

Abstract
Background:
Dental caries is the most common chronic disease of children aged 6–11 years. The International Caries Detection and Assessment System—Lesion Activity Assessment (ICDAS-LAA) is a precise tool for the clinical assessment of dental caries by visual appearance, tactile feeling, and potential for plaque accumulation. Ora test is a chairside tool to estimate the ability of acid produced by bacteria to cause demineralization, in a suitable environment. Aim of this study is to correlate ICDAS-LAA and Ora test in assessing the caries risk of a patient on the dental chair.
Materials and Methods:
A total of 60 school children aged between 6 and 9 years were included in the study. Of 60 children, 30 (Group A) were caries free and 30 (Group B) had decayed missing extraction, filled (DMF) score of 1–3. All the children were initially subjected to ICDAS-LAA scoring, which was assessed by one examiner followed by chairside Ora test performed by another examiner.
Results:
Statistical analysis was done using Pearson correlation test, and a negative linear relation was found between the time taken for color change in Ora test and ICDAS-LAA scores.
Conclusion:
A direct correlation exists between ICDAS-LAA scores and Ora test, which shows that microbial activity correlates well with lesion activity.
KEYWORDS: Caries risk assessment, ICDAS-LAA, Ora test
INTRODUCTION
Dental caries is an outcome of interaction between oral environment and the host. The caries process begins with loss of apatite crystals and ends with cavitation. Owing to its multifactorial etiology, dentists are left with surgical restorative interventions and are in need of simple clinical caries detection method with sensitivity and reliability for the early medicine therapeutic approach. In spite of a number of advancements in the diagnostic methods, the detection of an individual at risk for developing caries before its occurrence has limited accomplishments. Currently, most of the caries activity tests are targeting specific microorganisms.[1,2,3]
International Caries Detection and Assessment System—Lesion Activity Assessment (ICDAS-LAA) is one of the methods of assessing the caries risk with combination of three clinical parameters: (1) visual signs of carious lesions (color and severity code); (2) lesion location in an area of plaque stagnation; and (3) surface texture determined by tactile sensation using a WHO probe to gently probe across the lesion (for the presence of rough/soft or smooth/hard surface). Although the procedure is reliable, it is time-consuming and requires prior training for the proper calibration.[4,5]
Most of these caries activity tests are time-consuming and expensive, requiring special equipment, whereas Ora test (OT) is found to be a simple, economical, noninvasive chairside test for estimating the oral microbial level.[6,7] OT is based on the rate of oxygen depletion by microorganisms in expectorated milk samples. The purpose of this study was to correlate ICDAS-LAA scores with that of ora test for the caries risk assessment in children.
MATERIALS AND METHODS
Approval from the institutional ethics committee was obtained. The details of the study were explained to all patients, and a written informed consent was obtained from every child and their parents before the start of the study.
A total of 60 healthy children were randomly selected from the outpatient section of the Department of Pedodontics and Preventive Dentistry. Of the selected 60 children, 30 (Group A) were caries free and 30 (Group B) had DMF score between 1 and 3.
Children who are undergoing orthodontic treatment or on antibiotic therapy, any previous topical fluoride application and children who were physically or mentally handicapped were excluded from this study.
Patients were made to sit comfortably on the dental chair for dental examination. One examiner performed the ICDAS scoring as shown in Figure 1 after proper calibration followed by LAA Figure 2. The ICDAS-LAA assessment was done as shown in Figure 3. Another examiner who was blinded about the ICDAS scores carried out the OT with the armamentarium as shown in Figure 4.
Figure 1.

ICDAS scoring criteria
Figure 2.

LAA scoring criteria
Figure 3.

ICDAS-LAA scoring
Figure 4.

Ora test armamentarium
Principles of Ora test
OT is based on the rate of oxygen depletion by microorganisms in expectorated milk samples. In normal conditions, the bacterial enzyme, aerobic dehydrogenase, transfers electrons or protons to oxygen. Once oxygen gets utilized by the aerobic organisms, methylene blue acts as an electron acceptor and gets reduced to leucomethylene blue. Thus, the reduction of methylene blue reflects the metabolic activity of oral aerobic microorganisms.
The children were asked to rinse their mouth vigorously for 30 seconds with 10 mL of ultrahigh-temperature sterilized cow’s milk (double-toned cow milk, 3% fat, pH 6.5). The expectorated milk was collected in a sterile beaker. Using a disposable syringe, 3 mL of the collected expectorated milk was immediately transferred to a screw cap test tube, which contained 0.12 mL of 0.1% methylene blue (NICE chemicals P. LTD, Kochi, Kerala, India). The expectorated milk and methylene blue were thoroughly mixed, and the test tube was placed on a stand in a well-illuminated area, as shown in Figure 5. A mirror was used to detect any color change from blue to white at the bottom of the test tube at intervals of every 15 minutes for about 3 hours. The time taken for the formation of 6-mm-diameter white ring, as shown in Figure 6, at the bottom of the test tube was recorded.
Figure 5.

Ora test samples
Figure 6.
Ora test showing white ring formation
RESULTS
Table 1 shows the OT values and ICDAS-LAA scores for caries free group (Group A), and Table 2 depicts OT values and ICDAS-LAA scores for carious group (Group B).
Table 1.
Ora test values and ICDAS-LAA scores for caries free group (Group A)
| S. no. | Ora test (time taken in min) | ICDAS-LAA score |
|---|---|---|
| 1A | 165 | 4 |
| 2A | 115 | 4 |
| 3A | 105 | 4.66 |
| 4A | 150 | 0 |
| 5A | 110 | 4.2 |
| 6A | 120 | 4.44 |
| 7A | 130 | 4 |
| 8A | 115 | 4.45 |
| 9A | 120 | 4.2 |
| 10A | 110 | 4 |
| 11A | 105 | 4 |
| 12A | 120 | 4.8 |
| 13A | 100 | 4 |
| 14A | 115 | 4 |
| 15A | 140 | 0 |
| 16A | 115 | 4 |
| 17A | 120 | 4 |
| 18A | 110 | 4.4 |
| 19A | 105 | 4.8 |
| 20A | 120 | 4 |
| 21A | 145 | 4 |
| 22A | 120 | 4 |
| 23A | 150 | 0 |
| 24A | 120 | 4.2 |
| 25A | 135 | 4 |
| 26A | 140 | 4 |
| 27A | 115 | 4 |
| 28A | 115 | 4 |
| 29A | 130 | 0 |
| 30A | 140 | 0 |
ICDAS-LAA = International Caries Detection and Assessment System—Lesion Activity Assessment
Table 2.
Oratest values and ICDAS-LAA scores for carious group (Group B)
| S. no. | Ora test (time taken in min) | ICDAS-LAA score |
|---|---|---|
| 1B | 85 | 6.4 |
| 2B | 90 | 7.2 |
| 3B | 85 | 6.5 |
| 4B | 65 | 7.77 |
| 5B | 85 | 6.67 |
| 6B | 85 | 6.4 |
| 7B | 80 | 7.5 |
| 8B | 65 | 7.2 |
| 9B | 70 | 6.4 |
| 10B | 75 | 6.6 |
| 11B | 85 | 7.77 |
| 12B | 75 | 6.5 |
| 13B | 90 | 6.2 |
| 14B | 90 | 6.4 |
| 15B | 70 | 6.8 |
| 16B | 55 | 8 |
| 17B | 90 | 7.5 |
| 18B | 105 | 6.4 |
| 19B | 85 | 6.6 |
| 20B | 85 | 6 |
| 21B | 120 | 6.5 |
| 22B | 85 | 7.2 |
| 23B | 75 | 7 |
| 24B | 85 | 7 |
| 25B | 85 | 6.8 |
| 26B | 95 | 7 |
| 27B | 110 | 6 |
| 28B | 95 | 6.4 |
| 29B | 65 | 8 |
| 30B | 100 | 7.2 |
ICDAS-LAA = International Caries Detection and Assessment System—Lesion Activity Assessment
The age of children in both the groups ranged between 5 and 9 years. The present study was performed on 60 children: 30 had dental caries and 30 were caries free. The time taken for color change (formation of 6-mm-diameter white ring at the bottom of the test tube) in Group A and Group B and their respective ICDAS-LAA scores are shown in Tables 1 and 2.
Statistical analysis was done using Pearson correlation test. The mean time taken for the change of color from blue to white was 84.33 ± 20.67 minutes and 123.33 ± 45.67 minutes in Group B and Group A, respectively. The difference between the two groups was found to be highly statistically significant at a P value of 0.05, as shown in Graph 1.
Graph 1.
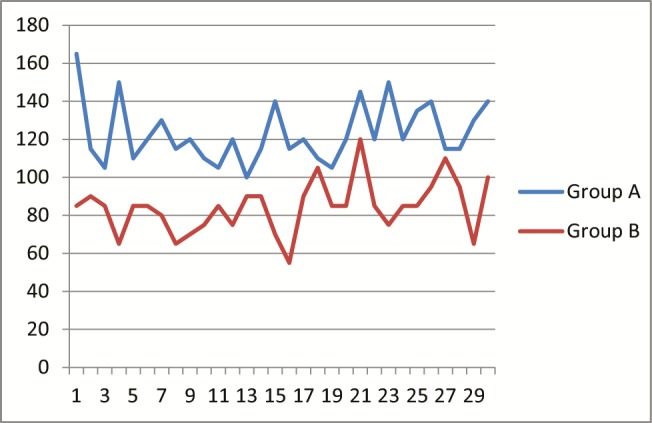
Time taken for color change between the two groups
It can be seen that when the time taken for the change in color increases, the ICDAS-LAA scores decrease, which proves that a negative correlation exists between the two groups and the difference is highly statistically significant, as shown in Graph 2. When the mean values of the two groups were compared (as shown in Table 3), it was found that the mean value of the ICDAS-LAA scores of Group B (6.863666667) was almost double in value than that of mean score of Group A (3.472666667).
Graph 2.
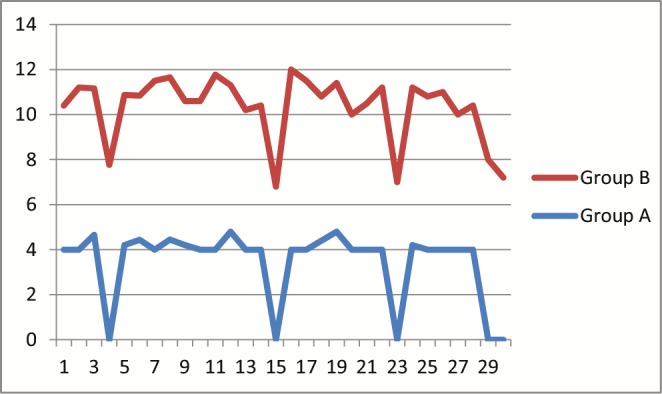
ICDAS-LAA scores between the two groups
Table 3.
Mean values between the two groups
| Time taken | ICDAS-LAA score | |
|---|---|---|
| Group A | 123.333333 | 3.472666667 |
| Group B | 84.3333333 | 6.863666667 |
ICDAS-LAA = International Caries Detection and Assessment System—Lesion Activity Assessment
The mean time taken for the color change in OT was found to be higher in Group A (123.3333333), whereas Group B had a lower mean value (84.3333333), as shown in Table 3.
From this we can infer that the caries status showed a positive linear relationship with ICDAS-LAA scores, whereas a negative linear relationship exists between the caries status and the color change in OT.
DISCUSSION
By definition, dental caries is an infectious and transmissible disease. Unlike most infectious diseases affecting humans, caries is the result of an imbalance of the indigenous oral biota rather than a nonindigenous, exogenous pathogen.[8] The growing interest in the microbiological aspects of dental caries has led to the development of a variety of diagnostic procedures. A number of caries activity tests have been developed to help detect the presence of oral conditions associated with increased caries risk. For individuals, currently no single caries activity test can be relied upon to predict caries with a high degree of confidence. Many of these tests rely on the samples of salivary bacteria. The reliability of such tests is limited because of the free-floating bacteria in the saliva that may not necessarily represent the bacteria in plaque.[9] ICDAS-LAA is used to assess the caries risk by visual appearance, tactile feeling, and potential for plaque accumulation. These tests may also need extensive working time and an expensive armamentarium.
Individual caries activity tests, despite their limitations, can be a useful adjunct to the clinical practitioner, by guiding the clinician in making decisions concerning the need for control measures, the timing of recall appointments, the determination of the prognosis, the types of indicated restorative procedures, and the materials used. A simple, inexpensive technique, which does not demand sophisticated skills or which consumes less chairside time, can help to know the status of the caries activity in a routine clinical practice.[10] The test results can also be used to motivate patients and to determine patient compliance with treatment regimes.
In this comparative study, we have used OT, which is a simple, economical, noninvasive, and less time-consuming test for estimating the oral microbial level along with ICDAS-LAA. Modified Nyvad system of LAA was carried out, which uses a ball-ended probe to gently probe across the surface to assess its texture (rough or smooth) and also to remove the biofilm.[11]
For the present study, 60 children were randomly selected from the Department of Pedodontics and Preventive Dentistry. The ICDAS-LAA scoring was done by one examiner and the results were tabulated before OT was carried out.
OT was carried out by the second examiner who was blinded from the results of the ICDAS-LAA. These samples collected from the subjects in the study were taken only after a lapse of 90 minutes since the last intake of food or drink as it is well known that the correlations can be altered by drinking or eating before the test. The test was based on whole mouth rinsing with sterile milk, which is a suitable vehicle as it dislodges microorganisms mildly yet effectively. It is nontoxic and is readily accepted by the children.
The expectorated milk was then added with the methylene blue and the time taken for the initiation of color change was noted. The time taken for color change of methylene blue to leucomethylene blue was noted and tabulated. When both scores were compared, a significant correlation was found to exist between ICDAS-LAA and OT (P = 0.031). Pearson correlation for intragroup comparison was set at P < 0.05. A negative correlation existed between the time taken for color change for OT and ICDAS-LAA, which indicates that there is a direct correlation between microbial activity and lesion activity.
A similar study conducted on 48 school-going children of Mangalore city by Bhasin et al.[12] to estimate the efficacy of OT found a high statistical significance when the means of control and test groups were compared, and stated that the OT was found to be a simple chairside, less time-consuming, and inexpensive caries activity test.
In another study conducted by Jindal et al.[13] to evaluate caries activity by a simple chairside caries activity test, 90 students were examined: 30 had caries, 30 were children with special health care needs, and 30 were caries free (control group). They found that OT proved to be a simple, inexpensive, and rapid technique for assessing caries activity as statistically highly significant correlation was observed among the three groups.[13]
OT can be easily learnt by the auxiliary personnel, and hence, can be used as a diagnostic tool in school health programs. The positive results can be easily visualized by the practitioner, child, and the parents, and thus can also be used to motivate. As it does not require any special instruments, it can be used to monitor the treatment progress. It can provide a baseline with which subsequent changes in clinical status and oral hygiene (i.e., following oral prophylaxis) can be monitored in a chairside or even in a home environment.
The present study thus proved the hypothesis that higher the level of infection, the lesser was the time taken for the change in color of the expectorate, reflecting higher oral microbial levels, which was in accordance with the findings of Rosenberg et al.[10]
CONCLUSION
OT is a simple and economical chairside assessment tool that can be performed to estimate the caries risk of an individual without any need of specialized training. It serves as an index for the success of therapeutic measures and also helps to motivate and monitor the effectiveness of educational programs relating to dietary and oral hygiene practices.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the Institutional Ethical and Research Committee.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Renuka P, Pushpanjali K, Sangeetha R. Review on influence of host genes on dental caries. IOSR J Dent Med Sci. 2013;4:86–92. [Google Scholar]
- 2.Muthu M MS, Sivakumar N. Paediatric Dentistry: Principles and Practice; Chapter 12. Caries Risk Assessment and caries activity tests. First edition. Elsevier publications; 2009. pp. 137–49. [Google Scholar]
- 3.Yadav K, Prakash S. Dental caries: A microbiological approach. J Clin Infect Dis Pract. 2017;2:1. [Google Scholar]
- 4.Wyne AH, Guile EE. Caries activity indicators. A review. Indian J Dent Res. 1993;4:39–46. [PubMed] [Google Scholar]
- 5.Freitas LA, Santos MT, Guaré RO, Lussi A, Diniz MB. Association between visual inspection, caries activity status, and radiography with treatment decisions on approximal caries in primary molars. Pediatr Dent. 2016;38:140–7. [PubMed] [Google Scholar]
- 6.Rechmann P, Jue B, Santo W, Rechmann BMT, Featherstone JDB. Calibration of dentists for caries management by risk assessment research in a practice based research network —CAMBRA PBRN. BMC Oral Health. 2018;18:1–9. doi: 10.1186/s12903-017-0457-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Arora R, Lahiri PK, Masih U. Oratest: A simple chair side aid for caries risk assessment. Int J Dent Clin. 2009;1:20–2. [Google Scholar]
- 8.Caufield PW, Li Y, Dasanayake A. Dental caries: An infectious and transmissible disease. Compend Contin Educ Dent. 2005;26:10–6. [PubMed] [Google Scholar]
- 9.Sundaram M, Nayak UA, Ramalingam K, Reddy V, Rao AP, Mathian M. A comparative evaluation of Oratest with the microbiological method of assessing caries activity in children. J Pharm Bioallied Sci. 2013;5:S5–9. doi: 10.4103/0975-7406.113283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rosenberg M, Barki M, Portnoy S. A simple method for estimating oral microbial level. J Microbiol Methods. 1989;9:253–256. [Google Scholar]
- 11.Diniz MB, Rodrigues JA, Lussi A. [Accessed online on 08 March 2019];Traditional and novel caries detection methods. https://www.intechopen.com/books/contemporary-approach-to-dental-caries/traditional-and-novelcaries-detection-methods . [Google Scholar]
- 12.Bhasin S, Sudha P, Anegundi R. Chairside simple caries activity test: Ora test. J Indian Soc Pedod Prev Dent. 2006;24:76–9. doi: 10.4103/0970-4388.26020. [DOI] [PubMed] [Google Scholar]
- 13.Jindal R, Dua R, Sachdeva J. Evaluation of caries activity by Oratest. Int J Enhanc Res Med Dent Care. 2016;3:6–10. [Google Scholar]