

Abstract
Background
Pharmacotherapies for smoking cessation increase the likelihood of achieving abstinence in a quit attempt. It is plausible that providing support, or, if support is offered, offering more intensive support or support including particular components may increase abstinence further.
Objectives
To evaluate the effect of adding or increasing the intensity of behavioural support for people using smoking cessation medications, and to assess whether there are different effects depending on the type of pharmacotherapy, or the amount of support in each condition. We also looked at studies which directly compare behavioural interventions matched for contact time, where pharmacotherapy is provided to both groups (e.g. tests of different components or approaches to behavioural support as an adjunct to pharmacotherapy).
Search methods
We searched the Cochrane Tobacco Addiction Group Specialised Register, clinicaltrials.gov, and the ICTRP in June 2018 for records with any mention of pharmacotherapy, including any type of nicotine replacement therapy (NRT), bupropion, nortriptyline or varenicline, that evaluated the addition of personal support or compared two or more intensities of behavioural support.
Selection criteria
Randomised or quasi‐randomised controlled trials in which all participants received pharmacotherapy for smoking cessation and conditions differed by the amount or type of behavioural support. The intervention condition had to involve person‐to‐person contact (defined as face‐to‐face or telephone). The control condition could receive less intensive personal contact, a different type of personal contact, written information, or no behavioural support at all. We excluded trials recruiting only pregnant women and trials which did not set out to assess smoking cessation at six months or longer.
Data collection and analysis
For this update, screening and data extraction followed standard Cochrane methods. The main outcome measure was abstinence from smoking after at least six months of follow‐up. We used the most rigorous definition of abstinence for each trial, and biochemically‐validated rates, if available. We calculated the risk ratio (RR) and 95% confidence interval (CI) for each study. Where appropriate, we performed meta‐analysis using a random‐effects model.
Main results
Eighty‐three studies, 36 of which were new to this update, met the inclusion criteria, representing 29,536 participants. Overall, we judged 16 studies to be at low risk of bias and 21 studies to be at high risk of bias. All other studies were judged to be at unclear risk of bias. Results were not sensitive to the exclusion of studies at high risk of bias. We pooled all studies comparing more versus less support in the main analysis. Findings demonstrated a benefit of behavioural support in addition to pharmacotherapy. When all studies of additional behavioural therapy were pooled, there was evidence of a statistically significant benefit from additional support (RR 1.15, 95% CI 1.08 to 1.22, I² = 8%, 65 studies, n = 23,331) for abstinence at longest follow‐up, and this effect was not different when we compared subgroups by type of pharmacotherapy or intensity of contact. This effect was similar in the subgroup of eight studies in which the control group received no behavioural support (RR 1.20, 95% CI 1.02 to 1.43, I² = 20%, n = 4,018). Seventeen studies compared interventions matched for contact time but that differed in terms of the behavioural components or approaches employed. Of the 15 comparisons, all had small numbers of participants and events. Only one detected a statistically significant effect, favouring a health education approach (which the authors described as standard counselling containing information and advice) over motivational interviewing approach (RR 0.56, 95% CI 0.33 to 0.94, n = 378).
Authors' conclusions
There is high‐certainty evidence that providing behavioural support in person or via telephone for people using pharmacotherapy to stop smoking increases quit rates. Increasing the amount of behavioural support is likely to increase the chance of success by about 10% to 20%, based on a pooled estimate from 65 trials. Subgroup analysis suggests that the incremental benefit from more support is similar over a range of levels of baseline support. More research is needed to assess the effectiveness of specific components that comprise behavioural support.
Plain language summary
Does more support increase success amongst people using medications to quit smoking?
Background
Medications (including all types of nicotine replacement therapy, bupropion and varenicline) have been shown to help people quit smoking, and people who want help to quit will often be offered medication (pharmacotherapy). Behavioural support also helps people to quit. Behavioural support may include brief advice or more intensive counselling, and may be provided face‐to‐face on a one‐to‐one basis or in groups, or by telephone, including 'quitlines'. It has been unclear how much additional benefit is gained from adding support, or providing more intensive support for people who are using medication to help them quit.
Study characteristics
We looked for studies that included smokers and provided or offered medication to everyone. People in the studies were then randomly split into groups which received different amounts or kinds of behavioural support. To assess whether the support given helped people to quit, the studies had to count the number of people not smoking after six months or more. We did not look at studies that only included pregnant women.
Key results
We searched for studies in June 2018. We included 83 studies, with almost 30,000 people. Most studies included people who wanted to quit smoking, but a small number of studies offered support to people who were not trying to quit. Combining results from 65 trials suggested that increasing the amount of behavioural support for people using a stop‐smoking medication increases the chances of quitting smoking. About 17% of people in the groups receiving less or no support quit smoking, compared to about 20% in the groups receiving more support. Providing some support via personal contact, face‐to‐face or telephone, is helpful. Few studies compared different types of support. More research is needed to find out if some types of behavioural support help more people using medication to quit smoking.
Quality of the evidence
We judged the overall quality of evidence to be high, meaning further research is very unlikely to change our results. This review has been updated twice and both times the findings remained very similar, even though many new studies were added.
Summary of findings
Summary of findings for the main comparison. Behavioural interventions as adjuncts to pharmacotherapy for smoking cessation.
| Behavioural interventions as adjuncts to pharmacotherapy for smoking cessation | ||||||
| Patient or population: People using smoking cessation pharmacotherapy Settings: Healthcare and community settings Intervention: Behavioural interventions as adjuncts to pharmacotherapy | ||||||
| Outcomes | Illustrative absolute effects* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed successful quitters without intervention | Estimated quitters with intervention | |||||
|
Pharmacotherapy (with variable level of behavioural support) |
Additional behavioural support (in addition to pharmacotherapy) |
|||||
| Smoking cessation at longest follow‐up Follow‐up: 6 ‐ 24 months | Study population1 | RR 1.15 (1.08 to 1.22) | 23,331 (65 studies) | ⊕⊕⊕⊕ high2,3 | Effect very stable over time: updates of this analysis (15 new studies added 2015; 18 new studies added 2019) have had minimal impact on the effect estimate. Little evidence of differences in effect based on amount of support or type of pharmacotherapy provided. | |
| 171 per 1000 | 197 per 1000 (185 to 209) | |||||
| The estimated rate of quitting with behavioural intervention (and its 95% confidence interval) is based on the assumed quit rate in the control group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; RR: Risk ratio; | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1Based on the control group crude average
2Sensitivity analysis removing studies at high risk of bias yielded results consistent with those from the overall analysis. A funnel plot was inconclusive but suggested there may have been slightly more small studies with large effect sizes than with small effect sizes. However, asymmetry was not clear and we did not downgrade on this basis; given the large number of included studies and the degree of homogeneity between them, it is unlikely that smaller unpublished studies showing no effect, if they existed, would significantly alter our results.
Background
Description of the condition
Giving up smoking is the most effective way for people who smoke to reduce their risk of premature death and disability. People who smoke need to quit as soon as possible using evidence‐based aids to increase their chances of success. These aids include behavioural support and pharmacotherapies.
Description of the intervention
Behavioural support interventions range from written materials containing advice on quitting to multisession group therapy programmes or repeated individual counselling in person or by telephone. Providing standard self‐help materials alone seems to have a small effect on success, but there is good evidence of a benefit of individually tailored self‐help materials or more intensive advice or counselling (Lancaster 2017; Livingstone‐Banks 2019). There is also good evidence that nicotine replacement therapy products (NRT), varenicline, and bupropion all increase the long‐term success of quit attempts (Cahill 2016; Hartmann‐Boyce 2018; Hughes 2014).
How the intervention might work
Clinical practice guidelines recommend that healthcare providers offer people who are prepared to make a quit attempt both pharmacotherapy and behavioural support. The two types of treatment are believed to have complementary modes of action, and to independently improve the chances of maintaining long‐term abstinence (Cofta‐Woerpel 2007; Hughes 1995). Although guidelines recommend intensive support to improve abstinence rates, it is also recognised that many people will not attend multiple sessions. NRT products are available over the counter without a prescription in many countries, and people who purchase them may not access any specific behavioural support. People who obtain prescriptions for pharmacotherapies may receive some support, but this may be focused on explaining the proper use of the drug and not on counselling. It therefore may be that offering additional behavioural support increases quit rates above those seen in people given pharmacotherapy alone.
Why it is important to do this review
Other Cochrane Tobacco Addiction reviews have evaluated the evidence on behavioural and pharmaceutical interventions individually (Cahill 2016; Hartmann‐Boyce 2018; Hughes 2014; Lancaster 2017; Livingstone‐Banks 2019; Matkin 2019; Stead 2017). These reviews restrict inclusion to trials where interventions are unconfounded. Trials of pharmacotherapies must provide the same amount of behavioural support (materials, advice, counselling contacts) to all participants, whether they receive active treatment, or a placebo or no medication. Likewise, when behavioural interventions are evaluated there should be no systematic difference in the offer of medications between the active and control arms of the trial. Only reviews that evaluate interventions by specific providers (e.g. nurses, Rice 2017), or in specific settings (e.g. hospitals, Rigotti 2012), may include trials of interventions that combine behavioural therapies and various medications (e.g. NRT, bupropion, varenicline).
This review is one of two that systematically identify trials of interventions that combine effective pharmacotherapies (NRT, varenicline, bupropion, nortriptyline) with behavioural support (tailored materials, brief advice, in‐person or telephone counselling). This review evaluates trials that compare different levels of behavioural intervention for people receiving any pharmacotherapy for smoking cessation, to provide an estimate of the effectiveness of intensifying behavioural support as an adjunct to pharmacotherapy, and, as such, overlaps with some separate reviews evaluating intervention types included here (e.g. Matkin 2019), which include studies of relevant behavioural therapies both on their own and as adjuncts to pharmacotherapy. The companion review (Stead 2016) includes trials in which an intervention combining pharmacotherapy and behavioural support is compared to standard care or a brief behavioural intervention without pharmacotherapy.
Objectives
To evaluate the effect of adding or increasing the intensity of behavioural support for people using smoking cessation medications, and to assess whether there are different effects depending on the type of pharmacotherapy, or the amount of support in each condition. We also look at studies which directly compare behavioural interventions matched for contact time, and where pharmacotherapy is provided to both groups (e.g. tests of different components or approaches to behavioural support as an adjunct to pharmacotherapy).
Methods
Criteria for considering studies for this review
Types of studies
Randomised or quasi‐randomised controlled trials.
Types of participants
We included trials that recruited people who smoke, recruited in any setting. We excluded trials that only recruited pregnant women; this population is considered in Coleman 2015. Trial participants did not need to be selected according to their interest in quitting, or their suitability for pharmacotherapy. However, since pharmacotherapy was offered or provided, participants were expected to be relatively motivated and prepared to use medication as part of their quit attempt.
Types of interventions
We included trials of smoking cessation interventions where all participants had access to a smoking cessation pharmacotherapy (including NRT, varenicline, bupropion and nortriptyline, or a combination or choice of these) and in which one or more intervention conditions received more intensive behavioural support than the control condition. Control group participants could be offered any level of support from minimal (e.g. written information provided as part of the medication prescription) to multisession counselling. The intervention could use different or additional types of therapy content (e.g. cognitive behaviour therapy, motivational interviewing). The additional support had to involve person‐to‐person contact which could be face‐to‐face or by telephone. In this update, we also included trials testing specific behavioural components that used a control matched for contract frequency and duration.
Types of outcome measures
Following the standard methodology of the Cochrane Tobacco Addiction Group, the primary outcome was smoking cessation at the longest follow‐up using the strictest definition of abstinence, i.e. preferring sustained over point prevalence abstinence and using biochemically‐validated rates, where available. In addition we noted any other abstinence outcomes reported, and conducted sensitivity analyses if the choice of outcome in a study might have altered the results of a meta‐analysis. We excluded studies which did not set out to assess smoking cessation at six months or longer.
Search methods for identification of studies
We identified trials from the Cochrane Tobacco Addiction Group's Specialised Register (the Register), and the clinical trials registries: clinicaltrials.gov, and the ICTRP. The Register is generated from regular searches of the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, Embase, and PsycINFO, for trials of smoking cessation or prevention interventions. We ran our most recent searches in June 2018. At the time of the search, the Register included the results of searches of the Cochrane Central Register of Controlled trials (CENTRAL), issue 1, 2018; MEDLINE (via OVID) to update 20180531; EMBASE (via OVID) to week 201824; PsycINFO (via OVID) to update 201800528. See the Cochrane Tobacco Addiction Group website for full search strategies and list of other resources searched.
We searched the Register for records with any mention of pharmacotherapy, including any type of NRT, bupropion, nortriptyline or varenicline in title, abstract or indexing terms (see Appendix 1 for the final search strategy). We checked titles and abstracts to identify trials of interventions for smoking cessation that combined pharmacotherapy with behavioural support. We also considered for inclusion trials with a factorial design that varied both pharmacotherapy and behavioural conditions. For the first version of this review, we also tested an additional MEDLINE search using the smoking‐related terms and design limits used in the standard Register search and the MeSH terms ‘combined modality therapy’ or (Drug Therapy and (exp Behavior therapy or exp Counseling)). This search retrieved a subset of records already screened for inclusion in the Register, and was used to assess whether it might retrieve studies where there was no mention of a specific cessation pharmacotherapy in the title, abstract or indexing. We did not find any additional studies from this approach, and so did not use it for subsequent updates.
Data collection and analysis
Selection of studies
For this version of the review, two reviewers (BH, HW, JHB) independently screened all studies for inclusion, with disagreements resolved by discussion or referral to a third reviewer.
Data extraction and management
For this version of the review, two reviewers (BH, HW, JHB, CM, JLB) independently extracted data and assessed risk of bias for each included study, with disagreements resolved by discussion or referral to a third reviewer. We extracted the following information:
Country and setting of trial
Study design
Method of recruitment, including any selection by motivation to quit
Characteristics of participants including gender, age, smoking rate
Characteristics of intervention deliverer
Common components: type, dose and duration of pharmacotherapy
Intervention components: type and duration of behavioural support
Control group components: type and duration of behavioural support
Outcomes: primary outcome length of follow‐up and definition of abstinence, other follow‐up and abstinence definitions, use of biochemical validation, adverse events
Sources of funding & potential conflicts of interest
Information used to assess risk of bias (see below)
Assessment of risk of bias in included studies
We evaluated studies on the basis of the randomisation procedure, allocation concealment, incomplete outcome data assessment and any other bias using the standard Cochrane methods (Cochrane Handbook 2011). We also judged studies on the basis of detection bias, according to standard methods of the Cochrane Tobacco Addiction Group. For trials of behavioural interventions (such as those included here), it is not relevant to assess performance bias as blinding of participants and personnel is not feasible due to the nature of the intervention. In these trials, we assessed detection bias based on the outcome measure; e.g. if the outcome was objective (biochemically‐validated) or if contact was matched between arms, or both, we judged the studies as having low risk of bias, but if the outcome was self‐reported and the intervention arm received more support than the control arm, we judged differential misreport to be possible and rated these studies as having high risk of bias.
Measures of treatment effect
We expressed trial effects as a risk ratio (RR) (calculated as: quitters in treatment group/total randomised to treatment group)/(quitters in control group/total randomised to control group), alongside 95% confidence intervals (CIs). A risk ratio greater than 1 indicates a better outcome in the intervention group than in the control condition.
Unit of analysis issues
We included both individually and cluster‐randomised trials. In extracting data from cluster‐randomised trials, we considered whether study authors had made allowance for clustering in the data analysis reported, and planned to use data adjusted for clustering effects, where available.
Dealing with missing data
We reported numbers lost to follow‐up by group in the 'Risk of bias' table. Following standard Cochrane Tobacco Addiction Group methods, we assumed people lost to follow‐up to be smoking and included them in the denominators for calculating the risk ratio. We have reported any exceptions to this assumption in the 'Risk of bias' table. We noted separately any deaths during follow‐up and excluded them from denominators.
Assessment of heterogeneity
We assessed statistical heterogeneity using the I² statistic (Higgins 2003). As guided by Higgins 2003, we considered a value greater than 50% as evidence of substantial heterogeneity.
Assessment of reporting biases
We used funnel plots to assess small‐study effects and investigate the possibility of publication bias.
Data synthesis
For groups of trials where we judged meta‐analysis appropriate, we pooled RRs using a Mantel‐Haenszel random‐effects model, and reported a pooled estimate with a 95% CI.
If trials had more than one intervention condition, we compared the most intensive combination of behavioural support and pharmacotherapy to the control in the main analysis.
We categorised the intensity of behavioural support in both intervention and control conditions based on two of the categories used in the US Guidelines (Fiore 2008): ‘Total amount of contact time’ (Categories: 0, 1 to 30*, 31 to 90, 91 to 300, > 300 minutes (*guideline categories '1 to 3' and '4 ‐ 30' combined for this review)) and ‘Number of person‐to‐person sessions’ (Categories: 0*, 1 to 3*, 4 to 8, > 8 (*guideline categories '0 to 1', and '2 to 3' combined for this review)). Additionally we used the number and duration of contacts as continuous predictors in meta‐regression, described below.
Subgroup analysis and investigation of heterogeneity
We used the difference in average intensity of support (number or duration of contacts) between intervention and control conditions as the main potential feature to explain any heterogeneity. In an exploratory analysis new to this version of the review, we planned to use a non‐linear meta‐regression model in R version 3.5.2 (R program) to explore the effect of difference in number and duration of contacts on intervention effect, anticipating that differences in the intensity of support would have the largest impact when the amount of contact in the control group was smallest. However, graphs of intervention effect against these factors did not provide evidence of this non‐linear trend, and so instead results were presented graphically and summarised using a standard meta‐regression model with each of the factors as a linear predictor. Studies where the intensity of support could not be determined for one or more treatment groups were excluded from the meta‐regression.
Sensitivity analysis
We considered whether the main results were sensitive to the exclusion of studies at high risk of bias in any domain. We also considered whether the definition and duration of follow‐up or the inclusion of intermediate‐intensity arms in trials with more than two relevant arms had any impact on treatment effect.
Summary of findings table
Following standard Cochrane methodology, we created a 'Summary of findings' table for our primary outcome using the five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the certainty of the body of evidence for each outcome, and to draw conclusions about the certainty of evidence within the text of the review.
Results
Description of studies
Results of the search
Our combined searches for all versions of this review retrieved approximately 3837 records. We excluded most of them as not relevant based on title and abstract. Of the records that did relate to trials of interventions for smoking cessation, most were not relevant because they were placebo‐controlled trials of pharmacotherapies, in which the behavioural support was the same for intervention and control conditions. We identified 83 studies for inclusion and listed 63 as excluded. We identified 36 ongoing studies. Further studies of combined pharmacotherapy and behavioural support that did not offer pharmacotherapy to the control group are included in Stead 2016. Some studies had multiple study arms and contributed to both Stead 2016 and to this review. The flow of studies is reported in Figure 1.
1.
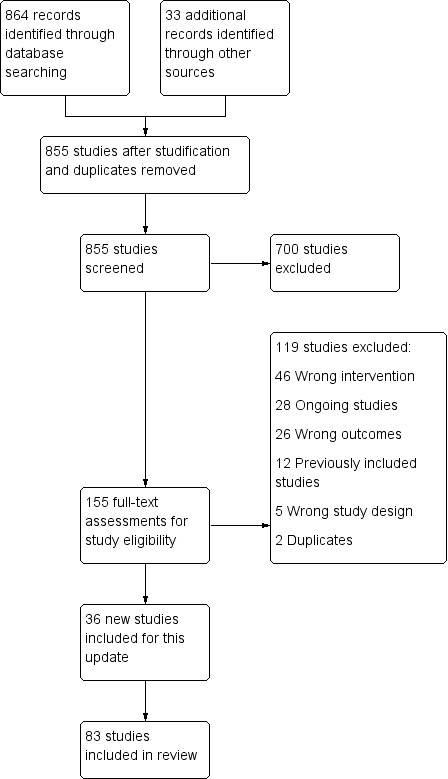
Study flow diagram for 2019 update
Included studies
We identified 83 studies as relevant for inclusion, of which 36 were new for the 2019 update. 29,536 participants are now included in relevant arms of these studies. Details of each study are given in the Characteristics of included studies table, and a summary of intervention and control group characteristics in Table 2.
1. Summary of control and intervention characteristics.
| Intervention | Control | ||||||
| Study ID | Pharmacotherapy |
Modality (included face‐to‐face/ telephone only) |
Number of contacts | Total duration (minutes) | Number of contacts | Total duration (minutes) | Comments |
| Ahluwalia 2006 | NRT | Face‐to‐face | 6 | 120 | 6 | 120 | |
| Aimer 2017 | NRT | Face‐to‐face | 4 | Unclear | Unclear | Unclear | |
| Alterman 2001 | NRT | Face‐to‐face | 16 | 4290 | 1 | 30 | Multiple arms ‐ highest vs lowest intensity |
| Aveyard 2007 | NRT | Face‐to‐face | 7 | 140 | 4 | 80 | |
| Bailey 2013 | NRT | Face‐to‐face | 19 | 950 | 10 | 500 | |
| Baker 2015 | NRT | Face‐to‐face | 17 | 1050 | 17 | 290 | |
| Bastian 2012 | NRT | Telephone | 5 | 100 | 5 | 100 | |
| Begh 2015 | NRT | Face‐to‐face | 7 | 112 | 7 | 112 | |
| Berndt 2014 | NRT | Face‐to‐face | 7 | 285 | 7 | 105 | |
| Bloom 2017 | NRT | Face‐to‐face | 20 | 400 | 20 | 880 | Exercise sessions/time excluded |
| Bock 2014 | NRT | Face‐to‐face | 3 | Unclear | 1 | Unclear | |
| Boyle 2007 | Choice | Face‐to‐face | 9 | Unclear | 0 | 0 | |
| Bricker 2014 | NRT | Telephone | 5 | 90 | 5 | 90 | |
| Brody 2017 | NRT & Bupropion | Face‐to‐face | 22 | 970 | 12 | 720 | |
| Brown 2013 | NRT | Face‐to‐face | Unclear | Unclear | Unclear | Unclear | |
| Busch 2017 | NRT | Face‐to‐face | 6 | 220 | 6 | 87.5 | |
| Bushnell 1997 | NRT | Face‐to‐face | 8 | 480 | 4 | 240 | |
| Calabro 2012 | NRT | Face‐to‐face | 2 | 120 | 1 | 5 | Intervention also had "access to 5 web‐based booster sessions" |
| Cook 2016 | NRT | Face‐to‐face | 11 | 130 | 0 | 0 | Multifactorial ‐ highest vs lowest intensity |
| Cropsey 2015 | NRT | Face‐to‐face | 4 | 100 | 1 | Unclear | |
| Ellerbeck 2009 | Choice | Face‐to‐face | 6 | Unclear | 0 | 0 | Multiple arms ‐ highest vs lowest intensity |
| Ferguson 2012 | NRT | Telephone | 6 | Unclear | Unclear | Unclear | |
| Fiore 2004 | NRT | Face‐to‐face | 5 | Unclear | 0 | 0 | Multiple arms ‐ highest vs lowest intensity |
| Gariti 2009 | Choice | Face‐to‐face | 10 | 125 | 4 | 30 | |
| Gifford 2011 | Bupropion | Face‐to‐face | 20 | Unclear | 1 | 60 | |
| Ginsberg 1992 | NRT | Face‐to‐face | 5 | Unclear | 2 | Unclear | |
| Hall 1985 | NRT | Face‐to‐face | 14 | 1050 | 4 | Unclear | |
| Hall 1987 | NRT | Face‐to‐face | 14 | 1050 | 5 | 300 | |
| Hall 1994 | NRT | Face‐to‐face | 10 | 1200 | 5 | 450 | |
| Hall 1998 | Nortriptyline | Face‐to‐face | 10 | 1200 | 5 | 450 | |
| Hall 2002 | Bupropion/Nortriptyline | Face‐to‐face | 5 | 450 | 4 | 30 | |
| Hall 2009 | NRT & Bupropion | Face‐to‐face | 11 | 330 | 5 | Unclear | Multifactorial study design |
| Hasan 2014 | NRT | Face‐to‐face | 7 | 195 | 6 | 105 | |
| Hollis 2007 | NRT | Telephone | 4 | 100 | 1 | 15 | Multiple arms ‐ highest vs lowest intensity |
| Huber 2003 | NRT | Face‐to‐face | 5 | 450 | 5 | 225 | |
| Humfleet 2013 | NRT | Face‐to‐face | 6 | 300 | 1 | 'Brief' | Multiple arms ‐ highest vs lowest intensity |
| Jorenby 1995 | NRT | Face‐to‐face | 8 | 480 | 0 | 0 | Multiple arms ‐ highest vs lowest intensity |
| Kahler 2015 | NRT | Face‐to‐face | 6 | 210 | 6 | 210 | |
| Killen 2008 | NRT & Bupropion | Face‐to‐face | 10 | 300 | 10 | 200 | |
| Kim 2015 | NRT | Face‐to‐face | 8 | 320 | 8 | 80 | |
| LaChance 2015 | NRT | Face‐to‐face | 7 | 420 | 7 | 420 | |
| Lando 1997 | NRT | Face‐to‐face | 4 | 48 | 0 | 0 | Multiple arms ‐ highest vs lowest intensity |
| Lifrak 1997 | NRT | Face‐to‐face | 20 | 736.5 | 4 | 82.5 | |
| Lloyd‐Richardson 2009 | NRT | Face‐to‐face | 5 | Unclear | 2 | Unclear | |
| MacLeod 2003 | NRT | Telephone | 5 | 60 | 0 | 0 | |
| Macpherson 2010a | NRT | Face‐to‐face | 8 | 480 | 8 | 480 | |
| Matthews 2018 | NRT | Face‐to‐face | 6 | 540 | 6 | 540 | |
| McCarthy 2008 | Bupropion | Face‐to‐face | 13 | Unclear | 13 | Unclear | Control received 80 minutes less contact than intervention |
| NCT00879177 | NRT & Varenicline | Face‐to‐face | 9 | Unclear | 5 | Unclear | |
| Ockene 1991 | NRT | Face‐to‐face | 5 | 45 | 2 | 15 | |
| O'Cleirigh 2018 | NRT | Face‐to‐face | 10 | 600 | 5 | 100 | |
| Okuyemi 2013 | NRT | Face‐to‐face | 6 | 105 | 1 | 12.5 | |
| Otero 2006 | NRT | Face‐to‐face | 4 | 240 | 1 | 20 | Multiple arms ‐ highest vs lowest intensity |
| Patten 2017 | NRT | Face‐to‐face | 36 | 1080 | 36 | 1080 | Intervention group: "exercise counselling delivered while the participant was engaged in exercise" ‐ have left this time in as also counselling |
| Prapavessis 2016 | NRT | Face‐to‐face | 64 | 1985 | 59 | 1860 | Multiple arms ‐ highest vs lowest intensity |
| Reid 1999 | NRT | Face‐to‐face | 6 | Unclear | 3 | 45 | |
| Rohsenow 2014 | NRT | Face‐to‐face | 3 | 65 | 3 | 35 | |
| Rovina 2009 | Bupropion | Face‐to‐face | 9 | 540 | 1 | 15 | Multiple arms ‐ highest vs lowest intensity |
| Schlam 2016 | NRT | Face‐to‐face | 12 | 320 | 4 | 200 | Multifactorial study design |
| Schmitz 2007a | Bupropion | Face‐to‐face | 7 | 420 | 7 | 420 | |
| Simon 2003 | NRT | Face‐to‐face | 6 | 195 | 1 | 10 | |
| Smith 2001 | NRT | Face‐to‐face | 6 | 90 | 0 | 0 | Multiple arms ‐ highest vs lowest intensity |
| Smith 2013a | NRT | Telephone | 4 | 67 | 4 | 60 | Exact duration of contact not recorded, but averages given, intervention: 67.0 (± 25.8), control: 60.1 (± 23.9) |
| Smith 2014 | Varenicline | Face‐to‐face | 5 | Unclear | 5 | Unclear | Comparing culturally‐tailored with standard counselling ‐ duration of sessions not stated |
| Solomon 2000 | NRT | Telephone | See note | See note | 0 | 0 | Control = "access to quitline"; intervention = "up to 12 calls" ‐ averaged 7 calls at 9 minutes each |
| Solomon 2005 | NRT | Telephone | 8.2 | 80 | 0 | 0 | Intervention numbers based on average number/duration of calls |
| Stanton 2015 | NRT | Face‐to‐face | 7 | Unclear | 3 | Unclear | |
| Stein 2006 | NRT | Face‐to‐face | 3 | 65 | 2 | 5 | Control offered "up to 2 visits", intervention only offered 3rd visit if ready to quit |
| Strong 2009 | Bupropion | Face‐to‐face | 12 | 1440 | 12 | 1440 | |
| Swan 2003 | Bupropion | Telephone | 4 | Unclear | 1 | 7.5 | Multiple arms ‐ highest vs lowest intensity |
| Swan 2010 | Varenicline | Telephone | 5 | 67 | 0 | 0 | |
| Tonnesen 2006 | NRT | Face‐to‐face | 12 | 270 | 10 | 150 | |
| Van Rossem 2017 | Varenicline | Face‐to‐face | 10 | 120 | 1 | 20 | Duration of sessions not stipulated, but maximum amounts recorded in paper. Intervention: 120, control: 20 |
| Vander Weg 2016 | Choice | Telephone | 6 | 150 | 0 | 0 | Intervention sessions listed as 20 to 30 minutes ‐ control was referral to a quitline, but there were no mandated sessions, so contact listed as 0 |
| Vidrine 2016 (CBT) | NRT | Face‐to‐face | 8 | 960 | 4 | 40 | Vidrine study intervention 2 (control split) |
| Vidrine 2016 (MBAT) | NRT | Face‐to‐face | 8 | 960 | 4 | 40 | Vidrine study intervention 1 (control split) |
| Wagner 2016 | NRT | Face‐to‐face | 12 | Unclear | 12 | Unclear | Sessions' duration not reported |
| Warner 2016 | NRT | Face‐to‐face | 1 | 5 | 1 | 5 | |
| Webb Hooper 2017 | NRT | Face‐to‐face | 9 | 945 | 9 | 945 | Exact duration not listed, but approximate range given |
| Wewers 2017 | NRT | Face‐to‐face | 7 | 210 | 6 | 180 | Compared 2 interventions, less intensive counted as control |
| Wiggers 2006 | NRT | Face‐to‐face | 3 | Unclear | 1 | Unclear | |
| Williams 2010 | NRT | Face‐to‐face | 24 | 1080 | 9 | 180 | |
| Wu 2009 | NRT | Face‐to‐face | 4 | 240 | 4 | 240 | |
| Yalcin 2014 | Choice | Face‐to‐face | 14 | 730 | 9 | 150 | |
Study setting, participant recruitment and motivation
Twenty‐nine studies were conducted in a healthcare setting (excluding smoking cessation clinics); this included ten studies in primary care (Aveyard 2007; Bock 2014; Cook 2016; Ellerbeck 2009; Fiore 2004; Ockene 1991; Schlam 2016; Smith 2014; Stanton 2015; Van Rossem 2017; Wagner 2016), one in a chest clinic (Tonnesen 2006), one in a cardiovascular disease outpatient clinic (Wiggers 2006), one in a rheumatology clinic (Aimer 2017), one in an immunology clinic (Stanton 2015), three in HIV clinics (Lloyd‐Richardson 2009; Humfleet 2013; O'Cleirigh 2018), one in a lesbian, gay, bisexual, and transgender health centre (Matthews 2018), one in mental health clinics (Williams 2010), one in a mental health research centre (Baker 2015), three in substance abuse clinics (Lifrak 1997; Rohsenow 2014; Stein 2006), two in a Veterans Administration hospital (Brody 2017; Simon 2003), and three in cardiac wards (Berndt 2014; Busch 2017; Hasan 2014) or any ward (Warner 2016).
Since the intervention included the provision of pharmacotherapy, many of the studies recruiting in a healthcare setting recruited volunteers who were interested in making a quit attempt, but motivation to quit was not always an explicit eligibility criterion. Wiggers 2006 used a motivational interviewing approach and participants did not all make quit attempts. Ockene 1991 offered nicotine replacement therapy (NRT) and participants were not initially selected by motivation, and Ellerbeck 2009 included a small proportion of people in the 'precontemplation stage' of the transtheoretical model.
A further four studies recruited members of health maintenance organisations (HMOs) (Boyle 2007; Lando 1997; Swan 2003; Swan 2010). Boyle 2007 proactively recruited HMO members who had filled a prescription for smoking cessation medication, while the others sought volunteers by advertising to HMO members. Universities or research facilities were the study sites for five studies (Baker 2015;Bloom 2017; Prapavessis 2016; Schmitz 2007a; Webb Hooper 2017).
Forty studies recruited community volunteers interested in quitting, including three which recruited people who were attending cessation clinics (Alterman 2001; Rovina 2009; Yalcin 2014). The study setting was not explicitly stated in four studies (LaChance 2015; Macpherson 2010a; Strong 2009; Vidrine 2016).
One study recruited adolescents (Bailey 2013); all other studies were conducted in adults.
Characteristics of intervention and control conditions
Pharmacotherapy
NRT was offered in the majority of studies, with 41 providing nicotine patch only. While most of these provided a supply of NRT for between eight and 12 weeks, three studies offered only a two‐week supply (Bricker 2014; MacLeod 2003; Warner 2016). Eight studies used nicotine gum only (Ahluwalia 2006; Ginsberg 1992; Hall 1985; Hall 1987; Hall 1994; Huber 2003; Ockene 1991; Wewers 2017), one used sublingual tablets (Tonnesen 2006), and three did not specify the type (Aimer 2017; Bushnell 1997; Wagner 2016). Five studies offered patch and/or gum (Bricker 2014; Cook 2016; Humfleet 2013; Schlam 2016; Smith 2013a). Seven studies provided bupropion alone (Cropsey 2015; Gifford 2011;McCarthy 2008; Rovina 2009; Schmitz 2007a; Strong 2009; Swan 2003), one provided nortriptyline alone (Hall 1998) and four provided varenicline alone (NCT00879177; Smith 2014; Swan 2010; Van Rossem 2017). Three studies offered a choice of pharmacotherapy; NRT or bupropion (Boyle 2007; Ellerbeck 2009), or NRT, bupropion, or varenicline (Yalcin 2014). Gariti 2009 randomised participants to NRT or bupropion using a double‐dummy design. Hall 2002 randomised participants to either bupropion or nortriptyline (placebo arms not used in this review). Three studies provided combination therapy of both NRT and bupropion (Hall 2009; Killen 2008; Vander Weg 2016).
Behavioural support
The intensity of the behavioural support, in both the number of sessions and their duration, was very varied for both intervention and control conditions.
In seven trials, there was no counselling contact for the controls: in six, participants received pharmacotherapy by mail (Boyle 2007; Ellerbeck 2009; MacLeod 2003; Solomon 2000; Solomon 2005; Vander Weg 2016), and in Fiore 2004 there was no counselling or advice for the control group although there was face‐to‐face contact with study staff. In 30 studies, the control arms had between one and three contacts (which could be face‐to‐face or by telephone) and most of these had a total contact duration of between four and 30 minutes, although three had between 31 and 90 minutes contact scheduled (Gifford 2011; Lando 1997; Reid 1999). In 34 studies, the control group was scheduled to receive between four and eight contacts, with all except eight (Aveyard 2007; Bricker 2014; Cook 2016; Gariti 2009; Kim 2015; Smith 2013a; Vidrine 2016; Wu 2009) involving a total contact duration of over 90 minutes. Twelve studies offered over eight contacts for the controls (Bailey 2013; Baker 2015; Begh 2015; Bloom 2017; Brody 2017; McCarthy 2008; Patten 2017; Prapavessis 2016; Strong 2009; Webb Hooper 2017; Williams 2010; Yalcin 2014).
Typically, the intervention involved only a little more contact than the control, so that the most intensive interventions were compared with more intensive control conditions. In five trials, the intervention consisted of between one and three sessions, with a total duration of 31 to 90 minutes in most of them (Calabro 2012; Rohsenow 2014; Stein 2006; Wiggers 2006), although Calabro 2012 also provided access to a tailored internet programme. Warner 2016 offered a brief (under 5 minutes) quitline facilitation intervention. Forty‐five studies tested interventions of between four and eight sessions, about half of which were in the 91 to 300 minute‐duration category. The remaining 32 studies offered more than eight sessions, typically providing over 300 minutes of counselling in total. The number of contacts planned was not always delivered, but generally using the average number delivered would not have changed the coding category. In a few cases where the number of contacts was either not specified or open‐ended, we coded the average number delivered and noted this in the Characteristics of included studies table.
In Analysis 1.2, we grouped trials by the number of intervention and control contacts. In 12 trials, the intervention and control condition fell into the same coding category for number of contacts (one to three contacts: Calabro 2012; Rohsenow 2014; Stein 2006; Wiggers 2006; four to eight contacts: Aveyard 2007; Bushnell 1997; Huber 2003; Tonnesen 2006; Wu 2009; more than eight contacts: McCarthy 2008; Williams 2010; Yalcin 2014). A summary of the number of sessions and duration for intervention and control conditions for each trial is provided in Table 2.
1.2. Analysis.
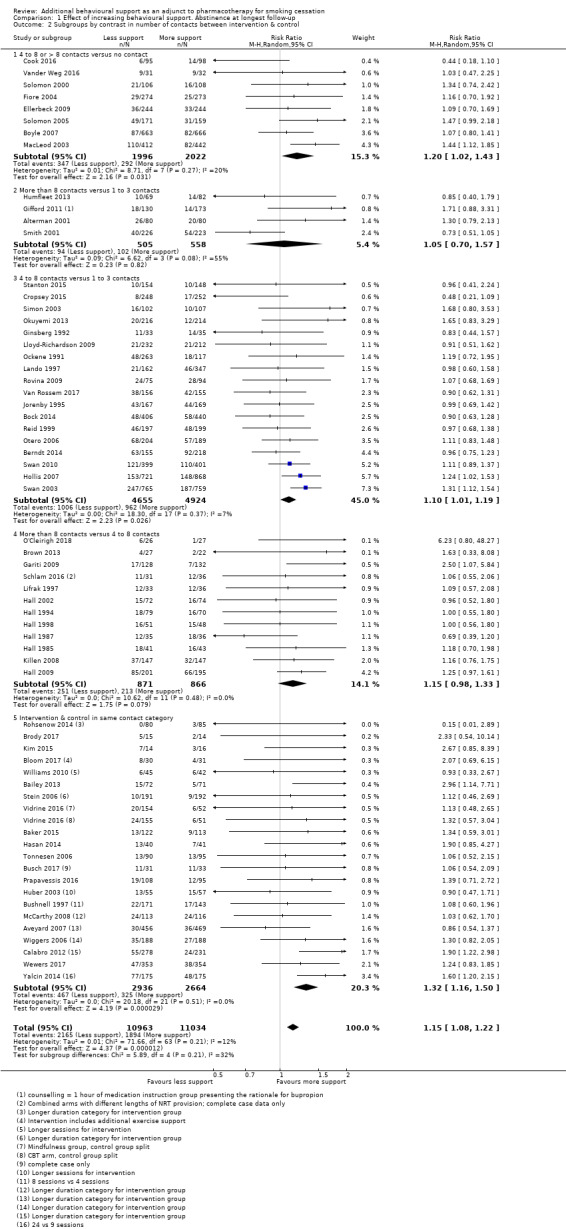
Comparison 1 Effect of increasing behavioural support. Abstinence at longest follow‐up, Outcome 2 Subgroups by contrast in number of contacts between intervention & control.
Length of follow‐up and definitions of abstinence
The majority of the included studies followed participants for a duration of six to 12 months from the target quit date, or entry into the study. Exceptions were Hall 2009 and Ellerbeck 2009 which each had a two‐year follow‐up, and Baker 2015 with a three‐year follow‐up. The design of the Ellerbeck study, in which participants were repeatedly offered support to quit, means that participants who had quit at the end of follow‐up would not necessarily have been quit for as long as two years. Thirty‐five studies only followed participants for six months.
The majority of studies reported abstinence as a prevalence measure, rather than requiring reported sustained abstinence, or abstinence at multiple follow‐up points. Fifteen studies did not attempt any biochemical verification of self‐reported abstinence; this is discussed further in Risk of bias in included studies.
Excluded studies
We listed 63 studies as excluded, along with reasons for their exclusion, in the Characteristics of excluded studies table. The majority were excluded because they provided less than six months follow‐up. Studies in which the intervention group received both pharmacotherapy and behavioural support and the control group received neither (or just brief behavioural support) were eligible for the companion review and are included or excluded there (Stead 2016).
Risk of bias in included studies
Overall, we judged 16 studies to be at low risk of bias (low risk of bias across all domains) and 21 studies to be at high risk of bias (high risk of bias in at least one domain). All other studies were judged to be at unclear risk of bias. A summary of 'risk of bias' judgements can be found in Figure 2.
2.

Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
Allocation
We judged 24 studies to be at low risk of selection bias, based on the reported method of random sequence generation and allocation concealment. We judged three studies to be at high risk of selection bias, due to the method of sequence generation (Yalcin 2014), or allocation concealment (Berndt 2014; Brown 2013; Yalcin 2014). The remaining studies did not given enough detail on one or both of these aspects so we rated the risk of bias as unclear.
Blinding (detection bias)
Following standard Cochrane Tobacco Addiction Group guidance, we did not formally assign a risk of performance bias for each trial as, due to the nature of the intervention, people providing the behavioural support could not be blinded.
We judged detection bias on the basis of biochemical validation of abstinence and, where biochemical validation was not provided, on the basis of differential levels of contact. Twelve studies were judged to be at high risk of detection bias as outcomes were via self‐report only and the intervention and control arms received different levels of support, making differential misreport possible (Aimer 2017; Berndt 2014; Boyle 2007; Cook 2016; Hollis 2007; MacLeod 2003; Ockene 1991; Otero 2006; Solomon 2005; Swan 2003; Swan 2010; Vander Weg 2016). The remainder of studies were judged to be at low risk for this domain.
Incomplete outcome data
Loss to follow‐up is often relatively high in smoking cessation trials. If trials lost fewer than 20% of participants at longest follow‐up, we judged the risk of bias to be low in this domain. In most of the included trials, the proportion lost to follow‐up was more than 20% but losses were balanced across groups and less than 40%; for these, we also classified the risk of bias as low. We rated eight studies as having unclear risk of bias, either because attrition was not reported or because overall losses to follow‐up of greater than 20% were reported and a breakdown by treatment arm was not provided (Bushnell 1997; Hall 1994; NCT00879177; Otero 2006; Schlam 2016; Smith 2001; Strong 2009; Tonnesen 2006). We judged seven studies to be at high risk of bias due to high (> 50%) attrition overall or differential rates of attrition between arms (> 20% difference between arms), as per Cochrane Tobacco Addiction Group guidance (Bock 2014; Calabro 2012; Gifford 2011; Macpherson 2010a; O'Cleirigh 2018; Smith 2014; Wagner 2016).
Other potential sources of bias
We found no studies to be at risk of other potential sources of bias.
Effects of interventions
See: Table 1
Intensive versus less intensive or no support
When comparing more intensive versus less intensive behavioural support or to no support, we pooled 65 studies contributing data to this comparison, including a total of over 23,331 participants (note: in subgroups by intervention intensity, a slightly smaller number of studies was included as, in some cases, intensity of intervention or control group contact was not clear). There was little evidence of statistical heterogeneity (I² = 8%). Hall 2002 contributed separate data to two subgroups in the primary meta‐analysis. Seventeen of the studies had point estimates below 1, that is, with higher quit rates in the less intensive condition, but all these had wide confidence intervals (CIs) which crossed the line of no effect. Seven studies detected benefits of the intervention with confidence intervals that excluded 1. The estimated risk ratio (RR) was 1.15, with 95% CI 1.08 to 1.22. This suggests that increasing the intensity of behavioural support for people making a cessation attempt with the aid of pharmacotherapy increases the proportion who are quit at six to 12 months (Figure 3; Analysis 1.1; Table 1).
3.
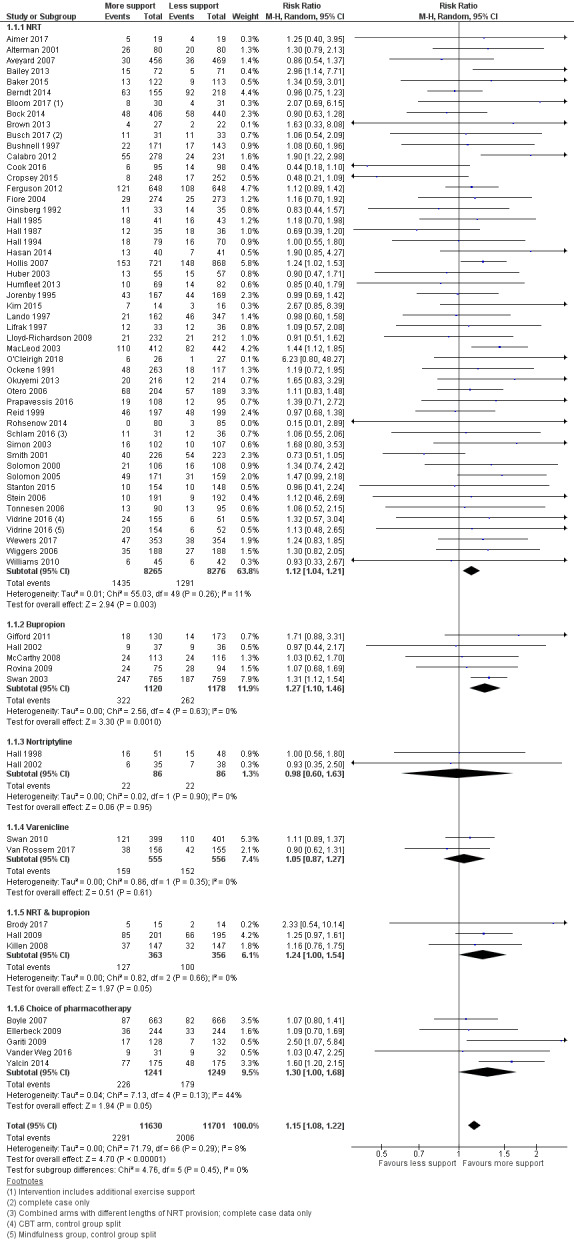
Effect of increasing behavioural support. Abstinence at longest follow‐up.
Subgroups by type of pharmacotherapy
1.1. Analysis.
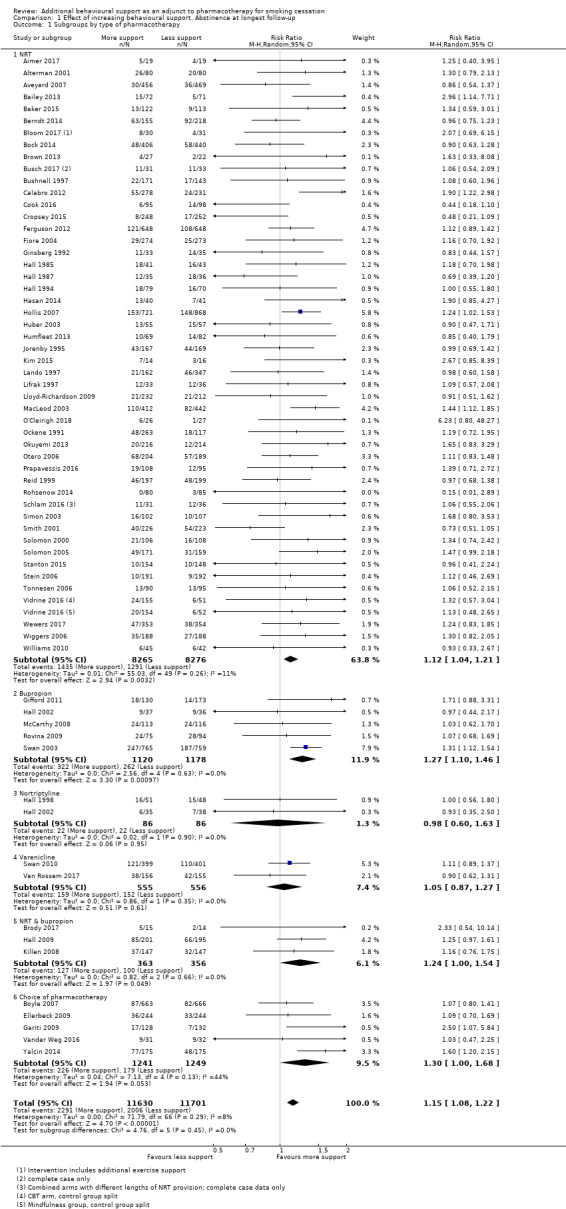
Comparison 1 Effect of increasing behavioural support. Abstinence at longest follow‐up, Outcome 1 Subgroups by type of pharmacotherapy.
Difference in pharmacotherapy
The effect size was similar across subgroups (test for subgroup differences, P = 0.45, I² = 0%). Though in some subgroups the confidence interval included no effect, this was likely to reflect the smaller number of studies and lower precision rather than a true difference in effect.
Subgroups by difference in intensity
Analysis 1.2 categorised trials based on the relative difference in the number of contacts between groups, with the subgroups with the largest contrast in intensities listed first and studies where the intensity of intervention and control fell into the same category shown last. There was little evidence of subgroup differences (P = 0.21, I² = 32%) nor was there evidence of any dose‐response. We did not repeat this approach for duration of intervention categories, as inspection suggested that the number of studies falling into different categories was small and that further subgroup analysis could be misleading.
At the suggestion of a peer reviewer, we conducted two additional subgroup analyses. In Analysis 1.3, we categorised by the level of control group contact to investigate whether there might be a difference between trials where the control could be categorised as a brief intervention (up to 30 minutes) and trials which might be characterised as testing a dose‐response for behavioural support, which we defined as being where the controls received more than 30 minutes of behavioural support. The eight trials where controls had no advice or contact formed a third subgroup. Twenty‐two trials and just over half the participants were in the 'brief intervention' subgroup, and 32 trials and a third of participants were in the 'dose‐response' category. Again, there was no significant difference between the subgroups (P = 0.41, I² = 0%).
1.3. Analysis.
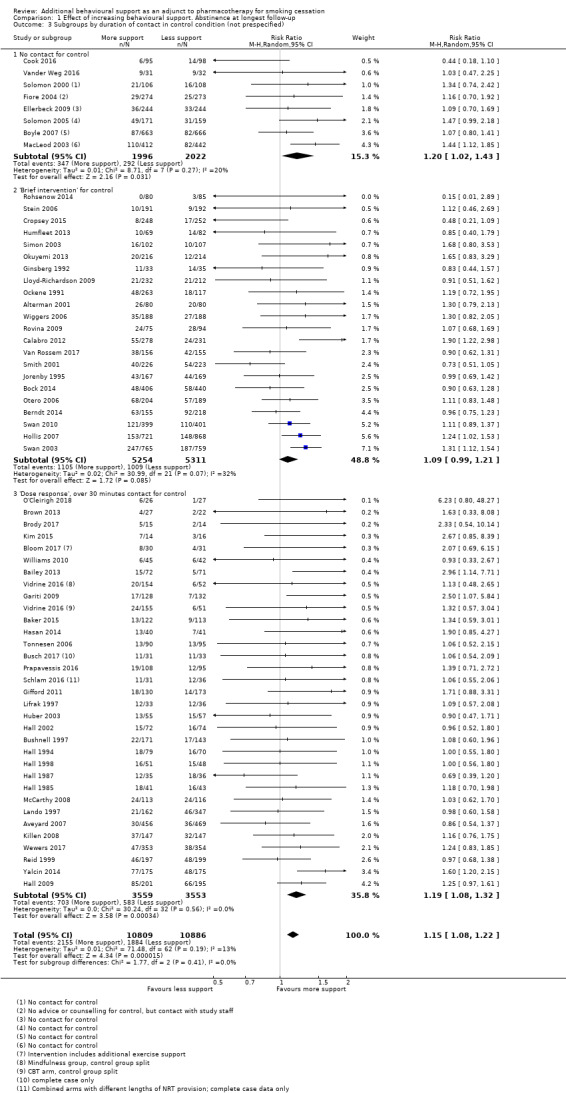
Comparison 1 Effect of increasing behavioural support. Abstinence at longest follow‐up, Outcome 3 Subgroups by duration of contact in control condition (not prespecified).
In this version of the review, we also conducted an exploratory meta‐regression to explore associations between effect sizes and number and duration of contacts. A comparison of the intervention effect (log risk ratio) by the difference between the treatment groups in the duration and number of contacts is shown in Figure 4. There was no clear effect of either increasing duration of contact (RR 1.00 per 100 minutes additional contact time, 95% CI 0.99 to 1.01) or increasing number of contacts (RR 1.00 per additional contact, 95% CI 0.99 to 1.02).
4.
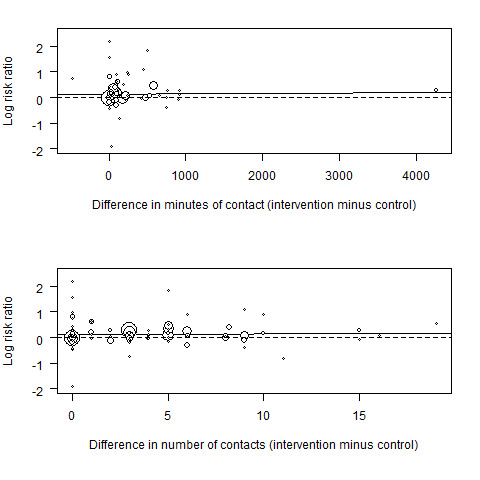
Meta‐regression results (the fitted meta‐regression trend is shown as the solid line)
Differences in modality of intervention contact
In the second non‐prespecified analysis, we categorised studies according to whether there was some face‐to‐face contact as part of the intervention, or whether all support was given by telephone (Analysis 1.4). Here, the test for subgroup differences was significant (P = 0.03, I² = 78%), with telephone counselling showing greater relative benefit than face‐to‐face support. In the subgroup of eight studies using telephone counselling (which had some overlap with studies where there was no personal contact for the control), the point estimate was 1.25 (95% CI 1.15 to 1.37, I² = 0%, 6670 participants) in favour of additional behavioural support. In the remaining 57 studies where all intervention and most control conditions had face‐to‐face support, there was also evidence of benefit of additional behavioural support in this update, although the estimate was slightly smaller (RR 1.11, 95% CI 1.03 to 1.19, I² = 9%; 16,661 participants).
1.4. Analysis.
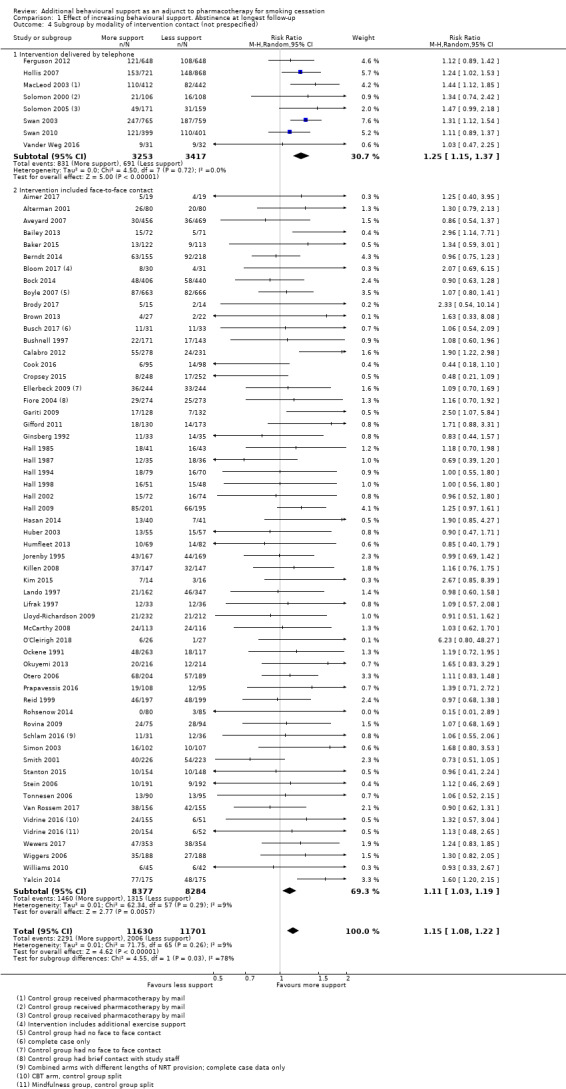
Comparison 1 Effect of increasing behavioural support. Abstinence at longest follow‐up, Outcome 4 Subgroup by modality of intervention contact (not prespecified).
Inclusion of medium‐intensity intervention from studies with multiple intervention conditions
Eight studies (Alterman 2001; Ellerbeck 2009; Fiore 2004; Hollis 2007; Humfleet 2013; Jorenby 1995; Prapavessis 2016; Smith 2001; Swan 2010) included an intervention condition intermediate in intensity between the highest intensity and the control. We have not included these arms in the primary analysis in case they reduced the contrast between intervention and control. In a sensitivity analysis, we added in these arms. This had almost no impact on the estimated effect (RR 1.13, 95% CI 1.07 to 1.20, I² = 8%; 65 studies, n = 27,425; Analysis 2.1), tending to support the finding that there was not a clear dose‐response relationship with the amount of support.
2.1. Analysis.
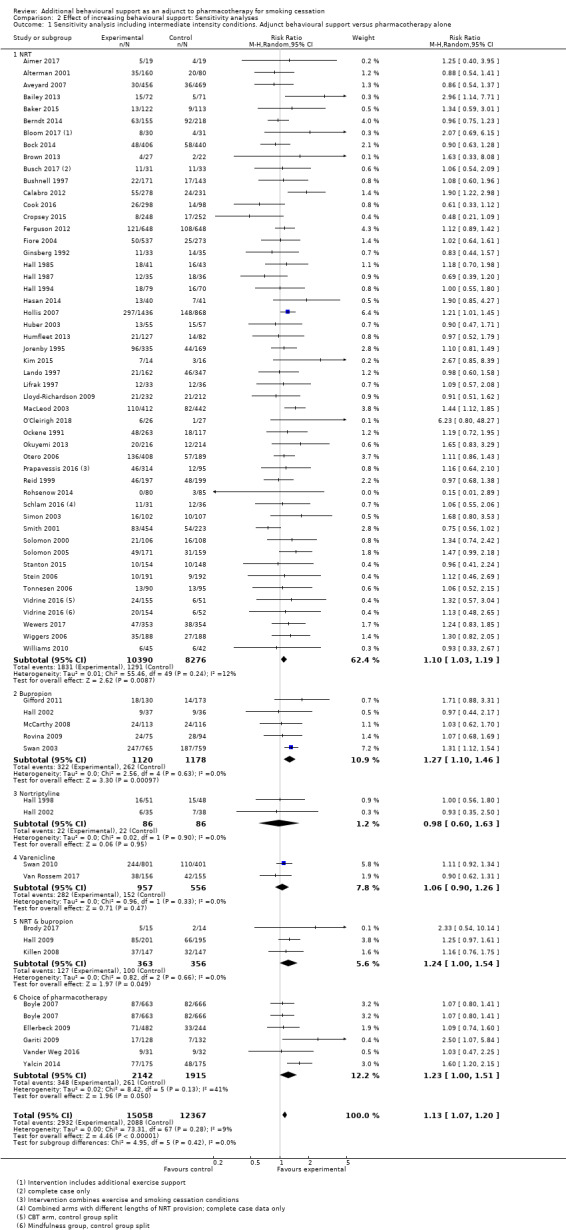
Comparison 2 Effect of increasing behavioural support: Sensitivity analyses, Outcome 1 Sensitivity analysis including intermediate intensity conditions. Adjunct behavioural support versus pharmacotherapy alone.
Definition of abstinence
We considered whether the way in which abstinence was defined was related to the effect size, and also to absolute quit rates. Here again, there were no significant subgroup differences (P = 0.22, I² = 30%, Analysis 2.2). Some studies that reported sustained outcomes also reported point prevalence rates, but substituting the less stringent definition did not change the overall findings. However, studies with point prevalence outcomes had, on average, higher quit rates in both intervention and control arms. A study comparing outcomes based on different abstinence definitions reported within studies found that, for pharmacotherapy studies, point prevalence and sustained abstinence outcomes were strongly related, with sustained abstinence averaging around 74% of point prevalence rates (Hughes 2010).
2.2. Analysis.
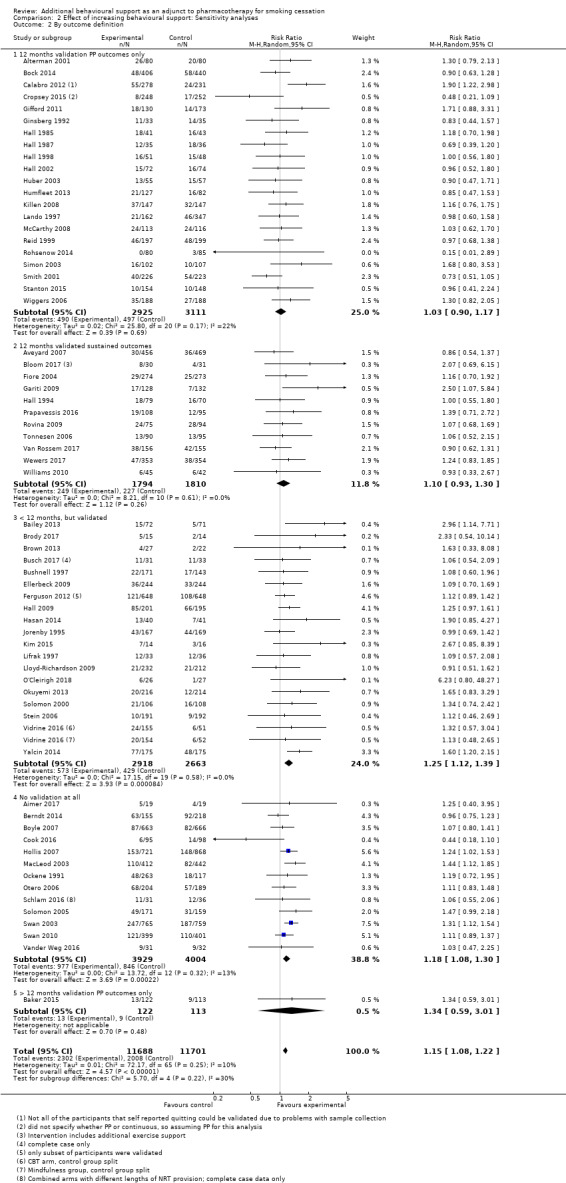
Comparison 2 Effect of increasing behavioural support: Sensitivity analyses, Outcome 2 By outcome definition.
Unit of analysis issues
Two included studies were cluster‐randomised trials (Berndt 2014; Lando 1997). One of these (Berndt 2014) performed an analysis adjusting for clustering effects and found them to be not significantly different from zero, and so we used the original data values. The other (Lando 1997) also allowed for clustering but did not report adjusted results, and so the magnitude of clustering effects was unknown. As the number of included studies in the review was large, this was not likely to have any noticeable effect on our overall conclusions.
Risk of bias
In a sensitivity analysis, removing studies judged to be at high risk of bias in at least one domain, the effect observed was consistent with that of the main analysis (RR 1.09, 95% CI 1.01 to 1.17, I² = 0%; 47 studies, n = 13355).
Studies not included in meta‐analysis
Two studies comparing more versus less intensive support were not included in the meta‐analysis due to a lack of usable data. NCT00879177 is a completed study that was not yet published at the time of searching, and while numerical data were not available, the author indicated that results were broadly comparable between groups. Wagner 2016 compared individual counselling with group counselling, and although follow‐up was conducted at later time points, the only data available at time of searching was for 12‐week quit rates, where there was no evidence of difference in quit rates (RR 0.96, 95% CI 0.51 to 1.81; n = 400).
Studies matched for contact time
Seventeen studies compared interventions matched for contact time. Fifteen of these provided usable data, which is available in Analysis 3.1. Of the 12 comparisons, all had small numbers of participants and events. Only one, comparing motivational interviewing to health education (which the authors described as standard counselling containing information and advice), detected a statistically significant effect, in this case in favour of health education (RR 0.56, 95% CI 0.33 to 0.94, n = 378). Only one comparison included more than one study; this group of studies compared culturally‐tailored support with non‐tailored support. Four studies (n = 929) contributed to this comparison (RR 1.14, 95% CI 0.68 to 1.92). Statistical heterogeneity was substantial (I² = 78%) and was driven by one small study (Wu 2009; n = 139) in Chinese smokers which found a significant benefit in favour of the culturally‐tailored intervention (RR 2.26, 95% CI 1.47 to 3.49). For comparisons in which only one study contributed, see Analysis 3.1 for data and effect estimates.
3.1. Analysis.
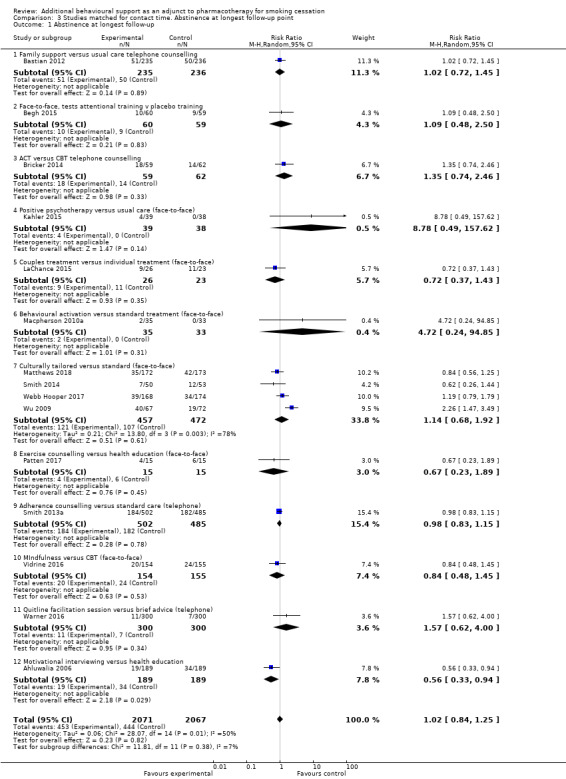
Comparison 3 Studies matched for contact time. Abstinence at longest follow‐up point, Outcome 1 Abstinence at longest follow‐up.
A further two studies compared interventions matched for contact time but had insufficient data to be recorded in Analysis 3.1:
Schmitz 2007a compared cognitive behavioural therapy to standard therapy but quit rates in the control group could not be accessed.
Strong 2009 also compared cognitive behavioural therapy (CBT) to standard therapy (ST) but we could not access quit rates beyond 12 weeks. At 12 weeks, there was "no significant difference in the risk of lapse or relapse across CBT and ST psychosocial treatments" (abstinence data not reported).
Discussion
Summary of main results
A meta‐analysis pooling 65 studies with a total of over 23,000 participants found high‐certainty evidence that providing more intensive behavioural support for people making a cessation attempt with the aid of pharmacotherapy will typically increase the success rates by about 10% to 20% (Table 1). This held true when comparing more versus less support and when comparing behavioural support to no behavioural support. This effect estimate has remained stable over time: with the addition of nine trials in 2015, the number of participants increased by 20% and yet the risk ratio remained almost the same, changing from 1.16 to 1.17; and with the addition of a further 18 trials in 2019, the number of participants increased by a further 25% and the risk ratio was 1.15. This increases confidence that there is a benefit. There continues to be little evidence of statistical heterogeneity overall, despite the variability in the amount and nature of the behavioural support tested. Direct comparisons indicate a benefit of providing more support regardless of the baseline level of support provided. Sensitivity analyses suggest that this estimate is quite robust. Although the relative effect is generally smaller than when testing behavioural support in the absence of pharmacotherapy, it is important to put the effect in the context of control conditions that were offering effective pharmacotherapy and, typically, some behavioural support, i.e. a level of support consistent with guideline best practice. Quit rates in the control groups reflected this, with a median quit rate across trials of around 17%, meaning the estimated relative increase translates into an absolute increase of around two to three percentage points. Given the importance of smoking cessation for future health outcomes, this is a clinically relevant difference (West 2007).
Overall completeness and applicability of evidence
The studies identified for this review have largely been conducted in the USA or Europe. It is possible that we have failed to find relevant studies conducted in other places. Participants were typically moderate to heavy smokers and were interested in quitting. Most studies recruited participants who had already tried to quit a number of times. Most of the evidence came from studies testing additional face‐to‐face support. The eight trials which tested the addition of telephone counselling found a stronger effect in favour of additional contact, but we are unable to determine if this was based on true differences in effects or other differences between the studies.
A potential limitation of the review is that the between‐trial analysis focussed on the amount of behavioural support rather than the specific components, or the quality of delivery. However, in this update, we included studies directly comparing interventions matched for contact time (e.g. testing different behavioural approaches or types of support). Only one of the 15 comparisons detected a significant effect, but most comparisons only included one study, and all comparisons had small numbers of participants. The question of specific components of behavioural support and associations with effectiveness is being investigated further in a separate Cochrane review (Hartmann‐Boyce 2018a).
Certainty of the evidence
We judged the evidence regarding additional behavioural support to be of high certainty, meaning further research is judged very unlikely to change our confidence in the effect. This judgement is supported by the consistency of the effect estimate over time, and this is likely to be the last update of this review. However, despite high certainty in results, some areas relating to the five GRADE considerations (risk of bias, imprecision, indirectness, inconsistency, and publication bias) warrant discussion, namely risk of bias, inconsistency, and publication bias.
Risk of bias
While we judged most of the trials to be at low or unclear risk of bias, we rated 21 studies as having high risk of bias. Reassuringly, sensitivity analysis excluding studies at high risk of bias did not change the overall effect. The quality of the trials was typical of smoking cessation research in general. We did not formally evaluate whether there was a risk of performance bias due to a lack of blinding of providers or participants. Blinding of providers would not have been possible, and it was difficult to determine whether participants knew how their treatment compared to the other options offered. All participants were getting an active pharmacotherapy and would have been aware of this (apart from a small proportion in placebo‐controlled factorial studies). Expectancy effects for the behavioural components would probably have been small, and we do not think the small effect of the interventions could be attributed entirely to higher expectancies in intervention conditions.
Inconsistency
There were potentially important differences between trials in the relative difference in the support given to the intervention and control groups. Despite the lack of statistical heterogeneity, we undertook a number of subgroup analyses, including some that were not prespecified. In response to a concern that we were combining tests of behavioural support versus no support with tests of a dose‐response to intensity of support, we divided trials into those where the control did not involve personal contact; where the control group provided a brief intervention, operationalised as under 30 minutes contact; and those where the control condition was more intensive (Analysis 1.3). There was no evidence of a difference in the relative effect between these three subgroups. In this update, we also conducted an exploratory meta‐regression, in which results continue to suggest that the dose‐response curve is shallow for behavioural support. We drew similar conclusions in a companion review to this, which compared combined pharmacotherapy and behavioural support to minimal support; indirect comparisons between trials using more and less intensive behavioural interventions also failed to detect large differences (Stead 2016). The present review also detected a clearer benefit of more support in studies where all contact was delivered by telephone, but this too was not prespecified and may reflect the larger size of trials done in quitline settings, or possibly that most of these studies did not use biochemical validation of abstinence.
Publication bias
A funnel plot was inconclusive, suggesting there may have been slightly more small studies with large effect sizes than with small effect sizes (Figure 5). However, asymmetry was not clear and when we investigated further by conducting sensitivity analyses excluding outliers this did not substantially alter the effect. Given the large number of included studies and the degree of homogeneity between them, it is unlikely that smaller unpublished studies showing no effect, if they existed, would significantly alter our results.
5.
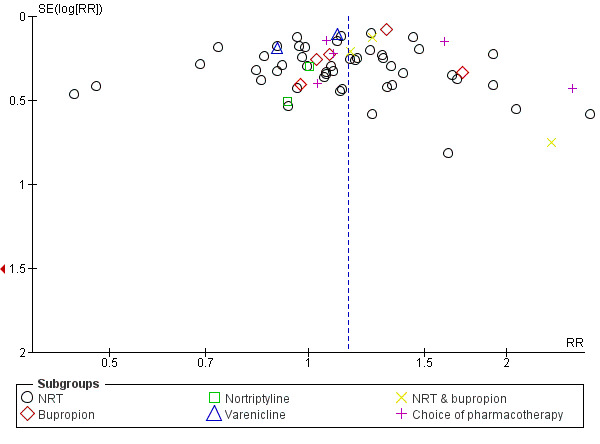
Funnel plot of comparison: 1 Effect of increasing behavioural support. Abstinence at longest follow‐up, outcome: 1.1 Subgroups by type of pharmacotherapy.
Potential biases in the review process
We used the Cochrane Tobacco Addiction Group's Specialised Register and searched trial registries to identify studies. The Register includes reports of trials identified from the major bibliographic databases. There is no straightforward term for the type of intervention we were interested in but we screened any trial report that mentioned a pharmacotherapy. It is possible that the Register does not include all relevant trial reports or that we failed to identify some. Our methods for data extraction and analysis are those used for other Cochrane reviews. The practice of imputing missing data as smoking has been traditionally used for primary and secondary research in smoking cessation and has the advantage that absolute cessation rates are not inflated by ignoring loss to follow‐up. Bias in the relative effect will only be introduced if misclassification differs for people who are lost from the intervention condition compared to the control. If proportionately more of those who are lost in the control group are assumed to be smokers but have in fact quit, then the treatment effect would be overestimated.
Agreements and disagreements with other studies or reviews
The major source of systematic data about the dose‐response to behavioural support is the US Public Heath Service Clinical Practice Guideline, last updated in 2008 (Fiore 2008). This includes meta‐analyses (last updated in 2000) for different levels of support and contact time. The analyses included trials of different levels of support versus control. These showed trends towards increasing effects in trials that had more sessions and more contact time, compared to minimal conditions. For example, estimated effects compared to minimal contact differed between trials with four to 30 minutes of contact time (OR 1.9, 95% CI 1.5 to 2.3) and trials with 91 to 300 minutes (OR 3.2, 95% CI 2.3 to 4.6) (Fiore 2008 Table 6.9) and between two to three treatment sessions (OR 1.4, 95% CI 1.1 to 1.7) and over eight sessions (OR 2.3, 95% CI 2.1 to 3.0) compared to 0 to 1 sessions (Fiore 2008 Table 6.10). These analyses were not limited to direct (within trial) comparisons of treatment intensity. They also did not distinguish between studies with and without pharmacotherapy, and the majority of studies in our analysis were published after 2000 so would not have been included. Our review is likely to give a more precise estimate of the effect of additional support alongside pharmacotherapy, based on the analysis of trials directly comparing different levels of support.
There is observational evidence that access to more behavioural support is associated with greater success in quitting. For example, a study of English Stop Smoking Services, in which there was a high use of pharmacotherapy, found a positive association between the number of scheduled sessions and short‐term quit rates (West 2010). A study of NRT users calling the California quitline found that people who received multiple sessions of counselling had higher quit rates after one year (Zhu 2000).
Increasingly, studies which test the effects of behavioural support provide pharmacotherapy to both arms. That means that many of the studies included here are covered (as subsets only) in other reviews of behavioural interventions. These include telephone counselling and face‐to‐face counselling, both in person and in groups (Lancaster 2017; Matkin 2019; Stead 2017). Our results from the subgroup of trials in which additional support was delivered via telephone are remarkably consistent with those from the Cochrane review of telephone counselling (Matkin 2019). Matkin 2019 also included studies without pharmacotherapy and thus had substantially more studies than our eight, but the point estimate was the same as ours in studies that recruited smokers who did not call a helpline (RR 1.25, 95% CI 1.15 to 1.35; 65 trials; 41,233 participants, I² = 52%). In the Cochrane review of individual behavioural counselling (Lancaster 2017), effects were again consistent with our findings: there was moderate‐quality evidence (downgraded due to imprecision) of a modest benefit of counselling when all participants received pharmacotherapy (RR 1.24, 95% CI 1.01 to 1.51; 6 studies, 2662 participants; I2 = 0%). The effect was stronger in studies in which participants did not receive pharmacotherapy. Similarly, in the Cochrane review of group behaviour therapy programmes (Stead 2017), the effect was stronger in studies in which participants did not receive pharmacotherapy; only five trials included pharmacotherapy, with a point estimate indicating a modest benefit but with wide confidence intervals incorporating no effect (RR 1.11, 95% CI 0.93 to 1.33, I2 = 0%; n = 1523).
Finally, one explanation for the relatively small impact of providing more behavioural support is that it is not provided at the time when it could be most effective. Relapse after initial success is the norm for quit attempts, and by the time people are getting additional calls they may already have relapsed. Various study authors commented on this (e.g. Reid 1999; Smith 2001). Although these studies are not typically characterised as being about 'relapse prevention', there is a small overlap between this review and the Cochrane review of relapse prevention interventions (Livingstone‐Banks 2019a), which concluded that there was no evidence of a benefit of additional behavioural support to prevent relapse. On the other hand, in some cases, an initial benefit of the intervention disappeared once treatment ended, and authors suggested that further extended support might have made a difference (e.g. Killen 2008; Solomon 2000), although replication of one of these studies with more extended support (Solomon 2005) still showed the same pattern of late relapse. Another possible explanation is that uptake of extended treatment may be poor, so the actual number of contacts received may not vary substantially by group. Few studies reported uptake measures.
Authors' conclusions
Implications for practice.
Providing behavioural support for smokers using established medication in an attempt to stop smoking will increase the proportion of successful attempts. This is true when comparing more versus less support and when comparing behavioural support to no behavioural support.
Implications for research.
Identifying the optimal amount of behavioural support to use alongside pharmacotherapy remains a challenge. Studies need to be appropriately powered for small treatment effects, and test interventions that are acceptable and accessible to smokers, and affordable to deliver. More studies are needed outside of the USA and Europe. Further research is needed to test associations between effectiveness and different behavioural components of interventions (which will be covered by a separate review moving forward).
What's new
| Date | Event | Description |
|---|---|---|
| 13 March 2019 | New search has been performed | Updated with 36 new included studies. Searches run June 2018. |
| 13 March 2019 | New citation required but conclusions have not changed | New studies and analyses added; now includes contact‐matched studies and meta‐regression. Conclusions not changed. |
History
Protocol first published: Issue 2, 2012 Review first published: Issue 12, 2012
| Date | Event | Description |
|---|---|---|
| 10 August 2015 | New citation required but conclusions have not changed | New author PK added for update |
| 10 August 2015 | New search has been performed | Searches updated, 9 new included studies |
| 21 February 2013 | Amended | Correction to 2 forest plot labels |
Acknowledgements
Thanks to Clare Miles for her assistance with data extraction. Thanks to A. Eden Evins for providing additional information on an excluded study for the previous version of this review. Thanks to Dr Karen Cropsey, Dr Stephen Smith, Dr Jessica Cook, Dr Erika Bloom, Dr Arthur Brody, Professor Harry Prapavessis, and Professor William White for providing clarifications or further information on their papers for this review update.
Lindsay Stead and Tim Lancaster conceived of and were authors of the first and second versions of this review. Pria Koilpillai was an author of the second version. Their input is greatly appreciated.
This project was supported by the National Institute for Health Research (NIHR), via Cochrane Infrastructure and Cochrane Programme Grant funding to the Cochrane Tobacco Addiction Group. The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the Systematic Reviews Programme, NIHR, NHS or the Department of Health and Social Care. JHB is also part‐funded by the NIHR Oxford Biomedical Research Centre (BRC).
Appendices
Appendix 1. Register Search
Search used in the Cochrane Register of Studies.
NRT:TI,AB,KW
(nicotine NEAR (replacement OR patch* OR transdermal OR gum OR lozenge* OR sublingual OR inhaler* OR inhalator* OR oral OR nasal OR spray)):TI,AB,KW
(bupropion OR zyban OR wellbutrin):TI,AB,KW,MH,EMT
(varenicline OR champix OR chantix):TI,AB,KW,MH,EMT
combined modality therapy:MH,KW
((behavio?r therapy) AND (drug therapy)):KW,MH,EMT,TI,AB
((counsel*) AND (*drug therapy)):KW,MH,EMT,TI,AB
#1 OR #2 OR #3 OR #4 OR #5
#6 OR #7 OR #8
#9 AND INREGISTER
Data and analyses
Comparison 1. Effect of increasing behavioural support. Abstinence at longest follow‐up.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Subgroups by type of pharmacotherapy | 65 | 23331 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [1.08, 1.22] |
| 1.1 NRT | 49 | 16541 | Risk Ratio (M‐H, Random, 95% CI) | 1.12 [1.04, 1.21] |
| 1.2 Bupropion | 5 | 2298 | Risk Ratio (M‐H, Random, 95% CI) | 1.27 [1.10, 1.46] |
| 1.3 Nortriptyline | 2 | 172 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.60, 1.63] |
| 1.4 Varenicline | 2 | 1111 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.87, 1.27] |
| 1.5 NRT & bupropion | 3 | 719 | Risk Ratio (M‐H, Random, 95% CI) | 1.24 [1.00, 1.54] |
| 1.6 Choice of pharmacotherapy | 5 | 2490 | Risk Ratio (M‐H, Random, 95% CI) | 1.30 [1.00, 1.68] |
| 2 Subgroups by contrast in number of contacts between intervention & control | 63 | 21997 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [1.08, 1.22] |
| 2.1 4 to 8 or > 8 contacts versus no contact | 8 | 4018 | Risk Ratio (M‐H, Random, 95% CI) | 1.20 [1.02, 1.43] |
| 2.2 More than 8 contacts versus 1 to 3 contacts | 4 | 1063 | Risk Ratio (M‐H, Random, 95% CI) | 1.05 [0.70, 1.57] |
| 2.3 4 to 8 contacts versus 1 to 3 contacts | 18 | 9579 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [1.01, 1.19] |
| 2.4 More than 8 contacts versus 4 to 8 contacts | 12 | 1737 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [0.98, 1.33] |
| 2.5 Intervention & control in same contact category | 21 | 5600 | Risk Ratio (M‐H, Random, 95% CI) | 1.32 [1.16, 1.50] |
| 3 Subgroups by duration of contact in control condition (not prespecified) | 62 | 21695 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [1.08, 1.22] |
| 3.1 No contact for control | 8 | 4018 | Risk Ratio (M‐H, Random, 95% CI) | 1.20 [1.02, 1.43] |
| 3.2 'Brief intervention' for control | 22 | 10565 | Risk Ratio (M‐H, Random, 95% CI) | 1.09 [0.99, 1.21] |
| 3.3 'Dose response', over 30 minutes contact for control | 32 | 7112 | Risk Ratio (M‐H, Random, 95% CI) | 1.19 [1.08, 1.32] |
| 4 Subgroup by modality of intervention contact (not prespecified) | 65 | 23331 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [1.08, 1.22] |
| 4.1 Intervention delivered by telephone | 8 | 6670 | Risk Ratio (M‐H, Random, 95% CI) | 1.25 [1.15, 1.37] |
| 4.2 Intervention included face‐to‐face contact | 57 | 16661 | Risk Ratio (M‐H, Random, 95% CI) | 1.11 [1.03, 1.19] |
Comparison 2. Effect of increasing behavioural support: Sensitivity analyses.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Sensitivity analysis including intermediate intensity conditions. Adjunct behavioural support versus pharmacotherapy alone | 65 | 27425 | Risk Ratio (M‐H, Random, 95% CI) | 1.13 [1.07, 1.20] |
| 1.1 NRT | 49 | 18666 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [1.03, 1.19] |
| 1.2 Bupropion | 5 | 2298 | Risk Ratio (M‐H, Random, 95% CI) | 1.27 [1.10, 1.46] |
| 1.3 Nortriptyline | 2 | 172 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.60, 1.63] |
| 1.4 Varenicline | 2 | 1513 | Risk Ratio (M‐H, Random, 95% CI) | 1.06 [0.90, 1.26] |
| 1.5 NRT & bupropion | 3 | 719 | Risk Ratio (M‐H, Random, 95% CI) | 1.24 [1.00, 1.54] |
| 1.6 Choice of pharmacotherapy | 5 | 4057 | Risk Ratio (M‐H, Random, 95% CI) | 1.23 [1.00, 1.51] |
| 2 By outcome definition | 65 | 23389 | Risk Ratio (M‐H, Random, 95% CI) | 1.15 [1.08, 1.22] |
| 2.1 12 months validation PP outcomes only | 21 | 6036 | Risk Ratio (M‐H, Random, 95% CI) | 1.03 [0.90, 1.17] |
| 2.2 12 months validated sustained outcomes | 11 | 3604 | Risk Ratio (M‐H, Random, 95% CI) | 1.10 [0.93, 1.30] |
| 2.3 < 12 months, but validated | 19 | 5581 | Risk Ratio (M‐H, Random, 95% CI) | 1.25 [1.12, 1.39] |
| 2.4 No validation at all | 13 | 7933 | Risk Ratio (M‐H, Random, 95% CI) | 1.18 [1.08, 1.30] |
| 2.5 > 12 months validation PP outcomes only | 1 | 235 | Risk Ratio (M‐H, Random, 95% CI) | 1.34 [0.59, 3.01] |
Comparison 3. Studies matched for contact time. Abstinence at longest follow‐up point.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Abstinence at longest follow‐up | 15 | 4138 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.84, 1.25] |
| 1.1 Family support versus usual care telephone counselling | 1 | 471 | Risk Ratio (M‐H, Random, 95% CI) | 1.02 [0.72, 1.45] |
| 1.2 Face‐to‐face, tests attentional training v placebo training | 1 | 119 | Risk Ratio (M‐H, Random, 95% CI) | 1.09 [0.48, 2.50] |
| 1.3 ACT versus CBT telephone counselling | 1 | 121 | Risk Ratio (M‐H, Random, 95% CI) | 1.35 [0.74, 2.46] |
| 1.4 Positive psychotherapy versus usual care (face‐to‐face) | 1 | 77 | Risk Ratio (M‐H, Random, 95% CI) | 8.78 [0.49, 157.62] |
| 1.5 Couples treatment versus individual treatment (face‐to‐face) | 1 | 49 | Risk Ratio (M‐H, Random, 95% CI) | 0.72 [0.37, 1.43] |
| 1.6 Behavioural activation versus standard treatment (face‐to‐face) | 1 | 68 | Risk Ratio (M‐H, Random, 95% CI) | 4.72 [0.24, 94.85] |
| 1.7 Culturally tailored versus standard (face‐to‐face) | 4 | 929 | Risk Ratio (M‐H, Random, 95% CI) | 1.14 [0.68, 1.92] |
| 1.8 Exercise counselling versus health education (face‐to‐face) | 1 | 30 | Risk Ratio (M‐H, Random, 95% CI) | 0.67 [0.23, 1.89] |
| 1.9 Adherence counselling versus standard care (telephone) | 1 | 987 | Risk Ratio (M‐H, Random, 95% CI) | 0.98 [0.83, 1.15] |
| 1.10 MIndfulness versus CBT (face‐to‐face) | 1 | 309 | Risk Ratio (M‐H, Random, 95% CI) | 0.84 [0.48, 1.45] |
| 1.11 Quitline facilitation session versus brief advice (telephone) | 1 | 600 | Risk Ratio (M‐H, Random, 95% CI) | 1.57 [0.62, 4.00] |
| 1.12 Motivational interviewing versus health education | 1 | 378 | Risk Ratio (M‐H, Random, 95% CI) | 0.56 [0.33, 0.94] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Ahluwalia 2006.
| Methods | Setting: community health centre, USA Recruitment: African‐American light smokers recruited from the clinic and using various routes of advertisement |
|
| Participants | 755 smokers of ≤ 10 cigarettes per day; the characteristics of 378 participants in the relevant arm were as follows: 66.1% to 68.3% female; average age 43.5 to 45.2; average cigarettes per day 7.5 to 7.8 Therapists: trained counsellors who followed semi‐structured scripts |
|
| Interventions | Pharmacotherapy: NRT; 2 mg nicotine gum for 8 weeks including weaning period. Dose depended on the number of cigarettes smoked per day 1. Motivational interviewing: 3 sessions in person and 3 sessions by telephone, each lasting 20 minutes 2. Health education: 3 sessions in person and 3 sessions by telephone, each lasting 20 minutes |
|
| Outcomes | 7‐day point prevalence abstinence at weeks 1, 3, 6, 8, 16 and 6 months Validation: cotinine‐verification (≤ 20 ng/mL), expired carbone monoxide ≤ 10 ppm |
|
| Source of Funding/CoI | National Cancer Institute at the National Institutes of Health (R01CA091912) Glaxo‐SmithKline provided study medication. No declarations of interest | |
| Notes | New for 2019 update. Previously excluded. Reason: Conselling conditions had same number of contacts and duration. Compared Motivational Interviewing and Health Education (HE) in a factorial trial with nicotine gum or placebo (results favoured HE (control) condition). Included in Lindson‐Hawley 2015 Cochrane review of motivational interviewing |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details given |
| Allocation concealment (selection bias) | Low risk | Sealed envelope with pre‐assigned randomisation numbers |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 11.1% to 16.9% lost to follow‐up at 6 months |
Aimer 2017.
| Methods | Setting: rheumatology clinic (single centre), Christchurch, New Zealand Recruitment: smokers with rheumatoid arthritis. No mention of intended selection for motivation but the authors mentioned that the study population was likely to have been highly motivated |
|
| Participants | 39 smokers; 55% female; average age 56.5; average cigarettes per day 16.5 Therapists: community‐based arthritis educators trained in smoking cessation |
|
| Interventions | Pharmacotherapy: NRT for 8 weeks 1. usual care (brief advice and subsidised NRT) for 3 months 2. usual care + rheumatoid arthritis‐specific programme for 3 months via face‐to‐face, telephone and email; 4 sessions at week 0, 1, 4, 8 |
|
| Outcomes | Continuous abstinence at 3 and 6 months Validation: none |
|
| Source of Funding/CoI | New Zealand Health Research Council, Arthritis New Zealand and University of Otago Research Fund. Authors declared receipt of consultant fees, speaking fees, and/or honoraria from AbbVie and Janssen (less than $10,000 each). | |
| Notes | New for 2019 update One participant was excluded from analysis after intervention and follow‐up when found not to have rheumatoid arthritis. Did not contribute to analysis 1.2 or analysis 1.3 as duration of control group contact not specified |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random sequence generated by a biostatistician using an Excel spreadsheet in 6 blocks x 8 allocations |
| Allocation concealment (selection bias) | Unclear risk | Insufficient details given |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 0‐15.8% lost to follow‐up at 6 months |
Alterman 2001.
| Methods | Setting: cessation clinic, USA Recruitment: community volunteers | |
| Participants | 240 smokers of > 1 pack/day; 45% to 54% female, average age 40, average cpd 27 Therapists: Nurse practitioners (NP) and trained counsellors | |
| Interventions | Pharmacotherapy: NRT; 21 mg patch for 8 weeks (including weaning period) 1. Low intensity. Single 30‐minute session with nurse practitioners 2. Moderate intensity. as 1 plus additional 3 x 15 to 20‐minute sessions at weeks 3, 6, 9 with nurse practitioners 3. High intensity. As 2 plus 12 45 to 50‐minute sessions cognitive behavioural therapy with trained therapist within 15 weeks | |
| Outcomes | Abstinence at 1 year Validation: urine cotinine < 50 ng/mL, CO ≤ 9 ppm | |
| Source of Funding/CoI | National Institute on Drug Abuse. No declarations of interest | |
| Notes | 3 versus 1 in main analysis. Quit rates significantly lower in 2 than 1 or 3. 35/160 quit when 2 & 3 combined | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Urn technique" |
| Allocation concealment (selection bias) | Unclear risk | No details given. Allocation took place after baseline session common to all conditions |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Small and similar rate lost to follow‐up in each group (approx 7%). "Intent to treat" analyses reported in the paper excluded 2 deaths and 2 who did not provide cotinine samples |
Aveyard 2007.
| Methods | Setting: 26 general practices (primary care clinics), UK Recruitment: 92% volunteers in response to mailings | |
| Participants | 925 smokers; 51% F, av. age 43, 50% smoked 11 to 20 cpd Therapists: practice nurses trained to provide cessation support & manage NRT | |
| Interventions | Pharmacotherapy: NRT; 16 mg patch for 8 weeks 1. Basic support; 1 visit (20 to 40 mins) before quit attempt, phone call on TQD, visits/phone calls at 7 to 14 days & at 21 to 28 days (10 to 20 mins); 4 contacts, ˜80 mins 2. Weekly support; as 1. plus additional call at 10 days & visits at 14 & 21 days; 7 contacts, ˜140 mins | |
| Outcomes | Abstinence at 12 months (sustained at 1, 4, 12, 26 weeks) Validation: CO < 10 ppm at treatment visits, saliva cotinine < 15 ng/mL at follow‐up | |
| Source of Funding/CoI | Cancer Research UK. Authors declared interests. | |
| Notes | Therapists were not full‐time specialist counsellors. Difference between support conditions relatively small | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number generator |
| Allocation concealment (selection bias) | Low risk | Numbered sealed envelopes |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Over 30% lost to follow‐up but similar percentage followed up in both groups (69% intervention vs 68% control, no evidence of differential attrition) |
Bailey 2013.
| Methods | Setting: high schools in San Francisco, USA Recruitment: adolescent smokers were recruited over a period of 3 years on a non‐rolling basis, with a new cohort participating each academic school year. Selected for motivation to quit |
|
| Participants | 143 smokers; 37.6% female; average age 16.9; average cigarettes smoked per week 97.1 Therapists: research intervention staff with Bachelor's degree or higher. Supervised by the project director (clinical psychologist) |
|
| Interventions | Pharmacotherapy: NRT (nicotine patch); 9 weeks (dosage and titration schedule determined by number of cigarettes smoked per day) 1. Group based cognitive behavioural therapy and skills training (10 weeks) 2. Group based cognitive behavioural therapy and skills training (10 weeks) + extended face‐to‐face group sessions (9 sessions over 14 weeks) |
|
| Outcomes | 7‐day point prevalence abstinence at 6 months Validation: expired carbon monoxide using Bedfont Smokerlyzers |
|
| Source of Funding/CoI | National Cancer Institute at the National Institutes of Health (R01 CA 118035 to JDK). No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | Insufficient details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Lost to follow‐up rate: extended group 16.7%; other 16.9% |
Baker 2015.
| Methods | Setting: Centre for Brain and Mental health Research, University of Newcastle, New South Wales; School of Public Health, University of New South Wales, Sydney; Monash Alfred Psychiatry Research Centre, Monash University and the Alfred, Melbourne, Australia Recruitment: smokers recruited from three sites in Newcastle, Sydney and Melbourne, Australia. Referral sources included health services, media advertisement and other research programmes or registers. |
|
| Participants | 235 smokers; 41.3% female; average age 41.6; average cigarettes smoked per day 28.6 Therapists: psychologists guided by intervention manuals |
|
| Interventions | Pharmacotherapy: NRT; 24 weeks’ supply of NRT delivered at weeks 1, 4 and 8 and thereafter by arrangement. Participants smoking ≥ 30 cigarettes per day were eligible to receive double patching in addition to up to 12 x 2 mg lozenges per day, with NRT tapering occurring in the last month of delivery. 1. Predominantly telephone‐based (17 sessions; 290 minutes in total) 2. Face‐to‐face healthy lifestyle therapy (17 sessions; 1050 minutes in total) |
|
| Outcomes | 7‐day point prevalence abstinence at week 15 and months 12, 18, 24, 30, 36 Validation; carbon monoxide ≤ 10 ppm |
|
| Source of Funding/CoI | Australian National Health and Medical Research Council and the Commonwealth Department of Health and Aging. NRT was provided free of charge by GlaxoSmithKline. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Permuted block randomisation approach mentioned but no further detail |
| Allocation concealment (selection bias) | Low risk | Sealed randomisation envelope by an independent person displaying a participant identification code. Participants opened the envelope at the end of the initial intervention session. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 39.8 to 45.9% lost to follow‐up at 3 years |
Bastian 2012.
| Methods | Setting: USA Recruitment: participants identified from electronic medical records. Eligibility assessment in person and selected for motivation to quit |
|
| Participants | 471 smoker; 8.5% female, average age 59; heaviness of smoking index mean 2.8 Therapists: masters‐level counsellors with training |
|
| Interventions | Pharmacotherapy: NRT; inhaler, patch, spray and/or bupropion (regimen and dosage dependent on the number of cigarettes smoked per day and tobacco cessation anxiety) 1. Usual care: 5 telephone sessions every 3‐4 weeks; each session lasting 20 minutes 2. Family‐supported 5 telephone sessions every 3‐4 weeks; each session lasting 20 minutes |
|
| Outcomes | 7‐day point prevalence abstinence at 5 and 12 months Validation: attempted verification by mailing saliva‐sampling kits to test for cotinine level but the return rates were low (50.5%) |
|
| Source of Funding/CoI | Department of Veterans Affairs, Veterans Health Administration, Office of Research and Development, and Health Services Research and Development. Authors declared a consultancy to Gilead Sciences and Watermark Research Partners. | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Insufficient details given |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Low rates of return when biochemical validation was attempted, but contact‐matched so differential misreport judged unlikely |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 21.7 to 28.4% lost to follow‐up rate |
Begh 2015.
| Methods | Setting: NHS Stop Smoking clinic, UK Recruitment: smokers recruited from the participating general practices and Stop Smoking services. Selected for motivation to quit |
|
| Participants | 119 smokers; 69% female; average age 44.8; average cigarettes smoked per day 20.8 Therapists: trained research nurses and Stop Smoking advisors |
|
| Interventions | Pharmacotherapy: NRT; 21 mg per 24 hour nicotine patches for 8 to 12 weeks 1. 7 weekly sessions of withdrawal support, of which 5 sessions included placebo training (16 minutes each) starting one week prior to quit date 2. 7 weekly sessions of withdrawal support, of which 5 sessions included attentional retraining (16 minutes each) starting one week prior to quit date |
|
| Outcomes | Prolonged abstinence at weeks 4, 8, and at 6 months Validation: exhaled carbon monoxide < 10 ppm |
|
| Source of Funding/CoI | National Institute for Health Research. Authors declared research and consultancy for manufacturers of smoking cessation medication, including consultancy for GlaxoSmithKline Consumer Healthcare and research‐initiated project grant funding from Pfizer. | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated simple randomisation scheme |
| Allocation concealment (selection bias) | Low risk | An independent programmer entered the sequence onto a dedicated online database which was accessed by study staff in clinics |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 30.0% to 40.7% lost to follow‐up at 6 months |
Berndt 2014.
| Methods | Setting: cardiac wards, Netherlands Recruitment: inpatients by ward nurses, at the bedside |
|
| Participants | 372 in relevant arms, excl 7 deaths (5 TC, 2 FC) 73% M, av age 56, av cpd 21 Therapists: face‐to‐face counselling (FC) provided by recently trained cardiac nurses, telephone counselling (TC) provided by experienced telephone counsellors |
|
| Interventions | Pharmacotherapy: NRT; patches (21 mg/day or 14 mg/day (10 to 20 cpd) for 8 weeks incl weaning) 1. UC (control): brief quit advice from ward nurses + brochure; no NRT (historical control, before wards assigned to interventions, not used in review) 2. TC: usual care + 7 x 15‐min telephone sessions, weekly for 5 weeks, week 7, week 12 3. FC: usual care + 6 x 45‐min + 1 x 15 min face‐to‐face sessions, same schedule as TC |
|
| Outcomes | Abstinence at 6 months (90 day PP since last counselling session) Validation: none |
|
| Source of Funding/CoI | ZonMw, the Dutch Organization for Health Research and Development. Authors declared no conflicts of interest. | |
| Notes | 3 vs 2 in analyses, patch use was similar across TC & FC groups Intraclass correlation coefficient assessed; "intraclass correlations were small and not statistically different from zero" |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Cluster randomisation with sequential cross‐over design. Method of randomising wards to begin with FC or TC not described |
| Allocation concealment (selection bias) | High risk | Nurses knew assignment when recruiting patients. "Although not reported by the nurses, they may have been selective in their recruitment because patients in the intervention groups appeared more motivated in their drive to quit smoking". However, this probably had greater impact on comparison with usual care, not used in this review. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Approximately 20% lost to follow up in each group (TC = 22%, FC = 21%) |
Bloom 2017.
| Methods | Setting: research fitness facility, USA Recruitment: smokers recruited from newspaper and radio advertisements |
|
| Participants | 61 smokers; 63.3% to 67.7% female; average age 47; average cigarettes smoked per day 19.4 to 20.3 Therapists: aerobic exercise sessions were supervised by exercise physiologist. Unclear who provided health education sessions |
|
| Interventions | Pharmacotherapy: NRT; 8 weeks of transdermal nicotine patch (21 mg for weeks 5 to 8, 14 mg for weeks 9 to 10, 7 mg for weeks 11 to 12) 1. 8 sessions of telephone counselling (20 minutes each) + 12 weekly group health education sessions (60 minutes each) 2. 8 sessions of telephone counselling (20 minutes each) + 12 weekly sessions of group aerobic exercise (20 to 40 minutes) + 12 weekly cognitive behavioural sessions just before the exercise sessions (20 minutes each) |
|
| Outcomes | Continuous abstinence at months 3, 6, 12 Validation: expired carbon monoxide < 10 ppm |
|
| Source of Funding/CoI | National Institute on Drug Abuse. No declarations of interest | |
| Notes | New for 2019 update Authors confirmed a typographical error in the abstinence rate in Bloom 2017 paper and stated the figures in Abrantes 2014 are correct. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Urn randomisation |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 10.0‐12.9% lost to follow‐up at 12 months |
Bock 2014.
| Methods | Setting: 3 primary care clinics, New England, USA Recruitment: smokers identified by clinic personnel during registration. Research assistants screened interested individuals |
|
| Participants | 846 smokers 69% F, av age: 40, av cpd not described Therapists: smoking cessation specialists |
|
| Interventions | Pharmacotherapy: NRT; patch for 8 weeks 1. Standard care: brief physician advice, patch education 2. Motivational enhancement treatment: standard care + 45‐min individual counselling session & 2 counselling calls either on quit day & 2 weeks later or at 2 & 4 weeks after 1st session |
|
| Outcomes | Abstinence at 12 months (7‐day PP) Validation: carbon monoxide < 5 ppm |
|
| Source of Funding/CoI | National Institute on Drug Abuse. Authors declared no conflicts of interest. | |
| Notes | Data previously confirmed with authors for another review; 48/406 vs 58/440 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer randomised |
| Allocation concealment (selection bias) | Low risk | Research assistants enrolled prior to computer randomisation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropout over 50%; 58.6% in SC 238/440) and 52.7% in ME (232/406) |
Boyle 2007.
| Methods | Setting: Health Maintenance Organization, USA Recruitment: proactive recruitment of members filling a prescription for cessation medications; selected if motivated to quit | |
| Participants | 1329 HMO members; 58% F, av age 47, 66% smoked > pack/day | |
| Interventions | Pharmacotherapy: all participants had filled a prescription. Almost 95% used; ˜51% only bupropion, 26% only NRT, remainder both 1. No further intervention 2. Proactive call to offer counselling, up to 9 calls, given choice of structured course or unstructured format | |
| Outcomes | Abstinence at 12 months (repeated 7‐day PP at 3 months & 12 months) Validation: none | |
| Source of Funding/CoI | Robert Wood Johnson Foundation Addressing Tobacco in Managed Care Program. No declarations of interest | |
| Notes | 49% of intervention group reached, 36% of those declined, 31% of total accepted counselling. Average N of calls 5. There was no evidence of a greater relative effect in those reached or those accepting counselling. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, stratified by presence of chronic disease. Method not described |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Over 30% lost to follow‐up but similar percentage followed up in both groups (66% intervention vs 65% control, no evidence of differential attrition) |
Bricker 2014.
| Methods | Setting: Quitline in South Carolina, USA Recruitment: recruited uninsured callers to the South Carolina State Quitline |
|
| Participants | 121 smokers; 69% female; average age 39.1; 65% smoked more than half pack per day Therapists: counsellors were Bachelors or Masters level providers with at least 3 years of general counselling experience |
|
| Interventions | Pharmacotherapy: NRT; 2‐week course of nicotine patch or gum (participant’s choice) 1. 5 sessions of cognitive behavioural therapy telephone intervention (1st call 30 minutes and each subsequent call 15 minutes) 2. 5 sessions of acceptance and commitment therapy telephone intervention (1st call 30 minutes and each subsequent call 15 minutes) |
|
| Outcomes | 30‐day point prevalence abstinence at 6 months Validation: none |
|
| Source of Funding/CoI | National Institute on Drug Abuse, National Cancer Institute. Authors declared consultancy for Pfizer | |
| Notes | New for 2019 update. Previously excluded. Reason: both the control and the intervention received equal amounts behavioural counselling; telephone‐delivered acceptance and commitment therapy (ACT) versus cognitive behavioral therapy (CBT) for smoking cessation was being assessed. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation sequence |
| Allocation concealment (selection bias) | Unclear risk | Insufficient details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Self‐report only but contact matched in both groups so differential misreport judged unlikely |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 27.1‐38.7% lost to follow‐up at 6 months |
Brody 2017.
| Methods | Setting: Veterans Affairs Los Angeles Healthcare System, USA Recruitment: smokers recruited via flyer advertisement from the smoking and schizophrenia treatment programmes. Selected for motivation |
|
| Participants | 42 smokers; 100% male; average age 56.3 to 57.5 years; average cigarettes smoked per day 18.5 to 19.6 Therapists: cognitive behavioural therapy by a psychologist; home visits by the study investigators |
|
| Interventions | Pharmacotherapy: NRT; ‐ combination extended treatment groups (with or without home visit): combination of three medications (bupropion, nicotine patch, nicotine lozenge) for 6 months ‐ usual care: single smoking cessation medication (patch, bupropion or varenicline) typically for at least 2 to 4 weeks 1. combination extended treatment without home visit: 12 weekly sessions of cognitive behavioural therapy (60 minutes each) 2. combination extended treatment plus home visit: 12 weekly sessions of cognitive behavioural therapy (60 minutes each) + biweekly home visits (20 to 30 minutes each) 3. usual care (excluded from our meta‐analyses due to different pharmacotherapy to the other groups) |
|
| Outcomes | 7‐day point prevalence abstinence at week 12 and at 6 months Validation: exhaled carbon monoxide ≤ 3 ppm |
|
| Source of Funding/CoI | National Institute on Drug Abuse, Department of Veterans Affairs Office of Research and Development and Tobacco‐Related Disease Research Program. No declarations of interest | |
| Notes | New for 2019 update Lost to follow‐up numbers were obtained from the authors via email correspondence |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation sequence |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Lost to follow‐up rates were 21.4% to 28.6% in combination extended treatment groups and 7.1% in usual care group at 6 months. |
Brown 2013.
| Methods | Setting: community, USA Recruited: community volunteers who had “previous difficulty quitting for even short periods of time." Selected if motivated to quit |
|
| Participants | N = 49; dropouts: 7 49% F, av age: standard = 48.30; distress tolerance = 47.19, av. cpd standard = 22; distress = 21 Therapists: doctoral‐level psychologists or trainees (psychology interns/postdoctoral fellows) delivered the treatment. |
|
| Interventions | Pharmacotherapy: “8 weeks of nicotine replacement therapy in the form of the nicotine patch (Nicoderm CQ) beginning on quit day, including 4 weeks of the 21 mg patch, 2 weeks of 14 mg, and 2 weeks of 7 mg.” 1. standard smoking cessation treatment 2. distress tolerance treatment = incorporated elements of exposure‐based therapies and Acceptance and Commitment Therapy |
|
| Outcomes | Abstinence at 26 weeks (7‐day PP) Validation: expired carbon monoxide (CO, 5 ppm or less) + cotinine verification (cotinine, 10 ng/mL or less) |
|
| Source of Funding/CoI | National Institute on Drug Abuse. Authors declared no conflicts of interest. | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Participants treated in groups, 3 groups for each condition; “each treatment assignment was randomly selected from the fixed pool of possible assignments” |
| Allocation concealment (selection bias) | High risk | Type of treatment allocated for next group likely to have been known before participant recruitment |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Overall 14% lost; standard 9% (2/22), distress 19% (5/27) |
Busch 2017.
| Methods | Setting: Miriam and Rhode Island Hospitals in Providence, USA Recruitment: inpatient cardiac units at the Miriam and Rhode Island Hospitals in Providence |
|
| Participants | 64 smokers; 27.1% female; average age 55.6; average cigarettes smoked per day 16.4 Therapists: research team members (licenced clinical psychologist and clinical psychology post‐doctoral fellow) |
|
| Interventions | Pharmacotherapy: NRT; 8 weeks of nicotine patches starting on 21 mg patch for those smoking > 10 cigarettes per day and on 14 mg for those starting ≤ 10 cigarettes per day 1. Usual care: one in‐hospital counselling session (50 minutes) + 5 mailings of print materials + 5 brief “check‐in” calls from a health educator following each mailing (5 to 10 minutes each) 2. One in‐hospital counselling session + > 5 post‐discharge contacts at 1, 3, 6, 9 and 12 weeks. Sessions 1 & 2 (50 minutes each) in‐person at a research clinic or in the participant’s home; Sessions 3 to 6 (30 minutes each) by phone |
|
| Outcomes | 7‐day point prevalence abstinence at weeks 12 and 24 post‐discharge from the hospital Validation: carbon monoxide < 10 ppm |
|
| Source of Funding/CoI | National Heart, Lung, and Blood Institute of the National Institutes of Health. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated randomisation |
| Allocation concealment (selection bias) | Low risk | The study statistician provided sequenced randomisation envelopes. The randomisation envelopes were opened by counsellors following the completion of each in‐hospital smoking cessation session. Counsellors then immediately informed the participant of their treatment condition. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 21.2 to 22.6% lost to follow‐up at 24 weeks post‐discharge |
Bushnell 1997.
| Methods | Setting: community with large military population, USA Recruitment: community volunteers Group size: max 50 American Cancer Society (ACS) or 15 Vanderbilt University Medical Center (VUMC) | |
| Participants | 314 military and civilian smokers, excluded 198 people, assignment NS, who did not attend any sessions after randomisation. 44% F, age and smoking not described Therapists: ACS‐trained volunteers, VUMC‐healthcare professionals | |
| Interventions | All participants offered free NRT (in group 2 conditional on attending 75% classes) 1. ACS: 4 x 1 hour large group sessions (max 50), no TQD 2. VUMC: 8 x 1 hour group sessions (max 15), relapse prevention model including stress management, diet, exercise | |
| Outcomes | Abstinence at 6 months (PP) Validation: CO < 8 ppm, salivary cotinine ≤ 10 mg/mL | |
| Source of Funding/CoI | ||
| Notes | Early benefit of VUMC lost at 6 months. No observed effect in active duty participants at any time | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | "randomly assigned", method not stated, stratified by military or civilian |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 198 (out of 512 randomised) did not participate, group not stated, not clear if participants knew what group they were assigned to before attending first session. |
Calabro 2012.
| Methods | Setting: university student body, USA Recruitment: advertised through flyers in campus halls, newsletters, email, and during presentations in classes Smoking cessation counsellors enrolled participants |
|
| Participants | 509 smokers (≥ 1 cpd) 53% F, av age 24.5, 39% smoked 11‐20 cpd Therapists: counsellors trained specifically in behaviour change/cigarette counselling |
|
| Interventions | Pharmacotherapy: NRT; patch offered to participants smoking ≥ 5 cpd 1. Self‐help written material, ≤ 5 mins minimal counselling, and no persuasive communication or assistance to participants 2. In‐person motivational counselling with health feedback, 2 x 60 to 120 mins over 3 months, and access to 5 web‐based booster sessions |
|
| Outcomes | Abstinence at 12 m (30‐day PP) Validation: 46 of 79 who reported abstinence provided a salivary cotinine value ≤ 5 ng/mL. |
|
| Source of Funding/CoI | National Cancer Institute. Authors declared no conflicts of interest. | |
| Notes | Coded as validated, however not all self‐reported quitters were validated due to problems with sample collection. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Statistical software package generated randomisation. |
| Allocation concealment (selection bias) | Low risk | Randomisation by computer occurred after enrolment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Dropout high and differential; intervention 43% (120/278), control 66% (153/231) |
Cook 2016.
| Methods | Setting: primary care clinics, USA Recruitment: adult smokers recruited during primary care visits who were willing to reduce their smoking but not quit |
|
| Participants | 517 smokers; 63.4% female, average age 47.0; average number of cigarettes smoked per day 17.5 Therapists: no details given |
|
| Interventions | Pharmacotherapy: NRT; 14 mg patches daily for 6 weeks and/or 2 mg gum for 6 weeks (≥ 9 per day, 1 piece for 1 to 2 hours) 1. behavioural reduction: an initial 20 minute in‐person counselling session followed by 6 weekly 10‐minute counselling calls; 7 sessions in total 2. motivational interviewing: an initial 20‐minute in‐person counselling session followed by three biweekly, 10‐minute counselling calls over 6 weeks; 4 sessions in total |
|
| Outcomes | 7‐day point prevalence abstinence at week 12 and at 6 months Validation: none |
|
| Source of Funding/CoI | National Cancer Institute, the Wisconsin Partnership Program. Authors supported by National Research Service Award from the Health Resources and Services Administration, NSF grant, NIH grants, Merit Review Award from the US Department of Veterans Affairs. No declarations of interest | |
| Notes | New for 2019 update Abstinence data received from authors via email correspondence |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | “staff were blinded to randomisation until eligibility was confirmed but not beyond that point; participants were blinded until consent was provided”. |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Lost to follow up n = 66; withdrawn n = 17 |
Cropsey 2015.
| Methods | Setting: community corrections offices, USA Recruitment: smokers under community corrections supervision were recruited via flyers posted at the community corrections offices |
|
| Participants | 500 smokers; 33.0% female, average age 37.4; average number of cigarettes smoked per day 17.9 Therapists: counsellors were doctoral or masters level clinical psychologists who had been trained in smoking cessation counselling |
|
| Interventions | Pharmacotherapy: NRT; 12 weeks’ supply of bupropion 1. one session of face‐to‐face brief advice 2. four weekly sessions of face‐to‐face brief advice and intensive counselling, each lasting 20 to 30 minutes |
|
| Outcomes | Abstinence (carbon monoxide level ≤ 3 ppm) at all study visits (weeks 8, 12 and months 6, 9, 12) Validation: carbon monoxide level (≤ 3 ppm) measured using the Vitalograph Breath Carbone Monoxide monitor |
|
| Source of Funding/CoI | The National Cancer Institute and the National Institute of Heatlh. No declarations of interest | |
| Notes | New for 2019 update Data on the number of abstinent participants received from the authors via email correspondence |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “randomisation scheme was blocked on race…”. No further details given |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Lost to follow‐up rates at 12 months: no counselling arm 25.8%; counselling arm 23.4% |
Ellerbeck 2009.
| Methods | Settng: primary care patients, 50 rural practices, Kansas, USA Recruitment: smoking patients not selected for motivation, but 67% of those eligible enrolled, only 8.7% in pre‐contemplation stage of change | |
| Participants | 750 smokers of > 10 cpd, 59% F, av age 47, av cpd 24, 61% contemplation, 30% preparation | |
| Interventions | All participants mailed an offer of free pharmacotherapy every 6 months, 4 times in total. Nicotine patch 21 mg for 6 weeks or bupropion SR (150 mg twice daily) for 7 weeks 1. Control. No other contact 2. Moderate intensity disease management: up to 2 calls from counsellor in each cycle encouraging uptake of pharmacotherapy, newsletter mailings & periodic progress reports with counselling suggestions faxed to physician 3. High‐intensity disease management, up to 6 calls at approx 1, 3, 6, 9, 12 weeks from start of each cycle |
|
| Outcomes | Abstinence at 24 months (PP). Study also reported analysis based on combination of effects at all follow‐up points. Sustained abstinence not a suitable outcome since no quit date and repeated intervention Validation: attempted saliva cotinine (< 15 ng/mL) by mail at 12 and 24 months. Proxy report used at 24 months for non‐returners. Rate of validation similar across groups |
|
| Source of Funding/CoI | National Cancer Institute. Medication provided by GlaxoSmithKline, "The funding sources were not involved in the design, conduct or analysis of this study or the decision to submit the study for publication". No declarations of interest | |
| Notes | Participants could have multiple courses of pharmacotherapy; 23%, 33%, 23%, 12%, and 9% of participants requested 0, 1, 2, 3, or 4 courses, Disease management conditions increased use in first cycle and reduced it later. 41% of cycles used bupropion & 59% patch. Over 24 months, average number of calls 3.6 in 2. and 8.2 in 3. Fewer calls in later cycles No evidence of effect based on PP, but some evidence of benefit when all follow‐ups taken into account High intensity vs control in main comparison. Moderate intensity quit almost identical (35/238 14.7%) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "computer generated random numbers table was utilized to generate allocation cards in blocks of 24 with allocation equally distributed across treatment groups". |
| Allocation concealment (selection bias) | Low risk | Quote: "cards were placed in sequentially numbered, opaque, sealed envelopes". |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated and proxy report used for non‐returners; rate of non‐return similar across groups |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Less than 20% lost to follow‐up, similar distribution amongst groups (11% control, 16% in both moderate‐ and high‐intensity intervention arms) |
Ferguson 2012.
| Methods | Setting: National quitline, Engalnd Recruitment: non‐pregnant smokers aged ≥ 16 years, residing in England who called the quitline and agreed to set a quit date |
|
| Participants | 2591 smokers in total (1295 in the relevant arms); 52.3% female, average age 38; average number of cigarettes smoked per day: 497 in ≤ 10 cpd category; 1226 in 11 to 20 cpd category; 547 in 21 to 30 cpd category; 230 in ≥ 31 cpd category Therapists: trained advisors from two helpline centres |
|
| Interventions | Pharmacotherapy: NRT; no cost vouchers for 21 days’ supply of 15 mg per 16 hour transdermal nicotine patches which were redeemed by a telephone call. A second 21 days’ supply could be redeemed in the same way three weeks after the initial batch. 1. usual care (support materials by email, letter or text message before, on and after quit date + proactive telephone contact + brief motivational messages) 2. 6 sessions of more intensive, proactive support by telephone |
|
| Outcomes | Prolonged abstinence at months 1 and 6 Validation: a minority of participants (255 out of 2591 had face‐to‐face follow‐up for validation of abstinence by carbon monoxide (cut‐off of < 10 ppm)) |
|
| Source of Funding/CoI | The English Department of Health, the UK Centre for Tobacco Control Studies. No declarations of interest | |
| Notes | New for 2019 update Previously excluded. Contact amount not known so excluded from analyses 1.2 and 1.3. Use of pharmacotherapy was low; only 42.9% of those offered NRT reported receiving any and of those only 51.3% used every day. There was also little difference between number of calls completed between proactive and standard telephone counselling conditions. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Lost to follow‐up rate: NRT + usual care arm 44.7%; NRT + proactive support arm 45.5% |
Fiore 2004.
| Methods | Setting: primary care patients, 16 clinics, USA Recruitment: clinic attenders willing to accept treatment | |
| Participants | 961 smokers of ≥ 10 cpd. (a further 908 were allowed to select treatment, not included in review. Demographic details based on 1869); 58% F, av age 40, av cpd 22 Therapists: trained cessation counsellors | |
| Interventions | Pharmacotherapy: NRT (patch, 22 mg, 8 weeks including tapering) 1. NRT alone 2. As 1 plus Committed Quitters programme, single telephone session and tailored self‐help 3. As 2 plus face‐to‐face individual counselling, 4 x 15 to 25‐min sessions, pre‐quit, ˜TQD, next 2 weeks |
|
| Outcomes | Continuous abstinence at 1 year (no relapse lasting 7 days), also PP Validation: CO, cut‐off not specified. 2 discordant | |
| Source of Funding/CoI | National Cancer Institute. SmithKline Beecham provided nicotine patches and access to the CQ program, but did not participate in any aspect of study design or data analysis. | |
| Notes | 3 versus 1 used in primary analysis. 3 & 2 versus 1 was more conservative since 2 had lower quit rates than 1. Use of PP outcome did not alter findings. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, method not described |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | People who did not pick up patches were excluded from analyses, similar distribution amongst groups (17% control, 16% in intervention arm 1, 14% intervention arm 2). No reported loss to follow‐up for remaining participants |
Gariti 2009.
| Methods | Setting: academic research centre, USA Recruitment: community volunteers, interested in quitting | |
| Participants | 260 light smokers (6 ‐ 15 cpd), 57% F, av age ˜43, av cpd 11, approx 1/3 smoked < 10 cpd, approx 50% had history of smoking 20 cpd Therapists: cessation counsellors |
|
| Interventions | 2 x 2 double‐blind double‐dummy. Participants randomised to either nicotine patch (21 mg/day or 14 mg/day (< 10 cpd) for 8 wks incl weaning) or bupropion (9 wks) 1. Pharmacotherapy & medication management, 4 x 5‐10 min visits over 6 wks 2. Pharmacotherapy & counselling, 10 weekly individual 10‐15 min sessions |
|
| Outcomes | Abstinence at 1 yr, sustained with no relapse of over 7 days smoking (study primary outcome was PP abstinence) Validation: CO ≤ 9 ppm & cotinine (NicAlert) ≤ 200 ng/mL or cotinine < 50 ng/mL |
|
| Source of Funding/CoI | National Institute on Drug Abuse. No declarations of interest | |
| Notes | NRT & bupropion conditions not reported separately by counselling condition, so 2 vs 1 entered in NRT or bupropion section. Favoured NRT but no significant difference at any follow‐up. More evidence of effect on sustained than PP rates at 1 yr, but substituting PP in MA did not affect findings | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated "urn" randomisation by independent data analyst |
| Allocation concealment (selection bias) | Low risk | Randomisation after enrolment, not predictable |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 108 (84%) intervention and 108 (82%) control reached at 1 yr |
Gifford 2011.
| Methods | Setting: academic research centre, USA Recruitment: community volunteers |
|
| Participants | 303 smokers with at least 1 quit attempt in past 2 years 58.7% F, av age: 45.99, av cpd 24 Therapists: abuse therapist + clinical psychology doctoral students |
|
| Interventions | Pharmacotherapy: bupropion for 10 weeks. 1. Control; 1 hr of "medication instruction group presenting the rationale for bupropion" 2. Bupropion plus functional analytic psychotherapy (FAP) and acceptance and commitment therapy (ACT), 20 sessions, 1 group & 1 individual session per wk for 10 wks |
|
| Outcomes | Abstinence at 1 yr (7‐day PP). Continuous abstinence also reported but denominators not clear Validation: CO ≤ 10 ppm |
|
| Source of Funding/CoI | National Institute on Drug Abuse. No declarations of interest | |
| Notes | Numbers quit calculated from percentages. Included in brief intervention subgroup 1.1.1, sensitivity analysis in dose‐response did not alter estimates | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised using generator www.randomizer.org |
| Allocation concealment (selection bias) | Low risk | Randomisation did not occur until after enrolment. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | 38% intervention & 67% control lost to follow‐up, including 10 intervention & 2 control dropouts before treatment |
Ginsberg 1992.
| Methods | Setting: academic research centre, USA Recruitment: community volunteers | |
| Participants | 99 smokers with an acquaintance willing to participate as a support partner; 54% F, av age 38, av cpd 26 | |
| Interventions | Pharmacotherapy: nicotine gum, 2 mg, duration not specified 1. Instruction for gum use & educational materials, 2 brief sessions over 2 weeks 2. Instructions as 1. included with a group‐based behavioural programme including skill training, 5 sessions over 4 weeks. Duration not specified, assumed to be 91 to 300 min 3. As 1. plus behavioural programme and partner‐support programme, 8 sessions over 5 weeks. Not included in this review |
|
| Outcomes | Abstinence at 52 weeks (not clear if abstinence required at prior assessment at wks 4, 12, 26) Validation: CO < 10 ppm, urine cotinine < 50 ng/mL. Paper stated that cotinine levels failed to confirm self‐report in 7 people, 3 of whom were still coded as abstinent on the balance of evidence. | |
| Source of Funding/CoI | ||
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Quote: "randomly assigned to 3‐6 member groups in order of entrance into treatment within time constraints. Treatment for each group was randomly selected ...". |
| Allocation concealment (selection bias) | Unclear risk | No details reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 9 participants lost to follow‐up counted as smokers. 1 participant who died excluded from analyses |
Hall 1985.
| Methods | Setting: clinic, USA Recruitment: referred by physicians, friends or self | |
| Participants | 84 smokers in relevant arms; 53% M, av age 38, av cpd 30.5 Therapists: 2 psychologists | |
| Interventions | Pharmacotherapy: NRT; gum (2 mg, available for 6 months) 1. Intensive behavioural treatment (incl relapse prevention skill training, relaxation, 30 seconds aversive smoking of 3 cigs). 14 x 75 min sessions over 8 weeks 2. Low‐contact . Met x 4 in 3 weeks, educational materials, written exercises, group discussion 3. Intensive behavioural, no gum. Not included in this review |
|
| Outcomes | Abstinence at 52 weeks (assume PP) Validation: CO < 10 ppm, thiocyanate < 85 mg/mL, reports of significant others (biochemical measures failed to confirm self‐report in 3 instances) | |
| Source of Funding/CoI | National Institute on Drug Abuse. No declarations of interest | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomly assigned within time constraints." Author clarification: "There were two or more treatment conditions available within any time block, and participants were randomly assigned to conditions within that time block". |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 3 dropouts from group 2 and 3 from group 3. Assumed to be included in denominator for reported % abstinent used to derive numbers quit |
Hall 1987.
| Methods | Setting: clinic, USA Recruitment: community volunteers or referrals | |
| Participants | 139 smokers; 53% M, av age 39, av cpd 30 (71 in relevant arms) Therapists: advanced graduates in clinical psychology or health psychology | |
| Interventions | Pharmacotherapy: NRT (gum). Placebo arms of factorial trial not used in review 1. Intensive behavioural treatment, 14 x 75 min sessions (period not stated) (incl 6 seconds aversive smoking, RP skills training, written exercises) 2. 'Low contact' 5 x 60 min sessions (incl written exercises, educational materials, group discussions, quitting techniques) | |
| Outcomes | Abstinence at 52 wks (assume PP) Validation: thiocyanate < 95 mm/L (unless marijuana use reported), CO < 8 ppm, significant other | |
| Source of Funding/CoI | National Institute on Drug Abuse. No declarations of interest | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised; method not described |
| Allocation concealment (selection bias) | Unclear risk | No details reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 2 dropouts in 1 & 2 in 2 included in ITT analyses. "Differences between conditions were not statistically significant." |
Hall 1994.
| Methods | Country: USA Recruitment: community volunteers or referrals | |
| Participants | 149 smokers (> 10 cpd) 52% F, av age 41, av cpd 25, 31% had history of MDD Therapists: physician, psychologist. Both received training. | |
| Interventions | Pharmacotherapy: NRT (gum, 2 mg for up to 12 wks, tapering from wk 4)
1. Mood Management. 10 x 2 hr sessions over 8 wks. Similar to control, plus specific cognitive‐behavioural components for developing skills for coping with situations leading to poor mood. Thought stopping, rational‐emotive techniques, relaxation etc. 2. Standard group therapy. 5 x 90 min sessions over 8 wks. Information and group support for planning and implementing individual strategies |
|
| Outcomes | Continuous abstinence at 52 wks (confirmed quit at all prior assessments and no smoking in previous wk) Validation: CO ≤ 10 ppm and urine cotinine ≤ 60 ng/mL | |
| Source of Funding/CoI | National Institute on Drug Abuse. Merrell Dow Pharmaceuticals Inc. provided drugs. No declarations of interest. | |
| Notes | Both behavioural interventions were relatively intensive. Positive effect reported for subgroup with history of major depression | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, method not described |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Dropouts included as smokers, but numbers not specified |
Hall 1998.
| Methods | Setting: cessation clinic, USA Recruitment: community volunteers. Exclusion criteria included MDD within 3 m of baseline | |
| Participants | 199 smokers of ≥ 10 cpd; 55% F, av age 40, av cpd 21‐25; 33% had history of MDD Therapists: 3 doctoral‐level clinical psychologists | |
| Interventions | Pharmacotherapy: nortriptyline (titrated to therapeutic levels ‐ usually 75‐100 mg/day for 12 wks). Placebo arms of factorial trial not used in review
1. Mood management. 10 x 2 hr sessions over 8 wks 2. Standard group therapy control. 5 x 90 min sessions over 8 wks (see Hall 1994 for description of each intervention) |
|
| Outcomes | Abstinence at 64 wks (1 yr post‐treatment). Continuous abstinence rates not reported by psychological treatment group Validation: CO < 10 ppm and cotinine < 341 nmol/L | |
| Source of Funding/CoI | National Institute on Drug Abuse. No declarations of interest | |
| Notes | Both behavioural interventions were relatively intensive. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised by computer, after stratification on history of MDD and number of cigs smoked |
| Allocation concealment (selection bias) | Low risk | Computer randomisation after data collection |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 16% lost to follow‐up at 1 yr, no difference by group, included in denominators for MA |
Hall 2002.
| Methods | Country: USA Recruitment: community volunteers. Exclusion criteria included current MDD | |
| Participants | 220 smokers (146 in relevant arms); ≥ 10 cpd; 40%‐47% F, av age 37‐43, av cpd 20‐23; 33% had history of MDD | |
| Interventions | Pharmacotherapy: bupropion (300 mg for 12 wks) or nortriptyline (titrated to therapeutic levels, typically 75 or 100 mg/d). Factorial 3 x 2 design, placebo arms not used in this review 1. Medical Management (MM) control: physician advice, S‐H, 10‐20 min 1st visit, 5 min at 2, 6, 11 wks 2. Psychological Intervention (PI) as MM plus 5 x 90 min group sessions in wks 4, 5, 7 & 11 | |
| Outcomes | PP abstinence at 1 yr (47 wks post‐quit date). Continuous abstinence not reported by subgroup Validation: CO ≤ 10 ppm, urine cotinine ≤ 60 ng/mL | |
| Source of Funding/CoI | National Institute on Drug Abuse. No declarations of interest | |
| Notes | Bupropion PI vs MM & nortriptyline PI vs MM used in relevant subgroups. Trial also contributed to review of combined interventions Stead 2016, using different combination of arms. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, method not specified, "double blind" |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 19% lost to follow‐up at 12 m, similar numbers across groups |
Hall 2009.
| Methods | Setting: cessation clinic, USA Recruitment: community volunteers |
|
| Participants | 402 smokers (≥ 10 cpd) aged ≥ 50; 40% F, av age 57, av cpd 21 | |
| Interventions | Pharmacotherapy: NRT (gum, 10 weeks, 2 or 4 mg) & bupropion (12 weeks). 2 arms had extended access to gum 1. "Standard treatment"; 5 group sessions over 8 weeks, 'Clear Horizons' manual 2. Extended CBT; 11 individual 20 to 40 min sessions from week 10 to week 52, schedule front‐loaded. Incl motivation, mood management, weight control, social support, coping with withdrawal 3. Extended NRT. nicotine gum available until week 52, no additional behavioural support 4. Extended combined, CBT & NRT; 3 & 4 |
|
| Outcomes | Abstinence at 104 weeks (one year after end of all treatment) (PP) Validation: CO ≤ 10 ppm and urine anatabine/anabasine ≤ 2 mg/mL |
|
| Source of Funding/CoI | National Institute on Drug Abuse. No declarations of interest | |
| Notes | Meta‐analysis comparison was 2 & 4 vs 1 & 3 | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised at end of initial treatment, computerised allocation list by statistician who had no contact with participants. Stratified on gender, history of MDD, current cigarette abstinence status |
| Allocation concealment (selection bias) | Low risk | "The assignment of individual participants by subject number was then transmitted electronically to clinical staff." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Less than 20% lost to follow‐up in each group, denominator excluded participants who died during the study but counted all others lost to follow‐up as smokers. |
Hasan 2014.
| Methods | Setting: North Shore Medical Center in Salem, USA Recruitment: smokers admitted with a cardiac or pulmonary illness were electronically identified |
|
| Participants | 122 smokers in total (81 in the relevant arms); 39.5% female, average age 54.4 to 55.3; average number of cigarettes smoked per day 20.5 to 21.2 Therapists: no details given |
|
| Interventions | Pharmacotherapy: NRT; free one‐month supply of nicotine patches with the initial dose based on the number of cigarettes they smoked prior to hospitalisation. Also given nicotine gum or lozenges to administer as needed 1. one intensive in‐hospital counselling (30 minutes) + five telephone calls with additional counselling at 1, 2, 4, 8 and 12 weeks post‐discharge (15 minutes each) 2. one intensive in‐hospital counselling (30 minutes) + five telephone calls with additional counselling at 1, 2, 4, 8 and 12 weeks post‐discharge (15 minutes each) + one in‐person hypnotherapy session within 1 to 2 weeks of hospital discharge (90 minutes) |
|
| Outcomes | 7‐day point prevalence abstinence at week 12 and at 6 months Validation: urinary cotinine levels (< 15 mg/mL). In case of no urine sample returned, abstinence was confirmed by contacting a household proxy. |
|
| Source of Funding/CoI | The Norman H. Read CharitableTrust Foundation. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | “permuted blocks of three (1:1:1)”. No further details given |
| Allocation concealment (selection bias) | Low risk | “Assignments sequentially numbered and schedule was maintained independent of the study by the project coordinator. Randomised assignments were concealed from both patients and research staff until patients had signed the informed consent document and were enrolled in the study”. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Lost to follow‐up rates: Counselling arm 29.3%; counselling + hypnotherapy arm 32.5% |
Hollis 2007.
| Methods | Setting: community‐based telephone quitline programme, Oregon, USA Recruitment: callers invited to participate; assumed to be fully or partly motivated to quit | |
| Participants | 4614 smokers randomised to: brief counselling (872, no NRT; 868, with NRT); moderate counselling (718, no NRT; 715, with NRT); intensive counselling (720, no NRT; 721, with NRT) 40% M, av age 41, 90% white, av cpd 21 |
|
| Interventions | Factorial design; arms that were offered free NRT (patches, initial 5‐wk supply, 3 more wks available) contributed to this review Intervention 1. Brief counselling (usual care), 15‐min call + referral material + tailored S‐H materials Intervention 2. Moderate counselling: 40 mins counselling based on MI + 1 brief call to encourage use of community services, tailored S‐H materials Intervention 3. Intensive counselling: As 2, plus offer of up to 4 additional telephone calls. Each call incorporated MI techniques, stage assessment, RP as needed | |
| Outcomes | 30‐day PPA at 6 and 12 months Validation: none | |
| Source of Funding/CoI | National Cancer Institute. GlaxoSmithKline supplied nicotine patches. Two authors employed by Free & Clear, Inc, a for‐profit company providing telephone counselling services | |
| Notes | 3 vs 1 in main comparison. Actual contact in 3; mean 2.9 sessions, 60.6‐min contact Also contributed to review of combined interventions Stead 2016 |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "a computer algorithm randomly assigned participants". |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only and different amounts of contact between arms |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Moderate level of attrition but balanced between groups, and participants lost to follow‐up counted as smokers (72% followed up in groups 1 and 2, 68% followed up in group 3) |
Huber 2003.
| Methods | Setting: academic research centre, Germany Recruitment: community volunteers | |
| Participants | 225 smokers (102 in relevant arms); 55% F, av age 38, av cpd 28 | |
| Interventions | Pharmacotherapy: nicotine gum, 2 or 4 mg 1. 5 x 90‐min weekly meetings. Included contracting, reinforcement, relaxation, skills training 2. Same schedule of meetings, 45‐min only, focus on sharing experiences 3. As 1, no nicotine gum. Not included in this review 4. Wait‐list control for 6 m. Not included in this review |
|
| Outcomes | PP abstinence at 12 m Validation: CO ≤ 4 ppm | |
| Source of Funding/CoI | Not specified. No declarations of interest | |
| Notes | Control and intervention fell into same categories for number and duration of sessions. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, method not described |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 31 people attending 2 or fewer meetings not included in analysis. Said to be evenly distributed. Later dropouts included as smokers; 90% of those receiving therapy (excluded wait‐list group 4, who were also excluded from this review) followed up at 12 m. |
Humfleet 2013.
| Methods | Setting: HIV clinics, USA Health Care Recruitment: HIV clinic patients, volunteering for study |
|
| Participants | 209 smokers 82% M, av age 45, av cpd 20 Therapists: clinicians specialising in smoking cessation/social work/psychology |
|
| Interventions | Pharmacotherapy: NRT; patch or gum for 10 weeks, available to those who smoked ≥ 5 cpd, number not eligible, not specified 1. Self help: "How to Quit Smoking"; brief meeting with study staff who reviewed guide and recommended establishing a quit date 2. Individual counselling: 6 x 40 to 60‐min sessions of CBT targeted towards needs of HIV positive smokers, weeks 1, 2, 3, 4, 8 & 12 3. Computer‐based: each component structured into a “step” roughly corresponding to the first 5 sessions of the counselling intervention. Individuals were directed to complete self‐assessment exercises and homework assignments. |
|
| Outcomes | Abstinence at 52 weeks (7‐day PP) Validation: CO ≤ 10 ppm |
|
| Source of Funding/CoI | National Institute on Drug Abuse. California Tobacco‐Related Disease Research Program. Authors declared no conflicts of interest. | |
| Notes | Individual counselling compared to self‐help in main MA, added computer‐based arm in sensitivity analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Smokers stratified based on N cpd, gender, history of depression and then within each stratum randomised via computer algorithm to 1 of 3 conditions in 1:1:1 fashion into a parallel‐group design |
| Allocation concealment (selection bias) | Low risk | Randomisation occurred after enrolment & stratification. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 19% overall loss to follow‐up |
Jorenby 1995.
| Methods | Country: 2 academic research sites, USA Recruitment: community volunteers | |
| Participants | 504 smokers (≥ 15 cpd); ˜53% F, av age 44, av cpd 26‐29 Therapists: trained smoking cessation counsellors | |
| Interventions | Compared 22 mg vs 44 mg nicotine patch and 3 types of adjuvant treatment. Patch groups collapsed. All participants had 8 weekly assessments by research staff 1. Minimal: Given S‐H pamphlet by physician during screening visit for trial entry, and instructed not to smoke whilst wearing patch. No further contact with counsellors 2. Individual: Given S‐H pamphlet at screening visit along with motivational message. Also met nurse counsellor x 3 following quit date. Nurse helped generate problem‐solving strategies and provided praise and encouragement. 3. Group: Given S‐H pamphlet at screening visit along with motivational message. Received 8 x 1‐hour weekly group sessions. Skills training, problem‐solving skills | |
| Outcomes | 7‐day PP abstinence at 26 wks Validation: CO < 10 ppm | |
| Source of Funding/CoI | Elan Pharmaceutical Research Corporation. Authors declared potential conflicts of interest. | |
| Notes | No significant difference in dose‐related outcome and no dose‐counselling interaction at 26 weeks reported. Patch arms collapsed in analysis. 3 vs 1 used in primary comparison, RR 0.99 (95% CI 0.69 to 1.42). RRs for other comparisons: 2 & 3 vs 1 = 1.10 (95% CI 0.81 to 1.49), 2 vs 1 = 1.21 (95% CI 0.86 to 1.70), 3 vs 2 = 0.82 (95% CI 0.58 to 1.15) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised, method not stated |
| Allocation concealment (selection bias) | Unclear risk | "In a double blind manner" for NRT, but not specified for counselling |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses not specified by group, relatively low rate lost to follow‐up overall (16.3%), Counted as smokers in report & MA |
Kahler 2015.
| Methods | Setting: community, USA Recruitment: smokers recruited through advertisements on multiple media |
|
| Participants | 77 smokers; 50% female, average age 47.4 to 44.5; average number of cigarettes smoked per day 18.7 to 18.8 Therapists: six female doctoral level counsellors with prior experience in behavioural health counselling |
|
| Interventions | Pharmacotherapy: NRT; 8 weeks of nicotine patches beginning on their scheduled quit date, which coincided with the third session (2 weeks after the initiation of treatment). Dosage dependent on the number of cigarettes smoked per day 1. Usual care: six sessions (five weekly and a final session that occurred 2 weeks later); session 1 lasted 60 minutes and the later sessions 30 minutes; 30 minutes of the session 1 and 20 minutes of the subsequent sessions were dedicated to teaching progressive muscle relaxation. 2. Positive psychotherapy: same as the usual care in terms of the number and duration of the sessions but 30 minutes of the session 1 and 20 minutes of the subsequent sessions were dedicated to positive psychotherapy‐specific content. |
|
| Outcomes | Continous abstinence at weeks 8, 16, 26 Validation: alveolar carbon monoxide (≤ 8 ppm) using a Bedfont Scientific Smokelyzer breath carbon monoxide monitor; saliva cotinine (≤15 ng/mL) radioimmune assay analysis |
|
| Source of Funding/CoI | The National Cancer Institute. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Low risk | “data for the randomisation were sent by research assistant to the project coordinator who conducted the computer‐based urn randomisation and informed the treatment provider of treatment assignment”. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Lost to follow‐up rates: Usual care arm 31.6%; positive psychotherapy arm 25.6% |
Killen 2008.
| Methods | Setting: community cessation clinic, USA Recruitment: community volunteers |
|
| Participants | 301 smokers (≥ 10 cpd or 3.5 packs/wk) (excluded 3 participants who received wrong treatment); 40% F, av age ˜46, av cpd ˜20 | |
| Interventions | Pharmacotherapy: bupropion (300 mg, 9 wks) & NRT (21 mg patch, 8 wks incl tapering) Common behavioural therapy: 6 x 30‐min individual CBT sessions at baseline, TQD, 1, 2, 4, 6 wks 1. Extended therapy: 4 x 30‐min sessions at 8, 12, 16, 20 wk, & weekly check‐in calls to automated system; report of relapse or craving prompted proactive calls. 2. Control: 5‐min general support calls at 8, 12, 16, 20 wks |
|
| Outcomes | Abstinence at 52 wks (7‐day abstinence at both 20 & 52 wks) (continuous abstinence also reported but not used in MA as could underestimate any effect on recycling) Validation: CO < 10 ppm (11 self‐reported quitters no longer living in study area accepted as quitters without validation) |
|
| Source of Funding/CoI | National Institute on Drug Abuse. Authors declared no conflicts of interest. | |
| Notes | Tested extended duration therapy | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised using a permuted block method (block size = 4), stratified on gender |
| Allocation concealment (selection bias) | Low risk | Participants assigned to next available ID number in corresponding gender. Researchers & participants were blinded to extended treatment assignment to the end of the open‐label phase. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 89% followed up in standard‐care group, 90% followed up intervention group. |
Kim 2015.
| Methods | Setting: community centre or office, USA Recruitment: smokers recruited via advertisements in Korean newspapers. Selected for motivation to quit |
|
| Participants | 30 smokers; 23.3% female, average age 46.5; average number of cigarettes smoked per day 19.0 Therapists: two Korean bilingual clinicians |
|
| Interventions | Pharmacotherapy: NRT; 8 weeks’ supply of nicotine patches 1. Eight weekly sessions of face‐to‐face individualised counselling focusing on medication management, each lasting 10 minutes 2. Eight weekly sessions of face‐to‐face individualised and culturally tailored cognitive behavioural therapy, each lasting 40 minutes |
|
| Outcomes | Continuous abstinence at weeks 1, 4 and months 3, 6 Validation: carbon monoxide (< 6 ppm) measured by a Micro+ Smokerlyzer Carbone Monoxide monitor; saliva cotinine (≤ 1 ng/mL) assessed by the NicAlert test |
|
| Source of Funding/CoI | National Institute of Drug Abuse. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Lost to follow‐up rates: Control 25.0%; intervention 21.4% |
LaChance 2015.
| Methods | Setting: USA (no further detail reported) Recruitment: from the community via newspaper and television advertisement |
|
| Participants | 49 participants, 32.7% female, average age: 42.8 ± 11.2, average cigs/day: 18.2 ± 5.2 Therapists: five therapists; a licensed psychologist, a master's level clinician, an intern, and two bachelor's level therapists |
|
| Interventions | Pharmacotherapy: 8 weeks of transdermal nicotine replacement therapy Intervention: behavioural couples treatment. Total contact time: 60 minutes each x 7 = 420 minutes Control: individual standard treatment. Total contact time: 60 minutes each x 7 = 420 minutes |
|
| Outcomes | 7‐day point prevalence abstinence at 3 and 6 months Validation: CO ≤ 8 ppm, or urinary cotinine |
|
| Source of Funding/CoI | Funding: National Institute on Durg Abuse and National Heart Lung and Blood Institute at the National Institutes of Health, and the Department of Veterans Affairs No declaration of interest |
|
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Urn randomisation |
| Allocation concealment (selection bias) | Unclear risk | No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Similar drop‐out rates (BCT‐S: 23.0%; ST: 21.7%) |
Lando 1997.
| Methods | Setting: Health Maintenance Organization, USA Recruitment: physician referral and HMO clinic newsletters | |
| Participants | 509 smokers of > 20 cpd, motivated to quit; 56% F, av age 42, av cpd 28 | |
| Interventions | All participants received prescriptions for free nicotine patch (Prostep), 22 mg for a maximum of 6 weeks plus 11 mg for 2 wks. All attended 90‐min group orientation session describing study, use of patch, behavioural information, set quit date. Standard written materials with patch included description of a toll‐free telephone help line. 1. No further support 2. Orientation session included encouragement to call toll‐free number and a registration card. 3. Additional proactive telephone counselling, 4 x 10 to 15‐min calls (approx 1, 4, 7, 9, 12 weeks from quit date). Reinforced success or negotiated a new quit date | |
| Outcomes | Abstinence at 12 months (from quit date) Validation: CO at 6 months. 96% of quitters were confirmed. | |
| Source of Funding/CoI | Lederle Laboratories. No declarations of interest | |
| Notes | Also contributed to Cochrane review of telephone counselling (Matkin 2019) Effect of counselling compared to contact & quitline alone (1 & 2 combined since fewer than 1% called quitline and no difference between quit rates). Participants who did not return questionnaires at 2, 5, 8, 12 weeks were called by telephone. Average number of calls completed 3.76 Cluster‐randomised trial: analysis reported stated that it was adjusted for clustering effects via a mixed model, but these results were not reported except that group comparisons did not "approach statistical significance". |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Cluster‐randomised, method not described |
| Allocation concealment (selection bias) | Unclear risk | Allocation by orientation session attended; participants did not know condition in advance so risk of selection bias probably low |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 82% response rate at 12 m, no difference between groups, missing treated as smoking |
Lifrak 1997.
| Methods | Setting: substance abuse outpatient facility, USA Recruitment: community volunteers | |
| Participants | 69 smokers; 61% F, av age 39, av cpd 25 | |
| Interventions | Pharmacotherapy: nicotine patch (24‐hr, 10‐wk tapered dose) 1. Moderate intensity ‐ 4 meetings with nurse practitioner who reviewed S‐H materials and instructed in patch use 2. High intensity. As 1 plus 16 weekly 45‐min cognitive behavioural relapse prevention therapy from clinical social worker or psychiatrist experienced in addiction treatment | |
| Outcomes | Abstinence at 12 months, 1‐week PP Validation: urine cotinine for some participants, but no corrections made for misreporting | |
| Source of Funding/CoI | None stated | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation (block size 10) |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low rate of attrition (though breakdown by group not provided): 12 administrative dropouts/exclusions not included in analyses |
Lloyd‐Richardson 2009.
| Methods | Setting: 6 outpatient HIV clinics & 2 primary care clinics, USA Recruitment: eligible patients identified by physicians, motivation to quit not required | |
| Participants | 444 HIV+ smokers; 37% F, av age 42, av cpd 18 | |
| Interventions | Pharmacotherapy: nicotine patch for up to 8 weeks if willing to set quit date 1. 2 brief counselling sessions, biweekly patch collection without counselling contact 2. 4 x 30‐min sessions plus quit day call, using motivational interviewing approach |
|
| Outcomes | 7‐day point prevalence abstinence at 12 months Validation: carbon monoxide < 10 ppm |
|
| Source of Funding/CoI | National Institute on Drug Abuse. Authors declared no conflicts of interest. | |
| Notes | 72% used patch at some point during study. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomised, stratified by gender and motivation to quit |
| Allocation concealment (selection bias) | Unclear risk | No details provided |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 75% intervention, 71% control followed up at 6 m. ITT and available‐case analyses reported |
MacLeod 2003.
| Methods | Setting: community, Australia Recruitment: community volunteers | |
| Participants | 854 smokers interested in quitting; 51% F, av age 42, av cpd 24 | |
| Interventions | All participants received a free 2‐wk supply of nicotine patch by mail, instructed to purchase further supply; 14 or 21 mg depending on body weight 1. No further intervention 2. As 1. + 5 proactive telephone counselling calls at 1, 2, 3, 6 & 10 wks. 20‐min session 1 wk, 10‐min others. Toll‐free hotline, S‐H materials |
|
| Outcomes | Abstinence at 6 m (90‐day continuous) Validation: none, warning of CO test only | |
| Source of Funding/CoI | GlaxoSmithKline funded study and all authors were employed by GSK. "The conduct of the study was independently monitored and the data verified by Datapharm Australia. GlaxoSmithKline took part in discussions about study design, but had no direct role in the analysis or interpretation of the results or preparation of the report for publication." | |
| Notes | Also contributed to Cochrane review of telephone counselling (Matkin 2019). No face‐to‐face contact Average number of calls 4.7. 9% of participants called hotline. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Randomized" by shuffling folders each day after participants to be included were listed. Since there was no personal contact with participants, risk of bias judged to be low |
| Allocation concealment (selection bias) | Low risk | Potential for bias since allocation sequence not fixed in advance; however, baseline characteristics similar across groups so no evidence of selection bias |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only and differential levels of support |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | No significant difference in loss to follow‐up, 17% in NRT only, 15% in NRT+ at 6 m |
Macpherson 2010a.
| Methods | Setting: USA (no further detail reported) Recruitment: using radio, web‐based, and newspaper advertisements |
|
| Participants | 68 participants, 48.6% female, average age: intervention: 45 ± 12.2, control: 42.6 ± 11.5, average cigs/day: intervention: 18.8 ± 7.1, control: 17.3 ± 8.1 Therapists: two therapists with clinical psychology doctoral degrees and three therapists who were clinical psychology doctoral students |
|
| Interventions | Pharmacotherapy: NRT; nicotine patches from quit date with an initial dose of 21 mg for 4 weeks, followed by 2 weeks of 14 mg, and 2 weeks of 7 mg. Participants who smoked on average 10 to 12 cigarettes per day started with 14 mg for the first 6 weeks. Intervention: 8 weekly sessions of behavioural activation treatment. Total contact time: 60 minutes each x 8 = 480 minutes Control: 8 weekly sessions of standard treatment. Total contact time: 60 minutes each x 8 = 480 minutes |
|
| Outcomes | Abstinence: continuous abstinence at 1, 4, 16 weeks, and 6 months Validation: carbon monoxide ≤ 10 ppm, cotinine ≤ 5 ng/mL |
|
| Source of Funding/CoI | Funding: National Institute on Drug Abuse No declarations of interest |
|
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No detail given |
| Allocation concealment (selection bias) | Unclear risk | No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | High losses to follow‐up in both arms: control: 63.6%; intervention: 57.1% |
Matthews 2018.
| Methods | Setting: USA, LGBT health centres Recruitment: from the community |
|
| Participants | 345 participants, 20.3% to 22.8% female, average age: 38.6‐39.4, average cigs/day: 12.1 to 13.8 Therapists: a professional and a lay counsellor who identified as lesbian, gay, bisexual or transgender facilitated each group. |
|
| Interventions | Pharmacotherapy: NRT; nicotine patches for 8 weeks (dose regimen dependent on the number of cigarettes) Intervention: 6 weekly culturally tailored smoking cessation therapy sessions commencing two weeks before the quit date Control: 6 weekly standard smoking cessation therapy sessions commencing two weeks before the quit date |
|
| Outcomes | Abstinence: 7‐day point prevalence at 1, 3, 6, and 12 months Validation: carbon monoxide at 1 and 3‐month follow‐up |
|
| Source of Funding/CoI | Funding: National Institute on Drug Abuse, National Ceneter for Advancing Translational Sciences, National Institutes of Health, and National Cancer Institute Declarations of interest: one of the authors consulted with the Respiratory Health Association and served on a Health Advisory Board for Pfizer Inc. |
|
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "The study statistician conducts the permuted‐block randomization using a software program developed by programmers at UIC." |
| Allocation concealment (selection bias) | Low risk | "The study statistician place the results of the assignments in sealed, solid envelopes. All study participants are blinded and retain no knowledge of CTQ or CTQ‐CT group". |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Similar attrition between groups: intervention: 33.7%; control: 34.1% |
McCarthy 2008.
| Methods | Setting: clinic, USA Recruitment: community volunteers | |
| Participants | 463 smokers; 50% F, av age 36 to 41 across arms, av cpd 22 Therapists: trained college‐aged or bachelor's level staff, supervised by experienced counsellor | |
| Interventions | Factorial trial of bupropion or placebo pharmacotherapy and counselling versus support 1. Bupropion & counselling; 13 office visits, 8 included additional 10‐min counselling, 2 prequit, TQD, 5 over 4 weeks (classified as > 300 mins contact) 2. Bupropion & psychoeducation about medication, support & encouragement. 13 office visits, 80 mins less contact time than 1. (classified as 91 to 300 mins contact) 3. Placebo & counselling. Not included in this review 4. Placebo & psychoeducation. Not included in this review | |
| Outcomes | 7‐day PP abstinence at 12 months (prolonged abstinence reported but not verified so PP used in MA) Validation: CO ≤ 10 ppm | |
| Source of Funding/CoI | National Institute on Drug Abuse & National Cancer Institute. GlaxoSmithKline provided complimentary active and placebo medication used in this study. "GlaxoSmithKline was not involved in the design, data collection, analysis, or reporting of this study." Authors declared potential conflicts of interest. | |
| Notes | 1 vs 2 used as test of adjunct behavioural support Also contributed to Cochrane reviews of combined interventions (1 vs 4) (Stead 2016), antidepressants (collapsing behavioural conditions) (Hughes 2014) and individual behavioural counselling (collapsing pharmacotherapy) (Lancaster 2017) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random number table |
| Allocation concealment (selection bias) | Low risk | Staff who screened and enrolled participants were unaware of the experimental condition to be assigned. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 63% reached at 12 m, but attrition rates did not differ by condition at any point |
NCT00879177.
| Methods | Setting: University of Connecticut Health Center, USA Recruitment: smokers with self‐reported desire to stop smoking |
|
| Participants | 203 smokers Therapists: no details given |
|
| Interventions | Pharmacotherapy: NRT; varenicline 1 tablet 0.5 mg once a day for three days followed by 1 tablet 0.5 mg twice a day for four days and then 1 tablet 1 mg twice a day for 11 weeks 1. Brief smoking cessation counselling weekly for five weeks 2. Brief smoking cessation counselling weekly for five weeks + behavioural therapy for weeks 2 to 5; ≥ 9 sessions in total |
|
| Outcomes | Abstinence at 12 months Validation: carbon monoxide and cotinine levels |
|
| Source of Funding/CoI | Unpublished study | |
| Notes | New for 2019 update Contacted Professor White (Co‐principal investigator) by email who informed us that the results were comparable for the two groups with quit rates about 50% in each group at 6 months. The results have not yet been published so we were only able to report this study narratively. |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Unpublished study |
| Allocation concealment (selection bias) | Unclear risk | Unpublished study |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Unpublished study |
O'Cleirigh 2018.
| Methods | Setting: HIV primary care clinics, USA Recruitment: providers told potentially eligible patients about the study and offered them study coordinator's contact details. Selected for motivation to quit |
|
| Participants | 53 smokers; 15.1% female; average age 49.7‐51.2; average number of cigarettes smoked per day 14.4 Therapists: intervention was provided by doctoral level clinical psychology interns and postdoctoral fellows supervised by the first author. The control group sessions were conducted by the study coordinator or research associate. |
|
| Interventions | Pharmacotherapy: transdermal nicotine replacement therapy provided on the quit day 1. Psychoeducation session before randomisation (60 minutes) + face‐to‐face hybrid treatment that targeted smoking cessation, anxiety and depression simultaneously (60 minutes x 9 sessions) 2. Psychoeducation session before randomisation (60 minutes) + post‐quit sessions in person (10 minutes x 4 sessions) |
|
| Outcomes | 7‐day point prevalence abstinence at 1, 2, 4, 6 months Validation: carbon monoxide level ≤ 4 ppm |
|
| Source of Funding/CoI | National Institute on Drug Abuse. Authors declared potential conflicts of interest. | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation in blocks of 4 conducted by the study coordinator |
| Allocation concealment (selection bias) | Low risk | "Before the study's start, a randomisation chart was created, corresponding to each study identification number. The chart was secured on a password‐protected document accessible only by the study coordinator and the principal investigator. Assignment to study condition was concealed from participants and study clinicians until the end of session 1". |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Lost to follow‐up rate: intervention group 50.0%; control group 22.2% |
Ockene 1991.
| Methods | Setting: primary care clinics, USA Recruitment: clinic attenders, not selected for interest in quitting | |
| Participants | 380 smokers in relevant arms (excluded deaths and some who did not receive intervention); of 1223 smokers in study; 57% F, av age 35, av cpd 23 | |
| Interventions | Pharmacotherapy: nicotine gum; offer of free gum 2 x 3 factorial design, physician intervention ± follow‐up 1. Physician counselling (initial session and 1 follow‐up) and offer of NRT. Follow‐up telephone counselling by psychologist or health educator, 3 calls (1, 2, 3 months) approx 10 mins, behavioural recommendations. Letters 2. Physician counselling as 1. No additional follow‐up |
|
| Outcomes | Abstinence at 6 m (7‐day); (3 m sustained abstinence rates not given by condition) Validation: none | |
| Source of Funding/CoI | ||
| Notes | Marginal to include since relatively low use of pharmacotherapy; in intervention condition; of those reached, 33% refused use and 18% tried for 2 days or less 12 m abstinence rates reported in Ockene 1994 but not given by follow‐up condition. Also contributed to review of combined interventions (Stead 2016) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, method not described |
| Allocation concealment (selection bias) | Unclear risk | Allocated prior to physician encounter |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only and differential support between arms |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 19% lost to follow‐up, higher in telephone follow‐up group. All included as smokers in analysis |
Okuyemi 2013.
| Methods | Setting: homeless shelters, Minnesota, USA community Recruitment: homeless adults willing to use nicotine patch |
|
| Participants | 430 smokers (≥ 1 cpd for last 7 days) 25.3% female, av age 44.4, av cpd 19.3 Therapists: trained counsellors |
|
| Interventions | Pharmacotherapy: NRT; 21 mg patch for 8 weeks 1. Single session 10 to 15‐min brief advice 2. Motivational interviewing, 6 x 15 to 20‐min sessions, baseline, 1, 2, 4. 6 & 8 weeks Focus on encouraging cessation and NRT adherence |
|
| Outcomes | Abstinence at 26 weeks (7‐day PP) Validation: CO < 5 ppm |
|
| Source of Funding/CoI | National Heart Lung and Blood Institute. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "At the baseline visit, pre‐assigned randomization numbers prepared by the study statistician determined which study arm the participant would be enrolled." |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Overall 25% lost to follow‐up, not significantly different across groups |
Otero 2006.
| Methods | Setting: Brazil Recruitment: community volunteers | |
| Participants | 1199 smokers (included 254 non‐attenders); 63% F, av age 42, 46% smoked > 20 cpd Therapists: trained doctors, nurses or psychologists | |
| Interventions | Factorial design with NRT (21 mg or 14 mg patch for 8 weeks including tapering) or no NRT and 5 levels of behavioural support collapsed into 3 for analysis. Arms without NRT did not contribute to this review. 1. Single 20‐min session ‐ classified as brief intervention control in meta‐analysis 2. Cognitive behavioural, 1 or 2 weekly x 1 hour sessions 3. As 2, with 3 or 4 weekly sessions. Maintenance or recycling sessions provided to all groups at 3, 6, 12 months | |
| Outcomes | Abstinence at 12 months (7‐day PP) Validation: none | |
| Source of Funding/CoI | ||
| Notes | 3 vs 1 in patch condition only in primary analysis. Also contributed to review of combined interventions (Stead 2016) | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised, stratified by age & sex, by independent specialist |
| Allocation concealment (selection bias) | Low risk | Trial administrators blind |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only and differential levels of support between arms |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Number lost to follow‐up not provided. Non‐participants and losses to follow‐up included as smokers |
Patten 2017.
| Methods | Setting: USA, YMCA and worksite fitness centres Recruitment: by provider referrals and flyers posted in the clinics, and radio and newspaper advertisements. Willing to quit |
|
| Participants | 30 participants, 100% female, average age: control: 38.0 ± 11.0; intervention: 37.0 ± 10.0, average cigs/day: ≥ 10 Therapists: certified wellness coaches with a master's degree in clinical psychology or bachelor's degree in health education |
|
| Interventions | Pharmacotherapy: 4‐week supply of nicotine patches at weeks 2 and 6 Intervention: exercise counselling delivered while the participant was engaged in exercise. The individual‐based counselling included social cognitive theory–based assessment and problem‐solving of exercise barriers, reinforcement (shaping) of exercise, and methods to enhance exercise self‐efficacy, using a motivational interviewing counselling style. Total contact time: 36 X 30‐ to 40‐minute sessions = 1080 minutes Control: health education. Individual‐based sessions, lectures, handouts, films, and discussions covered various women's health and lifestyle issues. Total contact time: 36 X 30‐ to 40‐minute sessions = 1080 minutes |
|
| Outcomes | Abstinence: 7‐day point prevalence at 12 weeks and 6 months Validation: saliva cotinine (abstinent if < 10 ng/mL) |
|
| Source of Funding/CoI | Funding: National Center for Advancing Translational Sciences of the National Institutes of Health No declarations of interest |
|
| Notes | New for 2019 update A small number of participants attended all 36 sessions (n = 3 for intervention and n = 1 for control) |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details reported |
| Allocation concealment (selection bias) | Unclear risk | "[A]llocation to treatment conditions was unknown to the study staff or investigators prior to assignment and participants completed baseline assessments prior to being informed of their allocation to treatment condition. A study coordinator blinded to allocation group conducted all follow‐ups in‐person". However, no description of how allocation was concealed. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Low attrition in each group: 15.6% |
Prapavessis 2016.
| Methods | Setting: Exercise and Health Psychology Laboratory, Canada Recruitment: from local businesses, hospitals, academic institutions and organisations and through advertisements placed in newspapers, radio stations and city buses in London, Ontario. Motivated to quit |
|
| Participants | 409 participants, 100% female, average age: exercise plus smoking maintenance: 41.96 (± 12.70); exercise plus contact control 43.47 (± 14.02); smoking maintenance plus contact control: 43.45 (± 12.22); contact control: 40.36 (± 11.92) Average cigs/day: exercise plus smoking maintenance: 17.04 (± 6.79); exercise plus contact control 16.71 (± 6.96); smoking maintenance plus contact control: 16.88 (± 5.16); contact control: 16.41 (± 6.78) Therapists: trained facilitator |
|
| Interventions | Pharmacotherapy: transdermal NRT after 4 weeks of exercising (10 week programme: 21 mg once daily for weeks 4 to 9, followed by 14 mg once daily for weeks 10 to 11 and 7 mg once daily during weeks 12 to 13) Exercise maintenance + smoking cessation maintenance ‐ 14‐week exercise‐aided smoking cessation programme (33 x 45‐minute sessions) ‐ Weeks 8 to 14: five 25‐minute weekly cognitive behavioural therapy group sessions, for long‐term exercise adherence ‐ Received a set of Brandon’s “Forever Free” booklets after first 14 weeks ‐ After week 14: seven 15‐minute telephone counselling sessions biweekly for the first months + monthly for the next two months + bimonthly for the last 8 months to maintain exercise behaviour ‐ Total contact: 64 sessions, 1985 minutes Exercise maintenance + contact control ‐ 14‐week exercise‐aided smoking cessation programme (33 x 45‐minute sessions) ‐ Weeks 8 to 14: five 25‐minute weekly cognitive behavioural therapy group sessions, for long‐term exercise adherence ‐ After week 14: seven 15‐minute telephone counselling sessions biweekly for the first months + monthly for the next two months + bimonthly for the last 8 months ‐ to maintain exercise behaviour ‐ Total contact: 64 sessions, 1985 minutes Smoking cessation maintenance + contact control ‐ 14‐week exercise programme (33 x 45‐minute sessions) and 10 weeks NRT (starting from week 4) ‐ Weeks 8 to 14: received messages reinforcing women’s health issues ‐ Received a set of Brandon’s 'Forever Free' booklets after first 14 weeks ‐ After week 14: seven 15‐minute telephone counselling sessions biweekly for the first months + monthly for the next two months + bimonthly for the last 8 months ‐ messages reinforcing the Forever Free booklets and/or women’s health issues (e.g. vitamin D intake, oral hygiene, sleep disorders) ‐ Total contact: 59 sessions, 1860 minutes Contact control ‐ 14‐week exercise programme (33 x 45‐minute sessions) and 10 weeks NRT (starting from week 4) ‐ Weeks 8 to 14: received messages reinforcing women’s health issues ‐ After week 14: seven 15‐minute telephone counselling sessions biweekly for the first months + monthly for the next two months + bimonthly for the last 8 months ‐ messages reinforcing the Forever Free booklets and/or women’s health issues (e.g. vitamin D intake, oral hygiene, sleep disorders) ‐ Total contact: 59 sessions, 1860 minutes |
|
| Outcomes | Abstinence: continuous abstinence at 14, 26, and 56 weeks Validation: CO < 6 ppm considered abstinent |
|
| Source of Funding/CoI | Funding: Canadian Cancer Society No declarations of interest |
|
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | The project manager for trial used numbered containers to implement the random allocation sequence, and the sequence was concealed until interventions were assigned. However, the method of concealment was not specified. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 54.8% of participants lost to follow‐up, but attrition similar between groups |
Reid 1999.
| Methods | Setting: community, Canada Recruitment: volunteers | |
| Participants | 396 smokers interested in quitting within 30 days, smoking ≥ 15 cpd; 48% F, av age 38, av cpd 23 to 24 | |
| Interventions | Pharmacotherapy: NRT; patch (15 mg x 8 wks, 10 mg x 2 weeks, 5 mg x 2 weeks) free 1. Physician advice (3 x 15‐min, 2 weeks before, 4 weeks, 12 weeks after quit date) 2. As 1, plus telephone calls from nurse counsellors, x 3 at 2, 6, 13 weeks |
|
| Outcomes | Abstinence at 12 m (PP) Validation: CO, but self‐reported rates reported. Only 1 disconfirmation | |
| Source of Funding/CoI | National Cancer Institute of Canada with funds from the Canadian Cancer Society Nicotine replacement therapy was provided at no cost by McNeil Consumer Products. "The University of Ottawa Heart Institute Research Corporation has a contract with Johnson & Johnson–Merck Consumer Pharmaceuticals to manage the 'Stop Smoking Now!' telephone counselling service offered to users of Nicotrol NRT. The authors received a grant from Johnson & Johnson–Merck to conduct a pilot study before the clinical trial; no payment was received from the company for the clinical trial or its analysis and write‐up." | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised using table of random numbers, stratified by sex and nicotine dependence |
| Allocation concealment (selection bias) | Unclear risk | Concealment unclear but physician blind to allocation |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 84% intervention, 86% control, followed up at 12 m |
Rohsenow 2014.
| Methods | Setting: residential substance abuse treatment programme, USA Recruitment: research therapist assessed patients for eligibility |
|
| Participants | 165 alcoholic smokers (≥ 10 cpd for 6 m), 60% M, av age 34, av cpd 21 Therapists: research therapists |
|
| Interventions | Pharmacotherapy: NRT; patch preferred, mostly used for 2‐3 months 1. Brief advice ˜15 mins, assessed smoking rate and interest in quitting, ± 2 x 5 to 15‐min boosters at 7 & 30 days 2. Motivational interviewing, 45 min, ± 2 x 5 to 15‐min boosters at 7 & 30 days |
|
| Outcomes | Abstinence at 12 months (7‐day PP) Validation: CO < 10 ppm |
|
| Source of Funding/CoI | National Institute of Alcohol Abuse and Alcoholism, United States Department of Veterans Affairs. No declarations of interest | |
| Notes | Booster and no‐booster conditions combined in analyses. Only 51% used NRT during the first month, 34% during the subsequent 2 months | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Random numbers table |
| Allocation concealment (selection bias) | Low risk | Assignment in sealed envelope opened just before the first treatment session |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Overall 32% lost to follow‐up; MI 35%, (28/80 including 1 death), BA 29% (25/85 including 3 deaths) |
Rovina 2009.
| Methods | Setting: smoking cessation clinic, Greece Recruitment: clinic attenders invited to participate | |
| Participants | 205 smokers | |
| Interventions | Pharmacotherapy: bupropion 300 mg/day for 19 weeks 1. Control: 15 mins physician counselling 2. Nonspecific group therapy (NSGT), 1‐hour weekly for 1 month, then every 3 weeks until 19 weeks 3. Cognitive behavioral group therapy (CBGT), same schedule 4. CBGT without bupropion ‐ not used in review |
|
| Outcomes | Abstinence at 12 months after end of treatment (continuous) Validation: CO ≤ 10 ppm |
|
| Source of Funding/CoI | No source of funding reported. Authors declared no conflicts of interest. | |
| Notes | 2 & 3 vs 1 in primary analysis, same intensity | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, method not stated, 3:1:1:1 ratio |
| Allocation concealment (selection bias) | Unclear risk | No details reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 90% followed up at 12 months |
Schlam 2016.
| Methods | Setting: USA, primary care clinics Recruitment: from primary care clinics, participants willing to quit |
|
| Participants | 544 participants, 59% female, average age: 46.2 ± 12.8, average cigs/day: 18.6 ± 8.8 Therapists: bachelor's level study staff supervised a licensed clinical psychologist |
|
| Interventions | Pharmacotherapy: 8 weeks OR 26 weeks of nicotine patch plus nicotine gum (factorial design) Intervention: 4 sessions of face‐to‐face counselling plus 8 sessions of telephone counselling Control: 4 sessions of face‐to‐face counselling |
|
| Outcomes | Abstinence: 7‐day point prevalence abstinence at 6 and 12 months Validation: none |
|
| Source of Funding/CoI | National Cancer Institute, Wisconsin Partnership Program, and Department of Veterans Affairs. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Low risk | Staff could not view the allocation sequence. The database did not reveal participants' treatment condition to staff until participants' eligibility was confirmed. Participants did not know treatment allocation until they provided consent. |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Quote: "The percentage of participants missing abstinence outcome data was 20.4% at Week 26 and 30.0% at Week 52, with no differences observed in missingness across the two levels (on vs. off) of any of the factors." No further details provided |
Schmitz 2007a.
| Methods | Setting: outpatient treatment research clinic, Department of Psychiatry and Behavioral Sciences Substance Abuse Research Center, USA Recruitment: by local radio, television and print adverts. Motivated to quit |
|
| Participants | 154 participants (78 in 2 groups receiving pharmacotherapy), 100% female, average age: 47.8 ± 9.3, average cigs/day: 21.4 ± 9.1 Therapists: a therapist and co‐therapist pair; four female, master's level therapists were trained on each therapy manual and supervised weekly by a doctoral‐level clinical psychologist |
|
| Interventions | Pharmacotherapy: 6 weeks of sustained‐release bupropion (300 mg/day; 150 mg/day for 3 days, followed by 150 mg twice daily) Intervention: 7 x 60‐minute sessions of cognitive behavioural therapy (CBT) Control: 7 x 60‐minute sessions of standard therapy (ST) |
|
| Outcomes | Abstinence: 7‐day point prevalence at 3, 6, 9, and 12 months Validation: CO (abstinent if ≤ 10 ppm) and salivary cotinine (abstinent if ≤ 15 ng/mL) |
|
| Source of Funding/CoI | Funded by National Institute on Drug Abuse. GlaxoSmithKline provided the bupropion. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method of randomisation not specified |
| Allocation concealment (selection bias) | Low risk | Quote: "Investigators and research staff were blind to the randomization codes, which were kept by a faculty member independent of the research and treatment team." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attrition was high, but similar between study arms. Control: 56.8%; intervention: 53.7% |
Simon 2003.
| Methods | Setting: hospital for military veterans, USA Recruitment: inpatients (all diagnoses) invited to participate | |
| Participants | 223 smokers, ≥ 20 cigs in week before admission, contemplation or action stage of change, able to use NRT, av age 55, av cpd 23 | |
| Interventions | Pharmacotherapy: NRT; patches (tailored dose) in hospital and for 8 weeks post‐discharge 1. Intervention: nurse or health educator counselling; 30 to 60 mins initial session. 5 calls at 1, 3 weeks, 1 month, 2 months, 3 months, < 30 min/call & S‐H materials 2. Control: brief counselling (10 mins) + S‐H only |
|
| Outcomes | Abstinence: 7‐day PP at 12 months Validation: saliva cotinine < 15 ng/mL (alternative analysis allowed spousal corroboration) | |
| Source of Funding/CoI | California Tobacco‐Related Disease Research Program. No declarations of interest | |
| Notes | Relative effect similar if spousal corroboration allowed | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Randomised using computer algorithm |
| Allocation concealment (selection bias) | Unclear risk | No details reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Losses to follow‐up (3 intervention, 4 control) included as smokers. Deaths (5 intervention, 9 control) excluded from denominator |
Smith 2001.
| Methods | Setting: clinic, USA Recruitment: community volunteers | |
| Participants | 677 smokers (> 10/day) attempted to quit for 1 week; 57% F, av age 42; av cpd 25 | |
| Interventions | Pharmacotherapy: NRT, patches for 8 wks. All participants had attended 3 brief (5 to 10‐min) individual counselling sessions pre‐quit, quit day and 8 days post‐TQD & NCI booklet 'Clearing The Air'. 1. Cognitive behavioural skills training, x 6 from 1 week post‐TQD, incl managing negative affect, homework, manual 2. Motivational interviewing, supportive group counselling, x 6 from 1 week post‐TQD. No homework or manual 3. No further intervention | |
| Outcomes | Abstinence at 12 months (7‐day PP) Validation: CO < 10 ppm | |
| Source of Funding/CoI | National Institute on Drug Abuse. Lederle Laboratories supplied the nicotine patches. No declarations of interest | |
| Notes | Marginal to include as the counselling was intended for relapse prevention. 1 vs 3 in primary analysis. Including 2 did not alter findings; 17.6% quit in 1, 18.8% in 2. No evidence found for hypothesised differences in relative efficacy for smokers at high or low risk of relapse. High‐risk smokers expected to do better with motivational intervention |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised 1 wk after TQD, stratified by ± any smoking post‐TQD. Method not stated |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Number lost to follow‐up not reported, all missing included as smokers |
Smith 2013a.
| Methods | Setting: quitline, USA Recruitment: adult smokers willing to quit who called the Wisconsin Tobacco Quit Line |
|
| Participants | 987 participants, 57.6% female, average age: 41.9 ± 13, average cigs/day: 20.7 ± 9.6 Therapists: trained cessation counsellors |
|
| Interventions | Pharmacotherapy: 2 or 6 weeks of NRT (nicotine patch only vs patch plus nicotine gum) (factorial design) Intervention: 4 telephone counselling sessions including medication adherence counselling Control: 4 telephone counselling sessions |
|
| Outcomes | Abstinence: 7‐day point prevalence at 2, 6, and 12 weeks, and at 6 months Validation: none |
|
| Source of Funding/CoI | National Cancer Institute. Authors declared potential conflicts of interest. | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Allocation computer‐randomised |
| Allocation concealment (selection bias) | Unclear risk | No detail reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Self‐report only but similar amounts of contact between groups |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Attrition low and similar between groups. Intervention: 24.9%, control: 21.6% |
Smith 2014.
| Methods | Setting: Menominee Tribal Clinic (primary care centre), USA Recruitment: all participants were receiving health care at the Menominee Tribal Clinic and were motivated to quit smoking. |
|
| Participants | 103 participants, 62.1% female, average age: 39.8 (SD 13.1), average cigs/day: 14.4 (SD 7.9) Therapists: a study coordinator who was an enrolled member of the Menominee Tribe and trained as a counsellor |
|
| Interventions | Pharmacotherapy: 12 weeks of varenicline Intervention: 5 x face‐to‐face culturally tailored counselling sessions, duration not reported Control: 5 x face‐to‐face standard counselling sessions, duration not reported |
|
| Outcomes | Abstinence: 7‐day point prevalence abstinence at weeks 1, 3, and 7, and at 3 and 6 months Validation: CO < 10 ppm |
|
| Source of Funding/CoI | Wisconsin Partnership Program, the Spirit of Eagles Community Network Program, the University of Wisconsin Carbone Cancer Center, and the University of Wisconsin Center for Tobacco Research and Intervention. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No detail given |
| Allocation concealment (selection bias) | Unclear risk | No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Attrition rate high and differed between study arms: intervention: 47.2%; control: 66.0% |
Solomon 2000.
| Methods | Setting: community, USA Recruitment: volunteers for free nicotine patch trial | |
| Participants | 214 female smokers, > 4 cpd, intending to quit in next 2 weeks; av age 33, av cpd 24 | |
| Interventions | Pharmacotherapy: NRT; free nicotine patch (dose based on smoking level) for up to 10 weeks, after 1 m contingent on abstinence 1. Access to Nicoderm support line 2. As 1. and proactive telephone counselling from female ex‐smoker, 7 hours training. Up to 12 calls for up to 3 months, starting pre‐quit, quit day, day 4, average 7 |
|
| Outcomes | Abstinence at 6 months (multiple PP; 7 days at 3 months & 6 months) Validation: CO ≤ 8 ppm. 7% to 12% disconfirmation rate. Participants who did not provide samples remained classified as quitters. | |
| Source of Funding/CoI | Vermont Department of Health (part). SmithKline Beecham provided nicotine patches. No declarations of interest | |
| Notes | Intervention participants received on average 7 calls of 9 mins. Classified in 4 to 8 subgroup analysis. 95% received at least 1 call. Participants could call Nicoderm support line, 21% of control vs 8% of intervention did so. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, method not described |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Approximately 73% followed up in each group |
Solomon 2005.
| Methods | Setting: community, USA Recruitment: volunteers for free nicotine patch trial | |
| Participants | 330 female smokers > 4 cpd, intending to quit in next 2 weeks; av age 34, av cpd 24 | |
| Interventions | Pharmacotherapy: NRT; free nicotine patch (dose based on smoking level) for up to 10 weeks, 2nd & 3rd prescriptions dependent on reporting abstinence 1. No additional support 2. Proactive telephone counselling from female ex‐smoker, 8 hrs training. Calls for up to 4 months, starting pre‐quit, quit day, day 4 |
|
| Outcomes | Abstinence at 6 m (30 days at 3 months & 6 months) Validation: none | |
| Source of Funding/CoI | Vermont Department of Health. SmithKline Beecham provided nicotine patches. No declarations of interest | |
| Notes | Similar to Solomon 2000 with more extended telephone contact Average number of calls 8.2, average duration 10 min. Classified in 4 to 8 subgroup analysis | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, method not described |
| Allocation concealment (selection bias) | Unclear risk | No details given |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only and differential amounts of contact between groups |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 87% response in both conditions at 6 m |
Stanton 2015.
| Methods | Setting: immunology clinics, USA Recruitment: adult smokers who have been diagnosed with HIV and identified themselves as Latino/Hispanic. Not selected for motivation to quit |
|
| Participants | 302 participants, 36% female, average age: 45, average cigs/day: not reported but stated 50% of the participants were heavy (> 10 cigarettes per day) smokers Therapists: 10 health educators who were at least Masters level professionals or had equivalent years of clinical research experience |
|
| Interventions | Pharmacotherapy: 8 weeks of nicotine patches Intervention: self‐help and culturally sensitive print materials and videos, tailored behavioural counselling, two in‐person sessions, two additional in‐person sessions focused on tailored relapse prevention, one phone call on the quit date, two 10‐minute booster phone calls, option to bring a social support buddy to attend all sessions Control: self‐help print materials, two in‐person sessions, one phone call on the quit date |
|
| Outcomes | Abstinence: 7‐day point prevalence at 3, 6 and 12 months Validation: exhaled carbon monoxide level < 10 ppm |
|
| Source of Funding/CoI | National Institute on Drug Abuse, National Cancer Institute, National Institute of Allergy and Infectious Diseases, Lifespan/Tufts/Brown Center for AIDS Research, Clinical Core of the Center for AIDS Research at the Albert Einstein College of Medicine and Montefiore Medical Center funded by the National Institutes of Health. Authors declared no conflicts of interest. | |
| Notes | New for 2019 update Not included in analysis 1.3 because durations of sessions were not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No details provided |
| Allocation concealment (selection bias) | Unclear risk | No details provided |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Similar follow‐up rates (control 67%; intervention 60%) |
Stein 2006.
| Methods | Setting: 5 methadone maintenance treatment programme centres, USA Recruitment: smokers routinely attending maintenance clinic. Willingness to quit not required | |
| Participants | 383 methadone‐maintained adult smokers. 53% M, av age 40, av cpd 27 | |
| Interventions | Pharmacotherapy: NRT; all participants willing to make quit attempt offered patches (8 to 12 weeks, dose and duration tailored to smoking rate) 1. Motivational interview‐based tailored intervention: up to 3 visits from study counsellor, i.e. 1 x 30‐min + 15 to 30‐min quit‐date session, + follow‐up relapse prevention session. Those not ready to quit only received 2 sessions. 2. Control: Brief advice using NCI's 4As model (< 3 mins), + S‐H materials. Up to 2 visits, i.e. baseline and quit date (if set) | |
| Outcomes | Abstinence at 6 months (PP) Validation: CO < 8 ppm | |
| Source of Funding/CoI | National Cancer Institute. GlaxoSmithKline provided nicotine patches. No declarations of interest | |
| Notes | Included since most participants in both conditions did make quit attempts and received NRT; 81% intervention and 80% control | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, methods not stated |
| Allocation concealment (selection bias) | Unclear risk | No details reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Approx 82% followed up in both groups at 6 months |
Strong 2009.
| Methods | Setting: USA Recruitment: via newspaper, radio, and television advertisements |
|
| Participants | 524 participants, 47.5% female, average age: 44.27 ± 10.38, average cigs/day: 24.6 ± 10 Therapists: doctoral level therapist |
|
| Interventions | Pharmacotherapy: 12 weeks of bupropion, initiated during the second week of treatment, 2 weeks prior to quit day Intervention: 12 x 120‐minute sessions of standard cessation group counselling with CBT for depression Control: 12 x 120‐minute sessions of standard cessation group counselling |
|
| Outcomes | Abstinence: 7‐day point prevalence abstinence at 2, 6, and 12 months Validation: CO (abstinent if ≤ 10 ppm) and salivary cotinine (abstinent if ≤ 15 ng/mL) |
|
| Source of Funding/CoI | Funding: National Institutes of Health Declarations of interest: one of the authors served on the Pfizer Speakers Bureau and a Pfizer Scientific Advisory Board. |
|
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No detail given |
| Allocation concealment (selection bias) | Unclear risk | No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Study reported "8 smokers did not provide any follow‐up data". However, this was only for the 12‐week follow‐up. |
Swan 2003.
| Methods | Setting: HMO, USA Recruitment: volunteers from Group Health Co‐op membership | |
| Participants | 1524 smokers ≥ 10 cpd; 57% F, av age 45, av cpd 23, 44% history of depression | |
| Interventions | Pharmacotherapy: randomised to bupropion 300 mg/day or 150 mg/day 1. Free & Clear proactive telephone counselling (4 brief calls), access to quitline and S‐H materials 2. Zyban Advantage Program (ZAP); tailored S‐H materials, single telephone call after TQD, access to Zyban support line | |
| Outcomes | Abstinence at 12 m (7‐day PP) Validation: none | |
| Source of Funding/CoI | National Cancer Institute. "The authors have no relevant financial interest in this article, and received no financial support or medication from GlaxoSmithKline". | |
| Notes | Prescription was mailed. No face‐to‐face contact during enrolment or prescription. Estimated as 31 to 90 minutes contact. No dose/behavioural treatment interaction at 12 m, bupropion arms collapsed |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Open‐label randomized trial...The computer code for the procedure calculated probabilities of group assignment that were dynamically modified based on the number of members in each group so that final group sizes were equal. No restrictions such as stratification or blocking were used as part of the randomization process." |
| Allocation concealment (selection bias) | Low risk | Procedure built into study database |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only and differential levels of support |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 83% intervention, 88% control followed up at 12m |
Swan 2010.
| Methods | Setting: HMO (Group Health), Seattle, WA, USA Recruitment: Group Health members contacted by phone & mail from Free & Clear |
|
| Participants | 1202 smokers (≥ 10 cpd); 67% F, av age 47, av cpd 22 | |
| Interventions | Pharmacotherapy: varenicline for 12 weeks (1 mg x 2/day, titrated 1st week). All received 5 to 10‐min orientation call, printed Quit Guides and access to a free support line for ad hoc calls. 1. Web‐based counselling: access to online programme, including quit plan, online library, quit calendar, cost calculator, progress tracker, email links to friends and family and discussion forums 2. Proactive telephone‐based counselling: Free & Clear Quit for Life programme. Up to 5 'brief' one‐to‐one phone sessions initiated by F&C counsellor. Timed for convenience and at relapse‐sensitive stages. Used MI techniques 3. Combination: proactive calls + web access; counsellor could view info entered online. Participants encouraged to use website for additional info and social support, and to track cpd. Counsellors could view quit status, last log‐in and last use of discussion forum. | |
| Outcomes | Abstinence at 6 m (PP) Validation: none | |
| Source of Funding/CoI | National Cancer Institute. "Varenicline and nominal support for recruiting participants was provided by Pfızer, Inc. Neither entity [NCI or Pfizer] had any role in the study design; the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the report for publication." Authors declared potential conflicts of interest. | |
| Notes | 3 vs 1 in main analysis, 2 & 3 vs 1 had little effect on result. 60‐min contact on average for 3 64% were no longer taking varenicline at 3 months, but no between‐group differences in non‐compliance or reasons for stopping |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "Group assignment was randomly allocated using an automated algorithm built into the study database". |
| Allocation concealment (selection bias) | Unclear risk | Not stated |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only and differential levels of support |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Participants lost to follow‐up counted as smokers in ITT analysis; equal losses between groups (103 web, 107 phone, 100 web + phone) |
Tonnesen 2006.
| Methods | Setting: 7 chest clinics, Denmark Recruitment: outpatient attender | |
| Participants | 370 smokers of > 1 cpd with COPD (185 in relevant arms); 52% F, av age 61, av cpd 20 Therapists: 20 nurses with cessation experience, trained to support medication use and provide standardised counselling |
|
| Interventions | Pharmacotherapy: NRT; sublingual. Factorial trial included placebo tablets; only active treatment groups used in this review. 1. High support: 7 x 20 to 30‐min clinic visits (0, 2, 4, 8, 12 wks, 6 m, 12 m) & 5 x 10‐min phone calls (1, 6, 10 wks, 4½ m, 9 m), total contact time 4½ hrs 2. Low support: 4 clinic visits (0, 2 wks, 6 m, 12 m) & 6 phone calls (1, 4, 6, 9, 12 wks, 9 m), total time 2½ hrs | |
| Outcomes | Sustained abstinence at 12 m (validated at all visits from wk 2, PP also reported) Validation: CO < 10 ppm | |
| Source of Funding/CoI | "The Danish Medical Research Council provided the major grant for this study ($375,000). Pfizer Consumer Healthcare, Sweden, supplied the study drugs used in the trial and provided grant support ($25,000)." First author declared potential conflicts of interest. | |
| Notes | Also contributed to review of combined therapy review (Stead 2016), using placebo low‐support arm as control. Therapists were not full‐time specialist counsellors. Using PP outcome did not alter effect. Only contacts before 12 wks counted for classification of intensity. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Block randomisation list at each centre |
| Allocation concealment (selection bias) | Unclear risk | Allocation process not described |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | 42/185 (23%) of active NRT participants not followed up at 12 m and counted as smokers. Not reported by support condition. Of those who were followed up at 12 m, 52% had withdrawn from study treatment. Authors stated: "One potential bias may have been the large early dropout of failures from the study. Consequently, these patients were not exposed to the possible effect of more intensive support." |
Van Rossem 2017.
| Methods | Setting: Netherlands, primary care Recruitment: by practice assistants, GPs, and practice nurses and via a leaflet displayed in the waiting room |
|
| Participants | 311 participants, 52.9% female, average age: 48 ± 13.2, average cigs/day: 19 ± 8.1 Therapists: practice nurse or general practitioner |
|
| Interventions | Pharmacotherapy: 12‐week course of varenicline Intervention: intensive counselling with practice nurse. 3 face‐to‐face plus 7 telephone sessions Control: brief advice with GP |
|
| Outcomes | Abstinence: prolonged abstinence (maximum of five cigarettes after a grace period of 9 weeks) at weeks 9 and 26, and at 12 months Validation: CO < 10 ppm |
|
| Source of Funding/CoI | Eindhoven Corporation of Primary Health Care Centres, Pfizer, and Research School CPHRI. Authors declared potential conflicts of interest. | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Allocation randomised by computer |
| Allocation concealment (selection bias) | Low risk | Quote: "The computer disclosed the allocation once during a phone call by a member of the research team with the assistants of the health‐care centre, who then contacted the patient to schedule an appointment with the GP or PN." |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rates similar. Intervention: 18.6%, control: 25.8% |
Vander Weg 2016.
| Methods | Setting: quitline, USA Recruitment: by mail to rural veteran daily cigarette smokers aged ≥ 18 years. Selected for motivation to quit |
|
| Participants | 63 participants Therapists: doctoral‐level social worker with expertise in substance abuse and a masters‐level counsellor |
|
| Interventions | Pharmacotherapy: free of charge 12‐week supply of pharmacotherapy mailed to the participants. Medication options included several forms of nicotine replacement therapy (patch, gum, lozenge), bupropion and varenicline. Combinatoin therapy was also available, as appropriate. 1. Quitline referral 2. Tailored tobacco intervention: 6 weekly sessions over phone each lasting 20 to 30 minutes |
|
| Outcomes | 7‐day point prevalence abstinence at 12 weeks and 6 months after quit‐date Validation: none |
|
| Source of Funding/CoI | Department of Veterans Affairs Office of Rural Health. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Computer‐generated |
| Allocation concealment (selection bias) | Unclear risk | Insufficient details provided |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Self‐report only and differential levels of support |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Tailored tobacco intervention 25.8%; quitline referral 12.5% |
Vidrine 2016.
| Methods | Setting: USA Recruitment: from the Houston metropolitan area via local print media. Motivated to quit |
|
| Participants | 412 participants, 54.9% female, average age: 48.7 ± 11.9, average cigs/day: 19.9 ± 10.1 Therapists: two master's level therapists |
|
| Interventions | Pharmacotherapy: 6 weeks of NRT patches Mindfulness‐based addiction treatment (MBAT): 8 x 120‐minute in‐person group counselling sessions Cognitive behavioural treatment (CBT): 8 x 120‐minute in‐person group counselling sessions Control: 4 x 5‐ to 10‐minute individual counselling sessions |
|
| Outcomes | Abstinence: 7‐day point prevalence abstinence at 4 weeks and 6 months Validation: CO (abstinent if < 6 ppm) and salivary cotinine (abstinent if < 20 ng/mL) |
|
| Source of Funding/CoI | National Institute on Drug Abuse, Centers for Disease Control and Prevention, National Cancer Institute, National Center for Complementary and Integrative Health, and the Oklahoma Tobacco Settlement Endowment Trust. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No detail given |
| Allocation concealment (selection bias) | Unclear risk | No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Dropout rates similar between groups. Control: 35.9%; MBAT: 33.1%; CBT: 34.8% |
Wagner 2016.
| Methods | Setting: USA, community‐based primary health care clinic Recruitment: word of mouth and flyers |
|
| Participants | 400 participants, 58.7% female, average age: 45 ± 10.5, average cigs/day: ≥ 3 Therapists: individual sessions by a nurse practitioner or a physician. Group sessions by a social worker and a nurse practitioner |
|
| Interventions | Pharmacotherapy: NRT (unclear about duration or type) Group counselling: could attend up to 12 sessions but frequency and scheduling determined by clinician according to the standard of care at the healthcare facility. Individual counselling: could attend up to 12 sessions but frequency and scheduling determined by clinician according to the standard of care at the healthcare facility |
|
| Outcomes | Abstinence: planned follow‐up at 1, 2, 3, 4, 5, 6, and 9 months Validation: carbon monoxide |
|
| Source of Funding/CoI | National Institute on Minority Health and Health Disparities, National Institute on Drug Abuse, and Pfizer Inc. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Method not specified |
| Allocation concealment (selection bias) | Unclear risk | Not specified |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | High risk | Quote: "In addition, because of the very low follow‐up rates that could be achieved with this population, in spite of intensive efforts, the data was censored at the end of the 12th week, i.e., at the end of the intervention." |
Warner 2016.
| Methods | Setting: Mayo Clinic Hospitals, USA Recruitment: recruited from Mayo Clinic Hospitals |
|
| Participants | 600 participants Sex: control: 49% female; intervention: 48% female, average age: control: 46.0 (± 14.7); intervention: 46.7 (± 14.9), average cigs/day: control: 14.2 (± 9.6); intervention: 14.6 (± 9.0) Therapists: study personnel |
|
| Interventions | Pharmacotherapy: NRT while hospitalised and a free 2‐week supply of NRT at discharge, with instructions to purchase over‐the‐counter patches if desired Intervention: brief quitline facilitation session designed to overcome cognitive barriers to quitline utilisation. Also given a written brochure and a wallet‐sized 'quit‐card'. If amenable, directly referred to a quitline provider (1 x 5‐minute session) Control: brief advice (1 x 5‐minute session) |
|
| Outcomes | Abstinence: 7‐day point prevalence abstinence at 7 days, 1 month, and 6 months Validation: urine continine < 2 ng/mL |
|
| Source of Funding/CoI | ClearWay Minnesota. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Quote: "randomized using dynamic randomization allocation based on the Mayo Clinic Study Data Management System, a proprietary web application for data entry and management." |
| Allocation concealment (selection bias) | Unclear risk | No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Similar attrition rates. Intervention: 30.3%; control: 26.0% |
Webb Hooper 2017.
| Methods | Setting: USA, university‐based research clinic Recruitment: through advertisements on public transportation, community‐based organisations, street outreach, and word‐of‐mouth. Inclusion criteria included motivation to quit |
|
| Participants | 342 participants, intervention: 39% female; control: 48% female; average age: intervention: 49.48 (± 9.44); control: 49.52 (± 8.73); average cigs/day: intervention:18.20 (± 11.53); control: 17.88 (± 10.03) Therapists: doctoral and masters or bachelors level co‐therapy pairs and supervision by the principal investigator or a co‐investigator |
|
| Interventions | Pharmacotherapy: 8 weeks of nicotine patches, including 4 weeks at 21 mg, 2 weeks at 14 mg, and 2 weeks at 7 mg (doses adjusted for smoking history) Intervention: NRT plus culturally‐specific CBT (9 x 90‐ to 120‐minute sessions) Control: NRT plus standard CBT (9 x 90‐ to 120‐minute sessions) |
|
| Outcomes | Abstinence: 7‐day point prevalence abstinence at 3 and 6 months Validation: saliva cotinine < 7 ng/mL, exhaled CO < 8 ppm |
|
| Source of Funding/CoI | National Cancer Institute of the National Institutes of Health. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No detail given |
| Allocation concealment (selection bias) | Unclear risk | No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Similar attrition rates: culturally‐specific CBT: 15.5%; standard CBT: 19.5% |
Wewers 2017.
| Methods | Setting: USA, community Recruitment: recruited from Ohio Appalachian counties. Inclusion criteria included willingness to participate in study protocol. |
|
| Participants | 707 participants Female: Community Health Worker Face‐to‐Face (CHWF2F): 65.7%; Community Health Worker Quitline (CHWQL): 69.8% Age: • CHWF2F: 18 to 24: 4.5%; 25 to 54: 62.9%; ≥ 55: 32.6% • CHWQL: 18 to 24: 5.4%; 25 to 54: 65.8%; ≥ 55: 28.8% Average cigs/day: CHWF2F: 22.3 (SD 11.7); CHWQL: 20.9 (SD 9.2) Therapists: • CHWF2F: community health worker and a registered nurse employed in the county public health department clinic • CHWQL: community health worker and quitline services provided by trained counsellors from National Jewish Health |
|
| Interventions | Pharmacotherapy: • CHWF2F: a new 21 mg nicotine patch at the start of each visit, beginning on quit‐day and lasting for 8 weeks • CHWQL: up to two mailings of a 4‐week supply of free 21 mg nicotine patches. To receive the second 4‐week supply of free NRT, each participant was required to have completed at least two proactive counselling calls 1. CHWF2F: 7 face‐to‐face 30‐minute sessions with a community health worker 2. CHWQL: 1 face‐to‐face 30‐minute session with a community health worker, followed by up to five proactive telephone counselling sessions, and unlimited reactive calls from the participant, with a quitline |
|
| Outcomes | Abstinence: prolonged abstinence at 3, 6, and 12 months, after a 2‐week post‐quit date grace period Validation: saliva cotinine level < 15 ng/mL, expired air CO level < 8 ppm |
|
| Source of Funding/CoI | National Institutes of Health. No declarations of interest | |
| Notes | New for 2019 update | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | No detail given |
| Allocation concealment (selection bias) | Unclear risk | No detail given |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Similar attrition in study groups. CHWF2F: 14.4%; CHWQL: 14.7% |
Wiggers 2006.
| Methods | Setting: cardiovascular outpatient department, Netherlands Recruitment: patients attending regular consultation; consenting patients referred to nurse practitioner | |
| Participants | 385 smokers (8 deaths excluded from outcomes). 37% F, av age 59, av cpd 21 Therapist: nurse practitioner | |
| Interventions | Pharmacotherapy: NRT; patch (8 wks, dose based on smoking rate) for smokers making a quit attempt. In both groups, participants planning to quit received 8 wks nicotine patch with instruction from nurse 1. "Minimal Intervention Strategy for cardiology patients" (C‐MIS). 15 to 30 mins at baseline, 1 phone call at 2 wks, additional session on request. Assessment of dependency & motivation, barriers; TQD set for motivated participants 2. Usual care without motivational counselling | |
| Outcomes | Abstinence at 12 m (7‐day PP) Validation: Urine or saliva nicotine/cotinine/thiocyanate. Self‐reported smokers also tested; validated rates included smokers with negative biochemical results, so self‐reported non‐smoking used in MA. | |
| Source of Funding/CoI | Netherlands Heart Foundation. Novartis Consumer Health provided nicotine patches 'for prime cost'. | |
| Notes | Participants were referred to nurse practitioner for counselling; not part of usual care. Unclear how many participants used NRT; in a subgroup who responded to a questionnaire (Wiggers Int J Behav Med 2006), 16% did not start patch therapy | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "A computerized balanced randomization programme taking prognostic factors (e.g. clinic attendance, age and gender) into account." |
| Allocation concealment (selection bias) | Low risk | "While patients completed their baseline questionnaire (and signed a written informed consent) nurses randomly assigned ...". Judged low risk as participant data had to be entered |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 89% intervention and 85% control followed up at 12 m. 8 deaths excluded from final denominators |
Williams 2010.
| Methods | Setting: mental health outpatient clinics, USA Recruitment: patients with schizophrenia or schizoaffective disorder, willing to use NRT |
|
| Participants | 100 smokers (> 10 cpd) using an atypical antipsychotic; 16% F, av age ˜46, av cpd 23 Therapists: trained mental health clinicians provided both conditions. |
|
| Interventions | Pharmacotherapy: nicotine patch (21 mg for 16 wks incl tapering) 1. Treatment of Addiction to Nicotine in Schizophrenia (TANS); 24 x 45‐min individual counselling sessions over 26 wks 2. Medical Management (MM); 9 x 20‐min over 26 wks |
|
| Outcomes | Continuous abstinence at 12 m Validation: CO < 10 ppm |
|
| Source of Funding/CoI | National Institute on Drug Abuse. Authors also reported support from Pfizer but unclear how it related to this study; "The authors are also supported in part by grants from the National Institute of Mental Health (JMW); National Institute on Drug Abuse (to MLS); Pfizer, Inc.; and the New Jersey Department of Health and Senior Services, Office of the State Epidemiologist, through funds from New Jersey Comprehensive Tobacco Control Program (JMW, MLS)." | |
| Notes | ||
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | "adaptive urn randomization procedure that accounts for motivation, gender, ethnicity, and heavy versus light smoking status" |
| Allocation concealment (selection bias) | Low risk | Judged that process for randomisation prevented prior knowledge of condition |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 75% followed up at 12 m, authors reported "not different between groups" |
Wu 2009.
| Methods | Setting: research unit for Asian health, NYC, USA Recruitment: via Asian Community Health Coalition member organisations | |
| Participants | Chinese smokers (any smoking in previous wk); 12% F, av age 44, av cpd NS, 25% smoked < 10 cpd, 49% had never attempted to quit | |
| Interventions | Pharmacotherapy: NRT. Patch for 8 wks (could start at any time in 6 m period) 1. Culturally‐tailored counselling in Chinese, 4 x 60‐min & S‐H 2. Health education in Chinese: 4 x 60‐min, including general health, nutrition, exercise & tobacco |
|
| Outcomes | Abstinence at 6 m (PP) Validation: CO < 6 ppm |
|
| Source of Funding/CoI | National Cancer Institute Community Network Program. Authors declared no conflicts of interest. | |
| Notes | Conditions had same contact time, but control did not focus on smoking. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Randomised, method not stated |
| Allocation concealment (selection bias) | Unclear risk | Details not reported |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 10% intervention and 14% control lost to follow‐up at 6 m and counted as smokers in ITT analysis |
Yalcin 2014.
| Methods | Setting: general practice smoking cessation clinic, Turkey Recruitment: smokers motivated to quit within 6 months |
|
| Participants | 350 smokers 50% M, av age 36.22, cpd not reported Therapists: smoking cessation clinic specialists |
|
| Interventions | Pharmacotherapy: NRT (gum or patch), bupropion, or varenicline for 3 m or as long as necessary 1. Control; 8 visits & 1 call; baseline, day 8, 20, 23, 30, 45, 60, 120, 210, ˜150 mins 2. Same as control plus CBT‐oriented anger management and stress control programme, 5 x 90‐min sessions, in 1st month, ˜730 mins total |
|
| Outcomes | Abstinence at 180 days, continuous abstinence (from quit‐day) Validation: CO ≤ 10 ppm |
|
| Source of Funding/CoI | No funding. Authors declared no conflicts of interest. | |
| Notes | Pharmacotherapy was only used if the participant wanted to. | |
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | High risk | Alternated allocation, based on order that they were added to the participant list |
| Allocation concealment (selection bias) | High risk | Not specified whether this randomisation order was known to those enrolling |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Biochemically validated |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | 6.3% lost to follow‐up |
ACS: American Cancer Society ACT: acceptance and commitment therapy av.: average BCT‐S: behavioural couples treatment CBGT: cogntive behavioural group therapy CBT: cognitive behavioural therapy CHWF2F: community health worker face‐to‐face CHWQL: community health worker quitline cigs: cigarettes C‐MIS: "Minimal intervention strategy for cardiology patients" CO: carbon monoxide cpd: cigarettes per day CQ: Committed Quitters programme F: female FAP: functional analytic psychotherapy FC: face‐to‐face counselling F&C: Free & Clear HE: health education HMO: health maintenance organisation hr: hour incl: included ITT: intention‐to‐treat LGBT: lesbian, gay, bisexual, transgender M: male m: month MA: meta‐analysis MBAT: mindfulness‐based addiction treatment MDD: major depressive disorder MI: motivational interviewing mins: minutes NCI: National Cancer Institute NP: nurse practitioners NRT: nicotine replacement therapy NS: not specified NSGT: non‐specific group therapy PI: principal investigator PP: point prevalence abstinence ppm: parts per million RP: relapse prevention SC: smoking cessation SD: standard deviation S‐H: self help TANS: treatment of addiction to nicotine in schizophrenia TC: telephone counselling TQD: target quit date UC: usual care VUMC: Vanderbild University Medical Center vs: versus wk(s): week(s) yr: year ZAP: Zyban advantage programme
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Asfar 2010 | Compared delivery of quitline counselling: counsellor‐ versus participant‐initiated |
| Bastian 2013 | Tested motivational interviewing to promote smoking cessation. Low use of NRT; only 59% of participants requested nicotine patches. Included in Lindson‐Hawley 2015 Cochrane review of motivational interviewing |
| Batra 2010 | Experimental intervention was tailored for at‐risk subgroups, and included recommendation to use combination NRT. Standard treatment control recommended single type of NRT. |
| Bock 2008 | Only participants interested in quitting (17% at baseline) were offered NRT. Main intervention was motivational interviewing. |
| Bonevski 2018 | Pharmacotherapy was only offered to the participants in the intervention arm. |
| Borland 2008 | Pharmacotherapy was only offered to participants interested in quitting; 24% reported use. |
| Brandon 2017 | Only 3 months follow‐up |
| Breland 2014 | Intervention delivered by computer, no personal support. |
| Brown 2007 | Factorial trial of bupropion/placebo and mood management CBT or standard cessation CBT. Both behavioural interventions were intensive, and experimental treatment was specifically devised for people with depression. |
| Buchanan 2004 | Only 3 months follow‐up (42 participants) |
| Carlin‐Menter 2011 | Only 3 months follow‐up. Compared 2 versus 4 counselling callbacks for smokers calling a quitline who received up to 6 weeks of free NRT. |
| Chandrashekar 2015 | Only 12 weeks follow‐up |
| Chouinard 2005 | Pharmacotherapy was only offered to participants interested in quitting; 24% used. |
| Christenhusz 2007 | Pharmacotherapy differed by arm: control arm advised to use pharmacotherapy but had to pay for it; intervention arm provided with bupropion free of charge. |
| Cooney 2007 | Both pharmacotherapy and behavioural components varied by trial arm. |
| Cooper 2004 | Main study results have not been published. |
| Costello 2011 | Only 5 weeks follow‐up. Compared 2 intensities of pharmacist‐led behavioural support for participants using NRT. |
| Cropsey 2017 | Only 12 weeks follow‐up |
| Cummins 2016 | Control group participants may or may not have received NRT. |
| Dezee 2013 | Only 12 weeks follow‐up |
| Emmons 2013 | Compared web‐based versus print formats of smoking cessation intervention. |
| Evins 2007 | Only 12 weeks follow‐up |
| Fang 2006 | Only 3 months follow‐up |
| Garvey 2012a | Both behavioural interventions were of similar intensity, differing only in scheduling of sessions. |
| Hall 1996 | Both behavioural interventions were of similar intensity. |
| Hall 2004 | Factorial trial crossing extended behavioural support (CBT) with medical management only, and nortriptyline or placebo, for 1 year, as adjuncts to nicotine patch and 5 group counselling sessions. Placebo arms could have been compared, but no other trials confounded behavioural support with placebo, and the support common to all conditions was also much more intensive than in other trials. |
| Hall 2011 | Similar design to Hall 2004: factorial trial crossing extended behavioural support (CBT) with medical management only, and bupropion or placebo, as adjunct to nicotine patch and 5 group support sessions over 11 weeks. As with Hall 2004, placebo arms could have been compared, but no other trials confounded behavioural support with placebo, and the support common to all conditions was also much more intensive than in other trials. |
| Hegaard 2003 | Study population pregnant smokers, not eligible |
| Ingersoll 2009 | Only 3 months follow‐up. Test of motivational interviewing as adjunct to nicotine patch therapy for HIV+ smokers |
| Japuntich 2006 | Intervention was access to an internet site; no person‐to‐person behavioural support |
| Joseph 2004 | Intervention and control did not differ on use of pharmacotherapy or intensity of behavioural support. Test of timing in relation to alcohol dependence treatment |
| Joyce 2008 | Test of reimbursement for pharmacotherapy and counselling |
| Kim 2012 | Pilot study of a culturally‐tailored intervention for Koreans, with only 30 participants |
| Kinnunen 2008 | Main intervention was exercise, not eligible for this review. Recruitment to the standard care control was halted early. |
| Klesges 2015 | Compared proactive and reactive telephone counselling. Both conditions could get same intensity of counselling. |
| Kotz 2009 | Tested a specific behavioural intervention: feedback of biomedical information. |
| Levine 2010 | Behavioural interventions were matched for intensity; specifically tested a weight‐related intervention. |
| Marshall 1985 | Only offer of nicotine gum |
| McCarthy 2016 | Only 10 weeks follow‐up |
| Moadel 2012 | Only 3 months follow‐up |
| Mochizuki 2004 | Only 3 months follow‐up. Small study of pharmacist advice as adjunct to NRT |
| NCT00781599 | Only 3 months follow‐up |
| Nilsson 1996 | Only 4 months follow‐up. Intervention was offer of group support and free NRT. |
| Nollen 2007 | No difference in intensity of behavioural support |
| Nollen 2011 | Only 3 months follow‐up. Study of an intervention to increase adherence to varenicline |
| Okuyemi 2006 | All participants received same intensity of motivational interviewing, group sessions and offer of NRT. Tested different targets for motivational interviewing. |
| Pakhale 2015 | Pharmacotherapy not offered in same way to both arms |
| Peckham 2015 | Pharmacotherapy not offered in same way to both arms |
| Ramon 2013 | Not all participants were offered pharmacotherapy. |
| Reid 2007 | Intervention participants did not automatically receive additional behavioural support; intervention consisted of automated telephone calls to identify participants at risk of relapse. Only this subgroup then received further counselling. |
| Schnoll 2005 | Only 3 months follow‐up, behavioural interventions similar in intensity as adjuncts to nicotine patch |
| Severson 2015 | Participants were smokeless tobacco users not smokers |
| Shiffman 2000 | Only 12 weeks follow‐up from start of treatment. Study of computer‐tailored materials as adjunct to nicotine gum |
| Shiffman 2001 | Only 12 weeks follow‐up from start of treatment. Study of computer‐tailored materials as adjunct to nicotine patch |
| Sorensen 2003 | Short follow‐up (preoperative period) |
| Strecher 2005 | Only 12 weeks follow‐up from start of treatment. No personal behavioural support, study of web‐based tailored materials as adjunct to nicotine patch |
| Velicer 2006 | Intervention was automated telephone counselling messages, no personal contact. |
| Vial 2002 | Compared intervention from 2 different types of pharmacist, not between different intensities of support. |
| Ward 2001 | Compared 2 group‐based behavioural interventions similar in intensity as adjuncts to nicotine patch, see Stead 2017. |
| Wilson 1988 | Use of nicotine gum was substantially different between the relevant arms of the trial, and the intervention condition was also a test of the impact of training. |
| Wolfenden 2005 | Only 3 month follow‐up. Test of multifaceted intervention including offer of NRT at preoperative clinics |
| Yu 2006 | Only 12 weeks follow‐up from start of treatment |
| Zwar 2015 | Trial of methods of delivery of care rather than of intensity of support |
CBT: cognitive behavioural therapy NRT: nicotine replacement therapy
Characteristics of ongoing studies [ordered by study ID]
ACTRN12614000876695.
| Trial name or title | Improving radiotherapy outcomes in head and neck cancer patients: a preliminary comparison of smoking cessation intervention ‘Varenicline plus support’ with ‘treatment as usual’ |
| Methods | Study design: randomised controlled trial Setting: New South Wales, Australia Recruitment: potential participants identified in the month preceding the new patient clinic using treatment planning software |
| Participants | Target: 40 |
| Interventions | Pharmacotherapy: varenicline for 3 months course initially then an offer of an additional 3 months course depending on the successful completion of the first course 1. Treatment as usual: standard New South Wales Health Tobacco assessment and smoking cessation advice 2. Multicomponent smoking cessation programme including 10 behaviour change sessions with a psychologist |
| Outcomes | Abstinence at 6 months post‐radiotherapy Validation: not specified |
| Starting date | August 2014 |
| Contact information | Benjamin Britton, University of Newcastle |
| Notes | Stopped due to a higher than anticipated number of ineligible patients and time‐limited funding Only the intervention group was offered varenicline. |
Asfar 2018.
| Trial name or title | A cluster‐randomised pilot trial of a tailored worksite smoking cessation intervention targeting Hispanic/Latino construction workers: intervention development and research design |
| Methods | Study design: cluster‐randomised pilot trial Setting: South Florida, USA Recruitment: identification of potential participants through research partnership with local construction companies |
| Participants | Target: 126 Hispanic/Latino smokers (63 per arm) |
| Interventions | Pharmacotherapy: 8 weeks of free NRT (6 weeks supply provided by the study team and 2 weeks by the quitline) 1. Enhanced care: single face‐to‐face behavioural group counselling session delivered at the food truck + two brief follow‐up counselling phone calls + usual care 2. Usual care: fax referral to the Florida quitline (quitline to provide four brief counselling sessions by phone) + informative handout about the quitline |
| Outcomes | Abstinence at 6 months Validation: saliva cotinine < 15 ng/mL |
| Starting date | April 2017 |
| Contact information | David Lee, University of Miami |
| Notes |
Choi 2011.
| Trial name or title | Culturally‐tailored smoking cessation for American Indians |
| Methods | Study design: RCT (cluster randomisation) Setting: American Indian and Alaskan Native smokers in 2 sites (Kansas and Oklahoma) Participants will form temporal clusters in recruiting order, and then pairs of clusters will be assigned to the groups using randomised permuted blocks based on computer‐generated random numbers. |
| Participants | 58 groups totaling 448 participants |
| Interventions | Pharmacotherapy: choice of free pharmacotherapy, including Chantix®, Zyban®, Nicotine Replacement Therapy (NRT, patches, gum, or lozenges), or a combination of the latter 2 1. Non‐native tailored intervention using American Cancer Society guide to educate about the risks of smoking + assisting with planning for cessation (included pharmacotherapy) 2. “All Nations Breath of Life” (ANBL) programme (culturally‐tailored) = group support sessions, telephone motivational interviewing, culturally‐tailored educational curriculum, pharmacotherapy, and participants' incentives |
| Outcomes | Abstinence: continuous abstinence Validation: salivary cotinine analysis for verification |
| Starting date | September 2010 |
| Contact information | Won Choi, University of Kansas |
| Notes | Both usual care and intervention received intensive behaviour counselling; however the types of counselling were different. The study aimed to assess culturally‐tailored smoking cessation interventions among American Indian populations. ‐ study completed in January 2015 |
Cummins 2012.
| Trial name or title | Nicotine patches and quitline counselling to help hospitalised smokers stay quit: study protocol for a randomised controlled trial |
| Methods | Setting: hospitalised patients recruited from 2 healthcare systems in San Diego county Recruitment: motivation: respiratory therapists/research recruiters at bedside; interested in quitting, selected if they were motivated |
| Participants | 1640 participants |
| Interventions | Pharmacotherapy: 6 to 10 cpd = 6 weeks 14 mg + 2 weeks 7 mg; ≥ 11 cpd = 4 weeks 21 mg, 2 weeks 14 mg & 2 weeks 7 mg nicotine patches 1. Usual care ‐ brief bedside intervention (< 10 minutes), educational materials & state quitline number provided 2. Just nicotine patches (8 weeks, step‐down programme) 3. Proactive telephone counselling provided by the state quitline after discharge 4. Both patch + telephone counselling |
| Outcomes | Abstinence at 6 months ‐ 30‐day PP Validation: cotinine‐validated smoking status |
| Starting date | Date of registration: February 1, 2011; date of first participant: August 3, 2011 |
| Contact information | Shu‐Hong Zhu, University of California San Diego |
| Notes | Analysis will use 4 vs 2 |
Garvey 2012b.
| Trial name or title | Duration of behavioural counselling treatment needed to optimise smoking abstinence |
| Methods | RCT |
| Participants | 450 |
| Interventions | Pharmacotherapy: 1. 3 months of counselling 2. 6 months of counselling 3. 12 months of counselling |
| Outcomes | Abstinence: 1 year Validation: not specified |
| Starting date | February 2008 |
| Contact information | arthur_garvey@hms.harvard.edu |
| Notes | There are no study results yet. |
Kim 2017.
| Trial name or title | A pilot study of a smoking cessation intervention for women living with HIV: study protocol |
| Methods | Study design: randomised controlled trial Setting: USA Recruitment: convenience sampling. To be recruited offline and online across the nation |
| Participants | 50 women diagnosed with HIV and residing in a community |
| Interventions | Pharmacotherapy: eight weeks of nicotine patches Eight weekly individualised counselling sessions of 30‐minute cognitive behavioural therapy via: 1. telephone video call 2. telephone voice call |
| Outcomes | Abstinence at 6 months Validation: salivary cotinine < 10ng/mL |
| Starting date | Protocol published in February 2017 |
| Contact information | Sun S Kim, University of Massachusetts Boston |
| Notes |
NCT00851357.
| Trial name or title | Telephone counselling and the distribution of nicotine patches to smokers |
| Methods | Study design: randomised controlled trial (factorial) Setting: University of California, California Smokers’ Helpline, USA Recruitment: recruitment of eligible participants through the Helpline |
| Participants | 4200 participants |
| Interventions | Pharmacotherapy: eight weeks of nicotine patch 1. Telephone counselling: pre‐quit session + five proactive follow‐up calls 2. Self‐help materials: reading materials mailed to the participants |
| Outcomes | Abstinence at 6 months Validation: unspecified in the trials registry |
| Starting date | February 2009 |
| Contact information | Shu‐Hong Zhu, University of California |
| Notes |
NCT00937235.
| Trial name or title | Treatment of smoking among individuals with PTSD: a phase II, randomised study of varenicline and cognitive behavioural therapy |
| Methods | RCT |
| Participants | 166 |
| Interventions | Pharmacotherapy: varenicline 1 mg tablets, orally, twice daily x 12 weeks 1. Control = 5‐min weekly counselling x 12 weeks, focused on medication adherence and smoking cessation 2. Control = 75 to 90‐min weekly psychotherapy sessions x 12 weeks, focused on gradually confronting distressing trauma‐related memories and reminders |
| Outcomes | Abstinence: 7‐day PP at 6 months |
| Starting date | January 2009 |
| Contact information | Edna B Foa, University of Pennsylvania |
| Notes |
NCT00984724.
| Trial name or title | Reducing tobacco‐related health disparities |
| Methods | Study design: randomised controlled trial Setting: not known Recruitment: not known |
| Participants | 639 participants |
| Interventions | Pharmacotherapy: 300 pieces of nicotine gum issued at baseline visit 1. Standard treatment: mailed packet with standard self‐help materials delivered four times + referral to quitline 2. MAPS‐6 (standard treatment + six phone counselling sessions over a two‐year period) 3. MAPS‐12 (standard treatment + 12 phone counselling sessions over a two‐year period) 4. Standard treatment + NRT 5. MAPS‐6 + NRT 6. MAPS‐12 + NRT |
| Outcomes | Abstinence at 24 months Validation: carbon monoxide < 10 ppm, saliva cotinine < 20 ng/mL |
| Starting date | January 2011 |
| Contact information | Larkin Strong, M.D. Anderson Cancer Center |
| Notes |
NCT01063972.
| Trial name or title | Smoking cessation in rural hospitals |
| Methods | Study design: randomised controlled trial Setting: Recruitment: |
| Participants | 606 participants (303 in each arm) |
| Interventions | Pharmacotherapy: not specified in the trials registry 1. In‐hospital smoking cessation counselling by phone + four outpatient counselling sessions by phone 2. Counselling as above but with coordination of pharmacotherapy with their insurance coverage and their health care provider |
| Outcomes | Abstinence at 12 months Validation: not specified in the trials registry |
| Starting date | March 2010 |
| Contact information | Edward Ellerbeck, University of Kansas Medical Center |
| Notes |
NCT01098955.
| Trial name or title | Smoking cessation treatment for head & neck cancer patients: acceptance and commitment therapy |
| Methods | RCT |
| Participants | 108 |
| Interventions | Pharmacotherapy: varenicline 2 mg daily for 12 weeks 1. Acceptance and Commitment Therapy (ACT): 6 x 60‐min counselling sessions delivered over a 5‐week period 2. Motivational and Behavioral Counselling (MBC): 6 x 60‐min counselling sessions delivered over a 5‐week period |
| Outcomes | Abstinence: 14 and 26 weeks Validation: cotinine verification |
| Starting date | March 2010 |
| Contact information | Jan Blalock M. D. Anderson Cancer Center |
| Notes |
NCT01162239.
| Trial name or title | Maintaining nonsmoking |
| Methods | Setting: USA |
| Participants | 271 |
| Interventions | Pharmacotherapy: varenicline: 12 weeks, 1 mg bid 1. Participants have monthly meetings with medical staff 2. Participants receive monthly counselling with content based on a health education model 3. Participants receive monthly counselling with content based on a relapse prevention model plus access to ongoing medication treatment with varenicline 4. Participants receive monthly counselling with content based on a relapse prevention model |
| Outcomes | Abstinence at 12, 24, 52, 64, 104 months |
| Starting date | May 2010 |
| Contact information | University of California. No PI listed |
| Notes |
NCT01186016.
| Trial name or title | Developing genetic education for smoking cessation |
| Methods | Study design: randomised controlled trial Setting: USA Recruitment: not given in the trials registry |
| Participants | 103 participants |
| Interventions | Pharmacotherapy: 6 weeks of transdermal nicotine replacement therapy 1. Two educational sessions about genetics and smoking 2. Two educational sessions about nutrition |
| Outcomes | Abstinence at 6 months Validation: not given in the trials registry |
| Starting date | April 2012 |
| Contact information | Julia F Houfek, University of Nebraska |
| Notes |
NCT01257490.
| Trial name or title | Integrated smoking cessation treatment for low‐income community corrections |
| Methods | RCT |
| Participants | 689 |
| Interventions | Pharmacotherapy: bupropion 1. Brief physician advice to quit plus bupropion 2. 4 sessions of intensive counselling plus bupropion |
| Outcomes | Abstinence: at 3, 6, 9, 12 months Validation: verified by expired carbon monoxide |
| Starting date | October 2009 |
| Contact information | Karen L Cropsey, University of Alabama at Birmingham |
| Notes |
NCT01736085.
| Trial name or title | Providing free Nicotine patches to quitline smokers |
| Methods | Study design: randomised controlled trial Setting: USA Recruitment: smokers aged 18 years or older recruited from the quitline |
| Participants | 3710 participants |
| Interventions | Pharmacotherapy: nicotine patches 1. self‐help materials only 2. self‐help materials + a voucher for 2 weeks’ worth of nicotine patches 3. self‐help materials + 2 weeks’ worth of nicotine patches 4. up to 5 sessions of telephone counselling 5. up to 5 sessions of telephone counselling + a voucher for 2 weeks’ worth of nicotine patches 6. up to 5 sessions of telephone counselling + 2 weeks’ worth of nicotine patches |
| Outcomes | 6 months prolonged abstinence Validation: none specified in the trials registry |
| Starting date | April 2013 |
| Contact information | Shu‐Hong Zhu, University of California |
| Notes |
NCT01800019.
| Trial name or title | The Canadian HIV Quit Smoking Trial: tackling the comorbidities of depression and cardiovascular disease in HIV+ smokers |
| Methods | RCT |
| Participants | 256 |
| Interventions | Pharmacotherapy: NRT = 7 mg to 42 mg depending on cpd; varenicline = 0.5 mg/daily for 3 days, 0.5 mg twice daily for 4 days and 1 mg twice daily for the remainder of the treatment period 1. NRT only 2. NRT + HIV‐tailored smoking cessation counselling 3. Varenicline only 4. Varenicline + HIV‐tailored smoking cessation counselling |
| Outcomes | Abstinence: 7‐day PP at week 48 Validation: expired carbon monoxide levels measured using a piCO+ Smokerlyzer; CO < 10 ppm |
| Starting date | January 2014 |
| Contact information | Louise Balfour, Ottawa Research Hospital |
| Notes |
NCT01901848.
| Trial name or title | CPT and smoking cessation |
| Methods | Study design: randomised controlled trial Setting: USA Recruitment: US veteran smokers with post‐traumatic stress disorder, aged between 18 and 65 years. Selected for motivation to quit smoking |
| Participants | 69 participants |
| Interventions | Pharmacotherapy: bupropion, nicotine patches and a rescue method (e.g. nicotine gum, lozenge, inhaler) 1. 12 sessions of combined cognitive processing therapy and integrated care for smoking cessation, involvement in smokefreeVET.gov’s text messaging programme for smoking cessation 2. 12 sessions of integrated care for smoking cessation, involvement in smokefreeVET.gov’s text messaging programme for smoking cessation |
| Outcomes | Abstinence at 6 months Validation: exhaled carbon monoxide < 4ppm |
| Starting date | December 2013 |
| Contact information | Eric A Dedert, Durham VA Medical Center |
| Notes |
NCT01965405.
| Trial name or title | Behavioural smoking cessation for people living with HIV/AIDS |
| Methods | Study design: randomised controlled trial Setting: USA Recruitment: smokers with HIV or AIDS diagnosis and aged 18 years or older |
| Participants | 400 participants |
| Interventions | Pharmacotherapy: a prescription for bupropion for all groups 1. Brief counselling 2. Brief counselling + brief high‐magnitude prize contingency management 3. Continued counselling + monitored support to quit smoking 4. Monitored support to quit smoking + prize contingency management for abstinence 5. Pharmacotherapy only 6. Continued monitoring + low intensity prize contingency management |
| Outcomes | Abstinence at 6 and 12 months Validation: urinary cotinine, carbon monoxide |
| Starting date | August 2013 |
| Contact information | David Ledgerwood, Wayne State University |
| Notes |
NCT02048917.
| Trial name or title | Smoking cessation strategies in community cancer programmes for lung and head and neck cancer patients |
| Methods | Setting: USA |
| Participants | 180 |
| Interventions | 1. High‐intensity counselling + long‐acting NRT + PRN NRT 2. High‐intensity counselling + bupropion + PRN NRT 3. High‐intensity counselling + varenicline + PRN NRT 4. High‐intensity counselling + long‐acting NRT 5. High‐intensity counselling + bupropion 6. High‐intensity counselling + varenicline 7. Low‐intensity counselling + long‐acting NRT + PRN NRT 8. Low‐intensity counselling + bupropion + PRN NRT 9. Low‐intensity counselling + varenicline + PRN NRT 10. Low‐intensity counselling + long‐acting NRT 11. Low‐intensity counselling + bupropion 12. Low‐intensity counselling + varenicline |
| Outcomes | Abstinence: 7‐day PP at 8 weeks Validation: CO |
| Starting date | July 2014 |
| Contact information | Joseph Valentino, University of Kentucky |
| Notes |
NCT02164383.
| Trial name or title | A quit smoking study using smartphones |
| Methods | RCT |
| Participants | 30 |
| Interventions | Pharmacotherapy: nicotine patch 1.Nicotine patch plus behavioural cessation counselling without access to Mobile Games 2. Nicotine patch plus behavioural cessation counselling with access to Mobile Games |
| Outcomes | Abstinence: change between baseline mean cigarettes smoked per day and mean cigarettes smoked per day during the first 4 weeks of the quit attempt |
| Starting date | October 2014 |
| Contact information | Tanya R. Schlam, University of Wisconsin Center for Tobacco Research and Intervention |
| Notes |
NCT02378714.
| Trial name or title | Behavioural activation and varenicline for smoking cessation in depressed smokers |
| Methods | Study design: randomised controlled trial Setting: Chicago, USA Recruitment: smokers with major depressive disorder |
| Participants | 576 participants |
| Interventions | Pharmacotherapy: varenicline or placebo for 12 weeks 1. Standard behavioural cessation treatment (45 minutes x 8 sessions) 2. Behavioural activation integrated with standard behavioural cessation treatment (45 minutes x 8 sessions) |
| Outcomes | Abstinence at 27 weeks Validation: expired carbon monoxide ≤ 8 ppm |
| Starting date | June 2015 |
| Contact information | Brian L Hitsman, Northwestern University |
| Notes |
NCT02460900.
| Trial name or title | Optimising smoking cessation for people with HIV/AIDS who smoke |
| Methods | Study design: randomised controlled trial (factorial) Setting: University of Maryland Medical Center, USA Recruitment: not specified in the trials registry |
| Participants | 300 participants |
| Interventions | Pharmacotherapy: varenicline 1. Standard care: low intensity, brief counselling 2. Positively Smoke Free (details unspecified in the trials registry) |
| Outcomes | Abstinence at 24 weeks Validation: not specified in the trials registry |
| Starting date | July 2016 |
| Contact information | Seth Himelhoch, University of Maryland |
| Notes |
NCT02767908.
| Trial name or title | Hospital to home, smoker support trial |
| Methods | Study design: randomised controlled trial Setting: hospital and home Recruitment: smokers leaving hospital |
| Participants | 404 participants |
| Interventions | Pharmacotherapy: nicotine replacement products 1. Usual care: behavioural support before leaving hospital, referral to NHS Stop Smoking Services after discharge 2. Home visit as soon as practicable after discharge and typically within 48 hours to deliver a multicomponent intervention; tailored support package including telephone support, carbon dioxide measurements, home air quality measurements, signposting to support groups, self‐help materials |
| Outcomes | Abstinence at 4 weeks and 12 weeks post‐discharge according to the information on the trials registry Validation: exhaled carbone monoxide < 6 ppm |
| Starting date | June 2016 |
| Contact information | John Britton, University of Nottingham |
| Notes |
NCT02898597.
| Trial name or title | Smoking cessation intervention for women with HIV/AIDS |
| Methods | Study design: randomised controlled trial Setting: USA Recruitment: smokers with diagnosis of HIV infection and aged between 18 and 75 years |
| Participants | 50 participants |
| Interventions | Pharmacotherapy: nicotine replacement therapy (habitrol patch) 1. cognitive behavioural therapy via video‐conferencing 2. cognitive behavioural therapy via telephone |
| Outcomes | Abstinence at 6 months Validation: saliva cotinine |
| Starting date | June 2016 |
| Contact information | Sun S Kim, University of Massachusetts |
| Notes |
NCT02905656.
| Trial name or title | Strategies to promote cessation in smokers who are not ready to quit (PACE) |
| Methods | Study design: randomised controlled trial Setting: USA Recruitment: smokers aged 18 years or older |
| Participants | 828 participants |
| Interventions | Pharmacotherapy: nicotine gum 1. brief advice + typical smoking cessation resources 2. motivational interviewing 3. rate reduction 4. motivational interviewing + rate reduction |
| Outcomes | Abstinence at 12 months Validation: not specified in the trials registry |
| Starting date | September 2016 |
| Contact information | Robert Klesges, University of Virginia |
| Notes |
NCT03072511.
| Trial name or title | Pilot trial of a smoking cessation intervention informed by construal level theory |
| Methods | Study design: randomised controlled trial Setting: USA Recruitment: not specified in the trials registry |
| Participants | 23 participants |
| Interventions | Pharmacotherapy: eight weeks of transdermal nicotine patch 1. Standard informational treatment: in‐person session, text messaging 2. Spotlight on smoke‐free living 1.5 hour intervention session combined with daily text messaging for up to 1 week pre‐quit and 4 weeks post‐quit. |
| Outcomes | Abstinence at 13 weeks Validation: not specified in the trials registry |
| Starting date | December 2016 |
| Contact information | Richard Yi, University of Florida |
| Notes |
NCT03342027.
| Trial name or title | Smoking cessation interventions for people living with HIV in Nairobi, Kenya |
| Methods | Study design: randomised controlled trial (factorial) Setting: Nairobi, Kenya Recruitment: smokers living with HIV and receiving care in a methadone maintenance programme in Nairobi, Kenya |
| Participants | 300 participants |
| Interventions | Pharmacotherapy: bupropion 1. Standard care: brief advice to quit provided in a standardised format 2. Positively smoke free: eight sessions of tailored behavioural treatment for smoking cessation |
| Outcomes | Abstinence at 36 months Validation: carbon monoxide level < 7ppm |
| Starting date | January 2019 |
| Contact information | Seth Himelhoch, University of Maryland |
| Notes |
NCT03538938.
| Trial name or title | Improving quitline support study: optimising remotely delivered smoking cessation services for low‐income smokers |
| Methods | Study design: four‐factor, fully‐crossed randomised controlled trial Setting: USA Recruitment: smokers aged 18 years or older selected for motivation to quit |
| Participants | 1600 participants |
| Interventions | Pharmacotherapy: 2 weeks of nicotine patches and lozenges 16 conditions of four factors: phone call, SmokefreeTXT, financial incentive, nicotine replacement (patches +/‐ lozenges) |
| Outcomes | Abstinence at 6 months Validation: saliva cotinine < 4ng/mL |
| Starting date | July 2018 |
| Contact information | Danielle E McCarthy, University of Wisconsin |
| Notes |
NCT03603496.
| Trial name or title | Post‐discharge smoking cessation strategies: helping HAND 4 |
| Methods | Study design: randomised controlled trial Setting: three hospitals in USA Recruitment: not specified in the trials registry |
| Participants | 1350 participants |
| Interventions | Pharmacotherapy: eight weeks of nicotine replacement therapy 1. Electronic referral to State tobacco quitline 2. Personalised tobacco care management: seven proactive contacts over three months delivered by automated interactive voice response phone calls, text messaging and/or email + offer of a return call from the hospital‐based tobacco coach who offer counselling, medication advice and coordination of care with the patient’s outpatient health care team |
| Outcomes | Abstinence at 6 months after hospital discharge Validation: not specified in the trials registry |
| Starting date | August 2018 |
| Contact information | Nancy Rigotti, Massachusetts General Hospital |
| Notes |
Ojo‐Fati 2015.
| Trial name or title | Integrating smoking cessation and alcohol use treatment in homeless populations |
| Methods | Study design: randomised controlled trial Setting: homeless shelters Recruitment: homeless smokers aged 18 years or older |
| Participants | 645 participants |
| Interventions | Pharmacotherapy: 12 weeks of nicotine patch plus nicotine gum or lozenge 1. Integrated intensive smoking plus alcohol intervention using cognitive behavioural therapy 2. Intensive smoking intervention using cognitive behavioural therapy 3. Usual care: brief smoking cessation and brief alcohol counselling |
| Outcomes | Abstinence at 52 weeks Validation: cotinine‐verified 7‐day smoking abstinence |
| Starting date | January 2015 |
| Contact information | Olamide Ojo‐Fati, Universtiy of Minnesota |
| Notes |
Powers 2016.
| Trial name or title | Efficacy of smoking cessation therapy alone or integrated with prolonged exposure therapy for smokers with PTSD |
| Methods | Study design: randomised controlled trial Setting: USA Recruitment: smokers with post‐traumatic stress disorder aged between 18 and 64 years selected for motivation to quit |
| Participants | 80 participants |
| Interventions | Pharmacotherapy: nicotine patch 1. Standard smoking cessation treatment: once‐weekly 45‐minute sessions of cognitive behavioural therapy over a 12‐week period 2. Integrated PTSD and smoking treatment: once‐weekly 90‐minute sessions over a 12‐week period. Incorporated standard treatment with therapy for reducing PTSD symptoms and anxiety sensitivity and enhancing tolerance for nicotine withdrawal sensations. |
| Outcomes | Abstinence at 24 weeks Validation: saliva cotinine < 10ng/mL for stated abstinence of 2 weeks or more, carbon monoxide analysis of breath samples < 8ppm for stated abstinence of 24 hours to 2 weeks |
| Starting date | October 2013 |
| Contact information | Mark B Powers, University of Texas |
| Notes |
Reid 2011.
| Trial name or title | Interactive voice response telephone technology for the treatment of smoking in patients with heart disease (IVR) |
| Methods | Setting: smokers recently hospitalised with CHD, Canada Health Care Recruitment: study co‐ordinator recruited within 24 hours of admission |
| Participants | N randomised: 100 (but 99 used in calculations). Dropouts: 15 + 1 death Sex: 67.4% M, Age: 54, av cpd 16‐25 Therapists: nurse specialist |
| Interventions | Pharmacotherapy: NRT in hospital before quit date 1. Access to NRT during hospitalisation, brief bedside counselling by nurse, self‐help guide 2. Interactive Voice Response system posted questions "concerning current smoking status, confidence in staying smoke‐free, use of pharmacotherapy, and self‐help materials" |
| Outcomes | Abstinence at 12 m, 7‐day PP Validation: none |
| Starting date | July 2006 |
| Contact information | Robert Reid, University of Ottawa Heart Institute |
| Notes |
Salgado 2018.
| Trial name or title | Planning a change easily: a randomised controlled trial for smokers who are not ready to quit |
| Methods | Study design: randomised controlled trial Setting: not specified in the protocol Recruitment: smokers recruited via flyers, business cards, medical referrals, Facebook, Pandora Radio, and ‘refer‐a‐friend’ programme |
| Participants | 840 participants |
| Interventions | Pharmacotherapy: 4 mg nicotine gum for rate reduction group and motivational interviewing + rate reduction group. 1. Brief advice 2. Motivational interviewing 3. Rate reduction 4. Motivational interviewing + rate reduction |
| Outcomes | Abstinence at 12 months Validation: saliva cotinine |
| Starting date | Not specified in the protocol |
| Contact information | Francisco I Salgado Garcia, Universtiy of Tennesse |
| Notes |
Vander Weg 2018.
| Trial name or title | Community‐based physical activity as adjunctive smoking cessation treatment: rationale, design, and baseline data for the Lifestyle Enhancement Program (LEAP) randomised controlled trial |
| Methods | Study design: randomised controlled trial Setting: community, USA Recruitment: smokers who are sedentary or minimally active during leisure time, and aged between 18 and 65 years |
| Participants | 392 participants |
| Interventions | Pharmacotherapy: 6 weeks of transdermal nicotine 1. Behavioural counselling + physical activity intervention 2. Behavoural counselling + wellness intervention |
| Outcomes | Abstinence at 12 months Validation: expired carbon monoxide < 10ppm |
| Starting date | January 2003 |
| Contact information | Kenneth D Ward, University of Memphis |
| Notes |
Vidrine 2012.
| Trial name or title | Enhancing cancer outreach for low‐income adults with innovative smoking cessation. Project ACTION (Adult smoking Cessation Treatment through Innovative Outreach to Neighborhoods) |
| Methods | Cluster RCT Setting: community, USA |
| Participants | 756 |
| Interventions | 1. Standard care: brief coach advice to quit smoking, nicotine replacement therapy (NRT), and self‐help written materials 2. Enhanced care: As 1. plus a single motivational interviewing counselling session and a cell phone‐delivered text/graphical messaging component 3. Intensive care: As 2. plus a series of 11 cell phone‐delivered proactive counselling sessions and a cell phone‐delivered text/graphical messaging component |
| Outcomes | Abstinence at 12 months |
| Starting date | June 2010 |
| Contact information | Alex Prokhorov, University of Texas MD Anderson Cancer Center |
| Notes |
Webb 2018.
| Trial name or title | Reducing racial/ethnic tobacco cessation disparities via cognitive behavioural therapy: design of a dual‐site randomised controlled trial |
| Methods | Study design: randomised controlled trial Setting: USA Recruitment: African American/black, Hispanic, or white non‐Hispanic smokers aged 18 years or older |
| Participants | 354 participants |
| Interventions | Pharmacotherapy: up to 8 weeks of transdermal nicotine patch 1. Group cognitive behavioural therapy 2. General health education |
| Outcomes | Abstinence at 12 months Validation: not specified in the trials registry |
| Starting date | August 2015 |
| Contact information | Monica Webb Hooper, Case Western Reserve University School of Medicine |
| Notes |
ACT: Acceptance and commitment therapy
bid: bis in die (twice a day) CHD: cornary heart disease cpd: cigarettes per day CPT: cognitive processing therapy IVR: interactive voice response NRT: nicotine replacement therapy PI: prinicipal investigator PRN: pro re nata (when necessary) PTSD: post‐traumatic stress disorder
Differences between protocol and review
We added two additional subgroup analyses. We had initially planned to assess risk of bias based on blinding of participants and personnel, but given the nature of the studies, we provided a narrative discussion of this instead.
In this version of the review, we switched from fixed‐effect to random‐effects meta‐analyses in accordance with revised guidance from the Cochrane Tobacco Addiction Group. We also introduced a new, exploratory meta‐regression based on the number of contacts. In addition, we included eligible studies where contact was matched between arms (previously excluded). We expanded our inclusion criteria to include studies in adolescents.
Contributions of authors
For this version of the review: JLB ran the searches; BH, HW and JHB screened search results; BH, HW, JHB, CM and JLB extracted data; JLB, JHB and TF conducted analyses; BH, TF, JLB and JHB updated the text; and all authors reviewed and commented on the text.
For the original and second version of the review, LS developed the search strategy, screened search results and extracted data. For the original review TL agreed inclusion or exclusion of potentially relevant studies and checked data extraction. For the second version of the review, PK agreed inclusion or exclusion of potentially relevant studies and extracted data. All authors contributed to the text.
Sources of support
Internal sources
Nuffield Department of Primary Care Health Sciences, Oxford University, UK.
External sources
NHS National Institute for Health Research, UK.
-
Faculty of Medicine Marvin Burke Summer Studentship, Dalhousie University, Canada.
Funding for travel and accommodation
Declarations of interest
JHB: none known
BH: none known
JLB: none known
HW: none known
TRF: none known
New search for studies and content updated (no change to conclusions)
References
References to studies included in this review
Ahluwalia 2006 {published data only}
- Ahluwalia JS, Okuyemi K, Nollen N, Choi WS, Kaur H, Pulvers K, et al. The effects of nicotine gum and counseling among African American light smokers: a 2 x 2 factorial design. Addiction 2006;101(6):883‐91. [DOI] [PubMed] [Google Scholar]
- Nollen NL, Mayo MS, Sanderson Cox L, Okuyemi KS, Choi WS, Kaur H, et al. Predictors of quitting among African American light smokers enrolled in a randomized, placebo‐controlled trial. Journal of General Internal Medicine 2006;21(6):590‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okuyemi KS, Faseru B, Sanderson Cox L, Bronars CA, Ahluwalia JS. Relationship between menthol cigarettes and smoking cessation among African American light smokers. Addiction 2007;102(12):1979‐86. [DOI] [PubMed] [Google Scholar]
Aimer 2017 {published data only}
- Aimer P, Treharne GJ, Stebbings S, Frampton C, Cameron V, Kirby S, et al. Efficacy of a rheumatoid arthritis‐specific smoking cessation programme; a pilot randomized controlled trial. Arthritis Care & Research 2017;69(1):28‐37. [DOI] [PubMed] [Google Scholar]
Alterman 2001 {published data only}
- Alterman AI, Gariti P, Cook TG, Cnaan A. Nicodermal patch adherence and its correlates. Drug & Alcohol Dependence 1999;53(2):159‐65. [DOI] [PubMed] [Google Scholar]
- Alterman AI, Gariti P, Mulvaney F. Short‐ and long‐term smoking cessation for three levels of intensity of behavioral treatment. Psychology of Addictive Behaviors 2001;15(3):261‐4. [PubMed] [Google Scholar]
Aveyard 2007 {published data only}
- Aveyard P, Brown K, Saunders C, Alexander A, Johnstone E, Munafò MR, et al. Weekly versus basic smoking cessation support in primary care: a randomised controlled trial. Thorax 2007;62(10):898‐903. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greaves C. Smoking cessation trial may be missing the point [comment]. Thorax 2008;63(3):291‐2. [PubMed] [Google Scholar]
Bailey 2013 {published data only}
- Bailey SR, Hagen SA, Jeffery CJ, Harrison CT, Ammerman S, Bryson SW, et al. A randomized clinical trial of the efficacy of extended smoking cessation treatment for adolescent smokers. Nicotine & Tobacco Research 2013;15(10):1655‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Baker 2015 {published data only}
- ACTRN12609001039279. Healthy lifestyle intervention for cardiovascular disease risk reduction among smokers with psychotic disorders. Australia and New Zealand Clinical Trials Registry (first received 4 December 2009).
- Baker AL, Richmond R, Kay‐Lambkin FJ, Filia SL, Castle D, Williams JM, et al. Randomised controlled trial of a healthy lifestyle intervention among smokers with psychotic disorders: outcomes to 36 months. Australian and New Zealand Journal of Psychiatry 2018;52(3):239‐52. [DOI] [PubMed] [Google Scholar]
- Baker AL, Richmond R, Kay‐Lambkin FJ, Filia SL, Castle D, Williams JM, et al. Randomized controlled trial of a healthy lifestyle intervention among smokers with psychotic disorders. Nicotine & Tobacco Research 2015;17(8):946‐54. [DOI] [PubMed] [Google Scholar]
Bastian 2012 {published data only}
- Bastian LA, Fish LJ, Gierisch JM, Rohrer LD, Stechuchak KM, Grambow SC. Comparative effectiveness trial of family‐supported smoking cessation intervention versus standard telephone counseling for chronically ill veterans using proactive recruitment. Comparative Effectiveness Research 2012;2:45‐56. [Google Scholar]
- NCT00448344. Family‐supported smoking cessation for chronically ill veterans. ClinicalTrials.gov/show/NCT00448344 (first received 16 March 2007).
Begh 2015 {published data only}
- Begh R, Munafo MR, Shiffman S, Ferguson SG, Nichols L, Mohammed MA, et al. Lack of attentional retraining effects in cigarette smokers attempting cessation: a proof of concept double‐blind randomised controlled trial. Drug and Alcohol Dependence 2015;149:158‐65. [DOI] [PMC free article] [PubMed] [Google Scholar]
Berndt 2014 {published data only}
- Berndt N, Bolman C, Froelicher ES, Mudde A, Candel M, Vries H, et al. Effectiveness of a telephone delivered and a face‐to‐face delivered counseling intervention for smoking cessation in patients with coronary heart disease: a 6‐month follow‐up. Journal of Behavioral Medicine 2014;37(4):709‐24. [CENTRAL: 1000936; CRS: 9400107000001638; PUBMED: 23760610] [DOI] [PubMed] [Google Scholar]
- Berndt N, Bolman C, Lechner L, Mudde A, Verheugt FW, Vries H. Effectiveness of two intensive treatment methods for smoking cessation and relapse prevention in patients with coronary heart disease: study protocol and baseline description. BMC Cardiovascular Disorders 2012;12:33. [CENTRAL: 840357; CRS: 9400123000016156; EMBASE: 2012574240; PUBMED: 22587684] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berndt N, Lechner L, Vries H, Acker F, Mudde A, Froelicher E, et al. Effectiveness of two intensive smoking cessation interventions for the secondary prevention of coronary heart disease: benefits for patients with low socioeconomic status and low quit motivations. European Heart Journal 2013;34:475. [CENTRAL: 1006097; CRS: 9400050000000077; EMBASE: 71259288] [Google Scholar]
Bloom 2017 {published data only}
- Bloom EL, Minami H, Brown RA, Strong DR, Riebe D, Abrantes AM. Quality of life after quitting smoking and initiating aerobic exercise. Psychology, Health & Medicine 2017;22(9):1127‐35. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bock 2014 {published data only}
- Bock BC, Papandonatos GD, Dios MA, Abrams DB, Azam MM, Fagan M, et al. Tobacco cessation among low‐income smokers: motivational enhancement and nicotine patch treatment. Nicotine & Tobacco Research 2014;16(4):413‐22. [CENTRAL: 986341; CRS: 9400050000000050; EMBASE: 2014185069; PUBMED: 24174612] [DOI] [PMC free article] [PubMed] [Google Scholar]
Boyle 2007 {published data only}
- Boyle RG, Solberg LI, Asche SE, Boucher JL, Pronk NP, Jensen CJ. Offering telephone counseling to smokers using pharmacotherapy. Nicotine & Tobacco Research 2005;7 Suppl 1:S19‐27. [DOI] [PubMed] [Google Scholar]
- Boyle RG, Solberg LI, Asche SE, Maciosek MV, Boucher JL, Pronk NP. Proactive recruitment of health plan smokers into telephone counseling. Nicotine & Tobacco Research 2007;9(5):581‐9. [DOI] [PubMed] [Google Scholar]
Bricker 2014 {published data only}
- Bricker JB, Bush T, Zbikowski SM, Mercer LD, Heffner JL. Randomized trial of telephone‐delivered acceptance and commitment therapy versus cognitive behavioral therapy for smoking cessation: a pilot study. Nicotine & Tobacco Research 2014;16(11):1446‐54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heffner JL, Mull K, Mercer L, Vilardaga R, Bricker J. Effects of two telephone‐delivered smoking cessation interventions on hazardous drinking rates: ACT vs. CBT. Alcoholism, Clinical and Experimental Research 2014;38(Suppl 1):137A. [CENTRAL: 993969; CRS: 9400129000002292; EMBASE: 71503629] [Google Scholar]
- Vilardaga R, Heffner JL, Mercer LD, Bricker JB. Do counselor techniques predict quitting during smoking cessation treatment? A component analysis of telephone‐delivered Acceptance and Commitment Therapy. Behaviour Research and Therapy 2014;61:89‐95. [DOI] [PMC free article] [PubMed] [Google Scholar]
Brody 2017 {published data only}
- Brody AL, Zorick T, Hubert R, Hellemann GS, Balali S, Kawasaki SS, et al. Combination extended smoking cessation treatment plus home visits for smokers with schizophrenia: a randomized controlled trial. Nicotine & Tobacco Research 2017;19(1):68‐76. [DOI] [PMC free article] [PubMed] [Google Scholar]
Brown 2013 {published data only}
- Brown RA, Reed KM, Bloom EL, Minami H, Strong DR, Lejuez CW, et al. Development and preliminary randomized controlled trial of a distress tolerance treatment for smokers with a history of early lapse. Nicotine & Tobacco Research 2013;15(12):2005‐15. [CENTRAL: 915430; CRS: 9400129000000262; EMBASE: 2013716990; PUBMED: 23884317] [DOI] [PMC free article] [PubMed] [Google Scholar]
Busch 2017 {published data only}
- Busch AM, Tooley EM, Dunsiger S, Chattillion EA, Srour JF, Pagoto SL, et al. Behavioral activation for smoking cessation and mood management following a cardiac event: results of a pilot randomized controlled trial. BMC Public Health 2017;17(1):323. [DOI] [PMC free article] [PubMed] [Google Scholar]
Bushnell 1997 {published data only}
- Bushnell FK, Forbes B, Goffaux J, Dietrich M, Wells N. Smoking cessation in military personnel. Military Medicine 1997;162(11):715‐9. [PubMed] [Google Scholar]
Calabro 2012 {published data only}
- Calabro KS, Marani S, Yost T, Segura J, Mullin Jones M, Nelson S, et al. Project SUCCESS: results from a randomized controlled trial. International Scholarly Research Network Public Health 2012;2012:1‐9. [CENTRAL: 836719; CRS: 9400123000016091] [Google Scholar]
- Prokhorov AV, Marani S, Vost T, Luca M, Mullen M. Project SUCCESS: students using computerized coaching to end smoking successfully. Society for Research on Nicotine & Tobacco 17th Annual Meeting, 2011 February 16‐19; Toronto. 2011:18. [CENTRAL: 795274; CRS: 9400123000006112; 31113; PA2‐3]
Cook 2016 {published data only}
- Cook JW, Collins LM, Fiore MC, Smith SS, Fraser D, Bolt DM, et al. Comparative effectiveness of motivation phase intervention components for use with smokers unwilling to quit: a factorial screening experiment. Addiction 2016;111(1):117‐28. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cropsey 2015 {published data only}
- Cropsey KL, Clark CB, Zhang X, Hendricks PS, Jardin BF, Lahti AC. Race and medication adherence moderate cessation outcomes in criminal justice smokers. American Journal of Preventive Medicine 2015;49(3):335‐44. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ellerbeck 2009 {published data only}
- Cox LS, Cupertino AP, Mussulman LM, Nazir N, Greiner KA, Mahnken JD, et al. Design and baseline characteristics from the KAN‐QUIT disease management intervention for rural smokers in primary care. Preventive Medicine 2008;47(2):200‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cox LS, Wick JA, Nazir N, Cupertino AP, Mussulman LM, Ahluwalia JS, et al. Predictors of early versus late smoking abstinence within a 24‐month disease management program. Nicotine & Tobacco Research 2011;13(3):215‐20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cupertino AP, Mahnken JD, Richter K, Cox LS, Casey G, Resnicow K, et al. Long‐term engagement in smoking cessation counseling among rural smokers. Journal of Health Care for the Poor and Underserved 2007;18(4 Suppl):30‐51. [DOI] [PubMed] [Google Scholar]
- Cupertino AP, Wick JA, Richter KP, Mussulman L, Nazir N, Ellerbeck EF. The impact of repeated cycles of pharmacotherapy on smoking cessation: a longitudinal cohort study. Archives of Internal Medicine 2009;169(20):1928‐30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellerbeck EF, Mahnken JD, Cupertino AP, Cox LS, Greiner KA, Mussulman LM, et al. Effect of varying levels of disease management on smoking cessation: a randomized trial. Annals of Internal Medicine 2009;150(7):437‐46. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ferguson 2012 {published data only}
- Coleman T, McEwen A, Bauld L, Ferguson J, Lorgelly P, Lewis S. Protocol for the Proactive Or Reactive Telephone Smoking ceSsation Support (PORTSSS) trial. Trials 2009;10:26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ferguson J, Docherty G, Bauld L, Lewis S, Lorgelly P, Boyd KA, et al. Effect of offering different levels of support and free nicotine replacement therapy via an English national telephone quitline: randomised controlled trial. BMJ 2012;344(7854):1‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
Fiore 2004 {published data only}
- Fiore MC, McCarthy DE, Jackson TC, Zehner ME, Jorenby DE, Mielke M, et al. Integrating smoking cessation treatment into primary care: an effectiveness study. Preventive Medicine 2004;38(4):412‐20. [DOI] [PubMed] [Google Scholar]
Gariti 2009 {published data only}
- Gariti P, Lynch K, Alterman A, Kampman K, Xie H, Varillo K. Comparing smoking treatment programs for lighter smokers with and without a history of heavier smoking. Journal of Substance Abuse Treatment 2009;37(3):247‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
Gifford 2011 {published data only}
- Gifford EV, Kohlenberg BS, Hayes SC, Pierson HM, Piasecki MP, Antonuccio DO, et al. Does acceptance and relationship focused behavior therapy contribute to bupropion outcomes? A randomized controlled trial of functional analytic psychotherapy and acceptance and commitment therapy for smoking cessation. Behavior Therapy 2011;42(4):700‐15. [CENTRAL: 814642; CRS: 9400123000012398; 6939; PUBMED: 22035998] [DOI] [PubMed] [Google Scholar]
Ginsberg 1992 {published data only}
- Ginsberg D, Hall SM, Rosinski M. Partner support, psychological treatment, and nicotine gum in smoking treatment: an incremental study. International Journal of the Addictions 1992;27(5):503‐14. [DOI] [PubMed] [Google Scholar]
Hall 1985 {published data only}
- Hall SM, Killen JD. Psychological and pharmacological approaches to smoking relapse prevention. National Institute on Drug Abuse Research Monograph 1985;53:131‐43. [PubMed] [Google Scholar]
- Hall SM, Tunstall C, Rugg D, Jones R, Benowitz N. Nicotine gum and behavioral treatment in smoking cessation. Journal of Consulting and Clinical Psychology 1985;53(2):256‐8. [DOI] [PubMed] [Google Scholar]
Hall 1987 {published data only}
- Hall SM, Tunstall CD, Ginsberg D, Benowitz NL, Jones RT. Nicotine gum and behavioral treatment: a placebo controlled trial. Journal of Consulting and Clinical Psychology 1987;55(4):603‐5. [DOI] [PubMed] [Google Scholar]
Hall 1994 {published data only}
- Hall SM, Muñoz RF, Reus VI. Cognitive‐behavioral intervention increases abstinence rates for depressive‐history smokers. Journal of Consulting and Clinical Psychology 1994;62(1):141‐6. [DOI] [PubMed] [Google Scholar]
Hall 1998 {published data only}
- Hall SM, Reus VI, Muñoz RF, Sees KL, Humfleet G, Hartz DT, et al. Nortriptyline and cognitive‐behavioral therapy in the treatment of cigarette smoking. Archives of General Psychiatry 1998;55(8):683‐90. [DOI] [PubMed] [Google Scholar]
- Hall SM, Reus VI, Muñoz RF, Sees KL, Humfleet GL, Frederick S. Nortriptyline and cognitive‐behavioral treatment of cigarette smoking. College on Problems of Drug Dependence Annual Meeting; 1996; San Juan, Puerto Rico. 1996:52.
Hall 2002 {published data only}
- Hall SM, Humfleet GL, Reus VI, Muñoz RF, Hartz DT, Maude‐Griffin R. Psychological intervention and antidepressant treatment in smoking cessation. Archives of General Psychiatry 2002;59(10):930‐6. [DOI] [PubMed] [Google Scholar]
- Hall SM, Lightwood JM, Humfleet GL, Bostrom A, Reus VI, Muñoz R. Cost‐effectiveness of bupropion, nortriptyline, and psychological intervention in smoking cessation. Journal of Behavioral Health Services & Research 2005;32(4):381‐92. [DOI] [PubMed] [Google Scholar]
Hall 2009 {published data only}
- Hall SM, Humfleet GL, Muñoz RF, Reus VI, Robbins JA, Prochaska JJ. Extended treatment of older cigarette smokers. Addiction 2009;104(6):1043‐52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hendricks PS, Delucchi KL, Hall SM. Mechanisms of change in extended cognitive behavioral treatment for tobacco dependence. Drug & Alcohol Dependence 2010;109(1‐3):114‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hasan 2014 {published data only}
- Hasan FM, Zagarins SE, Pischke KM, Saiyed S, Bettencourt AM, Beal L, et al. Hypnotherapy is more effective than nicotine replacement therapy for smoking cessation: results of a randomized controlled trial. Complementary Therapies in Medicine 2014;22:1‐8. [DOI] [PubMed] [Google Scholar]
- NCT01791803. Smoking cessation after hospitalization for a cardiopulmonary illness (STOPP). ClinicalTrials.gov/show/NCT01791803 (first received 15 February 2013).
Hollis 2007 {published data only}
- Hollis JF, McAfee TA, Fellows JL, Zbikowski SM, Stark M, Riedlinger K. The effectiveness and cost effectiveness of telephone counselling and the nicotine patch in a state tobacco quitline. Tobacco Control 2007;16(Suppl 1):i53‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Huber 2003 {published data only}
- Huber D. Combined and separate treatment effects of nicotine chewing gum and self‐control method. Pharmacopsychiatry 1988;21(6):461‐2. [DOI] [PubMed] [Google Scholar]
- Huber D, Gastner J. Smoking cessation: a comparison of behavior therapy, nicotine replacement therapy and their combination. Verhaltenstherapie und Verhaltenshmedizin 2003;24:167‐85. [Google Scholar]
Humfleet 2013 {published data only}
- Humfleet GL, Hall SM, Delucchi KL, Dilley JW. A randomized clinical trial of smoking cessation treatments provided in HIV clinical care settings. Nicotine & Tobacco Research 2013;15(8):1436‐45. [CENTRAL: 861196; CRS: 9400123000017501; EMBASE: 2013472501; OI:SOURCE:: NLM. PMC3715392 [Available on 08/01/14]; PUBMED: 23430708] [DOI] [PMC free article] [PubMed] [Google Scholar]
Jorenby 1995 {published data only}
- Jorenby DE, Smith SS, Fiore MC, Hurt RD, Offord KP, Croghan IT, et al. Varying nicotine patch dose and type of smoking cessation counseling. JAMA 1995;274(17):1347‐52. [PubMed] [Google Scholar]
Kahler 2015 {published data only}
- Kahler CW, Spillane NS, Day AM, Cioe PA, Parks A, Leventhal AM, et al. Positive psychotherapy for smoking cessation: a pilot randomized controlled trial. Nicotine & Tobacco Research 2015;17(11):1385‐92. [DOI] [PMC free article] [PubMed] [Google Scholar]
Killen 2008 {published data only}
- Killen JD, Fortmann SP, Schatzberg AF, Arredondo C, Murphy G, Hayward C, et al. Extended cognitive behavior therapy for cigarette smoking cessation. Addiction 2008;103(8):1381‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kim 2015 {published data only}
- Kim SS, Kim SH, Fang H, Kwon S, Shelley D, Ziedonis D. A culturally adapted smoking cessation intervention for Korean Americans: a mediating effect of perceived family norm toward quitting. Journal of Immigrant and Minority Health 2015;17(4):1120‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
LaChance 2015 {published data only}
- LaChance H, Cioe PA, Tooley E, Colby SM, O'Farrell TJ, Kahler CW. Behavioral couples therapy for smoking cessation: a pilot randomized clinical trial. Psychology of Addictive Behaviors 2015;29(3):643‐52. [DOI] [PMC free article] [PubMed] [Google Scholar]
Lando 1997 {published data only}
- Lando HA, Rolnick S, Klevan D, Roski J, Cherney L, Lauger G. Telephone support as an adjunct to transdermal nicotine in smoking cessation. American Journal of Public Health 1997;87(10):1670‐4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rolnick SJ, Klevan D, Cherney L, Lando HA. Nicotine replacement therapy in a group model HMO. Health Maintenance Organization Practice 1997;11(1):34‐7. [PubMed] [Google Scholar]
Lifrak 1997 {published data only}
- Lifrak P, Gariti P, Alterman AI, McKay J, Volpicelli J, Sparkman T, et al. Results of two levels of adjunctive treatment used with the nicotine patch. American Journal on Addictions 1997;6(2):93‐8. [PubMed] [Google Scholar]
Lloyd‐Richardson 2009 {published data only}
- Dios MA, Stanton CA, Cano MA, Lloyd‐Richardson E, Niaura R. The influence of social support on smoking cessation treatment adherence among HIV+ smokers. Nicotine & Tobacco Research 2016;18(5):1126‐33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lloyd‐Richardson EE, Stanton CA, Papandonatos GD, Shadel WG, Stein M, Tashima K, et al. Motivation and patch treatment for HIV+ smokers: a randomized controlled trial. Addiction 2009;104(11):1891‐900. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanton CA, Lloyd‐Richardson EE, Papandonatos GD, Dios MA, Niaura R. Mediators of the relationship between nicotine replacement therapy and smoking abstinence among people living with HIV/AIDS. AIDS Education & Prevention 2009;21(3 Suppl):65‐80. [DOI] [PMC free article] [PubMed] [Google Scholar]
MacLeod 2003 {published data only}
- Macleod ZR, Charles MA, Arnaldi VC, Adams IM. Telephone counselling as an adjunct to nicotine patches in smoking cessation: a randomised controlled trial. Medical Journal of Australia 2003;179(7):349‐52. [DOI] [PubMed] [Google Scholar]
Macpherson 2010a {published data only}
- Macpherson L, Tull MT, Matusiewicz AK, Rodman S, Strong DR, Kahler CW, et al. Randomized controlled trial of behavioral activation smoking cessation treatment for smokers with elevated depressive symptoms. Journal of Consulting and Clinical Psychology 2010;78(1):55‐61. [DOI] [PMC free article] [PubMed] [Google Scholar]
Matthews 2018 {published data only}
- Matthews AK, McConnell EA, Li CC, Vargas MC, King A. Design of a comparative effectiveness evaluation of a culturally tailored versus standard community‐based smoking cessation treatment program for LGBT smokers. BMC Psychology 2014;2(1):12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Matthews AK, Steffen A, Kuhns L, Ruiz R, Ross N, Burke L, et al. Evaluation of a randomized clinical trial comparing the effectiveness of a culturally targeted and non‐targeted smoking cessation intervention for lesbian, gay, bisexual and transgender (LGBT) smokers. Nicotine & Tobacco Research 2018;31:nty184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT01633567. Culturally targeted & individually tailored smoking cessation study: LGBT smokers. ClinicalTrials.gov/show/NCT01633567 (first received 4 July 2012).
McCarthy 2008 {published data only}
- McCarthy DE. Mechanisms of tobacco cessation treatment: self‐report mediators of counseling and bupropion sustained release treatment. Dissertation Abstracts International: Section B: The Sciences and Engineering 2007;67(9‐B):5414. [Google Scholar]
- McCarthy DE, Piasecki TM, Lawrence DL, Jorenby DE, Shiffman S, Baker TB. Psychological mediators of bupropion sustained‐release treatment for smoking cessation. Addiction 2008;103(9):1521‐33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCarthy DE, Piasecki TM, Lawrence DL, Jorenby DE, Shiffman S, Fiore MC, et al. A randomized controlled clinical trial of bupropion SR and individual smoking cessation counseling. Nicotine & Tobacco Research 2008;10(4):717‐29. [DOI] [PubMed] [Google Scholar]
NCT00879177 {published data only}
- NCT00879177. Smoking study with behavioral therapy for hypertensive patients. ClinicalTrials.gov/show/NCT00879177 (first received 9 April 2009).
O'Cleirigh 2018 {published data only}
- NCT01393301. Integrated treatment for smoking cessation & anxiety in people with HIV. ClinicalTrials.gov/show/NCT01393301 (first received 13 July 2011).
- O'Cleirigh CO, Zvolensky MJ, Smits JAJ, Labbe AK, Coleman JN, Wilner JG, et al. Integrated treatment for smoking cessation, anxiety, and depressed mood in people living with HIV: a randomized controlled trial. Journal of Acquired Immune Deficiency Syndromes 2018;79:261‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Ockene 1991 {published data only}
- Ockene JK, Kristeller J, Goldberg R, Amick TL, Pekow PS, Hosmer D, et al. Increasing the efficacy of physician‐delivered smoking interventions: a randomized clinical trial. Journal of General Internal Medicine 1991;6(1):1‐8. [DOI] [PubMed] [Google Scholar]
- Ockene JK, Kristeller J, Pbert L, Hebert JR, Luippold R, Goldberg RJ, et al. The physician‐delivered smoking intervention project: can short‐term interventions produce long‐term effects for a general outpatient population?. Health Psychology 1994;13(3):278‐81. [DOI] [PubMed] [Google Scholar]
Okuyemi 2013 {published data only}
- Goldade K, Jarlais D, Everson‐Rose SA, Guo H, Thomas J, Gelberg L, et al. Knowing quitters predicts smoking cessation in a homeless population. American Journal of Health Behavior 2013;37(4):517‐24. [CENTRAL: 993944; CRS: 9400107000000703; PEER: Reviewed Journal: 2013‐08953‐009; PUBMED: 23985232] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldade K, Whembolua GL, Thomas J, Eischen S, Guo H, Connett J, et al. Designing a smoking cessation intervention for the unique needs of homeless persons: a community‐based randomized clinical trial. Clinical Trials 2011;8(6):744‐54. [CENTRAL: 814647; CRS: 9400123000012422; 6866; PUBMED: 22167112] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okuyemi KS, Goldade K, Whembolua GL, Thomas JL, Eischen S, Guo H, et al. Smoking characteristics and comorbidities in the power to quit randomized clinical trial for homeless smokers. Nicotine & Tobacco Research 2013;15(1):22‐8. [CENTRAL: 814589; CRS: 9400103000000015; EMBASE: 2012756123; PUBMED: 22589422] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Okuyemi KS, Goldade K, Whembolua GL, Thomas JL, Eischen S, Sewali B, et al. Motivational interviewing to enhance nicotine patch treatment for smoking cessation among homeless smokers: a randomized controlled trial. Addiction 2013;108(6):1136‐44. [CENTRAL: 921008; CRS: 9400107000001568; PEER: Reviewed Journal: 2013‐16822‐021; PUBMED: 23510102] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinson CD, Rogers CR, Okuyemi KS. Depression symptoms among homeless smokers: effect of motivational interviewing. Substance Use & Misuse 2016;51(10):1393‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warner C, Sewali B, Olayinka A, Eischen S, Wang Q, Guo H, et al. Smoking cessation in homeless populations: who participates and who does not. Nicotine & Tobacco Research 2014;16(3):369‐72. [CENTRAL: 977672; CRS: 9400129000000793] [DOI] [PMC free article] [PubMed] [Google Scholar]
Otero 2006 {published data only}
- Otero UB, Perez CA, Szklo M, Esteves GA, DePinho MM, Szklo AS, et al. Randomized clinical trial: effectiveness of the cognitive‐behavioral approach and the use of nicotine replacement transdermal patches for smoking cessation among adults in Rio de Janeiro, Brazil [Ensaio clinico randomizado: efetividade da abordagem cognitivo‐comportamental e uso de adesivos transdermicos de reposicao de nicotina, na cessacao de fumar, em adultos residentes no Municipio do Rio de Janeiro, Brasil]. Cadernos de Saude Publica 2006;22:439‐49. [DOI] [PubMed] [Google Scholar]
Patten 2017 {published data only}
- Patten CA, Bronars CA, Vickers Douglas KS, Ussher MH, Levine JA, Tye SJ, et al. Supervised, vigorous intensity exercise intervention for depressed female smokers: a pilot study. Nicotine & Tobacco Research 2017;19(1):77‐86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Prapavessis 2016 {published data only}
- Prapavessis H, Jesus S, Fitzgeorge L, Faulkner G, Maddison R, Batten S. Exercise to enhance smoking cessation: the getting physical on cigarette randomized control trial. Annals of Behavioral Medicine 2016;50(3):358‐69. [DOI] [PubMed] [Google Scholar]
Reid 1999 {published data only}
- D'Angelo ME, Reid RD, Brown KS, Pipe AL. Gender differences in predictors for long‐term smoking cessation following physician advice and nicotine replacement therapy. Canadian Journal of Public Health 2001;92(6):418‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reid RD, Pipe A, Dafoe WA. Is telephone counselling a useful addition to physician advice and nicotine replacement therapy in helping patients to stop smoking? A randomized controlled trial. Canadian Medical Association Journal 1999;160(11):1577‐81. [PMC free article] [PubMed] [Google Scholar]
Rohsenow 2014 {published data only}
- Rohsenow DJ, Martin RA, Monti PM, Colby SM, Day AM, Abrams DB, et al. Motivational interviewing versus brief advice for cigarette smokers in residential alcohol treatment. Journal of Substance Abuse Treatment 2014;46(3):346‐55. [CENTRAL: 959232; CRS: 9400130000000480; EMBASE: 2014038589; PUBMED: 24210533] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rohsenow DJ, Monti PM, Colby SM, Martin RA. Brief interventions for smoking cessation in alcoholic smokers. Alcoholism, Clinical and Experimental Research 2002;26(12):1950‐1. [CENTRAL: 434257; CRS: 9400123000003065; PUBMED: 12500132] [DOI] [PubMed] [Google Scholar]
Rovina 2009 {published data only}
- Rovina N, Nikoloutsou I, Katsani G, Dima E, Fransis K, Roussos C, et al. Effectiveness of pharmacotherapy and behavioral interventions for smoking cessation in actual clinical practice. Therapeutic Advances in Respiratory Disease 2009;3(6):279‐87. [DOI] [PubMed] [Google Scholar]
Schlam 2016 {published data only}
- Schlam TR, Cook JW, Baker TB, Hayes‐Birchler T, Bolt DM, Smith SS, et al. Can we increase smokers' adherence to nicotine replacement therapy and does this help them quit?. Psychopharmacology 2018;235(7):2065‐75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schlam TR, Fiore MC, Smith SS, Fraser D, Bolt DM, Collins LM, et al. Comparative effectiveness of intervention components for producing long‐term abstinence from smoking: a factorial screening experiment. Addiction 2016;111(1):142‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
Schmitz 2007a {published data only}
- Schmitz JM, Stotts AL, Mooney ME, Delaune KA, Moeller GF. Bupropion and cognitive‐behavioral therapy for smoking cessation in women. Nicotine & Tobacco Research 2007;9(6):699‐709. [DOI] [PubMed] [Google Scholar]
Simon 2003 {published data only}
- Simon JA, Carmody TP, Hudes ES, Snyder E, Murray J. Intensive smoking cessation counseling versus minimal counseling among hospitalized smokers treated with transdermal nicotine replacement: a randomized trial. American Journal of Medicine 2003;114(7):555‐62. [DOI] [PubMed] [Google Scholar]
Smith 2001 {published data only}
- Smith SS, Jorenby DE, Fiore MC, Anderson JE, Mielke MM, Beach KE, et al. Strike while the iron is hot: can stepped‐care treatments resurrect relapsing smokers?. Journal of Consulting and Clinical Psychology 2001;69(3):429‐39. [DOI] [PubMed] [Google Scholar]
Smith 2013a {published data only}
- Smith SS, Keller PA, Kobinsky KH, Baker TB, Fraser DL, Bush T, et al. Enhancing tobacco quitline effectiveness: identifying a superior pharmacotherapy adjuvant. Nicotine & Tobacco Research 2013;15(3):718‐28. [DOI] [PMC free article] [PubMed] [Google Scholar]
Smith 2014 {published data only}
- NCT01083654. Menominee stop tobacco abuse renew tradition study. ClinicalTrials.gov/show/NCT01083654 (first received 10 March 2010).
- Smith SS, Rouse LM, Caskey M, Fossum J, Strickland R, Culhane JK, et al. Culturally‐tailored smoking cessation for adult American Indian smokers: a clinical trial. Journal of Counseling Psychology 2014;42(6):852‐86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Solomon 2000 {published data only}
- Solomon LJ, Scharoun GM, Flynn BS, Secker‐Walker RH, Sepinwall D. Free nicotine patches plus proactive telephone peer support to help low‐income women stop smoking. Preventive Medicine 2000;31(1):68‐74. [DOI] [PubMed] [Google Scholar]
Solomon 2005 {published data only}
- Solomon LJ, Marcy TW, Howe KD, Skelly JM, Reinier K, Flynn BS. Does extended proactive telephone support increase smoking cessation among low‐income women using nicotine patches?. Preventive Medicine 2005;40(3):306‐13. [DOI] [PubMed] [Google Scholar]
Stanton 2015 {published data only}
- Stanton CA, Papandonatos GD, Shuter J, Bicki A, Lloyd‐Richardson EE, Dios MA, et al. Outcomes of a tailored intervention for cigarette smoking cessation among Latinos living with HIV/AIDS. Nicotine & Tobacco Research 2015;17(8):975‐82. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stein 2006 {published data only}
- Stein MD, Anderson BJ, Niaura R. Smoking cessation patterns in methadone‐maintained smokers. Nicotine & Tobacco Research 2007;9(3):421‐8. [DOI] [PubMed] [Google Scholar]
- Stein MD, Weinstock MC, Herman DS, Anderson BJ. Respiratory symptom relief related to reduction in cigarette use. Journal of General Internal Medicine 2005;20(10):889‐94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stein MD, Weinstock MC, Herman DS, Anderson BJ, Anthony JL, Niaura R. A smoking cessation intervention for the methadone‐maintained. Addiction 2006;101(4):599‐607. [DOI] [PubMed] [Google Scholar]
Strong 2009 {published data only}
- Strong DR, Kahler CW, Leventhal AM, Abrantes AM, Lloyd‐Richardson E, Niaura R, et al. Impact of bupropion and cognitive‐behavioral treatment for depression on positive affect, negative affect, and urges to smoke during cessation treatment. Nicotine & Tobacco Research 2009;11(10):1142‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Swan 2003 {published data only}
- Jack LM, Swan GE, Thompson E, Curry SJ, McAfee T, Dacey S, et al. Bupropion SR and smoking cessation in actual practice: methods for recruitment, screening, and exclusion for a field trial in a managed‐care setting. Preventive Medicine 2003;36(5):585‐93. [DOI] [PubMed] [Google Scholar]
- Javitz HS, Swan GE, Zbikowski SM, Curry SJ, McAfee TA, Decker DL, et al. Cost‐effectiveness of different combinations of bupropion SR dose and behavioral treatment for smoking cessation: a societal perspective. American Journal of Managed Care 2004;10(3):217‐26. [PubMed] [Google Scholar]
- Swan GE, Jack LM, Curry S, Chorost M, Javitz H, McAfee T, et al. Bupropion SR and counseling for smoking cessation in actual practice: predictors of outcome. Nicotine & Tobacco Research 2003;5(6):911‐21. [DOI] [PubMed] [Google Scholar]
- Swan GE, Jack LM, Javitz HS, McAfee T, McClure JB. Predictors of 12‐month outcome in smokers who received bupropion sustained‐release for smoking cessation. Central Nervous System Drugs 2008;22(3):239‐56. [DOI] [PubMed] [Google Scholar]
- Swan GE, Javitz HS, Jack LM, Curry SJ, McAfee T. Heterogeneity in 12‐month outcome among female and male smokers. Addiction 2004;99(2):237‐50. [DOI] [PubMed] [Google Scholar]
- Swan GE, McAfee T, Curry SJ, Jack LM, Javitz H, Dacey S, et al. Effectiveness of bupropion sustained release for smoking cessation in a health care setting: a randomized trial. Archives of Internal Medicine 2003;163(19):2337‐44. [DOI] [PubMed] [Google Scholar]
- Swan GE, Valdes AM, Ring HZ, Khroyan TV, Jack LM, Ton CC, et al. Dopamine receptor DRD2 genotype and smoking cessation outcome following treatment with bupropion SR. Pharmacogenomics Journal 2005;5(1):21‐9. [DOI] [PubMed] [Google Scholar]
Swan 2010 {published data only}
- Catz SL, Jack LM, McClure JB, Javitz HS, Deprey M, Zbikowski SM, et al. Adherence to varenicline in the COMPASS smoking cessation intervention trial. Nicotine & Tobacco Research 2011;13(5):361‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Halperin AC, McAfee TA, Jack LM, Catz SL, McClure JB, Deprey TM, et al. Impact of symptoms experienced by varenicline users on tobacco treatment in a real world setting. Journal of Substance Abuse Treatment 2009;36(4):428‐34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McClure JB, Jack L, Deprey M, Catz S, McAfee T, Zbikowski S, et al. Canary in a coal mine? Interest in bupropion SR use among smokers in the COMPASS trial. Nicotine & Tobacco Research 2008;10(12):1815‐6. [DOI] [PubMed] [Google Scholar]
- McClure JB, Swan GE, Jack L, Catz SL, Zbikowski SM, McAfee TA, et al. Mood, side‐effects and smoking outcomes among persons with and without probable lifetime depression taking varenicline. Journal of General Internal Medicine 2009;24(5):563‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swan GE, McClure JB, Jack LM, Zbikowski SM, Javitz HS, Catz SL, et al. Behavioral counseling and varenicline treatment for smoking cessation. American Journal of Preventive Medicine 2010;38(5):482‐90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zbikowski SM, Jack LM, McClure JB, Deprey M, Javitz HS, McAfee TA, et al. Utilization of services in a randomized trial testing phone‐ and web‐based interventions for smoking cessation. Nicotine & Tobacco Research 2011;13(5):319‐27. [DOI] [PMC free article] [PubMed] [Google Scholar]
Tonnesen 2006 {published data only}
- Tonnesen P, Mikkelsen K, Bremann L. Nurse‐conducted smoking cessation in patients with COPD using nicotine sublingual tablets and behavioral support. Chest 2006;130(2):334‐42. [DOI] [PubMed] [Google Scholar]
Vander Weg 2016 {published data only}
- NCT01592695. Tailored tobacco quitline for rural veterans. ClinicalTrials.gov/show/NCT01592695 (first received 7 March 2012).
- Vander Weg MW, Cozad AJ, Howren MB, Cretzmeyer M, Scherubel M, Turvey C, et al. An individually‐tailored smoking cessation intervention for rural veterans: a pilot randomized trial. BMC Public Health 2016;16:811. [DOI] [PMC free article] [PubMed] [Google Scholar]
Van Rossem 2017 {published data only}
- Rossem C, Spigt M, Smit ES, Viechtbauer W, Mijnheer KK, Schayck CP, et al. Combining intensive practice nurse counselling or brief general practitioner advice with varenicline for smoking cessation in primary care: study protocol of a pragmatic randomized controlled trial. Contemporary Clinical Trials 2015;41:298‐312. [CENTRAL: 1066790; CRS: 9400131000001477; EMBASE: 2015828707] [DOI] [PubMed] [Google Scholar]
- Rossem C, Spigt M, Viechtbauer W, Lucas AEM, Schayck OCP, Kotz D. Effectiveness of intensive practice nurse counselling versus brief general practitioner advice, both combined with varenicline, for smoking cessation: a randomized pragmatic trial in primary care. Addiction 2017;112(12):2237‐47. [DOI] [PubMed] [Google Scholar]
Vidrine 2016 {published data only}
- Vidrine JI, Businelle MS, Reitzel LR, Cao Y, Cinciripini PM, Marcus MT, et al. Coping mediates the association of mindfulness with psychological stress, affect, and depression among smokers preparing to quit. Mindfulness 2014 [Epub ahead of print]. [CENTRAL: 1038659; CRS: 9400129000001024] [DOI] [PMC free article] [PubMed]
- Vidrine JI, Spears CA, Heppner WL, Reitzel LR, Marcus MT, Cinciripini PM, et al. Efficacy of mindfulness‐based addiction treatment (MBAT) for smoking cessation and lapse recovery: a randomized clinical trial. Journal of Consulting and Clinical Psychology 2016;84(9):824‐38. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wagner 2016 {published data only}
- Wagner FA, Sheikhattari P, Buccheri J, Gunning M, Bleich L, Schutzman C. A community‐based participatory research on smoking cessation intervention for urban communities. Journal of Health Care for the Poor and Underserved 2016;27(1):35‐50. [DOI] [PMC free article] [PubMed] [Google Scholar]
Warner 2016 {published data only}
- Warner DO, Nolan MB, Kadimpati S, Burke MV, Hanson AC, Schroeder DR. Quitline tobacco interventions in hospitalized patients: a randomized trial. American Journal of Preventive Medicine 2016;51(4):473‐84. [DOI] [PubMed] [Google Scholar]
Webb Hooper 2017 {published data only}
- Webb Hooper M, Antoni MH, Okuyemi K, Dietz NA, Resnicow K. Randomized controlled trial of group‐based culturally specific cognitive behavioral therapy among African American smokers. Nicotine & Tobacco Research 2017;19(3):333‐41. [DOI] [PubMed] [Google Scholar]
Wewers 2017 {published data only}
- Nemeth JM, Cooper S, Wermert A, Shoben A, Wewers ME. The relationship between type of telephone service and smoking cessation among rural smokers enrolled in quitline tobacco dependence treatment. Preventive Medicine Reports 2017;8:226‐31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wewers ME, Shoben A, Conroy S, Curry E, Ferketich AK, Murray DM, et al. Effectiveness of two community health worker models of tobacco dependence treatment among community residents of Ohio Appalachia. Nicotine & Tobacco Research 2017;19(12):1499‐507. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wiggers 2006 {published data only}
- Wiggers LC, Oort FJ, Dijkstra A, Haes JC, Legemate DA, Smets EM. Cognitive changes in cardiovascular patients following a tailored behavioral smoking cessation intervention. Preventive Medicine 2005;40(6):812‐21. [DOI] [PubMed] [Google Scholar]
- Wiggers LC, Oort FJ, Peters RJ, Legemate DA, Haes HC, Smets EM. Smoking cessation may not improve quality of life in atherosclerotic patients. Nicotine & Tobacco Research 2006;8(4):581‐9. [DOI] [PubMed] [Google Scholar]
- Wiggers LC, Smets EM, Oort FJ, Peters RJ, Storm‐Versloot MN, Vermeulen H, et al. The effect of a minimal intervention strategy in addition to nicotine replacement therapy to support smoking cessation in cardiovascular outpatients: a randomized clinical trial. European Journal of Cardiovascular Prevention and Rehabilitation 2006;13(6):931‐7. [DOI] [PubMed] [Google Scholar]
- Wiggers LC, Smets EM, Oort FJ, Storm‐Versloot MN, Vermeulen H, Loenen LB, et al. Adherence to nicotine replacement patch therapy in cardiovascular patients. International Journal of Behavioral Medicine 2006;13(1):79‐88. [DOI] [PubMed] [Google Scholar]
Williams 2010 {published data only}
- Williams JM, Steinberg ML, Zimmermann MH, Gandhi KK, Stipelman B, Budsock PD, et al. Comparison of two intensities of tobacco dependence counseling in schizophrenia and schizoaffective disorder. Journal of Substance Abuse Treatment 2010;38(4):384‐93. [DOI] [PMC free article] [PubMed] [Google Scholar]
Wu 2009 {published data only}
- Wu D, Ma GX, Zhou K, Zhou D, Liu A, Poon AN. The effect of a culturally tailored smoking cessation for Chinese American smokers. Nicotine & Tobacco Research 2009;11(12):1448‐57. [DOI] [PMC free article] [PubMed] [Google Scholar]
Yalcin 2014 {published data only}
- Yalcin BM, Unal M, Pirdal H, Karahan TF. Effects of an anger management and stress control program on smoking cessation: a randomized controlled trial. Journal of the American Board of Family Medicine 2014;27(5):645‐60. [CENTRAL: 1014527; CRS: 9400129000003402] [DOI] [PubMed] [Google Scholar]
References to studies excluded from this review
Asfar 2010 {unpublished data only}
- Asfar T, Klesges RC, Sanford SD, Sherrill‐Mittleman D, Robison LL, Hudson MM, et al. Trial design: the St Jude Children's Research Hospital Cancer Survivors Tobacco Quit Line study. Contemporary Clinical Trials 2010;31(1):82‐91. [CENTRAL: 742881; CRS: 9400123000005579; PUBMED: 19766734] [DOI] [PMC free article] [PubMed] [Google Scholar]
Bastian 2013 {published data only}
- Bastian LA, Fish LJ, Peterson BL, Biddle AK, Garst J, Lyna P, et al. Assessment of the impact of adjunctive proactive telephone counseling to promote smoking cessation among lung cancer patients' social networks. American Journal of Health Promotion 2013;27(3):181‐90. [CENTRAL: 921003; CRS: 9400107000000800; PEER: Reviewed Journal: 2013‐01449‐008; PUBMED: 23286595] [DOI] [PubMed] [Google Scholar]
- Bastian LA, Fish LJ, Peterson BL, Biddle AK, Garst J, Lyna P, et al. Proactive recruitment of cancer patients' social networks into a smoking cessation trial. Contemporary Clinical Trials 2011;32(4):498‐504. [CENTRAL: 801365; CRS: 9400123000011889; 39796; PUBMED: 21382509] [DOI] [PMC free article] [PubMed] [Google Scholar]
Batra 2010 {published data only}
- Batra A, Collins SE, Schröter M, Eck S, Torchalla I, Buchkremer G, et al. A cluster‐randomized effectiveness trial of smoking cessation modified for at‐risk smoker subgroups. Journal of Substance Abuse Treatment 2010;38(2):128‐40. [DOI] [PubMed] [Google Scholar]
Bock 2008 {published data only}
- Bock BC, Becker BM, Niaura RS, Partridge R, Fava JL, Trask P. Smoking cessation among patients in an emergency chest pain observation unit: outcomes of the Chest Pain Smoking Study (CPSS). Nicotine & Tobacco Research 2008;10(10):1523‐31. [DOI] [PubMed] [Google Scholar]
Bonevski 2018 {published data only}
- Bonevski B, Twyman L, Paul C, D'Este C, West R, Siahpush M, et al. Smoking cessation intervention delivered by social service organisations for a diverse population of Australian disadvantaged smokers: a pragmatic randomised controlled trial. Preventive Medicine 2018;112:38‐44. [DOI] [PubMed] [Google Scholar]
Borland 2008 {published data only}
- Borland R, Balmford J, Bishop N, Segan C, Piterman L, McKay‐Brown L, et al. In‐practice management versus quitline referral for enhancing smoking cessation in general practice: a cluster randomized trial. Family Practice 2008;25(5):382‐9. [DOI] [PubMed] [Google Scholar]
- McKay‐Brown L, Borland R, Balmford J, Segan CJ, Andrews C, Tasker C, et al. The challenges of recruiting and retaining GPs in research: findings from a smoking cessation project. Australian Journal of Primary Health 2007;13(1):61‐7. [Google Scholar]
Brandon 2017 {published data only}
- Brandon TH, Unrod M, Drobes DJ, Sutton SK, Hawk LW, Simmons VN, et al. Facilitated extinction training to improve pharmacotherapy for smoking cessation: a pilot feasibility trial. Nicotine & Tobacco Research 2017;20(10):1189‐97. [DOI] [PMC free article] [PubMed] [Google Scholar]
Breland 2014 {published data only}
- Breland AB, Almond L, Kienzle J, Ondersma SJ, Hart AJ, Weaver M, et al. Targeting tobacco in a community‐based addiction recovery cohort: results from a computerized, brief, randomized intervention trial. Contemporary Clinical Trials 2014;38(1):113‐20. [CENTRAL: 994445; EMBASE: 2014317617; PUBMED: 24721481] [DOI] [PubMed] [Google Scholar]
Brown 2007 {published data only}
- Brown RA, Niaura R, Lloyd‐Richardson EE, Strong DR, Kahler CW, Abrantes AM, et al. Bupropion and cognitive‐behavioral treatment for depression in smoking cessation. Nicotine & Tobacco Research 2007;9(7):721‐30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strong DR, Kahler CW, Leventhal AM, Abrantes AM, Lloyd‐Richardson E, Niaura R, et al. Impact of bupropion and cognitive‐behavioral treatment for depression on positive affect, negative affect, and urges to smoke during cessation treatment. Nicotine & Tobacco Research 2009;11(10):1142‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
Buchanan 2004 {published data only}
- Buchanan LM, Banna M, White A, Moses S, Siedlik C, Wood M. An exploratory study of multicomponent treatment intervention for tobacco dependency. Journal of Nursing Scholarship 2004;36(4):324‐30. [DOI] [PubMed] [Google Scholar]
Carlin‐Menter 2011 {published data only}
- Carlin‐Menter S, Cummings KM, Celestino P, Hyland A, Mahoney MC, Willett J, et al. Does offering more support calls to smokers influence quit success?. Journal of Public Health Management and Practice 2011;17(3):E9‐15. [DOI] [PubMed] [Google Scholar]
Chandrashekar 2015 {published data only}
- Chandrashekar M, Sattar FA, Bondade S, Kiran Kumar K. A comparative study of different modalities of treatment in nicotine dependence syndrome. Asian Journal of Psychiatry 2015;17:29‐35. [DOI] [PubMed] [Google Scholar]
Chouinard 2005 {published data only}
- Chouinard MC, Robichaud‐Ekstrand S. The effectiveness of a nursing inpatient smoking cessation program in individuals with cardiovascular disease. Nursing Research 2005;54(4):243‐54. [DOI] [PubMed] [Google Scholar]
Christenhusz 2007 {published data only}
- Christenhusz L, Pieterse M, Seydel E, Palen J. Prospective determinants of smoking cessation in COPD patients within a high intensity or a brief counseling intervention. Patient Education & Counseling 2007;66(2):162‐6. [DOI] [PubMed] [Google Scholar]
Cooney 2007 {published data only}
- Cooney N, Pilkey D, Steinberg H, Cooney J, Litt M, Oncken C. Ecological momentary assessment of alcohol‐tobacco interactions after concurrent alcohol‐tobacco treatment. Society for Research on Nicotine and Tobacco 11th Annual Meeting, 20‐23 March 2005; Prague, Czech Republic. 2005.
- Cooney N, Pilkey D, Steinberg H, Cooney J, Litt M, Oncken C. Efficacy of intensive versus brief smoking cessation treatment concurrent with intensive outpatient alcohol treatment. Society for Research on Nicotine and Tobacco 9th Annual Meeting; 2003 February 19‐22; New Orleans, Louisiana. 2003. [POS4‐62]
- Cooney NL, Litt MD, Cooney JL, Pilkey DT, Steinberg HR, Oncken CA. Concurrent brief versus intensive smoking intervention during alcohol dependence treatment. Psychology of Addictive Behaviors 2007;21(4):570‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cooper 2004 {published data only}
- Cooper TV, Debon MW, Stockton M, Klesges RC, Steenbergh TA, Sherrill‐Mittleman D, et al. Correlates of adherence with transdermal nicotine. Addictive Behaviors 2004;29(8):1565‐78. [DOI] [PubMed] [Google Scholar]
Costello 2011 {published data only}
- Costello MJ, Sproule B, Victor JC, Leatherdale ST, Zawertailo L, Selby P. Effectiveness of pharmacist counseling combined with nicotine replacement therapy: a pragmatic randomized trial with 6,987 smokers. Cancer Causes and Control 2011;22(2):167‐80. [DOI] [PubMed] [Google Scholar]
Cropsey 2017 {published data only}
- Cropsey KL, Clark CB, Stevens EN, Schiavon S, Lahti AC, Hendricks PS. Predictors of medication adherence and smoking cessation among smokers under community corrections supervision. Addictive Behaviors 2017;65:111‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cummins 2016 {published data only}
- Cummins SE, Gamst AC, Brandstein K, Seymann GB, Klonoff‐Cohen H, Kirby CA, et al. Helping hospitalized smokers: a factorial RCT of nicotine patches and counseling. American Journal of Preventive Medicine 2016;51(4):578‐86. [DOI] [PMC free article] [PubMed] [Google Scholar]
Dezee 2013 {published data only}
- Dezee KJ, Wink JS, Cowan CM. Internet versus in‐person counseling for patients taking varenicline for smoking cessation. Military Medicine 2013;178(4):401‐5. [CENTRAL: 959429; CRS: 9400130000000072; PUBMED: 23707824] [DOI] [PubMed] [Google Scholar]
Emmons 2013 {published data only}
- Moor JS, Puleo E, Ford JS, Greenberg M, Hodgson DC, Tyc VL, et al. Disseminating a smoking cessation intervention to childhood and young adult cancer survivors: baseline characteristics and study design of the partnership for health‐2 study. BMC Cancer 2011;11:165. [CENTRAL: 836717; CRS: 9400123000011658; PUBMED: 21569345] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Emmons KM, Puleo E, Sprunck‐Harrild K, Ford J, Ostroff JS, Hodgson D, et al. Partnership for health‐2, a web‐based versus print smoking cessation intervention for childhood and young adult cancer survivors: randomized comparative effectiveness study. Journal of Medical Internet Research 2013;15(11):e218. [CENTRAL: 993946; CRS: 9400126000000377; PUBMED: 24195867] [DOI] [PMC free article] [PubMed] [Google Scholar]
Evins 2007 {published data only}
- Evins AE, Cather C, Culhane MA, Birnbaum A, Horowitz J, Hsieh E, et al. A 12‐week double‐blind, placebo‐controlled study of bupropion SR added to high‐dose dual nicotine replacement therapy for smoking cessation or reduction in schizophrenia. Journal of Clinical Psychopharmacology 2007;27:380‐6. [DOI] [PubMed] [Google Scholar]
- NCT00320723. Nicotine replacement therapy for smoking cessation in schizophrenia. ClinicalTrials.gov/show/NCT00320723 (first received 3 May 2006).
Fang 2006 {published data only}
- Fang CY, Ma GX, Miller SM, Tan Y, Su X, Shive S. A brief smoking cessation intervention for Chinese and Korean American smokers. Preventive Medicine 2006;43(4):321‐4. [DOI] [PubMed] [Google Scholar]
Garvey 2012a {published data only}
- Garvey AJ, Hoskinson RA, Wadler BM, Wood EE, Kinnunen T, Kalman D, et al. Effects of front‐loaded vs. standard weekly counseling on 6‐month abstinence rates. Society for Research on Nicotine and Tobacco 13th Annual Meeting; 2007 February 21‐24; Austin, Texas. 2007. [POS1‐66]
- Garvey AJ, Kalman D, Hoskinson RA Jr, Kinnunen T, Wadler BM, Thomson CC, et al. Front‐loaded versus weekly counseling for treatment of tobacco addiction. Nicotine & Tobacco Research 2012;14(5):578‐85. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hall 1996 {published data only}
- Hall SM, Muñoz RF, Reus VI, Sees KL, Duncan C, Humfleet GL, et al. Mood management and nicotine gum in smoking treatment ‐ a therapeutic contact and placebo‐controlled study. Journal of Consulting and Clinical Psychology 1996;64(5):1003‐9. [DOI] [PubMed] [Google Scholar]
Hall 2004 {published data only}
- Hall SM, Humfleet GL, Reus VI, Muñoz RF, Cullen J. Extended nortriptyline and psychological treatment for cigarette smoking. American Journal of Psychiatry 2004;161(11):2100‐7. [DOI] [PubMed] [Google Scholar]
Hall 2011 {published data only}
- Hall SM, Humfleet GL, Muñoz RF, Reus VI, Prochaska JJ, Robbins JA. Using extended cognitive behavioral treatment and medication to treat dependent smokers. American Journal of Public Health 2011;101(12):2349‐56. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hegaard 2003 {published data only}
- Hegaard HK, Kjaergaard H, Møller LF, Wachmann H, Ottesen B. Multimodal intervention raises smoking cessation rate during pregnancy. Acta Obstetricia et Gynecologica Scandinavica 2003;82(9):813‐9. [DOI] [PubMed] [Google Scholar]
Ingersoll 2009 {published data only}
- Ingersoll KS, Cropsey KL, Heckman CJ. A test of motivational plus nicotine replacement interventions for HIV positive smokers. AIDS & Behavior 2009;13(3):545‐54. [DOI] [PMC free article] [PubMed] [Google Scholar]
Japuntich 2006 {published data only}
- Japuntich SJ, Zehner ME, Smith SS, Jorenby DE, Valdez JA, Fiore MC, et al. Smoking cessation via the internet: a randomized clinical trial of an internet intervention as adjuvant treatment in a smoking cessation intervention. Nicotine & Tobacco Research 2006;8 Suppl 1:S59‐67. [DOI] [PubMed] [Google Scholar]
Joseph 2004 {published data only}
- Joseph AM, Nelson DB, Nugent SM, Willenbring ML. Timing of alcohol and smoking cessation (TASC): smoking among substance use patients screened and enrolled in a clinical trial. Journal of Addictive Disease 2003;22(4):87‐107. [DOI] [PubMed] [Google Scholar]
- Joseph AM, Willenbring ML, Nugent SM, Nelson DB. A randomized trial of concurrent versus delayed smoking intervention for patients in alcohol dependence treatment. Journal of Studies on Alcohol 2004;65(6):681‐91. [DOI] [PubMed] [Google Scholar]
Joyce 2008 {published data only}
- Joyce GF, Niaura R, Maglione M, Mongoven J, Larson‐Rotter C, Coan J, et al. The effectiveness of covering smoking cessation services for Medicare beneficiaries. Health Services Research 2008;43(6):2106‐23. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kim 2012 {published data only}
- Kim SS, Kim SH, Ziedonis D. Tobacco dependence treatment for Korean Americans: preliminary findings. Journal of Immigrant and Minority Health 2012;14(3):395‐404. [DOI] [PMC free article] [PubMed] [Google Scholar]
Kinnunen 2008 {published data only}
- Kinnunen T, Leeman RF, Korhonen T, Quiles ZN, Terwal DM, Garvey AJ, et al. Exercise as an adjunct to nicotine gum in treating tobacco dependence among women. Nicotine & Tobacco Research 2008;10(4):689‐703. [DOI] [PMC free article] [PubMed] [Google Scholar]
Klesges 2015 {published data only}
- Berger VW. Randomization, permuted blocks, masking, allocation concealment, and selection bias in the Tobacco Quit Line study. Contemporary Clinical Trials 2010;31(3):201. [CENTRAL: 863870; CRS: 9400123000018617] [DOI] [PubMed] [Google Scholar]
- Klesges RC, Krukowski RA, Klosky JL, Liu W, Srivastava DK, Boyett JM, et al. Efficacy of a tobacco quitline among adult cancer survivors. Preventive Medicine 2015;73:22‐7. [CRS: 9400131000000650; EMBASE: 2015705104; PUBMED: 25572620] [DOI] [PMC free article] [PubMed] [Google Scholar]
Kotz 2009 {published data only}
- Kotz D, Wesseling G, Huibers MJ, Kotz D, Wesseling G, Huibers MJ, et al. Efficacy of confronting smokers with airflow limitation for smoking cessation. European Respiratory Journal 2009;33:754‐62. [DOI] [PubMed] [Google Scholar]
- Kotz D, Wesseling G, Huibers MJ, Schayck OC. Efficacy of confrontational counselling for smoking cessation in smokers with previously undiagnosed mild to moderate airflow limitation: study protocol of a randomized controlled trial. BMC Public Health 2007;7:332. [DOI] [PMC free article] [PubMed] [Google Scholar]
Levine 2010 {published data only}
- Levine MD, Perkins KA, Kalarchian MA, Cheng Y, Houck PR, Slane JD, et al. Bupropion and cognitive behavioral therapy for weight‐concerned women smokers. Archives of Internal Medicine 2010;170(6):543‐50. [DOI] [PMC free article] [PubMed] [Google Scholar]
Marshall 1985 {published data only}
- Marshall A, Raw M. Nicotine chewing gum in general practice: effect of follow up appointments. British Medical Journal 1985;290(6479):1397‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
McCarthy 2016 {published data only}
- McCarthy DE, Bold KW, Minami H, Yeh VM. A randomized clinical trial of a tailored behavioral smoking cessation preparation program. Behaviour Research and Therapy 2016;78:19‐29. [DOI] [PMC free article] [PubMed] [Google Scholar]
Moadel 2012 {published data only}
- Moadel AB, Bernstein SL, Mermelstein RJ, Arnsten JH, Dolce EH, Shuter J. A randomized controlled trial of a tailored group smoking cessation intervention for HIV‐infected smokers. Journal of Acquired Immune Deficiency Syndromes 2012;61(2):208‐15. [CENTRAL: 839925; CRS: 9400123000016203; EMBASE: 2012577962; PEER: Reviewed Journal: 2012‐26825‐008; PUBMED: 22732470] [DOI] [PMC free article] [PubMed] [Google Scholar]
Mochizuki 2004 {published data only}
- Mochizuki M, Hatsugaya M, Rokujoh E, Arita E, Hashiguchi M, Shimizu N, et al. Randomized controlled study on the effectiveness of community pharmacists' advice for smoking cessation by Nicorette ‐ evaluation at three months after initiation. Yakugaku Zasshi 2004;124(12):989‐95. [DOI] [PubMed] [Google Scholar]
NCT00781599 {published data only}
- NCT00781599. Improving medication compliance and smoking cessation treatment outcomes for African American smokers. ClinicalTrials.gov/show/NCT00781599 (first received 29 October 2008).
Nilsson 1996 {published data only}
- Nilsson P, Lundgren H, Söderström M, Fagerström KO, Nilsson Ehle P. Effects of smoking cessation on insulin and cardiovascular risk factors ‐ a controlled study of 4 months' duration. Journal of Internal Medicine 1996;240(4):189‐94. [DOI] [PubMed] [Google Scholar]
Nollen 2007 {published data only}
- Nollen N, Ahluwalia JS, Mayo MS, Richter K, Choi WS, Okuyemi KS, et al. A randomized trial of targeted educational materials for smoking cessation in African Americans using transdermal nicotine. Health Education & Behavior 2007;34(6):911‐27. [CENTRAL: 627383; CRS: 9400123000004636; PUBMED: 17576774] [DOI] [PubMed] [Google Scholar]
Nollen 2011 {published data only}
- Nollen NL, Cox LS, Nazir N, Ellerbeck EF, Owen A, Pankey S, et al. A pilot clinical trial of varenicline for smoking cessation in black smokers. Nicotine & Tobacco Research 2011;13(9):868‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Okuyemi 2006 {published data only}
- Okuyemi KS, Thomas JL, Hall S, Nollen NL, Richter KP, Jeffries SK, et al. Smoking cessation in homeless populations: a pilot clinical trial. Nicotine & Tobacco Research 2006;8(5):689‐99. [DOI] [PubMed] [Google Scholar]
Pakhale 2015 {published data only}
- Pakhale S, Baron J, Armstrong MA, Garde A, Reid RD, Alvarez G, et al. A pilot randomized controlled trial of smoking cessation in an outpatient respirology clinic. Canadian Respiratory Journal 2015;22(2):91‐6. [CRS: 9400131000001433; EMBASE: 2015888546; PUBMED: 25647168] [DOI] [PMC free article] [PubMed] [Google Scholar]
Peckham 2015 {published data only}
- Peckham E, Man MS, Mitchell N, Li J, Becque T, Knowles S, et al. Smoking Cessation Intervention for severe Mental Ill Health Trial (SCIMITAR): a pilot randomised control trial of the clinical effectiveness and cost‐effectiveness of a bespoke smoking cessation service. Health Technology Assessment 2015;19(25):1‐148. [CRS: 9400131000001435; EMBASE: 2015892977; PUBMED: 25827850] [DOI] [PMC free article] [PubMed] [Google Scholar]
Ramon 2013 {published data only}
- Ramon JM, Nerin I, Comino A, Pinet C, Abella F, Carreras JM, et al. A multicentre randomized trial of combined individual and telephone counselling for smoking cessation. Preventive Medicine 2013;57(3):183‐8. [CENTRAL: 871209; CRS: 9400107000001894; EMBASE: 2013515081; PUBMED: 23732247] [DOI] [PubMed] [Google Scholar]
Reid 2007 {published data only}
- Reid RD, Pipe AL, Quinlan B, Oda J. Interactive voice response telephony to promote smoking cessation in patients with heart disease: a pilot study. Patient Education & Counseling 2007;66(3):319‐26. [DOI] [PubMed] [Google Scholar]
Schnoll 2005 {published data only}
- Schnoll RA, Rothman RL, Wielt DB, Lerman C, Pedri H, Wang H, et al. A randomized pilot study of cognitive‐behavioral therapy versus basic health education for smoking cessation among cancer patients. Annals of Behavioral Medicine 2005;30(1):1‐11. [DOI] [PubMed] [Google Scholar]
Severson 2015 {published data only}
- Severson HH, Danaher BG, Ebbert JO, Meter N, Lichtenstein E, Widdop C, et al. Randomized trial of nicotine lozenges and phone counseling for smokeless tobacco cessation. Nicotine & Tobacco Research 2015;17(3):309‐15. [CRS: 9400131000001679] [DOI] [PMC free article] [PubMed] [Google Scholar]
Shiffman 2000 {published data only}
- Shiffman S, Paty JA, Rohay JM, Marino ME, Gitchell J. The efficacy of computer‐tailored smoking cessation material as a supplement to nicotinepolacrilex gum therapy. Archives of Internal Medicine 2000;160(11):1675‐81. [DOI] [PubMed] [Google Scholar]
Shiffman 2001 {published data only}
- Shiffman S, Paty JA, Rohay JM, Marino ME, Gitchell JG. The efficacy of computer‐tailored smoking cessation material as a supplement to nicotine patch therapy. Drug & Alcohol Dependence 2001;64(1):35‐46. [DOI] [PubMed] [Google Scholar]
Sorensen 2003 {published data only}
- Sorensen LT, Jorgensen T. Short‐term preoperative smoking cessation intervention does not affect postoperative complications in colorectal surgery: a randomised clinical trial. Colorectal Disease 2003;5:347‐52. [DOI] [PubMed] [Google Scholar]
Strecher 2005 {published data only}
- Strecher VJ, Shiffman S, West R. Moderators and mediators of a web‐based computer‐tailored smoking cessation program among nicotine patch users. Nicotine & Tobacco Research 2006;8 Suppl 1:S95‐101. [DOI] [PubMed] [Google Scholar]
- Strecher VJ, Shiffman S, West R. Randomized controlled trial of a web‐based computer‐tailored smoking cessation program as a supplement to nicotine patch therapy. Addiction 2005;100(5):682‐8. [DOI] [PubMed] [Google Scholar]
Velicer 2006 {published data only}
- Velicer WF, Friedman RH, Fava JL, Gulliver SB, Keller S, Sun X, et al. Evaluating nicotine replacement therapy and stage‐based therapies in a population‐based effectiveness trial. Journal of Consulting and Clinical Psychology 2006;74(6):1162‐72. [DOI] [PubMed] [Google Scholar]
Vial 2002 {published data only}
- Vial RJ, Jones TE, Ruffin RE, Gilbert AL. Smoking cessation program using nicotine patches linking hospital to the community. Journal of Pharmacy Practice and Research 2002;32(1):57‐62. [Google Scholar]
Ward 2001 {published data only}
- Ward T. Using psychological insights to help people quit smoking. Journal of Advanced Nursing 2001;34(6):754‐9. [DOI] [PubMed] [Google Scholar]
Wilson 1988 {published data only}
- Wilson DM, Taylor DW, Gilbert JR, Best JA, Lindsay EA, Willms DG, et al. A randomized trial of a family physician intervention for smoking cessation. JAMA 1988;260(11):1570‐4. [PubMed] [Google Scholar]
Wolfenden 2005 {published data only}
- Wolfenden L, Wiggers J, Knight J, Campbell E, Rissel C, Kerridge R, et al. A programme for reducing smoking in pre‐operative surgical patients: randomised controlled trial. Anaesthesia 2005;60(2):172‐9. [DOI] [PubMed] [Google Scholar]
Yu 2006 {published data only}
- Yu H, Zang Y, Lin J. The effect of the abstinence from smoking with nicotine replacement therapy combining with psychological and behavior intervention. Zhongguo Kangfu Yixue Zazhi 2006;21(12):1104‐6. [Google Scholar]
Zwar 2015 {published data only}
- Zwar N, Richmond R, Halcomb E, Furler J, Smith J, Hermiz O, et al. Quit in general practice: a cluster randomised trial of enhanced in‐practice support for smoking cessation. BMC Family Practice 2010;11:59. [CENTRAL: 760389; CRS: 9400123000005743; PUBMED: 20701812] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zwar NA, Richmond RL, Halcomb EJ, Furler JS, Smith JP, Hermiz O, et al. Quit in general practice: a cluster randomized trial of enhanced in‐practice support for smoking cessation. Family Practice 2015;32(2):173‐80. [CRS: 9400131000001410; EMBASE: 2015912086; PUBMED: 25670206] [DOI] [PubMed] [Google Scholar]
References to ongoing studies
ACTRN12614000876695 {published data only}
- ACTRN12614000876695. Improving radiotherapy outcomes with smoking cessation: feasibility trial in head and neck cancer patients. www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=366605 (first received 7 July 2014).
Asfar 2018 {published data only}
- Asfar T, Caban‐Martinez AJ, McClure LA, Ruano‐Herreria EC, Sierra D, Gilford Clark G Jr, et al. A cluster randomized pilot trial of a tailored worksite smoking cessation intervention targeting Hispanic/Latino construction workers: intervention development and research design. Contemporary Clinical Trials 2018;67:47‐55. [DOI] [PMC free article] [PubMed] [Google Scholar]
Choi 2011 {published data only}
- Choi WS, Faseru B, Beebe LA, Greiner AK, Yeh HW, Shireman TI, et al. Culturally‐tailored smoking cessation for American Indians: study protocol for a randomized controlled trial. Trials 2011;12:126. [CENTRAL: 799922; CRS: 9400123000011550; 6318; PUBMED: 21592347] [DOI] [PMC free article] [PubMed] [Google Scholar]
Cummins 2012 {published data only}
- Cummins S, Zhu SH, Gamst A, Kirby C, Brandstein K, Klonoff‐Cohen H, et al. Nicotine patches and quitline counseling to help hospitalized smokers stay quit: study protocol for a randomized controlled trial. Trials 2012;13(1):128. [CENTRAL: 853500; CRS: 9400123000015205; EMBASE: 2012559958; PUBMED: 22853197] [DOI] [PMC free article] [PubMed] [Google Scholar]
Garvey 2012b {published data only}
- Garvey AJ, Kalman D, Hoskinson RA, Kinnunen T, Armour CD, Copp S, et al. Effects of extended‐duration counseling vs. shorter‐duration counseling after 1.5 years of follow‐up (POS4‐49). Society for Research on Nicotine and Tobacco 18th Annual Meeting; 2012 March 13‐16; Houston, Texas. 2012:139. [CENTRAL: 814595; CRS: 9400103000000026]
Kim 2017 {published data only}
- Kim SS, Darwish S, Lee SA, Demarco RF. A pilot study of a smoking cessation intervention for women living with HIV: study protocol. Open Access Journal of Clinical Trials 2017;9:11‐20. [Google Scholar]
NCT00851357 {published data only}
- NCT00851357. Telephone counseling and the distribution of nicotine patches to smokers. Clinicaltrials.gov/ct2/show/NCT00851357 (first received 25 February 2009).
NCT00937235 {published data only}
- NCT00937235. Treatment of smoking among individuals with PTSD: a phase II, randomized study of varenicline and cognitive behavioral therapy. clinicaltrials.gov/show/NCT00937235 (first received 10 July 2009). [CRS: 9400131000001780]
NCT00984724 {published data only}
- NCT00984724. Reducing tobacco related health disparities. ClinicalTrials.gov/show/NCT00984724 (first received 25 September 2009).
NCT01063972 {published data only}
- NCT01063972. Smoking cessation in rural hospitals. ClinicalTrials.gov/show/NCT01063972 (first received 5 February 2010).
NCT01098955 {published data only}
- NCT01098955. Smoking cessation treatment for head & neck cancer patients: acceptance and commitment therapy. clinicaltrials.gov/show/NCT01098955 (first received 5 April 2010). [CRS: 9400131000001782]
NCT01162239 {published data only}
- NCT01162239. Maintaining nonsmoking. clinicaltrials.gov/show/NCT01162239 (first received 14 July 2010). [CRS: 9400131000001784]
NCT01186016 {published data only}
- NCT01186016. Developing genetic education for smoking cessation. ClinicalTrials.gov/show/NCT01186016 (first received 20 August 2010).
NCT01257490 {published data only}
- NCT01257490. Integrated smoking cessation treatment for low income community corrections. clinicaltrials.gov/show/NCT01257490 (first received 9 December 2010). [CRS: 9400107000001341]
NCT01736085 {published data only}
- NCT01736085. Providing free nicotine patches to quitline smokers. ClinicalTrials.gov/show/NCT01736085 (first received 29 November 2012).
NCT01800019 {published data only}
- NCT01800019. The Canadian HIV quit smoking trial: tackling the co‐morbidities of depression and cardiovascular disease in HIV+ smokers. clinicaltrials.gov/show/NCT01800019 (first received 27 February 2013). [CRS: 9400129000001211]
NCT01901848 {published data only}
- NCT01901848. CPT and smoking cessation. ClinicalTrials.gov/show/NCT01901848 (first received 17 July 2013).
NCT01965405 {published data only}
- NCT01965405. Smoking cessation for people living with HIV/AIDS. ClinicalTrials.gov/show/NCT01965405 (first received 18 October 2013).
NCT02048917 {published data only}
- NCT02048917. Optimization of smoking cessation strategies in community cancer programs for newly diagnosed lung and head and neck cancer patients. Clinicaltrials.gov/show/NCT02048917 (first received 29 January 2014). [CENTRAL: 1013511; CRS: 9400050000000094]
NCT02164383 {published data only}
- NCT02164383. A quit smoking study using smartphones. clinicaltrials.gov/show/NCT02164383 (first received 16 June 2014). [CRS: 9400131000001038]
NCT02378714 {published data only}
- NCT02378714. Behavioral activation and varenicline for smoking cessation in depressed smokers. Clinicaltrials.gov/ct2/show/NCT02378714 (first received 4 March 2015).
NCT02460900 {published data only}
- NCT02460900. Optimizing smoking cessation for people with HIV/AIDS who smoke. ClinicalTrials.gov/show/NCT02460900 (first recived 3 June 2015).
NCT02767908 {published data only}
- NCT02767908. Hospital to home, smoker support trial. ClinicalTrials.gov/show/NCT02767908 (first received 11 May 2016).
NCT02898597 {published data only}
- NCT02898597. Smoking cessation intervention for women living with HIV. ClinicalTrials.gov/show/NCT02898597 (first received 13 September 2016).
NCT02905656 {published data only}
- NCT02905656. Strategies to promote cessation in smokers who are not ready to quit. ClinicalTrials.gov/show/NCT02905656 (first received 19 September 2016).
NCT03072511 {published data only}
- NCT03072511. Smoking cessation intervention. ClinicalTrials.gov/show/NCT03072511 (first received 7 March 2017).
NCT03342027 {published data only}
- NCT03342027. Smoking cessation interventions for people living with HIV in Nairobi, Kenya. ClinicalTrials.gov/show/NCT03342027 (first received 14 November 2017).
NCT03538938 {published data only}
- NCT03538938. Improving quitline support study. ClinicalTrials.gov/show/NCT03538938 (first received 28 May 2018).
NCT03603496 {published data only}
- NCT03603496. Post‐discharge smoking cessation strategies: helping HAND 4. ClinicalTrials.gov/show/NCT03603496 (first received 27 July 2018).
Ojo‐Fati 2015 {published data only}
- Ojo‐Fati O, John F, Thomas J, Joseph AM, Raymond NC, Cooney NL, et al. Integrating smoking cessation and alcohol use treatment in homeless populations: study protocol for a randomized controlled trial. Trials 2015;16:385. [DOI] [PMC free article] [PubMed] [Google Scholar]
Powers 2016 {published data only}
- Powers MB, Kauffman BY, Kleinsasser AL, Lee‐Furman E, Smits JA, Zvolensky MJ, et al. Efficacy of smoking cessation therapy alone or integrated with prolonged exposure therapy for smokers with PTSD: study protocol for a randomized controlled trial. Contemporary Clinical Trials 2016;50:213‐21. [DOI] [PMC free article] [PubMed] [Google Scholar]
Reid 2011 {published data only}
- Reid RD, Aitken DA, McDonnell L, Armstrong A, Mullen KA, Jones L, et al. Randomized trial of an automated telephone follow‐up system for smoking cessation in smokers with CHD. Canadian Journal of Cardiology 2011;27(5 Suppl 1):S67. [CENTRAL: 814379; CRS: 9400123000012493] [Google Scholar]
Salgado 2018 {published data only}
- Salgado Garcia FI, Derefinko KJ, Bursac Z, Hand S, Klesges RC. Planning A Change Easily (PACE): a randomized controlled trial for smokers who are not ready to quit. Contemporary Clinical Trials 2018;68:14‐22. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vander Weg 2018 {published data only}
- Vander Weg MW, Coday M, Stockton MB, McClanahan B, Relyea G, Read MC, et al. Community‐based physical activity as adjunctive smoking cessation treatment: rationale, design, and baseline data for the Lifestyle Enhancement Program (LEAP) randomized controlled trial. Contemporary Clinical Trials Communications 2018;9:50‐9. [DOI] [PMC free article] [PubMed] [Google Scholar]
Vidrine 2012 {published data only}
- Vidrine DJ, Fletcher FE, Danysh HE, Marani S, Vidrine JI, Cantor SB, et al. A randomized controlled trial to assess the efficacy of an interactive mobile messaging intervention for underserved smokers: Project ACTION. BMC Public Health 2012;12:696. [DOI] [PMC free article] [PubMed] [Google Scholar]
Webb 2018 {published data only}
- Webb Hooper M, Lee DJ, Simmons VN, Brandon KO, Antoni MH, Unrod M, et al. Reducing racial/ethnic tobacco cessation disparities via cognitive behavioral therapy: design of a dualsite randomized controlled trial. Contemporary Clinical Trials 2018;68:127‐32. [DOI] [PubMed] [Google Scholar]
Additional references
Cahill 2016
- Cahill K, Stead LF, Lancaster T. Nicotine receptor partial agonists for smoking cessation. Cochrane Database of Systematic Reviews 2016, Issue 5. [DOI: 10.1002/14651858.CD006103.pub7] [DOI] [PubMed] [Google Scholar]
Cochrane Handbook 2011
- Higgins JP, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.1 [Updated March 2011]. The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Cofta‐Woerpel 2007
- Cofta‐Woerpel L, Wright KL, Wetter DW. Smoking cessation 3: multicomponent interventions. Behavioral Medicine 2007;32(4):135‐49. [DOI] [PubMed] [Google Scholar]
Coleman 2015
- Coleman T, Chamberlain C, Davey MA, Cooper SE, Leonardi‐Bee J. Pharmacological interventions for promoting smoking cessation during pregnancy. Cochrane Database of Systematic Reviews 2015, Issue 12. [DOI: 10.1002/14651858.CD010078.pub2] [DOI] [PubMed] [Google Scholar]
Fiore 2008
- Fiore MC, Jaén CR, Baker TB, Bailey WC, Benowitz NL, Curry SJ, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. AHRQ publication No. 00‐0032. Rockville, MD: US Dept of Health and Human Services, Public Health Services, 2008. [Google Scholar]
Hartmann‐Boyce 2018
- Hartmann‐Boyce J, Chepkin SC, Ye W, Bullen C, Lancaster T. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database of Systematic Reviews 2018, Issue 5. [DOI: 10.1002/14651858.CD000146.pub5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Hartmann‐Boyce 2018a
- Hartmann‐Boyce J, Fanshawe TR, Lindson N, Livingstone‐Banks J, Ordóñez‐Mena J, Aveyard P. Behavioural interventions for smoking cessation: an overview and network meta‐analysis. Cochrane Database of Systematic Reviews 2018, Issue 12. [DOI: 10.1002/14651858.CD013229] [DOI] [PMC free article] [PubMed] [Google Scholar]
Higgins 2003
- Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta‐analyses. BMJ 2003;327(7414):557‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hughes 1995
- Hughes JR. Combining behavioral therapy and pharmacotherapy for smoking cessation: an update. National Institute on Drug Abuse Research Monograph 1995;150:92‐109. [PubMed] [Google Scholar]
Hughes 2010
- Hughes JR, Carpenter MJ, Naud S. Do point prevalence and prolonged abstinence measures produce similar results in smoking cessation studies? A systematic review. Nicotine & Tobacco Research 2010;12(7):756‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Hughes 2014
- Hughes JR, Stead LF, Hartmann‐Boyce J, Cahill K, Lancaster T. Antidepressants for smoking cessation. Cochrane Database of Systematic Reviews 2014, Issue 1. [DOI: 10.1002/14651858.CD000031.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Lancaster 2017
- Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane Database of Systematic Reviews 2017, Issue 3. [DOI: 10.1002/14651858.CD001292.pub3] [DOI] [PubMed] [Google Scholar]
Lindson‐Hawley 2015
- Lindson‐Hawley N, Thompson TP, Begh R. Motivational interviewing for smoking cessation. Cochrane Database of Systematic Reviews 2015, Issue 3. [DOI: 10.1002/14651858.CD006936.pub3] [DOI] [PubMed] [Google Scholar]
Livingstone‐Banks 2019
- Livingstone‐Banks J, Ordóñez‐Mena JM, Hartmann‐Boyce J. Print‐based self‐help interventions for smoking cessation. Cochrane Database of Systematic Reviews 2019, Issue 1. [DOI: 10.1002/14651858.CD001118.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
Livingstone‐Banks 2019a
- Livingstone‐Banks J, Norris E, Hartmann‐Boyce J, West R, Jarvis M, Hajek P. Relapse prevention interventions for smoking cessation. Cochrane Database of Systematic Reviews 2019, Issue 2. [DOI: 10.1002/14651858.CD003999.pub5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Matkin 2019
- Matkin W, Ordóñez‐Mena J, Hartmann‐Boyce J. Telephone counselling for smoking cessation. Cochrane Database of Systematic Reviews 2019, Issue 5. [DOI: 10.1002/14651858.CD002850.pub4] [DOI] [PMC free article] [PubMed] [Google Scholar]
R program [Computer program]
- R Foundation for Statistical Computing. R. Version 3.5.2. R Foundation for Statistical Computing, 2018.
Rice 2017
- Rice VH, Health L, Livingstone‐Banks J, Hartmann‐Boyce J. Nursing interventions for smoking cessation. Cochrane Database of Systematic Reviews 2017, Issue 12. [DOI: 10.1002/14651858.CD001188.pub5] [DOI] [PMC free article] [PubMed] [Google Scholar]
Rigotti 2012
- Rigotti NA, Clair C, Munafò MR, Stead LF. Interventions for smoking cessation in hospitalised patients. Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD001837.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Stead 2016
- Stead LF, Koilpillai P, Fanshawe TR, Lancaster T. Combined pharmacotherapy and behavioural interventions for smoking cessation. Cochrane Database of Systematic Reviews 2016, Issue 3. [DOI: 10.1002/14651858.CD008286.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
Stead 2017
- Stead LF, Carroll AJ, Lancaster T. Group behaviour therapy programmes for smoking cessation. Cochrane Database of Systematic Reviews 2017, Issue 3. [DOI: 10.1002/14651858.CD001007.pub3] [DOI] [PMC free article] [PubMed] [Google Scholar]
West 2007
- West R. The clinical significance of "small" effects of smoking cessation treatments. Addiction 2007;102(4):506‐9. [DOI] [PubMed] [Google Scholar]
West 2010
- West R, Walia A, Hyder N, Shahab L, Michie S. Behavior change techniques used by the English Stop Smoking Services and their associations with short‐term quit outcomes. Nicotine & Tobacco Research 2010;12(7):742‐7. [DOI] [PubMed] [Google Scholar]
Zhu 2000
- Zhu SH, Tedeschi GJ, Anderson CM, Rosbrook B, Byrd M, Johnson CE, et al. Telephone counseling as adjuvant treatment for nicotine replacement therapy in a "Real‐World" setting. Preventive Medicine 2000;31(4):357‐63. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Stead 2012a
- Stead LF, Lancaster T. Behavioural interventions as adjuncts to pharmacotherapy for smoking cessation. Cochrane Database of Systematic Reviews 2012, Issue 2. [DOI: 10.1002/14651858.CD009670] [DOI] [PubMed] [Google Scholar]
Stead 2012b
- Stead LF, Lancaster T. Behavioural interventions as adjuncts to pharmacotherapy for smoking cessation. Cochrane Database of Systematic Reviews 2012, Issue 12. [DOI: 10.1002/14651858.CD009670.pub2] [DOI] [PubMed] [Google Scholar]
Stead 2015
- Stead LF, Koilpillai P, Lancaster T. Additional behavioural support as an adjunct to pharmacotherapy for smoking cessation. Cochrane Database of Systematic Reviews 2015, Issue 10. [DOI: 10.1002/14651858.CD009670.pub3] [DOI] [PubMed] [Google Scholar]