

Abstract
This study examined the agreement of subjective ratings of upper extremity exposures with corresponding direct measurements obtained simultaneously from workers. Psychophysical ratings of exposure, based on the Borg CR-10 scale, were obtained for the period of time in which direct measurements were acquired using electrogoniometers (wrist), electroinclinometers (shoulder) and electromyography (grip force). Subjects were selected from workers at two automobile manufacturing plants. Significant relationships between subjective ratings of wrist position and measured wrist posture or motion and between ratings of shoulder position and measured shoulder posture were not found. Ratings of manual effort were significantly correlated with directly measured grip force (% maximum voluntary contraction). Ratings of pace were significantly correlated with directly measured wrist motion and this relationship was strengthened with the addition of relative grip force as a covariate. Workers with hand/wrist symptoms provided ratings that were more strongly related to the directly measured exposures than those without symptoms. Self-report by workers is an alternative to more resource-intensive and invasive exposure assessment methods. However, the validity of workers’ self-reported exposure assessments has been questioned. The objective of this study was to examine the agreement of selected questionnaire items with corresponding direct measurements from bioinstrumentation and to provide a better understanding of worker self-reports.
Keywords: ergonomic exposure assessment, bioinstrumentation, electrogoniometry, electromyography, self-report, questionnaire
1. Introduction
Numerous methods for performing ergonomics exposure assessment have been developed. These commonly employ either observation or bioinstrumentation for determining postures and forces. The time required to use these methods for analysis of multiple exposures on multiple body parts for each subject limits their applicability to epidemiological research (Kilbom 1994). In addition, the down-time required for set-up and calibration of bioinstrumentation may interfere with production.
Analysis of posture data varies from the calculation of simple summary statistics (mean, maximum, minimum) to more complex analyses. A commonly used approach for visual assessment of postures involves determining the percentage of time spent in various posture categories (e.g. Armstrong et al. 1982, Keyserling 1986, Buchholz et al. 1996, Punnett et al. 2000). However, with the increasing use of electrogoniometers in exposure studies, the velocity and acceleration of body segment motions can also be determined. Acceleration and velocity are thought to be important factors in the development of hand and wrist musculoskeletal disorders (Marras and Schoenmarklin 1993) and may be predictive of a worker’s subjective experience and assessment of postures.
Self-report by workers is an alternative to more resource-intensive and invasive exposure assessment methods. However, several investigators have questioned the validity of workers’ self-reported exposure assessments (e.g. Wiktorin et al. 1993, Winkel and Mathiassen 1994, Viikari-Juntura et al. 1996, van der Beek and Frings-Dresen 1998, Torgén et al. 1999). Punnett et al. (1998, 2004) used a questionnaire with psychophysical ratings to obtain workers’ assessments of ergonomic exposures in automobile manufacturing. In a subset of respondents, direct measurements were also obtained of upper extremity exposures, using electrogoniometers (wrist), electroinclinometers (shoulder) and electromyography (EMG) (grip force). The objective was to examine the agreement of selected questionnaire items with the corresponding direct measurements and to provide a better understanding of worker self-reports.
2. Methods
This research was conducted at an automobile manufacturing stamping plant (SP) and an engine plant (EP) in 1998–1999. Subjects were selected from 519 workers participating in interviews and examinations carried out as part of a follow-up study of musculoskeletal disorders (Miranda et al. 2006, d’Errico et al. 2007). All workers were interviewed and examined on paid work time. A standardised, interviewer-administered questionnaire obtained demographic data, a detailed work history, information about musculoskeletal symptoms in the year preceding the interview and ergonomic exposure ratings. As part of a structured physical examination, grip and pinch strength testing by dynamometer was carried out on both hands. Other data from this examination were not used in this sub-study.
The questionnaire data on ergonomic stressors in subjects’ current jobs were collected with a set of psychophysical (relative intensity) ratings of non-neutral postures, work pace, manual forces, segmental and whole-body vibration, and mechanical pressure concentrations from tools and equipment. The Borg CR-10 scale (Borg and Ottoson 1986, Borg 1990) was used to grade subjects’ responses.
Subjects for the bioinstrumentation sub-study were chosen from those participating in the follow-up interviews. For each psychophysical item to be validated, an attempt was made to select 20 workers in each of three levels of psychophysical score. The three levels were meant to cover the range of the Borg CR-10 scale, with enough separation to differentiate between levels, i.e. the low range corresponding to a score of 1 or 2 (preferably 1), moderate to 4, 5 or 6 (preferably 5) and high to 8, 9 or 10 (preferably 10). They were sought individually on the plant floor and voluntary participation in this phase of data collection was requested.
Workers were re-interviewed immediately following the direct measurements to obtain musculoskeletal symptoms and psychophysical exposure ratings for the analysed work time. The wording of the psychophysical items that were used in the bioinstrumentation sub-study is shown in Table 1. After initial data collection at both plants, the scores from each psychophysical rating were examined for divergence from a uniform distribution. Additional workers were then recruited in order to increase the number of workers with low psychophysical ratings.
Table 1.
Wording of ergonomic exposure questions that were compared with corresponding direct measurements.
| Self-reported exposure | Wording of ergonomic exposure question |
|---|---|
| Overall physical exertion | What was the level of physical exertion as you experienced it? |
| Pace | How would you rate the pace at which you worked? |
| Shoulder positions | How awkward were your shoulder positions? |
| Arm positions | How awkward were your arm positions? |
| Wrist/hand positions | How awkward were your wrist and hand positions? |
| Manual effort | How would you rate the manual effort (grip force or muscle strength in the hands and arms) required in this job? |
| Weight of typical part | What was the weight of the most usual or typical part (or the average weight part) that you handled? |
All measurements were made on work time. Wrist postures and motions were measured using an electrogoniometer, shoulder postures were measured using an electroinclinometer and grip force was estimated using EMG. For all subjects, all three devices were used simultaneously and all measurements were made bilaterally. The study protocol was approved by the University of Massachusetts Lowell Institutional Review Board and the UAW-company Scientific Advisory Committee.
Wrist posture and motion were ascertained using biaxial flexible wire electrogoniometers (model # XM-65; Penny and Giles Blackwood Ltd., Gwent, UK). The distal endblock of the goniometer was mounted on the dorsal surface of the hand in-line and directly over the third metacarpal. While the subject’s wrist was held in full flexion, the spring between the goniometer endblocks was stretched to its extent and the proximal endblock was then mounted on the posterior surface of the wrist, so that the spring was straight when the wrist was in neutral radio-ulnar deviation. The goniometer was attached with the forearm in neutral rotation. The goniometer amplifier was then zeroed for both flexion-extension and radio-ulnar deviation. The system was precalibrated with a linear relationship between joint angle and output voltage:
Shoulder posture was evaluated using electroinclinometers (PN#960424; Desktop Laboratories, Inc., Tannersville, NY, USA) mounted on and parallel to the lateral portions of both upper arms. In this configuration, the inclinometers measured shoulder elevation with regard to gravity. The output of the inclinometer was approximately 2 volts with the arm pointed down, 3 volts with the arm horizontal and about 4 volts with the arm pointed up. The relationship between angle and output voltage was not linear and a third- order polynomial (r2 > 0.99) was used to calibrate the inclinometer.
Grip forces were estimated using surface EMG of the extrinsic finger flexors of both hands. The EMG electrodes were carefully positioned on the anterior surface of the forearm about two-thirds of the distance from the wrist to the elbow. In order to maximise the signal from the finger flexors and minimise the signal from the wrist flexors, electrode locations were palpated manually. The EMG signals were processed in hardware using a root mean square (RMS) converter with a 55 ms time constant. The processed EMG signals were calibrated to grip force using a hand dynamometer prior to data collection (Armstrong et al. 1979). Since workers were expected to rate their manual effort relative to their own strength, measured grip force was also standardised to the subject’s grip strength and expressed as a percentage of maximum voluntary contraction (% MVC).
Workers were videotaped during the direct measurements in order that the direct measurements could be associated with specific tasks. Goniometer data (four channels), inclinometer data (two channels) and electromyographic data (two channels) were stored on a data logger (Tattletale Model 5F; Onset Computer Corp., Bourne, MA, USA) at 60 Hz to allow numerical differentiation of the wrist posture data. The sampling rate chosen here was a compromise between the storage capabilities of the data logger and the requirements for numerical differentiation. Schoenmarklin (1991) determined that 300 Hz was optimal based on the requirements of maximal wrist movements. The data logger had 0.5-mega byte of memory, which allowed approximately 9 min of data collection per subject.
For each subject, the middle 5 min of data were used in the analysis. The mean posture for each plane of motion was calculated along with the maximum posture in each direction of motion. Since differentiation is a noise-producing operation, posture data were smoothed using a one-sixth of a second moving average prior to numerical differentiation to velocity and the calculated velocity data were smoothed using the same algorithm prior to differentiation to acceleration. Numerical differentiation was performed using finite difference methods. Maximum velocity and acceleration were determined for each direction of motion, and mean velocity and acceleration were calculated using absolute values.
Summary statistics were calculated for the entire population, for the two plants separately and for the departments from which nine or more workers were sampled. Simple Pearson correlation coefficients were computed at the individual level between selected exposure items and the corresponding direct measurements. When the correlation coefficient was greater than 0.20, linear regression was used to examine significance of the relationship. Multivariate linear regression modelling was then employed to explore effect modification and/or potential confounding. Covariates that were examined included symptom status, gender, age, seniority, shift and time since the start of the shift. For symptom status, subjects were dichotomised by whether or not they reported symptoms (pain, aching, stiffness, burning, cramping, soreness, numbness or tingling) in the wrist or hand immediately after the direct measurements were made. All statistical analyses were performed using Microsoft Excel (Microsoft Corporation, Redmond, WA, USA). ‘Statistical significance’ was defined as a p-value of 0.05 or less for all analyses.
3. Results
In all, 76 workers participated in the direct measurement study (Table 2). The largest groups of workers were SP welding assemblers (n = 22), followed by EP workers in engine assembly (n = 14), SP inspectors (n = 10) and large press operators (n = 9). A number of measurements were lost due to equipment failure in the field: 32 flexion/extension samples; 29 for radial/ulnar deviation; 37 for shoulder elevation; 52 for EMG. Thus, the total number of measurements that were available for analysis varied by instrument (Table 2). For workers with bilateral measures available, the mean, maximum and minimum measures for the two arms were averaged to create a single measure for each worker to correspond with the self-report data.
Table 2.
Automobile manufacturing workers (n) included in direct instrumentation sub-study, by plant and department, and number of measurements obtained with each instrument.
| Plant | Department | n | Wrist flexion/ extension measures* |
Wrist radio/ulnar deviation measures* |
Shoulder elevation measures* |
Grip force measures* |
|---|---|---|---|---|---|---|
| SP | Inspection | 10 | 10 | 13 | 6 | 1 |
| SP | Large press | 9 | 14 | 11 | 8 | 0 |
| SP | Metal finishing | 2 | 4 | 4 | 0 | 0 |
| SP | Small press | 1 | 0 | 1 | 0 | 2 |
| SP | Spot welder | 22 | 35 | 37 | 26 | 10 |
| SP | All | 44 | 63 | 66 | 40 | 13 |
| EP | Tool store | 1 | 1 | 2 | 0 | 0 |
| EP | Cutter grind | 2 | 4 | 4 | 0 | 2 |
| EP | Cylinder head machining (700) | 3 | 6 | 5 | 0 | 2 |
| EP | Cylinder head machining (701) | 1 | 2 | 2 | 2 | 0 |
| EP | Cylinder block machining | 2 | 4 | 3 | 4 | 1 |
| EP | Camshaft machining | 1 | 2 | 2 | 2 | 2 |
| EP | Piston machining | 3 | 4 | 4 | 2 | 0 |
| EP | Connecting rod machining | 2 | 4 | 4 | 2 | 4 |
| EP | Rocker arm machining | 2 | 4 | 4 | 4 | 0 |
| EP | Engine assembly | 14 | 24 | 25 | 22 | 15 |
| EP | Piston assembly | 1 | 2 | 2 | 0 | 2 |
| EP | All | 32 | 57 | 56 | 38 | 28 |
| Total | Measurements* | 76 | 120 | 122 | 78 | 41 |
| Total | Subjects** | 76 | 67 | 70 | 39 | 23 |
SP = stamping plant; EP = engine plant.
All measurements were bilateral, so total possible number of measurements was 2n.
The last row indicates the data used in the analyses. Some are unilateral measures and some are averaged bilateral measures.
Self-reported exposure ratings of pace, wrist/hand posture awkwardness and manual effort were all higher in the EP than the SP. Differences among departments in direct-measured and self-reported wrist posture were small and not statistically significant (Table 3). The workers in the EP engine assembly department had the largest wrist motion (velocity and acceleration) characteristics, followed by SP welding assemblers, especially in the flexion/extension plane. Mean flexion/extension velocity for engine assemblers was significantly higher than for SP large press operators and inspectors. The inspectors had relatively high velocities and accelerations in the radial/ulnar deviation plane. The large press operators had the least amount of shoulder elevation. Grip forces were higher in the SP than in the EP.
Table 3.
Direct-measured and self-reported exposures by plant: Automobile manufacturing workers.
| Stamping Plan Mean (SD) | Engine Plant Mean (SD) | All Mean (SD) | |
|---|---|---|---|
| Wrist goniometer measures | |||
| Mean F/E (°) | −14.75 (9.49) | −16.43 (9.91) | −15.50 (9.64) |
| Max extension | −68.39 (15.73) | −70.89 (10.90) | −69.53 (13.71) |
| Mean duration extension >45° (%time) | 6.76 (9.56) | 10.21 (13.49) | 8.38 (11.60) |
| Max flexion | 41.32 (15.23) | 51.23 (16.93) | 45.76 (16.65) |
| Mean duration flexion > 30° (%time) | 0.63 (0.82) | 1.26 (1.71) | 0.92 (1.34) |
| Mean R/U dev. (°) | −0.26 (6.32) | −1.39 (4.99) | − 0.74 (5.77) |
| Max ulnar dev. | −34.91 (10.64) | −36.64 (11.97) | −35.65 (11.18) |
| Mean duration ulnar dev. > 30° (%time) | 1.56 (4.27) | 1.76 (4.76) | 1.65 (4.46) |
| Max radial dev. | 32.20 (8.43) | 34.12 (13.27) | 33.03 (10.73) |
| Mean F/E velocity (°/s) | 25.7 (11.8) | 28.1 (11.9) | 26.8 (11.8) |
| Max extension velocity | −336.2 (139.5) | −379.5 (85.8) | −355.6 (119.6) |
| Max flexion velocity | 358.4 (129.1) | 382.7 (80.7) | 369.3 (110.0) |
| Mean R/U dev. velocity (°/s) | 16.3 (6.7) | 16.1 (7.8) | 16.2 (7.1) |
| Max ulnar dev. velocity | −194.4 (54.6) | −205.7 (65.1) | −199.2 (59.1) |
| Max radial dev. velocity | 186.2 (50.4) | 196.3 (64.5) | 190.5 (56.7) |
| Mean F/E acceleration (°/s2) | 207 (104) | 219 (102) | 212 (102) |
| Max extension acceleration | −3061 (962) | −3445 (928) | −3233 (959) |
| Max flexion acceleration | 3123 (1598) | 3454 (965) | 3271 (1353) |
| Mean R/U dev. acceleration (°/s2) | 129 (61) | 121 (61) | 126 (61) |
| Max ulnar dev. acceleration | −1719 (528) | −1838 (701) | −1770 (606) |
| Max radial dev. acceleration | 1687 (478) | 1816 (700) | 1743 (582) |
| Shoulder inclinometer measures | |||
| Mean elevation (°) | 43.5 (27.10) | 44.96 (30.95) | 44.23 (28.66) |
| Min elevation | 8.54 (26.01) | 4.02 (9.97) | 6.34 (19.76) |
| Max elevation | 138.60 (30.56) | 129.26 (38.92) | 134.05 (31.75) |
| Mean duration elevation > 60° (%time) | 18.46 (16.15) | 36.13 (24.84) | 27.53 (22.62) |
| Mean duration elevation >90° (%time) | 2.47 (4.32) | 7.63 (13.33) | 5.12 (10.22) |
| Grip electromyography measures | |||
| Mean grip force (lbs) | 18.85 (9.45) | 13.86 (7.58) | 15.60 (8.42) |
| Min grip force | 1.44 (0.88) | 1.21 (0.87) | 1.29 (0.86) |
| Max grip force | 85.41 (33.83) | 60.42 (20.06) | 69.11 (27.72) |
| Mean grip force (%MVC) | 17.65 (16.66) | 8.74 (5.77) | 11.84 (11.33) |
| Self-reported exposures | |||
| Overall physical exertion | 3.44 (1.74) | 3.21 (2.14) | 3.34 (1.91) |
| Pace | 4.14 (1.97) | 5.11 (2.61) | 4.55 (2.29) |
| Shoulder positions | 3.93 (2.21) | 4.68 (3.11) | 4.24 (2.63) |
| Arm positions | 3.42 (1.59) | 4.11 (2.97) | 3.71 (2.28) |
| Wrist/hand positions | 4.38 (2.56) | 6.03 (2.76) | 5.07 (2.75) |
| Manual effort | 4.58 (2.18) | 5.63 (2.49) | 5.02 (2.36) |
| Weight of typical part | 3.94 (1.80) | 3.77 (2.81) | 3.87 (2.24) |
F/E = flexion/extension; R/U = radial/ulnar; dev. = deviation; MVC = maximum voluntary contraction.
Self-rated wrist and hand position was not correlated with any of the electrogoniometry measurements of wrist posture or movement (Table 4), although there were weak associations (p < 0.1) with flexion–extension velocity and duration (% time) of ulnar deviation greater than 30°.
Table 4.
Pearson product-moment correlation coefficients between selected subjective ratings of exposure and corresponding direct-measured exposures.
| Self-reported exposure | Direct-measured exposure | Correlation |
|---|---|---|
| Wrist/hand positions | Flexion–extension posture | −0.03 |
| Wrist/hand positions | Radio–ulnar posture | −0.12 |
| Wrist/hand positions | Flexion–extension velocity | 0.22 |
| Wrist/hand positions | Radio–ulnar velocity | 0.12 |
| Wrist/hand positions | Flexion–extension acceleration | 0.20 |
| Wrist/hand positions | Radio–ulnar acceleration | 0.10 |
| Wrist/hand positions | Duration wrist extension >45° | 0.10 |
| Wrist/hand positions | Duration wrist flexion > 30° | −0.17 |
| Wrist/hand positions | Duration wrist ulnar dev. > 30° | 0.23 |
| Arm positions | Duration shoulder elevation > 60° | −0.08 |
| Arm positions | Duration shoulder elevation > 90° | 0.20 |
| Shoulder positions | Shoulder elevation | −0.04 |
| Shoulder positions | Maximum shoulder elevation | −0.20 |
| Shoulder positions | Duration shoulder elevation > 60° | −0.11 |
| Shoulder positions | Duration shoulder elevation > 90° | 0.13 |
| Shoulder positions | Flexion–extension velocity | 0.37*** |
| Shoulder positions | Radio–ulnar velocity | 0.31* |
| Shoulder positions | Flexion–extension acceleration | 0.36*** |
| Shoulder positions | Radio–ulnar acceleration | 0.31** |
| Manual effort | Grip force | 0.12 |
| Manual effort | Maximum grip force | −0.18 |
| Manual effort | Grip force (%MVC) | 0.52* |
| Overall physical exertion | Grip force (%MVC) | 0.34 |
| Pace | Grip force (%MVC) | 0.09 |
| Pace | Duration wrist extension >45° | 0.23 |
| Pace | Flexion–extension velocity | 0.38*** |
| Pace | Radio–ulnar velocity | 0.28* |
| Pace | Flexion–extension acceleration | 0.40*** |
| Pace | Radio–ulnar acceleration | 0.28* |
| Weight of typical part | Grip force | 0.13 |
| Weight of typical part | Grip force (%MVC) | 0.25 |
dev. = deviation; MVC = maximum voluntary contraction.
p < 0.05.
p < 0.01.
p < 0.005.
There was no association between rating of shoulder position and any of the directly measured shoulder variables (mean posture angle, maximum angle or percent time with arm above 60° or 90°). Shoulder position was moderately correlated with all four wrist motion measurements, but each one was only able to explain 10% or less of the variability in the shoulder position ratings (Table 4).
There was a weak, but not significant, correlation between self-reported manual effort and grip force (N) as estimated from EMG and calibrated to force on an absolute scale. This relationship was much stronger and significant when grip force was expressed as a percentage of each subject’s strength (%MVC) (Figure 1). Although there was a substantial amount of scatter around the regression line, the resulting regression equation was able to explain 27% of the variability in the manual effort ratings.
Figure 1.
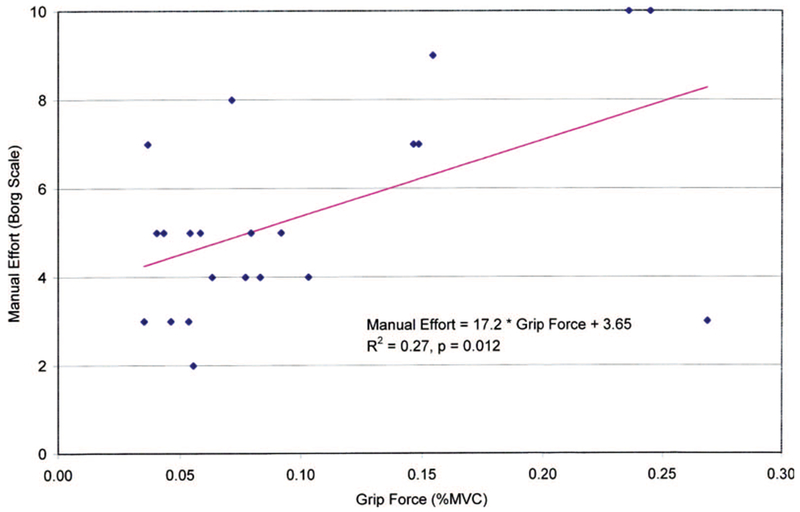
Linear regression of subjective ratings of manual effort on grip force estimated using direct measurements of muscle activity (by electromyography), standardised to grip strength. MVC = maximum voluntary contraction.
Worker ratings of overall physical exertion, their work pace and the weight of the ‘most usual or typical part’ handled were all weakly correlated with grip force expressed as a percentage of MVC (Table 4). On the other hand, work pace was moderately correlated with all of the wrist movement variables. Figure 2 shows the relationship between pace and flexion–extension acceleration. In a multivariate regression model, the combination of normalised grip force and flexion-extension acceleration predicted the psychophysical pace ratings. This relationship explained 35% of the variability in the subjective ratings of work pace:
Figure 2.

Linear regression of subjective ratings of pace on wrist flexion–extension acceleration measured using electrogoniometry.
Symptom status had a significant effect on many of the relationships between the self-reported exposures and the direct-measured exposures. For workers without hand/wrist symptoms, the slope of the relationship was negligible or negative, while for workers with symptoms the slope was substantially larger and statistically significant (Table 5, Figure 3). In fact, a significant relationship between rating of wrist/hand position and flexion-extension acceleration was found for the symptomatic subjects, although not for the pooled data.
Table 5.
Multivariate linear regression models of selected subjective ratings of exposure and corresponding direct-measured exposures, stratified on presence/absence of wrist/hand symptoms at the time of measurement.
| Self-reported exposure (Y) | Direct-measured exposure (X1) | Intercept (β0) | Slope (β1): no symptoms (X2 = 0) | Slope (β1 + β2): symptoms (X2 = 1) | R2 |
|---|---|---|---|---|---|
| Wrist/hand positions | Flexion–extension acceleration | 4.75 | −0.00128 | 0.00607* | 0.13 |
| Manual effort | Grip force (%MVC) | 5.16 | −9.91 | 9.24** | 0.45 |
| Pace | Flexion–extension acceleration |
2.98 | 0.00490 | 0.00946* | 0.21 |
MVC = maximum voluntary contraction.
Note: Slopes are determined from a single regression model with a term for interaction of the direct-measured exposures and a dummy variable for presence/absence of symptoms.
Y = β0 + β1 × X1 + β2 × X1 × X2 , where X2 = 0 or 1.
p < 0.05.
p < 0.01.
Figure 3.
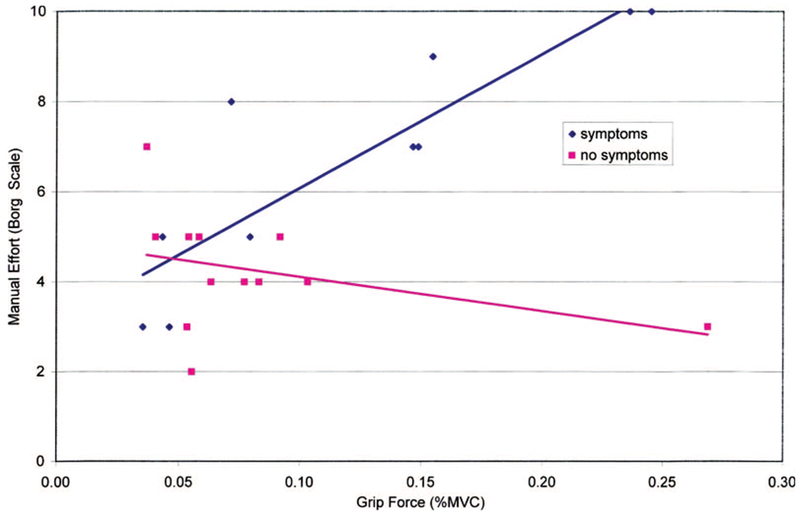
Linear regression of subjective ratings of manual effort on grip force estimated using direct measurements of muscle activity (by electromyography), standardized to grip strength and stratified on presence/absence of wrist/hand symptoms at the time of measurement. MVC = maximum voluntary contraction.
No other covariate, including gender, age, seniority, shift and time since the start of the shift, contributed to the models of any of the subjective ratings.
4. Discussion
Although differences between departments in general were not large, the departments with a large number of workers did have exposure characteristics relative to each other, which were consistent with a priori expectations. The assemblers (light, hand-intensive tasks) in both the EP and SP had higher wrist velocities and accelerations than the large press operators (heavy manual material handling) or inspectors in the SP. Grip forces were higher in the SP, where large pieces of sheet metal were handled manually, than in the EP.
There was a weak, but not significant, correlation between self-reported manual effort and grip force (N) as estimated from EMG and calibrated to force on an absolute scale. Koppelaar and Wells (2005) found moderate correlation between self-reported hand force from a visual-analogue scale and EMG of the flexor digitorum superficialis. The relationship found in this study was much stronger and significant when grip force was expressed relative to grip strength. A number of observational job analysis methods have used %MVC to express the intensity of exertion (e.g. Rodgers 1988, 1992, Moore and Garg 1995, American Conference of Governmental Industrial Hygienists 2001). Work pace rating was predicted by the combination of wrist flexion–extension acceleration and grip force relative to grip strength. This suggests that work pace may be experienced by workers as a combination of movement speed and effort. Demands on the hand–forearm system are not likely the result of grip force alone (Wells and Greig 2001).
It is interesting to note that direct measures of wrist motion were significantly associated with ratings of shoulder but not wrist posture awkwardness. Although, clearly, the shoulder and wrist are key links in the upper extremity kinematic chain, it is not obvious why only the wrist measurements should be related to shoulder posture ratings. Another direct-measured exposure that was evaluated was the percentage of time that workers’ shoulders were elevated more than 60°, which has been suggested as a threshold value for problematic shoulder postures (Bjelle et al. 1979). However, this variable did not predict any self-rated exposures.
There are many sources of potential error in the instrumentation data. The Penny and Giles goniometer has been shown to be an effective device for quantifying joint postures and motions, but when measuring flexion/extension and radial/ulnar deviation of the wrist there is cross-talk between the channels associated with wire twist due to forearm rotation (Moore et al. 1991, Buchholz and Wellman 1997). The errors due to cross-talk may be minimised with careful selection and placement of the goniometer (Wells et al. 1994, Buchholz and Wellman 1997) and/or corrected for by using an algorithm developed for this purpose (Buchholz and Wellman 1997). Newer models of the Penny and Giles goniometer have a shorter wire, so that the proximal endblock can be attached closer to the wrist, minimising twist in the wire and therefore cross-talk. In this study a goniometer model with a shorter wire was selected so that cross-talk would be minimised but would probably still exist when large forearm rotations occur.
Differentiation is a noise-inducing operation, which will lead to errors in the calculation of wrist velocity and acceleration. In addition, the sampling rate used in this study was less than the optimal rate of 300 Hz for wrist movements determined by Schoenmarklin (1991), which may result in an underestimate of the true velocities and accelerations. The velocities and accelerations found in this study are considerably less when compared with those found in the jobs measured by Marras and Schoenmarklin (1993), which is, at least in part, a result of the low sampling rate.
The electroinclinometers have been shown to be accurate within 3° for static measurement of shoulder elevation in a range of 180° (Paquet and Buchholz 1999). They use accelerometers as transducers and, therefore, dynamic activities may induce errors in these measurements. The wrist flexors are located very close to the finger flexors and are actually superficial to the finger flexors on the anterior aspects of the forearm. Wrist flexion therefore may have increased the EMG signal in some cases.
The equipment failures in the field were due to a variety of problems. The Penny and Giles electrogoniometers will wear out over time. Fortunately, the amplifier has a digital display, so these failures were noted quickly. The connectors on the electroinclinometers were subject to abrasion, which was not detected until considerable data were lost. Electromyographic data are subject to noise and artefacts due to motion. In addition, the SP was quite warm, so that workers were sweating, which led to poor conduction between the skin and electrodes. Data would appear clean during EMG calibration, but data collected during work would be noisy.
Another possible source of error, of course, is in the psychophysical exposure ratings. Workers may not recall their exposure accurately or may misunderstand the nature of the rating scales presented. In a more complex scenario, workers may both recall and understand accurately but may have difficulty partitioning physical vectors or stimuli into separate dimensions such as ‘posture’, ‘force’ and ‘vibration’ (Punnett and van der Beek 2000). There is both epidemiological and laboratory evidence that these dimensions interact with each other (e.g. Silverstein et al. 1987, Rempel et al. 1998). Thus, it may be that workers’ experience of force, for example, is so highly conditional on posture that the individual ratings do not appear valid even while the combined scores have epidemiological predictive value (Punnett et al. 2004).
The wording of the self-reported exposure question may have contributed to the lack of correlation with the direct measures. This seems especially relevant for the questions on the awkwardness of shoulder, arm and wrist/hand positions. A subjective feeling of awkwardness may not correspond to any specific posture or motion that may be directly measured and may be greater for a given posture or motion for a worker with musculoskeletal symptoms than for one without symptoms. In addition, some of the questions (e.g. wrist/hand position) may not be specific enough to correspond to a single direct measure (i.e. wrist goniometry).
An attempt was made to select workers to ensure that each subjective exposure rating to be analysed would be evenly distributed across the Borg CR-10 scale. However, at the time the direct measurements were collected, the ratings were clustered much more in the low-middle area of their respective ranges than those obtained earlier from the same subjects. The reduced ranges undoubtedly reduced the power available for analysis of correlations. This may have resulted from ‘regression to the mean’ in the ratings, or it is possible workers gave different ratings because they were actually performing different tasks at follow-up (Gold et al. 2006).
Another concern, especially for exposure data that will be utilised in an epidemiological study, is whether there might be differential error in self-reported ergonomic exposures with regard to musculoskeletal disorder symptoms (i.e. information bias). Several studies have examined the likelihood of such a systematic effect, with mixed results; some risk estimates were biased away from the null value, some towards the null and others not at all (e.g. Wiktorin et al. 1993, Viikari-Juntura et al. 1996, Torgén et al. 1999, Hansson et al. 2001). In the REBUS study follow-up population, with both absolute and psychophysical ratings of multiple physical stimuli, including work exposures, compared to laboratory measurements, Toomingas et al. (1997) found no evidence that individual subjects systematically over-rated or under-rated either exposures or symptoms. The Malmö Shoulder–Neck Study found that subjects with musculoskeletal complaints rated their exposure higher than those without complaints, even though the direct measured exposure was the same (Hansson et al. 2001).
In this study, hand/wrist symptom status did have an effect on the relationship between subjective exposure ratings and direct measures of hand force and wrist acceleration. For those with symptoms, there was a significant relationship between their rating and the direct measured exposure, while for those without symptoms there was no significant relationship. In fact, for workers with symptoms, there was a significant relationship between ratings of wrist posture awkwardness and direct measured wrist motion. This was not true for the pooled data, indicating that the workers without symptoms were diluting the relationship. Those with symptoms could have been more interested in the study and thought more carefully about their ratings, while those without symptoms may have been more likely to rate their exposure at a ‘middle’ level. Another explanation is that workers with symptoms are more conscious of their posture, either because certain postures elicit symptoms and are therefore more awkward or because individuals with symptoms are anxious to avoid aggravating them.
5. Conclusions
Direct measurements explained some of the variability in several psychophysical exposure ratings by automobile manufacturing workers. Significant relationships between self-reported manual effort and grip force measured using EMG and between workers’ ratings of pace and grip force and wrist motion directly measured were found. Musculoskeletal disorder symptom status did have an effect on these relationships; workers with hand/wrist symptoms provided ratings that were more strongly related to the directly measured exposures.
While this study does not provide a concrete answer to the question of the validity of ratings of self-reported exposure, it does provide some insight into these ratings. There are indications that the ratings used here have both a mechanical component and a psychosocial component. Due to the wording of the self-reported exposure questions, there may not have been direct correspondence with the directly measured mechanical exposures and the psychosocial component may have been emphasised.
Acknowledgements
This work was funded by grant number R01-OH03514 from the National Institute for Occupational Safety and Health (NIOSH). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of NIOSH. This research could not be possible without the assistance of the United Auto Workers and the company. Participation of the individual workers is greatly appreciated. The authors thank John Cotnam for his help with data collection and Drs. Rebecca Gore, Chang Deok Won and Kwangseog Ahn for their help with data analysis.
References
- American Conference of Governmental Industrial Hygienists, 2001. Hand activity level In: TLVs and BEIs – Threshold limit values for chemical substances and physical agents. Cincinnati, OH: ACGIH, 110–112. [Google Scholar]
- Armstrong TJ, Chaffin DB, and Foulke J, 1979. A methodology of documenting hand positions and forces during manual work. Journal of Biomechanics, 12, 131–133. [DOI] [PubMed] [Google Scholar]
- Armstrong TJ, et al. , 1982. Investigation of cumulative trauma disorders in a poultry processing plant. American Industrial Hygiene Association Journal, 43, 103–116. [DOI] [PubMed] [Google Scholar]
- Bjelle A, Hagberg M, and Michaelsson G, 1979. Clinical and ergonomic factors in prolonged shoulder pain among industrial workers. Scandinavian Journal of Work Environment and Health, 5, 205–210. [DOI] [PubMed] [Google Scholar]
- Borg G, 1990. Psychophysical scaling with applications in physical work and the perception of exertion. Scandinavian Journal of Work Environment and Health, 16, 55–58. [DOI] [PubMed] [Google Scholar]
- Borg G and Ottoson D, eds., 1986. The perception of exertion in physical work. London: MacMillan Press Ltd. [Google Scholar]
- Buchholz B, et al. , 1996. PATH: A work sampling-based approach to ergonomic job analysis for construction and other non-repetitive work. Applied Ergonomics, 26, 177–187. [DOI] [PubMed] [Google Scholar]
- Buchholz B and Wellman H, 1997. Practical operation of a biaxial goniometer at the wrist joint. Human Factors, 39, 119–129. [DOI] [PubMed] [Google Scholar]
- d’Errico A, Gore R, Gold JE, Park JS and Punnett L, 2007. Medium- and long-term reproducibility of self-reported exposure to physical ergonomics factors at work. Applied Ergonomics, 38, 167–175. [DOI] [PubMed] [Google Scholar]
- Gold JE, Park JS, and Punnett L, 2006. Work routinization and implications for ergonomic exposure assessment. Ergonomics, 49, 12–27. [DOI] [PubMed] [Google Scholar]
- Hansson G-Å, et al. , Malmö Shoulder–Neck Study Group, 2001. Questionnaire versus direct technical measurements in assessing postures and movements of the head, upper back, arms and hands. Scandinavian Journal of Work Environment and Health, 27, 30–40. [DOI] [PubMed] [Google Scholar]
- Keyserling WM, 1986. Postural analysis of the trunk and shoulders in simulated real time. Ergonomics, 29, 569–583. [DOI] [PubMed] [Google Scholar]
- Kilbom Å, 1994. Assessment of physical exposure in relation to work-related musculoskeletal disorders: what information can be obtained from systematic observations. Scandinavian Journal of Work Environment and Health, 20, 30–45. [PubMed] [Google Scholar]
- Koppelaar E and Wells R, 2005. Comparison of measurement methods for quantifying hand force. Ergonomics, 48, 983–1007. [DOI] [PubMed] [Google Scholar]
- Marras WS and Schoenmarklin RW, 1993. Wrist motions in industry. Ergonomics, 36, 341–351. [DOI] [PubMed] [Google Scholar]
- Miranda H, Gold JE, Gore R and Punnett L, 2006. Recall of prior musculoskeletal pain. Scandinavian Journal of Work Environment and Health, 32, 294–299. [DOI] [PubMed] [Google Scholar]
- Moore A, Wells R, and Ranney D, 1991. Quantifying exposure in occupational manual tasks with cumulative trauma disorder potential. Ergonomics, 3, 1433–1453. [DOI] [PubMed] [Google Scholar]
- Moore JS and Garg A, 1995. The strain index: A proposed method to analyze jobs for risk of distal upper extremity disorders. American Industrial Hygiene Association Journal, 56, 443–458. [DOI] [PubMed] [Google Scholar]
- Paquet V and Buchholz B, 1999. An evaluation of an electronic system for the continuous and simultaneous assessment of shoulder, knee and trunk postures. In: Proceedings of the Human Factors and Ergonomics Society 43rd annual meeting, 27 September – 1 October, Houston, TX. Santa Monica, CA: HFES, 656–659. [Google Scholar]
- Punnett L, 1998. Ergonomic stressors and upper extremity disorders in vehicle manufacturing: Cross-sectional exposure-response trends. Occupational and Environmental Medicine, 55, 414–420. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Punnett L, et al. , 2000. Shoulder disorders and non-neutral postures in automobile assembly workers. Scandinavian Journal of Work Environment and Health, 26, 283–291. [DOI] [PubMed] [Google Scholar]
- Punnett L and van der Beek AJ, 2000. A comparison of approaches to modeling the relationship between ergonomic exposures and upper extremity disorders. American Journal of Industrial Medicine, 37, 645–655. [DOI] [PubMed] [Google Scholar]
- Punnett L, et al. , 2004. Ergonomic stressors and upper extremity musculoskeletal disorders in automobile manufacturing: A one-year follow-up study. Occupational and Environmental Medicine, 61, 668–674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rempel DM, Dahlin L, and Lundborg G, 1998. Biological response of peripheral nerves to loading: Pathophysiology of nerve compression syndromes and vibration induced neuropathy In: Work-related musculoskeletal disorders: The research base. Washington, DC: National Academy Press. [Google Scholar]
- Rodgers SH, 1988. Job analysis in worker fitness determination. Occupational Medicine State of the Art Reviews, 3, 219–239. [PubMed] [Google Scholar]
- Rodgers SH, 1992. A functional job analysis technique. Occupational Medicine State of the Art Reviews, 7, 679–711. [PubMed] [Google Scholar]
- Schoenmarklin RW, 1991. Biomechanical analysis of wrist motions in highly repetitive, hand-intensive industrial jobs. Dissertation (PhD) Ohio State University. [Google Scholar]
- Silverstein BA, Fine LJ, and Armstrong TJ, 1987. Occupational factors and carpal tunnel syndrome. American Journal of Industrial Medicine, 11, 343–358. [DOI] [PubMed] [Google Scholar]
- Toomingas A, Alfredsson L, and Kilbom Å, 1997. Possible bias from rating behavior when subjects rate both exposure and outcome. Scandinavian Journal of Work Environment and Health, 23, 370–377. [DOI] [PubMed] [Google Scholar]
- Torgén M, et al. , 1999. Evaluation of questionnaire-based information on previous physical loads. Scandinavian Journal of Work Environment and Health, 25, 246–254. [DOI] [PubMed] [Google Scholar]
- van der Beek AJ and Frings-Dresen MHW, 1998. Assessment of mechanical exposure in ergonomic epidemiology. Occupational and Environmental Medicine, 55, 291–299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Viikari-Juntura E, et al. , 1996. Validity of self-reported physical work load in epidemiologic studies on musculoskeletal disorders. Scandinavian Journal of Work Environment and Health, 22, 251–259. [DOI] [PubMed] [Google Scholar]
- Wells R and Greig M, 2001. Characterizing human hand prehensile strength by force and moment wrench. Ergonomics, 44, 1392–1402. [DOI] [PubMed] [Google Scholar]
- Wells R, et al. , 1994. Assessment of risk factors for development of work-related musculoskeletal disorders (RSI). Applied Ergonomics, 25, 157–164. [DOI] [PubMed] [Google Scholar]
- Wiktorin C, et al. , 1993. Validity of self-reported exposures to work postures and manual material handling. Scandinavian Journal of Work Environment and Health, 19, 208–214. [DOI] [PubMed] [Google Scholar]
- Winkel J and Mathiassen SE, 1994. Assessment of physical work load in epidemiologic studies: Concepts, issues and operational considerations. Ergonomics, 37, 979–988. [DOI] [PubMed] [Google Scholar]