

Abstract
Aim:
The aim of this study was to evaluate the distribution of sealer at different levels of the root canal using three different sealers in a single-cone obturation technique.
Materials and Methods:
Thirty freshly extracted mandibular premolar teeth were selected and access opening was performed. Working length was determined. Cleaning and shaping were done till 25 size K file followed by ProTaper till F2 size. Teeth were then obturated with matching gutta-percha points with the following sealers: Group I, 10 teeth with zinc oxide eugenol sealer; Group II, 10 teeth with AH plus sealer; and Group III, 10 teeth with NanoSeal-S sealer. Teeth were cross sectioned at 3 and 6 mm from the apex. Color photographs of sections were taken at a magnification of ×40 using a camera connected to a stereo-operating microscope and the images were transferred to a computer. Sealer distribution was observed and the canal perimeters coated or uncoated with the sealer can be calculated using a computer digital imaging system.
Results:
Of the three groups, zinc oxide eugenol showed least sealer distribution. AH Plus and Nanoseal-S showed no significant difference between the distribution at the 3- and 6-mm levels.
Conclusion:
Both AH Plus and Nanoseal-S showed excellent sealer distribution when compared to zinc oxide eugenol.
KEYWORDS: AH plus, Nanoseal, sealer, single-cone obturation, stereo-operating microscope
INTRODUCTION
One of the keys to a complete root canal therapy is to adequately obturate the prepared root canal space.[1] Obturation of the canal space has been achieved with gutta-percha and sealer.[2] Ingle and Bakland[3] found that around 60% of endodontic failures were due to the incomplete obturation of the root canal system.
The major aim and objective of obturation was to achieve three-dimensional sealing of the pulp space to create fluid-tight seal and prevent ingress of microorganisms and their toxins[2] and their flow into the periapical tissues.[4] Owing to the complexity of root canal system, numerous techniques and sealers have been innovated to ensure better seal. Ideally, the root canal sealer plays a major role in producing a bond between the core material and the root dentine, effectively preventing leakage.[5] Single-cone method had more sealer distribution than other groups, indicating that the sealer would have been displaced by condensation procedure.[6]
Aim
The aim of this study was to evaluate and compare the distribution of sealer at different levels of the root canal using three different sealers in a single-cone obturation technique.
MATERIALS AND METHODS
Inclusion and exclusion criteria
Thirty freshly extracted human mandibular premolars having single root and single canal with fully formed apices were taken. All teeth with calcifications, immature apices, root fracture, root caries, and root resorption were excluded from the study.
Methodology
All the selected teeth were cleaned to remove calculus and stains. The teeth were immersed in 3% sodium hypochlorite for 5 minutes to remove tissue tags if present and were stored in distilled water to prevent dehydration, until the study was completed.
Sample distribution
Group I: 10 teeth with sealer zinc oxide eugenol.
Group II: 10 teeth with sealer AH Plus.
Group III: 10 teeth with sealer NanoSeal-S.
Root canal preparation
After access opening, the full working length was established with size 15 K-file until the tip of the file was visible at the apical foramen and then subtracting 0.5 mm. Circumferential filing was performed up to size 25 K-file. Further cleaning and shaping were carried out with ProTaper till size F2 and obturated using matching gutta-percha F2 with the three sealers: zinc oxide eugenol, AH Plus, and NanoSeal-S.
Sealer placement
All the sealers were mixed according to the manufacturer’s instructions. A small amount of carbon black powder was added to mixed sealer, which makes it visible after sectioning the roots.[7] The 25-mm lentulo spiral coated with sealer was introduced into the root canal, 1 mm short of the working length, using a slow-speed handpiece. To standardize the length, a visual reference was marked on the lentulo spiral.
Then the gutta-percha cone lightly coated with sealer was gently placed up to the working length and sealed off at cemento enamel junction.
Access cavity was filled with intermediate restorative material and stored in 100% humidity at 37°C for 1 week. Later, using a slow-speed diamond disc, each root was sectioned horizontally at 3 and 6 mm from apex. Color photographs of sections were taken at a magnification of ×40 using a camera connected to a stereo-operating microscope, and the images were then transferred to a computer. Sealer distribution was observed, and the canal perimeters coated or uncoated with the sealer can be calculated using a computer digital imaging system:
Scoring criteria
Scoring criteria include PSCP, mean, standard deviation value, and P value of each group.
Statistical analysis
The obtained results were statistically analyzed using SPSS software, version 18, and the difference between three groups was assessed using analysis of variance followed by post hoc test.
RESULTS
Distribution of sealers at 3 mm from the apex is shown in Figure 1 and at 6 mm in Figure 2. Tables 1–3 show the mean, standard deviation, and P value of each of the three sealers. At 3 mm, there is significant difference between Group I with Group II and Group III and no significant difference between Group II and Group III. At 6 mm, there is significant difference between the three groups
Figure 1.

NanoSeal-S at 3 mm
Figure 2.
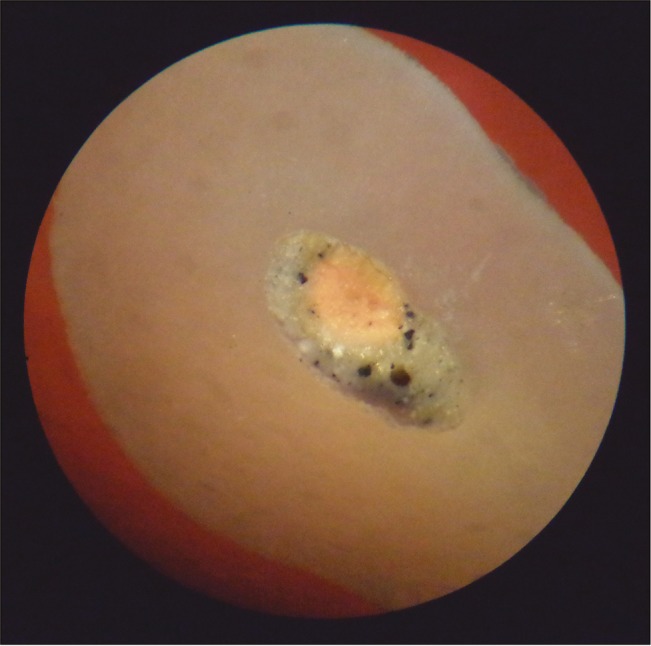
NanoSeal-S at 6 mm
Table 1.
Zinc oxide eugenol
| Levels (mm to apex) | Mean | Standard deviation | P value | Inference |
|---|---|---|---|---|
| 3 | 86.30 | 8.33 | 0.2787 | P > 0.05 |
| 6 | 82.92 | 4.71 | Not significant | |
| 3 + 6 | 84.61 | 6.52 |
Table 3.
NanoSeal-S
| Levels (mm to apex) | Mean | Standard deviation | P value | Inference |
|---|---|---|---|---|
| 3 | 93.63 | 5.43 | 0.3845 | P > 0.05 |
| 6 | 95.20 | 1.24 | Not significant | |
| 3 + 6 | 94.415 | 3.335 |
Table 2.
AH Plus
| Levels (mm to apex) | Mean | Standard deviation | P value | Inference |
|---|---|---|---|---|
| 3 | 92.18 | 2.97 | 0.7864 | P > 0.05 |
| 6 | 91.85 | 2.36 | Not significant | |
| 3 + 6 | 92.015 | 2.665 |
At 3 + 6 mm, there is significant difference between Group I with Group II and Group III and no significant difference between Group II and Group III. Of the three groups, zinc oxide eugenol showed least sealer distribution at 3 mm. AH Plus and NanoSeal-S showed no significant difference between the distribution at the 3 and 6 mm levels.
DISCUSSION
Tight apical seal and three-dimensional obturation are the ultimate objectives of root canal therapy.[8] Gutta-percha is the widely used material that was given by Bowman in 1867,[9] but it alone cannot seal the canal space because it has no adherence to dentin.[10] To achieve fluid-tight apical seal, the sealer should fill the space, irregularities, and minor discrepancies between the gutta-percha and canal wall.[6] Hence, sealer is necessary for the integrity of obturation of canal space.[11] Most studies have shown that the use of sealer results in significantly reduced leakage.[12] Kazemi et al.[13] showed that most of the sealers dissolve over a period[14] but gutta-percha is dimensionally stable. PSCP values reflect the quality of root canal fillings (larger area of gutta-percha requires a smaller area of sealer and results in fewer voids).[15]
Seltzer S, found that particular attention was given to evaluation of sealer distribution in apical 6-mm region because it is the area where accessory canals are most commonly found.[16] Zinc oxide eugenol sealers have been successfully used in root canal obturation for the past 100 years. Zinc oxide eugenol sealer gets resorbed even if extruded into the periapical tissue. It has a prolonged setting time, shrinks on setting, is highly soluble, and can stain the tooth structure. The advantages of zinc oxide eugenol sealer are its antimicrobial activity and popularity among clinicians.[17] Localized inflammation with zinc oxide eugenol sealers is seen both in soft tissue and in the bone.[18] Among various sealers used today, AH plus is popular due to its radiopacity, biocompatibility, ease to use, and availability. It is a bisphenol epoxy resin–based sealer, which also contains adamantine and bonds to root canal.[17] NanoSeal-S is a cold flowable polydimethylsiloxane root canal sealer with nanosilver. Nanosilver enhances antimicrobial efficacy and acts as a preservative. Carbon powder improves the visibility. The rod-shaped active nanoparticles can penetrate the dentinal tubules and enter accessory canals to ensure that all the spaces are effectively sealed.[19]
None of the sealers showed a thorough coating between the gutta-percha and walls of the canal, nor totally filled the spaces between the cones, where the gutta-percha was condensed. The gutta-percha closely adapted to the dentin wall, so the sealer squeezed out from portion, and thus formed voids between the gutta-percha and dentin interface or to the displacement of the compressed gutta-percha.[20]
CONCLUSION
AH plus and NanoSeal-S have excellent apical seal, statistically way much better than zinc oxide eugenol.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Epley SR, Fleischman J, Hartwell G, Cicalese C. Completeness of root canal obturations: Epiphany techniques versus gutta-percha techniques. J Endod. 2006;32:541–4. doi: 10.1016/j.joen.2005.10.059. [DOI] [PubMed] [Google Scholar]
- 2.Michaud R, Burgess J, Barfield R, Cakir D, McNeal S, Eleazer P. Volumetric expansion of gutta-percha in contact with eugenol. J Endod. 2008;34:1528–32. doi: 10.1016/j.joen.2008.08.025. [DOI] [PubMed] [Google Scholar]
- 3.Ingle JI, Bakland LK, editors. Endodontics. 5th ed. Canada: BC Decker Inc; Obturation of the radicular space; p. 571. [Google Scholar]
- 4.James BL, Brown CE, Legan JJ, Moore BK, Vail MM. An in vitro evaluation of the contents of root canals obturated with gutta percha and AH-26 sealer or resilon and epiphany sealer. J Endod. 2007;33:1359–63. doi: 10.1016/j.joen.2007.07.021. [DOI] [PubMed] [Google Scholar]
- 5.Aptekar A, Ginnan K. Comparative analysis of microleakage and seal for 2 obturation materials: Resilon/epiphany and gutta-percha. J Can Dent Assoc. 2006;72:245. [PubMed] [Google Scholar]
- 6.Tegginmani VS, Nalluri JK, Saler S, Dhope SD, Nainani AJ. Sealer distribution in root canals obturated by three techniques—An in vitro study. Endodontology. 2013;25:78–84. [Google Scholar]
- 7.Hall MC, Clement DJ, Dove SB, Walker WA. A comparison of sealer placement techniques in curved canals. J Endod. 1996;22:638–42. doi: 10.1016/S0099-2399(96)80055-0. [DOI] [PubMed] [Google Scholar]
- 8.Schilder H. Filling root canals in three dimensions. Dent Clin North Am. 1967;1:723–44. [PubMed] [Google Scholar]
- 9.Nguyen NT. Obturation of root canal system. In: Cohen S, Burns RC, editors. Pathways of the pulp. 6th ed. St Louis (MO): Mosby; 1991. pp. 219–71. [Google Scholar]
- 10.Green HA, Wong M, Ingram TA., 3rd Comparison of the sealing ability of four obturation techniques. J Endod. 1990;16:423–28. doi: 10.1016/S0099-2399(06)81884-4. [DOI] [PubMed] [Google Scholar]
- 11.Dalat DM, Spångberg LS. Comparison of apical leakage in root canals obturated with various gutta percha techniques using a dye vacuum tracing method. J Endod. 1994;20:315–9. doi: 10.1016/s0099-2399(06)80092-0. [DOI] [PubMed] [Google Scholar]
- 12.De Gee AJ, Wu MK, Wesselink PR. Sealing properties of Ketac-Endo glass ionomer cement and AH26 root canal sealers. Int Endod J. 1994;27:239–44. doi: 10.1111/j.1365-2591.1994.tb00262.x. [DOI] [PubMed] [Google Scholar]
- 13.Kazemi RB, Safavi KE, Spångberg LS. Dimensional changes of endodontic sealers. Oral Surg Oral Med Oral Pathol. 1993;76:766–71. doi: 10.1016/0030-4220(93)90050-e. [DOI] [PubMed] [Google Scholar]
- 14.Wu MK, Ozok AR, Wesselink PR. Sealers distribution in root canals obturated by three techniques. Int Endod J. 2000;33:340–45. doi: 10.1046/j.1365-2591.2000.00309.x. [DOI] [PubMed] [Google Scholar]
- 15.van der Borden WG, Wu MK, Wesselink PR. Percentage of gutta-percha-filled canal area observed after increased apical enlargement. J Endod. 2010;36:139–42. doi: 10.1016/j.joen.2009.08.011. [DOI] [PubMed] [Google Scholar]
- 16.Seltzer S, Bender IB, Ziontz M. The interrelationship of pulp and periodontal disease. Oral Surg Oral Med Oral Pathol. 1963;16:1474–90. doi: 10.1016/0030-4220(63)90385-2. [DOI] [PubMed] [Google Scholar]
- 17.Zhang W, Li Z, Peng B. Ex vivo cytotoxicity of a new calcium silicate-based canal filling material. Int Endod J. 2010;43:769–74. doi: 10.1111/j.1365-2591.2010.01733.x. [DOI] [PubMed] [Google Scholar]
- 18.Gutmann JL, Rakusin H. Perspectives on root canal obturation with thermoplasticized injectable gutta-percha. Int Endod J. 1987;20:261–70. doi: 10.1111/j.1365-2591.1987.tb00625.x. [DOI] [PubMed] [Google Scholar]
- 19.Kumaravadivel MS, Pradeep S. Recent advancements of endodontic sealers—A review. IJPT. 2016;8:4060–75. [Google Scholar]
- 20.Setya G, Nagpal A, Kumar S, Ingle NA. Comparison of root canal sealer distribution in obturated root canal: An in-vitro study. J Int Soc Prev Community Dent. 2014;4:193–7. doi: 10.4103/2231-0762.142028. [DOI] [PMC free article] [PubMed] [Google Scholar]