

Abstract
Thoughts and emotions following marital conflict have received little attention but almost certainly contribute to marriage’s long-term health effects. Consistent with emotion theories of aging, we expected the effects of post-conflict thoughts on important neuroendocrine and immune outcomes, cortisol levels and full-thickness wound healing, to differ by age. An age-diverse sample of married couples received a punch biopsy wound and discussed a marital problem, then privately recorded their thoughts and rated their mood. Salivary cortisol was sampled throughout the day, and wound healing was measured for 32 days. Older adults reported more positive mood post-conflict than younger adults. Thoughts with more positive emotional content related to lower subsequent cortisol levels. Only older adults who expressed more positive thoughts after conflict experienced faster wound healing, not younger adults. These findings point to the increased physiological importance of regulatory post-stressor processes in older age, and broaden our understanding of social-emotional age differences in close relationships. These data also stimulate questions of whether marriage has more widespread health consequences for older partners, undetected in studies of short-term outcomes.
Keywords: marital conflict, aging, post-stressor thoughts, wound healing, health
1. Introduction
Marital quality influences long-term health and longevity, similar to the effect sizes reported for regular exercise and healthy eating (Robles et al., 2014). Mechanistic studies have focused on cardiovascular, endocrine, and immune reactivity to hostility during marital disagreement (Robles et al., 2014). Similar to other stressors’ disruption of wound repair (Broadbent et al., 2003), behaving more negatively during conflict slowed married couples’ blister wound healing (Kiecolt-Glaser et al., 2005). Little is known about the health significance of thoughts and emotions following marital conflict, though improving couples’ conflict reappraisal can successfully curb marital quality decline (Finkel et al., 2013). The current study examined the roles of post-disagreement mood and thoughts in punch biopsy wound healing. Compared to superficial blisters, full-thickness punch biopsy wounds require more time to heal and serve as an important clinical endpoint, particularly for older adults who are more likely to develop chronic wounds and face more serious wound-related consequences (Gould et al., 2015).
1.1. Negative and Positive Thoughts, Stressor Reactivity, and Health
Thoughts and appraisals can amplify reactivity to a stressful event, expedite recovery, and even trigger a stress response in the absence of an external event. Whether a thought is positive or negative, its valence partially determines how constructive it is (Watkins, 2008). More negative thoughts are typically considered unconstructive because they can perpetuate a stressor’s noxious effects (Kashdan and Roberts, 2007; Watkins, 2008). Indeed, a meta-analysis of 60 studies showed that rumination heightened cardiovascular and neuroendocrine reactivity in the lab and in daily life (Ottaviani et al., 2016). People prompted to ruminate after a stressful speech had elevated cortisol one hour later (Zoccola et al., 2014). Higher salivary cortisol accompanied people’s everyday worries about work (Slatcher et al., 2010); cardiovascular reactivity was sustained up to two hours after worry episodes (Pieper et al., 2010).
Conversely, positive thoughts may hasten physiological recovery and protect health. People with human immunodeficiency virus (HIV) who reframed the illness more positively had higher 5-year survival rates and slower HIV progression than less positive thinkers (Ickovics et al., 2006). Low socioeconomic status parents and children who shifted and persisted, i.e. found greater meaning and positively reframed stressors, had lower inflammation and less glucocorticoid insensitivity than those who reframed less (Chen et al., 2015).
Because rumination reactivity has only been examined one to two hours post-stressor (Ottaviani et al., 2016) and positive-thought studies have focused on general self-report measures, studies linking acute post-stressor thoughts to later outcomes will help to assess the viability of thoughts as an explanation for long-term stress-related health risks.
1.2. Age Differences and Their Effects on Stressor Reactivity
According to aging theories, changes in time perspective, motivation, and physiology across adulthood alter affect and stressor reactivity. Socioemotional Selectivity Theory (SST) posits that older adults increasingly value and invest in close relationships to optimize emotional well-being (Carstensen, 1995). According to the Strength and Vulnerability Integration (SAVI) model, through experience, older adults hone the ability to positively reframe challenges, and, thus, can maintain positive affect, minimize negative mood, and circumvent stressor-related health risks (Charles, 2010).
Consistent with SAVI, older adults reported ruminating less and using more positive appraisal compared to their younger counterparts (Scheibe et al., 2016). Furthermore, when older adults were instructed to ruminate, their blood pressure remained higher than younger adults’ and older adults’ in the control condition (Robinette and Charles, 2016). On the other hand, when asked to focus on the positive aspect of upsetting films, older adults did so more successfully and reacted less physiologically compared to a neutral condition (Lohani and Isaacowitz, 2014). Studies addressing age differences have relied largely on emotion-provoking lab tasks, such as showing emotional films, that may lack active engagement and personal relevance for older adults, a disconnect known to produce variable results (Stanley and Isaacowitz, 2015). Marital disagreement, a potent stressor, is an active, personal task that can inform our understanding of age differences in post-stressor processes.
1.3. Age Differences and Marital Conflict
Some evidence exists for age differences in conflict, but we know less about post-conflict thoughts, emotions, and their physiological sequelae. Consistent with theory, older couples express less hostility than middle-aged couples during disagreement (Carstensen et al., 1995), but it is unclear whether they reap health benefits from this relative positivity. In two studies, older couples exhibited lower heart rate reactivity to conflict, but not in other peripheral measures (Levenson et al., 1994; Smith et al., 2009). Older partners may enjoy a larger advantage in their post-conflict thoughts and mood, more controllable than the course of a marital discussion.
1.4. The Current Study
To assess the immune effects of post-stressor marital processes, we examined partners’ post-conflict self-reported mood and emotional content of thoughts as predictors of wound healing in an age-diverse sample of married couples who received a punch biopsy and discussed a marital problem. Cortisol disrupts healing by inhibiting inflammation at the wound site (Ebrecht et al., 2004); thus, we also tested effects on afternoon-evening cortisol, as an intermediate indicator of wound healing relevance. The parent study documented marital conflict’s disruptive effects on blister wound healing (Kiecolt-Glaser et al., 2005). The full-thickness punch biopsy wound was better suited to test the longer-term immune relevance of post-conflict thoughts and feelings, and to probe age differences.
Our first objective was to examine age differences in post-conflict self-reported mood and emotional content of thoughts. Consistent with theory and past empirical evidence (Scheibe et al., 2016), we hypothesized that older adults’ mood would be more positive and less negative; they would also express more positive and fewer negative emotion words post-conflict. The next objective was to examine the effects of post-conflict mood and thoughts on cortisol and wound healing, as well as age differences in these associations. We predicted that more positive and less negative mood and thoughts would relate to lower cortisol levels, as well as faster wound healing (Kiecolt-Glaser et al., 1998). Stronger effects were expected in older adults than younger adults (Lohani and Isaacowitz, 2014; Robinette and Charles, 2016).
2. Method
2.1. Participants
Heterosexual married couples (N = 42; 84 individuals) were recruited for a larger study on marital stress and wound healing through newspaper and radio ads, notices posted on campus and in the community, and referrals from other participants. Couples married fewer than 2 years were ineligible. We excluded couples if either spouse took blood pressure medication, smoked, or used excessive alcohol or caffeine. We also excluded couples with health problems that involved immunological or endocrinological dysfunction, or otherwise had consequences for wound healing (e.g., cancer, recent surgeries, strokes, diabetes mellitus, peripheral vascular disease, conditions such as asthma or arthritis that required regular use of antiinflammatories, etc.). In total, 224 couples were excluded because at least one spouse did not meet our stringent health criteria. The Ohio State University Biomedical Research Review Committee approved the project; all subjects gave written informed consent prior to participation.
The sample ranged in age from 22 to 77 years old (M = 37.0, SD = 13.0) and had been married for 2 – 52 years (M = 12.2, SD = 10.8). More than half were college-educated (66.67%), and most were employed (84.5%) and white (88.1%). Most couples were in their first marriage (85.7%) and had at least one child (70.7%; M = 1.6, SD = 1.3). The parent study was powered to detect the association between marital quality and neuroendocrine and immune outcomes. Specifically, a sample of 76 subjects was required for detecting small to moderate effect sizes (a population squared multiple correlation of .20), using multiple regression analyses with 10 independent variables, a .01 significance level, and a desired power of .80. Past wound healing studies had shown relatively large stress-related effects (Kiecolt-Glaser et al., 1998).
2.2. Data Collection Procedure
Participants completed two full-day study visits at the Clinical Research Center (CRC), a hospital research unit. The procedures and timetable were similar across these two admissions. We asked couples not to drink or eat anything after midnight before admission; all couples were served the same meals in the CRC, thus controlling for dietary factors such as sodium. To assure consistent physical activity across dyads and admissions, couples remained together in the same room.
At the first visit, nurses raised suction blisters on both partners’ arms, then couples engaged in two social support discussions and an oral history interview about their relationship. Biological samples were collected throughout the day. These data are not of direct interest to the current study and are described in detail elsewhere (Kiecolt-Glaser et al., 2005).
At the second visit (M = 2.37 months later), couples arrived at the CRC at 7 AM, and at 9:45 AM received a 2-mm dermal punch biopsy on the upper arm, near the shoulder, a common dermatological research procedure (Nemeth et al., 1991). Trained staff nurses prepared the skin with 70% isopropyl alcohol before injecting lidocaine hydrochloride with 1:100,000 epinephrine, a local anesthetic. After the biopsy was performed (Miltex, Plainsboro, NJ), the nurse used ferric subsulfate solution to stop the bleeding then applied a wound dressing.
Next, couples engaged in a marital problem discussion. Beginning at 11 AM, to initiate the discussion, partners completed a relationship problem inventory and a 20-minute interview to identify conflictual topics (e.g., money, communication, in-laws). At 11:20 AM, couples were given 30 minutes to discuss and try to resolve one or more marital issues that the interviewer judged to be most contentious. Partners then spent 2 minutes in separate rooms speaking into a tape recorder and describing the thoughts they had regarding the problem discussion task. They were assured that responses would not be shared with the spouse. Throughout the day and into the evening (10 PM), partners also provided hourly mood ratings and saliva samples. Following this CRC visit, participants’ punch biopsy wound healing was measured daily for 8 days, and then on days 12, 16, 20, 24, 28, and 32.
2.3. Measures
2.3.1. Post-conflict thoughts.
The thought-listing procedure is applicable for use in examining the most accessible thought processes evoked by any personally significant stimulus or situation. Prior studies of rumination and cognitive-affective coping strategies such as positive reappraisal have successfully used the procedure to assess study manipulations of thoughts (Gerin et al., 2006; Witvliet et al., 2015). As adapted from Petty et al. (1981), participants were given the following instructions:
“We are now interested in what you were thinking about or feeling during your previous discussion of marital issues. During the next two minutes, use the recorder to list what it was you were thinking about or feeling when the two of you were talking. You might have had thoughts or feelings about yourself or your spouse that were positive, or negative, or a mixture, or they might have been irrelevant to the discussion. Don’t worry about grammar or speaking in complete sentences, just state your thoughts and feelings as clearly and concisely as possible. Please list whatever you remember thinking or feeling during the time you were talking with your spouse and be completely honest; your responses will not be shared with your spouse.”
Transcribed thought-listings were processed with Linguistic Inquiry and Word Count (Pennebaker, Austin, TX), text analysis software that produces percentages of words in psychologically relevant categories based on a standardized dictionary. Of interest for the current study were positive and negative emotion words to capture positively and negatively valenced thoughts post-conflict. Evidence supports LIWC as a valid method of capturing emotional valence in unstructured speech, and as distinct from self-reported mood (Kahn et al., 2007). These word counts lack the semantic context that would allow us to measure higher-order cognitive and affective processes such as rumination, benefit-finding, and positive reappraisal. However, positive and negative emotion word use categories are sensitive to strategy-switching, thus suggesting that LIWC categories reflect a component of these more complex constructs. For instance, people’s thoughts contained more negative emotion words and fewer positive emotion words after ruminating compared to after positively reappraising a stressor (Witvliet et al., 2015). Thus, prior work on rumination and positive reappraisal provided the best foundation for understanding and making predictions about the emotional content of couples’ post-conflict thoughts. Accordingly, we also take care to not suggest that couples were ruminating about or positively reappraising the conflict per se, as standard self-report measures of rumination and appraisal were not collected.
2.3.2. Self-rated mood.
Morning and post-conflict positive and negative affect were assessed using the 20-item Positive and Negative Affect Schedule (PANAS, Watson et al., 1988).
2.3.3. Marital satisfaction.
The Marital Adjustment Test (MAT) (Locke and Wallace, 1959), part of the initial phone interviews, is widely used in marital research because of its reliability and validity in discriminating between satisfied and dissatisfied couples.
2.3.4. Problem discussion behavior.
Marital disagreement discussions were coded using the Rapid Marital Interaction Coding System (RMICS), which discriminates well between distressed and nondistressed couples (Heyman, 2004). Distressed marriages are characterized by negative affect, conflictual communication, and poor listening skills. To capture these dimensions in composite indexes, we summed the top 3 RMICS codes in the 11-category hierarchy: psychological abuse (e.g., disgust, contempt, belligerence, as well as nonverbal behaviors like glowering or talking in a threatening or menacing manner), distress-maintaining attributions (e.g., “You’re only being nice so I’ll have sex with you tonight” or “You were being mean on purpose”), and hostility (e.g., criticism, hostile voice tone, or rolling the eyes dramatically), consistent with past approaches (Kiecolt-Glaser et al., 2005). Interrater reliability was acceptable (κ = .63).
2.3.5. Cortisol.
Saliva was collected using a salivette (Sarstedt, Newton, NC), an untreated sterile cotton roll. Each subject’s samples were frozen after collection and analyzed within the same assay using the Cortisol Coat-A-Count radioimmunoassay (Siemens Medical Solutions Diagnostics, Los Angeles, CA). Intra-assay and inter-assay coefficients of variation were 4.3% and 5.2%, respectively. To capture cortisol levels post-conflict, saliva samples collected immediately, 15 minutes after the task, then hourly until 10 PM, were used to calculate area under the curve (AUC) to ground, taking into account the absolute cortisol levels (Pruessner et al., 2003).
2.3.6. Punch biopsy wound healing.
Measurement of transepidermal water loss (TEWL) through human skin provides a noninvasive method to monitor changes in the stratum corneum barrier function of the skin at the punch biopsy site. Because skin can appear intact before TEWL levels return to baseline, TEWL is considered a particularly sensitive measure of healing (Silverman et al., 1989). Following established guidelines (Pinnagoda et al., 1990), a computerized evaporimetry instrument, the DermaLab (CyberDERM, Media, Pa), measured TEWL at the biopsy site and control values from adjacent nonwounded skin, at each of the 14 measurement occasions (baseline during visit, then days 1–8, 12, 16, 20, 24, 28, and 32). After subtracting the average control values from the average daily measurement, AUC was calculated across all points to provide an overall measure of healing (Hirsch et al., 2008) that maximized available data. Missing data were minimal: 90% of participants had at least 10 of the 14 measurements. Those who healed faster would return to baseline more quickly and, therefore, have lower AUC values compared to those who healed more slowly.
2.4. Analytic Approach
Research questions were addressed using linear mixed models, which accounted for within-couple correlation. TEWL AUC was natural-log transformed to better approximate normality of residuals. The Kenward-Roger degrees of freedom adjustment was used to control type I error. Continuous variables were grand-mean-centered for ease of interpretation.
Four models tested age differences in negative and positive post-conflict mood and thoughts. Covariates included sex, marital satisfaction, and observed negative behavior during the conflict to isolate the role of age from general relationship quality and hostility during the interaction. Morning baseline positive mood was controlled in positive post-conflict mood and thoughts models, and negative morning mood was a covariate for negative post-conflict mood and thoughts outcomes. Residuals of each model were examined for non-normality. Models with post-conflict negative mood as outcome had slightly non-normal residuals. Because transforming the variable did not successfully normalize the residual distribution, post-conflict negative mood was left in its raw scale. Nevertheless, results from the mixed models were robust to violations of normality assumptions (Jacqmin-Gadda et al., 2007).
Hypothesized effects for cortisol levels and wound healing were tested in a two-model sequence. Models with punch-biopsy healing AUC as outcome had skewed residuals that were fully corrected by natural-log-transforming this outcome (see Supplemental Figure 1 for the distribution of log-transformed healing AUC). The reduced model contained body mass index (BMI), sex, marital satisfaction, negative behavior during the conflict, age, morning baseline mood, and one of the four predictors of interest: post-conflict positive mood, post-conflict negative mood, post-conflict positive thoughts, or post-conflict negative thoughts. These models examined the individual effects of post-conflict mood and thoughts while testing alternative explanations such as general relationship quality and hostility during the conflict, and accounting for biological confounds such as BMI. Baseline positive moods and post-conflict positive moods were highly correlated (Spearman’s r = 0.70, p<.0001), and thus models with both and only post-conflict positive moods were compared and no significant differences were noticed. In addition to reduced model covariates, full models included all four predictors of interest to ascertain their independent contributions to short- and long-term neuroendocrine and immune outcomes. These models also included use of positive and negative emotion words during the conflict, as calculated by LIWC. Interactions with age were tested to address moderation hypotheses. Non-significant interactions were removed, and significant interactions were investigated using simple slopes at 25, 40, and 60 years of age, corresponding to typical benchmarks for young, middle-aged, and older adulthood. These also approximated the mean and one standard deviation above and below the mean. All analyses were conducted in SAS version 9.4 (Cary, NC).
Because the objective of the study was to examine age differences in the link between post-conflict thoughts and mood and endocrine and immune outcomes, mediation was not of direct interest. However, given cortisol’s biological relevance to wound healing (Kiecolt-Glaser et al., 1998), we explored whether afternoon-evening cortisol explained additional variance in 32-day punch biopsy wound healing beyond predictors in the full model and whether it reduced the effect of post-conflict mood and thoughts. To evaluate the potential age-moderated mediating effect through afternoon-evening cortisol levels, we included a two-way interaction of age by cortisol predicting wound healing.
3. Results
Key study variables and their zero-order correlations are summarized in Table 1.
Table 1.
Description of Key Study Variables
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | M (SD) | Range | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age, years | 37.0 (13.1) | 22 – 77 | |||||||||||||
| 2. BMI, kg/m2 | 0.22* | 26.0 (5.2) | 18.3 – 50.4 | ||||||||||||
| 3. Marital satisfaction | 0.11 | −0.07 | 116.6 (19.8) | 61 – 144 | |||||||||||
| 4. Morning baseline positive mood | 0.23* | 0.13 | 0.02 | 22.3 (8.3) | 10 – 43 | ||||||||||
| 5. Morning baseline negative mood | −0.09 | −0.04 | −0.16 | −0.14 | 11.2 (2.3) | 10 – 25 | |||||||||
| 6. Couple hostile behavior during conflict | 0.23* | 0.22* | −0.28* | 0.05 | 0.06 | 15.0 (15.8) | 0 – 62.5 | ||||||||
| 7. Expressed positive emotion words during conflict | −0.33** | −0.10 | −0.09 | −0.07 | −0.04 | −0.28** | 2.3 (0.8) | 0.7 – 4.6 | |||||||
| 8. Expressed negative emotion words during conflict | −0.24* | −0.15 | −0.07 | −0.28* | 0.02 | −0.054 | 0.31** | 0.9 (0.5) | 0.1 – 3.0 | ||||||
| 9. Post-conflict positive mood | 0.38** | 0.10 | 0.22* | 0.70*** | −0.16 | −0.07 | 0.01 | −0.22* | 22.0 (8.1) | 10 – 46.7 | |||||
| 10. Post-conflict negative mood | −0.07 | −0.19 | −0.32** | 0.06 | 0.30** | 0.26* | −0.01 | −0.01 | −0.04 | 12.9 (4.3) | 10 – 33 | ||||
| 11. Post-conflict positive thoughts | −0.14 | −0.11 | −0.04 | −0.002 | 0.18 | −0.14 | 0.06 | 0.14 | 0.12 | 0.06 | 3.4 (1.7) | 0 – 7.7 | |||
| 12. Post-conflict negative thoughts | −0.20 | 0.05 | −0.03 | 0.02 | −0.03 | 0.09 | 0.17 | 0.39** | 0.05 | 0.17 | 0.03 | 1.6 (1.3) | 0 – 6.3 | ||
| 13. Log-transformed Punch Biopsy Healing | −0.14 | 0.17 | −0.19 | 0.01 | 0.02 | 0.41** | −0.03 | 0.03 | −0.15 | 0.09 | 0.06 | 0.08 | 4.8 (0.9) | 2.5 – 7.2 | |
| 14. Afternoon-Evening Cortisol Levels | −0.27* | −0.25* | −0.05 | −0.14 | 0.09 | −0.24* | 0.11 | 0.14 | −0.11 | −0.16 | −0.23* | 0.07 | −0.004 | 0.8 (0.2) | 0.4 – 1.6 |
Note. All coefficients reflect Spearman’s correlations to account for non-normality in some study variables. N = 84.
p < 0.05
p < 0.01
p < 0.001
3.1. Age Differences on Post-Conflict Mood and Thoughts
As displayed in Table 2, age was significantly associated with post-conflict positive mood. With each year of older age, post-conflict mood was 0.12 units more positive, adjusting for morning baseline positive mood, gender, marital satisfaction, and couple hostile behavior during conflict (p = 0.009). The age effect was not significant in models with post-conflict negative mood and post-conflict positive or negative thoughts in either the reduced or full model, adjusting for the same covariates (all ps > 0.189). Models with standardized coefficients can be found in Supplemental Table 1.
Table 2.
Age Differences on Post-conflict Mood and Thoughts
| Post-conflict positive mood | Post-conflict negative mood | Post-conflict positive thoughts | Post-conflict negative thoughts | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | p | B | SE | p | B | SE | p | B | SE | p | |
| Intercept | 22.006 | 0.550 | <.001 | 12.873 | 0.423 | <.001 | 3.433 | 0.197 | <.001 | 1.632 | 0.164 | <.001 |
| Morning baseline mood | 0.710 | 0.070 | <.001 | 0.647 | 0.188 | 0.001 | 0.019 | 0.026 | 0.463 | −0.085 | 0.068 | 0.219 |
| Gender | 1.248 | 1.119 | 0.268 | 0.651 | 0.768 | 0.402 | 0.259 | 0.40 | 0.520 | 0.199 | 0.273 | 0.470 |
| Marital satisfaction | 0.040 | 0.030 | 0.190 | −0.021 | 0.023 | 0.366 | −0.007 | 0.011 | 0.497 | −0.007 | 0.009 | 0.457 |
| Couple hostile behavior | −0.064 | 0.038 | 0.101 | 0.080 | 0.030 | 0.010 | −0.018 | 0.013 | 0.176 | 0.011 | 0.011 | 0.332 |
| Age | 0.122 | 0.046 | 0.009 | −0.024 | 0.035 | 0.499 | −0.021 | 0.016 | 0.189 | −0.015 | 0.013 | 0.253 |
Note. All models included random couple intercepts.
3.2. Post-Conflict Mood and Thoughts on Afternoon-Evening Cortisol Production
There was a significant main effect of post-conflict positive thoughts on afternoon-evening cortisol production (p = 0.019), adjusting for BMI, gender, marital satisfaction, morning baseline positive mood, couple hostile behavior during conflict, and age. Specifically, each percentage point of more positive thoughts corresponded with 0.042 lower afternoon-evening cortisol AUC. This main effect remained significant in the fully adjusted model (p = 0.022, Table 3). The interaction between age and post-conflict positive thoughts was not significant in either reduced or fully adjusted models (both ps > 0.250). There was a significant two-way interaction between age and post-conflict negative thoughts (p = 0.042) predicting afternoon/evening cortisol production, adjusting for BMI, gender, marital satisfaction, morning baseline negative mood, and couple hostile behavior during conflict. However, this interaction effect was not significant in the fully adjusted model (p = 0.132). The relationships between post-conflict negative or positive mood and afternoon-evening cortisol levels were not significant in either reduced or fully adjusted model (all ps > 0.250). Models with standardized coefficients can be found in Supplemental Table 2.
Table 3.
Post-Conflict Mood and Thoughts on Afternoon-Evening Cortisol Levels
| B | SE | 95% CI | p | |
|---|---|---|---|---|
| Intercept | 0.808 | 0.032 | (0.742, 0.873) | <.001 |
| BMI | −0.012 | 0.006 | (−0.024, 0.0003) | 0.057 |
| Gender | 0.025 | 0.065 | (−0.106, 0.156) | 0.698 |
| Marital satisfaction | −0.001 | 0.002 | (−0.005, 0.002) | 0.516 |
| Morning baseline negative mood | 0.008 | 0.014 | (−0.021, 0.037) | 0.569 |
| Morning baseline positive mood | −0.006 | 0.006 | (−0.018, 0.006) | 0.322 |
| Couple hostile behavior | −0.001 | 0.003 | (−0.006, 0.004) | 0.600 |
| Expressed positive emotion words during conflict | 0.025 | 0.046 | (−0.068, 0.117) | 0.592 |
| Expressed negative emotion words during conflict | 0.005 | 0.074 | (−0.143, 0.153) | 0.949 |
| Age | −0.004 | 0.003 | (−0.010, 0.002) | 0.151 |
| Post-conflict negative mood | −0.002 | 0.009 | (−0.019, 0.015) | 0.820 |
| Post-conflict positive mood | 0.007 | 0.007 | (−0.007, 0.020) | 0.318 |
| Post-conflict negative thoughts | −0.001 | 0.027 | (−0.056, 0.053) | 0.959 |
| Post-conflict positive thoughts | −0.046 | 0.019 | (−0.085, −0.007) | 0.022 |
Note. Depicted is the model fully adjusted for all covariates. Non-significant interactions between post-conflict mood/thoughts and age were removed from final models and were not listed. Model included random couple intercepts.
3.3. Post-Conflict Mood and Thoughts on Punch Biopsy Healing AUC
There was a significant interaction between age and post-conflict positive thoughts (p = 0.038) predicting punch biopsy healing AUC, adjusting for BMI, gender, marital satisfaction, morning baseline positive mood, and couple hostile behavior during conflict. The interaction effect remained significant in the fully adjusted model (p = 0.023, Table 4) and was not gender-specific (age by post-conflict positive thoughts by gender interaction p > .250). Older participants healed faster with increasing post-conflict positive thoughts. As shown in Figure 1, for 60 year-old participants, a 1 percentage-point increment in positive thoughts was associated with a 28.7% lower geometric mean of punch biopsy AUC (95% CI: 1.5% - 48.4%; p = 0.040). In contrast, for young and middle-aged adults (25 or 40 years old, respectively), post-conflict positive thoughts did not relate to wound healing (p = 0.139 and p = 0.316, respectively). The associations between punch biopsy AUC and post-conflict positive or negative mood, as well as post-conflict negative thoughts were not significant in either reduced or fully adjusted models (all ps > 0.250). Variance in wound healing itself did not significantly differ by age (see distribution of age in Supplemental Figure 2; variance in wound healing by age in Supplemental Figure 3). Supplemental Figure 2 shows that among the 84 participants who completed the conflict task, 10.7% (n = 9) were 55 or older, and 16.7% (n = 14) were at least 50 years of age. Models with standardized coefficients can be found in Supplemental Table 3.
Table 4.
Post-Conflict Mood and Thoughts on Punch Biopsy Healing
| B | SE | 95% CI | p | |
|---|---|---|---|---|
| Intercept | 4.707 | 0.117 | (4.467, 4.948) | <.001 |
| BMI | 0.005 | 0.021 | (−0.037, 0.047) | 0.808 |
| Gender | −0.410 | 0.199 | (−0.815, −0.005) | 0.048 |
| Marital satisfaction | −0.011 | 0.006 | (−0.023, 0.002) | 0.090 |
| Morning baseline negative mood | −0.052 | 0.052 | (−0.155, 0.051) | 0.318 |
| Morning baseline positive mood | −0.013 | 0.021 | (−0.056, 0.029) | 0.535 |
| Couple hostile behavior | 0.020 | 0.009 | (0.002, 0.038) | 0.031 |
| Expressed positive emotion words during conflict | 0.242 | 0.164 | (−0.087, 0.570) | 0.146 |
| Expressed negative emotion words during conflict | 0.027 | 0.256 | (−0.487, 0.540) | 0.917 |
| Age | −0.030 | 0.011 | (−0.051, −0.008) | 0.008 |
| Post-conflict negative mood | 0.014 | 0.030 | (−0.045, 0.074) | 0.629 |
| Post-conflict positive mood | 0.025 | 0.025 | (−0.024, 0.074) | 0.310 |
| Post-conflict negative thoughts | −0.053 | 0.093 | (−0.240, 0.133) | 0.570 |
| Post-conflict positive thoughts | −0.035 | 0.067 | (−0.170, 0.100) | 0.604 |
| Age X Post-conflict positive thoughts | −0.013 | 0.006 | (−0.025, −0.002) | 0.023 |
Note. Depicted is the model fully adjusted for all covariates. Outcome punch biopsy healing AUC was natural-log transformed. Non-significant interactions between post-conflict moods/thoughts and age were removed from final model and were not listed. Model included random couple effects.
Figure 1.
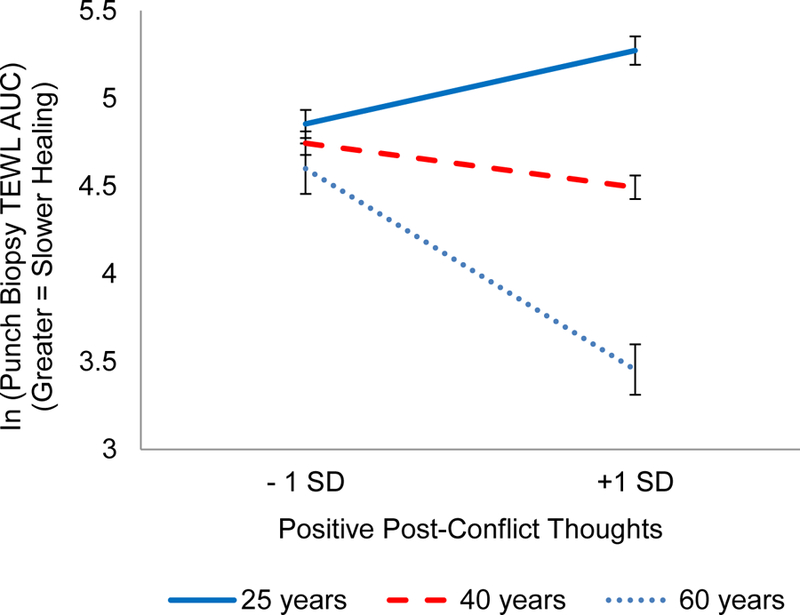
Estimated slope in natural-log transformed punch biopsy healing AUC as a function of post-conflict positive thoughts and age. Results are from a linear mixed model controlling for morning/baseline positive moods, BMI, gender, marital satisfaction, and couple hostile behavior during conflict. Error bars represent + / - 1 standard error.
Consistent with prior work (Kiecolt-Glaser et al, 2005), hostile behavior during the discussion was a statistically significant predictor of slower wound healing (Table 4). The age main effect (a lower order term of the two-way interaction) was also statistically significant. To determine the unconditional effect of age, we removed the age X positive-emotion-word interaction term but kept remaining covariates, which did result in a significant negative estimate, indicating faster wound healing among older adults, likely due to medical exclusions (B = −0.02, SE = 0.01, p = 0.04). However, in the reduced model this effect was not significant (B = −0.01, SE = 0.01, p = 0.09).
3.4. Exploratory Moderated Mediation Analysis
Because of the significant age-moderated effect of post-conflict positive thoughts on punch biopsy healing, and the significant main effect of post-conflict positive thoughts on afternoon-evening cortisol production, we examined whether afternoon-evening cortisol levels mediated the effect of post-conflict positive thoughts on punch biopsy healing. However, including afternoon-evening cortisol AUC as a covariate in the fully adjusted model did not reduce the interaction effect of age by post-conflict positive thoughts on punch biopsy healing. The interaction of age by afternoon-evening cortisol AUC was not significant (p > .250). After removing this non-significant interaction, the main effect of afternoon-evening cortisol AUC was also not significantly related to punch biopsy healing (p > .250).
4. Discussion
Following the marital disagreement, partners who expressed more positive emotion in their privately recorded thoughts had lower cortisol than those who expressed less positive emotion. Only among older adults did more positive thoughts also relate to faster full-thickness wound healing. Thus, not only does negative behavior during marital conflict incite neuroendocrine and immune reactivity (Kiecolt-Glaser et al., 2005; Robles et al., 2014), but also the thoughts that linger after the disagreement uniquely predict these responses. Indeed, the positivity of marriage-relevant thoughts between disagreements may help to explain the health disparities between happy and unhappy couples. Further, the finding that only older adults experienced thoughts’ associations with wound healing may indicate that, with increasing age, health consequences are even more extensive than what are captured in most studies, which often measure outcomes 1–2 hours post-stressor.
Using more positive emotion words in post-conflict thoughts was related to same-day cortisol levels for couples of all ages, whereas associations with wound healing, an objective clinical outcome, were limited to older couples. This finding extends the importance of post-conflict marital processes to health (Finkel et al., 2013), controlling for hostile behavior during disagreement, a powerful predictor of healing (Kiecolt-Glaser et al., 2005). It also provokes questions about whether the risks of conflict and its aftermath accumulate across adulthood, sensitizing older adults’ responses. Alternatively, the inclusion of older couples may amplify marriage’s effects on health outcomes in single-cohort samples. Prior work has found that older couples’ conflict was associated with neuroendocrine reactivity and immune dysfunction (Kiecolt-Glaser et al., 1997), but no such studies have drawn age comparisons. Our older adults’ relatively stronger effects contrast with a previous study that found only young women’s partner support related to baseline IL-6 (Whisman and Sbarra, 2012). In addition to the limitations of those cross-sectional data, generalized self-reports may have been more susceptible to older adults’ positivity bias than our impromptu post-conflict thought-listings.
We expected both positive and negative post-conflict mood and thoughts to predict health outcomes, but effects arose exclusively for positive emotion word use. Positive feelings and thoughts have consistently related to better health, independent of negativity, perhaps by expediting recovery from stressors and promoting health outside the stressor context. Many consequences of the stress response can interfere with wound healing; a few include increased cortisol, heightened catecholamines, lower oxytocin and vasopressin, lower local inflammation, and lower oxygen availability at the wound site (Gouin and Kiecolt-Glaser, 2011; Kiecolt-Glaser et al., 1998). In a tape-stripping wound study, trait positive emotion buffered the slowing effects of a stressful speech task on skin barrier recovery (Robles et al., 2009). Positive thoughts and feelings may also help individuals to avoid unnecessary stressors in daily life (Ong, 2010), thus minimizing barriers to healing. Finally, positivity can encourage restorative health behaviors such as high-quality sleep (Pressman and Cohen, 2005), which in turn promotes wound healing (Gouin and Kiecolt-Glaser, 2011).
Given the many pathways from positivity to better health, it was surprising that self-reported positive mood did not significantly predict post-conflict cortisol or wound healing. This may be due to the presentation bias associated with self-report measures (Fazio and Olson, 2003); our linguistic analysis measured the emotional content of thoughts unobtrusively and, therefore, may have been less subject to such bias. Also, the PANAS captures high-arousal positive mood, for which evidence of stress-related health benefits has been equivocal (Pressman and Cohen, 2005).
The null results for self-reported negative mood and expressed negative emotion post-conflict were similarly unexpected, but also consistent with a few studies that have juxtaposed positive and negative processes in a single model (Monin et al., 2012; Pressman and Cohen, 2012). Positive emotion and thoughts may be comparatively more potent because of their ability to neutralize negativity in the context of a stressor as well as promote restorative effects outside of the stress context. Furthermore, self-reported negative mood and negative emotion words had smaller ranges than the positive factors and, therefore, less statistical power. Couples may have been less cognizant of withholding positive thoughts than disclosing negative ones. Also, post-conflict negative mood was correlated with observed hostile behavior during the disagreement, a strong predictor of wound healing in the present study and prior work (Kiecolt-Glaser et al., 2005).
This study bridges the gap between short-term and longitudinal examinations of positive and negative thoughts. Unlike panel studies with general self-report measures (e.g., Ickovics et al., 2006), our partners freely listed their thoughts post-conflict; thoughts with more positive emotion made a difference after accounting for morning mood, conflict behavior, and emotion words used during disagreement. Events that occur near the time of wounding are uniquely important because they impact the initiation of the immunological wound healing cascade (Kiecolt-Glaser et al., 1998). Accordingly, if post-conflict positive-emotion word use reflects couples’ characteristic emotional responses in their daily lives, these reactions may be perpetuated through their day-to-day interactions (e.g., Robles et al., 2014). Among older couples who have longer histories together, this ripple effect seemed to resonate farther to the clinical endpoint of interest, punch biopsy wound healing.
Theory and selective evidence suggest that older adults dwell on positive stimuli and reframe stressors to maintain emotional well-being. We found inconsistent support for this hypothesis: older partners reported more positive mood after the disagreement than younger partners, but emotion word use and negative self-reported mood did not differ by age. In past marital studies powered to test age differences, older adults’ better marital quality explained their lower negative affect and less expressed anger during disagreement (Carstensen et al., 1995). Our older couples reported more positive mood regardless of their marital satisfaction or how hostilely they behaved. Nevertheless, the socioemotional drive to maintain well-being and emotion regulation expertise did not fully determine older couples’ experience, including the emotional content of post-disagreement thoughts. Accumulating evidence suggests that age differences disappear when a task has personal relevance for all ages, reinforcing the importance of testing theory in real-life scenarios and existing relationships (Stanley and Isaacowitz, 2015).
According to aging theories, older adults suffer greater physiological consequences when forced to face stressors. Yet, their physiological vulnerability to marital conflict has received mixed support (Levenson et al., 1994; Smith et al., 2009). We found that cortisol levels and wound healing depended on post-conflict thoughts, a factor within older adults’ control, in addition to conflict behavior itself. The fact that physiological differences between older and younger couples were only apparent in longer-term wound healing data, not the same-day cortisol response, suggests that biological aging may account for the disparity. It also points to the possibility that, for older adults, more widespread health consequences lurk, uncaptured in short-term outcome studies. Couples were selected based on strict health criteria (e.g., excluding diabetes, peripheral vascular disease, and other comorbidities disruptive to healing), so the study’s older couples were particularly healthy compared to their peers. Thus, chronically ill couples’ outcomes could be even poorer than results suggest (Kiecolt-Glaser and Wilson, in press). This explanation also likely accounts for older adults’ trend toward faster healing. Older adults’ greater sensitivity to post-conflict thoughts highlights the importance of managing thoughts after unavoidable stressors in older age, though consequences may not manifest immediately. As discussed, older adults’ more positive mood after conflict did not translate to cortisol and wound healing benefits—consistent with the weaker correspondence between mood changes and physiological reactivity (Denson et al., 2009) compared to post-event thoughts.
Afternoon-evening cortisol did not statistically mediate the association between positive thoughts and wound healing. Although the biological relationship is known—that cortisol production hinders wound healing (Kiecolt-Glaser et al., 1998)—this path was not of primary interest because the exact functional form of the association across days is unknown. Simulations suggest that mismatch between change processes and measurement designs is problematic, especially in mediation (Collins, 2006).
Although we chose to focus on thoughts’ emotional valence, their concreteness also has theoretical importance (Watkins, 2008). However, the LIWC operational definition of concreteness-abstractness has not been well-established, one limitation. One study found that more abstract language contained fewer articles, numbers, and human references, but correlations were only moderate (Beukeboom et al., 2012). Next, we cannot draw conclusions about engaging in conflict versus not; all participants completed the disagreement task. A neutral condition would be required to determine whether positive appraisal after conflict is, in fact, more beneficial for health than no disagreement. Like most studies of age differences in marital processes (e.g., Smith et al., 2009), older couples had also been married longer; therefore, we cannot separate the effects of age from the length of time together. Nevertheless, older couples married for many years are population-representative. The PANAS best captures high-arousal affect (Pressman and Cohen, 2012), which may have accounted for self-reported mood’s null associations. As well, future studies should test age differences with a larger number of older adults, especially for other health outcomes: 14 participants were at least 50 years old, and 9 were 55 or older. Though these are modest subsamples, they are comparable in size to those of studies demonstrating robust effects of stress on wound healing, e.g., in a sample of 11 dental students (mean age = 24.36, Marucha et al., 1998). Because psychosocial stress’s effects on wound healing are quite large even among young people (Kiecolt-Glaser et al., 1998), it was plausible to detect wound healing effects among a small group of older adults. Last, we cannot comprehensively address the biopsychosocial processes that link post-conflict thoughts to month-long wound healing—whether they are attributable to biological dysregulation, or reflect repetitive psychosocial patterns that hinder healing.
In this study of wound healing and marital disagreement, we found that partners of all ages whose thoughts contained more positive emotion after conflict produced less cortisol; older partners who used more positive emotion words also healed faster. Contrary to aging theory, age differences were limited to more positive post-conflict subjective mood among older partners, which did not confer health benefits. On the other hand, older partners’ physiological sensitivity to post-conflict positive thoughts underscores the increased importance of regulatory post-stressor processes in older age. This finding also sparks questions of whether marriage has more widespread health consequences for older partners, undetected in studies of short-term outcomes.
Supplementary Material
Acknowledgments
Support included NIH grants P01 AG16321, P50 DE13749, K05 CA172296, T32 DE014320, UL1RR025755 and a Pelotonia Postdoctoral Fellowship from Ohio State University’s Comprehensive Cancer Center.
References
- Beukeboom CJ, Tanis M, Vermeulen IE, 2012. The Language of Extraversion: Extraverted People Talk More Abstractly, Introverts Are More Concrete. Journal of Language and Social Psychology 32, 191–201. [Google Scholar]
- Broadbent E, Petrie KJ, Alley PG, Booth RJ, 2003. Psychological stress impairs early wound repair following surgery. Psychosomatic Medicine 65, 865–869. [DOI] [PubMed] [Google Scholar]
- Carstensen LL, 1995. Evidence for a Life-Span Theory of Socioemotional Selectivity. Current Directions in Psychological Science 4, 151–156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carstensen LL, Gottman JM, Levenson RW, 1995. Emotional behavior in long-term marriage. Psychology and Aging 10, 140–149. [DOI] [PubMed] [Google Scholar]
- Charles ST, 2010. Strength and vulnerability integration: A model of emotional well-being across adulthood. Psychological Bulletin 136, 1068–1091. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen E, McLean KC, Miller GE, 2015. Shift-and-Persist Strategies. Psychosomatic Medicine 77, 371–382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins LM, 2006. Analysis of Longitudinal Data: The Integration of Theoretical Model, Temporal Design, and Statistical Model. Annual Review of Psychology 57, 505–528. [DOI] [PubMed] [Google Scholar]
- Denson TF, Spanovic M, Miller N, 2009. Cognitive appraisals and emotions predict cortisol and immune responses: a meta-analysis of acute laboratory social stressors and emotion inductions. Psychol Bull 135, 823–853. [DOI] [PubMed] [Google Scholar]
- Ebrecht M, Hextall J, Kirtley LG, Taylor A, Dyson M, Weinman J, 2004. Perceived stress and cortisol levels predict speed of wound healing in healthy male adults. Psychoneuroendocrinology 29, 798–809. [DOI] [PubMed] [Google Scholar]
- Fazio RH, Olson MA, 2003. Implicit measures in social cognition. research: their meaning and use. Annu Rev Psychol 54, 297–327. [DOI] [PubMed] [Google Scholar]
- Finkel EJ, Slotter EB, Luchies LB, Walton GM, Gross JJ, 2013. A brief intervention to promote conflict reappraisal preserves marital quality over time. Psychol Sci 24, 1595–1601. [DOI] [PubMed] [Google Scholar]
- Gerin W, Davidson KW, Christenfeld NJ, Goyal T, Schwartz JE, 2006. The role of angry rumination and distraction in blood pressure recovery from emotional arousal. Psychosom Med 68, 64–72. [DOI] [PubMed] [Google Scholar]
- Gouin J-P, Kiecolt-Glaser JK, 2011. The Impact of Psychological Stress on Wound Healing: Methods and Mechanisms. Immunology and allergy clinics of North America 31, 81–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gould L, Abadir P, Brem H, Carter M, Conner-Kerr T, Davidson J, DiPietro L, Falanga V, Fife C, Gardner S, Grice E, Harmon J, Hazzard WR, High KP, Houghton P, Jacobson N, Kirsner RS, Kovacs EJ, Margolis D, McFarland Horne F, Reed MJ, Sullivan DH, Thom S, Tomic-Canic M, Walston J, Whitney JA, Williams J, Zieman S, Schmader K, 2015. Chronic wound repair and healing in older adults: current status and future research. J Am Geriatr Soc 63, 427–438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heyman RE, 2004. Rapid Marital Interaction Coding System (RMICS), in: Kerig PK, Baucom DH (Eds.), Couple Observational Coding Systems Lawrence Erlbaum Associates, Nahwah, New Jersey, pp. 67–94. [Google Scholar]
- Hirsch T, Ashkar W, Schumacher O, Steinstraesser L, Ingianni G, Cedidi C, 2008. Moist exposed burn ointment (MEBO) in partial thickness burns. European Journal of Medical Research 13, 505–510. [PubMed] [Google Scholar]
- Ickovics JR, Milan S, Boland R, Shoenbaum E, Schuman P, Vlahov D, 2006. Psychological resources protect health: 5-year survival and immune function among HIV-infected women from four US cities. AIDS 20, 1851–1860. [DOI] [PubMed] [Google Scholar]
- Jacqmin-Gadda H, Sibillot S, Proust C, Molina J-M, Thiébaut R, 2007. Robustness of the linear mixed model to misspecified error distribution. Computational Statistics & Data Analysis 51, 5142–5154. [Google Scholar]
- Kahn JH, Tobin RM, Massey AE, Anderson JA, 2007. Measuring emotional expression with the Linguistic Inquiry and Word Count. The American Journal of Psychology 120, 263–286. [PubMed] [Google Scholar]
- Kashdan TB, Roberts JE, 2007. Social anxiety, depressive symptoms, and post-event rumination: affective consequences and social contextual influences. J Anxiety Disord 21, 284–301. [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, Glaser R, Cacioppo JT, MacCallum RC, Snydersmith M, Cheongtag K, Malarkey WB, 1997. Marital conflict in older adults: Endocrinological and immunological correlates. Psychosomatic Medicine 59, 339–349. [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, Loving TJ, Stowell JR, Malarkey WB, Lemeshow S, Dickinson SL, Glaser R, 2005. Hostile marital interactions, proinflammatory cytokine production, and wound healing. Arch. Gen. Psychiatry 62, 1377–1384. [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, Page GG, Marucha PT, MacCallum RC, Glaser R, 1998. Psychological influences on surgical recovery: Perspectives from psychoneuroimmunology. American Psychologist 53, 1209–1218. [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, Wilson SJ, in press Lovesick: How couples’ relationships influence health. Annual Review of Clinical Psychology 17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Levenson RW, Carstensen LL, Gottman JM, 1994. The Influence of Age and Gender on Affect, Physiology, and Their Interrelations: A Study of Long-Term Marriages. Interpersonal Relations and Group Processes 67, 56–68. [DOI] [PubMed] [Google Scholar]
- Locke HJ, Wallace KM, 1959. Short marital adjustment and prediction tests: Their reliability and validity. Marriage and Family Living 21, 251–255. [Google Scholar]
- Lohani M, Isaacowitz DM, 2014. Age differences in managing response to sadness elicitors using attentional deployment, positive reappraisal and suppression. Cogn Emot 28, 678–697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marucha PT, Kiecolt-Glaser JK, Favagehi M, 1998. Mucosal wound healing is impaired by examination stress. Psychosom Med 60, 362–365. [DOI] [PubMed] [Google Scholar]
- Monin JK, Schulz R, Lemay EP, Cook TB, 2012. Linguistic markers of emotion regulation and cardiovascular reactivity among older caregiving spouses. Psychology and Aging 27, 903–911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ong AD, 2010. Pathways Linking Positive Emotion and Health in Later Life. Current Directions in Psychological Science 19, 358–362. [Google Scholar]
- Ottaviani C, Thayer JF, Verkuil B, Lonigro A, Medea B, Couyoumdjian A, Brosschot JF, 2016. Physiological concomitants of perseverative cognition: A systematic review and meta-analysis. Psychol Bull 142, 231–259. [DOI] [PubMed] [Google Scholar]
- Petty RE, Cacioppo JT, Goldman R, 1981. Personal involvement as a determinant of argument-based persuasion. Journal of Personality and Social Psychology 41, 847–855. [Google Scholar]
- Pieper S, Brosschot JF, van der Leeden R, Thayer JF, 2010. Prolonged cardiac effects of momentary assessed stressful events and worry episodes. Psychosom Med 72, 570–577. [DOI] [PubMed] [Google Scholar]
- Pinnagoda J, Tupker RA, Agner T, Serup J, 1990. Guidelines for transepidermal water loss (TEWL) measurement. Contact Dermatitis 22, 164–178. [DOI] [PubMed] [Google Scholar]
- Pressman SD, Cohen S, 2005. Does positive affect influence health? Psychol Bull 131, 925–971. [DOI] [PubMed] [Google Scholar]
- Pressman SD, Cohen S, 2012. Positive emotion word use and longevity in famous deceased psychologists. Health Psychol 31, 297–305. [DOI] [PubMed] [Google Scholar]
- Pruessner JC, Kirschbaum C, Meinlschmid G, Hellhammer DH, 2003. Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 28, 916–931. [DOI] [PubMed] [Google Scholar]
- Robinette JW, Charles ST, 2016. Age, Rumination, and Emotional Recovery From a Psychosocial Stressor. J Gerontol B Psychol Sci Soc Sci 71, 265–274. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robles TF, Brooks KP, Pressman SD, 2009. Trait positive affect buffers the effects of acute stress on skin barrier recovery. Health Psychology 28, 373–378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robles TF, Slatcher RB, Trombello JM, McGinn MM, 2014. Marital quality and health: A meta-analytic review. Psychological Bulletin 140, 140–187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scheibe S, Spieler I, Kuba K, 2016. An Older-Age Advantage? Emotion Regulation and Emotional Experience After a Day of Work. Work, Aging and Retirement 2, 307–320. [Google Scholar]
- Silverman RA, Lender J, Elmets CA, 1989. Effects of occlusive and semiocclusive dressings on the return of barrier function to transepidermal water loss in standardized human wounds. Journal of the American Academy of Dermatology 20, 755–760. [DOI] [PubMed] [Google Scholar]
- Slatcher RB, Robles TF, Repetti RL, Fellows MD, 2010. Momentary Work Worries, Marital Disclosure, and Salivary Cortisol Among Parents of Young Children. Psychosomatic Medicine 72, 887–896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith TW, Uchino BN, Berg CA, Florsheim P, Pearce G, Hawkins M, Henry NJM, Beveridge RM, Skinner MA, Ko KJ, Olsen-Cerny C, 2009. Conflict and collaboration in middle-aged and older couples: II. Cardiovascular reactivity during marital interaction. Psychology and Aging 24, 274–286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanley JT, Isaacowitz DM, 2015. Caring more and knowing more reduces age-related differences in emotion perception. Psychol Aging 30, 383–395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watkins ER, 2008. Constructive and unconstructive repetitive thought. Psychol Bull 134, 163–206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson D, Clark LA, Tellegen A, 1988. Development and validation of brief measures of positive and negative affect: The PANAS scales. Journal of Personality and Social Psychology 54, 1063–1070. [DOI] [PubMed] [Google Scholar]
- Whisman MA, Sbarra DA, 2012. Marital adjustment and interleukin-6 (IL-6). Journal of Family Psychology 26, 290–295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Witvliet C.v., Hofelich Mohr AJ, Hinman NG, Knoll RW, 2015. Transforming or restraining rumination: The impact of compassionate reappraisal versus emotion suppression on empathy, forgiveness, and affective psychophysiology. The Journal of Positive Psychology 10, 248–261. [Google Scholar]
- Zoccola PM, Figueroa WS, Rabideau EM, Woody A, Benencia F, 2014. Differential effects of poststressor rumination and distraction on cortisol and C-reactive protein. Health Psychol 33, 1606–1609. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.