

Abstract
The establishment of physical training programs for people living with HIV/AIDS (PLWHA) has several benefits. The study aimed to analyze the effect of resistance training using prediction of intensity by subjective perception of effort (SPE) on body composition, muscle strength, and TCD4+ lymphocyte levels in PLWHA. This a randomized controlled trial study. Participants (11 men and 8 women), were divided in two groups: exercise group (EG) and control group (CG). The EG was submitted to 12 weeks of a resistance-training program based in the prediction of intensity by SPE. Body mass percentages were evaluated using tetrapolar bioelectrical impedance and skinfold methods. We used Flow Cytometry to quantify CD4+ T lymphocytes. Patients showed significant changes in Body Fat Percentage (Δ%=-6.23%), Lean Body Mass (Δ%=2.45%), and CD4T lymphocytes levels (Δ%=15.77%). They also showed significant increase in muscular strength presented in the test for one repetition maximum in all the evaluated exercises. Our data suggest that exercising program prescribed by SPE is capable of improving immune function, body composition, and muscular strength in PLWHA.
Key words: AIDS, body composition, immunity, muscle strength, resistance training
Introduction
The practice of physical activity has been essential for the prevention of physical and emotional disorders and maintenance of better quality of life in individuals with chronic diseases. Resistance training uses the muscular framework to perform specific movements with overloads, with the purpose of generating physiological adaptations. This type of training can be used as a resource to reduce the depletion of muscle functionality due to its chronic effects.1
The prescription of intensity of the loads in resistance exercises is one of the most impressive factors to guarantee the results on muscular hypertrophy. This deserves special attention in PVHA in antiretroviral therapy due the fact that many components of the immune system present adverse responses to strenuous and/or longterm exercise.2 Thus, for the monitoring and control of intensity during resistance exercise in PLWHA, subjective perception of effort (SPE) has can great support, especially due to its close relationship with key physiological stress markers during exercises. 3 The SPE can be defined as the interaction of peripheral signals (muscles and joints) and central signals (ventilation) that, after the interpretation of the sensory cortex, produces an individual perception of the effort for the person in a global or localized way in the body related to the commitment to perform certain activity. Based on this perspective, SPE would be produced through the translation of sensory stimuli through a feedback mechanism.4
The establishment of physical training programs to PLWHA has very important and has several benefits, as increase functional status in patients with HIV wasting, both by increasing strength and by increasing lean body mass.5 Aerobic and concurrent training improve maximal oxygen consumption (Vo2 max), likewise resistance and concurrent training improve muscular strength, but did not cause changes in CD4 T cell expression.6 In this way, the exercise may play a role of an important complementary therapy to patients using antiretroviral, since the Antiretroviral therapy (ART) promotes significant improvement in the quality of life of PLWHA, also psychological and social, as well as prolonging the patient’s survival and reducing the possibility of transmission of the virus to others. However, this modality of treatment presents a series of adverse reactions, being the lipodystrophy syndrome one of the most severe of them. This change is characterized by the deformed accumulation of fat, and causes an increased risk for cardiovascular diseases and metabolic disorders.7
The prediction of intensity by the SPE is based on the individual response of each subject to the effort, expressed in a scale form, and has the advantage of greater adherence to training programs, compared to training with imposed intensities for healthy individuals.8 However, few studies have evaluated its use and beneficial effects in PLWHA. Therefore, the present study aimed to analyze the effect of resistance training, based in SPE, on body composition, muscle strength, and CD4+ T lymphocyte levels in PLWHA.
Materials and Methods
Subjects
This study enrolled 19 patients (11 men and 8 women), with an average age of 39.16±5.11 years, diagnosed over a year by the Brazilian Unified Health System (SUS) as PLWHA, who presented TCD4+ lymphocyte count equal to or greater than 380 cells/mm3; submitted to standard antiretroviral therapy, provided by the Unified Health System; and performed regular clinical follow-up at the Rafael Fernandes Hospital, located in the city of Mossoró- RN, Brazil. The individuals were divided into two randomized groups: Exercise Group [(EG) - 6 men and 3 women]; and Control Group [(CG) - 5 men and 5 women]. Excluded from participation were subjects who used androgens, growth hormone, or glucocorticoid therapy; those who were receiving current therapy with insulin, had a history of diabetes mellitus; individuals actively engaged in substance abuse; pregnant women, actively seeking pregnancy or women, or breastfeeding; or individuals who underwent an acute infection or initiated a new antiretroviral therapy regimen within 1 month of the study. The sample size was selected by convenience.
Ethical aspects
The study was conducted in accordance with the Declaration of Helsinki and had its ethical aspects evaluated and approved at 12/18/15 by the Ethics Committee of the University Hospital Onofre Lopes (Hélio Roberto Hekis - coordinator) under the number 1,375,236 and C.A.A.E. 46999015.0.0000.5292. All subjects have signed a written informed consent.
Training protocol
The individuals were divided into two groups: exercise group (EG) and control group (CG). The EG, consisting of nine individuals (6 men and 3 women) was submitted to one week of familiarization with resistance exercises and SPE, consisting of two sessions with intervals between 48 hours, using 3 sets of 6 to 8 repetitions per exercise, between the indexes 6 and 7 of the OMNI-Resistance Exercise Scale (OMNIRES). When used in the context of perceived exertion metrics, OMNI means a Ratings Perceived Exertion (RPE) scale having broadly generalizable properties. The scale has both verbal and mode specific pictorial descriptors distributed along a comparatively narrow numerical response ranging from 0-10. The pictorial descriptors depicting a weight lifter are positioned along the response range consonant with corresponding verbal descriptors. The scale is presented in a visually discernible exertional format, i.e., an intensity gradient.3
After the week of familiarization, the EG was submitted to 12 weeks of a resistance- training program, with two weekly sessions, fixedly distributed on Mondays and Thursdays in the morning. The program was composed of three sets, with 1-minute rest between them, performing 8 to 10 repetitions of the following exercises − performed in this order, both during the week of familiarization and in the 12 weeks of intervention − bench press, leg press 45°, lat pulldown, knee flexion, elbow flexion, ankle extension, and triceps pulley. The participants used free weight or weight assisted machines to perform the exercises. Before each intervention, the EG was submitted to a warming stage performing five minutes of ergometer cycling in comfortable intensity.
The participants were questioned about SPE at the end of each series, demonstrating how they felt about the exercise through the OMNI-RES scale, using loads related to indexes 7 and 8 of the same scale during the 12 weeks of intervention. The individual intensity of the exercises was progressively altered according to the evolution of the participants in order to maintain the SPE in the indices 7 to 8. The training was realized at the Department of Physical Education, University of Rio Grande do Norte, Mossoró, Brazil, under supervising of a physical educator.
The control group, consisting of 10 participants (5 men and 5 women), did not undergo any training program and did not have their routine altered, being instructed not to practice any physical exercise during the 12-week period, as well as the EG was instructed not to perform any exercise other than those performed in the present study. None of the groups underwent dietary control.
Experimental procedures
Anthropometric characteristics assessment
Scales and stadiometer, respectively measured body mass and height. Fat and lean body mass percentages were evaluated using the methods of tetra-polar bioelectrical impedance and skinfold. The skinfolds were measured three time using a Sanny® adipometer with a variation of 1 mm, the folds being measured in three shots and alternating in the right hemisphere. The skinfolds sites evaluated were subscapular and midaxillary for men; and suprailiac, abdominal and medial calf for women. It was chosen to evaluate these skinfolds sites using the protocol of Florindo,9 since it is a validated protocol for PLWHA and presents a higher correlation (r=0.92) and higher coefficient of determination (R2=0.83 for men and R2=0.81 for women) and lower standard error of the mean (SEM=2.42% for men and SEM=4.62% for women), compared to Dual-energy X-ray absorptiometry (DEXA), considered a gold standard for evaluation of body composition. One-repetition maximum (1RM - see supplementary material for loads) was performed according to Kraemer & Fry.10 1RM measurement consists of a trial and error procedure in which progressively heavier loads are lifted until the heaviest successful lift was determined. Briefly, it was realized by the following steps: warm-up from 5 to 10 replicates, lightweight (40% to 60% of the 1RM estimate); 1 minute interval; light elongation (static stretching with 10 seconds for the requested muscle group); warm-up of 3 to 5 replicates, moderate weight (60% to 80% of the 1RM estimate); 2 minutes apart; tried 1RM with a load close to the maximum, when the practitioner completed 2 to 3 repetitions, added for upper limb tests, of 4 kg to 9 kg or 5% to 10%, and for lower limb tests of 14 kg to 18 kg or 10% to 20%; repeated this step, in cases when the practitioner completed 2 to 3 repetitions - after 3 to 5 minutes of interval.
Peripheral blood CD4+ T cells count
Quantification of CD4+ T lymphocytes was performed using Flow Cytometry.11 Briefly, peripheral blood, collected with anticoagulant, was mixed with red blood cell lysis buffer and incubated with anti- CD4 (BD MultitestTM CD3/CD8/CD45/ CD4 342417). Subsequently, the samples were acquired by the FACSCaliburTM BD cytometer (Beckton, Dickinson and Company, Franklin Lakes, NJ, USA).
Statistical analysis
The normality of the distribution from the obtained data was verified through Shapiro-Wilk test. Almost all variables showed normal distribution values (P>0.05), except for the force in one repetition maximum in the knee flexion, which was not normally distributed (P=0.026).
In order to compare intragroup data, we used Paired t test. To compare the intergroup results, the Student’s t-test was used for independent samples. The Wilcoxon test was used to evaluate the maximum flexor strength, the only variable that did not present a normal distribution. The statistical analyses were performed using the SPSS software version 20.0 (IBM), and P<0.005 was considered statistically significant.
Results
Baseline Demographic Characteristics of the study participants are presented on Table 1. The patients submitted to the exercise program showed significant changes in the Body Fat percentages and lean body mass after the intervention period (Table 2 and Figure 1). It was also observed a significant increase in the muscular strength presented in the test for one repetition maximum (1RM) in all the evaluated exercises, when comparing the periods pre- and postintervention, with the highest positive variation of strength being noticed for the extension of the ankle, followed by squat, and lat pull down (Table 3). The levels of CD4+ T lymphocytes also showed a significant increase after the training period for the EG, and no similar variations were noted for the control group after the same period of time (Table 2 and Figure 2).
Table 1.
Baseline demographic characteristics.
| Variable | Exercise group (n: 9) | Control group (n: 10) | P value* |
|---|---|---|---|
| Age (years) | 37.78±2.11 | 40.40±6.69 | 0.276 |
| Height (cm) | 162.44±7.95 | 162.30±6.46 | 0.966 |
| Body weight (Kg) | 61.41± 8.56 | 67.71±4.70 | 0.060 |
| Time of HIV/AIDS diagnosis (years) | >1 | >1 | - |
Data are presented as mean ± standard deviation. n, number of participants. *Value calculated by t-student test for independent samples.
Table 2.
Body composition and immune parameters.
| Exercise Group (n: 9) | Control Group (n: 10) | P-value, baseline comparison* | P-value, treatment effect ** | |||
|---|---|---|---|---|---|---|
| Baseline | After 12 wk | Baseline | After 12 wk | |||
| Body fat (%) | 28,20±6,80 | 26,40±6,70 | 35,17±9,47 | nm | 0.086 | <0.001 |
| Lean body mass (%) | 71,80±6,80 | 73,60±6,70 | 64,83±9,47 | nm | 0.309 | <0.001 |
| CD4+ (cell/mm3) | 483.44±61.35 | 559.67±61.98 | 449.60±39.89 | 449.30±37.28 | 0.168 | <0.001 |
| HIV rna level (copies/mL) | <40 | <40 | <40 | <40 | - | - |
Data are presented as mean ± standard deviation. n, number of participants; nm; not measured.
**Value calculated by t student test for independent samples
*value calculated by paired t test.
Figure 1.
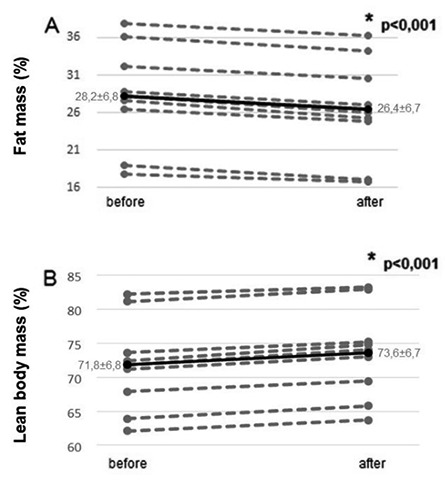
Variation of fat (A) and lean body mass (B) percentages of patients living with HIV/AIDS before and after submission to the training period. Full lines indicate the mean variation of all patients evaluated; dotted lines indicate the individual data of each study participant. P-value calculated by the Paired T test for related samples.
Table 3.
Comparison of loads used by exercise group patients in the 1RM test before and after the intervention.
| Exercises | Baseline | After 12 wk | Δ% | P |
|---|---|---|---|---|
| Bench press | 24.67±6.32 | 29.33±7.87 | 18.92 | <0.001* |
| Lat pulldown | 41.22±8.84 | 54.56±12.88 | 32.35 | <0.001* |
| Triceps pulley | 31.89±7.67 | 34.89±6.19 | 9.41 | 0.010* |
| Elbow flexion | 17.78±2.73 | 20.33±3.24 | 14.38 | <0.001* |
| Squat | 49.78±20.67 | 69.22±21.63 | 39.06 | <0.001* |
| Leg press 45° | 152.22±55.75 | 186.67±59.79 | 22.63 | <0.001* |
| Knee flexion | 37.22±5.65 | 39.22±7.12 | 5.37 | 0.042# |
| Ankle extension | 33.55±10.50 | 60.44±9.66 | 80.14 | <0.001* |
Data are presented as mean ± standard deviation. 1RM, one repetition maximum; n, number of participants.
*Significant difference calculated by paired t test
#Significant difference calculated by the Wilcoxon test.
Figure 2.
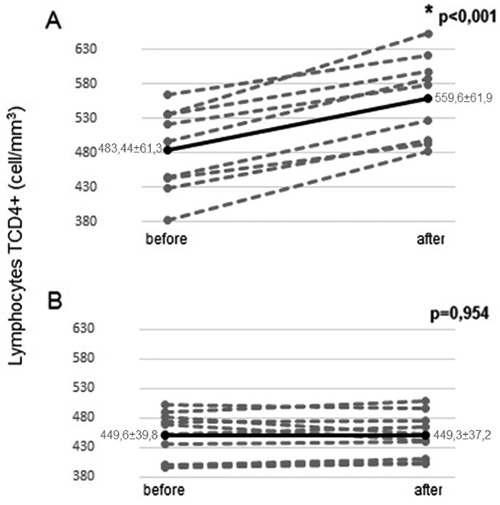
Variation of the CD4+ T lymphocytes counting of patients living with HIV/AIDS before and after submission to the training period (A) and the group that did not undergo the intervention (B). Full lines indicate the mean variation of all patients evaluated; dotted lines indicate the individual data of each study participant. P-value calculated by the Paired T test for related samples.
Discussion
The reduction in fat percentage was probably obtained as a result of the mechanisms of metabolic adaptation also observed in individuals without HIV, where a mobilization of the lipid reserves of the organism is observed in order to restore glycogen stores, both muscular and hepatic, during the rest periods between training sessions. 12 Among the possibilities of scales, already validated for use in resistance training, we opted for the intensity prescription through the SPE, using the OMNI-RES scale of Robertson et al.3 because it is a scale specifically developed for resistance training, besides an illustration directed to the modality facilitates the understanding of the participants who were not familiar with the practice. Moreover, the use of SPE as a way of prescribing training leads to the idea that decisions about exercise, modulation of intensity and interruption, go through several aspects, especially psychological ones, such as motivation and the sensation of pleasure or the meaning of exercise for the individual.13 These last aspects were very important for us at the time of deciding on the prescription of the training. The significant increase in the percentage of lean body mass, even with the use of lower intensity training, common in SPE exercise programs, indicates that even that less intense exercises are capable of generating significant gains in muscle mass for these patients. Some investigations have already shown that SPE is a reliable method for the prescription of resistance training intensity and correlates with % 1RM.14,15 In addition to what has already been mentioned, SPE has several advantages in the prescription of resistance training. The most traditional way of prescribing resistance training involves the determination of one repetition maximum (1RM) and then choose the intensity ranges (% of 1RM) in accordance with the objective.16 1RM tests are, from a practical point of view, tricky to perform, especially with people with little or no training experience. Among these difficulties, it is emphasized that these tests are specific to the exercise tested, which limits their use in the daily life of the clubs and the academies that offer their practice. The use of SPE is inexpensive, affordable, easy to use and understanding and has been validated in several populations. Thus, the training prescription from the SPE monitoring point of view, produces greater individualization of the training and, consequently, can contribute to greater adherence to the training program.8
It is believed that these gains in muscle mass occurred through sarcoplasmic hypertrophy, resulting from cellular adaptation to potentiate the number of organelles and nutrients required for muscle contraction under metabolic stress, with a lower rate of cellular micro-lesion.17 In addition to the low relative intensity, the participants were also not taken to concentric failure, and even so, they obtained improvements in the gain of lean body mass. These findings corroborate with other studies that have demonstrated that some special groups, such as pregnant women and hypertensives, can gain strength and body composition benefits with resistance training, even if they are not submitted to muscle failure or to very high training intensities.17
In the present study, the increase in lean body mass was accompanied by a sharp and significant increase in strength. Similar results were observed in other study, although they used fixed frames of load to be worked.6 Other studies with different populations that used SPE intensity prediction also observed substantial gains in strength even when the exercise intensities used according to the participants’ selection were lower than the training recommendations for their respective specificities.18,19
It is known that increased strength has two main factors: muscle hypertrophy and optimization of muscle coordination,20 which could generate greater activation of motor units to perform a certain movement.21,22 Thus, it is believed that in addition to the increase in lean body mass, the strength gains evidenced by PLWHA may have been influenced by the coordinative adaptations caused during the training period on the motor units. The most significant increases in multi-articular exercises reinforce this hypothesis of the request of a greater number of motor units, when compared to the uniarticular exercises.21,22
The significant increase in CD4+ T lymphocyte levels, found only in patients who underwent the proposed training, guided by the method of SPE, show the importance and benefits of this modality of exercise for PLWHA under ART. Physical exercise might have an immunosuppressive effect.23 Aerobic and resistance training programs of moderate intensity, to avoid possible exercise- induced immunodepression, did not harmed the levels of CD4+ T-lymphocytes in PLWHA.24 Furthermore, training with lower intensities (60-80% of 12 maximal repetitions) showed a slight enhancement trend of CD4+ T-lymphocytes in the exercise group (16%, P=0.19).25 In its turn, 3- month progressive resistance exercise training program (strength training periodization - 1RM 50-80%) was an effective and safe way to improve immune function - CD4+ cell count was increased (23%, P=0.0005), in PLWHA.26
Our intervention was based on the method of SPE. It is believed that the increase in CD4+ T lymphocytes observed in our study can be attributed to the type of training used, guided by the method of SPE, since its characteristics of moderate intensity and adequate volume of training tend to promote increase in the expression of interleukin- 2 (IL-2), important in the proliferation of T lymphocytes and increased cytotoxic activity of Natural Killer (NK) cells, essential for the death of virus-infected cells.27 In addition, the combined effects of reducing fat percentage and cardiovascular adaptations to exercise may indirectly potentiate the immune response by increasing the circulation of immune cells between lymphoid tissues and peripheral organs, reducing the production of stress-related hormones, which are associated with immunosuppression, and improve T lymphocyte signaling.27 However, other variables could affect the changes on CD4+ cell count, like patient’s age, smoking habits, use of illicit drugs, hospital treatment, changing doctors and the use of ART.
Recent meta-analyzes of primary studies using physical activity in PLWHA show that the training does not cause significant changes in circulating levels of CD4 T cells (28, 29). However, when the data from the primary studies are analyzed stratified, significant differences favoring the increase of CD4+ T cells are found in PLWHA who performed aerobic exercises three times a week as a duration between 41 and 50 minutes per session. Exercise sessions of less than 40 minutes and greater than 51 minutes were not able to cause positive changes in CD4+ T cell levels. In the same way, interval exercise had a positive effect on CD4 levels, when compared to continuous exercise (30). These contradictory results may be due to the fact that there are many variations regarding the frequency, type, mode, duration, intensity, interval, and time of the exercises used in the studies.
Finally, some limitations may have affected the results of the study. Accordingly, even with proper care, the failure to measure variables, including the hormone levels, other biochemistry markers, sleep time, and nutrition may affect, to some extent, the analysis of these results. In addition, it is important to conduct new studies examining exercises combinations, different methods, distinct and larger sample sizes.
Conclusions
Despite the use of relatively lower loads than those commonly used in strength training, 12 weeks of intervention, with resistance training and prescribed by the subjective perception of effort, were able to improve body composition, muscle strength and increase the number of CD4+ T cells in patients submitted to the training. The increase of CD4+ T cells in the circulation may be related to the intensity of the training.
We suggest that more studies with this theme be carried out, with more extensive laboratory research with a larger sample size, in order to obtain more reliable and consensual results, so that the results can be extrapolated to the entire population living with the HIV/AIDS.
Acknowledgments
The Coordination for the Improvement of Higher Education Personnel (CAPES) and the National Council for Scientific and Technological Development (CNPq) funded this study.
Funding Statement
Funding: none.
References
- 1.Gentil P, Bottaro M, Noll M, et al. Muscle activation during resistance training with no external load - effects of training status, movement velocity, dominance, and visual feedback. Physiol Behav 2017;179:148-52. [DOI] [PubMed] [Google Scholar]
- 2.Matthews CE, Ochene SE, Freedson PS, et al. Moderate to vigorous physical activity and risk of upper-respiratory tract infection. Med Sci Sports Exerc 2002;34:1242-8. [DOI] [PubMed] [Google Scholar]
- 3.Robertson RJ, Goss FL, Rutkowski J, et al. Sci Sports Exerc 2003;35:333-41. [DOI] [PubMed] [Google Scholar]
- 4.Borg GA. Psychophysical bases of perceived exertion. Med Sci Sports Exerc 1982;14:377-81. [PubMed] [Google Scholar]
- 5.Roubenoff R, Wilson IB. Effect of resistance training on self-reported physical functioning in HIV infection. Med Sci Sports Exerc 2001;33:1811-7. [DOI] [PubMed] [Google Scholar]
- 6.Dolan SE, Frontera W, Librizzi J, et al. Effects of a supervised home-based aerobic and progressive resistance training regimen in women infected with human immunodeficiency virus: a randomized trial. Arch Intern Med 2006;166:1225-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Valente AM, Reis AF, Machado DM, et al. Metabolic alterations in HIV-associated lipodystrophy syndrome. Arq Bras Endocrinol Metabol 2005;49:871-81. [DOI] [PubMed] [Google Scholar]
- 8.Williams DM, Dunsiger S, Ciccolo JT, et al. Acute affective response to a moderate- intensity exercise stimulus predicts physical activity participation 6 and 12 months later. Psychol Sport Exerc 2008;9:231-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Florindo A, Latorre M, Borelli A, et al. Validation of Equations Of Skinfold Thickness For Fat Mass Estimation In Hiv/Aids Subjects: A Comparison Of Dual Energy X-Ray Absorptiometry And Computed Tomography Of Abdomen. Rev Bras Atividade Física Saúde 2008;13:75-83. [Google Scholar]
- 10.Kraemer WJ, Fry AC. Strength testing: development and evaluation of methodology. Maud PJ, Foster C, eds. Physiological assessment of human fitness. Champaign, IL: HumanKinetics; 1995. [Google Scholar]
- 11.Neves I, Morgado MG. Immunological evaluation of human immunodeficiency virus infected individuals by flow cytometry. Memorias Instituto Oswaldo Cruz 2000;95:393-400. [DOI] [PubMed] [Google Scholar]
- 12.Egan B, Zierath JR. Exercise Metabolism and the Molecular Regulation of Skeletal Muscle Adaptation. Cell Metabolism 2013;17:162-84. [DOI] [PubMed] [Google Scholar]
- 13.Noakes TD. Time to move beyond a brainless exercise physiology: the evidence for complex regulation of human exercise performance. Appl Physiol Nutr Metab 2011;36:23-35. [DOI] [PubMed] [Google Scholar]
- 14.Haddad M, Stylianides G, Djaoui L, et al. Session-RPE Method for Training Load Monitoring: Validity, Ecological Usefulness, and Influencing Factors. Front Neurosci 2017;11:612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Sweet TW, Foster C, McGuigan MR, et al. Quantitation of resistance training using the session rating of perceived exertion method. J. Strength Cond Res 2004;18:796-802. [DOI] [PubMed] [Google Scholar]
- 16.Garber CE, Blissmer B, Deschenes MR, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc 2011;43:1334-59. [DOI] [PubMed] [Google Scholar]
- 17.Burd NA, West DWD, Staples AW, et al. Low-Load High Volume Resistance Exercise Stimulates Muscle Protein Synthesis More Than High-Load Low Volume Resistance Exercise in Young Men. PLoS ONE 2010;5:e12033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Portugal EMM, Lattari E, Santos TM, et al. Affective Responses to Prescribed and Self-Selected Strength Training Intensities. Perceptual Motor Skills 2015;121:465-81. [DOI] [PubMed] [Google Scholar]
- 19.Alves RC, Prestes J, Souza-Junior TP, et al. Acute effect of weight training at a self-selected intensity on affective responses in obese adolescents. J Exerc Physiol Online 2014;17:66-73. [Google Scholar]
- 20.Ahtiainen JP, Hoffren M, Hulmi JJ, et al. Panoramic ultrasonography is a valid method to measure changes in skeletal muscle cross-sectional area. Eur J Appl Physiol 2010;108:273-9. [DOI] [PubMed] [Google Scholar]
- 21.Cannon J, Marino FE. Early-phase neuromuscular adaptations to high- and low-volume resistance training in untrained young and older women. J Sports Sci 2010;28:1505-14. [DOI] [PubMed] [Google Scholar]
- 22.Ferrari R, Kruel LFM, Cadore EL, et al. Efficiency of twice weekly concurrent training in trained elderly men. Exp Gerontol 2013;48:1236-42. [DOI] [PubMed] [Google Scholar]
- 23.Kruger K, Mooren FC. Exerciseinduced leukocyte apoptosis. Exerc Immunol Rev 2014;20:117-34. [PubMed] [Google Scholar]
- 24.Paes LS, Borges JP, Santos FM, et al. Effects of a 2-Year Supervised Exercise Program Upon the Body Composition and Muscular Performance of HIVInfected Patients. Open AIDS J 2015;9:80-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gomes RD, Borges JP, Lima DB, Farinatti PTV. Effects of physical exercise in the perception of life satisfaction and immunological function in HIVinfected patients: Non-randomized clinical trial. Revista Brasileira Fisioterapia 2010;14:390-5. [PubMed] [Google Scholar]
- 26.Bessa A, Lopez JC, Masi DF, et al. Lymphocyte cd4+ cell count, strength improvements, heart rate and body composition of hiV-positive patients during a 3-month strength training program. J Sports Med Phys Fitness 2017;57:1051-6. [DOI] [PubMed] [Google Scholar]
- 27.Lancaster GI, Febbraio MA. Exercise and the immune system: implications for elite athletes and the general population. Immunol Cell Biol 2016;94:115-6. [DOI] [PubMed] [Google Scholar]
- 28.O’Brien KK, Tynan AM, Nixon SA, et al. Effectiveness of Progressive Resistive Exercise (PRE) in the context of HIV: systematic review and metaanalysis using the Cochrane Collaboration protocol. BMC Infect Dis 2017;17:268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Pedro RE, Guariglia DA, Peres SB, et al. Effects of physical training for people with HIV-associated lipodystrophy syndrome: a systematic review. J Sports Med Phys Fitness 2017;57:685-94. [DOI] [PubMed] [Google Scholar]
- 30.Kamitani E, Sipe TA, Higa DH, et al. Evaluating the effectiveness of physical exercise interventions in persons living with HIV: overview of systematic reviews. AIDS Educ Prevent 2017;29:347-63. [DOI] [PMC free article] [PubMed] [Google Scholar]