

Abstract
Health inequalities persist, in part, because people in socioeconomically advantageous positions possess resources to avoid new health risks when medicine advances. Although these health decisions rarely occur in isolation, we know less about the specific role of networks. We examine whether social capital mediates the relationship between individual educational attainment and decisions about a medical advance: H1N1 vaccination during pregnancy. Building on prior work that defines social capital as the resources of network members, we examine two mechanisms through which social capital may affect health decisions, facilitating information flow and exerting influence. Using egocentric network data collected from 225 pregnant women during the 2009-10 H1N1 pandemic, we measure social capital as the proportion of networks that are college-educated H1N1 discussants (information flow) and the proportion of college-educated H1N1 supporters (influence). Findings reveal that college-educated women knew more college-educated H1N1 discussants and supporters. Further, both measures of social capital predicted higher probabilities of vaccination, with the latter mechanism emerging as a particularly strong predictor. Our findings provide evidence that health decisions are shaped by individual resources as well as social capital available through network ties, offering a unique perspective of the ways that social networks contribute to producing, and potentially reproducing, unequal health.
Keywords: egocentric networks, education, mediation, health, health behaviors
1. Introduction
Understanding the persistence of socioeconomic inequalities in health requires that we examine the specific processes that generate them (Link and Phelan, 1995; Lutfey and Freese, 2005; Glied and Lleras-Muney, 2008; Chang and Lauderdale, 2009; Hernandez, 2013). These socioeconomic inequalities in health persist, in part, because people in socioeconomically advantageous positions possess the resources necessary to avoid newly identified health risks when medical research advances (Link et al., 1998). As medicine advances and people learn about new health hazards (e.g., a new cancer screening test), those in more favorable social positions may have more concern about their health, have better access to new health information, and have the means to adopt advantageous health behaviors. For example, socioeconomic differences have emerged or widened across a wide array of health behaviors and outcomes following medical advances, particularly by educational attainment (Link et al., 1998; Frisbie et al., 2004; Lichtenberg and Lleras-Muney, 2005; Glied and Lleras-Muney, 2008; Price and Simon, 2009; Polonijo and Carpiano, 2013; Yang et al., 2014), as educational attainment has both direct (e.g., ability to access and process health information) and indirect (e.g., higher income) benefits (Hummer and Hernandez 2013).
Given that information about new health hazards may prompt or accentuate socioeconomic inequalities in health, we investigate the role that social networks play in this process. In other words, when faced with a new health hazard we posit that whom you know matters (Song 2010:479). To understand the role of social networks we focus on social capital. We examine whether social capital mediates the relationship between individual educational attainment and decisions about a medical advance developed to avoid a new health hazard. Building on prior work that defines social capital as the resources of network members (Song 2011; Lin 2001), we examine two specific mechanisms through which social capital may affect health decisions (Lin, 2017), by (1) facilitating the flow of health information and/or (2) exerting influence on health decisions. Prior research supports the notion that social capital mediates the relationship between individual social or socioeconomic factors and health (Moore, Stewart, and Teixeira 2014; Song 2011; Song, Pettis, and Piya 2017). Through interpersonal interactions, network members serve as lay health consultants, directly influencing health or medical decisions (Friedson, 1960; Pescosolido, 1992), providing individuals with information that influences subjective beliefs, or exerting normative influences on their health behaviors (Kohler et al., 2001; Umberson et al., 2010). Yet, we know less about the specific role that networks play in contributing to socioeconomic inequalities in health when new health information becomes available (Carpiano et al., 2008; Song et al., 2010), for example, when people face new health hazards.
Our example is H1N1 vaccination among pregnant women during the H1N1 pandemic, and we use survey interviews collected from 225 prima gravida (first time pregnant) women. We operationalize social capital as resources available to women through their personal networks. Specifically, we enumerate networks using a name generator, and measure social capital using name interpreter data on alter educational attainment and attitudes about H1N1 vaccination. We then test whether social capital mediates the relationship between ego educational attainment and H1N1 vaccination when holding health care access constant. Specifically, we measure social capital as the proportion of the network that is well-educated (i.e., completed a college degree) and (1) with whom individuals discussed H1N1 vaccination (i.e., flow of health information) or (2) supported H1N1 vaccination during pregnancy (i.e., influencing health decisions).
In the sections that follow, we begin by describing how medical advances, or newly identified health hazards, can act as a catalyst for inequalities in a new health behavior. Next, we delineate how the networks in which individuals are embedded may mediate socioeconomic inequalities in health processes. We then describe our dataset and methodological approach, which we use to (1) affirm that there was an educational gradient in vaccination behavior and (2) test whether network members’ resources operate by facilitating the flow of information and influencing vaccination behavior. Our findings offer evidence that, when responding to a new health hazard, people’s decisions are shaped both by their own resources as well as the resources of their network ties. Specifically, we find evidence that being embedded in a network composed of a higher proportion college-educated H1N1 vaccine supporters is a strong predictor of vaccination. In this way, our example merges and extends our current theoretical perspectives on the fundamental association between socioeconomic status and health, and identifies the important role of social capital in producing, and potentially reproducing, unequal health.
2. Background
2.1. Social Networks and the Emergence of Socioeconomic Inequalities in Health Following Medical Advances
For over a century, scholars have observed remarkably persistent social inequalities in health, across an array of socioeconomic measures (Kitagawa and Hauser, 1973; Feldman et al., 1989; Elo and Preston, 1996). People who are socioeconomically advantaged, who possess more flexible resources—defined as knowledge, money, prestige, and beneficial social connections that are adaptable within a variety of situations—are consistently able to avoid health hazards. These social conditions represent a fundamental cause of socioeconomic inequalities in health because they correspond to access to resources that affect a broad range of health outcomes (Link and Phelan 1995). Conditional upon disease preventability, social inequalities perpetuate socioeconomic inequalities in health by enabling socioeconomically advantaged people to avoid health risks and delay mortality (House et al., 1994). As a result, new health knowledge or medical technology often precipitate the emergence of social inequalities in health. As health knowledge emerges and medical technology advances, flexible resources enable some to avoid newly discovered health hazards, resulting in a social gradient in health behaviors and outcomes (Link et al., 1998).
Among available flexible resources, educational attainment is often key. Learned effectiveness enables people to expand cognitive abilities, develop communication skills, and build confidence for problem-solving (Mirowsky and Ross, 2003). This process enhances individuals’ abilities to decipher, understand, and react to new health information following medical advances, resulting in a higher level of health literacy and health consciousness to make informed decisions to protect their health (Nutbeam 2008: 2073) For example, educational differences in health behaviors and outcomes emerged or were exacerbated following advances in cancer screening and treatment (Link et al., 1998; Glied and Lleras-Muney, 2008); the development of new pharmaceutical drugs (Lichtenberg and Lleras-Muney, 2005; Price and Simon, 2009); and the availability of new vaccines (Polonijo and Carpiano, 2013).
Health decisions or problems rarely occur in isolation, though, instead prompting people to activate their social connections as they seek help (Perry and Pescosolido, 2015). In this sense, health decisions are a process, an episode, rather than a single choice (Pescosolido, 1992). An array of evidence supports the claim that the people we know affect how we behave. Social ties influence health (Durkheim, [1897] 1979; House et al., 1988) and decision-making about health (Pescosolido, 1992; Umberson et al., 2010; Liu et al., 2010). Beyond individual resources, it is networks that may contribute to unequal health behaviors and health outcomes (Link and Phelan, 2002; Phelan et al., 2004). Yet, as Carpiano and colleagues (2008: 251) describe, “although beneficial social connections are implicated in the underlying mechanisms of fundamental causes [of unequal health],” they have been relatively understudied as a mechanism generating socioeconomic inequalities in health. There are notable exceptions, including studies that have examined whether social connections serve as a mechanism generating health inequalities. Song and colleagues (2017) found that the average educational attainment of alters, along with athletic identity, mediated the relationship between an individual’s educational attainment and their body weight rating. This finding further affirms prior research by Song (2010) that the occupational prestige of alters mediated the association between social factors and psychological distress. In a third study, Moore and colleagues (2013) also found that social capital acted as an intervening mechanism between individual educational attainment and health (i.e., self-rated health, physical activity, and hypertension). These more recent studies lend further weight to the idea that social connections play an important role in generating health inequalities, and merit further investigation into their role when people react to a newly identified health hazard or medical advance.
We address this need by examining the role of social networks when medical advances prompt the emergence of educational inequalities in health behaviors. Social networks offer access to social capital. Although a range of social scientists offer different perspectives on social capital (Lin 1999; Bourdieu [1983] 1986; Coleman 1990; Putnam 2000), we define it as the range of collective resources that alters possess, which are available to people in their networks (Lin, 2001, 2017; Carpiano, 2006; Song et al., 2010). Social capital may affect health through a range of mechanisms (Lin 2001), potentially generating health inequalities (Song, Frazier, and Pettis 2018). In a recent review, Song and colleagues describe a range of mechanisms through which these network members’ resources can affect health positively, ranging from influencing macro-level health policies to biological responses such as boosting the immune system (see Song, Frazier, and Pettis 2018 for full review). We examine two specific mechanisms through which social capital as network members’ resources may affect health decisions (Lin, 2001; Song et al., 2010), by (1) facilitating the flow of health information from well-educated alters and (1) exerting normative influence from well-educated alters.
First, possessing more social capital may facilitate the flow of information about a new medical advance (Song et al., 2010; Lin, 2017). Prior work by Song and Chang (2012) provides evidence that social capital represents a resource that stratifies the way people learn new health information. They found that being embedded within networks with a higher proportion of well-educated people is predictive of more active searches for health information from more diverse sources, net of individual educational attainment and other sociodemographic resources. Possessing more social capital makes individuals both more active as health information seekers, and more adept at mobilizing social ties and making use of diverse resources to which they have access (Song & Chang, 2012). We theorize that the combined effect of possessing more social capital in the form of well-educated alters and being in networks with a greater flow of information about a new health hazard will result in more beneficial health decisions.
Second, with regard to health decisions, social capital as network members’ resources (Song & Chang, 2012) may operate by exerting normative influences that impact how they perceive, manage, and make decisions about their health (Pescosolido et al., 1998), including decisions about newly identified health hazards. As described, network ties directly influencing health decisions (Friedson, 1960; Pescosolido, 1992), providing information and exerting normative influences on their health behaviors (Kohler et al., 2001; Umberson et al., 2010). In this way, being linked to highly educated alters or embedded in a highly educated network may enhance their ability to avoid a new health hazard. For example, seminal work by Christakis and Fowler (2008) found that individuals were themselves more likely to quit smoking when highly educated friends stopped smoking. This suggests that highly educated networks or alters may be more successful at influencing friends, and that, at least for certain behaviors, these processes differ for those embedded in more educated networks. Thus, women may directly benefit from being embedded within more highly educated networks that socially influence them, even though they may know little or nothing about the benefits of the behavior. Again, we theorize that the combined effect of possessing more social capital in the form of well-educated alters and being in networks with a greater amount of (beneficial) normative influence about a new health hazard will result in more beneficial health decisions.
2.2. H1N1 Influenza Vaccination Among Pregnant Women
Using H1N1 influenza vaccination among pregnant women as an empirical example of a medical advance (i.e., in response to the risks of H1N1 prenatal infection), we conceptualize network member’s resources as the proportion of their network with a higher level of educational attainment. We then examine whether the flow of information and social influence from networks with a higher proportion of well-educated alters mediate the relationship between women’s educational attainment and vaccination decisions. The 2009 H1N1 influenza pandemic emerged in Mexico in the spring, garnering significant media attention. Clinicians quickly identified pregnant women to be particularly vulnerable to respiratory complications induced by infection (MMWR 2009). In the U.S., between April and August 2009, there were 788 confirmed cases of H1N1 among pregnant women. Half of these women were hospitalized, 115 were treated in intensive care units, and 30 died (Siston et al., 2010). When the H1N1 vaccine became available in November 2009, pregnant women were placed on the priority list to receive it because they were at high risk of adverse maternal and neonatal outcomes if infected (CDC, 2011).
This example offers a number of benefits. First, the relatively swift spread of the H1N1 pandemic resulted in the H1N1 vaccine being available during a concentrated period of time, making it a unique opportunity to observe how people react to a new health hazard. Second, pregnant women were placed on the priority list to receive the new H1N1 vaccine when it became available. Third, the women who are the focus of this study had access to prenatal care and insurance to pay for the vaccine, helping to rule these out as barriers to vaccination.1 Fourth, women were frequently embedded within networks through which they received advice and opinions about their prenatal behaviors. Finally, participants in this study were pregnant for the first time, meaning that their decisions would not be influenced by prior pregnancies. These benefits allow us to hold constant many potential barriers to vaccination, and prior decision-making about prenatal health behaviors, and focus on the ways that education and social capital as network members’ resources operate to influence vaccination behavior.
2.3. Hypotheses: The Role of Social Networks on Decision Making about a Medical Advance
Our innovative example and data allow us to test specific processes through which social networks operate when people make a decision about a medical advance. We begin by testing a series of hypotheses. Given that socioeconomic inequalities are a fundamental cause of health inequalities (Link and Phelan 1995), we anticipate a similar association between personal education and vaccination behavior. As described, educational attainment affords an array of flexible resources, enhancing learned effectiveness, health literacy, and health consciousness. We expect that the availability of the H1N1 vaccine prompted an educational gradient in H1N1 vaccination.
Hypothesis 1: Compared to those who did not complete college, women will have a higher probability of being vaccinated if they completed a college degree.
Next, we test whether personal education operates indirectly through social capital, by providing information and exerting influence from well-educated alters. Personal socioeconomic status, in this case educational attainment, can be converted into social capital through three pathways (Bourdieu [1983] 1986; Lin 2001; Song 2010; Song et al. 2017). These pathways help explain how social capital mediates the relationship between personal education and decisions about vaccinations. First, possessing a college degree affords women more opportunities to interact with others who also possess a college degree; a higher socioeconomic status allows for more structural opportunities for these types of encounters. Along these lines, college-educated women will be more able to engage in social networking, again resulting in more opportunities to interact with college-educated alters. Finally, due to homophily, college-educated women will be more likely to socialize with other similarly educated alters.
We propose two hypotheses to test whether social capital mediates the association between personal education and vaccination behavior.
Hypothesis 2: The proportion of college-educated H1N1 discussants in personal networks will mediate the relationship between personal education and H1N1 vaccination.
Hypothesis 3: The proportion of college-educated H1N1 supporters in personal networks will mediate the relationship between personal education and H1N1 vaccination.
Specifically, we expect that having a higher proportion of college-educated alters in their personal networks will lead to a greater amount of (accurate) information about the substantial risks associated with H1N1 infection during pregnancy. This will be due, in part, to the fact that women with college degrees are better able to mobilize their social ties, who possess diverse resources, when they need to make a health decision. Likewise, we expect that having a higher proportion of college-educated alters in their personal networks will influence them to receive the vaccine because well-educated alters understand the substantial risks of H1N1 infection during pregnancy. For instance, a woman’s sister—who is a physician—might warn her that the H1N1 vaccine is particularly important for pregnant women, influencing her to be vaccinated. Of note, building upon prior work on social capital and social influence, this study offers a unique empirical test of the way that the network resources available to people is associated with an important health decision. In this way, it offers important theoretical insights about the ways that network processes contribute to socioeconomic inequalities in health. In the sections that follow we describe our data and analytic approach.
3. Data and Methods
3.1. Research Design
Health Information and Behaviors during Pregnancy Study.
The Health Information and Behaviors during Pregnancy Study (HIBPS) is an original study designed to assess prenatal health behaviors among prima gravida women (women who are pregnant with their first child); it combines a quantitative component and two qualitative components (not included in this analysis). Women were sequentially enrolled from four health clinics in one of two large, urban Midwestern cities over the course of thirteen months, yielding a final sample size of 225, and 1,290 social network ties. Enrollment began the month that the H1N1 influenza vaccine became available to pregnant women (November 2009). Participants were included if they were over the age of 18, prima gravida, under 27 weeks pregnant, and spoke English, regardless of whether their pregnancy was planned or not.2 During their pregnancies, they followed the standard prenatal protocol for care, which included an initial nurse intake visit and follow-up visits, of increasing frequency, with an obstetrician or midwife.
Women completed a 20-minute survey interview, the HIBPS questionnaire, which included questions from the Behavioral Risk Factor Surveillance System (BRFSS; CDC, 2009), the Pregnancy Risk Assessment Monitoring System (PRAMS; Gilbert et al., 1999), the National Health Interview Survey (NHIS; National Center for Health Statistics, 2009), and the Kenya Diffusion and Ideational Change Project female questionnaire (KDICP; Kohler et al., 2001). Three obstetricians and obstetrics residents reviewed the questionnaire prior to collecting data, and it was pre-tested on 30 women from the clinics. Approximately 68 percent of eligible women agreed to participate and most were interviewed in-person by a trained survey interviewer, although they were also given the option to complete the interview over the phone. These modes ensured more reliable social network data compared to a written survey.3
3.2. Measures
H1N1 Vaccination.
The CDC, the American Medical Association, and the American Congress of Obstetricians and Gynecologists all uniformly recommended that pregnant women receive the H1N1 influenza vaccine during the 2009-2010 and the 2010-2011 flu seasons (ACOG 2010). For the duration of the HIBPS data collection, pregnant women were strongly encouraged by all of their health care providers to receive the H1N1 influenza vaccine, and were assured that the H1N1 vaccine safety level was equivalent to the annual influenza vaccine. The HIBPS questionnaire included a modified question from the 2009 NHIS, which asks about influenza vaccination: “Have you had the H1N1 or ‘swine’ flu shot? This shot protects against the H1N1 or “swine” flu.” We coded vaccinations dichotomously (vaccinated = 1; not vaccinated = 0).
Education.
The HIBPS measure of education level is based on a question from the 2009 NHIS, coded as a dichotomous measure: less than a bachelor’s degree (i.e., less than a high school degree, General Educational Development test, high school degree, Associate’s degree or some college) and Bachelor’s degree or higher (i.e., master’s degree, professional degree or doctoral degree).4
Network Measures.
The HIBPS questionnaire included a modified name generator and name interpreters (Knoke and Yang, 2008; Perry, Pescosolido, and Borgatti 2018), which we use to create network measures. The name generator prompted respondents to list their egocentric social network—specifically, their pregnancy discussion networks. Questions were adapted from the Kenya Diffusion and Ideational Change Project (Kohler et al. 2001), which aims to examine the role of social networks in changing attitudes related to family planning in Kenya. Women were asked, “[w]ho do you talk to about your pregnancy?5 When listing alters—members of their pregnancy discussion networks—all women were asked twice if there was “anyone else,” and they were able to list up to 20 alters. Women then answered a series of questions (name interpreters) for each alter they listed, of which we focus on three: (1) “[w]hat is___’s education level?” (1 = less than high school, 2 = high school graduate, 3 = some college, 4 = college graduate, 5 = graduate or professional degree); (2) “[h]ave you had any discussions with___ about getting the H1N1 flu shot during your pregnancy?” (yes, no); and (3) “[d]o you think this person agrees with receiving the H1N1 flu shot during pregnancy? (agrees, disagrees, don’t know).”
We then constructed measures to test our hypotheses. Using (1) and (2) above, we calculated the proportion of women’s H1N1 networks that were college educated H1N1 discussants (Hypothesis 2).
We used (1) and (3) to calculate the proportion of their entire network that was both college educated and H1N1 supporters (Hypothesis 3).
For each, sensitivity analysis using categorical variables divided into quartiles revealed substantively identical results.
There are two important caveats. First, there were two types of missing data. Women did not have full information for every alter (within-network missing data). Out of 225 women, 13 were unsure about the educational attainment of one of their alters (i.e., 13 alters out of 1,290 included in the analysis). Women were less certain about their alters’ opinions about being vaccinated during pregnancy: 70 percent were missing data for at least one alter. This within network missing data was set to missing prior to generating all network-level variables. Excluding within-network data may bias the results if there were systematic differences between the alters included or excluded in the network percent totals; thus, women may not have an accurate representation of the opinions of those in their entire network. Yet, in-depth interviews with a stratified random subset of 39 respondents revealed that their perceptions of their alters’ opinions were most salient, and they rarely speculated about their alters’ opinions. What mattered for women was their perception of the opinions of their partners, friends, relatives, and health care providers. Additionally, 34 women did not know any of their alters’ opinions about being vaccinated during pregnancy. A chi-square test revealed that the women who did not know whether any of their alters agreed or disagreed about H1N1 vaccination did not significantly vary by education level (p = 0.56).
Second, similar women may have a higher propinquity due to any number of social, cultural, or educational factors (Haas, 2010).6 Using a name generator requires that women select a specific pregnancy social network—people with whom they discuss their pregnancy. Thus, the HIBPS data are not designed to isolate the selection processes that may influence health behaviors. Rather, the results presented here represent the association of specific social network processes with vaccination behaviors net of pregnancy network selection processes.
Control Variables.
We control for age and race/ethnicity (1 = white non-Hispanic; 0 = other/minority). Although women were under 27 weeks pregnant when they participated in the HIBPS survey interview, and 65 percent were under 20 weeks pregnant, we include a measure accounting for the number of weeks pregnant the woman was at the time of the survey for the HIBPS analysis. We also control for network size.
3.3. Analytic Strategy
The hypothesized pathways were estimated using a Bayesian structural equation modeling (BSEM) approach. Bayes is a full-information estimator that minimizes sample loss and bias due to multivariate missingness by using all available data. Like comparable estimators (e.g., FIML), it generates unbiased parameter estimates and standard errors when variables are missing at random (MAR or MCAR; Asparouhov and Muthén, 2010a, 2010b). Moreover, compared to commonly used frequentist estimators that rely on large-sample theory (e.g., ML or WLSMV), Bayesian estimation is more computationally efficient and often offers better performance with small samples and when missing data are present (Asparouhov and Muthén 2010a; Muthén and Asparouhov 2012). All models were estimated using default (aka “non-informative”) priors specified in Mplus 7.4. The default priors are designed to minimize the effects of the prior distribution on posterior estimates while maximizing model convergence, which permits complex modeling while producing likelihood-driven results that are comparable to those generated by frequentist alternatives (see Asparouhov and Muthén 2010a, 2010b).7
The analysis proceeded with three separate BSEM models corresponding to each of the three study hypotheses. The first model regressed H1N1 vaccination on education and exogenous control variables to assess whether there was an educational gradient in H1N1 vaccination. The second and third models, respectively, regressed H1N1 vaccination on education, controls, and one of the two network mechanisms (Model 2: proportion college-educated H1N1 discussants; Model 3: proportion college-educated H1N1 supporters). These models also simultaneously regressed the respective network mechanism on education and controls, which permitted formal tests of mediation hypotheses.
Distal outcome models predicting H1N1 vaccination were modeled using binary probit regression. Mediator-as-outcome models predicting network mechanisms (Models 2 and 3) were treated as continuous normal variables and modeled with linear regression. Indirect effects of education on H1N1 vaccination via network mechanisms were estimated using the conventional product-of-coefficients approach (see Hayes, 2013). The estimated path coefficients are conditioned on control variables; paths from control variables to each endogenous variable and covariances among exogenous covariates were included in the model but only summarized in figures and not included in tabled results. In general, results and discussion focus on the unstandardized probit estimates from portions of the BSEM models predicting H1N1 vaccination, with select estimates from these models transformed into the predicted probability metric to aid interpretation of results.
4. Results
4.1. Descriptive Statistics
In Table 1, we present descriptive statistics for each of these variables. About half (53.4 percent) of respondents were vaccinated (Table 1), which was comparable to the national rate (Ding 2011). Of note, respondents were more highly educated than the average pregnant woman: 40 percent completed a master’s, professional or doctoral degree. This distribution provides an opportunity to observe how social processes occur at the higher end of the educational distribution, among women with relatively high levels of social capital. As a point of reference, in 2010 approximately 35 percent of U.S. females ages 25-34, within one standard deviation of the mean age of HIBPS respondents, completed a college degree or higher; the average was slightly higher in the Midwestern state where the HIBPS took place, where approximately 43 percent of women completed college (U.S. Census, 2018). Women were about 30 years old, they tended to be non-Hispanic white (67.9 percent) and at the time of the survey interview they were about 19 weeks pregnant.
Table 1.
Education, Demographic, Social Relationship, and Behavioral Measures from the Health Information and Behaviors during Pregnancy Study (HIBPS)
| %/Mean | (SD) | |
|---|---|---|
| Vaccinations | ||
| Percent receiving H1N1 influenza vaccine | 53.4 | |
| Educational degree | ||
| Individual Educational Attainment | ||
| High school degree or less | 8.9 | |
| Some college or associate’s degree | 12.5 | |
| Bachelor’s degree | 38.8 | |
| Master’s degree | 24.1 | |
| Professional degree (MD, JD) | 5.8 | |
| Doctoral degree (PhD) | 9.8 | |
| Network Measures | ||
| Proportion of network… | ||
| …college-educated | 75.2 | |
| …H1N1 vaccine discussant | 33.8 | |
| …H1N1 vaccine supporter | 81.2 | |
| …college-educated and H1N1 vaccine discussant | 54.7 | |
| …college-educated and H1N1 vaccine supporter | 52.0 | |
| Network size | 5.7 | 3.4 |
| Demographic | ||
| Age | 29.9 | 5.3 |
| Percent of advanced maternal age women | 16.4 | |
| Race/Ethnicity | ||
| Non-Hispanic White | 67.6 | |
| Non-Hispanic Black | 5.4 | |
| Non-Hispanic Other | 21.5 | |
| Hispanic | 5.8 | |
| Number of weeks pregnant | 18.9 | 6.4 |
| 43 | ||
Note: N = 223 for all except age, advanced maternal age, and number of weeks pregnant (N = 221) and H1N1 vaccine supporter (N = 189). See text for more details about the social network measures.
With regard to women’s social networks, on average women listed 5.7 alters with whom they discussed their pregnancies (pregnancy discussion networks); two reported no alters, and only 13 percent listed 10 alters or more. To provide additional information, not listed in Table 1, women tended to report discussing their pregnancy with females (70 percent of their networks), family members (60 percent of their networks), friends (80 percent of their networks), and health care providers (40 percent of their networks; categories not mutually exclusive). Among alters listed, about 1 in 3 had a child in the past ten years or were currently expecting. The mean level of education within networks was 3.9 (standard deviation 0.7) on a 5 point scale (described above). Women discussed H1N1 with about 34 percent of their networks, and about 55 percent of their networks were college-educated H1N1 discussants. If they knew their alters’ opinions, on average women reported that 81.2 percent agreed with H1N1 vaccination during pregnancy. They reported that about 52 percent of their network was college-educated and supported H1N1 vaccination during pregnancy, on average.
4.2. Bivariate patterns
In Figures 1 and 2, we show the bivariate relationships between our social network measures and vaccination behavior. Both figures show a similar pattern: the higher the proportion of network members who are both college-educated and either H1N1 discussants or H1N1 vaccine supporters, the higher the proportion of respondents vaccinated. Among respondents reporting that none of their network was college-educated, nor had they discussed it with anyone, a greater proportion was not vaccinated (0.61). Conversely, among respondents reporting that 75-100% of their network was college-educated H1N1 discussants, a greater proportion (0.83) were vaccinated. The pattern is even clearer for the measure reflecting the proportion of college-educated H1N1 vaccine supporters in personal networks. If respondents reported that none of their network was college-educated, nor did anyone support H1N1 vaccination, a greater proportion of them were not vaccinated (0.81). This ratio was flipped among those whose networks were comprised solely of college-educated vaccine supporters, who nearly all received the vaccine (0.93).
Figure 1.
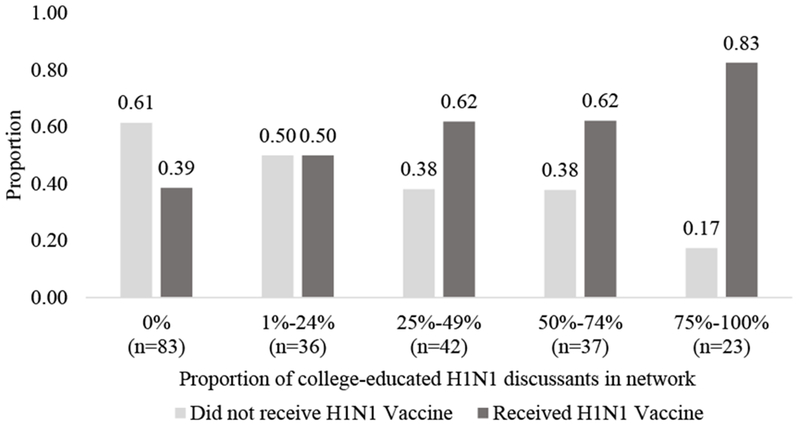
Bivariate Relationships between Social Capital/Information Flow and H1N1 Vaccination Decision
Figure 2.
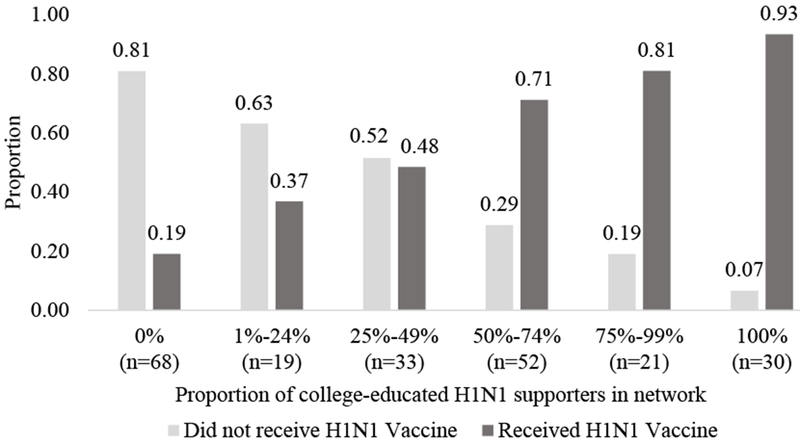
Bivariate Relationships between Social Capital/Normative Influence and H1N1 Vaccination Decision
4.3. Structural Equation Models
Model 1 (Educational Gradient).
The first panel in Table 2 presents path estimates from a model assessing whether there was an educational gradient in H1N1 vaccination decisions in this sample of prima gravida women, net of controls. Consistent with Hypothesis 1, results show college-educated respondents were more likely to report receiving the H1N1 vaccination. In the probit metric, college education is associated with a .48 increase (b=.48, p=.01, 95% CI [.09, .92]) in the z-score of the latent continuous variable representing the probability of H1N1 vaccination. However, the pseudo-R2 statistic indicates that only approximately 9% of the explainable variance in the underlying continuous latent vaccination variable was accounted for by education and controls (R2=.09, 95% CI [.02, .17]), suggesting the likely existence of other unobserved sources of heterogeneity in vaccination decisions.
Table 2.
Bayesian SEM Estimates of Relationships between Education, Network Mechanisms, and H1N1 Vaccination Decision
| Est. | [95% HDI] | (SD) | P-Value | (Pseudo)R2 | |
|---|---|---|---|---|---|
| Model 1: Hypothesis 1 | |||||
| education → vaccination | .48 | [.09, .92] | (.21) | .01* | .09 [.02, .17] |
| Model 2: Hypothesis 2 | |||||
| education → vaccination | .39 | [.02, .89] | (.25) | .02 * | .17 [.07, .29] |
| proportion of college-educated H1N1 discussants → vaccination | 1.04 | [.24, 1.63] | (.34) | .00 * | |
| education → proportion of college-educated H1N1 discussants | .11 | [.00, .21] | (.06) | .02 * | .11 [.05, .17] |
| education → proportion of college-educated H1N1 discussants → vaccination (indirect) | .10 | [.00, .27] | (.07) | .02 * | |
| Model 3: Hypothesis 3 | |||||
| education → vaccination | .23 | [−.27, .80] | (.29) | .20 | .45 [.29, .57] |
| proportion of college-educated H1N1 supporters → vaccination | 2.27 | [1.60, 2.83] | (.31) | .00 * | |
| education → proportion of college-educated H1N1 supporters | .16 | [.02, .27] | (.06) | .01 * | .09 [.04, .18] |
| education → proportion of college-educated H1N1 supporters → vaccination (indirect) | .35 | [.03, .66] | (.15) | .01 * |
NOTES: N = (maximum) 223. Table entries are probit estimates from Bayesian structural equation models specifying default priors in Mplus 7.4. “Est.” is the effect estimate, or the median of the Bayesian posterior probability density. 95% highest posterior density interval (HDI) is in brackets. “SD” is the posterior standard deviation of the estimate. “P-Value” is the one-sided Bayesian posterior probability, given the data and default priors, that the true effect is equal to zero or in the opposite direction than that observed.
Asterisk indicates 95% credible interval does not contain zero.
Rows with one arrow represent direct effect estimates; rows with multiple arrows represent indirect effect estimates. Paths from control variables (number of weeks pregnant, race/ethnicity, advanced maternal age, and network size) to endogenous variables and covariance among exogenous covariates are also estimated but not presented here. Each Bayes model matched the data well, with posterior predictive p-values ranging from .32 to .58 (PPP > .05 indicates good fit).
For a more intuitive interpretation of the magnitude of this association, we used the MODEL CONSTRAINT command in Mplus 7.4 to calculate discrete marginal effects (ME) of college education on the predicted probability of H1N1 vaccination at the mean or baseline values of exogenous covariates.8 According to Model 1, at covariate means/baselines, college education is associated with approximately a 19 percentage-point increase in the predicted probability of vaccination (ME=.19, p=.01, 95% CI [.02, .54]). This predicted difference is close in magnitude to the mean difference in vaccination rates observed across education groups in the data, as 37.0% of respondents without a college degree were reportedly vaccinated compared to 57.1% of respondents with a college degree (diff = 20.1).
Model 2 (Information Flow).
The second panel in Table 2 presents path estimates from a model assessing whether group differences in exposure to vaccine-related information from highly educated social network members mediate the educational gradient in H1N1 vaccination decisions. These estimates are also displayed in a path diagram in Figure 3. Consistent with Hypothesis 2, results show that the proportion of college-educated H1N1 discussants in participants’ personal networks mediates the association between education and H1N1 vaccination. In the probit metric, college education is predicted to indirectly increase the z-score of vaccination probability by .10 via the information flow network mechanism (b=10, p=.02, 95% CI [.00, .27]). However, these results also suggest college education is directly associated with a 0.39 increase in the z-score of vaccination probability, net of controls and the information flow network mechanism (b=.39, p=.02, 95% CI [.02, .89]). Overall, inclusion of this network mechanism into the model predicting H1N1 vaccination resulted in a modest increase in pseudo-R2, with education, controls, and information flow accounting for about 17% of the explainable variance in the underlying continuous latent vaccination variable (R2=.17, 95% CI [.07, .29]).
Figure 3.
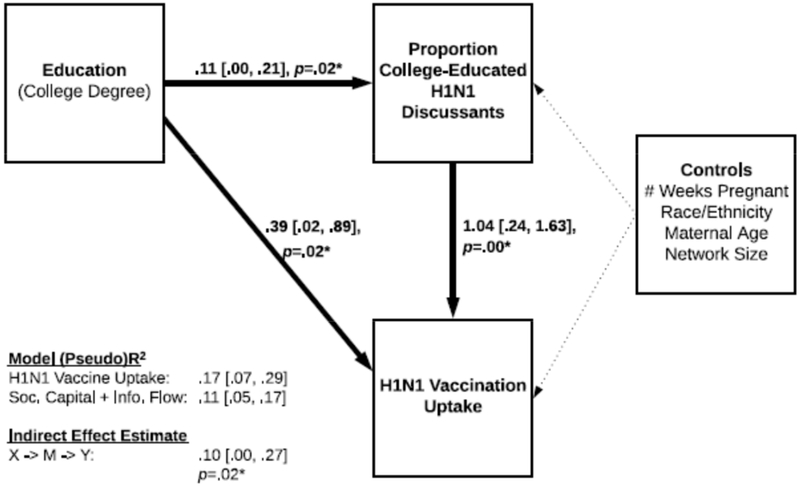
Relationships between Education, Social Capital and Information Flow, and Vaccination Decision (Model 2, Hypothesis 2)
Despite observing support for Hypothesis 2, an examination of the magnitude of the indirect and direct effects in Model 2 calls into question the extent to which the educational gradient in vaccination decisions is explained by differences in college educated and non-college educated respondent’s access to information from highly educated social network members. According to Model 2, at covariate means/baselines, college education is predicted to have a small discrete marginal indirect effect (MIE) via the proportion of college-educated H1N1 discussants network mechanism equating to approximately a three percentage-point increase in the predicted probability of vaccination (MIE=.03, p=.02, 95% CI [.00, .11]). In contrast, the discrete marginal direct effect (MDE) of college education at covariate means/baselines is notably larger, with college education directly accounting for about a 13 percentage-point increase in the predicted probability of vaccination (MDE=.13, p=.02, 95% CI [.00, .50]).
Model 3 (Normative Influence).
The relatively large direct effect, contrasted with the small indirect effect of education on vaccination observed in Model 2, suggests that there are other mechanisms beyond network information flow. It may be that health-related decisions are more responsive to the normative influence from educated alters. Hence, the third panel in Table 2 presents path estimates from a model assessing whether the educational gradient in H1N1 vaccination decisions reflects group differences in exposure to support for vaccination among highly educated alters. These estimates are also displayed in a path diagram in Figure 4.
Figure 4.
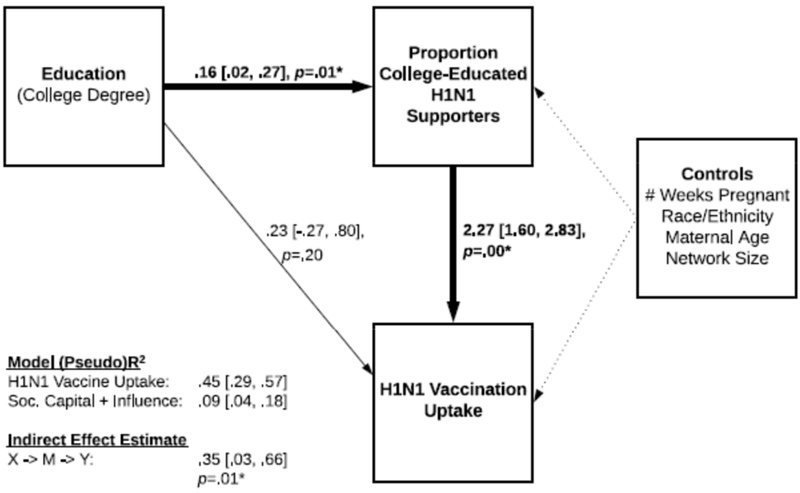
Relationships between Education, Social Capital and Normative Influence, and Vaccination Decision (Model 3, Hypothesis 3)
Consistent with Hypothesis 3, results from Model 3 show that the proportion of college educated H1N1 vaccine supporters in personal networks mediates the association between education and H1N1 vaccination. In the probit metric, college education is predicted to indirectly increase the z-score of vaccination probability by .35 via the normative influence network mechanism (b=.35, p=.01, 95% CI [.03, .66]). Inclusion of this network mechanism into the model predicting H1N1 vaccination resulted in a sizeable increase in pseudo-R2, with education, controls, and normative influence accounting for about 45% of the explainable variance in the underlying continuous latent vaccination variable (R2=.45, 95% CI [.29, .57]).
Still, based on results from Model 3, it is unclear whether education is directly associated with vaccination after accounting for network influence. Specifically, college education is associated with a 0.23 predicted increase in the z-score of the probability of vaccination net of controls and the normative influence network mechanism (b=.23, p=.20, 95% CI [−.27, .80]). However, the one-tailed p-value indicates a 20% chance that the true direct effect is zero or negative, which exceeds conventional statistical significance thresholds.
Examination of discrete marginal effects on predicted probabilities calculated from Model 3 provide additional clarity. First, the discrete marginal indirect effect of college education via the normative influence network mechanism at covariate means/baselines is equivalent to an approximately eight percentage-point increase in the predicted probability of vaccination (MIE=.08, p=.01, 95% CI [.00, .33]). In contrast, the discrete marginal direct effect of college education at covariate means/baselines is smaller, with college education directly accounting for about a five percentage-point increase in the predicted probability of vaccination (MDE=.05, p=.20, 95% CI [−.05, .36]). While this estimate does not surpass conventional alpha thresholds for statistical significance, a small sample size results in low statistical power and low precision, as indicated by wide credibility intervals. Taken together, these results suggest the education-vaccination association is substantially (if not wholly) mediated by the normative influence network mechanism.
Sensitivity Analysis.
Finally, we conducted sensitivity analyses to assess the consequences of alternative coding decisions for our social capital and information flow/normative influence measures. In the Appendix A, we show results when we modeled the proportion of respondents’ networks that (1) had a college degree (i.e., social capital as network members resources), (2) with whom they discussed the H1N1 vaccine (i.e., information flow), and (3) supported H1N1 vaccinations during pregnancy (i.e., normative influence). In Model A, we show how personal education indirectly increased the z-score of vaccination probability by .25 via (1) (b=.25, p=.01, 95% CI [.02, .53]) and directly increased the z-score by .29 (b=.29, p=.12, 95% CI [−.26, .83]). The next two models replicate this with the network measures (2) and (3). In contrast to Model A, Models B and C reveal that respondent education indirectly increased the z-score of vaccination probability by .01 (b=.01, p=.42, 95% CI [−.11, .11]) and .04 (b=.04, p=.36, 95% CI [−.26, .29]) for the measures of network discussion and normative influence, respectively. Models B and C also show respondent education directly increased the z-score of vaccination probability by .50 (b=.50, p=.02, 95% CI [.01, 1.02]) and .56 (b=.56, p=.02, 95% CI [.04, 1.18]) net of network discussion and normative influence, respectively.
Based upon existing theoretical frameworks of social capital and health (Lin 2001; Song 2011; Song et al. 2017), we include a full model with measures of social capital and its mechanisms in Appendix B. Specifically, we test whether (1) the proportion of H1N1 discussants in respondent’s networks (i.e., information flow), and (2) the proportion of H1N1 supporters in respondent’s networks (i.e., normative influence) further mediate the effect of social capital.
Consistent with patterns reported above, we find that the association between respondent’s education and vaccination decisions is mediated by the proportion of respondents’ networks that had a college degree. However, this association appears direct rather than indirect. To explain, respondents with higher education and more educated networks were more likely to choose H1N1 vaccination, but seemingly not due to differences in network information flow or normative support for vaccination. Moreover, despite finding support for an indirect pathway linking education to vaccination via the proportion of network college-educated, the proportion of college-educated supporters once again emerged as the strongest predictor of vaccination decisions.
Results using these alternative measures of network mechanisms are presented for transparency purposes. In the following discussion, we focus on results from models employing our preferred measures, which combine network education with network discussion/influence processes. The preferred measures reflect our theoretical expectations that one’s educational attainment indirectly influences health decisions by simultaneously structuring the educational levels (i.e., social capital) of one’s network as well as the information flow and normative influences experienced within one’s network. Results seem to bear out these expectations, as the best-fitting model for explaining vaccination behavior is Model 3 of Table 2, which includes the combined network education and normative influence mechanism (pseudo-R2 = .45, 95% CI [.29, .57]).
There are two reasons why we do not use the results from our appendices as our primary analytic strategy. First, based upon supplementary analyses of our stratified random subset of survey respondents we found evidence that women were particularly swayed by highly educated alters who supported vaccination. Compared to those without a college-degree, women who had completed college described more conversations with highly educated vaccine supporters (e.g., a friend in health care who warned them to be vaccinated). Second, our data afford the relatively unique opportunity to examine whether alters were both college-educated and vaccine supporters. This allows us to isolate the exact individuals described in the in-depth interview analysis. Finally, in additional analyses (not shown) we found that the proportion of college-educated H1N1 alters who oppose the vaccine did not mediate the association between personal education and vaccination. This analysis provides further evidence that it is not solely the proportion of network college-educated that mediates the relationship between personal education and vaccination.
5. Discussion
Findings from a range of studies support the idea that medical advances generate socioeconomic inequalities in health (Link et al., 1998; Glied and Lleras-Muney, 2008; Miech, 2008; Chang and Lauderdale, 2009), underscoring the importance of marshaling individual flexible resources for health decisions. Although there is evidence to support the idea that the networks in which people are embedded play a role in generating these socioeconomic inequalities in health (Pampel et al., 2010; Freese and Lutfey, 2011; DiMaggio and Garip, 2012), the process is not entirely clear (Carpiano et al., 2008; Song et al., 2010), especially when making decisions about a new health hazard. Building on prior evidence that social capital as network members’ resources mediate the association between socioeconomic status and health (Moore et al. 2014; Song 2011; Song et al. 2017), we specifically address this gap asking: Do social network processes mediate socioeconomic (i.e., educational) inequalities in health decisions about a new health hazard? Based on social capital theory, we hypothesize that social capital mediates the relationship, facilitating the flow of information and exerting influence on health decisions.
Using H1N1 as an empirical example, we test these hypotheses empirically. As discussed, this example is ideal because (1) the pandemic created the opportunity to observe how people react to a new vaccine, (2) pregnant women were on the vaccine priority list, (3) women had access to prenatal care and insurance to pay for the vaccine, and (4) these women were embedded within networks that socially influenced their decisions. As anticipated in our first hypothesis, individual educational attainment was positively associated with H1N1 vaccination. Education, and the multitude of other benefits it affords, serves a type of flexible resource to be tapped in the face of health decisions and new health hazards.
In our next hypotheses, we examined whether the combined effect of being embedded in networks with more social capital (i.e., well-educated) and (1) more information flow about H1N1 vaccinations or (2) more support of prenatal H1N1 vaccinations (i.e., normative influence), would mediate this education-vaccination relationship. We theorized that possessing more social capital (i.e., well-educated networks) and being embedded in networks with a greater flow of information about a health hazard would be beneficial for health decisions. Indeed, we found that the proportion of college-educated H1N1 discussants partially mediated the education-vaccination relationship (Hypothesis 2). Likewise, we also hypothesized that the proportion of college-educated H1N1 supporters would represent an important mechanism. In contrast to our results for Hypothesis 2, the proportion of college-educated H1N1 supporters substantially, if not entirely, mediated the relationship between education and H1N1 vaccination (Hypothesis 3). Moreover, including the social capital and normative influence network measure improved the model fit statistics considerably compared to prior models.
In addition to their own resources, being connected to other well-educated supporters may offer a host of additional resources that shape their likelihood of adopting this new medical advance. Put simply, our findings reveal that well-educated women tend to have well-educated alters who support the use of a new vaccine against a pandemic. It may be that having more educated alters leads to more active searches for health information (or more alter directed conversations), which may partly explain educational differences in vaccination behavior. Ultimately, though, normative influence from well-educated alters is the stronger mechanism since it more substantially (if not wholly) mediates the influence of individual educational attainment on vaccination behavior. In this way, well-educated alters may directly influence vaccination uptake by encouraging the use of vaccines. They may also indirectly affect vaccination behavior, as embeddedness in a network of well-educated vaccine supporters might normalize and promote the acceptability of the vaccine. Importantly, if we solely focus on individuals’ own education, we miss important network mechanisms that help explain why more educated women decide to receive vaccinations than do their less educated counterparts.
5.1. Theoretical Implications, Limitations, and Opportunities for Future Research
How do these findings contribute to our understanding of the mechanisms generating socioeconomic inequalities in health? Using a carefully designed study, our example extends our current theoretical perspective on the way socioeconomic status operates through social capital to generate health inequalities. These findings speak to a range of literatures from fundamental cause theory to the effect of social capital on health. We describe three theoretical contributions that emerge from this study. First, we offer an example demonstrating that social capital mediates the relationship between individual educational attainment and vaccination behavior. These findings align with prior work that social capital is one mechanism through which socioeconomic inequalities generate unequal health (Moore et al. 2014; Song 2011; Song et al. 2017). Second, building on prior social capital theory (Lin 2001), we tested two hypothesized mechanisms through which educational attainment is associated with a health behavior: information flow and social influence. Our evidence points to the latter mechanism, specifically influence from well-educated alters, as a particularly important determinant of H1N1 vaccination. As described, this matches evidence from qualitative interviews, in which women described trusting the advice of well-educated family members who were in the health care field, for example.
Finally, our study design and empirical example afford us the opportunity to isolate these processes when people react a new health hazard – the H1N1 pandemic. Building on prior evidence that information about new health hazards prompts the emergence of socioeconomic inequalities in health (Gortmaker and Wise, 1997; Link et al., 1998; Frisbie et al., 2004; Lichtenberg and Lleras-Muney, 2005; Glied and Lleras-Muney, 2008; Chang and Lauderdale, 2009; Price and Simon, 2009; Polonijo and Carpiano, 2013; Yang et al., 2014), these findings yield new insights about the role of social networks in the face of a new health hazard. Under these circumstances, people rely on more than their own resources when responding to a new health hazard – their decisions are also shaped by the social capital at their disposal. This finding sheds light on the ways that social capital as network members’ resources contribute to socioeconomic inequalities in health, and, importantly, illustrates ways that embedded network resources contribute to producing (or reproducing) unequal health. Two other advantages of this study are noteworthy. Due to the study design, we were able to isolate decisions about a new health behavior among women pregnant for the first time and we were able to hold access to health care constant.
Beyond our specific empirical example, it is likely that networks operate similarly when people face other health hazards and have new tools at their disposal following medical advances. That is, networks may represent a key impetus for the adoption of health behaviors based on medical advances among educated, affluent people (Valente 1998) and, likewise, may be a salient factor in perpetuating socioeconomic inequalities in health. Moreover, our findings resonate with prior work suggesting that health decisions rarely occur in isolation (Perry and Pescosolido, 2015; Pescosolido, 1992), and they suggest that social networks play a key role in helping people manage the uncertainty of health information based on newly discovered health hazards.
Although the current study provides a unique perspective of the role of social networks in contributing to educational differences in vaccinations, it is not without limitations. First, arguably, assessing the creation of a health inequality requires differences in morbidity and mortality outcomes. Although the current study does not directly assess H1N1 infection or morbidity among pregnant women, other evidence points to inequalities in morbidity. Doyle and colleagues (2013) found Floridian women with less education were more likely to contract H1N1. Nationally, among pregnant women who became infected, over 75 percent were admitted to the ICU, with many experiencing severe and sometimes fatal maternal and neonatal outcomes (CDC, 2011). In combination, these findings suggest the existence of educational inequalities in H1N1 outcomes.
Second, although most women were able to provide information about alters in their networks, they were unable to provide complete information for everyone. Nonetheless, the results remained robust across sensitivity analyses employing a variety of coding strategies to account for missing network data. Moreover, results from in-depth interviews confirmed that women focused on the information they had in hand, or even avoided discussing the vaccine with untrustworthy alters.
Future research examining how social networks prompt the emergence of educational inequalities in health behaviors following new medical advances might improve upon the present study in the following ways. First, data that include information about social position, social networks, health behaviors or outcomes are rare, particularly those related to a medical advance. In this light, using multiple methods, particularly ones that incorporate a qualitative approach that allows researchers to inquire directly about health decisions, provides a valuable perspective to understand how networks contribute to the ways social inequalities are generated and maintained. Triangulating interviews would further strengthen researchers’ capacity to understand network processes – for example, interviews with a partner (Moen and Hernandez, 2009) or health-care providers (Hernandez, 2013). Second, future research on the role of network mechanisms in socioeconomic inequalities in health need to account for the fact that people do not weigh influence from others equally. Asking respondents who influences their health decisions would be a valuable way to explore network mechanisms and the ripple effect they have across networks (Umberson and Montez, 2010). Third, in developing and testing a theoretical framework to understand how social connections can serve as a flexible resource, it is imperative to emphasize the negative consequences of social connections. Future research should draw from an array of research on the negative consequences of social ties for health behaviors (Umberson et al., 2010; Pampel et al., 2010) to understand how networks may impede healthy decisions, and how these processes may occur with differing frequency depending on educational attainment (or social position). Finally, future research should utilize available data to examine the flow of information and decisions about new medical advances (Valente 1998).
Ultimately, the findings presented here reinforce the notion that socioeconomically advantaged people disproportionately benefit from a wide array of resources, a process that is particularly visible after a medical advance. By testing the role of social capital and network processes, we elucidate one way that beneficial social connections serve as a flexible resource, in addition to individual educational attainment. As an empirical example of this process, this study pushes the boundaries of our understanding of the multitude of factors that are at play when people make health decisions and how those decisions accumulate to produce unequal health. Given the complexity of network processes, these findings invite further research on the processes that generate and perpetuate socioeconomic inequalities in health.
Highlights.
Personal and network resources afford unequal chances to avoid new health risks.
We examine whether social capital mediates the education-H1N1 vaccination link.
Personal education stratifies access to college-educated H1N1 supporters.
Knowing more college-educated vaccine supporters predicts vaccination.
Network processes contribute to producing, and reproducing, unequal health.
Acknowledgements
We are very grateful to John Robert Warren, Phyllis Moen, Bernice Pescosolido, Robert Hummer, David Knoke, Andrew Halpern-Manners, Mark Hayward, Michael Davern, Kathleen Call, Eric Grodsky, J. Michael Oakes, Jeylan Mortimer, Debra Umberson, Chris Uggen, Jeremy Freese, Brea Perry, Fabio Rojas, Ann McCranie, and Ross MacMillan for their assistance and feedback on various aspects of this research. We would also like to acknowledge Helen Ding and James A. Singleton at the Centers for Disease Control and Prevention. This study was supported by the Department of Sociology, the Graduate School Thesis Research Grant and the Children, Youth and Family Consortium at the University of Minnesota as well as the Foundation for Informed Medical Decision Making, the National Science Foundation, and the National Institute of Child Health and Human Development (grant 1 F32 HD070595-01). We are also indebted to Laura Cudzilo, Victoria Dutcher, Melissa Fousek, Molly Laney, Krista Reagan, Sarah Simpson, Jane van Dis and Remy Wong for their research assistance, advice about the medical accuracy of this study, and transcription as well as the anonymous staff at four health care clinics. However, errors and omissions are solely our responsibility.
Appendix A.
Associations between Network Mechanisms and H1N1 Vaccination Decision
| Est. | [95% HDI] | (SD) | P-Value | (Pseudo)R2 | |
|---|---|---|---|---|---|
| Supplementary Model A: Network Social Capital | |||||
| education → vaccination | .29 | [−.26, .83] | (.27) | .12 | .14 [.04, .25] |
| proportion of network college-educated → vaccination | .90 | [.07, 1.64] | (.40) | .01 * | |
| education → proportion of network college-educated | .29 | [.20, .37] | (.05) | .00 * | .27[.17, .37] |
| education → proportion of network college-educated → vaccination (indirect) | .25 | [.02, .53] | (.12) | .01 * | |
| Supplementary Model B: Network Discussants | |||||
| education → vaccination | .50 | [.01, 1.02] | (.27) | .02 * | .16[.06, .32] |
| proportion of network H1N1 discussant → vaccine | .83 | [.29, 1.32] | (.27) | .00 * | |
| education → proportion of network H1N1 discussant | .01 | [−.13, .12] | (.06) | .42 | .06 [.01, .12] |
| education → proportion of network H1N1 discussant → vaccination (indirect) | .01 | [−.11, .11] | (.06) | .42 | |
| Supplementary Model C: Network Influence | |||||
| education → vaccination | .56 | [.04, 1.18] | (.30) | .02 * | .43 [.27, .55] |
| proportion of network vaccine supporting → vaccination | 1.83 | [1.33,2.27] | (.26) | .00 * | |
| education → proportion of network vaccine supporting | .03 | [−.14, .15] | (.08) | .36 | .04 [.01, .09] |
| education → proportion of network vaccine supporting → vaccination (indirect) | .04 | [−.26, .29] | (.14) | .36 | |
NOTES: N = (maximum) 223. Table entries are probit estimates from Bayesian structural equation models specifying default priors in Mplus 7.4. “Est.” is the effect estimate, or the median of the Bayesian posterior probability density. 95% highest posterior density interval (HDI) is in brackets. “SD” is the posterior standard deviation of the estimate. “P-Value” is the one-sided Bayesian posterior probability, given the data and default priors, that the true effect is equal to zero or in the opposite direction than that observed.
Asterisk indicates 95% credible interval does not contain zero.
Rows with one arrow represent direct effect estimates; rows with multiple arrows represent indirect effect estimates. Paths from control variables {number of weeks pregnant, race/ethnicity, advanced maternal age, and network size) to endogenous variables and covariance among exogenous covariates are also estimated but not presented here. Each Bayes model matched the data well, with posterior predictive p-values ranging from .27 to .50 (PPP > .05 indicates good fit).
Appendix B.
Coefficients from MultipleSerial Mediation Models Predicting H1N1 Vaccination Decision
| Est. | [95% HDI] | (SD) | P-Value | (Pseudo)R2 | |
|---|---|---|---|---|---|
| Supplementary Serial Mediation Model 1: Network Discussants | |||||
| education → vaccination | .20 | [−.25, .77] | (.25) | .11 | .18 [.07, .28] |
| proportion of network college-educated (M1) → vaccination | .81 | [.04, 1.52] | (.40) | .01 * | |
| proportion of network H1N1 discussant (M2) → vaccination | .78 | [.28, 1.31] | (.27) | .00 * | |
| education → proportion of network H1N1 discussant (M2) | −.01 | [−.14, .14] | (.07) | .41 | .06 [.02, .14] |
| prop. college-educated (M1)→ proportion of network H1N1 discussant (M2) | .05 | [−.13, .25] | (.09) | .29 | |
| education → proportion of network college-educated (M1) | .29 | [.22, .36] | (.04) | .00 * | .27 [18, .35] |
| education → proportion of network college-educated (M1) → vaccination (indirect) | .22 | [.01, .46] | (.12) | .01 * | |
| education → proportion of network H1N1 discussant (M2) → vaccination (indirect) | −.01 | [−.13, .12] | (.06) | .41 | |
| education → prop. college-educated (M1) → prop. discussant (M2) → vaccination (indirect) | .01 | [−.03, .06] | (.02) | .11 | |
| Supplementary Serial Mediation Model 2: Network Influence | |||||
| education → vaccination | .22 | [−.20, .82] | (.26) | .11 | .44 [32, .53] |
| proportion of network college-educated (M1) → vaccination | .86 | [.00, 1.70] | (.43) | .02 * | |
| proportion of network vaccine supporting (M2) → vaccination | 1.82 | [1.41, 2.38] | (.23) | .00 * | |
| education → proportion of network vaccine supporting (M2) | −.01 | [−.17, .17] | (.09) | .44 | .04 [01, .10] |
| prop. college-educated (M1)→ proportion of network vaccine supporting (M2) | −.08 | [−.13, .33] | (.11) | .21 | |
| education → proportion of network college-educated (M1) | .29 | [.21, .36] | (.04) | .00 * | .27 [18, .35] |
| education → proportion of network college-educated (M1) → vaccination (indirect) | .23 | [.00, .48] | (.13) | .02 * | |
| education → proportion of network vaccine supporting (M2) → vaccination (indirect) | −.03 | [−.30, .32] | (.16) | .44 | |
| education → prop. college-educated (M1) → prop. supporting (M2) → vaccination (indirect) | .05 | [−.08, .19] | (.06) | .21 | |
NOTES: N = (maximum) 223. Table entries are probit estimates from Bayesian structural equation models specifying default priors in Mplus 7.4. “Est.” is the effect estimate, or the median of the Bayesian posterior probability density. 95% highest posterior density interval (HDI) is in brackets. “SD” is the posterior standard deviation of the estimate. “P-Value” is the one-sided Bayesian posterior probability, given the data and default priors, that the true effect is equal to zero or in the opposite direction than that observed.
Asterisk indicates 95% credible interval does not contain zero.
Rows with one arrow represent direct effect estimates; rows with multiple arrows represent indirect effect estimates. Paths from control variables (number of weeks pregnant, race/ethnicity, advanced maternal age, and network size) to endogenous variables and covariance among exogenous covariates are also estimated but not presented here. Each Bayes model matched the data well, with a posterior predictive p-value equal to .833 for both models (PPP > .05 indicates good fit).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
If women were uninsured when they became pregnant then they qualified for the state Medicaid program, which paid for prenatal care and the vaccine.
Women were enrolled up through their second trimester to include those who lacked access to care during their first trimester, and they also qualified if they had previously experienced an elected or spontaneous abortion (i.e., miscarriage).
85 percent completed the survey in-person and 15 percent completed it by phone.
Results were consistent after sensitivity analysis that included a linear specification of education. A minority of women may not have completed their schooling at the time of the survey, but results were consistent when excluding this small subset of women under age 22. Results were similar using a three category measure of education (i.e., graduate/professional degree, college degree, less than college degree), but we dichotomize the variable to maintain adequate cell sizes.
All women, except two, named at least one person in their pregnancy network. These two women were excluded from the analyses.
In-depth interview results with women and their health care providers, as well as 14 months of observation in clinic waiting rooms, indicate that the participants did not befriend each other at the health clinics.
A few interpretational differences between BSEM and classic SEM are noteworthy. First, BSEM point estimates (e.g., unstandardized regression coefficients) represent the median of the posterior distribution, which itself is a function of both the observed data and the default prior distribution. Second, BSEM credibility intervals have a more straightforward interpretation than classical confidence intervals: given the data and priors, there is a 95% probability that the true parameter falls within a reported credibility interval (aka, highest density interval or HDI). Third, the one-tailed posterior p-value in BSEM also has a more straightforward interpretation compared to a classic p-value: given the data and default priors, it is the probability that the true parameter is equal to zero or in the opposite-signed direction of the point estimate.
Contributor Information
Elaine M. Hernandez, Department of Sociology, Indiana University – Bloomington.
Erin Pullen, Indiana University Network Science Institute, Indiana University – Bloomington.
Jonathan Brauer, Department of Criminal Justice, Indiana University – Bloomington.
References
- American College of Obstetricians and Gynecologists (ACOG). 2010. “2009 H1N1 Influenza Virus and Seasonal Influenza Virus.” Retrieved January 5, 2010 (http://www.acog.org/).
- Asparouhov Tihomir and Muthén Bengt. (2010a). Bayesian analysis of latent variables using Mplus. Technical Report. Version 4. Available at: https://www.statmodel.com/download/BayesAdvantages18.pdf.
- Asparouhov Tihomir, and Muthén Bengt. (2010b). “Bayesian analysis using Mplus: Technical implementation.” Technical report. Version 3. Available at: http://www.statmodel2.com/download/Bayes3.pdf40.
- Bourdieu Pierre. 1986. “The Forms of Capital” in Richardson J (Ed) Handbook of Theory and Research for the Sociology of Education. Westport, CT: Greenwood, pp. 241–58. [Google Scholar]
- Carpiano Richard M. 2006. “Toward a neighborhood resource-based theory of social capital for health: Can Bourdieu and sociology help? Social Science & Medicine 62: 165–175. [DOI] [PubMed] [Google Scholar]
- Carpiano Richard M., Link Bruce G., and Phelan Jo C.. 2008. “Social Inequality and Health” in Conley A and Conley D (Eds) Social Class: How Does It Work? New York: Russell Sage Foundation. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). 2009. Behavioral Risk Factor Surveillance System Survey Data. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. [Google Scholar]
- Centers for Disease Control and Prevention (CDC). 2011. “Maternal and Infant Outcomes Among Severely Ill Pregnant and Postpartum Women with 2009 Pandemic Influenza A (H1N1)—United States, April 2009-August 2010.” Morbidity and Mortality Weekly Report 60:1193–1196. [PubMed] [Google Scholar]
- Chang Virginia W. and Lauderdale Diane S.. 2009. “Fundamental Cause Theory, Technological Innovation, and Health Disparities: The Case of Cholesterol in the Era of Statins.” Journal of Health and Social Behavior 50:245–260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Christakis Nicholas A. and Fowler James H.. 2008. The Collective Dynamics of Smoking in a Large Social Network. The New England Journal of Medicine 358:2249–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coleman James S. 1990. Foundations in Social Theory. Cambridge, MA: The Belknap Press of Harvard University Press. [Google Scholar]
- DiMaggio Paul and Garip Filiz. 2012. “Network Effects and Social Inequality.” Annual Review of Sociology 38:93–118. [Google Scholar]
- Doyle Timothy J., Goodin Kate, and Hamilton Janet J.. 2013. “Maternal and Neonatal Outcomes among Pregnant Women with 2009 Pandemic Influenza A(H1N1) Illness in Florida, 2009-2010: A Population-Based Cohort Study.” PLoS ONE 8:1–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Durkheim Emile. [1897] 1979. Suicide. New York: The Free Press. [Google Scholar]
- Elo Irma T. and Preston Samuel H.. 1996. “Educational Differentials in Mortality: United States, 1979-85.” Social Science & Medicine 42:47–57. [DOI] [PubMed] [Google Scholar]
- Feldman Jacob J., Makuc Diane M., Kleinman Joel C., and Cornoni-Huntley Joan. 1989. “National trends in educational differentials in mortality”. American Journal of Epidemiology 129: 919–933. [DOI] [PubMed] [Google Scholar]
- Parker Frisbie, W., Song, Seung-Eun E, Powers Daniel A., & Street Julie A. 2004. “The increasing racial disparity in infant mortality: Respiratory distress syndrome and other causes.” Demography 41: 773–800. [DOI] [PubMed] [Google Scholar]
- Freese Jeremy and Lutfey Karen. 2011. “Fundamental causality: challenges of an animating concept for medical sociology” In Handbook of the Sociology of Health, Illness and Healing: A Blueprint for the 21st Century, ed. Pescosolido BA, Martin JK, McLeod JD, Rogers A, pp. 67–81. New York: Springer. [Google Scholar]
- Freidson Eliot. 1960. “Client control and medical practice.” American Journal of Sociology 654, 374–382. [Google Scholar]
- Gilbert Brenda Colley, Shulman Holly B., Fischer Laurie A. and Rogers Mary M.. 1999. “The Pregnancy Risk Assessment Monitoring System (PRAMS): Methods and 1996 Response Rates from 11 States.” Maternal and Child Health Journal 3:199–209. [DOI] [PubMed] [Google Scholar]
- Glied Sherry and Adriana Lleras-Muney. 2008. “Technological Innovation and Inequality in Health.” Demography 45: 741–761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haas Steven. 2010. “Health and the Structure of Adolescent Social Networks.” Journal of Health and Social Behavior 51:424–439. [DOI] [PubMed] [Google Scholar]
- Hayes Andrew F. (2013). Introduction to mediation, moderation, and conditional process analysis. A regression-based approach. New York, NY: Guilford. [Google Scholar]
- Hernandez Elaine M. 2013. “Provider and Patient Influences on the Formation of Socioeconomic Health Behavior Disparities Among Pregnant Women.” Social Science & Medicine 82: 35–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- House James S., Landis Karl R. and Umberson Debra. 1988. “Social Relationships and Health.” Science 241:540–545. [DOI] [PubMed] [Google Scholar]
- House James S., Lepkowski James M., Kinney Ann M., Mero Richard P., Kessler Ronald C., and Herzog A. Regula. 1994. “The Social Stratification of Aging and Health.” Journal of Health and Social Behavior 35:213–234. [PubMed] [Google Scholar]
- Kitagawa Evelyn M. and Hauser Philip M.. 1973. Differential Mortality in the United States: A Study in Socioeconomic Epidemiology. Cambridge, Massachusetts: Harvard University Press. [Google Scholar]
- Knoke David and Yang Song. 2008. Social Network Analysis, Second Edition Thousand Oakes, CA: Sage Publications. [Google Scholar]
- Kohler Hans-Peter, Behrman Jere R., and Watkins Susan C.. 2001. “The Density of Social Networks and Fertility Decisions: Evidence From South Nyanza District, Kenya.” Demography 38:43–58. [DOI] [PubMed] [Google Scholar]
- Lichtenberg Frank and Adriana Lleras-Muney. 2005. “The effect of education on medical technology adoption: are the more educated more likely to use new drugs?” Annals d’Economie et Statistique 79/80:671–696. [Google Scholar]
- Lin Nan. 1999. “Social networks and status attainment.” Annual Review of Sociology 25:467–487. [Google Scholar]
- Lin Nan. 2001. Social Capital: A Theory of Social Structure and Action. Cambridge: Cambridge University Press. [Google Scholar]
- Lin Nan. 2017. “Building a Network Theory of Social Capital” Ch. 1 Pp. 3–28 in Social Capital: Theory and Research (Eds Nan Lin, Karen Cook, and Burt Ronald S.). Routledge, New York, NY. [Google Scholar]
- Link Bruce G., Northridge Mary E., Phelan Jo C., & Ganz Michael L.. 1998. “Social Epidemiology and the Fundamental Cause Concept: On the Structuring of Effective Cancer Screens by Socioeconomic Status.” The Milbank Quarterly 76:375–402 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Link Bruce G. and Phelan Jo C.. 1995. “Social Conditions as Fundamental Causes of Disease.” Journal of Health and Social Behavior 35:80–94. [PubMed] [Google Scholar]
- Link Bruce G. and Phelan Jo C. 2002. “McKeown and the Idea That Social Conditions Are Fundamental Causes of Disease.” American Journal of Public Health 92:730–732. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liu Ka-Yuet, King Marissa, and Bearman Peter S.. 2010. “Social Influence and the Autism Epidemic.” American Journal of Sociology 115:1387–1434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lin Nan. 2001. Social Capital: A Theory of Social Structure and Action. Cambridge: Cambridge University Press. [Google Scholar]
- Lutfey Karen and Freese Jeremy. 2005. “Toward some Fundamentals of Fundamental Causality: Socioeconomic Status and Health in the Routine Clinic Visit for Diabetes.” American Journal of Sociology 110:1326–1372. [Google Scholar]
- Miech Richard. 2008. “The Formation of a Socioeconomic Health Disparity: The Case of Cocaine Use during the 1980s and 1990s.” Journal of Health and Social Behavior 49: 352–366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mirowsky John and Ross Catherine. 2003. Education, Social Status, and Health. New Jersey: Aldine Transaction. [Google Scholar]
- Moen Phyllis, and Hernandez Elaine. 2009. “Social Convoys: Studying Linked Lives in Time, Context, and Motion” In The Craft of Life Course Research, edited by Elder G Jr and Giele J, pp. 258–279. New York: Guilford Press. [Google Scholar]
- Moore Spencer, Stewart Steven, and Teixeira Ana. 2014. “Decomposing social capital inequalities in health.” Journal of Epidemiology and Community Health 68(3): 233–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Morbidity and Mortality Weekly Report. 2009. “Outbreak of Swine-Origin Influenza A (H1N1) Virus Infection—Mexico, March-April 2009.” April 30, 2009: 58. [PubMed]
- Muthen Bengt and Asparouhov Tihomir. (2012). Bayesian structural equation modeling: A more flexible representation of substantive theory. Psychological Methods 17:313–335. [DOI] [PubMed] [Google Scholar]
- National Center for Health Statistics. 2009. Data File Documentation, National Health Interview Survey, 2009. National Center for Health Statistics, Centers for Disease Control and Prevention, Hyattsville, Maryland: 2009. [Google Scholar]
- Nutbeam Don. 2008. “The evolving concept of health literacy.” Social Science & Medicine 67:2072–2078. [DOI] [PubMed] [Google Scholar]
- Pampel Fred C., Krueger Patrick M. and Denney Justin T.. 2010. “Socioeconomic Disparities in Health Behaviors.” Annual Review of Sociology 36:349–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perry Brea and Pescosolido Bernice. 2015. “Social network activation: The role of health discussion partners in recovery from mental illness.” Social Science & Medicine 125:116–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perry Brea L., Pescosolido Bernice A., and Borgatti Steve. Egocentric Network Analysis: Foundations, Methods, and Models. New York, NY: Cambridge University Press. [Google Scholar]
- Pescosolido Bernice. 1992. “Beyond Rational Choice, the Social Dynamics of How People Seek Help.” American Journal of Sociology 97:1096–11383. [Google Scholar]
- Pescosolido Bernice, Gardner Carol Brooks, and Lubell Keri M.. 1998. “How people get into mental health services: Stories of choice, coercion, and ‘muddling through’ from ‘first timers’.” Social Science & Medicine 46: 275–286. [DOI] [PubMed] [Google Scholar]
- Phelan Jo C., Link Bruce G., Ana Diez-Roux Ichiro Kawachi, and Levin Bruce. 2004. “‘Fundamental Causes’ of Social Inequalities in Mortality: A Test of the Theory.” Journal of Health and Social Behavior 45:265–85. [DOI] [PubMed] [Google Scholar]
- Polonijo Andrea N. and Carpiano Richard M.. 2013. “Social inequalities in adolescent human papillomavirus (HPV) vaccination: A test of fundamental cause theory” Social Science & Medicine 82:115–125. [DOI] [PubMed] [Google Scholar]
- Price Joseph and Simon Kosali. 2009. “Patient Education and the Impact of New Medical Research.” Journal of Health Economics 28 :1166–1174. [DOI] [PubMed] [Google Scholar]
- Putnam Robert D. 2000. Bowling Alone : The Collapse and Revival of American Community. New York, NY: : Simon & Schuster. [Google Scholar]
- Siston Alicia M., Rasmussen Sonja A., Honein Margaret A.. 2010. “Pandemic 2009 Influenza A(H1N1) Virus Illness Among Pregnant Women in the United States.” JAMA 303:1517–1525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Song Lijun. 2011. “Social capital and psychological distress.” Journal of Health and Social Behavior 52(4): 478–492. [DOI] [PubMed] [Google Scholar]
- Song Lijun and Chang Tian-Yun. 2012. “Do resources of network members help in help seeking? Social capital and health information search.” Social Networks 34 : 658–669. [Google Scholar]
- Song Lijun, Pettis Philip J., and Piya Bhumika. 2017. “Does your body know who you know ? Multiple roles of network members’ socioeconomic status for body weight ratings.” Sociological Perspectives 60(6) : 997–1018. [Google Scholar]
- Song Lijun, Son Joonmo, and Lin Nan. 2010. “Social Capital and Health” in Cockerham William C. (Ed.) The New Companion to Medical Sociology. Malden, MA: John Wiley & Sons Ltd. [Google Scholar]
- Song Lijun, Frazier Cleothia, and Pettis Philip J.. 2018. “Do Network Members’ Resources Generate Health Inequality? Social Capital Theory and Beyond” Pp. 233–253 in Elgar Companion to Social Capital and Health, edited by Folland S and Nauenberg E. Cheltenham, UK: Edward Elgar Ltd. [Google Scholar]
- Umberson Debra, Crosnoe Robert and Reczek Corinne. 2010. “Social Relationships and Health Behavior Across the Life Course.” Annual Review of Sociology 36:139–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Umberson Debra and Jennifer Karas Montez. 2010. “Social Relationships and Health: A Flashpoint for Health Policy.” Journal of Health and Social Behavior 51(S):S54–S66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Census Bureau. 2018. American Community Survey, 2010 American Community Survey 1-Year Estimates (generated by Elaine Hernandez using American FactFinder). <http://factfinder2.census.gov> (August 9, 2018).
- Valente Thomas. 1996. “Social network thresholds in the diffusion of innovations. ” Social Networks 18:69–89. [Google Scholar]
- Yang Seungmi, Platt Robert W., Dahhou Mourad, and Kramer Michael S.. 2014. “Do Population-Based Interventions Widen or Narrow Socioeconomic Inequalities? The Case of Breastfeeding Promotion.” International Journal of Epidemiology 43: 1284–1292. [DOI] [PMC free article] [PubMed] [Google Scholar]