, DB = 2, W = 1. Total = 5/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "computer‐generated" |
| Allocation concealment (selection bias) | Low risk | Remote allocation; "other research personal at the central office would then assign the participant to ..... a sequence of treatments" |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "All drug preparations appeared opaque yellow in color and were indistinguishable from one another" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "All drug preparations appeared opaque yellow in color and were indistinguishable from one another" |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Withdrawals ≥ 10% for each treatment. Imputation not mentioned |
| Size | High risk | < 50 participants per treatment arm |
Kanai 2006.
| Methods | Single‐centre, randomised, double‐blind, placebo‐controlled, cross‐over study Single dose: 2 x 0.1 ml spray into affected nostril while lying supine with neck extended 30 to 45 degrees and maintained for 30 seconds. 7‐day washout, then cross‐over to other treatment |
|
| Participants | Idiopathic trigeminal neuralgia (IHS criteria), triggered in anatomical region of trigeminal nerve, painful paroxysms ≥ 3 months, PI ≥ 4/10 N = 25 M 5, F 20 Mean age 63 years (44 to 85) Baseline pain intensity 8/10 (SD 2) |
|
| Interventions | Lidocaine 8% spray Placebo (saline) spray Conventional analgesics discontinued ≥ 12 h before treatment, until recurrence of pain or failure of treatment |
|
| Outcomes | PI: 10 cm VAS, before and 15 min after treatment, while still supine Time to return of pain Adverse events |
|
| Notes | Oxford Quality Score: R = 2, DB = 1, W = 1. Total = 4/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Patients were randomised by blindly taking a number from a closed container" |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not described |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants included in results |
| Size | High risk | < 50 participants per treatment group |
Kanai 2009a.
| Methods | Study 1. Single‐centre, randomised, double‐blind, placebo‐controlled, cross‐over study Dose from pump spray individually determined to completely cover painful site (each spray 0.1 ml, maximum 30 sprays). Single dose given while lying supine, 7‐day washout, then cross‐over to other treatment |
|
| Participants | Postherpetic neuralgia ≥ 3 months after healing of lesions, typical PI ≥ 4/10, age ≥ 20 years N = 24 M 13, F 11 Mean age 71 years (32 to 91) Baseline pain intensity 7.7/10 |
|
| Interventions | Lidocaine 8% spray Placebo (saline) spray Usual analgesics discontinued ≥ 12 h before treatment, until recurrence of pain or failure of treatment |
|
| Outcomes | PI: 10 cm VAS at rest and tactile allodynia, before and 15 min after treatment, while still supine Patient? assessment: 4‐point scale (worse to markedly better) Time to return of pain Adverse events |
|
| Notes | Oxford Quality Score: R = 1, DB = 1, W = 1. Total = 3/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not described |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants included in results of single‐dose study |
| Size | High risk | < 50 participants per treatment arm |
Kanai 2009b.
| Methods | Single‐centre, randomised, double‐blind, placebo‐controlled, cross‐over study Dose from pump spray individually determined to completely cover painful site (each spray 0.1 ml, maximum 30 sprays). Single dose given while lying supine, 7‐day washout, then cross‐over to other treatment |
|
| Participants | Post‐traumatic peripheral neuropathy, ≥ 3 months with typical PI ≥ 4/10, age ≥ 20 years N = 31 M 17, F 14 Mean age 55 years (20 to 80) Baseline pain intensity 7/10 |
|
| Interventions | Lidocaine 8% spray Placebo (saline) spray Usual analgesics discontinued ≥ 12 h before treatment, until recurrence of pain or failure of treatment |
|
| Outcomes | PI: 10 cm VAS at rest and tactile allodynia, before and 15 min after treatment, while still supine Patient? assessment: 4‐point scale (worse to markedly better) Return of pain Adverse events |
|
| Notes | Oxford Quality Score: R = 2, DB = 1, W = 1. Total = 4/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Patients randomized by blindly taking a number from a closed container" |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Unclear risk | Not described |
| Blinding of outcome assessment (detection bias) All outcomes | Unclear risk | Not described |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | All participants included in results |
| Size | High risk | < 50 participants per treatment arm |
Meier 2003.
| Methods | Three‐centre, randomised, double‐blind, placebo‐controlled, cross‐over study Maximum of 4 plasters applied to painful area for 12 h daily for 7 days. 1‐week washout (extended if pain not returned (± 20%) to pretreatment value), then other treatment |
|
| Participants | Peripheral neuropathic pain syndromes with superficial pain in a localised skin area and PI 40/100, stable consumption of pain medication. Mean duration of pain 36 months N = 58 M 28, F 30 Mean age 65 years (SD 12.5) Baseline pain intensity 65/100 |
|
| Interventions | Lidocaine 5% plaster (Neurodol Tissugel®) Placebo plaster Usual oral medication continued, no topical treatments |
|
| Outcomes | PI: 100 mm VAS, at 2, 4, 6, 8 h after first application and daily after plaster removal Mechanical allodynia, daily McGill Pain Questionnaire, before and at end of each treatment period Quality of sleep, daily Adverse events |
|
| Notes | Oxford Quality Score: R = 2, DB = 2, W = 1. Total = 5/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "computerized randomization" |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "identical patches" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "identical patches" |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Withdrawals > 10%, completer analysis |
| Size | High risk | < 50 participants per treatment group who contributed data |
Rowbotham 1995.
| Methods | Single‐centre, randomised, placebo‐controlled, cross‐over study Lidocaine and placebo gel applied simultaneously to painful area and contralateral mirror‐image unaffected area: active treatment applied to painful area, to unaffected area, or neither. For limbs and torso, gel applied with occlusion for 24 h; for head or neck application gel applied without occlusion for 8 h. Minimum 72 h between applications (pain returned to ≥ 75% of pre study level) |
|
| Participants | Postherpetic neuralgia ≥ 1 month after healing of rash in well‐defined area of skin N = 47 (39 completed) M 18, F 21 (completers) Mean age > 70 years (55 to 85) Baseline pain intensity ˜40/100 for head and neck pain, ˜50/100 for torso pain |
|
| Interventions | Lidocaine 5% gel Placebo gel Any topical pain treatment stopped ≥ 7 days before study. Established oral medications continued, unchanged |
|
| Outcomes | PI: 100 mm VAS before application and at 0.5, 1, 2, 4, 8 h after application, and 24 h for torso applications PR: 6‐point VRS (worse to complete relief) at same time points Adverse events: 27‐item checklist at same time points Severity of allodynia before application and after removal: 4‐point scale (0 to 3) |
|
| Notes | Oxford Quality Score: R = 1, DB = 2, W = 0. Total = 3/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Vehicle placebo gel was identical except for the absence of lidocaine". Investigators wore gloves for application and removal |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Vehicle placebo gel was identical except for the absence of lidocaine". Investigators wore gloves for application and removal |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Withdrawals > 10%. Completer analysis |
| Size | High risk | < 50 participants per treatment group |
Rowbotham 1996.
| Methods | Single‐centre, randomised, placebo‐controlled, cross‐over study: 4 sessions Up to 3 plasters applied to painful area for 12 h: 2 x lidocaine, 1 x placebo. Additional session with observation only. Minimum 72 h between applications (pain returned to ≥ 75% of pre study level) |
|
| Participants | Postherpetic neuralgia ≥ 1 month after healing of rash in well‐defined area of skin on torso or limbs N = 40 (36 treated, 35 completed) M 20, F 15 (completers) Mean age 75 years (50 to 90) Mean baseline pain intensity ˜50/100 Duration of pain ≥ 4 months |
|
| Interventions | Lidocaine 5% plaster (Lidoderm ®) Placebo plaster Any topical pain treatment stopped ≥ 2 weeks before study. Established oral medications continued, unchanged |
|
| Outcomes | PI: 100 mm VAS before application and at 0.5, 1, 2, 4, 9, 12 h after application Daily pain level PR: 6‐point VRS (worse to complete relief) at same time points Additional medication Adverse events: 27‐item checklist at same time points, and check for irritation under plaster at 6 h |
|
| Notes | Oxford Quality Score: R = 1, DB = 2, W = 1. Total = 4/5 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Not described |
| Allocation concealment (selection bias) | Unclear risk | Not described |
| Blinding of participants and personnel (performance bias) All outcomes | Low risk | "Vehicle patches were identical except for the absence of lidocaine" |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | "Vehicle patches were identical except for the absence of lidocaine" |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Withdrawals < 3%, judged unlikely to affect lidocaine and placebo groups |
| Size | High risk | < 50 participants per treatment group |
DB: double‐blind; F: female; h: hours; IHS: International Headache Society; M: male; min: minutes; N: number of participants in study; NRS: numerical rating scale; NRS: numerical rating scale; PGIC: Patient Global Impression of Change; PI: pain intensity; PR: pain relief; R: randomised; SD: standard deviation; VAS: visual analogue scale; VRS: verbal rating scale; W: withdrawals
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| NCT00609323 | No lidocaine only treatment arm |
| NCT01155986 | Study terminated due to problems with enrolment |
| Tajti 1999 | Does not state that study was randomised |
Characteristics of studies awaiting assessment [ordered by study ID]
NCT00904202.
| Methods | Multicenter, randomised, double‐blind, placebo‐controlled (double‐dummy), parallel‐group study. Duration 5 weeks |
| Participants | Patients with postherpetic neuralgia (PHN), diabetic neuropathy (DN), complex regional pain syndrome (CRPS), carpal tunnel syndrome, HIV neuropathy, idiopathic sensory neuropathy, or other peripheral neuropathy (≥ 3 months)
N = 62
M + F Adults PI: ≥ 4/10 |
| Interventions | Lidocaine 5% plaster (Lidoderm ®) Gabapentin 1800 mg daily Lidocaine patch + gabapentin Placebo |
| Outcomes | PI: Brief Pain Inventory PQAS PGIC Allodynia Patient disability assessment Adverse events |
| Notes | Sponsor: Endo Pharmaceuticals |
PGIC: Patient Global Impression of change; PI: pain intensity; PQAS: Pain Quality Assessment Scale
Characteristics of ongoing studies [ordered by study ID]
EudraCT 2009‐015415‐41.
| Trial name or title | Lidocaine patches in postoperative and posttraumatic neuropathic chronic skin pain ‐ A prospective, randomized, double‐blinded, placebo‐controlled, parallel, multicentre, investigator initiated study according to clinical guidelines |
| Methods | Randomised, double‐blind, placebo‐controlled, parallel groups. Duration 12 weeks |
| Participants | Participants with postoperative or post‐traumatic neuropathic chronic cutaneous pain (≥ 3 months) N = 222 M and F Adults PI: ≥ 5/10 LANSS ≥ 12 |
| Interventions | Lidocaine 5% plaster (Versatis ®) Placebo plaster |
| Outcomes | PI: NRS (0 to 10)
PGIC
Additional analgesic use Adverse events Additional assessments for size of painful area, cutaneous sensory symptoms, neuropathic pain, quality of life |
| Starting date | Not reported |
| Contact information | Guy Hans. E‐mail: guy.hans@uza.be |
| Notes |
EudraCT 2012‐000347‐28.
| Trial name or title | Efficacy and safety of lidocaine 5% medicated plaster in localized chronic post‐operative neuropathic pain |
| Methods | Randomised, double‐blind, placebo‐controlled, parallel groups. Duration 12 weeks |
| Participants | Participants with moderate to severe localised chronic postoperative neuropathic pain (≥ 3 months)
N = 360
M and F Adults PI: ≥ 4/10 |
| Interventions | Lidocaine 5% plaster (Versatis ®) Placebo plaster |
| Outcomes | PI: NRS (0 to 10)
Responders: ≥ 30% and ≥ 50% PI reduction PGIC: 7‐point scale painDETECT questionnaire scores Additional assessments for psychological factors, allodynia, quality of life, sleep |
| Starting date | Not reported |
| Contact information | GRT Trial Information Desk. E‐mail: Clinical‐Trials@grunenthal.com |
| Notes |
EudraCT 2012‐003077‐26.
| Trial name or title | Topical lidocaine for the treatment of focal peripheral neuropathic pain: response in relation to pain phenotype |
| Methods | Randomised, double‐blind, placebo‐controlled, cross‐over. Duration 2 x 4 weeks |
| Participants | Patients with chronic peripheral neuropathic pain caused by postherpetic neuralgia and traumatic/surgical nerve injury, ± irritable nociceptors
N = 46
M and F Adults PI: ≥ 4/10 |
| Interventions | Lidocaine 5% plaster (Versatis ®) Placebo plaster |
| Outcomes | PI: NRS (0 to 10) PR: 5‐point scale Additional assessments for allodynia and hyperalgesia Additional medication |
| Starting date | Not reported |
| Contact information | Søren hein Sindrup. Telephone number: +45 65412471 |
| Notes |
NCT00686127.
| Trial name or title | A Randomized, Double‐Blind, Placebo‐Controlled Trial (RDBPCT) of the Effectiveness of the Lidocaine Patch in the Management of Neuropathic Pain After Breast Cancer Surgery |
| Methods | Randomised, double‐blind, placebo‐controlled, parallel groups. Duration 12 weeks. Patch changed every 24 hours |
| Participants | Women with pain in breast scar area or ipsilateral arm. Age ≥ 18 years N = 27 |
| Interventions | Lidocaine 5% plaster (Lidoderm ®) Placebo |
| Outcomes | PI Pain interference with function |
| Starting date | September 2003 |
| Contact information | Study sponsor: University of California, San Francisco |
| Notes | Estimated completion date December 2013 |
NCT01752322.
| Trial name or title | Efficacy and tolerability of lidocaine plaster for treatment of long‐term local nerve pain |
| Methods | Multicentre. Randomised, double‐blind, placebo‐controlled, parallel groups. Duration 12 weeks |
| Participants | Moderate to severe (≥ 4/10) localised chronic postoperative neuropathic pain (eg thoracotomy, total knee replacement, cholecystectomy, mastectomy, inguinal hernia repair, varicose vein stripping) M and F Age ≥ 18 years Estimated enrolment 600 |
| Interventions | Lidocaine 5% plaster (Versatis ®) Placebo plaster |
| Outcomes | End of treatment and change from baseline measures: PI painDETECT questionnaire (total score) Additional assessments for psychological factors, quality of life, sleep |
| Starting date | October 2012 |
| Contact information | Study sponsor: Grünenthal GmbH |
| Notes | Estimated final data collection for primary outcome in July 2015 |
F: female; LANSS: Leeds Assessment of Neuropathic Symptoms and Signs; M: male; N: number of participants; NRS: numerical rating scale; PGIC: Patient Global Impression of Change; PI: pain intensity; PR: pain relief
Differences between protocol and review
There are no differences between the protocol and the review.
Contributions of authors
SD and RAM wrote the protocol.
SD, PW, and RAM were involved in searching, data extraction, and the limited analysis that was possible. All authors contributed to the final drafting of the review and approved it.
Sources of support
Internal sources
-
Oxford Pain Relief Trust, UK.
General institutional support
External sources
-
National Institute for Health Research (NIHR), UK.
NIHR Cochrane Incentive Scheme 2013. Award Reference Number:13/101/13.
Declarations of interest
JQ has no known conflicts of interest. SD, PW, and RAM have no conflicts relating to this review or any similar product.
Stable (no update expected for reasons given in 'What's new')
References
References to studies included in this review
Binder 2009 {published data only}
- Binder A, Bruxelle J, Rogers P, Hans G, Bösl I, Baron R. Topical 5% lidocaine (lignocaine) medicated plaster treatment for post‐herpetic neuralgia: results of a double‐blind, placebo‐controlled, multinational efficacy and safety trial. Clinical Drug Investigation 2009;29(6):393‐408. [DOI: 10.2165/00044011-200929060-00003] [DOI] [PubMed] [Google Scholar]
Bischoff 2013 {published data only}
- Bischoff JM, Petersen M, Uçeyler N, Sommer C, Kehlet H, Werner MU. Lidocaine patch (5%) in treatment of persistent inguinal postherniorrhaphy pain: a randomized, double‐blind, placebo‐controlled, crossover trial. Anesthesiology 2013;119(6):1444‐52. [DOI: 10.1097/ALN.0b013e3182a2a243] [DOI] [PubMed] [Google Scholar]
Cheville 2009 {published data only}
- Cheville AL, Sloan JA, Northfelt DW, Jillella AP, Wong GY, Bearden Iii JD, et al. Use of a lidocaine patch in the management of postsurgical neuropathic pain in patients with cancer: a phase III double‐blind crossover study (N01CB). Supportive Care in Cancer 2009;17(4):451‐60. [DOI: 10.1007/s00520-008-0542-x] [DOI] [PMC free article] [PubMed] [Google Scholar]
Galer 1999 {published data only}
- Galer BS, Rowbotham MC, Perander J, Friedman E. Topical lidocaine patch relieves postherpetic neuralgia more effectively than a vehicle topical patch: results of an enriched enrollment study. Pain 1999;80(3):533‐8. [DOI: 10.1016/S0304-3959(98)00244-9] [DOI] [PubMed] [Google Scholar]
Galer 2002 {published data only}
- Galer BS, Jensen MP, Ma T, Davies PS, Rowbotham MC. The lidocaine patch 5% effectively treats all neuropathic pain qualities: results of a randomized, double‐blind, vehicle‐controlled, 3‐week efficacy study with use of the neuropathic pain scale. Clinical Journal of Pain 2002;18(5):297‐301. [DOI] [PubMed] [Google Scholar]
- Rowbotham MC, Davies PS, Galer BS. Multicenter, double‐blind, vehicle‐controlled trial of long term use of lidocaine patches for postherpetic neuralgia [abstract 184]. Abstracts of the 8th World Congress of the International Association for the Study of Pain (Vancouver, British Columbia, Canada, August 17–22). 1996:274.
Ho 2008 {published data only}
- Ho KY, Huh BK, White WD, Yeh CC, Miller EJ. Topical amitriptyline versus lidocaine in the treatment of neuropathic pain. Clinical Journal of Pain 2008;24(1):51‐5. [DOI: 10.1097/AJP.0b013e318156db26] [DOI] [PubMed] [Google Scholar]
Kanai 2006 {published data only}
- Kanai A, Suzuki A, Kobayashi M, Hoka S. Intranasal lidocaine 8% spray for second‐division trigeminal neuralgia. British Journal of Anaesthesia 2006;97(4):559‐63. [DOI: 10.1093/bja/ael180] [DOI] [PubMed] [Google Scholar]
Kanai 2009a {published data only}
- Kanai A, Kumaki C, Niki Y, Suzuki A, Tazawa T, Okamoto H. Efficacy of a metered‐dose 8% lidocaine pump spray for patients with post‐herpetic neuralgia. Pain Medicine 2009;10(5):902‐9. [DOI: 10.1111/j.1526-4637.2009.00662.x] [DOI] [PubMed] [Google Scholar]
Kanai 2009b {published data only}
- Kanai A, Segawa Y, Okamoto T, Koto M, Okamoto H. The analgesic effect of a metered‐dose 8% lidocaine pump spray in posttraumatic peripheral neuropathy: a pilot study. Anesthesia and Analgesia 2009;108(3):987‐91. [DOI: 10.1213/ane.0b013e31819431aa] [DOI] [PubMed] [Google Scholar]
Meier 2003 {published data only}
- Meier T, Wasner G, Faust M, Kuntzer T, Ochsner F, Hueppe M, et al. Efficacy of lidocaine patch 5% in the treatment of focal peripheral neuropathic pain syndromes: a randomized, double‐blind, placebo‐controlled study. Pain 2003;106(1‐2):151‐8. [DOI: 10.1016/S0304-3959(03)00317-8] [DOI] [PubMed] [Google Scholar]
- Wasner G, Kleinert A, Binder A, Schattschneider J, Baron R. Postherpetic neuralgia: topical lidocaine is effective in nociceptor‐deprived skin. Journal of Neurology 2005;252(6):677‐86. [DOI: 10.1007/s00415-005-0717-z] [DOI] [PubMed] [Google Scholar]
Rowbotham 1995 {published data only}
- Rowbotham MC, Davies PS, Fields HL. Topical lidocaine gel relieves postherpetic neuralgia. Annals of Neurology 1995;37(2):246‐53. [DOI: 10.1002/ana.410370216] [DOI] [PubMed] [Google Scholar]
Rowbotham 1996 {published data only}
- Rowbotham MC, Davies PS, Verkempinck C, Galer BS. Lidocaine patch: double‐blind controlled study of a new treatment method for post‐herpetic neuralgia. Pain 1996;65(1):39‐44. [DOI: 10.1016/0304-3959(95)00146-8] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
NCT00609323 {unpublished data only}
- A Randomized, Double‐Blind, Crossover Study Comparing Pliaglis™ (Lidocaine and Tetracaine) Cream 7%/7% to Placebo Cream When Applied for 60 Minutes in the Treatment of Patients With Postherpetic Neuralgia. http://clinicaltrials.gov/ct2/show/NCT00609323 (accessed 5 February 2014) 2014. [NCT: NCT00609323]
NCT01155986 {unpublished data only}
- Lidocaine 5% Medicated Plaster for the Topical Treatment of Localized Chronic Postoperative Neuropathic Pain. http://clinicaltrials.gov/ct2/show/NCT01155986 (accessed 5 February 2014) 2014. [NCT: NCT01155986]
Tajti 1999 {published data only}
- Tajti J, Szok D, Vécsei L. Topical acetylsalicylic acid versus lidocaine for postherpetic neuralgia: results of a double‐blind comparative clinical trial. Neurobiology (Bp) 1999;7(2):103‐8. [PubMed] [Google Scholar]
References to studies awaiting assessment
NCT00904202 {unpublished data only}
- A Multicenter, Randomized, Double‐Blind, Placebo‐Controlled, Parallel‐Group Study Of Lidocaine Patch 5% Alone, Gabapentin Alone, And Lidocaine Patch 5% And Gabapentin In Combination For The Relief Of Pain In Patients With Diverse Peripheral Neuropathic Pain Conditions. http://clinicaltrials.gov/ct2/show/NCT00904202 (accessed 5 February 2014) 2014. [NCT: NCT00904202]
References to ongoing studies
EudraCT 2009‐015415‐41 {unpublished data only}
- Lidocaine patches in postoperative and posttraumatic neuropathic chronic skin pain ‐ A prospective, randomized, double‐blinded, placebo‐controlled, parallel, multicentre, investigator initiated study according to clinical guidelines. www.clinicaltrialsregister.eu/ctr‐search/search?query=eudract_number:2009‐015415‐41 (accessed 5 February 2014) 2014. [Eudract number: 2009‐015415‐41]
EudraCT 2012‐000347‐28 {unpublished data only}
- Efficacy and safety of lidocaine 5% medicated plaster in localized chronic post‐operative neuropathic pain. www.clinicaltrialsregister.eu/ctr‐search/search?query=eudract_number:2012‐000347‐28 (accessed 5 February 2014) 2014. [Eudract number: 2012‐000347‐28]
EudraCT 2012‐003077‐26 {unpublished data only}
- Topical lidocaine for the treatment of focal peripheral neuropathic pain: response in relation to pain phenotype. www.clinicaltrialsregister.eu/ctr‐search/search?query=eudract_number:2012‐003077‐26 (accessed 5 February 2014) 2014. [Eudract number: EudraCT 2012‐003077‐26]
NCT00686127 {published data only}
- A Randomized, Double‐Blind, Placebo‐Controlled Trial (RDBPCT) of the Effectiveness of the Lidocaine Patch in the Management of Neuropathic Pain After Breast Cancer Surgery. ClinicalTrials.gov (accessed 5 February 2014) 2014.
NCT01752322 {published data only}
- Efficacy and Tolerability of Lidocaine Plaster for Treatment of Long‐term Local Nerve Pain. Clinical trials.gov (accessed 5 February 2014) 2014.
Additional references
Apkarian 2011
- Apkarian AV, Hashmi JA, Baliki MN. Pain and the brain: specificity and plasticity of the brain in clinical chronic pain. Pain 2011;152(3 Suppl):S49‐64. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bouhassira 2008
- Bouhassira D, Lantéri‐Minet M, Attal N, Laurent B, Touboul C. Prevalence of chronic pain with neuropathic characteristics in the general population. Pain 2008;136(3):380‐7. [DOI] [PubMed] [Google Scholar]
Campbell 2002
- Campbell BJ, Rowbotham M, Davies PS, Jacob P 3rd, Benowitz NL. Systemic absorption of topical lidocaine in normal volunteers, patients with post‐herpetic neuralgia, and patients with acute herpes zoster. Journal of Pharmaceutical Sciences 2002;91(5):1343‐50. [DOI] [PubMed] [Google Scholar]
Chronicle 2004
- Chronicle EP, Mulleners WM. Anticonvulsant drugs for migraine prophylaxis. Cochrane Database of Systematic Reviews 2004, Issue 3. [DOI: 10.1002/14651858.CD003226.pub2] [DOI] [PubMed] [Google Scholar]
Cochrane PaPaS Group 2011
- Cochrane Pain, Palliative and Supportive Care Group. PaPaS author and referee guidance. http://papas.cochrane.org/sites/papas.cochrane.org/files/uploads/L%20‐%20PaPaSAuthor%26RefereeGuidance.pdf (accessed 22 January 2013).
Derry 2012
- Derry S, Moore RA. Topical capsaicin (low concentration) for chronic neuropathic pain in adults. Cochrane Database of Systematic Reviews 2012, Issue 9. [DOI: 10.1002/14651858.CD010111] [DOI] [PMC free article] [PubMed] [Google Scholar]
Derry 2013
- Derry S, Sven‐Rice A, Cole P, Tan T, Moore RA. Topical capsaicin (high concentration) for chronic neuropathic pain in adults. Cochrane Database of Systematic Reviews 2013, Issue 2. [DOI: 10.1002/14651858.CD007393.pub3] [DOI] [PubMed] [Google Scholar]
Dworkin 2008
- Dworkin RH, Turk DC, Wyrwich KW, Beaton D, Cleeland CS, Farrar JT, et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. Journal of Pain 2008;9(2):105‐21. [DOI] [PubMed] [Google Scholar]
Elbourne 2002
- Elbourne DR, Altman DG, Higgins JP, Curtin F, Worthington HV, Vail A. Meta‐analyses involving cross‐over trials: methodological issues. International Journal of Epidemiology 2002;31(1):140‐9. [DOI: 10.1093/ije/31.1.140] [DOI] [PubMed] [Google Scholar]
EMC 2013
- Electronic Medicines Compendium. Versatis 5% Medicated Plaster. Summary of Product Characteristics. www.medicines.org.uk/emc/medicine/19291 (accessed 17 December 2013).
Garnock‐Jones 2009
- Garnock‐Jones KP, Keating GM. Lidocaine 5% medicated plaster: a review of its use in postherpetic neuralgia. Drugs 2009;69(15):2149‐65. [DOI: 10.2165/11203220-000000000-00000] [DOI] [PubMed] [Google Scholar]
Geborek 2002
- Geborek P, Crnkic M, Petersson IF, Saxne T, South Swedish Arthritis Treatment Group. Etanercept, infliximab, and leflunomide in established rheumatoid arthritis: clinical experience using a structured follow up programme in southern Sweden. Annals of the Rheumatic Diseases 2002;61(9):793‐8. [DOI: 10.1136/ard.61.9.793] [DOI] [PMC free article] [PubMed] [Google Scholar]
Gustorff 2008
- Gustorff B, Dorner T, Likar R, Grisold W, Lawrence K, Schwarz F, et al. Prevalence of self‐reported neuropathic pain and impact on quality of life: a prospective representative survey. Acta Anaesthesiologica Scandinavica 2008;52(1):132‐6. [DOI] [PubMed] [Google Scholar]
Hall 2008
- Hall GC, Carroll D, McQuay HJ. Primary care incidence and treatment of four neuropathic pain conditions: a descriptive study, 2002‐2005. BMC Family Practice 2008;9:26. [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2011
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Jadad 1996
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17(1):1‐12. [DOI] [PubMed] [Google Scholar]
Jensen 2011
- Jensen TS, Baron R, Haanpää M, Kalso E, Loeser JD, Rice AS, et al. A new definition of neuropathic pain. Pain 2011;152(10):2204‐5. [DOI] [PubMed] [Google Scholar]
Katusic 1991
- Katusic S, Williams DB, Beard CM, Bergstralh EJ, Kurland LT. Epidemiology and clinical features of idiopathic trigeminal neuralgia and glossopharyngeal neuralgia: similarities and differences, Rochester, Minnesota, 1945‐1984. Neuroepidemiology 1991;10:276‐81. [DOI] [PubMed] [Google Scholar]
Khan 1996
- Khan KS, Daya S, Jadad A. The importance of quality of primary studies in producing unbiased systematic reviews. Archives of Internal Medicine 1996;156(6):661‐6. [PubMed] [Google Scholar]
Koopman 2009
- Koopman JS, Dieleman JP, Huygen FJ, Mos M, Martin CG, Sturkenboom MC. Incidence of facial pain in the general population. Pain 2009;147(1‐3):122‐7. [DOI] [PubMed] [Google Scholar]
L'Abbé 1987
- L'Abbé KA, Detsky AS, O'Rourke K. Meta‐analysis in clinical research. Annals of Internal Medicine 1987;107:224‐33. [DOI] [PubMed] [Google Scholar]
Lunn 2009
- Lunn MP, Hughes RA, Wiffen PJ. Duloxetine for treating painful neuropathy or chronic pain. Cochrane Database of Systematic Reviews 2009, Issue 4. [DOI: 10.1002/14651858.CD007115.pub2] [DOI] [PubMed] [Google Scholar]
McQuay 1998
- McQuay H, Moore R. An Evidence‐based Resource for Pain Relief. Oxford: Oxford University Press, 1998. [ISBN: 978‐0192630483] [Google Scholar]
McQuay 2007
- McQuay HJ, Smith LA, Moore RA. Chronic pain. In: Stevens A, Raftery J, Mant J, Simpson S editor(s). Health Care Needs Assessment. 3rd Edition. Oxford: Radcliffe Publishing, 2007. [ISBN: 978‐1846190636] [Google Scholar]
Mick 2012
- Mick G, Correa‐Illanes G. Topical pain management with the 5% lidocaine medicated plaster ‐ a review. Current Medical Research and Opinion 2012;28(6):937‐51. [DOI] [PubMed] [Google Scholar]
Moher 2009
- Moher D, Liberati A, Tetzlaff J, Altman DG, the PRISMA Group. Preferred reporting items for systematic reviews and meta‐analyses: the PRISMA statement. PLoS Medicine 2009;6(7):e1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moisset 2007
- Moisset X, Bouhassira D. Brain imaging of neuropathic pain. Neuroimaging 2007;37(Suppl 1):S80‐8. [DOI] [PubMed] [Google Scholar]
Moore 1998
- Moore RA, Gavaghan D, Tramèr MR, Collins SL, McQuay HJ. Size is everything ‐ large amounts of information are needed to overcome random effects in estimating direction and magnitude of treatment effects. Pain 1998;78(3):209‐16. [DOI] [PubMed] [Google Scholar]
Moore 2008
- Moore RA, Barden J, Derry S, McQuay HJ. Managing potential publication bias. In: McQuay HJ, Kalso E, Moore RA editor(s). Systematic Reviews in Pain Research: Methodology Refined. Seattle: IASP Press, 2008:15‐24. [ISBN: 978–0931092695] [Google Scholar]
Moore 2009
- Moore RA, Straube S, Wiffen PJ, Derry S, McQuay HJ. Pregabalin for acute and chronic pain in adults. Cochrane Database of Systematic Reviews 2009, Issue 3. [DOI: 10.1002/14651858.CD007076.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moore 2010a
- Moore RA, Eccleston C, Derry S, Wiffen P, Bell RF, Straube S, et al. "Evidence" in chronic pain ‐ establishing best practice in the reporting of systematic reviews. Pain 2010;150(3):386‐9. [DOI] [PubMed] [Google Scholar]
Moore 2010b
- Moore RA, Moore OA, Derry S, Peloso PM, Gammaitoni AR, Wang H. Responder analysis for pain relief and numbers needed to treat in a meta‐analysis of etoricoxib osteoarthritis trials: bridging a gap between clinical trials and clinical practice. Annals of the Rheumatic Diseases 2010;69(2):374‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moore 2010c
- Moore RA, Straube S, Paine J, Phillips CJ, Derry S, McQuay HJ. Fibromyalgia: moderate and substantial pain intensity reduction predicts improvement in other outcomes and substantial quality of life gain. Pain 2010;149(2):360‐4. [DOI] [PubMed] [Google Scholar]
Moore 2010d
- Moore RA, Smugar SS, Wang H, Peloso PM, Gammaitoni A. Numbers‐needed‐to‐treat analyses ‐ do timing, dropouts, and outcome matter? Pooled analysis of two randomized, placebo‐controlled chronic low back pain trials. Pain 2010;151(3):592‐7. [DOI] [PubMed] [Google Scholar]
Moore 2011a
- Moore RA, Wiffen PJ, Derry S, McQuay HJ. Gabapentin for chronic neuropathic pain and fibromyalgia in adults. Cochrane Database of Systematic Reviews 2011, Issue 3. [DOI: 10.1002/14651858.CD007938.pub2] [DOI] [PMC free article] [PubMed] [Google Scholar]
Moore 2011b
- Moore RA, Straube S, Paine J, Derry S, McQuay HJ. Minimum efficacy criteria for comparisons between treatments using individual patient meta‐analysis of acute pain trials: examples of etoricoxib, paracetamol, ibuprofen, and ibuprofen/paracetamol combinations after third molar extraction. Pain 2011;152(5):982‐9. [DOI] [PubMed] [Google Scholar]
Moore 2011c
- Moore RA, Mhuircheartaigh RJ, Derry S, McQuay HJ. Mean analgesic consumption is inappropriate for testing analgesic efficacy in post‐operative pain: analysis and alternative suggestion. European Journal of Anaesthesiology 2011;28(6):427‐32. [DOI] [PubMed] [Google Scholar]
Moore 2012
- Moore RA, Derry S, Aldington D, Cole P, Wiffen PJ. Amitriptyline for neuropathic pain and fibromyalgia in adults. Cochrane Database of Systematic Reviews 2012, Issue 12. [DOI: 10.1002/14651858.CD008242.pub2] [DOI] [PubMed] [Google Scholar]
Moore 2013a
- Moore RA, Straube S, Aldington D. Pain measures and cut‐offs ‐ 'no worse than mild pain' as a simple, universal outcome. Anaesthesia 2013;68(4):400‐12. [DOI: 10.1111/anae.12148] [DOI] [PubMed] [Google Scholar]
Moore 2013b
- Moore A, Derry S, Eccleston C, Kalso E. Expect analgesic failure; pursue analgesic success. BMJ 2013;346:f2690. [DOI] [PubMed] [Google Scholar]
Moore 2014a
- Moore RA, Derry S, Taylor RS, Straube S, Phillips CJ. The costs and consequences of adequately managed chronic non‐cancer pain and chronic neuropathic pain. Pain Practice 2014;14(1):79‐94. [DOI] [PubMed] [Google Scholar]
Moore 2014b
- Moore RA, Cai N, Skljarevski V, Tölle TR. Duloxetine use in chronic painful conditions ‐ individual patient data responder analysis. European Journal of Pain 2014;18(1):67‐75. [DOI] [PMC free article] [PubMed] [Google Scholar]
O'Brien 2010
- O'Brien EM, Staud RM, Hassinger AD, McCulloch RC, Craggs JG, Atchison JW, et al. Patient‐centered perspective on treatment outcomes in chronic pain. Pain Medicine 2010;11(1):6‐15. [DOI] [PubMed] [Google Scholar]
O'Connor 2009
- O'Connor AB, Dworkin RH. Treatment of neuropathic pain: an overview of recent guidelines. American Journal of Medicine 2009;122(10 Suppl):S22‐32. [DOI] [PubMed] [Google Scholar]
Rappaport 1994
- Rappaport ZH, Devor M. Trigeminal neuralgia: the role of self‐sustaining discharge in the trigeminal ganglion. Pain 1994;56:127‐38. [DOI] [PubMed] [Google Scholar]
Review Manager 2013 [Computer program]
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2013.
Sabatowski 2012
- Sabatowski R, Hans G, Tacken I, Kapanadze S, Buchheister B, Baron R. Safety and efficacy outcomes of long‐term treatment up to 4 years with 5% lidocaine medicated plaster in patients with post‐herpetic neuralgia. Current Medical Research and Opinion 2012;28(8):1337‐46. [DOI: 10.1185/03007995.2012.707977] [DOI] [PubMed] [Google Scholar]
Sawynok 2014
- Sawynok J. Topical analgesics for neuropathic pain: preclinical exploration, clinical validation, future development. European Journal of Pain 2014;18(4):465‐81. [DOI: 10.1002/j.1532-2149.2013.00400.x] [DOI] [PubMed] [Google Scholar]
Snedecor 2014
- Snedecor SJ, Sudharshan L, Cappelleri JC, Sadosky A, Mehta S, Botteman M. Systematic review and meta‐analysis of pharmacological therapies for painful diabetic peripheral neuropathy. Pain Practice 2014;14(2):167‐84. [DOI: 10.1111/papr.12054] [DOI] [PubMed] [Google Scholar]
Soni 2013
- Soni A, Batra R, Gwilym S, Spector T, Hart D, Arden N, et al. Neuropathic features of joint pain: a community‐based study. Arthritis & Rheumatism 2013;65(7):1942‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Straube 2008
- Straube S, Derry S, McQuay HJ, Moore RA. Enriched enrollment: definition and effects of enrichment and dose in trials of pregabalin and gabapentin in neuropathic pain. A systematic review. British Journal of Clinical Pharmacology 2008;66(2):266‐75. [DOI] [PMC free article] [PubMed] [Google Scholar]
Straube 2010
- Straube S, Derry S, Moore RA, Paine J, McQuay HJ. Pregabalin in fibromyalgia ‐ responder analysis from individual patient data. BMC Musculoskeletal Disorders 2010;11:150. [DOI] [PMC free article] [PubMed] [Google Scholar]
Sultan 2008
- Sultan A, Gaskell H, Derry S, Moore RA. Duloxetine for painful diabetic neuropathy and fibromyalgia pain: systematic review of randomised trials. BMC Neurology 2008;8:29. [DOI] [PMC free article] [PubMed] [Google Scholar]
Torrance 2006
- Torrance N, Smith BH, Bennett MI, Lee AJ. The epidemiology of chronic pain of predominantly neuropathic origin. Results from a general population survey. Journal of Pain 2006;7(4):281‐9. [DOI] [PubMed] [Google Scholar]
Tracey 2011
- Tracey I. Can neuroimaging studies identify pain endophenotypes in humans?. Nature Reviews Neurology 2011;7(3):173‐81. [DOI] [PubMed] [Google Scholar]
Treede 2008
- Treede RD, Jensen TS, Campbell JN, Cruccu G, Dostrovsky JO, Griffin JW, et al. Neuropathic pain: redefinition and a grading system for clinical and research purposes. Neurology 2008;70(18):1630‐5. [DOI] [PubMed] [Google Scholar]
van Hecke 2014
- Hecke O, Austin SK, Khan RA, Smith BH, Torrance N. Neuropathic pain in the general population: a systematic review of epidemiological studies. Pain 2014;155(4):654‐62. [DOI: 10.1016/j.pain.2013.11.013] [DOI] [PubMed] [Google Scholar]
Vos 2012
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380(9859):2163‐96. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wehrfritz 2011
- Wehrfritz A, Namer B, Ihmsen H, Mueller C, Filitz J, Koppert W, et al. Differential effects on sensory functions and measures of epidermal nerve fiber density after application of a lidocaine patch (5%) on healthy human skin. European Journal of Pain 2011;15(9):907‐12. [DOI: 10.1016/j.ejpain.2011.03.011] [DOI] [PubMed] [Google Scholar]
Wolff 2010
- Wolff RF, Bala MM, Westwood M, Kessels AG, Kleijnen J. 5% lidocaine medicated plaster in painful diabetic peripheral neuropathy (DPN): a systematic review. Swiss Medical Weekly 2010;140(21‐2):297‐306. [DOI: ] [DOI] [PubMed] [Google Scholar]
Wolff 2011
- Wolff RF, Bala MM, Westwood M, Kessels AG, Kleijnen J. 5% lidocaine‐medicated plaster vs other relevant interventions and placebo for post‐herpetic neuralgia (PHN): a systematic review. Acta Neurologica Scandinavica 2011;123(5):295‐309. [DOI: 10.1111/j.1600-0404.2010.01433.x] [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Khaliq 2007
- Khaliq W, Alam S, Puri N. Topical lidocaine for the treatment of postherpetic neuralgia. Cochrane Database of Systematic Reviews 2007, Issue 2. [DOI: 10.1002/14651858.CD004846.pub2] [DOI] [PubMed] [Google Scholar]