

Abstract
Objective:
Echocardiographic screening for Rheumatic Heart Disease (RHD) in Africa has revealed prevalence rates in the range of 0.5 – 7.4%. There are no recent large population-based studies in Nigeria. The objective of the study was to determine the prevalence of RHD in a large sample of Nigerian school children.
Methods:
Using portable transthoracic echocardiography and auscultation, school children aged 5 years to 16 years in Lagos, Nigeria were screened for RHD. Diagnosis was based on the 2012 World Heart Federation echocardiographic criteria.
Results:
The 4,107 children screened had mean age of 11.3 years (SD=2.6) and 2,206 (53.7%) were females. There were 38 children with abnormal echocardiograms, of which 11 (0.27%) showed RHD including two cases of definite RHD giving a prevalence of 2.7/1000 [2.9/1000 in the peri-urban, 2.4/1000 in the urban area). Echocardiography detected RHD 10 times better than auscultation [echocardiography 11 (0.27%) versus auscultation 1 (0.02%); p=0.003]. The remaining 27 children with abnormal echocardiograms had congenital heart defects (CHD) giving a prevalence of 6.6/1000 for CHD, a yield higher than for RHD.
Conclusion:
Prevalence of RHD among school children in Lagos, South West Nigeria is low compared to other African countries, possibly due to better access to medical care and antibiotic treatment for infections. Our data provides evidence that RHD prevalence may vary substantially within sub-Saharan Africa, necessitating targeted population-based sampling to better understand disease burden and distribution. Further work is needed to compare within- and between-country RHD prevalence as a basis for program planning and control efforts.
Keywords: Rheumatic Heart Disease in Nigeria, Prevalence, School children, echocardiography screening, World Heart Federation Criteria
Introduction
Rheumatic heart disease (RHD) is a chronic pathology occurring as a complication of acute rheumatic fever (ARF), which occurs in a subset of susceptible individuals who have suffered a Group A streptococcal infection. It is the commonest acquired heart disease in developing countries and is especially prevalent in Oceania, Central sub-Saharan Africa and South Asia.1 In 2015, it was estimated that there were 33.4 million people with RHD; 319,400 annual deaths attributed to both RHD and ARF and 10 million disability-adjusted life-years due to RHD globally.1
Although clinical evaluation has been used to diagnose RHD for decades, recent studies2–4 show that echocardiography-based screening improves detection of RHD. This has revealed a higher burden of RHD than previously suspected by auscultation-based studies (less than 1 to 14/1000 in sub-Saharan Africa). The estimated prevalence of RHD in sub-Saharan Africa has been reported to be 7.5–51.6/1000 with use of echocardiographic screening,5 thus making echocardiography the standard method for RHD diagnosis. The consensus criteria for echocardiographic diagnosis of RHD by the WHF released in 2012 provided the much-needed standardization for diagnosis.6 These criteria are currently the adopted gold standard criteria for echocardiographic screening of RHD.
Data on RHD prevalence using the WHF criteria in West Africa are scarce and none exist for Nigeria, the most populous country in Africa. The most recent study to determine the prevalence of RHD in school children in Lagos, Nigeria, was done more than three decades ago. In that study which utilized only cardiac auscultation by final year medical students to detect RHD, the prevalence was 0.5/1000 school children.7 Given the marked changes in the environment and better access to medical care and antimicrobial therapy in the intervening period, it is possible disease burden has decreased. However, the improved sensitivity of echocardiography may also result in increased detectable RHD burden.
The aim of the study therefore was to determine the contemporary prevalence of RHD in a large sample of Nigerian school children using echocardiography as a screening tool; compare the yield of echocardiography screening and auscultation for diagnosis of RHD as well as document the prevalence of recent streptococcal infection among children with RHD using the Antistreptolysin O (ASO) titer test.
Methods
Setting
The study was a cross sectional population-based study of Nigerian school children resident in Lagos State, South West Nigeria (Figure 1) conducted from March 2016 to February 2017. Lagos state is a diverse, multi-ethnic state with people from a wide range of socio-economic classes with an objective poverty profile of 75.9% in the lower class (living below $2 a day), 18.7% and 1.8% in the middle and upper class (living above $10 a day) respectively.8. The city of Lagos is the most populous city in Nigeria with an estimated population of 21 million as of 2014.9 (Fig. 1). It is one of the top 10 fastest growing cities and urban areas globally.10 The urban metropolitan part of Lagos extends over 16 of the 20 local government areas and contains 85% of the population of the state. The city is the economic hub of Nigeria and the West African sub-region and accounts for 65% of manufacturing activity in Nigeria. Lagos State offers free education in all public primary and secondary schools.
Figure 1.
Map of Nigeria and Lagos State (Red arrow shows study sites)
Ethics
Ethical approval was obtained from the Lagos University Teaching Hospital (LUTH) Health Research Ethics Committee. In addition, approval was obtained from the Lagos State Ministry of Education and Tutor Generals of Educational districts I11 and VI for the secondary schools and Lagos State Universal Basic Education Board (SUBEB) for primary schools.
Sample size estimates
Currently, there is no recent population-based study of RHD done among a large number of Nigerian children. Using the median figure (2.5%) from recent prevalence figures from sub-Saharan African countries2–4, a sample size of 3731 is needed to estimate the prevalence of RHD by echocardiography with a precision of + 5/1000 (0.5%). Assuming a non-completion or dropout rate of 10%, the target sample size was 4,000. A total number of 4,107 children were eventually enrolled.
Sampling procedures
A multistage sampling procedure was used to enroll subjects (Figure 2). The sampling frame consisted of all public primary and secondary schools in Lagos State. From the 20 Local government areas (LGAs) of Lagos, two were randomly selected consisting of one LGA randomly selected from all the LGAs in Metropolitan Lagos (urban) and one LGA from outside Lagos Metropolis (peri-urban). The master list of schools in each of the two selected LGAs was stratified into primary and secondary schools. A systematic random sampling procedure was used to select four primary and six secondary schools in each LGA. By design, this procedure over-sampled secondary schools since RHD is more prevalent among older children. From each school, depending on class size in the school one or two classes were randomly selected from the classes in each year to attain a minimum sample of 200 children per school.
Figure 2.
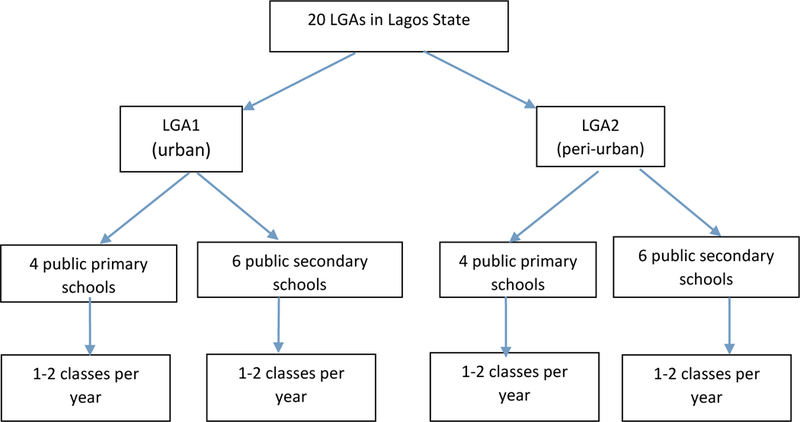
Multistage sampling method for enrollment of school children.
Data collection
In each of the selected schools, consent forms were given to children aged 5 years to 16 years for parental consent. In addition, assent forms were administered on children aged ≥7 years. Only children whose parents provided informed consent and who provided assent (if age appropriate) were enrolled for the study. The project team included six health personnel including at least two physicians skilled in performance and interpretation of echocardiography. Demographic information and anthropometric data (height and weight) were obtained from the children using a structured questionnaire. Socioeconomic class was assessed using a method proposed by Oyedeji which utilizes occupation and educational attainment of parents/guardians.11 Targeted clinical examination focused on cardiac auscultation for murmurs, other heart sounds and signs of ARF was done in a designated room provided by the school where privacy of the participants was ensured. Screening echocardiography with 2D, continuous-wave and color-Doppler studies using portable echocardiography machines (Philips CX50 Compact Xtreme Cardiovascular ultrasound machine with S3 and S5 transducer probes and GE Vivid E ultrasound machine) was done on all enrolled children.
Any child with mitral or aortic valve thickening and/or pathological regurgitation, or CHD was considered to have an abnormal echocardiogram. Those with abnormal echocardiogram had a full echocardiography test done with recording of images for review by 3 independent physicians blinded to the clinical information of participants. Based on the 2012 WHF Criteria for echocardiographic diagnosis of RHD, participants with RHD were categorized as either having a “definite RHD” or “borderline RHD”.5 The participants with RHD diagnosis had specific information related to RHD and whole venous blood (5mls) obtained for ASO titer test for evidence of recent streptococcal infection. The criteria for a positive ASO titer (i.e. indicative of recent streptococcus infection) was >267IU/mL.12 Children with definite RHD were advised to start secondary prophylaxis and referred to a tertiary hospital while those with borderline RHD were counselled to report promptly to a nearby health center anytime they had sore throat and fever.
Data Analysis
Data analysis was done using IBM SPSS® Statistics for Windows, Version 20.0 (IBM Corp, Armonk, NY). Categorical variables were summarized as frequencies and percentages. Quantitative variables were summarized using means and standard deviations (SD). Means and proportions between cases of RHD and those without were compared using Student t-test and chi square test respectively. All comparisons were two-tailed and p values <0.05 were considered significant.
Results
A total number of 4,107 school children aged five to 16 years with mean age of 11.3 years (SD=2.6) were screened for RHD. Half of the study population were screened in schools located in the urban area of Lagos (2060; 50.2%). Females constituted a little more than half of the study population (2,206; 53.7%). Only 3.9% (162) of the children belonged to the higher socioeconomic classes: I and II. (Table 1).
Table 1.
Demographic characteristics of study population
| Characteristic | Frequency | Percentage |
|---|---|---|
| Age in years | ||
| 5 – 10 | 1381 | 33.6 |
| 11 −16 | 2726 | 66.4 |
| Sex | ||
| Male | 1901 | 46.3 |
| Female | 2206 | 53.7 |
| Socioeconomic class | ||
| Class I & II (“high’) | 154 | 3.7 |
| Class III (“middle”) | 1039 | 25.3 |
| Class IV & V (“low”) | 2914 | 71.0 |
| Location | ||
| Urban | 2060 | 50.2 |
| Peri-urban | 2047 | 49.8 |
Prevalence
Thirty-eight children had abnormal echocardiograms. Eleven (0.27%) of the 4,107 school children had RHD including two cases of definite RHD and nine cases of borderline RHD giving a prevalence of 2.7/1000. This estimate implies that to detect one case of RHD among apparently healthy school children in Lagos, Nigeria, 400 children have to undergo echocardiography. The remaining 27 children with abnormal echocardiograms had CHD with no associated RHD, giving a prevalence of 6.6/1000 for CHD. Six of the 2047 children screened in the peri-urban schools had RHD, giving a prevalence of 2.9/1000 in the peri-urban area. In the urban area, five cases of RHD of the 2060 screened gave a prevalence of 2.4/1000. Three cases of RHD were identified among 1281 school children aged 5–10 years, giving an RHD prevalence of 2.3/1000. Eight cases of RHD were diagnosed among 2726 children aged 11–16 years, giving a prevalence of 2.9/1000.
Clinical, echocardiography and laboratory findings
Seven (63.6%) of the eleven children with RHD including the two cases with definite RHD were males. The mean age of children with RHD was similar to that of those without RHD [11.64 SD±2.38 years versus 11.3±2.65 years respectively, with a mean difference of 0.31 and 95% CI (−1.26, 1.88); p=0.3]. No child aged <10 years had RHD. Among the cases with RHD, seven were aged 10–12 years while four were aged 13–16 years. Of the eleven cases of RHD detected by echocardiography, only one child was suspected to have RHD by cardiac auscultation. Echocardiography therefore, was 10 times more sensitive than auscultation [p=0.003]. The majority (10 of 11 or 90.9%) of children with RHD had mitral valve affectation and all cases of RHD were asymptomatic. None of the cases with RHD recalled having a recent episode of sore throat. There was a 95% agreement among the reviewers on the recorded images.
The two cases of definite RHD were aged 13 years and 14 years; had pathological mitral regurgitation (MR) with MR jet length of 4.2 cm and 5.1 cm; and MR jet velocity of 4.4 m/s and 4.7 m/s respectively. (Figure 3). Thickened anterior mitral valve leaflet (AMVL) measuring 5mm and 6.1mm respectively, chordal thickening and restricted posterior mitral valve leaflet (PMVL) motion were the morphological features of RHD observed. Neither of the two cases of definite RHD had mitral stenosis. The aortic valve was not affected in either cases of definite RHD.
Figure 3.
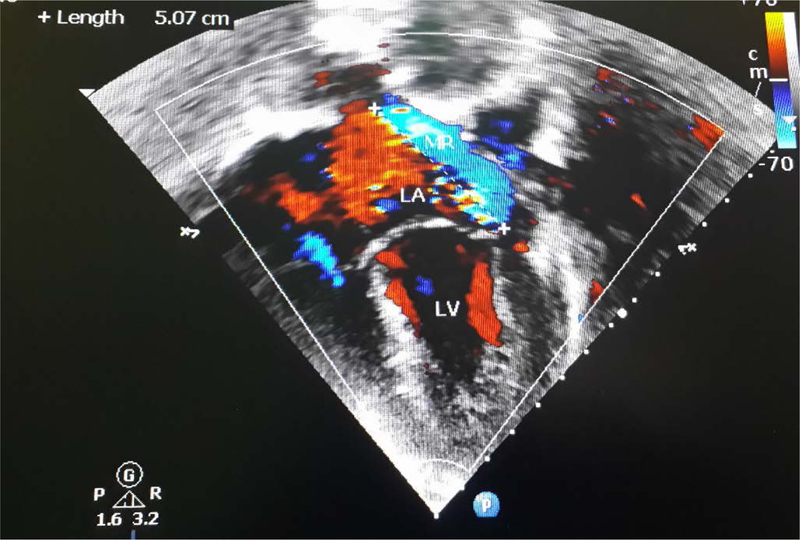
Echocardiography Colour Doppler image of case 1 with definite RHD showing pathological mitral regurgitation in a 14-year-old male
The nine cases of borderline RHD comprised of four females and five males with ages ranging from 10 to 16 years (Table 2). Seven (77.8%) of the nine cases with borderline RHD had pathological MR while two (22.2%) had pathological AR. Among the seven cases with pathological MR, four also had morphological features of MV affectation (AMVL thickening ranging from 3.4 mm to 4.6 mm and chordal thickening). The two cases with pathological AR had AR jet lengths of 1.8 cm and 2.7 cm; and AR jet velocities of 3.1 m/s and 3.2 m/s respectively. ASO titer levels in the RHD cases ranged from 65IU/ML to – 233IU/ML with a mean of 149.5 ± 63IU/ML. Therefore, no RHD cases had evidence of recent streptococcus infection based on the criterion of > 267 IU/ML.
Table 2.
Characteristics of children with RHD
| RHD cases |
Age(Y) | Sex | Location | Echocardiography findings | RHD diagnosis | ||||
|---|---|---|---|---|---|---|---|---|---|
| Pathological MR |
Pathological AR |
MS | Morphological features of RHD on MV |
Morphological features of RHD on AV |
|||||
| Case 1 | 14 | M | Peri-urban | Present | Absent | Absent | Thickened AMVL (6mm) with hockey stick deformity; chordal thickening; Restricted PMVL motion. | Absent | Definite RHD |
| Case 2 | 13 | M | Peri-urban | Present | Absent | Absent | Thickened AMVL (4mm); chordal thickening; restricted PMVL motion. | Absent | Definite RHD |
| Case 3 | 10 | M | Peri-urban | Present | Absent | Absent | Thickened AMVL (4mm); chordal thickening. | Absent | Borderline RHD |
| Case 4 | 16 | F | Peri-urban | Present | Absent | Absent | Absent | Absent | Borderline RHD |
| Case 5 | 11 | M | Peri-urban | Present | Absent | Absent | Thickened AMVL (4.5mm); chordal thickening. | Absent | Borderline RHD |
| Case 6 | 10 | F | Urban | Present | Absent | Absent | Thickened AMVL (4.1mm) | Absent | Borderline RHD |
| Case 7 | 10 | F | Urban | Present | Absent | Absent | Absent | Absent | Borderline RHD |
| Case 8 | 13 | M | Peri-urban | Present | Absent | Absent | Thickened AMVL (4.4mm); chordal thickening. | Absent | Borderline RHD |
| Case 9 | 12 | M | Urban | Present | Absent | Absent | Absent | Absent | Borderline RHD |
| Case 10 | 11 | M | Urban | Present | Present | Absent | Absent | Absent | Borderline RHD |
| Case 11 | 11 | F | Urban | Absent | Present | Absent | Absent | Absent | Borderline RHD |
Discussion
RHD results from the consequences of inadequately treated streptococcal infections and ARF. Echocardiographic screening for RHD is superior to clinical screening alone which underestimates the burden of RHD. Since the standardization of criteria for echocardiographic screening of RHD by WHF, several studies13-18 have been done on school children in Africa and other regions. There are regional variations in prevalence of RHD as risk factors of the disease are largely socioeconomic in nature. The estimated prevalences of RHD among school children in Africa using the WHF criteria and standard echocardiography have ranged from 11.8/1000 to 44.97/1000 and notably the rates13-19 are in the double digits per thousand. Our comparison of studies among school children using echocardiographic screening with WHF consensus criteria in different countries of Africa reveal a lower prevalence of RHD in the present study compared to findings from other parts of Africa (Table 3). The closest prevalence to our finding is a figure of 11.8/1000 reported from Zambia. Explanations for this variation include differences in exposure to streptococcal infection, access to prompt antimicrobial treatment for throat infections and health care access. The apparently low prevalence of RHD in the present study compared with studies from other African countries should be considered against the following context: (1) the study took place at a single site (Lagos) and is not a nationwide survey, (2) the study site has better health care resources and better access to health care for children than most parts of the country, (3) the study site is located in the southern part of the country that previous hospital based studies have shown to have a lower RHD prevalence compared to the northern part of the country, (4) children who have severe RHD or are too ill from RHD do not attend school at all or regularly and would have been missed by the study. Therefore, our figures should not be taken to represent the prevalence of RHD for the whole of Nigeria.
Table 3.
Prevalence of RHD among school children in African countries using WHF criteria for echocardiographic screening
| Region of study |
Period of study |
Population of study |
Age range studied (years) |
Mean age of subjects [years (SD)] |
Prevalence of RHD/1000 |
|---|---|---|---|---|---|
| Uganda11 | 2014 | 956 | 5–17 | 11.1±2.5 | 44.97 |
| Malawi12 | 2014 | 1450 | 5–16 | - | 34.0 |
| Egypt13 | 2009–2014 | 3062 | 5–15 | 10±2.6 | 31.0 |
| Ethiopia14 | 2008–2013 | 2000 | 4–24 | 10.7±2.5 | 31.0 |
| South Africa14 | 2008–2013 | 2720 | 4–24 | 12.2±4.2 | 20.2 |
| Ethiopia 15 | 2016 | 3238 | 6–18 | 13.2±3.2 | 19.0 |
| Senegal16 | 2011 | 2019 | 5–18 | 9.7±3.3 | 16.3 |
| Zambia17 | 2015 | 1102 | 10–24 | 15.4±1.9 | 11.8 |
| Lagos, Nigeria (Present study) | 2016–2017 | 4107 | 5–16 | 11.3±2.7 | 2.1 |
In contrast to the present study, screening for RHD among school children done in Lagos, Nigeria more than three decades ago documented a low prevalence rate of 0.5/1000.7 This is probably due to the use of clinical screening alone in that study. In light of the fact that echocardiographic screening for RHD is more sensitive than clinical screening3 the prevalence reported from that study is likely to be an underestimate. Indeed, the true estimate in the previous study is likely to be in the order of 5/1000 if we utilize the findings of the present study of echocardiography being able to detect RHD ten times as frequently as cardiac auscultation to adjust the previous estimate. The implication is that while it would appear that the prevalence of 2.7/1000 in this study is higher than that reported in the previous study, the different screening methods implies that that prevalence of RHD in Lagos is about one-half what was reported in the earlier study.
School-based screening programs have been considered to be prone to underestimates due to out-of-school children who may be most at risk of the disease.208 In the present study, it is important to note that Lagos State offers free education in all the public primary and secondary schools which boosts school attendance for children in the low socioeconomic class who may not otherwise be able to afford school fees. Hospital based studies provide another perspective of RHD. However, they are subject to selection (and other) biases and are often not a good representation of the community prevalence. Nonetheless, it is pertinent to note that a recent hospital-based report from one of the tertiary health facilities in Lagos reported a prevalence of RHD among children visiting the hospital over a 10-year period as 1.1/10,000 hospital visits.21
Achieving lower prevalence of RHD involves implementation of control programs and improvements in the health care systems.1 In general, good access to medical care and prompt treatment of streptococcal infections and ARF are instrumental to prevention of RHD. While there is currently no specific program targeted at the control of RHD in Nigeria, it should be noted that access to health care in Lagos State is unusually good compared to the rest of the country. Health services are provided free for all patients under 12 years of age in public health institutions. There are primary health care centers in more than 90% of all wards, 25 hospitals/secondary health centers and three university teaching hospitals/tertiary health institutions in the state. There are also numerous private medical facilities that provide services in parallel with the public institution especially in the urban areas. The density of health care institutions have been shown to be related to RHD as in a study from Uganda that showed that the risk of acquiring RHD increases with every kilometer increase from the nearest health center.22 In addition, Lagos has the highest number of health personnel in the country, including the pediatrician work force as the state had the highest proportion (17.9%) of practicing pediatricians and the highest pediatrician-child ratio in the country.23 Another factor that could be responsible for the low prevalence of RHD in our study is the nationwide indiscriminate use of antibiotics and anti-inflammatory medications for pain which are readily obtainable over the counter even without a prescription. It is therefore postulated that the easy access to these medications encourages self-medication following sore throats and probably contributes to prevention of RHD. The implication of these is that despite a high prevalence of people in the lower socioeconomic class in the city, a child with a streptococcal infection in Lagos is likely to be recognized and treated as such in the health care system and/or get antibiotics over-the-counter for having a febrile illness or sore throat. Nonetheless, the effect of socioeconomic status was still observed in the study as all cases of RHD that were identified belonged to the lower socioeconomic class.
The lack of significant difference in RHD prevalence as it relates to urban or peri-urban areas is similar to findings in Malawi and Ethiopia.14, 17 In a multicenter study across six regions in Ethiopia, although cases of definite RHD were slightly more in the urban area, the difference was not significant. On the contrary, some studies3, 18 have documented significant differences in prevalence of RHD between urban and peri-urban communities. However, it appears that the actual location is less important as a risk factor for RHD than the characteristics associated with a location such as poverty, inadequate access to health care and poor treatment of streptococcal infections.
While the absolute numbers of cases in the present study are few, many were males unlike in other studies3, 17 where females were in the majority. Our finding of male preponderance is similar to observations from other studies in Nigeria including a tertiary health facility in Lagos.21, 24 Other studies from Africa14, 15 have reported no significant difference in prevalence between gender and a recent systematic review and meta-analysis of 33 studies on RHD also reported no significant differences in the overall prevalence between girls and boys.25 In our series, older children had RHD with no case in children less than ten years of age. A recent report from Australia similarly documented the highest number of cases of RHD to be in children aged 10–14 years.26 This is comparable to observations from other studies on children where prevalence of RHD increased with advancing age. 25 – 27 Recurrent attacks of ARF and resultant cumulative damage to the heart were contributory factors.
Sub-clinical manifestation of RHD detected by echocardiography was 10 times more prevalent than clinical RHD in this present study. This is similar to an early report from Cambodia and Mozambique with 10 times greater prevalence of RHD from echocardiographic screening compared to clinical screening.3 This pattern of higher sensitivity of echocardiography in identifying cases of RHD in a screening exercise has equally been reported by several other studies with varying rates.13–18 A meta-analysis of nine studies pooled from different regions of the world including Africa revealed that clinically silent RHD was seven to eight times higher than clinically manifest RHD.25 These findings further confirm the usefulness of echocardiography in early diagnosis of RHD and opportunity for early commencement of secondary prophylaxis with an anticipated outcome of reduced morbidity and mortality.
The mitral valve was the most commonly affected heart valve. This pattern of rheumatic valve disease in children has been widely reported.13–20 Mitral regurgitation remains the commonest cardiac pathological finding in children. Similar to our findings in this present study, no other study from Africa using the WHF criteria for echocardiographic screening of RHD has reported heart valve stenosis except one study in Ethiopia17 with mitral stenosis. This is largely because while our study population was predominantly children, the report from Ethiopia with mitral stenosis, had a population that extended beyond childhood into adulthood. RHD is known to be a progressive disease with ongoing valvular scarring and remodeling that occur even in the absence of recurrent episodes of ARF. 28 None of the identified cases of RHD had evidence of a recent Strep infection using ASO titer. This could partly explain the lack of recollection of sore throat or ARF by all the cases with RHD. Findings similar to reports from South Africa and Ethiopia.16 Many cases of asymptomatic sore throats preceding ARF have also been reported.29
One limitation of the present study is that it examines only a single region of a diverse and populous country with marked variation in socioeconomic indices, access to health care and other key health and economic indices between different regions. Notably, hospital-based studies on RHD have reported contrasting prevalence rates of RHD with the northern region of the country having a significantly higher rate. 30, 31 Related studies in recent times have shown no change in the disparity of RHD prevalence across the two regions.21, 27 Therefore, our estimates may not be generalizable to other parts of the country.
Control of RHD remains important in Nigeria, as in other sub Saharan African countries. An important public health question is whether screening is a cost-effective tool for control of RHD. In this regard, it is important to note that to detect one case of RHD among apparently healthy school children in Lagos, Nigeria, 400 children have to undergo echocardiography. The yield from clinical screening is lower still. Thus, methods other than screening might be more cost-effective. The recent adoption of a global resolution on ARF and RHD by member states of WHO should be a catalyst to the much needed action in the outlined areas of strengthening primary and secondary prevention of ARF and RHD, integrating RHD services into primary health care, securing a reliable supply of benzathine penicillin G for prophylaxis, and ensuring a well-resourced and trained health workforce to provide RHD services.32 In addition, instituting and implementing economic policies that will improve the standard of living of citizens is critical in ensuring the elimination of RHD.
Conclusion
We estimated the prevalence of RHD in school children in Lagos, Nigeria, to be 2.7/1000 using echocardiography and the WHF criteria. The observed prevalence was low compared to other African countries. These findings provide an up-to-date picture of the burden of RHD in this part of Nigeria and yielded useful information for input into program planning. Given varying disease burden by country and often within country differences, both national and targeted sub-national estimates would be helpful to guide prevention and control efforts.
Acknowledgements
We acknowledge the support of the Lagos State Ministry of Education and Tutor Generals of Educational districts I11 and VI for the secondary schools and SUBEB for primary schools, as well as Head and entire staff of the schools whose students were studied. We also appreciate the assistance of interns and residents in the cardiology units of LUTH. We are grateful to Mr Peter Udoh and Mr Silas John for their technical support.
This work was supported by the Central Research Committee grant of University of Lagos, Nigeria (CRC No. 2015/14). Funding source had no involvement in the study design, data collection, analysis and interpretation of data, writing of the report, and in the decision to submit the article for publication.
References
- 1.Watkins DA, Johnson CO, Colquhoun SM, Karthikeyan G, Beaton A, Bukhman G et al. Global, Regional, and National Burden of Rheumatic Heart Disease, 1990–2015. N Engl J Med 2017; 377(8):713–22. [DOI] [PubMed] [Google Scholar]
- 2.Beaton A, Okello E, Lwabi P, Mondo C, McCarter R, Sable C. Echocardiography Screening for Rheumatic Heart Disease in Ugandan School children. Circulation 2012; 25:3127–3132. [DOI] [PubMed] [Google Scholar]
- 3.Marijon E, Ou P, Celermajer DS, Ferreira B, Mocumbi AO, Jani D et al. Prevalence of Rheumatic Heart Disease Detected by Echocardiographic Screening. N Engl J Med 2007; 357:470–6. [DOI] [PubMed] [Google Scholar]
- 4.Kane A, Mirabel M, Toure K, Périer MC, Fazaa S, Tafflet M et al. Echocardiographic screening for rheumatic heart disease: age matters. Int J Cardiol 2012;168(2):888–91. [DOI] [PubMed] [Google Scholar]
- 5.Zühlke L, Mirabel M, Marijon E. Congenital heart disease and rheumatic heart disease in Africa: recent advances and current priorities. Heart 2013; 99:1554–1561. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Remenyi B, Wilson N, Steer A, Ferreira B, Kado J, Kumar K, Lawrenson J, Maguire G, Marijon E, Mirabel M, et al. 2012. World Heart Federation criteria for echocardiographic diagnosis of rheumatic heart disease – an evidence-based guideline. Nature Reviews Cardiology 9 297–309. (10.1038/nrcardio.2012.7) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ogunbi O, Fadahunsi HO, Ahmed I, Animashaun A, Daniel SO, Onuoha DU et al. An epidemiological study of rheumatic fever and rheumatic heart disease in Lagos. Journal of Epidemiology and Community Health 1978; 32:68–71 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lagos State Government. Poverty profile for Lagos State 2014. Available at https://mepb.lagosstate.gov.ng/wp-content/uploads/sites/29/2017/01/Poverty-Profile-for-LASG-2014.pdf Accessed 07 03 2019
- 9.National Population Commission. Population of Lagos State. Available at http://www.population.gov.ng Accessed 19 03 2015
- 10.http://www.citymayors.com/statistics/urban_growth1.html Accessed 06062018
- 11.Oyedeji GA. Socio‑economic and cultural background of hospitalized children in Ilesha. Niger J Paediatr 1985;12:111–7. [Google Scholar]
- 12.Steer AC, Vidmar S, Ritika R, Kado J, Batzloff M, Jenney AW et al. Normal ranges of streptococcal antibody titers are similar whether streptococci are endemic to the setting or not. Clin Vaccine Immunol 2009; 16:172–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ploutz M, Lu JC, Scheel J, Webb C, Ensing GJ, Aliku T et al. Handheld echocardiographic screening for rheumatic heart disease by non-experts. Heart 2016; 102:35–39. [DOI] [PubMed] [Google Scholar]
- 14.Sims Sanyahumbi A, Sable CA, Beaton A, Chimalizeni Y, Guffey D, Hosseinipour M et al. School and Community Screening Shows Malawi, Africa, to Have a High Prevalence of Latent Rheumatic Heart Disease. Congenit Heart Dis. 2016. December;11(6):615–621 [DOI] [PubMed] [Google Scholar]
- 15.Kotit S, Said K, ElFaramawy A, Mahmoud H, Phillips DIW, Yacoub MH. Prevalence and prognostic value of echocardiographic screening for rheumatic heart disease. Open Heart 2017; 4:e000702. doi: 10.1136/openhrt-2017-000702 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Engel ME, Haileamlak A, Zühlke L, Lemmer CE, Nkepu S, van de Wall M et al. Prevalence of rheumatic heart disease in 4720 asymptomatic scholars from South Africa and Ethiopia. Heart 2015; 101:1389–1394. [DOI] [PubMed] [Google Scholar]
- 17.Yadeta D, Hailu A, Haileamlak A, Gedlu E, Guteta S, Tefera E. Prevalence of rheumatic heart disease among school children in Ethiopia: A multisite echocardiography-based screening. Int J Cardiol. 2016. October 15;221:260–3. doi: 10.1016/j.ijcard.2016.06.232 Epub 2016 Jul 1. [DOI] [PubMed] [Google Scholar]
- 18.Ngaïdé AA, Mbaye A, Kane A, Ndiaye MB, Jobe M, Bodian M et al. Prevalence of rheumatic heart disease in Senegalese school children: a clinical and echocardiographic screening. Heart Asia 2015; 7:40–45. doi: 10.1136/heartasia-2015-010664 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Musuku J, Engel ME, Musonda P, Lungu JC, Machila E, Schwaninger S, Mtaja A, Mulendele E, Kavindele D, Spector J, Tadmor B, Gutierrez MM, Van Dam J, Colin L, Long A, Fishman MC, Mayosi BM, Zühlke LJ. Prevalence of rheumatic heart disease in Zambian school children. BMC Cardiovasc Disord. 2018. July 3;18(1):135. doi: 10.1186/s12872-018-0871-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Roberts K, Maguire G, Brown A, Atkinson D, Reményi B, Wheaton G, et al. Echocardiographic screening for rheumatic heart disease in high and low risk Australian children. Circulation 2014; 129:1953–61. [DOI] [PubMed] [Google Scholar]
- 21.Animasahun BA, Wobo ADM, Itiola AY, Adekunle MO, Kusimo OY, Bode Thomas F. The burden of rheumatic heart disease among children in Lagos: how are we faring? The Pan African Medical Journal. 2018; 29:150. doi: 10.11604/pamj.2018.29.150.12603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Okello E, Kakande B, Sebatta E, Kayima J, Kuteesa M, Mutatina B et al. Correction: Socioeconomic and Environmental Risk Factors among Rheumatic Heart Disease Patients in Uganda. PLOS ONE 2013; 8(12): 10.1371/annotation/c6d4b7b9-bf5f-4d99-8df7-027ce99daf50 10.1371/annotation/c6d4b7b9-bf5f-4d99-8df7-027ce99daf50 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Ekure EN, Esezobor CI, Balogun MR, Woo JG, Mukhtar-Yola M, Ojo OO et al. Paediatrician Workforce in Nigeria: Impact on Child Health. Paediatric Association of Nigeria Technical Report. Niger J Paed 2013; 40 (2): 112–118 [Google Scholar]
- 24.Akpa M, Dodiyi-Manuel S, Agada Z, Odia O. Rheumatic heart disease in Port Harcourt, Nigeria: clinical, demographic and echocardiographic features. Port Harcourt Med J. 2012; 6: 3. [Google Scholar]
- 25.Rothenbühler M, O’Sullivan CJ, Stortecky S, Stefanini GG, Spitzer E, Estil J et al. Active surveillance for rheumatic heart disease in endemic regions: a systematic review and meta-analysis of prevalence among children and adolescents Lancet Glob Health 2014;2: e717–26 [DOI] [PubMed] [Google Scholar]
- 26.Cannon J, Roberts K, Milne C, Carapetis JR. Rheumatic Heart Disease Severity, Progression and Outcomes: A Multi‐State Model. J Am Heart Assoc. 2017; 6:e003498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Sani UM, Ahmed H, Jiya NM. Pattern of acquired heart diseases among children seen in Sokoto, North-Western Nigeria. Niger J Clin Pract 2015; 18:718–25 [DOI] [PubMed] [Google Scholar]
- 28.Sika-Paotonu D, Beaton A, Raghu A, et al. Acute Rheumatic Fever and Rheumatic Heart Disease 2017. March 10 [Updated 2017 Apr 3]. In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes: Basic Biology to Clinical Manifestations [Internet]. Oklahoma City (OK): University of Oklahoma Health Sciences Center; 2016- Available from: https://www.ncbi.nlm.nih.gov/books/NBK425394/ [PubMed] [Google Scholar]
- 29.Veasy LG, Tani LY, Hill HR. Persistence of acute rheumatic fever in intermountain area of united states. J Pediatr. 1994; 124:9–26. [DOI] [PubMed] [Google Scholar]
- 30.Okoromah CAN, Ekure EN, Ojo OO, Animasahun BA and Bastos MI Structural heart disease in children in Lagos: profile, problems, and prospects. Niger Postgrad Med J. 2008. June;15(2):82–8. 2008 Jun; 15 (2):82–8. [PubMed] [Google Scholar]
- 31.Bode-Thomas F, Ige OO, Yilgwan C. Childhood acquired heart diseases in Jos, north central Nigeria. Niger Med J 2013; 54:51–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.RHD ACTION. Breaking News: Governments Adopt a Global Resolution on Rheumatic Fever and Rheumatic Heart Disease at the World Health Assembly. Available from: http://rhdaction.org/news/ Accessed 04 06 2018