

Abstract
Background
Length of stay evaluations are very common to determine the burden of nosocomial infections. However, there exist fundamentally different methods to quantify the prolonged length of stay associated with nosocomial infections. Previous methodological studies emphasized the need to account for the timing of infection in order to differentiate the length of stay before and after the infection.
Methods
We derive four different approaches in a simple multi-state framework, display their mathematical relationships in a multiplicative as well as additive way and apply them to a real cohort study (n=756 German intensive-care unit patients of whom 124 patients acquired a nosocomial infection).
Results
The first approach ignores the timing of infection and quantifies the difference of eventually infected and eventually uninfected; it is 12.31 days in the real data. The second approach compares the average sojourn time with infection with the average sojourn time of being hypothetically uninfected; it is 2.12 days. The third one compares the average length of stay of a population in a world with nosocomial infections with a population in a hypothetical world without nosocomial infections; it is 0.35 days. Finally, approach four compares the mean residual length of stay between currently infected and uninfected patients on a daily basis; the difference is 1.77 days per infected patient.
Conclusions
The first approach should be avoided because it compares the eventually infected with the eventually uninfected, but has no prospective interpretation. The other approaches differ in their interpretation but are suitable because they explicitly distinguish between the pre- and post-time of the nosocomial infection.
Keywords: Multi-state model, Hospital-acquired infections, Sojourn time, Length of hospital stay
Introduction
Length of stay (LOS) is one of the most important outcomes in clinical epidemiology since it is directly linked to patients’ morbidity and economic costs [1]. It is easy to measure and often routinely collected in surveillance data bases. During the stay in hospital, patients are at risk to acquire nosocomial infections (NI) which belong to the major common adverse events in hospitals. Many observational reports have studied the impact of NI on length of stay by using different statistical methods. When evaluating the prolonged LOS of NI, the timing of NI plays an important role to distinguish between pre-infection time and consequence of NI. Several methodological papers showed the magnitude of the so-called time-dependent (aka immortal-time) bias which occurs if the timing of infection is not adequately addressed or rather ignored in the analysis [2, 3]. Multi-state models or time-dependent matching techniques account for the timing of NI to avoid the time-dependent bias [2–4]. However, there exist fundamentally different estimands to quantify this prolonged LOS associated with NI. In this article, we describe four different approaches and estimands in a simple multi-state framework [5], display their mathematical relationships in a multiplicative as well as additive way and apply them to a real cohort study.
Methods
We consider a time-homogeneous multi-state model (Fig. 1) with the three states 0=admission, 1=nosocomial infection, 2=discharge/death and assume constant hazard rates λ01,λ02 and λ12 between the corresponding states. The hazards λij are interpreted as the daily risk of moving from state i to state j.
Fig. 1.
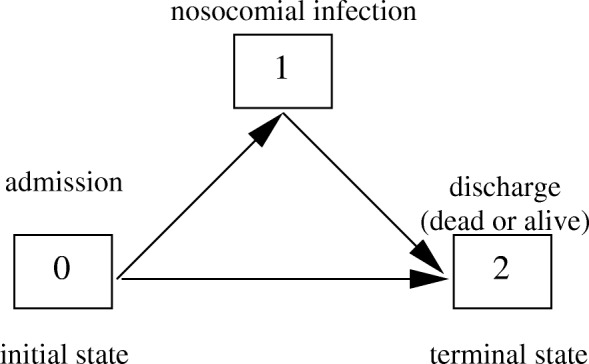
Multi-state model
The infection hazard λ01, also denoted as the incidence density of NI, is estimated by dividing the number of NI events by the number of summed patient-days in state 0 [5]. Analogously, the event densities λ02 and λ12 are estimated by dividing the discharge/death events by the number of summed patient-days in state 0 and 1, respectively [5]. These estimates are formally obtained via maximum likelihood estimation [6]. Since the hazard rates are assumed to be time-constant, the time to leave state 0 follows an exponential distribution with the hazard rate λ01+λ02. Thus, the average sojourn time in state 0 is . Analogously, the time to leave state 1 follows an exponential distribution with the hazard rate λ12 leading to an average sojourn time in state 1 of . The probability to acquire a NI is equal to .
We can write the average LOS in terms of the hazards from the multi-state model, which is the sum of the sojourn time in state 0 and the sojourn time in state 1 multiplied with the probability to acquire a NI:
If we assume the common case that NI reduce the discharge hazard, i.e. , we can use some algebra to derive following relationship:
where is interpreted as the average LOS in a hypothetical world without NI. The first inequality is shown as . The second inequality is shown as
These inequalities mean that the mean LOS in a world without NI is smaller than the mean LOS in a real world and this is smaller than the mean sojourn time in state 1. Based on the multi-state model, four different approaches to quantify the LOS associated with NI can be derived.
Restrospective stratification of eventually infected and uninfected
The most common approach (A1) is to compare the average overall LOS of eventually infected patients with the average overall LOS of eventually uninfected patients. It addresses the following medical question of interest (see Table 1): ’How many days do patients with NI stay, on average, eventually longer in hospital than patients who will never acquire a NI?’. In terms of the multi-state model, the average overall LOS of eventually infected patients is the sum of the average sojourn times of state 0 and state 1, . The average overall LOS of eventually uninfected patients is the sojourn time in state 0, . Thus, approach A1 is mathematically expressed by
Table 1.
Medical question of interest
| Approach | Medical question of interest / meaning of corresponding estimand |
|---|---|
| A 1 | - How many days do patients with NI stay, on average, eventually longer in hospital than patients who will never acquire a NI? |
| - How many days do patients with NI stay, on average, after the NI? | |
| A 2 | - How many hospital days are, on average, attributable to NI per patient? |
| - How many hospital days, on average, would a patient have stayed shorter if he/she would not have acquired a NI? | |
| A 3 | - How many hospital days are, on average, attributable to NI in a hospital population? |
| - How many hospital days would the average length of stay be shorter if all NI in the population would be eliminated? | |
| A 4 | - How many days does a patient with NI stay, on average, longer in hospital? |
| - How many days, on average, is the expected prolonged stay for patients with NI? |
which is the average sojourn time in state 1, given the patient has reached this state, i.e., has acquired a NI. In this approach, the classification of infected and uninfected is done retrospectively at the end of hospital stay.
This approach does not distinguish between pre- and post-infection LOS and thus does not allow a prospective associational (or even causal) interpretation. The limitation is that the LOS before NI which is included in the LOS of eventually infected patients can not be interpreted as LOS attributed due to NI. Instead, the LOS before NI (which is per-se not attributable to NI) should count as uninfected LOS. Therefore, the following approaches have been developed.
Differentiating between pre- and post-infection length of stay
In contrast to the previous approach, the following approaches will differentiate between the pre-infection time and consequence of NI in terms of LOS.
The second approach A2, termed as attributable LOS [7, 8], compares the average sojourn time in state 1 with the average sojourn time in state 0 in a hypothetical world without NI . The medical question of interest (see Table 1) is ’How many hospital days, on average, would a patient have stayed shorter if he/she would not have acquired a NI?’.
This is quantified by
In contrast to approach A1, the left part of the difference in approach considers only the post-infection LOS of infected patients. Moreover, the right part considers a longer LOS than the one of approach A1 as . This corrects for the limitations of approach A1. However, the limitation of approach A2 is that is not a real world mean time and is therefore a hypothetical quantity for LOS of uninfected patients.
In the third approach A3, we substract the average LOS in a hypothetical world from the one in a real world addressing the medical question ’How many hospital days would the average length of stay be shorter if all NI in the population would be eliminated?’. Algebraically, it is
This estimand is called the population-attributable LOS [8, 9], which is a population measure of extra LOS and compares the average LOS of a population in a world with NI with a population in a hypothetical world without NI.
In the fourth approach A4, we subtract the average length of stay from the sojourn time in state 1 which aims to answer the medical question ’How many days does a patient with NI stay, on average, longer in hospital?’ (see Table 1). It is
This estimand, also called the change of length of stay, is the established multi-state approach [10] and compares mean residual LOS between currently infected and uninfected patients using landmarking on each day in the hospital, it is a difference per infected patient.
Basic properties related to the hazard ratio
In this section we consider basic relationships to the hazard ratio . The hazard ratio is often calculated and it describes in a multiplicative way if and how NI prolongs LOS. A hazard ratio of 1 means that the daily chance to be discharged does not change if the patient acquires a NI meaning that NI does not prolong the LOS. It is more often the case that the hazard ratio is smaller than 1 indicating a prolonged LOS associated with NI. It is rarely the case that the hazard ratio is greater than 1 which would mean a shortened LOS associated with NI. It is obvious that approach A1 is always larger than 0 (A1>0) as λ12>0. Since it further does not depend on λ02, A1 always means that NI patients stay eventually longer than patients who never acquired NI, even if or which is not a required property. For the other approaches we have: . It is also easily shown that and . Thus, approaches A2, A3 and A4 have the required mathematically equivalent properties regarding the direction of the hazard ratio whereas approach A1 does not.
In Table 2, the properties of all approaches are displayed, summarized and contrasted to each other.
Table 2.
Approaches and their properties
| Approach | Properties / pros and cons |
|---|---|
| A 1 | - is a real quantity |
| - undesired properties related to hazard ratio | |
| - yields positive values even if NI patients are discharged faster, i.e., | |
| - does not distinguish between pre- and post-infection time | |
| - does not allow causal interpretation about attributable length of stay associated with NI | |
| - not appropriate to quantify the burden of NI | |
| A 2 | - is a hypothetical quantity |
| - desired properties related to hazard ratio | |
| - considers only the post-infection time for NI patients | |
| - contributes pre-infection time to patients without NI | |
| - allows a causal interpretation about attributable length of stay associated with NI | |
| - appropriate to quantify the burden of NI at patient-level | |
| A 3 | - is a hypothetical quantity |
| - desired properties related to hazard ratio | |
| - considers only the post-infection time for NI patients | |
| - contributes pre-infection time to patients without NI | |
| - allows a causal interpretation about attributable length of stay associated with NI | |
| - appropriate to quantify the burden of NI at population-level | |
| A 4 | - is a real quantity |
| - desired properties related to hazard ratio | |
| - distinguishes between pre- and post-infection time | |
| - appropriate to quantify the burden of NI at patient-level |
Additive and multiplicative comparisons of approaches
Before we compare the approaches in a additive and multiplicative way, we note that approaches A1 and A2 do not depend on infection hazard λ01 whereas approaches A3 and A4 do. Further, approaches A1, A2 and A4 are at the patient-individual level and therefore directly comparable whereas A3 is at the population-level. All approaches are displayed in the Table 3. We further note that there is also following relationship: A3+A4=A2.
Table 3.
Overview and relationships of approaches to quantify prolonged hospital stay associated with nosocomial infections
| Approach | real data example (SIR-3 study) |
|---|---|
| 12.31 days | |
| 2.12 days | |
| 0.35 days | |
| 1.77 days | |
| Additive relationships between approaches (differences) | |
| 10.54 days | |
| 11.97 days | |
| 10.19 days | |
| 1.43 days | |
| 1.77 days | |
| 0.35 days | |
| Following relationship holds: A3+A4=A2 | |
| Multiplicative relationships between approaches (ratios) | |
| 6.94 | |
| 35.4 | |
| 5.80 | |
| 0.196 | |
| 0.164 | |
| 1.20 | |
| Following relationship holds if λ01≤λ02:A3≤A4≤A2≤A1 | |
Comparing approaches A1 and A2
The additive relationship between approaches A1 and A2 is just the average length of stay of a population in a hypothetical world without NI . The multiplicative relationship is .
Comparing approaches A1 and A3
As before, the relationship between approaches A1 and A3 is best described and communicable in an additive way. The difference between A1 and A3 is (Table 3). It is mainly the average length of stay of a population in a hypothetical world without NI ; multiplied with the factor which is often larger than 1 as λ02 is often larger than λ12. In contrast, the multiplicative relationship is .
Comparing approaches A1 and A4
The relationship between approaches A1 and A4 is best described in an additive way. The difference is (Table 3). Thus, it mainly depends on the average sojourn time of state 1 which is ; the factor is usually lower than 1 as λ02 is often larger than λ12. The multiplicative relationship is .
Comparing approaches A2 and A3
Approaches A3 and A2 are best compared in a multiplicative way: . The additive comparison is .
Comparing approaches A2 and A4
Approach A2 is linked to approach A4 with . Based on this formula, it follows that both approaches give similar results if the nosocomial infection is rare (risk is smaller than 10%). The additive comparison is .
Comparing approaches A3 and A4
In contrast to the previous comparisons to approach A1, approaches A3 and A4 are best compared in a multiplicative way. There is the following simple relationship: . Thus, the factor odds(NI) links the population-level approach A3 to the individual-level approach A4. The additive relationship is rather complex: .
Real data example
We use publicly available data from the R-package etm [11]. This is an observational prospectively collected cohort study including 756 intensive care patients from Germany of whom 124 patients acquired a nosocomial pneumonia (NI) during their stay in the intensive care unit (ICU). The data used here is a random sample from a larger cohort which is described in detail elsewhere [12].
Results
The cohort study followed 756 patients during their stay at the intensive-care unit. Of these patients, 124 patients acquired a NI during their stay in the ICU. The summed patient-days without NI was 6442 and with NI 1527. Thus, the constant hazards can be estimated as follows: , , and . The average length of stay of this cohort is days; the sojourn time in state 0 is days and days in state 1, respectively. The results of the different approaches are diverse, however, with different interpretation. As expected, A1 provides a exaggerated value of 12.31 days which just means that patients with NI stay eventually 12.31 days longer at ICU then eventually uninfected patients. In contrast, A4 yields that a NI prolongs the LOS by mean 1.77 ICU days per infected patient. The population-attributable LOS (A3) is 0.35 days meaning that there are on average 0.35 additional ICU days attributable to NI at the population level. The attributable LOS (A2) is 2.12 ICU days, interpreted as the average LOS which is attributable to NI for an infected patient.
Discussion
A multi-state model was used to mathematically derive four fundamentally different approaches to quantify the prolonged length of stay associated with nosocomial infections or other adverse events [13]. The relationships were displayed in an additive as well as a multiplicative way.
As in previous articles [2, 4], we encourage researchers to not retrospectively stratify by infection status and, consequently, to avoid the use of approach A1 because it does not differentiate between pre- and post-infection time and thus does not allow a causal interpretation.
The other approaches are suitable because they implicitly distinguish between the pre-infection time (which might be a risk factor) and post-infection time (which might be a consequence) of nosocomial infections. The main difference is the interpretation and we showed mathematical formulas how they are linked to each other. Thus, this knowledge can be used to better understand apparent discrepancies in the literature and transfer published values from one approach to the other.
The question whether nosocomial infections prolong hospital stay is - from the methodological point of view - related to ’life years lost among patients with a given disease’ [14] by replacing discharge with death and length of stay with age. Andersen [14] considered also a multistate model, the classical illness-death model, in order to study different statistical variants and extensions of our approach A4 including time-inhomogeneous Markov models, censoring and semi-Markov models. Approaches A1- A3 are not considered by Andersen and complement his considerations.
This study has following limitations. First, we focused on the basic approaches and did not consider any other covariates such as characteristics from the patient-, hospital- or even country-level (for instance, as in Stewardson et al. [15]). Even though there exists regression models [16] which allows for adjusting the change of length of stay (approach A4), we believe that the choice of the fundamental approach has a much stronger impact on the results than the adjustment for covariates. For instance, previous studies indicated that the time-dependent bias could not be redeemed by adjustment of several patient-level covariates [4]. Second, the hazard rates are often not time-homogeneous in real-data settings. Even though time-inhomogeneous approaches exist, we are convinced that this simplification is required to provide a clear transparency which leads to a better understanding of basic distinctions. Third, we combined the diametrically opposed endpoints discharge (alive) and death. We think that this combination is reasonable if the focus is on length of stay and their related economic costs, the topic of this paper. However, as rapid death results in shorter LOS, a length-of-stay analysis should always be accompanied with an analysis with respect to mortality. This can be done by using an extended multi-state model that distinguishes between inpatient death and discharge alive [5, 6].
Conclusion
We conclude that a clear distinction between different estimands is needed to better understand apparently large discrepancies in the literature. We recommend the use of approaches which differentiates between pre- and post-infection time.
Acknowledgements
Not Applicable.
Authors’ contributions
MW, JB and GR performed the formulas and data analysis. MW wrote the first draft. SH and MS had insightful contributions to conception and revised the article critically for important intellectual content. All authors read and approved the final manuscript.
Funding
This work has been funded by the German Research Foundation (Deutsche Forschungsgemeinschaft)(grant No WO 1746/1-2); MW received this funding. This work was also supported by the Innovative Medicines Initiative Joint Undertaking resources (composed of financial contribution from the European Union’s Seventh Framework Programme (FP7/2007-2013) and EFPIA companies) [grant number 115737-2 – COMBACTE-MAGNET and 115523 – COMBACTE-NET]. The funding bodies had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript. The article processing charge was funded by the German Research Foundation (DFG) and the Albert Ludwigs University Freiburg in the funding programme Open Access Publishing.
Availability of data and materials
Data are publicly available in the R-package etm (https://cran.r-project.org/web/packages/etm/index.html).
Ethics approval and consent to participate
Not applicable as data are publicly available.
Consent for publication
Not applicaple.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Lambert ML, Suetens C, Savey A. Palomar M, Hiesmayr M, Morales I, et al. Clinical outcomes of health-care-associated infections and antimicrobial resistance in patients admitted to European intensive-care units: a cohort study. Lancet Infect Dis. 2011;11:30–38. doi: 10.1016/S1473-3099(10)70258-9. [DOI] [PubMed] [Google Scholar]
- 2.Barnett AG, Beyersmann J, Allignol A, Rosenthal VD, Graves N, Wolkewitz M. The Time-Dependent Bias and its Effect on Extra Length of Stay due to Nosocomial Infection. Value Health. 2011;14:381–386. doi: 10.1016/j.jval.2010.09.008. [DOI] [PubMed] [Google Scholar]
- 3.Nelson RE, Nelson SD, Khader K, Perencevich EL, Schweizer ML, Rubin MA, et al. The Magnitude of Time-Dependent Bias in the Estimation of Excess Length of Stay Attributable to Healthcare-Associated Infections. Infect Control Hosp Epidemiol. 2015;36(9):1089–1094. doi: 10.1017/ice.2015.129. [DOI] [PubMed] [Google Scholar]
- 4.Beyersmann J, Kneib T, Schumacher M, Gastmeier P. Nosocomial infection, length of stay, and time-dependent bias. Infect Control Hosp Epidemiol. 2009;30:273–276. doi: 10.1086/596020. [DOI] [PubMed] [Google Scholar]
- 5.Wolkewitz M, von Cube M, Schumacher M. Multistate Modeling to Analyze Nosocomial Infection Data: An Introduction and Demonstration. Infect Control Hosp Epidemiol. 2017;38(8):953–959. doi: 10.1017/ice.2017.107. [DOI] [PubMed] [Google Scholar]
- 6.von Cube M, Schumacher M, Wolkewitz M. Basic parametric analysis for a multi-state model in hospital epidemiology. BMC Med Res Methodol. 2017;17(1):111. doi: 10.1186/s12874-017-0379-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bootsma MC. Mathematical studies of the dynamics of antibiotic resistance, PhD thesis; 2005. www.staff.science.uu.nl/boots102/PhD-thesis٪20Bootsma.pdf.
- 8.Schulgen G, Schumacher M. Estimation of prolongation of hospital stay attributable to nosocomial infections: new approaches based on multistate models. Lifetime Data Anal. 1996;2:219–240. doi: 10.1007/BF00128975. [DOI] [PubMed] [Google Scholar]
- 9.Bernoulli D, Blower S. An attempt at a new analysis of the mortality caused by smallpox and of the advantages of inoculation to prevent it. Reviews in medical virology. 2004;14(5):275–288. doi: 10.1002/rmv.443. [DOI] [PubMed] [Google Scholar]
- 10.Allignol A, Schumacher M, Beyersmann J. Estimating summary functionals in multistate models with an application to hospital infection data. Computational statistics. 2011;26(2):181–197. doi: 10.1007/s00180-010-0200-x. [DOI] [Google Scholar]
- 11.Allignol A, Schumacher M, Beyersmann J. Empirical Transition Matrix of Multi-State Models: The etm Package. Journal of Statistical Software. 2011;38(4):1–15. doi: 10.18637/jss.v038.i04. [DOI] [Google Scholar]
- 12.Wolkewitz M, Vonberg RP, Grundmann H, Beyersmann J, Gastmeier P, Barwolff S, et al. Risk factors for the development of nosocomial pneumonia and mortality on intensive care units: application of competing risks models. Crit Care. 2008;12(2):R44. doi: 10.1186/cc6852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.de Vries EN, Ramrattan MA, Smorenburg SM, Gouma DJ, Boermeester MA. The incidence and nature of in-hospital adverse events: a systematic review. BMJ Quality & Safety. 2008;17(3):216–223. doi: 10.1136/qshc.2007.023622. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Andersen PK. Life years lost among patients with a given disease. Statistics in medicine. 2017;36(22):3573–3582. doi: 10.1002/sim.7357. [DOI] [PubMed] [Google Scholar]
- 15.Stewardson AJ, Allignol A, Beyersmann J, Graves N, Schumacher M, Meyer R, et al. The health and economic burden of bloodstream infections caused by antimicrobial-susceptible and non-susceptible Enterobacteriaceae and Staphylococcus aureus in European hospitals, 2010 and 2011: a multicentre retrospective cohort study. Euro Surveill. 2016;21(33):30319. doi: 10.2807/1560-7917.ES.2016.21.33.30319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bluhmki T, Allignol A, Ruckly S, Timsit JF, Wolkewitz M, Beyersmann J. Estimation of adjusted expected excess length-of-stay associated with ventilation-acquired pneumonia in intensive care: A multistate approach accounting for time-dependent mechanical ventilation. Biometrical Journal. 2018;60(6):1135–1150. doi: 10.1002/bimj.201700242. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data are publicly available in the R-package etm (https://cran.r-project.org/web/packages/etm/index.html).