

Abstract
Electronic health record patient portal usage has been associated with improvement in chronic disease parameters, patient functional status and patient satisfaction. Our institution’s patient portal is a secure, online health management tool that connects patients to portions of their electronic health record.
Our quality improvement project aimed to increase patient portal enrolment significantly in our Internal Medicine resident patient panels.
This study was conducted in a large, multisite health system in Kansas City, Kansas that serves a diverse patient population. Our clinic includes 65 resident patient panels. We followed a subset of 16 resident patient panels in this quality improvement project. A baseline audit showed that 35% of the 1628 patients in these panels were enrolled in the patient portal system. A standardised, nurse-initiated portal sign-up process following patient rooming was implemented. Initial results indicated a 9.6% increase in patient portal sign-up at the end of the first 4-week cycle. We then implemented educational sessions for our clinic nurses as well as attending physicians, and achieved a 15.1% increase from baseline to the end of the second 4-week cycle, resulting in 86 patient portal activations (p<0.01).
Resident physicians worked with clinic nurse partners in two formats for this project. Nurses assigned to patient rooming for residents during the clinic sessions being studied (rooming nurses) initiated the portal sign-up process. Nurses assigned to partner with the resident for longitudinal patient care management, anchor nurses, worked with residents on items such as phone messages or portal messages. Semi-structured interviews of the four anchor nurses aligned with the 16 residents were conducted at the end of the study and revealed that nursing staff perceived increased patient portal activity to be associated with a decrease in nursing workload and an increase in patient engagement.
Keywords: ambulatory care, quality improvement, patient satisfaction
Problem
A frequent challenge faced in resident continuity clinics is a lack of timely communication of test results to patients. Delays in timely action on test results lead to patient dissatisfaction and have been identified as a serious quality gap in the management of test results.1 We hypothesised that increasing enrolment in the patient portal (MyChart; Epic Systems Corporation, Verona, WI, USA), associated with our electronic health record (Epic Systems; Epic O2, Verona, WI, USA) would streamline result communication between resident physicians and patients. We also expected that increased patient portal enrolment would lessen the nursing workload and decrease nursing telephone call volume.
Our internal medicine (IM) clinic supports 65 resident patient panels and is housed on the main campus of a large, multisite health system in Kansas City, Kansas. In this educational structure, a resident physician refers to a learner who has completed medical school and is completing post-graduate IM residency training. Residents have a goal patient panel size of 90 patients balanced across age, gender, complex medical comorbidities, as well as payor sources. At our institution, our residents rotate on an ‘x+y’ block schedule, which separates their educational rotations to traditional 3 week inpatient rotations when they do not have continuity clinic, followed by a 1 week dedicated continuity clinic rotation. Each resident is assigned to a specific faculty along with an anchor nurse for their longitudinal continuity clinic education over the length of their residency. Their anchor nurse handles all telephone calls, refills and other administrative duties in support of the resident’s practice—both while the resident is seeing patients during their continuity clinic week and while the resident is on a different rotation. To streamline clinic workflow, the anchor nurse does not always ‘room’ scheduled clinic patients for their aligned resident physicians. There is a cohort of ‘rooming’ nurses that follow standard protocols for this activity in a busy clinic setting.
During a resident’s non-continuity clinic rotations, there is often a delay in clinic result communication to patients. Results from tests ordered in the residents’ clinic can be communicated to patients in a variety of ways: (1) in person at a follow-up visit, (2) via a telephone call from the resident physician to the patient, (3) via a telephone call from the anchor nurse to the patient after the resident has entered electronic comments and recommendations, (4) via a letter to the patient, or (5) via the patient portal associated with the electronic health record (EHR).
Our primary aim was to increase patient portal enrolment in the General Internal Medicine resident continuity clinic by at least 10% over 1 month, representing a statistically significant and clinically meaningful increase. Our secondary aim was to assess anchor nurse perceived workload in result communication as a direct consequence of improved patient portal enrolment.
Background
Recent reports have shown that patient access to the EHR via patient portals can help facilitate medication refills, coordinate appointments and billing activities,2 and can increase patient satisfaction by making clinical information, assessments and results readily available.3–5 Patient portal usage has been associated with improvement in chronic disease parameters6 and patient functional status,7 as well as with a reduction in high-cost healthcare utilisation in primary care practices.7 We are not aware of any published studies addressing the unique complexities of EHR patient portal use in a resident continuity clinic.
Measurement
Baseline measurement
A baseline audit showed that 35% or 570 patients out of 1628 total patients in 16 resident patient panels were enrolled in the patient portal. Anchor nurses completed surveys at baseline to determine the facilitators and potential barriers to effective implementation of the project. Survey items addressed their perceptions of their aligned residents’ timeliness of result notification and the frequency of patient concerns related to timeliness of result notification. Other survey items addressed the nurses’ current telephone call volume, time spent making and answering calls about patient test results, and time spent answering patients’ clarifying questions regarding test results. Nurses also were asked for suggestions to improve their workload as it related to patient results. At the end of the study, the same nurses also participated in semi-structured interviews to explain how the patient portal intervention affected (1) how residents responded to patient results, (2) patient call volume and (3) the amount of time spent making and answering telephone calls about patients’ test results.
Design
Our primary intervention was to introduce a standard patient portal sign-up process at the end of the patient rooming process. Nurses identified that one major barrier to patient portal enrolment was difficulty remembering the sign-up process in a long list of tasks necessary for ‘rooming’ a patient. Many intervention projects have used visual reminders to improve or change the behaviour of healthcare professionals.8–11 Similarly, to address this barrier, we implemented a visual reminder for the nurse to increase patient portal sign-ups. Further, by having the nurse launch an electronic sign-up page for patients at the end of the typical rooming process, it allowed the patient an opportunity to sign up while waiting for the physician, so the patients’ wait time would not be lengthened significantly.
Specific components of the intervention included: (1) placement of a visual reminder on exam room computer monitors (see figure 1), (2) creation of a script with visual aids to help nurses speak to patients about sign-up and find the sign-up button in the EHR, (3) placement of patient portal brochures with space to record the patient’s chosen log-on information in each exam room, and (4) education on the project for all nurses and attending physicians via email and regularly scheduled meetings.
Figure 1.

Visual reminder to enrol patients into portal system.
The primary end point was to increase patient enrolment significantly at the end of the first cycle.
Strategy
Our objective was to increase the number of patient portal enrolments in the IM resident continuity clinic at a large, academic medical centre using two distinct Plan-Do-Study-Act (PDSA) cycles. A PDSA cycle is a guide for improvement that maps small tests of change by planning the intervention, doing the intervention, studying the intervention for outcomes and modifying the intervention based on observation of outcomes.12 To reach our goal of a clinically meaningful and statistically significant increase in patient portal enrolments in the eligible resident clinic population, the two PDSA cycles were conducted over a 3-month period. Baseline data were gathered, identifying 570 patients of the 1628 eligible patients with active patient portal access (35%). To assess the change between baseline and 3-month follow-up in the proportion of patients who were enrolled in the portal system, a χ2 test of independence was performed. Statistical analysis was performed using SPSS (IBM SPSS Statistics V.21.0; New York, NY, USA), and significance was determined at the 0.05 alpha level. Additional baseline data in the form of surveys were gathered from four specific anchor nurses of the targeted resident continuity panels.
Pre-intervention survey results of anchor nurses revealed that they believed residents have difficulty responding to patient results in a timely fashion. Anchor nurses rated their call volume as moderate (not too many calls but a steady flow) to excessive (very high with too many calls). Two out of four nurses reported that they took too much time answering clarifying questions when calling patients about their test results. All nurses perceived that too much time is spent answering clarifying questions when calling patients about their test results. When asked for suggestions to reduce the nursing workload, the nurses shared that they believed that patient portal sign-up would help reduce the amount of time spent related to result communication.
PDSA cycle 1
Given baseline data, we identified four resident continuity clinic panels including 16 IM residents to study for a 4-week period. Specifically, we chose one panel of four residents to study each of the 4 weeks. This allowed us to learn each week what was going well and what our challenges were. Each week, four residents received preparatory refresher education on patient portal utility and function from their aligned attending. This occurred in person and via email. All nurses were reminded of the leadership initiative of 100% patient portal enrolment during a standing scheduled staff meeting. Visual reminders were placed on examination room monitors reminding the rooming nurses of our project initiative. All rooming nurses were directed to activate the portal-enrolment screen at the completion of the standard rooming process and invite the patient to enrol in the portal while awaiting their physician. Additionally, patients were offered an information card from nursing on the benefits of enrolment.
PDSA cycle 2
Given the positive results in cycle 1, our direct focus for cycle 2 was educational outreach to continue to enhance patient portal enrolment. At standing staff meetings, we provided additional education to clinic nurses. We also met with the attending physicians who supervise the residents in clinic and provided training on the sign-up process. Results from cycle 1 were relayed to all care team members. We heard feedback from the nursing team on ways to improve the process, many of which were implemented. For example, nurses relayed that signing patients up using a tablet instead of a desktop computer introduced complexity to the process. We shifted to only using desktop computers for sign-ups after hearing this feedback. Overall, the nursing team gave positive feedback about our interventions. We continued to monitor the specific 16 resident physician–patient panels for a duration of 4 weeks.
Results
Patient portal enrolment was measured for the 16 IM resident panels weekly. A Health Information Technology Services analyst provided electronic reports detailing the number of clinic patients who signed up for the portal during their appointment. Our team reported the enrolment numbers for each resident physician and compiled them for the two cycles.
At the end of PDSA cycle 1, patient portal enrolments increased from 570 to 625, representing a 9.6% increase over a 4-week period (X2(1)=1.19, p=0.27). Anchor nurse interviews indicated that the nursing workload was reduced significantly with the additional patient portal enrolments, which was perceived to be due to the decreased amount of time that was required to answer patients’ clarifying questions. Additionally, anchor nurses offered that the direct communication of clinical result information from the resident to the patient was valuable and enhanced the doctor–patient relationship.
At the end of PDSA cycle 2, 656 patients were active on the patient portal, which represents a 15.1% increase from baseline (X2(1)=7.37, p<0.01) (see figure 2). Interviews with the anchor nurses revealed several common themes about the implementation of the patient portal intervention. Nurses noticed positive changes in resident responsiveness to results in the form of increased patient portal messages and decreased telephone encounters. Nurses perceived improved patient understanding regarding results communication, noting fewer patient result-related questions. No patients reported concerns with patient portal communication of results. Further, nurses stated that patients shared unsolicited positive feedback about how happy they were with the prompt results. Nurses were pleased that the patient portal intervention seemed to decrease the time spent making and answering phone calls regarding patient results and clarifying questions.
Figure 2.
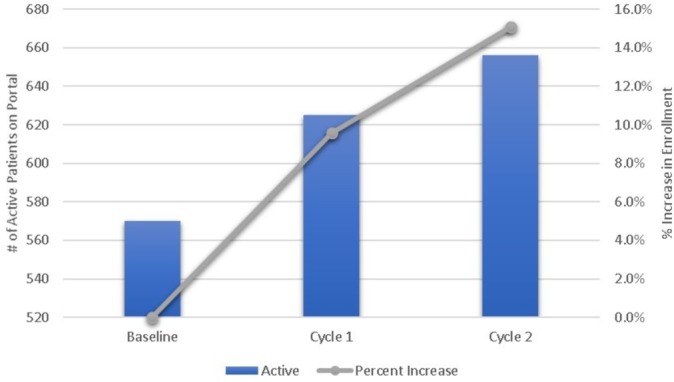
Patient portal enrolment.
Retrospectively, we looked at patient portal enrolment via portal activation rates across all 65 resident patient panels and compared it with the subset of 16 resident patient panels (figure 3). Patient portal activation rates were obtained using reportable data from the EHR. The rate of portal activation was calculated based on the number of patients with active patient portal status out of the number of patients with an IM resident listed as their primary care provider in the EHR. Baseline data showed that the activation rate across the entire resident patient population was 37% compared with a 35% activation rate for the subset of 16 residents in the study. One-month postcompletion of two PDSA cycles, the activation rate was 38% for all resident providers and the subset of 16 residents.
Figure 3.
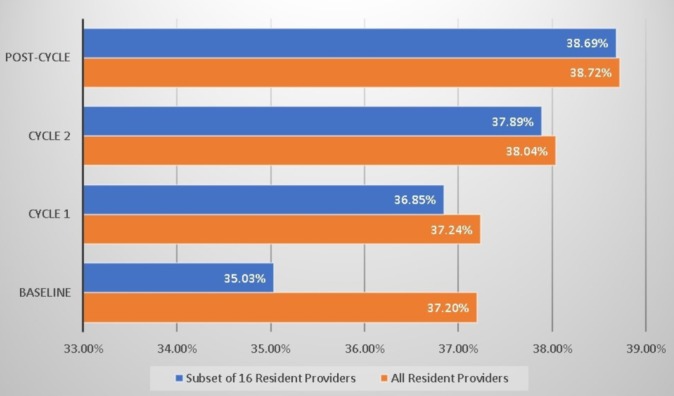
All resident panel activation rate.
Lessons and limitations
The project aim was twofold: to significantly increase patient portal enrolment and to evaluate nursing perceptions about patient portal utilisation on their workload in the ambulatory setting. Our findings demonstrated success in both aims with a simple, low-cost intervention. We encountered a few barriers. Some of our rooming nurses work in more than one clinic, and the intervention only occurred at our main campus location. We found that some nurses needed reminders from our clinic manager to continue to offer portal sign-ups. Our clinic manager sent reminders to nurses often, which is not a sustainable intervention. Additionally, we encountered patients who prefer more traditional means of communication from their physician, and we discussed a more realistic goal of having the majority of our patients enrolled in the portal, as opposed to all of them.
Our quality improvement project was conducted at a single academic medical centre, which is a limitation. However, this intervention would be easy to implement in other primary care academic settings that have similar hurdles with timely communication of patient test results in a resident continuity clinic setting.
This quality improvement project highlighted many positive lessons. Specifically, the use of two PDSA cycles allowed for the adaptability and reassessment of the project. Choosing a project that was important to leadership, clinicians and nurses functioned as a key component to the success of this project. A future investigation could include the effect of various incentives for physicians and nurses on enrolment rates. Future efforts should expand this quality initiative project to include multiple providers across different clinic settings to determine if our findings can be replicated. Additionally, while patient portal activation rates continue to increase, a future direction will be to evaluate how well patients manage their care and medical conditions once they actively engage via the patient portal.
Conclusion
This is the first report of an EHR patient portal enrolment intervention in a resident clinic patient population. Previous studies have evaluated patient portal use in academic specialty clinics,13 academic and non-academic primary care clinics,5 6 Veteran’s Health Administration clinics14 and other clinic settings, but studies involving resident primary care clinics are lacking.
Resident clinics pose unique challenges regarding provider to patient communication. We demonstrated that EHR patient portal enrolment in a large resident continuity clinic can be increased with a standardised, simple, low-cost intervention. We utilised existing clinic workflows and capitalised on previously unused patient wait time. We demonstrated how this intervention improved nursing satisfaction and nursing perception of phone call burden.
Because of the simplicity of the intervention, our clinic has continued sign-ups using this new workflow, and dissemination of the intervention has been achieved by incorporation of the process into onboarding and training of new nurses.
Future direction will be to continue to assess patient portal access and sustainability of the intervention. We plan to expand the analysis to include all 65 resident’s patient panels. Additionally, we plan to monitor the nursing workload as more patients are enrolled on the patient portal, potentially using more quantitative measures, such as electronic telephone call logs. We also plan to use the new academic year as a test of change for sustainability of the intervention.
Future PDSA cycles could also include involving residents in signing up their own patients, front desk staff assisting in sign-up and patient self-enrolment prior to their appointment.
Acknowledgments
The authors are particularly grateful to Beth Geist and Bethany Crum for their assistance and valuable suggestions during the development and implementation of this QI project. They thank Megan Larson for providing data regarding patient portal sign-up percentages. Special thanks go to anchor nurses, Kimberly Beem, Trisha Finn, Tracy McBratney and Sarah Wargin.
Footnotes
Contributors: BL and CR: initiated the project. BC, BL, CG, CR, CS and JB: study design. BL, CS, JB, SS and VW: performed the literature review. CG, CR and CS: designed the data collection tools. BL, CR, JB and VW: completed the abstract. CG: completed the nurse interviews; designed and conducted the statistical analysis, and wrote the strategy and results sections. CR and CS: facilitated the nursing surveys. BC, BL, CR, JB and SS: manually collected data regarding portal sign-ups weekly during cycle 1. CS: collected and managed the computerized data. All authors reviewed/edited all sections of the manuscript and approved the final version.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Ethics approval: According to the Kansas University Medical Center (KUMC) Human Subjects Committee, this work met criteria for quality improvement activity exempt from ethics review.
Provenance and peer review: Not commissioned; externally peer reviewed.
Patient consent for publication: Not required.
References
- 1. Poon EG, Gandhi TK, Sequist TD, et al. "I wish I had seen this test result earlier!": Dissatisfaction with test result management systems in primary care. Arch Intern Med 2004;164:2223–8. 10.1001/archinte.164.20.2223 [DOI] [PubMed] [Google Scholar]
- 2. Young HM, Nesbitt TS. Increasing the capacity of primary care through enabling technology. J Gen Intern Med 2017;32:398–403. 10.1007/s11606-016-3952-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Bashshur RL, Howell JD, Krupinski EA, et al. The empirical foundations of telemedicine interventions in primary care. Telemed J E Health 2016;22:342–75. 10.1089/tmj.2016.0045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Rozenblum R, Donzé J, Hockey PM, et al. The impact of medical informatics on patient satisfaction: a USA-based literature review. Int J Med Inform 2013;82:141–58. 10.1016/j.ijmedinf.2012.12.008 [DOI] [PubMed] [Google Scholar]
- 5. Wald JS, Businger A, Gandhi TK, et al. Implementing practice-linked pre-visit electronic journals in primary care: patient and physician use and satisfaction. J Am Med Inform Assoc 2010;17:502–6. 10.1136/jamia.2009.001362 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Osborn CY, Mayberry LS, Wallston KA, et al. Understanding patient portal use: implications for medication management. J Med Internet Res 2013;15:e133 10.2196/jmir.2589 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Sorondo B, Allen A, Fathima S, et al. Patient portal as a tool for enhancing patient experience and improving quality of care in primary care practices. EGEMS 2016;4:1262 10.13063/2327-9214.1262 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Etter JF, Rielle JC, Perneger TV. Labeling smokers' charts with a "smoker" sticker: results of a randomized controlled trial among private practitioners. J Gen Intern Med 2000;15:421–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Ritchie S, Scanlon N, Lewis M, et al. Use of a preprinted sticker to improve the prescribing of prophylactic antibiotics for hip fracture surgery. Qual Saf Health Care 2004;13:384–7. 10.1136/qshc.2003.009696 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Melendez-Rosado J, Thompson KM, Cowdell JC, et al. Reducing unnecessary testing: an intervention to improve resident ordering practices. Postgrad Med J 2017;93:476–9. 10.1136/postgradmedj-2016-134513 [DOI] [PubMed] [Google Scholar]
- 11. Kumar P. Improving timely medical reviews for patients discharged from intensive care. BMJ Qual Improv Rep 2015;4:u207871.w3816 10.1136/bmjquality.u207871.w3816 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Reed JE, Card AJ. The problem with Plan-Do-Study-Act cycles. BMJ Qual Saf 2016;25:147–52. 10.1136/bmjqs-2015-005076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Mendel A, Chow S. Impact of health portal enrolment with email reminders at an academic rheumatology clinic. BMJ Qual Improv Rep 2017;6:u214811.w5926 10.1136/bmjquality.u214811.w5926 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Fix GM, Hogan TP, Amante DJ, et al. Encouraging patient portal use in the patient-centered medical home: three stakeholder perspectives. J Med Internet Res 2016;18:e308 10.2196/jmir.6488 [DOI] [PMC free article] [PubMed] [Google Scholar]