

Abstract
Introduction:
Roadside sobriety checkpoints are an intervention in which law enforcement officers stop passing vehicles to check whether drivers are impaired. There is clear evidence that a program of roadside sobriety checkpoints is an effective approach to reducing alcohol-involved motor vehicle crashes, likely because of general deterrent effects across the entire population of drivers. The aim of this study is to assess the duration of time over which individual roadside sobriety checkpoints are associated with alcohol-involved motor vehicle crashes, within the context of a broader checkpoint program.
Methods:
In August 2018, the authors accessed incident-level data for alcohol-involved motor vehicle crashes and roadside sobriety checkpoints for the City of Los Angeles, California, 2013–2017. Counts of crashes and checkpoints were computed within three different temporal units: days (n=1,826), weeks (n=260), and months (n=60). The number of checkpoints were then calculated at different lagged periods (up to 7 days, up to 4 weeks, and up to 3 months). Autoregressive integrated moving average analyses related counts of checkpoints over these lagged periods to subsequent crashes.
Results:
Fewer alcohol-involved motor vehicle crashes occurred when there were more roadside sobriety checkpoints over the previous 4 days, 5 days, 6 days, 7 days, and 1 week.
Conclusions:
Individual roadside sobriety checkpoints affected alcohol-involved motor vehicle crashes in Los Angeles, California for approximately 1 week. The temporal configuration of individual checkpoints is an important consideration when designing an overall roadside sobriety checkpoint program.
INTRODUCTION
Alcohol-involved road crashes have been shown to be preventable and reductions in traffic crash deaths, especially from alcohol, are one of the great public health achievements of the 20th century.1 Between 1982 and 1999, the proportion of fatal crashes involving a driver with a blood alcohol concentration 0.08 g/mL or more fell from 35% to 20%,2 credited largely to key interventions introduced during that period (e.g., raising the minimum legal drinking age from 18 to 21 years; limiting blood alcohol concentrations for licensed drivers to 0.08 g/mL).3,4 After this sustained reduction, the incidence of alcohol-involved crashes has remained roughly constant for the last two decades, and upwards of 12,000 deaths are attributable to alcohol-involved crashes each year.5 Achieving further reductions requires concerted efforts to implement evidence-based strategies.
Roadside sobriety checkpoints have empirical support from studies around the globe as a cost-effective and high-impact intervention to reduce alcohol-involved motor vehicle crashes.6,7 In this broad class of intervention, a team of law enforcement officers establishes a roadside checkpoint at which passing drivers are systematically stopped for a possible sobriety test. The intervention is predicated on deterrence theory, which separates the deterrent effect against drunk driving among those who pass through the checkpoint (specific deterrence) from the deterrent effect among the entire population of drivers (general deterrence).8 The proportion of all drivers who are tested at roadside sobriety checkpoints is very low, as are arrest rates among those who are tested,8,9 so specific deterrent effects are likely to be minimal.10 Rather, the main goal is to increase the perceived risk of detection and arrest among all drivers, which will raise the perceived individual costs of drunk driving, thereby leading to fewer people choosing to drive after drinking and resulting in reduced rates of alcohol-involved crashes.8 Multiple published reviews3,11–15 have concluded that crash rates are at least 8% lower in jurisdictions that use roadside sobriety checkpoints compared with those that do not. If extended, this could translate into thousands of motor vehicle crashes averted and hundreds of lives saved each year in the U.S.
Roadside sobriety testing was first used in the U.S. in the early 1980s.16 The intervention was challenged in the 1990 U.S. Supreme Court, Michigan Department of State Police versus Sitz (496 U.S. 444, 1990),17 in which it was ruled that selective breath testing (where police may conduct a sobriety test only among drivers whom they have reason to suspect may have been drinking) was a minor and acceptable intrusion on drivers’ civil liberties, but that random breath testing (where police may randomly stop drivers and may conduct sobriety tests among any driver without having reasonable cause) would violate their 4th Amendment rights against unreasonable searches and seizures.6 In order to allow population-level breath alcohol testing that is compliant with the 4th Amendment, U.S. law enforcement officers must stop vehicles using a neutral protocol that does not target any specific type of vehicle or driver. Law enforcement agencies must also publicize the times and locations of the sobriety checkpoints.18 Today, roadside sobriety testing programs are permitted by statutory or case law in 38 states.19 Nevertheless, only around one third of these states conduct checkpoints at least weekly.20 Law enforcement agencies in the U.S. emphasize that the burden on human resources is the primary impediment to more regular use of roadside sobriety testing.21
From the results of their 2014 systematic review,11 the Community Preventive Services Task Force concluded that evidence in support of the effectiveness of roadside sobriety checkpoints was no longer required. Rather, future research should seek to identify the impacts of different spatial configurations (where checkpoints are held), temporal configurations (when checkpoints are held), site configurations (the checkpoint duration and number of officers involved), and publicity campaigns (how widely and which avenues are used to promote checkpoint activity) on alcohol-involved motor vehicle crashes. Such information provides critical implementation guidance for law enforcement agencies seeking to balance public health benefits and scarce law enforcement resources. Given this history and gap in knowledge, the current study specifically examines temporal configurations of roadside sobriety checkpoints. The aim is to assess the duration of time over which individual roadside sobriety checkpoints are associated with alcohol-involved motor vehicle crashes. Current evidence and the theory of general deterrence provide little, if any, guidance regarding the period over which an individual roadside sobriety checkpoint might affect incidence of alcohol-involved motor vehicle crashes, so associations ranging from 1 day to 3 months are tested in a large U.S. city.
METHODS
Study Sample
The setting for this study was the City of Los Angeles, California, which the commercial alert service DUI Block nominates as the U.S. city in which the most sobriety checkpoints are conducted.22 The city has a population of 4.0 million and covers a land area of 502.7 square miles. Incorporated cities that are wholly surrounded by Los Angeles were excluded (e.g., Santa Monica, Beverley Hills, Culver City).
The outcome was alcohol-involved crashes in the City of Los Angeles for January 1, 2013–December 31, 2017. The University of California, Berkeley, Transport Injury Mapping System provided a registry of crashes in California compiled from the California Statewide Integrated Traffic Records System. These data included all crashes in which at least one victim was injured and required medical treatment, or in which there was >US$1,000 of property damage. Available crash-level variables included the date and time of the crash and an indicator for whether the attending police officer believed the crash involved a party that had been drinking any alcohol (i.e., with estimated blood alcohol concentration >0.00 g/dL).
The exposure of interest was sobriety checkpoints within the City of Los Angeles from October 1, 2012 to December 31, 2017. In accordance with Michigan Department of State Police versus Sitz,17 Los Angeles Police Department (LAPD) provides notice to the public of future sobriety checkpoints. Historical press releases from the LAPD website23 provided the date and time of sobriety checkpoints that occurred within the study city during the study period.
The LAPD press releases also provided notice of saturation patrols, which are a planned increase in police presence in a concentrated area at a prescribed time. Whereas roadside sobriety checkpoints are a noticeable cluster of police vehicles and are likely to be recognizable to drivers, saturation patrols are simply an increase in the number of marked or unmarked police vehicles on streets in an area and passing drivers may not be aware of this activity.24 Thus, general deterrence theory predicts roadside sobriety checkpoints will be more strongly related than saturation patrols to subsequent alcohol-involved motor vehicle crashes. The LAPD does not publicize the number of law enforcement officers involved in roadside sobriety checkpoints or saturation patrols.
This analysis of publicly available data was conducted in August 2018 and involved no human subjects.
Measures
For this time-series analysis, alcohol-involved crashes, sobriety checkpoints, and saturation patrols were aggregated as counts within three different temporal units: days (n=1,826), weeks (n=260), and months (n=60). Because sobriety checkpoints and saturation patrols were often held over 2 calendar days (e.g., from 8:00PM to 2:00AM), the temporal partitions for days began at 4:00AM and ended at 3:59AM. Weeks began on January 1 of each year, and months were specified as calendar months. Counts of alcohol-involved crashes were approximately normally distributed in the weekly time series but were positively skewed in the daily and monthly time series (Appendix Figure 1). The daily and monthly time series were square root transformed prior to analysis.
To assess associations between alcohol-involved crashes in temporal unit, t, and sobriety checkpoints and saturation patrols conducted in previous temporal units, lagged versions of the interventions were calculated at t minus k (t-k) units, where k was an integer that ranged from 1 to 7 for the daily time series, from 1 to 4 for the weekly time series, and from 1 to 3 for the monthly time series. Three months was the largest temporal window because this was an extreme and unlikely extent over which individual roadside sobriety checkpoints would affect alcohol-involved crash incidence across the extent of Los Angeles. General deterrence theory predicts that accumulated exposure to sobriety checkpoints (and possibly saturation patrols) for the city population will lead to fewer alcohol-involved crashes over time, rather than within specific subsequent temporal units (e.g., precisely 2 weeks later), so exposures were calculated as the sum of interventions that occurred between t-k and t-1 (Figure 1).
Figure 1.
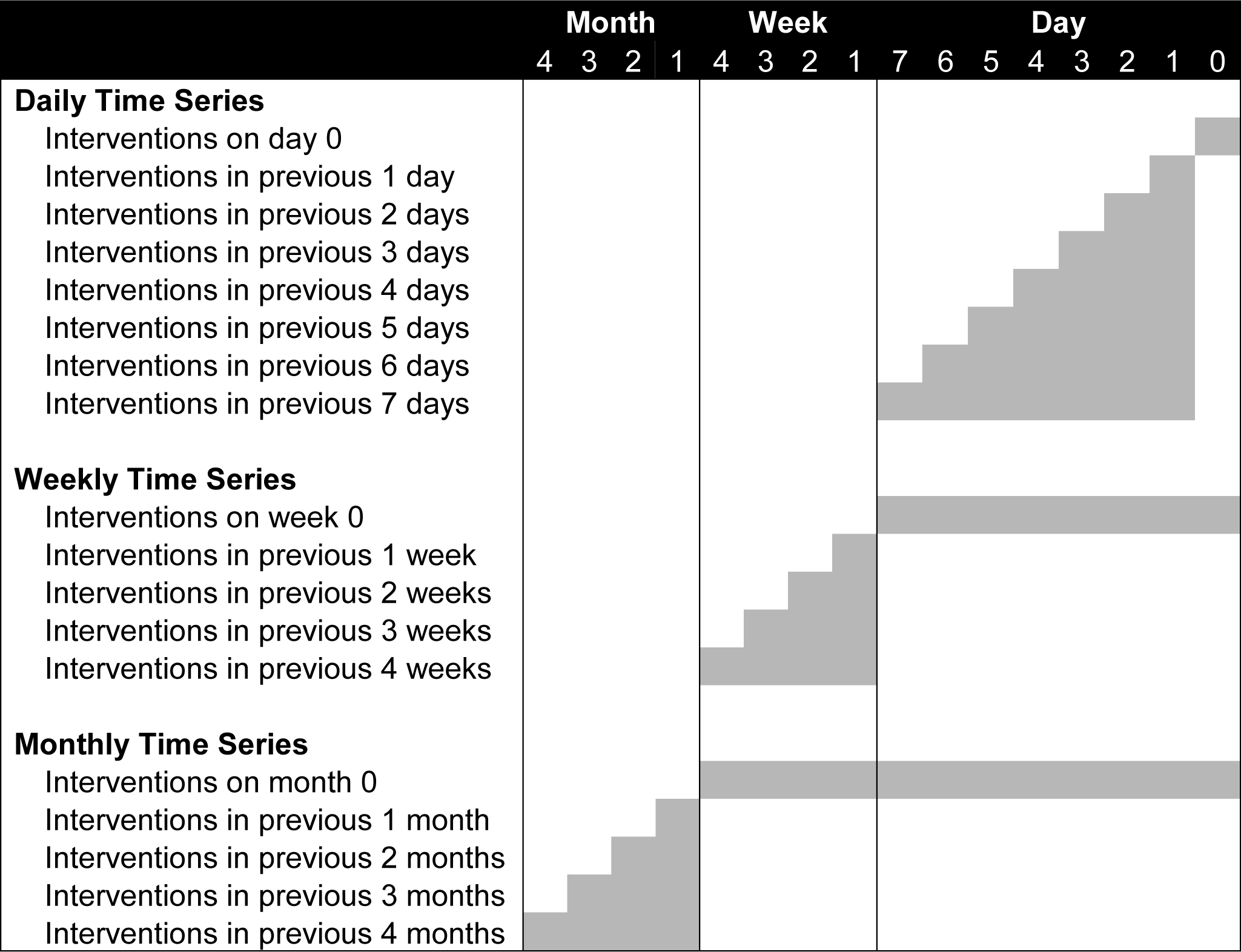
Construction of sobriety checkpoint and saturation patrol interruption variables.
Statistical Analysis
Autoregressive integrated moving average (ARIMA) models—implemented in Stata, version 14.1—assessed temporal relationships between sobriety checkpoints and saturation patrols and alcohol-involved crashes. This approach assumes that the outcome variable is approximately normally distributed and stationary (i.e., with a constant mean and variance over time). ARIMA models can be fitted to count outcomes, including motor vehicle crashes, when values are approximately normally distributed.25
To identify the ARIMA models the authors inspected line plots and summary statistics for each time series. In each case the Augmented Dickey–Fuller unit root test provided evidence against the null hypothesis that the time series was stationary,26 so first-order differences were calculated by subtracting the observed count of alcohol-involved crashes for the previous temporal unit (t-1) from each temporal unit (t). This procedure removes temporal trends from the time series,27 so it is not necessary to adjust for potential confounders that might be causally related to the outcome and vary systematically with the exposure (such as greater incidence of impaired driving and sobriety checkpoints and saturation patrols over the Christmas holiday period). To select the model that best fit each time series the authors visually inspected plots of the autocorrelation functions and partial autocorrelation functions and calculated Ljung–Box Q-statistics at lags of 40 units.28 Model variants included an autoregressive term (p), a moving average term (q), and a constant term. These parameters were retained if they were significant at p<0.05 and contributed to a lower value for the Q-statistic. Seasonality (s) was tested at lags of 7 units for daily time series, 52 units for the weekly time series, and 12 units for the monthly time series, to account for additional autocorrelation across these periods. Specifications for the identified models are described as ARIMA(p,d,q)(P,D,Q)s. After identifying the null models (i.e., without exposure variables), the authors retained the same model specifications when adding the exposure variables.
Most sobriety checkpoints and saturation patrols occurred on weekend nights (Fridays to Sundays), so sensitivity analyses were conducted using weekends as the units of analysis, commencing at 4:00AM Friday and ending at 3:59AM Monday. Additional sensitivity analyses used the proportion of all crashes that were alcohol-involved as the outcome to account for the possibility that all crashes vary systematically according to overall crash risks (e.g., resulting from weather, traffic volume), though it is noted that this procedure adds noise to the outcome and is likely to inflate SEs, potentially leading to false negative findings.
RESULTS
There were 11,006 alcohol-involved crashes in the City of Los Angeles from 2013 to 2017, which amounted to a median of 4 alcohol-involved crashes per day (IQR, 4–6), 41 per week (IQR, 37–47), and 178 per month (IQR, 169.5–195; Figure 2). The LAPD conducted 557 sobriety checkpoints and 330 saturation patrols during the study period (Table 1). Sobriety checkpoints mostly commenced on Fridays (48.7%) and Saturdays (40.4%) and were 5 (48.1%) or 6 hours (48.1%) in duration. Saturation patrols were most commonly conducted on Sundays (34.5%) and were typically advertised as continuing for 8 hours (94.5%).
Figure 2.
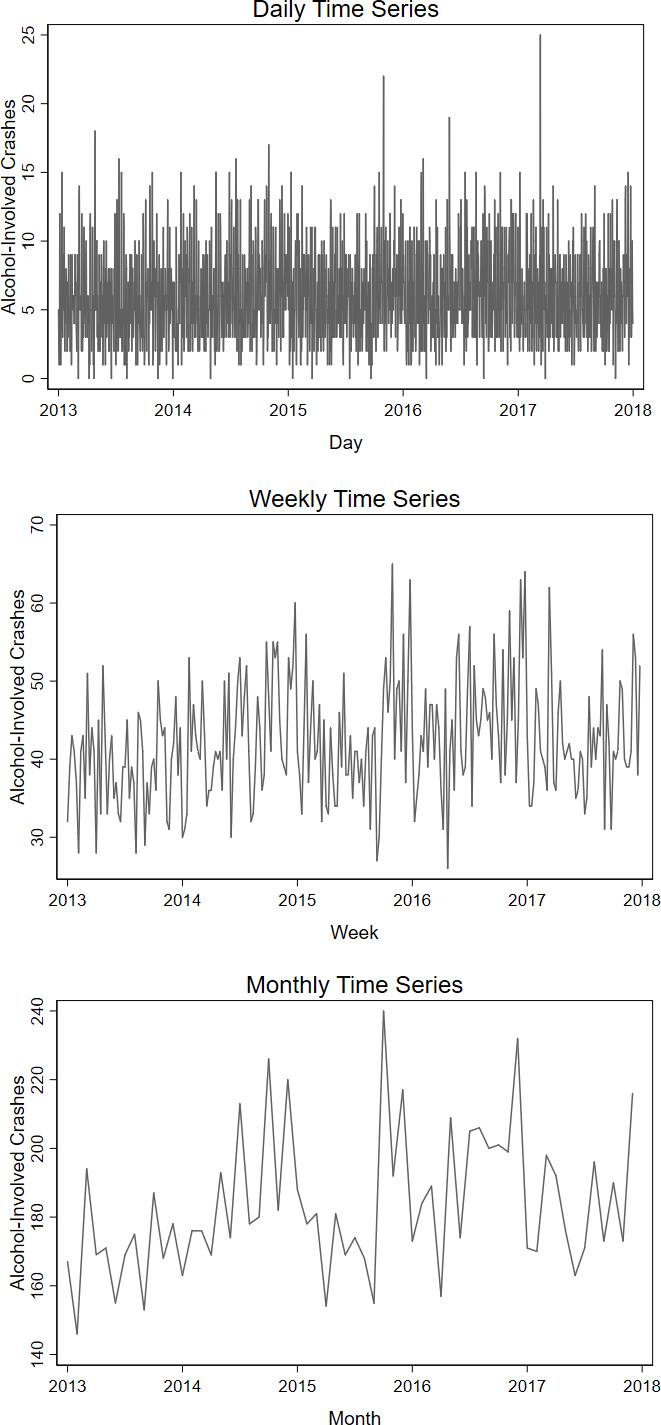
Line plots for alcohol-involved crashes within three temporal partitions, 2013–2017.
Table 1.
Characteristics of Alcohol-Involved Crashes, Sobriety Checkpoints, and Saturation Patrols; Los Angeles, 2013–2017
| Time period | Alcohol-involved crashes (n=11,006) n (%) |
Roadside sobriety checkpoints (n=557) n (%) |
Saturation patrols (n=330) n (%) |
|---|---|---|---|
| Day of week | |||
| Sunday | 1,788 (16.3) | 14 (2.5) | 114 (34.5) |
| Monday | 1,059 (9.6) | 2 (0.4) | 2 (0.6) |
| Tuesday | 1,107 (10.1) | 2 (0.4) | 2 (0.6) |
| Wednesday | 1,142 (10.4) | 3 (0.5) | 1 (0.3) |
| Thursday | 1,437 (13.1) | 40 (7.2) | 77 (23.3) |
| Friday | 2,107 (19.1) | 271 (48.7) | 70 (21.2) |
| Saturday | 2,366 (21.5) | 225 (40.4) | 64 (19.4) |
| Month | |||
| January | 862 (7.8) | 50 (9.0) | 46 (13.9) |
| February | 854 (7.8) | 43 (7.7) | 21 (6.4) |
| March | 938 (8.5) | 50 (9.0) | 34 (10.3) |
| April | 841 (7.6) | 50 (9.0) | 29 (8.8) |
| May | 930 (8.5) | 46 (8.3) | 27 (8.2) |
| June | 835 (7.6) | 56 (10.1) | 19 (5.8) |
| July | 932 (8.5) | 47 (8.4) | 26 (7.9) |
| August | 923 (8.4) | 41 (7.4) | 23 (7.0) |
| September | 861 (7.8) | 48 (8.6) | 20 (6.1) |
| October | 1,044 (9.5) | 28 (5.0) | 22 (6.7) |
| November | 914 (8.3) | 45 (8.1) | 25 (7.6) |
| December | 1,072 (9.7) | 53 (9.5) | 38 (11.5) |
| Duration | |||
| <5 hours | — | 1 (0.2) | 1 (0.3) |
| 5 hours | — | 268 (48.1) | 4 (1.2) |
| 6 hours | — | 268 (48.1) | 3 (0.9) |
| 7 hours | — | 13 (2.3) | 3 (0.9) |
| 8 hours | — | 7 (1.3) | 312 (94.5) |
| >8 hours | — | 0 (0.0) | 7 (2.1) |
Table 2 presents the results of the ARIMA models. Within the daily time series, there was no evidence of an association between sobriety checkpoints on day t and alcohol-involved crashes. The point estimate of –0.01 suggests that each additional sobriety checkpoint was associated with a decrease of 0.01 in the square root of alcohol-involved crashes on the same day, however the 95% CI= –0.06, 0.03 includes the possibility that checkpoints were associated with additional crashes (p=0.617). By contrast, each additional sobriety checkpoint conducted over the previous 4 days was associated with a decrease of –0.02 in the square root of alcohol-involved crashes, but in this instance the 95% CI= –0.04, 0.00 does not include the possibility that checkpoints were associated with additional crashes (p=0.036). Sobriety checkpoints in the 5, 6, and 7 previous days were also associated with fewer alcohol-involved crashes (p<0.05). Results for the weekly time series also indicate that sobriety checkpoints within week t was not associated with the incidence of alcohol-involved crashes in week t (b= –0.07, 95% CI= –0.60, 0.46, p=0.793); however, additional sobriety checkpoints in the previous 1 week were associated with a 0.56 decrease in the square root of crashes (b= –0.56, 95% CI= –1.06, –0.06, p=0.029) during week t. Sobriety checkpoints were not associated with alcohol-involved crashes in the monthly time series, and saturation patrols were not associated with alcohol-involved crashes in the daily, weekly, or monthly time series.
Table 2.
Results of ARIMA Models for Counts of Alcohol-Involved Crashes, Los Angeles
| DUI interventions | Sobriety checkpoints |
Saturation patrols |
||
|---|---|---|---|---|
| b (95% CI) | p-value | b (95% CI) | p-value | |
| Dailya,b | ||||
| On day t | –0.01 (–0.06, 0.03) | 0.617 | 0.02 (–0.04, 0.08) | 0.539 |
| In previous 1 day | –0.02 (–0.07, 0.02) | 0.312 | 0.03 (–0.03, 0.08) | 0.389 |
| In previous 2 days | –0.01 (–0.04, 0.02) | 0.425 | 0.00 (–0.03, 0.04) | 0.875 |
| In previous 3 days | –0.01 (–0.04, 0.01) | 0.190 | –0.02 (–0.05, 0.01) | 0.305 |
| In previous 4 days | –0.02 (–0.04, 0.00) | 0.036 | –0.02 (–0.04, 0.00) | 0.120 |
| In previous 5 days | –0.02 (–0.03, 0.00) | 0.031 | –0.01 (–0.03, 0.01) | 0.286 |
| In previous 6 days | –0.02 (–0.03, 0.00) | 0.011 | –0.01 (–0.03, 0.01) | 0.449 |
| In previous 7 days | –0.02 (–0.03, 0.00) | 0.028 | –0.01 (–0.03, 0.01) | 0.413 |
| Weeklyc | ||||
| On week t | –0.07 (–0.60, 0.46) | 0.793 | –0.29 (–0.87, 0.28) | 0.314 |
| In previous 1 week | –0.56 (–1.06, –0.06) | 0.029 | 0.02 (–0.61, 0.65) | 0.956 |
| In previous 2 weeks | –0.31 (–0.66, 0.04) | 0.085 | –0.28 (–0.70, 0.15) | 0.202 |
| In previous 3 weeks | –0.08 (–0.38, 0.21) | 0.593 | –0.11 (–0.48, 0.27) | 0.568 |
| In previous 4 weeks | –0.02 (–0.28, 0.25) | 0.901 | –0.01 (–0.33, 0.32) | 0.970 |
| Monthlya,d | ||||
| On month t | –0.01 (–0.06, 0.04) | 0.679 | 0.02 (–0.03, 0.08) | 0.420 |
| In previous 1 month | 0.01 (–0.03, 0.04) | 0.635 | 0.02 (–0.05, 0.08) | 0.615 |
| In previous 2 months | 0.02 (0.00, 0.05) | 0.100 | 0.03 (–0.02, 0.08) | 0.273 |
| In previous 3 months | 0.00 (–0.03, 0.03) | 0.988 | 0.01 (–0.03, 0.05) | 0.548 |
Notes: Boldface indicates statistical significance (p<0.05).
Outcome variable square root transformed for the daily and monthly time-series.
Daily time series null model: ARIMA(0,1,1)(0,1,1)7: Q(40 lags)=33.9.
Weekly time series null model: ARIMA(0,1,1)(1,1,0)52: Q(40 lags)=43.2.
Monthly time series null model: ARIMA(0,1,1)(0,1,1)12: Q(40 lags)=12.3.
ARIMA, autoregressive integrated moving average; DUI, driving under the influence (of alcohol).
The relative associations were used to calculate the absolute impacts of individual sobriety checkpoints on alcohol-involved crashes. Additional checkpoints in the previous 6 days were associated with 1.6% (95% CI=2.8%, 0.4%) fewer crashes compared with the mean number of crashes per day. Additional checkpoints in the previous week were associated with 1.3% (95% CI=2.5%, 0.1%) fewer crashes.
The results for the sensitivity analyses using weekends as the units of analysis are presented in Appendix Table 1, and the sensitivity analyses using the proportion of injury crashes that were alcohol-involved as the outcome are presented in Appendix Table 2. Point estimates were negative for sobriety checkpoints in the daily and weekly time series (indicating they were associated with fewer crashes), though the CIs included the possibility of a null association.
DISCUSSION
This study provides evidence that individual roadside sobriety checkpoints conducted in Los Angeles for 2013–2017 were followed by fewer alcohol-involved motor vehicle crashes for a period of about 1 week. Saturation patrols were not significantly associated with the number of alcohol-involved motor vehicle crashes in any measured time frame.
The study findings are consistent with general deterrence theory.8 This theoretic mechanism emphasizes that sobriety checkpoints will not necessarily produce fewer alcohol-involved crashes on the days and times when they are in operation. The advertising of checkpoint schedules may provide impaired drivers an opportunity to avoid detection, and population exposure to advertisements (e.g., through LAPD press releases) is likely to be low. Nevertheless, motorists who pass through a checkpoint, see it in action, or otherwise become aware of its operation may be less likely to drive while impaired at a later date because of the perceived increased risks of detection.21 The analysis found that these benefits are detectable in the City of Los Angeles for about 1 week. Benefits dissipate beyond that window, perhaps because the effects become undetectable because of aggregation bias, or because drivers’ perceptions of arrest risks return to homeostasis as memories of the checkpoints become more distant. Associations from weekend-to-weekend were not detected, suggesting that—per the general deterrence theory—effects are not specific to days of the week on which checkpoints are conducted. Saturation patrols are less visually impressive than sobriety checkpoints and may be less noticeable to drivers. Consistent with these findings, saturation patrols are theoretically less likely to affect drivers’ perceived risks of detection.
This study differs from prior published analyses of sobriety checkpoints in one very important way. All previous analyses consider sobriety checkpoint programs in their entirety, examining the impact of the program’s presence on alcohol-involved crashes regardless of the temporal configuration of individual checkpoints within the program. This collective evidence suggests that roadside sobriety checkpoints are associated with overall reductions in crashes, that observed reductions in crashes are greatest within 3 months of the checkpoint program beginning with effect sizes diminishing over time,12 that stopping more drivers is associated with fewer crashes,29,30 that greater publicity may make checkpoints additionally effective,31 and that small checkpoints staffed by few officers are similarly effective to large checkpoints staffed by many officers.11,15 The current analysis is the first to consider the impact of the temporal configurations of individual sobriety checkpoints within the context of a broad program. These findings suggest the deterrent effect of any one checkpoint is relatively short-lived and the resultant reduction in alcohol-involved crashes is small (around 1.5% over a week). However, assuming these effects are independent and additive, the cumulative impacts of an entire sobriety checkpoint program could be considerable, and the more frequently checkpoints are held, the greater the reduction in alcohol-related crashes will be. Operating checkpoints in the week prior to anticipated increases in impaired driving is advisable for large cities such as Los Angeles. Whether these associations are generalizable to other smaller cities is an important area for further research.
Limitations
This study may be affected by the limitations common to all time-series analyses. The most important threat to internal validity is reverse causation, whereby LAPD purposefully schedules checkpoints on days when the incidence of impaired driving is likely to be greatest (e.g., on the July 4 holiday).32 If these days are systematically followed by temporal units with lower incidence of impaired driving, the analysis would erroneously detect an association between checkpoints and reduced incidence of alcohol-involved crashes. The authors are confident that the results are not affected by such bias because checkpoints were not associated with increased crash incidence on the same day, because no association was detected at 1-day lags (e.g., July 4 versus July 5, when risks for impaired driving are lower), and because models controlled for seasonal temporal autocorrelation (e.g., across weeks for the daily time series). Additionally, the authors were unable to verify that the sobriety checkpoints were carried out as advertised in the LAPD press releases. Associations between crashes and sobriety checkpoints less than 4 days prior may be undetectable because too few checkpoints had occurred to enable meaningful analysis (i.e., because of limited variation in the exposure variable over time).
CONCLUSIONS
Roadside sobriety checkpoints are an effective approach to reducing alcohol-involved motor vehicle crashes. This study adds that the temporal configuration of individual checkpoints within an overall program are an important consideration. Law enforcement agencies that do not implement checkpoints in the week before anticipated increases in impaired driving are potentially foregoing opportunities to reduce the incidence of alcohol-involved motor vehicle crashes.
Supplementary Material
ACKNOWLEDGMENTS
Research reported in this publication was supported by the National Institute on Alcohol Abuse and Alcoholism of NIH under Awards Number R21AA025749 and K01AA026327. The content is solely the responsibility of the authors and does not necessarily represent the official views of NIH. CNM compiled the data, led the statistical analyses, and drafted the manuscript. JF supported the statistical analyses and helped draft the manuscript. DJW, CPA, and CCB assisted with study design and interpretation and reviewed the manuscript. The authors report no financial disclosures.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
REFERENCES
- 1.Division of Unintentional Injury Prevention, National Center for Injury Prevention and Control, CDC. Achievements in public health, 1900–1999 motor-vehicle safety: a 20th century public health achievement. MMWR Morb Mortal Wkly Rep 1999;48(18):369–374. [PubMed] [Google Scholar]
- 2.National Highway Traffic Safety Administration. Fatality analysis reporting system data files, 1982–2014 Washington, DC: U.S. Department of Transportation; 2016. [Google Scholar]
- 3.Shults RA, Elder RW, Sleet DA, et al. Reviews of evidence regarding interventions to reduce alcohol-impaired driving. Am J Prev Med 2001;21(4 suppl):66–88. 10.1016/S0749-3797(01)00381-6. [DOI] [PubMed] [Google Scholar]
- 4.Wagenaar AC, Toomey TL. Effects of minimum drinking age laws: review and analyses of the literature from 1960 to 2000. J Stud Alcohol Suppl 2002;14:206–225. [DOI] [PubMed] [Google Scholar]
- 5.National Center for Statistics and Analysis. Traffic safety facts, crash stats: early estimate of motor vehicle traffic fatalities for the first half (Jan–Jun) of 2016 DOT HS 812 332. Washington, DC: U.S. Department of Transportation, National Highway Traffic Safety Administration; 2016. [Google Scholar]
- 6.Community Preventive Services Task Force. Publicized sobriety checkpoint programs to reduce alcohol-impaired driving. Am J Prev Med 2014;46(5):540–541. 10.1016/j.amepre.2014.01.019. [DOI] [PubMed] [Google Scholar]
- 7.Miller TR, Galbraith MS, Lawrence BA. Costs and benefits of a community sobriety checkpoint program. J Stud Alcohol 1998;59(4):462–468. 10.15288/jsa.1998.59.462. [DOI] [PubMed] [Google Scholar]
- 8.Homel R. Drivers who drink and rational choice: random breath testing and the process of deterrence. In: Clarke RV, Felson M, eds. Routine Activity and Rational Choice: Advances in Criminological Theory New Brunswick, NJ: Transaction Publishers; 1993. [Google Scholar]
- 9.Voas RB. A new look at NHTSA’s evaluation of the 1984 Charlottesville Sobriety Checkpoint Program: implications for current checkpoint issues. Traffic Inj Prev 2008;9(1):22–30. 10.1080/15389580701682114. [DOI] [PubMed] [Google Scholar]
- 10.Watson B, Freeman J. Perceptions and experiences of random breath testing in Queensland and the self-reported deterrent impact on drunk driving. Traffic Inj Prev 2007;8(1):11–19. 10.1080/15389580601027360. [DOI] [PubMed] [Google Scholar]
- 11.Bergen G, Pitan A, Qu S, et al. Publicized sobriety checkpoint programs: a Community Guide systematic review. Am J Prev Med 2014;46(5):529–539. 10.1016/j.amepre.2014.01.018. [DOI] [PubMed] [Google Scholar]
- 12.Erke A, Goldenbeld C, Vaa T. The effects of drink-driving checkpoints on crashes—a meta-analysis. Accident Anal Prev 2009;41(5):914–923. 10.1016/j.aap.2009.05.005. [DOI] [PubMed] [Google Scholar]
- 13.Elder RW, Shults RA, Sleet DA, et al. Effectiveness of sobriety checkpoints for reducing alcohol-involved crashes. Traffic Inj Prev 2002;3(4):266–274. 10.1080/15389580214623. [DOI] [Google Scholar]
- 14.Peek-Asa C. The effect of random alcohol screening in reducing motor vehicle crash injuries. Am J Prev Med 1999;16(1):57–67. 10.1016/S0749-3797(98)00116-0. [DOI] [PubMed] [Google Scholar]
- 15.Stuster JW, Blowers PA. Experimental evaluation of sobriety checkpoint programs DOT HS 808 287. Washington, DC: U.S. Department of Transportation, National Highway Traffic Safety Administration; 1995. [Google Scholar]
- 16.National Highway Traffic Safety Administration. The use of safety checkpoints for DWI enforcement DOT HS 857 606. Washington, DC: U.S. Department of Transportation, National Highway Traffic Safety Administration; 1983. [Google Scholar]
- 17.Michigan Department of State Police et al. v. Sitz et al., 496 U.S. 444, 110 L. Ed. 2d 412 (1990).
- 18.National Highway Traffic Safety Administration. Saturation patrols and sobriety checkpoints: A how-to guide for planning and publicizing impaired driving enforcement efforts DOT HS 809 063. Washington, DC: U.S. Department of Transportation, National Highway Traffic Safety Administration; 2000. [Google Scholar]
- 19.National Highway Traffic Safety Administration. Digest of impaired driving laws, 29th ed. DOT HS 809 063. Washington, DC: U.S. Department of Transportation, National Highway Traffic Safety Administration; 2014. [Google Scholar]
- 20.Governors Highway Safety Association. Sobriety Checkpoint Laws www.ghsa.org/state-laws/issues/sobriety%20checkpoints. Published 2016. Accessed September 5, 2018.
- 21.Fell JC, Ferguson SA, Williams AF, Fields M. Why are sobriety checkpoints not widely adopted as an enforcement strategy in the United States? Accident Anal Prev 2003;35(6):897–902. 10.1016/S0001-4575(02)00097-0. [DOI] [PubMed] [Google Scholar]
- 22.DUIBlock. DUI Checkpoint Alerts Sarasota, FL: AlertMedia, Inc; www.duiblock.com. Accessed February 26, 2019. [Google Scholar]
- 23.Los Angeles Police Department. Newsroom www.lapdonline.org/newsroom. Published 2018. Accessed August 16, 2018.
- 24.Fell JC, Langston EA, Tippetts AS. Evaluation of four state impaired driving enforcement demonstration programs: Georgia, Tennessee, Pennsylvania and Louisiana. 49th Annual Proceedings, Association for the Advancement of Automotive Medicine; 2005 Sep 12–14 Boston, MA: Association for the Advancement of Automotive Medicine, 2005. [PMC free article] [PubMed] [Google Scholar]
- 25.Quddus MA. Time series count data models: an empirical application to traffic accidents. Accident Anal Prev 2008;40(5):1732–1741. 10.1016/j.aap.2008.06.011. [DOI] [PubMed] [Google Scholar]
- 26.Dickey DA, Fuller WA. Distribution of the estimators for autoregressive time series with a unit root. J Am Stat Assoc 1979;74:427–431. 10.1080/01621459.1979.10482531. [DOI] [Google Scholar]
- 27.McCleary R, Hay RA Jnr. Applied Time Series Analysis for the Social Sciences Thousand Oaks, CA: Sage Publications, Inc; 1980. [Google Scholar]
- 28.Box G, Jenkins G. Time Series Analysis: Forecasting and Control San Francisco, CA: Holden-Day; 1970. [Google Scholar]
- 29.Ferris J, Mazerolle L, King M, et al. Random breath testing in Queensland and Western Australia: examination of how the random breath testing rate influences alcohol related traffic crash rates. Accident Anal Prev 2013;60:181–188. 10.1016/j.aap.2013.08.018. [DOI] [PubMed] [Google Scholar]
- 30.Ferris J, Devaney M, Sparkes-Carroll M, Davis G. A National Examination of Random Breath Testing and Alcohol-Related Traffic Crash Rates (2000–2012) Canberra, Australia: Foundation for Alcohol Research and Education; 2015. [Google Scholar]
- 31.Voas RB, Holder HD, Gruenewald PJ. The effect of drinking and driving interventions on alcohol-involved traffic crashes within a comprehensive community trial. Addiction 1997;92(suppl 2):S221–S236. 10.1111/j.1360-0443.1997.tb02993.x. [DOI] [PubMed] [Google Scholar]
- 32.Farmer C, Williams A. Temporal factors in motor vehicle crash deaths. Inj Prev 2005;11(1):18–23. 10.1136/ip.2004.005439. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.