

Abstract
Objective
Negative views of the both the self and the world are commonly seen in individuals who have suffered psychological trauma. These negative cognitions are thought to be significant as they are likely to play a critical role in furthering, if not promoting, other symptoms and exacerbating the dysfunction sometimes seen after a traumatic event. This has led to the inclusion of “Persistent negative beliefs and expectations about oneself or the world” in the DSM-5 (APA, 2013). While there is considerable self-report and behavioral evidence for negative biases after trauma, there is less concurrent neurophysiological data. This study used the N400, an event related potential sensitive to semantic expectancies, to assess negative expectations in a trauma sample.
Method
In this study, thirty-nine participants completed an N400 task in which they read ambiguous sentence stems that ended either with a positive final word (Things will turn out….fine) or a negative final word (Things will turn out…badly). We predicted that those trauma survivors with negative cognitions (as measured by the PTCI: Foa et al., 1999) would show N400 amplitudes indicating expectancies for negative endings. Augmenting the previous self-report data, this would provide evidence for negative expectancies that are fairly early and relatively automatic.
Results
N400 amplitudes to negative sentence endings were significantly related to negative views of the world as measured by the PTCI.
Conclusions
This suggests that negative world views in trauma survivors have demonstrable neurophysiological correlates and impact on expectations in ambiguous situations.
Keywords: Posttraumatic Stress Disorder, Negative Expectancies, Bias, Trauma, N400
Introduction
Using DSM-5 criteria, recent research suggests that prevalence rates for psychological trauma are as high as 90% in the U.S. population (Kilpatrick, Resnick, Milanak, Miller, Keyes, & Friedman, 2013). While most of the individuals who experience such an event do not go on to develop significant psychopathology such as PTSD, others develop a more chronic reaction to the event that severely disrupts their ability to return to their previous lifestyle (Kilpatrick et al., 2013; Tanielen & Jaycox, 2008; Brewin, 2003; McFarlane & Potts, 1999). Although chronic responses to a traumatic event are not as common as the acute reactions, the National Stressful Events Survey (Kilpatrick et al., 2013) and the National Comorbidity Study (Kessler et al., 1995) found estimated lifetime prevalence for PTSD at 8.3% (DSM-5) and 7.8% (DSM-IV) respectively in U.S. adults.
For those that do develop a chronic reaction to traumatic events, the impact on their lives is considerable. The effects of trauma can include a range of signs, symptoms, and behaviors that include increased arousal states, avoidant coping strategies, and recurrent distressing recollections of the event (American Psychiatric Association, 2013). Included among these concerns are biases in both attention and expectation. Attentional biases after trauma have attracted a tremendous amount of focus in the past two decades in the form of behavioral paradigms, such as the modified Stroop tasks, dot probe tasks, and event related potential tasks like the auditory oddball or mismatch negativity tasks (Kimble, Frueh, & Marks, 2009; Buckley, Blanchard, & Neill, 2000; Dalgleish et al., 2003, Pineles, Shipherd, Welch, & Yovel, 2007; Kimble, Fleming, Bandy, Kim, & Zambetti, 2010; Metzger, Orr, Lasko, & Pitman, 1997; Karl, Malta, & Maercker, 2006). As a whole, this work has supported an automatic processing bias toward threatening information consistent with long standing reports of hypervigilance after trauma.
Somewhat less theoretically and empirically established is the concept and symptoms of a negative expectancy bias. The term negative expectancy bias, as used in the conditioning literature, refers rather specifically to an overestimation of negative outcomes after being exposed to threat-relevant stimuli (Cavanaugh & Davey, 2000; Olatunji, Cisler, Meunier, Connolly, & Lohr, 2008; McNally & Heatherton 1993). In applied work, the term is used somewhat more broadly to refer to a cognitive tendency to interpret ambiguous stimuli negatively or to predict negative outcomes from neutral events. A general appreciation for how trauma can generate negative expectations has long-standing roots in the trauma literature. In the earliest versions of the PTSD diagnosis, the DSM included a “foreshortened sense of future” (American Psychiatric Association, 1980) in which survivors did not expect a career, marriage, or a long life. Since that earliest conceptualization, the concept of negative expectancies has broadened to include a range of appraisals that go beyond an assessment of the future. Theoretically, the cognitive model of Ehlers and Clark (2000) has delineated the nature and effects of negative expectancy biases in trauma survivors. Expanding on literature suggesting that post-trauma cognitions involved perceiving the world as dangerous and the self as negative (Janoff-Bullman, 1989; Foa, Steketee, & Rothbaum, 1989), Ehlers and Clark argue that excessive negative appraisals of the trauma and its sequelae contribute to a sense of ongoing, serious threat. These negative appraisals have consistently been hypothesized to be associated with hyperarousal, re-experiencing symptoms, and avoidance behavior (Bomyea, Risbrough, & Lang, 2012; Mitchell, Brennan, Curran, Hanna, & Dyer, 2017)
Understanding negative appraisals is critical because they are prevalent and highly correlated with posttraumatic pathology (Cox, Resnick, & Kilpatrick, 2014; Foa, Ehlers, Clark, Tolin & Orsillo, 1999; Smith & Bryant, 2000; Warda & Bryant, 1998). Cox et al. (2014) found that DSM-5 D2 symptoms (persistent negative expectations of self and world) was present in 24% of all trauma survivors and 75% of those with a PTSD diagnosis. Such negative expectancies have been shown to predict subsequent PTSD after exposure to a trauma (Beevers, Lee, Wellis, Ellis, & Telch, 2011; Disner et al., 2013; Dunmore, Clark, & Ehlers, 1999; Ehlers, Mayou, & Bryant, 2003; Engelhard, de Jong, van der Hout, & van Overveld, 2009; Engelhard, van den Hout, Arntz, & McNally, 2002). While there has been considerable self-report work in this area, there has been relatively little research investigating behavioral, neurophysiological, or biological correlates of negative expectancies. Doing so may have important implications for a better understanding of the disorder as well as avenues for treatment. For example, behavioral or neurophysiological tasks can produce data about expectancies that are less vulnerable to demand characteristics, social desirability biases, and malingering. In addition, inexpensive and quick assessments of expectancy bias could be quite valuable in treatment outcomes studies to investigate the impact of treatment on discrete cognitive changes. In general, new and innovative ways of understanding this phenomenon are important for the advancement of the field.
Event-related brain potentials, a measure of averaged brain electrical activity, have served as a tool to investigate neurophysiological correlates of behavior in individuals both with and without psychological disorders and thus may help to clarify aspect of post-trauma cognitive processes. This is because the amplitude and latency of ERPs can vary systematically as a function of ongoing cognitive processes (Andreassi, 1995). For example, ERP components change with stimulus relevance, subjective probability, expectancy, and semantic congruity (Johnson, 1986; Kutas & Hillyard, 1980; Tecce & Cattanach, 1987). The fact that one ERP component, the N400, varies as a function of semantic expectancy makes it a promising tool for studying negative appraisals after trauma. The N400 is a negative going waveform that peaks approximately 400 milliseconds (ms) after stimulus onset and is sensitive to incongruities in semantics and meaning. The N400 has been theorized to index the integration of a stimulus into a given context, with larger N400s occurring to stimuli that require more cognitive effort for integration (Kutas & Federmeier, 2011; Rugg, Doyle, & Holdstock, 1994). This effect occurs because context serves to pre activate meaning and facilitates subsequent stimulus processing. When violations of context occur, more effort is needed to retrieve information from semantic memory, resulting in a larger N400.
If individuals with PTSD expect threat and are vigilant for it, as indicated in the clinical and empirical literature, they might maintain different expectancies for how ambiguous stimuli, including ambiguous sentence stems, might end. We explored this hypothesis (Kimble, et al., 2002) in a non-N400 study, in combat veterans using a sentence completion task. In this task, veterans with and without PTSD filled out unfinished sentence stems that could be sensibly completed with words that were either trauma or not trauma related. For example, the sentence stem “The field was littered with ______” could be sensibly completed with the word “trash” or with a word such as “bodies”. Those veterans with PTSD completed the ambiguous sentence stems with trauma relevant (i.e., military) endings more frequently than did veterans without PTSD. This suggests that veterans with PTSD were using existing biases to interpret ambiguous sentence stems. The study was limited however insofar as participants could easily identify the demand characteristics and alter their responses.
In an N400 version of the above sentence task, we were able minimize this limitation while providing further evidence for a negativity bias (Kimble, Batterink, Marks, Ross, & Fleming, 2012). In that study, trauma survivors read sentences off a computer screen that had either a threatening final word or a neutral final word. Individuals with PTSD demonstrated small N400s to threatening endings compared to those without PTSD in contrast to their larger N400s to neutral final words. This finding suggested that those with PTSD expected negative endings and this was reflected in their neurophysiological response. The smaller N400 to the negative endings would indicate that they were primed for such an ending. However, a limitation of that study was that it included a majority of combat veterans and that the threatening sentences endings were mostly combat related. Therefore, participants were primarily male and the trauma sample limited.
The current study was designed to improve on the previous study in a number of ways. First, we intended to explore whether we could replicate the previous findings in a mixed trauma that included a larger percentage of females and non-military participants. In addition, we used sentence endings that were generally negative (He thought things would turn out….badly) as opposed to specifically negative in a military context. This design also allowed to control for emotional valence in that the comparison sentences were generally positive as opposed to neutral (He thought things would turn out…well). A replication using this paradigm with this sample would demonstrate the robustness of the effect, the paradigm's broader applicability, and the capacity to measure negative expectancies across a range of traumas.
In addition, we used the Posttraumatic Cognition Inventory to precisely identify the cognitions that might be reliably associated with neurophysiological indicators of a negative expectancy bias. Because PTSD has a heterogeneous presentation, with multiple symptom clusters and variable trauma types, it is unlikely that the overall diagnosis, would reliably covary with a fairly specific cognitive symptom (i.e., negative expectations). In the DSM-5, “persistent negative beliefs and expectations about oneself or the world” is one of only twenty symptoms of the disorder. In order to study this phenomenon in trauma survivors better, a more precise index is required.
Finally, the value of this work lies in its ability to assess negative expectations using a neurophysiological measure rather one that is self-report. Self-report data is valuable as it can reflect the subjective experience of the individual, but it is also quite vulnerable to demand characteristics and malingering in ways that this neurophysiological data is not. Second, the fact that discriminations are made within 500 milliseconds indicates that these biased expectations are reflected in the earliest stages of cognitive processing. A small N400 to negative endings would represent top down influences that impact cognitive processing almost immediately. For clinicians and researchers alike, such data would highlight how embedded negative cognitions are to even ambiguous stimuli. Such data would suggest that the work of clinicians comes in changing the negative expectations that automatically bias the processing of neutral or ambiguous information as threatening or negative.
To investigate whether the negative expectations can be indexed neurophysiologicially, we used subscales of the PTCI (Negative views of Self, Negative Views of the World, and Self Blame) to see which best predicted N400 amplitudes to negative endings. We predicted that negative expectancies, as measured by the PTCI, would predict smaller N400s to the negative sentence endings but not predict N400 amplitudes to positive or incongruent endings. These smaller N400s to negative final words would suggest a fairly automatic expectancy for negative outcomes to the ambiguous sentence stems.
Methods and Materials
Participants
The participants in this study were 46 members of the surrounding community who responded to a CraigsList® advertisement or flyers hung on local community boards. The ads and flyers asked for individuals who have experienced some type of psychological trauma to participate in a study for $70.00. Interested participants called and were screened over the phone for eligibility. Because the study involved EEG assessment, participants were screened out for a history of head injury associated with a loss of consciousness, any neurological disorder, any medications that might affect an EEG, current substance abuse, history of substance dependence, epilepsy or seizures, history of fever over 104 degrees, or history of significant malnutrition. All participants were between 18 and 70 years of age. Participants could be male or female, of any racial background, and either left or right handed. Of the 46 participants who came into the lab, data from seven additional participants could not be used either because of subsequent discovery of exclusionary criteria or unusable EEG data, leaving a sample of 39 who completed the entire protocol.
The average age of the participants was 36.6 (15.4) years of age. Twenty participants were female, 19 were male. The sample, on average, completed a partial college education. All participants reported at least one item on the Trauma Experiences Scale (TES: Vrana & Lauterbach, 1994). Traumas included natural disasters, motor vehicle accidents, physical or sexual assault, exposure to combat, and nearly losing one's life. Twenty-one of the 39 reported physical or sexual abuse as a child. The average number of different traumas endorsed on the TES was 4.51 (SD=1.97).
Procedure
Psychometrics and Demographics
The project was approved by the local Institutional Review Board and all participants started their participation by signing the study consent form. Then they completed with the investigator basic demographic information and the Vrana-Lauterbach Traumatic Events Scale. Participants then completed a number of study psychometrics which included the Posttraumatic Stress Scale (PSS: Foa, Riggs, Dancu & Rothbaum, 1993). The PSS is a 17-item scale that directly assesses the DSM-IV criteria for PTSD. It has been found to have high reliability and validity and a score above 14 has been found to be consistent with a diagnosis of PTSD (Coffey et al., 2006). In this sample, 18 of the 39 participants had a score above 14 on the PSS and were placed in the high PSS group as compared to 21 placed in the low PSS group. The PSS was used primarily to place individuals into “high” and “low” PTSD “groups.” The participants also completed the Posttraumatic Cognitions Inventory (PTCI: Foa et al., 1999). This is a 36-item inventory that assesses negative cognitions about the self, negative cognitions about the world, and self-blame. This instrument was used for regression analyses in order to increase precision in the prediction of ERP responses to negative final words.
N400 Sentence Paradigm
Each participant read 60 sentences off a computer screen presented one word at a time. Sentences ranged from 5 to 9 words and each word appeared on the screen for 1000 ms with a 200 ms interstimulus interval between words. The final word of each sentence was presented for 3000 ms, followed by a 200 ms ISI, after which an asterisk appeared. The asterisk indicated that the participant should push the “Yes” button if the sentence made sense and a “No” button if it did not. Following the button-press from participants, a second asterisk was presented for 3000 ms before the next trial began. The entire task was programmed using SuperLab® stimulus presentation software (Cedrus Corporation, San Pedro, CA) with digital outputs sent to the analysis software.
The sentences used in this study were different than those used in our previously published study (Kimble et al., 2012). The current sentences reported in this study were designed to be applicable to a mixed trauma sample. In all, twenty sentences stems were presented three times each and each time ended either with 1) an incongruent final word (“She found the stranger to be orange”), or 2) a congruent positive ending (“She found the stranger to be friendly”), or 3) a congruent negative ending (“She found the stranger to be threatening”). Incongruent sentences had final words that were semantically nonsensical. Both the positive and negative congruent final words made sense syntactically and semantically. The only difference between the positive and negative congruent final words was the valence of their final words. Negative sentences ended with negative final words. Positive sentences ended with positive final words. Final words averaged 6.67 letters and across the three conditions were equated for word length, number of syllables, and frequency in the English language (Kucera & Francis, 1967). The order of the trials throughout the paradigm was randomized to avoid confounding variables such as fatigue and order effects.
ERP acquisition, filtering, averaging, and analyses
To begin the EEG procedure, participants were asked to sit approximately 1.5 meters from a 21-inch computer monitor. They were connected, via an electrode cap (ElectroCap International, Eaton OH) to the BioSemi Active II system (Amsterdam, Netherlands). Electrode gel was placed in each electrode site in the cap to ensure optimal conductivity. All electrode offsets were within 40 mV, the acceptable range as recommended by the manufacturer. The 32 active electrodes and two mastoid reference electrodes were connected to the A/D converter box which sent signals along to the acquisition computer installed with ActiView software.
When the participant was ready to begin the task, the researchers explained the paradigm. Participants were asked to remain still as they silently read each word that appeared on the computer screen. After the sentence was completed, participants pressed either a “yes” or “no” button to indicate if they thought the sentence “made sense”. All 60 sentences took approximately 20 minutes to present. Upon completion of the task, participants were debriefed and were given the PI's contact information if they had any further questions or concerns. Following the debriefing session, each participant received $70 each for participating in the study.
EEG was continuously recorded from 32 channels using a BioSemi Active II amplifiers and electrodes manufactured by BioSemi (Amsterdam, Netherlands). Active electrodes were embedded in an elastic cap at standard distances consistent with American Electroencephalographic Society Guidelines (Pivik et al., 1993). The EEG was measured using a combined ground/reference (CMS/DRL) circuit. EEG was digitally sampled at 1024 Hz.
Data was stored off line and analyzed using Brain Electrical Source Analysis Software (BESA: Megis Software, Grafelfing, Germany). The data was baseline corrected and filtered at .1 to 30 Hz. Continuous EEG was epoched with 100 ms pre-stimulus baseline and continued for 1000 ms post stimulus. Eye blinks were removed using BESA eye blink correction routines. Trials were then averaged using an artifact rejection routine in which trials with amplitudes greater than 120 uV were removed from analyses. N400 amplitude was measured as the most negative peak between 300 and 600 ms with baseline established as the average voltage between -100 and 0. The loss of over 50% of the trials due artifact for any given condition resulted in the removal of the participant from the study. As a result, six participants were removed.
Data Reduction and Analyses
In order to avoid spurious findings associated with a single electrode, analyses were done across a number of central electrode sites. For analyses in which “Electrode” was a within subjects factor, Cz, FC1, FC2, CP1, CP2 electrodes were used. For multivariate analyses, in which only one outcome variable could be used, Cz and its four surrounding electrodes (FC1, FC2, CP1, CP2) were averaged together to create a central montage. This is consistent both with convention, in which the N400 is typically largest at central sites, and our own data in which we saw largest amplitudes at Cz. This also avoided reporting effects that could be due to values at a single site.
Testing Assumptions for Multivariate Analyses
We tested for violations of the underlying assumptions for multivariate analyses. All independent and dependent variables were normal in their distribution and were acceptable with respect to kurtosis and skew. No variable needed to be transformed. While the bivariate correlations in Table 1 show that the predictors were significantly correlated, they did not violate guidelines of multicollinearity as measured by SPSS statistics tolerance indicators and variance inflations indexes.
Table 1. Bivariate Correlations (n=39).
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| Mean | 36.7 | 4.2 | 2.5 | 2.8 | -.31 | .46 | -2.7 | 15.4 |
| SD | 15.4 | 1.6 | 1.3 | 1.7 | 3.6 | 3.9 | 3.5 | 10.8 |
| 1. Age | -- | -.26 | -.14 | -.32* | -.35* | -.13 | -.10 | -.05 |
| 2. PTCI-World | -- | .45* | .37* | .43* | .24 | .19 | .46* | |
| 3. PTCI-Self | -- | .59* | .17 | .00 | .07 | .55* | ||
| 4. PTCI-Self Blame | -- | .21 | .15 | .24 | .32* | |||
| 5. Neg. N400 | -- | .57* | .38* | .01 | ||||
| 6. Pos. N400 | -- | .31 | .02 | |||||
| 7. Inco. N400 | -- | .16 | ||||||
| 8. PSS | -- |
p<.05
Results
Manipulation Check
In standard N400 paradigms, sentence stems with unexpected (incongruent) final words demonstrated larger amplitude (more negative) N400s compared to those with expected (congruent) final words. Our paradigm demonstrated this effect. See Figure 1. This analysis is highlighted separately here in order to emphasize the presence of the effect when using our novel, non-standard N400 task. This effect was tested using Condition × Electrode ANOVA with Condition (Congruent Positive vs. Congruent Negative vs. Incongruent) as one factor and Electrode (Cz, FC1, FC2, CP1, and CP2) as the second factor. Those sentences with incongruent final words had significantly larger N400s than did sentences that ended with congruent final words, [Condition effect: F(2,37)=10.60; p<.01, η2=.36]. Follow up analyses confirmed that the incongruent condition was significantly more negative than both the congruent positive and congruent negative conditions. When comparing just the incongruent condition versus the congruent positive condition, the effect was significant, F(1,38)=20.60, p < .01, η2=.35. The same effect for Condition was found when comparing the incongruent final words to the congruent negative endings, F(1,38)=14.24, p<.01, η2=.27.
Figure 1.
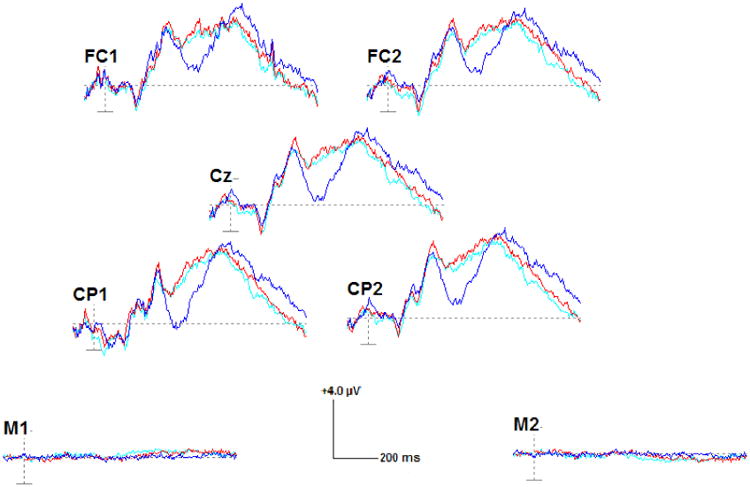
ERP waveforms to the positive congruent (light blue), negative congruent (red), and incongruent (dark blue) conditions.
We also investigated, again in the entire sample, whether there was a difference in N400 amplitude between the congruent positive endings and the congruent negative endings. We predicted that there would be no difference in the overall sample. If there were a difference between these two conditions, particularly in those without pathology, this would likely represent poorly designed sentences in which one type of congruent sentence was less expected than the other congruent sentence type. Analyses suggest that while both congruent sentence types were different from the incongruent condition, they were not different from each other, F(1,38)=1.99, p>.05, η2=.05.
Bivariate Correlations: Psychometrics and Demographics
Psychometric instruments performed as would be expected. See Table 1 for the correlation matrix. All PTCI (World, Self, and Self Blame) subscales correlated significantly and positively with each other. The Self-Blame subscale on the PTCI also correlated significantly and negatively with age (r=-.32, p<.05), suggesting that individuals blame themselves less as they got older which may be a function of the amount of time since trauma.
Analysis of Variance: Group differences
In an effort to replicate our 2012 findings, differences between those high and low on the PSS scale were tested using a 2 × 3 × 5 mixed model, repeated measures ANOVA. Group (PTSD v. No PTSD) was the between subjects factor and Condition (Incongruent v. Congruent Positive v. Congruent Negative) and Electrode (Cz, FC1, FC2, CP1, CP2) were the within subjects factors. This analyses using a central montage directly comparable to the 2012 study. There were no overall Group effects [F(1,37)=0.27, p>.05, η2=.01] nor were there any interactions with Group. A replication of our previous work would have been supported by a Group × Condition effect, which would have specifically tested whether the groups differed to the negative condition, but it was not significant, F(2,36)=0.24, p>.05, η2=.01). Similarly, the effect was not present at any particular electrode; Group × Condition × Electrode [F(8,30)=0.65, p>.05, η2=.15].
Regression Analyses 1: Predictors of N400 amplitude to negative endings
The relationship between N400 amplitudes to the negative endings and the PTCI scores were tested using a hierarchical multiple regression in which age was entered first and PTCI-Self, PTCI-World, and PTCI-Self Blame were entered second. Twenty-five percent of the variance in N400 amplitude to negative congruent endings was accounted for by age and PTCI score. R was significantly different from zero, F(4,38)=2.77, p<0.05. In the first step age predicted smaller N400s to negative endings (t=-2.29, p<0.05) but was no longer significant in the second step (t=-1.57, p>0.05). In the second step, however, PTCI-World scores were significant (t=2.19, p<.05). See Figure 2, Table 2.
Figure 2. Negative congruent N400 amplitudes as a function of PTCI-World Scores.
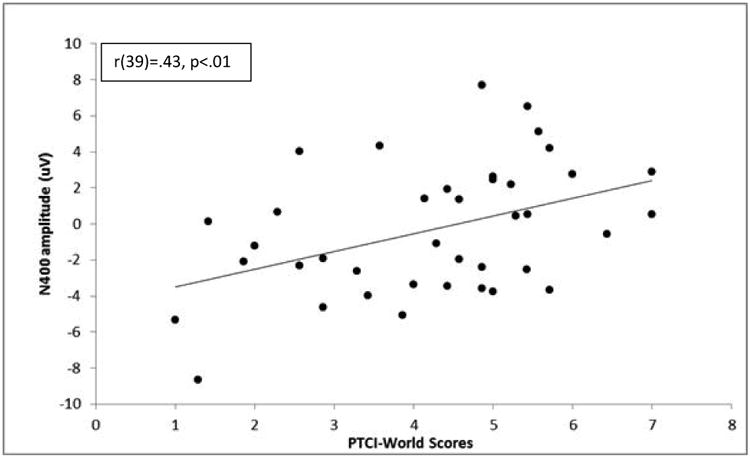
Table 2. Summary of Hierarchical Regression for Variables Predicting N400 Amplitudes to Negative Final Worlds.
| Variable | B | SE B | β | t | Sig |
|---|---|---|---|---|---|
| Step 1 | |||||
| Age | -.08 | .04 | -.35 | -1.57 | .13 |
| Step 2 | |||||
| PTCI-Self | -.15 | .56 | -.05 | -.27 | .79 |
| PTCI-World | .87 | .40 | .38 | 2.18 | .04* |
| PTCI-Self Blame | .05 | .41 | .02 | .12 | .90 |
Note: R2=.25,
p<.05
Regression Analyses 2: Predictors of N400 amplitude to positive endings
The same regression model was used to predict the N400 to congruent positive endings. Only nine percent of the variance could be explained and R was not significantly different from zero, F(4,38)=.86, p>.05.
Regression Analyses 3: Predictors of N400 amplitude to incongruent endings
The same regression model was used to predict the N400 to incongruent endings. Again, only nine percent of the variance could be explained, and R was not significantly different from zero, F(4,38)=.83, p>.05.
Discussion
In this study, expectancies, as measured by N400 amplitudes, varied as a function of negative world views. In particular, N400 amplitudes during the negative trials were smaller in those participants who had more negative views of the world as measured by their PTCI-World scores. This finding suggests that those with more negative world views expected the ambiguous sentence stems to end negatively, i.e., those with more negative world views were “primed” to expect negative outcomes. An ambiguous sentence stem, at least in the context in which negative endings might occur, seemed to generate negative expectations in those who scored high on the PTCI-World scale.
This interpretation is further supported by recent N400 data suggesting that the N400 is also sensitive to violations of fact or “world knowledge” (Van Berkum, 2009; also see Kutas & Federmeier, 2011 for a brief review of this issue). As Kutas and Federmeier (2011) point out, Dutch participants produce a large N400s to sentences such as “Dutch trains are white and very crowded” because Dutch trains are yellow. This suggests that individuals can bring their personal experience to generate expectations and this can be reflected in N400 amplitudes. It would be a similar “top-down” process that would likely generate small N400s to negative endings in those with high PTCI-World scores. Because the sentence stem itself is ambiguous, the broader context (in this case the individuals' perceptions of the world) impact N400 amplitudes. This process is likely automatic and unintentional, certainly relative to the manner in which negative expectancies are typically measured by self-report. (Wang et al., 2015). While there is some argument among neurophysiologists regarding the automaticity of the N400, there is little indication that an individual could exert control over N400 amplitudes. While it would be possible for an individual to bias self-reports and even certain behavioral responses, there is no evidence that they could influence the N400 response. Therefore, the data provide objective evidence for the negative expectancies in some trauma survivors.
While the N400 varied as function of world views, it is not clear why the N400 was not related to negative views of the self or self-blame as measured by the PTCI. We would have predicted that negative views of the self would also have been related to N400 amplitudes to negative endings as well. Many of the sentence stems referenced negative views of the self, not just negative views of the world. For example, our stimuli included the following sentences: “Basically, I feel that I am …worthless” (congruent negative) vs. “valuable” (congruent positive) vs. “watered” (incongruent). Despite the self-oriented sentences, it was only world scores that were uniquely predictive of N400 amplitude to negative endings.
We can only speculate as to why this is the case, although it may be related to our mixed trauma sample. While almost all traumas are likely to result in seeing the world as dangerous (i.e., combat, natural disasters, motor vehicle accidents, sexual assault), only certain types of trauma are likely to lead negative views of the self (i.e., sexual assault, child abuse: Freyd, 1996; Branscombe, Wohl, Owen, Allison, & N'gbala, 2003; Miller, Handley, Markman, & Miller, 2010; Mokma, Eshelman, & Messman-Moore, 2016). While the majority of participants may have had a negative view of the world, there may not have been enough individuals in the sample with negative views of the self to generate a significant effect. This would be supported by the fact that negative world views (M=4.2, SD=1.6) were more prominent and significantly higher in this sample than were negative views of the self (M=2.5, SD=1.3) or self-blame (M=2.8, SD=1.7). This pattern in the data may have resulted in an effect that was present for world views that were not there for self-views.
While this study revealed some novel associations between N400 amplitude and world views, it did not replicate the findings of a previous study in which N400 amplitude was related to PTSD status (Kimble et al., 2012). While our findings are generally consistent with that finding, as those with PTSD reliably report higher PTCI-World scores, we could not replicate that previous work. In this case, the more specific symptom profile was necessary to identify a relationship.
This is understandable in light of the fact that PTSD is a heterogeneous disorder with four separable symptoms clusters, none of which specifically assess negative views of the world. This is particularly true in that the PSS version used in this study was consistent with DSM-IV criteria in which only the symptoms of hypervigilance and foreshortened sense of future are conceptually related to negative expectancies. Having said that, the previous study had those same limitations and still found that those with PTSD had smaller N400s to negative endings. However, that study did differ from the current study in three significant ways, and these factors may have contributed to a PTSD effect present in the first study that could not be replicated in our current work. First, the previous study had more combat veterans and used sentences from a previous study in which the completion (“cloze”) probability was determined using military related sentences completed by veterans. There is growing evidence that the type of trauma, separate from the development of PTSD, can have impact on a whole range of outcomes including cognitions and neurophysiology (Vythilingham et al., 2002; Vythilingham et al., 2005; Karl et al., 2006; McEwen & Lasley, 2007). For example, we had found that trauma in and of itself impacted on P300 amplitude in military cadets (Kimble, Fleming, & Bandy, 2010) and that deployment to a warzone had as much impact on hypervigilance symptoms as did PTSD status (Kimble, Fleming, & Bennion, 2013). Second, this study used generally negative sentences rather than trauma specific sentences. Finally, the first study diagnosed individuals using the Clinician Administered PTSD Scale (CAPS: Blake et al., 1995) rather than a cut-off of 14 using the PSS. As used in this study, the PSS has limitations as a diagnostic tool. In addition, this sample may have had less severe symptoms with an average PSS score of 15.4 (10.8) that was lower than in the previous sample (M=19.2, SD=14.1).
Implications
These findings have a number of implications worth considering. The first is that the work demonstrates how early and automatic evidence for these types of biases can be. While some neurophysiologists might argue with the definition of automatic, we use it to highlight how evidence for the biases are 1) present at the earliest stages of cognitive processing, 2) resistant to demand characteristics, malingering, and social desirability biases. This is particularly true relative to self -reports regarding posttraumatic negative appraisals such as the PTCI. For both clinicians and researchers alike, such data suggest that those with negative world views are not consciously deciding to look at outcomes negatively. Such negative world views do not appear to be a part of some deliberative process but are implicit and represent a cognitive frame or schema that influence the interpretation on incoming information. Therefore, the identification of such negative schemas and a recognition of their impact on the interpretation of events is an important target for treatment.
Further, the data suggest that this may be particularly true in situation that are ambiguous or may have uncertain outcomes. While some events are clearly of negative or positive valence, ambiguous events present a distinct opportunity for schemas to impact on appraisal. Many everyday events, such as facial stimuli, body posture, tone of voice, or the outcome of a future event are frequently ambiguous. Such experiences would be challenging for those with the types of biases seen in this study. Negative appraisals of neutral events could initiate a feedback loop that is not likely to initiate functional behavior. As a result, an individual may not respond in an appropriate manner or be willing to persist in an effort that is worthwhile. Such negative evaluations are likely to result in withdrawal or aggressive responses that further exacerbate circumstance and end up confirming the initial negative belief.
Finally, this paradigm could be valuable in treatment outcomes studies that target negative cognitions and appraisals. Because the paradigm is not vulnerable to demand characteristics or social desirability biases, with further study, it could serve as a useful index. In a prospective design, a measure like the N400 could potentially predict either treatment recovery or treatment resistance. For example, it is possible that negative appraisals at the outset of treatment might inhibit treatment compliance, belief in treatment efficacy, and persistence. At the conclusion of a study, the paradigm could be used to evaluate the effectiveness of an intervention.
Conclusions
In this study, there was evidence to suggest that neurophysiological indicators of expectation varied as a function of negative world views. Those participants who reported more negative views of the world on the PTCI had smaller N400s to negative endings. These finding suggests that those with more negative world views were primed to expect negative outcomes. This is consistent with “persistent negative expectations” found in the DSM-5 and provides confirmatory and measurable neurophysiological evidence for the phenomena.
Acknowledgments
This publication was made possible by an AREA Grant (R15 MH081276) to Matthew Kimble from the National Institute of Mental Health. Thank you to Andrew Hyatt and Cade Schreger for technical assistance on the project.
Contributor Information
Matthew Kimble, Department of Psychology, Middlebury College.
Abhishek Sripad, Program in Neuroscience, Middlebury College.
Rachel Fowler, Program in Neuroscience, Middlebury College.
Sara Sobolewski, Program in Neuroscience, Middlebury College.
Kevin Fleming, Department of Psychology, Norwich University.
References
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 3rd. Washington, DC: American Psychiatric Association; 1980. [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th. Washington, DC: American Psychiatric Association; 2013. [Google Scholar]
- Andreassi JL. Psychophysiology: Human behavior and physiological response. 3rd. Hillsdale, NJ, England: Lawrence Erlbaum Associates, Inc.; 1995. [Google Scholar]
- Beevers CG, Lee H, Wells TT, Ellis AJ, Telch MJ. Association of predeployment gaze bias for emotion stimuli with later symptoms of PTSD and depression in soldiers deployed in Iraq. The American Journal of Psychiatry. 2011;168(7):735–741. doi: 10.1176/appi.ajp.2011.10091309. [DOI] [PubMed] [Google Scholar]
- Blake DD, Weathers FW, Nagy LM, Kaloupek DG, Gusman FD, Charney DS, Keane TM. The development of a clinician-administered PTSD scale. Journal of Traumatic Stress. 1995;8(1):75–90. doi: 10.1002/jts.2490080106. [DOI] [PubMed] [Google Scholar]
- Bomyea J, Risbrough V, Lang AJ. A consideration of select pre-trauma factors as key vulnerabilities in PTSD. Clinical Psychology Review. 2012;32(7):630–641. doi: 10.1016/j.cpr.2012.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Branscombe NR, Wohl MJA, Owen S, Allison JA, N'gbala A. Counterfactual thinking, blame assignment, and well-being in rape victims. Basic and Applied Social Psychology. 2003;25(4):265–273. doi: 10.1207/S15324834BASP2504_1. [DOI] [Google Scholar]
- Brewin CR. Posttraumatic stress disorder: Malady or myth? New Haven, CT: Yale University Press; 2003. [Google Scholar]
- Buckley TC, Blanchard EB, Neill WT. Information processing and PTSD: A review of the empirical literature. Clinical Psychology Review. 2000;20(8):1041–1065. doi: 10.1016/S0272-7358(99)00030-6. [DOI] [PubMed] [Google Scholar]
- Cavanagh K, Davey GCL. UCS expectancy biases in spider phobics: Underestimation of aversive consequences following fear-irrelevant stimuli. Behaviour Research and Therapy. 2000;38(7):641–651. doi: 10.1016/S0005-7967(99)00077-7. [DOI] [PubMed] [Google Scholar]
- Coffey SF, Gudmundsdottir B, Beck JG, Palyo SA, Miller LM. Screening for PTSD in motor vehicle accident survivors using the PSS-SR and IES. Journal of Traumatic Stress. 2006;19(1):119–128. doi: 10.1002/jts.20106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cox KS, Resnick HS, Kilpatrick DG. Prevalence and correlates of posttrauma distorted beliefs: Evaluating DSM-5 PTSD expanded cognitive symptoms in a national sample. Journal of Traumatic Stress. 2014;27(3):299–306. doi: 10.1002/jts.21925. [DOI] [PubMed] [Google Scholar]
- Dalgleish T, Taghavi R, Neshat-Doost H, Moradi A, Canterbury R, William Y. Patterns of processing bias for emotional information across clinical disorders: A comparison of attention, memory, and prospective cognition in children and adolescents with depression, generalized anxiety, and posttraumatic stress disorder. Journal of Clinical Child and Adolescent Psychology. 2003;32(1):10–21. doi: 10.1207/15374420360533022. [DOI] [PubMed] [Google Scholar]
- Disner SG, Beevers CG, Lee H, Ferrell RE, Hariri AR, Telch MJ. War zone stress interacts with the 5-HTTLPR polymorphism to predict the development of sustained attention for negative emotion stimuli in soldiers returning from Iraq. Clinical Psychological Science. 2013;1(4):413–425. doi: 10.1177/2167702613485564. [DOI] [Google Scholar]
- Dunmore E, Clark DM, Ehlers A. Cognitive factors involved in the onset and maintenance of posttraumatic stress disorder (PTSD) after physical or sexual assault. Behaviour Research and Therapy. 1999;37(9):809–829. doi: 10.1177/2167702613485564. [DOI] [PubMed] [Google Scholar]
- Ehlers A, Clark D. A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy. 2000;38(4):319–345. doi: 10.1016/S0005-7967(99)00123-0. [DOI] [PubMed] [Google Scholar]
- Ehlers A, Mayou RA, Bryant B. Cognitive predictors of posttraumatic stress disorder in children: Results of a prospective longitudinal study. Behaviour Research and Therapy. 2003;41(1):1–10. doi: 10.1016/S0005-7967(01)00126-7. [DOI] [PubMed] [Google Scholar]
- Engelhard IM, de Jong PJ, van den Hout MarcelA, van Overveld M. Expectancy bias and the persistence of posttraumatic stress. Behaviour Research and Therapy. 2009;47(10):887–892. doi: 10.1016/j.brat.2009.06.017. [DOI] [PubMed] [Google Scholar]
- Engelhard IM, van den Hout MarcelA, Arntz A, McNally RJ. A longitudinal study of “intrusion-based reasoning” and posttraumatic stress disorder after exposure to a train disaster. Behaviour Research and Therapy. 2002;40(12):1415–1434. doi: 10.1016/S0005-7967(02)00018-9. [DOI] [PubMed] [Google Scholar]
- Foa EB, Ehlers A, Clark DM, Tolin DF, Orsillo SM. The posttraumatic cognitions inventory (PTCI): Development and validation. Psychological Assessment. 1999;11(3):303–314. doi: 10.1037/1040-3590.11.3.303. [DOI] [Google Scholar]
- Foa EB, Riggs DS, Dancu CV, Rothbaum BO. Reliability and validity of a brief instrument for assessing post-traumatic stress disorder. Journal of Traumatic Stress. 1993;6(4):459–473. doi: 10.1002/jts.2490060405. [DOI] [Google Scholar]
- Foa EB, Steketee G, Rothbaum BO. Behavioral/cognitive conceptualizations of post-traumatic stress disorder. Behavior Therapy. 1989;20(2):155–176. doi: 10.1016/S0005-7894(89)80067-X. [DOI] [Google Scholar]
- Freyd JJ. Betrayal trauma: The logic of forgetting childhood abuse. Cambridge, MA: Harvard University Press; 1996. Retrieved from http://ezproxy.middlebury.edu/login?url=http://search.proquest.com/docview/619034655?accountid=12447. [Google Scholar]
- Janoff-Bulman R. Assumptive worlds and the stress of traumatic events: Applications of the schema construct. Social Cognition Special Issue: Stress, Coping, and Social Cognition. 1989;7(2):113–136. doi: 10.1521/soco.1989.7.2.113. [DOI] [Google Scholar]
- Johnson R. A triarchic model of P300 amplitude. Psychophysiology. 1986;23(4):367–384. doi: 10.1111/j.1469-8986.1986.tb00649.x. [DOI] [PubMed] [Google Scholar]
- Karl A, Malta LS, Maercker A. Meta-analytic review of event-related potential studies in post-traumatic stress disorder. Biological Psychology. 2006;71(2):123–147. doi: 10.1016/j.biopsycho.2005.03.004. [DOI] [PubMed] [Google Scholar]
- Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CM. Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry. 1995;52(12):1048–1060. doi: 10.1001/archpsyc.1995.03950240066012. [DOI] [PubMed] [Google Scholar]
- Kilpatrick DG, Resnick HS, Milanak ME, Miller MW, Keyes KM, Friedman MJ. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. Journal of Traumatic Stress. 2013;26(5):537–547. doi: 10.1002/jts.21848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimble MO, Fleming K, Bandy C, Kim J, Zambetti A. Eye tracking and visual attention to traumatic stimuli in veterans of the Iraq War. Journal of Anxiety Disorders. 2010;24(3):293–299. doi: 10.1016/j.janxdis.2009.12.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimble MO, Frueh BC, Marks L. Does the modified Stroop effect exist in PTSD? Does the modified Stroop effect exist in PTSD? Evidence for the file drawer effect from dissertation abstracts and the peer reviewed literature. Journal of Anxiety Disorders. 2009;23(5):650–655. doi: 10.1016/j.janxdis.2009.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimble MO, Kaufman ML, Leonard LL, Nestor PG, Riggs DS, Kaloupek DG, Bachrach P. Sentence completion test in combat veterans with and without PTSD: Preliminary findings. Psychiatry Research. 2002;113(3):303–307. doi: 10.1016/S0165-1781(02)00229-9. [DOI] [PubMed] [Google Scholar]
- Kimble MO, Fleming K, Bennion K. Contributors to hypervigilance in a military and civilian sample. Journal of Interpersonal Violence. 2013;28(8):1672–1692. doi: 10.1177/0886260512468319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimble MO, Batterink L, Marks L, Ross C, Fleming K. Negative expectancies in posttraumatic stress disorder: Neurophysiological (N400) and behavioral evidence. Journal of Psychiatric Research. 2012;46(7):849–855. doi: 10.1016/jjpsychires.2012.03.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimble MO, Fleming K, Bandy C. Attention to novel and target stimuli in trauma survivors. Psychiatry Research. 2010;178(3):501–506. doi: 10.1016/j.psychres.2009.10.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kučera H, Francis W. Computational analysis of present day American English. Providence, RI: Brown University Press; 1967. [Google Scholar]
- Kutas M, Federmeier K. Thirty years and counting: Finding meaning in the N400 component of the event-related brain potential (ERP) Annual Review of Psychology. 2011;62:621–647. doi: 10.1146/annurev.psych.093008.131123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kutas M, Hillyard SA. Reading senseless sentences: Brain potentials reflect semantic incongruity. Science. 1980;207(4427):203–205. doi: 10.1126/science.7350657. [DOI] [PubMed] [Google Scholar]
- McEwen B, Lasley EN. Allostatic load: When protection gives way to damage. In: Monat A, Lazarus RS, Reevy G, editors. The Praeger Handbook on Stress and Coping. Vol. 1. Westport, CT: Praeger Publishers/Greenwood Publishing Group; 2007. pp. 99–109. [Google Scholar]
- McFarlane AC, Potts N. Posttraumatic stress disorder: Prevalence and risk factors relative to disasters. In: Saigh PA, Bremner JD, editors. Posttraumatic stress disorder: A comprehensive text. Needham Heights, MA: Allyn & Bacon; 1999. pp. 92–102. [Google Scholar]
- McNally RJ, Heatherton TF. Are covariation biases attributable to a priori expectancy biases? Behaviour Research and Therapy. 1993;31(7):653–658. doi: 10.1016/0005-7967(93)90118-E. [DOI] [PubMed] [Google Scholar]
- Metzger LJ, Orr SP, Lasko NB, Pitman RK. Auditory event-related potentials to tone stimuli in combat-related posttraumatic stress disorder. Biological Psychiatry. 1997;42(11):1006–1015. doi: 10.1016/S0006-3223(97)00138-8. [DOI] [PubMed] [Google Scholar]
- Miller AK, Handley IM, Markman KD, Miller JH. Deconstructing self-blame following sexual assault: The critical roles of cognitive content and process. Violence Against Women. 2010;16(10):1120–1137. doi: 10.1177/1077801210382874. [DOI] [PubMed] [Google Scholar]
- Mitchell R, Brennan K, Curran D, Hanna D, Dyer KFW. A meta-analysis of the association between appraisals of trauma and posttraumatic stress in children and adolescents. Journal of Traumatic Stress. 2017;30(1):88–93. doi: 10.1002/jts.22157. [DOI] [PubMed] [Google Scholar]
- Mokma TR, Eshelman LR, Messman-Moore T. Contributions of child sexual abuse, self-blame, posttraumatic stress symptoms, and alcohol use to women's risk for forcible and substance-facilitated sexual assault. Journal of Child Sexual Abuse. 2016;25(4):428–448. doi: 10.1080/10538712.2016.1161688. [DOI] [PubMed] [Google Scholar]
- Olatunji BO, Cisler JM, Meunier S, Connolly K, Lohr JM. Expectancy bias for fear and disgust and behavioral avoidance in spider fearful individuals. Cognitive Therapy and Research. 2008;32(3):460–469. doi: 10.1007/s10608-007-9164-8. [DOI] [Google Scholar]
- Pineles SL, Shipherd JC, Welch LP, Yovel I. The role of attentional biases in PTSD: Is it interference or facilitation. Behavior Research and Therapy. 2007;45(8):1903–1913. doi: 10.1016/j.brat.2006.08.021. [DOI] [PubMed] [Google Scholar]
- Pivik RT, Broughton RJ, Coppola R, Davidson RJ, Fox N, Nuwer MR. Guidelines for the recording and quantitative analysis of electroencephalographic activity in research contexts. Psychophysiology. 1993;30(6):547–558. doi: 10.1111/j.1469-8986.1993.tb02081.x. [DOI] [PubMed] [Google Scholar]
- Rugg MD, Doyle MC, Holdstock JS. Modulation of event-related brain potentials by word repetition: Effects of local context. Psychophysiology. 1994;31(5):447–459. doi: 10.1111/j.1469-8986.1994.tb01048.x. [DOI] [PubMed] [Google Scholar]
- Smith K, Bryant RA. The generality of cognitive bias in acute stress disorder. Behaviour Research and Therapy. 2000;38(7):709–715. doi: 10.1016/S0005-7967(99)00096-0. [DOI] [PubMed] [Google Scholar]
- Tanielian T, Jaycox L. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corporation; 2008. [Google Scholar]
- Van Berkum JosJA, Brown CM, Zwitserlood P, Kooijman V, Hagoort P. Anticipating upcoming words in discourse: Evidence from ERPs and reading times. Journal of Experimental Psychology: Learning, Memory, and Cognition. 2005;31(3):443–467. doi: 10.1037/0278-7393.31.3.443. [DOI] [PubMed] [Google Scholar]
- Vrana S, Lauterbach D. Prevalence of traumatic events and post-traumatic psychological symptoms in a nonclinical sample of college students. Journal of Traumatic Stress. 1994;7(2):289–302. doi: 10.1002/jts.2490070209. [DOI] [PubMed] [Google Scholar]
- Vythilingam M, Heim C, Newport J, Miller AH, Anderson E, Bronen R, Brummer M, Staib L, Vermetten E, Charney DS, Nemeroff CB, Brenmer JD. Childhood trauma associated with smaller hippocampal volume in women with major depression. American Journal of Psychiatry. 2002;159(12):2072–2080. doi: 10.1176/appi.ajp.159.12.2072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vythilingam M, Luchenbaugh DA, Lam T, Morgan CA, Lipschitz D, Charney DS, Bremner JD, Southwick SM. Smaller head of the hippocampus in Gulf War- related posttraumatic stress disorder. Psychiatry Research: Neuroimaging. 2005;139(2):89–99. doi: 10.1016/j.pscychresns.2005.04.003. [DOI] [PubMed] [Google Scholar]
- Wang P, Yang Y, Tan C, Zhao X, Liu Y, Lin C. Stereotype activation is unintentional: Behavioural and event-related potential evidence. International Journal of Psychology. 2015;51(2):156–162. doi: 10.1002/ijop.12135. [DOI] [PubMed] [Google Scholar]
- Warda G, Bryant RA. Cognitive bias in acute stress disorder. Behaviour Research and Therapy. 1998;36(12):1177–1183. doi: 10.1016/S0005-7967(98)00071-0. [DOI] [PubMed] [Google Scholar]