

Abstract
Reductions of intraocular pressure during trabeculotomy result from relieving the resistance to aqueous flow by cleavage of the trabecular meshwork and inner walls of Schlemm's canal at the point of outflow resistance of the aqueous humor. Since trabeculotomy does not result in bleb formation, development of late-onset sight-threatening complications, such as hypotony maculopathy and endophthalmitis, that are associated occasionally with trabeculectomy develop less frequently after trabeculotomy. The ab-interno approach is used in several new procedures, including the Trabectome, Kahook Dual Blade, microhook abinterno trabeculotomy, and 360° suture trabeculotomy, instead of the ab-externo approach as in conventional trabeculotomy. These newly developed novel, minimally invasive, and trabeculotomy-related glaucoma surgeries can be good options for certain glaucoma cases, including early-stage open-angle glaucoma, developmental glaucoma, and glaucoma in elderly patients.
Keywords: Ab-externo trabeculotomy, Kahook Dual Blade, microhook ab-interno trabeculotomy, minimally invasive glaucoma surgery, suture ab-interno trabeculotomy, Trabectome
Introduction
The goal of trabeculotomy is reduction of the intraocular pressure (IOP) in patients with glaucoma.[1,2,3,4] The mechanism by which this is accomplished may be by elimination of the aqueous flow resistance by cleavage of the trabecular meshwork (TM) and inner walls of Schlemm's canal at the point of outflow resistance of the aqueous humor. The ab-externo approach that involves incision of the TM after a scleral flap is created has been used traditionally to perform trabeculotomy in combination with metal trabeculotomes.[1,2,3,4] A new technique, i.e., the ab-interno approach, for performing trabeculotomy has been reported recently, in which the TM is incised or excised using specialized devices under direct observation of the anterior-chamber angle structure. These novel trabeculotomy approach included the Trabectome procedure during which the surgeon removes the TM using a small diathermy/irrigation/aspiration handpiece [Figure 1a];[5] the Kahook Dual Blade is used to excise the TM in a strip using a curette with two blades [Figure 1b];[6,7] microhook ab-interno trabeculotomy, which uses a small metal hook to incise the TM [Figure 1c];[8,9,10] and ab-interno 360° suture trabeculotomy/gonioscopy-assisted transluminal trabeculotomy, by which the entire TM is incised using a suture after circumferential insertion of the suture into Schlemm's canal [Figure 1d].[11,12]
Figure 1.

Various devices for novel trabeculotomy-related surgeries. (a) The Trabectome provided by Kowa Company Ltd. (http://www.kowa.co.jp). (b) The Kahook Dual Blade provided by JFC sale Plan (http://www.jfcsp.co.jp). (c) The Tanito ab interno Trabeculotomy Microhook provided by Inami and Co., Ltd. (http://inami.co.jp). (d) The Chin trabeculotomy suture provided by Handaya Co., Ltd. (http://www.handaya.co.jp)
Microhook Ab-Interno Trabeculotomy, A Novel Minimally Invasive Glaucoma Surgery
Three different microhooks are used during microhook ab-interno trabeculotomy. A straight [M-2215S, Figure 1c] hook is used to incise the nasal angle, and angled-right [M-2215R, Figure 1c] and angled-left [M-2215 L, Figure 1c] hooks (all from Inami and Co., Ltd.) are used to incise the temporal angle. A Swan Jacob gonioprism lens (Ocular Instruments) is used to observe the angle opposite to the corneal port, and a microhook is inserted into the anterior chamber through the corneal port [Figure 2a and b]. The microhook tip then is inserted into Schlemm's canal and moved circumferentially to incise the inner wall of the canal and TM over 3 clock hours. Trabeculotomy then is performed in the opposite angle using the same procedure by insertion of the microhook through another corneal port. We recommend perforating the meshwork by gently sliding and not stabbing the tip into the meshwork surface to minimize damage to the outer wall of Schlemm's canal when inserting the tip of the hook into Schlemm's canal. After inserted the tip of the hook, the depth of the tip can be visualized thorough the TM. When the tip cannot be visualized through the TM, this usually indicates that the tip is too deep. With adequate direction and depth, only minor resistance is encountered when the tip is moved circumferentially; any resistance usually indicates that the tip is too deep. Avoiding iatrogenic tissue damage around the TM requires careful monitoring of the correct insertion, direction, and depth of the tip of the hook. Intraoperative use of microscope-integrated optical coherence tomography (OCT) (RESCAN 700, Carl Zeiss Meditec Japan) in combination with a gonioprism[13] or by anterior-segment OCT (Casia 2, Tomey Corporation) postoperatively can visualize correct opening of the TM [Figure 3a and b].[9] The surgical video is available at https://www.youtube.com/watch? v = VPWhsEsfrn8.[14]
Figure 2.
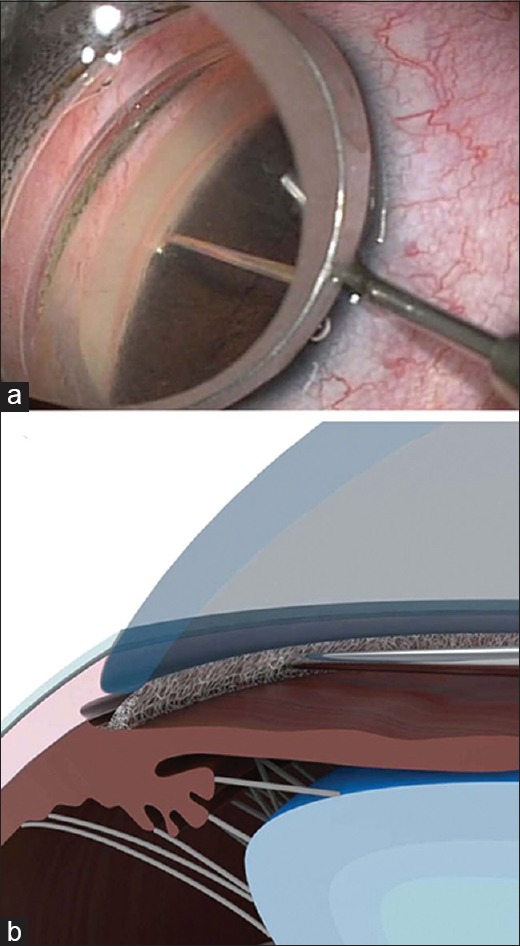
Surgical procedure of microhook ab-interno trabeculotomy. (a) Observation of the anterior-chamber angle using a Swan-Jacob gonioprism lens shows the trabecular meshwork and that inner wall of Schlemm's canal is incised circumferentially using the tip of the microhook inserted into the anterior chamber through the small corneal incision. (b) A schematic drawing of the meshwork incision by the tip of the hook. This schema is provided by Inami Co. Ltd
Figure 3.
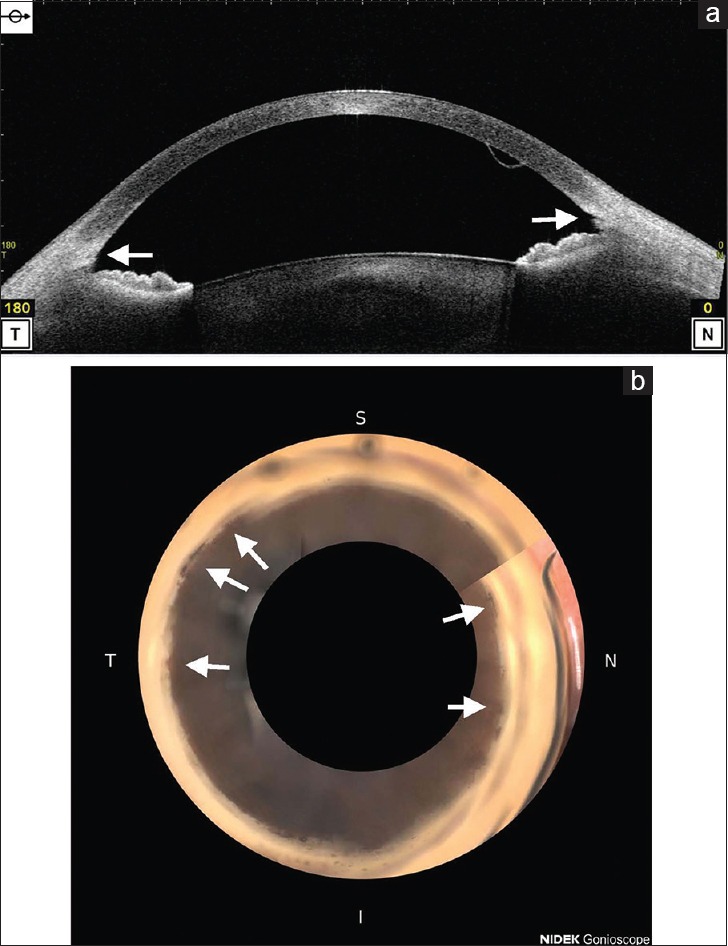
Anterior-chamber angle findings after microhook ab-interno trabeculotomy. (a) Observation of the anterior-chamber angle using anterior-segment optical coherence tomography (Casia 2, Tomey). A trabeculotomy cleft is seen in both the temporal and nasal angles (arrows) postoperatively in the right eye. (b) Observation of the entire anterior-chamber angle using a 360° gonioscope (GS-1, Nidek).[21] Small but interrupted peripheral anterior synechiae (arrows) are seen postoperatively in the right eye
An initial case series reported that at the final 6-month examination, microhook ab-interno trabeculotomy alone decreased the IOP from 25.9 mmHg preoperatively to 14.7 mmHg postoperatively, a 43% decrease.[9] Microhook ab-interno trabeculotomy combined with cataract surgery decreased the IOP from 16.4 mmHg preoperatively to 11.8 mmHg postoperatively at the final 9.5-month examination, a 28% decrease.[10] The complications reported included transient IOP spikes, cataract progression, vitreous hemorrhages, and macular edema.[9,10]
Features of Conventional and Novel Trabeculotomy-Related Surgeries
The features of the new trabeculotomy-related surgeries are shown in Table 1. Since the ab-interno approach does not require conjunctival and scleral incisions, the new trabeculotomy-related procedures are minimally invasive to the ocular surface, which allows these procedures to be performed safely in the eyes with scleral thinning.[8] The smaller surgical incisions created in the ocular surface with ab-interno trabeculotomy-related procedures cause less induced postoperative astigmatism than astigmatism that develops following trabeculectomy.[15] Direct visualization of the anterior-chamber angle achieved using a gonioprism lens during ab-interno trabeculotomy facilitates easier identification of Schlemm's canal compared with identification of the anterior-chamber angle under the scleral flap during conventional ab-externo trabeculotomy. The extent of the trabeculotomy (90–120°) the conventional ab-externo trabeculotomy [Figure 4a], the Trabectome procedure, and the Kahook Dual Blade [Figure 4b] is wider, i.e., 180–240° for microhook ab-interno trabeculotomy [Figure 4c] and 360° with suture trabeculotomy when a suture is inserted successfully into the entire circumference of Schlemm's canal [Figure 4d]. In a perfusion study of autopsy eyes, the investigators reported that incisions in the TM that extended for 1, 4, and 12 clock hours eliminated 30%, 44%, and 51%, respectively, of the outflow resistance at 7 mmHg of perfusion pressure and 30%, 56%, and 72%, respectively, of the outflow resistance at 25 mmHg of perfusion pressure.[16] Those findings indicated that wider trabeculotomies combined with a novel trabeculotomy-related procedure other than conventional ab-externo trabeculotomy are advantageous. However, the future comparative studies are needed to corroborate the results. The Kahook Dual Blade requires a single-use handpiece, and the Trabectome procedure requires a single-use handpiece and a surgical machine, all of which increase the surgical costs compared with other procedures.
Table 1.
Comparisons among conventional trabeculotomy and recent trabecular meshwork surgeries
| Procedure | Trabeculotomy ab externo | Goniotomy | Trabectome | Kahook Dual Blade | Microhook ab-interno trabeculotomy | 360° ab-interno trabeculotomy |
|---|---|---|---|---|---|---|
| Trabeculotomy extent | 1/4 circumference | 1/4 circumference | 1/4 circumference | 1/4 circumference | 1/2-2/3 circumference | ~Entire circumference |
| Ocular surface invasiveness | ++ | Minimal | Minimal | Minimal | Minimal | Minimal |
| Procedural difficulty | Difficult | Difficult | Easy | Moderate | Moderate | Difficult |
| Reason for difficulty | Require Schlemm’s canal identification | Require incision depth control | Large device tip, difficulty in strip excision | Require left-handed procedure | Difficulty in entire circumference suture insertion | |
| Surgical cost | Low | Low | High | Moderate | Low | Low |
This table was adopted from my previous publication[20] with English translation with the permission of the journal
Figure 4.
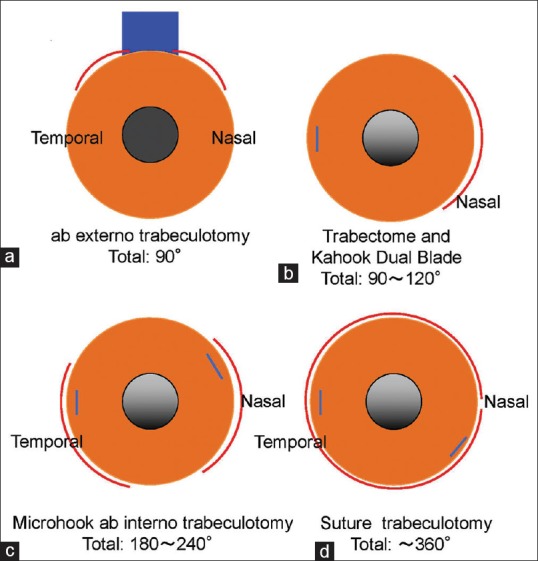
The typical extents of the incisions created in traditional ab-externo trabeculotomy and novel trabeculotomy-related glaucoma surgeries. (a) Conventional ab-externo trabeculotomy. (b) The Trabectome and Kahook Dual Blade. (c) Microhook ab-interno trabeculotomy. (d) Suture ab-interno trabeculotomy. The red arcs indicate the extent of the trabeculotomy, the blue lines the corneal side ports, and the blue box the scleral flap. These panels are adopted from our previous publication[20] with modification with the permission of the journal
Indications for Ab-Interno Trabeculotomy-Related Surgeries
The indications and contraindications of trabeculotomy-related surgeries are shown in Table 2. Trabeculotomy is the first-choice procedure for most steroid-induced and developmental glaucomas. Early-stage open-angle glaucoma including primary open-angle and exfoliation glaucomas are also candidates for trabeculotomy. Compared with trabeculotomy, trabeculectomy, the gold-standard glaucoma surgery, results in the need for more frequent postoperative procedures, e.g., laser suture lysis and needling, and possibly is associated with bleb-related complications. The IOP reduction achieved with trabeculotomy might be enhanced by older age and simultaneous cataract surgery.[3,4,17] Since elderly patients may have difficulties traveling frequently for hospital visits, they can be good candidates for trabeculotomy.[18] Although the surgical indications for ab-externo and ab-interno surgeries are the same, the safer profile of the latter, i.e., less invasiveness of the ocular surface, less difficult surgical procedure, and shorter surgical duration, enables surgeons to perform these novel procedures in eyes with an earlier stage of glaucoma than conventional trabeculotomy.
Table 2.
Indications for trabeculotomy-related procedures
| Indication |
| Early-stage open-angle glaucoma (i.e., primary open-angle glaucoma, exfoliation glaucoma, steroid-induced glaucoma) |
| Developmental glaucoma without corneal opacity |
| Glaucoma accompanying visual disturbance due to cataract (combined cataract and glaucoma surgeries) |
| Primary angle-closure glaucoma (combined cataract and glaucoma surgeries) |
| Glaucoma in elderly patients (difficulty with frequent hospital access, life expectancy) |
| Contraindication |
| Ocular inflammation |
| Neovascular glaucoma |
| Aphakic glaucoma |
| Vitreous collapse into the anterior chamber |
| Advanced glaucoma |
This table is adopted from my previous publication[20] with English translation with the permission of the journal
Financial support and sponsorship
Nil.
Conflicts of interest
The microhooks used were codeveloped by Masaki Tanito, MD, PhD, and Inami and Co., Ltd. (Tokyo, Japan) and provided by Inami and Co., Ltd. Dr. Tanito receives royalties from Inami and Co., Ltd.
Acknowledgment
This review includes text extracts from reference[19] and English-translated text extracts from reference[20] with the permission of the journals.
References
- 1.Chihara E, Nishida A, Kodo M, Yoshimura N, Matsumura M, Yamamoto M, et al. Trabeculotomy ab externo: An alternative treatment in adult patients with primary open-angle glaucoma. Ophthalmic Surg. 1993;24:735–9. [PubMed] [Google Scholar]
- 2.Tanihara H, Negi A, Akimoto M, Terauchi H, Okudaira A, Kozaki J, et al. Surgical effects of trabeculotomy ab externo on adult eyes with primary open angle glaucoma and pseudoexfoliation syndrome. Arch Ophthalmol. 1993;111:1653–61. doi: 10.1001/archopht.1993.01090120075025. [DOI] [PubMed] [Google Scholar]
- 3.Tanito M, Ohira A, Chihara E. Surgical outcome of combined trabeculotomy and cataract surgery. J Glaucoma. 2001;10:302–8. doi: 10.1097/00061198-200108000-00010. [DOI] [PubMed] [Google Scholar]
- 4.Tanito M, Ohira A, Chihara E. Factors leading to reduced intraocular pressure after combined trabeculotomy and cataract surgery. J Glaucoma. 2002;11:3–9. doi: 10.1097/00061198-200202000-00002. [DOI] [PubMed] [Google Scholar]
- 5.Minckler DS, Baerveldt G, Alfaro MR, Francis BA. Clinical results with the trabectome for treatment of open-angle glaucoma. Ophthalmology. 2005;112:962–7. doi: 10.1016/j.ophtha.2004.12.043. [DOI] [PubMed] [Google Scholar]
- 6.Seibold LK, Soohoo JR, Ammar DA, Kahook MY. Preclinical investigation of ab interno trabeculectomy using a novel dual-blade device. Am J Ophthalmol. 2013;155:524–900. doi: 10.1016/j.ajo.2012.09.023. [DOI] [PubMed] [Google Scholar]
- 7.Dorairaj SK, Kahook MY, Williamson BK, Seibold LK, ElMallah MK, Singh IP, et al. A multicenter retrospective comparison of goniotomy versus trabecular bypass device implantation in glaucoma patients undergoing cataract extraction. Clin Ophthalmol. 2018;12:791–7. doi: 10.2147/OPTH.S158403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Tanito M, Sano I, Ikeda Y, Fujihara E. Microhook ab interno trabeculotomy, a novel minimally invasive glaucoma surgery, in eyes with open-angle glaucoma with scleral thinning. Acta Ophthalmol. 2016;94:e371–2. doi: 10.1111/aos.12888. [DOI] [PubMed] [Google Scholar]
- 9.Tanito M, Sano I, Ikeda Y, Fujihara E. Short-term results of microhook ab interno trabeculotomy, a novel minimally invasive glaucoma surgery in Japanese eyes: Initial case series. Acta Ophthalmol. 2017;95:e354–60. doi: 10.1111/aos.13288. [DOI] [PubMed] [Google Scholar]
- 10.Tanito M, Ikeda Y, Fujihara E. Effectiveness and safety of combined cataract surgery and microhook ab interno trabeculotomy in Japanese eyes with glaucoma: Report of an initial case series. Jpn J Ophthalmol. 2017;61:457–64. doi: 10.1007/s10384-017-0531-z. [DOI] [PubMed] [Google Scholar]
- 11.Grover DS, Godfrey DG, Smith O, Feuer WJ, Montes de Oca I, Fellman RL, et al. Gonioscopy-assisted transluminal trabeculotomy, ab interno trabeculotomy: Technique report and preliminary results. Ophthalmology. 2014;121:855–61. doi: 10.1016/j.ophtha.2013.11.001. [DOI] [PubMed] [Google Scholar]
- 12.Sato T, Hirata A, Mizoguchi T. Prospective, noncomparative, nonrandomized case study of short-term outcomes of 360° suture trabeculotomy ab interno in patients with open-angle glaucoma. Clin Ophthalmol. 2015;9:63–8. doi: 10.2147/OPTH.S75739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tanito M. Optical Coherence Tomography Observation of Gonio Structures during Microhook Ab Interno Trabeculotomy. J Ophthalmol. 2017;2017:6310835. doi: 10.1155/2017/6310835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tanito M. Microhook ab interno trabeculotomy, a novel minimally invasive glaucoma surgery. Clin Ophthalmol. 2018;12:43–8. doi: 10.2147/OPTH.S152406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tanito M, Matsuzaki Y, Ikeda Y, Fujihara E. Comparison of surgically induced astigmatism following different glaucoma operations. Clin Ophthalmol. 2017;11:2113–20. doi: 10.2147/OPTH.S152612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Rosenquist R, Epstein D, Melamed S, Johnson M, Grant WM. Outflow resistance of enucleated human eyes at two different perfusion pressures and different extents of trabeculotomy. Curr Eye Res. 1989;8:1233–40. doi: 10.3109/02713688909013902. [DOI] [PubMed] [Google Scholar]
- 17.Hara K, Takai Y, Tanito M. Outcomes after combined deep sclerectomy and trabeculotomy to treat primary open-angle glaucoma and exfoliation glaucoma. Shimane J Med Sci. 2019;35:43–52. [Google Scholar]
- 18.Tanito M, Sugihara K, Hara K, Takai Y. Different glaucoma types and glaucoma surgeries among different age groups. Graefes Arch Clin Exp Ophthalmol. 2018;256:2013–4. doi: 10.1007/s00417-018-4058-x. [DOI] [PubMed] [Google Scholar]
- 19.Tanito M. Novel trabeculotomy-related glaucoma surgeries. Shimane J Med Sci. 2019;35:31–5. doi: 10.4103/tjo.tjo_38_19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Tanito M. What's the differences among various trabeculotomy-related surgeries [author's translation] Jpn J Ophthalmic Surg. 2018;31:98–9. [Google Scholar]
- 21.De Giusti A, Pajaro S, Tanito M. Automatic Pigmentation Grading of the Trabecular Meshwork in Gonioscopic Images. Proceeding Computational Pathology Ophthalmic Medical Image Analysis (COMPAY-OMIA 2018) 2018:193–200. [Google Scholar]